Embed Size (px)
Citation preview

Ž .Psychiatry Research 89 1999 21]27
Plasma levels of tumor necrosis factor-alpha in patientswith panic disorder: effect of alprazolam therapy
Francesca BrambillaU, Laura Bellodi, Giampaolo Perna
Dipartimento di Scienze Neuropsichiche, Istituto Scientifico Ospedale S. Raffaele, Via Prinetti 29, 20127 Milano, Italy
Received 16 November 1998; received in revised form 15 June 1999; accepted 12 July 1999
Abstract
Ž .Plasma concentrations of tumor necrosis factor-a TNF-a were measured in 10 outpatients with panic disorder,Ž . Ž .twice at a 48-h interval before and twice on days 30]32 of treatment with alprazolam 2]2.5 mgrday , and twice in
10 age- and sex-matched healthy controls. TNF-a concentrations did not differ in patients and control subjects,either before therapy or at days 30]32 of therapy. In five patients before therapy, and in three of them after therapy,TNF-a values were higher than the maximal concentrations of the cytokine in controls. Q 1999 Elsevier ScienceIreland Ltd. All rights reserved.
Keywords: Anxiety; Agoraphobla; Cytokines; Immunology; Alprazolam
1. Introduction
Data in the literature on the immune functionŽ .of patients with panic disorder PD are scanty
and controversial, with only a trend toward anactivation of the T-lymphocyte system having been
Žreported in some but not all studies Surman et
U Corresponding author. Tel.: q39-02-26433376; fax: q39-02-70122889.
al., 1986; Andreoli et al., 1990, 1992; Ramesh etal., 1990, 1991; Schleifer et al., 1990; McDaniel etal., 1991; Brambilla et al., 1992; Rapaport et al.,
.1994; Perini et al., 1995 . The T-lymphocyte sys-tem is one of the major sources of production ofcytokines, which in turn stimulate brain nora-
Ž . Ž .drenalin NE and serotonin 5-HT secretion, inparticular in the hippocampus and the hypothala-mus, modulating neuroendocrine, autonomic,cognitive, affective, and behavioral processesŽ .Pauli et al., 1998 . Because of the biological and
0165-1781r99r$ - see front matter Q 1999 Elsevier Science Ireland Ltd. All rights reserved.Ž .PII: S 0 1 6 5 - 1 7 8 1 9 9 0 0 0 9 1 - 8

( )F. Brambilla et al. r Psychiatry Research 89 1999 21]2722
psychological effects of cytokines, alterations oftheir secretion might influence the developmentand course of mental disorders.
In a previous study, we measured plasma inter-Ž .leukin-1b Il-1b concentrations in a group of
patients with PD and agoraphobia at two timepoints: in an active phase of illness when thepatients were drug-free, and after 1 month ofalprazolam therapy when symptomatology was
Ž .improving Brambilla et al., 1994 . Il-1b levelswere significantly higher in PD patients than inage- and sex-matched healthy controls on bothoccasions, which confirmed the functional activa-tion of the immune system. The fact that thephenomenon was still present during a period ofsymptomatic improvement suggested that the al-teration could not be simply symptom-related butmight be a trait marker of the disorder and per-haps responsible for some of its clinical aspects.
