Embed Size (px)
Citation preview

PMB ReviewIntroductory remarks at Clinical Advisory
Committee meetings
August and September 2009
Boshoff Steenekamp
REF Project Specialist

Process to date
• PMB Review workshops early in 2008
• 3 drafts of a PMB review consultation document
• Numerous stakeholder submissions on these drafts

Essential healthcare
• Essential healthcare is made up of critical and relevant services that are: – necessary to preserve or improve the health of an
individual;
– scientifically sound, cost-effective, and of good quality;
– if not available, will result in death or serious morbidity; and
– delivered in a timely manner.

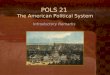
Number of individuals involved
Cla
ims
cost
per
ben
efic
iary
Few Many
Low
HighClaims cost per
beneficiary
Ab
ove
-th
resh
old
ben
efit
s fo
r al
l PM
Bs
Bel
ow
-th
resh
old
ben
efit
s fo
r sp
ecif
ied
se
rvic
es a
nd
co
nd
itio
ns
Hig
h c
ost
eve
nts
co
vere
d t
hro
ugh
PM
Bs
(mo
stly
in h
osp
ital
)
CD
L an
d o
ther
co
nd
itio
ns
on
cat
ego
rica
l lis
t
Spec
ifie
dse
rvic
es
Day-to-day expenses on an out-of-pocket basis or paid from MSA
EDL

Frequently raised matters
• EDL inappropriate in current environment– The intention of the EDL list is not to limit medicine
use to drugs on this list, but simply to state that any of the drugs on the list must be covered from first Rand
• Exclusions: Annexure I– The intention is that these conditions should be
excluded within the specified setting, not a general exclusion
• Challenges– Constitutional rights, mandate of DoH & Council

Concurrent Processes impacting on revised PMB regulations
Number of individuals involved
Cla
ims
cost
per
ben
efic
iary
Few Many
Low
HighClaims cost per
beneficiary
Ab
ove
-th
resh
old
ben
efit
s fo
r al
l PM
Bs
Bel
ow
-th
resh
old
ben
efit
s fo
r sp
ecif
ied
se
rvic
es a
nd
co
nd
itio
ns
Hig
h c
ost
eve
nts
co
vere
d t
hro
ugh
PM
Bs
(mo
stly
in h
osp
ital
)
CD
L an
d o
ther
co
nd
itio
ns
on
cat
ego
rica
l lis
t
Spec
ifie
dse
rvic
es
Day-to-day expenses on an out-of-pocket basis or paid from MSA
Proposed Essential Care Package
NHI Process
Technical analysis of economic
impact, affordability
pricing, construct,
related reforms
Clinical Advisory
committees
Drafting of Regulations
Stakeholder comments

Governance Structure
STEERING
COMMITTEE
PROJECT
MANAGER
HEALTHCARE
INTERVENTIONSREF PRICING
Participative
Co
nsu
ltat
ive

Sources for consideration
• Existing PMB regulations
• Third draft of the PMB review consultation document
• Stakeholder comments on the consultation document relevant to the specific advisory committee
• Final submissions by committee members to the committee

Terms of reference
I. BackgroundII. Policy FrameworkIII. Composition of clinical advisory committees (CACs)IV. Criteria for evaluating a recommendationV. Role of the ChairVI. Code of conduct for CAC membersVII.Logistics
Annexure A: Clinical Advisory Committee agenda items, meeting dates, and relevant comments on the PMB review consultation documents

IV. Criteria for evaluating a recommendation
Submitted recommendations must comply with the principles of evidence-based medicine decision making and therefore it is crucial that sufficiently detailed information on how the evidence was obtained is provided. In addition, the criteria outlined below should be adhered to:
1. Clinical effectiveness2. Degree of discretion3. Urgency4. Cost-effectiveness/ economic evaluation5. The health benefits of the recommendation should be compared
with the next best available alternative treatment. If possible a balance sheet of the benefits, harms and major costs of recommendation should be itemised against those of the available alternative

