Embed Size (px)
Citation preview

Pc
DC
a
ARR1AA
KI7SA
1
bmtvIph2a
B
0d
Vaccine 30 (2012) 2206– 2211
Contents lists available at SciVerse ScienceDirect
Vaccine
j ourna l ho me pag e: www.elsev ier .com/ locate /vacc ine
neumococcal disease in South Australia: Vaccine success but no time foromplacency
avid R. Johnson ∗, Katina D’Onise, Ros A. Holland, Jane C.A. Raupach, Ann P. Koehlerommunicable Disease Control Branch, SA Health, Australia
r t i c l e i n f o
rticle history:eceived 22 September 2011eceived in revised form2 December 2011ccepted 23 December 2011vailable online 23 January 2012
eywords:nvasive pneumococcal diseasevPCV effectivenesserotype replacementustralia
a b s t r a c t
Background: Trends in age specific and serotype specific incidence rates for invasive pneumococcal disease(IPD) were examined in South Australia 4 years before and 5 years after the commencement of theAustralian universal childhood 7 valent pneumococcal conjugate vaccine (7vPCV) program.Methods: IPD cases were identified by routine enhanced surveillance. IPD serotypes were groupedaccording to those covered by the 7vPCV, the six serotypes specific to the 13 valent pneumococcalconjugate vaccine (13vPCV), the 11 serotypes specific to the 23 valent pneumococcal polysaccharidevaccine (23vPPV), as well as non-13vPCV and non-23vPPV groups. Poisson regression was used to calcu-late age-specific and serotype-specific incident rate ratios (IRRs) comparing pre (2002–2004) and post(2007–2009) universal childhood 7vPCV periods.Results: Following the introduction of the 7vPCV program, the rate of IPD in children aged <2 yearsdecreased by 81% for all serotypes (IRR 0.19, 95% CI, 0.13–0.28) and by 98% for 7vPCV serotypes (IRR 0.02,95% CI, 0.007–0.07). At the same time, there was some evidence for an increase in IPD caused by 13vPCVspecific serotypes (IRR 1.58, 95% CI, 0.78–3.21) and non-13vPCV serotypes (IRR 1.80, 95% CI, 0.45–7.21).Among adults aged ≥65 years, overall there was a 27% reduction in IPD caused by all serotypes followingintroduction of the 7vPCV program (IRR 0.73, 95% CI, 0.58–0.93). However, the rate of IPD increased in thelast 2 years of the study period. The initial decrease was a result of a 74% reduction in the rate of IPD dueto 7vPCV serotypes (IRR 0.26, 95% CI, 0.17–0.40). At the same time, the rate of IPD increased for 13vPCV
specific serotypes (IRR 1.55, 95% CI, 0.94–2.54), 23vPPV specific serotypes (IRR 1.91, 95% CI, 0.99–3.71)and particularly non-23vPPV serotypes (IRR 5.3, 95% CI, 1.83–15.34).Conclusion: There has been a large direct and sustained benefit from the universal 7vPCV program in chil-dren, particularly those aged <2 years, with some evidence for serotype replacement. There is also goodevidence that the childhood program has provided indirect benefits to adults aged ≥65 years, althoughserotype replacement has reduced the initial benefits.. Introduction
Invasive pneumococcal disease (IPD), defined as disease causedy Streptococcus pneumoniae in a normally sterile body site, is aajor public health problem worldwide with children <2 years and
he elderly carrying the major burden of disease [1]. A number ofaccines aimed at reducing the incidence of IPD (as well as non-PD) are currently available. In Australia, a publicly funded 7 valentneumococcal conjugate vaccine (7vPCV) program commenced for
igh-risk children in 2001 involving a 3 dose schedule given at, 4 and 6 months of age. This program was subsequently madevailable to all children aged <2 years from 1 January 2005. Prior∗ Corresponding author at: Communicable Disease Control Branch, SA Health, POox 6, Rundle Mall, Adelaide, South Australia 5000, Australia. Tel.: +61 8 8273 7200.
E-mail address: [email protected] (D.R. Johnson).
264-410X/$ – see front matter © 2012 Elsevier Ltd. All rights reserved.oi:10.1016/j.vaccine.2011.12.119
© 2012 Elsevier Ltd. All rights reserved.
to the introduction of the universal childhood program in 2005,serotypes included in the 7vPCV accounted for 84% of IPD in chil-dren aged <5 years in Australia [2]. In 2005, vaccination coveragewith 3 doses of 7vPCV for children in South Australia (SA) was 91%[3]. From 1 July 2011, a 13 valent pneumococcal conjugate vaccine(13vPCV) replaced the 7vPCV in the Australian universal childhoodprogram [4]. In addition, a nationally funded 23-valent pneumo-coccal polysaccharide vaccine (23vPPV) program has been availablesince 1999 for Aboriginal and Torres Strait Islander Australians aged≥50 years and for those aged 15–49 years with high risk condi-tions. Since the beginning of 2005, this has also been funded for allAustralians aged ≥65 years [5].
