Embed Size (px)
Citation preview

Case Report
Pneumopericardium and Severe SubcutaneousEmphysema after Laparoscopic Surgery
Ma-Lee Ko, MD, MHA*From the Department of Obstetrics and Gynecology, Cheng-Hsin General Hospital, Taipei, Taiwan.
ABSTRACT Subcutaneous emphysema is a known complication of laparoscopic surgery. Occasionally, subcutaneous emphysema is severe
The author has no
ucts or companie
Corresponding au
and Gynecology,
E-mail: perpie_pa
Submitted Decem
Available at www
1553-4650/$ - see
doi:10.1016/j.jmi
enough to cause pneumopericardium. This case report describes a rare but potentially serious complication of pneumopericar-
dium occurring after laparoscopy. Contributing factors and possible etiologies are discussed. Journal of Minimally Invasive
Gynecology (2010) 17, 531–533 � 2010 AAGL. All rights reserved.
Keywords: Pneumopericardium; Subcutaneous emphysema
Laparoscopic surgery is being performed with increasing
frequency in gynecology because of its advantages including
shorter hospital stay, less operative wound pain, and faster
recovery. Laparoscopic surgery in gynecology, however, is
not free of complications. Subcutaneous emphysema is one
of the most common but perhaps most underreported compli-
cation of this procedure. According to McAllister et al [1],
subcutaneous emphysema occurs in 20% to 60% of all lapa-
roscopic operations. When subcutaneous emphysema was
evaluated on postoperative x-ray films, Wolf et al [2] found
the incidence to be 34% to 77%. Occasionally, carbon
dioxide (CO2) accidentally enters the mediastinum and
even the pericardium. Although most often this resolves in-
stantaneously, at times it may be severe enough to be life-
threatening. Herein, we report a case of severe subcutaneous
emphysema with pneumopericardium that was observed
during laparoscopic adnexectomy of a borderline tumor.
Case Report
A 29 year old G0 P0 woman with a body mass index of 20
was admitted to the emergency room with severe and sudden
onset of lower abdominal pain. The patient denied sexual
intercourse within the last 48 hours. However, she reported
dyspareunia and painful menstruation for the last 3 years.
commercial, proprietary, or financial interest in the prod-
s described in this article.
thor: Ma-Lee Ko, MD, MHA, Department of Obstetrics
Cheng-Hsin General Hospital, Taipei 112, Taiwan.
ber 18, 2009. Accepted for publication March 7, 2010.
.sciencedirect.com and www.jmig.org
front matter � 2010 AAGL. All rights reserved.
g.2010.03.006
In the emergency room, her vital signs were stable. Physical
examination revealed direct and rebound tenderness of the
right lower abdomen. Blood tests demonstrated leukocystosis
(19 000/mL3) with 97% neutrophils. The patient was referred
for gynecologic consultation, and a pelvic examination
elicited cervical motion tenderness. The right adnexa was
enlarged and tender. Ultrasound examination of the pelvis
demonstrated a cystic right adnexa measuring 8 ! 6 cm.
There was also fluid in the cul-de-sac, which was estimated
at 400 mL. The patient was scheduled for emergency laparo-
scopic surgery because of a ruptured right ovarian cyst.
General anesthesia was administered with endotracheal
intubation, and the patient was placed in the dorsolithotomy
position. A uterine manipulator was fixed on the cervix via
a tenaculum to enable uterine mobilization. A Veress needle
was first placed in the umbilicus, and insufflation was started
at 1 L/min, with an initial pressure of less than 8 mm Hg.
Hyperdistention of the abdominal cavity to an insufflation
pressure of 25 mm Hg was achieved before inserting the
ports: one 10-mm trocar for visualization and three 5-mm tro-
cars for instruments (1 placed in the suprapubic area and 2
ports placed laterally on each side of the abdomen). After
the ports were inserted, insufflation pressure was reduced
to 15 mm Hg, which was maintained during the operative
procedure. Ventilation parameters during insufflation in-
cluded oxygen saturation as measured using pulse oximetry
(SpO2), 99 mm Hg; extrapolated end-tidal CO2 tension
(PETCO2), 35 mm Hg; and airway pressure, 21 cm of water.
