Embed Size (px)
Citation preview

8/3/2016
1
Clinical Significance of RBE
Variations in Proton Therapy
H. Paganetti PhD Professor, Harvard Medical School
Director of Physics Research, Massachusetts General Hospital, Radiation Oncology
• Prescriptions are based on dose (physics), not
outcome (biology; tumor control probability (TCP) or
normal tissue complication probability (NTCP))
• The dose in proton therapy is prescribed as
Gy(RBE); RBE is a dose modifying factor
• Proton therapy is using a generic RBE of 1.1
Introduction
Why RBE (relative biological effectiveness) ?
• The RBE is defined as the ratio of doses to reach the same
level of effect when comparing two modalities
Introduction
• RBE for TCP could potentially deduced from tumor control
data
• RBE for NTCP is difficult to assess based on clinical data
because photons generally deliver a more uniform dose to
critical structures and the probability of radiation damage for
a specified dose is sensitive to the volume of normal tissues
irradiated
• The majority of laboratory data are on RBE for cell survival
in vitro

8/3/2016
2
Cells with higher repair capacity (low α/β) show higher RBE
S(D) = e-(aD+bD2)
RBE for cell survival – Endpoint dependency
Carbon ions Photons
© M. Scholz, GSI
Uncertainties due to α/β
Carabe, España, Grassberger, Paganetti:
Phys Med Biol 2013 58: 2103-2117 McNamara, Schuemann, Paganetti:
Phys Med Biol 2015 60; 8399-8416
RBE for cell survival – Endpoint dependency
Inter-patient variability on cell survival RBE can be substantial
Liu, Ghosh, Magpayo, Testa, Tang, Biggs, Paganetti, Efstathiou, Lu, Held, Willers:
Int J Radiat Oncol Biol Phys 2015 91: 1081-1089
“Links Fanconi Anemia/BRCA pathway
defects to elevated proton RBE”
Grosse, Fontana, Hug, Lomax, Coray, Paganetti, Sartori, Pruschy:
Int J Radiat Oncol Biol Phys 2014 88: 175-181
“Repair kinetics in HR-deficient cells
were significantly delayed after proton
irradiation, with elevated amounts of
residual gH2AX foci”
RBE for cell survival – Endpoint dependency

8/3/2016
3
RBE relevant for NTCP: Effect of interest (organ level):
• early effects such as erythema
• late effects such as lung fibrosis, lung function, spinal cord
injury, or necrosis
Typically measured other than cell survival (cellular level):
• Double-strand break induction
• Foci formation
• Chromosome aberrations
• Micronuclei formation
• Cell cycle disruption …
RBE for cell survival – Endpoint dependency
0.001
0.01
0.1
1
0 1 2 3 4 5 6 7 8 Dose [Gy]
Cell
Su
rviv
al
g protons
S(D) = e-(aD+bD2
)
RBE L,dH , a b L
a b L 2
4 a b LRBEmax dH 4RBEmin
2 dH2 a b
L
2dH
RBE≈1.3
RBE≈1.6 2 4 6 8 10
0.8
0.9
1
1.1
1.2
1.3
1.4
1.5
Dose (Gy)
RB
E
(a/b)x = 1 Gy
Our Model
Carabe et al.
Wedenberg et al.
2 4 6 8 100.8
0.9
1
1.1
1.2
1.3
1.4
1.5
Dose (Gy)
RB
E
(a/b)x = 2 Gy
2 4 6 8 100.8
0.9
1
1.1
1.2
1.3
1.4
1.5
Dose (Gy)
RB
E
(a/b)x = 10 Gy
2 4 6 8 100.8
0.9
1
1.1
1.2
1.3
1.4
1.5
Dose (Gy)
RB
E
(a/b)x = 15 Gy
LETd = 2.5 keV/mm
McNamara, Schuemann, Paganetti:
Phys Med Biol 2015 60; 8399-8416
RBE for cell survival – Dose dependency
• Most experiments in vitro look at cell
survival
• Precise measurements of cell
survival below 2 Gy are sparse
• Prescription doses are typically
2Gy/fraction
• There are only a few data points
regarding dose dependency of RBE
in vivo below 4 Gy for protons
Aoki-Nakano et al. J Rad Res 2014
RBE for cell survival – Dose dependency

