Embed Size (px)
Citation preview

Post-traumatic Complications of Severe Luxations and replanted Teeth
The Journal of Contemporary Dental Practice, January 2015;16(1):13-19 13
JCDP
ABSTRACTAim: The aim of this study was to evaluate the main post-traumatic complications of severe luxation and replanted teeth using clinical and radiographic analyses.
Materials and methods: Eighty-three patients aged between 7 and 55 years old presenting 180 traumatized teeth that suffered extrusive luxation (n = 67), lateral luxation (n = 69), intrusive luxation (n = 10) and tooth avulsion (n = 34) followed by replantation were evaluated. The follow-up period was 24 months. The complications examined were: pulp canal obliteration, pulp necrosis and root resorption (inflammatory and replacement). Furthermore, the relationship between time elapsed before receiving dental attendance and development of inflammatory resorption was observed.
Results: Pulp necrosis was the main complication, occurring in 147 teeth (82.7%). All of the teeth that suffered intrusive luxation and tooth avulsion were diagnosed with pulp necrosis, with significant difference in comparison with another traumas (p < 0.001/Fisher’s exact test). Inflammatory root resorption was observed in 20.5% of the cases and replacement resorption was more related to tooth replantation (94.1%), showing significant prevalence among tooth luxations (p < 0.001/Fisher’s exact test). In addition, it was noted that patients who seek treatment 9 weeks after the trauma episode presented 10 times more chance of developing inflammatory resorption when compared with patients who seek treatment soon after dental trauma (Odds ratio test).
Conclusion: It may be concluded that pulp necrosis was the main post-traumatic complication observed in traumatized teeth and that delay in seeking treatment may damage the prognosis of severe luxation and replanted teeth.
Clinical significance: Clinical studies describing the main complications that may affect traumatized teeth present great relevance to make the population aware of the importance of seeking immediate treatment and to alert the professional to the need for follow-up. When traumatic injuries are diagnosed and
ORIGINAL RESEARCH10.5005/jp-journals-10024-1628
Post-traumatic Complications of Severe Luxations and replanted Teeth1Thiago Farias Rocha Lima, 2Juliana Yuri Nagata, 3Francisco José de Souza-Filho, 4Adriana de Jesus Soares
1Department of Restorative Dentistry, Endodontics Area Federal University of Paraíba, João Pessoa, Paraiba, Brazil2Department of Dentistry, Federal University of Sergipe Lagarto, Brazil3,4Department of Restorative Dentistry, Endodontics Area Piracicaba Dental School, State University of Campinas Piracicaba, Brazil
Corresponding Author: Thiago Farias Rocha Lima, Professor Department of Restorative Dentistry, Endodontics Area Federal University of Paraíba, João Pessoa, Paraiba, Brazil Phone: 982226564, e-mail: [email protected]
treated early, post-traumatic complications may be controlled, allowing conservation of the tooth in oral cavity.
Keywords: Tooth injury, Root resorption, Dental pulp necrosis.
How to cite this article: Lima TFR, Nagata JY, de Souza-Filho FJ, de Jesus Soares A. Post-traumatic Complications of Severe Luxations and replanted Teeth. J Contemp Dent Pract 2015;16(1):13-19.