When injected systemically or intracerebroven-tricularly into experimental animals, Il-1b induceschanges in exploratory behavior, motor activity,operant performances, defensive withdrawal, andbehavioral despair } all symptoms that mimic
Žsome of the clinical aspects of PD ChemilckaSchorr and Arnason, 1990; Del Cerro and Borrell,
.1990; Dunn et al., 1991; Tazi et al., 1991 .After activation of the immune system, a vari-
ety of other cytokines are released into the bloodŽ .and in the brain Besedowsky and Del Rey, 1996 ,
possibly with different forms of functional sig-nificance. In particular, tumor necrosis factor-aŽ .TNF-a is secreted in parallel with Il-1b butdoes not affect hippocampal 5-HT neurotransmis-sion, which has been proposed to be involved inthe cognitive, affective, and behavioral aspects ofthe Il-1b-linked symptomatic behaviors. Intra-cerebroventricular administration of TNF-a intoexperimental animals does not result in behav-ioral signs of illness, which suggests that not allcytokines are equally effective in modifying amineequilibrium and that there is no overlap amongthe psychological]behavioral effects that they
Ž .produce Pauli et al., 1998 .For that reason, we measured the levels of
TNF-a in the same plasma samples used to mea-sure Il-1b concentrations. The aims of this study
Ž .were to determine 1 whether plasma levels of
TNF-a are increased in PD patients before andafter 1 month of alprazolam therapy, as are those
Ž .of Il-1b; 2 whether the increase, if any, parallelsŽ .that of Il-1b; 3 whether levels of TNF-a are
correlated with some of the symptomatologicalaspects of the disorder.
2. Methods
The patients studied and the methods used areŽthe same as those described previously Brambilla
. Žet al., 1994 . Ten outpatients four men and six. Žwomen , aged 20]48 years means33.4, S.D.s
.8.4 , with diagnoses of PD and agoraphobia ac-Žcording to DSM-III-R criteria American Psychi-
.atric Association, 1987 , entered the study. Diag-noses were made with the Structured Clinical
ŽInterview for DSM-III-RrUpjohn version SCID;.Spitzer and Williams 1983 . Duration of illness
Ž .was 1]16 years means5.7, S.D.s5.8 . Fourpatients had been previously treated with benzo-
Ždiazepines lorazapam, diazepam, fluorazepam,.chlordesmethyldiazepam and one with amitripty-
Žline all medication stopped at least 15 days be-.fore the study began , while the other five patients
had never received psychotropic medication.Ten physically healthy age- and sex-matched
volunteers, recruited from the hospital staff,formed the control group. They were interviewedwith the Diagnostic Interview Schedule RevisedŽ .DIS-III-R; Robins et al., 1989 .
Criteria for exclusion from the study forpatients and controls were organic disorders, in-fections, inflammatory disorders, allergopathies,immune and autoimmune disorders, endocrino-pathies, obesity or recent weight loss, alcohol or
Ždrug abuse, and any Axis I especially present or.past history of depression or Axis II disorder
other than PD in the patients. Patients and con-trol subjects provided informed consent to partici-pate in the study.
EDTA-treated blood for TNF-a assays wasdrawn from patients and controls at 08.30 h, after12 h of fasting and 1 h of bed rest in a recumbentposition. Blood was drawn twice, at 48-h intervals,and the values of the two assays were averaged.
The patients were then given alprazolam for 32

( )F. Brambilla et al. r Psychiatry Research 89 1999 21]27 23
days in a divided oral daily dose of 2.0]2.5 mg.On days 30 and 32, blood for the TNF-a assaywas drawn again by the procedure explainedabove. TNF-a concentrations were measured ra-dioimmunologically with the commercial kits of
Ž .Medgenix Diagnostics Italy . The immununora-Ž .diometric assay IRMA is based on a coated tube
separation of TNF-a, and on the oligoclonal sys-tem R, in which several monoclonal antibodiesdirected against distinct epitopes of TNF-a wereused. The sensitivity of the method is 5 pgrml,and there is no cross-reactivity with interferon-a ,b, and g, interleukin-1b, interleukin-2, or tumornecrosis factor-b. The intra-assay coefficient ofvariation was 2.2%, and the inter-assay coefficientof variation was 2.8%.
