Embed Size (px)
Citation preview

continued on page 2
Healthy Schools Partnership RDCoach A Closer Look . . . . . . . . . . 3
May 2009 Board Certifications 3
Chair’s Corner . . . . . . . . . . . . . . . . .4
Webinar Review . . . . . . . . . . . . . . 4
Member Spotlight . . . . . . . . . . . . 5
Calorically Dense Infant
Formulas Using Household
Measurements . . . . . . . . . . . . . . . 6
Volume 20, Number 3 SPRING 2010
PNPG POSTA publication of the Pediatric Nutrition Practice Group
Next Submission Deadline
Summer 2010 .................. April 16, 2010
Editorial Staff
EditorMonica Nagle, RD, CNSD, LDN
Co-EditorHolly Van Poots, RD, CSP, LDN
Communications ChairCarolyn Silzle, MS, MBA, RD, LD
Communications Co-ChairLiesje Nieman, RD, CNSD, LDN
Inside...
Featured StoryRD Coaching:
Making Big Strides with Small StepsBy Katie Brown, EdD, RD, LD
National Nutrition Education DirectorRD Coach Project
American Dietitic Association Foundation
“I only eat half the bag of chips now, and save the rest for later” is just one of manysmall steps Kansas City, Missouri, “tweens” are taking thanks to RD Coaching. You willnot find a definition of RD Coaching in Wikipedia, but it could be described as being amini-counseling session with individuals or small groups of students that is fun, interac-tive, and performed during physical education (PE) class, while the students are beingphysically active!
In 2007 the American Dietetic Association Foundation and a group of professionalsready to think “outside the box” formed a coalition to design the blueprint for RDNutrition Coaches in schools. When they partnered with the American Council forFitness and Nutrition Foundation (ACFN) and PE4Life, the Healthy SchoolsPartnership (HSP) was born. The HSP program is funded through a grant by ACFN aspart of the Healthy Weight Commitment Foundation (HWCF). Katie Brown, EdD, RD, LD,became the first Head RD Nutrition Coach and formed a team of six RD Coaches inter-ested in helping with this innovative project. This small RD Coach team developed acomprehensive curriculum with over 70 lessons focusing on energy balance that spansseven grade levels. The lessons include RD Coaching during PE class while kids arebeing active, classroom presentations, PE games, cafeteria promotions, posters, morn-ing announcements, school newsletter articles, and family fun nights.
The Healthy Schools Partnership piloted its first project with over 800 students in theFall semester of 2007 in Kansas City schools, including two elementary schools, onemiddle school, and one high school. In just the first two years, over 2,000 students werereached.
Within the first week of the original interventions students were forming bonds withthe RD Coaches, starting to ask questions, and reporting impressive behavior changes.
One student said she ate pizza every day for lunch; after comparing her diet to theUSDA’s MyPyramid, she said she needed to eat more fruits and vegetables. She thenplanned to stop by the salad bar after getting her pizza to add baby carrots and fruit tocomplete her meal. Although she didn’t say she wanted to stop eating pizza every day,this small step of adding more fruits and vegetables to her diet was encouraging afterjust one week of interventions. By week five students were reporting significant behav-ior changes and attitudes towards healthy eating. A seventh grader told her RD Coachthat she was having her mom buy more fruits and vegetables to make sure she hashealthy snacks available when she gets home from school.
EvaluationTo evaluate the project’s effectiveness at achieving behavior change in fourth- to
sixth-grade students through the Healthy Schools Partnership, ADAF consulted theUniversity of California, Berkeley premier team of researchers (Pat Crawford, PhD, RD,and Dana Gerstein, MS, RD). For the 2008-2009 school year, four new elementaryschools and two control schools were selected. Students completed surveys prior tobeginning the intervention and again at the end of the 14-week intervention whichasked questions regarding nutrition, knowledge of energy balance, and behavior.
PNPG POSTPage 2 SPRING 2010
continued from page 1Photos were taken of student’s lunch traysboth before and after meal consumption atpretest and post-test.
Did the RD Coach make a difference inwhat children know, believe, and doregarding energy intake?
Yes, students’ nutrition knowledgeincreased significantly compared to the con-trol group. The most promising finding wasthat students participating in HSP significant-ly increased their consumption of vegetablesto a level nearly twice as much as the controlgroup (30% intervention group, 17% controlgroup). Students reported eating more veg-etables, which was impressive, but they actu-ally did eat more vegetables at lunch, as pho-tos of their lunch trays were examined andproved consistent with students’ reportedbehavior.
Showing behavior change is a challengewith nutrition education programs and theADAF was extremely pleased to unveil thatthe intervention by the RD Nutrition Coachesin the HSP program led to increased nutritionknowledge and attitudes which resulted inparticipants eating more fruits and vegeta-bles. The HSP program is now entering a twoand a half year study to follow fourth- tosixth-grade students to evaluate long-termeffects the program has on their knowledge,beliefs, energy intake and energy output.
RD CoachingThe RD Nutrition Coaching in the HSP pro-
gram is provided in a variety of settings.Sometimes an RD Coach will talk with a fewstudents at a time while they are exercisingon weight machines, running on treadmills,or moving through a lesson-specific activity.RD Coaching consists of short activities andconversations that reinforce the theme of theweek, usually accompanied with some per-sonal goal-setting. For example, during“Snacks & Beverages” week in the springsemester, students measure out sugar cubesthat represent the amount of sugar in bever-ages and then discuss what changes theywant to work on in this area.
Classroom PresentationsShort ten-minute presentations were cre-
ated to teach the overall concepts of theweek. There are in-class activities that rein-force the nutrition messages, handouts totake home to share with families, a corre-sponding homework assignment, or a con-test such as a “Breakfast Poster Contest.” Each
grade level of the classroom presentationshas its own set of objectives, presentation,and coaching outlines, and each year pro-gresses and builds on the previous one sothat the program stays fresh for the students.
Nutrition GamesGames are a good way to reinforce the
HSP key messages. Students have to thinkfast and work as a team all while they are par-ticipating in physical activity. Each semesterthe RD Coaches are adapting or developingnew games. Often this occurs in collaborationwith the PE teachers.
Cafeteria PromotionsAs the Healthy Schools Partnership, leav-
ing out the education opportunities thatabound in the schools’ cafeterias would havebeen a mistake. “Power Pick” (i.e. nutrientdense) choices are highlighted using anexclusive logo created to symbolize theHealthy Schools Partnership focus on PowerFoods. RD Coaches help reinforce “PowerPick” choices, acknowledging students whohave a “Power Pick” lunch tray by taking his orher picture to place on the “I Power PickedMy Plate” banner displayed prominently inthe school’s cafeteria.
Nutrition PostersEach week several nutrition posters that
relate to the week’s theme are hung through-out the school in hallways, cafeterias, andlocker rooms. This nutrition information seep-ing into the school environment begins toaffect the school staff positively as well.Several of the school staff ask for RDCoaching programming for the adults.