8/3/2016
4
M. K
räm
er e
t al
.:
Tec
hn.
Can
cer
Res
. T
reat
m.
2, 4
27
-43
6, 2
00
3
Photons Low-LET (Protons)
High-LET (12C)
Radiation is more effective when energy depositions are more concentrated in space
0 5 10 15 20
1
2
3
4
LETd (keV/mm)
RB
E
(a/b)x = 1.22 Gy
0 5 10 15 20
1
2
3
4
LETd (keV/mm)
RB
E
(a/b)x = 2 Gy Our model
Carabe et al.
Wedenberg et al.
Guan et al.
0 5 10 15 20
1
2
3
4
LETd (keV/mm)
RB
E
(a/b)x = 3 Gy
0 5 10 15 20
1
2
3
4
LETd (keV/mm)
RB
E
(a/b)x = 3.49 Gy
0 5 10 15 20
1
2
3
4
LETd (keV/mm)
RB
E
(a/b)x = 10 Gy
0 5 10 15 20
1
2
3
4
LETd (keV/mm)
RB
E
(a/b)x = 15 Gy
Dp = 2 Gy
McNamara, Schuemann, Paganetti:
Phys Med Biol 2015 60; 8399-8416
RBE for cell survival – LET dependency P
ag
anetti: P
hys
. M
ed
. B
iol. 1
998;
43,
2147-2
157
Implication of RBE(LET) for RBE(depth)
Dose = Fluence [1/cm2] × LET [keV/cm] / r [g/cm3]
1
1
2
2
3
3
RBE for cell survival – LET dependency
Entrance: ~1.1 Center: ~1.15 Distal edge: ~1.35 Distal fall-off: ~1.7 (values averaged over all cell lines and SOBPs for in vitro cell survival)
Healthy tissue
RBE for cell survival – LET dependency
Paganetti H: Phys Med Biol 2014 59: R419-R472
1.1 is a conservative estimate!

8/3/2016
5
Increased effectiveness as a function of depth
RBE might be higher close to the ‘target’ edge (mainly in OAR)
Average RBE across a typical SOBP is, on average, about 1.1
RBE depends on LET
RBE seems to be higher for tissues with a low a/b ratio (mainly OAR)
RBE values for endpoints other than cell survival are less well known.
The RBE for normal tissue response is unclear
RBE depends on a/b
RBE increases with decreasing dose
Indicates higher RBE for OAR
Measurements (in vitro and in vivo) typically do not provide high resolution below 2 Gy
RBE depends on dose
RBE for cell survival
Dose x 1.1
Gy(R
BE
)
54
5.4
keV
/μm
5
1 LET
Gy
(RB
E)
59.
4
5.4 Dose x RBE
Clinical evidence ?
Gy(R
BE
)
11
-11
Dose(RBE-weighted) – Dose (RBE=1.1)
Gia
nts
oud
i, S
eth
i, Y
eap
, E
ato
n,
Eb
b, C
aru
so, R
ap
alin
o, C
hen,
Ad
am
s, Y
ock,
Tarb
ell,
Pag
anetti, M
acD
onald
: In
t. J
. R
ad
iat. O
ncol. B
iol. P
hys
. 2016 9
6; 287-2
96
Note:
All 119 cases had similar LET distributions
Only 4 with symptomatic treatment change
Only 1 symptomatic change correlated with LET
Correlation of toxicity and LET
RBE increases with LET
LET is not the sole indicator
Clinical evidence ?
Gia
nts
oud
i, S
eth
i, Y
eap
, E
ato
n,
Eb
b, C
aru
so, R
ap
alin
o, C
hen,
Ad
am
s, Y
ock,
Tarb
ell,
Pag
anetti, M
acD
onald
: In
t. J
. R
ad
iat. O
ncol. B
iol. P
hys
. 2016 9
6; 287-2
96

8/3/2016
6
There is currently no clinical evidence for a correlation
between areas of elevated LET (RBE) and toxicities
Should we consider RBE for NTCP in treatment
planning?
Clinical evidence ?
Planning technique maximizing target conformality
Dose x 1.1 LET Dose x RBE
Gy
(RB
E)
50.4
2.52
keV
/μm
6
1
Gy
(RB
E)
55.4
2.52
Brainstem
Target
Brainstem
Target
Brainstem
Target
Giantsoudi, Adams, Kim, MacDonald, Paganetti: Int. J. Radiat. Oncol. Biol. Phys. 2016 under review
RBE considerations in treatment planning
Dose x 1.1 LET Dose x RBE
Gy
(RB
E
)
50.4
2.52
keV
/μm
6
1
Gy
(RB
E
)
55.4
2.52
Brainstem
Target
Brainstem
Target
Brainstem
Target
Planning technique minimizing maximum LET in the brainstem
RBE considerations in treatment planning
Giantsoudi, Adams, Kim, MacDonald, Paganetti: Int. J. Radiat. Oncol. Biol. Phys. 2016 under review