Most evidence for the effectiveness of childhood pneumococ-
cal vaccination comes from studies examining 7vPCV programswithin the United States where there has been a universal pro-gram in place for over 10 years. These data, from a number ofjurisdictions, consistently show substantial direct benefits through
ccine 30 (2012) 2206– 2211 2207
rbdnrlAopafie
morsmretSfiAs
IwoeS
2
2
mioifs
2
JedudtU
2
sttgt
Table 1Serotypes included in the 7vPCV, 13vPCV and 23vPPV.
Serotype 7vPCV 13vPCV 23vPPV
4√ √ √
6B√ √ √
9V√ √ √
14√ √ √
18C√ √ √
19F√ √ √
23F√ √ √
1√ √
3√ √
5√ √
6A√
7F√ √
19A√ √
2√
8√
9N√
10A√
11A√
12F√
15B√
17F√
20√√
D.R. Johnson et al. / Va
eduction in IPD rates in children aged <2 years [6–9]. Indirectenefits following universal childhood vaccination have also beenocumented in other age groups, most likely due to reducedasopharyngeal carriage of 7vPCV serotypes in children and henceeduced transmission to older unvaccinated populations. There isimited evidence documenting the effects of the 7vPCV program inustralia, with the most recent study evaluating national IPD datanly 2 years after the introduction of the universal childhood 7vPCVrogram [10]. This showed substantial direct benefits in childrenged <2 years as well as lesser, although still large, indirect benefitsor all other age groups. The only other published data availablen Australia are from two smaller regional studies where similarffects were observed [11,12].
Despite these benefits, there is evidence that serotype replace-ent following the commencement of 7vPCV programs is
ccurring. In the United States, continuing decreases in overall IPDates have been offset by increases in IPD caused by non-7vPCVerotypes in all age groups, although absolute increases remainodest overall [6]. Of particular concern, however, is the increased
ate of IPD caused by serotype 19A, a serotype exhibiting high lev-ls of antibiotic resistance [13]. These increases led to the decisiono replace the 7vPCV with the higher valency 13vPCV in the Unitedtates [14] and other jurisdictions such as the United Kingdom haveollowed suit [15]. Despite the recent incorporation of the 13vPCVnto the Australian childhood vaccination program, there is limitedustralian evidence regarding the effect of the 7vPCV program onerotype replacement.
Given the wealth of data generated for enhanced surveillance ofPD in Australia, further analysis is timely. The aims of this study
ere to: (1) document the impact of the 7vPCV program in the statef SA; (2) assess the degree of serotype replacement IPD; and (3) tostimate the benefit of incorporating the 13vPCV into the currentA childhood immunisation program.
. Methods
.1. Setting and participants
South Australia is a state of Australia with a population of 1.57illion (7% of the total Australian population) [16]. Cases of IPD
n the resident population of SA notified to the SA Departmentf Health between 1 January 2001 and 31 December 2009 werencluded in the study. A case of IPD was defined as the isolationrom, or the detection in, blood, cerebrospinal fluid (CSF) or otherterile site, of Streptococcus pneumoniae.
.2. Surveillance
IPD became a notifiable disease under legislation in SA on 1anuary 2001. This requires all laboratories and medical practition-rs to notify the SA Department of Health of each case of IPD. Basicemographic data is collected at notification and a case note reviewsing a standard enhanced surveillance form provides additionalata including risk factors for IPD, clinical presentation and vaccina-ion status. Isolates are also forwarded to the Melbourne Diagnosticnit for serotyping using the Quellung method.
.3. Analysis
Pneumococcal serotypes causing IPD were grouped by vaccineerotype coverage (see Table 1). The 13vPCV contains an addi-
ional six serotypes to the 7vPCV whilst the 23vPPV includes 12 ofhe 13vPCV serotypes plus an additional 11. Therefore the vaccineroupings were: (1) 7vPCV; (2) 13vPCV, including only the six addi-ional serotypes not contained in the 7vPCV; (3) 23vPPV, including22F33F
√
only the 11 additional serotypes not contained in 13vPCV. Addi-tional non-vaccine groupings included all serotypes not containedin the 13vPCV (non-13vPCV) and all serotypes not contained in the23vPPV (non-23vPPV).
Annual population estimates for SA were obtained from theAustralian Bureau of Statistics using 2001 and 2006 census data.To assess the effect of vaccination, Poisson regression was usedto calculate age-specific (analysis stratified by age) and serotypespecific incident rate ratios (IRRs) for notified IPD comparing pre(2002–2004) and post (2007–2009) universal childhood vaccina-tion periods. Data from 2001 was excluded to reduce ascertainmentbias given this was the first year of a new surveillance system. Inaddition, data from 2005 and 2006 were also excluded to allow forestablishment of the 7vPCV universal childhood program and tomore accurately assess indirect vaccine effects [17]. Further, Abo-riginal data was excluded from the analysis given that a funded7vPCV program began in 2001 for all Aboriginal and Torres Straitislander children and so the effectiveness of the vaccine tested forthis study would be underestimated. All analyses were performedin Stata version 11 (Stata Corp, TX, USA). The analysis focused onthe high risk groups for IPD, those aged <5 years and ≥65 years.