Morning AnnouncementsEvery day a Healthy Schools Partnership
announcement is read over the intercom,once again to help reinforce the weekly mes-sage. “Be a Power Pick Champion every day.Brighten up your lunch tray with fruits andvegetables. Swap those fries or chips for asalad and a piece of fresh fruit” is one exam-ple of announcements students hear.
School Newsletter ArticlesTo help take the message home to par-
ents, short nutrition articles are provided tothe schools to be incorporated into parentnewsletters, giving tips such as choosinghealthier foods when dining out or selectingbetter beverage choices for kids, which are
common concerns that many parents have.
Family Fun NightsFamily Fun Nights are an important way to
teach the whole family about nutrition. Witha “Walk Through the Pyramid” activity, par-ents and their children participate in activitiesin each of the five food groups and collectitems to make a trail mix to take home.
Where to Next?The Healthy Schools Partnership is taking
big steps in the spring semester of 2010 byexpanding to 11 schools in Kansas City andinto four schools in Des Moines, Iowa, closelyfollowed by Washington, D.C., and Chicago,Illinois. Keep an eye out for more news aboutthe effective ways that RD Coaches in PE classhelp to change children’s eating behaviors.
For more information about the HealthySchools Partnership project, contact ADAF’sNational Nutrition Education Director KatieBrown, Ed.D, RD, LD, at [email protected]
19th National Conferenceon Advances in Perinatal
& Pediatric Nutrition Stanford University, Stanford
California The conference will tackle some of the
most interesting topics and provocative issues that concern
nutrition practitioners today. Topicsinclude:
What are the roles of feedings, humanmilk, and lactoferrin in the prevention of
NEC?
Who needs vitamin D, and how much?
What are important updates on the useof human milk for the ELBW infant?
What nutritional intricacies must be considered when treating food refusal or
selectivity in children with autism?
July 19-21, 2010http://nutritionconference.stanford.edu

PNPG POSTSPRING 2010 Page 3
Congratulations to the November 2009 Board Certified Specialists in Pediatric NutritionArkansas
Christy BanksMegan GreenRenita Snow
ArizonaLisa Kandell KotlerHeather Ottenbacher
CaliforniaErin FeldmanJennifer JordanEmily LaRoseJennifer MurrayKimberly Olson
ColoradoJacqueline Keller
ConnecticutEileen Tichy
FloridaLaura HearePamela LegoskiSonia Motolongo
GeorgiaJennifer DavisAruna NavatheAlyssa Withee
IdahoJoanna BorkLinda Diamond
IndianaMary EngellandJean Wyss
KentuckyAmy Sapsford
MarylandAngela EshlemanCheryl IssaAmy Toscano
MichiganCatherine Larrman
New JerseyMichele Colin
New MexicoSusan JonesAna Llinas
New YorkNancy Garrison
North Carolina Arlecia PhillipsSharon Wallace
OhioKatherine Dart
OklahomaLaura Cooper
OregonLori BrizeeJulie Stahl
PennsylvaniaLiesje CarneyElizabeth PaulAncy Thomas
South DakotaMelissa Kruce
TennesseeKimberly Ann BaxterKristy Gibbons
TexasDiane AndersonKimberly BilgerRachel DavisCynthia FloydKatherine GreenAmy KapichElisabeth LeeJill RockwellBrittany Szarek
UtahEllen LechtenbergCatherine McDonald
VirginiaAshleigh Sellman
West VirginiaAmy Spadafora
WisconsinJessica Balliet
Healthy SchoolsPartnership and RD
Coaching: A Closer LookBy Stephanie Howard, MPH, RD, LD
The RD Coaches working with the HealthySchools Partnership (HSP) will tell you thattheir job is multi-faceted, high-paced, ever-changing, and most importantly, rewarding.Many registered dietitians (RD) considerthemselves “coaches” to their clients andpatients, and in the Healthy SchoolsPartnership, weekly individual coaching ses-sions are a cornerstone to the program.These one-on-one interactions allow RDs toaddress individual barriers to change foreach student and to praise even the smallestimprovements. Positive encouragement fromthe RD Coach when the students choose the“Power Pick” foods offered in the cafeteriaalso provides a unique opportunity forcoaching in the school setting.
“What I like the most about my RDCoaching job is the fact that we meet thekids where they are, and we can tailor nutri-tion messages to their level of knowledgeand readiness,” says Tammi Linnebur ,MS, RD,LD, a second-year RD Coach. She enjoys mak-ing that personal connection with the kidsand having the ability to “build up their con-fidence and help them feel good about eventhe smallest change they make in eating andactivity behaviors.” Even better, she says, isthe ripple effect that she has seen when onechild takes home an energy balance messagethat results in positive lifestyle changes forthe entire family.
Kuda Chimanya, MPH, MS, RD, LD, one ofthe original RD Coaches, says, “Being an RDCoach is a great opportunity to touch thelives of students, in a fun and interactive way,that empowers them to make small stepstowards overall health and wellness. I lovebeing an RD Coach because each week, I amable to coach the students and see themprogress in their nutrition behaviors as wellas develop friendships where they begin tolook at me as their personal nutrition expert.”Not only do the Kansas City RD Coaches“meet kids where they are” figuratively speak-ing, they literally bring a rare health careexpertise to many schools and neighbor-hoods with lower socioeconomic status.
Many of the students and school staffmembers have never had the opportunity tovisit with a registered dietitian prior to theirinvolvement with the HSP program. With thisconnection to neighborhoods plagued byhealth disparities, the Kansas City RD
Coaches are motivated by the knowledgethat their investment today will lead to bigreturns in the future, thereby reducing theprevalence of obesity and its co-morbidities.In fact, the program received a “PromisingPractice Award” this year from the AmericanDiabetes Association for its strong focus onserving low-income and minority popula-tions. Chimanya believes this is an importantaspect of the program and stated, “We aremaking a difference by changing the lives ofkids who have lower access to healthcare andaddressing obesity to prevent its co-morbidi-ties over a lifetime.”
For Linnebur, another favorite aspect ofher job is witnessing a student having an“aha” moment during a one-on-one weeklyRD Coaching session. A recent example ofone such moment happened during an RDCoaching session with a fourth-grade studentafter Thanksgiving break. This wise fourthgrader shared that cherry pie was beingoffered for dessert, and she remembered thatit was a “noodle-arm” food (a lower-powerfood) not a “strong-arm” food (power food),so she chose to have a smaller piece of pieand made sure she went outside to play laterin the day. The student hadn’t rememberedthe terms “power” food or “low-power” food,but she clearly understood the fun illustra-tion used by the RD Coach who demonstrat-ed the strong muscle arm pose or the “noo-dle-arm.” More importantly, the student hadthe ability to apply the energy balance mes-
sage to her own life. Similar success storiesabout behavior change related to energy bal-ance can be found throughout all of the par-ticipating schools. But as any RD Coach willtell you, there is an enormous amount of timeand energy involved in achieving those posi-tive results.
