Embed Size (px)
Citation preview
Sponsored by
AAGLAdvancing Minimally Invasive Gynecology Worldwide
Plenary 3: Hysteroscopy
DISCUSSANTS
MODERATORS
Aarthi Cholkeri-Singh, MD Stephanie N. Morris, MD
Jorge Dotto, MDKirsten Sasaki, MD
Marit Lieng, MD, PhDGeorge A. Vilos, MD
Philip G. Brooks, MD Donald L. Chatman, MD Richard J. Gimpelson, MD
Attilio Di Spiezio Sardo, MD, PhDChandrew Rajakumar, MD
Tarek Shokeir, MD
Ayman Oraif, MDCrystal M. Santiago, MDMichael W.H. Suen, MD

Professional Education Information Target Audience This educational activity is developed to meet the needs of residents, fellows and new minimally invasive specialists in the field of gynecology. Accreditation AAGL is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. The AAGL designates this live activity for a maximum of 1.0 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. DISCLOSURE OF RELEVANT FINANCIAL RELATIONSHIPS As a provider accredited by the Accreditation Council for Continuing Medical Education, AAGL must ensure balance, independence, and objectivity in all CME activities to promote improvements in health care and not proprietary interests of a commercial interest. The provider controls all decisions related to identification of CME needs, determination of educational objectives, selection and presentation of content, selection of all persons and organizations that will be in a position to control the content, selection of educational methods, and evaluation of the activity. Course chairs, planning committee members, presenters, authors, moderators, panel members, and others in a position to control the content of this activity are required to disclose relevant financial relationships with commercial interests related to the subject matter of this educational activity. Learners are able to assess the potential for commercial bias in information when complete disclosure, resolution of conflicts of interest, and acknowledgment of commercial support are provided prior to the activity. Informed learners are the final safeguards in assuring that a CME activity is independent from commercial support. We believe this mechanism contributes to the transparency and accountability of CME.

Table of Contents
Course Description ........................................................................................................................................ 1 Disclosure ...................................................................................................................................................... 2 A Single Injection of Depomedroxyprogesterone Acetate (Dmpa) Immediately After Rollerball Endometrial Ablation Significantly Improves Clinical Outcomes in Women With Heavy Menstrual Bleeding Ayman Oraif .................................................................................................................................................. 4 Accuracy of Hysteroscopic Metroplasty With the Combination of Pre Surgical Three‐Dimensional Ultrasonography and a Novel Graduated Intrauterine Palpator: A Randomized Controlled Trial Attilio Di Spiezio Sardo .................................................................................................................................. 7 Complications and Compliance of Hysteroscopic Sterilization With Essure in an Inner City Hospital Crystal M. Santiago ..................................................................................................................................... 10 Hysteroscopic Metroplasty in Women With Unexplained Primary Infertility: A Prospective Cohort Study Tarek Shokeir .............................................................................................................................................. 12 Hysteroscopic Management of a Stenotic Cervix Michael W.H. Suen ...................................................................................................................................... 15 Hysteroscopic Removal of Retained Placental Tissue Allieviates Postpartum Hypertension Chandrew Rajakumar .................................................................................................................................. 16 Cultural and Linguistics Competency ......................................................................................................... 17
Plenary 3: Hysteroscopy
Moderators: Philip G. Brooks, Donald L. Chatman, Richard J. Gimpelson
Discussants: Aarathi Cholkeri-Singh, Jorge Dotto, Marit Lieng, Stephanie N. Morris, Kristen Sasaki, George A. Vilos
Faculty: Attilio Di Spiezio Sardo, Ayman Oraif, Chandrew Rajakumar,
Crystal M. Santiago, Tarek Shokeir, Michael W.H. Suen This session provides a group of advanced hysteroscopic techniques dealing with uterine anomalies and acquired abnormalities, along with several recommendations to make hysteroscopic procedures more effective. Learning Objectives: At the conclusion of this course, the clinician will be able to: 1) Describe advanced indications; and 2) discuss additional surgical techniques to improve outcomes of hysteroscopic surgery.
