Embed Size (px)
Citation preview

AUSTRAliAN PHYSIOTHERAPY
Jill illiamsJane Unwin
TOPICAL THERAPY
Physiotherapy managementofminimalcerebraldysfu.nctioninAustralia:currentpracticeand future challenges
Theaim of this study was to identify strategiescurrently used by Australian physiotherapistsinvolved in the management of children withminimal cerebral dysfunction (MCD) as a firststep in exploring the role of physiotherapy inthis area. A questionnaire was developedcontaining both closed and open endedquestions regarding physiotherapyassessmentand intervention in the management ofMGD. Atotal of 464 subjects were reached throughAustralian PhysiotherapyAssociation resources,of which 76 per cent responded. Of theserespondents, 31 percent(n =105)were involvedin the management of children with MCD.Analysis of survey responses revealed ahighlyeclectic and inconsistent approach toeward theassessmentandtreatmentofchildren with MCDby Australian physiotherapists. These findingspresent a strong challenge to currentphysiotherapy practice in thisclientgroup. Thepresent diversity ofpractice suggests an urgentneed to establish more consistent assessmentprocedures and methods of outcomemeasurement.[WiliiamsJ and Unwin J: Physiotherapymanagement of minimal cerebral dysfunctionin Australia: current practice and futurechallengeso AustralianJournalofPhysiotherapy43: 135~143]
Key words: Child Development;Child Development Disorders;Pediatrics
inimalcerebraldysfunction(MCD) is one of many termsused to describe clusters of
sensory-motor problems adverselyaffecting a child's ability to functionsuccessfully at home and at school.MCn is reported to occur.in 5 to 20per cent of the school-aged population,depending on the definition applied(Watter and Bullock 1987a). Whiledefinitions differ among authors, thereis agreement·on the central commonfeature of motor skill impairment inthe absence of any overt physical orintellectual disorder (Henderson1987). In addition, children with MeDmay develop secondary socialemotional problems such as poor selfesteem, compounding the difficultiesfaced (Watter and Bullock 1989b).
Minimal.cerebral dysfunction is anumbrella term rather than a diagnosticlabel, although findings of a recentstudy suggest there may he clinicalsubtypes ofMCD (Hadders-Algra et al
J Williams BAppSc(Phty)(Hons)is aphysiotherapist at the Royal Adelaide Hospital.J Unwin MAppSc{Phty), MAPA isa lecturer intheSchool ofPhysiotherapy,UniversityofSouthAustralia.
1988). Therefore, itis not surprisingthat many perspectives on assessmentand intervention for thisheterogeneous client group appear inthe literature. In a review of theinternational literature, no singleapproach was identified as consistentlyused or agreed upon. In the Australianliterature, information detailing thephysiotherapy management of childrenwith MCD is limited primarily to adescriptive paper authored by SouthAustralian physiotherapist MargaretAbbie (Abbie 1978) and a series ofstudies investigating the efficacy ofaneurodevelopmental interventionapproach, by Queenslandphysiotherapists Pauline Watter andMargaret Bullock (Watter and Bullock1987a and 1987b). The manyassessment and interventionapproaches discussed throughout theliterature reflect the range ofstrategiespotentially used by Australian
Correspondence: Jill Williams, PhysiotherapyDepartment, Royal Adelaide Hospital, NorthTerrace, Adelaide, South Australia 5000.This study was supported by the AustralianPhysiotherapyAssociation {SAHranch}HesearchFund Committee.

TOPICAL THERAPY AUSTRAliAN PHYSIOTHERAPY
From Page 135physiotherapists in the management ofMCD.