The severity of clinical symptomatology wasinvestigated at the time of blood sampling, beforetreatment with alprazolam, and after 30 days oftreatment. Measures included the Hamilton Rat-
Ž .ing Scale for Anxiety HRSA , the State-TraitŽ .Anxiety Inventory STAI , and the Panic Attack
Ž .and Anticipatory Anxiety Scale PAAS .The TNF-a and clinical data were analyzed by:
Ž .1 MANOVA and the non-parametricMann]Whitney test, to compare values of TNF-aof controls against those of patients before and
Ž .after treatment with alprazolam; 2 Kruskal]
Wallis test to compare the TNF-a variables inŽ .patients and controls; 3 non-parametric
Wilcoxon test to compare TNF-a concentrationsin patients before and after treatment with alpra-zolam, and rating scales scores before and after
Ž .treatment; and 4 Spearman rank analysis tolook for correlations between TNF-a values be-fore and after treatment with alprazolam anddemographic or clinical data in patients.
3. Results
The severity and frequency of panic attackswere elevated in basal conditions and were sig-nificantly improved after treatment with alpra-
Žzolam PAAS: pretreatment, mean score s 2,S.D.s 2; post-treatment, mean score s 0.3,
.S.D.s0.1; ts2.6, d.f.s18, P-0.01 . Pretreat-ment levels of anxiety were also elevated and hadimproved significantly on day 30 of therapyŽHRSA: pretreatment, mean scores68.5, S.D.s27; post-treatment, mean scores26, S.D.s19;ts4, d.f.s18, P-0.0008; STAI: pretreatment,mean score s51, S.D.s9; post-treatment, mean
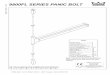
.scores40, S.D.s10; ts2.21, d.f.s18, P-0.03 .Mean plasma concentrations of TNF-a before
treatment were not significantly different in
Ž . Ž .Fig. 1. Plasma concentrations of tumor necrosis factor-a TNF-a in 10 controls dotted bar and in 10 patients with panic disorderŽ .before and after alprazolam therapy black bars .

( )F. Brambilla et al. r Psychiatry Research 89 1999 21]2724
Žpatients and controls patients: mean s 27.5pgrml, S.D.s26.4; controls: means14.7 pgrml,S.D.s6.9; Mann]Whitney, Kruskal]Wallis and
.MANOVA, all N.S. . After 1 month of treatmentwith alprazolam, patients showed no significantdifferences from control values or from their pre-treatment plasma concentrations of TNF-aŽmeans26.4 pgrml, S.D.s30.0; Mann]Whitneyand MANOVA tests between patients and con-trols, N.S.; Wilcoxon test between patients before
. Ž .and after treatment, N.S. Fig. 1 . There were nodifferences in TNF-a concentrations between thesamples drawn at 48-h intervals for either thecontrols or the patients before and after treat-ment. The apparently higher values of patientsbefore and after treatment relative to controlvalues were due to five patients before treatmentand to three patients after therapy whose TNF-aconcentrations were much higher than the maxi-
Žmal values of controls high-value patients beforetherapy: means52.2 pgrml; S.D.s32.3; low-value patients: means11.9 pgrml, S.D.s1.9;high-value patients after therapy: mean s67.3pgrml, S.D.s42.2; low-value patients after ther-apy: means11.8, S.D.s2.7; controls: mean s
.14.7 pgrml, S.D.s6.7, N.S. .For the patients there were no significant cor-
relations between age, sex, duration of illness,PAAS, STAI, and HRSA scores and TNF-a val-ues before or after treatment with alprazolam.When the patients were divided into two groups,with and without previous psychopharmacologicaltreatment, neither group showed a correlationbetween TNF-a levels and clinical data before orafter therapy. When the five patients who hadelevated values and the seven who had normalvalues of TNF-a were compared, no significantdifferences emerged for demographic or clinicaldata. Spearman rank analysis between pretreat-ment and post-treatment concentrations of TNF-a
Žand Il-1b data reported elsewhere; see Brambilla.et al., 1994 revealed no correlations between
values for the two cytokines.
4. Discussion
Although our data were obtained in too small a
group of subjects to permit us to draw definitiveconclusions, they suggest that the plasma TNF-aconcentrations, consistent at 48-h intervals, arenot altered in PD patients, do not change afteralprazolam treatment, and are not correlated withdemographic characteristics and clinical symp-tomatology of the patients. Since five of the 12
Ž .patients 41.8% had pretreatment values thatwere higher than the highest control value, andthree of them also had elevated post-treatmentvalues, it cannot be excluded that studies of largerpopulations would reveal significantly higher thannormal concentrations of the cytokine, at least ina subgroup of patients.
