Embed Size (px)
Citation preview

PoCT for the Early Detection of Acute Kidney Injury
Dr. Gustavo F Méndez Machado MD MSC FESC
Cardiología / Fellow of the European Society of Cardiology
Sub-Director Médico [Nocturno L-M-V]
Hospital General de Zona No 11 Xalapa IMSS

Evolución en el Diagnóstico Cardiaco y
Renal
1950 ’s
1960 ’s
1970 ’s
1980 ’s
1990 ’s
2000
The renal testing arena is in need of the introduction
of novel, early and more sensitive and specific biomarkers
AMI
WBC count
LDH, SGOT, SGPT
CPK
CK -MB
Troponin -T
Troponin - I
AKI
Change in serum creatinine
Change in serum creatinine
No
Ch
an
ge
Time
Conger JD, Am J Kidney Dis 26:565-576, 1995.
Star RA, Kidney Int 54:1817-1831, 1998.

3
Daño renal agudo (AKI)
AKI, anteriormente denominado
insuficiencia renal aguda, es comun
– Definicion de AKI es subjectiva y condiciona
dificultades en la detecion y diagnostico
La disminucion subita de la funcion renal
condiciona la acumulacion de los
desechos nitrogenados, tales como el
nitrogeno ureico, urea y creatinina
La nomenclatura de AKI describe
condiciones con daño estructural y
disfuncion Devarajan P. J Am Soc Nephrol. 2006;17:1503-1520.
Ricci Z, Ronco C. Crit Care. 2008;12:230-236.

4
Daño Renal Agudo (AKI):
Incidencia y Prevalencia
Incidencia de 1% a 25% en países desarrollados
– Incidencia de terapia de reemplazo renal (RRT) entre 3.4% a 4.9%
– Mortalidad Hospitalaria secundaria a falla renal aguda severa con necesidad de terapia de reemplazo 60 al 70% en varios países.
Prevalencia en la Terapia Intensiva (ICU)
– 5% to 6% requieren RRT en ICU
– Mortalidad General en pacientes con AKI de hasta 60.3%
Uchino S. Curr Opin Crit Care. 2006:12:538-543.
Uchino S, et al. JAMA. 2005;294:813-818.
5
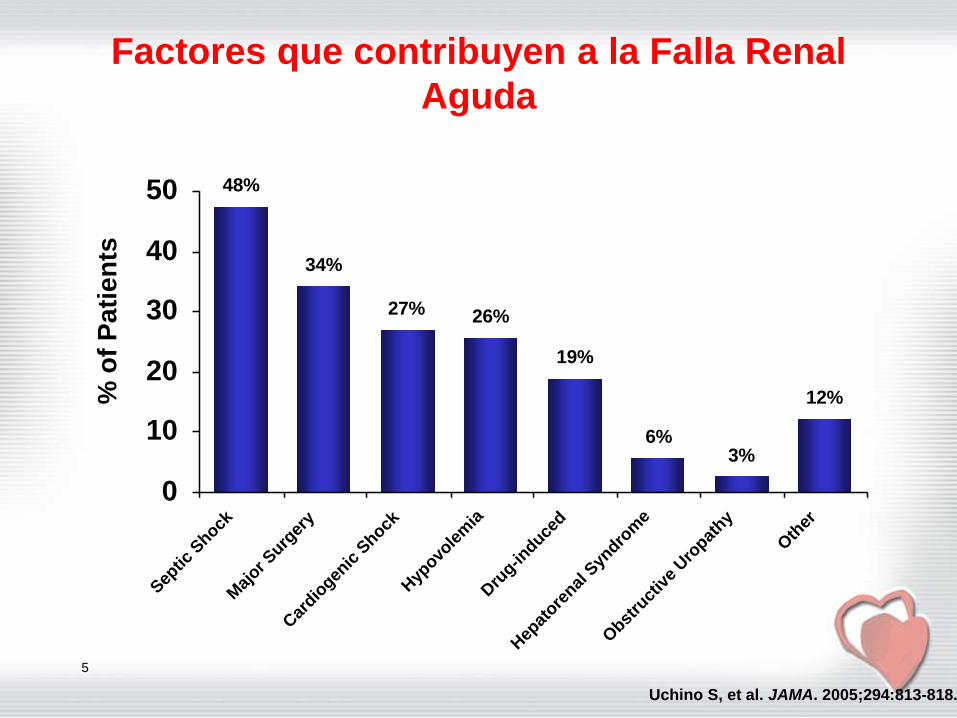
Factores que contribuyen a la Falla Renal
Aguda
48%
34%
27% 26%
19%
6%3%
12%
0
10
20
30
40
50
Sep
tic S
hock
Maj
or Surg
ery
Car
diogen
ic S
hock
Hyp
ovole
mia
Dru
g-induce
d
Hep
atore
nal S
yndro
me
Obst
ruct
ive
Uro
pathy
Oth
er
% o
f P
ati
en
ts
Uchino S, et al. JAMA. 2005;294:813-818.