Assessment of MCDBritish psychologist Henderson (1987)broadly categorised the approach tothe physical assessment of childrenwith Men as quantitative andqualitative. The quantitative approachincorporates tests which assess theperformance of actions, yieldingquantitative scores. These includesimple pass/fail scores and continuousmeasures such as rating scales. Thescores can then be compared withnormative data for chronological age.Qualitative approaches involvedocumentation of how actions areperformed rather than what isachieved. Recording may involve theuse of longhand descriptions,movement notation or a qualitativeobservation checklist (Henderson1987, Laszlo and Bairstow 1985).
Assessment items may generally be
considered as either motor tests orperceptual tests. It has been suggestedthat motor test items (for examplehopping) provide little insight into theunderlying cause of difficulties. On theother hand, perceptually based tests
(for example gesture imitation) enableidentification of those perceptualmotor processes not adequatelydeveloped and thus the basis of specificdifficulties (Laszlo et aI1988).
Several test batteries designed for the

AUSTRAliAN PHYSIOTHERAPY TOPICAL THERAPY
figure 1.State by state profile of study sample.
Figure 2..Current practice settings of responding physiotherapists involvedin Men management
assessment of children with MeDappear frequently in the internationalliterature. The Bruininks-OseretskyTest ofMotor Proficiency (Bruininks1978) has been used by both physicaland occupational therapists in theassessment of motor proficiency inchildren with MCD, providingquantitative measures (MoxelyHaegart and Ladd 1989, Schoemakerand Kalverboer 1990). The PeabodyDevelopmental Motor Scales (PDMS)(Folio and Fewell 1983) have beenused by occupational therapists in theassessment of motor function inchildren with sensory-motor problems(DeGangi et al 1993, Stokes et al1990).
Abbie (1978) described theassessment of children with MeD atthe Adelaide Children's Hospital,involving both a physiotherapist andphysical educator. The assessmentincluded a modified neurologicalexamination, the imitation of gesturesand a number of other observationalitems. A neurodevelopmentalassessment developed by Burns andWatter (1974) has been adapted for thephysiotherapy assessment of children
with MCD (Bullock and Watter 1978,Watter 1984, Watter and Bullock1987a and 1987b). In this, the degreeof abnormality in performance ofassessment items is quantified using afour point rating scale (Bullock andWatter 1978). Assessment itemsrelating to the older child included inthe NSMDA PhysiotherapyAssessment for Infants and YoungChildren (Burns 1992) are also relevantto the child with MCD.
Treatment of MCDMany of the treatment programs usedclinically in the management ofMeDare adaptations of those originallydevised for more general or severedisabilities (Moxley-Haegert and Ladd1989). A range of approaches(summarised in Table 1) are identifiedin the international literature asfrequently used by professionals ofvarious disciplines in the treatment ofchildren with MCD.In the current economic climate,
there is an increasing requirement forhealth professionals to demonstratetheir role and the efficacy of theservices which they provide. The aim
of the study was to identify anddocument strategies currently in use byAustralian physiotherapists in themanagement of children with MeD, asthe first step in demonstrating the roleof physiotherapists in this area ofmanagement.
MethodThe self-administered questionnairesurvey has been identified as a reliable,relatively non-reactive and inexpensiveresearch tool and, as such, provided themost appropriate method of datacollection for this study (French 1993).Questionnaire development wasassisted by discussion with aphysiotherapist with more than 15years of experience in the managementofMCD. This discussion helped toidentify potential areas of interest inthe management of children withMeD among physiotherapistscurrendy practising in this area,enhancing content validity of thequestionnaire.
Questionnaire items were developedto determine the specifi~ approaches ..

From Page 137and strategies currently used byAustralian physiotherapists in themanagement ofMCD. The Australianand international literature wasreviewed to identify MCDmanagement strategies employed byprofessionals in the fields of healtheducation and psych~logy.Details~fthese provided abasi~~for open-endedquestions and response options for theclosed-ended questionnaire items.
The questionnaire was piloted onfour physiotherapists with experiencein the management ofMCD and twoprofessionals with experience .inquestionnaire construction.. It was thenredrafted with minor alterations incontent and format. The questionnaireconsisted of two sections: the firstcontaining questions relating to theassessment and intervention strategiesused in the physiotherapy managementof children with MCD; the secondcontaining questions regardingprofessional experience anddemographic. information.
