Embed Size (px)
Citation preview

65W.C.G. Peh (ed.), Pitfalls in Diagnostic Radiology,DOI 10.1007/978-3-662-44169-5_4, © Springer-Verlag Berlin Heidelberg 2015
Abbreviations
DTPA Diethylenetriaminepentaacetic acid ECG Electrocardiogram FDG F-18 fl uorodeoxyglucose MAA Macroaggregated albumin MDP Methylene diphosphonate MIBG Metaiodobenzylguanidine MUGA Multi-gated acquisition PET Positron emission tomography PET-CT PET computed tomography PET-MRI PET magnetic resonance imaging SPECT Single-photon emission computed
tomography SPECT-CT SPECT computed tomography SUV Standardized uptake value V/Q Ventilation-perfusion
D. C. E. Ng , MBBS, FRCP (Edin) (*) • W. W. C. Lam , MBBS, FRCR • A. S. W. Goh , MBBS, MSc (Nuclear Med) Department of Nuclear Medicine and PET , Singapore General Hospital , Outram Road , Singapore 169608 , Republic of Singapore e-mail: [email protected]; [email protected]; [email protected]
4 Nuclear Medicine Imaging
David Chee Eng Ng , Winnie Wing Chuen Lam , and Anthony Soon Whatt Goh
Contents
4.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . 664.1.1 Single-Photon Imaging . . . . . . . . . . . . . . . . 664.1.2 Positron Emission Tomography . . . . . . . . . . 66
4.2 Types of Pitfalls in Nuclear Medicine Imaging. . . . . . . . . . . . . . . . . . . . 66
4.2.1 Radiopharmaceuticals Pitfalls . . . . . . . . . . . 674.2.2 Technical Pitfalls: Scanning
Procedure and Scanner Factors . . . . . . . . . . 684.2.3 Clinical/Interpretation Pitfalls . . . . . . . . . . . 71
4.3 Pitfalls in SPECT-CT and PET-CT Imaging. . . . . . . . . . . . . . . . . 79
4.3.1 Technical Limitations. . . . . . . . . . . . . . . . . . 794.3.2 Clinical Interpretative Pitfalls . . . . . . . . . . . 80
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 85
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 85

66
4.1 Introduction
Nuclear medicine imaging traces its beginnings from the year 1923 when de Hevesy and Paneth studied the transport of radioactive lead in plants. Since then, the use of radiotracers for studying metabolism has grown into an imaging technique through the use of various kinds of imaging probes and early rectilinear scanners and, later in 1956, through the development of the prototype gamma scanner design by Anger. There was further progress in the design of the gamma scanner, including the introduction of solid-state scanners; further improvement in detector tech-nology and software techniques such as iterative reconstruction; development of single- photon emis-sion computed tomography (SPECT), positron emis-sion tomography (PET); development of hybrid imaging such as SPECT computed tomography (SPECT-CT), PET-CT, and PET magnetic resonance imaging (PET- MRI); as well as concurrent develop-ments in the use of new isotopes, improved cyclotron design, and further radiochemistry and radiopharma-ceutical development. The progress over these many subfi elds has allowed nuclear medicine techniques to probe and image events at the smaller scale, at the cellular and molecular level, and allowed an unprec-edented insight into molecular events that underlie many physiological and pathological processes. Typically, nuclear medicine imaging captures gamma radiation emitted from nuclear processes within isotopes, as well as gamma emissions from annihilation reactions from positron emission from PET isotopes, and even bremsstrahlung radiation from interactions of beta particles with tissues to be imaged.
4.1.1 Single-Photon Imaging
Single-photon imaging uses gamma-emitting radionuclides (isotopes which produce single gamma photon emission at each nuclear disinte-gration) such as Tc-99m, Ga-67, or I-123 pre-pared in the form of radiopharmaceuticals. These radiopharmaceuticals such as Tc-99m MDP, Tc-99m DTPA, or I-123 MIBG can be adminis-tered intravenously, intraperitoneally, orally, or in other ways into the human body. These radio-pharmaceuticals are highly specifi c to cellular
receptors or physiological processes in the body. The biodistribution of such radiotracers is cap-tured by a dedicated gamma scanner for imaging. Data acquisition may be planar or tomographic (SPECT or with SPECT-CT).
4.1.2 Positron Emission Tomography
The principle of PET imaging is based on positron emission. Isotopes which are positron emitters include fl uorine-18, oxygen-15, nitrogen-13, carbon-11, gallium-68, and rubid-ium-82. The most commonly used PET radiopharmaceutical is F-18 fl uorodeoxyglucose (FDG). The administered radionuclide decays due to the emission of a positron which in turn collides with an electron and is annihilated. In the process, by the principle of conservation of energy and momentum, two 511 keV gamma rays originate simultaneously and leave the anni-hilation site in essentially opposite directions. Current ring PET cameras take advantage of the annihilation process for imaging. If two scintilla-tion events are detected simultaneously in two opposed detectors, one assumes that an annihila-tion reaction occurred somewhere on an imagi-nary line (line of action) connecting the two detectors. Various forms of tomographic image reconstruction techniques are used to reconstruct images from these acquired emission data sets.
4.2 Types of Pitfalls in Nuclear Medicine Imaging
In view of the above, pitfalls in nuclear medicine imaging may be technical or clinical in nature and the root problems may be classifi ed under three main categories:• Radionuclide or radiotracer • Scanning techniques, procedure, or scanner
hardware or software issues • Clinical, relating to patient factors and inter-
pretation of scans Reducing artifacts from all these sources is
vital for the correct performance and interpretation of nuclear medicine studies. Distinction of artifacts
D.C.E. Ng et al.

