Embed Size (px)
Citation preview

Pocket Guidelinesfor the Care
ofMalaria Patients
Suparp Vannaphan
WHO Collaborating Center for Clinical Managementof Malaria
Faculty of Tropical Medicine, Mahidol UniversityBangkok, Thailand

First Edition 2009; 3000 copies,Printed and Published byWHO Collaborating Center for Clinical Management of MalariaBangkok, Thailand
All rights reserved. No part of this may be reproduced, stored in a retrieval system or transmitted in any form or by any means without the prior written permission of the copyright owner.Printed in Thailand.
Publication Data
Pocket Guidelines for the Care of Malaria PatientsP. cm.Include bibliographies and index.Vannaphan, Suparp
ISBN 978-974-11-1075-9

Contents
Preface 4Acknowledgements 5Introduction 6Map 7Part 1: The science of malaria in humans 8 Life cycle 9 Pathology 11 Pathogenesis 16Part 2: Nursing care of malaria infected patients 17 Early detection 17 Early treatment 22 Referral 27Part 3: Algorithm 31 Fever with negative blood film 31 Fever with positive blood film 32 Severe malaria 33 Cerebral malaria 34 Respiratory failure 35 Acute renal failure 36 Jaundice 37 Disseminated intravascular coagulation 38 Fever 39 Hypoglycemia 40 Prevention of secondary bacterial infection 41 Severe anemia 42 Hemoglobinuria 43 Health education 44 Algorithm Index 45Bibliography 46Index 47

Preface
This is the first set of pocket guidelines produced by theWHOCollaboratingCenter forClinicalManagementofMalaria fornursing care in the treatment of malaria. The contents compriseepidemiologicaldataregardingmalaria,basicmalariapathologyandpathogenesis,andguidelinesforpatientcare,includingclinicalcare,diagnosis and referral. It covers emergency treatment and effectivenursingcareduringthepre-referral,transfer,andpost-referralperiods.Inaddition,theseguidelinescontainalgorithmsforthemanagementofmalaria. Thisbooklet canbeused tohelpnurses care forpatientswithmalaria,enablingthemtorecovermorerapidly,andreducemorbidityand mortality rates from malaria. The nurse must have a soundknowledgeofthepathophysiologyofmalariaandshouldbesensitivetotheneedsofthepatient.Expertcarebythephysician,combinedwithgoodnursingcare, isneededtohelpthepatient recover fully.Research regarding new medication and medical care techniqueswill provide better management of malaria, resulting in a betterprognosis. Ihopethisbookletwillbeofbenefittobothnursesandpatients.
SuparpVannaphan,BScNursingTheHospitalforTropicalDiseases,FacultyofTropicalMedicineMahidolUniversity,Bangkok,ThailandFebruary2009
� Pocket Guidelines for the Care of Malaria Patients

Acknowledgements
I would like to express my thanks to Assoc. Prof. PratapSinghasivanon, Dean of the Faculty of Tropical Medicine, MahidolUniversity,forhiscontinuoussupportduringthepreparationofthisbook.ThanksalsotothelateProf.SornchaiLooareesuwan,Prof.PolratWilairatana,Prof.SrivichaKrudsood,Prof.NicholasJ.White,Assoc.Prof. Parnpen Viriyavejakul, Assoc. Prof. Pornthep Chanthavanich,Asst. Prof. Watcharee Chokejindachai, and Dr. Nick Walters, forreviewing this booklet. I would like to thank Assoc. Prof. SuvaneeSupavejforhermanyhelpfulsuggestionsforimprovingthisbooklet.Iwouldalsoliketothankmyparents,teachersandthepatientswhohavehelpedmetogaintheknowledgetowritethisbooklet.IwouldliketoacknowledgetheWHOSEAROfortheirgeneroussupportinthe printing of this booklet, without whose financial support, thisbookletwouldnothavebeenpublished.
Pocket Guidelines for the Care of Malaria Patients �

Introduction
MalariaiscausedbyprotozoanparasitesofthegenusPlasmodium,themostserious formbeing thespeciesP. falciparum.Patientswithseveremalariahave15to20%mortality. Itisestimatedthat300-660millionclinicalepisodesofP. falciparummalariaoccurred in2002(Snowet al.,2005).Previouslyextremelywidespread, malaria is now mainly confined to tropical regions ofAfrica,AsiaandLatinAmerica.Theproblemofcontrollingmalariainthesecountriesisaggravatedbyinadequatehealthinfrastructuresandpoorsocioeconomicconditions. The treatment of this condition requires hospitalization andsometimesintensivecare.Thesignsandsymptomsofseveremalariaarenon-specificandcanoccurwithotherseverefebrilediseasessuchasmeningitis,encephalitis,septicemia,typhoidfever,leptospirosisandviralinfectionswhicharecommonlyseeninmalariousareas.Inviewofthenon-specificpresentation,itisdifficulttorecommendastandardclinicalcasedefinitionforthedisease.Furthermore,thetreatmentofseveremalaria involvestheuseofmedicineswhichmaybetoxic.P. falciparum is becoming increasingly resistant tomany antimalarials.Thediagnosisofmalariabymicroscopyor rapiddiagnostic tests isveryimportant. Severe malaria should be treated in an intensive care unit, ifpossible.Inahospitalwherenecessaryequipmentforthemanagementofseveremalaria,suchasventilatorsforthemanagementofrespiratoryfailure,isnotavailable,thepatientshouldbereferredtoahigherlevelhospital.
� Pocket Guidelines for the Care of Malaria Patients