It was intended that the questionnairesurvey reach the maximum number ofphysiotherapists currently involved inthe management of children withMCD in Australia. The majority ofi~tial subjects we!e reached througheIther.~e Austrahan PhysiotherapyAsSOCIatIOn (APA) Paediatric Special<?r?up \pSG) membership listings orhStlngs In the APA National PaediatricServices Directory (1991). Listings werenot available in the APADirectory forTas,?anian paediatric physiotherapy~ervtces, therefore appropriate listingsIn Tasmanian Telecom Directorieswere also utilised.
The questionnaire, a covering letterand reply paid envelope were mailed toeach subject. Each subject was offereda mailed summary of the results of thestudy. Following a given time period,non-respondents were included in asecond round mail-out ofquestionnaires and reminder letters.Closed-ended resporl~eswere codedand the.da.tacomputer analysed usingthe StatIstical Package for the SocialSciences (SPSS). Open-endedresponses were manually coded by one
TOPICAL THERAPY
Figure 3.Sources of Men referrals tophysiotherapists.
coder based on naturally developingcategories and subsequently manuallyanalysed.Cross-tabu1ations wereperformed to investigate possiblerelationships between responses toseveral of the closed-endedquestionnaire items.
ResultsOf 464 initial subjects, a surveyresponse rate of 76 per cent wasobtained. Of these respondents, 31 percent{n = 105) were involved in themanagement ofchildren with MCDand .completed the questionnaire. Thenumber of initial subjects, subsequentrespondents and respondents involvedin the management ofMCDwithineach state and territory in Australianare shown in Figure 1.
The wide variety of practice settingsreported by those involved in themanagement ofMCD appear in Figure~. The community setting categoryIncorporates employment in bothschools and community health centres.
The percentage of total caseloadassociated withMCD management wasreported as 1-30 per cent by 57 per
AUSTRAliAN PHYSIOTHERAPY
cent of respondents and 30-60 per centby 17 per cent of respondents. AnMCD caseloadof greater than 60 percent was reported by 22 per cent ofrespondents. Respondents employed inmetropolitan areas tended to havehigherMCD caseloads compared withrespondents employed in rural areas,although this was a non-significanttrend.
The number ofyears of experiencereported in physiotherapy, paediatricsand specifically in the management ofchildren with MCD, variedconsiderably and is shown in Table 2.There was a weak relationship betweenrespondents with more experience inpaediatrics and greater MCDcaseloads.
Nearly three quarters of therespondents (72 percent) reportedparticipation in further education inthe area ofMCD. Half of theserespondents had participated incontinuing education programs inMCD offered by the APA'sQueensland Branch or by theDepartment of Physiotherapy at TheUniversity of Queensland.
The sources of routine referral ofchildren with MCD for physiotherapyreported are displayed in Figure 3.
AssessmentForty-one per cent of respondentsreported involvement of otherprofessionals during initial assessment.These included occupational therapists(26 per cent), both occupationaltherapists and speech pathologists(9 per cent) and other professionals (5per cent). Methods ofobtainingsubjective information in theassessment ofMCD reported were:verbally (56 percent); through parentquestionnaire forms (5 per cent); bothof the above (23 per cent) and throughreports .and letters from referralsources (16 per cent).