Course Outline 2:15 A Single Injection of Depomedroxyprogesterone Acetate (Dmpa) Immediately
After Rollerball Endometrial Ablation Significantly Improves Clinical Outcomes in Women With Heavy Menstrual Bleeding A. Oraif
2:21 Discussant A. Cholkeri-Singh
2:25 Accuracy of Hysteroscopic Metroplasty With the Combination of Pre-Surgical Three-Dimensional Ultrasonography and a Novel Graduated Intrauterine Palpator: A Randomized Controlled Trial A. Di Spiezio Sardo
2:31 Discussant K. Sasaki
2:35 Complications and Compliance of Hysteroscopic Sterilization With Essure in an Inner City Hospital C.M. Santiago
2:41 Discussant M. Lieng
2:45 Hysteroscopic Metroplasty in Women With Unexplained Primary Infertility: A Prospective Cohort Study T. Shokeir
2:51 Discussant G.A. Vilos
2:55 Video: Hysteroscopic Management of a Stenotic Cervix M.W.H. Suen
3:01 Discussant S.N. Morris
3:05 Video: Hysteroscopic Removal of Retained Placental Tissue Allieviates Postpartum Hypertension C. Rajakumar
3:11 Discussant J. Dotto
3:15 Adjourn
1

PLANNER DISCLOSURE The following members of AAGL have been involved in the educational planning of this workshop and have no conflict of interest to disclose (in alphabetical order by last name). Art Arellano, Professional Education Manager, AAGL* Amber Bradshaw Speakers Bureau: Myriad Genetics Lab Other: Proctor: Intuitive Surgical Erica Dun* Frank D. Loffer, Medical Director, AAGL* Linda Michels, Executive Director, AAGL* Johnny Yi* SCIENTIFIC PROGRAM COMMITTEE Arnold P. Advincula Consultant: Intuitive Royalty: CooperSurgical Sarah L. Cohen* Jon I. Einarsson* Stuart Hart Consultant: Covidien Speakers Bureau: Boston Scientific, Covidien Kimberly A. Kho Contracted/Research: Applied Medical Other: Pivotal Protocol Advisor: Actamax Matthew T. Siedhoff Other: Payment for Training Sales Representatives: Teleflex M. Jonathon Solnik Consultant: Z Microsystems Other: Faculty for PACE Surgical Courses: Covidien FACULTY DISCLOSURE The following have agreed to provide verbal disclosure of their relationships prior to their presentations. They have also agreed to support their presentations and clinical recommendations with the “best available evidence” from medical literature (in alphabetical order by last name). Philip G. Brooks* Donald L. Chatman* Aarathi Cholkeri-‐Singh Speakers Bureau: Bayer Healthcare Corp., Ethicon Endo-‐Surgery Other: Advisory Board Member: Bayer Healthcare Corp., Ethicon Endo-‐Surgery Consultant: Smith & Nephew Endoscopy Attilio Di Spiezio Sardo Consultant: Bayer Healthcare Corp., Johnson & Johnson, Karl Storz Jorge Dotto* Richard J. Gimpelson Contracted Research: Minerva Surgical Royalty: CooperSurgical, Inc., Halt Medical Other: Advisory Board: Boston Scientific Corp. Inc. Other: Clinical Events Committee: Halt Medical Other: Scientific Advisory Board: Mirabilis Medica Marit Lieng*
2
Stephanie N. Morris* Ayman Oraif* Chandrew Rajakumar* Crystal M. Santiago* Kirsten J. Sasaki* Tarek Shokeir* Michael W.H. Suen* George A. Vilos* Asterisk (*) denotes no financial relationships to disclose.
3

A Single Injection of DepomedroxyprogesteroneAcetate (Dmpa) Immediately After Rollerball Endometrial Ablation Significantly Improves Clinical Outcomes in Women With Heavy Menstrual
Bleeding
Ayman Oraif, MD,FRCSC
The Fertility Clinic, LHSC, Department of Obstetrics and Gynecology, Western University, London, Canada
Department of Obstetrics and Gynecology, King Abdulaziz University, Jeddah, Saudi Arabia
Disclosure
I have no financial relationships to disclose.
Objective:
Discuss clinical outcomes of DMPA in women with heavy
menstrual bleeding
Background
• First generation endometrial ablation techniques (FEATs) were introduced in the 1980’s as an alternative to hysterectomy to treat women with abnormal uterine bleeding from benign causes.
• These included endometrial laser ablation and radiofrequency rollerball/bar or transcervical resection of the endometrium (TCRE).
Papadopoulos NP, Magos A (2007) First‐generation endometrial ablation: roller‐ball vs loop vs laser. Best Pract Res Clin Obstet Gynaecol 21:915–929
ACOG Practice Bulletin No. 81, May 2007: endometrial ablation. Obstet Gynecol 109(5):1233‐48
Background
• Second generation endometrial ablation technologies (SEATs), also referred to as global endometrial ablation (GEA) or non‐hysteroscopic endometrial ablation (non‐HEA), were introduced in the 1990’s as automated, easier, and safer alternatives to hysteroscopic endometrial ablation requiring less skill and could be performed in the office.
Garry R, for the Endometrial Ablation Group (2002) Evidence and techniques in endometrial ablation: consensus. 2002. Gynecol Endosc 11(1):5–17
Madhu CK, Nattey J, Naeem T (2009) Second generation endometrial ablation techniques: an audit of clinical practice. Arch Gynecol Obstet 280:599–602
Problem with the FEATs & SEATs
•Following endometrial ablation by any technique, long‐term outcomes (within 10 years) indicate that 15 to 30 % of women require additional surgery such as hysterectomy for persistent AUB, uterine/pelvic pain, or both.
