Embed Size (px)
Citation preview
Polytrauma patient
State University of Medicine and Pharmacy “Nicolae Testemitanu”,
Gh. Ciobanu,
Head of the Department of Emergency Medicine, PhD, professor
OBJECTIVES Introduction
Definition of polytrauma
Response to major injury
Polytrauma patients selection who might benefit from the damage control surgery
Initial Assessment: Advanced Trauma Life Support (ATLS 10-ed.) Protocol
Damage Control Resuscitation Once Bleeding Has Been Stopped
Conclusions
References
Introduction. Severe trauma is a major global public health issue. Globally, injuries contribute
to around 10% of total deaths and 15% of disability-adjusted life-years, resulting in the annual
worldwide death of more than 5.8 million people, a number that is predicted to increase to >8
million by 2020. According to the World Health Organization (WHO), road traffic accidents,
suicides and homicides are the three leading causes of injury and violence-related deaths, with a
greater share of hospitalizations, deaths, disabilities and socioeconomic losses in young and
middle-age populations. Massive bleeding following injury remains the main cause of
potentially preventable death with better control of bleeding. Within the largest European trauma
registry, true polytrauma (ISS> 17 with at least two AIS 3+ injuries) using abbreviated injury
scale criteria occurs, in only 12% (2008-2013) of cases but causes up to one third of all deaths in
patients reaching hospital alive, mainly in adults <65 years. Uncontrolled hemorrhage is reported
to be responsible for 40% of trauma deaths Most of the deaths occur due to poor decision and
inappropriate interventions. Damage control resuscitation (DCR) is a strategic approach to the
trauma patient who presents in extremis.
Defining polytrauma. Polytrauma can be defined as significant injury in at least two out of the
following six body regions :
Head, neck and cervical spine
Face
Chest and thoracic spine
Abdomen and lumbar spine
Limbs and bony pelvis
External(skin)
Note: Significant injury=abbreviated injury score of ≥ 3out of 6
Evidence – based definition of polytrauma: Polytrauma can be defined as patients with an
Abbreviated Injury Scale (AIS) score great than 2 points and at least one of the following
covariables :
Hipotension (systolic blood pressure < 90 mmHg);
Level of consciousness (Glasgow Coma Scale score < 8 points);
Acidosis (base excess ≥ 6,0);
Coagulopathy (international normalized ratio 1.4/ partial thromboplastin time ≥ 40 s);
Age > 70 years.
Injury severity score (ISS) ISS is an anatomical scoring system that provides an overall score for
patients with multiple injuries. Each injury is assigned an AIS and is allocated to one of six body
regions (Head, Face, Chest, Abdomen, Extremities (including Pelvis), External). Only the highest
AIS score in each body region is used .
The 3 most severely injured body regions have their score squared and added together to produce
the ISS score. An example of the ISS calculation is shown in table1.
Table 1 Calculation of the injury severity score (ISS)
Region Injury Description AIS Square Top Three
Head,neck and cervical spine Cerebral contusion 3 9
Face No injury 0
Chest and thoracic spine Flail Chest 4 16
Abdomen and lumbar spine Minor Contusion of Liver
Complex Rupture of Spleen
2
5
25
Limbs and bony pelvis Fractured femur 3
External(skin) No injury 0
Injury Severity Score 50
Note:The ISS score takes values from 0 to 75.If an injury is assigned an AIS of 6 (usurvivable
injury), the ISS score is automatically assigned to 75, AIS – Abbreviated Injury Scale.
Abbreviated injury scale (AIS) AIS is an anatomical scoring system first introduced in
1969.Injuries are ranked on a scale of 1 to 6 with 1 being minor,5 severe, and 6 a nonsurvivable
injury (Table 2).
Table 2. Abbreviated Injury Scale(AIS)
Injury AIS Score
1 Minor
2 Moderate
3 Serious
4 Severe
5 Critical
6 Unsurvivable
Note: AIS -abbreviated injury scale.
Response to major injury The systemic inflammatory response syndrome (SIRS) after
injury occurs as a result of a complex set of interactions which result in a substantial host immune
cell response and activation of both the complement and coagulation cascades. SIRS is defined as
two or more of the following: (Table 3). This SIRS response occurs within minutes of injury as a
result of tissue hypoperfusion and tissue injury.
Table 3. Systemic inflammatory response syndrome (SIRS) criteria
Two or more of the following
Heart rate >90 bpm
WBC < 4000/mm3 or >12000/mm3 or >10% immature PMNs
Respiratory rate>20/mm with PaCO2<32 mmHg
Core temperature < 360C or > 380C
Note: SIRS - systemic inflammatory response syndrome,
PMN-polymorphonuclear leukocytes.
Tissue ischemia-reperfusion after hemorrhage or tissue damage from trauma can elicit a
sterile inflammatory response caused by release of damage-associated molecular patterns
(DAMPs). This injury results in activation of the innate immune system, coagulation pathway, and
complement cascade leading to a systemic inflammatory response (SIRS) and host tissue injury.
The exaggerated host response to the severe injury can lead to significant tissue injury, end organ
dysfunction, and ultimately multiple organ failure (MOF). MOF is defined as progressive,
potentially reversible dysfunction of two or more organ systems including the lung, liver, gastroin-
testinal tract, renal, and hematologic systems [68]. Post-injury MOF is the most significant cause
of late deaths in trauma patients [41].
A sustained inflammatory response to injury has been correlated with increased morbidity and
mortality in trauma patients.
Physiological response to injury include:
Inflammatory immune response
Innate immune response
Adaptive immune response
Systemic Inflammatory Response Syndrome (SIRS)
Compensatory Anti-inflammatory Response Syndrome (CARS)
Multiple Organ Dysfunction Syndrome (MODS)
Lethal Triad. The term “lethal triad” was used to describe the physiologic derangement observed
in these patients and refers to the triad of the deteriorating status of acute coagulopathy,
hypothermia, and acidosis of exsanguinating trauma patients (Fig. 1).