The observation that both the normal and theelevated concentrations of TNF-a were stablewhen measured at 48-h intervals suggests that thevalues were neither chance occurrences nor re-lated to spontaneous fluctuations of the cytokine.Since a circadian rhythm of function has been
Žproposed for the immune system Petitto et al.,1993; Dhabhar et al., 1994; Hiemke et al., 1995;
.Young et al., 1995 , and since we measured TNF-aconcentrations only in the morning, we cannotstate that values would be consistently normal orhigher than normal over a 24-h period. A study ofthe circadian rhythm of secretion of the cytokinewould be necessary to validate the stability of thevalues obtained over a 24-h period.
Another bias of our study is the fact that wemeasured TNF-a values in controls only twice, at48-h intervals, and used the mean of these twovalues for comparison with those of patients,which were assayed twice before and twice 1month later after treatment with alprazolam.However, because TNF-a values in controls didnot differ in the two specimens obtained 2 daysapart, we would suggest that no marked variationsshould be expected in specimens drawn 1 monthlater.
The difference between the significantly higherthan normal concentrations of Il-1b, which werefound in PD patients both before and after treat-ment, and the TNF-a values, which were elevatedonly in subgroups of patients before and after
Ž .treatment ns5 and ns3, respectively , and thelack of correlation between the levels of the twocytokines are difficult to explain. Positive cy-

( )F. Brambilla et al. r Psychiatry Research 89 1999 21]27 25
tokine]cytokine interactions between Il-1b andTNF-a have been reported in experimental ani-mals, and the two cytokines seem to exert somesimilar effects on central secretions of serotonin,noradrenalin, and dopamine and on behaviorŽPauli et al., 1998; Plata Salaman, 1998; Song et
.al., 1998 . On the basis of the work in experimen-tal animals, we had expected to find a significantlink between their secretion levels in our patientsas well.
The increased secretion of Il-1b observed inŽ .these patients Brambilla et al., 1994 and that of
TNF-a in a subgroup of them could be due to theŽ .prolonged norepinephrine NE hyperactivity that
has been suggested to be one of the dysfunctionsŽinvolved in PD Charney et al., 1984, 1989; Red-
.mond, 1986 Gorman et al., 1989 . NE hypersecre-tion might impair immune function in general,and cytokine secretion in particular, by down-reg-ulating and reducing the density of noradrenergicreceptors, characteristics that have been de-
Žscribed in lymphocytes of PD patients Besedow-sky et al., 1979; Maes et al., 1988, 1991; Takamotoet al., 1991; Felsner et al., 1992; Maddock et al.,
.1992 . This should result in a blunting of theinhibitory effect of NE on the immune systemwith ensuing increases in both Il-1b and TNF-a.
The same might be true for the hyperactivity ofŽ .the hypothalamo-pituitary-adrenal HPA axis
that has been reported to occur in PD patientsŽ .Holsboer, 1988; Brambilla et al., 1991 . Gluco-corticoids have an inhibitory effect on immunefunction, and on cytokine production in particularŽ .Besedowsky et al., 1986; Butler et al., 1989 .Down-regulation of the lymphocyte glucocorti-coid receptor sensitivity linked to the HPA hyper-activity might result in a blunting of the inhibitoryeffects of glucocorticolds on the immune systemin general and on cytokine production in particu-lar. The Il-1b secretion of PD patients mightresemble that of patients with major depressivedisorders who have elevated HPA activity and
Želevated cytokine levels Besedowsky et al., 1986;.Maes et al., 1988 .