An RD Coach with Healthy SchoolsPartnership wears many hats during thecourse of a day. Coordinating schedules withbusy teachers and coaches, providing class-room sessions, hauling food and all the equip-ment needed for taste-testings, and memoriz-ing the names of all the students is just a start.An RD Coach may begin the day teaching ahands-on cooking class to a group of hungrysecond graders, then run to the gym to lead anutrition game as part of the physical educa-tion class, take “power pick” photos in the cafe-teria, and then provide some one-on-onecoaching sessions. Following that, she mightstop by the principal’s office to provide a pro-gram update to the school leadership teamand contribute information for the schoolnewsletter. Many of the RD Coaches will visit atleast two and sometimes three schools perday to achieve all their weekly goals at eachassigned location.
To accomplish all of those tasks effective-ly, the job requires some special attributesfrom the RD Coaches, including patience,flexibility, passion for educating others aboutthe importance of nutrition and physicalactivity, and most important of all, a “strong
continued on page 5

PNPG POSTPage 4 SPRING 2010
Chair’s CornerJust as you manage
your professional andpersonal lives, PNPGplans for the future aswe work in the pres-ent. We are hard atwork on our manyPNPG activities thisspring and planningthe new PNPG year!
The Program of Work (POW) for thecoming year – June 2010 through May2011 – has been approved by the PNPGExecutive Committee and sent on to ADAfor their approval. The POW, developed byChair-Elect Beverly Henry, PhD, RD andTreasurer Linda Heller, MS, RD, CSP, CLE, isbased on the PNPG Strategic Plan. Thisplan focuses on meeting the needs of thePNPG membership and aligns with theAmerican Dietetic Association StrategicPlan. As you see, PNPG and ADA worktogether to support the professional needsof our members. An exciting addition tothe POW is the return of the PNPGPediatric Nutrition Symposium in spring2011. We also plan an increase in supportfor a number of pediatric nutrition projectsthrough the ADA Foundation. More aboutthese plans in the near future! We will con-tinue to offer our highly valued member
benefits: our publications, the BuildingBlock for Life and the PNPG Post; our rap-idly developing website, www.pnpg.org;our webinars for CEUs; awards and scholar-ships; and so much more!
Working in the present to support ourPNPG members, the following projects arein progress:• An invitation to participate in the PNPG
Member Survey, from our Member Support Committee led by Chair Mimi Kaufman, MPH, RD, LD, will have arrived by eblast notice. We are hoping you have taken this opportunity to express your views on how PNPG leadership can best support your pediatric nutrition professional development and what you truly value in your membership. Member responses will be used on Strategic Plan revision.
• The PNPG Strategic Plan will be revised in a workshop as part of the PNPG Spring Meeting at the end of April. Information gathered from the MemberSurvey will be used to help us shape our strategic direction for the next three years. Your opinions, stated through our survey, make PNPG your dietetic practice group.
• Please “drop in” to the PNPG website,
www.pnpg.org, for up-to-date information on many topics including CEU opportunities and news about pediatric nutrition. Our wonderful Forum remains available to post your pediatric nutrition questions as well as serve as a support for your colleagues by responding to posted Forum questions. Check out information from the many committees in PNPG by visiting our Officer’s Page, when you log in as a member.Many thanks to all of you have taken
the NCP Survey. The information providedto our NCP Ad Hoc Committee, led bySandy Spann, MS, RD, LD, will help thisgroup develop a plan to support our mem-ber needs in this important area of practice.
As always, PNPG is thankful to all of ourdevoted and active volunteers who give oftheir time and talents to make this a greatdietetic practice group! And we thank allof you for your membership in PNPG!
Please contact me [email protected] if you have ques-tions or comments about your PNPG!
Sue Konek, MA, RD, CSP, CNSD, LDNChair – PNPG
On November 10, 2009, PNPG hosted awebinar titled “Balancing the NutritionalNeeds of VLBW Infants with the ProtectiveProperties of Human Milk,” presented by Dr.Paula “Polly” Sisk, PhD, RD, IBCLC. Dr. Sisk hasover 23 years experience as a neonatal dieti-tian and 20 years as a lactation consultant.Paula currently works in the NeonatalIntensive Care Unit (NICU) at Forsyth MedicalCenter in Winston-Salem, North Carolina. Inaddition to clinical work, Paula is a researchinstructor in the Department of Pediatrics atWake Forest University School of Medicine.Her research and publications focus on thenutritional needs of the premature infant,human lactation, and specifically the healthoutcomes of premature infants receivinghuman milk.
Dr. Sisk initially explained the benefits ofhuman milk in the NICU population and thechallenges of using it. She then raised theimportance of communication with mothersof infants in the NICU about the many bene-fits of human milk. This communication mayhelp alleviate the anxiety that new mothersfeel, and less anxiety may contribute toincreased milk supply for the mother. Dr. Siskalso reviewed strategies for using humanmilk in the NICU to ensure nutrient require-ments are provided.
If you missed this wonderful piece of edu-cation in November, don’t worry! You can stillsee the webinar and receive two continuingeducation hours. To view the webinar, go towww.pnpg.org and log in as a member. Thenclick on “My Courses” on the upper left hand
side of the website. From there, scroll downto the bottom of the page and look under“Webinar” for “VLBW Infants and HumanMilk,” Click there to download the handouts,view the webinar, and take the quiz thatmust be passed to receive your continuingeducation credits. Please note that it maytake several minutes for the handouts andthe webinar to load.
PNPG would like to give a special thanksto Medela for sponsoring this webinar.Medela develops innovative and high-quali-ty breastfeeding and phototherapy productsand supports mothers and health care pro-fessionals to successfully provide humanmilk to all newborns for as long as possible.
Webinar Review: “Balancing the Nutritional Needs of VLBW Infantswith the Protective Properties of Human Milk”
By Amy Brandes, RD, LD, CNSD, IBCLCManager of Neonatal Nutrition & Lactation Services
Steton Family of [email protected]

PNPG POSTSPRING 2010 Page 5
muscle arm” attitude. Although the HSP RDCoaches receive financial compensation fortheir hard work, the common motivation isthe personal reward earned every day theystep into a school and give students a betterchance for health and success.
An Interview with First-Year Healthy SchoolsPartnership RD Coach Stephanie Howard, MPH,RD, LD
Interviewer: What is the most rewardingaspect of your RD Coaching position?
Stephanie Howard: To be able to gain thetrust of a student and see that the knowledgeand encouragement I provided led to a posi-tive behavior change that will hopefully belong-lasting. I have always believed that it is somuch easier and more effective to spend timeshaping a young person’s behaviors than totry to change behaviors later in life when thereare already existing health problems.