The use of a standard in-houseassessment form based ona previouslypublished format was reported bynearly one-half (48 per cent) ofrespondents. This information wassought using an open-ended question~o t:hat while a number ofresponden~IndIcated that their assessment forms

AUSTRAliAN PHYSIOTHERAPY TOPICAl THERAPY
Treatrnent philosophyUOftenI SometimesI Often
70100
90 6080
70 50
E3 60 23I=l (:lQ) (1)
""'0 "'0 40~ 50 ~0 0~ ~VJ 40 VJOJ <1)$....t l-I
?fi- ef? 3030
20 2010
0 10
~ ~U (I) "'0 40J t) ~ U':J 0 ~:> ~
t/) 0~
;.... (J)Po.! > ~ J...I [; ~
~ Z 0 0
Neurodevelopmentaltherapy
!{ey:GM =gross motor skills
FM = fine motor skills
PC == postural control
Vis = visual system
Aud =auditory system
Vest =vestibular system
Tact =tactile system
Prop =proprioception
MS =musculoskeletal factors
Neura =neurological.factors•D Sensory integration
therapy
Perceptual motortraining
Other
figure 4.Areas included in objectivephysiotherapv assessment of MGD.
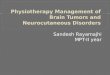
Figure 5.Treatment philosophies applied in Men management
were based on the work of Queenslandphysiotherapists Burns (19 per cent)and Watter (27 per cent), the exactsources were not reported. Otherrespondents identified included theassessment form used at the AdelaideChildren's Hospital (3 per cent) and arange of assessments described in theinternational literature (9 per cent).The inclusion ofspecific publishedtests in assessment was reported by 34per cent of respondents. These weremost frequently identified as testsincluded in assessments described byBurns (1992), BullockandWatter:1978) (17 percent), the PeabodyDevelopmental Motor Scales (7 per
cent) and the Bruininks-OseretskyTest of Motor Proficiency (7 per cent).
The obiective assessmentThe reported frequency of inclusion ofeach area of function in objectiveassessment is displayed in Figure 4. Inthe assessment of fine motor abilities,several respondents specificallyindicated that the extent of assessmentwas dependent upon the level ofoccupational therapy involvement withthe child.
Qualitative scoring methods were farmore frequently used by respondents(91 per cent) compared withquantitative methods (43 per cent).
The qualitative scoring methods mostfrequently applied were longhanddescriptions (49 per cent),whilst 14per cent ofrespondents usedqualitative observation checklists and28 per cent of respondents used both.Rating scales were the quantitativescoring methods most frequentlyreported (36 per cent). Interestingly,14 per cent of respondents specifiedthat the rating scales used were .basedon qualitative descriptions, as in therating scale developed by Bullock andWatter (1978).

Nearly all respondents (99 per cent)reported implementation ofahomeprogram in the management ofchildren with MCD.Recommendations regarding theamount of time to be spent on theprogram varied considerably. Themajority of respondents recommendeda single session of home programactivities per day (63 per cent).Incorporation of activities into dailytasks, rather than undertaking a formalprogram, was recommended by 9 percent of respondents. Parentinvolvement in home programimplementation was expected by 98per cent of respondents, whilst only 55per cent of respondents expected thisduring physiotherapy treatmentsessions. The existence of a supportgroup for parents ofchildren withMCD was reported by one quarter ofrespondents.
TOP I CAL THE RAPY
from Page 139Treatmentapproachand implementationMulti-disciplinary formation ofmanagement goals was reported by 84percent of respondents. Occupationaltherapists (58percent),speechpathologists (43 per cent) and thechild's teacher (39 per cent) were theprofessionals most likely to beinvolved.
Combined treatment sessions withother professionals were used by 72 percent of respondents. Professionalsinvolved in such joint or sharedtreatment sessions includedoccupational therapists (36 per cent),both· occupational therapists andspeech pathologists (15 per cent),teachers (12 percent), anotherphysiotherapist (4per cent) and otherprofessionals (2 per cent).