Fig.
1G
loba
lmal
aria
dis
trib
utio
n(C
ourt
esy
ofW
HO
Wor
ldM
alar
iaR
epor
t,20
06).
U
RLS
ourc
e:h
ttp:
//w
ww.
who
.int/
mal
aria
/mal
aria
ende
mic
coun
trie
s.ht
ml
Pocket Guidelines for the Care of Malaria Patients �
Are
asw
here
mal
aria
tran
smis
sion
occ
urs
Are
asw
ithli
mite
dris
k
No
mal
aria
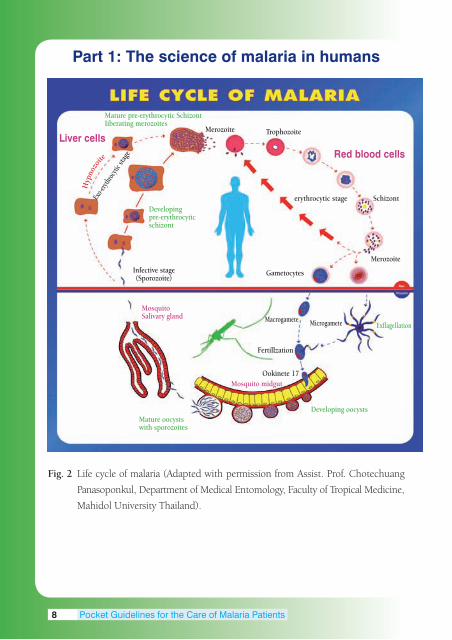
Part 1: The science of malaria in humans
Fig. 2 Lifecycleofmalaria(AdaptedwithpermissionfromAssist.Prof.Chotechuang
Panasoponkul,DepartmentofMedicalEntomology,FacultyofTropicalMedicine,
MahidolUniversityThailand).
Liver cells
Hyp
nozo
ite
Exo-e
rythro
cytic
stage
Mature pre-erythrocytic SchizontIiberating merozoites
Merozoite Trophozoite
Developingpre-erythrocyticschizont
Red blood cells
erythrocytic stage Schizont
Merozoite
GametocytesInfective stage(Sporozoite)
MosquitoSalivary gland
Mosquito midgutOokinete 17
Fertillzation
Macrogamete Microgamete Exflagellation
Developing oocystsMature oocystswith sporozoites
� Pocket Guidelines for the Care of Malaria Patients

Life cycle
Theinfectiveagentisthesporozoite,whichisinjectedintohumansbythebiteofan infectedfemaleanophelinemosquito.Sporozoitesdisappear fromthebloodwithin1hourandenter livercellswheretheyproliferateintomerozoitesandtheexoerythrocyticcyclestarts.Development in liver cells requires1-2weeksdependingupon thespeciesofPlasmodium (P. falciparum andP. vivax1week,P. malariae andP. ovale2weeks,nodataatpresentforP. knowlesiinhumans).InP. vivaxandP. ovale,somesporozoitesremaindormant(hypnozoites)formonthsoroccasionallyayearormorebeforeproliferation(relapse).Afterreplicationintheliver,parasitesundergoasexualmultiplicationintheerythrocytes.Themerozoitesinfecterythrocytesandconstitutetheerythrocyticformsoftheparasite.
Erythrocyticparasitedevelopment can follow twopathways. Inthe first pathway, asexual parasites develop from young ring formsthrough trophozoites and schizonts, which subsequently rupture,then reinvade erythrocytes. The erythrocytic cycle of schizogony isrepeatedover andover again, thus continuing the cycle ofmalariainfection. In the second pathway in P. falciparum infection afterapproximately1week,someerythrocyticparasitesdifferentiateintomaleandfemalegametocytes,thusenteringthesexualpathway.Whenmale and female gametocytes are ingested by female mosquitoesduringabloodmeal,fertilizationoccurs,resultinginazygote,whichpenetrates themosquitomidgutwall to formanoocyst containingsporozoites. When oocysts mature (10-14 days), they rupturereleasingsporozoites,whichinvadethesalivaryglandandarereadytobe injectedback intohumans, completing themalaria life cycle(White,2000).Table1 shows the characteristicsofP. falciparum, P. vivax, P. ovaleandP. malariae.ThedetailedcharacteristicsofP. knowlesiinhumansarenotavailableintheliteratureatpresent.
Pocket Guidelines for the Care of Malaria Patients �

Table 1.Characteristicsof4speciesofhumanmalaria(Looareesuwan et al.,1990)
P. falciparum P. vivax P. ovale P. malariae
Pre-erythrocyticstage(days) 5.5 8 9 14-15 Presenceofhypnozoites - + + - Pre-patentperiod(days) 8-25 8-27 9-27 15-30 Incubationperiod(days) 12(9-14) 15(12-17) 17(16-18) 28(18-40) orupto6-12 orlonger orlonger months Erythrocyticcycle(hours) 48 48 48 72 Natureofhosterythrocyte All Reticulocytes Reticulocytes Normocytes andyoung andyoung normocytes, normocytes Duffygroup positive Enlargementofhosterythrocyte - ++ + - Parasitemia/mm3
Average 40,000 2,000,000 20,000 50,000 Maximum 9,000 30,000 6,000 20,000 Primaryattack Severein Mildto Mild Mild non-immune severe Febrileparoxysm(hours) 16-36 8-12 8-12 8-10 orlonger Relapse - ++ ++ - Periodofrecurrence Short Variable Variable Verylong Durationofuntreated infection(years) 1-2 2-5 2-5 3-50 Stripplingofhosterythrocyte Maurer’s Schüffner’s Schüffner’s Ziemann’s clefts dots dots strippling
10 Pocket Guidelines for the Care of Malaria Patients

Pathology
In fatal falciparum malaria, autopsy specimens usually showcerebral edema. Brain herniation and brainstem compression canhappen,butthisoccursinlessthan5%ofcases(Fig2a)(Looareesuwanet al.,1990).Cutsurfacesofthebrainrevealpetechialhemorrhages(Fig2b).Microscopically,minutepetechialhemorrhagesarefrequent,particularlyinthewhitematter(Fig3a).Themicrovasculatureofthevitalorgansispackedwitherythrocytescontainingmatureformsoftheparasite.Bloodvesselsbecomeoccludedduetosequestrationofparasitizedredbloodcells(PRBCs).TheprocessofsequestrationispossibleduetotheattachmentofPRBCstothevascularendothelium(Fig 3b). Sequestration is not uniformlydistributed; it tends to begreatestinthebrainfollowedbytheheart,lungs,andsmallintestine(Pongponratnet al.,1991).
There isabundant intra-andextra-erythrocyticpigmentdepositinvitalorgans,suchastheliver(Fig4a),spleen,andplacenta.Intheliver, thesehemosiderinpigmentsareseentobepackedwithinthesinusoidalareas(Fig4b).Thekidneysoffatalmalariacasesoftenshowcongestionandareasofpetechialhemorrhage(Fig5a).PRBCs,aswellas hemosiderin pigment, are densely found within the glomerulartufts(Fig5b).
Pocket Guidelines for the Care of Malaria Patients 11

Fig. 2 Brainofcerebralmalaria.a)Brainedemawithherniationcanbeseen.b)Cut
surface of the cerebrum shows dispersed petechial hemorrhages, particularly
in the white matter (Courtesy, Department of Tropical Pathology, Faculty of
TropicalMedicine,MahidolUniversity,Thailand).
12 Pocket Guidelines for the Care of Malaria Patients

