Embed Size (px)
Citation preview

2101Physiology of the Gastrointestinal Tract, Two Volume Set. DOI: © 2012 Elsevier Inc. All rights reserved.2012
10.1016/B978-0-12-382026-6.00079-8
Recruitment of Inflammatory and Immune Cells in the Gut: Physiology and PathophysiologyD. Neil Granger, Christopher G. Kevil, and Matthew B. Grisham
79.1 INTRODUCTION
The recruitment of leukocytes to sites of inflamma-tion, infection, or tissue injury is a complex process that involves a tightly coordinated sequence of adhesive inter-actions between leukocytes and the walls of microscopic blood vessels. These adhesive interactions are regulated by a variety of molecules that are expressed on (e.g., adhesion glycoproteins) or released (chemokines, nitric oxide) by activated leukocytes, endothelial cells, and different auxil-iary cells (e.g., mast cells, macrophages, platelets). While leukocyte recruitment in most tissues is generally associ-ated with pathology, the GI tract is considered to normally exist in a state of controlled inflammation, wherein there is a constant trafficking of leukocytes to both lymphoid and non-lymphoid regions of the mucosa. However, many GI diseases and disorders are characterized by a more pro-nounced and persistent recruitment of leukocytes into gut tissue, coupled with dysregulated activation of the infiltrat-ing cells, which ultimately contributes to tissue injury and organ dysfunction. Consequently, the factors regulating leukocyte recruitment in the GI tract have been extensively studied over the past decade in an effort to develop novel strategies for treatment of GI inflammation. This chap-ter provides an overview of the factors that regulate the recruitment and activation of inflammatory and immune cells under conditions of acute and chronic GI inflam-mation. After a review of the adhesion glycoproteins that mediate leukocyte adhesion to vascular endothelial cells, this chapter (1) will focus on the factors that regulate blood cell–endothelial cell interactions in non-lymphoid tissues, (2) will provide a brief overview of gut-associated lym-phoid tissue and intestinal immunity, (3) will address the mechanisms that determine leukocyte movement through the interstitium of inflamed tissue, and (4) will discuss the role of leukocyte trafficking in experimental models of acute and chronic GI inflammation.
79.2 ADHESION MOLECULES
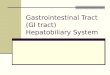
Cell–cell adhesion can be accomplished through homo-typic or heterotypic protein interactions, namely recep-tor-ligand interactions. These events normally govern the homeostatic functions of cells; however, these molecules are of great importance during pathological conditions. Of the many diverse groups of cell adhesion molecules, proteins from the selectin, integrin, cadherin, immu-noglobulin, occludin, and claudin family of proteins have all been implicated in inflammatory diseases. Table 79.1 reports several of these adhesion molecules along with their molecular function, tissue expression, and respec-tive ligands. All of these proteins have been reported to be involved in immune cell homing and recruitment to the GI system under physiological and pathological conditions. Figure 79.1 illustrates the multistep paradigm of leuko-cyte adhesion to microvascular endothelium and identifies adhesion molecules involved at these steps. The following section addresses the specific function of various adhe-sion molecules in respect to the process of immune cell trafficking.
79.2.1 Cell Adhesion Molecules
79.2.1.1 Selectins
The selectin proteins were first discovered through the use of monoclonal antibodies that inhibited leukocyte homing (L-selectin) and leukocyte binding to endothelial cells (E-selectin).1,2 P-selectin was also found as a mem-brane protein within platelet granules with an unknown function, and also later identified in endothelial cells.3,4 It is now known that the selectins are critically important for leukocyte–endothelial cell rolling interactions, par-ticularly during pathological states of inflammation. The selectin proteins consist of a short cytoplasmic domain, a
Chapter 79

SECTION | VI Consequences of Disregulated Physiology2102
transmembrane domain, a series of short consensus repeat domains (SCR domains), a single epidermal growth factor (EFG)-like domain, and a Ca2-dependent lectin binding domain at the amino terminus. The cytoplasmic domain can be phosphorylated on tyrosine, threonine, and serine
residues; however, the importance of phosphorylation is unknown. It is believed that the SCR domains may be involved in maintaining protein structure and can possibly enhance ligand binding. Similarly, the EGF-like domain is quite homologous among all selectins and has been
TABLE 79.1
Adhesion Molecule
Primary Tissue Expression Major Ligands Primary Function
P-selectin Endothelial cells, platelets PSGL-1, Sialylated Lewis X Leukocyte capture and rolling, thrombosis
E-selectin Endothelial cells ESL-1, sialyated Lewis X Leukocyte rolling and firm adhesion
L-selectin Neutrophils, monocytes, most lymphocytes
CD34, GLYCAM-1, MadCAM-1 Leukocyte rolling and homing
ICAM-1 Endothelial and epithelial cells, lymphocytes, fibroblasts, and others
LFA-1, Mac-1, p150/95, fibrinogen, fibronectin (connecting segment-1)
Leukocyte adhesion and extravasation, leukocyte and endothelial cell motility, cell activation
ICAM-2 Endothelial cells, lymphocytes LFA-1 Leukocyte adhesion and extravasation, cell activation
ICAM-3 Neutrophils, monocytes, lymphocytes LFA-1 Leukocyte adhesion, cell activation
VCAM-1 Endothelial cells VLA-4 Leukocyte adhesion and extravasation, cell activation
PECAM-1 Endothelial cells, neutrophils, platelets, lymphocytes
PECAM-1 Leukocyte extravasation
MadCAM Endothelial cells L-selectin, α4β7 Leukocyte homing and adhesion
JAM Endothelial and epithelial cells, neutrophils, monocytes, platelets
JAM, LFA-1, Mac-1, VLA-4 Cell–cell adhesion, regulation of polarity, cell motility
LFA-1 Neutrophils, monocytes, lymphocytes, most other leukocytes
ICAM-1,2,3, JAM Leukocyte adhesion and extravasation, cell activation, cell migration
Mac-1 Neutrophils, monocytes, platelets ICAM-1, JAM, Factor X, iC3b, fibrinogen
Leukocyte adhesion and extravasation, cell activation
VLA-1 Neutrophils, lymphocytes, most other leukocytes
Collagen, laminin Cell-matrix adhesion
VLA-2 Neutrophils, lymphocytes, most other leukocytes
Collagen, laminin Cell-matrix adhesion
VLA-3 Neutrophils, lymphocytes, most other leukocytes
Fibronectin, collagen, laminin Cell-matrix adhesion
VLA-4 Neutrophils, lymphocytes, most other leukocytes
VCAM-1, fibronectin Leukocyte rolling, adhesion, extravasation, cell-matrix adhesion
VLA-5 Neutrophils, lymphocytes, most other leukocytes
Fibronectin Cell-matrix adhesion
E-cadherin Epithelial cells E-cadherin, αEβ7 Leukocyte adhesion
GPIb-IX-V Platelets vWF, Mac-1, thrombin, P-selectin Platelet adhesion, thrombosis
GPIIa-IIIb Platelets vWF, fibrinogen Platelet adhesion, thrombosis
vWF Platelets GPIIa-IIIb, collagen, P-selectin, GPIb
Platelet adhesion, thrombosis

Chapter | 79 Recruitment of Inflammatory and Immune Cells in the Gut: Physiology and Pathophysiology 2103
reported to be involved in cell adhesion. The most critical domain for selectin function is the Ca2-dependent lectin domain. X-ray crystallography studies have shown that Ca2 binding induces a conformational change within this domain, which can facilitate ligand binding.