•The subsequent 30 % hysterectomy rate after endometrial ablation together with a high satisfaction rate of women who chose hysterectomy as 1ry treatment of their AUB has raised some serious issues and concerns regarding the cost‐effectiveness, ongoing utilization, and indeed the future of both hysteroscopic (HEA) and non‐hysteroscopicendometrial ablation (NHEA) for the treatment of AUB.
Munro MG (2006) Endometrial ablation. Where have we been? Where are we going? Clin Obstet Gynecol 49(4):736–766
Longinotti MK, Jacobson GF, Hung YY, Learman LA (2008) Probability of hysterectomy after endometrial ablation. Obstet Gynecol112(6):1214–1220
Bhattacharya S, Middleton LJ, Tsourapas A et al (2011) Hysterectomy, endometrial ablation and Mirena® for heavy menstrual bleeding: a systematic review of clinical effectiveness and cost‐effectiveness analysis. Health Technol Assess 15(19):iii–xvi, 1‐252
4

Solutions to FEATs & SEATs1. Go back to hysterectomy
• Many gynecologists resort to hysterectomy for both as primary treatment of AUB and as the next logical step in women who fail primary endometrial ablation.Zupi E, Centini G, Lazzeri L, et al. HEA v. LSH for AUB:Long‐term follow up of an RCT. JMIG 2015;22:841‐5
•However, in spite of major technological advances in minimally invasive gynecological surgery, hysterectomy remains a major surgical procedure associated with significant morbidity, mortality, and health care costs and resources.
Wright JD, Devine P, Shah M et al (2010) Morbidity and mortality of peripartum hysterectomy. Obstet gynecol115:1187–1193
Boyd LR, Novesky AP, Curtin JP (2010) Effect of surgical volume on route of hysterectomy and short‐term morbidity. Obstet Gynecol 116:909–915
Roberts TE, Tsourapas A, Middleton LJ et al (2011) Hysterectomy, endometrial ablation, and levonorgestrelreleasing intrauterine system (Mirena) for treatment of heavy menstrual bleeding: cost effectiveness analysis. BMJ 342:d2202. doi:10.1136/bmj.d2202
Clark‐Pearson DL, Geller EL (2013) Complications of hysterectomy. Clin Exp Ser Obstet Gynecol 121:654–673
Potential Savior to FEATs & SEATs2. Use adjunct Therapy
• 1990 Townsend et al: 400 mg medroxyprogesterone given post‐rollerball ablation –amenorrhea rates at 6‐12 months were 100% (25/25) vs. 40% (10/25) in study group and control group, respectively
•1994 Jacobs and Blumenthal: injection of150 mg DMPA post‐TCRE ‐ amenorrhea rates at 6, 12 and >12 months were 66.7%, 59.3% and 55.6% compared to 34.4%, 31.3% and 26.1% in the DMPA group and control group, respectively
•1995 Goldrath: injection of 150 mg DMPA after hysteroscopic endometrial photocoagulation with the Nd:YAG laser fiber ‐amenorrhea rates at >6 months post‐ablation were 69% vs. 37% in the DMPA group and control group, respectively
Objective: Adjunct Therapy
To determine patient satisfaction and the clinical effectiveness of a single dose of Depo Medroxyprogesterone Acetate (DMPA) injection immediately after rollerball endometrial ablation (REA) in women with heavy menstrual bleeding (HMB).
Proposed Mechanism of Action of DMPA
• Progesterone down regulates estrogen receptors
• When progesterone is given in the form of DMPA injection, its effect lasts 3 months
• By decreasing/eliminating the influence of estrogen on any residual endometrium through receptor down‐regulation for 3 months, any residual/non‐ablated endometrium may atrophy/die or scar down before unopposed estrogen can revitalize it.
Materials and Methods
• 83 women received a single dose of DMPA 150 mg, IM, immediately after REA.
• Inclusion criteria: Women receiving REA for HMB with a normal uterine cavity and normal endometrial biopsy pre‐operatively.
• Endometrium was ablated using a 26F (9 mm) resectoscope with a 5 mm rollerball, 1.5% glycine and 120 w of power.
• Outcomes were compared with a historical control group (n=47) who had REA only.