Source of support: Nil
Conflict of interest: None
INTRODUCTION
Dental trauma may be considered a dental emergency, and its treatment requires a multidisciplinary approach. Epidemiological studies have revealed that dental trauma affects 10 to 35% of population, and due to this high preva-lence, it may be considered a world public health problem.1,2
Trauma to supporting tissues (extrusive luxation, late-ral luxation, intrusive luxation and tooth avulsion) com-prises 15 to 61% of traumatic episodes and is considered the most severe lesions.2,3 Complications related to these types of trauma may occur in weeks, months and even years after the traumatic accident.4 Pulp canal oblitera-tion, pulp necrosis and root resorption refer to the most common sequelae, with the worst prognosis being related to root resorption.5,6 These complications have shown prevalence values that depend on the severity of the lesion and root development stage. Pulp canal obliteration after luxation and tooth avulsion shows prevalence between 3 to 24%.7-10 On the other hand, pulp necrosis may occur in 64% and 77% of extrusive and lateral luxation, respec-tively, and for intrusive luxation and tooth avulsion this value may reach 100%.11,12
The prevalence of root resorption after luxations and avulsion has also been shown to vary a great deal. In dental replantations, the extra-alveolar period and storage medium are crucial aspects in the development of this type of sequela. Some studies have revealed that inflammatory resorption occurs in 5 to 70% of luxations and 20 to 50% of avulsions.5,10,13,14 Similarly, replace-ment resorption has been shown to be more frequent in intrusive luxation, with a prevalence of 20 to 40%, and in tooth replantation this sequela occurs in 50 to 70% of the cases.5,10,13,14
Therapeutic measures related to luxation and dental replantation vary according to the type of trauma,
JCDP

Thiago Farias Rocha Lima et al
14
pulp and periapical condition, and stage of root end development. In all these situations, patients should be followed-up for long periods of time to enable immediate intervention in cases of complications with a view to maintaining the tooth healthy and in the oral cavity.
Considering the foregoing, the aim of this study was to evaluate the main post-traumatic complications of teeth that suffered severe luxations and avulsions followed by replantation, and associate some of the factors that may be related to the development of these sequelae.
MATERIALS AND METHODS
This research was approved by Ethics Committee—CEP, of Piracicaba Dental School, State University of Campinas.
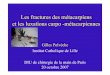
The present study evaluated 83 patients aged between 7 and 55 years old, presenting 180 traumatized teeth that suffered extrusive luxation (n = 67), lateral luxation (n = 69), intrusive luxation (n = 10) and tooth avulsion (n = 34) followed by replantation (Figs 1A to D) Emergency attendance was performed in hospitals, health centers or private clinics, and afterwards, patients were referred to the Dental Trauma Center in the area of Endodontics at the Piracicaba Dental School, State University of Campinas in the State of Sao Paulo, Brazil. Exclusion criteria included presence of crown fractures without
supporting tissue involvement and/or patients who presented primary tooth trauma.
Data were collected from standard clinical charts and included information, such as age, gender, etiology and teeth involved. In addition, for cases of replantation, data such as the extra-alveolar period and storage medium of avulsed teeth were considered. Initial clinical aspects, such as the presence or absence of splinting, type of splinting, initial endodontic approach and time elapsed between trauma date and first attendance at the Dental Trauma Center were also collected.
Evaluation of Post-traumatic Complications
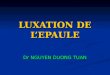
Clinical and radiographic data were collected for 24 months. The following parameters were recorded: pulp necrosis, pulp canal obliteration and inflammatory and/or replacement root resorption (Figs 2A to D). Pulp sensitivity was assessed by the cold thermal test, using carbon dioxide negative test (–50ºC) (EndoFrost® -Roeko, Langenau, Germany). The absence of response to the cold test associated with radiographic data was diagnosed as pulp necrosis. In cases of pulp canal obliteration, a cavity test was performed to confirm diagnosis.
Pulp canal obliteration and root resorption were diagnosed by radiographic evaluation. All radiographs
Figs 1A to D: Clinical view of severe luxations and replanted teeth (A), Extrusive luxation of the right central incisor (B), lateral luxation of the anterior teeth associated alveolar bone fractures (C) and intrusive luxation of the left lateral incisor (D)
A B
C D

Post-traumatic Complications of Severe Luxations and replanted Teeth
The Journal of Contemporary Dental Practice, January 2015;16(1):13-19 15
JCDP
were taken with periapical films (Kodak, São José dos Campos, São Paulo, Brazil) associated with an intraoral positioner (Indusbello indústria de instrumentos Odon-tológicos Ltda., Londrina, Paraná, Brazil), to ensure the quality and standardization of images. Radiographic analyses was performed by 2 trained Endodontic spe-cialists, using a negatoscope (Lumatron, Encor Indústria Fotográfica Ltda., Rio Claro, São Paulo, Brazil) coupled to a lens providing 4× magnification.