3. Results
Between January 2001 and December 2009, 1247 cases of IPD(693 males and 554 females) were notified to the SA Departmentof Health and serotype data were available for 1149 (92%) of cases.
3.1. Change in IPD rates
The annual rate of IPD for all ages began to fall from the first yearof the universal 7vPCV program in 2005 until 2007 but increasedagain in the final 2 years of the study (Fig. 1). Overall, there was a40% reduction in IPD rates for all ages (IRR 0.60, 95% CI, 0.52–0.68)(Table 2). There was a large 81% reduction in the incidence of IPDin children aged <2 years (IRR 0.19, 95% CI, 0.13–0.28), a large,
although less pronounced, 65% reduction in those aged 2–4 years(IRR 0.35, 95% CI, 0.21–0.57) and a smaller, although still significant,27% reduction in adults aged ≥ 65 years (IRR 0.73, 95% CI, 0.58–0.93)(Fig. 2 and Table 2). For adults aged ≥ 65 years, an initial decrease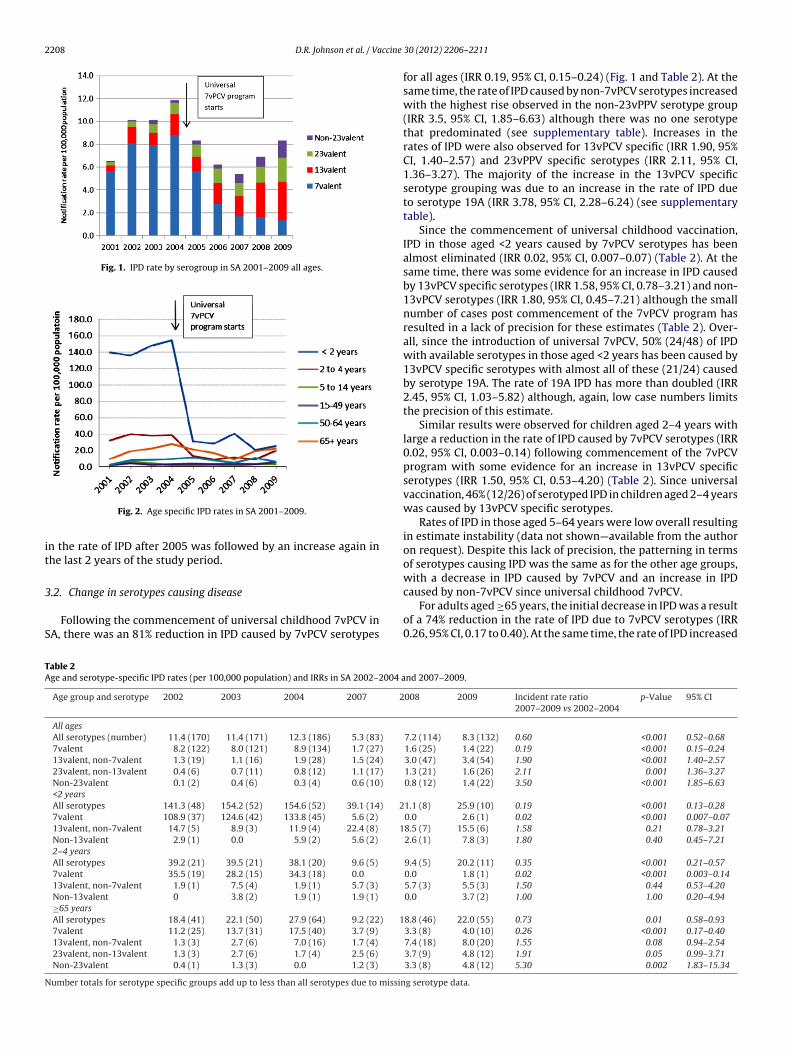
2208 D.R. Johnson et al. / Vaccine
Fig. 1. IPD rate by serogroup in SA 2001–2009 all ages.
it
3
S
caused by non-7vPCV since universal childhood 7vPCV.
TA
N
Fig. 2. Age specific IPD rates in SA 2001–2009.
n the rate of IPD after 2005 was followed by an increase again inhe last 2 years of the study period.