Eighty per cent of respondents used a Treatment outcomes,combination of two or more reassessment andphilosophies in their treatment review assessmentapproach. The percentages ofrespondents adopting each philosophy Formal reassessment of the child within their treatment approach are shown MCD at the end of the treatmentin Figure 5. An enormous range of period was reported by 70.5 per cent ofspecific hands-on techniques were respondents. Inaddition,- 6.7 per centreported as utilised in treatment of respondents reported that airnplementationand have been.. summary of changes and currentsummarised in Table 3. The majOrIty functional status was provided to(98 per cent) of respondents reported parents and/or referral sourcesthe use ofequipment during treatment following formal reassessment.implementation. Theequipr.nent items - Treatment outcomes were evaluatedmost used included trampohnes,balls,mobile surfaces and scooter boards. through reassessment by 51.4 per cent
of respondents. Several respondentsMost of the respondents used specified that reassessment to
individual treatment sessions· (96 per determine treatment outcomescent) but a smaller percentage reported primarily utilised quantitative measuresutilising group treatment sessions (63 (13.3 per cent), with 15.2 per cent ofper cent). Generally, children w~re respondents reporting application ofincluded in group treatment seSSIOns primarily qualitative measures. Forty-when sufficient numbers ofchildren one per cent of respondents alsowith similar functioning levels existed reported treatment outcome measuresto form a group (25 per cent), when as based on subjective feedback fromnot easily distracted (11 percent) and parents, teachers, the child and otherwhen improved social skills were a professionals involved in management.management goal (5 per cent). Information regarding improved self-Individual treatment sessions were esteem and confidence in the childemployed specifically when the child with MCD obtained subjectively waspresented with greater levels of specifically identified as an indicator ofdysfunction (13 per cent) and when the treatment outcome by 10.5 per cent ofchild was easily distracted or had respondents.behavioural problems (5 per cent).
AUSTRAliAN PHYSIOTHERAPY
Discussio>nThe results of the questionnaire surveyprovide a description of strategiescurrently used ·by physiotherapistswithin the study population in themanagement of children with MCD.The survey response rate was highcompared·with those typically reportedfor mail-out surveys (Lebow 1982).This high response rate and theinterest of respondents, demonstratedby the number of requests forasummary ofstudy findings, suggests·adesire forincreased dialogue amongstAustralian physiotherapists regardingstrategies utilised in the managementafMCD. However, considering thehigh percentage of c~l~renrep?~tedto·suffer from MeD, It IS surprISIngthat less than one-third of the totalresponding physiotherapists. wereinvolved with such a potentially largeclient group. The reasons behind thisfinding should be explore~. Som~
physiotherapists may feel Ill-equIppedto manage these children; others mayplace less value on the treatment ofMCD compared with more severe .paediatric conditions; perhaps .there ISinadequate referral of these childrenfor physiotherapy services in someareas. Predictably, the amount ofprofessional experience reported inpaediatrics and Men was markedlyless than that in physiotherapygenerally. The relatively small numberof physiotherapists with considerableexperience in the management ofMCDhighlights the importance of thecurrent study as a starting poi~t f~r
further dialogue between paedIatrICphysiotherapists involved in this areaof management.
The identification of strategiesemployed by physiotherapists in themanagement ofMCD could providesome basis for evaluation andcomparison of treatment efficacy.However, respondents' definitions ofthe client population they label asMCDwere not sought. Due to theheterogeneous nature ofthis client .group, any multicentre or collaborativeresearch would require.carefuldefinition and selection of groups. Thedifficulty ofaccurately identifying the

AUSTRAliAN PHYSIOTHERAPY
MeD client group is not a uniquelyAustralian problem and is reflected inthe range of operational definitionsfound in the international literature.Agreement on the definition ofMCDis an ongoing clinical and researchchallenge. As an initial step,physiotherapists must urgently reach aconsensus with regard·to relevant,reproducible assessment techniques forchildren with MCD. The findings ofthis survey suggest that this is sadlylacking. Physiotherapists involved inthe management ofMeD must alsocritically appraise any new researchfindings as an integral part oftheirpractice evaluation.
