Embed Size (px)
Citation preview

1
Post-Acute COVID-19 Syndrome and the
Lung
Pulmonary Symposium
Robert G. Penn, M.D., FACP, FSHEA, FIDSA
Healthcare Epidemiologist and ID Specialist
Medical Director of Healthcare Epidemiology and Infection Prevention
Methodist Hospital
Infectious Diseases Associates, PC
March 12, 2021
There are no conflicts of interest relevant to this
presentation to report.
Slides presented are my own and those modified
and referenced from various experts.
The content in this presentation is being made available for
informational and educational purposes only. This content is
provided on the understanding that it does not constitute
medical or other professional advice or services. Always work
with a qualified healthcare practitioner when making changes
to your medication, diet or overall healthcare plan.

2
The Story…
The Story…
The Story…
CHARACTERS
SETTING
PLOT
CONFLICT
RESOLUTION

3
The Story…
CHARACTERS
SETTING
PLOT
CONFLICT
RESOLUTION
The Story…
CHARACTERS
SETTING
PLOT
CONFLICT
RESOLUTION
The Story…
CHARACTERS
SETTING
PLOT
CONFLICT
RESOLUTION

4
The Story…
CHARACTERS
SETTING
PLOT
CONFLICT
RESOLUTION
Objectives and Outline
What do we now understand about acute
COVID-19?
What do we understand about the late
sequelae of post-acute COVID-19?
What can be done to manage post-COVID-19
late sequelae?
Create awareness of a Post-COVID-19 study
for healthcare personnel in the NMHS.
THE FOREWORD

5
--Paul Garner, professor of infectious diseases at Liverpool School of Tropical Medicine
https://blogs.bmj.com/bmj/2020/05/05/paul-garner-people-who-have-a-more-protracted-illness-need-help-to-understand-and-cope-with-the-constantly-shifting-bizarre-symptoms/
--Paul Garner, professor of infectious diseases at Liverpool School of Tropical Medicine
https://blogs.bmj.com/bmj/2020/05/05/paul-garner-people-who-have-a-more-protracted-illness-need-help-to-understand-and-cope-with-the-constantly-shifting-bizarre-symptoms/
“A roller coaster of ill health, extreme emotions, and
utter exhaustion. Although not hospitalized, it has
been frightening and long. The illness ebbs and
flows, but never goes away.”
--Paul Garner, professor of infectious diseases at Liverpool School of Tropical Medicine
https://blogs.bmj.com/bmj/2020/05/05/paul-garner-people-who-have-a-more-protracted-illness-need-help-to-understand-and-cope-with-the-constantly-shifting-bizarre-symptoms/

6
“Riding the coronacoaster of uncertainty”
Lancet Infect Dis. 2020 Jun; 20(6): 629.
THIS STORY BEGINS IN
DECEMBER 2019…

7
THE PROLOGUE
“THE SETUP”
Timeline of the reconstruction and recovery of rSARS-CoV-2
in relation to key events of the COVID-19 pandemic
Modified from Hayden M. SHEA COVID-19 Town Hall, Round 37, January 10, 2021
Timeline of the reconstruction and recovery of rSARS-CoV-2
in relation to key events of the COVID-19 pandemic
Modified from Hayden M. SHEA COVID-19 Town Hall, Round 37, January 10, 2021

8
virological.org/t/novel-2019-coronavirus-genome/319
Timeline of the reconstruction and recovery of rSARS-CoV-2
in relation to key events of the COVID-19 pandemic
Modified from Hayden M. SHEA COVID-19 Town Hall, Round 37, January 10, 2021
AND THEN…

9
Timeline of the reconstruction and recovery of rSARS-CoV-2
in relation to key events of the COVID-19 pandemic
Modified from Hayden M. SHEA COVID-19 Town Hall, Round 37, January 10, 2021
Emma visits the
Women’s Hospital ED
5 Mar
THE BODY
“THE CONFRONTATION”
Case Report
36-year old female presents to the ED with a progressive
illness of nasal congestion, dry cough, headache, and
fever on Day 10 of illness, onset in London (1-2 weeks
before) on March 5, 2020
Medical conditions – include but not limited to
hypothyroidism, hypertension, diabetes mellitus, chronic
obstructive pulmonary disease, and anxiety
Exam shows vital signs -- temperature 101.1°F, pulse
102, respiratory rate 25, BP 139/79, and oxygen
saturation of 80% on room air, rising to 93% on 3L by
nasal cannula, wt 249 lbs, BMI 42.5
Chest X-ray performed

10
Case Report
Admission arranged and Infection Prevention and
Control contacted
Informed that the Health Department declined COVID-19
testing
EMR reviewed
Chest CT scan recommended and performed
11
Case Report
Nasopharyngeal specimen collected for COVID-19 PCR
test
Admitted to acute care with special droplet and contact
precautions
Transport via Isolation Pod….
Sunday Omaha World-Herald. May 17, 2020.
Timeline of the reconstruction and recovery of rSARS-CoV-2
in relation to key events of the COVID-19 pandemic
Modified from Hayden M. SHEA COVID-19 Town Hall, Round 37, January 10, 2021

12
COVID-19 Dashboard by the Center for Systems
Science and Engineering at Johns Hopkins University
U.S. total 28,895,975 - U.S. deaths 522,872 - NE total 202,310; NE deaths 2,112
Global Cases 116,192,227 – Global Deaths 2,582,259
As of March 6, 2021, 8:22 AM
COVID-19 Dashboard by the Center for Systems
Science and Engineering at Johns Hopkins University
U.S. Case Fatality Rate = 1.8% -- NE Case Fatality Rate = 1.0%
Global Case Fatality Rate = 2.2%
As of March 6, 2021, 8:22 AM
WHAT DO WE UNDERSTAND
ABOUT THE VIRUS?