P-selectin expression is found in both platelets and endothelial cells, whereas E-selectin expression is only observed in endothelium. Both E- and P-selectin facili-tate leukocytes rolling on the endothelial cell surface and P-selectin is also utilized for platelet adhesion. P-selectin is contained in preformed pools within platelet α granules and Weibel-Palade bodies of endothelial cells. Inflammatory activation of platelets and the endothelium results in a rapid mobilization of P-selectin to the cell surface within a matter of minutes. Interestingly, plate-let P-selectin has not been shown to be important for leukocyte recruitment, whereas endothelial P-selectin is important for leukocyte and platelet rolling on stimulated endothelium.5–7 Moreover, both E- and P-selectin expres-sion are transcriptionally induced by several inflammatory cytokines such as TNF-α, IL-1β, or bacterial lipopolysac-charides (LPS). Together, these proteins facilitate leuko-cyte rolling, the initial step in leukocyte recruitment from the vascular lumen to the extravascular tissue.
The role of selectins during an inflammation response can be varied depending upon the type of inflammatory stimuli, the time period of inflammation (acute vs. chronic),
and the organ studied. However, the overall interpretations of multiple studies suggests that P-selectin is important for immediate leukocyte rolling in response to inflamma-tory stimuli and trauma, and that the role of E-selectin may be important during longer periods of inflammation (4 hours) and may also influence leukocyte firm adhesion. The initial reports of P-selectin knockout mice showed that loss of this molecule results in a decrease in early leuko-cyte rolling in response to trauma and inflammatory stimuli, increased leukocyte rolling velocities during longer peri-ods of inflammation (1 hour), and decreased leukocyte recruitment into the peritoneum over a 4 hour period.8,9 It is interesting that the cytoplasmic domain of P-selectin is important for proper targeting to endothelial cell Weibel-Palade bodies in vivo, and that mice containing P-selectin cytoplasmic domain deletions demonstrate many of the phe-notypic features of P-selectin knockout mice.10
Consistent with these observations, loss of P-selectin has been reported to be protective in several inflammatory settings, such as ischemia/reperfusion (I/R) injury, perito-nitis, sepsis, allergic inflammation, contact hypersensitiv-ity, and atherosclerosis.11–20 Interestingly, certain organ vascular beds and disease conditions have been reported to be selectin independent. For example, in lung, brain, and liver inflammatory settings P- or E-selectin have been shown to be unnecessary or minimally involved in leu-kocyte recruitment.21–23 However, these findings may be
Leukocyte capture
Endothelial activation
Rolling Adhesion-Selecins-VLA-4-PNad-GLYCAM-1-MadCAM-1
Leukocyteactivation
Leukocytecrawling-ICAM-1-Mac-1
Extravasation -ICAM-1 -VCAM-1 -PECAM-1 -JAM -VE-cadherin -Occludin -Claudin
MatrixTransmigration
Chemokines
Tissue inflammatorymediators
-Chemokines-LFA-1-VLA-4
Firm adhesion-ICAM-1, -2-VCAM-1-MadCAM-1-LFA-1-Mac-1-VLA-4
Adhesion molecules
Proteoglycans
Inflammationstimulus
FIGURE 79.1 The multistep process of leukocyte recruitment. Stimulation of leukocyte recruitment involves three major steps: leukocyte rolling, firm adhesion, intraluminal crawling, and extravasation. Tissue inflammatory mediators, including cytokines and chemokines, are important in initiating these cellular responses through increased gene expression of various adhesion molecules and functional changes of adhesion molecule affinity/avidity. Adhesion molecules, cytokines, and chemokines also play important roles in regulating leukocyte motility through the extracellular matrix, thus facili-tating immune cell migration through tissue interstitium.

SECTION | VI Consequences of Disregulated Physiology2104
stimulus or injury specific, since an in vitro study using P-selectin mutant brain endothelial cells reported TNF-α- and IL-1β-mediated neutrophil adhesion to be significantly influenced by P-selectin expression.24
While the importance of P-selectin in inflammation has been well identified, the exact role of E-selectin has remained somewhat elusive. This may be due to the manner in which both of the molecules are regulated and expressed. As mentioned earlier, P-selectin is synthesized and stored in Weibel-Palade bodies, which can be mobilized in min-utes after an inflammatory response. In contrast, preformed pools of E-selectin do not exist and induction of this mol-ecule requires transcriptional activation. However, these same signaling mechanisms also induce transcription of the P-selectin gene. Therefore, an increase in both selectin molecules can be observed simultaneously during a given inflammatory response. This concept has lead to the reali-zation that there can be considerable overlap of function between the molecules.25 Careful examination of E-selectin mutant mice has shown that this molecule is important for leukocyte slow rolling and mediates increased leukocyte transit times, thereby allowing adequate leukocyte sampling of the endothelial cell surface and facilitating interaction between cell types.26 This notion is further supported by the observation that loss of E-selectin results in decreased firm adhesion of leukocytes and may be necessary for proper integration of signals involved in leukocyte arrest.16,27,28
L-selectin expression is observed in most leukocytes including lymphocytes, granulocytes, and monocytes. L-selectin has been shown to be an important mediator of lymphocyte homing to peripheral lymph nodes and Peyer’s patches (PPs) in response to inflammatory stimuli.2,29–31 Engagement of ligands, such as peripheral lymph node addressin (PNad) or MAdCAM, stimulates L-selectin-mediated outside-in signaling that can enhance additional adhesion molecule interactions such as β2 integrin/ligand association.32–34 Importantly, L-selectin is proteolytically cleaved from the leukocyte surface following activation, which has become a useful indicator to determine specific immune cell states.35,36
79.2.1.2 Immunoglobulin Superfamily
The immunoglobulin superfamily proteins share a simi-lar structural motif, in that these proteins all contain Ig like extracellular domains that are responsible for cell adhesion. These molecules have been demonstrated to be important for normal immune surveillance, leukocyte adhesion, and leukocyte emigration. The proteins involved in these functions are intercellular adhesion molecule-1, 2, and 3 (ICAM-1, 2, and 3), vascular cell adhesion mol-ecule (VCAM), platelet endothelial cell adhesion mol-ecule (PECAM), mucosal adressin cell adhesion molecule (MAdCAM), and junctional adhesion molecule (JAM).
ICAM-1 was originally discovered through stud-ies using blocking monoclonal antibodies against the integrin LFA-1 (CD11a/CD18).37 ICAM-1 also binds to the integrins, Mac-1 (CD11b/CD18) and p150/95 (CD11c/CD18). ICAM-1 is constitutively expressed at low levels and is transcriptionally induced by several inflammatory mediators. ICAM-1-ligand interactions are involved in leu-kocyte firm adhesion and emigration through engagement with the endothelium and are also involved in leukocyte–leukocyte aggregation and activation. These cellular events are facilitated by ICAM-1-mediated outside-in signaling through integrin binding. Cross-linking of ICAM-1 has been shown to stimulate many endothelial cell signal trans-duction cascades, such as MAP kinase, src kinase, and NOX4 pathways.38–41 Recent work has also revealed that ICAM-1-dependent signaling responses regulate endothe-lial cell redox status by increasing intracellular glutathione levels that control cellular activation and inflammatory responses.39,42,43
Inhibition or genetic deficiency of ICAM-1 has been shown to protect mice against I/R injury in several organs, such as the heart, kidney, and brain.16,22,44–47 ICAM-1 is also important during the progression of chronic inflam-matory diseases, such that genetic loss of the molecule protects against experimentally induced colitis, SLE-associated vasculitis and glomerulonephritis, and reduces susceptibility to collagen induced arthritis.48–50
Given the diverse functions of ICAM-1 during an immune response, the precise role of this molecule in mediating leukocyte-endothelial cell interactions has been examined. Interestingly, the loss of ICAM-1 specifically influences the adhesion of certain leukocyte types in a stimulus-dependent manner. For example, loss of ICAM-1 decreases eosinophil adhesion in mesenteric venules in response to ragweed allergen challenge.51,52 However, TNF-α stimulation of neutrophil adhesion in ICAM-1 mutant mice has revealed that this protein is not required for adhesion or is redundant with other adhesion mol-ecules.27 Closer examination of this finding suggests that ICAM-1 is required for chemoattractant-mediated leuko-cyte adhesion in resting venules, but not TNF-α-stimulated venules.53 In vitro studies using endothelial cells from ICAM-1-deficient mice have shown that this molecule is important for monocyte firm adhesion and T-cell emigra-tion across endothelial monolayers.54–57 Studies have shown that ICAM-1 is necessary for optimal selectin-mediated rolling, in that leukocyte rolling velocities on TNF-α-stimulated vessels and endothelium were faster compared to wild-type controls.58,59 Recent studies have revealed a previously unappreciated step of the leukocyte recruitment cascade involving intraluminal crawling after firm adhesion but before transmigration.60,61 ICAM-1 interaction with the Mac-1 counter-ligand appears to gov-ern intraluminal neutrophil crawling on the endothelial cell

Chapter | 79 Recruitment of Inflammatory and Immune Cells in the Gut: Physiology and Pathophysiology 2105
surface perpendicular to the direction of blood flow, thus allowing the leukocyte to locate cell–cell junction regions for transmigration.60 These findings highlight a complex role for ICAM-1 in regulating endothelial responses during inflammation, suggesting all of these characteristics may be important in leukocyte-endothelial cell interactions.