The explanation for the influence of putativelyelevated NE and HPA activity on the secretion ofIl-1b in our PD patients and on that of TNF-a insome of them is unclear. It should be remem-
bered, however, that studies of other immuneŽparameters cell counts of T, B, T-4, T-8, CD-3,
CD-3-DR, CD-4, CD-8, CD-16, CD-18, HLA-DR,peripheral blood mononuclear cell proliferative
.responses to mitogen stimulation have also hadinconsistent results, ranging from normal to
Žabnormal values Surman et al., 1986; Ramesh etal., 1990; Schleifer et al., 1990; McDaniel et al.,1991; Andreoli et al., 1992; Brambilla et al., 1992;
.Perini et al., 1995 . To the best of our knowledge,no previous studies have been done of TNF-asecretion in PD, and there is only one study onplasma cytokine concentrations in these patients,which found normal levels of Il-1b and elevated
Žlevels of Il-2 and sIl-2 receptors Rapaport and.Stein, 1994 . The contrasting findings regarding
concentrations of Il-1b in our previous workŽ .Brambilla et al., 1994 and that of Rapaport et
Ž .al. 1994 are difficult to explain apart from thefact that we used a radioimmunoassay to measurethe cytokine levels and the Rapaport group useda competitive enzyme immunoassay; the twomethods of measurement may detect differentepitopes of Il-b.
Since there were no correlations between theseverity of symptomatology in our PD patientsand concentrations of TNF-a or Il-1b, it is un-clear what the significance of the cytokine secre-tions, normal or impaired, could be for the devel-opment, course, and response to treatment of PD.A study of larger groups of subjects examinedlongitudinally is necessary.
References
American Psychiatric Association, 1987. Diagnostic and Statis-tical Manual of Mental Disorders, 3rd ed., revised. Ameri-can Psychiatric Press, Washington, DC.
Andreoli, A., Keller, S.E., Taban, C., Rabeus, M., Garrone, G.,1990. Immune function in major depressive disorder: rela-tion to panic disorder comorbity. Biological Psychiatry 27Ž .Suppl. 9A , 95A.
Andreoli, A., Keller, S.E., Rabaeus, M., Zangg, L., Garrone,G., Taban, C., 1992. Immunity, major depression and panicdisorder comorbidity. Biological Psychiatry 31, 896]908.
Besedowsky, K., Del Rey, A., 1996. Immune-neuro-endocrineinteractions: facts and hypotheses. Endocrine Review 17,64]102.
Besedowsky, K., Del Rey, A., Sorkin, E., Da Prada, M., Keller,

( )F. Brambilla et al. r Psychiatry Research 89 1999 21]2726
H., 1979. Immunoregulation mediated by the sympatheticnervous system. Cellular Immunology 48, 346]355.
Besedowsky, K., Del Rey, A., Sorkin, E., Dinarello, C.A., 1986.Immunoregulatory feedback between interleukin-1 and glu-cocorticoid hormones. Science 233, 652]654.
Brambilla, F., Picotti, G.B., Bondiolotti, G.P., Catalano, M.,Lucca, A., Della Maggiora, P., Genazzani, A.R., Petraglia,F., Smeraldi, E., 1991. Neurochemical]hormonal investiga-tion of panic disorder: effects of alprazolam therapy. In:Genazzani, A.R., Nappi, G., Petraglia, F., Martignoni, A.Ž .Eds. , Stress and Related Disorders. Parthenon Press,Cansterton, pp. 175]182.
Brambilla, F., Bellodi, L., Perna, G., Battaglia, M., Sciuto, G.,Diaferia, G., Petraglia, F., Panerai, A., Sacerdote, P., 1992.Psychoimmunoendocrine aspects of panic disorder. Neu-ropsychobiology 26, 12]22.
Brambilla, F., Bellodi, L., Perna, G., Bertani, A., Panerai,A.E., Sacerdote, P., 1994. Plasma interleukin-1-beta plasmaconcentrations in panic disorder. Psychiatry Research 54,135]142.