External inflammatory resorption was defined accor- ding to the presence or absence of cortical alveolar bone associated with the presence of bone radiolucence. Inter- nal inflammatory resorption was diagnosed when a change in root canal continuity could be observed. Replace ment resorption was verified when the replace-ment of radicular dentin by bone tissue was observed. The root development stage was also observed, being considered complete in teeth with a closed apex and incomplete in those with an open apex.
Statistical Analysis
Results were analyzed in BioEstat 5.0 (Instituto Sustentável Mamirauá, Belém, PA, Brazil) and SAS Software 9.1 (The SAS Institute, Cary, NC, USA) programs, at a level of significance of 5%. Data related to patients (age, gender,
etiology of trauma) and to post-traumatic complications (pulp necrosis and root resorption) were analyzed using Fisher’s exact test. The Odds ratio test was used to verify the relationship between time elapsed before the first attendance at the Dental Trauma Service and development of inflammatory resorption.
RESULTS
Male gender and age group between 7 and 14 years old were the most frequently injured patients, without statistical difference between age and gender (p = 0.4592/Fisher’s exact test) (Table 1). The main etiological factor associated with trauma was cycling accidents followed by falls (Table 2). The most affected teeth were the maxillary central incisors.
Patients received emergency attendance in hospitals (n = 36), at private clinics (n = 17) and at health centers (n = 16). Only 14 patients received their first attendance at the Dental Trauma Center. As regards the time elapsed before treatment began, 37 patients were treated 15 days after trauma date (44.58%), 22 after 3 to 8 weeks (26.51%) and 24 patients were treated after a period longer than eight weeks (28.91%).
Most of the affected teeth were maxillary central incisors (n = 116), followed by maxillary lateral incisors (n = 38), mandibular central incisors (n = 15), mandibular lateral incisors (n = 5), mandibular canines (n = 6) and
Figs 2A to D: Post-traumatic complications evaluated in this study: (A) Pulp canal obliteration, (B) pulp necrosis and periapical lesion, (C) inflammatory root resorption and (D) replacement resorption
Table 1: Percentage distribution of patients according to age group and gender (n = 83)
AgeGender
n (%)Male (%) Female (%)7-14 years 32 (65.31) 17 (34.69) 49 (59.04)15-20 years 14 (82.35) 3 (17.65) 17 (20.48)21- 26 years 5 (62.50) 3 (37.50) 8 (9.64)≥ 27 years 5 (55.56) 4 (44.44) 9 (10.84)Total 56 (67.47) 27 (33.53) 83 (100)p = 0.4592 (Fisher’s exact test)
Table 2: Etiology of severe luxation and replanted teeth (n = 83)
Etiology n (%)Bicycle 28 (33.7)Fall 20 (24)Sports 13 (15.7)Car accident 14 (16.9)Work accident 4 (4.8)Aggression 4 (4.8)Total 83 (100)
A B C D

Thiago Farias Rocha Lima et al
16
maxillary canines (n = 3). As regards the extra-alveolar period of avulsed teeth, only 7 teeth were replanted in a period of less than 30 minutes. Most of these teeth were kept in dry conditions (26.5%) and for a period of 60 to 120 minutes of extra-alveolar time (35.3%). Other avulsed teeth were stored in milk (n = 8), water (n = 7), saline solution (n = 6) and saliva (n = 4).
Considering initial clinical aspects, it was observed that 36 patients (43.4%) were referred to the Dental Trauma Center presenting rigid splinting; 22 patients (26.5%) with flexible splinting and 25 patients (30.1%) without splinting. In addition, it was verified that in only 9 patients, endodontic treatment began at the place of the first attendance.