67
from normal variants and pathological entities may be a diffi cult task. If an artifact is not recog-nized during acquisition and interpretation of a study, it can simulate a pathological process and lead to a misdiagnosis. We will discuss some of the major pitfalls in nuclear medicine imaging under the broad headings of radiopharmaceuticals, procedural technique, and clinical/ interpretation. We will also discuss some of the pitfalls encountered in various hybrid imaging techniques such as in SPECT-CT and PET-CT, in terms of CT- related, motion- related, partial-volume-related, and attenuation- related pitfalls.
4.2.1 Radiopharmaceuticals Pitfalls
Radiopharmaceuticals are quality-tested for radionuclidic purity, radiopharmaceutical purity, chemical purity, and biological purity as a general rule, before they can be administered to patients. Even if a radiopharmaceutical has passed qual-ity control, it is possible for radiopharmaceuti-cals to degrade over time or interact with other substances or drugs. Errors in radiopharmaceu-tical preparation may alter biodistribution and may introduce scan artifacts. Clinically impor-tant examples include free dissociated Tc-99m pertechnetate and various kinds of drug interac-tions with radiopharmaceuticals.
4.2.1.1 Free Dissociated Pertechnetate Free dissociated Tc-99m pertechnetate can occur in various labeled radiopharmaceuticals such as Tc-99m diphosphonates or Tc-99m DTPA, partic-ularly after prolonged standing or change in pH. These free Tc-99m pertechnetate ions may give rise to unintended uptake in the thyroid and stomach on routine bone scans (Fig. 4.1 ), renal scans, and V/Q lung scan employing Tc-99m DTPA as the aerosol ventilation tracer. In one report, an unexpected biodistribution of nebulized Tc-99m DTPA was detected after the ventilation of a patient referred for diagnosis of pulmonary embolism. Radiochemical purity testing of the stock vial showed more than 95 % labeling. Further investigation indicated that the problem was possi-bly associated with a cleaning agent used for the nebulizer, leading to the dissociation of the Tc-99m
DTPA (Hinton and Clauss 2011 ). This free dissoci-ated pertechnetate artifact occurs occasionally, and to reduce the occurrence of this artifact, all radio-pharmaceuticals should be used within the time of validity and have proper quality control documen-tation before being used on patients.
4.2.1.2 Drug Interactions with Radiopharmaceuticals
It is well known that various drugs or substances in vivo can cause scan deviations and artifacts. Some of the well-documented interactions are listed below:• In bone scan imaging using Tc-99m diphos-
phonates, it is well known that increased kid-ney uptake of bone tracer and prominent renal visualization can be due to various types of administered cytotoxic drugs such as cispla-tin, doxorubicin, and cyclophosphamide, as well as the presence of aluminum and ferrous ions. Increased liver visualization may be due to iron excess.
• In thyroid imaging using Tc-99m pertechne-tate or I-123 or I-131 iodide, exogenous thy-roxine and high iodine-containing substrates such as intravenous (IV) contrast agents and amiodarone can suppress uptake.
• In I-123 or I-131 MIBG imaging, various drugs are documented to affect the uptake of MIBG. These include tricyclic antidepres-sants, phenothiazines, opiates, calcium chan-nel blockers, and angiotensin-converting enzyme inhibitors (Bomardieri et al. 2010 ).
• For labeling of red blood cells with Tc-99m pertechnetate for MUGA or gastrointestinal bleeding studies, it is known that reduced effi -ciency of red cell labeling has been reported with heparin, tin overload, aluminum, prazo-sin, methyldopa, hydralazine, digoxin, quini-dine, beta-blockers, calcium channel blockers, nitrates, anthracycline antibiotics, and IV contrast agents. In particular, it has been advised that red cell labeling be performed prior to IV contrast administration as labeling effi ciency may be severely affected (Corbett et al. 2006 ).
• For PET imaging, FDG uptake in tumors may be reduced in the presence of high blood glu-cose or use of steroids.
4 Nuclear Medicine Imaging

