Embed Size (px)
Citation preview
Quality Strategic Framework Page 1 of 18
PORTSMOUTH CLINICAL COMMISSIONING GROUP Quality Strategic Framework
1. Introduction and Background
This framework sets out how NHS Portsmouth Clinical Commissioning Group (PCCG) will manage the Clinical Quality agenda from transition to authorisation and beyond.
1.1 There is an expectation that CCG’s will have appropriate constitutional and
governance arrangements along with the relevant capacity and capability to deliver against their duties and responsibilities as they relate to the clinical quality agenda.
1.2 The purpose of this framework is to:
Outline NHS Portsmouth CCG’s approach to clinical quality
Ensure that quality is placed at the heart of the health care the Portsmouth CCG commissions
Ensure that there is a robust link between commissioning and clinical quality to ensure the health needs of the local population (outlined in the Joint Strategic Needs Assessment) are met.
Ensure there are internal systems and processes to provide assurance that NHS Portsmouth CCG is able to discharge its responsibilities.
Set out the accountability arrangements for NHS PCCG and Commissioning Support South (CSS) associated with this agenda.
Provide a basis for contractual quality requirements with providers.
1.3 The Clinical Commissioning Committee is accountable to the NHS Portsmouth CCG Governing Body, and will take overall responsibility for ensuring that robust arrangements are in place to provide assurance on the quality of services commissioned.
2. Scope of the Framework
NHS Portsmouth CCG is responsible for commissioning health services for a population of 215,000 people across the city and has 27 member practices. The geographical area covered by NHS Portsmouth CCG is Portsmouth City as defined by the Portsmouth City Council Local Authority boundaries. NHS Portsmouth CCG (during 2012/13) commissions health care on behalf of the population of Portsmouth from mainly 4 providers, Portsmouth Hospitals NHS Trust, Solent NHS Trust, Care UK (Independent Sector Treatment Centre and Primary Care) and South Central Ambulance Service. Currently this is via a newly establishing Commissioning Support Unit, Commissioning Support South (CSS).The framework acknowledges the importance of the relationship with CSS and local providers and seeks to clarify and contextualise these relationships. It is noted that NHS Portsmouth CCG may use alternative arrangements in the future.
Quality Strategic Framework Page 2 of 18
3. Definition
3.1 Clinical Quality is a framework to ensure that systems and processes are in place
across the CCG for maintaining, improving and safeguarding the quality of care we commission and that this is encouraged and supported.
3.2 It requires clear lines of responsibility and accountability for the overall quality of
clinical care, a comprehensive programme of quality improvement activity and clear policies and procedures aimed at managing risk and identifying and improving performance.
3.3 It requires systematic approaches to support staff to identify strengths and
weaknesses and to readily share learning with others.
4. Quality Agenda
4.1 The White Paper, Equity and Excellence: Liberating the NHS set out how the improvement of healthcare outcomes for all will be the primary purpose of the NHS. This means ensuring that the accountabilities running throughout the system are focused on the outcomes achieved for patients not the processes by which they are achieved. The NHS Outcomes is structured around five improvement domains, which set out the high level national outcomes that the Clinical Commissioning Groups could aim to improve. They focus on:
1. Preventing people from dying prematurely 2. Enhancing quality of life for people living with long term conditions 3. Helping people to recover from episodes of ill health following injury 4. Ensuring that people have a positive experience of care 5. Treating and caring for people in a safe environment and protecting them
from avoidable harm
4.2 The NHS Outcomes Framework is intrinsically linked to the national and local quality agenda which consists of 3 main areas:
Patient Safety including: o Safeguarding o Infection prevention and control o Serious Incidents Requiring Investigation management o Establishing and monitoring Early Warning Systems o Complaints
Clinical Effectiveness including: o Positive patient outcomes o Evidence based practice o Research based practice o Experience and competency based practice
Patient Experience including: o Real time patient and carer experience, inclusive of the diversity of
the population o National and local primary, community and secondary care patient
and staff survey data
Quality Strategic Framework Page 3 of 18
o Complaints and plaudits
4.3 During the NHS Portsmouth CCG transition phase this will be managed through the Commissioning Support Unit – Commissioning Support South. This excludes Adult Safeguarding and Continuing Health Care arrangements already in existence through Integrated Commissioning with Portsmouth City Council.
5. Strategic Framework
5.1 Aim
To ensure that all patients have access to high quality clinical care delivered in a timely and effective way and with regard to the NHS Portsmouth CCG
commissioning plan, which has quality as the organising principle, including patient and public engagement, clinical leadership and focus, promoting equality and diversity, reducing inequalities and encouraging partnership working.
