Embed Size (px)
Citation preview

Public Health Then and Now
The Limits of Thresholds: Silica andthe Politics of Science, 1935 to 1990Gerald Markowitz, PhD, and David Rosnet; PAiD, MPH
Introduction
(Am I -ft*.c 1995$5.253.
c26r:
FeuayI9Y% ,~N.
In recent years, asbestos litigationhas focused attention on the rolc ofprofessionals in protecting workers andthe broader public from exposure todangerous substances. Many public healthadvocates believe there are certain sub-stances, especially carcinogens, to whichhumans should not be exposed at anylevel bccausc thcy arc inhcrcntly dangcr-ous. Historically, however, occupationalhealth professionals have assumed thatanv toxic substance can be used inindustrial proccsses if exposurc is kcptbelow a spccified level or threshold.Bccause assumptions about the mcaningof safety have changed. scholars andindustrial hygicnists have bcgun to focustheir attention on the history of thedevclopmcnt of standards and on theintellectual (and political proccsscs thatled the industrial hygicnc community toput its faith in those standards. Forexample, Barry Castleman and othershavc documcntcd that threshold limitvalues for asbcstos were not developcdsolely as the rcsult of scientific debatesabout safcty and health, but wcrc part ofan intensc ncgotiation in which manage-mcnt intcrcsts shaped the scicntific dis-coursc. '
The currcnt concern w\ith asbestoshas obscured the fact that it was theongoing debaLtes about silicosis during thefirst half of the 20th century that shapedthe public and scientific dcbatcs aboutthreshold limits for the various pncumoco-niosis-producing dusts. Furthcr, the grow-ing attention paid to asbestos during the1970s and carly 1980s hid the ongoingcontcntion about the adequacy of thesilica threshold limit value and its use as a
legal standard.- In this paper, wc explore
the early debates over the establishmentof threshold limit values for occupationalexposure to silica dust, illustrating theintense political negotiation that accompa-nied their establishment.
Since the 1930s there has been apublic perception that threshold limitvalues represent an objectively estab-lished measure of safcty. Advertisements,public pronouncements by industryspokespeople, and reports of industrialhygienists have publicized the view thatequipment and modern engineering tech-niques keep dust exposures below 'accept-able" limits and therefore protect theworkforce from disease. Yet, as we willshow, there have been important intellec-tual, technical, and scientific questionsregarding the adequacy of threshold limitvalues for protecting workers from silico-sis and a continual questioning of thethreshold limit value among professionalsand within industry. The fact that silicosisis still prevalent and continues to bedocumented throughout the nation hauntspublic health officials, some ofwhom haveargued that modern methods of protec-tion have made silicosis a disease of thepast. We will also show that the process bywhich threshold limit values and, ulti-mately, standards have been set, whetherfor asbestos, silica, or other dangeroussubstances. has been part of a compro-mise between the health of workers andthe economic health of industry.
The atuthors are with the City University ofNew! York Graduate Center; in addition.Gerald Markowitz is with John Jay College ofCriminal Justice and David Rosner is withBaruch College and Mt Sinai School ofMedicine, New York, NY.
Requests for reprints should he sent to
Gerald Markowitz. PhD. John Jay College ofCriminal Justice, The City University of New'York. 899 Tenth Ave, New' York. NY 100 19.
American Journal of Public Health 253
............ ........ .. ....

Public Health Then and Now
The Early Silicosis CrisisCrystalline silica, the basic compo-
nent of sand, quartz, and granite rock, isthe agent responsible for silicosis amonghard-rock miners, sandblasters, painters,foundry and steelworkers, potters, insula-tion workers, and workers in cleansermanufacturing establishments, concrete,and other industries. Caused by thedeposit of fine particles of crystalline silicain the lungs, silicosis is progressive, longterm, and incurable. Except in its acuteform, it begins with few, if any, symptomsand terminates with workers gasping forbreath, completely incapacitated by mas-
sive fibrosis of the lung tissue. Theresulting inability of the lungs to transferoxygen to the blood can cause the heart to
weaken and enlarge. As early as 1917,Anthony J. Lanza, at the time a PublicHealth Service physician, described thesymptoms that metal miners experienceas the disease progresses: "If we can
imagine a man with his chest bound withtransparent adhesive plaster, we can forma mental picture of how useless [are] theefforts at deep inhalation made by these
patients."3 Unlike asbestosis, coal work-ers' pneumoconiosis, and other occupa-tional pneumoconioses, silicosis predis-poses its victims to tuberculosis, andsilico-tuberculosis victims are at great risk
of death.4 Researchers have also becomeconcerned about a possible link betweensilica and lung cancer and autoimmunediseases.5
Although silicosis has affected work-ers since antiquity, during the early 1930sit "jumped from [an] obscure, scarcelyrecognized [disease] hidden for centuriesin the chests of workers in various dustyindustries to front-page headlines in thedaily press and to wide discussion in thetechnical journals of the United Statesand other countries."6 Hundreds of thou-sands of workers were said to have beenexposed to potentially dangerous levels ofdust and, therefore, to the disabling andoften deadly disease.7Thousands ofwork-ers in the dusty trades, laid off during theDepression, brought lawsuits against em-ployers seeking damages for exposure to
silica. This led to a broad liability crisisthreatening the "closing of industrial plantsand a vast economic loss."8 In part, thecrisis was caused by an increased incidenceof silicosis resulting from the introductionof pneumatic tools in the early 20th centuryand from workers' increased exposure to
fine particles of silica dust. In part, how-
ever, the crisis was social and economic.9In the 1930s and early 1940s, a
coalition of business, public health, insur-
ance, and political interests, which was
formed in response to the widespreadlitigation, developed a program that led tothe virtual elimination of silicosis frompopular discourse, confining future discus-sion of the issue to the business andprofessional communities. During the1940s, despite continuing discussions ofthe importance of the disease amongpublic health workers, medical specialists,and the business community, the publicceased to read of this disease and workerscame to believe that engineering andmedical reforms had virtually eliminateddanger and made this condition a diseaseof the past. This resulted in what a 1950US Bureau of Mines Health and SafetyDivision report said was an "apparentlyconcerted effort to hide the facts regard-ing dust diseases in industry."10
What became known as thresholdlimit values and maximum allowable con-centrations were established in the late1930s and early 1940s and played animportant role in this process. Engineer-ing initiatives and respiratory equipmentclaimed to purify the air breathed byworkers to meet the threshold limitvalues, thereby protecting workers fromthe disease.11 These values were the basisfor all subsequent revisions through the1960s.12 In the 1970s, following a NationalInstitute for Occupational Safety andHealth (NIOSH) recommendation tolower the threshold limit value for silicaand eliminate sand as an abrasive inblasting, industry mobilized to fight offattempts to make the existing thresholdlimit value more stringent.
