Embed Size (px)
Citation preview
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 1
TM
August 9th, 2019
#POFPS44
Dennis J. Dowling, D.O., FAAO
Director of Manipulative Medicine Services
Department of Physical Medicine & Rehabilitation
Family Medicine Department
Nassau University Medical Center
East Meadow, New York
Director of OMM Assessment
COMLEX-Level 2 PE
National Board of Osteopathic Medical Examiners
Chair of POCKET Project
Former Professor & Chairman
Stanley Schiowitz, D.O., FAAO
Department of
Osteopathic Manipulative Medicine
New York College of Osteopathic Medicine
New York Institute of Technology
#POFPS44
I HAVE NOTHING to DECLARE
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 2
No OFF-Label uses will be discussed
(and probably no ON-Label uses as well).
#POFPS44
Disclosure: I Have No Financial Interests
#POFPS44
PINSA Method of Finding
and
Treating Osteopathic Key Lesions
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 3
TIGHTER
RESTRICTED
PART
LOOSER MORE
NOTICEABLE END
#POFPS44
progressive inhibition of neuromuscular structures
(PINS), a system of diagnosis and treatment in which the osteopath locates two related points and sequentially applies inhibitory pressure along a series of related points between the two points.
2.Developed by Dennis Dowling,DO.
GLOSSARY OF OSTEOPATHIC TERMINOLOGY
osteopathic manipulative treatment (OMT):
#POFPS44
DOWLING’S
UNIVERSAL
METHOD of
BALANCING
DUMB
DOWLING’S
UNIVERSAL
METHOD of
BALANCING
TECHNIQUE#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 4
PROGRESSIVE
INHIBITION of
NEUROMUSCULAR
STRUCTURES
PINS
PROGRESSIVE
INHIBITION of
NEUROMUSCULAR
STRUCTURES
#POFPS44
MAY 2000 JAOA
http://www.aoa-net.org/Publications/JAOA/fulltext/500dowling.pdf
#POFPS44
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 5
#POFPS44
#POFPS44
PROGRESSIVE
INHIBITION of
NEUROMUSCULAR
STRUCTURES
PINS?
OSKELETAL FA
SC
IAL
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 6
How does one apply
Osteopathic
Manipulative
Medicine?
#POFPS44
Use your
knowledge of
STRUCTURE
&
FUNCTION.
#POFPS44
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 7
Hey, Doc, I told you
the pain was on the
right!
#POFPS44
#POFPS44
SS SYMPTOM
WHEN YOU GET STUCK…
… Don’t just look
at the symptom…
… LOOK FOR THE
CAUSE…
… and determine the
connection.
Ah,ha!
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 8
HEADACHE#POFPS44
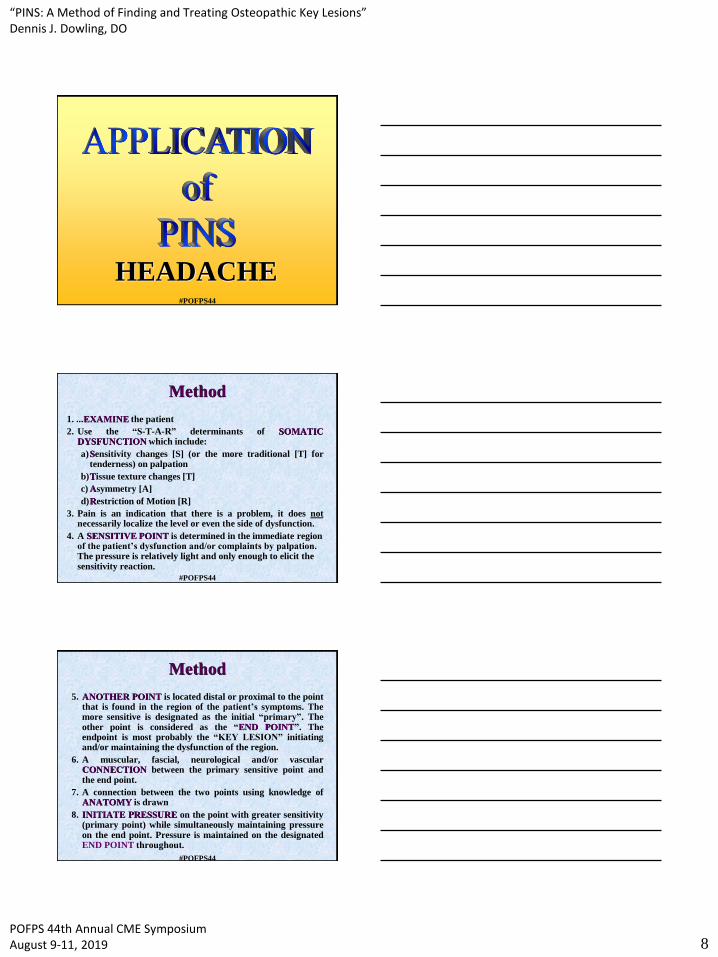
Method
1. ...EXAMINE the patient
2. Use the “S-T-A-R” determinants of SOMATICDYSFUNCTION which include:
a)Sensitivity changes [S] (or the more traditional [T] fortenderness) on palpation
b)Tissue texture changes [T]
c) Asymmetry [A]
d)Restriction of Motion [R]
3. Pain is an indication that there is a problem, it does notnecessarily localize the level or even the side of dysfunction.
