Embed Size (px)
Citation preview
10/26/2016
1
©2015 MFMER | slide-1
What is new in the new WHO Classification of lung cancer
And the impact on small biopsy diagnosis
Marie-Christine Aubry, M.D.
Mayo Clinic
©2015 MFMER | slide-2
Objectives
• Review the changes to lung cancer in the 2015 WHO classification
• Focus on the interpretation in small biopsies
©2015 MFMER | slide-3
2015 WHO Classification of Lung Cancer 4th Ed.
©2015 MFMER | slide-4
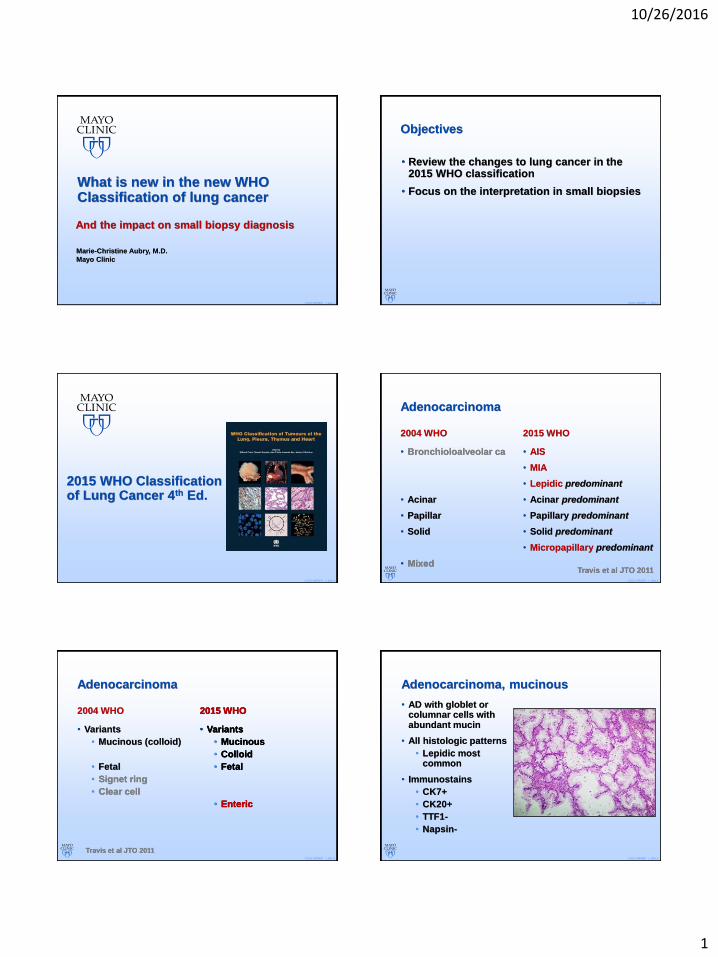
Adenocarcinoma
2004 WHO
• Bronchioloalveolar ca
• Acinar
• Papillar
• Solid
• Mixed
2015 WHO
• AIS
• MIA
• Lepidic predominant
• Acinar predominant
• Papillary predominant
• Solid predominant
• Micropapillary predominant
Travis et al JTO 2011
©2015 MFMER | slide-5
Adenocarcinoma
2004 WHO
• Variants
• Mucinous (colloid)
• Fetal
• Signet ring
• Clear cell
2015 WHO
• Variants
• Mucinous
• Colloid
• Fetal
• Enteric
Travis et al JTO 2011
2015 WHO
• Variants
• Mucinous
• Colloid
• Fetal
• Enteric
©2015 MFMER | slide-6
Adenocarcinoma, mucinous
• AD with globlet or columnar cells with abundant mucin
• All histologic patterns
• Lepidic most common
• Immunostains
• CK7+
• CK20+
• TTF1-
• Napsin-

10/26/2016
2
©2015 MFMER | slide-7
Adenocarcinoma, enteric subtype
• Resembles morphology of colorectal carcinomas
• Immunostains
• Should retain CK7
• CK20+
• CDX2+
• Issues
• Still could be 1ary GI, pancreaticobiliary
©2015 MFMER | slide-8
2015 WHO recommendation
• For non mucinous AD, assign most predominant growth pattern
• Grading scheme
• Grade 1= lepidic
• Grade 2= papillary and acinar
• Grade 3= solid and micropapillary
• Prognostic value
• Reproducibilty?