A large right ovarian mass occupying the entire pelvis was
observed, and approximately 350 mL of mucinous fluid was
aspirated from the cyst. Minute papillary excrescences were
also noted to protrude from the cyst capsule. A frozen section

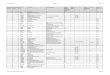
Fig 1. Chest radiograph reveals subdiaphragmatic air and a clearly identifi-
able pneumopericardium.
532 Journal of Minimally Invasive Gynecology, Vol 17, No 4, July/August 2010
of the ovarian tissue fragment demonstrated a mucinous bor-
derline tumor, with mild to moderate nuclear atypia. There
was no evidence of destructive stromal invasion. Unilateral
adnexectomy was performed, followed by appendectomy.
Midway through the appendectomy (85 minutes into the
surgery), an increase in PETCO2 (60 mm Hg) and acidosis
(arterial blood gas pH, 7.13; PCO2, 80 mm Hg; PO2, 521
mm Hg; base excess, 23.8) were observed. A central line
was not placed.
Meticulous examination of the upper part of the body un-
der the surgical drapes revealed subcutaneous emphysema
over the thorax, neck, and face. Crepitus was also palpated
over the same areas. Hypercarbia was corrected by increasing
fraction of inspired oxygen to 1 (100% O2). The insufflation
pressure was also lowered and maintained at 12 mm Hg, and
the surgery was then completed. The operation lasted for 180
minutes, and pneumoperitoneum for 120 minutes. Blood loss
was minimal (100 mL). Assisted ventilation was adminis-
tered for another 15 minutes after surgery. The patient’s vital
signs remained stable. Extubation requirements were met,
and no hypercarbia was demonstrated. The patient was
observed in the postanesthesia care unit. Half an hour postop-
eratively, the patient suddenly developed sharp localized sub-
sternal chest pain. The pain was aggravated by breathing and
was associated with cold sweating, pallor, and difficulty in
breathing. Heart sounds were distant at auscultation. An elec-
trocardiogram showed diffuse T-wave abnormalities, with
T-wave inversion in leads V2 to V6. Because of concern for
evolving myocardial ischemia, the patient was transferred
to the intensive care unit. The serum creatine kinase-MB con-
centration was within normal limits. Troponin T and D-dimer
were both negative. A chest radiograph revealed subdiaph-
ragmatic air and a clearly identifiable pneumopericardium
(Fig 1). The pneumopericardium was managed expectantly,
and the chest pain with naproxen sodium (Naprosyn; Kojar
Pharmaceutical Industrial Co Ltd., Taiwan), 500 mg 3 times
a day. The symptoms decreased, and finally resolved by
postoperative day 3, at which time an electrocardiogram
demonstrated resolution of the T-wave abnormalities.
Follow-up chest x-ray films showed progressive reduction
of the pneumopericardium. Five days later, the patient was
discharged from the hospital without symptoms.
Discussion
Subcutaneous emphysema is a known complication of
laparoscopic surgery, and is caused by extravasation of
CO2 into the subcutaneous tissues. It has been perceived as
a relatively harmless complication [3]. However, severe sub-
cutaneous emphysema could lead to severe hypercarbia. This
is brought about by gaseous interchange between the subcu-
taneous CO2 and blood perfusing into the subcutaneous
tissue [3–5]. Occasionally, subcutaneous CO2 may dissect
into the prefascial planes, leading to pneumothorax,
pneumomediastinum, and pneumopericardium [5]. Although
pneumopericardium has been recognized after laparoscopic
urologic and gastrointestinal procedures, it has rarely been
reported after a gynecologic laparoscopy procedure. Most
cases were asymptomatic and were diagnosed incidentally
at radiography. Some patients reported abdominal pain as
the initial symptom, which led to the diagnosis [6].In some
cases, pneumopericardium mimics acute myocardial
ischemia, severe enough to cause electrocardiograph
abnormalities, as in our patient [7,8].