68
4.2.2 Technical Pitfalls: Scanning Procedure and Scanner Factors
Scan technical factors may give rise to pitfalls in images. These are related to the scanning procedure and scanner and include inadvertent deposition of tracer on parts of the body, cloth-ing, scanner, metallic objects causing attenua-tion artifacts, scanner defects such as defective photomultiplier tube, erroneous setting for pulse height analyzer leading to image degra-dation, counts overfl ow, patient motion arti-facts, attenuation artifacts, presence of other radiotracers, use of inappropriate collimator, poor ECG gating, and misaligned center of rotation. Some of these factors are discussed further below.
4.2.2.1 Unintended Tracer Deposition in Body, Clothing, and Scanner
This is one of the most common pitfalls in nuclear medicine imaging, causing scan artifacts that resemble focal lesions. Deposition of tracer can occur due to inadvertent spray of tracer during injection at an improperly secured injection port or due to urinary contamination or salivary secre-tions. A common occurrence is the appearance of a focal uptake seen in the chest in a radioiodine (I-123 or I-131) whole body scan, in which the abnormality is not to any structural lesion but from a small collection of swallowed activity in the esophagus. Tracer contamination has been observed in the hair, ears, chest wall, abdominal wall, and pelvic regions as well as in the extremi-ties (Fig. 4.2 ). Occasionally, these cause interpre-tive challenges that may have to be resolved by
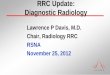
Fig. 4.1 A 65-year-old man with esophageal carcinoma. Tc-99m diphosphonate bone scintiscans done for staging show abnormal soft tissue visualization of the stomach as
well as the thyroid gland, consistent with free dissociated pertechnetate
D.C.E. Ng et al.

69
a b
c
Fig. 4.2 A 33-year-old woman with papillary thyroid carcinoma, status post total thyroidectomy with left neck dissection. Recent neck CT showed left TEG recurrence. Redo left TEG clearance and neck dissection were per-formed. ( a ) Whole body Tc-99m diphosphonate bone
scintiscan shows artifacts due to iodine-131 contamina-tion in the hair, face, and chest. ( b , c ) Subsequent images repeated 1 day later, after washing and cleaning, show much less contamination and disappearance of most of the scan artifacts
re-scanning the patient after the tracer contamination is removed (e.g., by washing). A very common occurrence is the presence of a focus of tracer activity in the extremities, due to slight tracer extravasation at the injection site or a collection in a tortuous vessel. Another scan arti-fact is due to tracer in a long peripheral line or central line that had not been adequately fl ushed with normal saline after tracer injection. This may
occasionally cause confusion in scan interpretation or obscure structures.
4.2.2.2 Metallic Objects Photopenic (photon-defi cient) defects can be seen on the various kinds of nuclear medicine scans, more commonly in bone scans, due to attenuation from metallic or dense objects. These include pacemakers (Fig. 4.3 ), buttons, buckles,
4 Nuclear Medicine Imaging

70
jewelry bangles, coins in pockets, breast prosthe-ses, and orthopedic prostheses. Patients should be informed to remove these objects if clinically possible before the scan is started. Occasionally, they cause confusion with osteolytic lesions or obscure parts of the scan.
4.2.2.3 Patient Motion Artifacts Patient motion may introduce loss of resolution of the image and scan artifacts. This is particu-larly important in myocardial perfusion imaging and renography imaging. Patient motion in a renography study will typically cause artifactual abnormalities on the time-activity curves, and care must be exercised in reducing this possibil-ity. In myocardial perfusion imaging, patient motion may give rise to apparent perfusion defects. Patient motion can be detected by cine displays, sinograms, and summed planar images. There are a number of software algorithms for correcting patient motion, but the best way to
avoid this pitfall is to be aware of its possible occurrence and minimize patient motion or to repeat the study if suspected.
4.2.2.4 Presence of Other Tracers Occasionally, a patient may have performed two nuclear medicine imaging studies within a short period of time, such that the images super-impose. This produces the occasional unusual scan appearance that can be misleading. For example, a Tc-99m diphosphonate bone scan that is performed within 24 h of a myocardial perfusion imaging using Tc-99m sestamibi will show apparent cardiac, hepatic, thyroid, and bowel uptake of “bone” tracer. Sometimes, when a bone scan is performed 1 week after a patient has received therapeutic activity of I-131 for thyroid remnant ablation, the high energy photons of iodine-131 will cause septal penetration and obscure the Tc-99m bone scan image.
a b Fig. 4.3 A 74-year-old woman with left breast carcinoma, status post simple mastectomy and axillary clearance. ( a ) Tc-99m diphosphonate bone scintiscan shows a photopenic defect over the left upper chest wall that is due to a pacemaker. ( b ) The corre-sponding chest radiograph confi rms presence of the pacemaker
D.C.E. Ng et al.