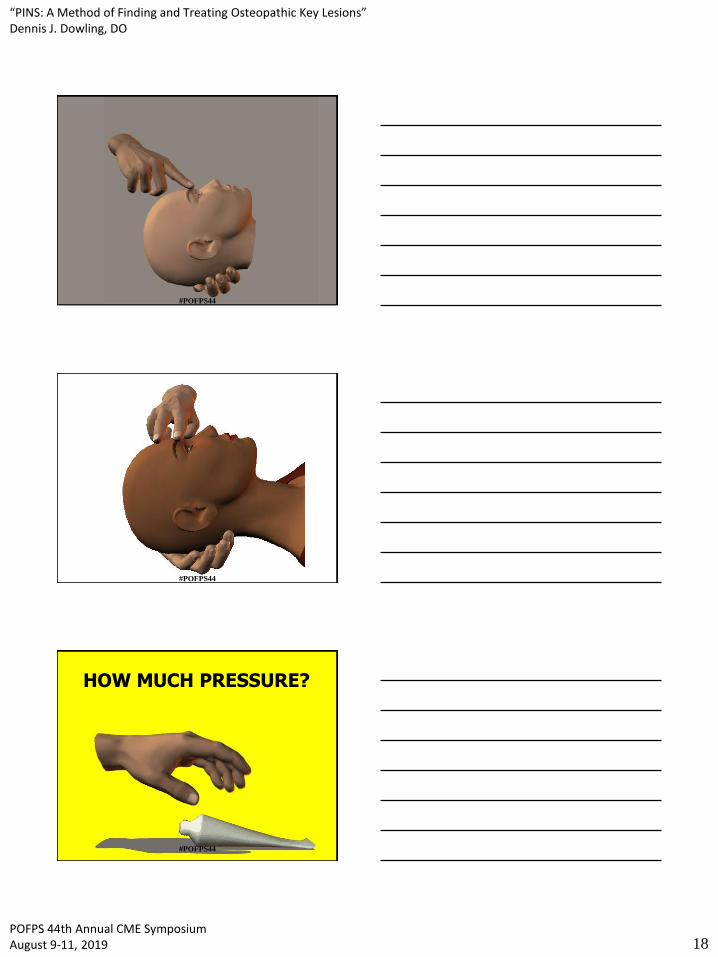
4. A SENSITIVE POINT is determined in the immediate region of the patient’s dysfunction and/or complaints by palpation. The pressure is relatively light and only enough to elicit the sensitivity reaction.