6
Age-Adjusted Hospitalization Rates for
Kidney Disease by Type of Kidney Failure
(1980-2005)
MMWR Morb Mortal Wkly Rep. 2008;57:309-312.
Rate of hospitalization from ARF increased from
1.8 per 10,000 population in 1980 to 36.5 in 2005

7
Mortality in Acute Renal Failure
No ARF ARF0%
25%
50%
75%M
ort
ali
ty
ARF is an independent risk factor for death
Star RA, Kidney Int 54:1817-1831, 1998.
7%
34%

8
RIFLE Criteria for Defining Acute Renal
Failure
Bellomo R, et al. Crit Care. 2004;8:R204-R212.
ARF, acute renal failure; GFR, glomerular filtration rate; SCr, serum creatinine
*With an acute rise >0.5 mg/dL
GFR Criteria Urine Output Criteria
Increased SCr x 1.5 or
GFR decrease >25%<0.5 mL/kg/h x 6 h
Increased SCr x 2 or
GFR decrease >50%<0.5 mL/kg/h x 12 h
Increased SCr x 3
GFR decrease 75%
or SCr ≥4 mg/dL*
<0.3 mL/kg/h x 24 h
or
anuria x 12 hours
Persistent ARF = complete loss
of kidney function >4 weeks
End stage kidney disease
(>3 months)
Risk
Injury
Failure
Loss
ESKD
High
Sensitivity
High
Specificity

9
Acute Kidney Injury Network Criteria
for the Definition and Classification of AKI
RRT, renal replacement therapy; SCr, serum creatinine
Stage SCr Criteria
Urine Output
Criteria
Stage 1Increase in SCr ≥26.4 µmol/L
or increase to ≥1.5-2.0-fold
from baseline
<0.5 mL/kg/h for >6 h
Stage 2Increase in SCr to >2.0-3.0-fold
from baseline<0.5 mL/kg/h for >12 h
Stage 3
Increase in SCr to ≥3-fold
or SCr ≥354 µmol/L
with an acute rise >44 µmol/L
or initiation of RRT
<0.3 mL/kg/h for >24 h
or anuria ≥12 h
Mehta RL, et al. Crit Care. 2007;11:R31.

Serum Creatinine
Gold standard, but far from ideal
• Not sensitive to kidney insults that don’t affect
filtration
• Creatinine is affected by non-renal factors:
– Protein intake
– Muscle mass
– Age
– Race
– Sex
• In AKI it takes 24-48 hours for serum creatinine to
rise.
– As much as 50% of kidney function can be lost in that
time

11
Creatinina Serica
AKI es actualmente diagnosticado utilizando la
creatinina serica
Indicador no confiable durante cambios agudos
– Concentraciones podrian no cambiar hasta una
reduccion del 50% de la funcion renal
– No refleja de forma aguda la funcion renal hasta que se
alcanza un estado de estabilidad (puede tomar hasta 48
hrs)
– El daño renal ocurre durante el retraso en el
diagnostico
Util marcador para estimar la GFR
Pobre valor en el periodo postquirurgico
El retraso en el diagnostico previene el optimo
traamiento de AKI Bellomo R, et al. Intensive Care Med. 2004;30:33-37.
Nguyen MT, et al. Pediatr Nephrol. 2008;23:2151-2157.
Star RA. Kidney International. 1998;54:1817-1831.