Post-traumatic Complications of Severe Luxation and Replanted Teeth
The follow-up time was 24 months. In this period, com-plications, such as pulp necrosis, inflammatory and replacement resorptions were observed (Table 3). Of the total number of teeth analyzed (n = 180), 33 teeth (16.3%) remained vital and 147 teeth (82.7%) suffered pulp necrosis. There was statistical difference related to the presence of necrosis for the 4 types of dental trauma (p < 0.001/ Fisher’s exact test), considering that for extru-sive luxation this frequency was lower (59.7%). Inflamma-tory resorption was verified in 37 cases (20.5%). There was no statistical difference between inflammatory resorption and types of trauma (p = 0.258/ Fisher’s exact test). Rep-lacement resorption was diagnosed in 36 cases (20%). Statistical difference was observed when the presence of this resorption was compared with the types of dental trauma (p < 0.001/ Fisher’s exact test). Replanted teeth presented a higher frequency of replacement resorption (94.2%), followed by intrusive luxation (30%).
Pulp canal obliteration were diagnosed only in cases of extrusive luxation (3%). Lateral luxation, intrusive luxa-tion and tooth replantation did not present pulp canal obliteration.
Eighteen teeth presented immature root development, of which 11 teeth suffered extrusive luxation, 1 tooth suffered lateral luxation, 2 teeth intrusive luxation and 4 suffered avulsion. Considering the stage of root development, only 5 teeth maintained vitality (27.28%).
It was observed that time elapsed from trauma date to the beginning of treatment influenced the development of inflammatory resorption in extrusive luxation (p = 0.001/Fisher’s exact test) and in lateral luxation (p = 0.0135/Fisher’s exact test). There was no statistical relationship between intrusive luxation and avulsion (Table 4).
The Odds ratio test allowed a study of the relationship between the development of inflammatory resorption and time elapsed between the trauma date and begin-ning of treatment, irrespective of the type of treatment. Patients that started treatment between the third and eighth week presented 4 times more chance of developing inflammatory resorption when compared with patients who received attendance soon after dental trauma. On the other hand, patients that with treatment after 8 weeks presented 10 times more chance of developing inflam-matory resorption, when compared with all the studied patients (Table 5).
DISCUSSION
The sample of this study was composed of patients that suffered severe luxation and avulsion. The studied population was constituted mainly of male patients (65.71%), aged between 7 and 14 years of age (59.04%), with the maxillary central incisors being the group of teeth more frequently affected by trauma (64.4%). As regards
Table 3: Post-traumatic complications observed in severe luxations and replanted teeth (Fisher’s exact test)
Type of injury n (%)Necrosis Inflammatory resorption Replacement resorption
n (%) p n (%) p n (%) pExtrusive luxation 67 (100) 40 (59.7) < 0.0001 13 (19.4) 0.258 0 (0) < 0.0001Lateral luxation 69 (100) 63 (91.3) 11 (15.94) 1 (1.45)Intrusive luxation 10 (100) 10 (100) 2 (20) 3 (30)Avulsion 34 (100) 34 (100) 11 (32.35) 32 (94.12)
Table 4: Relation between initial attendance after trauma and development of inflammatory root resorption in severe luxations and replanted teeth (Fisher’s exact test)
Type of injuryPresence of inflammatory resorption (n)
Time elapsed between trauma date and beginning of the treatment p-value< 2 weeks n(%) 3 < n < 8 weeks n(%) > 9 weeks n(%)
Extrusive luxation 13 1 (7.69) 2 (15.39) 10 (76.92) 0.0001Lateral luxation 11 1 (9.1) 5 (45.45) 5 (45.45) 0.0135Intrusive luxation 2 0 (0) 1 (50) 1 (50) 0.4667Avulsion 11 3 (27.27) 6 (54.54) 2 (18.18) 0.2985Total 37 5 (13.51) 14 (37.84) 17 (45.95) —

Post-traumatic Complications of Severe Luxations and replanted Teeth
The Journal of Contemporary Dental Practice, January 2015;16(1):13-19 17
JCDP
etiologic factors, bicycle accidents (33.7%) followed by falls (24%) were the main factors related to traumatic epi-sodes. The epidemiological profile of luxation and tooth replan tation has also been studied by other authors, who observed similar results.5,10,15,16
The majority of the studies demonstrated that the emergency attendance, treatment and patient follow-up are generally performed in the same place.13,14,17-22 On the contrary, the present study showed that most of eva- luated patients received emergency care in other clinics and were afterwards referred to the Dental Trauma Cent-er of Piracicaba Dental School for clinic and radiographic follow-up. According to Al Jundi,23 the delay in seeking dental care influence the prognosis of traumatized teeth.