71
4.2.2.5 Misalignment of the Center of Rotation in SPECT
Center of rotation error occurs when the point of reference used by the scanner in reconstructing images is not aligned with the mechanical axis of the SPECT scanner. If the center of rotation is properly calibrated, a radioactive point source placed at the center of the camera orbit should proj-ect to the center of the reconstructed image. Errors of misalignment of the center of rotation may man-ifest as areas of reduced counts or ring artifacts which may mimic true defects. It is important for nuclear medicine technologists to properly cali-brate the center of rotation for the scanner on a rou-tine basis as a quality control procedure.
4.2.3 Clinical/Interpretation Pitfalls
Clinical/interpretation pitfalls include failure to recognize variation of normal (including age-related normal variations), effects due to clinical conditions (such as right–left systemic shunt, ectopic organs, or presence of other concomitant disorders) or drugs, effects due to prior treatment such as radiotherapy and chemotherapy (such as fl are response), and specifi c interpretative false- positives and false-negatives in various types of nuclear medicine imaging.
4.2.3.1 Age-Related Factors (Including Children)
Nuclear medicine imaging in the young can be fraught with subtleties. For example, bone scans in the young up to 20 years old typically demonstrate increased epiphyseal plate activity, and this requires care in interpretation as some of these may mimic trauma or conceal subtle changes of trauma. In younger subjects, increased tracer uptake at the manubriosternal junction is often a normal variant. In some patients, a small photopenic defect in the inferior aspect of the sternal body due to incomplete fusion of the cartilaginous bars can be seen. This photopenic area, called the sternal foramina, is typically surrounded by uniform radioactivity and should not be mistaken for an osteolytic lesion. Horizontal lines of uptake in the sternal body can
also be seen in younger subjects, and these are often very uniform, regular spaced, and are in keeping with bone fusion centers in a growing sternum.
Radiotracer changes due to degeneration can often be seen in the older subjects. Focal irregularities in uptake of bone tracer can be seen at the knees due to osteoarthritis or in the lumbar spine due to spondylosis. They tend to have usual appearance of distribution at the joint surfaces and at the margins of the vertebrae or facet joints. Most of these pattern if equivocal on planar imaging can be further characterized with SPECT-CT.
The uptake of FDG or radiotracers for cere-bral amyloid imaging by the cerebral hemi-spheres and deep cerebral structures may show age-related changes, and experience and care should be exercised. Cortical FDG uptake decreases with age, particularly in the frontal lobes. In contrast, metabolic activity of the basal ganglia, visual cortices, and cerebellum remains unchanged. The normal thymus may be visual-ized on a routine FDG PET-CT as an FDG-avid anterior mediastinal mass in a young person. Occasionally, the normal thymus or lactating breasts can be visualized on the I-123/I-131 whole body scan (Fig. 4.4 ).
4.2.3.2 Right–Left Systemic Shunt In V/Q lung scanning, the radiotracers used are typically Xe-133 gas, Tc-99m Technegas, or Tc-99m DTPA aerosol for ventilation and Tc-99m MAA for perfusion. The particle size for Tc-99m MAA is usually 20–80 μm and largely trapped in the pulmonary capillary vas-culature. Only less than 4 % of administered MAA activity escapes into the systemic circula-tion. This small amount of radioactivity is usu-ally not visually detectable. Routinely, minimal or no kidney activity is visualized in both the ventilation and perfusion images. The visual-ization of the kidney, thyroid, and brain cere-bral hemispheres after the injection of Tc-99m MAA is thus highly indicative of a right–left systemic shunt. Care must be taken in attribut-ing thyroid and kidney uptake to systemic shunting as these may be seen if free pertechnetate is present.
4 Nuclear Medicine Imaging

72
4.2.3.3 Ectopic Locations Ectopic organs are potential sources of inter-pretation errors. Examples include ectopic thy-roid gland in the lingual or hyoid position (Fig. 4.5 ), ectopic kidney in the pelvis, and ectopic parathyroid adenomas in the mediasti-num. A transplanted kidney seen in the iliac fossa can be missed or mistaken for bone pathology (Fig. 4.6 ).
4.2.3.4 Clinical Conditions Causing Possible Interpretative Errors During Bone Scans
Extraosseous Uptake For bone scans, extraosseous uptake can occa-sionally be identifi ed and is important for correct interpretation. Common causes of extraosseous uptake have been well tabulated by Gnanasegaran et al. ( 2009 ). Foci of soft tissue bone tracer uptake
Fig. 4.4 A 27-year-old woman with papillary thyroid carci-noma with nodal metastases, status post total thyroidectomy, central neck and right modifi ed radical neck dissection. She was 3 months’ postpartum when this post- therapy whole
body Tc-99m diphosphonate bone scintiscan was performed and had stopped breastfeeding for at least 1 month prior. The images show I-131 uptake projected over the chest due to lactating breast uptake
D.C.E. Ng et al.

73
causing interpretive diffi culties may be caused by non-osseous metastases from osteosarcoma and liposarcoma or even in primary tumors such as breast carcinoma. Additionally, extraosseous uptake of bone tracer may occasionally cause interpretative pitfalls and diffi culties, including:• Cardiac focal uptake – caused by myocardial
necrosis, myocardial contusion, ventricular aneurysm, and diffuse uptake can be seen in amyloidosis, hypercalcemia, alcoholic cardio-myopathy, and pericarditis.
• Skeletal muscle uptake can be observed in trauma, excessive muscular activity, polymyo-sitis, dermatomyositis, scleroderma, and het-erotopic ossifi cation after trauma or paralysis.
• Renal uptake can be observed following cyto-toxic chemotherapy such as vincristine, doxo-rubicin, and cyclophosphamide and in
nephrocalcinosis, hypercalcemia, iron over-load, and sickle cell disease.
• Gastric uptake can be seen in hypercalcemia or gastric tumor (Fig. 4.7 ).
• Liver uptake can be seen in conditions where there is increased iron deposition in the liver, such as hemochromatosis and secondary hemosiderosis from thalassemia major, as well as with hepatic metastases (Fig. 4.8 ) and primary hepatic neoplasms.
Bone Scan Flare Response A fl are response typically described in a bone scan is a transient increase in tracer uptake in the bone lesions previously seen or even appearance of new bone lesions due to early response of the bone metastases to systemic hormonal therapy or chemo-therapy. Typically described for breast and prostate
a b
Fig. 4.5 ( a ) Anterior and lateral planar Tc-99m pertech-netate images show absence of thyroid gland in the usual anatomic position. However, there is a midline upper neck focal uptake (seen between the submandibular glands) which is abnormal. This appearance of focal Tc-99m
pertechnetate uptake in this location is highly indicative of ectopic thyroid (lingual or hyoid thyroid). ( b ) SPECT-CT image shows the submental nodule with tracer uptake, suggestive of a hyoid thyroid
4 Nuclear Medicine Imaging