.2. Change in serotypes causing disease
Following the commencement of universal childhood 7vPCV inA, there was an 81% reduction in IPD caused by 7vPCV serotypes
able 2ge and serotype-specific IPD rates (per 100,000 population) and IRRs in SA 2002–2004 a
Age group and serotype 2002 2003 2004 2007 2
All agesAll serotypes (number) 11.4 (170) 11.4 (171) 12.3 (186) 5.3 (83)
7valent 8.2 (122) 8.0 (121) 8.9 (134) 1.7 (27)
13valent, non-7valent 1.3 (19) 1.1 (16) 1.9 (28) 1.5 (24)
23valent, non-13valent 0.4 (6) 0.7 (11) 0.8 (12) 1.1 (17)
Non-23valent 0.1 (2) 0.4 (6) 0.3 (4) 0.6 (10)
<2 yearsAll serotypes 141.3 (48) 154.2 (52) 154.6 (52) 39.1 (14) 27valent 108.9 (37) 124.6 (42) 133.8 (45) 5.6 (2)
13valent, non-7valent 14.7 (5) 8.9 (3) 11.9 (4) 22.4 (8) 1Non-13valent 2.9 (1) 0.0 5.9 (2) 5.6 (2)
2–4 yearsAll serotypes 39.2 (21) 39.5 (21) 38.1 (20) 9.6 (5)
7valent 35.5 (19) 28.2 (15) 34.3 (18) 0.0
13valent, non-7valent 1.9 (1) 7.5 (4) 1.9 (1) 5.7 (3)
Non-13valent 0 3.8 (2) 1.9 (1) 1.9 (1)
≥65 yearsAll serotypes 18.4 (41) 22.1 (50) 27.9 (64) 9.2 (22) 17valent 11.2 (25) 13.7 (31) 17.5 (40) 3.7 (9)
13valent, non-7valent 1.3 (3) 2.7 (6) 7.0 (16) 1.7 (4)
23valent, non-13valent 1.3 (3) 2.7 (6) 1.7 (4) 2.5 (6)
Non-23valent 0.4 (1) 1.3 (3) 0.0 1.2 (3)
umber totals for serotype specific groups add up to less than all serotypes due to missin
30 (2012) 2206– 2211
for all ages (IRR 0.19, 95% CI, 0.15–0.24) (Fig. 1 and Table 2). At thesame time, the rate of IPD caused by non-7vPCV serotypes increasedwith the highest rise observed in the non-23vPPV serotype group(IRR 3.5, 95% CI, 1.85–6.63) although there was no one serotypethat predominated (see supplementary table). Increases in therates of IPD were also observed for 13vPCV specific (IRR 1.90, 95%CI, 1.40–2.57) and 23vPPV specific serotypes (IRR 2.11, 95% CI,1.36–3.27). The majority of the increase in the 13vPCV specificserotype grouping was due to an increase in the rate of IPD dueto serotype 19A (IRR 3.78, 95% CI, 2.28–6.24) (see supplementarytable).
Since the commencement of universal childhood vaccination,IPD in those aged <2 years caused by 7vPCV serotypes has beenalmost eliminated (IRR 0.02, 95% CI, 0.007–0.07) (Table 2). At thesame time, there was some evidence for an increase in IPD causedby 13vPCV specific serotypes (IRR 1.58, 95% CI, 0.78–3.21) and non-13vPCV serotypes (IRR 1.80, 95% CI, 0.45–7.21) although the smallnumber of cases post commencement of the 7vPCV program hasresulted in a lack of precision for these estimates (Table 2). Over-all, since the introduction of universal 7vPCV, 50% (24/48) of IPDwith available serotypes in those aged <2 years has been caused by13vPCV specific serotypes with almost all of these (21/24) causedby serotype 19A. The rate of 19A IPD has more than doubled (IRR2.45, 95% CI, 1.03–5.82) although, again, low case numbers limitsthe precision of this estimate.
Similar results were observed for children aged 2–4 years withlarge a reduction in the rate of IPD caused by 7vPCV serotypes (IRR0.02, 95% CI, 0.003–0.14) following commencement of the 7vPCVprogram with some evidence for an increase in 13vPCV specificserotypes (IRR 1.50, 95% CI, 0.53–4.20) (Table 2). Since universalvaccination, 46% (12/26) of serotyped IPD in children aged 2–4 yearswas caused by 13vPCV specific serotypes.
Rates of IPD in those aged 5–64 years were low overall resultingin estimate instability (data not shown—available from the authoron request). Despite this lack of precision, the patterning in termsof serotypes causing IPD was the same as for the other age groups,with a decrease in IPD caused by 7vPCV and an increase in IPD
For adults aged ≥65 years, the initial decrease in IPD was a resultof a 74% reduction in the rate of IPD due to 7vPCV serotypes (IRR0.26, 95% CI, 0.17 to 0.40). At the same time, the rate of IPD increased
nd 2007–2009.