13
2019-Novel Coronavirus – The Basics(2019-nCoV)
What? COVID-19 caused by SARS-CoV-2
Pandemic
Potential to cause severe illness especially in vulnerable patients
2019-Novel Coronavirus – The Basics
What? COVID-19 caused by SARS-CoV-2
Pandemic
Potential to cause severe illness especially in vulnerable patients
How spread?
Droplets (≥5 µ)
Close contact (<6ft >10 min.)
Aerosols (<5 µ)
Fomite
Asymptomatic/presymptomatic
2019-Novel Coronavirus – The Basics
What? COVID-19 caused by SARS-CoV-2
Pandemic
Potential to cause severe illness especially in vulnerable patients
How spread?
Droplets (>5 µ)
Close contact (<6ft >10 min.)
Aerosols (<5 µ)
Fomite
Asymptomatic/presymptomatic
Incubation Period? 2-14 days (median 4 to 5 days)

14
Teaching Points
COVID-19 is unprecedented, unpredictable, and highly
transmissible.
https://timesofindia.indiatimes.com/life-style/spotlight/beer-brand-corona-is-willing-to-pay-15-million-to-change-the-name-of-coronavirus/articleshow/73928431.cms
Copyrights apply

15
Spike (S) protein binds with high affinity to the angiotensin-converting
enzyme 2 (ACE2) receptor
ACE2 is expressed in type II alveolar cells and in most organs
Protease activation is required for entry into the human host cell
https://www.genetex.com/Research/Overview/infectious_diseases/SARS-CoV-2
Receptors for SARS-CoV-2 Present in
Wide Variety of Human Cells
Baraniuk C. TheScientist. April 29, 2020.
Human cell types within corresponding organs that express the genes for both ACE2
and CTSL (green dot) or both ACE2 and TMPRSS2 (orange dot).ANNA HUPALOWSKA
Kevin J. Clerkin. Circulation. COVID-19 and Cardiovascular Disease,
Volume: 141, Issue: 20, Pages: 1648-1655, DOI:
(10.1161/CIRCULATIONAHA.120.046941) © 2020 American Heart Association, Inc.
16
WHAT IS THE CLINICAL
PRESENTATION OF COVID-19?
WHAT IS THE CLINICAL
PRESENTATION OF COVID-19?
a.k.a. “The Body Snatcher with Spectrum of Illness”
Course of COVID-19 Infection
Seheult R. MedCram COVID19 #66 Webcast. May 1, 2020.

17
Course of COVID-19 Infection
Seheult R. MedCram COVID19 #66 Webcast. May 1, 2020.
20 to 30% Asymptomatic
Johansson, M, et al. JAMA Network. 2021.

18
Course of COVID-19 Infection
Seheult R. MedCram COVID19 #66 Webcast. May 1, 2020.
Course of COVID-19 Infection
Seheult R. MedCram COVID19 #66 Webcast. May 1, 2020.
Clinical Spectrum of SARS-CoV-2 Infection
Asymptomatic or Presymptomatic Infection: Individuals who test positive for SARS-
CoV-2 using a virologic test (i.e., a nucleic acid amplification test or an antigen test)
but who have no symptoms that are consistent with COVID-19.
Mild Illness: Individuals who have any of the various signs and symptoms of COVID-
19 (e.g., fever, cough, sore throat, malaise, headache, muscle pain, nausea,
vomiting, diarrhea, loss of taste and smell) but who do not have shortness of breath,
dyspnea, or abnormal chest imaging.
Moderate Illness: Individuals who show evidence of lower respiratory disease during
clinical assessment or imaging and who have saturation of oxygen (SpO2) ≥94% on
room air at sea level.
Severe Illness: Individuals who have SpO2 <94% on room air at sea level, a ratio of
arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) <300
mm Hg, respiratory frequency >30 breaths/min, or lung infiltrates >50%.
Critical Illness: Individuals who have respiratory failure, septic shock, and/or multiple
organ dysfunction.
https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/

19
Datta SD, et al. JAMA. December 8, 2020.
What are the symptoms of acute COVID-19?
Fever
Shortness of breath
Cough
Other
Symptoms Associated with COVID-19¹
Fever
Cough
Dyspnea
¹https://www.cdc.gov/coronavirus/2019-nCoV/hcp/clinical-criteria.html
20
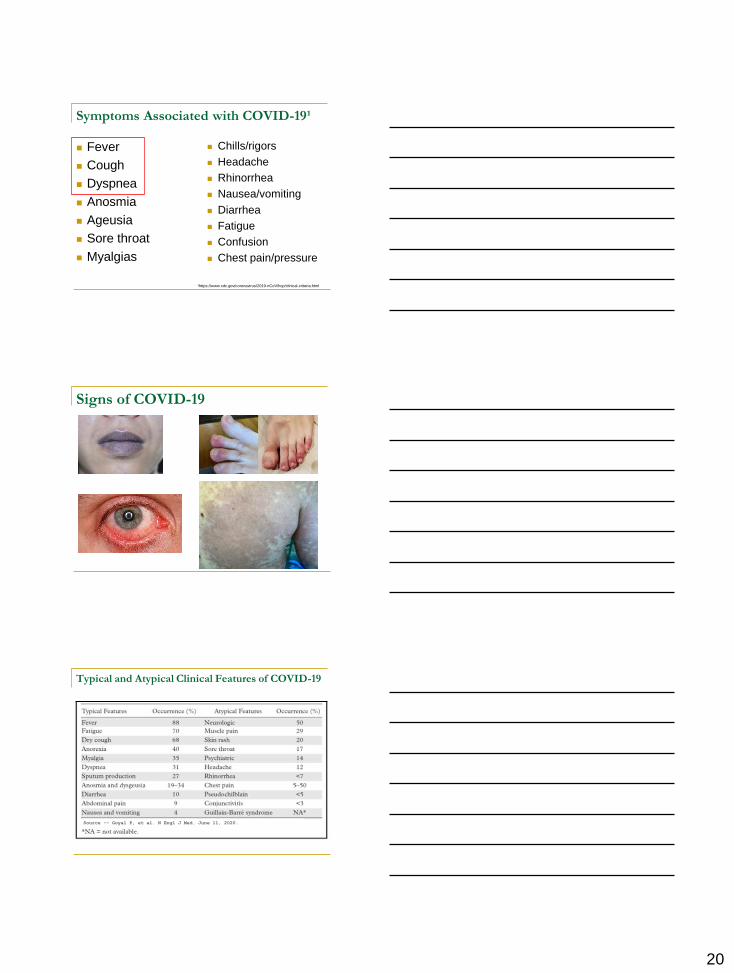
Symptoms Associated with COVID-19¹
Fever
Cough
Dyspnea
Anosmia
Ageusia
Sore throat
Myalgias
Chills/rigors
Headache
Rhinorrhea
Nausea/vomiting
Diarrhea
Fatigue
Confusion
Chest pain/pressure
¹https://www.cdc.gov/coronavirus/2019-nCoV/hcp/clinical-criteria.html
Signs of COVID-19
Typical and Atypical Clinical Features of COVID-19
Source -- Goyal P, et al. N Engl J Med. June 11, 2020.