5.2 Strategic Objectives
To ensure that clinical quality, leadership and accountability are clearly understood across the CCG
To ensure that mechanisms are in place and working to provide assurance to the CCG on the quality of local commissioned services
To ensure that any contracts/Memorandum of Understanding’s for commissioning support are clear regarding the CCG approach to clinical quality
To promote an open and transparent culture between the CCG and its providers in which untoward incidents and near misses are reported and investigated, and lessons learnt and shared across the patient pathway
To ensure that learning from complaints, litigation and claims is systematically analysed and disseminated throughout the CCG to improve commissioning processes
To ensure that national guidance from National Commissioning Board, National Institute of Clinical Excellence (NICE) including Quality Standards, the National Quality Board, Care Quality Commission (CQC) and other national bodies is implemented across the CCG
To ensure that national initiatives are implemented across the CCG
To ensure that all CCG professional development programmes reflect principles of clinical quality
To ensure that good practice, ideas, innovations are systematically disseminated across the CCG
To ensure active patient and public engagement, in order to influence CCG decision making
To ensure that patient experience is captured across care pathways and utilised to improve commissioning for quality

Quality Strategic Framework Page 4 of 18
5.3 Local Structures
It is important that the structures developed for Clinical Quality facilitate innovation and individual influence within a framework of shared values and clear direction. The structures should maximise the links between the various working groups and partnership mechanisms operating within and outside NHS Portsmouth CCG, including but not exclusive of:
The Compact arrangement with South Eastern Hampshire CCG and Fareham and Gosport CCG
Local Authority- Portsmouth City Council
Other Clinical Commissioning Groups
Providers
Portsmouth Health and Wellbeing Board
Adult Safeguarding Board
Children’s Safeguarding Board
Children’s Trust Board
Safer Portsmouth Partnership Board
The structures are designed to produce maximum efficiency, through operating clear and effective communication systems, avoiding duplication of effort and being explicit about accountability and reporting arrangement.
The NHS Portsmouth CCG Governance Model (Fig 1) identifies the range of stakeholders and groups that will work with the Clinical Commissioning Committee. These groups are supported by the work of teams and individuals within the CCG and wider health economy.
Fig 1
Quality Strategic Framework Page 5 of 18
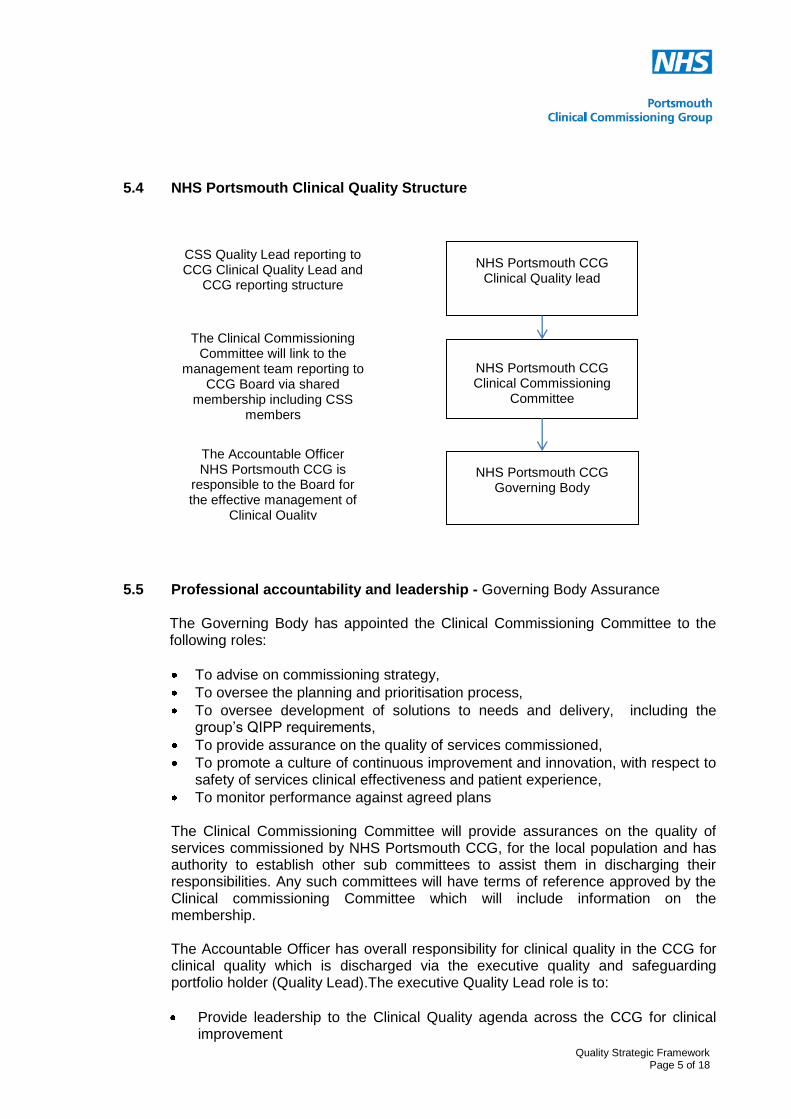
5.4 NHS Portsmouth Clinical Quality Structure
5.5 Professional accountability and leadership - Governing Body Assurance
The Governing Body has appointed the Clinical Commissioning Committee to the following roles:
To advise on commissioning strategy,
To oversee the planning and prioritisation process,
To oversee development of solutions to needs and delivery, including the group’s QIPP requirements,
To provide assurance on the quality of services commissioned,
To promote a culture of continuous improvement and innovation, with respect to safety of services clinical effectiveness and patient experience,
To monitor performance against agreed plans The Clinical Commissioning Committee will provide assurances on the quality of services commissioned by NHS Portsmouth CCG, for the local population and has authority to establish other sub committees to assist them in discharging their responsibilities. Any such committees will have terms of reference approved by the Clinical commissioning Committee which will include information on the membership. The Accountable Officer has overall responsibility for clinical quality in the CCG for clinical quality which is discharged via the executive quality and safeguarding portfolio holder (Quality Lead).The executive Quality Lead role is to:
Provide leadership to the Clinical Quality agenda across the CCG for clinical improvement
NHS Portsmouth CCG Clinical Quality lead
NHS Portsmouth CCG Clinical Commissioning
Committee
NHS Portsmouth CCG Governing Body
CSS Quality Lead reporting to CCG Clinical Quality Lead and
CCG reporting structure
The Clinical Commissioning Committee will link to the
management team reporting to CCG Board via shared
membership including CSS members
The Accountable Officer NHS Portsmouth CCG is
responsible to the Board for the effective management of
Clinical Quality
Quality Strategic Framework Page 6 of 18
Ensure that the CCG is able to meet its statutory responsibilities
Hold the service provided by the CSS to account for the delivery of timely, accurate information, robust systems and processes for monitoring providers’ contract quality criteria
Approve the systems and process that will be put in place with provider quality contract management
5.6 Role of Commissioning Support South (CSS)
Commissioning Support South is the local service provider from which the CCG may buy the elements of commissioning support they require. The CSS would through a “Service Level Agreement” provide a support service for the CCG in the area of quality and also support the efficient working of the clinical quality processes. The service to be provided by the CSS will include:
Clinical expertise and experience to synthesise qualitative and quantitative quality information from a broad spectrum of sources, in relation to the quality of services provided from local healthcare providers
Established relationship management with local providers with regard to quality performance
Appropriate and relevant reports via the CCG Quality Lead to the Clinical Commissioning Committee, the NHS Portsmouth CCG Governing Body as required and other sub-groups regarding providers’ compliance against the quality of patients care requirements in NHS Provider contracts (including clinical incidents or errors, adverse incidents and complaints)
Providing high quality information to monitor clinical care for the commissioned services for the CCG, including the development of Early Warning Systems for assurance of provider organisations
Work with local, regional and national networks to deliver the quality agenda, for example Links (Health watch)
In conjunction with the CCG and the providers, implement monthly provider quality meetings to review provider clinical quality performance against agreed quality contract requirements
Monitor Serious Incidents Requiring Investigation (SIRI) with regard to CCG requirements; manage day to day reporting and coordination from providers. Ensure timeframes and deadlines for SIRI RCA submission are met via provider
Governing Body
Accountable Officer
NHS Portsmouth CCG
Clinical Quality Lead
NHS Portsmouth CCG
Clinical Quality Lead In CSS
Quality Strategic Framework Page 7 of 18
contracts and supply for clinical review. Ensure learning from SIRI across pathways is disseminated
Ensure reporting to the National Reporting and Learning System is undertaken by providers, or CSS as necessary on behalf of the CCG
Work with Providers to ensure continued patient safety and risk management processes are in place so that risk of harm for patients is reduced to a minimum
Oversee that Providers document and highlight themes and lessons from incidents and embed these lessons into service developments and improvement
Work within the Operating Framework, Better Care Better Value metrics, and NHS Outcomes Framework, drawing on clinical guidance from national bodies alongside local priorities to ensure that the Provider is delivering against latest guidance/best practice
Agree in year trajectories in line with emerging national and local guidance and ensure the Provider is measuring and meeting the set trajectories, enabling peer review, where possible.