12
Adapted from Moran SM, Myers BD. Kidney International. 1985;27:928-937
GFR
(mL/min)
Serum
Creatinine (SCr)
(mg/dL)
Creatininina no es el Biomarcador Ideal
0
1
2
3
4
5
6
70
20
40
60
80
100
120 Surgery, MI, sepsis
Reversal of ischemia
0 7 14 21 28
Time, days

Urine Output
May be misleading
Legrand M and Payen D. Ann Intensive Care. 2011;1:13.
• A minimum of 6 hours must
pass to determine urine
output.• Nonsustained decreases of
urine output do not
necessarily imply decreased
GFR.
– Can represent a physiological
renal adaptation for
homeostasis

BIOMARKER NEEDS
AKI Biomarkers
BIOMARKERS
IL-18
NGAL
KIM1
L-FABP
Cystatin C
• Early detection
• Differential diagnosis
• Prognosis
MOST AKI MARKERS ARE NOT FDA
APPROVED
AND AVAILABLE ONES DO NOT MEET
CURRENT CLINICAL NEEDS.

Possible Utility of New Biomarkers
Early detection
Differential diagnosis
Prognosis
– Predict need for dialysis
– Reversibility
– Risk of death

Unmet Clinical Needs
AKI is difficult to assess.
Mortality is high and it carries a very
high cost.
Currently available methodologies
and biomarkers are not meeting
clinical needs.
New biomarkers are on the horizon
to assist with AKI risk assessment.

Biomarcadores de Daño Renal
17

Clasificacion ADHF
18

19

20
Fonarow GC JAMA 2005:572

21

22

23

24

25

26

Definition and Pathophysiology of Cardiorenal
Syndrome Subtypes – HF and AKI
Ronco C et al. Eur Heart J 2010;31:70-711

28
Neutrophil Gelatinase Associated Lipocalin
(NGAL), Lipocalin-2, Siderocalin: Physiology
and Clinical Relevance Member of the lipocalin superfamily
Normally expressed at very low levels in kidney, lungs, heart, stomach, and colon
Increased after injury and ischemia– One of the most highly induced proteins in kidney after
ischemic or nephrotoxic AKI in animal models
– Highly up-regulated in the distal convoluted tubule during injury/ischemia, leading to a marked increase of NGAL in the urine
Protective role– Murine models of renal ischemia-reperfusion showed
amelioration of morphologic and functional injury when treated with NGAL
Early diagnostic biomarker for AKI
Devarajan P. Nephrol Dial Transplant. 2008;23:3737-3743.
Parikh CR, Devarajan P. Crit Care Med. 2008;36(suppl):S159-S165.
Mishra J, et al. J Am Soc Nephrol. 2004;15:3073-3082.

29
Induction of Mouse Kidney NGAL After
Ischemia
25 kD
55 kD
Mishra J, et al. J Am Soc Nephrol. 2003;14:2534-2543.
Unilateral Ischemia Reperfusion Bilateral Ischemia Reperfusion
NGAL
Tubulin
NGAL
Tubulin
25 kD
55 kD
Con 3 hr 12 hr 24 hr Con 3 12 24 48 72 Hours
Con = control
NGAL expression was highly induced after ischemia

30
Ischemic Kidneys Synthesize Renal NGAL
mRNA
Adapted from Schmidt-Ott KM, et al. J Am Soc Nephrol. 2007;18:407-413.
mR
NA
Levels
, fo
ld c
han
ge
Hours Post-Ischemia
*P≤.05
NGAL
FGF2 (basic fibroblast growth factor)
HF (hypoxia-inducible factor)
BMP7 (bone morphogenic protein 7)
0 10 20 30 40 50
**
**
1000
100
10
1
0.1
0.01
*
*
***
*
*
** *
**

31
Function of NGAL
Role in kidney development
– Promotes epithelial differentiation by
targeting a stromal/intestinal/progenitor niche
at the periphery of the developing kidney
– Affects the structure of established epithelia
Binds labile iron in cytosol and
pericellular space
Iron-associated NGAL regulates iron-
responsive genes (ferritin, transferrin
receptor)
Devarajan P. Nephrol Dial Transplant. 2008;23:3737-3743.
Schmidt-Ott KM, et al. J Am Soc Nephrol. 2007;18:407-413.