Baseline Characteristics
REA + DMPA REA Only
Age 42.6 (25‐55) 40.7
Parity 2.1 (0‐6) 1.9
BMI 27.2 (19‐45) 27.7
5
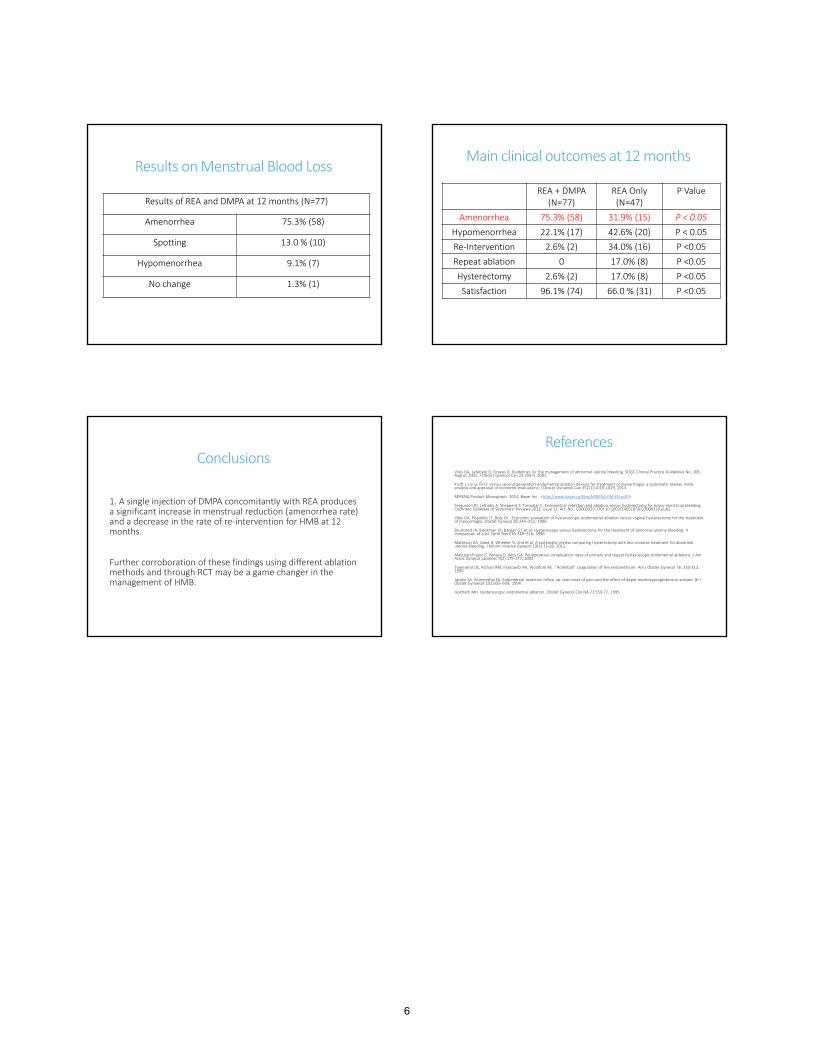
Results on Menstrual Blood Loss
Results of REA and DMPA at 12 months (N=77)
Amenorrhea 75.3% (58)
Spotting 13.0 % (10)
Hypomenorrhea 9.1% (7)
No change 1.3% (1)
Main clinical outcomes at 12 months
REA + DMPA(N=77)
REA Only (N=47)
P Value
Amenorrhea 75.3% (58) 31.9% (15) P < 0.05
Hypomenorrhea 22.1% (17) 42.6% (20) P < 0.05
Re‐Intervention 2.6% (2) 34.0% (16) P <0.05
Repeat ablation 0 17.0% (8) P <0.05
Hysterectomy 2.6% (2) 17.0% (8) P <0.05
Satisfaction 96.1% (74) 66.0 % (31) P <0.05
Conclusions
1. A single injection of DMPA concomitantly with REA produces a significant increase in menstrual reduction (amenorrhea rate) and a decrease in the rate of re‐intervention for HMB at 12 months.
Further corroboration of these findings using different ablation methods and through RCT may be a game changer in the management of HMB.
References
Vilos GA, Lefebvre G, Graves G. Guidelines for the management of abnormal uterine bleeding. SOGC Clinical Practice Guidelines No. 106, August 2001. J Obstet Gynecol Can 23:704‐9, 2001.
Kroft J, Liu G. First‐ versus second‐generation endometrial ablation devices for treatment of menorrhagia: a systematic review, meta‐analysis and appraisal of economic evaluations. J Obstet Gynaecol Can 35(11):1010‐1019, 2013.
MIRENA Product Monograph. 2014, Bayer Inc.<http://www.bayer.ca/files/MIRENA‐PM‐EN.pdf?>
Fergusson RJ, Lethaby A, Shepperd S, Farquhar C. Endometrial resection and ablation versus hysterectomy for heavy menstrual bleeding. Cochrane Database of Systematic Reviews 2013, Issue 11. Art. No.: CD000329. DOI:10.1002/14651858.CD000329.pub2.
Vilos GA, Pispidikis JT, Botz CK.: Economic evaluation of hysteroscopic endometrial ablation versus vaginal hysterectomy for the treatment of menorrhagia. Obstet Gynecol 85:244–252, 1996.
Brumsted JR, Blackman JA, Badger GJ, et al: Hysteroscopy versus hysterectomy for the treatment of abnormal uterine bleeding: A comparison of cost. Fertil Steril 65:310–316, 1996.
Matteson KA, Abed H, Wheeler TL 2nd et al. A systematic review comparing hysterectomy with less‐invasive treatment for abnormal uterine bleeding. J Minim Invasive Gynecol 19(1):13‐28, 2012.
MacLean‐Fraser E, Penava D, Vilos GA. Perioperative complication rates of primary and repeat hysteroscopic endometrial ablations. J Am Assoc Gynecol Laparosc 9(2):175‐177, 2002.