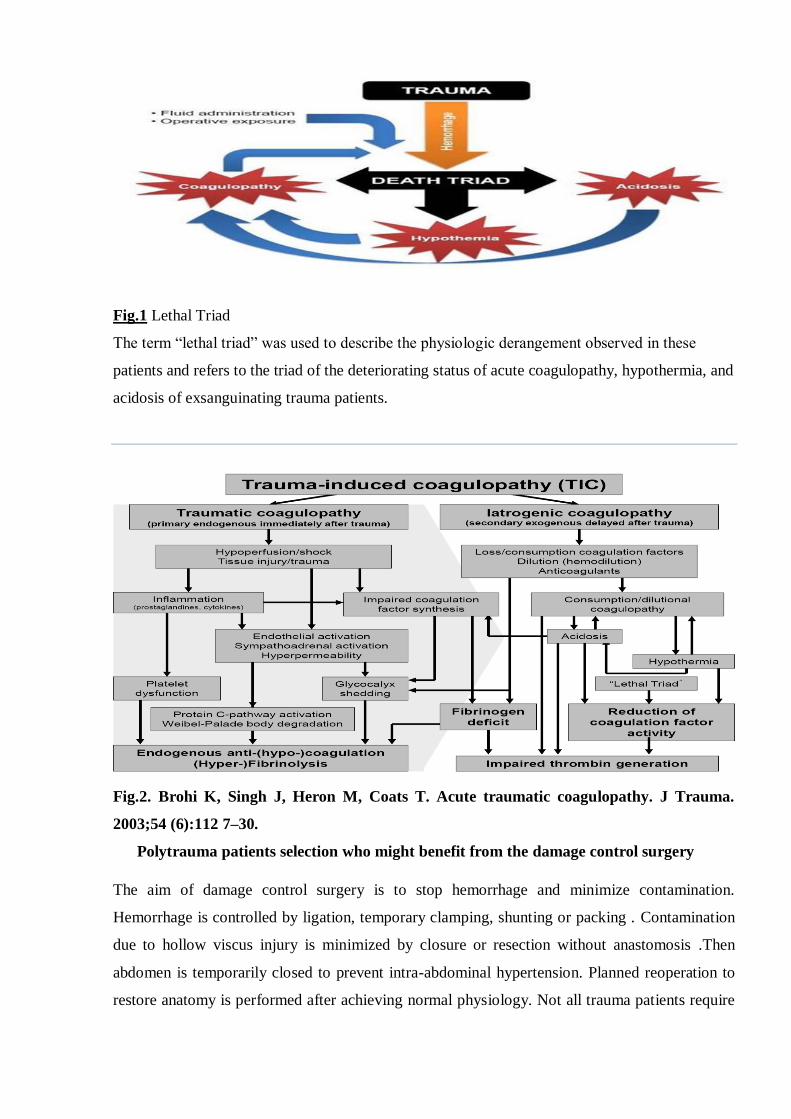
Fig.1 Lethal Triad
The term “lethal triad” was used to describe the physiologic derangement observed in these
patients and refers to the triad of the deteriorating status of acute coagulopathy, hypothermia, and
acidosis of exsanguinating trauma patients.
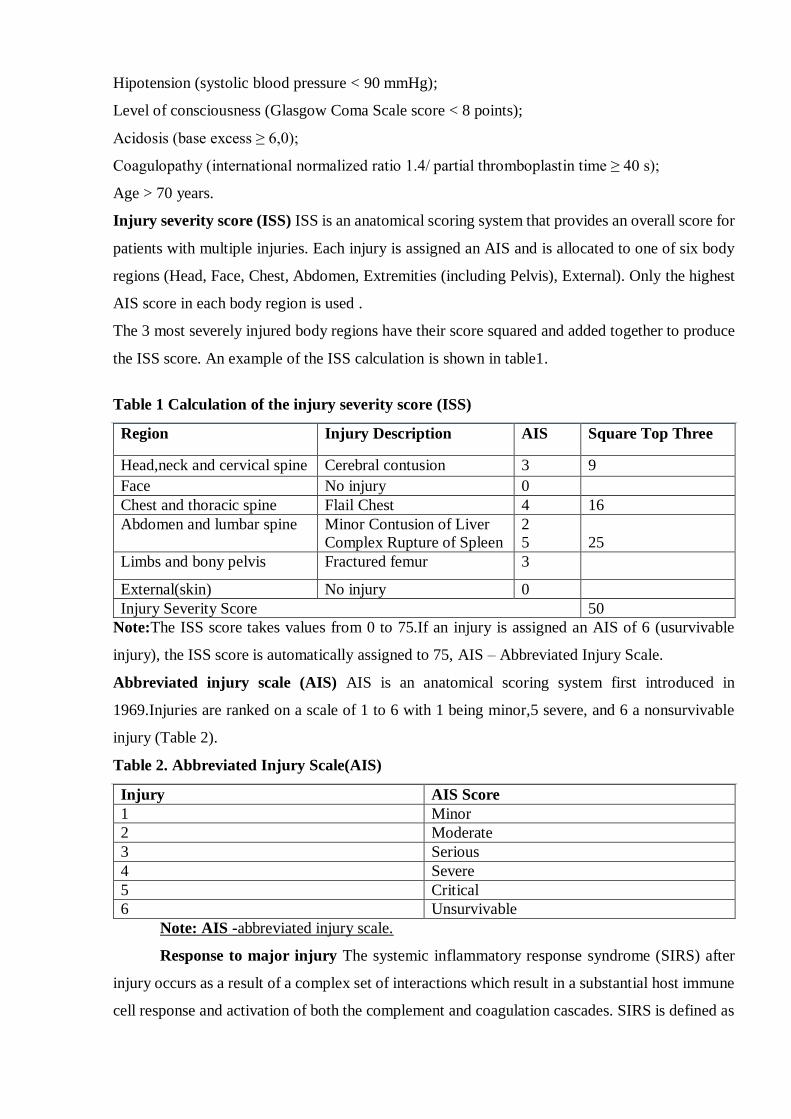
Fig.2. Brohi K, Singh J, Heron M, Coats T. Acute traumatic coagulopathy. J Trauma.
2003;54 (6):112 7–30.
Polytrauma patients selection who might benefit from the damage control surgery
The aim of damage control surgery is to stop hemorrhage and minimize contamination.