• 534 cases – 2 observers
• Exact match 51.7%
• 27.3% in same prognostic score
• 21% with different prognostic score
Percent surviv
al
0
20
40
60
80
100
Years
0 1 2 3 4 5
Figure 3a. Overall survival by observer 1 predominant score (mucinous in group 3).
Score 1 (n=124)Score 2 (n=263)Score 3 (n=147)
Perc
ent surv
ival
0
20
40
60
80
100
Years
0 1 2 3 4 5
Figure 4a. Overall survival by observer 2 predominant score (mucinous in group 3).
Score 1 (n=117)Score 2 (n=284)Score 3 (n=133)
Boland et al
©2015 MFMER | slide-9
AIS/MIA
• 3 cm and less
• No vascular, pleural invasion
• No airspace spread
• No necrosis
• Stromal invasion:
• Absent in AIS
• ≤ 5mm in MIA
• Predicts for 5-yr DFS of, or near 100%
©2015 MFMER | slide-10
AIS
©2015 MFMER | slide-11
MIA
Invasion 2mm
©2015 MFMER | slide-12
Lepidic predominant
• 3 cm and less
• >5mm of stromal invasion
• Pleural or vascular invasion
• Airspace spread
• Necrosis
• > 3cm
• Even if ≤ 5mm or no invasion

10/26/2016
3
©2015 MFMER | slide-13
LPA
Invasion > 5mm
©2015 MFMER | slide-14
Features of invasion
Papillary Micropapillary
©2015 MFMER | slide-15
Active fibroblasts/ Desmoplasia = Invasion
©2015 MFMER | slide-16
©2015 MFMER | slide-17
Interobserver variation
Rater 2
AIS MIA IA
Rater
1
AIS 11 (3.7%) 3 (1.0%) 0 ( 0.0%)
MIA 6 (2.0%) 71 (24.2%) 12 ( 4.1%)
IA 0 (0.0%) 36 (12.2%) 155 (52.7%)
Boland et al©2015 MFMER | slide-18
More than one area of invasion
• Several recommendations
• Measure the largest
• In the WHO section on MIA and LPA
• Estimate the % of invasive components
• X by the overall tumor diameter
10/26/2016
4
©2015 MFMER | slide-19
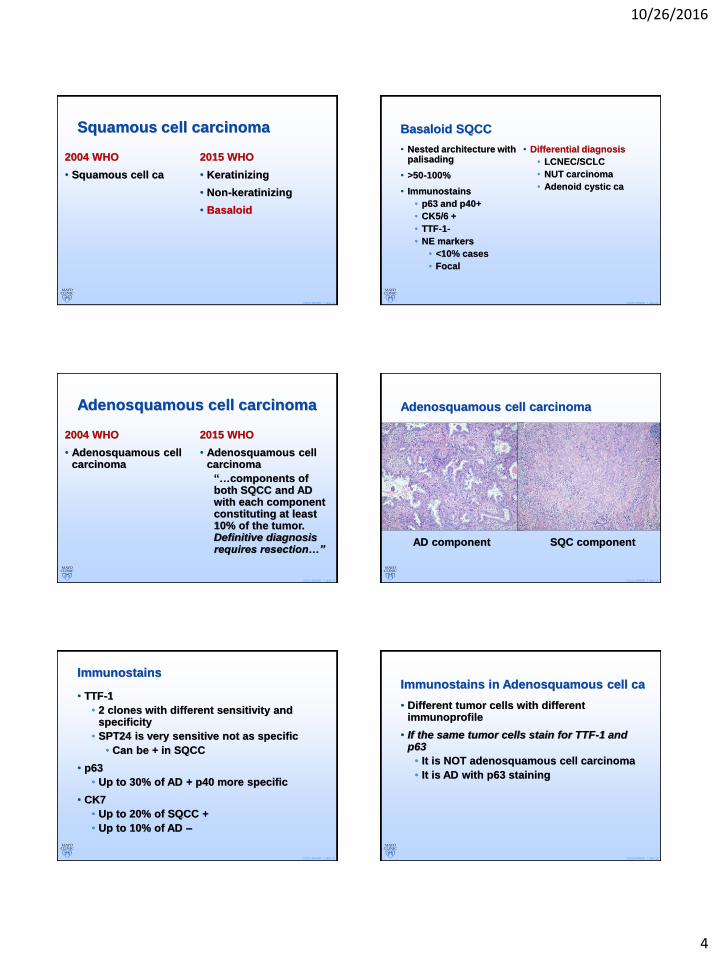
Squamous cell carcinoma
2004 WHO
• Squamous cell ca
2015 WHO
• Keratinizing
• Non-keratinizing
• Basaloid
©2015 MFMER | slide-20
Basaloid SQCC
• Nested architecture with palisading
• >50-100%
• Immunostains
• p63 and p40+
• CK5/6 +