Townsend DE, Richart RM, Paskowitz RA, Woolfork RE. “ Rollerball” coagulation of the endometrium. Am J Obstet Gynecol 76: 310‐313, 1990.
Jacobs SA, Blumenthal NJ. Endometrial resection follow up: late onset of pain and the effect of depot medroxyprogesterone acetate. Br J Obstet Gynaecol 101:605–609, 1994.
Goldrath MH. Hysteroscopic endometrial ablation. Obstet Gynecol Clin NA 22:559‐72, 1995.
6

Accuracy of hysteroscopic metroplasty with the combination of pre‐surgical three‐dimensional
ultrasonography and a novel graduated intrauterine palpator: A randomized controlled trial
Attilio Di Spiezio Sardo, MD, PhD
University of Naples “Federico II”Italy
• Consultant:
• Bayer Healthcare Corp.,
• Johnson & Johnson,
• Karl Storz
• Discuss the accuracy of hysteroscopicmetroplasty
METROPLASTY
American FertilitySociety (AFS), 1988
Classification of female genital
tract congenital anomalies
z
y
7

Pre‐surgical three‐dimensional transvaginal ultrasonography
(3D‐TVS)
5 Fr graduated intrauterine palpator
POSSIBILITY TO MEASURETHE DEPTH OF SECTION
ACCURACY OF METROPLASTY
Depth of the septum
fundus thickness
ACCURACY OF METROPLASTY
II SURGICAL TIMEFundal Notch: 1cm
Optimal (residual septum
≤ 5 mm)Suboptimal
(residual septumbetween 5 and 10mm)
Incomplete (residual septum >
10 mm)
90
GROUP TN: 45
PRE- SURGICAL ASSESSMENTOF UTERINE CAVITY
HSC 3D- TVS
GROUP CN: 45
POST- SURGICAL ASSESSMENTOF UTERINE
CAVITY
3D- TVS
MATERIALS AND METHODS
HSC
KEY POINTS
• Begin at the apex• Latero-lateral direction• Resection with 5 Fr
bipolar electrode in pulsed mode
• Finishing touch of the base of septum with 5Fr scissors
Metroplasty with miniature instruments
GROUP C
Depth of the septum
fundus thickness
GROUP TRESULTS (1)
GROUP T GROUP C RR 95% CI p
Optimal 32 (71.5%) 19 (41.2%) 1.684 1.116‐2.506 0.006
Suboptimal 13 (28.5%) 14 (31.1%) 0.929 0.457‐1.874 1.0
Incomplete 0 12 ( 26.7%) 0 0‐0.392 <0.0001
8

RESULTS (2)
OPTIMAL
INCOMPLETE
RESULTS (3)
CONCLUSIONS
Pre-surgical assessment Intraoperative (objective)data
Graduate intrauterine palpator
ONE SURGICAL STEP
3D‐ TVS
Grimbizis GF, Gordts S, Di Spiezio Sardo A, et al. The ESHRE/ESGE consensus on the classification of female
genital tract congenital anomalies. Human Reproduction 2013; 28: 2032–2044.
Francisco Raga, Celia Bauset, Jose Remohi, et al. Reproductive impact of congenital Mullerian anomalies.
Human Reproduction 1997; 112: 2277–2281
Venetis CA, Papadopoulos SP, Campo R, et al. Clinical implications of congenital uterine anomalies: a meta‐analysis of comparative studies. Reprod Biomed Online 2014; 29(6): 665‐83.
American Fertility Society. The AFS classification of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, Mullerian anomalies and intrauterine adhesions. Fertil Steril 1988; 49: 944‐955.
Fedele L, Arcaini L, Parazzini F, et al. Reproductive prognosis after hysteroscopic metroplasty in 102 women: life‐table analysis. Fertil Steril 1993; 59(4): 768‐72.
Pabuccu R, Gomel V. Reproductive outcome after hysteroscopic metroplasty in women with septate uterus and otherwise unexplained infertility. Fertil Steril 2004; 81(6): 1675‐8.
Nappi C, Di Spiezio Sardo A. State‐of‐the‐art Hysteroscopic Approaches to Pathologies of the Genital Tract. Endo‐Press 2014.
Porcu G, Cravello L, D’ Ercole C et al. Hysteroscopic metroplasty for septate uterus and repetitive abortions: reproductive outcome. Eur J Obstet Gynecol Reprod Biol 2000; 88: 81–84.
Mollo A, Nazzaro G, Granata M et al. Combined hysteroscopic findings and 3‐dimensional reconstructed coronal view of the uterus to avoid laparoscopic assessment for inpatient hysteroscopic metroplasty: pilot study. J Minim Invasive Gynecol 2011; 18: 112–117.
Di Spiezio Sardo A, Spinelli M, Bramante S et al. Efficacy of a polyethylene oxide‐sodium carboxymethylcellulose gel in prevention of intrauterine adhesions after hysteroscopic surgery. J Minim Invasive Gynecol 2011; 18(4): 462‐9.