ICAM-2 is constitutively expressed on the cell surface and was primarily described in endothelial cells.62 The structure of ICAM-1 and 2 are similar in that they con-sist of a cytoplasmic domain, a transmembrane domain, and Ig like regions. However, they differ in the number of extracellular Ig like domains in that ICAM-1 contains 5 Ig domains compared to 2 for ICAM-2. Unlike ICAM-1, ICAM-2 is not inducible by inflammatory mediators, suggesting that ICAM-2 is important for normal immune surveillance. Interestingly, gene-targeted loss of ICAM-2 does not alter lymphocyte homing or development of leu-kocytes. However, ICAM-2 deficiency reduces eosinophil transmigration across endothelial monolayers and pro-longs allergic eosinophil accumulation in certain organs.63 ICAM-3 is expressed on all resting leukocytes and also contains 5 Ig domains similar to ICAM-1.64,65 ICAM-3 is important for leukocyte aggregation and activation through its interaction with the counter-ligand LFA-1.64,66
VCAM-1 is a cytokine-inducible surface molecule that mediates adhesion of various leukocyte types, such as lymphocytes, monocytes, and eosinophils.67–69 VCAM-1 was identified through direct expression techniques using a cell–cell adhesion-based screening procedure with cytokine-induced cDNA genes. Candidate genes were transfected into epithelial cells and examined for adhe-sion to lymphocytic cell lines. Since this characterization, VCAM-1 has been shown to be involved in both acute and chronic inflammation, and is primarily expressed in endothelial cells. VCAM-1 binds α4β1 (VLA-4) and pos-sibly α4β7 integrin, and participates in leukocyte firm adhesion and migration. VCAM-1 ligand interactions have been reported to be mediated largely by domain 1 and pos-sibly domain 4. VCAM-1 has also recently been reported to bind the α9β1 integrin of neutrophils and facilitate neu-trophil migration across endothelial cells.70
PECAM-1 was originally identified through the sero-logical characterization of surface proteins of vascular endothelium and contains six Ig domains, a transmem-brane domain, and a cytoplasmic tail that can be differen-tially phosphorylated and palmitoylated.71 Modification of the cytoplasmic tail facilitates outside-in signaling, which can influence endothelial cell function (e.g., ang-iogenesis or cell survival) and leukocyte recruitment. PECAM-1 preferentially localizes at intercellular junc-tions of endothelial cells, suggesting a role in leukocyte emigration. Consistent with this hypothesis, blocking anti-bodies against PECAM-1 on the endothelium can prevent leukocyte emigration across endothelial monolayers.72,73
PECAM-1 has also been shown to be expressed on other cell types including platelets, monocytes, neutrophils, natural killer cells, and certain T-cell subsets that may facilitate adhesion and transmigration through homotypic binding of endothelial PECAM-1.
MAdCAM-1 was identified through monoclonal anti-body screening studies that showed discreet staining of high endothelial venules of mucosal lymph nodes (PPs).74 Additional studies of MAdCAM-1 expression identified constitutive expression in tissues involved in mucosal immunology as well as inducible expression by proin-flammatory mediators (e.g., TNF-α).75 As suggested by its tissue distribution, MAdCAM-1 mediates lymphocyte homing by directing adhesion and emigration across high endothelial venules of mucosal tissue. MAdCAM-1 contains 3 extracellular Ig domains with a mucin-like region between domains 2 and 3.76,77 Primary ligands for MAdCAM-1 include L-selectin and α4β7 integrin, which bind to Ig domain 1.30 Importantly, several reports have documented an important role for MAdCAM-1 in mediat-ing chronic inflammatory states involving GI tissue such as ulcerative colitis, Crohn’s disease, and experimental colitis models.78–81
The most recent immunoglobulin adhesion molecule that has been reported is JAM. Three different JAMs have been described in some detail and include JAM-A, B, and C.82 JAM expression is observed in endothelial and epithelial cells, leukocytes, and platelets, and consists of two extracellular Ig domains and a cytoplasmic tail that differentially associates with multiple signaling and cytoskeletal-associated proteins.83 The original identifica-tion of JAM (JAM-A) revealed junctional localization in endothelial cells that participated in monocyte transmi-gration.84 Studies demonstrate that JAM proteins localize to tight junctions in both epithelial and endothelial cells, and that members of the JAM subfamily homotypically bind other JAM molecules as well as heterotypic lig-ands.82,85–87 Specific heterotypic ligands for the JAM sub-family include the integrins LFA-1 (αLβ2), Mac-1 (αMβ2), VLA-4 (α4β1), and αVβ3, suggesting the role for these molecules in regulating leukocyte recruitment. Studies have shown that JAM–integrin interactions control leuko-cyte infiltration during inflammation.88–91 However, JAM may also regulate intestinal permeability and inflammatory responses through homotypic interactions. Recent work by Laukoetter et al. revealed complex roles of JAM-A in controlling intestinal inflammation.92 Interestingly, genetic deficiency of JAM-A did not alter GI epithelial architec-ture but did increase leukocyte infiltration and lymphoid aggregates concomitant with increased mucosal perme-ability. Surprisingly, these animals showed reduced clinical symptoms of dextran sodium sulfate (DSS_-induced coli-tis, less mucosal injury, and increased epithelial cell pro-liferation. Together, these results highlight that adhesion

SECTION | VI Consequences of Disregulated Physiology2106
molecule function often influences other histomorphologi-cal aspects of GI function besides leukocyte recruitment and inflammation.
79.2.1.2.1 Integrins
The integrin family of adhesion molecules consists of a wide array of heterodimeric proteins through various combinations of 17 α- and 8 β-subunit genes. Figure 79.2 illustrates the molecular associations between different α- and β-subunits. These proteins participate in cell–cell and cell–matrix adhesion, and have been shown to play important roles in regulating intracellular signal transduc-tion and cytoskeletal organization of all cell types. The α- and β-subunits are encoded by separate genes that do not necessarily show coordinate transcriptional regulation. As such, several α protein chains interact non-covalently with multiple β protein chains yielding a diverse array of heterodimer pairing. Several integrin ligands have been described and largely include members of the immu-noglobulin superfamily and extracellular matrix proteins.