Fig. 3 Microscopicfindingsofcerebralmalaria.a)Petechialhemorrhagesarefrequently
foundinthewhitematter(arrow)(H&EstainX100).b)Parasitizedredblood
cellsseenwithinthevascularlumenmostlycytoadheretoendothelialcellslining
thevascularwall(arrow)(H&EstainX400)(Courtesy,DepartmentofTropical
Pathology,FacultyofTropicalMedicine,MahidolUniversity,Thailand).
Pocket Guidelines for the Care of Malaria Patients 13

Fig. 4 Liverof severemalaria case. a)Liver is grossly enlargedandappears asdeep
browntored.Capsularhemorrhagesareseen.b)Microscopicfindingofliver
showingparasitizedredbloodcellsandhemosiderinpigmentspackedwithin
the sinusoids (arrow) (H&E stain X400) (Courtesy, Department of Tropical
Pathology,FacultyofTropicalMedicine,MahidolUniversity,Thailand).
1� Pocket Guidelines for the Care of Malaria Patients

Fig. 5 Kidneyofseveremalariacase.a)Cutsurfacesshowhemorrhagicappearance.
Petechialhemorrhagesarefrequentlyfound.b)Microscopicfindingofkidney
showingcongestedglomeruliandpresenceofpackedparasitizedredbloodcells
(arrow)(H&EstainX400)(Courtesy,DepartmentofTropicalPathology,Faculty
ofTropicalMedicine,MahidolUniversity,Thailand).
Pocket Guidelines for the Care of Malaria Patients 1�

Pathogenesis
Feverinmalariaresultsfromthereleaseoftumornecrosisfactor(TNF) and other endogenous cytokines in response to parasiteantigens. Signs and symptoms of malaria are associated with theruptureofparasitizederythrocytes.Inseveremalaria,tissuehypoxiais believed toplay an important role leading toorgandysfunction.However, the pathophysiological mechanisms are still not clearlyunderstood,especiallyincerebralmalaria.Duringthepast30years,manyhypotheseshavebeenput forward toexplain this condition.It is thought that sequestration of parasitized erythrocytes, thephenomenon of cytoadherence, rosette formation, and reducederythrocyte deformability, lead to microvascular obstruction, andalongwith the effectof cytokines contribute to tissuehypoxia andorgandysfunction(Looareesuwanet al.,1997).
1� Pocket Guidelines for the Care of Malaria Patients

Part 2: Nursing Care of Malaria Patients
A. Early detection Earlydetectionandcorrecttreatmentandnursingcareofmalariapatientswillresultinlowermortalityandmorbidityrates.Themortalityrateforcerebralmalariavariesfrom5-20%dependingonconcomitantmajororgancomplications.Earlydetectionshouldbeaccomplishedby careful evaluationof thehistory and correct examinationof thepatient. Thick and thin blood films should be examined. Antigendetection/striptests[bloodforP. falciparumHistidine-RichProtein-2 (Pf HRP2) or P. falciparum Lactate Dehydrogenase (Pf LDH)] arevaluablefortherapiddiagnosisoffalciparummalaria(WHO,2006).
1. History Asktherelativesorresponsiblepersonswhetherthepatienthastraveledtoamalariousarea,hasahistoryofmalariainfection,chronicmalaria, or has taken any anti-malarial drugs prior to admission/consultation.Ifso,checkthebloodfilmmorefrequently(ifthepatienthasrecentlytakenmedication,thebloodfilmmaybefalse-negative).Atleastthreenegativebloodfilmsareneededtoruleoutadiagnosisofmalaria.Askifthepatienthasreceivedabloodtransfusion.Evenifthepatienthasnevertraveledtoamalaria-endemicarea,buthasreceivedabloodtransfusionorhasworkedinalaboratorywithmalariainfectedblood,theyareatrisk.Ithasbeenreportedthatthosewholivenearanairport,eventhoughthereisnomalariaintheircommunity,cangetmalariafrommosquitoescarriedbyairplanes.Thosewhoworkinaninsectiarywithmosquitoesmayalsobeatriskofmalariaifinfectedmosquitoesbitethem.
Pocket Guidelines for the Care of Malaria Patients 1�

2. Physical examination The level of consciousness should be graded using either theModifiedGlasgowComaScaleforadultsorBlantyreComaScaleforchildren.Monitorvitalsignsandurineoutput,andlookforevidenceofshock.Lookforevidenceofanenlargedspleen,whichcouldindicateapreviousmalariainfection.Lookforsignsofanemiaandbleeding,and prepare for blood transfusion, if necessary. Patients who havereceivedquinineorarejaundiced,andwomeninlatepregnancy,areatriskofhypoglycemia.Monitoringbloodglucoseinthesepatientsisessential.Inpatientswhoremainseverelyill,thedoseofquinineshouldbe reducedonday3byone third.Frequently evaluate thenervous system for level of consciousness (hourly) (Training Unit-WHO,1995;HarinasutaandBunnag,1988).
1� Pocket Guidelines for the Care of Malaria Patients

Evaluation of level of consciousness with cerebral malaria based on the Modified Glasgow Coma Scale
(Adaptedfrom:RegionalGuidelinesfortheManagementofSevereFalciparumMalariainSmallHospitals,WHO,NewDelhi,2006)
Modified Glasgow Coma Scale for adults
Eyes open Spontaneously 4 Tospeech 3 Topain 2 Noresponse 1 Best verbal response (Nonintubated) Orientedandtalks 5 Disorientedandtalks 4 Inappropriatewords 3 Incomprehensiblesounds 2 Noresponse 1
(Intubated) Seemsabletotalk 5 Questionableabilitytotalk 3 Generallyunresponsive 1 Best motor response Verbalcommands 6 Localizestopain 5 Withdrawstopain 4 Decorticate 3 Decerebrate 2 None 1 Total score 3–15
Totalscore=eyeopeningscore+verbal(intubatedornonintubated)score+motorscore
Totalscorerangesfrom3to15;unrousablecomareflectedinascoreof<9.
Thisscalecanbeusedrepeatedlytoassessimprovementordeterioration.
Pocket Guidelines for the Care of Malaria Patients 1�

Blantyre Coma Scale for children(“Blantyre Coma Scale”)
Eye movements Directed(e.g.towardsmother’sface) 1 Notdirected 0Verbal response Appropriatecry 2 Inappropriatecryormoan 1 None 0Best motor response Localisestopainfulstimuli 2 Withdrawslimbfrompain 1 Non-specificorabsentresponse 0Total score 0–5
Totalscorecanrangefrom0-5;2orlessindicatesunrousablecoma.Thisscalecanbeusedrepeatedlytoassessimprovementordeterioration.
20 Pocket Guidelines for the Care of Malaria Patients