• TTF-1-
• NE markers
• <10% cases
• Focal
• Differential diagnosis
• LCNEC/SCLC
• NUT carcinoma
• Adenoid cystic ca
©2015 MFMER | slide-21
Adenosquamous cell carcinoma
2004 WHO
• Adenosquamous cell carcinoma
2015 WHO
• Adenosquamous cell carcinoma
“…components of both SQCC and AD with each component constituting at least 10% of the tumor. Definitive diagnosis requires resection…”
©2015 MFMER | slide-22
Adenosquamous cell carcinoma
AD component SQC component
©2015 MFMER | slide-23
Immunostains
• TTF-1
• 2 clones with different sensitivity and specificity
• SPT24 is very sensitive not as specific
• Can be + in SQCC
• p63
• Up to 30% of AD + p40 more specific
• CK7
• Up to 20% of SQCC +
• Up to 10% of AD –
©2015 MFMER | slide-24
Immunostains in Adenosquamous cell ca
• Different tumor cells with different immunoprofile
• If the same tumor cells stain for TTF-1 and p63
• It is NOT adenosquamous cell carcinoma
• It is AD with p63 staining
10/26/2016
5
©2015 MFMER | slide-25
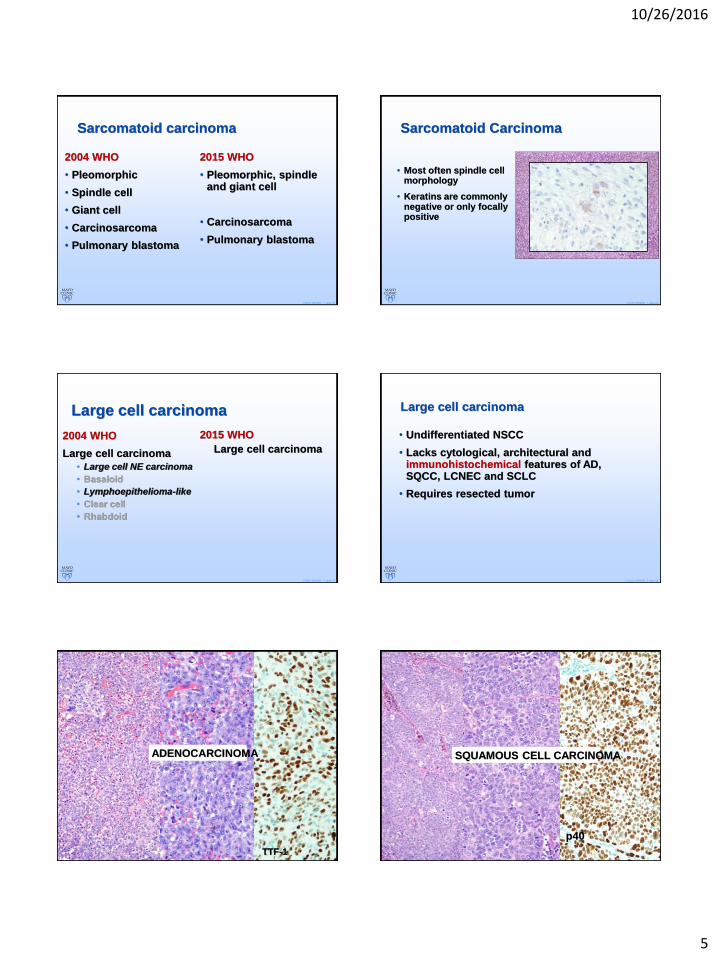
Sarcomatoid carcinoma
2004 WHO
• Pleomorphic
• Spindle cell
• Giant cell
• Carcinosarcoma
• Pulmonary blastoma
2015 WHO
• Pleomorphic, spindle and giant cell
• Carcinosarcoma
• Pulmonary blastoma
©2015 MFMER | slide-26
Sarcomatoid Carcinoma
• Most often spindle cell morphology
• Keratins are commonly negative or only focally positive
©2015 MFMER | slide-27
Large cell carcinoma
2004 WHO
Large cell carcinoma
• Large cell NE carcinoma
• Basaloid
• Lymphoepithelioma-like
• Clear cell
• Rhabdoid
2015 WHO
Large cell carcinoma
©2015 MFMER | slide-28
Large cell carcinoma
• Undifferentiated NSCC
• Lacks cytological, architectural and immunohistochemical features of AD, SQCC, LCNEC and SCLC
• Requires resected tumor
©2015 MFMER | slide-29
TTF-1
ADENOCARCINOMA
©2015 MFMER | slide-30
p40
SQUAMOUS CELL CARCINOMA

10/26/2016
6
©2015 MFMER | slide-31
LARGE CELL CARCINOMA