#POFPS44
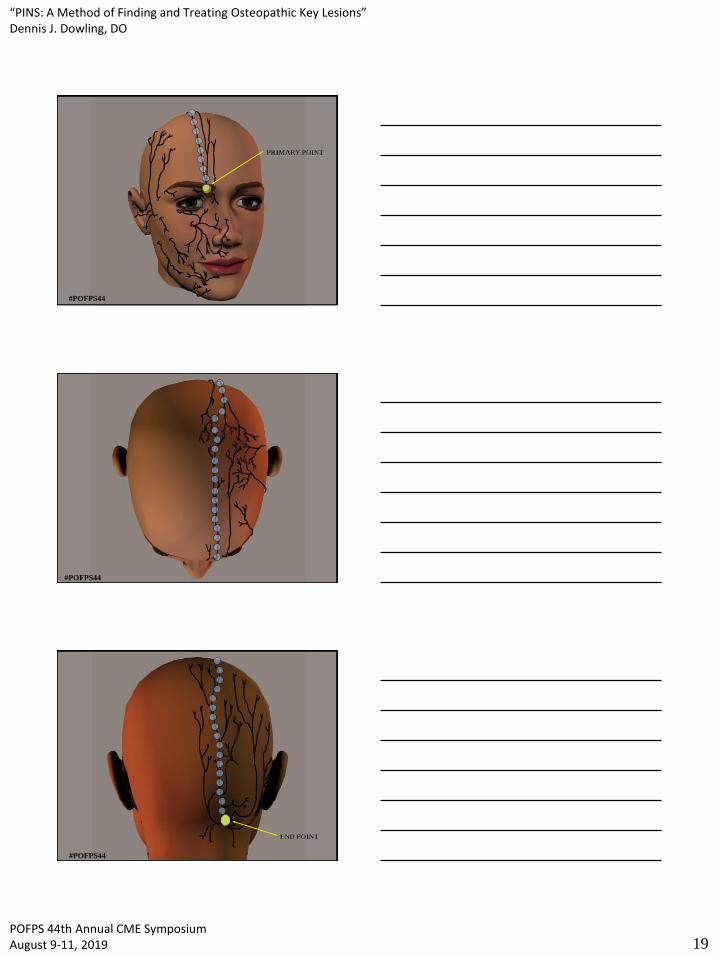
5. ANOTHER POINT is located distal or proximal to the pointthat is found in the region of the patient’s symptoms. Themore sensitive is designated as the initial “primary”. Theother point is considered as the “END POINT”. Theendpoint is most probably the “KEY LESION” initiatingand/or maintaining the dysfunction of the region.
6. A muscular, fascial, neurological and/or vascularCONNECTION between the primary sensitive point andthe end point.
7. A connection between the two points using knowledge ofANATOMY is drawn
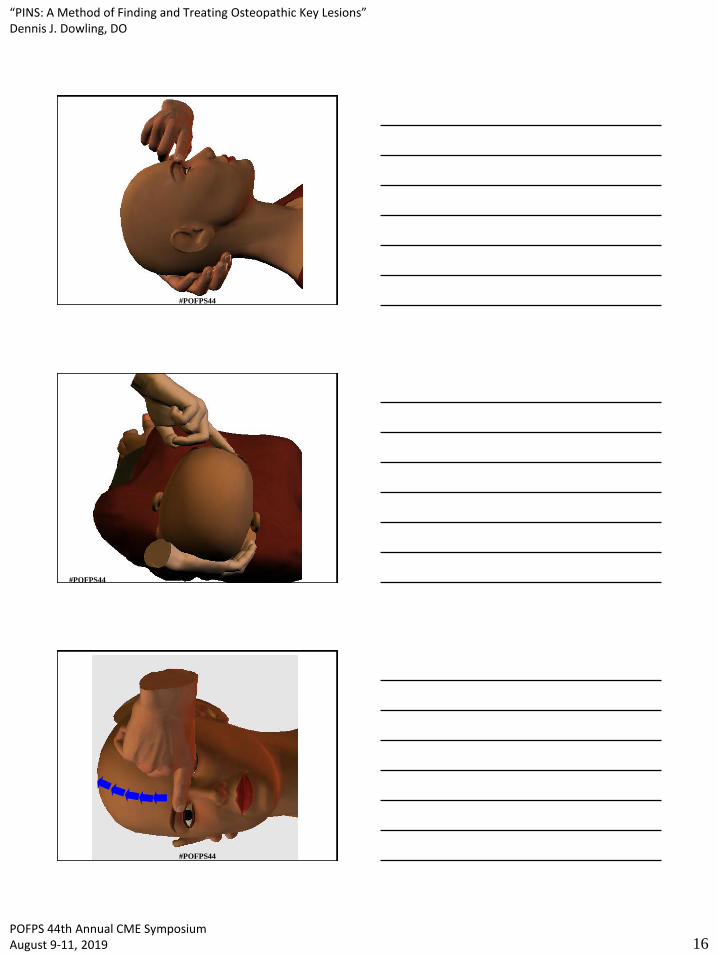
8. INITIATE PRESSURE on the point with greater sensitivity(primary point) while simultaneously maintaining pressureon the end point. Pressure is maintained on the designatedEND POINT throughout.