NGAL
Siderophore
Labile Iron
·O 2
-
Haber Weiss
Fe3+
Fe2+
O 2
OH ·H 2O 2
Fenton
Ferric Iron = Fe3
+ ; Ferrous iron= Fe2
+ ; hydrogen peroxide = H2
O2
;
Hydroxyl radical = OH. ;Hydroxide anion = OH - ; oxygen = O2;
superoxide anion = . O2
-
ACS
AKIOxidative Stress Reactions
OH-H2O
++

Pe
rce
nt
N>100,000 patients
Slide courtesy of Christopher De Filippi
Prevalence of Renal Dysfunction in Patients
with AHF
• Renal dysfunction is a likely element of pathophysiology of
heart failure and highly prevalent as demonstrated in
findings from the ADHERE database.
Adams KF et al. Am Heart J. 2005; 149:209-216

34
NGAL for the Diagnosis of AKI in the
Emergency Department
Nickolas TL, et al. Ann Intern Med. 2008;148:810-819.
N = 635
0
250
500
750
1000
1250
1500
*
*
*
* *
*
AKI Prerenal
Azotemia
CKD Normal
Kidney
Function
Uri
ne
NG
AL
, μ
g/g
0.00
2.00
4.00
6.00
8.00
10.00
12.00
14.00
16.00
18.00
20.00
*
*
*
**
***
*
AKI Prerenal
Azotemia
CKD Normal
Kidney
Function
Pre
se
nti
ng
Se
rum
Cre
ati
nin
e, m
g/d
L
NGAL Serum Creatinine

35
Meta-Analysis: Accuracy of NGAL in AKI
Meta-analysis of 19 diagnostic studies (2538 patients)
NGAL was a valuable and early predictor of AKI, both overall and across a diverse range of clinical settings
The cutoff NGAL value for optimum sensitivity and specificity across all settings was >100 ng/mL
A more consistent cutoff value of >150 ng/mL was identified when using standardized platforms Haase M, et al. Am J Kidney Dis. 2009;54:1012-1024.
Setting Specificity AUC-ROC
Diagnostic
Odds Ratio
AKI across settings 85.1 0.815 18.6
AKI after cardiac surgery 75.1 0.775 13.1
AKI in critically ill patients 75.5 0.728 10.0
AKI after contrast infusion 96.3 0.894 92.0
AKI prediction using
serum NGAL86.6 0.775 17.9
AKI prediction using
urine NGAL84.3 0.837 18.6
Diagnostic and Prognostic Accuracy of NGAL

Cardiorenal Syndrome Type 1: Creatinine
Increase in Acute HF Patients.
Gottlieb SS et al. J Card Fail. 2002;8:136. Smith G, J Card Fail. 2003 Feb;9(1):13-25
X X X X X X X X X X X X X X
X
0.5
0.4
0.3
0.2
0.1
0
20
40
60
80
100
1 3 5 7 9 11 13 15
Days
%
Cr
Small increases in Cr are associated with poor
outcomes and occur in 30% of patients
hospitalized for HF
“Type 1 CardioRenal Syndrome ”