74
Fig. 4.6 Tc-99m diphospho-nate bone scintiscans show a transplanted kidney in the right iliac fossa, partially obscuring the right iliac bone and appearing as a tracer- avid focus. There is also non-visualization of the native kidneys likely related to renal failure, bilateral femoral pros-theses, and spondylitic changes in the lumbar spine
D.C.E. Ng et al.

75
cancer, the increase in tracer uptake mimics disease progression, but it is due to a bone healing response in which increased osteoblastic reaction is seen. This fl are response may last as long as 6 months post-therapy, and subsequent bone scanning will demonstrate bone metastatic disease improvement rather than disease progression.
Malignant Lesions Causing Photopenic Lesions A subtle pitfall in bone scans can be caused by photopenic lesions, which can be missed due to the relative lack of bone tracer uptake. Such malignant lesions are generally predominantly osteolytic lesions, found in multiple myeloma (Fig. 4.9 ) and some bone metastases from thyroid carcinoma, renal cell carcinoma (Fig. 4.10 ),
hepatocellular carcinoma, lung carcinoma, and breast carcinoma.
4.2.3.5 Possible Interpretative Errors During Thyroid Scans
Various factors may affect the interpretation of thyroid scintigraphy using Tc-99m pertechnetate. Subacute thyroiditis in the destructive phase tends to show a decreased tracer uptake, but a reduced uptake may be caused by iodine excess due to drugs like amiodarone or IV contrast agents or exogenous thyroxine or iodide. Other drugs are known to suppress iodine uptake on thyroid scintigraphy, such as steroids, bromides, carbimazole, propylthiouracil, perchlorate, nitrates, salicylates, and sulfonamides. Prior administration of iodinated IV contrast agents
Fig. 4.7 Tc-99m diphosphonate bone scintiscans show skeletal metastases, with visualization of the stomach in the left lumbar region and mild diffuse uptake seen within
the thorax. This soft tissue uptake in the stomach of bone tracer (together with diffuse lung uptake) is typical of hypercalcemia
4 Nuclear Medicine Imaging

76
a b
Fig. 4.8 A 54-year-old woman with carcinoma of the sigmoid colon and liver metastases. ( a ) Tc-99m diphos-phonate bone scintiscan shows soft tissue uptake pro-jected over the right hypochondrium seen on the anterior
and posterior views, in keeping with hepatic metastatic uptake of bone tracer. ( b ) CT image of the abdomen shows the corresponding hepatic metastases
may block radionuclide uptake for as long as 2 months. Renal failure may also reduce uptake.
4.2.3.6 Possible Interpretative Errors During Renography
Pitfalls in interpretation may arise in renography when an apparent obstructive pattern of tracer stasis and prolonged excretion is seen in cases of inadequate hydration and diuresis, a fl accid pel-vicalyceal system without obstruction, or a
bladder back pressure effect. One must also be aware of ectopic or duplex kidneys in the inter-pretation of the scan images as well as on the analyses of the time-activity curves.
4.2.3.7 Possible Interpretative Errors During Radionuclide GIT Imaging
In Meckel’s diverticulum imaging with Tc-99m pertechnetate, one should be aware of the follow
D.C.E. Ng et al.

77
a
b
Fig. 4.9 Multiple myeloma gives rise to predominantly osteolytic bone lesions and does not produce increased uptake on the Tc-99m diphosphonate bone scintiscan. ( a ) CT image of the pelvis shows multiple osteolytic lesions in the iliac bones and sacrum. ( b ) Tc-99m diphosphonate
bone scintiscans show no corresponding abnormal increased uptake in the bony pelvis. The areas of uptake seen in the thoracic spine and ribs are likely to be related to fractures. One should be careful in the interpretation of the bone scintiscan if myeloma is suspected
4 Nuclear Medicine Imaging

78
a
b
Fig. 4.10 “Cold” or photopenic lesions are a potential source of pitfalls in nuclear medicine imaging. ( a ) Tc-99m diphosphonate bone scintiscans show a “cold” lesion in
the midsternum. ( b ) CT image shows the corresponding osteolytic sternal lesion due to renal cell carcinoma metastasis
D.C.E. Ng et al.

