Embed Size (px)
Citation preview

PNEUMONIA IN DAILY PRACTICE
Ananda Wibawanta Ginting, MD
THE 7TH JAKARTA INTERNATIONAL CHEST AND CRITICAL CARE INTERNAL MEDICINE (JICCIM)
6-7 APRIL, 2019

HISTORY• Was described 2,500 years ago by
Hippocrates
• William osler: captain of the men of
death
• 1930: the third leading cause of
death in USA
• “The Winter fever”
Figure 1. Pneumonia ranks third... Sources:
States U, Osler W. Whom does it affect?
2006;155–63.

DEFINITION
• Pneumonia is an inflammation of the lung, usually caused by an infection
• The most common cause: bacterial, virus, fungi
• Classification: community-acquired pneumonia (CAP); hospital-acquired
pneumonia (HAP); and ventilator-associated pneumonia (VAP)
• Can be transmitted by the aspiration or by inhalation of a pathogenic
microorganism

EPIDEMIOLOGY
Figure 2. Top 10 global causes of deaths, 2016.
Source: Global health estimates 2016: Deaths
by cause, age, sex, country and by region,
2000-2016. Geneva. WHO; 2018
Figure 3. Top 10 causes of death in 2017 and
percent change, 2007-2017, all ages, number.
Sources: http://www.healthdata.org/indonesia

• Pneumonia is caused by the invasion and
overgrowth of pathogens in the lung parenchym
• Infection can also spread from the lungs,
causing complications such as bacteraemia,
sepsis, meningitis, empyema and septic
embolism
• Summary pathogenesis of pneumonia are:
• Alteration of normal oropharyngeal flora
• Depressed cough and glottis reflexes
• Altered consciousness
• Impaired mucocilliary apparatus
mechanism
• Alveolar macrophage dysfunction
• Immune dysfunction
PATHOLOGY AND PATHOGENESIS
Table 1. Pathophysiological modes of spread.
Source: Singh Y D, Pathophysiology of community
acquired pneumonia

• Not always necessary
• Recommendations etiologic testing: patients with severe CAP or CAP unresponsive to the initial empiric treatment regimen, and ICU patients (VAP).
• In selected cases: galactomannan and (1-3)-β-D-glucan tests for fungi, the latest antigen or molecular biology tests for viruses and atypical pathogens
• Streptococcus pneumoniae (pneumococcus) is the most common pathogen causing community-acquired pneumonia.
• Hospital: wide range of pathogens (the patients and the hospital environment). Gram negative bacteria are more frequent than Gram-positive bacteria in these cases
MICROBIAL ETIOLOGY OF PNEUMONIA
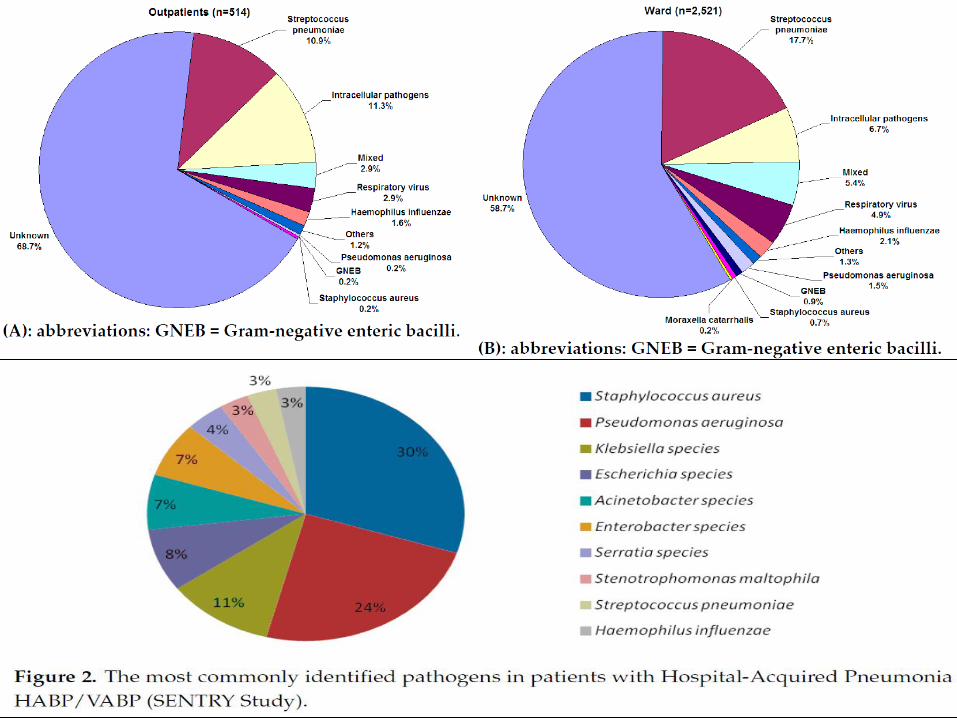

Figure 5. Pathogen associated with early-onset and late-onset pneumonia.
Sources: Cilloniz C et al. Int. J. Mol. Sci. 2016, 17, 2120

INVESTIGATIONS DIAGNOSTIC
History and Physical
Examination
Imaging Methods
Laboratorium and
biomarkers
Scoring systems
criteria

Source: Kaysin A, Viera AJ, Carolina N, Hill C, Carolina N.
Community-Acquired Pneumonia in Adults: Diagnosis and
Management. 2016;
Table 2. Risk Factors and Pathogens in
Community-Acquired Pneumonia
INVESTIGATIONS DIAGNOSTICHistory and Physical
Examination

Table 3. Factors associated with community-acquired pneumonia Bartolf A, Cosgrove C, Pneumonia, Medicine (2016), Torres A, et al.
Thorax 2013;68:1057–1065.

