Embed Size (px)
Citation preview
November 14, 2019
Postcards from the edge-how founder
populations and the universities that serve
them can change the world
Terry-Lynn Young, PhD
Professor and Director of Genomics Research


Founder Populations—why are they useful for gene discovery?
• Founder effect:• Mutations get amplified through
population bottleneck and subsequent amplification

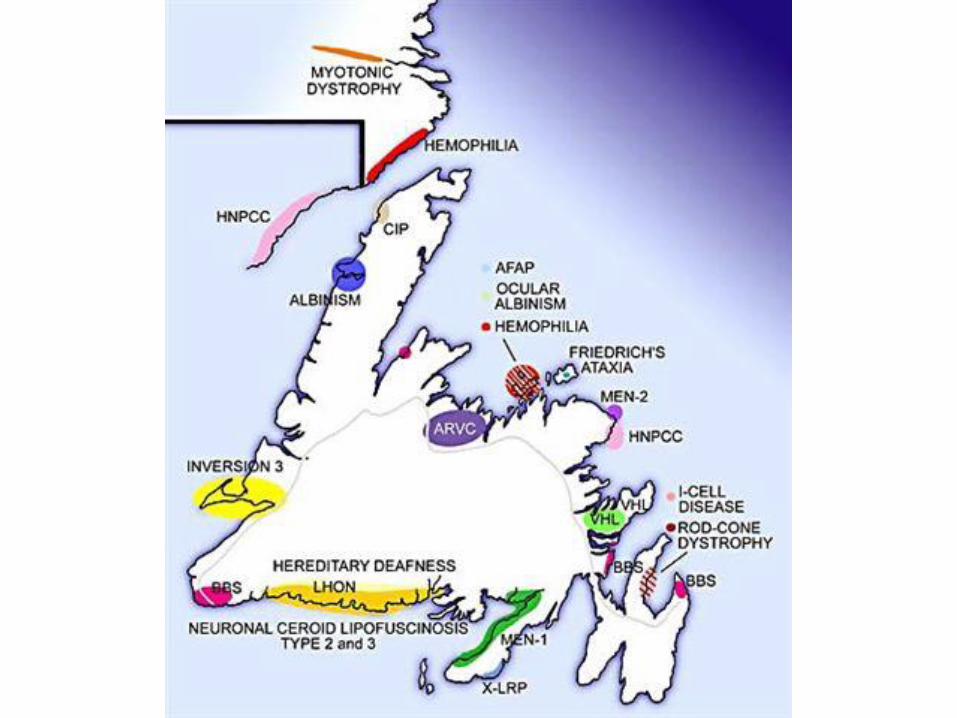
Founder Populations (Genetic isolates)
NewfoundlandAzores, Portugal
Holland
Finland
Sardinia, Italy
Costa Rica
Antioquia, Columbia
Afrikaner (South Africa)
NewfoundlandAzores, Portugal
Holland
Finland
Sardinia, Italy
Costa Rica
Antioquia, Columbia
Afrikaner (South Africa)
Quebec

Population History of the Island of Newfoundland
• 1497: John Cabot first reached NL
• 1610: established seasonal fishing colonies (outports)
• Mid-1700’s: Peak immigration, mainly Protestant settlers (south-west England), Catholic settlers (southern Ireland)

Settlement along the coast
(fishing villages=outports)
20,000-30,000 founders
Large families
50% of outports < 2000 resident
Little emigration or immigration
Segregation by religion
Founder effects
High coefficient of kinship

Founder Populations—limited variation in the human genome
• Founder effect:• Mutations get amplified through
population bottleneck and subsequent amplification

Clans-Clusters of related families


•Clinically difficult to diagnose
•First presentation SCD
•Lethal tachyarrhythmias: VT/VF
Arrhythmogenic Right Ventricular Cardiomyopathy






Genetic condition affecting heart muscle
• Autosomal Dominant (HIGH RECURRENCE RISK)
• Difficult to diagnose clinically
• Sudden cardiac death (SCD) often first presentation due to ventricular tachycardia (VT) or fibrillation (VF)