Several factors are associated with development of severe
subcutaneous emphysema at laparoscopy. According to Mur-
dock et al [9] and Esposito et al [10], development of emphy-
sema increases with age because the natural subcutaneous
resistance to gas insufflation decreases with age. A body
mass index less than 25 was also significantly associated
with development of subcutaneous emphysema [11]. Dura-
tion of the operative procedure, higher insufflation pressure,
use of more than 3 surgical ports, and the extraperitoneal
laparoscopic approach are among the operative factors
identified [3,12]. Creation of a false passage during trocar
placement, manipulation of instruments at acute angles, and
faulty trocar seals at entry and exit points are among other
causes [12,13].
The etiology of pneumopericardium as a result of laparo-
scopic procedure is unclear. According to Nicholson and
Berman [14], gas can reach the pericardial cavity and the
mediastinum via a path along the inferior vena cava through
the diaphragm. Thus, with increased insufflating pressure,
CO2 could track through an existing congenital defect of
the pericardial sac.
Pneumothorax has been reported during laparoscopic
procedures. During surgery, an increase in positive

Ko. Pneumopericardium 533
inspiratory pressure, a decrease in SpO2, and decreased breath
sounds on 1 side suggest the diagnosis, which should be con-
firmed at chest radiography [15]. The laparoscopist may be
able to demonstrate abnormal motion of 1 hemidiaphragm.
Reduced QRS amplitude in precordial electrocardiographic
leads further supports the diagnosis. The surgeon and the
anesthesiologist should be aware of decreasing mean arterial
pressure and SpO2, which suggests tension pneumothorax,
because immediate decompression is required.
Increased CO2 load observed during extraperitoneal insuf-
flation can usually be corrected with controlled ventilation,
and may be averted by increasing minute ventilation. Chest
tube drainage should not be performed during surgery
because it will make it difficult to maintain the pneumoperi-
toneum. Increasing the fraction of inspired oxygen to 100%,
addition of 5 cm of positive end-expiratory pressure, and
reduction of intra-abdominal pressure to less than 15 mm
Hg will maintain oxygenation and enable surgery to be
completed [16,17].
Subcutaneous emphysema at physical examination and
radiographic pneumodissection typically resolve over several
hours or sometimes after 3 to 4 days [17]. Both conditions are
usually self-limiting and are managed expectantly. Explana-
tion and reassurance may be necessary for the patient in the
postoperative care unit.
In conclusion, surgeons should be aware of the possibility
of pneumopericardium in patients with chest pain and electro-
cardiographic abnormalities after a laparoscopic procedure.
References
1. McAllister JD, D’Altorio RA, Snyder A. CT findings after uncompli-
cated percutaneous laparoscopic cholecystectomy. J Comput Assis
Tomogr. 1991;15:770–772.
2. Wolf JS, Clayman RV, Monk TG, McClennan BL, McDougall EM.
Carbon dioxide absorption during laparoscopic operation. J Am CollSurg. 1995;180:555–560.
3. Singh K, Sinhal A, Saggar VR, Sharma B, Sarangi R. Subcutanous
carbon dioxide emphysema following endoscopic extraperitoneal hernia
repair: possible mechanisms. J Laparoendosc Adv Surg Tech. 2004;14:
317–320.
4. Worrell JB, Cleary DT. Massive subcutaneous emphysema and hyper-
carbia: complications of carbon dioxide absorption during extraperito-
neal and intraperitoneal laparoscopic surgery; case studies. AANA
J. 2002;70:456–461.
5. Siu W, Weifman BD, Wolf JS. Subcutaneous emphysema, pneumome-
diastinum and bilateral pneumothoraces after laparoscopic pyeloplasty.
J Urol. 2003;170:1936–1937.