©2015 MFMER | slide-32
AD SQCC LCC
©2015 MFMER | slide-33
Neuroendocrine tumors
2004 WHO
• Small cell carcinoma
• Carcinoid tumors
• Typical
• Atypical
2015 WHO
Neuroendocrine tumors
• Small cell carcinoma
• Large cell NE carcinoma
• Carcinoid tumor
• Typical
• Atypical
©2015 MFMER | slide-34
Small cell carcinoma
• Still defined by H&E morphology
• About 10% of SCLC negative or focally weakly + for NE markers
• Up to 30% NSCLC + for NE markers
• IHC useful IF
• SCLC vs SQCC
• TTF-1+/p40-
• NOT p63 (20% +)
• SCLC vs carcinoid
• Ki-67
©2015 MFMER | slide-35
Large cell neuroendocrine carcinoma
• Neuroendocrine morphology
• Rosettes
• Trabecula
• Peripheral palisading
• Nucleoli prominent
• >10 mitosis/ HPF
• AND expresses IHC markers
©2015 MFMER | slide-36
Other unclassified
Lymphoepithelioma-like NUT carcinoma
t(15;19)
NUT
EBV ISH
10/26/2016
7
©2015 MFMER | slide-37
Interpretation on small biopsies
Recommendations of the 2015 WHO
©2015 MFMER | slide-38
GOAL
• To make a diagnosis on H&E or at least with the smallest number of immunostains
• Save tissue for molecular testing
• Most cancers in advanced stage
• If surgically resectable not as critical
©2015 MFMER | slide-39
Remember that…
• …our diagnosis dictates mostly additional studies to be performed…
• Everything but SQCC may be tested for EGFR, ALK, ROS etc
• …eventually SQCC with own studies
©2015 MFMER | slide-40
Tissue Processing
• Do not decalcify
• If can’t be avoided, consider making 2 blocks
• 1 with the calcified tissue
• 1 with softer tissue
• If more than 1 core or “abundant” aggregate of tissue
• Consider making 2 paraffin blocks
©2015 MFMER | slide-41
Most useful stains in Lung 1ary
• TTF-1 and p40
• Could even argue p40 is sufficient
• SQCC versus all others
©2015 MFMER | slide-42
A few things about IHC
• If not sure about tumor type
• Lymphoma? Melanoma? Carcinoma? Sarcoma?