3. Differential diagnosis Those who have altered consciousness must be evaluated forhypoglycemia,renalfailure,electrolyteimbalance,andpost-ictalstate.Examinethebloodsugar,BUN,creatinine,electrolytes,liverfunctiontestsandurineanalysis.Abloodcultureshouldbetaken.
Those with cerebral malaria will have a reduced level ofconsciousness.Priortoalteredconsciousness,thepatientsmayhavebeenhighfever,bodyaches,headache,nausea,vomitingorabdominalpain. After that, the consciousness level can deteriorate, resultingin confusion, decreased responsiveness, no communication orincontinence.Theremaybegeneralizedorfocalseizures,disconjugategaze or muscle twitches. The clinical signs and symptoms may besimilar toencephalitisormeningitis.A lumbarpunctureshouldbeperformedtodifferentiatebetweencerebralmalariaandothercentralnervoussystem(CNS)diseasesafteranormaleyegroundexamination(Warrell,1997).
�. The diagnosis of malaria Perform thick and thin blood films for malaria. The thick filmismorelikelytodetectasmallernumbersofparasitesthanthethinfilm,becausethethickfilmusesmoreblood.Thethinfilmisusefulindetectingthespeciesofmalaria,%infectedredbloodcells,stageofparasitedevelopment,andpresenceofneutrophilpigment(>5%ofneutrophilscontainingpigmentindicatesapoorprognosis)
Usually, the higher the percentage of infected red blood cells,themoreseriousthecaseis.However,someseverepatientsmaynothavehyperparasitemia, probablydue toperipheral sequestrationofthe parasite in the brain or other vital organs. Ideally, the numberofparasitizedredcellsper1,000RBCs(thinfilm)orthenumberofparasitesper200whitecells(thickfilm)shouldbereported.
Pocket Guidelines for the Care of Malaria Patients 21

Malaria Rapid Diagnostic Test (RDT)
TheRDTisarapidtesttoevaluatethepresenceofmalariaantigensin the blood of a patient suspected of having malaria. Some RDTcheck for P. falciparum only, while others check for other malarias.Thetestmaybeastrip,card,orcassette.Thetestsaresensitiveandas accurate as microscopy. They are good for people who do nothaveamicroscopeavailable,havenoelectricity,orwherenooneistrainedtouseamicroscope.However,theWorldHealthOrganization(WHO,2004)recommendsthatafterstartingtreatment,managementdecisionsshouldnotbebasedontheRDTalone.Aconfirmatorytestshouldbeperformedwithmicroscopy.
B. Early treatment
Thetreatmentofmalariaisseparatedinto2groups:uncomplicatedandcomplicatedmalaria.
1. Uncomplicated malaria. The patient has no signs ofcomplications.Thetreatmentconsistsof: A.Earlyandappropriateantimalarialmedication.Thechoiceofmedicineshouldbebasedonthedrugsensitivitiesofthemalariaparasites in that area. Artemisinin-based combination treatmentsarenowrecommendedasfirst-linetreatmentforfalciparummalariaby theWorldHealthOrganization(2006).Quininecombinedwithdoxycycline,fornon-pregnantadultsandchildren>8yearsold,orclindamycinforpregnantwomenandchildren<8yearsoldgivenfor7daysaresecond-linetreatments.Thefirsttreatmentdoseshouldbeobserved.Ifthedoseisvomitedwithinonehour,itshouldbegivenagain.
22 Pocket Guidelines for the Care of Malaria Patients

B. Symptomatic treatment. Treat symptoms, such asfever,bodyaches,nausea,vomitingorheadaches,withappropriatemedicine.Paracetamol(acetaminophen)(15mg/kg4–6hourly)maybeusedtoreducefever.
C. Nursing care. Give supportive care and symptomatictreatment, such as tepid sponging for fever. Give health educationregardingpersonalprotection,preventionofmalariaandcompliancewithtreatment.Thepatientshouldbetoldtoreturnifthereisfever,especiallyinthe2monthsaftertreatmentorwithP. vivaxorP. ovale infection. The patient should be advised to take the full course ofmedicationtopreventareturnofmalaria.Ifthereisvomitingoftheantimalarialdrug, take an antiemeticmedicine½ to1hourbeforetaking the antimalarial drug. If there is fever, take an antipyretic 1hourbeforetakingtheantimalarialmedicine.Thepatientshouldrestfor1–2hoursaftertakingthemedicine,duetotheriskofdizziness,vomiting,andhypotension.Thepatientshouldbegivenpsychosocialsupportbyencouragingthepatientandgivingcomfort.Allcasesofmalaria shouldbe recordedand reported to the appropriatehealthauthorities to help in the control of malaria. The patient shouldfollowupwiththedoctortoevaluateforcompliance,thetherapeuticresponsetothedrugandtoevaluateforevidenceofdrugresistance.
Pocket Guidelines for the Care of Malaria Patients 23

2. Complicated (severe) malaria: TheWHO(2006)criteriaforseveremalariaareasfollows:
Clinical manifestations: -Prostration -Impairedconsciousness -Respiratorydistress(acidoticbreathing) -Multipleconvulsions -Circulatorycollapse -Pulmonaryedema(radiological) -Abnormalbleeding -Jaundice -Hemoglobinuria
Laboratory tests: -Severeanemia -Hypoglycemia -Acidosis -Renalimpairment -Hyperlactatemia -Hyperparasitemia
Someexpertsdefinethelaboratorytestsasfollows:severeanemiaisaHb<5g/dl,especiallywith>100,000parasites/µl;hypoglycemiaisaserumglucose<2.2mmol/lor<40mg/dl;acidosisisaHCO3< 15 mmol/l; renal impairment is a serum creatinine > 3 mg/dlor250µmol/l;hyperlactatemiaisaserumlactate>5mmol/l;andhyperparasitemiais≥ 5%.
2� Pocket Guidelines for the Care of Malaria Patients