NO. OF PATIENTS
REFERENCE TP FP FN TN NGAL CUTOFF (NG/ML)
SENSITIVITY (%; 95% CI) SPECIFICITY (%; 95% CI)
Mishra et al, 2005 (p) 14 3 6 48 > 25 70.0 (45.7-87.2) 94.1 (82.8-98.5)
Mishra et al, 2005 (u) 20 1 0 50 > 50 100.0 (80.0-100.0) 98.0 (88.2-99.9)
Wagener et al, 2006 11 23 5 42 > 400 68.8 (41.5-87.9) 64.6 (51.7-75.8)
Dent et al, 2007 38 5 7 73 > 150 84.4 (69.9-93.0) 93.6 (85.0-97.6)
Zappitelli et al, 2007 12 7 4 16 > 10 75.0 (47.4-91.7) 69.6 (47.0-85.9)
Hirsch et al, 2007 (p) 8 1 3 79 >100 72.7 (39.3-92.7) 98.8 (92.3-99.9)
Hirsch et al, 2007 (u) 8 0 3 80 > 100 72.7 (39.3-92.7) 100.0 (94.3-100.0)
Wagener et al, 2008 44 172 24 186 > 450 64.7 (52.1-75.6) 52.0 (46.7-57.2)
Bennett et al, 2008 78 8 21 89 >150 78.8 (69.2-86.1) 91.8 (83.9-96.1)
Ling et al, 2008 10 8 3 19 -- 76.9 (46.0-93.8) 70.4 (49.7-85.5)
Koyner et al, 2008 (p) 8 13 10 41 > 280 44.4 (22.4-68.7) 75.9 (62.1-86.1)
Koyner et al, 2008 (u) 12 19 6 35 > 550 66.7 (41.2-85.6) 64.8 (50.6-77.0)
Nickolas et al, 2008 20 16 3 502 > 80 87.0 (65.3-96.6) 96.9 (94.9-98.2)
Lima et al, 2008 5 12 1 34 -- 83.3 (36.5-99.1) 73.9 (58.6-85.3)
Wheeler et al, 2008 19 74 3 47 > 140 86.4 (64.0-96.4) 38.8 (30.3-48.2)
Xin et al, 2008 2 8 1 22 > 250 66.7 (12.5-98.2) 73.3 (53.8-87.0)
Cruz et al, 2009 47 46 17 191 > 150 73.4 (60.7-83.3) 80.6 (74.9-85.3)
Makris et al, 2009 (CIN) 5 6 1 44 60 90.0 (54.1-99.5) 88.0 (75.0-95.0)
Makris et al, 2009 (ICU) 6 7 1 17 > 190 85.7 (42.0-99.3) 70.8 (48.8-86.6)
Constantin et al, 2009 43 1 9 35 > 155 82.7 (69.2-91.3) 97.2 (83.8-99.9)
Tuladhar et al, 2009 (p) 7 13 2 28 > 420 77.8 (40.2-96.1) 68.3 (51.8-81.4)
Tuladhar et al, 2009 (u) 8 9 1 32 > 390 88.9 (50.7-99.4) 78.1 (62.0-88.9)
Haase-Fielitz et al, 2009 18 17 5 60 > 150 78.3 (55.8-91.7) 77.9 (66.8-86.3)
Sensitivity and Specificity of Studies for NGAL to Predict AKI
Haase M, Bellomo R, Devarajan R et al. Am J Kidney Dis. 2009;54:1012-24.

Discusión
3.METODOS DE MEDIDA DE UNGAL
• Los diferentes métodos existentes son inmunoensayos (reacciones antígeno-anticuerpo)
• Dependiendo de las secuencias del antígeno (uNGAL) que reconocen los anticuerpos utilizados, las concentraciones de uNGAL pueden variar significativamente método a método
• El uNGAL no es una forma molecular única

Discusión
4. Isoformas de NGAL en orina
ORIGEN DEL uNGAL
-Epitelio renal: DRA
-Neutrófilos infiltrando epitelio renal: DRA
-:Neutrófilos activados: Infección tracto urinario (ITU)
-Tejidos extrarrenales
MONOMÉRICO (25 KDa)
HOMODIMÉRICO (50 KDa)
HETERODIMÉRICO (135 KDa)
DRA
ITU
DRA


©2013 Astute Medical, Inc. PN 0138 Rev B 2013/03/19

A Rigorous Discovery-Validation Path
Was Taken
44
Discovery Study
340 proteins analyzed
(including KIM-1, urine
NGAL, plasma NGAL,
Cystatin-C, IL-18, pi-GST,
and L-FABP)
Validation Study
Primary Endpoint:
moderate to severe AKI
(KDIGO stage 2-3) within
12 hours of
sample collection
(based on serum
creatinine and hourly
urine output)
Sapphire Study
35 sites
(20 North America, 15 Europe)
Age > 21, Critically Ill3,
no AKI (Stage 2 or 3)4
N = 744
Vienna Cohort
Age > 18,
in ICU + Sepsis
N = 134
Duke Cohort
Age > 18,
At least 1 risk factor1
N = 123
Mayo Cohort
Age > 18,
At least 1 risk factor2
N = 265
N = 7285
No AKI
N = 416
AKI Stage 1
N = 211
AKI Stage 2
N = 83
AKI Stage 3
N = 18
16 patients excluded
(2 withdrew consent, 7
lost to follow-up, 7 with
invalid or missing test
results)
Best Two Markers
Dis
cov
ery
Va
lid
ati
on
Within
12 hrs
Kashani et al. Critical Care 2013, 17:R25