Pulp necrosis was the main complication observed after luxation and dental replantation, data also noted by other studies.7,10,12,19,24-28 In addition, statistical diffe-rence was verified when the occurrence of necrosis was compared among the types of dental trauma (p < 0.001). In extrusive luxation, necrosis was observed in 59.1% of evaluated teeth. Some studies demonstrated similar prevalence, with 43 and 56% of teeth with nec-rotic pulp.7,19 Moreover, another study showed that when the sample is composed of mature teeth exclusively, only 2% of extrusive luxation cases maintained vitality.29 As regards lateral luxation, in the present study a prevalence of 91.3% of pulp necrosis was observed, a value that is considered high, when compared with other studies that demonstrated 4027 and 47.3%10 of pulp necrosis for lateral luxation. This difference may be explained considering that in a large number of those studies, the sample was composed of immature teeth, whereas in the present study, only 1 tooth that suffered lateral luxation was not completely developed.
In intrusive luxation and tooth replantation it was veri- fied that all teeth presented pulp necrosis. The literature is contradictory with regard to necrosis in intruded and avulsed teeth, with similar researches having presented high values,10,12 and others demonstrating low values (45.1 and 57%).30,31 This difference may be explained because in previous studies, the evaluated populations were composed only of children and young people.
Another relevant post-traumatic complication refers to root resorption. Inflammatory resorption was diagnosed in 20.5% of the cases, without statistical difference when compared with the prevalence of this resorption in the four types of trauma evaluated (p = 0.258). Many authors
have stated that this type of resorption may occur after severe dental trauma and is related to the presence of microorganisms inside root canal.22,25
Extrusive and lateral luxations presented inflammatory resorption in 19.4 and 11.94% of the cases, respectively. Other studies have observed lower frequencies varying from 0 to 10%.7,10,12,19,20 The higher values observed in the present study may be explained due to the delay in seeking treatment. In cases of extrusive luxation, 76.6% of the patients began receiving treatment in the Dental Trauma Center 9 weeks after dental trauma date. This was shown for lateral luxation as well, in which 45.5% of the patients sought attendance after the same period. It was verified that the time elapsed between the trauma date and the beginning of the treatment influenced the development of inflammatory resorption in extrusive and lateral luxations.
It was observed that in intrusive luxation, inflam-matory resorption was diagnosed in 20% of the cases, a result that is in agreement with studies presented in the literature.31,33-35 In replanted teeth, this type of resorp-tion was observed in 32.35% of the cases, which is a value similar to that in other studies.5,36 On the contrary, there are contradictory results in the literature related to the presence of inflammatory resorption, which have dem-onstrated lower values (12.8%),37 while another shows a prevalence of 62.5% in the total number of replanted teeth.32 This difference may be explained due to variables that may influence the occurrence of this complication such as extra-alveolar period, storage medium and patient age.