Contractual arrangements will ensure clinical quality systems and processes are specified for each provider. The system and processes including monthly clinical quality review meetings with each provider will address under-performance against quality requirements as appropriate.
6. Role of member practices
Ensure engagement in CCG processes and mechanisms
Provide real time patient information to Governing Body members to influence decision making
Offer real time quality feedback from patients on commissioned services.
7. Statutory Compliance
External scrutiny of the CCG;
The reconfiguration of NHS South of England to the National Commissioning Board is expected to result in the devolvement of key Clinical Quality responsibility to the Local Commissioning Board via local offices. The exact nature of the CCG reporting requirements is not yet clear. It could involve annual reporting of progress against CCG Clinical Quality development plan to the local commissioning board.
As reforms continue to develop, national drivers for compliance will be adhered to (to take into account changes post 2013/14)
The Care Quality Commission may review the CCG’s clinical quality arrangement from time to time
8. CCG Contracts with provider organisations
8.1 Any contract the NHS Portsmouth CCG has will be expected to provide a high
quality service.
Commissioning Support South CSS Quality Support will be determined by the CCG and clear reporting arrangements agreed. The contract between CCG and CSS needs to reflect a quality service. Commissioning Support South will report to the CCG under the
Quality Strategic Framework Page 8 of 18
signed term and conditions of the contract and the quality and safety element will have regular performance review - including annual review as a minimum- with the Executive Quality Lead of NHS Portsmouth CCG.
NHS Providers of Health and Social Care
NHS Portsmouth CCG will contract the CSS authority on its behalf - according to terms and conditions of the CCG/CSS contract- to monitor NHS provider quality and safety processes, including but not exclusive of the following organisations:
Portsmouth Hospitals NHS trust
The Solent NHS Trust
Care UK- St Marys Independent Sector Local Treatment Centre
South Central Ambulance Service
NHS Portsmouth CCG and CSS would ensure that agreed provider contracts fully
reflect the CCGs strategy for clinical quality and specify how they expect providers to meet the requirements of the strategy. They should require that any noncompliance with the strategy is brought to the attention of the CSS quality lead and contracts officer. Monitoring arrangements should include regular reports to the Clinical Leads Commissioning Committee and the CCG Board.
Aspects of Quality Assurance;
Clinical Quality Review Meetings (CQRM) will be implemented monthly with the main providers. These meetings will monitor all aspects of the quality elements of the providers’ contracts, including patient safety, patient and carer experience and clinical effectiveness. Within these meetings assurance on compliance will be sought and information reviewed within contractual limits. Any unresolved quality challenges that arise from CQRM will be escalated through the established route to the NHS Portsmouth CCG Clinical Commissioning Committee.
Contracts with providers will include both announced and unannounced access to providers and attendance by the CCG and/or CSS at provider initiated ‘walkabouts’
The providers will be required to publish the Quality Account every year. Quality Accounts are required by law to report performance on providers’ quality of care and services. The publication will be made public and incorporate the views of stakeholders via statements, including the CCGs and the public through Health watch.
9. Stay Ahead
NHS Portsmouth CCG will work with the academic and research community, to drive the research and innovation agenda in Portsmouth
Key clinical strategies across planned and unscheduled care across the Compact and wider health economy will be assessed for innovation potential and work will continue on areas of mutual interest such as technology, and local and national CQUINs with providers
The CCG will review also the incentives and levers in the system and ensure these realise the potential for innovation, such as how we contract with providers to maximise independence and reduce avoidable admissions for people living with long term conditions and vulnerable people including children and adults with dementia
Quality Strategic Framework Page 9 of 18
10. Independent Assurance:
Independent sources of assurance on the effectiveness of the CCG’s risk management and internal control systems include:
Audit Commission
National Quality Board
Internal Audit annual review of clinical Quality processes
External inspection agencies, e.g. Care Quality Commission. 11. Related CCG Strategy and Documentation
Communications and engagement strategy
HR Framework which includes Training and Education Policy and Whistleblowing Policy
Risk Management Strategy and associated policies
Medicine Management Strategy and Policy
Safeguarding Adults Policy
Safeguarding Children Policy
Compact Agreement
Integrated Commissioning Strategy and Policies
Clinical Audit Strategy
Infection Control and Prevention Strategy and Policy
Public Health Outcomes Framework
Social Care Outcomes Framework 12. Bibliography
NHS Portsmouth Clinical Commissioning Group Commissioning Plan http://www.portsmouth.nhs.uk/Downloads/Portsmouth%20CCG/120412%20PCCGCommissioningPlan.pdf
National Institute for Health and Clinical Excellence: How to use NICE guidance to commission high quality services, 2009.