8/3/2016
7
!!
RBE = 1.1 stop
RBE = 1.1 through
RBE var. stop
RBE var. through
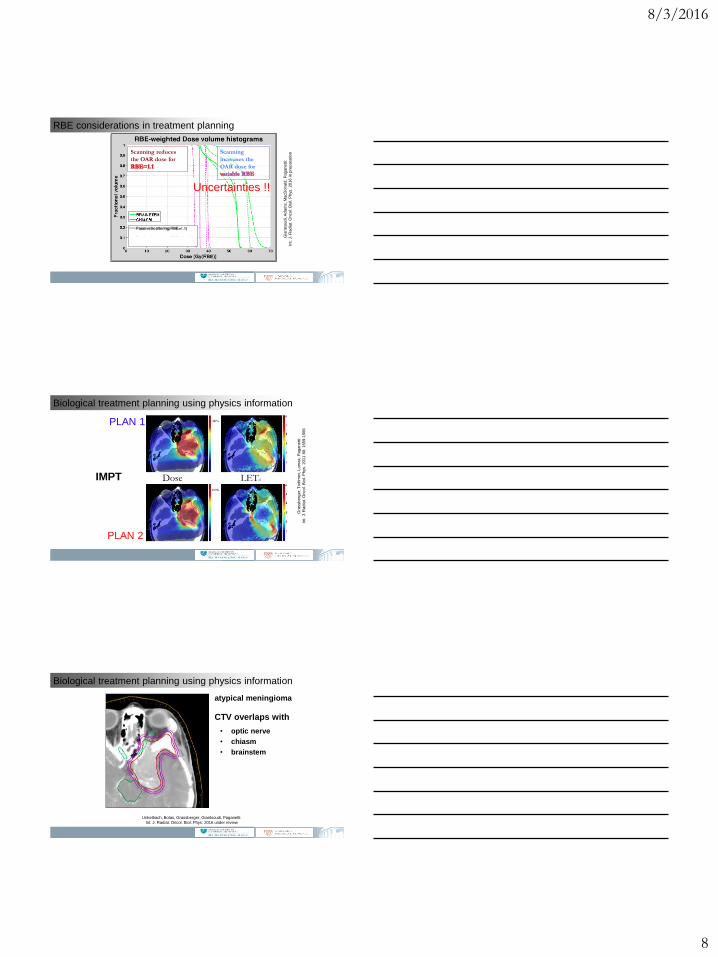
RBE considerations in treatment planning
Giantsoudi, Adams, Kim, MacDonald, Paganetti: Int. J. Radiat. Oncol. Biol. Phys. 2016 under review
Passive Scattering
Dose x RBE LET Dose x 1.1
Gy
(RB
E)
54
2.7
Pencil beam scanning
LET Dose x RBE Dose x 1.1
Gy
(RB
E)
54
2.7
RBE considerations in treatment planning
Gia
nts
oud
i, A
dam
s, M
acD
onald
, P
ag
anetti:
Int. J
. R
ad
iat. O
ncol. B
iol. P
hys
. 2016 in p
rep
ara
tion
CTV Brainstem Chiasm
Passive Scattering Beam Scanning
RBE considerations in treatment planning
Gia
nts
oud
i, A
dam
s, M
acD
onald
, P
ag
anetti:
Int. J
. R
ad
iat. O
ncol. B
iol. P
hys
. 2016 in p
rep
ara
tion
8/3/2016
8
Scanning reduces
the OAR dose for
Scanning
increases the
OAR dose for
RBE considerations in treatment planning
Gia
nts
oud
i, A
dam
s, M
acD
onald
, P
ag
anetti:
Int. J
. R
ad
iat. O
ncol. B
iol. P
hys
. 2016 in p
rep
ara
tion
Uncertainties !!
PLAN 2
Dose LETd
PLAN 1
IMPT
Gra
ssb
erg
er,
Tro
fim
ov, Lom
ax,
Pag
anetti:
Int. J
. R
ad
iat. O
ncol. B
iol. P
hys
. 2011 8
0: 1559-1
566
Biological treatment planning using physics information
atypical meningioma
CTV overlaps with
• optic nerve
• chiasm
• brainstem
Biological treatment planning using physics information
Unkelbach, Botas, Grassberger, Giantsoudi, Paganetti:
Int. J. Radiat. Oncol. Biol. Phys. 2016 under review
8/3/2016
9
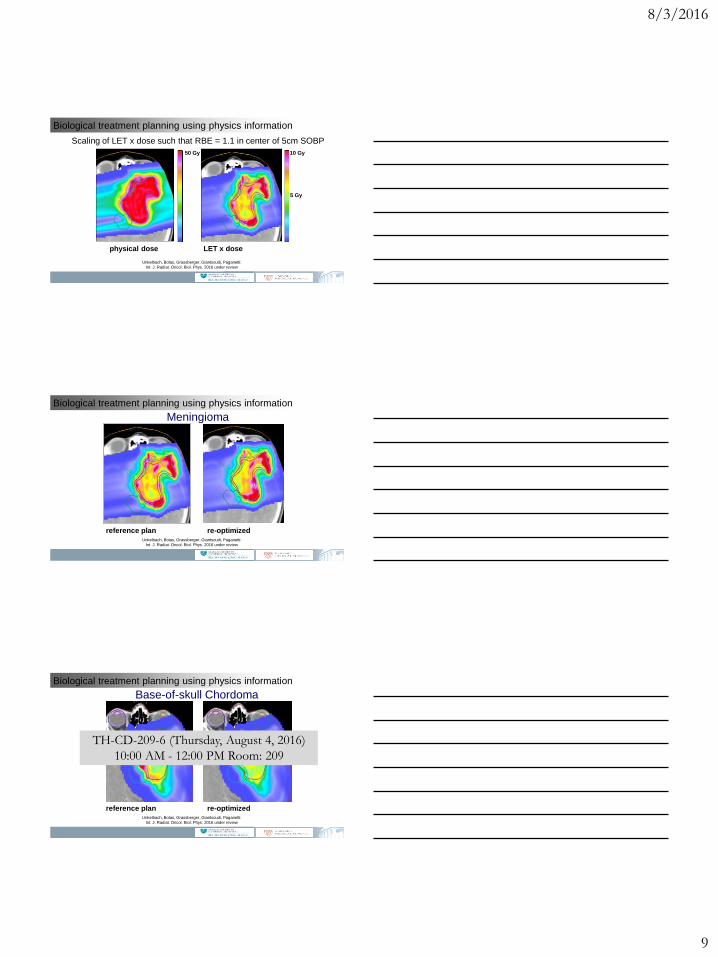
physical dose LET x dose
50 Gy 10 Gy
5 Gy
