Embed Size (px)
Citation preview

Please Remember to Silence Your Cell Phones

Adventures in Care Transitions

Sometimes You Just Have To Try To Fly!

Our Approach
Modified Coleman Plan Medication Self Management Red Flags Personal Health Record (PHR) Follow-up Visits with Primary
Care Provider or Specialist Home & Community Services Nutrition Assistance
Targeted Population of High Risk Dx Congestive Heart Failure Diabetes Chronic Obstructive Pulmonary
Disease (COPD) Pneumonia Heart Attack (Acute Myocardial
Infarction)
Social Risk Factors Lives alone or lack of able
bodied caregiver, Low literacy, Economic stress, History of falls

Forming Coalition
Dale Medical Center
Mizell Memorial Hospital
Andalusia Regional Hospital
Medical Center Barbour
Southeast Alabama Medical Center
Flowers Hospital
Medical Center Enterprise
Wiregrass Medical Center

Member Hospital Considerations
Southeast Alabama Medical Center 362 beds, 2,143 FFS Admissions
Flowers Hospital 235 beds, 1,143 FFS Admissions
Andalusia Regional Hospital 87 beds, 395 FFS Admissions
Mizell Memorial Hospital 58 beds, 152 FFS Admissions
Wiregrass Medical Center 75 beds, 152 FFS Admissions
Medical Center Enterprise 117 beds, 244 FFS Admissions
Medical Center Barbour 46 beds 148 FFS Admissions
Dale Medical Center 75 beds, 166 FFS Admissions

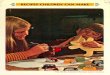
Compare Performance to Projections, Changing Standards!
0
50
100
150
200
250
Andalusia Regional Hospital
Dale Medical Center
Flowers Hospital
Medical Center
Barbour
Medical Center
Enterprise
MIZELL MEMORIAL HOSPITAL
SE Alabama Medical Center
Wiregrass Medical Center
22
37
87
6
37
15
94
13
78
8
100
15 18 19
95
14
30
14
95
12 20
13
179
13
41
19
133
17 28
18
250
18
Projected
Actual 5/1-5/31
Est. 25% FFS
Est. 35% FFS

Staffing Models
Dedicated Hospital Coaches, Lead Coaches & Recruitment Coaches
Hospital/Field Coaches Field Only Coaches Program Assistant or
Services Coordinators Program Coordinators Call Centers Area Coaches versus Stay
with Member Community Connections

Other Coaching Considerations
Non-Traditional Staff Gypsy Workers Potential Frictions
Right Skillsets Key Requirement: Communicators Organized Low Maintenance/Low Drama
Get Past Cultural Barriers “I’m Fine, I have family that looks after me” Meeting People where they are

Leveraging Information Systems
Evaluating Systems Web Based, Platforms Cost Track Record/Experience
What capabilities do you want to add? List Bills & Surveys Internal Data for Management

Lessons Learned

The Early Days
Figure start up in budget process Working out intake procedures takes time Growth requires developed relationships
Plan Hospital Processes but expect Adjustments Keep notes

Getting Them & Keeping Them
Be part of the Discharge Process Better Outcomes as the Hospital Culture Opt Out Extend the Picture of the Patient into the Home “Wellness Check”

Don’t Assume
Signature Sheet
Duplicated Services

Being the New Kid
Don’t Mess With My Rice Bowl Fitting your Coaches into the existing care
coordination landscape Intake w EMR vs without “Where’s the Chart?” Sifting through the screens
SNF Coordination

Scaling Barriers
Addressing CT Members with non-activation issues Nutrition Highest Utilization Meal Packs and Liquid Nutrition
Copays, DME Prescription and Physician Visit Same or Similar Non-Covered Items

Transportation Impact on prescription fills Impact on Follow up Doctor Appointments
Time of Day Family member burden
Community Service Project Groups Ramps Handicap Access Modifications Livability Repairs
Scaling Barriers (cont.)