Hallet L, Thompson M, Clinical Governance – a practical guide for managers, emap psm, 2001.
National Quality Board - Maintaining and improving quality during the transition: safety, effectiveness, experience, (part one 2011-12), March 2011.
National Quality Board – Quality in the NHS: A guide for provider boards, March 2011.

Annex I
Information Sheet for GP’s
HIGH QUALITY CARE FOR ALL:
Quality is a practice of meeting the needs and expectations of patients and health service staff. 1 The 3 main elements2 of Quality are:
COMMISSIONING FOR QUALITY IN 2012/13: Quality requirements are included in the contracts with our providers. The following documents have been key to their development, together with recognising the local needs of the population:
Both of these documents focus on five areas (domains ) within which each of the quality elements fits – these have been reflected in the quality elements of the 2012/13 contracts: Domain Quality Element Examples of quality focus areas in 2012/13 contracts
1 Preventing people from dying prematurely
Clinical Effectiveness
Mortality; Improving management of fragility fractures.
2 Enhancing quality of life for people with long-term conditions
Care in the most appropriate place; Improving the management of depression, dementia and delirium.
3 Helping people to recover from episodes of ill-health or following injury
Enhanced Recovery; Reducing Clinical Variations; Review of readmissions.
4 Ensuring that people have a positive experience of care Patient Experience
Improving care based on patient feedback; Improving end of life care; Meeting the needs of Military and Veterans.
5 Treating and caring for people in a safe environment and protecting them from avoidable harm
Patient Safety
Strengthening the Safeguarding of Children and Vulnerable Adults; Learning from and preventing incidents; Harm free care; Improving medicines reconciliation; Insulin Prescribing; Healthcare associated Infections; Improving timeliness and content of discharge summaries.
In addition to the above quality elements, the contract also focuses on the following areas:
1 World Health Organisation (2000)
2 Lord Darzi’s (2008) NHS Next Stage Review
QUALITY MATTERS
PATIENT SAFETY How safe will I be? PATIENT EXPERIENCE
What will my experience be like?
The NHS Outcomes framework acts as a catalyst for driving quality improvements and outcome measures. This provides focus for the local quality elements in the contract.
The NHS Operating framework sets out all national priorities for the NHS in the forthcoming year. The NHS Standard Contract reflects these requirements.
EFFECTIVENESS OF CARE How effective will my care be?
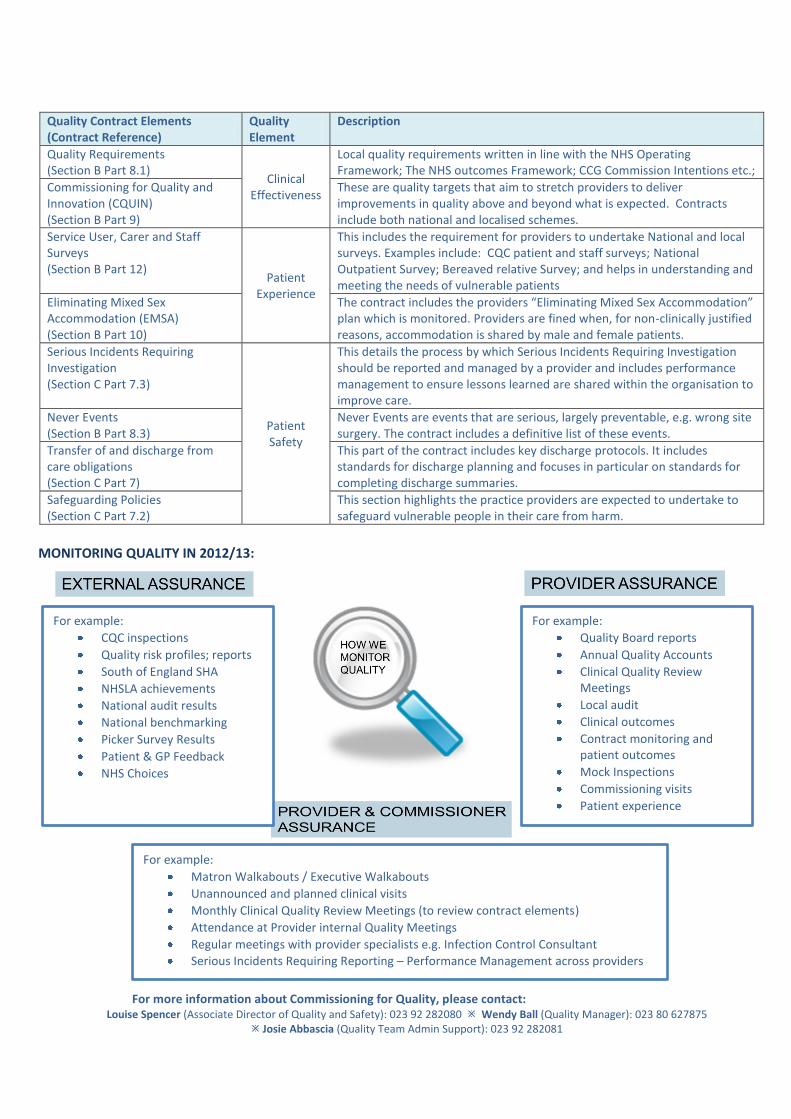
Quality Contract Elements (Contract Reference)
Quality Element
Description
Quality Requirements (Section B Part 8.1)
Clinical Effectiveness
Local quality requirements written in line with the NHS Operating Framework; The NHS outcomes Framework; CCG Commission Intentions etc.;
Commissioning for Quality and Innovation (CQUIN) (Section B Part 9)
These are quality targets that aim to stretch providers to deliver improvements in quality above and beyond what is expected. Contracts include both national and localised schemes.
Service User, Carer and Staff Surveys (Section B Part 12)
Patient Experience
This includes the requirement for providers to undertake National and local surveys. Examples include: CQC patient and staff surveys; National Outpatient Survey; Bereaved relative Survey; and helps in understanding and meeting the needs of vulnerable patients
Eliminating Mixed Sex Accommodation (EMSA) (Section B Part 10)