Interviewer: Why did you want to be a partof the Healthy Schools Partnership?
SH: I worked in school health programsalmost a decade ago, and since then havebeen passionate about the need for usingschools as the stronghold to address thehealth problems plaguing our nation. Afterlearning about the partnership with theADAF, ACFN, and PE4life, the energy balancemessage, and the ability to connect with stu-dents one-on-one in the school setting, Iwanted to be a part of the effort. For years,we have known about the rising number ofchildren who are overweight, and it is excit-ing to be a part of a national effort that is tak-ing action to address it with evidence-basedmethods.
Interviewer: What part of your experiencehas been the most challenging?
SH: Learning how to best connect with themiddle school-age students. They are in sucha flux with their own self-development, andso influenced by their peers and the media, itcan sometimes be challenging to guide themtoward making better nutrition and physicalactivity choices. On the other hand, theyhave more freedom to make their own foodand activity choices than a second- or third-grade student, so when they do make thedecision to move toward a healthier lifestyle,they have a greater ability to sustain it.
Interviewer: Tell me about the most funyou’ve had as an RD Coach.
SH: Last semester we taught a lesson on“power beverages” and part of the seventh-grade coaching sessions included studentsworking in groups to create a skit, song, rap,or public service announcement related to“power picking” their beverages. I had thebest time watching them create fun, educa-
tional messages and performing their cre-ations for their peers. Keeping the lessons funand exciting for the kids is always an impor-tant aspect of our program, but this day wasextra special for the kids.
Interviewer: What sets HSP apart fromother school-based nutrition programs?
SH: We only work in schools that have apre-existing partnership with PE4life, whichmeans the school already understands thebenefit of having health-related initiatives asa part of their curriculum. It also means wehave an existing ally, the PE Coach, in eachschool. We also have the ability to provideone-on-one interactions with the kids whilethey are being physically active, and that is arare component to any school-based healthor nutrition program. Being able to provideincentives that reinforce the messages, foodtastings, and other resources to schools isalso a beneficial aspect of the program.
Interviewer: Why do you think this programhas been so successful?
SH: There are many reasons for the pro-gram’s success: visionary creators, good fund-ing, essential partnerships with other organi-zations fighting childhood obesity, but mostimportant of all is the dedicated team of RDCoaches who started HSP here in Kansas City,Missouri, and continue to build and developthe program. We are fortunate to have adirector who has a doctorate degree in edu-cation, and a high-energy team of RDCoaches from a variety of backgrounds whodevote their talent, energy and passion forthe profession toward the overall success ofthe program. The level of expertise and com-mitment demonstrated by each and everyteam member toward a common goal hasbeen unmatched in my career as a dietitian.
For more information on the HealthySchools Partnership program, please contactAbby Manger at [email protected] also visit the Coach’s Corner blogfound on the ADA website www.eatright.org.First, sign in as a member using your ADAnumber and password, then type in “RDCoach Blog” in the search box in the upperright corner of the webpage. Once on theblog homepage, scroll down until you see abox on the right side of the page that says“RD Coaches Corner”. In that box, click on“Blog Home”, where you can read the latestentries.
Member Spotlight:Sabrina Candelaria
Sabrina Candelaria,MPH, RD was chosenearlier this year to participate in theAmerican DieteticAssociation’s (ADA)new DiversityLeadership program.The primary goal ofthis program is to advance the leadershipskills of underrepresented groups within theAssociation and dietetics profession. Thisnew program is part of the ADA’s StrategicPlan to provide service to a changing demo-graphic group of Registered Dietitians.Sabrina was one of four RDs chosen. She isof Puerto Rican heritage. The other RDs cho-sen were Indian, African American, and male.
Sabrina currently works in a public healthsetting through the University of MiamiMiller School of Medicine as a pediatric clini-cal dietitian. She also is the first registereddietitian from the Miller School to partici-pate in a long-term nutrition “Tele-Medicine”clinic servicing children with special healthcare needs and their families living in rural,medically underserved areas in St. LucieCounty, Florida. Her past experience includespediatric renal transplant, critical care pedi-atrics, maternity, wellness, and sports nutri-tion. She has served as a consultant dietitianfor the University of Miami’s medical schoolwellness center for the past few years. UntilJanuary 2010 she was a nutrition columnistfor two local parenting publications. A life-long learner, Sabrina is now in an executiveMBA program in Health Sector Managementand Policy at the University of Miami. Shehas a BS in nutrition from Cornell Universityand a MPH from New York University.
As a Diversity Leadership participant,Sabrina attended the Food & NutritionConference & Expo in Denver this fall and willbe participating in other ADA-sponsoredevents later this year including a visit to ADAheadquarters in Chicago, Illinois for theDiversity Committee meeting. She is current-ly serving on the Florida Dietetic Association’sfirst Diversity Task Force. Along with hermembership in PNPG, she is a member of theDietitians in Functional Medicine (DIFM) andSports, Cardiovascular and Wellness Nutrition(SCAN) DPGs. She is also a member of theMIG- Latinos and Hispanics in Dietetics andNutrition (LAHIDAN).