Method
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 9
9. The patient notes the initial amount of sensitivity (there willusually be a transient initial increase followed bysubsequent decreases).
10. After approximately 20-30 seconds, pressure issimultaneously placed on a NEW LOCATIONapproximately 2-3 centimeters from the primary point inthe direction of the end point. This can sometimes bedetermined by a subtle increase in subcutaneous tension, aslight twitch, or a pulsation.
11. EQUAL PRESSURE is exerted onto both the primary andsecondary points.
12. The patient is determines which of the two points(“PRIMARY” VS. “SECONDARY”) IS MORESENSITIVE.
Method
#POFPS44
13. If there is difficulty in determining a new secondary point:
– Sweep the area in an arc 30-45° at a distance 2-3 cms from the primary point to determine a secondary point;
– When the patient can not determine that there are two points being pressed,;
– When the two points elicit the same sensitivity, release the primary and maintain pressure on the secondary point
14.The process is continued until the last “secondary” point is two centimeters from the end point. THE ENDPOINT HAS RECEIVED INHIBITION THROUGHOUT.
15. Frequently, a point may be located approximately halfway between the initial primary point and the endpoint that is exquisitely sensitive and may appear to reinitiate the chief complaint symptoms or radiate to the primary point. This actually is an indicator that there was dysfunction of all of the involved tissues and not just the area of chief complaint. It also indicates excellent prognosis for success with the treatment.
Method
#POFPS44
16. Once the final two points are being inhibited, the physician can determine the amount of tension that persists at the end point location. The end point may not have greatly decreased in intensity, or it may have discontinued in sensitivity altogether.
17. If the endpoint remains persistent, the physician can choose to treat the residual component in whatever manner he wishes. PINS technique can be the sole approach to the dysfunctions that were found or can be used in conjunction with any modality of osteopathic manipulative treatment
18. The somatic dysfunction is REASSESSED.
19. The patient is advised that, despite the relative comfort of the treatment, there may be a post-treatment reaction. These can include transient soreness, aches, and fatigue. Bruising can occur in patients who are prone to this or if excessive pressure has been used. Generally, all of these will resolve in 24 to 48 hours.
Method
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 10
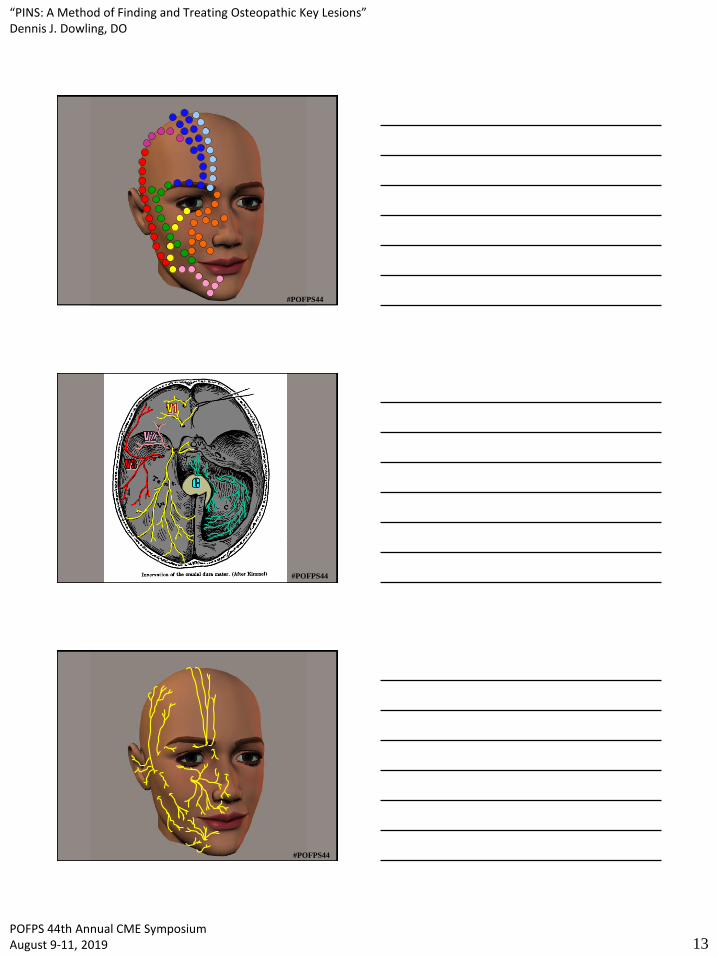
20. Patterns that are followed may indicate the actual structures inhibited:
- Straight paths may indicate involved muscles or specialized fascial components
- Zig-zag patterns may indicate nerves or blood vessels
21. More central patterns may actually cross midline (i.e. a frontal/trigeminal primary point on the right may have an endpoint located in the sub-occipital triangle on the left).