008 2009 Incident rate ratio2007–2009 vs 2002–2004
p-Value 95% CI
7.2 (114) 8.3 (132) 0.60 <0.001 0.52–0.681.6 (25) 1.4 (22) 0.19 <0.001 0.15–0.243.0 (47) 3.4 (54) 1.90 <0.001 1.40–2.571.3 (21) 1.6 (26) 2.11 0.001 1.36–3.270.8 (12) 1.4 (22) 3.50 <0.001 1.85–6.63
1.1 (8) 25.9 (10) 0.19 <0.001 0.13–0.280.0 2.6 (1) 0.02 <0.001 0.007–0.078.5 (7) 15.5 (6) 1.58 0.21 0.78–3.212.6 (1) 7.8 (3) 1.80 0.40 0.45–7.21
9.4 (5) 20.2 (11) 0.35 <0.001 0.21–0.570.0 1.8 (1) 0.02 <0.001 0.003–0.145.7 (3) 5.5 (3) 1.50 0.44 0.53–4.200.0 3.7 (2) 1.00 1.00 0.20–4.94
8.8 (46) 22.0 (55) 0.73 0.01 0.58–0.933.3 (8) 4.0 (10) 0.26 <0.001 0.17–0.407.4 (18) 8.0 (20) 1.55 0.08 0.94–2.543.7 (9) 4.8 (12) 1.91 0.05 0.99–3.713.3 (8) 4.8 (12) 5.30 0.002 1.83–15.34
g serotype data.

ccine
fsnssdCoww
4
htrgat
awamgiepaahufosh
<nurniificbaacpbbsbwfa[tt
t
D.R. Johnson et al. / Va
or 13vPCV specific serotypes (IRR 1.55, 95% CI, 0.94–2.54), 23vPPVpecific serotypes (IRR 1.91, 95% CI, 0.99–3.71) and particularlyon-23vPPV serotypes (IRR 5.30, 95% CI, 1.83–15.34). No oneerotype predominated in the non-23valent serotype group (seeupplementary table). Further, in adults aged ≥65 years, the inci-ence of IPD due to serotype 19A has almost tripled (IRR 2.92, 95%I, 1.17–7.31). Overall, in those aged ≥ 65 years, since the beginningf 2005, 32% (66/207) of IPD cases where the serotype was knownere caused by serotypes specific to the 13vPCV and 20% (42/207)ere caused by serotypes specific to the 23vPPV.
. Discussion
Since the introduction of universal childhood 7vPCV in SA, thereas been a large direct and sustained benefit in children, par-icularly those aged <2 years, with some evidence for serotypeeplacement. There is also good evidence that the childhood pro-ram has provided indirect benefits to adults aged ≥65 years,lthough it is likely that serotype replacement has begun to erodehe initial benefits.
Similar large direct benefits from 7vPCV programs for childrenged <2 years have been observed in the US and Canada whereell established, universally funded 7vPCV programs are delivered
nd where serotypes contained in the 7vPCV accounted for theajority of IPD prior to commencement of the vaccination pro-
ram [6–8,18]. Less impressive direct benefits have been observedn children in Europe [19–23], which may reflect lower 7vPCV cov-rage rates [19,22,23], lower rates of IPD caused by 7vPCV serotypesrior to 7vPCV commencement [24], differing clinical practice suchs thresholds for blood culture in febrile children or surveillancertefacts [17,25]. Large direct benefits for children aged <2 yearsave also been observed nationally in Australia after 2 years of theniversal 7vPCV program [10] and in Western Australia 3 yearsollowing the universal program [11]. Our study provides 5 yearsf data following the introduction of the 7vPCV program in SA andhows that the large reduction in IPD rates in children aged <2 yearsas been sustained.
The small increase in non-7vPCV serotypes in children aged2 years in this study is measured imprecisely due to small caseumbers and so could be the result of secular trends in individ-al serotypes. The most comprehensive data documenting serotypeeplacement is from the US and shows a significant 51% increase inon-7vPCV serotype IPD in children aged <5 years although this
ncrease remains modest when compared to the overall reductionn IPD following commencement of the 7vPCV program [6]. Datarom the England and Wales also provide evidence for substantialncreases in non-7vPCV in children aged <2 years since universalhildhood 7vPCV, although overall IPD rates have remained sta-le [26]. Results from other European jurisdictions also supportn increase in non-7vPCV following the 7vPCV vaccine program,lthough the effects on these studies are measured with low pre-ision. Importantly, however, since commencement of the 7vPCVrogram in SA, 50% of IPD in children aged <2 years has been causedy 13vPCV specific serotypes and almost all of these were causedy serotype 19A. Similar proportions of IPD caused by 13vPCVerotypes have been observed in the US with serotype 19A alsoeing responsible for the majority [6,27]. There is conjecture overhether the increase in serotype 19A is due to selection pressure
rom the 7vPCV program [28] as increases in serotype 19A havelso been observed in regions without universal 7vPCV programs29]. The large increase in the rate of serotype 19A, however, par-
icularly in the US, supports the role of vaccine pressure in drivinghis increase [6].For adults aged ≥65 years, our study provides some evidencehat the observed decrease in the rate of IPD is a result of an indirect
30 (2012) 2206– 2211 2209
benefit of the childhood 7vPCV program rather than an increaseduptake of 23vPPV as a result of the nationally funded programwhich commenced at the same time as the universal 7vPCV pro-gram. This is suggested by the large decrease in IPD caused by 7vPCVserotypes in those aged ≥65 years at the same time as increases inthe rate of IPD due to both 13vPCV and 23vPPV specific serotypes.Increases in IPD caused by the 16 serotypes included in the 23vPPVbut not the 7vPCV have previously been reported from the US [6]although these increases were modest in comparison to our data,possibly due to higher 23vPPV coverage rates in the US [30] com-pared to Australia [31,32]. Similar to our data, however, the largestproportion of IPD in those aged ≥65 years in the US is now causedby serotypes specific to the 13vPCV (41%) [6].