continued from page 3

PNPG POSTPage 6 SPRING 2010
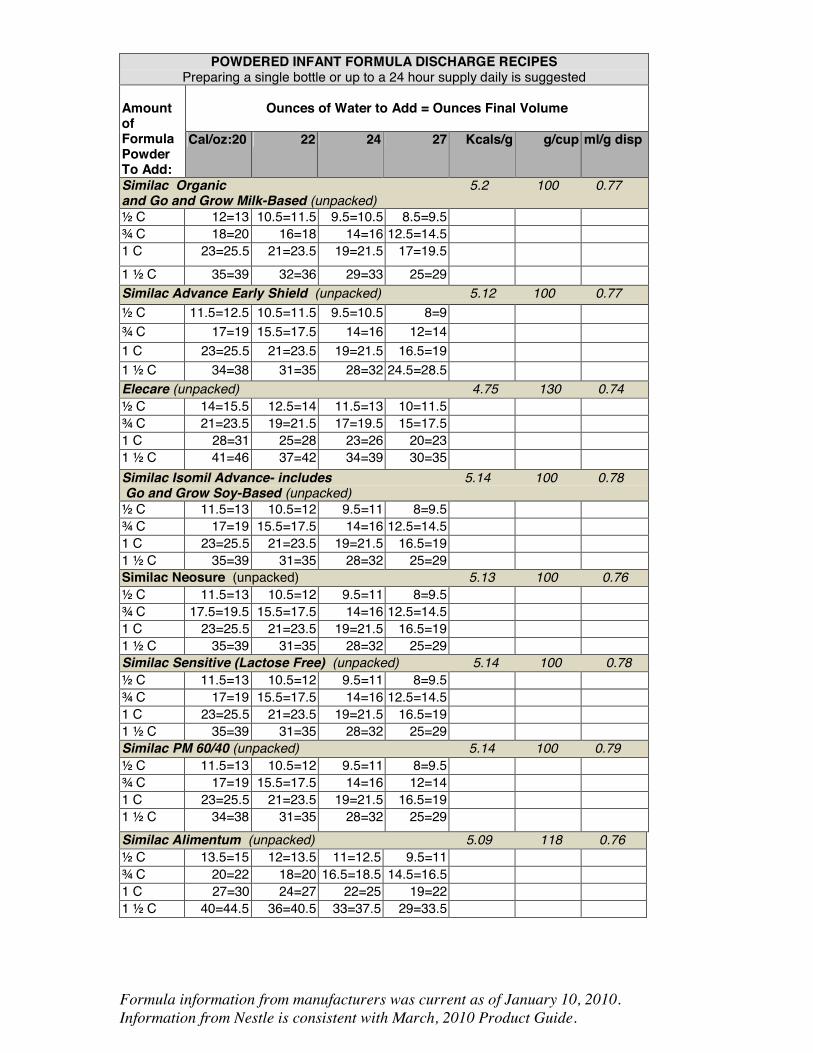
Calorically Dense Infant Formula Recipes Using Household MeasurmentsBy Deb Hustler MS, RD, LD
Akron Children’s Hospital, Akron, OHLiesje Neiman Carney RD, CSP, LDN
The Children’s Hospital of Philadelphia
Within the article below, the authors make ref-erence to “formula recipe tables”. Due to the lengthof the document, these tables will be available onthe PNPG website www.pnpg.org. From the homepage, log in using your last name and ADA mem-bership number. Click on the "Post" link in the col-umn titled "Members" (on the right-hand side ofthe page). In the PNPG Post table of contents, clickon the link to this article: Calorically Dense InfantFormula Recipes Using Household Measurements.Click on the link within the article to download thePDF file of these tables.
Please contact Liesje Nieman Carney with anyquestions or concerns: [email protected]
These recipes were designed for home useby families and caregivers. The intention is touse these recipes when an infant formulagreater than 20 calories per ounce is indicat-ed, and when a larger volume or daily supplyof formula is to be made using measuringcups (rather than using scoops provided inthe product can). If it is essential that a childreceive very precise amounts of certain nutri-ents, as in some metabolic conditions, arecipe using weighed amounts should beused instead. Household measures will havesome variance due to the degree of packingof the powder in the measuring cup orspoon. Standard measuring cups must beused, not a coffee cup, soup spoon, etc. Wheninstructing caregiver(s) about preparation ofthe formula, it is imperative to ascertainwhether they have standard measuringequipment for the required amounts in therecipe. In some circumstances providingmeasuring cups or spoons to the caregiver(s)may be necessary to ensure that the formularecipe will be prepared as instructed. A levelmeasurement should be used, not a roundedone. Also the cup should not be packed (withthe exception of Nutramigen and Pregestimil,for which the manufacturer recommendspacked measurements).
Powdered infant formula products are notsterile; however, these products are the mostpopular for home use due to their conven-ience and cost savings. Because powder for-mula is not sterile, it should not be fed toinfants with a compromised immune systemunless approved by the child’s physician.Formula prepared from powder should bekept in the refrigerator for no more than 24hours and at room temperature for no morethan two hours. Prepared formula in a bottlethat has been fed should be discarded withinone hour after the feeding begins.
The following topics are beyond the scopeof this article and thus have not beenaddressed: formula handling/preparation inthe acute-care setting, administering tubefeedings, and feeding considerations for theimmune-compromised infant and child.Detailed information on these issues can befound in the following resource: Robbins ST,Beker LT. Infant Feedings: Guidelines forPreparation of Formula and Breastmilk inHealth Care Facilities. Chicago, IL: AmericanDietetic Association; 2004. Please note that
an updated edition of this book is anticipatedin November 2010.
Methods Used in Creating FormulaRecipes
Calculations were based on each manufac-turer’s product information at the time ofpublication, included the following: grams ofpowder per cup or scoop, calories per gram,and volume displaced per gram of powderedformula. The volume of water added to thepowder was designed to provide the volume
Formula Preparation Guidelines
Child’s Name: ____________________________________________ Today’s Date: ________________
Formula: ________________________________________________ Calories per ounce: __________
Before mixing the formula:1. Wash all equipment you will use to make the formula (container to mix in, measuring spoons and
cups, mixing spoon or wire whisk) and the bottles, nipples, caps, etc. you will be using in a dishwasher or with clean warm soapy water. Rinse in hot water and dry with a clean cloth or allow to air dry on a clean towel.
2. Wash off the counter surface where you will be preparing the formula with soapy water or an antibacterial spray, rinse with clean water, and dry with a clean towel.
3. Have all of the needed ingredients ready.4. Wash your hands with soap and water just before starting formula preparation. 5. Talk to your health care provider to determine if you need to use sterile water. Water may be
sterilized by boiling for two minutes, then being allowed to cool to room temperature or refrigerated in a clean container for later use. Bottled water is not sterile unless specifically stated on the label.
To make an individual bottle of formula:Use the scoop from the can. Place the scoop back in the can with the handle facing up. Date the canwhen opening and throw away after one month. Mix ____ scoops of formula powder with ____ounces of water. Formula powder is added to the measured water and will make a larger amount.Refrigerate prepared formula until use.
To make a larger batch:Use standard measuring cups and mix _______ cup(s) formula powder with _____ ounces of water.The total volume will be more than the water added. Mix well with a spoon or wire whisk. Store in alarge covered container or pour into individual bottles with caps/covers. Refrigerate until use.
1. Follow mixing and cleaning instructions carefully so that your child receives the right amount and does not become sick from an improperly mixed or contaminated formula.
2. Shake or mix formula before pouring into bottles if storing in a larger container and also before feeding. Throw out any unused mixed formula after 24 hours.
3. Warm formula in a container of warm water, under warm running water, or in an approved bottle warmer, not in a microwave as hot spots may result.
4. Throw out any formula that is still in the bottle one hour after your child has started the feeding, do not refrigerate and reuse partial bottles.
5. If you will be traveling, use ice packs to keep the formula chilled.
If you have any questions about preparing the special formula, contact your dietitian. If your baby ishaving less than 6 wet diapers daily, vomiting, having multiple loose/watery stools, or feeding poorly,contact your child’s doctor or clinic.