The contract includes the providers “Eliminating Mixed Sex Accommodation” plan which is monitored. Providers are fined when, for non-clinically justified reasons, accommodation is shared by male and female patients.
Serious Incidents Requiring Investigation (Section C Part 7.3)
Patient Safety
This details the process by which Serious Incidents Requiring Investigation should be reported and managed by a provider and includes performance management to ensure lessons learned are shared within the organisation to improve care.
Never Events (Section B Part 8.3)
Never Events are events that are serious, largely preventable, e.g. wrong site surgery. The contract includes a definitive list of these events.
Transfer of and discharge from care obligations (Section C Part 7)
This part of the contract includes key discharge protocols. It includes standards for discharge planning and focuses in particular on standards for completing discharge summaries.
Safeguarding Policies (Section C Part 7.2)
This section highlights the practice providers are expected to undertake to safeguard vulnerable people in their care from harm.
MONITORING QUALITY IN 2012/13:
For more information about Commissioning for Quality, please contact:
Louise Spencer (Associate Director of Quality and Safety): 023 92 282080 Wendy Ball (Quality Manager): 023 80 627875 Josie Abbascia (Quality Team Admin Support): 023 92 282081
For example:
CQC inspections
Quality risk profiles; reports
South of England SHA
NHSLA achievements
National audit results
National benchmarking
Picker Survey Results
Patient & GP Feedback
NHS Choices
For example:
Quality Board reports
Annual Quality Accounts
Clinical Quality Review Meetings
Local audit
Clinical outcomes
Contract monitoring and patient outcomes
Mock Inspections
Commissioning visits
Patient experience
For example:
Matron Walkabouts / Executive Walkabouts
Unannounced and planned clinical visits
Monthly Clinical Quality Review Meetings (to review contract elements)
Attendance at Provider internal Quality Meetings
Regular meetings with provider specialists e.g. Infection Control Consultant
Serious Incidents Requiring Reporting – Performance Management across providers

Annex II
Quality and Safety specification
Portsmouth CCG Quality and Safety 1. Quality risks will be managed in line with the Portsmouth CCG Integrated Risk
Management Framework. Portsmouth CCG, via Commissioning Support South (CSS)
will deliver the development, negotiation and monitoring of quality outcome measures
within annual contracts with providers, with a planned and timely process including:
engagement with CCGs and the providers across the health economy
agreement of lead and associate commissioners for local contracts
the negotiation process with providers
the decision making processes
2. Building on work to date as appropriate, define and agree a Quality Framework based
on the vision for systematic improvement of quality of care as set out in High Quality
Care for All (Darzi), the Operating Framework, the NHS Outcomes Framework and
the Quality element of the SHA Compliance Framework, utilising accredited evidence,
for example NICE Quality Standards and Royal Colleges including:
2.1 Patient Experience
2.1.1 Ensuring that provider services use a comprehensive range of methods to capture, understand, measure and improve care which reflects the diversity of the patient population. Ensure that the output and learning is used to drive and prioritise service improvement and re-design. All provider services will be expected to implement a consistent and effective process for gathering and utilising patient and staff feedback, to improve staff and patient experience for all groups including vulnerable groups, and where appropriate demonstrate improvements.