Antimalarial drugs in severe malaria (WHO, 2006)
Antimalarial Dosage and drug administration
Artemisinin derivatives
Artesunate: 2.4 mg/kg body weight (bw)intravenous(IV)orintramuscular(IM)onadmission(time=0), followed by 2.4 mg/kg at 12 and 24hours,followedbyoncedailyfor7days.Oncethepatientcantolerateoraltherapy,treatmentshouldbe switched to a completedosageof artemisinin-based combination therapy (ACT) for 3 days, asrecommendedinthenationaltreatmentguidelinesforuncomplicatedmalaria.Artemether: 3.2 mg/kg bw IM on the first dayfollowedby1.6mg/kgbwdailyfor7days.Oncethepatientcantolerateoraltherapy,treatmentshouldbeswitchedtoacompletedosageofanACT.Arteether: 3.2 mg/kg bw IM on the first day,followed by 1.6 mg/kg bw for the next 4 days.Once thepatientcan tolerateoral therapy, switchtoacompletedosageofanACT.
Quinine Loading dose: Quinine dihydrochloride 20 mgsalt/kgbwdilutedin10ml/kgbwof5%dextroseordextrosesalineadministeredbyIVinfusionovera period of 4 hours. Maintenance dose: Quininedihydrochloride10mgsalt/kgbwdilutedin10ml/kgbwof5%dextroseordextrosesalineadministeredbyIVinfusion.Inadults,themaintenancedoseisinfusedoveraperiodof4hoursandrepeatedevery8hours.Inchildren,itisinfusedoveraperiodof
Pocket Guidelines for the Care of Malaria Patients 2�

2 hours and repeated every 8 hours (calculatedfromthebeginningofthepreviousinfusion)untilthe patient is in a position to swallow. An oralmedicationcanbegivenfollowingthis,tocompletethe 7-day treatment. The amount of fluid forinfusionofquinineshouldbeconsideredkeepingin mind the hydration status of the patient. Forinstance, if the patient has volume overload orpulmonary edema, quinine in 10 ml/kg IV fluidmaybeharmful.Therefore,thecalculationoffluidforquinineinfusionshouldbemadeaccordingly. Forchoiceoforaldrugsforfollow-ontreatment,it is recommended to prescribe a combinationtherapy:3daysofACTaccording to thenationaltreatment guidelines. If ACT is not in use in thecountry, quinine should be administered incombination with tetracycline or doxycycline orclindamycin, to complete the 7-day treatment,except for pregnant women and children <8yearsof age, forwhom tetracycline/doxycycline iscontraindicated.
2� Pocket Guidelines for the Care of Malaria Patients

Refer patient to a hospital with better facilities to care for severe malaria Indicationtoreferseveremalariapatients.Thedecisiontorefera patient with severe malaria is based on the ability of the facilityto give appropriate management for severe malaria. This includesmedications, hemofiltration or hemodialysis, artificial ventilation,multiple transfusions, treating pregnant women, postpartumpatients,multi-organfailure,activebleeding,andcerebralmalarianotrespondingtoappropriatetreatmentwithin48hours.
•Pre-referral. Provide information to the family, guardian andpatient about the diagnosis and treatment plan. Explain that thediseasecanbelethalifnottreatedearlyandproperlyinthehospital.Knowwheretoreferthepatientandhowtotransferthepatientsafely.Makesurethereferralfacilityhastheabilitytoperformdialysisandhas a ventilator for the management of respiratory failure. Checkbloodglucosebeforetransfer. When referring to another hospital, if possible, communicatedirectly with the hospital personnel about the patient’s diagnosisand condition. Send all information, laboratory results, malariasmearslidesandotherstudiesofthepatientwiththemtothereferralhospital. If possible, send the patient by ambulance with oxygen,medicinetocontrolbloodpressure,convulsions,andhypoglycemia.Adoctorornurseshouldaccompanythepatienttomanageproblemsduringtransport. Giveantimalarialdrugsbeforetransport.TheyshouldbegivenbyIV injection (artesunate), or rectal artesunate if possible. If quinineisgiven,itmustbegivenbyrate-controlledinfusionorIMinjection,since gastrointestinal absorption in severe malaria is poor and thepatientmayaspirate(Winstanley,2001).If thepatienthasreducedconsciousnessor respiratoryproblems, intubatebefore transport. Ifthepatienthasanuricrenalfailure,thenhemofiltrationordialysismayberequired.
Pocket Guidelines for the Care of Malaria Patients 2�

•During transfer.Maintaincontinuouscloseobservation.Givelifesupportbasedontheconditionofthepatient.Forexample,iftheoxygenlevelisloworthereisdyspnea,giveoxygen.Monitorintakeandoutputpreciselyinmillilitersperhour,byplacingaFoleycathetertomonitorurineoutput.Providepsychosocialsupportforthefamilyandpatientbyexplainingwhatishappeningandthatifthepatientreceivescorrectandearlytreatmenttheywillrecover. Makesuretheairwayissecure.Ifnoventilatorisavailable,giveoxygenbymask.Positionthepatientsotheairwayisclear.Suctionto clear the airway, as necessary. Use an oral airway as necessary,especiallywithbagandmask. Monitorthebloodpressure,pulse,intakeandoutputfrequently.IftoomuchIVfluidisgiven,fluidoverload(positivefluidbalance),and eventually pulmonary edema, may result. If too little IV fluidis given (negative fluid balance), renal insufficiency or failure (pre-renalazotemia)mayoccur.MaintainaFoleycathetertomonitorurineoutput. Monitorforhypoglycemia,particularlyinseveremalariapatients,whenusingquinineorintreatingpregnantwomenandchildrenbyfollowingbloodsugarlevelsregularly.Insertanasogastrictube(NG)andgiveglucoseviaNG tube.Stopping IVdextrose suddenlymayresult inhypoglycemia, especially inmalnourishedpatients.GivingglucosebymouthorbyNG tube is less likely to result in suddenhypoglycemia. If referral isnotpossible,maintain theaboveadvice.Treatmentwithearlyandcorrectantimalarialdrugsisthemostimportantfactortoimprovesurvival. Treatfeverwithtepidspongingandantipyreticdrugs.Inchildren<5yearsold, thismayprevent febrileseizures.Prevent falls from,andinjuriesin,bed. Thehematocritlevelshouldbefollowed.Thereisariskofsevereanemia with complicated malaria and hyperparasitemia. When
2� Pocket Guidelines for the Care of Malaria Patients