21
Teaching Points
COVID-19 is unprecedented, unpredictable, and highly
transmissible.
COVID-19 causes multi-system disease.
BEWARE OF THE
VULNERABLE
Underlying conditions among adults
hospitalized with COVID-19

22
Underlying conditions among adults
hospitalized with COVID-19
Prevalence of underlying conditions = 89.3%
Older Adults at Risk for COVID-19
https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/older-adults.html
Copyrights apply

23
Teaching Points
COVID-19 is unprecedented, unpredictable,
and highly transmissible.
COVID-19 causes multi-system disease.
Age and certain pre-existing medical
conditions make patients more vulnerable to
severe COVID-19 and a fatal outcome.
PATIENTS WITH PERSISTENT
SYMPTOMS
Patients with persistent symptoms…Various terms used…
Long-COVID
Post-COVID syndrome
Post-acute COVID-19 syndrome
Late sequelae of COVID-19
COVID Long haulers

24
Patients with persistent symptoms…Various terms used…and [PUBMED]
Long-COVID [2020-50; 2021-64]
Post-COVID syndrome [-94; -55]
Post-acute COVID-19 syndrome [-8; -16]
Late sequelae of COVID-19 [-263; -63]
COVID Long-haulers [-8; -4]
Chronic COVID syndrome [-10, -17]
[Range: 8 to 263 in 2020 and 4 to 64 in 2021]
March 7, 2021
Criteria for Post-COVID
Currently, there is no consensus on the case
definition for post-acute COVID-19 syndrome,
and no specific time frame has been established
to define late sequelae of COVID-19
However, the Centers for Disease Control and
Prevention (CDC) has proposed Post-COVID as
sequelae that extend beyond 4 weeks after
initial infection
https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/
Criteria for Long-COVID per NICE
Acute COVID-19: symptoms of COVID-19 for up
to 4 weeks following the onset of illness
Ongoing symptomatic COVID-19: symptoms
of COVID-19 from 4 to 12 weeks following the
onset of illness
Post-COVID-19: symptoms that develop during
or after COVID-19, continue for ≥ 12 weeks, not
explained by an alternative diagnosis
https://www.nice.org.uk/guidance/ng188

25
Biomedical and life sciences journal literature citations/abstracts*
*March 7, 2021
2020 - 2,627
- 686
2019-4
3,050 results
Biomedical and life sciences journal literature citations/abstracts*
*March 7, 2021
2020 - 5
- 2
7 results
Post-acute COVID-19 Pulmonary Complications
idsociety.org/covid-19-real-time-learning-network/disease-manifestations-complications/pulmonary-manifestations/
26
COVID-19 LungOverview
PulmonaryAdvisor 3/10/2020
“The extent and severity of the long term respiratory
complications of COVID-19 infection remain to be seen,
but emerging data indicate that many patients
experience persistent respiratory symptoms months
after their initial illness…
To summarize, persistent respiratory complications
following COVID-19 may cause substantial population
morbidity, and optimal management remains unclear.
Prospective studies are under way to evaluate these
complications further and to identify people at greatest
risk….”
Fraser E. BMJ. August 3, 2020.

27
Patient population: 172 former COVID-19 patients at a Shenzen, China, hospital who underwent high
resolution computed tomography of the thorax and pulmonary function tests at a follow-
up clinic visit 3 months after hospital discharge.
The median patient age was 47.5 (IQR 28-67) years.
The median duration from hospital discharge to radiological and pulmonary function test
was 90 (IQR 88-95) days.
Patient population: 172 former COVID-19 patients at a Shenzen, China, hospital who underwent high
resolution computed tomography of the thorax and pulmonary function tests at a follow-up
clinic visit 3 months after hospital discharge.
The median patient age was 47.5 (IQR 28-67) years.
The median duration from hospital discharge to radiological and pulmonary function test
was 90 (IQR 88-95) days.
Conclusion:
Of the COVID-19 survivors, 6.4% still present pulmonary function abnormality
three month after discharge, which did not vary by disease severity during
hospitalization. 85.9% patients had abnormalities on chest CT, with fibrous
stripes and ground glass opacity as the most common pattern.

28
Teaching Points
COVID-19 is unprecedented, unpredictable, and highly
transmissible.
COVID-19 causes multi-system disease.
Age and certain pre-existing medical conditions make
patients more vulnerable to severe COVID-19 and a fatal
outcome.
There is a high prevalence of residual chest CT
abnormalities in post COVID patients and this might
progress to pulmonary fibrosis, especially in severe cases.
Copyrights apply
Case Study Presentation
29-year-old female admitted with a progressive cough and fever on
January 31, 2021
History of developing fatigue and body aches the week of Christmas
Diagnosed with COVID-19 (so now ~6 weeks after onset)
Treated with monoclonal antibody (bamlanivimab) on approximately
day 3 or 4 of her illness
She stays in bed for the most part of ~10 days
Back to work -- city mail carrier, ambulating up to 6 miles a day
Subsequently develops a progressive cough, visits the ED, and is
diagnosed with pneumonia January 15, and treated with a 5-day
course of oral Levaquin

29
Case Study Presentation
She had no significant improvement, & developed diarrhea
Started having fever, and started taking acetaminophen regularly,
followed by sweats
Cough was progressive and dyspnea with coughing on exertion
Developed ongoing headache
Seen in the emergency room on January 29, into the early morning
hours of January 30, for further evaluation of her ongoing cough
CTA of the chest and pulmonary arteries performed (“no acute
process”)
Notes her symptoms-fever and post-occipital headache-associated
with her autoimmune cholangitisGI consulted for
recommendationsrecommend a course of oral ciprofloxacin and
metronidazoledischarged from the emergency room
What was "the clue everyone missed"?