22. Some apparent endpoints may actually be mid-point components either within a structure or at the end of a structure (i.e. an apparent endpoint located near the fibular head may represent the halway point from a primary point at the greater trochanter of the femur and the fifth metatarsal head) representing an overlap of contiguous structures (i.e. iliotibial band – peroneal brevis). This may not be determined until a subsequent visit.
23. When multiple counterstrain tenderpoints are located within a region, look for a PINS pattern.
Method
#POFPS44
PINSTreatment
#POFPS44
Chief Complaint
• 25 year old married female osteopathic medical student
• chief complaint of “migraine headache”.
• nausea, blurring of vision, increased lacrimation, and neck stiffness.
• The pain had begun a few days ago and was unrelieved by the use of
non-steroidal anti-inflammatory medications, sleep, or frequent doses
of Imitrex (sumatriptan succinate), which she took orally. She stated
that she takes between 21 and 30 Imitrex pills per month.
• Loud sounds, light and certain food smells appear to worsen the chief
complaint. There were no other visual, auditory, or olfactory
complaints or associations with the presence of headache.
• The current episode appeared to be unrelated to her menses since her
last menstrual period two weeks prior.
• 25 year old married female osteopathic medical student
• chief complaint of “migraine headache”.
• nausea, blurring of vision, increased lacrimation, and neck stiffness.
• The pain had begun a few days ago and was unrelieved by the use of
non-steroidal anti-inflammatory medications, sleep, or frequent doses
of Imitrex (sumatriptan succinate), which she took orally. She stated
that she takes between 21 and 30 Imitrex pills per month.
• Loud sounds, light and certain food smells appear to worsen the chief
complaint. There were no other visual, auditory, or olfactory
complaints or associations with the presence of headache.
• The current episode appeared to be unrelated to her menses since her
last menstrual period two weeks prior.
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 11
Past Medical History
• paresthesias to the upper extremities secondary
• MVA two months earlier. She was the driver of a vehicle, which was
stopped at a traffic light, when she was struck from behind. She did see
the other vehicle and braced herself for impact.
• Also a history of transient hematochezia, occasional vaginitis,
coccigodynia, and allergic rhinitis. She had neck pain, shoulder pain,
low back pain, and abdominal pain.
• She had a fall in which she struck the top of her head at age twelve and
has had migraines since that time.
• Family history is significant in that other members of the family have
had migraines, a brother has allergies, and her mother has “colon
problems”.
• The patient has two glasses of wine once per week, during religious
observations, and denies use of recreational drugs or tobacco. She has
had a tonsillectomy, rhinoplasty, and sinus cauterization.
• paresthesias to the upper extremities secondary
• MVA two months earlier. She was the driver of a vehicle, which was
stopped at a traffic light, when she was struck from behind. She did see
the other vehicle and braced herself for impact.
• Also a history of transient hematochezia, occasional vaginitis,
coccigodynia, and allergic rhinitis. She had neck pain, shoulder pain,
low back pain, and abdominal pain.
• She had a fall in which she struck the top of her head at age twelve and
has had migraines since that time.
• Family history is significant in that other members of the family have
had migraines, a brother has allergies, and her mother has “colon
problems”.