Degree of discretion
Apply principles Apply principles Apply principles
Apply principles Apply principles Exclusion
Exclusion Exclusion Exclusion
Discretion
Med
ical
nec
essi
ty
Low Medium High
Low
Medium
High

The health benefits
• The health benefits of the recommendation should be compared with the next best available alternative treatment. If possible a balance sheet of the benefits, harms and major costs of recommendation should be itemised against those of the available alternative

Cost weight of the top six REF risk factors, December 2008
NON 51%
MAT 8%
HYP 7%
DM2 5%
HYL 4%
IHD 3%
HIV 3%
Other19%

CDL groups
Lifestyle diseases HYP, IHD, HYL, DM2
Other cardiac CMY, CHF, DYS
Multiple chronic diseases CC2, CC3, CC4
Psychiatric BMD, SCZ
Renal CRF
Respiratory AST, COP, BCE
Endocrine DM1, TDH, ADS, DBI
Neurologic EPL, MSS
Autoimmune RHA, SLE, CSD, IBD
Other HAE, PAR, GLC

Total REF risk factor cost load by CDL groupDecember 2008
0
100,000
200,000
300,000
400,000
500,000
600,000
700,000
800,000
R 0
R 20,000,000
R 40,000,000
R 60,000,000
R 80,000,000
R 100,000,000
R 120,000,000
R 140,000,000
R 160,000,000
R 180,000,000
R 200,000,000
Un
de
r 1
1-4
5-9
10
-14
15
-19
20
-24
25
-29
30
-34
35
-39
40
-44
45
-49
50
-54
55
-59
60
-64
65
-69
70
-74
75
-79
80
-84
85
+
NON Lifestyle diseases MAT Multiple chronic diseases
Other cardiac Respiratory HIV Endocrine
Renal Neurologic Psychiatric Other
Autoimmune Population

Cost pbpm of the REF risk factors by age and CDL groupDecember 2008
R 0
R 200
R 400
R 600
R 800
R 1,000
R 1,200
Un
de
r 1
1-4
5-9
10
-14
15
-19
20
-24
25
-29
30
-34
35
-39
40
-44
45
-49
50
-54
55
-59
60
-64
65
-69
70
-74
75
-79
80
-84
85
+
Axi
s Ti
tle
NON Lifestyle diseases MAT Multiple chronic diseases Other cardiac
Respiratory HIV Endocrine Renal Neurologic
Psychiatric Other Autoimmune

Cost pbpm of the REF risk factors by age and CDL groupDecember 2008
0
100,000
200,000
300,000
400,000
500,000
600,000
700,000
800,000
R 0
R 200
R 400
R 600
R 800
R 1,000
R 1,200
Un
de
r 1
1-4
5-9
10
-14
15
-19
20
-24
25
-29
30
-34
35
-39
40
-44
45
-49
50
-54
55
-59
60
-64
65
-69
70
-74
75
-79
80
-84
85
+
Axi
s Ti
tle
NON Lifestyle diseases MAT Multiple chronic diseases
Other cardiac Respiratory HIV Endocrine
Renal Neurologic Psychiatric Other
Autoimmune Population

Cost pbpm of the REF risk factors by age and CDL groupDecember 2008
0
100,000
200,000
300,000
400,000
500,000
600,000
700,000
800,000
R 0
R 200
R 400
R 600
R 800
R 1,000
R 1,200
Un
de
r 1
1-4
5-9
10
-14
15
-19
20
-24
25
-29
30
-34
35
-39
40
-44
45
-49
50
-54
55
-59
60
-64
65
-69
70
-74
75
-79
80
-84
85
+
Axi
s Ti
tle
NON Lifestyle diseases MAT Multiple chronic diseases
Other cardiac Respiratory HIV Endocrine
Renal Neurologic Psychiatric Other
Autoimmune ICR Population

V. Role of the Chair
The Chair of each of the CACs will be appointed by the Steering committee and will be briefed by the project manager on the scope of the project.The chair will:
1. Guide the task of developing final recommendations and the process thereof.
2. Assist the team to work collaboratively and effectively together ensuring that there is balanced contribution from all members.
3. Steer the discussion according to the agenda4. Summarise the main points and key decisions from the debate,
noting any points of disagreement.5. Sign off minutes compiled the secretariat.

