Embed Size (px)
Citation preview

British Journal ofPlastic Surgery (1981) 34, 286-290 0 1981 The Trustees of British Association of Plastic Surgeons
0007-1226/H/0163-0286 $02.00
Post-mastectomy breast reconstruction using a rectus abdominis musculocutaneous island flap
THOMAS H. ROBBINS
Melbourne, Australia
Summary-Post-mastectomy breast reconstruction using a rectus abdominis musculocutaneous island flap has produced better results than other commonly used techniques. The operating time is reduced and prosthetic implants are not usually required. Some of the advantages and applications of this technique are indicated.
Breast reconstruction following mastectomy should not be withheld from any woman who wants it and whose prognosis is reasonable.
For many years post-mastectomy breast
It is a normal desire for any person to have a major
reconstruction has been denied to thousands of
deformity corrected or improved if possible: if breast reconstruction is exceptional it is only in that it is more important because of
women partly because of fear of operating in an
the role of the breast in sexual and social relationships and the physical discomfort that results from ill-fitting clothing.
area of potentially “recurrent” disease. Residual disease is seldom treatable by further surgery and the possibility of future local recurrence should not deprive the patient of the immediate benefit of breast reconstruction to improve the quality of her remaining life provided her expected survival is reasonable.
However, the poor aesthetic results of in- adequate techniques of reconstruction have provided another important reason for not of- fering breast reconstruction to many women. These techniques have included the multi-staged migration of tubed pedicles, subcutaneous prosthetic implants, with or without local flap augmentation for skin cover. Such procedures have often seemed to give considerable support to many patients but little satisfaction and encouragement to the reconstructive surgeon.
The recent one-stage technique of transposing a latissimus-dorsi musculocutaneous island flap to cover a silicone implant seems to produce a better and more acceptable result, with good tissue cover for the implant and an acceptable donor site scar. Because of the thinness of the
latissimus-dorsi muscle a prosthetic implant is usually required with all its disadvantages. The
Breast
position of the patient may need to be changed
reconstruction
during the operation. This technique is probably
using a
,unsafe if the thoraco-dorsal artery has been
musculo-
previously damaged and inadequate if the muscle has atrophied following damage to the nerve to
iutaneous
latissimus-dorsi. Damage to both of these
island flap on the rectus ab-
structures can occur during an axillary gland dissection as part of the radical mastectomy.
dominis muscle and overlying skin. has produced improved results in a one-stage procedure with a shorter operating time and an acceptable donor site scar. It has other advantages which will be discussed and it is considered to be a useful additional technique in the treatment of this difficult reconstructive problem.
Method
Pre-operative Markings
The flap is provided by the upper part of the ipsilateral rectus abdominis muscle along with the overlying skin and subcutaneous tissue. The flap is marked pre-operatively with the patient standing. The outline of the rectus abdominis muscle is marked from its upper limit above the costal margin to just below the level of the umbilicus. The upper and lower limits of the flap are angulated to allow direct closure of the donor site (Fig. 1).
A line’ is then drawn laterally from the base of this flap over the mastectomy defect to mark the approach to the breast defect that requires tilling.
286
POST-MASTECTOMY BREAST RECONSTRUCTION 287
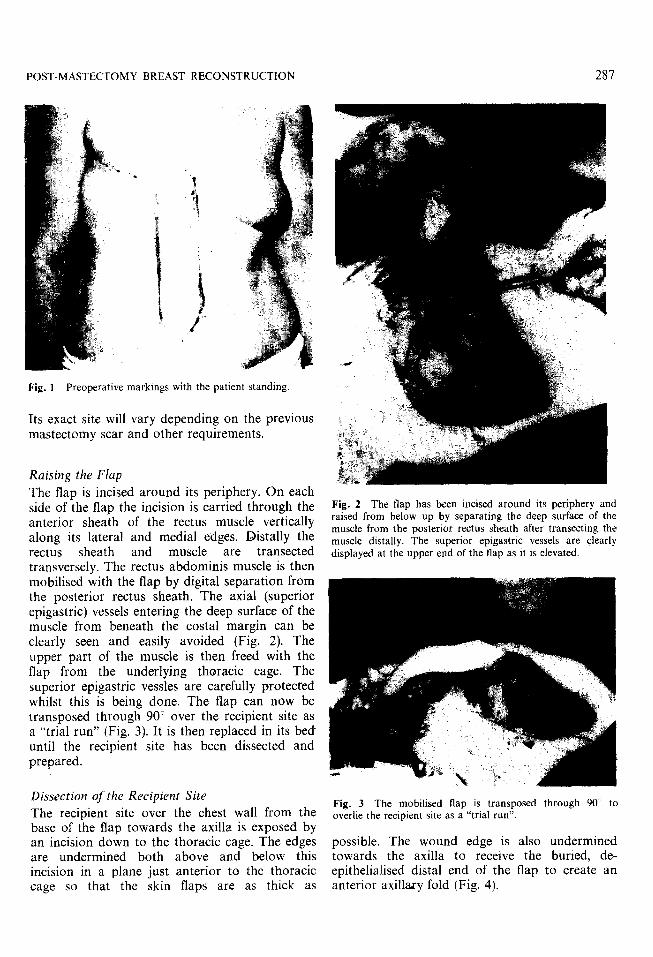
Fig. I Preoperative markings with the patient standing
Its exact site will vary depending on the previous mastectomy scar and other requirements.
Raising the Flap
The flap is incised around its periphery. On each side of the flap the incision is carried through the anterior sheath of the rectus muscle vertically along its lateral and medial edges. Distally the rectus sheath and muscle are transected transversely. The rectus abdominis muscle is then mobilised with the flap by digital separation from the posterior rectus sheath. The axial (superior epigastric) vessels entering the deep surface of the muscle from beneath the costal margin can be clearly seen and easily avoided (Fig. 2). The upper part of the muscle is then freed with the flap from the underlying thoracic cage. The superior epigastric vessles are carefully protecred whilst this is being done. The flap can now be transposed through 90” over the recipient site as a “trial run” (Fig. 3). It is then replaced in its bed until the recipient site has been dissected and prepared.
Dissection of the Recipient Site
The recipient site over the chest wall from the base of the flap towards the axilla is exposed by an incision down to the thoracic cage. The edges are undermined both above and below this incision in a plane just anterior to the thoracic cage so that the skin flaps are as thick as
Fig. 2 The flap has been incised around its periphery and raised from below up by separating the deep surface of the muscle from the posterior rectus sheath after transecting the muscle distally. The superior epigastric vessels are clearly displayed at the upper end of the flap as it is elevated.
Fig. 3 The mobilised flap is transposed through 90” to overlie the recipient site as a “trial run”.
possible. The wound edge is also undermined towards the axilla to receive the buried, de- epithelialised distal end of the flap to create an anterior axillary fold (Fig. 4).