79
ing possible false-positives, namely, ureteric activity and intussusception. In gastrointestinal bleeding imaging with labeled red blood cells, false-positives may be caused by arteriovenous malformations and endometrial activity. Some of these false-positives can be reduced through the use of hybrid imaging with fusion CT providing anatomic correlation.
4.3 Pitfalls in SPECT-CT and PET-CT Imaging
SPECT-CT and PET-CT have expanded rapidly because they combine sensitive imaging modal-ity (SPECT and PET) with high-resolution imaging modality (CT). There are several poten-tial pitfalls of these hybrid imaging modalities (van Dalen et al. 2007 ).
4.3.1 Technical Limitations
4.3.1.1 Partial Volume and Motion Pitfalls
SPECT-CT and PET-CT are limited in evaluation of small lesions, especially those less than 1 cm in size. Lesion detectability is dependent upon the degree of tracer uptake, size, and location being increased in areas with minimal motion (e.g., ret-roperitoneum) and minimal background activity (e.g., lungs) as well as on hardware characteristics (such as system resolution, time of fl ight) and image reconstruction algorithms (Reinhardt et al. 2006 ; Bamba et al. 2011 ; Mayerhoefer et al. 2012 ). In hybrid imaging such as SPECT-CT, PET-CT, and PET-MRI, the position of the dia-phragm on the SPECT or PET emission images should match as closely as possible that on the CT transmission images. Although a diagnostic CT scan of the chest typically is acquired during end-inspiration breath-holding, this technique is not optimal for SPECT-CT or PET-CT because SPECT or PET data is acquired throughout a period of several minutes, which then averages
out the respiratory motion, leading to substantial respiratory motion misregistration on PET and CT images (Goerres et al. 2002 ).
Some facilities perform CT transmission scans during breath-holding at mid-inspiration volume, while others prefer that the patient con-tinues shallow breathing during the CT acquisi-tion. Respiratory motion results in inaccurate localization of lesions at the base and periphery of the lungs, in the dome of the liver, or near any lung–soft tissue interface and may result in spuri-ous standardized uptake value (SUV) determina-tions. Motion correction or respiratory gating is recommended when available (Delbeke et al. 2006 ). Patient motion during SPECT-CT and PET-CT acquisition may lead to spurious local-ization of uptake, especially in the head and neck region. However, most of the instances of patient motion artifacts can be recognized by proper instruction to patients and careful interpretation of images (Osman et al. 2003 ).
4.3.1.2 Attenuation Artifacts Due to the use of CT-based attenuation correction, unusual high-density areas easily produce attenu-ation artifacts in PET imaging. Typically these artifacts are seen at areas of high radiographic density, e.g., barium, iodinated contrast material, and metal (Bujenovic et al. 2003 ; Cohade et al. 2003 ). For instance, at the hip joint, these could potentially mimic prosthesis infection. Dense barium in the colon could raise the possibility of false- positive tumor localization. Due to high photon absorption, metallic implants such as dental fi llings or hip prosthetics also generate streaking artifacts on CT images that may obscure underlying structures. Awareness of these possible artifacts is the fi rst step in dealing with them. In some cases, it is useful to use PET images that are not corrected for attenuation (uncorrected PET) for correlation. In modern PET-CT scanners, this presence of dense material is less likely to cause diagnostic dilemma on the PET image if interpreted with information obtained from the companion CT.
4 Nuclear Medicine Imaging

80
4.3.2 Clinical Interpretative Pitfalls
4.3.2.1 Normal Variants and Benign Processes on FDG-PET and PET-CT Imaging
Some infl ammatory processes can be highly visible on FDG-PET because the activated white cells (particularly granulomatous pathologies such as Mycobacterium tuberculosis infections, fungal infections, sarcoidosis) have increased glycolysis. It is not possible to list all potential nonneoplastic causes of FDG uptake. Common benign fi ndings include crossed cerebellar diaschisis (Fig. 4.11 ) and brown fat causing increased FDG uptake mim-icking muscle activity or malignancy. Correlation with clinical data should alert the interpreter to false-positive fi ndings, e.g., prominent diffuse tracer uptake in breasts during lactation and uptake at surgical scar/granulation tissue.
4.3.2.2 Limited Accuracy for Some Histologic Types on FDG-PET and PET-CT Imaging
There are malignant disease processes where FDG PET-CT has either or both relatively
poorer sensitivity and poorer specifi city, for example, prostate cancer, signet ring cell carci-nomas, and mucinous carcinomas (Yoshioka et al. 2003 ; Kim et al. 2006 ). Low FDG uptake is of limited value in differentiating benign from malignant soft tissue tumors because it could represent either a nonmalignant lesion or low-grade sarcoma. Of note is the interpretation of liposarcomas, which tend to give rise to hetero-geneous uptake of FDG – with minimal FDG uptake in areas of low cellularity and high adi-posity and higher uptake in more solid components.
4.3.2.3 Possible False-Positive Findings on FDG-PET (Nonmalignant Uptake)
These are some of the potential diffi culties in the interpretation of FDG-PET or PET-CT. The information obtained from the CT component of the PET-CT is often very useful to help in clarify-ing these potential pitfalls.
Normal Structures Head and neck
a b
Fig. 4.11 Crossed cerebellar diaschisis. Axial PET-CT images show ( a ) decreased FDG activity in the left frontopari-etal lobe secondary to ( b ) infarct causing a functional decrease in right cerebellar metabolism
D.C.E. Ng et al.