The β2 integrins are heterodimeric proteins that consist of a common β-subunit (CD18) non-covalently attached to different α-subunits (CD11a-d).93 The β2 integrin fam-ily, or CD18 integrins, consists of four different adhe-sion proteins: LFA-1 (CD11a/CD18), Mac-1 (CD11b/CD18), p150/95 (CD11c/CD18), and CD11d/CD18. Importantly, expression of the β2 integrins is limited to leukocytes and platelets, which suggests their importance for immune responses. Members of the immunoglobulin superfamily are major ligands for the β2 integrins, includ-ing ICAM-1, 2, and 3, and members of the JAM family of proteins.58,94 Integrin-mediated cell adhesion is controlled through multiple mechanisms, including alterations in sur-face density and changes in receptor affinity. The impor-tant role for β2 integrin/ligand interactions in inflammatory and immune processes is illustrated by several studies
using gene-targeted mutant mice of CD18 to attenuate inflammatory responses under various conditions.94,95 Data from numerous studies indicate that the β2 integrins are critical mediators of leukocyte adhesion and emigration, co-stimulation and activation, leukocyte-mediated tissue damage, and serve pathophysiological roles during autoim-mune disease.96–101 However, it is important to understand that complete inhibition of all β2 integrins (genetic dele-tion or immunoneutralization of CD18) is considerably different than selective inhibition of a single member of the family (i.e., inhibition of CD11a, CD11b, CD11c, or CD11d). Several studies have shown that genetic inhibition of CD11a can confer similar protection against inflamma-tion and immunological disorders as CD18; however, loss of CD11b may exacerbate inflammatory responses and injury indicating unique roles of each adhesion molecule within the family.96,98,99,102
The α4 integrins, α4β1 (VLA-4) and α4β7, are primarily expressed on lymphocytes, yet may also be found in gran-ulocytes and monocytes. These adhesion molecules are unique in that they can participate in all of the steps nec-essary for leukocyte recruitment such as tethering, rolling, and firm adhesion.103 VCAM-1 ligand binding occurs with both molecules, while MAdCAM is the primary ligand for α4β7.30,104 Through these interactions, α4β7 facilitates lymphocyte homing to the mesenteric lymph nodes and PPs while VLA-4 plays a role in facilitating immune cell recruitment in the blood circulation. VLA-4 may also play an important role in autoimmune responses, since antibody blockade of the molecule protects in several autoimmune disease models.105–107
79.2.1.2.2 Cadherins
The cadherin family of adhesion proteins is typically iden-tified as surface proteins located in the adherens junc-tion or desmosome with specific calcium requirements for homotypic interaction.108,109 The cadherin proteins contain three general structural regions, including a cyto-plasmic domain, a transmembrane domain, and extracel-lular cadherin repeat domains that are structurally similar to Ig domains. The amino terminal end of the extracel-lular region contains the HAV domain that is primarily involved in homotypic binding. Cadherin molecules pro-vide structural support to adherens junctions and desmo-somes through binding catenins, which link to the actin cytoskeleton. Moreover, cadherins also influence signal pathways and gene expression through differential asso-ciation with various catenins (e.g., β- or γ-catenin).110,111 Numerous cadherins have now been identified and have been divided into classical and non-classical groups.108,112 A primary function of nearly all cadherins is the regulation of homotypic adhesion of several cell types such as epi-thelial, endothelial, and neuronal, as well as others.113,114 The homotypic adhesion of cells typically involves one
β8 β7
β1
β4
α1
α2 α3α4
α6
α5αvα9
α8 α7
αIIbαL αM αX αD
αE
β6
β5
β2
β3
Cationbindingregion
α-chain β-chainCytoskeletion
bindingregion
(A) (B)
FIGURE 79.2 Integrin subunit interactions and molecular properties. (A) Various heterodimeric associations of α- and β-subunit associations. (B) Important molecular features of integrin subunits, including the cationic binding feature of the α-subunit and the cytoplas-mic cytoskeletal binding region of the β-subunit.

Chapter | 79 Recruitment of Inflammatory and Immune Cells in the Gut: Physiology and Pathophysiology 2107
predominant cadherin molecule; however, different cad-herin molecules may also be expressed in the same cell. For example, the lateral epithelial adherens junction is maintained by E-cadherin homotypic interactions, yet both N- and P-cadherin may also be expressed.115 Recent reports have also shown that cadherins may bind other adhesion molecules in a heterotypic manner. T-lymphocyte adhesion to epithelial cells has been reported to occur through T-cell αEβ7 integrin interaction with epithelial E-cadherin.116,117 The pathological importance of this het-erotypic interaction between E-cadherin and β7 integrin could be minimal, since genetic loss of β7 integrin does not prevent spontaneous colitis in IL-2-deficient mice and only delays the development of experimental colitis in the CD4CD45RBhigh transfer model.118
Endothelial cell specific vascular endothelial cadherin (VE-cadherin/cadherin-5) plays important roles in con-trolling endothelial cell growth, and solute barrier prop-erties, and leukocyte transmigration.118,119 Numerous reports have shown that various cytokines, chemokines, and biochemical mediators (e.g., reactive oxygen species, bradykinin, histamine, etc.) stimulate VE-cadherin phos-phorylation, dissociation from catenins, and redistribution away from lateral cell–cell junctions, resulting in increased endothelial and microvascular permeability.119–123 Recent findings suggest that leukocyte β2 integrin binding to counter-ligands such as ICAM-1 may activate signaling pathways that lead to transient and discreet disorganiza-tion of VE-cadherin homotypic junctional binding between endothelium to allow for leukocyte transmigration.124
79.2.1.2.3 Platelet Glycoproteins
An important role for platelet adhesion to the endothe-lium or subendothelial matrix has recently emerged in several immune-based diseases that involve the microv-asculature of numerous organs including the GI system. Platelets contain several unique adhesion molecules that facilitate interaction with endothelium and other platelets. The GPIb-IX-V complex of glycoproteins facilitates plate-let adhesion through binding counter-ligands P-selectin, von Willebrand factor (vWF), and Mac-1.125,126 GPIb-IX-V-dependent adhesion is important for platelet adherence under high shear stress to matrix vWF (e.g., denudation of arterial endothelium), bacterial endotoxin-mediated adhesion to the microvasculature, and platelet recruit-ment to mesenteric venules activated with histamine.127–130 Likewise, platelet GPIIa-IIIb (also classified as integrin αIIbβ3) also mediates platelet adhesion through lig-and binding to other GPIIa-IIIb molecules, ICAM-1 via fibrinogen bridging, Mac-1, and αvβ3 integrin. GPIIa-IIIb is important for platelet adhesion to venular endothelial cells experiencing low shear stress and binds to fibrino-gen linked to ICAM-1 in venules of post-ischemic intes-tine and liver.131–133 Both the GPIb-IX-V and GPIIa-IIIb
glycoproteins participate in intracellular signaling proc-esses with GPIb-IX-V demonstrating outside-in and inside-out signaling, while GPIIa-IIIb undergoes inside-out activation.125 The glycoprotein vWF is released from platelet α-granules as well as endothelial cell Weibel-Palade bodies that facilitate platelet–platelet binding and adhesion to the vessel wall. These adhesive interactions can be further aided by platelet P-selectin and P-selectin glycoprotein ligand-1 (PSGL) interaction among platelets or with endothelium.