• Carcinoma by far most common
• Keratin stains with unstained slides
• Keratin, CD45, S100 prot with unstained slides
• Use morphology to guide stains
• Best avoid many stains in 1st round
Avoid exhausting block
10/26/2016
8
©2015 MFMER | slide-43
A few things about IHC
• If considering metastasis from another site
• CDX2 can be + in Lung AD
• ER can be + in Lung AD
• STP24 clone of TTF-1 can be + in 1aries from other sites
Use clinical/radiologic information, compare to prior specimens, use and interpret IHC cautiously
©2015 MFMER | slide-44
A few things about IHC
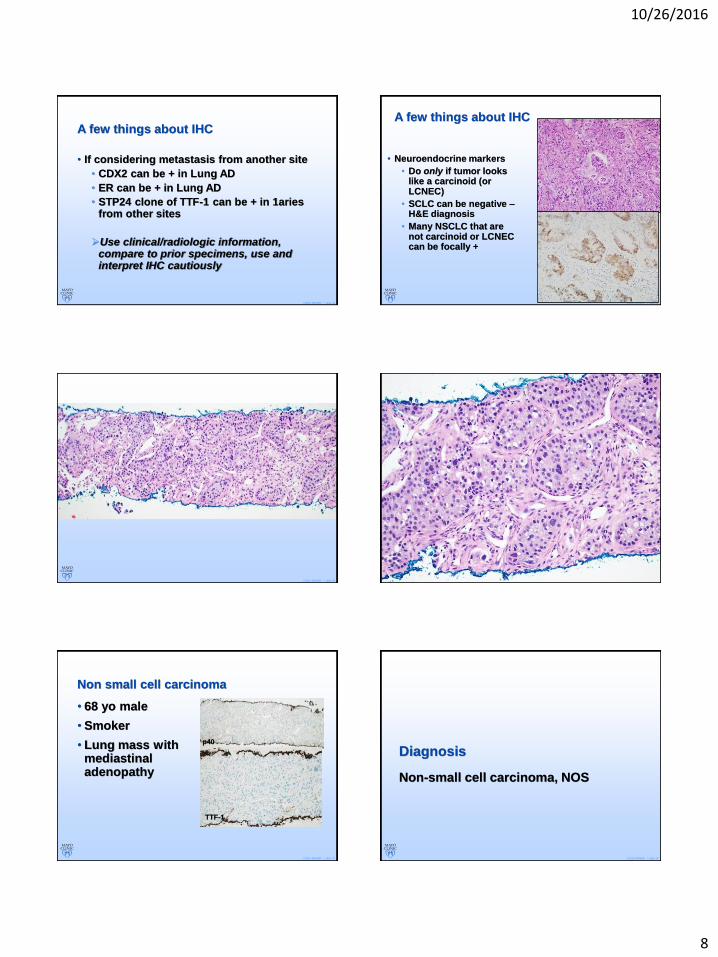
• Neuroendocrine markers
• Do only if tumor looks like a carcinoid (or LCNEC)
• SCLC can be negative –H&E diagnosis
• Many NSCLC that are not carcinoid or LCNEC can be focally +
©2015 MFMER | slide-45 ©2015 MFMER | slide-46
©2015 MFMER | slide-47
Non small cell carcinoma
• 68 yo male
• Smoker
• Lung mass with mediastinal adenopathy
p40
TTF-1
©2015 MFMER | slide-48
Diagnosis
Non-small cell carcinoma, NOS
10/26/2016
9
©2015 MFMER | slide-49 ©2015 MFMER | slide-50
©2015 MFMER | slide-51
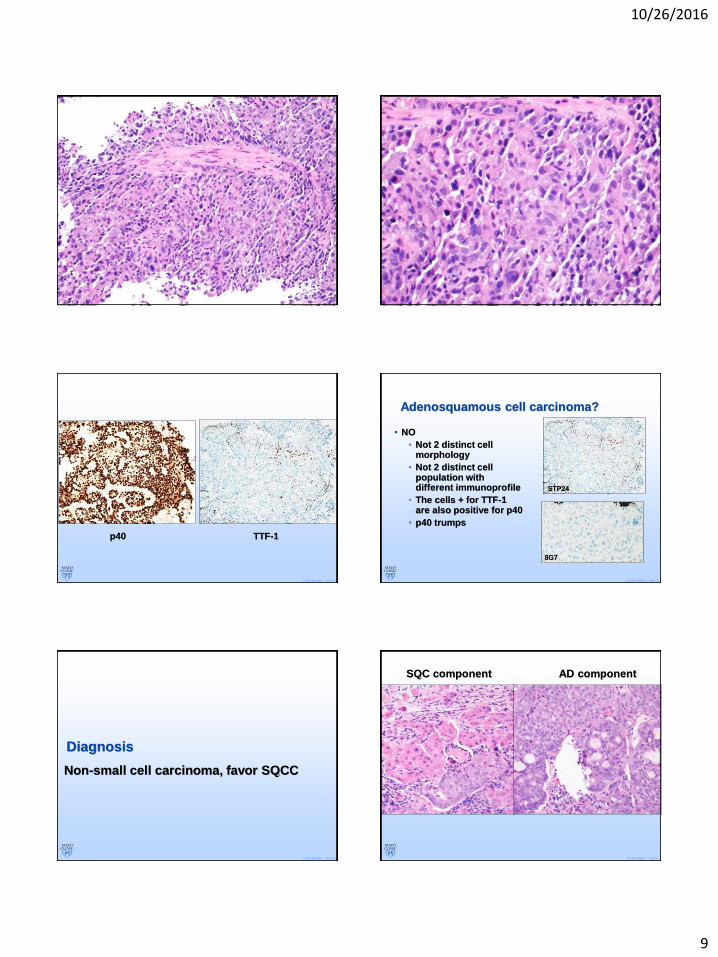
p40 TTF-1
©2015 MFMER | slide-52
Adenosquamous cell carcinoma?