Dietitian: __________________________________________ Phone Number: __________________
TABLE 1

Submission Deadlines
Submission Deadlines
Summer 2010 April 16, 2010
Fall 2010 June 21, 2010
Winter 2010 October 4, 2010
Editorial Staff
Editor Monica Nagle, RD, CNSD, LDNPhone: (215) 590-3967; Fax: (215) 590-4460Email: [email protected]
Co-Editor Holly Van Poots, RD, CSP LDNPhone: (336) 832-8172; Fax: (336) 832-8083Email: [email protected]
Communications ChairCarolyn Silzle, MS, MBA, RD, LD Phone: (404) 785-7763; Fax: (404) 785-7157Email: [email protected]
Communications Co-ChairLiesje Nieman Carney, RD, CNSD, LDNPhone: (267) 426-5347; Fax: (215) 590-4460Email: [email protected]
PNPG Post is a quarterly newsletter which keeps members up to date on
continuing education opportunities, educational resources, legislative issues,
publications, and communications regarding the various PNPG activities and
member benefits. The PNPG Post also provides members with Practice Points.
For information, contact the editor.
Publication of an advertisement in the PNPG Post should not be construed as
endorsement of the advertisement, of the advertiser or of the product by the
American Dietetic Association and/or the Pediatric Nutrition Practice Group.
The content of the newsletter does not imply endorsement by the Pediatric
Nutrition Practice Group of the American Dietetic Association © 2010. Copyright
by the Pediatric Nutrition Practice Group of the American Dietetic Association.
All rights reserved.
Monica Nagle, RD, CNSD, LDN
Children’s Hospital of Philadelphia
Department of Clinical Nutrition
34th Street and Civic Center Boulevard, Room 9NW82
Philadelphia PA 19104
PNPG POSTSPRING 2010 Page 7
Editor’s Notes
This publication is supported by a professionalgrant from the Nestlé Nutrition Institute
closest to the total volume for the desired caloric density (i.e.,kcals/oz) using !-ounce increments; these calculations did factor involume displacement of the powdered formula. The goal was lessthan a 0.5 kcal/oz variance. This is easier to achieve in most caseswith larger volumes.
These recipes are all calorically dense formulas created by using for-mula exclusively, which results in products with a higher renal soluteload and osmolality as compared to when that same formula is mixedto standard concentration (i.e., 20 kcal/oz). Depending on the amountof protein and other vitamins/minerals needed, use of a modular maybe more appropriate. Infants with restricted fluid intake must be care-fully evaluated to ensure nutritional needs are being met. Whenever amodified formula is used, the clinician must evaluate the impact onmeeting individual nutrient needs and tolerance.
How to Utilize the TablesWhen using the recipes provided in the tables, first decide on the
caloric density and final volume needed. Identify these on the corre-sponding formula table, and then look horizontally to the left-handcolumn for the amount of formula powder to add.
To provide reinforcement of your verbal instruction, it is recom-mended to use a standardized form to provide written formulapreparation instructions to caregiver(s)—refer to Table 1 for anexample. Notably, if the recipe calls for a !-ounce measurement,write out instructions as the full ounces, then add 1 tablespoon forthe !-ounce (e.g., 4 ! oz of water would be 4 ounces and 1 table-spoon).
DisclaimerProduct information may change. Please refer to the product
label or contact the manufacturer for the most current nutritioninformation and mixing/storage instructions. The RD is encouragedto double check each recipe before providing it to caregiver(s) forhome use. Depending on the caregiver’s ability to demonstrate for-mula preparation techniques, the RD may choose to adjust a givenrecipe. The Pediatric Nutrition Practice Group and the AmericanDietetic Association do not take responsibility for any harm causedto an infant due to improper use of these recipes.
AcknowledgmentsWe would like to take this opportunity to thank everyone else
who contributed to the creation and revision of these tables—AidaMiles, Sandy Robbins, Nikki Sanner and Nancy Wooldridge. We alsowould like to thank the following hospitals for sharing their educa-tion materials with us: Inova Fairfax Hospital for Children (Va),Children’s Hospital Boston, Denver Children’s Hospital, AkronChildren’s Hospital, and The Children’s Hospital of Philadelphia. It’sbeen a lot of work, but we’re thrilled to see it finally published!
TABLE 2: Manufacturer Contact Information
Abbot Nutrition www.abbotnutrition.com
Mead JohnsonNutrition
www.mjn.com/professional
Nestle Infant Nutrition www.medical.gerber.com
Nutrica AdvancedMedical Nutrition
www.nutrica-na.com

Stephanie Howard, MPH, RD, LD, CNSD127 East 46th St., Apt. #7Kansas City, MO 64112
This publication is supported by a professional grant fromthe Nestlé Nutrition Institute.
PRSRT STDU.S. Postage
PAIDLittle Rock, ARPermit No. 307
PNPG POSTPage 8 SPRING 2010
The American Dietetic Association is the world’s largestorganization of food and nutrition professionals. ADA is committed to improving the nation’s health andadvancing the profession of dietetics through research,education, and advocacy.
PNPG MEMBERS!! You are invited to register now for the PNPG and WeightManagement DPG Live Webcast: “Pediatric Weight Management:Nutrition Assessment and Intervention Strategies” on April 20,2010, Noon-2 p.m. CDT, with two hours of CEUs available.
The cost for registration for PNPG and WMDPG membersis $25 per person and $15 for students. The registrationfee for non-members is $35 per person.
To register for this event please go to www.wmdpg.org
For PNPG member questions please contact Lisa Grentzat [email protected]
For WMDPG member questions please contact KimGorman at [email protected]
Speakers:Paula Mrowczynski-Hernandez, RD, LDN and Shelley Kirk, PhD, RD, LD
Session Objectives:
1. Differentiate among assessment tools used for the underweight, healthy weight and obese child. 2. Identify key factors to consider in nutrition assessment and intervention for the overweight and obese child. 3. Learn communication strategies that incorporate parent participation/education during
weight management interventions.4. Implement two new age-appropriate weight management tools during parent/family counseling.

Formula information from manufacturers was current as of January 10, 2010. Information from Nestle is consistent with March, 2010 Product Guide.
Product Information was obtained from the Manufacturers listed below. Added water is in full oz unless the resulting cal/oz were not within 0.5 cals/oz for the designated cal/oz level, then ½ oz were used.