T7e Establishment ofthe AirHygiene Foundation
The origins of the threshold limitvalue for silica cannot be understoodwithout a brief review of the political andsocial environment within which it wasestablished. In 1935, as thousands ofworkers sued for damages and the liabilitycrisis deepened, the disclosure that ap-proximately 700 workers had died of anacute form of the disease while drilling atunnel for Union Carbide at GauleyBridge, WV, further heightened publicand business concern.13 Early in the year,business executives in the dusty trades,together with the Mellon Institute ofIndustrial Research in Pittsburgh, met atthe University Club to form an IndustrialDust Institute.14 Dr E. R. Weidlein,director of the Mellon Institute, suggestedthat the new organization identify thespecialists who "may not be properlyqualified and whose results might, there-
February 1995, Vol. 85, No. 2254 American Jolrnal of Public Health
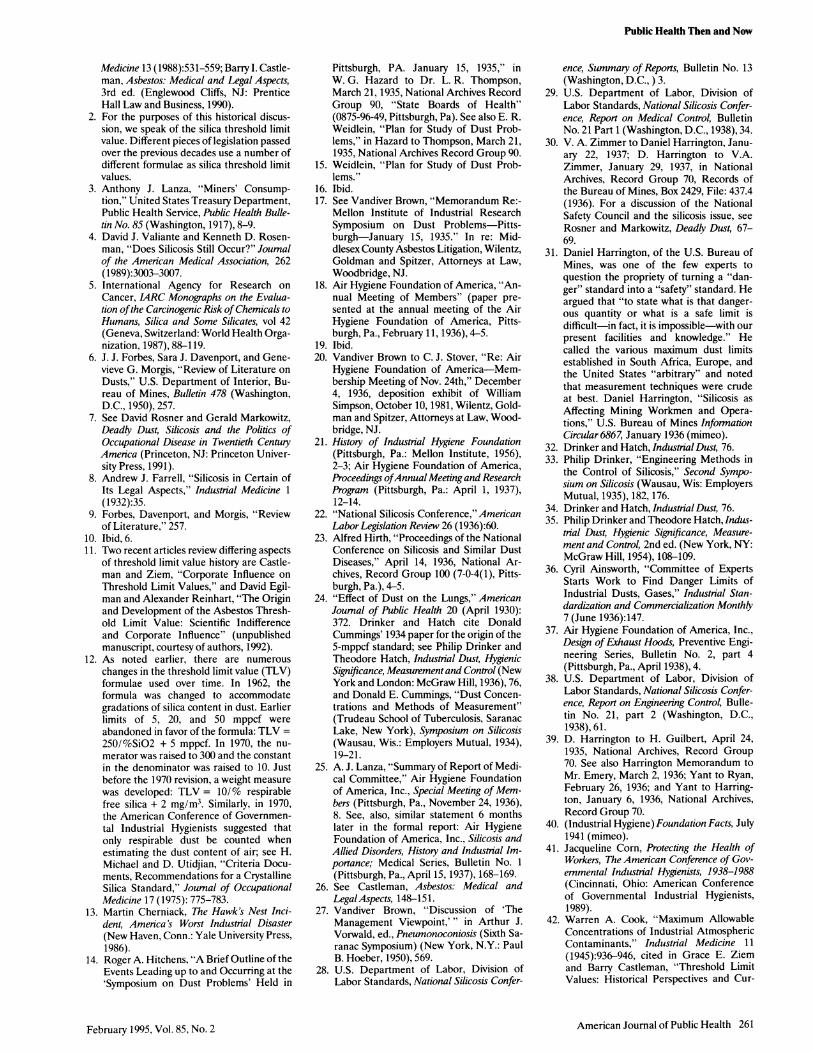
Collecting dust samples with a midget impinger in the vicinity of the sand slinger.Note dust visible in shafts of light. J. P. Harmon, 1946. From the NationalArchives, Still Picture Division, Record Group 70 (70-G-20-63197).

Public Health Then and Now
fore, not be entirely acceptable ... ; to bein position to make reasonable grants toqualified individuals and agencies to studyspecial problems or phases of problems."He wrote that industry should supportresearch that could be "important fromboth medical and legal standpoints in thepreparation of court cases" as well asassisting "in the preparation of safetycodes and fair laws."'5 Weidlein outlineda five-point program by which industrycould band together to set the agenda foritself and for the nation. One part of thatprogram was to establish "authoritativeand approved standards" for the permis-sible dustiness in the silica industries. Byvoluntarily establishing standards and aid-ing industry to live up to them, companieswould be able to erect a "defense againstpersonal injury suits."16 By January 15,1935, the time of the first meeting ofwhatwas to become the Air Hygiene Founda-tion, Vandiver Brown, general attorney ofthe Johns Manville Corporation, relatedthat most participants agreed that therewas a "need of some form of concertedaction on the part of those industriespresently or potentially involved."'17
At the end of 1935, the Air HygieneFoundation of America was incorporatedwith 20 company and industry groups. In aconfidential report of the foundation'sannual meeting in February 1936, H. B.Meller, the managing director, wrote that,without any counteracting body to quellthe "misleading publicity about silicosis,... this publicity will result in a flood ofclaims, whether justified or unjustified,and will tend toward improperly consid-ered proposals for legislation."'8 Thefoundation's solution to the liability disas-ter that awaited industry was to set theground rules that would protect industryfrom unjust claims of liability. Part of theprogram would be a legislative attempt toremove silicosis from the courts by incor-porating the disease into state workers'compensation systems. Another partwould be to improve work conditions."The primary object of the Foundationshould be to improve to practical limitsthe dust conditions in the industry andthat the successful carrying out of thebasic program will benefit labor andscience equally with the industries."'9Later in the year, Brown encouraged otherasbestos companies to join the foundation,writing that "although the Air HygieneFoundation is approaching various prob-lems . . . from an unbiased point of view, itis, nevertheless, the creature of industryand is the one institution upon which
employers can rely completely for a sympa-thetic appreciation of their viewpoint."20
By the time of its annual meeting onApril 1, 1937, the foundation's member-ship had grown to 168 industries andtrade associations. The foundation estab-lished immediate legitimacy in the fieldsof medicine, law, and engineering byattracting to its various working commit-tees nearly all of the top names in thesilicosis research and engineering commu-nities: A. J. Lanza, R. R. Sayers, DanHarrington, Leroy U. Gardner, R. R. Jones,0. A. Sander, and Philip Drinker. Theyestablished research links with Harvard,the Saranac Laboratory, and the Universityof Pennsylvania, as well as with the MellonInstitute itself. In the midst of the Depres-sion, with limited funds available and thefederal government incapable of embark-ing on a major research effort, the AirHygiene Foundation and the public healthresearchers associated with it emerged asmajor forces shaping occupational lungresearch and the technical debate aboutsilicosis in the United States.2'
The Development ofthe SilicosisThreshold Limit Value
Shortly after the foundation wasestablished, it was given an opportunity toplay a major role in shaping federalactivities regarding silicosis. This roleincluded the establishment of maximumallowable concentrations of silica. OnApril 14, 1936, the US Department ofLabor's Division of Labor Standardscalled together representatives of labor,industry, and the professions for a confer-ence on silicosis, which convened inWashington.22
In a major address to the conference,Alfred Hirth, a corporate lawyer workingfor Owens-Illinois Glass Company andchair of the foundation's Legal Commit-tee, argued that safe levels of dustexposure could be established and thatindustry could achieve these levels throughengineering and equipment technology.He argued that "the existence of a dusthazard is already on its way out,"23maintaining that small amounts of silicawould cause only small amounts of silicadust to be retained in the lungs. Thisminimal exposure was not expected to bedisabling or to affect an average workeradversely during his or her work life.