79.2.1.2.4 Occludin and Claudins
Endothelial and epithelial tight junctions represent a final barrier through which leukocytes pass to access intersti-tial tissue spaces. Tight junctions serve as both a “gate” function to regulate cell passage and as a barrier role in maintaining endothelial and epithelial solute permeability characteristics. Dysregulation of either function has been reported to contribute to leukocyte recruitment and inflam-matory responses.134,135 Occludin was the first integral tight junction protein identified through membrane frac-tion and immunolabeling techniques.136 Occludin is a 65 kDa integral membrane protein containing four trans-membrane domains with two hydrophobic extracellular loops with cytosolic amino and carboxy-terminal ends.137 The second extracellular loop mediates homotypic inter-action with itself as well as JAM and claudin proteins. The carboxy-terminus of occludin binds with ZO proteins (ZO-1 and ZO-2) that link it to the actin cytoskeleton. Importantly, junctional organization of occludin restricts leukocyte transmigration across both endothelial and epi-thelial cells, and is actively reorganized away from lateral cell–cell junctions by several agents (e.g., leukocytes, oxi-dants, cytokines, chemokines), thereby increasing solute permeability.123,138–144 Genetic deficiency of occludin does not alter morphological properties of tight junctions or dif-ferences in epithelial barrier properties, but does result in chronic inflammation and hyperplasia of GI epithelium.145 Interestingly, studies have shown that anti-CD3 stimulation of cultured T-cells and intraepithelial lymphocytes upregu-late occludin expression in vitro and in vivo.146,147 These findings demonstrate that occludin expression plays a role in regulating leukocyte recruitment and GI mucosal immu-nology that still remains poorly understood.
The claudin proteins are the largest protein family found within tight junctions, and they primarily regulate permselectivity of endothelial and epithelial cells. The claudin protein family consists of 24 different members with molecular weights ranging between 20 and 27 kDa.148 The structure of claudin proteins are similar to occludin in that they are tetra-span integral membrane proteins with two extracellular loops; yet they do not share sequence homology with occludin.137 The carboxy-terminal tail of claudin proteins also binds ZO proteins, which link them

SECTION | VI Consequences of Disregulated Physiology2108
to the actin cytoskeleton. Claudin proteins bind each other in a homo- and heterotypic manner as well as in cis or trans interaction formats. These binding properties form the basis for the characteristic tight junction protein strands as seen by freeze-fracture electron microscopy and provide a wide array of interactive binding conforma-tions that confer unique barrier functions of epithelial and endothelial cells from different tissues.149 Claudins 5 and 1 play important roles in regulating endothelial cell bar-rier function and have been suggested to be involved in modulating leukocyte recruitment.150–152 However, much less is known regarding the importance of claudin proteins in regulating leukocyte recruitment across endothelial and epithelial cells.
79.3 REGULATION OF BLOOD CELL–ENDOTHELIAL CELL INTERACTIONS IN NON-LYMPHOID TISSUES
79.3.1 Adhesion Molecules
The recruitment of leukocytes to sites of inflammation in the GI tract is an orderly and well-regulated process that allows for both a rapid and sustained accumulation of inflammatory cells in affected tissue. A multistep model of leukocyte binding to vascular endothelium (Figure 79.1) has been universally adopted to explain the sequence and time course of involvement of different adhesion mole-cules in the recruitment of leukocytes in inflamed tissue. The initial event in this process is a weak adhesive interac-tion that results in leukocyte rolling along the endothelial lining of blood vessels. This interaction, which can occur within minutes of an inflammatory challenge, is largely mediated by the selectins. The transiently bound (or teth-ered) leukocytes are exposed to low concentrations of chemoattractants/inflammatory mediators that can result in leukocyte activation, which rapidly (in minutes) leads to an increased expression and/or activation of integrins on the rolling leukocytes. The leukocyte integrins (e.g., CD11/CD18) can bind to counter-receptors that are con-stitutively expressed on the surface of endothelial cells (e.g., ICAM-1), thereby allowing leukocytes to become firmly attached to the endothelium and remain stationary. The subsequent transendothelial migration of leukocytes into the interstitial compartment involves the participation of additional adhesion glycoproteins such as PECAM-1, MAdCAM-1, or JAM-A.153,154
The dual radiolabeled monoclonal antibody tech-nique has provided novel insights into the magnitude and kinetics of endothelial CAM expression in GI tract and other vascular beds.155–158 Figure 79.3 illustrates the rela-tive magnitude of basal and induced (by LPS or TNF-α) expression of different endothelial CAMs in the murine intestinal vasculature. It further shows that members of the
immunoglobulin supergene family exhibit a high level of constitutive expression in the intestine, and that substantial sustained increases in expression can be demonstrated for ICAM-1, VCAM-1, and MAdCAM-1. However, the high basal levels of PECAM-1 and ICAM-2 appear to remain unchanged in the intestine even after stimulation with LPS or TNF-α. These responses for the Ig supergene family contrast with those seen for the selectins, which exhibit a much lower level of basal expression with more profound (yet transient) increases in expression after endothelial cell activation.75,155–161
Significant constitutive expression of P-selectin can be demonstrated in the intestine of wild-type mice, but not in mice that are genetically deficient in P-selectin.155 The high constitutive levels of P-selectin and other endothe-lial CAMs (see Table 79.2) in the gut are consistent with the view that this organ is normally in a state of control-led inflammation. Transcription-dependent upregulation of both P- and E-selectin can be induced by cytokines and LPS (Figure 79.3), with P-selectin expression reaching a
P-selectin
PECAM
MAdCAM-1
ICAM-1
ICAM-2
VCAM-1
P-selectin
(A)
(B)
End
othe
lial e
xpre
ssio
n
E-selectin
2 4 6 8 10 12
2 4 6 8 10
End
othe
lial e
xpre
ssio
n
12Time (hours)
Time (hours)
14 16 18 20 22 24
FIGURE 79.3 Kinetics of endothelial cell adhesion molecule expression in the mouse intestine after challenge with cytokines or endotoxin. Panel A selectins; panel B immunoglobulin supergene family. Also shown is the response of P-selectin expression to histamine challenge.75,155,158–160

Chapter | 79 Recruitment of Inflammatory and Immune Cells in the Gut: Physiology and Pathophysiology 2109
maximum between 4 and 8 hours and E-selectin requir-ing 3 to 5 hours for peak expression.155 The increment in selectin expression associated with transcription generally exceeds 10-fold. Histamine also significantly increases the expression of P-selectin, but not E-selectin in the GI tract and most vascular beds.155 However, unlike the tran-scription-dependent response, histamine produces approxi-mately a 2- to 4-fold increase in P-selectin expression on endothelial cells within 5 minutes and the adhesion mol-ecule remains elevated for as long as 1 hour. The rapid expression of P-selectin after histamine likely represents mobilization of a preformed pool of the adhesion mol-ecule from Weibel-Palade bodies. The histamine-induced P-selectin expression in all vascular beds is inhibited by a histamine-H1- (but not an H2)-receptor antagonist, indi-cating that histamine engagement of H1 receptors on endothelial cells results in the mobilization of preformed P-selectin to the endothelial cell surface.155
Direct visualization of the microvasculature in GI tis-sues that are either acutely or chronically inflamed has revealed that leukocytes selectively bind to endothelial cells that line post-capillary venules. Leukocyte sequestra-tion in capillaries can occur during GI inflammation, but steric hindrance of less deformable circulating leukocytes within long narrow capillaries, rather than cell–cell interac-tions mediated by adhesion molecules, is often offered as an explanation for this response.161 Endothelial cell swell-ing within capillaries as well as compression of the capil-lary lumen by an elevated interstitial fluid pressure caused by accumulation of edema fluid have also been impli-cated in the entrapment of leukocytes within capillaries of inflamed tissues.162 However, it is the endothelial cells that line the walls of post-capillary venules that appear to sustain most of the leukocyte trafficking that occurs in inflamed tissues. In rat mesenteric microcirculation, for
example, 39% of all leukocytes passing through venules are rolling, while only 0.6% of leukocytes roll in the upstream arterioles.163,164 Relatively higher shear rates in arterioles and higher endothelial CAM expression in venules are two explanations that are most often provided for the differences in leukocyte–endothelial cell adhesion between these two vascular segments.