2.1.2 Examples of methods to capture patient experience include:
o CQC patient and staff surveys o National outpatient Survey o Bereaved relative survey o Safety Culture survey o National Inpatients Diabetes Audit o Local provider surveys including real time electronic survey systems o Local patient experience narratives o Local patient experience groups o Experience based co design of services
2.1.3 Synthesise, monitor and triangulate patient experience information with other
elements of the quality agenda to provide information to enable Portsmouth
CCG to commission high quality services from providers across the patient
pathway.
2.1.4 Work closely through the CCG GP Quality Lead and CSS Quality team to
ensure that patient experience is reported to the CCG Governing Body,
subcommittee and commissioning work streams. This is to enable the CCG to
identify and act on patient feedback with regard to any quality and patient
safety issues.
2.2 Patient Safety
2.2.1 Portsmouth CCG via the CSS, will ensure continued patient safety and risk
management processes are in place with providers, so that risk of harm for
patients is reduced to a minimum. This will continue to be through robust
contractual methods and assurance processes whilst maintaining
collaborative relationships.
2.2.2 Portsmouth CCG via the CSS will work with local, regional and national
networks to deliver the quality and safety agenda.
2.2.3 To ensure quality is a priority and clinical views are foremost, the CCG GP
Quality Lead and CSS Quality team will work closely and with a programme of
reporting, to ensure that patient safety issues are reported regularly to the
CCG Governing Body, subcommittee and commissioning work streams. This
is to enable the CCG to identify and act on any safety issues.
2.2.4 Via the CSS we will ensure that providers document and highlight themes and
lessons from incidents, and then we will embed these lessons into service
developments and improvement through our commissioning cycle.
2.2.5 The CCG will manage the performance of providers on how they manage
Serious Incidents Requiring Investigation (SIRI) including Never Events in
conjunction with the CSS.
2.2.6 Portsmouth GP CCG Clinical Leads in conjunction with the CSS Quality Team
will develop a system to improve pathway learning across organisations and
the local health economy, from primary, community, secondary care and Any
Qualified Provider (AQP) settings.
2.2.7 Via the CSS Quality Team we will synthesise and triangulate provider
complaints, adverse incidents, SIRI and local and national patient safety
information.
2.2.8 We will ensure a clear line of accountability for Portsmouth CCG including
ensuring a process for reporting to the National Reporting and Learning
System is in place via the CSS
2.3 Clinical Outcomes
2.3.1 We will work within the Operating Framework, Better Care Better Value
metrics, the quality element of the SHA Compliance Framework and NHS
Outcomes Framework, drawing on clinical guidance from national bodies
alongside local priorities to ensure that the Providers are delivering against
latest guidance/best practice.
2.3.2 We will agree in year trajectories in line with emerging national and local
guidance and ensure the Provider is measuring and meeting the set
trajectories, enabling peer review, where possible.
2.3.3 The CCG GP Quality Lead and CSS Quality team will work closely together to
ensure that clinical outcomes are reported to the CCG Governing Body,
subcommittee and commissioning work streams. This is to enable the CCG to
identify and act on any clinical outcomes that may affect any quality and
patient safety issues.
2.4 Contract Monitoring
2.4.1 Based on all of the above, via the CSS, we will develop and implement
Contract Performance Monitoring processes (CPM) based on Contract Quality
Performance Indicators (CQPIs) to be agreed with each Provider. This is to
enable both measurement on a continuing basis the key indicators of quality
performance, and enable comparability of performance between Providers in
order to drive continuing improvements in patient care.
2.4.2 The CCG in conjunction with CSS will proactively engage all appropriate
stakeholders (primary, acute, mental health and community service and social
care providers, Public Health, Health watch) and regulators in the
development of the quality indicators. We will measure what is useful,
meaningful and relevant to the local population, and ensure it is outcome
focussed, avoiding unnecessary duplication and overly bureaucratic
processes.