POWDERED INFANT FORMULA DISCHARGE RECIPES
Preparing a single bottle or up to a 24 hour supply daily is suggested
Ounces of Water to Add = Ounces Final Volume
Amount of Formula Powder To Add: Cal/oz: 20 22 24 27 Kcals/g g/cup ml/g disp Enfamil AR, RestFull (unpacked) Max conc=24 cal/oz 5.0 97 0.73 ½ C 11=12 10=11 9=10 n/a ¾ C 16.5=18 15=16.5 13.5=15 n/a 1 C 22=24 20=22 18=20 n/a 1 ½ C 33=36.5 30=33 27=30 n/a Enfamil EnfaCare (unpacked) 4.9 114 0.73 ½ C 12.5=14 11.5=13 10.5=12 9=10.5 ¾ C 19=21 17=19 15.5=17.5 13.5=15.5 1 C 25.5=28 23=25.5 20.5=23 18=20.5 1 ½ C 38=42 34=38 31=35 27=31 Enfamil PREMIUM and Gentlease (unpacked) 5.1 111 0.76 ½ C 13=14.5 11.5=13 10.5=12 9=10.5 ¾ C 19=21 17=19 15.5=17.5 13.5=15.5 1 C 26=29 23=26 21=24 18=21 1 ½ C 38=42 34=38 31=35 27=31 Enfagrow PREMIUM Next Step (unpacked) 5.1 95 0.76 ½ C 11=12 10=11 9=10 8=9 ¾ C 16=18 14.5=16.5 13.5=15.5 11.5=13.5 1 C 22=24.5 19.5=22 18=20.5 15.5=18 1 ½ C 32=35.5 29=32.5 27 =30.5 23=26.5 Enfagrow Soy Next Step (unpacked) 4.8 101 0.71 ½ C 11=12 10=11 9=10 8=9 ¾ C 16=18 15=17 13.5=15.5 11.5=13.5 1 C 22=24.5 19.5=22 18=20.5 15.5=18 1 ½ C 32=35.5 29=32.5 27=30.5 23=26.5 Enfagrow Gentlease Next Step (unpacked) 5.0 108 0.76 ½ C 12=13.5 11=12.5 10=11.5 8.5=10 ¾ C 18=20 16.5=18.5 15=17 13=15 1 C 24=26.5 22=24.5 20=22.5 17=19.5 1 ½ C 36=40 33=37 30=34 26=30 Nutramigen with Enflora LGG (packed) 5.0 97 072 ½ C 11=12 10=11 9=10 8=9 ¾ C 16.5=18 15=16.5 13.5=15 11.5=13 1 C 22=24.5 20=22.5 18=20.5 15.5=18 1 ½ C 33=36.5 30=33.5 27=30.5 23.5=27 Enfamil Nutramigen AA (unpacked) 5.1 115 0.76 ½ C 13=14.5 12=13.5 10.5=12 9.5=11 ¾ C 20=22 18=20 16=18 14=16 1 C 26=29 24=27 21=24 19=22 1 ½ C 40=44.5 36=40.5 32=36.5 28=32.5 Pregestimil (packed) 5.0 128 0.79 ½ C 14.5=16 13=14.5 11.5=13 10=11.5 ¾ C 21.5=24 19.5=22 17.5=20 15.5=18 1 C 29=32.5 26=29.5 23=26.5 20=23.5 1 ½ C 43=48 39=44 35=40 31=36

Formula information from manufacturers was current as of January 10, 2010. Information from Nestle is consistent with March, 2010 Product Guide.
POWDERED INFANT FORMULA DISCHARGE RECIPES
Preparing a single bottle or up to a 24 hour supply daily is suggested
Ounces of Water to Add = Ounces Final Volume
Amount of Formula Powder To Add:
Cal/oz:20 22 24 27 Kcals/g g/cup ml/g disp
Enfamil ProSobee (unpacked) 5.0 128 0.69 ½ C 14.5=16 13=14.5 12=13.5 10.5=12 ¾ C 22=24 20=22 18=20 15.5=17.5 1 C 29=32 26=29 24=27 21=24 1 ½ C 44=48.5 39=43.5 36=40.5 31=35.5 Neocate Infant SHS Nutricia (unpacked) 4.21 114 0.7 ½ C 10.5=12 9.5=11 8.5=10 7.5=9 ¾ C 16=18 14.5=16.5 13=15 11.5=13.5 1 C 21=23.5 19=21.5 17=19.5 15=17.5 1 ½ C 32=36 29=33 26=30 23=27 Gerber Good Start Protect PLUS (unpacked) 5.12 103 0.76 ½ C 12=13.5 11=12.5 9.5=11 8.5=10 ¾ C 18=20 16=18 14.5=16.5 12.5=14.5 1 C 24=26.5 21.5=24 19.5=22 17=19.5 1 ½ C 36=40 32=36 29=33 25=29 Gerber Good Start Gentle PLUS (unpacked) 5.01 105 0.75 ½ C 12=13.5 10.5=12 9.5=11 8.5=10 ¾ C 18=20 16=18 14.5=16.5 12.5=14.5 1 C 23.5=26 21=23.5 19=21.5 17=19.5 1 ½ C 36=40 32=36 29=33 25=29 Gerber Good Start 2 Gentle PLUS (unpacked) 4.92 105 0.75 ½ C 11.5=13 10.5=12 9.5=11 8=9.5 ¾ C 17=19 15.5=17.5 14=16 12.5=14.5 1 C 23=25.5 21=23.5 19=21.5 16.5=19 1 ½ C 35=39 31=35 28=32 25=29 Gerber Good Start 2 Protect PLUS (unpacked) 5.03 105 0.75 ½ C 12=13.5 11=12.5 10=11.5 8.5=10 ¾ C 18=20 16=18 14.5=16.5 12.5=14.5 1 C 24=26.5 21=23.5 19=21.5 17=19.5 1½ C 36=40 32=36 29=33 25=29 Gerber Good Start Soy PLUS (unpacked) 5.01 105 0.75 ½ C 12=13.5 10.5=12 9.5=11 8.5=10 ¾ C 18=20 16=18 14.5=16.5 12.5=14.5 1 C 23.5=26 21=23.5 19=21.5 17=19.5 1 ½ C 36=40 32=36 29=33 25=29 Gerber Good Start 2 Soy PLUS (unpacked) 5.01 105 0.75 ½ C 12=13.5 10.5=12 9.5=11 8.5=10 ¾ C 18=20 16=18 14.5=16.5 12.5=14.5 1 C 23.5=26 21=23.5 19=21.5 17=19.5 1 ½ C 36=40 32=36 29=33 25=29
Formula information from manufacturers was current as of January 10, 2010. Information from Nestle is consistent with March, 2010 Product Guide.