Shear forces generated by the movement of blood within the microvasculature are generally higher in arte-rioles than in downstream venules. For example, a 30 μm diameter venules in rat mesentery is likely to exhibit a resting shear rate that is half that of an arteriole of com-parable diameter. Since wall shear stress, or shear rate, represent anti-adhesion forces that oppose the proadhesive forces generated by CAMs, vessels with a low spontane-ous shear rate (low blood flow) would tend to exhibit more leukocyte adhesion than vessels with high shear rates. For this reason, it has been proposed that leukocytes rarely roll and adhere in arterioles because the higher shear forces exceed the adhesive force in these vessels. Based on this proposal, one might predict that reductions in arteriolar shear rate to levels experienced by venules should pro-mote leukocyte adhesion in arterioles. However, this is not the case, because when mesenteric arterioles and venules of the same size are exposed to the same range of shear rates (100–1250 sec-1), venules exhibit far more leuko-cyte rolling and adherence than arterioles.165 Studies using retrograde perfusion of the microcirculation have also provided some insight into the role of shear rate in arteriolar-venous differences in leukocyte–endothelial cell adhesion. In the mesentery, retrograde perfusion is associ-ated with a reduced flux of rolling leukocytes in venules and increased leukocyte rolling in arterioles.166 However, more leukocytes still rolled in venules during normograde perfusion than rolled in arterioles during retrograde flow. These observations indicate that hemodynamic differences between arterioles and venules cannot explain the predi-lection for leukocyte rolling and adherence in venules, and that a higher density of counter-receptors (ligands) for leukocyte adhesion molecules on venular endothelium is a more likely explanation.111,166–169
79.3.2 Products of Endothelial Cell Activation
Bacterial toxins as well as a variety of cytokines produced by macrophages and mast cells that normally reside in the GI tract can engage with specific receptors on endothelial cells to elicit an increased expression of CAMs. Inducible gene expression, mediated by transcription factors, appears to be a key regulator mechanism that allows endothe-lial cells to increase the synthesis and surface expression of the CAMs that regulate leukocyte trafficking.153,154 Of the many transcription factors that have been identified
TABLE 79.2 Regional Differences in the Constitutive Expression of Endothelial Cell Adhesion Molecules
Organ Endothelial CAM Expression (molecules 106 per cm2)
P-selectin E-selectin ICAM-1 VCAM-1
Small intestine
254.9 87.8 171.0 32.7
Lung 26.6 1.10 268.1 23.7
Heart 5.7 46.5 92.5 81.8
Muscle 10.2 0.0 89.0 35.0
Brain 4.8 1.5 9.0 42.9
Data derived from 5–8.

SECTION | VI Consequences of Disregulated Physiology2110
and characterized to date, NF-κB and AP-1 appear to be most relevant to the regulation of endothelial CAMs. LPS, cytokines, and oxidative stress can result in the activation of both NF-κB and AP-1 in endothelial cells, and there is evidence that clearly links the activation of these transcrip-tion factors with the increased CAM expression caused by the well-established inducing factors. Binding sites for NF-κB have been identified in the promoter regions of the genes for E-selectin, VCAM-1, MAdCAM-1, and ICAM-1, while AP-1 has a binding site on the promoter region of the ICAM-1 gene.154,170–172
Reactive oxygen species (ROS) are products of endothe-lial cell activation that are frequently implicated in the reg-ulation of endothelial CAMs and show a strong linkage to both NF-κB and AP-1. ROS are capable of eliciting both a rapid and transient as well as a slow, prolonged increase in leukocyte-endothelial cell adhesion. The rapid response may be explained by the ability of ROS to induce the pro-duction of a variety of inflammatory mediators (e.g., PAF, C5a, and LTB4) that can elicit the rapid upregulation/acti-vation of β2 integrins on leukocytes, which in turn can rap-idly initiate the firm adhesion of leukocytes to endothelial cells. ROS rapidly induce the activation of phospholipase A2 (PLA2) in endothelial cells, leading to the generation of platelet-activating factor (PAF) and arachidonic acid metab-olites. When endothelial cell-derived hydrogen peroxide reacts with plasma, a C5a-like chemotactic factor is gener-ated through the hydrolysis of C5. The ability of H2O2 to activate, complement, and generate a chemotactic agent in plasma is enhanced by the presence of catalytically active iron (e.g., Fe EDTA, hemoglobin), suggesting that the proc-ess of complement activation is not brought about by H2O2 per se, but by an oxidant derived from H2O2.
170,171
ROS can also induce a rapid transient (transcription-independent) and slow prolonged increase in the expres-sion of endothelial CAMs. The rapid response reflects the ability of ROS to mobilize the preformed pool of P-selectin from Weibel-Palade bodies to the endothelial cell surface. Both in vitro and in vivo experiments sup-port a role for a ROS-dependent, rapid upregulation of P-selectin on vascular endothelial cells. Exposure of mesenteric venules to a superoxide-generating system results in an enhanced recruitment of rolling leukocytes, which is prevented in animals receiving a P-selectin-specific monoclonal antibody. Similarly, exposure of mon-olayers of cultured endothelial cells to an oxidative stress (e.g., anoxia-reoxygenation) results in the rapid surface expression of P-selectin, a response that is significantly blunted by catalase or allopurinol, suggesting that xan-thine oxidase-derived oxidants mediate the rapid P-selectin mobilization.154,170–172
The slow and prolonged increase in endothelial CAM expression induced by ROS reflects the ability of these endothelial cell products to activate the oxidant-sensitive
transcription factors NF-κB and AP-1. Antioxidants and iron-chelators have been shown to interfere with the acti-vation of these transcription factors in endothelial cells and lead to an attenuated upregulation of endothelial CAMs (e.g., VCAM-1, E-selectin) in response to a variety of stimuli, including cytokines, LPS, and exogenous oxi-dants. The CAM biosynthesis initiated by ROS through activation of NF-κB and AP-1 leads to a more intense and prolonged expression of CAMs on the endothelial cell sur-face, which serves to sustain leukocyte recruitment into inflamed tissue for a period of hours to days.154,170–172
Endothelial cell-derived nitric oxide (NO) has also been implicated as a modulator of leukocyte–endothe-lial cell adhesion in the GI tract. Inhibition of nitric oxide synthase (NOS) with L-arginine analogs (e.g., L-NAME) rapidly induces an inflammatory response that is charac-terized by the recruitment of rolling, adherent, and emi-grating leukocytes in mesenteric venules; the formation of platelet-leukocyte aggregates; and the degranulation of mast cells in the perivenular interstitium. NOS inhibi-tion is also accompanied by an oxidative stress in venular endothelium and in perivenular mast cells. Enhanced leu-kocyte adhesion in post-capillary venules has also been demonstrated in endothelial NOS-deficient mice, com-pared to their wild-type counterparts. These observations have lead to the proposal that NO is an endogenous inhibi-tor of leukocyte–endothelial cell adhesion. One mecha-nism that is frequently offered to explain the anti-adhesion properties of NO relates to the ability of this molecule to rapidly interact with and decompose superoxide. Because superoxide reacts with NO three times faster than superox-ide dismutase (SOD), it has been proposed that NO serves as a physiological scavenger of superoxide. The possibil-ity that NO exerts its anti-adhesive properties through this mechanism is supported by the observation that NOS inhi-bition elicits an oxidative stress in venular endothelium and that NO donating agents (e.g., NONOates) are only effective in inhibiting leukocyte–endothelial cell adhesion in models of inflammation wherein SOD also exerts an anti-adhesion effect. NO donors are also known to inhibit several of the other inflammatory responses that have been attributed to superoxide-mediated signaling PLA2 activa-tion, including the rapid mobilization of P-selectin in acti-vated endothelial cells, transcription-dependent endothelial CAM expression, mast cell degranulation, and platelet–leukocyte aggregation.154,170,171,173,174
While NO and superoxide per se are often ascribed anti- and proinflammatory roles, respectively, the reac-tive nitrogen oxide species (RNOS) that are produced by their chemical interaction can yield either phenotype (anti- or proinflammatory), depending on whether there is net oxidation or nitrosation of specific molecular targets that regulate the inflammatory response. These observa-tions have led to the concept that a critical determinant of

Chapter | 79 Recruitment of Inflammatory and Immune Cells in the Gut: Physiology and Pathophysiology 2111
the adhesive phenotype (pro- or anti-) assumed by venu-lar endothelium is the existing balance between ROS and NO.175 Under normal conditions, the balance between NO and ROS favors an anti-adhesive phenotype, because NO chemistry predominates as a result of the approximately 1000-fold greater production of NO compared to super-oxide (Figure 79.4; Control). The excess NO yields an anti-adhesive phenotype through sustained inhibi-tion (related to target-specific nitrosation) of transcrip-tion factor activation and endothelial CAM production/expression. The excess NO also favors cGMP-mediated, transcription-independent signaling that tends to promote an anti-inflammatory and anti-thrombogenic phenotype in endothelial cells. However, during inflammation (Figure 79.4; Inflammation), the flux of superoxide relative to NO increases such that ROS-dependent mechanisms predominate. Under these conditions, ROS-mediated transcription-dependent and -independent processes are initiated that favor (1) the production of inflammatory mediators that activate β2 integrins on leukocytes, (2) the mobilization of preformed pools of P-selectin, and (3) the transcription-dependent upregulation of different endothe-lial CAMs. These changes promote the rapid and sustained
leukocyte–endothelial cell adhesion that accompanies inflammation.