Hemorrhage is controlled by ligation, temporary clamping, shunting or packing . Contamination
due to hollow viscus injury is minimized by closure or resection without anastomosis .Then
abdomen is temporarily closed to prevent intra-abdominal hypertension. Planned reoperation to
restore anatomy is performed after achieving normal physiology. Not all trauma patients require
damage control measures. Certain conditions and complexes of injuries assessed both
preoperatively and intraoperatively require damage control.
At its core, damage control surgery attempts to identify those patients incapable of undergoing
a definitive surgery due to loss of physiologic reserve and exchange an improvement in survival
for increased morbidity. In general, there are two treatment strategies for fracture care in multiple-
trauma patients. The aforementioned concept of "damage control orthopedics" (DCO) is
characterized by temporary external fracture fixation in the primary phase with secondary
conversion to definitive osteosynthesis after stabilization of the patient's physiological and
immunological status in the intensive care unit.
In the majority of studies, it is accepted that stable patients benefit from the ETC concept,
whereas unstable patients and patients „in extremes might benefit from DCO. In this study,
borderline patients were shown to have a significantly higher incidence of acute lung injury (ALI)
after ETC treatment compared to fracture stabilization according to the DCO concept. For the
identification of these patients, the severity of thoracic trauma and physiological pulmonary
parameters are of central importance.
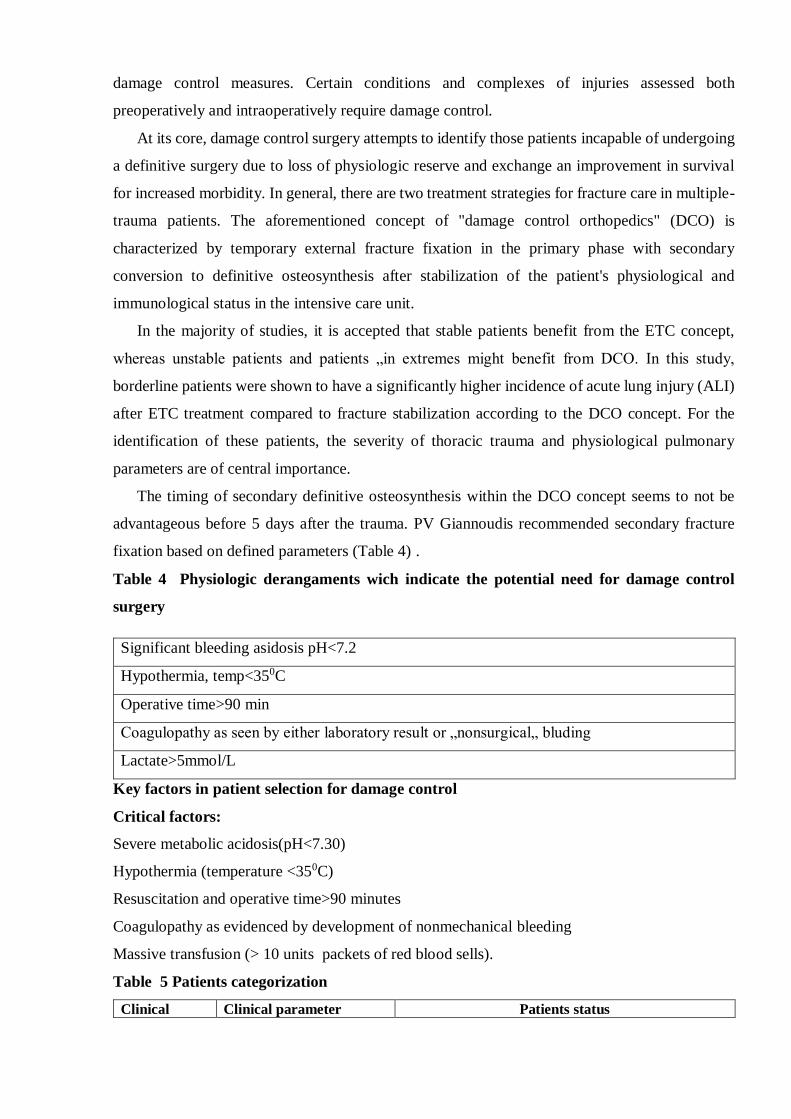
The timing of secondary definitive osteosynthesis within the DCO concept seems to not be
advantageous before 5 days after the trauma. PV Giannoudis recommended secondary fracture
fixation based on defined parameters (Table 4) .
Table 4 Physiologic derangaments wich indicate the potential need for damage control
surgery
Significant bleeding asidosis pH<7.2
Hypothermia, temp<350C
Operative time>90 min
Coagulopathy as seen by either laboratory result or „nonsurgical„ bluding
Lactate>5mmol/L
Key factors in patient selection for damage control
Critical factors:
Severe metabolic acidosis(pH<7.30)
Hypothermia (temperature <350C)
Resuscitation and operative time>90 minutes
Coagulopathy as evidenced by development of nonmechanical bleeding
Massive transfusion (> 10 units packets of red blood sells).
Table 5 Patients categorization
Clinical Clinical parameter Patients status

criteria Stable Borderline Unstable In
Extremis
Shock Systolic blood pressure ( mmHg)
≥100 80-100 ˂ 90 ˂70
Blood units given/ in 2hr 0-2 2-8 5-15 ˃15
Lactate levels(mg/dL) ˂ 2.0 2.5 ˃2.5 Severe
acidosis
Base deficit level
( mmoli/L)
Normal
range
No date No date ˃6-8
Urinary output (ml/h) ˃150 50-150 ˂ 100 ˂ 50
ATLS Classification I II-III III-IV IV
Coagulation Platelet count (mm3) ˃ 10000/L 90000-
11000/L
70000-
90000
˂ 70000
Factor II/V 90-100% 70-80% 50-70% ˂50%
Fibrinogen (g/dL) ˃1 1 ˂1 DIC
D-Dimer(µg/ml) Normal
range
Abnormal Abnormal DIC
Temperature 0C ˂ 34 33-35 30-32 ≤ 30
Soft tissue
injuries
AIS Chest Trauma Scores 1 sau2 ≥ 2 ≥ 2 ≥ 3
Lung Function (PaO2/FiO2) 350-400 300-400 200-300 ˂ 200
Abdominal Trauma
Abdominal trauma /Moor
None
˂ II
Slight
˂ III
Moderate
III
Severe
III or IV
Abdominal trauma (AO) A B or C C C
External(AIS)
1 or 2 2 or 3 3 or 4 Crush injury
Note: AIS – abbreviated injury score, ATLS – advanced trauma life support, PaO2 – partial
pressure of oxygen in arterial blood , :FiO2- fraction of inspired oxygen.