Similar indirect benefits for adults aged ≥65 years have also beenobserved in other Australian jurisdictions. The study by Lehmannet al. in Western Australia, observed a 50% reduction in IPD causedby 7vPCV serotypes but there was little evidence for increases innon-7vPCV serotypes [11]. This study only included data up until2007, which may not be sufficient time to detect serotype replace-ment IPD [17]. The other Australian study by Hanna et al. [12],including data up to 2009, also showed no evidence for an increasein non-7vPCV disease in this age group although the number ofstudy participants was small.
It is likely that the indirect benefits of the universal childhood7vPCV program in those aged ≥65 years are due to a reduction innasopharyngeal carriage of these serotypes in children and hencedecreased exposure of susceptible adults. At the same time, thereis evidence that an increase in colonisation of non-7vPCV serotypesin children has led to an increased exposure to these serotypes inadults [17,33–35].
A limitation of this study is the potential for ascertainment biasrelated to changes in the proportions of IPD cases serotyped duringthe study period. Data reported from England and Wales showeda marked increase in the proportion of IPD serotyped pre and postuniversal childhood 7vPCV (50–81%) which the authors correctedfor in their analysis [26]. For our study, however, there was onlya small increase in the proportion of IPD cases serotyped from91% prior to universal 7vPCV to 93% following and, as a result,this was not adjusted for in our analysis. Other potential ascertain-ment biases in our study related to changes in the testing practicesof doctors and/or laboratory diagnostic practices. In the five yearsprior to the introduction of universal childhood 7vPCV in Englandand Wales, increasing ascertainment of IPD as well as two otherinvasive bacterial diseases was detected. These were attributed topotential changes in blood culture practices or improved labora-tory practices and reporting efficiency [36], which was correctedfor in the analysis [26]. For our data, however, there was no con-sistent change in ascertainment for IPD across different age groupsprior to the introduction of the universal childhood 7vPCV. Further,in South Australia during the study period, there was no evidencefor an increase in ascertainment for other invasive bacterial infec-tions. Whilst ascertainment bias remains a potential limitation ofthis study, it was not possible to quantify this and hence correct forin our analysis.
A further limitation of this study is that vaccination status wasmeasured at a population level. Such an ecological approach can-not prove a cause and effect relationship between 7vPCV and bothdirect and indirect reductions in IPD rates. However, the main rea-son for taking such an approach was to examine the benefits ofthe childhood vaccination program at a population level, to cap-ture both direct and indirect benefits, something that an individuallevel analysis is not able to achieve. This approach can be justi-
fied by the high rate of childhood 7vPCV vaccination in SA from2005 (91%) [3]. Further, where individual level data was availablein this study for children aged <2 years, it revealed a vaccinationcoverage rate of 74% after commencement of the 7vPCV program
2 ccine
cio
7TiIot
it5f≥r
ATato[vs
A
oac
A
t
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
210 D.R. Johnson et al. / Va
ompared to a coverage rate of 2% prior to commencement, whichs high given that one would expect unvaccinated children to bever-represented in this dataset.
There may be factors other than the introduction of universalvPCV that have independently influenced IPD incidence over time.he pandemic H1N1 influenza outbreak in 2009 may have resultedn increased co-infection with pneumococcus and an increase inPD rates in 2009. In addition, smoking rates may have changedver time although it is unlikely that these would have influencedhe rate of IPD caused by some serotypes compared to others.
Our study provides evidence that incorporation of the 13vPCVnto the Australian universal childhood program has the potentialo decrease the rate of IPD in children aged <2 years in SA by up to0%. As well as direct benefits for children, there is also a potentialor indirect benefits for older age groups, particularly those aged65 years. Further, most of this benefit is likely to result from a
eduction in IPD caused by serotype 19A.It will be important to repeat this analysis at the national level in
ustralia to see if these findings are replicated in other jurisdictions.his study also highlights the importance of ongoing surveillancend vaccine development to keep up with the almost certain con-inued evolution of IPD serotypes. Looking to the future, the benefitsf offering conjugate vaccines to adults are currently being explored37] although, as many others have pointed out, the availability ofaccines that are not serotype specific offer the best solution toerotype replacement IPD.
cknowledgements
The authors acknowledge Graham Tucker from the Epidemiol-gy Branch of SA Health for providing statistical assistance duringnalysis of the results, and the journal reviewers for their usefulomments on the manuscript.
ppendix A. Supplementary data
Supplementary data associated with this article can be found, inhe online version, at doi:10.1016/j.vaccine.2011.12.119.
eferences
[1] Pneumococcal conjugate vaccine for childhood immunization—WHO positionpaper. Weekly epidemiological record/Health Section of the Secretariat of theLeague of Nations 2007; 82(12): 93–104.