• The patient has two glasses of wine once per week, during religious
observations, and denies use of recreational drugs or tobacco. She has
had a tonsillectomy, rhinoplasty, and sinus cauterization. #POFPS44
Medications
• AllegraTM (fexofenadine hydrochloride)
• oral contraceptives
• Excedrin PM (APAP/ASA/caffeine)
• Motrin (ibuprofen)
• Imitrex
#POFPS44
Structural findingsCranial
OA compression; Right condylar compression; restriction of frontal, right parietal, and right
temporal bone motion during flexion; occipitomastoid suture restriction on the right;
cranial rhythmic impulse of 4; Left sidebending-rotation pattern; facial asymmetry (right
narrow orbit; flattened nasolabial fold left; deviation of nose; etc.); sensitive point at the
supraorbital ridge; restriction of the right TMJ
Cervical
OAESR RL; AA RR; C2 E SR RR; C3 E SL RL; C6 SR RR; C7SR RR; spasm of the right
trapezius; spasm of the right sternocleidomastoid
Thoracic and Rib
spasm of the right levator scapula; spasm of the left scalene muscles; Right first rib
elevation; myofascial restriction of the hyoid and anterior strap muscles; multiple
thoracic Type II somatic dysfunctions
Lumbar
L5 F SR RR; thoracolumbar paravertebral muscle spasms
Sacrum and Pelvis
Unilateral sacral shear on the right; right anteriorly rotated ilium; right piriformis tender
point; Chapman points along the iliotibial band on the right; restriction of the coccyx
and pelvic diaphragmatic restriction on inhalation
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 12
#POFPS44
How do you make the
connection?
#POFPS44
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 13
#POFPS44
#POFPS44
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 14
#POFPS44
#POFPS44
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 15
#POFPS44
#POFPS44
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 16
#POFPS44
#POFPS44
#POFPS44

“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 17
#POFPS44
#POFPS44
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 18
#POFPS44
#POFPS44
HOW MUCH PRESSURE?
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 19
PRIMARY POINT
#POFPS44
#POFPS44
END POINT
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 20
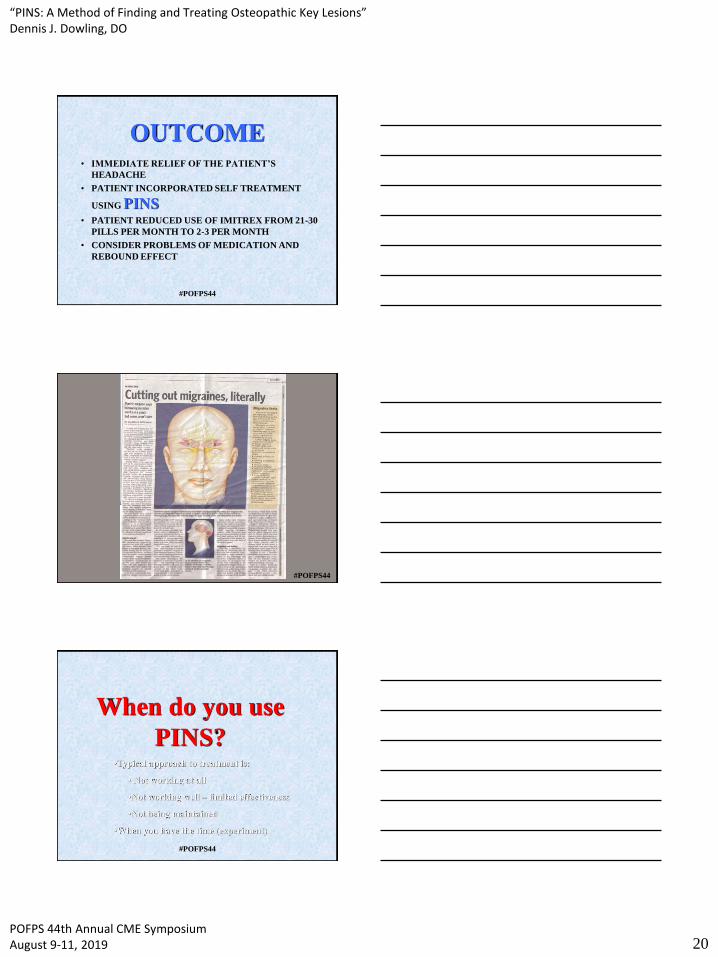
OUTCOME• IMMEDIATE RELIEF OF THE PATIENT’S
HEADACHE
• PATIENT INCORPORATED SELF TREATMENT
USING PINS• PATIENT REDUCED USE OF IMITREX FROM 21-30
PILLS PER MONTH TO 2-3 PER MONTH
• CONSIDER PROBLEMS OF MEDICATION AND
REBOUND EFFECT
#POFPS44
#POFPS44
When do you use
PINS?•Typical approach to treatment is:
• Not working at all
•Not working well – limited effectiveness
•Not being maintained
•When you have the time (experiment)
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 21
12
6
39
FPR & Still
Muscle Energy
HVLA
#POFPS44
00:00:0000:00:0500:00:1000:00:1500:00:2000:00:2500:00:3000:00:3500:00:4000:00:4500:00:5000:00:5500:01:0000:01:0500:01:1000:01:1500:01:2000:01:2500:01:30
#POFPS44
00:01:30
COUNTERSTRAIN
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 22
00:00:0000:00:0000:01:0000:02:0000:03:0000:04:0000:05:0000:06:0000:07:0000:08:0000:09:0000:10:00
PINS
MINUTES
#POFPS44
00:10:00
PINS
#POFPS44
…HOW CAN YOU AFFORD
NOT TO WHEN IT IS
NECESSARY#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 23
When it’s necessary
Why do you use
PINS?