Damage Control Resuscitation is defined as a systematic approach to major
exsanguinating trauma incorporating several strategies to decrease mortality and morbidity
[109,131,139]:
1. Permissive hypotension (Minimal Normotension)
2. Hemostatic resuscitation (Massive Transfusion Protocol)
3. Hemorrhage control (Damage Control Surgery).
Initial Assessment: Advanced Trauma Life Support (ATLS) Protocol
The treatment of bleeding is to stop the bleeding. Damage control resuscitation is a management
strategy of which goal is to enable survival of the trauma patient until bleeding is controlled while
keeping the risk of iatrogenicity to a minimum. Damage control resuscitation is part of ATLS
AB.CDE protocol that ensures oxygenation of the cells:
Airway: airway is most often secured by orotracheal intubation. When orotracheal
intubation is impossible and airway has to be secured, cricothyroidotomy is a DC
procedure. C-spine is protected by a cervical collar.
Breathing: trauma patient is given 100% O2. The SaO2 is monitored. If a pleural effusion
(pneumo- and/or haemothorax) is present, a chest tube is placed. A sucking thoracic
wound is treated by a vented chest seal.
Circulation: control of bleeding is initially achieved, depending on situations, by direct
pressure eventually enhanced by haemostatic dressings, by tourniquet placement or by
placement of a pelvic sling. ECG and blood pressure are monitored non-invasively. Two
large-bore intravenous lines or one intraosseous line is placed. Crystalloid perfusion is
started. In case of hemorrhagic shock, permissive hypotension and transfusion of red blood
cell unit (RBC) (O Rh- then type specific) and early plasma administration are
recommended. A FAST echography is performed to look for intraperitoneal bleeding and
cardiac tamponade.
Disability: GCS score is calculated, pupillary reactivity and symmetry are checked, and
focal neurological deficits are searched.
Exposure: patient's dresses are removed, and a logroll is performed to allow complete
examination including the back. Body temperature is monitored.
Fluid replacement in balanced resuscitation –initial fluid replacement with up to 1L
crystalloid. Titrate small bolus (250 ml) fluid administration to achieve permissive hypotension
SBP to 80 – 90 mmHg or normal mentation or palpable radial pulse (˃80 mm Hg) or brachial pulse
( ˃ 60 mmHg),until definitive control of bleeding is obtained. Role of fluid challenge (250-500
ml) in testing to stratify responder to fluid resuscitation
Damage Control Resuscitation is defined as a systematic approach to major
exsanguinating trauma incorporating several strategies to decrease mortality and morbidity:
1. Permissive hypotension (Minimal Normotension)
2. Hemostatic resuscitation (Massive Transfusion Protocol)
3. Hemorrhage control (Damage Control Surgery)
Targeted Blood Pressure with Permissive Hypotension and Restrictive Fluid
Administration
The concept of damage control resuscitation aims to achieve a lower than normal blood
pressure, also called 'permissive hypotension', and thereby avoid the adverse effects of early
aggressive resuscitation using high doses of fluids while there is a potential risk of tissue
hypoperfusion during short periods. Permissive hypotension and restrictive fluid administration
are therefore reciprocal components of this approach; initial fluid administration is delayed or
minimized, and less aggressive resuscitative end points are used. A targeted systolic blood pressure
(SBP) of 80-90 mmHg is recommended until major bleeding has been stopped in the initial phase
following trauma without brain injury. In patients with severe traumatic brain injury (GCS <8),
maintenance of a mean arterial pressure >80 mmHg is recommended. This approximately equates
to aiming for the restoration of a palpable radial pulse. A restrictive fluid administration strategy
is recommended to achieve target blood pressure until bleeding can be controlled. Such an

approach decreases both the severity and incidence of dilution coagulopathy and as such
complements a strategy of hemostatic resuscitation. Second, this reduces fluctuations in, and
elevation of, systolic blood pressure which may disrupt the premature blood clot forming in areas
of injury causing further bleeding.Damage control resuscitation Multidisciplinary approach to the
management of critically injured, updated European guidelines recommends [Figure3]:
Figure 3: Flow chart of initial management of traumatic hemorrhagic shock. In the acute phase
of traumatic hemorrhagic shock, the therapeutic priority is to stop the bleeding. As long as this
bleeding is not controlled, the physician must manage fluid resuscitation, vasopressors, and
blood transfusion to prevent or treat acute coagulopathy of trauma (AP = Arterial pressure,
SAP = Systolic arterial pressure, TBI = Trauma brain injury, Hb = Hemoglobin, PT =
Prothrombin time, APTT = Activated partial thromboplastin time).
Time elapsed between injury and operation should be minimized for patients in need of
urgent surgical bleeding control (Grade IA).

Patients presenting with hemorrhagic shock and an identified source of bleeding should
undergo an immediate bleeding control procedure unless initial resuscitation measures are
successful (Grade IB).
Early imaging (FAST or computed tomography) for detection of free fluid in patients with
suspected torso trauma (Grade IB). If FAST is positive, it should be followed by immediate
intervention.
A target SBP of 80-100 mmHg until major bleeding is stopped in the initial phase without
TBI (Grade IC). Low volume approach is contraindicated in TBI as adequate perfusion
pressure is crucial to ensure tissue oxygenation of injured central nervous system.
Target MAP of 65 mmHg or more, in controlled hypotensive resuscitation.
Adjunct tourniquet uses to stop life-threatening bleeding from open extremity injuries in
the presurgical setting.
Initial normoventilation of trauma patients if there are no signs of imminent cerebral
herniation. A low partial pressure of arterial carbon dioxide on admission to the emergency
room is associated with a worse outcome in trauma patients with TBI. Hyperventilation
and hypercapnia cause intense vasoconstriction with decreased cerebral blood flow and
impaired tissue perfusion.
Hemorrhagic shock with identified source of bleeding - initiate immediate bleeding control
procedure.