The main factors related to the prognosis of trauma-tized teeth are type of injury and stage of root develop-ment.12 However, it was observed that the delay in seeking treatment can also affect the prognosis. Considering the relationship between inflammatory resorption develop-ment and patient s delay to seek treatment, it was obser- ved that patients who begin treatment between third and eighth weeks after trauma presented 4 times more chance of developing inflammatory resorption. When this time for seeking treatment was longer than 8 weeks, the development of inflammatory resorption increased 10 times. This fact was also verified in previous studies that reported that late attendance performed 3 months after trauma may compromise the pulp and periodontal prognosis of traumatized teeth.23
Table 5: Odds ratio test to verify the relation between initial attendance date after trauma and development of inflammatory resorption
Initial attendance after trauma n Inflammatory resorption n (%) Odds Ic 95% p-value< 2 weeks 76 5 (6.58) 1 — —3 < n < 8 62 14 (22.58) 4.1417 1.3997-12.2550 0.0137> 9 weeks 42 18 (42.86) 10.65 3.5679-31.7896 < 0.0001

Thiago Farias Rocha Lima et al
18
Replacement resorption was not frequent in extru-sive and lateral luxations, which is in agreement with the literature.12,19,24,27,38 On the other hand, in intrusive luxation this type of resorption was diagnosed in 30% of the cases. Previous studies have also observed that replacement resorption may occur with a frequency of 20 to 40% in cases of intrusive luxation.13,26
In tooth replantation, replacement resorption was noted in 94.12% of the cases. Other authors also observed that this type of complication is frequently found in tooth avulsion.28,39,40 The extra-alveolar period and stor-age medium of the avulsed tooth are decisive factors for periodontal ligament repair.41 In the present study, of a total of 34 teeth, 29 teeth were replanted late/after a delay, which may have contributed to greater number of replacement resorption observed.
Pulp canal obliteration have been verified in 25-40% of luxations, being commonly noted in immature teeth.4,10,19,30 In the present research, pulp canal oblitera-tion were diagnosed in only 3% of extrusive luxations, and in lateral and intrusive luxations this sequela was not observed. The lower frequency may be explained due to a slower number of immature teeth and high prevalence of pulp necrosis.
Clinical studies describing the main complications that may affect traumatized teeth present great relevance to make the population aware of the importance of seek-ing immediate treatment and to alert the professional to the need for follow-up. When traumatic injuries are diag-nosed and treated early, post-traumatic complications may be controlled, allowing conservation of the tooth in oral cavity. Future studies that evaluate immediate and late complications after traumatic injuries should be conducted in order to develop new treatment alternatives.
CONCLUSION
The main post-traumatic complication of luxated and rep-lanted teeth observed was pulp necrosis. It was demons-trated that the longer the time elapsed between the dates of trauma and seeking treatment the greater the risk for developing inflammatory resorptions in severe luxation and replanted teeth. In addition, replacement resorption was most frequently observed in tooth replantations, with the extra-alveolar period being a decisive factor in the occurrence of this type of sequela.
CLINICAL SIGNIFICANCE
Clinical studies describing the main complications that may affect traumatized teeth present great relevance to make the population aware of the importance of seek-ing immediate treatment and to alert the professional
to the need for follow-up. When traumatic injuries are diagnosed and treated early, post-traumatic complica-tions may be controlled, allowing conservation of the tooth in oral cavity.
REFERENCES
1. Altun C, Ozen B, Esenlik E, Guven G, Gürbüz T, Acikel C, Basak F, Akbulut E. Traumatic injuries to permanent teeth in Turkish children, Ankara. Dent Traumatol 2009;25(3):309-313.
2. Schatz JP, Hakeberg M, Ostini E, Kiliaridis S. Prevalence of traumatic injuries to permanent dentition and its association with overjet in a Swiss child population. Dent Traumatol 2012;29(2):1-5.
3. Skaare AB, Jacobsen I. Etiological factors related to dental injuries in Nowergians aged 7-18 years. Dent Traumatol 2003;19(6):304-308.
4. Robertson A, Andreasen FM, Bergenholtz G, Andreasen JO, Norén JG. Incidence of Pulp Necrosis Susequent to Pulp Canal Obliteration form Trauma of Permanent Incisors. J Endod 1996;22(10):557-560.