Revolutionary Biomarkers Were Identified
Biomarkers identified through hypotheses based on AKI pathophysiology
340 candidate biomarkers identified
Biomarkers ranked by ability to predict development of AKI RIFLE I or F within 12 to 36 hours
All possible combinations of two-four biomarkers (novel or previously described) were ranked
Top performing biomarkers identified– Tissue Inhibitor of Metalloproteinases-2 (TIMP-2)
– Insulin-like Growth Factor Binding-Protein 7 (IGFBP7)
45Kashani et al. Critical Care 2013, 17:R25

TIMP-2 and IGFBP7 Outperform Existing
Biomarkers
AUC for [TIMP-2]•[IGFBP7] was significantly greater than any existing
biomarkers 46
Kashani et al. Critical Care 2013, 17:R25

47
TIMP-2 and IGFBP7 Work Well In
Important Subgroups
Sepsis Surgery
Kashani et al. Critical Care 2013, 17:R25

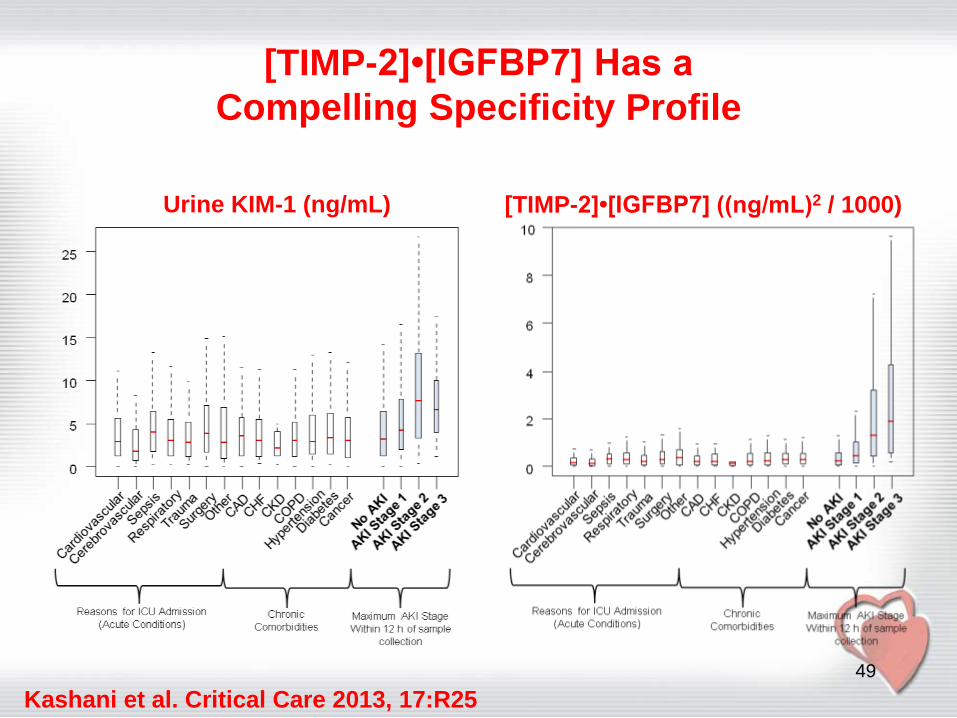
[TIMP-2]•[IGFBP7] Has a Compelling
Specificity Profile
48
Urine NGAL (ng/mL) [TIMP-2]•[IGFBP7] ((ng/mL)2 / 1000)
Kashani et al. Critical Care 2013, 17:R25
[TIMP-2]•[IGFBP7] Has a
Compelling Specificity Profile
49
Urine KIM-1 (ng/mL) [TIMP-2]•[IGFBP7] ((ng/mL)2 / 1000)
Kashani et al. Critical Care 2013, 17:R25