Multidisciplinary involvement in themanagement ofMCD has beendescribed in several studies in thepublished literature (McMahon et al1985). In this national Australiansurvey, a high level of multidisciplinaryinvolvement in· the physiotherapymanagement ofMCD was identifiedduring theinitial assessment, theformation of management goals,shared treatment sessions and in theuse of subjective feedback frommultidisciplinary team members. Itmay be valuable to assess parentsatisfaction ·and compare treatmentoutcomes when multidisciplinaryinvolvement does and does not occur.
In the objective assessment of thechild with MCD, fine motor abilitiesand the sensory systems (with theexception of proprioception) were theareas least often assessed. Manymultidisciplinary team members, suchas those often identified asconcurrently involved in. management(for example occupational therapists)may be concerned with the specificassessment of those aspects of function(Cermak and Henderson 1990). Theassessments by other multidisciplinaryteam members may then supplementthe physiotherapy examination of thechild with MCD, limiting the need foran expanded assessment of areas suchas fine motor abilities and sensoryfunctions. However, the less frequentinclusion of fine motor abilities and thesensory systems in assessment may infact indicate a need to educatephysiotherapists about the relevance of
TOP leAL THE RAP Y
these areas in the assessment ofchildren with MCD.
The infrequent referral of childrenwithMCD to physiotherapy bygeneral practitioners and communityhealth nurses suggests a need forincreased awareness amongst theseprofessionals about thephysiotherapist's role in themanagement ofMCD4 The relativelack of referral from allied healthprofessionals was particularlysurprising given the high level ofmultidisciplinary involvementidentified in other areas. It isimportant to consider that referral ofthe child with MCD to physiotherapymay indeed have been initiated by anallied health professional. However,this may be directed to thepaediatrician involved in the child'smanagement, who then formally makesthe referral. Thus the higherproportion of paediatricians and lowerproportion of allied healthprofessionalsreported may notrepresent the true initial referralsource.
The use of assessment formats,specific tests, scoring methods andtreatment approach based 01) the workof Australian physiotherapists (Bullockand Watter 1978, Burns 1992, Watterand Bullock 1987a, 1987b and 1989a)were all frequently reported and morethan a third of respondents hadparticipated in MCDcourses led bythese Queensland researchers. Thissuggests that Australianphysiotherapists.(and.educators withinthe Schools of Physiotherapy) areincorporating strategies describedwithin the Australian literature intotheir management ofMCD.
The fact that qualitative measuresand specifically longhand descriptionscomprised the most frequentlyreported scoring method is of concern.This method of recording. is not onlytime consuming but also difficult tostandardise4 It may therefore produceinconsistencies between individualobservers, making informationexchange between physiotherapists andother professionals problematic(Henderson 1987). Only a third of thesurvey respondents reported the
inclusion of specific published tests intheir assessment battery. The use ofquantitative methods allows functionalchanges following treatment to bedemonstrated interms that otherprofessionals can appreciate and apply.The development of a standard MCDassessment format by physiotherapistscan only assist in promotingconsistency in this area..Previouslypublished test items, particularly thosedemonstrated to he reliable and valid,should be included whenever possible.
No single treatment approach couldbe identified as consistendyadoptedbased upon information derived fromthe survey responses. The use ofcombinations of treatment philosophy,varied hands-on physiotherapytechniques and equipmentdemonstrated the eclectic. approach tomanagement of children with MCDadopted by the majority ofrespondents. If this situation remainsunchanged, it. is likely to be verydifficult for the physiotherapyprofession to demonstratethe.efficaeyof their input in this client group.Clinical research evaluating andcomparing the effects of majortreatment approaches andcombinations of treatment approachesshould be a priority forphysiotherapists working in this field.
Knowledge of treatment outcomesthrough reassessment, usingquantitative and qualitative measures,and through subjective feedback wasreported by less than three-quarters ofthe respondents. Inconsistency inscoring systems used at initialassessment and then at reassessmentappeared to exist, with quantitativemeasures less often used atreassessment than initial assessment tomeasure treatment outcome. Clearly,better functional and physical outcomemeasurement needs to.occur to reflectthe success or otherwise ofphysiotherapy programs.