Single mutation, single gene
*
Common
Ancestor*
** * * *
transmembrane protein: TMEM43
Single missense mutation (S358L)

Survival ICD No ICD
Median N/A 8.9yrs. (SE
1.7)
5 year 95.4% 64.6%
10 year 88.3% 36.7%
RR 9.3 (95% CI 3.3-26.0)
Survival ICD No ICD
Median 16.9 (SE
N/A)
4.5yrs. (SE
1.4)
5 year 100% 50%
10 year 81.6% 25.4%
RR 9.7 (95% CI 3.2-29.6)
Survival ICD No ICD
Median N/A 25.5yrs.
(SE 3.7)
5 year 96.7% 84.7%
10 year 88.2% 69.3%
RR 3.6 (95% CI 1.3-9.5)
Males with ICDs for primary prophylaxis compared with controls
Males with ICDs for secondary prophylaxis
compared with controls
Females with ICDs for primary prophylaxis
compared with controls
Time to death or last follow-up from the start of the study in 148 ICD individuals and 148
matched controls for PP in males (A), SP in males (B) and PP in females (C)



TMEM43 p.S358L mutation worldwide
European ancestry dating mutation to 400 – 700 AD
Denmark1
Germany2
Canada3,4
United States5
New Zealand3
Sri Lanka6
Spain6
1Christensen et al. Clin Genet 2011;80:256-64.2Klauke et al. Cell Tissue Res 2012;348:368.3Baskin et al. Hum Genet 2013;132:1245-52.4Merner et al. Am J Hum Genet 2008;82:809-21.5Milting et al. European heart journal 2015;36:872-81. 6Personal communication

Personalized Medicine:R&D Opportunities in revolutionizing hearing Aid (HA) technology

http://www.globalcarecompany.com/anatomy-of-the-ear.html

Hearing Loss-most cases due to mutations in genes
Genetics
50%Idiopathic
25%Environment
25%
• Most common sensory deficit
• Prevalence:
– Newborn: 1/500
– Adult: 1/5
• Causes:
– Environment
– Idiopathic
– Genetic

TECTACOL11A2
OTOFMYO7ACDH23PCDH17
GJB2GJB6GJB3
Animal research tell us about the functions of these genes in hearing
OTOASTRCMYO7ACDH23PCDH17


National Rural Healthcare Innovation in Grand Falls-Windsor,NL
The Genomics-Based R&D Centre for Health

The Project
Use NL families with mutations in these hearing genes to make models of different types of hearing loss
Improve efficacy of hearing devices
Create a competitive advantage for
industry

Challenges of Aiding Hearing Loss
Clinical testing (audiogram) does not provide accurate data
on specifics of loss
Lack of data restricts ability to customize
hearing device
Clinical community doesn’t understand the major role that
genetics plays

Addressing these Challenges
• Genomics reveals the exact site of lesion in the auditory pathway
Clinical testing (audiogram) does not provide accurate data
on specifics of loss
• Computer modeling will provide key data points to develop lesion-specific algorithms; multiplex families will provide patient feedback
Lack of data restricts ability to customize
hearing device
• Knowledge translation/education of audiologists/ENT clinicians, and patients is integral to this program of research
Clinical community doesn’t understand the major role that
genetics plays

The Process
Recruit research clients to GFW
Run sophisticated phenotype tests in GFW site to make the link between gene mutation
and hearing deficit
Design Computer models to mimic effect of lesion in auditory pathway
Develop novel algorithms to
address hearing deficit

University-community partnerships at work
Stay tuned…
Balance clinic for GFW
will be announced soon
New private-public
partnership

35
Phenotyping
Susan G. Stanton
Western
Amanda Morgan
Matthew Lucas
Modeling
Ian C. Bruce
McMaster
Michael R.
Wirtzfeld
Genetics
Terry Lynn Young
Memorial
University
Newfoundland
Data collection
Anne Griffin
Genomics-based
hearing research
centre,
Grand Falls-Windsor
Jill Lowther

Questions???????