288 BRITISH JOURNAL OF PLASTIC SURGERY
Fig. 4 The flap is then rotated through 90” into the recipient site to allow closure of the donor site. The distal and more proximal parts of the flap are “de-epithelialised” as required before the recipient site is closed.
The donor site is closed with 3/O nylon interrupted sutures in one layer which includes the skin, subcutaneous fat and the remaining lateral and medial edges of the anterior rectus sheath. No drainage tubes have been needed because of the relatively avascular plane of dissection.
Insetting of Flap
The distal and medial ends of the flap are de- epithelialised and buried under the extremities of the wound on the chest wall to create an anterior axillary fold laterally and to increase the cleavage medially. This is usually done by first burying the ends of the flap and marking the junction of the buried and exposed portions of the flap before de-epithelialising the parts to be left buried.
The transposition of the flap into the recipient position produces a large prominent dog-ear on the upper edge of the flap close to the medial end. This is de-epithelialised over a triangular area and buried by direct approximation of the wound edges.
Postoperative Care A firm gauze and elastoplast dressing is applied. The dressing is changed the following day to check the viability of the skin flaps and to exclude the existence of any haematoma. The patient is usually discharged from hospital on the third post-operative day wearing a brassiere over the gauze and elastoplast dressing. Sutures are removed two weeks later.
Discussion
The final aesthetic result has been better than that produced by other methods of reconstruction including the latissimus-dorsi musculocutaneous flap technique (Figs. 5, 6). The operating time has been considerably less. No inter-operative change of position of the patient is required. Much of the dissection in raising the flap involves relatively avascular planes so that blood loss is minimal and transfusion has not been necessary in any case. The viability of the flap has never been in doubt; this is easily confirmed at operation by noting the free bleeding from the de-epithelialised surfaces and the transected muscle ends.
No silicone or other prosthetic implant has been necessary. The rectus abdominis muscle provides sufficient bulk for an adequately large breast with a natural consistency to palpation (Figs. 7, 8). In one case a reduction of a very large opposite breast was required to achieve better symmetry. Skin sensation to touch in every case has been normal over the medial third of the new breast skin, present but diminished over the central part and lost over the lateral part of the flap. This is a further considerable advantage as all patients have volunteered that this contributes to their satisfaction with the results. They have all identified it as being “part of them” and this has added to their sexual and social confidence.
After a follow-up now of more than 1 year in the first case there is no evidence of any muscle atrophy and the retention of sensation to the overlying skin would suggest that some muscle innervation has been retained through the neurovascular pedicle. Should muscle atrophy occur it may well be masked by the normal involutional atrophy of the other breast. In any case the implantation of a silicone prosthesis would be a relatively simple procedure should the discrepancy in size prove troublesome.

POST-MASTECTOMY BREAST RECONSTRUCTION 289
Fig. 6 Postoperative view, right breast
r Fig. 8 Postoperative view following reconstruction with a 7 rectus abdominis musculocutaneous island flap without a
silicone implant. The patient did not request a nipple reconstruction.

290 BRITISH JOURNAL OF PLASTIC SURGERY
The donor site scar is represented by an upper para-median abdominal scar and a degree of contour depression in the area. It was however acceptable to all the patients and to the surgeon. Indeed some of the patients expressed some degree of pleasure from the tightening of the upper abdominal wall.
The technique can be used whatever the site and direction of the previous mastectomy scar, although a transverse mastectomy scar is preferable and gives a better result. The neurovascular bundle is deep to the thoracic cage and is therefore well protected. The axial vessels are large and easily displayed as the flap is folded upwards. No sharp dissection is required: this contributes to the safety of the procedure and reduces the operation time. This technique could well provide a rapidly and easily obtainable free flap with relatively large vessels for anastomosis if the bulk of it could be accommodated at the recipient site.
A delayed primary or early secondary reconstruction is the method of choice. It is felt that there is no need for women to suffer the torment resulting from an amputated breast for prolonged periods of time. The sooner the patient is rehabilitated the more easily she is rehabilitated. Nevertheless it may be important that the patient should see the effect of the ablative surgery and the problem that the reconstructive surgeon has to deal with, so that she can appreciate more the achievements of the reconstructive surgery and accept more readily the inevitable imperfections. The patient should not be reassured by the ablative surgeon in such a way that her expectations from reconstructive surgery become unrealistic.
The Author
Thomas H. Robbins, FRCS, FRCSEd, Suite 3, Southland Centre, Cheltenham 3192, Victoria, Australia.





