Physiotherapists often considerincreased confidence and.improvedbehaviour as important measures oftreatment outcome (Schoemaker et al1994, Watterand Bullock 1987a).Indicators of progress such as

TOPICAL TH ERA PY AUSTRAliAN PHYSIOTHERAPY
From Page 141improved confidence were reported asmeasures of treatmentoutcome,butthese improvements were notquantified by respondents. Theinclusion of a short, standardised scaleto.rate changes in confidence and selfesteem may prove a useful tool indemonstrating physiotherapyoutcomes in the child with MCD.
Recognition of the importance ofparent education and involvement inphysiotherapy·management.wasdemonstrated by the high proportionofrespondents who described parentparticipation in management goalformation, in providing subjectivefeedback and involvement duringtreatment sessions and home programimplementation. The home programwas the most consistently reportedmanagement strategy. Thisinvolvement has previously beenrecognised as an important feature inmanagement through increasing theparents'understanding of their child'sdifficulties (Abbie 1978, Watter andBullock 1987a). The high level ofparent education and involvement inthe physiotherapy management oftheir child appears to reflect thecurrent philosophy in health caredelivery of client empowerment andfamily-centred approach tomanagement.
ConclusionsThe results of this study.reveal thatamongst the study population ofAustralian paediatric physiotherapists,individual practitioners have adoptedand combined a wide .range ofstrategies in the management ofMeD.There appears to be very littleconsensus in the use of assessment~echniques and treatment practices orIn the measurement ofoutcomes inthis large and ill-defined client groupwThe heterogeneous nature ofMeDprovides a major challenge forphysiotherapists practising in this area.The next step must be to establishmore consistent assessment of thesechildren and more comprehensivemeas.uresof outcome followingphYSIotherapy intervention. Differing
intervention approaches must bespecifically defined and their impactexamined and compared. Anotherimportant task is clarification of aworking definition of the term MCD.The number ofphysiotherapists withlong-term experience in this area issmall, emphasising the need for furtherdialogue amongst physiotherapistsinvolved in the management ofMCD.T~ese survey findings act as a startingpOInt fo~ the evaluation ofapproachesand strategies, so that the role of thephysiotherapist in the management ofchildren with MCD maybe effectivelyevaluated.
ReferencesAbbie~ (1978): Physical treatment for clumsy
chIldren - not enough? Physiotherapy64: 198-203.
Arnheim D and Sinclair W (1979): The ClumsyChild: A Program of Motor Therapy. (2nded.) St Louis: CV Mosby.
Ayres] (1972): Sensory Integration and LearningDisorders. Los Angeles: WesternPsychological Services.
Ayres.] (1974): The Development .of SensoryIntegrative Theoryand Practice: ACollectionof the Works ofJean Ayres. Iowa: KendallHunt.
Bobath K (1967): The neurodevelopmentaltreatment of cerebral pal~y. DevelopmentalMedicine and Child Neurology 9: 373-390.
Bobath K (1980): A Neurophysiological Basis forthe Treatment of Cerebral Palsy. London:William Heinemann Medical Books Ltd.
BruininksR (1978): Bruininks-"Oseretsky Test ofMotor Proficiency. Minnesota: AmericanGuidance Service.
Bullock M~d Watter P(l978): A study of theeffectIveness of physiotherapy in the
.managementofyoung children with minimalcerebral dysfunction. Australian Journal ofPhysiotherapy 24: 111-119.
Burns Y and WatterP (1974): Identification anddevelopmental assessment of the child withneurological impairment. Australian JournalofPhysiotherapy 20: 5-14.
BurnsYR (1992): NSMDA PhysiotherapyAssessment for Infants and Young Children.Brisbane: CopyRight.