Ludwin A, Ludwin I, Kudla M et al. Diagnostic accuracy of three‐dimensional sonohysterography compared with office hysteroscopy and its interrater/intrarater agreement in uterine cavity assessment after hysteroscopic metroplasty. Fertil Steril 2014; 101(5): 1392–1399.
Di Spiezio Sardo A, Florio P, Nazzaro G et al. Hysteroscopic outpatient metroplasty to expand dysmorphic uteri (HOME‐DU technique): a pilot study. Reprod Biomed Online 2015; 30(2): 166‐74.
Homer H, Li T, Cooke I. The septate uterus: a review of management and reproductive outcome. Fertil Steril 2000; 73: 1–14.
Grimbizis GF, Camus M, Tarlatzis BC, Bontis JN, Devroey P. Clinical implications of uterine malformations and hysteroscopic treatment results. Hum Reprod Update 2001; 7(2): 161‐74.
Kormányos Z, Molnár BG, Pál A. Removal of a residual portion of a uterine septum in women of advanced reproductive age: obstetric outcome. Hum Reprod 2006; 21(4): 1047‐51.
Woelfer B, Salim R, Banerjee S et al. Reproductive outcomes in women with congenital uterine anomalies detected by three‐dimensional ultrasound screening. Obstet Gynecol 2001; 98(6): 1099‐103.
Wu MH, Hsu CC, Huang KE. Detection of congenital müllerian duct anomalies using three‐dimensional ultrasound. J Clin Ultrasound 1997; 25(9): 487‐92.
Jurkovic D, Geipel A, Gruboeck K et al. Three‐dimensional ultrasound for the assessment of uterine anatomy and detection of congenital anomalies: a comparison with hysterosalpingography and two‐dimensional sonography. Ultrasound Obstet Gynecol. 1995; 5(4): 233‐7.
Ghi T, Casadio P, Kuleva M et al. Accuracy of three‐dimensional ultrasound in diagnosis and classification of congenital uterine anomalies. Fertil Steril 2009; 92(2): 808‐13.
Gubbini G, Di Spiezio Sardo A, Nascetti D et al. New outpatient subclassification system for American Fertility Society Classes V
and VI uterine anomalies. J Minim Invasive Gynecol 2009; 16(5): 554‐61.
Bajka M, Badir S. Fundus Thickness Assessment by 3D Transvaginal Ultrasound Allows Metrics‐Based Diagnosis and Treatment of Congenital
Uterine Anomalies. Ultraschall in Med 2015
9

Complications and Compliance of Hysteroscopic Sterilization with Essure in an Inner City Hospital
Crystal Santiago, M.D.
Lincoln Medical and Mental Health CenterDepartment of Obstetrics and Gynecology
Bronx, New York
I have no financial relationships to disclose
• Discuss real life experience with Essurecompared to initial FDA studies
– Complications
– Failure of placement
– Subsequent pregnancies
• Follow up compliance rate in an inner city, high immigrant population
• Objective: assess complications from Essure sterilization and compliance rate for follow up with 3 month Hysterosalpingogram (HSG)
• Design: Retrospective chart review
• Setting: Academic affiliated community hospital
• Patients: All patients with attempted hysteroscopic Essure sterilization from January 2008 through August 2014
Overview:
Measurements & Main Results:• 175 procedures attempted on 173 patients
• Demographics
– 151 (87.3%) Hispanic
– 19 (11.0%) African/African‐American
– 3 (1.7%) Asian
– Average age 35 years
– Average parity of 3
– Body mass index (BMI) of 29.0 kg/m2
– Average surgical time 37 minutes
– Estimated blood loss 5 mL
Measurements & Main Results:• Of the 175 procedures, 16 (9.1%) were incomplete
– 4 unilateral placements
• Only able to visualize single ostium and placed
• 1 returned for successful placement in other tube
– 7 aborted procedures
• 5 unable to pass into 1 or both ostia
– 1 due to tubal spasm
• 1 proliferative endometrium, poor visualization
• 1 device misfired on 3 attempts
• 1 returned for successful placement bilaterally
– 5 converted to laparoscopic sterilization• 3 unable to visualize 1 or more ostia
• 2 tubal spasm
10
Measurements & Main Results:• Of the 161 successful bilateral Essure placements
– 99 (62%) patients had HSG performed
• 84 (85%) no spillage bilaterally
• 14 (14%) with unilateral/bilateral spillage
• 1 (1%) incomplete studies
– 62 (39%) patients did not have HSG
• 35 (57%) failed to keep appointment
• 16 (25%) HSG orders were cancelled from the system upon discharge (system error)
• 10 (16%) had no HSG order placed
• 1 (2%) has a pending appointment
Measurements & Main Results:
• Of the 161 successful bilateral Essure placements
– 3 (1.8%) had subsequent pregnancies
• 2 (1.2%) with confirmed bilateral blockage on HSG
• 1 (0.6%) had no HSG performed
Conclusions:• Failure rate of Essure placement at first attempt
– 9.1% our patients
– 14% in Pivotal study
• Post procedure HSG noncompliance rate – 38% in our patients
– 4.4% in Pivotal study, 3.0% in Phase II study
• The rate of initial tubal patency on HSG– 14.1% our patients
– 3.5% from both Phase II and Pivotal studies
• Post procedure pregnancy rate
– 1.2% over the 8 years for our patients
– 0.2% over 2 years from Essure studies
Conclusions:• Expulsion rate
– 1.2% for our patients
– 2.9% for Pivotal study, 0.5% for Phase II study
• Perforation
– 0% for our patients
– 2.9% for Phase II study, 1.1% for Pivotal study
– Tubal spasm rate: 1.7% of our procedures
• Phase 2:
– Recall process for all previous procedures (secondary analysis)
– Up to date log of new procedures
– Fix system error of disappearing HSG appointments
• Goals:
– Improve compliance with HSG follow up
– Decrease complication rates
• Cooper JM, Carignan CS, Cher D, Kerin JF; Selective Tubal Occlusion Procedure 2000 Investigators Group. “Microinsert nonincisionalhysteroscopic sterilization.” Obstet Gynecol. 2003 Jul;102(1):59‐67.