Shortly after Hirth's speech, the AirHygiene Foundation's Medical Commit-tee, chaired by Lanza, suggested a stan-dard of 5 million particles per cubic foot(mppcf) of air.24 Yet in an analysis aimed
at their own membership, the foundationraised serious questions about the validityof the standard. While agreeing that itwould be most beneficial to be able to"state what are permissible thresholds ofdustiness to which workmen are ex-posed," the committee concluded that"there is not available ... the knowledgeupon which to base such thresholds."Nevertheless, it allowed that "there isevidence that a concentration of morethan five million particles per cubic foot ofa highly siliceous dust is dangerous" andthus recommended that as the limit.25
Johns Manville was successful in pro-mulgating the 5-mppcfvalue as the thresh-old limit value for asbestos based on theview that asbestosis was a less seriousdisease than silicosis.26 In 1950, VandiverBrown, Johns Manville's secretary andgeneral attorney, observed the impor-tance of the silica debate in shaping theasbestos standard itself. He questioned"whether there exists sufficient data corre-lating the disease [asbestosis] to the degreeof exposure to warrant any determinationthat will even approximate accuracy," buthe surmised that the asbestos thresholdlimit value may have been set "because ithad already been prescribed for silicosis."27
The National Silicosis Conferenceadopted the 5-mppcf standard for silicosisas one below which workers would notexperience disease but did not issue anywarning about the limitations of its use asa standard. Despite the presence of theAir Hygiene Foundation on its majormedical and engineering committees andthe fact that its own report was drafted byindustry representatives, the conferencesuggested that "dust concentrations ofless than 5 million particles per cubic footof air are considered safe even in caseswhere the dust contains a high percentageof free silica."28 The conference endorsedthe prevalent notion that every industrycould adopt standards that would reduceor eliminate the silicosis hazard.29 Theauthor of the conference's summary docu-ment was W. Dean Keefer, director of theIndustrial Division of the National SafetyCouncil.?0
We now think of standards as being aresult of scientific study and analysis, butthis was clearly not the case for silica. Thestandard for silica was developed retro-spectively and as part of a politicalcompromise that traded on workers'health.3' Philip Drinker and TheodoreHatch, two of the leading engineersconcerned with the problem of silicosisand both associated with the Air HygieneFoundation, stated in their 1936 textbook,
American Journal of Public Health 255February 1995, Vol. 85, No. 2

Public Health Then and Now
Man wearing American Optical Company R-9100 Respirator, which was approvedfor use in pneumoconlosis-producing and nuisance dusts. Companies claimed Intheir advertisements that half-face respirators such as this could protect againstsilicosis. H. H. Schrank, 1940. From the National Archives, Still Picture Division,Record Group 70 (70-G-1 1-51799).
Industrial Dust, Hygienic Significance, Mea-surement and Control that the 5-mppcfstandard "lacks entirely any publisheddata in its support."32 Earlier, Drinkerhad traced the origins of the thresholdlimit value to Donald E. Cummings butbelieved that Cummings "must have ar-rived at it by a process of 'intuitivecorrelation' " based on "his own seasonedopinion."33 In their text, Drinker andHatch concluded that "adopting stan-dards of permissible dustiness for each
harmful dust has a medicolegal appealthat is not at all justified by the dataavailable today."m Nearly 20 years later,in their 1954 edition, their statement iseven more telling. The standard had beendeveloped because it was "about as lowas modern engineering methods canachieve."35 Others who helped to developstandards recognized that they were de-signed not only to protect the workers andto provide governments with a basis forprotective legislation, but also to "protect
industrial concerns from racketeering inliability cases."36
Despite the acknowledgment amongsome professionals that the silica thresh-old limit value was based on practicalengineering rather than on health criteria,the standard promoted a sense of safetyand security among workers exposed tosilica dust. In the mid-1930s, the distinc-tion between reducing dust levels to whatwas practical and reducing them to whatwas safe became blurred in publicationsaimed at explaining criteria for the devel-opment of respiratory protection devicessuch as respirators, exhaust hoods, andfilters. For example, the Air HygieneFoundation's report on the design ofexhaust hoods maintained that equipmentcould reduce dust concentrations to a"safe level." Even though the report citesDrinker and Hatch in its bibliography, itdoes not acknowledge any uncertaintyabout what is a safe level.37 The NationalSilicosis Conference Report on EngineeringControl said that "improved designs inabrasive-blasting equipment [includingposi-tive pressure helmets] are available that willkeep the exposures to less than 5 millionparticles per cubic foot."38 Advertisementsfor respirators often claimed that theirproducts provided safety because they metthe Bureau of Mines criteria, which werepartly based on the threshold limit value.
As early as 1935, experts in theBureau of Mines were writing of theirmisgivings about the promotion of respira-tors as an alternative to improved ventila-tion, the substitution of nonsilica materi-als in sandblasting, and other forms ofprotection. Donald Harrington, for ex-ample, chief of the bureau's Health andSafety Branch, saw the respirator as "onlya sort of stop gap, allowing the employerto use the fact of having furnished therespirator as a bar to being responsible forany condition which might arise throughthe breathing of dust by employees."39But by 1941, the Air Hygiene Foundation,pleased with its role during the Depres-sion of "having helped calm the hysteria[about silicosis] then rampant," decidedto apply its expertise more broadly andchanged its name to the Industrial Hy-giene Foundation.40
Threshold Limit Valuesand theAmerican ConferenceofGovernmental IndustrialHygienists
After the Depression decade, theAmerican Conference of Governmental
February 1995, Vol. 85, No. 2256 American Journal of Public Health

Public Health Then and Now
Industrial Hygienists, a voluntary associa-tion made up primarily of professionalsemployed by the various levels of govern-ment, took up the task of issuing yearlythreshold limit values and maximum allow-able concentrations for a variety of sub-stances.41 In 1945, Warren Cook pub-lished an article listing maximum allowableconcentrations for 118 substances.42 By1946, the conference adopted the Indus-trial Hygiene Foundation and NationalSilicosis Conference standards as its own,setting the threshold limit value for silicaat 5 mppcf for high silica content dust. Butthroughout the 1940s, there was anongoing discussion within the organiza-tion about what these limits meant. Withinthe American Conference of Governmen-tal Industrial Hygienists' Threshold Lim-its Committee, there were two competinginterpretations about the meaning of theterm "maximum allowable concentra-tions" and, later, "threshold limit values."On the one hand, some held that themaximum allowable concentration valueshould represent a firm line between anexposure that results in illness and onethat represents healthfulness. On theother hand, some maintained that themaximum allowable concentration shouldprovide a margin of safety for workerswho might be overly susceptible to certaintoxins. Given the understanding that thescience of industrial hygiene was inca-pable of determining which levels wereabsolutely safe and which were potentiallyharmful, it was accepted that standardswere not established truths but weresubject to annual evaluation and revision:"They should not be adopted as fixed orlegal values, but merely as guides to assistus in defining more or less safe workingconditions."43 The threshold limit valuewas understood to be a "rubber yardstick"rather than a concrete divider betweensafety and danger.44 The ambiguous mean-ing of the threshold limit values andmaximum allowable concentrations rarelyescaped the confines of discussion withinthe professional community.45
By the 1950s and early 1960s, asthreshold limit values were accepted byindustrial hygienists, a few experts re-mained skeptical of both their use as astandard and the accuracy of the measure-ments that were essential for their imple-mentation. In 1950, a Bureau of Minesreport reviewing the literature on dustsconcluded that, despite the perceivedassurance of safety that the establishedstandard implied, "what constitutes thatquantity limit no one knows, not withstand-ing the fact that numerous so-called
Pangborn-type CE-supplied air respirator. These respirators were tested by theBureau of Mines in their laboratories but not at work sites. S. J. Pierce, 1942.From the National Archives, Still Picture Division, Record Group 70(70-G-1 1-54285).