Serum lactate and base deficit measurement to estimate and monitor extent of bleeding and
shock (Grade IB). Serum lactate is diagnostic parameter and prognostic marker of
hemorrhagic shock. The amount of lactate produced by anaerobic glycolysis is an indirect
marker of oxygen debt, tissue hypo-perfusion and the severity of hemorrhagic shock. Base
deficit gives indirect estimation of acidosis due to impaired perfusion. Repeated lactate
determinations represent a reliable prognostic index for patients with circulatory shock.
DCR should be employed in severely injured patient presenting with deep hemorrhagic
shocks, signs of ongoing bleeding and coagulopathy, hypothermia, acidosis, inaccessible
major anatomical injury.
Crystalloid should be applied initially for bleeding trauma patients (Grade IB). Hypertonic
saline (HTS) to be considered for hemodynamically unstable patients (Grade 2B). Addition
of colloid to be considered within the prescribed limits for each solution in
hemodynamically unstable patients (Grade 2C).
Early FFP in patients with massive bleeding (Grade IB). Platelets to be administered to
maintain the count above 50 × 10 9 /L (Grade IC). However, maintain the count above 100
× 10 9 /L in patients with multiple trauma who are severely bleeding or have traumatic
brain trauma (Grade 2C).
Tranexamic acid 10-15 mg/kg followed by infusion of 1-5 mg/kg/h (Grade IB).
Target hemoglobin of 7-9 gm% (Grade IC).
Monitoring of ionized calcium during massive transfusion (Grade IC). Calcium chloride to
be administered if ionized calcium levels are low or electrocardiographic changes suggests
hypocalcemia (Grade 2C).
Vasopressor Agents
Vasopressors may be required transiently to sustain life and maintain tissue perfusion in
the presence of life-threatening hypotension, even when fluid expansion is in progress and
hypovolemia has not yet been corrected. If used, it is essential to respect the recommended
objectives for SBP (80-90 mmHg) in patients without traumatic brain injury. Norepinephrine is
the agent of choice to restore and maintain target arterial pressure in hemorrhagic shock.
Management of coagulopathy in trauma patients
DCS is a resuscitation strategy that was devised to avoid these physiological disorders. DCR
directly addresses the trauma-induced coagulopathy immediately upon patient admission [21] or
in the pre-hospital setting [22]. DCR consists of balanced resuscitation, hemostatic resuscitation,
and prevention of acidosis, hypothermia, and hypocalcemia.
Balanced resuscitation
The patient’s response to the rapid infusion of isotonic fluid or blood is the indicator of the need
for surgical or interventional hemostatic procedures. Aggressive fluid resuscitation was the initial
fluid therapy recommended for many decades. However, this approach may contribute to increased
blood loss and higher mortality [23].
Increasing evidence has shown that aggressive crystalloid-based resuscitation strategies are
associated with cardiac and pulmonary complications [25], gastrointestinal dysfunction,
coagulation disturbances, and disorders of immunological and inflammatory mediators [26].
Disturbances in cell volume then disrupt numerous regulatory mechanisms responsible for
controlling the inflammatory cascade. For these reasons, an alternative approach to the treatment
of hemorrhagic patients was recently proposed and practiced. The approach was introduced as
permissive hypotension, delayed resuscitation, or controlled resuscitation. The aim of these
resuscitation strategies is not hypotension but rather to balance the risk of decreased tissue
perfusion with the benefits from the prevention of coagulopathy.
In 1994, Bickell and colleagues investigated the benefit of delayed fluid resuscitation in a
randomized controlled trial. Five hundred eighty-nine adult patients with penetrating injuries and
a pre-hospital systolic blood pressure of less than 90 mmHg were enrolled in the trial [27]. The

application of delayed fluid resuscitation increased the survival rate of of the patients from 62 to
70%.
After this report, several randomized or retrospective studies concerning balanced resuscitation
were reported; however, the benefit to mortality varied among the studies [28, 29, 30, 31]. Duke
et al. retrospectively compared cohorts with standard and restricted fluid resuscitation and reported
that restricted fluid resuscitation showed a survival benefit [31].
When evaluating the effects of balanced resuscitation, these results should be interpreted
cautiously. A recent Cochrane database analysis on crystalloids versus colloids published in
2013 that the resuscitation using colloids compared with crystalloids reduces the risk of death in
patients with trauma, burns or following surgery. The use of HES may increase
mortality. [38] Cochrane review concluded that since colloid use is not associated with improved
survival, and they are considerably more expensive than crystalloids, it is hard to see how their
continued use in clinical practice can be justified. [39] Further clinical trials of colloid use need to
justify carefully the potential for patient benefit.
The tenth edition of the Advanced Trauma Life Support emphasizes the concept of balanced
resuscitation, and the term “aggressive resuscitation” has been eliminated. The standard use of
1 L of crystalloid resuscitation as the starting point for all resuscitation has been modified to the
initiation of 1 L of crystalloid infusion. Early use of blood and blood products for patients in
shock is emphasized [32].
The most recent randomized controlled trial to evaluate the efficacy of balanced resuscitation was
reported in 2015 [33]. This multicenter study was performed in 19 emergency medical services
systems in the USA and Canada. The controlled resuscitation resulted in a reduction of early
crystalloid resuscitation volume and an increase in the early transfusion of blood products.
Although mortality at 24 h was not different among all patients, it improved in the subgroup with
blunt trauma. The controlled resuscitation strategy can be successfully and safely implemented in
a civilian environment beginning with the out-of-hospital setting and extending into early hospital
care.
Hemostatic resuscitation
In 2007, Borgman and Holcomb et al. reported a survival benefit for the high ratio of
plasma to red blood cell (RBC) in patients who received massive transfusions at a combat support
hospital [34]. The most recent randomized trial to evaluate the suitable ratio of plasma to RBCs
for patients with severe trauma and major bleeding was performed in the pragmatic, randomized
optimal platelet and plasma ratios (PROPPR) study [44], in which 680 patients were randomized
to receive either a 1:1:1 or 1:1:2 ratio of plasma, platelets, and RBCs. Although the mortality was
not significantly different between the two groups, more patients in the 1:1:1 group achieved

hemostasis. Exsanguination, which was the predominant cause of death within the first 24 h, was
significantly decreased in the high-ratio group.