hyperparasitemia and a low hematocrit are present, if possible,crossmatchandprepareforabloodtransfusion.Bloodisusuallygivenifhematocrit<20%.If there isaconcomitant lowserumalbuminlevel,givepackedredcellswithserumalbuminorwholeblood. If there is severeanemiaand thepatient is volumeoverloaded,givepackedredcellsandadiuretic. Givedextrose10%byIVifbloodsugarislow. If there are seizures, givediazepamasneeded tocontrol them.Considerphenobarbitalorphenytoinonlyif facilitiesforventilationare available. Hypoglycemia can cause seizures. Check the glucoselevel to rule this out if there are seizures, and if present, treat asmentionedabove. If the patient is short of breath, look for other evidence ofpulmonaryedema,suchascrackles in the lungs.Check the intakeandoutputrecordforapositivefluidbalance.Ifpulmonaryedemaispresent,giveadiureticandconsiderusingacolloid,especiallyforthosewithlowserumalbumin.
• Post-referral care. After the patient returns from treatment,theyneedtofollowupforperiodicbloodmalariachecks.Iftheyhavefeverafterleavinghospital,checkandevaluateabloodfilmformalariaforrelapseorrecrudescence.Encouragethepatienttocompletethecourseofdrugs.
•Prevention.Educate thepatientand familyaboutpreventivemeasures.Use amosquitonet, repellent,mosquito coil, orfire, todecrease bites. Stay indoors at night during the malaria season. Ifgoingout,coverthearmsandlegs.Residualmosquitosprayingtheinsidewallsofthehousecanhelptoreducebites.
• Advice for travelers. Besides the prevention advice alreadymentioned, travelersmaychoose tousemalaria-chemoprophylactic
Pocket Guidelines for the Care of Malaria Patients 2�

drugs. Commonly used drugs for prophylaxis include: mefloquine(Lariam®),doxycycline,atovaquone-proquanil(Malarone®).Chloroquine,inmostpartsoftheworld,doesnotprotectagainstfalciparummalaria.PrimaquineisusedafteraninfectionwithP. vivaxorP. ovale,topreventrelapse(Wilairatanaet al.,1997). Malarial chemoprophylactic drugs are not 100% effective, andtheymayalter thehistoryandmasksymptomsofmalariapatients.Incubation periods may be prolonged and the drugs may induceresistance (Wilairatana et al., 2002). They may also cause a falsenegativebloodsmearformalaria. If there is ahistory of travel to amalaria-endemic area, even ifmalariachemoprophylaxiswastaken,thereshouldbeahighindexofsuspicionformalaria,evenwithanegativebloodfilm.
• No malaria. If no malaria is found, other causes of illnessshouldbeinvestigatedandtreatedaccordingtotheetiology.Ifthereisnoclinicalconfirmationofanotherdiseaseandthereisahighriskofmalaria,thepatientmaybetreatedashavingmalaria.Iftheystillhavefever andhavebeen suspectedofmalaria, a bloodfilm formalariashouldberepeatedfrequently.
30 Pocket Guidelines for the Care of Malaria Patients

Part 3: Algorithms
Fever with negative blood film
Fever
Peripheralbloodsmear
Negative
Lookforother causesoffever
Noothercausefound Othercauses
Ifriskofmalaria Givespecific repeatbloodfilms6-hourly treatment
Health education Refer to Table 2
Algorithm 1 Sequential guideline for patients suspected of havingmalaria,presentingwithfeverandnegativebloodfilm.
Pocket Guidelines for the Care of Malaria Patients 31

Fever with positive blood film
Fever
Bloodfilm
Positive Positive Positive Positive Positive P. falciparum P. vivax P. malariae P. ovale P. knowlesi
Uncomplicated
Ifthepatientcantakeoraldrug Ifthepatientcannottakeoraldrug
Giveantimalarial Admit drugorally Giveantiemeticand Advisetotakeall antipyreticIM/IV themedicineand followupin2days Giveantimalarial Giveantimalarialdrug orearlierifthe drugorally parenterallyifunable patientdeteriorates totakeorally Checkbloodfilm Repeatbloodfilm dailyuntilnegative Recordintakeand formalariauntil outputtoprevent negativebloodfilm fluidimbalance thenfollowup Takecomplete bloodfilmondays antimalarialdrugand 7,14,21,and28 followupbloodfilm ondays7,14,21 and28
Health education Refer to Table 2
Algorithm 2 Sequential guideline formalariapatientpresentingwithfeverandpositivebloodfilm.
32 Pocket Guidelines for the Care of Malaria Patients

Severe malaria (WHO criteria)Severemalaria
Ifunabletomanagecomplicationsofseveremalaria,e.g.respiratoryandrenalfailure,thenrefertohigherfacilityhospital
Beforereferral
GiveantimalarialdrugIV/IMorsuppository,giveantipyreticandantiemetic,asneeded
Ifreducedconsciousness,intubatebeforetransfer
Duringtransfer: •Giveoxygen •Maintainairway •Havesuctionavailable •Havedextroseavailableforhypoglycemia •Haveanticonvulsantmedicineavailableforseizures •HaveIVlineinplace •HavereplacementIVcatheteravailable •PlaceFoleycatheterbeforetransport
Athospital
Admitdirectlyintensivecareunit(ICU)withoutdelay
Placeonrespirator •Repeatbloodfilm •Doarterialbloodgas •Dolabs* •Monitorvitalsigns,neurologicalsignsandfluid intakeandoutput •Continueantimalarialdrugs
Cerebralmalaria Acuterenalfailure DIC** Hypoglycemia Severeanemia
Respiratoryfailure Jaundice Fever Preventsecondary Hemoglobinuria bacterialinfection
**DIC=Disseminatedintravascularcoagulation Algorithm 3 Sequentialguidelineformanagementofseveremalaria.
Labs* - Electrolytes,including Plasmabicarbonate - Completebloodcount(CBC) - Serumbloodsugar - Liverfunctiontest - Bloodureanitrogen(BUN), creatinine - CXR(chestx-ray) - U/A(urineexam) - HIVtestforacute renalfailurepatients
Pocket Guidelines for the Care of Malaria Patients 33

Cerebral malaria
Cerebralmalaria
Ruleoutothercausesofaltered consciousness 1. Hypoglycemia:checkbloodsugar 2. Meningitis/encephalitis:dolumbar punctureifnocontraindication forlumbarpuncture. 3. Post-ictalstate 4. Metabolicacidosis
Intubate
•Followbloodsugar •Keepairwayclear •Monitorvitalsignsfrequently •Monitorneurologicalsigns •Treatconvulsions •InsertNGtubeforfeeds •InsertFoleycatheter •Monitorintake/output •Preventaccidents–siderails •Changepositionofpatientevery2hours
Health education Refer to Table 2
Algorithm 4 Sequentialguidelineformanagementofcerebralmalaria.
3� Pocket Guidelines for the Care of Malaria Patients