threshold limits are now being an-nounced, some of them embodied in stateregulations or laws."46 The report as-serted that "the attempt to embody inlaws and regulations having the force oflaw rigid standards as to air dustinesswould seem to be a travesty ofjustice."47
Some of the participants in thedebate over the meaning of thresholdlimit values acknowledged that the settingof standards was a political compromisethat had to balance the interests ofemployers, employees, and equipmentmanufacturers. In 1948, Lawrence Fair-hall, chair of the American Conferenceof Governmental Industrial HygienistsThreshold Limits Committee, reported
that the committee had sought "valueswhich, on the one hand, protect theindividual workman, and on the otherhand, impose no impossible burden onthe manufacturer."48
In 1966, Hervey Elkins, an industrialhygienist who also served on the Thresh-old Limits Committee, identified threecompeting positions in the establishmentof the threshold limit values. First, equip-ment manufacturers generally pushed fora standard that would not, in Elkins'words, "adversely affect the value of hisproduct in the market place." Hence, thisgroup generally argued for standards thatwould allow them to build equipmentcapable of meeting less stringent criteria.
American Journal of Public Health 257February 1995, Vol. 85, No. 2

Public Health Then and Now
Second, the employer "would prefer alimit which will protect most workers, buthe would rather not undergo the extraexpense for providing for the most suscep-tible." Finally, workers themselves pre-ferred "to have the limit set at a concentra-tion where no one at all will be affected."49In the best of circumstances, scientificevidence would determine the standard.But in reality, the differing relative powerof participants in the process was critical.
Standards historically represented theperspectives of the first two participantsidentified by Elkins. During the NewDeal, when the Air Hygiene Foundationand other industry-sponsored groupstalked among themselves and amongother professionals, this processwas some-times made explicit. F. S. Mallette andH. B. Meller, managing director of theAir Hygiene Foundation, pointed out thetendency among even industrial hygieniststo be lulled "into false security by relianceon the protection given by strict adher-ence to these permissible limits." Butrather than inform workers of the poten-tial dangers they faced, the authorssuggested that companies conduct "peri-odic physical evaluations" as a "biologicalcheck" for "concentrations of hazardoussubstances which had been sanctioned asbeing safe." They maintained that thevery hazards of the job were effectivedevices for screening out workers whosephysique left them susceptible to illness.Calling this process "industrial selection,"they endorsed the idea that standards"are based on experience with workmenwho are best fitted to withstand industrialhazards, those who are vulnerable to theexposure being weeded out by naturalselection."50 In the Darwinian world ofthe factory, standards were set thatprotected the "average" worker whileoccupational illnesses and periodic screen-ing for disease became tools in the naturalprocess of industrial selection. Those whobecame sick were de facto defined as"unfit."
In the years following the acceptanceof the silica threshold limit value, a fewstudies continued to show that workerswere still getting silicosis. These studiesraised questions about the adequacy ofthe silica standard and the assurances ofindustries and equipment manufacturersregarding their good-faith efforts to pro-vide a safe working environment. In themid 1950s, Victoria Trasko told theAmerican Conference of GovernmentalIndustrial Hygienists ofUS Public HealthService data that indicated "that silicosiscontinues to be a widespread occupa-
tional health problem in the UnitedStates."51 Elsewhere, she and Henry Doylelamented the stubborn persistence ofsilicosis in the industrial landscape:"Should an early investigator of silicosisreturn to the industrial scene, he mightjustifiably be surprised that, after manydecades of study, this disease has still notbeen vanquished."52 They worried thatsome "have yielded to the complacencythat full control of silicosis has beenachieved."53 The Bureau of Mines' "Re-view of the Literature" in 1950 similarlyconcluded that silicosis was "a widespreadindustrial hazard which is probably in-creasing"54 and questioned the usefulnessof the threshold limit value given recentevidence: "No definite, absolutely reliablestandards of allowable dustiness areknown."55 Equally troubling to the bureauwas what it described as an "apparentlyconcerted effort to hide" the silicosisproblem rather than publicize it to work-ers and the general public. It recom-mended a new "remedy": the "educationof workers in the necessity of takingavailable precautions, including physicalexaminations."56
Despite the questions about theadequacy of the threshold limit value, theAmerican Conference of GovernmentalIndustrial Hygienists did not undertake aserious reassessment of the standardthrough the 1950s. Elkins rememberedthe process by which the same silica andasbestos threshold limit values were re-newed each year:
The first half of most meetings [of theThreshold Limits committee] was de-voted to minor changes in the wordingof the preface [of the threshold limitvalue list]. Then the chemicals weretaken up.... It was usually by then fiveor ten minutes to train or plane time.These were devoted to postponingaction on silica, asbestos and othermineral dusts.57Without both the impetus of a
barrage of lawsuits and the constantpressure from the popular press as oc-curred in the 1930s, the scrutiny that J. J.Forbes, Trasko, and Doyle called for didnot occur. Instead, the silica standardtook on a meaning well beyond that of a
"rubber yardstick" or hesitant guide forindustrial hygienists, and remained virtu-ally untouched from 1935 through themid-1960s. During this period, workerscontinued to get sick and industry contin-ued to believe it was safe from liabilitysuits. While the professionals and indus-tries had access to information thatindicated the limitations of their equip-ment and of the standard itself, workers
were largely left out of the discussion.Further, organized labor, then pressingfor higher wages and better benefits,rarely pressed issues that challengedmanagement perogatives over control ofthe shop floor.58
NIOSH, OSHA, and the Debateover Further Protective Measures
While the discussions over the silicastandard were largely carried out among asmall group of industrial hygienists, engi-neers, and industry representatives, abroader discussion over dangerwas emerg-ing within government and among thebroader public during the 1970s and1980s. The impetus for this concern wasthe passage of the Occupational Safetyand Health Act, which created NIOSH inthe Department of Health, Education,and Welfare and the Occupational Safetyand Health Administration (OSHA) inthe Department of Labor.59
NIOSH formulated criteria docu-ments to lay out the state of knowledge ofvarious chemical and other exposures,and to recommend standards that OSHAcould use to protect workers' health.Among the first substances that NIOSHsought to look at was silica, one of theoldest and presumably best-documentedoccupational dangers. It was believed thatdeveloping the scientific base for anenforceable standard for silica would bepolitically less controversial than establish-ing standards for newer toxic sub-stances.60 In the early 1970s, NIOSH hadcontracted for a survey of working condi-tions in sandblast operations. For theprevious 2 decades, it was assumed thatsilicosis could be prevented if workersused respirators that lowered inhaled dustto levels below the threshold limit value.But Austin Blair, an industrial hygienistfor the Boeing Corporation, made a bluntevaluation of respirators: "Some mentionshould be made of respirator fit. Theydon't. They're designed in a single sizewhich, in the opinions of the interviewedblasters, fit no one"; moreover, "mainte-nance was universally poor to non-
existent." Overall, he found, "the protec-tion afforded these workmen is, on theaverage, marginal to poor."'61
Although the companies that usedsandblasting were clearly lax in theirmaintenance of the equipment, Blair wasparticularly concerned that the equip-ment manufacturers themselves bore a