6. Barba MA, Saez L, Garcia-Molinero MJ, Aguilera M. Pneumopericar-
dium without subcutaneous emphysema, pneumomediastinum, or
pneumothorax after laparoscopy. Gastrointest Endosc. 1993;39:740.
7. Yeoh CJ, Dawson C, Wiseman OJ. Pneumopericardium: a rare compli-
cation of laparoscopic varicocoele ligation. Int Urol Nephrol. 2006;38:
671–672.
8. Beaver J, Safran D. Pneumopericardium mimicking acute myocardial
ischemia after laparoscopic cholecystectomy. South Med J. 1999;92:
1002–1004.
9. Murdock CM, Wolff AJ, Van Geem T. Risk factors for hypercarbia,
subcutaneous emphysema, pneumothorax, and pneumomediastinum
during laparoscopy. Obstet Gynecol. 2000;95:704–709.
10. Esposito C, Ascione G, Garipoli V, Bernardo De, Esposito G. Compli-
cations of pediatric laparoscopic surgery. Surg Endosc. 1997;11:
655–657.
11. Ng CS, Gill IS, Sung GT, Whalley DG, Graham R, Schweizer D. Retro-
peritoneoscopic surgery is not associated with increased CO2 absorp-
tion. J Urol. 1999;162:1268–1272.
12. Saggar VR, Singhal A, Singh K, Sharma B, Sarangi R. Factors influenc-
ing development of subcutaneous carbon dioxide emphysema in laparo-
scopic totally extraperitoneal inguinal hernia repair. J Laparoendosc
Adv Surg Tech. 2008;18:213–216.
13. Singh K, Singal A, Saggar VR, Sharma B, Sarangi R. Subcutaneous CO2
emphysema following endoscopic extraperitoneal hernia repair: possi-
ble mechanisms. J Laparoendosc Adv Surg Tech. 2004;14:317–320.
14. Nicholson D, Berman N. Pneumopericardium following laparoscopy.
Chest. 1979;76:605–607.
15. Perko G, Fernandez A. Subcutaneous emphysema and pneumothorax
during laparoscopy for ectopic pregnancy removal. Acta Anaesthesiol
Scand. 1997;41:742.
16. Chiche JD, Joris J, Lamy M. PEEP for treatment of intra-operative
pneumothorax during laparoscopic fundoplication. Br J Anaesth.
1994;72:A38.
17. Vorach-Brodsky L. Anesthesia. In: Nezhat C, Nezhat F, Nezhat C, editors.
Nehzat’s Operative Gynecologic Laparoscopy and Hysteroscopy. 3rd ed.
New York, NY: Cambridge University Press; 2008.









![Case Report Subcutaneous Emphysema, Pneumomediastinum, … · 2019. 7. 31. · [ ]E.Hillewig,E.Aghayev,C.Jackowski,A.Christe,T.Plattner, and M. J. ali , Gas embolism following intraosseous](https://img.dokumen.tips/doc/110x75/61254bca97cc8d09c20890f9/case-report-subcutaneous-emphysema-pneumomediastinum-2019-7-31-ehillewigeaghayevcjackowskiachristetplattner.jpg)

![Subcutaneous Emphysema in Critically Ill Children · the oropharyngeal, digestive or respiratory systems [1]. It occurs relatively frequently in pediatric patients, sometimes even](https://img.dokumen.tips/doc/110x75/5f8f0a33c22b2153eb36e621/subcutaneous-emphysema-in-critically-ill-children-the-oropharyngeal-digestive-or.jpg)



![Case Report Subcutaneous Emphysema, …downloads.hindawi.com/journals/criem/2015/134816.pdfpneumothorax, pneumomediastinum, pneumopericardium, or subcutaneous emphysema [ ]. Diagnosis](https://img.dokumen.tips/doc/110x75/5f4072ff5627821a5534fd08/case-report-subcutaneous-emphysema-pneumothorax-pneumomediastinum-pneumopericardium.jpg)