30
CTA Chest Pulmonary Arteries-1/29
FINDINGS:
There is no filling defect in the main, segmental or subsegmental pulmonary
arteries to suggest a pulmonary embolus. There is no thoracic aortic
aneurysm or dissection. There is no pleural or pericardial effusion.
There is groundglass opacity scattered in the right upper lobe to a lesser
degree left upper lobe as well as the lingula and right middle lobe. Findings
suggest multifocal pneumonia/COVID. There is no hilar, mediastinal or
axillary lymphadenopathy. Images to the upper abdomen show
pneumobilia.
IMPRESSION:
No CT evidence for pulmonary embolus.
Scattered areas of bilateral groundglass opacity from multifocal
pneumonia/COVID.

31
CTA Chest Pulmonary Arteries-1/29
FINDINGS:
There is no filling defect in the main, segmental or subsegmental pulmonary
arteries to suggest a pulmonary embolus. There is no thoracic aortic
aneurysm or dissection. There is no pleural or pericardial effusion.
There is groundglass opacity scattered in the right upper lobe to a lesser
degree left upper lobe as well as the lingula and right middle lobe. Findings
suggest multifocal pneumonia/COVID. There is no hilar, mediastinal or
axillary lymphadenopathy. Images to the upper abdomen show
pneumobilia.
IMPRESSION:
No CT evidence for pulmonary embolus.
Scattered areas of bilateral groundglass opacity from multifocal
pneumonia/COVID.
32
What is ground-glass opacity (GGO)?
Descriptive term referring to an area of increased attenuation in
the lung on computed tomography (CT) with preserved bronchial
and vascular markings
What is ground-glass opacity (GGO)?
Descriptive term referring to an area of increased attenuation in
the lung on computed tomography (CT) with preserved bronchial
and vascular markings
It is a non-specific sign with a wide etiology including infection,
chronic interstitial disease and acute alveolar disease
What is ground-glass opacity (GGO)?
Descriptive term referring to an area of increased attenuation in
the lung on computed tomography (CT) with preserved bronchial
and vascular markings
It is a non-specific sign with a wide etiology including infection,
chronic interstitial disease and acute alveolar disease
Ground glass opacification is also used in chest radiography to
refer to a region of hazy lung radiopacity, often fairly diffuse, in
which the edges of the pulmonary vessels may be difficult to
appreciate

33
What is ground-glass opacity (GGO)?
Descriptive term referring to an area of increased attenuation in
the lung on computed tomography (CT) with preserved bronchial
and vascular markings
It is a non-specific sign with a wide etiology including infection,
chronic interstitial disease and acute alveolar disease
Ground glass opacification is also used in chest radiography to
refer to a region of hazy lung radiopacity, often fairly diffuse, in
which the edges of the pulmonary vessels may be difficult to
appreciate
The use of the term ground glass derives from the industrial
technique in glassmaking whereby the surface of normal glass is
roughened by grinding it
Copyrights apply
Copyrights apply

34
Case Study Presentation
Symptoms continued to progress and, on January 31, she felt very
chilled and had significant facial flushing and checked her temperature
= 103 F°
Presented to the emergency room again late that evening
Laboratory tests showed mildly elevated inflammatory markers and
LFTs
CT scan of the abdomen and pelvis with contrast is completed
Rx IV levofloxacin in the emergency room, and admitted for treatment
of community-acquired pneumonia and Rx doxycycline
Continues to have fevers with temperatures up to 102.2 F° and
increased watery diarrhea, with episodes each time she is up to urinate
On day #3 of hospitalization an Infectious Disease Consultation is
requested
Case Study Presentation
PAST MEDICAL HISTORY
MEDICAL ILLNESSES: Antiphospholipid antibody syndrome,
autoimmune cholangitis, depression, history recurrent HSV-1
labialis
OPERATIONS: Laparoscopic cholecystectomy, multiple
ERCPs, tonsillectomy and adenoidectomy
MEDICATIONS: Hydroxychloroquine, mycophenolate mofetil,
mirtazapine, risperidone
ALLERGIES: AUGMENTIN causes rash, fever. CEFEPIME
causes rash. SULFA causes rash. ERTAPENEM causes
anaphylaxis
Case Study Presentation
FAMILY HISTORY
Mother has asthma
SOCIAL HISTORY
Married to her spouse who is her wife
Works as a mail carrier, doing a lot of physical activity, often
outdoors
She denies any significant travel history, and denies ever being out
of the Midwest region; no unusual hobbies
3 dogs at home that sleep in bed at night, a French Bulldog, a
Chihuahua/Terrier mix, and a Labrador/Doberman mix
Denies any tobacco or alcohol use
No illicit drug use

35
Case Study Presentation
Double quotidian fever pattern noted
Case Study Presentation
Frequent dry cough, exacerbated by deep breathing,
talking, and activity
Appetite is diminished and some nausea with
posttussive vomiting episodes
Diarrhea associated with antibiotics and denies
abdominal pain or cramping

36
Case Study PresentationPhysical Exam
29-year-old Caucasian female who is well-developed, well-nourished, and in
no acute distress
VITAL SIGNS: At 12:23 today, temperature 102.2 F°, pulse 104,
respirations 18, blood pressure 110/69, oxygen saturations 96% on room air
Height is 65.1 cm, weight is 100 kg (BMI = 36.7 kg/m²)
HEENT: Herpetic lesions on the upper and lower lips
RESPIRATORY: Lungs with diminished bibasilar breath sounds, right
greater than left. Breathing appeared nonlabored
CARDIOVASCULAR: Heart sounds have a regular rate and rhythm,
without murmur, rub or gallop
ABDOMEN: Soft, nondistended, nontender, with positive bowel sounds and
no palpable mass or hepatosplenomegaly
EXTREMITIES: Without edema or synovitis
Case Study Presentation
Laboratory tests:
WBC 4,800
Lymphocytes 800
Hemoglobin 12.7
Platelets 156,000
Chemistry: Glucose 96, sodium 134, potassium 4.2, BUN 3,
creatinine 0.63, calcium 8.5, total protein 5.8, albumin 3.3,
globulin 2.5, total bili 0.3, alk phos 200, ALT 54, AST 20, LD 262
Lactate 1.7
hsCRP 19.1
ESR 22
Procalcitonin 0.18
CT of Abdomen/Pelvis with contrast
IMPRESSION:
Progressive infiltrate in the lingula and right
middle lobe since chest CT of 01/29/2021.
No focal inflammatory process or acute
finding in the abdomen or pelvis.