• Kerin JF, Cooper JM, Price T, Herendael BJ, Cayuela‐Font E, Cher D, Carignan CS. “Hysteroscopic sterilization using a micro‐insert device: results of a multicentre Phase II study.” Hum Reprod. 2003 Jun;18(6): 1223‐30.
11

Hysteroscopic metroplasty in women with unexplained primary infertility: A prospective cohort
study
Tarek Shokeir,MD
Mansoura University, Egypt
I have no financial relationships to disclose.
Objectives
• To evaluate the effect of hysteroscopicmetropalsty as therapy for unexplainedprimary infertility in women with uterineseptum as a possible sole cause forreproductive failure.
• To define the factors influencing reproductivesuccess.
Objectives (contin.)
• Discuss clinical pregnancy rate (PR) according
to patient and septum characteristics using
HSG were the main outcome measures.
Materials and methods • From August 2011 through December 2014we enrolled 103 infertile women with uterineseptum as a possible sole cause forunexplained primary infertility.
• Uterine anomalies were diagnosed byhysterosalpingography (HSG) and transvaginalsonography (TVS) . Diagnosis was furtherconfirmed by office hysteroscopy.
Materials and methods (contin.)
• Elecrosurgical hysteroscopic metroplasty was
performed in the early follicular phase, under
general anesthesia with no preoperative
endometrial preparation.
12

Materials and methods (contin.)
• Only patients with follow‐up of at least 12 months duration are discussed in this study.
• Clinical pregnancy rate (PR) according to patient and septum characteristics defined by HSG (septum length) were the main outcome measures.
Results
• Follow‐up was complete for 88 patients.
• Forty‐two patients became pregnant (40.7%).
• There was short delay to conception (mean ±SD time to conception was 7.5 ± 6.2 months).
• Of 44 pregnancies in 42 women, 36 live newborns were delivered.
Patients’ characteristics according to fertility Pts. who Pts. who did P
conceived not conceive value
(no=42) (n=46)
_______________________________________________________________
Mean follow‐up 28.3±7.4 26.4±7.5NS
(months)
Pts. Age (ys,%)
>40 0 (0) 22 (100) NS<40 42 (63.6) 24 (36.4) <.001
≥35 14 (25.9) 40 (47.1) NS
<35 28 (82.4) 6 (17.6) <.001
Duration of infertility
≥3 ys. 6 (15) 34 (85) NS
<3ys. 36 (75) 12 (25) <.001
Septum characteristics according to fertility ____________________________________________________
Pts. Who Pts. Who P
conceived did not conceive value
(n=42) (n=46)
____________________________________________________
Longtudinal septum length
>½ uterus 12 (42.8) 6 (33.3) .12
<½ uterus 30 (66.2) 40 (57.2) NS
___________________________________________________
Values are pts.’ numbers (%)
Authors’ Conclusions
• Fertility and pregnancy after hysteroscopic
metroplasty in women with otherwise unexplained
primary infertility and uterine septum as a possible
sole cause for reproductive failure seems to depend
on patient age, duration of infertility, and uterine
septum length.
Conclusions (contin.)
• Women with a septum size larger than one‐
half of their uterine length have a higher
chance of successful pregnancy after
hysteroscopic metroplasty.
13
14

Hysteroscopic Management of a Stenotic Cervix
Michael W.H. Suen, MD University of British Columbia, Vancouver, British Columbia, Canada
Objective: To demonstrate a “see-and-treat” approach in an outpatient hysteroscopy setting for management of a stenotic cervix.
Design: Stepwise demonstration of the technique with narrated video and animations.