Figure 6. The impact of age on the incidence of patients hospitalized with community-
acquired pneumonia. Sources: Ramirez et al. Adults With Pneumonia: Incidence and
Mortality. CID 2017:65

Figure 7. The impact of comorbid conditions on the incidence of patients hospitalized
with community-acquired pneumonia. Sources: Ramirez et al. Adults With Pneumonia:
Incidence and Mortality. CID 2017:65

Table 4. Risk factors for drug-resistant pneumonia pathogens. Sources:
Rider AC. Community acquired pneumonia. Emerg Med Clin N Am 2018.

SYMPTOMS
• Productive cough
• Fever
• Chest pain
• Dyspnea
• Haemoptysis
• Decreased exercise tolerance
• Abdominal pain
• Malaise
• Non specific symptoms
SIGNS AND SYMPTOMSSIGNS
• Reduced expansions
• Crackles
• Bronchial breathing
• Reduced breath sound
• Lymphadenopathy
• High or low temperature,
• Tachypnoea
• Use of accessory muscles,
• Tachycardia
• Cyanosis
• Altered mental status
INVESTIGATIONS DIAGNOSTIC
History and Physical
Examination

INVESTIGATIONS DIAGNOSTICImaging Methods
• Chest Radiography: Standard method of diagnosing pneumonia.
differentiate lobar and bronchopneumonia and it can reveal cavitation,
effusion or air bronchograms.
• Further imaging, for example ultrasonography or computed
tomography, can be warranted in certain situations
• Lung ultrasonography has the potential to more accurately and
efficiently diagnose pneumonia, as well as pleural effusions,
pneumothorax, pulmonary embolism, and pulmonary contusions
• Chest CT is the most sensitive method for identifying infectious
involvement of the lung parenchym.


INVESTIGATIONS DIAGNOSTIC
Laboratorium and
biomarkers
• Blood tests: CBC, inflammatory markers, RFT and LFT and oxygen
saturation (blood gasses analysis)
• Sputum and blood cultures
• Urinary antigen tests for pneumococcal and legionella, nasopharyngeal
samples
• Inflammatory markers: CRP, Procalcitonin
• HIV testing, tuberculosis, PCP: high risk sexual exposures or history of
injection drug use
• For people presenting with symptoms of lower respiratory tract infection in
primary care, consider C-reactive protein test if after clinical assessment a
diagnosis of pneumonia has not been made and it is not clear whether
antibiotics should be prescribed
C-reactive protein test to guide antibiotic prescribing in people without a
clinical diagnosis of pneumonia
• CRP < 20 mg/litre: Do not routinely offer antibiotic
• CRP 20-100 mg/litre: Consider a delayed antibiotic prescription (a
prescription for use at a later if symptoms worsen)
• CRP > 100 mg/litre: Offer antibiotic therapy if the C-reactive protein

INVESTIGATIONS DIAGNOSTICLaboratorium and
biomarkers
Figure 8. Serum procalcitonin (PCT) levels in community-acquired pneumonia (CAP). Adapted
from Julián-Jiménez et al.

INVESTIGATIONS DIAGNOSTICLaboratorium and
biomarkers
Table 8. Diagnostic testing in patients with suspected CAP. Sources: , Kaysin A, Vera JA.
Community Acquired Pneumonia in Adults: Diagnosis and Management. American Family
Physician Volume 94, Number 9 November 1 2016

INVESTIGATIONS DIAGNOSTICLaboratorium and
biomarkers
Table 9. Samples and Diagnostic Testing in Pneumonia. Sources: Cilloniz et al, Int. J. Mol.
Sci. 2016, 17, 2120

INVESTIGATIONS DIAGNOSTICScoring systems
• Patients with a diagnosis of CAP should always be assessed for disease
severity, a precaution that has a direct positive impact on mortality
• PSI, CURB 65, SMART-COP, SCAP 2007 IDSA/ATS guidelines
Table 10. Pneumonia Severity Index Scoring and Risk stratification by the Pneumonia
Severity Index. Adapted from Correa et al.

INVESTIGATIONS DIAGNOSTICScoring systems
Figure 9. CURB-65 score and suggested site of care for patients with community-acquired pneumonia. CURB-
65: mental Confusion; Urea > 50 mg/dL; Respiratory rate > 30 breaths/min; Blood pressure (systolic < 90 mmHg
or diastolic < 60 mmHg); and age ≥ 65 years; and CAP: community-acquired pneumonia. Adapted from Correa et
al.