Scaling of LET x dose such that RBE = 1.1 in center of 5cm SOBP
Biological treatment planning using physics information
Unkelbach, Botas, Grassberger, Giantsoudi, Paganetti:
Int. J. Radiat. Oncol. Biol. Phys. 2016 under review
Meningioma
reference plan re-optimized
Biological treatment planning using physics information
Unkelbach, Botas, Grassberger, Giantsoudi, Paganetti:
Int. J. Radiat. Oncol. Biol. Phys. 2016 under review
Base-of-skull Chordoma
reference plan re-optimized
Biological treatment planning using physics information
Unkelbach, Botas, Grassberger, Giantsoudi, Paganetti:
Int. J. Radiat. Oncol. Biol. Phys. 2016 under review
TH-CD-209-6 (Thursday, August 4, 2016)
10:00 AM - 12:00 PM Room: 209
8/3/2016
10
SUMMARY
Proton therapy uses a generic RBE of 1.1 because of substantial
uncertainties in RBE as a function of dose, endpoint and LET
The RBE is potentially higher towards the distal end of an SOBP and for
low α/β.
The relevance of endpoints other than cell survival for defining clinical
RBEs is unclear.
For a given dose and organ, the RBE dependency on LET is monotone
(reasonably linear)
There is no evidence (yet) for a correlation between LET and toxicity or
recurrence
RBE/LET optimization may improve treatment outcome
Inter-patient variability (biomarkers?) is not well understood
MGH Radiation Oncology Monte Carlo and Biophysics Research Team
Aimee McNamara
Maria Marteinsdottir
Tracy Underwood
David Hall Stephen McMahon
Jan Schuemann Harald Paganetti
Drosoula Giantsoudi
Jan Unkelbach
Hakan Oesten
Clemens Grassberger
Changran Geng
Pablo Botas
Jungwook Shin