37
Case Study Presentation
IV levofloxacin readded and PO doxycycline continued
Fever and dry, hacky cough persists
Case Study Presentation Diagnostic Test/Procedure?

38
Sutton’s Law
Sutton’s Law
Case Study Presentation
OPERATIVE PROCEDURE
Exploratory left video-assisted thoracoscopy
with diagnostic left lower lobe wedge biopsies
x2.

39
Histopathology
Diagnosis
Parts A and B "Lung, left lower lobe, wedge biopsies
Acute fibrinous and organizing pneumonia (AFOP).
Organizing and recanalized thrombi/thromboemboli in
multiple muscular pulmonary arteries.
HistopathologyReview by Dr. Tao Huang at University of Michigan
Sections of both lung wedge biopsies are similar in showing a
patchy air-space-filling process. The air space exudate comprises a
combination of abundant fibrin, variably scant amount of organizing
spindle cells and a few chronic inflammatory cells, features
diagnostic of acute fibrinous and organizing pneumonia (AFOP).
The accompanying alveolar interstitium is slightly thickened by a
mild chronic inflammatory infiltrate composed of many mononuclear
inflammatory cells. The degree of the interstitial changes fall short
of a definitive diagnosis of chronic interstitial pneumonia based on
this sample alone and at least part of the interstitial changes can be
explained by the affiliated AFOP. Fibrin thrombi are noted in
multiple small pulmonary muscular arteries, some of which are also
associated with recannulization.
Diagnoses
Post-acute COVID-19 late sequelae with acute fibrinous and
organizing pneumonia (AFOP)
History of COVID-19 infection December 2020
Recurrent herpes simplex virus labialis
Immunocompromised host with autoimmune cholangitis
Antiphospholipid antibody syndrome. Contributing to above findings
of recanalized thrombi/thromboemboli in multiple muscular
pulmonary arteries.
Multiple antibiotic allergy syndrome, with ERTAPENEM,
AUGMENTIN, CEFEPIME, and SULFONAMIDES
History of depression

40
Treatment
Course of Valtrex completed
Levofloxacin and doxycycline discontinued
Rx IV methylprednisolone and transitioned to
oral Prednisone and discharged
ORGANIZING PNEUMONIA
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7509945/pdf/bmjresp-2020-000724.pdf
ABSTRACTReviews of COVID-19 CT imaging along with postmortem lung biopsies and autopsies indicate that the majority of patients with COVID-19 pulmonary involvement have secondary organising
pneumonia (OP) or its histological variant, acute fibrinous and organising pneumonia, both well-
known complications of viral infections. Further, many publications on COVID-19 have debated
the puzzling clinical characteristics of ‘silent hypoxemia’, ‘happy hypoxemics’ and ‘atypical ARDS’, all features consistent with OP. The recent announcement that RECOVERY, a
randomised controlled trial comparing dexamethasone to placebo in COVID-19, was terminated
early due to excess deaths in the control group further suggests patients present with OP given
that corticosteroid therapy is the first-line treatment. Although RECOVERY along with othercohort studies report positive effects with corticosteroids on morbidity and mortality of COVID-19,
treatment approaches could be made more effective given that secondary OP often requires
prolonged duration and/or careful and monitored tapering of corticosteroid dose, with ‘pulse’
doses needed for the well-described fulminant subtype. Increasing recognition of this diagnosis
will thus lead to more appropriate and effective treatment strategies in COVID-19, which may lead to a further reduction of need for ventilatory support and improved survival.