TIMP-2 and IGFBP7 Have Compelling Mechanistic Origins
in Early Cellular Injury
50
Proposed mechanismIGFBP7 & TIMP-2 are markers of G1
cell cycle arrest during early cell
injury
Renal tubular cells enter a short
period of G1 cell-cycle arrest
following injury
G1 cell-cycle arrest presumably
prevents the cells from dividing
when the DNA may be damaged
IGFBP7 & TIMP-2 may also signal in
autocrine and paracrine fashions,
spreading ‘alarm’ from the site of
injury
These processes and marker signals occur early enough in injury to take action
Kashani et al. Critical Care 2013, 17:R25
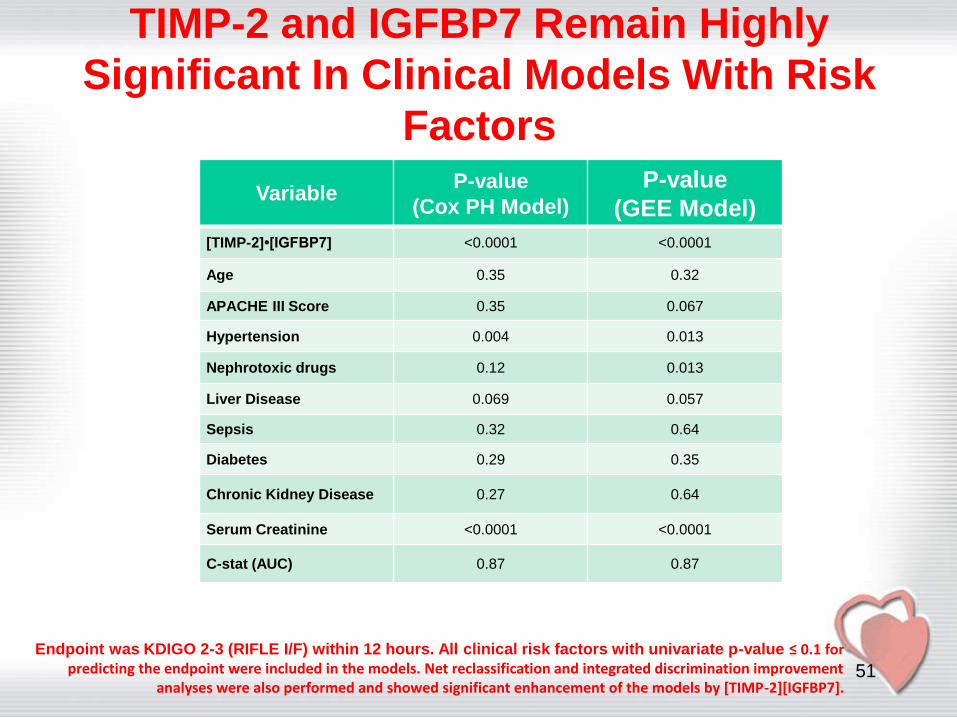
TIMP-2 and IGFBP7 Remain Highly
Significant In Clinical Models With Risk
Factors
51
VariableP-value
(Cox PH Model)
P-value
(GEE Model)
[TIMP-2]•[IGFBP7] <0.0001 <0.0001
Age 0.35 0.32
APACHE III Score 0.35 0.067
Hypertension 0.004 0.013
Nephrotoxic drugs 0.12 0.013
Liver Disease 0.069 0.057
Sepsis 0.32 0.64
Diabetes 0.29 0.35
Chronic Kidney Disease 0.27 0.64
Serum Creatinine <0.0001 <0.0001
C-stat (AUC) 0.87 0.87
Endpoint was KDIGO 2-3 (RIFLE I/F) within 12 hours. All clinical risk factors with univariate p-value ≤ 0.1 for predicting the endpoint were included in the models. Net reclassification and integrated discrimination improvement
analyses were also performed and showed significant enhancement of the models by [TIMP-2][IGFBP7].