• NO
• Not 2 distinct cell morphology
• Not 2 distinct cell population with different immunoprofile
• The cells + for TTF-1 are also positive for p40
• p40 trumps
STP24
8G7
©2015 MFMER | slide-53
Diagnosis
Non-small cell carcinoma, favor SQCC
©2015 MFMER | slide-54
SQC component AD component
10/26/2016
10
©2015 MFMER | slide-55
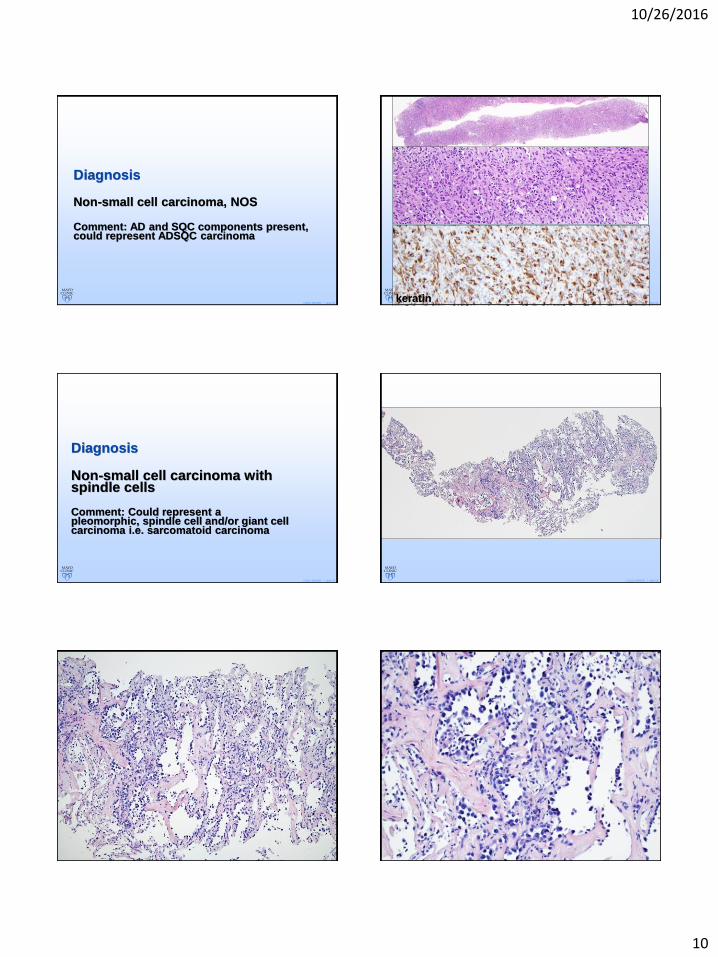
Diagnosis
Non-small cell carcinoma, NOS
Comment: AD and SQC components present, could represent ADSQC carcinoma
©2015 MFMER | slide-56keratin
©2015 MFMER | slide-57
Diagnosis
Non-small cell carcinoma with spindle cells
Comment: Could represent apleomorphic, spindle cell and/or giant cell carcinoma i.e. sarcomatoid carcinoma
©2015 MFMER | slide-58
©2015 MFMER | slide-59 ©2015 MFMER | slide-60
10/26/2016
11
©2015 MFMER | slide-61
Benign versus Neoplastic
• If benign reactive pneumocyte hyperplasia, reactive to what?
• AAH?