special responsibility for the poor state ofprotection afforded workers. He sug-gested that NIOSH and OSHA concen-
February 1995, Vol. 85, No. 2258 American Journal of Public Health

Public Health Then and Now
trate their reform efforts on this group:"The average abrasive blasting companycannot afford the luxury of a safety orindustrial hygiene staff or consultant. Thesupplier is their staff or consultant."62
The indictment of protective equip-ment provided by Blair's report wasserious enough. But shortly thereafter,NIOSH received evidence that silicosis,far from being a historical entity, re-mained a serious problem. In mid-1974,two other NIOSH-supported projects re-ported on cases of silicosis among ship-yard workers and steel fabricators in NewOrleans and elsewhere. One report byMorton Ziskind indicated that the bestway of protecting workers was to consideralternatives to sand as an abrasive insandblasting.63
The response ofNIOSH officials wasswift. In 1974, NIOSH issued a criteriadocument recommendation for a crystal-line silica standard that recommendedthat "occupational exposure shall becontrolled so that no worker is exposed toa time-weighted average concentration offree silica greater than 50 micrograms percubic meter of air." The document furthersuggested that silica be banned as anabrasive in blasting:
uncontrolled abrasive blastingwith silicasand is such a severe silicosis hazardthat special attention must be given tothis problem. Silica sand, or othermaterials containing more than 1% freesilica, should be prohibited as an abra-sive substance in abrasive blasting clean-ing operations.64
A few months after this documentappeared, a meeting at the IndustrialHealth Foundation in Pittsburgh broughttogether industry representatives, indus-trial health specialists, and government.At that time, many even within industryagreed that "silicosis, of all the pneumoco-nioses, is identified as claiming the largestnumber of victims, either alone or withtuberculosis."65 J. P. O'Neill, chief ofOSHA's Division of Health StandardsDevelopment, explained that "silicosisapparently is not, as they once hoped, anoccupational disease that would disap-pear." Instead, "the prevalence of silicosishas not really dropped at all. We havemuch better methods of control, but weneed a standard that would be much moreeffective, and be based upon better datathan the present standard that is on thebooks."66
The response from the affected indus-tries at this meeting was reminiscent oftheir historical rejoinders to previousattempts to reevaluate the standard. First,
A road construction worker sawing through pavement. Neither worker Is wearingan air-supplied hood. Photo courtesy of Kenneth Linch, National Institute ofOccupational Safety and Heafth, Division of Respiratory Disease Studies,Morgantown, WVa.
participants argued that medical informa-tion regarding the incidence rates ofsilicosis was incomplete and thereforecast doubt on any statement regarding theinadequacy of the current threshold limitvalues. Without better epidemiology, low-ering the threshold limit value or banningsand was premature.67 Second, there wascontention over "the ability of presentengineering technology to create ventila-tion and hooding systems efficient enoughto meet the new regulations." Finally,coming on the heels of the first OPEC oilcrisis and shortage, industry participantsargued that the investment in new equip-ment that would be needed to meet thenew standard would be "cost-prohibitiveor energy-wasteful."68
The NIOSH recommendation to banthe use of sand in blasting, along with thevarious studies that were being used tosupport the new standard, provoked animmediate, powerful response from sand-blasting equipment manufacturers, paint-ing contractors, and sand producers. Thefull history of the NIOSH proposal torevise the silica standard and the contro-versy that erupted following the publica-tion of NIOSH's criteria document re-mains to be written. However, therecommendation provoked a storm ofprotest and a massive organizing effort byindustry groups, especially those in Texasand California, to ensure that OSHA didnot adopt the recommendation.
In February 1975, just after theNIOSH document was published in theFederal Register, more than 50 peoplerepresenting these various industries gath-ered together in Houston to form theSilica Safety Association. Their purpose,they proclaimed, was to "investigate andreport on possible health hazards involvedin [the] use of silica products and torecommend adequate protective mea-sures considered economically feasible."69The president of the association, L. L.Sline, owner of Sline Industrial Painters,Inc, appealed for support among theaffected industries by warning that theNIOSH recommendation "could haveserious cost impact for all sandblastingoperations." He asserted that the primarypurpose of the organization was "torepresent interested parties in the at-tempt to assure the continued use of sandin abrasive blasting operations."70
Over the next few months, the SilicaSafety Association developed its argu-ment on behalf of the continued use ofsand. The organization held that if work-ers used "proper protective devices,"there was little danger of excessive expo-sure. Therefore, if equipment was capableof lowering exposure to "safe" levels,there was no need to change the existingthreshold limit value for silica. The associa-tion also argued that there was littleevidence that silicosis was a seriousproblem and no data to support federal
American Journal of Public Health 259February 1995, Vol. 85, No. 2

Public Health Then and Now
regulation of the industries that usedsandblasting.71 It mobilized industry andemployed a consulting firm to organize itslobbying efforts in Washington. Distrust-ful of NIOSH and its staffs strongadvocacy of a stringent standard, theassociation centered its efforts on convinc-ing OSHA to delay adoption of thestandard.72
While NIOSH was promulgating newdocuments, OSHA was consumed by theoverwhelming responsibility of decidingon which NIOSH recommendations toadopt with a relatively small, dispersedstaff. With competing demands for re-sources, OSHA focused on substancesother than silica.73 Following the appoint-ment of the widely respected Eula Bing-ham in 1977 as OSHA head, the agencyactively sought to ban sand in abrasiveblasting and to lower the threshold limitvalue for silica. In 1981, the Silica SafetyAssociation claimed credit for forestallingand delaying the adoption of the propos-als: "to date, the efforts of [the associa-tion] have been the major influence in thecontinuation of sand blasting in theStates."74 The final blow to the NIOSHproposal to ban sand was dealt by thechange in the federal government whenRonald Reagan was elected president. Asthe executive director of the Silica SafetyAssociation commented,
with the change in administration, theever increasing avalanche of govern-ment regulations have been reversed.Economic impact studies are now arequired part of every regulatory pro-cess. As a result, OSHA's proposedabrasive blasting standard has beenmoved from a top priority "target"regulation to the back burner.75
In February 1982, the Silica SafetyAssociation Newsletter noted that "it'sbeen a while since our last newsletter[because] Federal regulations have alsobeen few and far between; so, as we sayabout sleeping dogs...."76 Later, Slineappealed for continued support because"the SSA has been saving you anywherebetween $150.00 to $300.00 [for] everysandblaster you have had working for youeach year." He argued that industry oweda great deal to the association because ithad saved substantial sums "by not havingsandblasters and others working in thearea of Abrasive Blasting medically exam-ined and other unnecessary procedures."77
Slines' appeal to keep the associationopen, however, was unsuccessful. By June1983, in a special meeting of the associa-tion's board of directors, it was noted that"regulatory activity in and from Washing-
ton is at a dormant level, . . . no foreseenpush on abrasive blasting is seen as long asthe present administration is in power,[and] . . . requests to [the association] forinformation from members are rare." Theboard of directors therefore concludedthat "the association should be put onhold."78 The records of the organizationwere placed in storage and the officesclosed.