2.4.3 We will define and agree via CSS a strategy for negotiating the quality
elements of the contract in collaboration with other CCGs, and ensure
arrangements are in place with neighbouring CCGs in areas such as lead
commissioning, where there is more than one CCG contracting with a
provider. This will be negotiated via the Compact agreement with the 3 local
CCGs for local providers, and via arrangements with wider CCGs across the
health economy and CSS.
2.4.4 Via the CSS we will incentivise the health economy to deliver quantifiable and
sustainable improvements in quality through offering expertise and
professional guidance on the development and agreement of Commissioning
for Quality & Innovation Schemes (CQUIN).
For example - In 2011/12 it was agreed with providers to focus on ensuring care is delivered in the most appropriate place. This involves cross health economy working, including primary, secondary, community and ambulance services, to ensure inappropriate admissions are avoided and timely, appropriate referrals are made back into community care.
2.4.5 The CCG GP Quality lead through the CSS quality team will contribute to the
development and review of the Clinical Commissioning Group Quality, Innovation, and Productivity & Prevention (QIPP) programmes, informed by national and regional requirements. The Quality Team via the CSS will contribute expertise with regard to the quality agenda on how these can be delivered through the contract in order to provide the requisite assurance of performance.
3 Assuring Quality Improvement for Patients 3.1 Portsmouth CCG has a responsibility for assuring the quality of the services we
commission and is accountable to the local population for quality and patient experience. Portsmouth CCG will obtain support via the CSS Quality Team for monitoring provider quality performance and providing easy to understand assurance and reports. Work will include:
3.1.1 Continued development of systems and tools for assurance (including national,
regional and local assurance requirements) to provide Early Warning Signs of systematic quality failure. These systems and tools are to be based on CQPIs established with each Provider and the CPM reporting processes.
3.1.2 Developing and maintaining a reporting mechanism to ensure the evolving national, regional and local statutory requirements are met and agreeing content and frequency of assurance reports.
3.1.3 Supporting the development of a Quality Governance Framework for Clinical Commissioning Groups locally, including an escalation process to address dispute resolution as between (a) the CCGs and CSS and (b) the CCG/CSS and the Provider/other third party.
3.1.4 Management of clinical information, including data analysis and benchmarking to measure quality performance, ensuring that we have local knowledge, control and accountability for assuring desired results which reflect the local population needs.
3.1.4 To ensure effective working in partnership with providers to ensure contract
compliance and continuous improvement in quality and outcomes, Portsmouth CCG through the quality team in CSS will:
o Develop and agree outline Terms of Reference to align with governance
processes. o Utilise contracting including CPM as a powerful lever for change to deliver and
assure better patient experience, patient safety and clinical outcomes. o Ensure that monthly (or as otherwise agreed) Contract Quality Review
Meetings are managed with Providers and that exceptions or issues requiring follow-up contract action are fed into contract meetings.
o Report on the overall Provider position against the agreed plan for each agreed Contract Quality Performance Indicator (CQPI) and other accessible data.
o Work to address/challenge quality issues. o Provide variance analyses, investigate/challenge sub-optimal performance
and provide reports of remedial action and plans to assure Provider action that is timely and effective.
o In conjunction with the Contract Manager assigned via CSS manage the contract quality dispute resolution process appropriately where material variances against CQPIs persist/warrant this.
o Ensure professional relationships are continually developed and maintained with the Provider to minimise the need for contract quality management/dispute resolution.
o Hold organisations to account through contracting processes in order to provide assurance of delivery of sustainable quality.
o Work to drive quality improvements. o Implement early-warning procedures to recognise or anticipate decline in
quality performance and trigger a clear escalation/de-escalation process.
4 Continuing Professional Support & Development for Quality Improvement and Patient Safety. With Commissioning Support South we will:
4.1 Enable professional advice and leadership is available through an experienced,
energetic, well informed, expert team which is accessible and provides a proactive service.
4.2 Provide formal and informal education and development for Quality Improvement to our CCG members, member practices, providers and other stakeholders as appropriate.
4.3 Identify and share best practice and professional guidance with regard to quality and safety through a supporting team which will be available to Portsmouth CCG via a named/agreed individual, including access out-of-hours as required and on a basis, including response times, to be set out in a Service Level Agreement (SLA).
4.4 Ensure appropriate engagement with National, Regional and Local bodies and
develop mechanisms to support Portsmouth CCG in horizon scanning.
4.5 Demonstrate that quality is a priority and the assurance process is effective utilising contract development, review, escalation, early warning systems and quality reporting/outcomes as evidence of effectiveness.
End of paper





