Respiratory failure
Respiratoryfailure
ARDS* Pulmonaryedema
- Arterialbloodgas - Recordintake/output - CXR - Diuretic - UsePEEPventilator - Arterialbloodgases - Propuptheheadofthe - Ifgivingblood, patient45o givediuretic - Followintakeand - Keepheadofbedup output - Balancefluids - Ifbloodtransfusionneeded totreatanemia,use packedredcells(PRC) insteadofwholeblood
Health educationRefer to Table 2
*ARDS=AdultrespiratorydistresssyndromeAlgorithm 5 Sequentialguidelineformanagementofrespiratoryfailure
inseveremalaria.
Pocket Guidelines for the Care of Malaria Patients 3�

Acute renal failure
Acuterenalfailure
Excludedehydrationstatusandrehydratethepatient
Recordintake/outputCheckbloodforBUN/creatinine
Renalfailureconfirmed
Dialysisindications?
Yes No
Hemofiltration/ Conservativetreatment dialysis ofrenalfailure
HealtheducationRefertoTable2
Algorithm 6 Sequentialguidelineformanagementofacuterenalfailureinseveremalaria.
3� Pocket Guidelines for the Care of Malaria Patients

Jaundice
Jaundice
CheckliverfunctiontestLookforassociatedviralhepatitisinfections
Lookforothercomplicationsofseveremalaria,suchashypoglycemia,hemolysisandrapidfallofhemoglobinneededforbloodtransfusion.
HealtheducationRefertoTable2
Algorithm 7 Sequentialguidelineformanagementofjaundiceinseveremalaria.
Pocket Guidelines for the Care of Malaria Patients 3�

Disseminated intravascular coagulation (DIC )
DIC
CheckforRBCmorphology,hematocrit, hemoglobinuria,etc. Observeforevidenceofabnormalbleeding,e.g. subconjunctivalhemorrhage,epistaxis,bleeding pergums,petechiae,bleedingfrominjectionsites, hematemesisormelena.
Givereplacementtherapywithblood orbloodcomponents,e.g.freshwholeblood, packedredcells,freshfrozenplasmaorplatelet concentrate. Monitorintakeandoutputforrenalfailure.
Health educationRefer to Table 2
Algorithm 8 Sequential guideline for management of disseminatedintravascularcoagulationinseveremalaria.
3� Pocket Guidelines for the Care of Malaria Patients

Fever
Fever
Monitortemperaturefrequently. Monitorforseizures,especiallyinchildren <6yearsold.Giveparacetamol (acetaminophen).Usetepidsponging, coolingblanket.Removeblanketsandsheets. Ifseizures,preventaspirationandinjury byplacingonthesideandgivediazepamor phenobarbital.
Health educationRefer to Table 2
Algorithm 9 Sequential guideline for management of fever in severemalaria.
Pocket Guidelines for the Care of Malaria Patients 3�

Hypoglycemia
HypoglycemiaBloodglucose<40mg%
Lookforconsciousnesslevel
Altered Asymptomatic consciousness hypoglycemia
50%glucose 50ccIVpush
Preventfurtherhypoglycemia byintravenousinfusion of5-10%dextrose
Frequentmonitoring ofbloodglucose
Health educationRefer to Table 2
Algorithm 10 Sequentialguidelineformanagementofhypoglycemiainseveremalaria.
�0 Pocket Guidelines for the Care of Malaria Patients

Prevention of secondary bacterial infection
Preventionofsecondarybacterialinfection
Inseveremalariawithshock orunexplaineddeterioration,takeblood culturesandgiveappropriateantibiotics e.g.third-generationcephalosporin.
Health educationRefer to Table 2
Algorithm 11 Sequentialguidelineforpreventionofsecondarybacterialinfectioninseveremalaria.
Pocket Guidelines for the Care of Malaria Patients �1

Severe anemia
Severeanemia
Typeandcross-matchbloodonadmission. Followhematocritlevel.ReplacewithPRC orwholeblood.Diuretic(furosemide) maybegiventopreventvolumeoverload. Transfusebloodslowlytoavoidvolumeoverload andpulmonaryedema.Balancefluidintake andoutput.
HealtheducationRefertoTable2
Algorithm 12 Sequentialguidelineformanagementofsevereanemiainseveremalaria.
�2 Pocket Guidelines for the Care of Malaria Patients
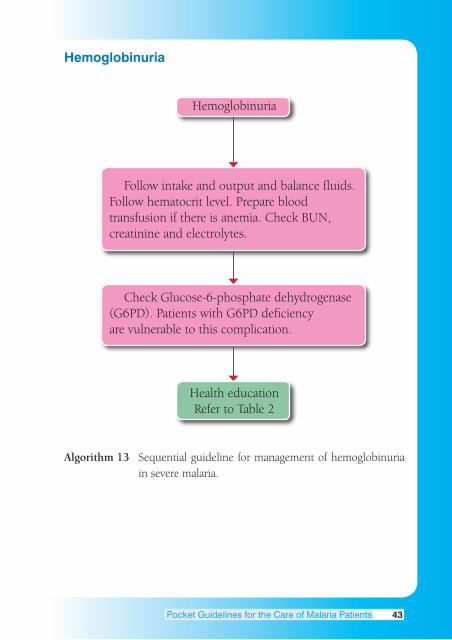
Hemoglobinuria
Hemoglobinuria
Followintakeandoutputandbalancefluids. Followhematocritlevel.Prepareblood transfusionifthereisanemia.CheckBUN, creatinineandelectrolytes.
CheckGlucose-6-phosphatedehydrogenase (G6PD).PatientswithG6PDdeficiency arevulnerabletothiscomplication.
HealtheducationRefertoTable2
Algorithm 13 Sequentialguidelineformanagementofhemoglobinuriainseveremalaria.
Pocket Guidelines for the Care of Malaria Patients �3

Health education
Table 2 Healtheducationfortreatedmalariapatients.
Health education ❐Takemedicineuntilcompleted. ❐ Iffeveroccurswithin2monthsaftertreatment, followuprightawaytoruleoutmixedinfection, resistanceorrecrudescence. ❐ Ifthepatienttraveledtoamalariaendemicarea andhasafeverwithin2weeksto2months aftertravel,beawareofriskofmalaria. ❐ IfthepatienthasG6PD,educatepatienttoinform thedoctorbeforetakinganymedicine. ❐ Preventionofmalaria. •Useinsecticide-treatedbednets. •Useresidualinsecticide. •Avoidgoingoutatnight;uselongsleeves andlongpants. •Userepellenttopreventmosquitobites.
�� Pocket Guidelines for the Care of Malaria Patients