The Renewed Interest in Revisingthe Slica Standard
The recent election of a Democraticpresident, and the attempt to revitalizethe Department of Labor in general andNIOSH and OSHA in particular, has onceagain led to a reconsideration of the silicastandard. From 1993 to 1994 alone, twomajor conferences on silica-related dis-eases were held in the United States. Inthe 1930s, with a severe liability crisisforcing industry to act, standards wereestablished that reflected the economicand technical capabilities of equipmentmanufacturers, industries that used sand,and insurance companies that paid liabil-ity claims. During the generally conserva-tive political environment of the yearsfollowing World War II, business effortsto downplay the seriousness of the silicahazard along with the incorporation ofsilicosis into state workers compensationlaws led to the cessation of efforts torevise the silica standard. Despite continu-ing studies that indicated that silicosisremained a problem, few voices called forlegislative action. In the 1970s, followingthe passage of Occupational Safety andHealth Act and the establishment ofNIOSH and OSHA, the issue of thestandard once again became important. Itappears that only the concerted efforts ofaffected industries and the conservativetriumph of the 1980s forestalled thebanning of sand as an abrasive in blasting.
Today, we tend to think that stan-dards have evolved from the intrinsic logicof scientific and technological impera-tives. Better equipment and greater under-standing of the physiology and chemistryof disease, for example, have led to moreaccurate measurement of toxins, moreprecise estimates of danger, and greatersafety for the worker. However, we haveshown that economic concerns and techni-cal feasibility interacted to promote theconcept of safety thresholds for specificsubstances and led to the adoption ofstandards. These standards, in turn, werepublicly promoted as safety levels, when,in fact, business representatives and tech-
nical experts understood them to be acompromise that represented the powerof different competing interests. In theface of a technical inability to measureless than 5 mppcf of dust and the scientificuncertainty regarding what is a safe level,industry spokesmen argued against lower-ing threshold limit values because such anact would force industry to bear the costsof potentially unnecessary safety mea-sures. From the late 1930s through thelate 1960s, this argument was accepted byindustrial hygienists and public healthofficials, providing a powerful politicalrationale for maintaining the value de-spite ongoing evidence that workers con-tinued to get silicosis.
Following the establishment ofOSHA and NIOSH, and a growing aware-ness that some substances are dangerousat any level, a serious effort arose to lowerthe threshold limit value for silica to thepoint where it would be virtually bannedin some industries. Faced with continuingcase findings of silicosis among workers inthe dusty trades and the ongoing scientificuncertainty regarding a truly safe level,officials in NIOSH and later OSHAsought ways to minimize the danger to theworkforce, even if it meant increased coststo industries. They argued that it was theresponsibility of government agencies toerr on the side of safety rather than on theside of the possibly adverse economicimpact to industry. In the 1980s, the olderargument that had prevailed for most ofthe century once again gained ascen-dancy. Although in the 1990s the argu-ments will be framed primarily in epide-miological and technical terms, thehistorical record indicates that importanteconomic and social issues are at work inframing the questions of when and inwhat amounts silica is safe or danger-ous. [1
AcknowledgmentsMost of the information was gathered duringthe course of writing our book Deadly Dust,Silicosis and the Politics ofOccupational Diseasein Twentieth Century America. We gratefullyacknowledge the support of the NationalEndowment for the Humanities, the Guggen-heim Foundation and the Professional StaffCongress-City University of New York facultygrants program. Some of the informationreported has been gathered in the course ofresearch funded by Cook and Butler, a law firmin Houston, Tex., representing silicotic work-ers.
References1. Barry I. Castleman and Grace E. Ziem,
"Corporate Influence on Threshold LimitValues," Amenican Journal of Industrial
260 American Journal of Public Health February 1995, Vol. 85, No. 2
Medicine 13 (1988):531-559; Barry I. Castle-man, Asbestos: Medical and Legal Aspects,3rd ed. (Englewood Cliffs, NJ: PrenticeHall Law and Business, 1990).
2. For the purposes of this historical discus-sion, we speak of the silica threshold limitvalue. Different pieces of legislation passedover the previous decades use a number ofdifferent formulae as silica threshold limitvalues.
3. Anthony J. Lanza, "Miners' Consump-tion," United States Treasury Department,Public Health Service, Public Health Bulle-tin No. 85 (Washington, 1917), 8-9.
4. David J. Valiante and Kenneth D. Rosen-man, "Does Silicosis Still Occur?" Journalof the American Medical Association, 262(1989):3003-3007.
5. International Agency for Research onCancer, IARC Monographs on the Evalua-tion ofthe Carcinogenic Risk ofChemicals toHumans, Silica and Some Silicates, vol 42(Geneva, Switzerland: World Health Orga-nization, 1987), 88-119.
6. J. J. Forbes, Sara J. Davenport, and Gene-vieve G. Morgis, "Review of Literature onDusts," U.S. Department of Interior, Bu-reau of Mines, Bulletin 478 (Washington,D.C., 1950), 257.
7. See David Rosner and Gerald Markowitz,Deadly Dust, Silicosis and the Politics ofOccupational Disease in Twentieth CenturyAmerica (Princeton, NJ: Princeton Univer-sity Press, 1991).
8. Andrew J. Farrell, "Silicosis in Certain ofIts Legal Aspects," Industrial Medicine 1(1932):35.
9. Forbes, Davenport, and Morgis, "Reviewof Literature," 257.
10. Ibid, 6.11. Two recent articles review differing aspects
of threshold limit value history are Castle-man and Ziem, "Corporate Influence onThreshold Limit Values," and David Egil-man and Alexander Reinhart, "The Originand Development of the Asbestos Thresh-old Limit Value: Scientific Indifferenceand Corporate Influence" (unpublishedmanuscript, courtesy of authors, 1992).
12. As noted earlier, there are numerouschanges in the threshold limit value (TLV)formulae used over time. In 1962, theformula was changed to accommodategradations of silica content in dust. Earlierlimits of 5, 20, and 50 mppcf wereabandoned in favor of the formula: TLV =250/%SiO2 + 5 mppcf. In 1970, the nu-merator was raised to 300 and the constantin the denominator was raised to 10. Justbefore the 1970 revision, a weight measurewas developed: TLV = 10/% respirablefree silica + 2 mg/m3. Similarly, in 1970,the American Conference of Governmen-tal Industrial Hygienists suggested thatonly respirable dust be counted whenestimating the dust content of air; see H.Michael and D. Utidjian, "Criteria Docu-ments, Recommendations for a CrystallineSilica Standard," Joumal of OccupationalMedicine 17 (1975): 775-783.