[2] Watson M, Roche P, Bayley K, Bell JM, Collignon P, Gilbert GL, et al. Laboratorysurveillance of invasive pneumococcal disease in Australia: 2003 predicting thefuture impact of the universal childhood conjugate vaccine program. Commu-nicable Diseases Intelligence 2004;28(4):455–64.
[3] Menzies R, Turnour C, Chiu C, McIntyre P. Vaccine preventable diseasesand vaccination coverage in Aboriginal and Torres Strait Islander peo-ple, Australia 2003 to 2006. Communicable Diseases Intelligence 2008;32Suppl.
[4] Australian Government Department of Health and Ageing. ImmuniseAustralia Program: Pneumococcal disease; 2011. Available from: http://www.immunise.health.gov.au/internet/immunise/publishing.nsf/Content/immunise-pneumococcal.
[5] National Health and Medical Research Council. The Australian immunisationhandbook. 9th ed. Canberra: Australian Government Department of Health andAgeing; 2008.
[6] Pilishvili T, Lexau C, Farley MM, Hadler J, Harrison LH, Bennett NM, et al. Sus-tained reductions in invasive pneumococcal disease in the era of conjugatevaccine. Journal of Infectious Diseases 2010;201(1):32–41.
[7] Black S, France EK, Isaacman D, Bracken L, Lewis E, Hansen J, et al. Surveil-lance for invasive pneumococcal disease during 2000–2005 in a populationof children who received 7-valent pneumococcal conjugate vaccine. PediatricInfectious Disease Journal 2007;26(9):771–7.
[8] Bruce MG, Deeks SL, Zulz T, Bruden D, Navarro C, Lovgren M, et al.
International circumpolar surveillance system for invasive pneumo-coccal disease: 1999–2005. Emerging Infectious Diseases 2008;14(1):25–33.[9] Albrich WC, Baughman W, Schmotzer B, Farley MM. Changing characteris-tics of invasive pneumococcal disease in Metropolitan Atlanta: Georgia, after
[
30 (2012) 2206– 2211
introduction of a 7-valent pneumococcal conjugate vaccine. Clinical InfectiousDiseases 2007;44(12):1569–76.
10] Roche PW, Krause V, Cook H, Barralet J, Coleman D, Sweeny A, et al. Invasivepneumococcal disease in Australia: 2006. Communicable diseases intelligence2008;32(1):18–30.
11] Lehmann D, Willis J, Moore HC, Giele C, Murphy D, Keil AD, et al. TheChanging Epidemiology of Invasive Pneumococcal Disease in Aboriginal andNon-Aboriginal Western Australians from 1997 through 2007 and Emer-gence of Nonvaccine Serotypes. Clinical Infectious Diseases 2010;50(11):1477–86.
12] Hanna JN, Humphreys JL, Murphy DM, Smith HV. Invasive pneumococcal dis-ease in non-indigenous people in north Queensland: 2001–2009. MedicalJournal of Australia 2010;193(7):392–6.
13] Hsu K, Shea K, Stevenson A, Pelton SI. Changing serotypes causing child-hood invasive pneumococcal disease: Massachusetts, 2001–2007. The PediatricInfectious Disease Journal 2010;29(4):289–93.
14] Centers for Disease Control and Prevention. Licensure of a 13-valent pneu-mococcal conjugate vaccine (PCV13) and recommendations for use amongchildren—Advisory Committee on Immunization Practices (ACIP), 2010. Mor-bidity and Mortality Weekly Report 2010;59(9):258–61.
15] NHS. Factsheet, Pneumococcal conjugate vaccine (PCV) for children;2010. Available from: http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH 114349.
16] Australian Bureau of Statistics. 3210.0 population by age and sex, Aus-tralian states and territories; 2010. Available from: http://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/3201.0Jun%202010?OpenDocument.
17] Weinberger DM, Malley R, Lipsitch M. Serotype replacement in disease afterpneumococcal vaccination. The Lancet 2011.
18] Kellner James D, Vanderkooi OG, MacDonald J, Church DL, Tyrrell GJ,Scheifele DW. Changing Epidemiology of Invasive Pneumococcal Diseasein Canada, 1998–2007: update from the Calgary-Area Streptococcus pneu-moniae Research (CASPER) Study. Clinical Infectious Diseases 2009;49(2):205–12.
19] Ruckinger S, van der Linden M, Reinert RR, von Kries R, Burckhardt F, Siedler A.Reduction in the incidence of invasive pneumococcal disease after general vac-cination with 7-valent pneumococcal conjugate vaccine in Germany. Vaccine2009;27(31):4136–41.