Butler, L.D., Layman, N.K., Ruedi, P., Cain, R.L., Shellhaas,J., Evans, G.F., Zuckerman, S.H., 1989. Neuroendocrineregulation of in vivo cytokine production and effects: I. Invivo regulatory network involving the neuroendocrine sys-tem, interleukin-1 and tumor necrosis factor-alpha. Journalof Neuroimmunology 24, 143]153.
Charney, D.S., Heninger, G.R., Breier, A., 1984. Noradrener-gic function in panic disorder. Archives of General Psychia-try 41, 751]763.
Charney, D.S., Woods, S.W., Heninger, G.R., 1989. Noradren-ergic function in generalized anxiety disorder: effects ofyohimbine in healthy subjects and patients with generalizedanxiety disorder. Psychiatry Research 27, 173]182.
Chemilcka Schorr, E., Arnason, B.G.W., 1990. Nervous sys-Ž .tem]immune system interactions. In: Waksman, B.H. Ed. ,
Immunologic Mechanisms in Neurological and PsychiatricDisease. Raven Press, New York, pp. 67]90.
Del Cerro, S., Borrell, J., 1990. Interleukin-1 affects the be-havioral despair response in rats by an indirect mechanismwhich requires endogenous CRF. Brain Research 528,162]164.
Dhabhar, F.S., Miller, A.H., Sytein, M., McEwen, B.S., Spencer,R.L., 1994. Diurnal and acute stress-induced changes indistribution of peripheral leukocyte subpopulation. Brain,Behavior and Immunity 8, 66]79.
Dunn, A.J., Antoon, M., Chapman, Y., 1991. Reduction ofexploratory behavior by intraperitoneal injection of inter-leukin-1 involves brain corticotropin-releasing factor. BrainResearch 26, 539]542.
Felsner, P., Hofer, D., Riiner, I., Mangge, H., Gruber, M.,Korsatko, W., Schauenstein, K., 1992. Continuous in vivotreatment with catecholamines suppresses in vitro reactivityof rat peripheral blood T-lymphocytes via alpha-mediatedmechanism. Journal of Neuroimmunology 37, 45]47.
Gorman, J., Liebowitz, M.R., Fryer, A.J., Stein, J.A., 1989. Aneuroanatomical hypothesis for panic disorder. AmericanJournal of Psychiatry 146, 148]161.
Hiemke, C., Brunner, R., Hammes, E., Muller, H., MeyerZum Buschenfelde, K.H., Lohse, A.W., 1995. Circadianvariations in antigen-specific proliferation of human T-lymphocytes and correlation to cortisol production. Psy-choneuroendocrinology 20, 335]342.
Holsboer, F., 1988. Implications of altered limbic-hypo-Ž .thalamic-pituitary-adreno-cortical LHPA function for
neurobiology of depression. Acta Psychiatrica ScandinavicaŽ .341 Suppl. , 72]111.
Maddock, R.J., Carter, C.S., Magliozzi, J.R., Gietzen, D.-W.,1992. Reduced lymphocyte beta-adrenoceptor function inpanic disorder with agoraphobia and changes with treat-
Ž .ment. Biological Psychiatry 31 Suppl. 5A , 67A.Maes, M., Bosmans, E., Suy, E., Minner, B., Raus, J., 1988.
Impaired lymphocyte stimulation by mitogens in severelydepressed patients } a complex interface with HPA-axishyperfunction, noradrenergic activity, and the ageingprocess. British Journal of Psychiatry 155, 793]798.
Maes, M., Bosmans, E., Suy, E., Minner, B., Raus, J., 1991. Afurther explorations of the relationships between immuneparameters and the HPA-axis activity in depressed patients.Psychological Medicine 21, 313]320.
Marazziti, D., Ambrogi, F., Vanacore, R., Mignani, V., Savino,M., Palego, L., Cassano, G.B., Akiskal, H.S., 1992. Immunecell imbalance in major depressive and panic disorders.Neuropsycobiology 26, 23]26.