CermakS and Henderson A (1990): Learningdisabilities. In UmphredDA (Ed.):Neurological Rehabilitation (2nd ed.) St.Louis: CV Mosby.
DeGangiG, WiedisbachS, GoodinMandScheinerN (1993): Acomparisonofstructuredsensorimotor therapy and child-centred activity inthe treatment of preschool children withsensori-motor problems. AmericanJournal ofOccupational Therapy 47: 777-786.
Densem J, Nuthall G, Bushnell J and Horn J(1989): Effectiveness ofa sensoryintegrativetherapyprogram for children with perceptualmotor deficits.Journal ofLearning Disabilities22: 221-229.
Folio R and Fewell R (1983): PeabodyDevelopmental Motor Scales. Allen TX:DLM Teaching Resources.
French. S (1993): Practical Research: A Guide forTherapists. Oxford: ButterworthHeinemann.
Hadders-Algra M, HuisjesH] and Touwen BCL(1988): Perinatal risk factors and minorneurological dysfunction: significance forbehaviour and school achievement at nineyears. Developmental Medicine and ChildNeurology 30: 482-491.
Henderson S (1987): The assessment of 'clumsy'children: old and new approaches. Journal ofChild Psychiatry 28: 511-"527.
Knott M and Voss D (1968): ProprioceptiveNeuromuscular Facilitation. (2nded.)London: Harper and Row.
LaszloJ and Bairstow P (1985): Perceptual-MotorBehaviour: Developmental Assessment andTherapy. London: Praeger Scientific.
Laszlo], Bairstow Pand Bartip] (1988): A newapproach to treatment ofperceptual-'motardysfunction previously called 'clumsiness'.Supportfor Learning 3: 35-40.
LebowJ(1982):Consumersatisfactionwith mentalhealth treatment. Psychological Bulletin91: 244-259.
McMahon C, Arrowsmith] and GardenerM (1985):A group approach to the treatment· of theclumsy child. Physiotherapy 71: 505-510.
Moxely~HaegertLand Ladd H(1989):Follow-upofchildren identified and treated for a motordelay of non-specificable aetiology. InfantMental Health Journal 10: 45 ...58.
SchoemakerM andKalverboerA(1990): Treatmentof clumsy children. In Kalverboer A (Ed.):Developmental Biopsychology. Experimentaland Observational Studies of Children atRisk. Ann Arbor: University of MichiganPress.
Schoemaker M, Hijlkema M and Kalverboer A(1994): Physiotherapy for clumsy children:an evaluation study. Developmental Medicineand Child Neurology 36: 143-155.
Stokes N, DeitzJand CroweT(1990): ThePeabodydevelopmental fine motor scales: an interrater reliability study. American .Journal ofOccupational Therapy 44: 4: 334-40.
Watter P (1984):Perceptual motor disorders:assessment forneurodevelopmentalphysiotherapy for minimal cerehraldysfunction. In Levitt S (Ed.). PaediatricDevelopmentalTherapy. London: BlackwellScientific Publications, pp. 153-160.
Watter P and Bullock M (1987a): Patterns ofimprovement in neurological functioning ofc~ldren~ithminimal cerebral dysfunctionWlth phYSIotherapy intervention. AustralianJournal ofPhysiotherapy 33: 215-224.

AUSTRAlIAN PHYSIOTHERAPY
WatterPand Bullock (1989a): A physiotherapydirected school-based group managementprogram for children with mild motor andcoordination problems. New ZealandJournalofPhysiotherapy 15: 239-242.
WatterP andBullockM (1987b): The maintenanceof sensory-motor performance afterphysiotherapy intervention for minimalneurological dysfunction. New ZealandJournalofPhysiotherapy Dec: 6-8.
Watter P and BullockM(l989b): MinimalCerebralDysfunction in adults. Australian Journal ofPhysiotherapy 35: 239-242.
TOPICAL THERAPY