79.3.3 Auxiliary Cells
Although endothelial cells remain a major focal point in the search for the source(s) of mediators that elicit and amplify the leukocyte–endothelial cell adhesion dur-ing inflammation, there is growing evidence that other cell populations also contribute to this component of the inflammatory response.176,177 Mast cells, macrophages, and platelets are good examples of auxiliary cells that are in proximity to venular endothelial cells and can produce a variety of inflammatory mediators (e.g., PAF, ROS) and cytokines that are known to promote leukocyte adhesion. Mast cell products have been implicated in the leukocyte–endothelial cell adhesion in different experimental models of GI inflammation.176Support for this view is provided by reports describing increased numbers of activated and/or degranulated mast cells in proximity to post-capillary venules. Further support is given by results obtained from experiments employing agents that degranulate (compound 48/80) or stabilize (ketotifen) mast cells or that antagonize
Pro-inflammatoryPhenotype
Anti-inflammatoryPhenotype
Pro-inflammatoryPhenotype
Anti-inflammatoryPhenotype
Transcription-independent
signaling
Transcription-independent
signaling
Transcription-independent
signaling
Transcription-independent
signaling
Transcription factoractivation
Target-specificoxidation
Target-specificoxidation
Target-specificnitrosation
Target-specificnitrosation
Transcription factoractivation
cGMPcGMPRNOS
ROS NO
Control Inflammation
ROS NO
RNOS
O2.–, H2O2
(N2 O
3 )(O
NOO*)
(ONOO*) (N
2 O3 )
O2.–, H2O2
FIGURE 79.4 A critical determinant of the adhesive phenotype (pro-or anti-) assumed by venular endothelial cells is the existing balance between reactive oxygen species (ROS) and nitric oxide (NO). Under normal conditions (Control), the balance between NO and ROS favors an anti-inflammatory phenotype because NO chemistry predominates. The excess NO yields an anti-inflammatory phenotype through sustained inhibition (related to target-specific nitrosation) of transcription factor activation, and cGMP-mediated, transcription-independent signaling. During inflammation (Inflammation), the balance between NO and ROS is shifted toward the latter species as a result of a reduction in NO biosynthesis, inactivation of NO by O2., or both. In this instance, the flux of O2. relative to NO increases such that ROS-dependent mechanisms predominate and NO-dependent mechanisms are rendered inactive. ROS (and possibly RNOS)-mediated transcription-dependent and -independent processes then promote a proinflammatory phenotype, the intensity of which not only depends on the relative fluxes of NO and O2. but also on the specific RNOS formed.175

SECTION | VI Consequences of Disregulated Physiology2112
mediators that are relatively unique to mast cells (antihista-mines). Relatively little information is available concerning the role of macrophages in the regulation of leukocyte–endothelial cell adhesion in the intact GI tract, largely as a result of the limited experimental strategies that are avail-able to selectively manipulate the numbers and activity of these resident phagocytic cells in GI tissues.177
A growing number of reports reveal that the develop-ment of a proinflammatory phenotype in the microvascu-lature is frequently accompanied by a prothrombogenic phenotype, which likely reflects molecular and chemi-cal changes in endothelial cells that create a hyperadhe-sive surface for both platelets and leukocytes.178 This link between hemostasis and inflammation appears to have important pathophysiological consequences, with plate-lets increasing the intensity of the inflammatory response and exacerbating microvascular dysfunction and tissue injury. Several experimental models of GI inflamma-tion are associated with the formation of platelet–leuko-cyte aggregates, the adhesion of platelets directly onto endothelial cells, and the attachment of platelets to already adherent leukocytes. There is mounting evidence that adherent leukocytes represent a major substrate for the binding of platelets to the walls of inflamed microvessels (Figure 79.5).179–181 Since platelets have also been shown to play a major role in the recruitment of leukocytes, a co-dependency of platelet and leukocyte adhesion appears to exist in inflamed venules.181 Platelet–leukocyte adhesion can be mediated by different ligand-receptor interactions, including P-selectin (platelet)–PSGL-1 (leukocyte) and GPIbα (platelet)–CD11b/CD18 (leukocytes) interactions. Neutrophils may also entrap platelets via the release of
neutrophil extracellular traps (NETs), which are largely comprised of DNA.182 Upon activation, neutrophils can release granular proteins and chromatin that combine to form the structural backbone of NETs. While NETs are thought to play a role in the entrapment and killing of pathogens, there is also evidence suggesting that platelets under flow in vitro bind avidly to NETs, thereby promot-ing thrombosis.183
Once platelets attach to leukocytes the capacity of the latter cells to produce superoxide is dramatically increased, suggesting that diffusible molecules liberated by the attached platelets and/or signaling mechanisms that are activated as a result of this heterotypic cell adhesion greatly enhance the activation state of the leukocyte.178 It is noteworthy that roughly half of the leukocytes that adhere in inflamed intestinal venules are platelet bear-ing and the other half are platelet free, suggesting that the subpopulation of adherent leukocytes that sustain platelet adhesion may achieve a higher state of activation that favors platelet adhesion. Since neutrophil-derived superoxide has also been implicated in the modulation of platelet adhesion in intestinal venules,184 an enhanced pro-duction of this ROS by the platelet-bearing leukocytes may account for the preferential binding to a subset of adher-ent leukocytes. A role for ROS is further supported by the observation that the formation of NETs by activated neu-trophils also depends on ROS formation by NADPH oxi-dase.182 Because the nature of underlying mechanisms and the pathophysiological importance of the platelet–vessel wall interactions that accompany inflammation remain poorly understood, additional work is needed to address this phenomenon.
PSGL-1P-selectimPSGL-1
vWF
GPIbα
GPIbα
GPIIb/IIIa
ICAM-1
Fibrinogen
GPIbα
P-selectin
P-selectin
Mac-1
ICAM-1
CD18
Leukocyte-independentplatelet adhesion
Leukocyte-dependentplatelet adhesion
FIGURE 79.5 Platelets are also recruited into the inflamed microcirculation via mechanisms that are dependent and independent of leukocyte adhesion. Platelets can directly interact with venular endothelium through interactions between adhesion molecules expressed on both cell types. Alternately, platelets can accumulate in venules by binding to the surface of adherent leukocytes or by entrapment in neutrophil extracellular traps (NETs).