Setting: Cervical stenosis is defined as narrowing of a cervix os with difficulty inserting a 2.5mm dilator. It is found most commonly in nulliparous and postmenopausal women, and can obstruct a number of gynecologic procedures that require intrauterine access. Technical difficulty increases the risk of cervical laceration, uterine perforation and the formation of false passages, which can worsen cervical scarring and lead to failure of a procedure. Outpatient hysteroscopy shows operative success with patient satisfaction, and can be used to overcome a stenotic cervix to complete an intended procedure.
Interventions: Hysteroscopic management of a stenotic cervix involves:
1. Optimizing the surgical environment 2. Vaginoscopy and “no-touch” hysteroscopy 3. Revision of the cervical canal, with microscissors, micrograspers or a cutting loop
electrode.
Conclusion: A number of strategies can be utilized when faced with a stenotic cervix. This video demonstrated the ease of a “see-and-treat” approach in an outpatient hysteroscopy setting.
15

Hysteroscopic Removal of Retained Placental Tissue Alleviates Postpartum Hypertension
Chandrew Rajakumar, MD, FRCSC The Ottawa Hospital, Ottawa, Ontario, Canada
Objective: Through office hysteroscopy identify an intrauterine cause for postpartum hypertension in a woman who had completed a pregnancy complicated by HELLP syndrome. Secondly, ameliorate the hypertension and dependence on antihypertensive medications through hysteroscopic-guided removal of retained placental fragments.
Design: Case report
Setting: Outpatient hysteroscopy suite and operating theater at university affiliated teaching hospitals
Interventions: Vaginoscopy followed by diagnostic hysteroscopy without sedation to confirm the presence of placental tissues within the uterine cavity followed by hysteroscopically-guided blunt curettage of placental tissues using a non-energized loop electrode.
Conclusion: Diagnostic hysteroscopy, when performed after vaginoscopy, allows of confirmation of retained placental fragments via biopsy without the need for sedation and can be performed in an outpatient setting. Visually guided removal of retained placental tissue fragments provided relief from post-partum hypertension and cessation of antihypertensive medications within 48 hours from the procedure. Furthermore, this technique replaces blind curettage, which may increase the risk of intrauterine synechiae and/or perforation.
16

CULTURAL AND LINGUISTIC COMPETENCY Governor Arnold Schwarzenegger signed into law AB 1195 (eff. 7/1/06) requiring local CME providers, such as
the AAGL, to assist in enhancing the cultural and linguistic competency of California’s physicians
(researchers and doctors without patient contact are exempt). This mandate follows the federal Civil Rights Act of 1964, Executive Order 13166 (2000) and the Dymally-Alatorre Bilingual Services Act (1973), all of which
recognize, as confirmed by the US Census Bureau, that substantial numbers of patients possess limited English proficiency (LEP).
California Business & Professions Code §2190.1(c)(3) requires a review and explanation of the laws
identified above so as to fulfill AAGL’s obligations pursuant to California law. Additional guidance is provided by the Institute for Medical Quality at http://www.imq.org
Title VI of the Civil Rights Act of 1964 prohibits recipients of federal financial assistance from
discriminating against or otherwise excluding individuals on the basis of race, color, or national origin in any of their activities. In 1974, the US Supreme Court recognized LEP individuals as potential victims of national
origin discrimination. In all situations, federal agencies are required to assess the number or proportion of LEP individuals in the eligible service population, the frequency with which they come into contact with the
program, the importance of the services, and the resources available to the recipient, including the mix of oral
and written language services. Additional details may be found in the Department of Justice Policy Guidance Document: Enforcement of Title VI of the Civil Rights Act of 1964 http://www.usdoj.gov/crt/cor/pubs.htm.
Executive Order 13166,”Improving Access to Services for Persons with Limited English
Proficiency”, signed by the President on August 11, 2000 http://www.usdoj.gov/crt/cor/13166.htm was the genesis of the Guidance Document mentioned above. The Executive Order requires all federal agencies,
including those which provide federal financial assistance, to examine the services they provide, identify any
need for services to LEP individuals, and develop and implement a system to provide those services so LEP persons can have meaningful access.
Dymally-Alatorre Bilingual Services Act (California Government Code §7290 et seq.) requires every
California state agency which either provides information to, or has contact with, the public to provide bilingual
interpreters as well as translated materials explaining those services whenever the local agency serves LEP members of a group whose numbers exceed 5% of the general population.
~
If you add staff to assist with LEP patients, confirm their translation skills, not just their language skills.
A 2007 Northern California study from Sutter Health confirmed that being bilingual does not guarantee competence as a medical interpreter. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2078538.
US Population
Language Spoken at Home
English
Spanish
AsianOther
Indo-Euro
California
Language Spoken at Home
Spanish
English
OtherAsian
Indo-Euro
19.7% of the US Population speaks a language other than English at home In California, this number is 42.5%
17





