#POFPS44
#POFPS44
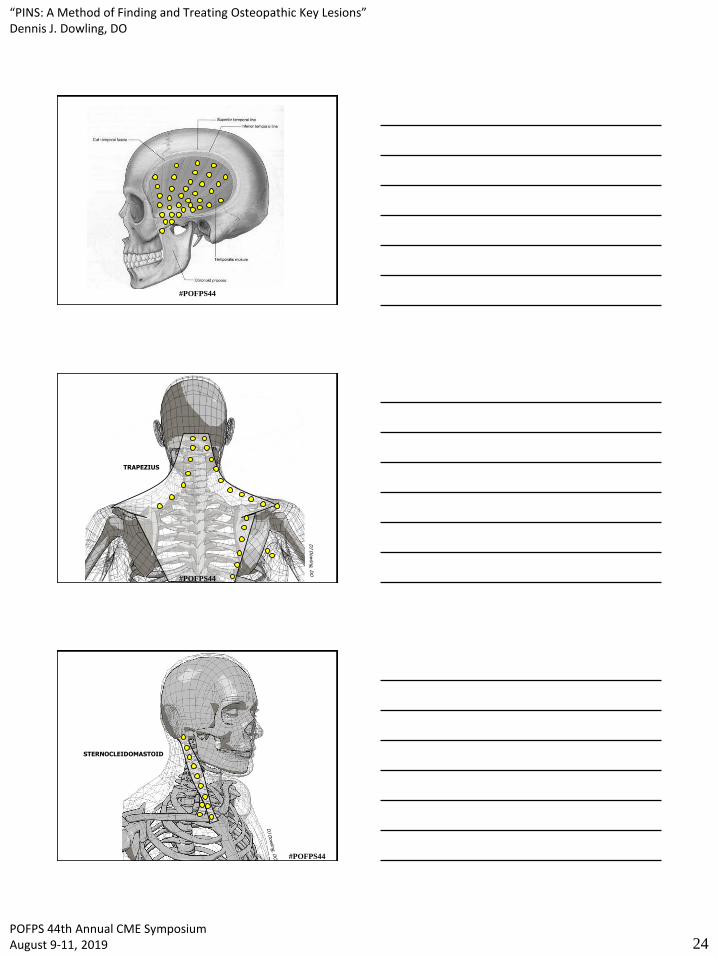
PINS
TREATMENT
of
HEAD
&
NECK
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 24
#POFPS44
TRAPEZIUS
#POFPS44
STERNOCLEIDOMASTOID
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 25
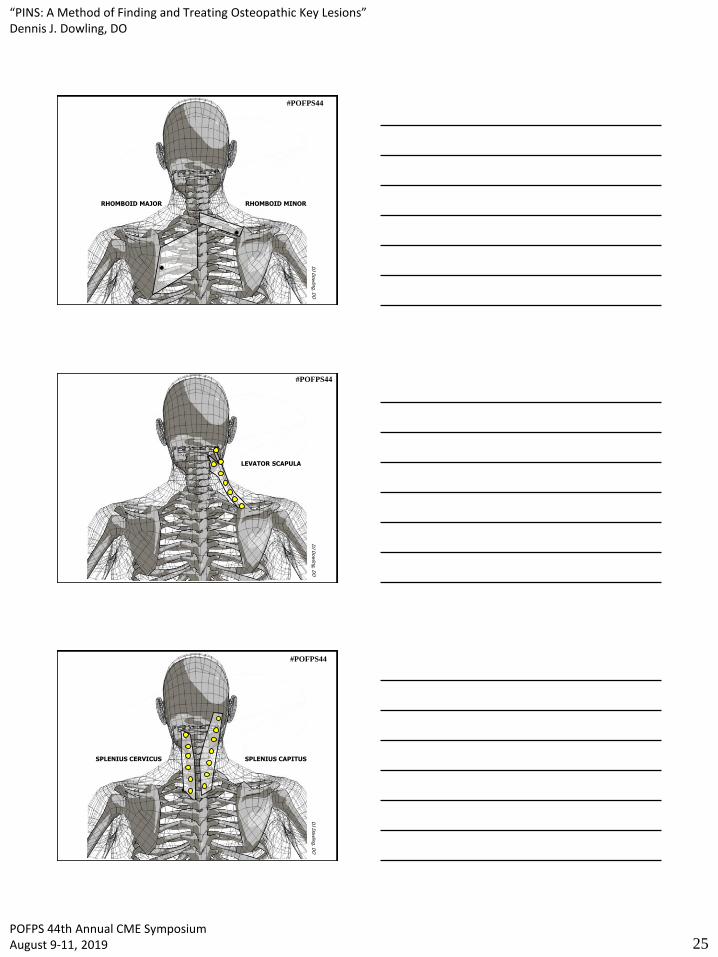
RHOMBOID MAJOR RHOMBOID MINOR
#POFPS44
LEVATOR SCAPULA
#POFPS44
SPLENIUS CERVICUS SPLENIUS CAPITUS
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 26
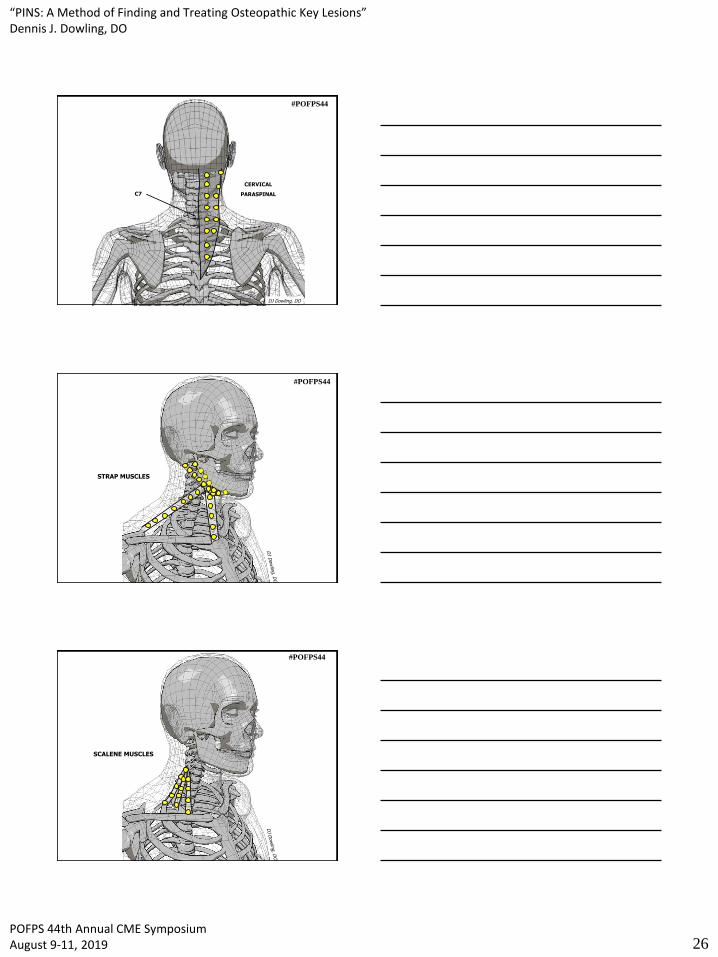
C7
CERVICAL
PARASPINAL
DJ Dowling, DO
#POFPS44
STRAP MUSCLES
#POFPS44
SCALENE MUSCLES
#POFPS44
“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 27
#POFPS44
a PINS secret
#POFPS44
QUICKER PINS
#POFPS44

“PINS: A Method of Finding and Treating Osteopathic Key Lesions”Dennis J. Dowling, DO
POFPS 44th Annual CME Symposium August 9-11, 2019 28
1 3
4
2
E
5
#POFPS44
6
7
8
9
#POFPS44
10
1112
13
Could reduce 10 to 3 minutes
#POFPS44





