Algorithm Index
Feverp.31
Postivep.32 Bloodfilmformlaria Negativep.31
WHOcriteria Lookforother Forseveremalariap.33 causesp.31
No Yes
Cantakeoraldrugs Refertohospitaliffacilities areinadequatep.33 Yesp.32 Nop.32 InICU,p.33
Giveantimalarial Giveantimalarial Stillunableto orally parenterally takedrugorally
Followupand Giveantimalarial Giveantimalarial repeatbloodfilm antimalarial antimalarial untilitisnegative, drugorally drugparenterally ifpossible
Healtheducationp.44
Cerebral Respiratory Acuterenal Jaundice DIC Malariap.34 Failurep.35 failurep.36 p.37 p.38
Fever Hypoglycemia Preventionof Severe Hemo- p.39 p.40 secondarybacteria anemia globinuria infectionp.41 p.42 p.43
Health education p.44
Algorithm 14 Summaryofsequentialguidelinesinthemanagementofseveremalaria.
Pocket Guidelines for the Care of Malaria Patients ��

Bibliography
HarinasutaT,BunnagD.Theclinicalfeaturesofmalaria.In:WernsdorferWH,McGregorI,eds.
Malaria: Principle and practice of malariology. Vol 1. Great Britain: Churchill Livingstone,
1988:709-32.
LooareesuwanS,WilairatanaP.Malaria.In: RakelRE,eds.Conn’sCurrentTherapy.Philadelphia:
WBSaunders,1997:104-15.
LooareesuwanS.Malaria. In:LooareesuwanS,BunnagD,HarinasutaT,eds.TheTextbookof
TropicalMedicine.Bangkok:RuamthasaPublishers,1990:39-44.
PongponratnE,RigantiM,PunpoowongB,AikawaM.Microvascularsequestrationofparasitized
erythrocytes inhuman falciparummalaria: apathological study.Am J Trop Med Hyg 1991;
44(2):168-75.
SnowRW,GuerraCA,NoorAM,MyintHY,HayS,I.Theglobaldistributionofclinicalepisodes
ofPlasmodium falciparum malaria. Nature2005;434:214-217.
TrainingUnit,DivisionofControlofTropicalDiseases.Thediagnosisandmanagementofsevere
andcomplicatedfalciparummalaria,part1:Learner’sguide.Geneva:WHO,1995:1-93.
WarrellDA.Cerebralmalaria: clinical features,pathophysiology and treatment.Ann Trop Med
Parasitol 1997;91:875-84.
WhiteNJ.Malaria. In:CookGC,ZumlaAI,eds.Manson’sTropicalDiseases.21sted.Geneva;
WHO,2000;1-69.
Wilairatana P, Looareesuwan S, Walsh DS. Chemotherapy of cerebral malaria: current
recommendationsfortreatmentandprophylaxis.CNS Drugs1997;7:366-80.
WilairatanaP,KrudsoodS,TreeprasertsukS,ChalermrutK,LooareesuwanS.Thefutureoutlook
ofantimalarialdrugsandrecentworkonthetreatmentofmalaria.Arch Med Res2002;33:
416-21.
WinstanleyP.Chemotherapeuticoptionsformalaria.Lancet Infect Dis2001;1:242-50.
WHO.GuidelinesfortheTreatmentofMalaria.Geneva:WHO,2006.
WHO.Managementofsevereandcomplicatedmalaria:apracticalhandbook(2nded.).London:
WBSaunders,2003:1-69.
WHO.Theuseofantimalarialdrugs.Geneva;WHO2000:5-141.
WHO.TheUseofMalariaRapidDiagnostictests.2004,(Cited2008Jan31).Availablefrom:
URL:http://www.searo.who.int/LinkFliles/Malaria_in_the_SEAR_RDTGuidelines_final1.pdf
WHO,TheWorldMapofMalariaandDrugResistance.2006,(Cited2008Feb25).Available
from:URL:http://www.who.int/malariaendemiccountries.html
�� Pocket Guidelines for the Care of Malaria Patients

Index
Acidosis24
Antimalarial22,25,27,28,32,33,45
Antipyretic23,28,32,33
Anemia18,24,28,35,42,43,45
Anticonvulsant33
Antiemetic32,33
Artemisinin22,25
Artesunate22,25,27
Artemether25
Arteether25
Arterialbloodgas33,35
Asexual9
Bednets44
Brainedema12
Cerebralmalaria12,17,21,33,34,45
Chloroquine29
Colloid29
Convulsion27,34
Coma 18,19,20
Cytokines16
Dialysis27,36
Diazepam29,39
Diuretic 29,35,42
Dizziness23
Drugresistance23
Disseminatedintravascularcoagulation
(DIC)33,38,45
Epistaxis38
Erythrocytes9,10,11,16
Encephalitis21,34
Electrolytes21,43
Fever 16,21,23,28,32,33,39,45
Gametocytes9
Hypnozoites 9,10
Hypoxia16
Hypoglycemia18,21,24,27,28,33,37,40,45
Hypotension23
Hyperparasitemia21,24,28,29
Hyperlactatemia24
Headache21,23
Hemodialysis 27
Hemofiltration 27,36
Hematocrit28,29,42,43
Hemoglobinuria24,33,38,43,45
Intubate27,33,34
Jaundice 24,33,37,45
Kidney11,15
Larium®29
Lumbarpuncture21,34
Merozoites9
Meningitis21,34
Melena38
Malarone®29
Mosquitocoils29
NGtube=nasogastrictube28,34
Nausea21,23
P. falciparum 9,10,11,22
P. knowlesi 9
P. malariae 9,10,32
P. ovale 9,10,29,32
P. vivax 9,10,23,29,32
Prophylaxis29
Parasites9,21
Paracetamol23,39
Pocket Guidelines for the Care of Malaria Patients ��

Phenobarbital29,39
Pregnancy18
Petechial11,12,13
Quinine18,22,25,27,28
Relapse30
Renalfailure21,27,33,36,38,45
Referral27,33
Respiratoryfailure27,33,45
Resistance23,30,44
Recrudescence29,44
Sporozoites 9
Schizont9
Sequestration11,21
Seizures21,29,33
Shock41
Trophozoites9
Treatment22,23,25,28,44
Unrousable19,20
Vomiting21,22
Volumeoverload29,42
Ventilator27
Zygote9
Index
�� Pocket Guidelines for the Care of Malaria Patients





