Red Blood Cell Transfusion
In the European guideline, the Hb threshold for PRBCs transfusion is set to 7-9 g/dL where
in US guideline Hb is set to 7 g/dL. These recommendations are based on studies showing that
PRBCs transfusions can be associated with increased mortality, lung injury, increased infection
rate and renal failure in injured patients and mainly on the Transfusion Requirements in Critical
Care (TRICC) study demonstrating no efficacy of liberal approach (Hb threshold of 10-12 g/dL)
versus restricted approach (7-9 g/dL) on mortality. For patients with concomitant hemorrhagic
shock and traumatic brain injury, recent studies demonstrate no beneficial effect of a higher Hb
threshold for RBCs transfusion on mortality or neurological outcomes but a higher risk of throm-
boembolic events, even if a higher Hb improves local cerebral oxygenation.
Plasma and Platelet
Transfusion in Hemostatic Resuscitation
The recent PROPPR randomized clinical trial compared 1:1:1 FFP-PLT-PRBCs ratio to
1:1:2 in severe trauma patients without survival bias. Unfortunately, the results showed a no
statistically significant reduction in mortality for the 1:1:1 ratio group, letting the question open.
The European guideline proposes to transfuse 1 FFP every two PRBCs during the initial
management of patients with expected massive hemorrhage, continued with goal-directed therapy
based on standard laboratory (PT or aPTT inferior to 1.5 times the normal controls) and/or
viscoelastic tests.
Fibrinogen, a key component in the coagulation cascade, is the first and; most depleted factor in
hemorrhagic trauma patients.
Platelet depletion or dysfunction in trauma patients needs to be addressed by platelet transfusion.
The European guideline proposes to transfuse platelets if platelet count is less than 50.109/L in
trauma patients or less than 100.10VL in case of ongoing bleeding or traumatic brain injury.
Viscoelastic Techniques and Administration of Concentrated Factors.
To adapt the treatment of hemostasis after the initial phase, viscoelastic techniques (VETs)
may be very useful. VETs have been developed for several years and represent a comprehensive
assessment of clot formation based on the mechanisms originating coagulopathy, including, in a
second stage, inflammatory phenomena.
According to the latest European guideline, VETs are accepted as alternative to standard
coagulation tests to guide the treatment of posttraumatic coagulopathy (grade 1C).

Principles of Clot Viscoelastic
Property Studies
Clot formation is assessed with ROTEM® (Tern GMBH, Munich, Germany) or with
TEG® (Haemoscope Corporation, Niles, Illinois, USA). These tools explore dynamics of clot
development, stabilization and dissolution (fibrinolysis).; The measured parameters are time (s),
amplitude (mm) or angles.
TEG® and ROTEM® allow a rapid and accurate diagnosis of hyperfibrinolyses but will
lack sensitivity to assess the intensity of fibrinolysis especially if minor or moderate.
Damage Control Resuscitation Once Bleeding Has Been Stopped
This step is devoted to reverse the sequelae of hypotension-related metabolic failure and
support physiological and biochemical restoration.
Increasing power of damage control. Damage control should be started in the field by the
paramedics who are trained to stop bleeding with local pressure or tourniquets, administer oxygen
and combat hypothermia. The race against the clock starts. The emergency team in the field should
strive for only minimal vascular filling, the objective being to obtain a systolic blood pressure of
90 mmHg; tranexamic acid should be administered. O-negative and then type-specific PRBC
transfusions are started with the objective of obtaining hemoglobin of 9 g/dL (according to
European guideline); coagulation disorders are corrected by administration of fibrinogen,
coagulation factors and platelet concentrates. The patient is transferred rapidly to the operating
room (or angiography suite, as necessary). When bleeding has been arrested, blood pressure should
return to normal. Damage control resuscitation should be pursued until preset objectives of
hemoglobin, temperature and coagulation parameters are attained. The comparison with naval
damage control can be made in that not only should the water inflow be stopped, but the vital
functions of the vessel must be restored as well (electricity, communications, propulsion, rudder)
Invasive monitoring devices are generally used to guide fluid administration and normalize
hemodynamics. Abramson and colleagues did show that serum lactate clearance correlates well
with patient survival and that the ability to clear lactate to normal levels within 24 h was paramount
to ensuing patient survival. Immediate and aggressive core rewarming not only improves perfusion
but also helps reverse coagulopathy. All of the warming maneuvers initiated in the trauma bay and
operating theatre should be duplicated in the intensive care unit. Gentilello showed that failure to
correct a patient's hypothermia after a damage control operation is a marker of inadequate resus-
citation or irreversible shock.
Rewarming
In DCR, hypothermia should be managed in conjunction with the efforts to correct the trauma-
induced coagulopathy. It is essential to rewarm the torso using passive warming measures, such
as insulting foil, blankets, and the removal of wet clothes. The initial fluid resuscitation should be
carried out with warmed infusions at a fluid temperature of 40–42 °C. Heated air inhalation, gastric
or body cavity lavage with warmed fluids, and heat radiation are widely performed as well as the
standardized use of warming measures with rapid infusers. The temperature in the emergency
room and the operating room should be raised, at best to a thermally neutral range (28–29 °C)
Reversing acidosis
Reversal of metabolic acidosis in the trauma patient is better obtained through fluid and blood
resuscitation and vasopressor support with surgical control of hemorrhage. Shock should be
reversed and end-organ perfusion is restored . Because vital signs such as blood pressure and heart
rate are not adequate to evaluate peripheral tissue perfusion, several endpoints of resuscitation are
addressed. Base deficit and lactate levels are the reliable indices with which to evaluate the
adequacy of the resuscitation and end-organ perfusion, and correlate with the mortality of trauma
patients.
Tranexamic acid
The clinical randomization of an antifibrinolytic in significant hemorrhage 2 (CRASH-2) study, a
large multi-center randomized controlled trial, investigated the effect of tranexamic acid on
mortality and blood product requirements in trauma patients with hemorrhagic shock .The study
was undertaken in 274 hospitals in 40 countries. More than 20,000 adult trauma patients were
randomized to receive either tranexamic acid or placebo within 8 h of injury. All-cause mortality
and the risk of death due to bleeding were significantly decreased with the administration of
tranexamic acid. Maximal beneficial effects were achieved if it was given within the first 3 h of
injury.