• Size ≤ 5mm
• Radiologic context is very helpful and knowing that the lesion has actually been sampled
©2015 MFMER | slide-62
©2015 MFMER | slide-63 ©2015 MFMER | slide-64
©2015 MFMER | slide-65
Clinical and radiologic findings
• 65 yo woman
• Single GGO 2.5cm
©2015 MFMER | slide-66
Concluded that it is neoplastic
• Adenocarcinoma with pure lepidic growth, no stromal invasion….
• AIS? MIA? LPA?
10/26/2016
12
©2015 MFMER | slide-67
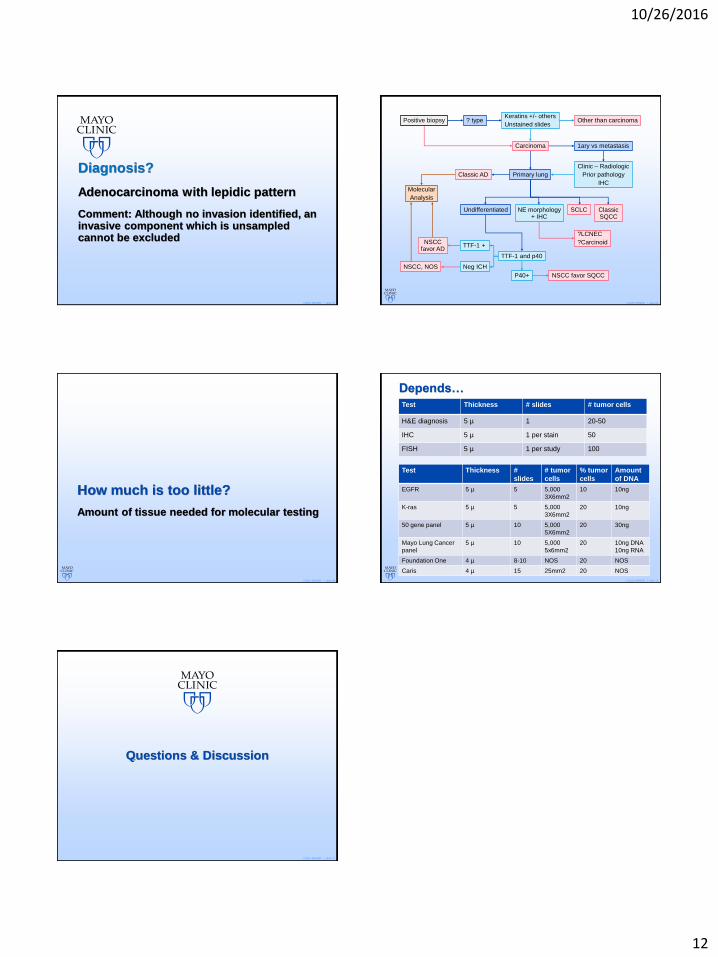
Diagnosis?
Adenocarcinoma with lepidic pattern
Comment: Although no invasion identified, an invasive component which is unsampledcannot be excluded
©2015 MFMER | slide-68
Positive biopsy ? typeKeratins +/- others
Unstained slidesOther than carcinoma
Carcinoma 1ary vs metastasis
Clinic – Radiologic
Prior pathology
IHC
Classic AD
ClassicSQCC
SCLCUndifferentiated
TTF-1 and p40
TTF-1 +
P40+ NSCC favor SQCC
NE morphology+ IHC
?LCNEC
?Carcinoid
Neg ICH
Primary lung
Molecular
Analysis
NSCCfavor AD
NSCC, NOS
©2015 MFMER | slide-69
How much is too little?
Amount of tissue needed for molecular testing
©2015 MFMER | slide-70
Depends…
Test Thickness # slides # tumor cells
H&E diagnosis 5 µ 1 20-50
IHC 5 µ 1 per stain 50
FISH 5 µ 1 per study 100
Test Thickness #
slides
# tumor
cells
% tumor
cells
Amount
of DNA
EGFR 5 µ 5 5,000
3X6mm2
10 10ng
K-ras 5 µ 5 5,000
3X6mm2
20 10ng
50 gene panel 5 µ 10 5,000
5X6mm2
20 30ng
Mayo Lung Cancer
panel
5 µ 10 5,000
5x6mm2
20 10ng DNA
10ng RNA
Foundation One 4 µ 8-10 NOS 20 NOS
Caris 4 µ 15 25mm2 20 NOS
©2015 MFMER | slide-71
Questions & Discussion