5. Soares AJ, Gomes BPFA, Zaia AA, Ferraz CCR, Souza-Filho FJ. Relationship between clinical radiographic evaluation and outcome of teeth replantation. Dental Traumatol 2008; 24(2):183-188.
6. Guan Y, Qin M. A retrospective study of pulp healing after luxation injuries. Zhonghua Kou Qiang Yi Xue Za Zhi 2008; 43(9):520-523.
7. Oikarinen K, Gundlach KK, Pfeifer G. Late complications of luxation injuries to teeth. Endod Dent Traumatol 1987;3(6):296-303.
8. Andreasen FM, Yu Z, Thomsen BL, Andersen PK. Occurence of pulp canal obliteration after luxation injuries in the permanent dentition. Endod Dent Traumatol 1987;3(3):103-115.
9. Crona-Larsson G, Bjarhason S, Norén JG. Effect of luxation injuries on permanent teeth. Endod Dent Traumatol 1991; 7(5):199-206.
10. Hecova H, Tzigkounakis V, Merglova V, Netolicky J. A retrospective study of 889 injured permanent teeth. Dent Traumatol 2010;26(6):466-475.
11. Andreasen JO. Etiology and pathogenesis of traumatic dental injuries. A clinical study: of 1298 cases. Scand J Dent Res 1970; 78(4):329-342.
12. Andreasen FM, Vestergaard Pedersen B. Prognosis of luxated permanent teeth—the development of pulp necrosis. Dent Traumatol 1985;1(6):207–220.
13. Neto JJ, Gondim JO, de Carvalho FM, Giro EM. Longitudinal clinical and radiographic evaluation of severely intruded permanent incisors in a pediatric population. Dent Traumatol 2009;25(5):510-514.
14. Werder P, von Arx T, Chappuis V. Treatment outcome of 42 replanted permanent incisors with a median follow-up of 2.8 years. Schweiz Monatsschr Zahnmed 2011;121(4):312-320.
15. Crona-Larsson G, Norén JG. Luxation injuries to permanent teeth—a retrospective study of etiological factors. Endod Dent Traumatol 1989;5(4):176-179.
16. Schatz JP, Joho JP. A retrospective study of dento-alveolar injuries. Endod Dent Traumatol 1994;10(1):11-14.
17. Qin M, Ge L, Bai R. Use of a removable splint in the treatment of subluxated, luxated and root fractured anterior permanent teeth in children. Dent Traumatol 2002;18(2):81-85.

Post-traumatic Complications of Severe Luxations and replanted Teeth
The Journal of Contemporary Dental Practice, January 2015;16(1):13-19 19
JCDP
18. Majorama A, Bardellini E, Conti G, Keller E, Pasini S. Root resorption in dental trauma: 45 cases followed for 5 years. Dent Traumatol 2003;19(5):262-265.
19. Lee R, Barrett EJ, Kenny DJ. Clinical outcomes for permanent incisor luxations in a pediatric population. II. Extrusions. Dent Traumatol 2003;19(5):274-279.
20. Ferrazzini Pozzi EC, von Arx T. Pulp and periodontal healing of laterally luxated permanent teeth: results after 4 years. Dent Traumatol 2008;24(6):658-662.
21. Stewart C, Dawson M, Phillips J, Shafi I, Kinirons M, Welbury R. A study of the management of 55 traumatically intruded permanent incisor teeth in children. Eur Arch Paediatr Dent 2009;10(1):25-28.
22. Petrovic B, Marković D, Peric T, Blagojevic D. Factors related to treatment and outcomes of avulsed teeth. Dent Traumatol 2010;26(1):52-59.
23. Al-Jundi SH. Type of treatment, prognosis, and estimation of time spent to manage dental trauma in late presentation cases at a dental teaching hospital: a longitudinal and retrospective study. Dent Traumatol 2004;20(1):1-5.