Fibrinogen concentrates
Fibrinogen plays a central role in the coagulation process. In patients with blood loss, fibrinogen
has been reported to decrease more rapidly under critically low concentrations than the other
coagulation factors. Thus, the supplementation of fibrinogen is a measure that makes sense when
treating the coagulopathy of trauma patients. The effect of the administration of fibrinogen
concentrates on outcome was investigated by matched-pairs analysis using the German Trauma
Registry. Although 30-day mortality was comparable, 6-h mortality was significantly lower in the
patients receiving fibrinogen. The fibrinogen concentrates might have delayed the cause of death
from early hemorrhagic collapse to late multiple organ failure.
Prothrombin complex concentrate
Recently, prothrombin complex concentrate, derived from human plasma and contains variable
amounts of factors II, VII, IX, and X, is used to correct coagulopathy. Goal-directed coagulation
management using thromboelastometry was used to evaluate requirements of clotting factors .The
administration of fibrinogen concentrate alone or in combination with prothrombin complex
concentrate resulted in a significant improvement of fibrin polymerization and shorter clotting
time. Schochl et al. used fibrinogen concentrate and prothrombin concentrate complex as first-line
therapies for coagulopathy based on thromboelastography in a study of 131 severely injured
patients.
Calcium
Calcium acts as an important cofactor in the coagulation cascade. Low levels of ionized calcium
at admission are associated with increased mortality and an increased requirement for massive
transfusion. Citrate, which is used as an anticoagulant in blood product components, chelates
calcium and exacerbates the hypocalcemia, particularly when used in the FFP. The faster the
transfusion is given, the faster the reduction of the calcium concentration occurs. An ionized
calcium concentration of less than 0.6–0.7 mmol/L could lead to coagulation defects. In addition,
contractility of the heart and systemic vascular resistance are diminished under decreased ionized
calcium levels. Because of its combined beneficial cardiovascular and coagulation effects, the
calcium concentration should be monitored periodically with every ten units of transfusion, and it
is recommended that a concentration of at least 0.9 mmol/L be maintained.
Massive transfusion protocol
Massive transfusion is typically defined as the transfusion of ten or more units of packed red blood
cells within the first 24 h of injury. It is important for the resuscitation staff to identify the patients
who might require massive transfusion early in the process of initial resuscitation. Following the
prediction of massive transfusion, blood products should be delivered in a quick and timely manner
at a high ratio of plasma, RBCs, and platelets. The protocol includes patient selection for activation
of the MTP, description of the staff who should declare the activation, and the means by which the
resuscitation team and the blood bank are informed of the protocol’s activation.
Remote DCR
The concept and practice of the DCR is recently applied in the pre-hospital setting and named as
remote DCR (RDCR). Not only the fixed-ratio coagulation therapy using the high ratio of plasma
and platelets to pRBC but also the coagulation factor concentrate-based treatment is proposed in
the RDCR. It includes three major components to a step-wise approach to achieve hemostasis: (1)
stop (hyper)fibrinolysis, tranexamic acid; (2) support clot formation, fibrinogen concentrate; and
(3) increase thrombin generation, prothrombin complex concentrate. Although RDCR warrants
further investigation concerning its effect on the mortality or the blood products requirement, and
the assessment of the patient’s coagulation function in the instrument limited environment, the
tranexamic acid has been implemented in the RDCR in the British, Norwegian, and Israeli civilian
ambulance services. A prospective cohort study in the civilian trauma center demonstrated
reduction in mortality and multiple organ failure for patients treated with tranexamic acid in the
subgroup of patients with shock .The updated European guideline suggests the administration of
the first dose of tranexamic acid in route to the hospital as a grade 2C recommendation..
Changes of surgical strategy in DCR
The severely hemorrhagic patient has a limited amount of physiologic reserve before irreversible
derangement, organ damage, and collapse occur. DCR restores this reserve, allowing more
definitive treatment that results in decreased postoperative complications and improved
outcomes .DCS is now incorporated as a component of DCR and should not be practiced in
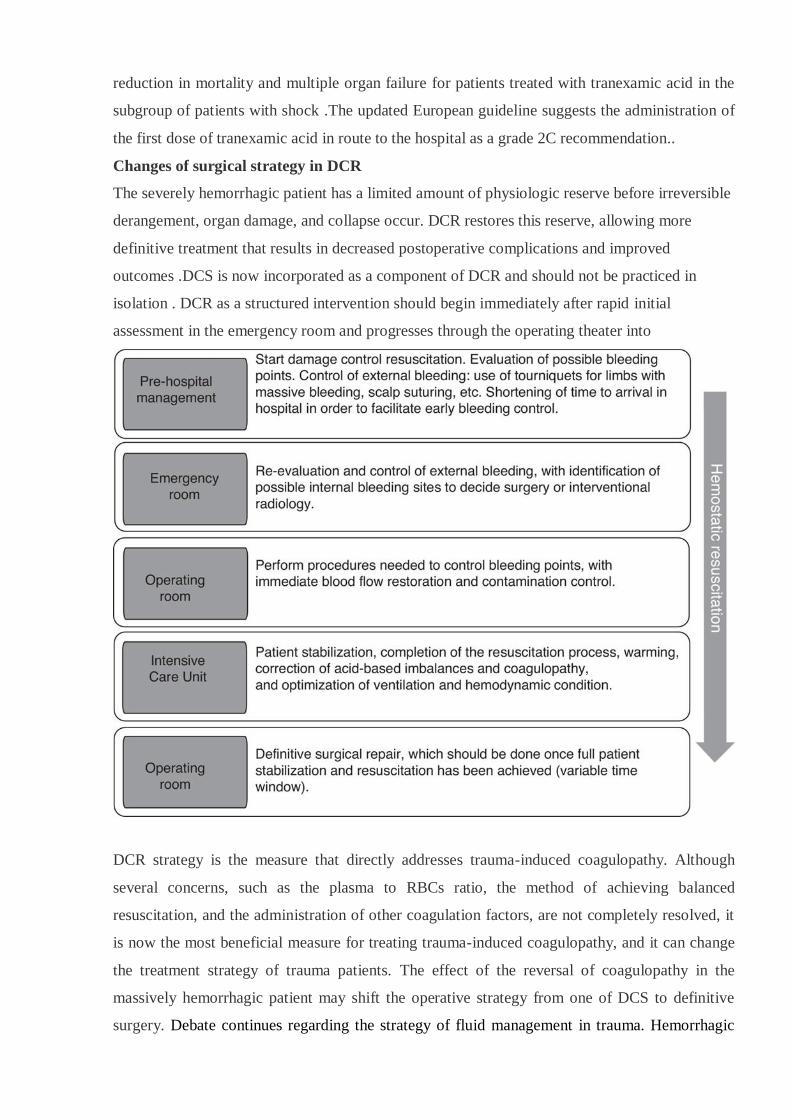
isolation . DCR as a structured intervention should begin immediately after rapid initial
assessment in the emergency room and progresses through the operating theater into
DCR strategy is the measure that directly addresses trauma-induced coagulopathy. Although
several concerns, such as the plasma to RBCs ratio, the method of achieving balanced
resuscitation, and the administration of other coagulation factors, are not completely resolved, it