41
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7509945/pdf/bmjresp-2020-000724.pdf
ABSTRACTReviews of COVID-19 CT imaging along with postmortem lung biopsies and autopsies indicate that the majority of patients with COVID-19 pulmonary involvement have secondary organising
pneumonia (OP) or its histological variant, acute fibrinous and organising pneumonia, both well-
known complications of viral infections. Further, many publications on COVID-19 have debated
the puzzling clinical characteristics of ‘silent hypoxemia’, ‘happy hypoxemics’ and ‘atypical ARDS’, all features consistent with OP. The recent announcement that RECOVERY, a
randomised controlled trial comparing dexamethasone to placebo in COVID-19, was terminated
early due to excess deaths in the control group further suggests patients present with OP given
that corticosteroid therapy is the first-line treatment. Although RECOVERY along with othercohort studies report positive effects with corticosteroids on morbidity and mortality of COVID-19,
treatment approaches could be made more effective given that secondary OP often requires
prolonged duration and/or careful and monitored tapering of corticosteroid dose, with ‘pulse’
doses needed for the well-described fulminant subtype. Increasing recognition of this diagnosis
will thus lead to more appropriate and effective treatment strategies in COVID-19, which may lead to a further reduction of need for ventilatory support and improved survival.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7509945/pdf/bmjresp-2020-000724.pdf
CONCLUSION
It is our view that, based on the similar clinical presentations, radiographic abnormalities, overlapping yet supportive histopathological patterns on autopsy in conjunction with studies
reporting that patients are ‘steroid-responsive’, early COVID-19 respiratory disease is better
understood primarily as ‘SARS-CoV-2 induced secondary OP’. Given this likely high prevalence
of OP, AFOP or both in early COVID-19, a concern is that the increasingly adoptedRECOVERY trial protocol (6mg dexamethasone daily for up to 10 days) may be insufficient
given that treatment of secondary OP often requires higher doses, prolonged duration of
treatment, and a careful and monitored tapering. Thus, additional studies comparing
corticosteroid type, dosing and duration should be conducted along with the use of other
immunosuppressive agents. Initial and maintenance corticosteroid dosing should be similar to that recommended to treat COP, although patients with secondary OP typically require a shorter
duration. Clinicians should also be aware of the higher ‘pulse’ doses required in the successful
treatment of fulminant cases of OP or AFOP. Although chronic macrolide therapy has
demonstrated efficacy as a steroid-sparing agent in the treatment of COP, there are insufficient data to support a recommendation for use in COVID-19 secondary OP.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7509945/pdf/bmjresp-2020-000724.pdf
CONCLUSION
It is our view that, based on the similar clinical presentations, radiographic abnormalities, overlapping yet supportive histopathological patterns on autopsy in conjunction with studies
reporting that patients are ‘steroid-responsive’, early COVID-19 respiratory disease is better
understood primarily as ‘SARS-CoV-2 induced secondary OP’. Given this likely high prevalence
of OP, AFOP or both in early COVID-19, a concern is that the increasingly adoptedRECOVERY trial protocol (6mg dexamethasone daily for up to 10 days) may be insufficient
given that treatment of secondary OP often requires higher doses, prolonged duration of
treatment, and a careful and monitored tapering. Thus, additional studies comparing
corticosteroid type, dosing and duration should be conducted along with the use of other
immunosuppressive agents. Initial and maintenance corticosteroid dosing should be similar to that recommended to treat COP, although patients with secondary OP typically require a shorter
duration. Clinicians should also be aware of the higher ‘pulse’ doses required in the successful
treatment of fulminant cases of OP or AFOP. Although chronic macrolide therapy has
demonstrated efficacy as a steroid-sparing agent in the treatment of COP, there are insufficient data to support a recommendation for use in COVID-19 secondary OP.

42
Histological response to acute lung injury
Diffuse alveolar damage (DAD)
Organizing pneumonia (OP)
Acute fibrinous organizing pneumonia (AFOP)
Eosinophilic pneumonia (EP)
Not yet described in COVID19
OP¹ versus AFOP²
Alveolar epithelial injury causes leakage of
coagulative proteins, which accumulate fibrin
due to diminished fibrinolytic activity
¹Organizing pneumonia
²Acute fibrinous organizing pneumonia
OP versus AFOP
Alveolar epithelial injury causes leakage of
coagulative proteins, which accumulate fibrin
due to diminished fibrinolytic activity
In OP, fibroblast activation and proliferation
then follow, producing a connective tissue
matrix in the alveolus and ducts
43
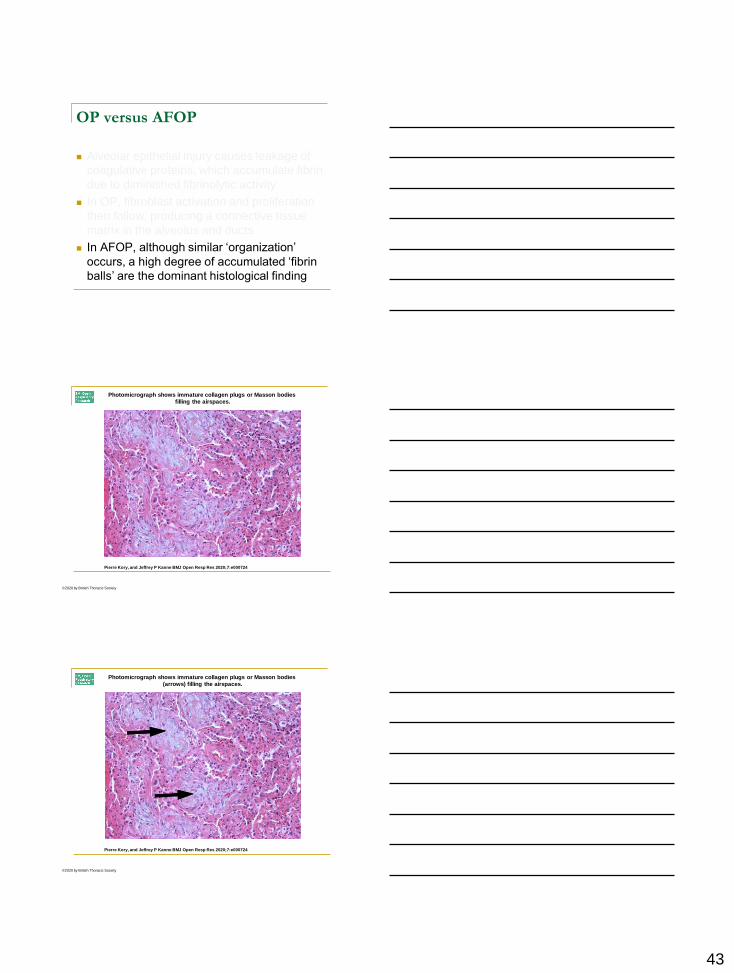
OP versus AFOP
Alveolar epithelial injury causes leakage of
coagulative proteins, which accumulate fibrin
due to diminished fibrinolytic activity
In OP, fibroblast activation and proliferation
then follow, producing a connective tissue
matrix in the alveolus and ducts
In AFOP, although similar ‘organization’
occurs, a high degree of accumulated ‘fibrin
balls’ are the dominant histological finding
Photomicrograph shows immature collagen plugs or Masson bodies
filling the airspaces.
Pierre Kory, and Jeffrey P Kanne BMJ Open Resp Res 2020;7:e000724
©2020 by British Thoracic Society
Photomicrograph shows immature collagen plugs or Masson bodies
(arrows) filling the airspaces.
Pierre Kory, and Jeffrey P Kanne BMJ Open Resp Res 2020;7:e000724
©2020 by British Thoracic Society

44
37-year-old woman with COVID-19 requiring FiO2
of 1.0 delivered via heated humidified
high-flow nasal cannula for 8 days.
Pierre Kory, and Jeffrey P Kanne BMJ Open Resp Res 2020;7:e000724
©2020 by British Thoracic Society
6 days after onset of symptomsPulse Steroids D82 weeks after discharge
Copin C-M, et al. Intensive Care Med. 2020.
Copin C-M, et al. Intensive Care Med. 2020.