24. Dumsha TC. Luxation injuries. Dent Clin North Am 1995; 39(1):79-91.
25. Trope M, Moshonov J, Nissan R, Buxt P, Yesilsoy C. Short vs. long-term calcium hydroxide treatment of established inflammatory root resorption in replanted dog teeth. Endod Dent Traumatol 1995;11(3):124-128.
26. Ebeleseder KA, Santler G, Glockner K, Hulla H, Pertl C, Quehenberger F. An analysis of 58 traumatically intruded and surgically extruded permanent teeth. Endod Dent Traumatol 2000;16(1):34-39.
27. Nikoui M, Kenny DJ, Barrett EJ. Clinical outcomes for perma-nent incisor luxations in a pediatric population. III. Lateral luxations. Dent Traumatol 2003;19(5):280-285.
28. Chappuis V, von Arx T. Replantation of 45 avulsed permanent teeth: a 1-year follow-up study. Dent Traumatol 2005;21(5): 289-296.
29. Dumsha T, Hovland EJ. Pulpal prognosis following extrusive luxation injuries in permanent teeth with closed apexes. J Endod 1982;8(9):410-412.
30. Humphrey JM, Kenny DJ, Barrett EJ. Clinical outcomes for permanent incisor luxations in a pediatric population. I. Intrusions. Dent Traumatol 2003;19(5):266-273.
31. Wigen TI, Agnalt R, Jacobsen I. Intrusive luxation of perma-nent incisors in Norwegians aged 6-17 years: a retrospective
study of treatment and outcome. Dent Traumatol 2008;24(6): 612-618.
32. Petrovic B, Marković D, Peric T, Blagojevic D. Factors related to treatment and outcomes of avulsed teeth. Dent Traumatol 2010;26(1):52-59.
33. Andreasen JO, Bakland LK, Matras RC, Andreasen FM. Trau-matic intrusion of permanent teeth. Part 1. An epidemiologi-cal study of 216 intruded permanent teeth. Dent Traumatol 2006;22(2):83-89.
34. Andreasen JO, Bakland LK, Andreasen FM. Traumatic intrusion of permanent teeth. Part 2. A clinical study of the effect of preinjury and injury factors, such as sex, age, stage of root development, tooth location, and extent of injury including number of intruded teeth on 140 intruded permanent teeth. Dent Traumatol 2006;22(2):90-98.
35. Andreasen JO, Bakland LK, Andreasen FM. Traumatic intrusion of permanent teeth. Part 3. A clinical study of the effect of treatment variables such as treatment delay, method of repositioning, type of splint, length of splinting and antibiotics on 140 teeth. Dent Traumatol 2006;22(2): 99-111.
36. Kinirons MJ, Gregg TA, Welbury RR, Cole BOI. Variations in the presenting and treatment features in reimplanted perma-nent incisors in children and their effect on the prevalence of root resorption. Brit Dent J 2000;189(5):263-275.
37. Donaldson M, Kinirons MJ. Factors affecting the onset of resorption in avulsed and replanted incisor teeth in children. Dent Traumatol 2001;17(5):205-209.
38. Cvek M. Prognosis of luxated non-vital maxillary incisors treated with calcium hydroxide and filled with gutta-percha. A retrospective clinical study. Endod Dent Traumatol 1992; 8(2):45-55.
39. Andersson L, Bodin I, Sörensen S. Progression of root resorption following replantation of human teeth after exten- ded extra oral storage. Endod Dent Traumatol 1989;5(1): 38-47.
40. Andersson L, Bodin I. Avulsed human teeth replanted within 15 minutes: a long-term clinical follow-up study. Endod Dent Traumatol 1990;6(1):37-42.
41. Andreasen JO, Borum MK., Jacobsen HL. Andreasen FM Replantation of 400 avulsed permanent incisors. 4. Factors related to periodontal ligament healing. Endod Dent Trau-matol 1995d;11(2):76-89.