81
• Lymphoid tissues in the head and neck such as in the posterior nasopharynx and tonsils
• Brown adipose tissue (Fig. 4.12 )• Skeletal and smooth muscles (e.g., scale-
nus anterior or sternomastoid muscles, hyperinsulinemia)
• Cricoarytenoid articulation Chest
• Thymus, especially in the young or post- chemotherapy, thymic rebound hyperplasia
• Lactating breast (Fig. 4.13 )• Refl ux esophagitis
Abdomen/pelvis• Bowel activity (which can cause confusion
with serosal deposits) • Urinary tract structures (ureters) • Female genital tract (e.g., endometrial uptake
during menstruation or corpus luteum cyst)
Infl ammatory Processes • Postsurgical infl ammation, infection, biopsy
site, and stitch granuloma (Fig. 4.14 )• Postirradiation (e.g., radiation pneumonitis) • Local infl ammatory disease, especially granu-
lomatous processes (e.g., sarcoidosis, fungal disease, or mycobacterial disease)
• Stoma site (e.g., trachea or colon) and drain-age tubes
• Injection site including long lines or chemoports • Thyroiditis or Graves disease
Benign Lesions • Thyroid follicular adenoma • Colonic hyperplastic polyps • Leiomyoma/fi broids • Bone marrow hyperplasia (e.g., anemia or
cytokine therapy) • Fibrous dysplasia or Paget disease• Benign salivary gland tumors
4.3.2.4 Possible False-Negative Findings on FDG-PET (Malignant Uptake)
Some possible causes of false-negative fi ndings on FDG-PET images include: small size of the lesions (typically <0.5 cm), recent chemotherapy
or radiotherapy suppressing uptake, recent high-dose steroid therapy, hyperglycemia and hyperinsulinemia reducing uptake, lesions occur-ring in sites with normal uptake such as brain metastases.
Certain tumors which are low grade, low FDG avidity, or large mucinous components include:• Small lymphocytic lymphoma or low-grade
follicular lymphomas • Some hepatocellular carcinomas, especially
well-differentiated tumors • Some mucinous gastric or colorectal carcino-
mas (Figs. 4.15 and 4.16 )• Some prostate carcinoma, especially well-
differentiated tumors (Fig. 4.17 )• Some neuroendocrine tumors, especially
well-differentiated tumors • Some thyroid carcinomas, especially well-
differentiated tumors • Some bronchioloalveolar or low-grade lung
adenocarcinoma • Some lobular carcinomas of the breast • Some sarcomas, such as low-grade liposarcoma• Astrocytoma and low-grade gliomas
4.3.2.5 Gallium-68 DOTA-Peptide PET-CT
Increased uptake can be seen in normal structures such as the uncinate process of the pancreas or in infl ammatory lesions, fractures, or benign lesions such as meningiomas.
4.3.2.6 Pitfalls in SUV Measurements The SUV is the measured activity at the region of interest which is normalized for body weight/surface area and injected activity. This semiquan-titative estimation of tumor glucose metabolism is based on relative lesion radioactivity, measured on images corrected for attenuation and normal-ized for the injected dose and body weight, lean body mass, or body surface area (Thie 2004 ). This measurement is obtained on a static emis-sion image typically acquired more than 45 min after injection. SUV can be affected by patient size, time of measurement relative to the injection of the tracer, plasma glucose levels, partial
4 Nuclear Medicine Imaging

82
Fig. 4.12 Axial PET-CT and matching CT images show brown fat FDG uptake in the neck, axillae, mediastinum and posterior intercostal spaces, suprarenal and paracolic regions, and perirenal fat
D.C.E. Ng et al.

83
Fig. 4.13 Prominent diffuse FDG uptake is seen in the breasts during lactation
4 Nuclear Medicine Imaging

84
a b
Fig. 4.14 ( a , b ) Axial PET-CT images show a new hypermetabolic soft tissue nodule at the surgical site after resection of an umbilical neuroendocrine tumor.
Subsequent excision biopsy of this nodule showed granu-lation tissue with foreign body giant cell reaction to suture material on histology
Fig. 4.15 Poorly differentiated gastric adenocarcinoma with signet ring cells. Axial PET-CT image shows no sig-nifi cant FDG uptake in the primary gastric cancer area of wall thickening in the distal stomach. Signet ring cell car-cinomas have low FDG uptake
a b
Fig. 4.16 Axial PET-CT image shows low FDG uptake in a liver metastasis from mucinous colonic carcinoma. ( a ) There is paucity of uptake in the hepatic metastasis in
the right lobe, despite ( b ) the relatively large lesion seen on the corresponding unenhanced CT image
D.C.E. Ng et al.