45
Teaching Points
COVID-19 is unprecedented, unpredictable, and highly
transmissible.
COVID-19 causes multi-system disease.
Age and certain pre-existing medical conditions make
patients more vulnerable to severe COVID-19 and a fatal
outcome.
There is a high prevalence of residual chest CT
abnormalities in post COVID patients and this might
progress to pulmonary fibrosis, especially in severe cases.
‘Steroid-responsive’ severe COVID-19 respiratory disease
may be better understood primarily as ‘SARS-CoV-2
induced secondary organizing pneumonia.
RESOURCES AND
ADDITIONAL
MANIFESTATIONS OF
LONG-COVID
Long-COVID Syndrome
It’s estimated that 10–30% of cases will
turn into long-COVID, where symptoms
such as dyspnea (shortness of breath),
fatigue, cognitive problems, joint pain,
myalgia, and gastrointestinal and cardiac
issues persist for a month or more
Can happen to anyone who got infected
by SARS-CoV-2, even children, students,
and those who only had mild-to-moderate
Covid-19
It’s 3–6 months and counting, so how
many more months?
The current data is insufficient to
make conclusions
Shin Jie Yong. https://medium.com/microbial-instincts/we-shouldnt-be-surprised-if-long-covid-will-last-for-years-d0c4dd4a3bf

46
Most commonly reported symptoms…
Fatigue
Dyspnea
Cough
Arthralgia
Chest pain
https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects.html
Other reported symptoms include…
Cognitive impairment
Depression
Myalgia
Headache
Fever
Palpitations

47
Less common more serious complications…
Cardiovascular: myocardial inflammation, ventricular
dysfunction
Respiratory: pulmonary function abnormalities
Renal: acute kidney injury
Dermatologic: rash, alopecia
Neurological: olfactory and gustatory dysfunction,
sleep dysregulation, altered cognition, memory
impairment
Psychiatric: depression, anxiety, changes in mood
Datta SD, et al. JAMA. December 8, 2020.

48
https://www.covid19treatmentguidelines.nih.gov/

49
idsociety.org/covid-19-real-time-learning-network/disease-manifestations-complications/post-covid-syndrome/
50
Huang C, et al. The Lancet. January 16, 2021.
Overall, in this large cohort study of 1,733 patients
with COVID-19 assessed 6 months after discharge,
most patients exhibited at least one symptom,
particularly fatigue or muscle weakness, sleep
difficulties, and anxiety or depression. More severely
ill patients had increased risk of pulmonary diffusion
abnormality, fatigue or muscle weakness, and
anxiety or depression. The seropositivity and titers
of the neutralizing antibodies were significantly lower
than at acute phase.
Huang C, et al. The Lancet. January 16, 2021.

51
Overall, in this study of patients with COVID-19 discharged
from the hospital with SARS-CoV-2 RNA clearance
by RT-PCR and interviewed approximately 2 months after
diagnosis, the majority of patients experienced continued
symptoms, with the most common symptoms
being fatigue and dyspnea.
COVID-19 Related Symptoms
The percentages of patients presenting with specific coronavirus disease 2019
(COVID-19)–related symptoms during the acute phase of the disease (left) and at the time of the follow-up visit (right).
Carfi A, et al. JAMA. 2020.

52
Copyrights apply
WHAT CAUSES LONG-COVID
AND HOW SHOULD WE
MANAGE?
Overview of the pathophysiology, symptoms, and
potential treatments involved in long-COVID-19
Shin Jie Yong. https://medium.com/microbial-instincts/we-shouldnt-be-surprised-if-long-covid-will-last-for-years-d0c4dd4a3bf

53
https://www.nice.org.uk/guidance/ng188
https://www.blf.org.uk/support-for-you/long-covid
General Evaluation of Long-COVID
Comprehensive history of the patient's COVID-19 illness
Illness timeline, duration and severity of symptoms
Types and severity of complications
COVID-19 testing results
Any management strategies
Identify modifiable personal lifestyle factors
Laboratory testing is determined by illness severity, prior
abnormal testing during their illness, and current symptoms
54
Focus on Cardiopulmonary Long-COVID Evaluation
Comprehensive history and physical examination
Cardiopulmonary Long-COVID Evaluation
Comprehensive history and physical examination
?ongoing dyspnea (at rest and exertion)
?cough, chest discomfort, pleuritic pain, and wheezing,
orthopnea, chest pain (exertional, positional), peripheral
edema, palpitations, dizziness, orthostasis, and pre-
syncope or syncope
Cardiopulmonary Long-COVID Evaluation
Comprehensive history and physical examination
?ongoing dyspnea (at rest and exertion)
?cough, chest discomfort, pleuritic pain, and wheezing,
orthopnea, chest pain (exertional, positional), peripheral
edema, palpitations, dizziness, orthostasis, and pre-
syncope or syncope
Health screening tools, 6-minute walking test, & Borg
Scale

55
Copyrights apply
Copyrights apply
Copyrights apply

56
Cardiopulmonary Long-COVID Evaluation
Comprehensive history and physical examination
?ongoing dyspnea (at rest and exertion)
?cough, chest discomfort, pleuritic pain, and wheezing,
orthopnea, chest pain (exertional, positional), peripheral
edema, palpitations, dizziness, orthostasis, and pre-
syncope or syncope
Health screening tools, 6-minute walking test, & Borg
Scale
Cardiopulmonary Exercise Test
Copyrights apply
Copyrights apply

57
Cardiopulmonary Long-COVID Evaluation
Comprehensive history and physical examination
?ongoing dyspnea (at rest and exertion)
?cough, chest discomfort, pleuritic pain, and wheezing,
orthopnea, chest pain (exertional, positional), peripheral
edema, palpitations, dizziness, orthostasis, and pre-
syncope or syncope
Health screening tools, 6-minute walking test, & Borg
Scale
Cardiopulmonary Exercise Test
Breathing exercises
Copyrights apply