McDaniel, J.S., Risby, E.D., Stipetic, M., Jevart, R.D., Candle,J., 1991. Natural killer cell activity in patients with panicdisorder. Anxiety 1, 192]195.
Pauli, S., Linthorst, A.C.E., Reul, J.M.H.M., 1998. Tumornecrosis factor-a and interleukin-2 differentially affect hip-pocampal serotoninergic neurotransmission, behavioral ac-tivity, body temperature and hypothalamic pituitary-adren-ocortical axis activity in the rat. European Journal of Neu-roscience 10, 868]878.
Perini, G.I., Zara, M., Carraro, C., Tosin, C., Gava, F., San-tucci, M.G., Valverde, S., De Franchis, G., 1995. Psychoim-munoendocrine aspects of panic disorder. Human Psy-chopharmacology 10, 461]465.
Petitto, J.M., Folds, J.D., Evans, D.L., 1993. Abnormal diurnalvariation of B-lymphocyte circulation patterns in majordepression. Biological Psychiatry 34, 268]270.
Plata Salaman, C.R., 1998. Cytokine action in the brain:Ž .behavioral-molecular interface Abstract . InternationalŽ .Journal of Psychopharmacology 1 Suppl. 1 , S62.
Ramesh, C., Yeragani, V.K., Balon, R., Pohl, R., 1990. Im-munological function in panic disorder patients and con-
Ž .trols. Biological Psychiatry 27 Suppl. A , 65A.Ramesh, C., Yeragani, V.K., Balon, R., Pohl, R., 1991. A
comparative study of immune status in panic disorderpatients and controls. Acta Psychiatrica Scandinavica 84,396]397.
Rapaport, M.H., Stein, M.B., 1994. Serum interleukin-2 andinterleukin-2 receptor levels in generalized social phobia.Anxiety 1, 50]53.
Redmond, D.E., 1986. The possible role of locus ceruleus

( )F. Brambilla et al. r Psychiatry Research 89 1999 21]27 27
noradrenergic activity in anxiety-panic. Clinical Neurophar-macology 9, 40]42.
Robins, L., Helzer, J.E., Cottler, L., Goldring, E., 1989. NIMHDiagnostic Interview Schedule: Version III-R. WashingtonUniversity School of Medicine, St. Louis, MO.
Schleifer, S.J., Keller, S.E., Scott, B.J., Vecchione, J., 1990.Lymphocyte function in panic disorder. Biological Psychia-
Ž .try 27 Suppl. 9A , 66A.Song, C., Connor, T., Merali, Z., Leonard, B.E., Anisman, H.,
1998. Behavioral, neurotransmitter, and endocrine respon-ses to cytokine administrations: the different role of cy-
Ž .tokines in the neuroimmune modulation in rats Abstract .International Journal of Neuropsychopharmacology 1Ž .Suppl. 1 , S63.
Spitzer, R.L., Williams, B.W., 1983. Structured Clinical Inter-view for DSM-III. Upjohn Version. New York State Psychi-atric Institute, New York.
Surman, O.S., Williams, G., Sheehan, D.V., Strom, T.B., Jones,K.J., Coleman, J., 1986. Immunological response to stressin agoraphobia and panic attacks. Biological Psychiatry 21,768]774.
Takamoto, T., Hori, Y., Koga, Y., Toshima, H., 1991. Nore-pinephrine inhibits human natural killer cell activity invitro. International Journal of Neuroscience 58, 127]131.
Tazi, A., Crestani, F., Dantzer, R., 1991. Avesive effects ofcentrally injected interleukin-1. Neuroscience ResearchCommunication 7, 159]165.
Young, M.R.I., Matthews, J.P., Kanabroki, E.L., Sothern, R.B.,Roitman Johnson, B., Scheving, L.E., 1995. Circadianrhythmometry of serum interleukin-2, interleukin-10, tu-mor necrosis factor-alpha and granulocyte]macrophagecolony-stimulating factor in men. Chronobiology Interna-tional 12, 19]27.