INVESTIGATIONS DIAGNOSTICScoring systems
Table 11. Criteria for severe acquired CAP. Adapted from Kaysin A, Vera JA.
Community Acquired Pneumonia in Adults: Diagnosis and Management. American
Family Physician Volume 94, Number 9 November 1 2016

Figure 10. Risk stratification in the emergency room. Sources: Kolditz M et al
INVESTIGATIONS DIAGNOSTIC

INVESTIGATIONS DIAGNOSTIC
Figure 12. Does patient have pneumonia, an alternative diagnosis, or
perhaps both?

INVESTIGATIONS DIAGNOSTIC
Figure 13. Profile of disease severity

INVESTIGATIONS DIAGNOSTIC
Table 12. The Clinical Pulmonary Infection score (CPIS). Source: Basyigit S et al.
• Simple tool for the diagnosis of VAP is a scoring system which
included 7 clinical parameters for VAP diagnosis

• Pneumonia can be prevented by the use of pneumococcal and
influenza vaccines in appropriate at risk populations.
• Smoking cessation should be promoted in all patients.
• Patients with severe pneumonia or a sepsis syndrome should have
antibiotic treatment within an hour, fluid resuscitation, oxygen therapy
and close observation with additional supportive treatment
• The initial antibiotic regimen is determined empirically
TREATMENT
Low-severity CAP• 5-day course of a single antibiotic to patients with low-severity CAP
pneumonia.
• Consider extending the course of the antibiotic for longer than 5 days as a
possible management strategy for patients with low-severity CAP whose
symptoms do not improve
• Do not routinely offer patients with low-severity CAP: a fluoroquinolone, dual
antibiotic therapy.

Moderate- and high-severity CAP
• Consider a 7- to 10-day course of antibiotic therapy for patients with moderate or
high-severity CAP.
• Consider dual antibiotic therapy with amoxicillin and a macrolide for patients
with moderate-severity CAP.
• Consider dual antibiotic therapy with a beta-lactam and a macrolide for patients with
high-severity CAP.
TREATMENT
Hospital-acquired pneumonia
Antibiotic therapy
• Offer antibiotic therapy as soon as possible after diagnosis, and certainly within
4 hours, to patients with HAP.
• Choose antibiotic therapy in accordance with local hospital policy (which should
take into account knowledge of local microbial pathogens) and clinical
circumstances for patients with HAP.
• Consider a 5- to 10-day course of antibiotic therapy for patients with HAP.

CAP is present
Outpatient therapy Inpatient therapy
No cardiopulmonary
disease, no modifiers
GROUP 1, TABLE 2
History of cardiopulmonary
disease, +/- modifiers
GROUP II, TABLE 3Mild-moderate illness Severe CAP
Cardiopulmonary disease +/or
modifiers
No Cardiopulmonary disease,
no modifiersNo Risk for P. Aeruginosa Risk for P. Aeruginosa
Group III, TABLE 4A Group III, TABLE 4B Group IV, TABLE 5A Group IV, TABLE 5B
TREATMENT

OUTPATIENT THERAPY

INPATIENT THERAPY

Table 13. Guideline recommendations on duration of antibiotic therapy for community-
acquired pneumonia. Sources: Correa et al. J Bras Pneumol. 2018;44(5):405-423

Table 14. Recommended Initial Empiric Antibiotic Therapy for Hospital-Acquired
Pneumonia (Non-Ventilator-Associated Pneumonia)
HAP TREATMENT

Table 15. Suggested Empiric Treatment Options for Clinically Suspected Ventilator-
Associated Pneumonia
VAP TREATMENT

PREVENTION
• Vaccination: influenza and pneumococcal
• Smoking cessation
• Immunocompromised patient should avoid close contact with person who
have lower respiratory tract infections
• Stop alcohol consumption
Ventilator-associated Pneumonia (VAP) Prevention Bundle. Sources: Miller F.
ATOTW 382- Ventilator associated pneumonia, june 2018

Do not routinely discharge patients with community-acquired pneumonia if in
the past 24 hours they have had 2 or more of the following findings:
• Temperature higher than 37.5°C
• Respiratory rate 24 breaths per minute or more
• Heart rate over 100 beats per minute
• Systolic blood pressure 90 mmHg or less
• Oxygen saturation under 90% on room air
• Abnormal mental status
• inability to eat without assistance.
DISCHARGE ATTENTION
Explain to patients with CAP that after starting treatment, their symptoms should
steadily improve, although the rate of improvement will vary with the severity of the
pneumonia.
1 week: fever should have resolved
4 weeks: chest pain and sputum production should have substantially reduced
6 weeks: cough and breathlessness should have substantially reduced
3 months: most symptoms should have resolved but fatigue may still be present
6 months: most people will feel back to normal.
PATIENT INFORMATION

COMPLICATIONS

Thank you





