58
Breath…the creation of human life
Genesis 2:7
-- then the Lord God formed the man of dust from
the ground and breathed into his nostrils the
breath of life, and the man became a living
creature.
Mechanism of Action of Halotherapy*

59
Cardiopulmonary Long-COVID Evaluation
Comprehensive history and physical examination
?ongoing dyspnea (at rest and exertion)
?cough, chest discomfort, pleuritic pain, and wheezing,
orthopnea, chest pain (exertional, positional), peripheral
edema, palpitations, dizziness, orthostasis, and pre-
syncope or syncope
Health screening tools, 6-minute walking test, & Borg
Scale
Cardiopulmonary Exercise Test
Breathing exercises
Sleep hygiene
Copyrights apply
Teaching Points
The COVID-19 pandemic has resulted in a growing
population of individuals with a wide range of persistent
symptoms after acute SARS-CoV-2 infection.
This comprises patients with symptoms that develop during or
after COVID-19, continue for ≥ 12 weeks, and are not explained
by an alternative diagnosis.
Whether the constellation of symptoms represents a new
syndrome unique to COVID-19, or if there is overlap with the
recovery from similar illnesses has not been determined.
There is a growing need for a multi-disciplinary approach to
management of Long-COVID.

60
Upcoming COVID-19 Study
Natural History of Post-Acute COVID-19 Convalescence
Among Healthcare Personnel at NMHS
Invitation to participate will be sent via email and Employee
Connections
Voluntary completion of an 8 to 10 minute anonymous
survey
For those who were diagnosed with COVID-19, addresses
physical/emotional experience of COVID-19 & health
behaviors
For those who were not diagnosed with COVID-19,
addresses emotional response to pandemic & health
behaviors
THE EPILOGUE
“THE RESOLUTION”
61
References Kory P, Kanne JP. SARS-CoV-2 organizing pneumonia: ‘Has there been a
widespread failure to identify and treat this prevalent condition in COVID-
19?’. BMJ Open Resp Res 2020;7:e000724. doi:10.1136/bmjresp-2020-
000724
Copin M-C, Parmentier E, Duburcq T, et al. Time to consider histologic
pattern of lung injury to treat critically ill patients with COVID-19 infection.
Intensive Care Med 2020;46:1124–6.
Beasley MB, Franks TJ, Galvin JR, Gochuico B, Travis WD. Acute fibrinous
and organizing pneumonia: a histological pattern of lung injury and possible
variant of diffuse alveolar damage. Arch Pathol Lab Med. 2002
Sep;126(9):1064-70. doi: 10.1043/0003-
9985(2002)126<1064:AFAOP>2.0.CO;2. PMID: 12204055.
https://www.idsociety.org/covid-19-real-time-learning-network/disease-
manifestations--complications/post-covid-syndrome/
https://www.idsociety.org/covid-19-real-time-learning-network/disease-
manifestations--complications/pulmonary-manifestations/
References Goyal P, Choi JJ, Pinheiro LC, et al. Clinical Characteristics of Covid-19 in New York
City. N Engl J Med 2020;382(24):2372–2374.
Liu Y, Yan LM, Wan L, et al. Viral dynamics in mild and severe cases of COVID-19.
Lancet Infect Dis 2020;20(6):656–657.
Revzin MV, et al. Multisystem Imaging Manifestations of COVID-19, Part 1: Viral
Pathogenesis and Pulmonary and Vascular System Complications. RadioGraphics
2020; 40:1574-1599.
Carfì A, Bernabei R, Landi F; Gemelli Against COVID-19 Post-Acute Care Study
Group. Persistent Symptoms in Patients After Acute COVID-19. JAMA.
2020;324(6):603-605. doi:10.1001/jama.2020.12603
McIntosh, K. Coronavirus disease 2019 (COVID-19): Clinical features. In: UpToDate,
Post, TW (Ed), UpToDate, Waltham, MA, 2021.
Mikkelsen, ME, Abramoff, B. Coronavirus disease 2019 (COVID-19): Evaluation and
management of adults following acute viral illness. In: UpToDate, Post, TW (Ed),
UpToDate, Waltham, MA, 2021.
Yong, S.J. Long-Haul COVID-19: Putative Pathophysiology, Risk Factors, and
Treatments. Preprints 2020, 2020120242 (doi: 10.20944/preprints202012.0242.v1).
References Baraniuk, C. Receptors for SARS-CoV-2 Present in Wide Variety of Human
Cells. TheScientist; April 29, 2020.
Johansson MA, Quandelacy TM, Kada S, et al. SARS-CoV-2 Transmission
From People Without COVID-19 Symptoms. JAMA Netw Open.
2021;4(1):e2035057. doi:10.1001/jamanetworkopen.2020.35057
Brooks JT, Beezhold DH, Noti JD, et al. Maximizing Fit for Cloth and
Medical Procedure Masks to Improve Performance and Reduce SARS-
CoV-2 Transmission and Exposure, 2021. MMWR Morb Mortal Wkly Rep
2021;70:254–257. DOI:
http://dx.doi.org/10.15585/mmwr.mm7007e1external icon

62
THANK YOU FOR YOUR
ATTENTION
Questions or Comments?
https://virologydownunder.com/the-swiss-cheese-infographic-that-went-viral/
63
Defending against COVID-19
This means masks are key. According to a
recent MMWR, if everyone wears a snug-fitting
mask, spread of the virus that causes COVID-19
can be reduced by up to 95%. The fit and
filtration of the mask is also key to preventing the
spread of COVID-19. Wear a mask that fits
snugly over your nose and mouth when in public
settings, stay 6 feet away from others, and avoid
crowds and poorly ventilated indoor spaces.

64
Defending against COVID-19












![Shrinking Lung Syndrome: A Pulmonary Manifestation of ... · scan]) and pulmonary function tests (PFTs). Pulmonary function tests were carried out in our pulmonary function laboratory,](https://img.dokumen.tips/doc/110x75/5f03189c7e708231d40783f1/shrinking-lung-syndrome-a-pulmonary-manifestation-of-scan-and-pulmonary-function.jpg)