13. Martin Cherniack, The Hawk's Nest Inci-dent, America's Worst Industrial Disaster(New Haven, Conn.: Yale University Press,1986).
14. Roger A. Hitchens, "A Brief Outline of theEvents Leading up to and Occurring at the'Symposium on Dust Problems' Held in
February 1995, Vol. 85, No. 2
Pittsburgh, PA. January 15, 1935," inW. G. Hazard to Dr. L. R. Thompson,March 21, 1935, National Archives RecordGroup 90, "State Boards of Health"(0875-96-49, Pittsburgh, Pa). See also E. R.Weidlein, "Plan for Study of Dust Prob-lems," in Hazard to Thompson, March 21,1935, National Archives Record Group 90.
15. Weidlein, "Plan for Study of Dust Prob-lems."
16. Ibid.17. See Vandiver Brown, "Memorandum Re:-
Mellon Institute of Industrial ResearchSymposium on Dust Problems-Pitts-burgh-January 15, 1935." In re: Mid-dlesex County Asbestos Litigation, Wilentz,Goldman and Spitzer, Attorneys at Law,Woodbridge, NJ.
18. Air Hygiene Foundation of America, "An-nual Meeting of Members" (paper pre-sented at the annual meeting of the AirHygiene Foundation of America, Pitts-burgh, Pa., February 11, 1936), 4-5.
19. Ibid.20. Vandiver Brown to C. J. Stover, "Re: Air
Hygiene Foundation of America-Mem-bership Meeting of Nov. 24th," December4, 1936, deposition exhibit of WilliamSimpson, October 10, 1981, Wilentz, Gold-man and Spitzer, Attorneys at Law, Wood-bridge, NJ.
21. History of Industrial Hygiene Foundation(Pittsburgh, Pa.: Mellon Institute, 1956),2-3; Air Hygiene Foundation of America,Proceedings ofAnnualMeeting and ResearchProgram (Pittsburgh, Pa.: April 1, 1937),12-14.
22. "National Silicosis Conference," AmericanLabor Legislation Review 26 (1936):60.
23. Alfred Hirth, "Proceedings of the NationalConference on Silicosis and Similar DustDiseases," April 14, 1936, National Ar-chives, Record Group 100 (7-0-4(1), Pitts-burgh, Pa.), 4-5.
24. "Effect of Dust on the Lungs," AmericanJoumal of Public Health 20 (April 1930):372. Drinker and Hatch cite DonaldCummings' 1934 paper for the origin of the5-mppcf standard; see Philip Drinker andTheodore Hatch, Industrial Dust, HygienicSignificance, Measurement and Control (NewYork and London: McGraw Hill, 1936),76,and Donald E. Cummings, "Dust Concen-trations and Methods of Measurement"(Trudeau School of Tuberculosis, SaranacLake, New York), Symposium on Silicosis(Wausau, Wis.: Employers Mutual, 1934),19-21.
25. A. J. Lanza, "Summary of Report of Medi-cal Committee," Air Hygiene Foundationof America, Inc., Special Meeting of Mem-bers (Pittsburgh, Pa., November 24, 1936),8. See, also, similar statement 6 monthslater in the formal report: Air HygieneFoundation of America, Inc., Silicosis andAllied Disorders, History and Industrial Im-portance; Medical Series, Bulletin No. 1(Pittsburgh, Pa., April 15, 1937), 168-169.
26. See Castleman, Asbestos: Medical andLegalAspects, 148-151.
27. Vandiver Brown, "Discussion of 'TheManagement Viewpoint,'" in Arthur J.Vorwald, ed., Pneumonoconiosis (Sixth Sa-ranac Symposium) (New York, N.Y.: PaulB. Hoeber, 1950), 569.
28. U.S. Department of Labor, Division ofLabor Standards, National Silicosis Confer-
Public Health Then and Now
ence, Summaty of Reports, Bulletin No. 13(Washington, D.C., ) 3.
29. U.S. Department of Labor, Division ofLabor Standards, National Silicosis Confer-ence, Report on Medical Control, BulletinNo.21 Part 1 (Washington, D.C., 1938),34.
30. V. A. Zimmer to Daniel Harrington, Janu-ary 22, 1937; D. Harrington to V.A.Zimmer, January 29, 1937, in NationalArchives, Record Group 70, Records ofthe Bureau of Mines, Box 2429, File: 437.4(1936). For a discussion of the NationalSafety Council and the silicosis issue, seeRosner and Markowitz, Deadly Dust, 67-69.
31. Daniel Harrington, of the U.S. Bureau ofMines, was one of the few experts toquestion the propriety of turning a "dan-ger" standard into a "safety" standard. Heargued that "to state what is that danger-ous quantity or what is a safe limit isdifficult-in fact, it is impossible-with ourpresent facilities and knowledge." Hecalled the various maximum dust limitsestablished in South Africa, Europe, andthe United States "arbitrary" and notedthat measurement techniques were crudeat best. Daniel Harrington, "Silicosis asAffecting Mining Workmen and Opera-tions," U.S. Bureau of Mines InformationCircular 6867, January 1936 (mimeo).
32. Drinker and Hatch, Industrial Dust, 76.33. Philip Drinker, "Engineering Methods in
the Control of Silicosis," Second Sympo-sium on Silicosis (Wausau, Wis: EmployersMutual, 1935),182,176.
34. Drinker and Hatch, Industrial Dust, 76.35. Philip Drinker and Theodore Hatch, Indus-
trial Dust, Hygienic Significance, Measure-ment and Control, 2nd ed. (New York, NY:McGraw Hill, 1954),108-109.
36. Cyril Ainsworth, "Committee of ExpertsStarts Work to Find Danger Limits ofIndustrial Dusts, Gases," Industrial Stan-dardization and Commercialization Monthly7 (June 1936):147.
37. Air Hygiene Foundation of America, Inc.,Design of Exhaust Hoods, Preventive Engi-neering Series, Bulletin No. 2, part 4(Pittsburgh, Pa., April 1938), 4.
38. U.S. Department of Labor, Division ofLabor Standards, National Silicosis Confer-ence, Report on Engineering Control, Bulle-tin No. 21, part 2 (Washington, D.C.,1938), 61.
39. D. Harrington to H. Guilbert, April 24,1935, National Archives, Record Group70. See also Harrington Memorandum toMr. Emery, March 2, 1936; Yant to Ryan,February 26, 1936; and Yant to Harring-ton, January 6, 1936, National Archives,Record Group 70.
40. (Industrial Hygiene) Foundation Facts, July1941 (mimeo).
41. Jacqueline Corn, Protecting the Health ofWorkers, The American Conference of Gov-emmental Industrial Hygienists, 1938-1988(Cincinnati, Ohio: American Conferenceof Governmental Industrial Hygienists,1989).