VII. Logistics
1.Committee members must review the comments made by other stakeholders as listed in Annexure A and submit their final proposals at least seven days prior to the scheduled meeting.
2.The chairperson of each advisory committee must make final recommendations to the PMB Review Steering Committee by 29 September 2009.

Purpose of today’s meeting
• Consider the respective agenda items in view of
– Existing regulations
– Proposals made in the 3rd draft of the PMB review document
– Stakeholder comments on the 3rd draft
– Final submissions must be introduced by committee members
• No time for additional presentations or the introduction of new items

Summary of Oncology DTPs
Code Diagnosis Treatment
950A Benign and malignant brain tumours,
treatable
Medical and surgical management which
includes radiation therapy and chemotherapy
950B Cancer of the eye and orbit - treatable Medical and surgical management, which
includes radiation therapy and chemotherapy
950C Cancer of oral cavity, pharynx, nose, ear,
and larynx - treatable
Medical and surgical management, which
includes chemotherapy and radiation therapy
950D Cancer of lung, bronchus, pleura,
trachea, mediastinum &
other respiratory organs - treatable
Medical and surgical management, which
includes chemotherapy and radiation therapy
952F Cancer of retroperitoneum, peritoneum,
omentum & mesentery - treatable
Medical and surgical management, which
includes chemotherapy and radiation therapy
950C Cancer of the gastro-intestinal tract,
including oesophagus, stomach, bowel,
rectum, anus - treatable
Medical and surgical management, which
includes chemotherapy and radiation therapy
950G Cancer of liver, biliary system and
pancreas – treatable
Medical and surgical management
950H Cancer of bones - treatable Medical and surgical management, which
includes chemotherapy and radiation therapy

950J Cancer of breast - treatable Medical and surgical management, which
includes chemotherapy and radiation
therapy
954J Cancer of skin, excluding malignant
melanoma - treatable
If histologically confirmed, Medical and
surgical management, which includes
radiation therapy
952J Cancer of soft tissue, including
sarcomas and malignancies of the
adnexa - treatable
Medical and surgical management, which
includes chemotherapy and radiation
therapy
953J Malignant melanoma of skin - treatable Medical and surgical management, which
includes radiation therapy
950K Cancer of endocrine system, excluding
thyroid - treatable
Medical and surgical management, which
includes chemotherapy and radiation
therapy
952K Cancer of thyroid - treatable; carcinoid
syndrome
Medical and surgical management, which
includes chemotherapy and radiation
therapy
954L Cancer of penis and other male genital
organ - treatable
Medical and surgical management, which
includes chemotherapy and radiation
therapy
953L Cancer of prostate gland - treatable Medical and surgical management, which
includes chemotherapy and radiation
therapy

950L Cancer of testis - treatable Medical and surgical management, which
includes chemotherapy and radiation therapy
952L Cancer of urinary system including
kidney and bladder -
treatable
Medical and surgical management, which
includes chemotherapy and radiation therapy
954M Cancer of cervix - treatable Medical and surgical management, which
includes chemotherapy and radiation therapy
952M Cancer of ovary - treatable Medical and surgical management, which
includes chemotherapy and radiation therapy
950M Cancer of uterus - treatable Medical and surgical management, which
includes chemotherapy and radiation therapy
953M Cancer of vagina, vulva and other
female genital organs NOS -
treatable
Medical and surgical management, which
includes chemotherapy and radiation therapy
901S Acute leukemias, lymphomas Medical management, which includes
chemotherapy, radiation therapy, bone
marrow transplantation
910S Multiple myeloma and chronic
leukaemias
Medical management which includes
chemotherapy and radiation therapy




Structure of today’s meeting
• Introduction – CMS / DoH
• Agenda items
– Regulations, Third draft proposals, Submissions & Summaries
• Lunch
• Attendance list

THANK YOU