POWDERED INFANT FORMULA DISCHARGE RECIPES
Preparing a single bottle or up to a 24 hour supply daily is suggested
Ounces of Water to Add = Ounces Final Volume
Amount of Formula Powder To Add:
Cal/oz:20 22 24 27 Kcals/g g/cup ml/g disp
Similac Organic 5.2 100 0.77 and Go and Grow Milk-Based (unpacked) ½ C 12=13 10.5=11.5 9.5=10.5 8.5=9.5 ¾ C 18=20 16=18 14=16 12.5=14.5 1 C 23=25.5 21=23.5 19=21.5 17=19.5 1 ½ C 35=39 32=36 29=33 25=29 Similac Advance Early Shield (unpacked) 5.12 100 0.77 ½ C 11.5=12.5 10.5=11.5 9.5=10.5 8=9 ¾ C 17=19 15.5=17.5 14=16 12=14 1 C 23=25.5 21=23.5 19=21.5 16.5=19 1 ½ C 34=38 31=35 28=32 24.5=28.5 Elecare (unpacked) 4.75 130 0.74 ½ C 14=15.5 12.5=14 11.5=13 10=11.5 ¾ C 21=23.5 19=21.5 17=19.5 15=17.5 1 C 28=31 25=28 23=26 20=23 1 ½ C 41=46 37=42 34=39 30=35 Similac Isomil Advance- includes 5.14 100 0.78 Go and Grow Soy-Based (unpacked) ½ C 11.5=13 10.5=12 9.5=11 8=9.5 ¾ C 17=19 15.5=17.5 14=16 12.5=14.5 1 C 23=25.5 21=23.5 19=21.5 16.5=19 1 ½ C 35=39 31=35 28=32 25=29 Similac Neosure (unpacked) 5.13 100 0.76 ½ C 11.5=13 10.5=12 9.5=11 8=9.5 ¾ C 17.5=19.5 15.5=17.5 14=16 12.5=14.5 1 C 23=25.5 21=23.5 19=21.5 16.5=19 1 ½ C 35=39 31=35 28=32 25=29 Similac Sensitive (Lactose Free) (unpacked) 5.14 100 0.78 ½ C 11.5=13 10.5=12 9.5=11 8=9.5 ¾ C 17=19 15.5=17.5 14=16 12.5=14.5 1 C 23=25.5 21=23.5 19=21.5 16.5=19 1 ½ C 35=39 31=35 28=32 25=29 Similac PM 60/40 (unpacked) 5.14 100 0.79 ½ C 11.5=13 10.5=12 9.5=11 8=9.5 ¾ C 17=19 15.5=17.5 14=16 12=14 1 C 23=25.5 21=23.5 19=21.5 16.5=19 1 ½ C 34=38 31=35 28=32 25=29 Similac Alimentum (unpacked) 5.09 118 0.76 ½ C 13.5=15 12=13.5 11=12.5 9.5=11 ¾ C 20=22 18=20 16.5=18.5 14.5=16.5 1 C 27=30 24=27 22=25 19=22 1 ½ C 40=44.5 36=40.5 33=37.5 29=33.5

Formula information from manufacturers was current as of January 10, 2010. Information from Nestle is consistent with March, 2010 Product Guide.
To Make a Single Bottle For All Formulas (EXCEPT NEOCATE, Neosure, EnfaCare and Elecare) 2 scoops=89 kcals and displaces 13-14 ml Cal/oz: 20 22 24 27 Scoops 2 2 3 3
Added Water
4 oz or 120 ml
3 ½ oz or 105 ml
5 oz or 150 ml
4 oz +1 ½ tsp or 127 ml
Approximate Final Volume
4 ½ oz 4 oz 5 ½ oz 5 oz
To Make a Single Bottle For EnfaCare/Neosure 2 scoops=96/99 kcals and displaces 12-15 ml Cal/oz 20 22 24 27 Scoops 2 2 3 5 Added Water
4 1/2 oz or 135 ml
4 oz or 120 ml
5 ½ oz or 165 ml
8 oz or 240 ml
Approximate Final Volume
5 oz 4 1/2 oz 6 oz 9 oz
To Make a Single Bottle For Elecare 2 scoops =89 kcals and displaces 14 ml Cal/oz 20 22 24 27 30 Scoops 2 2 5 5 4 Added Water
4 oz or 120 ml
3 1/2 oz or 105 ml
8 oz or 240 ml
7 oz or 210 ml
5 oz or 150 ml
Approximate Final Volume
4 1/2 oz 4 oz 9 oz 8 oz 6 oz
To Make a Single Bottle For Neocate Infant 1 scoop= 20 kcal and displaces 3.3 ml Cal/oz 20 22 24 27 Scoops 4 4 3 4 Added Water
To make final volume
3 oz or 90 ml
2 oz or 60 ml
2.5 oz or 75 ml
Approximate Final Volume
4 oz or 120 ml
3 ½ oz 70 ml 3 oz

Formula information from manufacturers was current as of January 10, 2010. Information from Nestle is consistent with March, 2010 Product Guide.
MAKING FORMULA FROM CONCENTRATED LIQUID
Cal/oz
Amount of Liquid
Concentrate
Amount of Sterile Water
Added
To Make
Final Volume 20 13 oz=390 ml 13 oz=390 ml 26 oz=780 ml
22 13 oz=390 ml 11 oz=330 ml 24 oz=720 ml
24 13 oz=390 ml 9 oz=270 ml 22 oz=660 ml
27 13 oz=390 ml 6 oz=180 ml 19 oz=570 ml
*All Concentrated Liquid Formulas come ONLY in 13 oz cans
Enfaport Cal/Oz Ready-to-Use Enfaport (oz) Water (oz) 20 8 4 22 8 2.9 24 8 2 27 8 0.9
Concentrated Liquid Formulas: 40 cal/oz or 1.33 cal/ml 30 ml = 1 oz
13 oz can = 390 ml
WIC provides concentrated liquid formulas, if specified. Formulas available in concentrated liquid:
Enfamil PREMIUM, Lactofree, Generic Store Brand, Generic Store Brand Soy, Good Start Gentle PLUS, Protect PLUS and Soy PLUS, Isomil Advance, Nutramigen, Prosobee, Similac Advance Early Shield, Similac Sensitive
Concentrated liquid formula is sterile and less vulnerable to preparation error and bacterial contamination.

Formula information from manufacturers was current as of January 10, 2010. Information from Nestle is consistent with March, 2010 Product Guide.
RECIPES FOR ADDING POWDERED INFANT FORMULA TO BREAST MILK
These recipes are designed for discharge instructions
Health care facilities should use commercially sterile forms of formula when available; any powdered formulas used should be measured by weight
Powdered Infant Formulas This chart was developed based on the following data: 1 tsp formula = approximately 13 cal 1 scoop formula = approximately 44 cal Always use the scoop that comes with the can of powder formula. Ensure family has liquid measuring containers (such as an accurate baby bottle) to measure liquids. Babies ready for discharge do not require the accurate formula calculations that are used in the hospital. *USE THE FOLLOWING RECIPES FOR ALL POWDERED INFANT FORMULAS (except Neocate) TO BE MIXED WITH BREAST MILK: Home Preparation Instructions: To make 24 cal/oz Breast Milk: 1 tsp formula + 3 oz Breast Milk or 1 scoop formula + 11 oz Breast Milk To make 26-27 cal/oz Breast Milk: 1 tsp formula + 2 oz Breast Milk or 1 scoop formula + 7 oz Breast milk It is best to prepare recipes for single feeding volumes to minimize risk of bacterial contamination. *Recipes for single feeding volumes are recommended for stability of the mixture and infection control purposes.
Manufacturer websites for further information: www.AbbottNutrition.com www.mjn.com/professional www.nestleinfantnutrition.com www.Nutricia-NA.com





