42. Warren A. Cook, "Maximum AllowableConcentrations of Industrial AtmosphericContaminants," Industrial Medicine 11(1945):936-946, cited in Grace E. Ziemand Barry Castleman, "Threshold LimitValues: Historical Perspectives and Cur-
American Journal of Public Health 261

Public Health Then and Now
rent Practice," Journal of OccupationalMedicine 31 (November 1989):911.
43. Corn, Protecting the Health of Workers.44. Warren Cook, in 1945, was one of the first
to suggest that the threshold limit valuecould be used as a "handy yardstick." Buthe warned against the view that "compli-ance with the figures listed would guaran-tee protection against ill health." SeeCook, "Maximum Allowable Concentra-tions," cited in Ziem and Castleman, 911.
45. Corn, 60.46. Forbes, Davenport, and Morgis, "Review
of Literature," 10.47. Ibid, 11-12.48. Corn, Protecting the Health of Workers,
36-37.49. Hervey B. Elkins, "Threshold Limit Values
and their Significance," Transactions of the28thAnnualMeetingoftheAmerican Confer-ence of Govemmental Industrial Hygienists,1966, 118.
50. H. Meller and F. S. Mallette, "ControllingAir Contaminants," National Safety News41 (1940):19.
51. Victoria M. Trasko, "Some Facts on thePrevalence of Silicosis in the United States,"Transactions of the 18th Annual Meeting ofthe American Conference of GovemmentalIndustial Hygienists (Philadelphia, Pa., April21-24, 1956), 53.
52. H. N. Doyle, et al., "Accomplishments inthe Epidemiologic Study of Silicosis in theUnited States," AMA Archives ofIndustrialHealth 12 (July-December, 1955):48.
53. Ibid, 54.54. Forbes, Davenport, and Morgis, "Review
of Literature," 2.55. Ibid, 6.56. Ibid.57. Hervey B. Elkins, Contribution to the
"History of Industrial Hygiene," Transac-tions of the 40th Annual Meeting of theAmerican Conference of Govemmental In-dustrial Hygienists (Los Angeles, Calif., May7-12, 1978) 86. See also the "Meeting ofSectional Committee-Z37," November27, 1941, in National Archives RecordGroup 100, "Records of the Division ofLabor Standards," Sectional Committee,1941-45, in which the agenda for theAmerican Standards Association Commit-tee on Allowable Concentrations of ToxicDusts and Gases (Z37) also places silica asthe very last item on the agenda. In another
262 American Journal of Public Health
retrospective look at the evolution ofstandards, D. D. Irish worried that a"serious problem is the possibility thatsomeone might hide behind the standardand use as his excuse, 'I was following thecode.'" D. D. Irish, "Evolution of OurConcepts of Standards," Archives of Envi-ronmental Health [29th Annual Meeting ofthe Industrial Hygiene Foundation, Pitts-burgh, Pa., 1964] 10 (April 1965):546.
58. Gerald Markowitz and David Rosner,"Seeking Common Ground: A History ofLabor and Blue Cross," Joumal of HealthPolitics, Policy and Law 16 (Winter 1991):695-718.
59. For the history of the Occupational Safetyand Health Act and policy concerns withinOSHA and NIOSH during the early 1970s,see Nicholas Askounes Ashford, Crisis inthe Workplace: Occupational Disease andInjury (Cambridge, Mass: MIT Press, 1976).
60. David Rosner, telephone interview withJohn Finklea, June 30,1993.
61. Austin Blair, "Abrasive Blasting Respira-tory Protective Practices," (Cincinnati,Ohio: U.S. Department of Health, Educa-tion and Welfare, National Institute forOccupational Safety and Health, Divisionof Laboratories and Criterion Develop-ment, April 1974).
62. Ibid.63. Morton Ziskind, "Accelerated Silicosis in
Sandblasters," 5 RO1 CH 00387, "Termi-nal Progress Report, June 1, 1971-August31, 1974" (New Orleans, La: TulaneUniversity School of Medicine). See also J.Leslie Goodier, et al., Industrial Health andSafety Criteria for Abrasive Blast CleaningOperations (Cincinnati, Ohio: U.S. Depart-ment of Health, Education and Welfare,National Institute for Occupational Safetyand Health, Division of Laboratories andCriteria Development, September 1974).
64. Occupational Safety and Health Reporter,"National Institute for Occupational Safetyand Health Criteria Document Recommen-dation for a Crystalline Silica Standard"(1974):716, 718. See also Federal Register39, no.250 (December 27,1974).
65. Joan C. Todd, "Silicosis: NIOSH CriteriaDocument on Respirable Free Silica PosesMany Questions," Engineering and MiningJoumal, 176 (May 1975):111.
66. J. P. O'Neill, "Silica Standard Implications,"Proceedings of the Symposium on Silicosis,
March 12-13, 1975 (Pittsburgh, Pa.: Indus-trial Health Foundation, 1976), 30.
67. Discussion from audience, Proceedings ofthe Symposium on Silicosis, March 12-13,1975 (Pittsburgh, Pa.: Industrial HealthFoundation, 1976),32.
68. Todd, "Silicosis," 113.69. Silica Safety Association, "Report of Pre-
liminary Meeting," Silica Safety Associa-tion Records, vol. 8 (February 5, 1975),222-223, deposition exhibit in the posses-sion of the law firm of Cook and Butler,Houston, Tex. (hereafter referred to as"SSA Papers").
70. L. L. Sline to Dear Sir, March 21, 1975.SSA Papers, vol. 1.
71. "More on Proposed OSHA Standard forCrystalline Silica Use," Materials Perfor-mance (May 1975):41-42.
72. See the Silica Safety Association's reactionto a letter by John Finklea, director ofNIOSH, which said, in part, that "NIOSHis currently exploring with OccupationalSafety and Health Administration (OSHA)the need to vigorously enforce the presentsilica standard and the possibility of takingemergency action including prohibition ofsilica sand in abrasive blasting to furtherprevent the future occurrence of acutesilicosis." See John Finklea to colleague,June 9, 1976, in SSA Papers, vol. 1,302-303.
73. See Ashford, Crisis in the Workplace.74. B.C. Wright, "Silica Safety Update-
History-Current Endeavors-FuturePlans," SSA Papers, vol. 9 (May 26,1981):184.
75. Ibid.76. Silica Safety Association Newsletter, Febru-
ary 22, 1982, SSA Papers.77. L. L. Sline, January 18, 1983, SSA Papers,
vol. 23, no. 146. In 1978, a similar requestwas made, pointing out the financialbenefits that the association afforded itsmembership: "[The Silica Safety Associa-tion] was formed in 1975 to prevent OSHAfrom eliminating or restricting sandblast-ing.... [The association] has saved youfrom heavy expenses.... YOU HAVEBENEFITTED. NOW WE NEEDYOU...." See L.L. Sline, Donald Wil-liams, Don Dean, Paul Knobloch, WalterWhite to SSA Membership, August 14,1978, SSA Papers.
78. B. C. Wright, Silica SafetyAssociation News-letter, June 22, 1983, SSA Papers.
February 1995, Vol. 85, No.2





