Key Messages
Both IGFBP7 and TIMP-2 are inducers of G1 cell cycle arrest, a key mechanism implicated in AKI
IGFBP7 and TIMP-2 are new biomarkers for AKI and perform better than existing biomarkers for predicting the development of moderate or severe AKI (KDIGO stage 2 or 3) within 12 hours of sample collection
[TIMP-2]•[IGFBP7] significantly improved risk stratification when analyzed using Cox proportional hazards model, generalized estimating equation, integrated discrimination improvement or net reclassification improvement
Risk for major adverse kidney events within 30 days (MAKE30) elevated sharply above [TIMP-2]•[IGFBP7] values > 0.3 and doubled when [TIMP-2]•[IGFBP7] values were > 2.0
52
Kashani et al. Critical Care 2013, 17:R25

The NEPHROCHECK® Test System
The NEPHROCHECK® Test quantitatively
measures two urinary biomarkers --
tissue inhibitor of metalloproteinase 2
(TIMP-2) and insulin-like growth factor
binding protein 7 (IGFBP-7), which are
thought to be involved in G1 cell cycle
arrest in the earliest phases of inju
53

The NEPHROCHECK® Test System
54

MediBeacon has created a research grade technique that is clinically applicable
for real-time point-of-care Glomerular Filtration Rate measurement (mGFR).
MediBeacon has invented a fluorescent tracer agent (MB-102) that is removed
from the blood exclusively by the GFR mechanism of the kidneys.

57
Conclusiones
Sìndrome Cardio-Renal
Se requieren predictores tempranos, confiables
y exactos de daño renal agudo Biomarcadores.
NGAL POCT
IGFBP7 and TIMP-2 POCT
Mayor investigación en el tema


59
Cystatina C
Inhibidor proteasa Cysteina
– Sintetizada y liberada dentro de la sangre en rangos constantes por todas las celulas nucleadas
Cuantificación GFR
– Sus niveles sanguineos no se afectan po rla edad, genero, raza o desarrollo muscular
– Ventajas en los niños, ancioanos, UCI y paciente de alto riesgo (diabetes)
– Detecta camibios ligeros en la funcion renal
Incremento mas temprano que la creatinina en AKI
Nguyen MT, et al. Pediatr Nephrol. 2008;23:2151-2157.
Koyner JL, et al. Kidney Int. 2008;74:1059-1069.
Herget-Rosenthal S, et al. Kidney Int. 2004;66:1115-1122.

60
Interleukin-18 (IL-18)
Citokina proinflamatoria
Inducida y liberada en le tubulo proximal y se detecta en la urina siguiendo AKI isquemico – Detección 4–6 hours post-cardiopulmonary bypass
– Deteccíon UCI 48 horas antes de AKI
Marcador predictivo temprano de AKI y mortalidad – Predice desarrollo de AKI 24 horas antes que la creatinina
serica
Puede diferenciar entre necrosis tubular aguda y otros tipos de enfermedad aguda renal
No predice AKI mas rapido que NGAL urinario
Puede ser influenciado por otras variables y estados fisiopatologicos.
Parikh CR, et al. J Am Soc Nephrol. 2005;16:3046-3052.
Coca SG, et al. Kidney International. 2008;73:1008-1016.
Devarajan P. Expert Opin Med Diagn. 2008;2:387-398.

61
Kidney Injury Molecule 1 (KIM-1)
Proteina de transmembrana, altamente sobreexpresada en celulas del tubulo proximal despues de AKI isquemico o nefrotoxico
Bueno para evaluar el diagnostico de AKI
– No es solido para facilitar el diagnostico temprano
KIM-1 urinario distingue AKI isquemico de azoemia prerenal y CKD
Puede predecir los desenlaces adeversos y se asocia con medidas de severidad de la enfermedad
– Predice el riesgo de mortalidad despues de AKI
Muy especifico en daño isquemico o nefrotoxico, pero no es sensible en estadios tempranos
Nguyen MT, et al. Pediatr Nephrol. 2008;23:2151-2157.
Coca SG, et al. Kidney International. 2008;73:1008-1016.
Parikh CR, et al. J Am Soc Nephrol. 2005;16:3046-3052.
Devarajan P. Expert Opin Med Diagn. 2008;2:387-398.