“What happens to me after 30 days?”
Many needs persist after our CT period Tie in to additional community resources Commitment to Partner Hospitals

Dealing with Rejection
Initial Submission Death by ~~ What’s in a Name? But the Hospital got paid! Managing Billing Single filing versus 2 filing Batch Processing versus Line Entry
Final Comparisons

What Could Go Wrong?
Welcome to the “Metric System” Lewin Group Measurements CMS Measurements
“The Big One”

Stories From the Field
Bobby M- member whose spouse has dementia, Meal packs have kept his weight and fluid stabilized.
Member was about to lose her Medicaid and had been eating from a dumpster. We ordered frozen meals for member and set her up with Medicaid Waiver so she could keep her medications.
Member was still weak from his hospital stay. His spouse (elderly) was having to help with all ADLs. We were able to help with equipment and set them up to receive a month of meals. I explained some of the other programs that they might be eligible for and his wife was brought to tears. She was very thankful and stated that no one ever helped them before.

Key Factor for Success...(One Coach’s Opinion)
Working well with member to identify true needs. Example: Member might state I haven't scheduled the appointment. After some questioning you realize this is due to lack of transportation. Another member was given three new prescriptions per discharge paperwork. After checking medications you realize they aren't filled. The member isn't always ready to say I need help with this or that. Sometimes it takes the right question and an attitude that doesn't make them fell bad for having to ask for the help. With this combination, we identify the needs, help with those needs, and have left the patient with the tools to help themselves in the future. --- I think our "Care Package" is wonderful

Kim's Story
I had been attempting to reach a member and had tried at various times and all numbers I could find but had been unsuccessful. After finishing another home visit, I decided to try stopping at his address on my way through that area. I did not get an answer at his door but more troubling was that I could see his order of insulin was sitting on the steps in the sun. I checked at the neighbors and told me he had gone for inpatient rehab and knew the facility. I was able to reach the member at the facility and he was unaware that his insulin supplies had been delivered. If I hadn't been trying to reach him and stopped by, he would not have known his medicine had most likely been damaged by the heat or that he needed to arrange for replacement medicine.

Amanda's Story
Do you remember Louise L.? She had trouble seeing due to macular degeneration. During my home visit I had to write her medication instructions in inch tall letters for her to make out when to take her medicine. After working with her on her medications and her discharge instructions, I realized how much her vision problems were impacting the rest of her health. I worked with Meg to get her some information and referred to the Alabama Institute for the Blind and Disabled (AIBD). She was given several things to make her life a little easier. She now has a large clock so she can see the time (and make it to appointments on time) and they gave her a reader so she can read her prescriptions and instructions. She was very happy to be able to do those things for herself again instead of having to get someone to help her. My experience with this patient really drove home how one issue can cause problems in so many different areas. The help we were able to get her made a big impact on multiple problems she was struggling with.

Spanning the Gap between Hospital and Home
Jennifer's Story: With this particular client, I was the hospital coach as well as the home coach. She expressed to me during the hospital visit that her illness had been present for approximately 3 years. Her symptoms included nausea, abdominal pain, and shortness of breath. Upon visiting with the client and her husband, member said she was more concerned about her husband health than hers. He had recently had heart surgery but he was the one that “cleaned the mold every day”. I discovered several walls in the home were covered in mold, as well as present on furniture. When I asked them about moving, they stated the "cheap" monthly rent had been the reason they stayed in the home. After further discussion, it was discovered the couple paid approximately $2000 during the winter months for propane. During these months they experienced a lack of food and medication due to the necessary redistribution of funds. They mentioned numerous times during the visit about their desire to move but the motivation to act was absent. We spoke for quite some time about the actual costs they were enduring due the mold. The health costs for the member's declining health, the declining health for the husband, the financial burden for living in an unsafe and uninsulated home, and the hopelessness experienced by both were discussed. I told them bluntly that they had to find another home immediately. I told them I would provide assistance ranging from going to the local housing authority to looking in the local newspapers. I insisted they chose where the search for a new home would begin. The next day, the member called to inform me that they had an appointment to look at a duplex apartment. By the end of the week, arrangements had been made for the couple to relocate. Luckily, the home was furnished and no "moldy" furniture had to be taken with them. The client and her husband reported during the 30 day period following the move that they felt much better physically and emotionally. No hospital admissions have been reported either. As a CT coach, clients not only look to you as resource for needed services but also as a motivator and/or a "good listener".