20] Rodenburg GD, de Greeff SC, Jansen AGCS, de Melker HE, Schouls LM, Hak E,et al. Effects of pneumococcal conjugate vaccine 2 years after its introduction:the Netherlands. Emerging Infectious Diseases 2010;16(5):816–23.
21] Harboe ZB, Valentiner-Branth P, Benfield TL, Christensen JJ, Andersen PH,Howitz M, et al. Early effectiveness of heptavalent conjugate pneumococ-cal vaccination on invasive pneumococcal disease after the introductionin the Danish Childhood Immunization Programme. Vaccine 2010;28(14):2642–7.
22] Lepoutre A, Varon E, Georges S, Gutmann L, Lévy-Bruhl D. Impact of infantpneumococcal vaccination on invasive pneumococcal diseases in France,2001–2006. Euro Surveillance Bulletin 2008;13(35).
23] Aristegui J, Bernaola E, Pocheville I, García C, Arranz L, Durán G, et al. Reduc-tion in pediatric invasive pneumococcal disease in the Basque Country andNavarre: Spain, after introduction of the heptavalent pneumococcal conju-gate vaccine. European Journal of Clinical Microbiology and Infectious Diseases2007;26(5):303–10.
24] Farrell DJ, Jenkins SG, Reinert RR. Global distribution of Streptococcus pneu-moniae serotypes isolated from paediatric patients during 1999–2000 and thein vitro efficacy of telithromycin and comparators. Journal of Medical Microbi-ology 2004;53(11):1109–17.
25] Chiu C, Ridley G, Menzies R, McIntyre P. Update on childhood pneumococcalvaccination. Pediatric Health 2008;2(3):351–65.
26] Miller E, Andrews NJ, Waight PA, Slack MPE, George RC. Herd immunity andserotype replacement 4 years after seven-valent pneumococcal conjugate vac-cination in England and Wales: an observational cohort study. The LancetInfectious Diseases 2011;11(10):760–8.
27] Centers for Disease Control and Prevention. Invasive pneumococcal diseasein young children before licensure of 13-valent pneumococcal conju-gate vaccine—United States, 2007. Morbidity and Mortality Weekly Report2010;59(9):253–7.
28] Hicks LA, Harrison LH, Flannery B, Hadler JL, Schaffner W, Craig AS, et al. Inci-dence of pneumococcal disease due to non- pneumococcal conjugate vaccine(PCV7) serotypes in the United States during the era of widespread PCV7 vac-cination: 1998–2004. Journal of Infectious Diseases 2007;196(9):1346–54.
29] Choi EH, Kim SH, Eun BW, Kim SJ, Kim NH, Lee J, et al. Streptococcus pneu-moniae serotype 19A in Children: South Korea. Emerging Infectious Diseases2008;14(2):275–81.
30] Lindley MC, Euler GL, Shimabukuro T. Influenza and pneumococcal vaccinationcoverage among persons aged >65 years—United States: 2004–2005. Morbidityand Mortality Weekly Report 2006;55(39):1065–8.
31] Andrews RM. Assessment of vaccine coverage following the introduction ofa publicly funded pneumococcal vaccine program for the elderly in Victoria:Australia. Vaccine 2005;23(21):2756–61.
32] Australian Institute of Health and Welfare. 2004 adult vaccination survey: sum-mary results. AIHW cat. no. PHE 56. Canberra: AIHW & DoHA; 2005.
33] O’Brien KL, Millar EV, Zell ER, Bronsdon M, Weatherholtz R, Reid R, et al. Effectof pneumococcal conjugate vaccine on nasopharyngeal colonization amongimmunized and unimmunized children in a community-randomized trial. Jour-nal of Infectious Diseases 2007;196(8):1211–20.

ccine
[
[
[
D.R. Johnson et al. / Va
34] Ghaffar F, Barton T, Lozano J, Muniz LS, Hicks P, Gan V, et al. Effect of the 7-valent pneumococcal conjugate vaccine on nasopharyngeal colonization by
Streptococcus pneumoniae in the first 2 years of life. Clinical Infectious Diseases2004;39(7):930–8.35] Kayhty H, Auranen K, Nohynek H, Dagan R, Mäkelä H, Jokinen J, et al. Nasopha-ryngeal colonization: a target for pneumococcal vaccination. Expert Review ofVaccines 2006;5(5):651–67.
[
30 (2012) 2206– 2211 2211
36] Flasche S, Slack M, Miller E. Long term trends introduce a poten-tial bias when evaluating the impact of the pneumococcal conjugate
vaccination programme in England and Wales. Eurosurveillance 2011;16(20).37] Metersky ML, Dransfield MT, Jackson LA. Determining the optimal pneumo-coccal vaccination strategy for adults: is there a role for the pneumococcalconjugate vaccine? Chest 2010;138(3):486–90.





