85
volume effects, extravasation of the injected activity, attenuation correction, and reconstruc-tion algorithms (Schoder et al. 2004 ). The repro-ducibility of SUV measurements depends on the
reproducibility of clinical protocols, for example, dose activity administered, time of imaging after 18F-FDG administration, type of reconstruction algorithms, type of attenuation maps, size of the region of interest, changes in uptake by organs other than the tumor, respiratory motion, and methods of analysis (e.g., maximum and mean SUV). In one study showing the effect of respi-ratory motion on SUV measurements, in 206 lung lesions in 155 subjects, the mean SUVmax value was 5.2 ± 5.1 SD on standard 3D PET-CT imaging, whereas the SUVmax value on 4D respiratory gated PET-CT imaging was 6.8 ± 6.1 ( p < 0.0001), with an average percentage increase of 30.8 % (Guerra et al. 2012 ). When SUV mea-surements are used for comparison, potential pit-falls in interpretation can occur if the acquisition parameters are signifi cantly different between studies.
Conclusion
Some of the major pitfalls in nuclear medicine imaging described here should be recognized and care taken to avoid them in the perfor-mance and interpretation of nuclear medicine imaging. As nuclear medicine imaging encompasses numerous kinds of radiochemi-cal/radiopharmaceutical techniques, complex image acquisition, and processing and recon-struction methodologies in order to obtain accurate clinical information in the context of physiological and pathological conditions, it is imperative that the nuclear medicine physi-cian is aware of the different sources of error and ensures that these pitfalls are reduced to the minimum.
References
Bamba Y, Itabashi M, Kameoka S (2011) Value of PET/CT imaging for diagnosing pulmonary metastasis of colorectal cancer. Hepatogastroenterology 58:1972–1974
Bomardieri E, Giammarile F, Aktolun C et al (2010) 131I/123I Metaiodobenzylguanidine (mIBG) scintig-raphy: procedure guidelines for tumor imaging. Eur J Nucl Med Mol Imaging 37:2436–2446
a
b
Fig. 4.17 ( a ) Axial PET-CT image shows low FDG avid-ity of a prostate carcinoma in the left peripheral zone of the prostate gland. Most primary prostate cancers have low FDG uptake. ( b ) PET MIP image shows multiple hypermetabolic bone metastases involving the spine, ribs, bony pelvis, and right proximal femur. FDG PET is more likely to detect distant metastases than local disease
4 Nuclear Medicine Imaging

86
Bujenovic S, Mannting F, Chakrabarti R et al (2003) Artifactual 2-Deoxy-2-[18F]Fluoro-D-glucose local-ization surrounding metallic objects in a PET/CT scanner using CT-based attenuation correction. Mol Imaging Biol 5:20–22
Cohade C, Osman M, Nakamoto Y et al (2003) Initial experience with oral contrast in PET/CT: phantom and clinical studies. J Nucl Med 44:412–416
Corbett JR, Akinboboye OO, Bacharach SL et al (2006) Equilibrium radionuclide angiography. J Nucl Cardiol 13:e56–e79
Delbeke D, Coleman RE, Guiberteau MJ (2006) Procedure guideline for tumor imaging with 18F-FDG PET/CT 1.0. J Nucl Med 47:885–895
Gnanasegaran G, Cook G, Adamson K et al (2009) Patterns, variants, artifacts, and pitfalls in conventional radionuclide bone imaging and SPECT/CT. Semin Nucl Med 39:380–395
Goerres GW, Kamel E, Seifert B et al (2002) Accuracy of image coregistration of pulmonary lesions in patients with non-small cell lung cancer using an integrated PET/CT system. J Nucl Med 43:1469–1475
Guerra L, De Ponti E, Elisei F et al (2012) Respiratory gated PET/CT in a European multicentre retrospective study: added diagnostic value in detection and charac-terization of lung lesions. Eur J Nucl Med Mol Imaging 39:1381–1390
Hinton PJ, Clauss RP (2011) Dissociation of Tc-99m DTPA in a nebulizer. Nucl Med Comm 32:659–661
Kim SK, Kang KW, Lee JS et al (2006) Assessment of lymph node metastases using 18F-FDG PET in patients
with advanced gastric cancer. Eur J Nucl Med Mol Imaging 33:148–155
Mayerhoefer ME, Prosch H, Herold CJ et al (2012) Assessment of pulmonary melanoma metastases with 18F-FDG PET/CT: which PET-negative patients require additional tests for defi nitive staging? Eur Radiol 22:2451–2457
Osman MM, Cohade C, Nakamoto Y et al (2003) Clinically signifi cant inaccurate localization of lesions with PET/CT: frequency in 300 patients. J Nucl Med 44:240–243
Reinhardt MJ, Wiethoelter N, Matthies A et al (2006) PET recognition of pulmonary metastases on PET/CT imaging: impact of attenuation-corrected and non- attenuation corrected PET images. Eur J Nucl Med Mol Imaging 33:134–139
Schoder H, Erdi YE, Chao K et al (2004) Clinical implica-tions of different image reconstruction parameters for interpretation of whole-body PET studies in cancer patients. J Nucl Med 45:559–566
Thie JA (2004) Understanding the standardized uptake value, its methods and implications for usage. J Nucl Med 45:1431–1434
van Dalen JA, Vogel WV, Corstens FH et al (2007) Multi- modality nuclear medicine imaging: artefacts, pitfalls and recommendations. Cancer Imaging 7:77–83
Yoshioka T, Yamaguchi K, Kubota K et al (2003) Evaluation of 18F-FDG PET in patients with advanced, metastatic or recurrent gastric cancer. J Nucl Med 44:690–699
D.C.E. Ng et al.