is now the most beneficial measure for treating trauma-induced coagulopathy, and it can change
the treatment strategy of trauma patients. The effect of the reversal of coagulopathy in the
massively hemorrhagic patient may shift the operative strategy from one of DCS to definitive
surgery. Debate continues regarding the strategy of fluid management in trauma. Hemorrhagic

shock remains a leading cause of morbidity and mortality worldwide. Time-consuming procedures
in the field should be avoided, and rapid transport to definitive care should be aimed at. Fluid
choice has not been shown to affect the outcome in trauma, however large volume of the crystalloid
resuscitation need to be avoided. In the absence of TBI, target SBP of 70-90 mmHg, normal
mentation and peripheral pulses in case of uncontrolled hemorrhage should be aimed at.
Normotension should be the aim in the presence of TBI. Tranexamic acid should be given to all
the patients with penetrating trauma who need transfusion. MTP with fixed ratios should be given.
Patients with penetrating trauma for whom definitive care is immediately available may benefit
from damage control surgery. While DCR requires further study, the early literature seems to be
promising.
Conclusions
1. Damage Control Surgery (DCS) is defined as the planned temporary sacrifice of normal
anatomy to preserve the vital physiology. This is a concept in which the initial surgery
becomes part of the resuscitation process rather than part of the curative process.
2. Once DCS was established, it was quickly marketed into other disciplines, including but
not limited to neck, vascular, orthopedic, thoracic and military injuries. Although each
discipline uses DCS in a slightly different manner, it is clear that the DCS approach leads
to improved survival in patients with either blunt or penetrating injures who are
approaching physiologic exhaustion.
3. It consists of 3 parts including the initial abbreviated laparotomy, ICU resuscitation and
subsequent reoperation for definitive resuscitation This process serves to limit the
physiological exposure to an unstable environment, allowing better resuscitation and
outcome in the critically ill trauma patients.
4. Permissive hypotension - also known as “Hypotensive” or “Balanced” resuscitation - is a
strategy of restricting fluid resuscitation until hemorrhage is controlled, while accepting a
limited period of suboptimal organ perfusion. It is ensured by restricted fluid resuscitation
to a volume sufficient to maintain a radial pulse. In polytrauma patients with head injuries,
the importance of maintaining cerebral perfusion pressure is well recognized, consequently
permissive hypotension is currently contraindicated in this setting.
5. DCR is a potent tool to hinder and even reverse the lethal triad. Damage control
resuscitation currently includes early blood product transfusion, immediate arrest and/or
temporization (i.e., TIVS and balloon tamponade) of ongoing hemorrhage, and restoration
of blood volume and physiologic/hematologic stability. As a result, DCR addresses the
early coagulopathy of trauma, avoids massive crystalloid resuscitation and leaves the

peritoneal cavity open when a patient approaches physiologic exhaustion without
improvement.
6. Future evolution of the DCR concept will include further elucidation of personalized
resuscitations (individual blood product ratios based on point of care testing) as well as
introduction of hybrid angiography operating suites in centers with resource availability.
Hypotensive Resuscitation Strategies prior to definitive hemorrage control.
References
1. Ausset S, Glassberg E, Nadler R, et al. Tranexamic acid as part of remote damage-control
resuscitation in the prehospital setting: a critical appraisal of the medical literature and
available alternatives. J Trauma Acute Care Surg. 2015;78(6 Suppl 1): S70–75.
2. Besen BA, Gobatto AL, Melro LM, et al. Fluid and electrolyte overload in critically ill patients:
an overview. World J Crit Care Med. 2015;4(2):116–129.
3. Brohi K, Singh J, Heron M, et al. Acute traumatic coagulopathy. J Trauma. 2003;54(6):1127–
1130
4. Global Status Report on Road Safety 2013. Geneva: World Health Organization 2013, at
http://www.who.int/ violence_injury_prevenuon/road_safety_status/2013/en/..
5. Holcomb JB, Tilley BC, Baraniuk S, et al. Transfusion of plasma, platelets, and red blood
cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR
randomized clinical trial. JAMA. 2015; 313:471-482.
6. Pape HC, Andruszkow H, Pfeifer R, et al. Options and hazards of the early appropriate care
protocol for trauma patients with major fractures: towards safe definitive surgery. Injury.
2016;47(4):787-791.
7. Pape HC, Lefering R, Butcher N, et all. The definition of polytrauma revisited: an international
consensus process and proposal of the new „Berlin definitionˮ. J Trauma Acute Care Surg.
2014;77(5):780-786.
8. Pape HC, Pfeifer R. Safe definitive orthopaedic surgery (SDS): repeated assessment for
tapered application of early definitive care and damage control: an inclusive view of recent
advances in polytrauma management. Injury. 2015;46(1): 1—3.
9. Wafaisade A, Lefering R, Bouillon B, et al. Prehospital administration of tranexamic acid in
trauma patients. Crit Care. 2016;20(1):143.
970s





