Chapter | 79 Recruitment of Inflammatory and Immune Cells in the Gut: Physiology and Pathophysiology 2113
79.4 GUT-ASSOCIATED LYMPHOID TISSUE AND INTESTINAL IMMUNITY
The intestinal mucosa encounters more antigens than any other tissue in the body and, consequently, represents the largest and most complex component of the immune sys-tem. Indeed, the intestinal tract is colonized by more than 100 trillion (1014) microorganisms with the vast major-ity residing within the colonic lumen.185,186 Fortunately, the intestinal immune system has evolved efficient mecha-nisms to distinguish between potentially pathogenic bacte-ria, parasites, and viruses from harmless dietary proteins and commensal bacteria. In addition to being able to respond to specific antigens, the mucosal immune system is able to choose the appropriate effector functions necessary to deal with each pathogen. Specific populations of lymphocytes play major roles in mediating and regulating these effector functions in vivo and are called T-lymphocytes or T-cells. The major T-cell population that protects the host from invading pathogenic bacteria are termed CD4 T-cells. Currently, there are three established subsets of CD4 effec-tor T-cells: the T-helper cell-1 (Th1), Th2, and Th17 effec-tor cells.187 Classical Th1 cells are produced in response to antigens derived from intracellular bacteria (and viruses) and secrete IFN-γ, IL-2, and lymphotoxin-α (LT-α). They
can be distinguished from other effector cells by their sur-face expression of CCR1, CCR5, and CXCR3.187 Th2 cells are generated in response to parasitic helminthes; produce IL-4, IL-5, and IL-13; and express CCR3 and CCR4.187 Th17 effector cells develop primarily in response to certain extracellular bacteria and fungi, produce IL-17A; IL17F, and IL-22; and express CCR4 and CCR6.187
To mount an effective immune response to potentially harmful enteric microorganisms or to maintain tolerance to commensal bacteria and food antigens, the intestinal tract has evolved a complex network of lymphoid tissue within the gut that is involved in antigen transport, processing, and presentation to T-cells. This gut-associated lymphoid tissue (GALT) is comprised of several discrete inductive sites that include the macroscopically visible PPs and the microscopic lymphoid aggregates (isolated lymphoid fol-licles) that are scattered throughout the lamina propria of the intestine. The PPs are “nodules” of lymphoid aggre-gates immediately underlying the intestinal epithelium and are found throughout the entire length of the small intes-tine. These structures consist of collections of large num-bers of T-cells separated by well-defined B-cell follicles. In addition, PPs are separated from the intestinal lumen by a single layer of columnar epithelial cells called folli-cle-associated epithelium (FAE; Figure 79.6). The space
Enteric Antigens
M Cell
DC
BCFT-cellAfferent
LymphaticsFree Ag
BloodAg-Loaded
DC
AfferentLymphatics
EfferentLymphaticSpleen
GUT
Peyer’sPatch MLN
FIGURE 79.6 Intestinal mucosal immune responses to enteric bacterial antigens. Enteric bacterial antigens may enter the Peyer’s patches via transport by the M cells where they are endocytosed by dendritic cells (DCs) within the subepithelial dome region. Antigen-loaded DCs may then inter-act with T-cells within the PPs to prime the lymphocytes or they may migrate from the PPs to the gut-draining mesenteric lymph nodes (MLNs) by way of the afferent lymphatics. Naive T-cells that enter the MLNs may interact with these antigen-loaded DCs resulting in the priming, polarization, and expansion of the T-cells to yield effector cells. These effector cells then exit the MLNs via the efferent lymphatics, return to the systemic circulation, and home to the gut lamina propria. Enteric antigens may also may be endocytosed by DCs within the gut lamina propria and migrate to the MLNs via the afferent lymphatics. Finally, free enteric antigens may be absorbed by the intestinal blood supply and transported to the spleen and/or peripheral lymph nodes by way of the systemic circulation. Once in these lymphoid tissues, free antigen may be processed and presented by DCs, thereby initiat-ing potential immune responses within the spleen. (Modified from 190 with permission.)

SECTION | VI Consequences of Disregulated Physiology2114
immediately underlying the FAE is referred to as the sub-epithelial dome (SED). The FAE can be distinguished from the epithelial cells that cover intestinal villi by its less pronounced brush border, reduced levels of digestive enzymes, and the large number of infiltrated lymphocytes (both T- and B-cells) and antigen-presenting dendritic cells (DCs). The most characteristic feature of the FAE is the presence of microfold (M) cells (Figure 79.6). These cells are specialized enterocytes that do not contain the surface microvilli or the layer of mucous that covers all other epi-thelial cells. The M cells play a critical role in binding invasive microorganisms and particulate antigens as well as transport of luminal antigens to the SED. In addition to the GALT, the mesenteric lymph nodes (MLNs) play an as important or even a more important role in mount-ing immune responses to invading microorganisms. This lymphoid tissue represents the largest lymph nodes in the body and serves to collect and concentrate antigens drain-ing from the intestinal mucosa.
The first step in mounting an effective immune response against enteric pathogens is the uptake and trans-port of enteric antigens to the PPs and MLNs. One of the best characterized pathways for this process involves the uptake of luminal antigens by the M cells and trans-fer to the underlying SED region of the PPs (Figure 79.6). There, the antigen is endocytosed by professional antigen-presenting cells (DCs) followed by migration of the DCs to the B-and T-cell regions of the PPs. Interaction of anti-gen-loaded DCs with the different B- and T-cell popula-tions primes/activates B-cells to produce the antimicrobial immunoglobulin IgA. Although it has been suggested that antigen-loaded DCs may also bind to and prime naive (antigen-inexperienced) T-cells to differentiate into differ-ent T-helper subsets within the PPs, the evidence defini-tively demonstrating a role for PPs as a major inductive site for the generation of antimicrobial Th1/Th17 effector cells is somewhat vague and ill defined.187–192 Much of the current evidence suggests that antigen-loaded DCs are transported from the PPs to the MLNs via the afferent lymphatics. Thus, it has been suggested that MLNs may function as the primary inductive site where naive T-cells encounter enteric antigens and are converted to disease-producing Th1 and/or Th17 effector cells.188–197
Luminal antigens may also gain access to the intesti-nal lamina propria via their endocytosis by DCs that reside within the intraepithelial cell compartment of the small bowel. Rescigno and co-workers have demonstrated that CX3CR1 and possibly CD11bTLR5 DCs migrate to the basolateral space between epithelial cells where they extend their pseudopodia apically/luminally between epithelial cells to “sample” the luminal environment.198 Because antigen-loaded CX3CR1 DCs are unable to migrate to the MLNs, they appear to promote the gen-eration of Th17 locally within the lamina propria of the
gut.198 Finally, enteric antigens may gain access to the intestinal tissue by simple paracellular and/or transcellu-lar diffusion processes (Figure 79.6). These antigens may then be endocytosed by interstitial DCs within the lamina propria where they may migrate to the MLNs or free anti-gen may diffuse from the lamina propria into the systemic circulation where they are captured/endocytosed by DCs localized within other secondary lymphoid tissue such as the spleen and/or peripheral lymph nodes (Figure 79.6).
79.4.1 T-Cell Homing, Priming, and Polarization
To mount an immune response toward enteric antigens, naive T-cells must traffic from the blood to the GALT and MLNs where gut-derived antigens have been concen-trated and presented upon the surface of DCs. Migration of naive T-cells from the blood to the GALT and MLNs is a complex process that is controlled by a sequence of three molecularly distinct adhesion and signaling steps that include tethering of T-cells to the endothelial sur-face, rolling along the endothelial cell surface and finally activation-induced firm adhesion of the lymphocytes to the endothelium. These processes occur exclusively by way of high endothelial venules (HEVs), which are com-posed of specialized post-capillary venular endothelial cells in the these lymphoid tissues.199–203 HEVs associ-ated with PPs contain MAdCAM-1, whereas HEVs within MLNs express both MAdCAM-1 and PNAd. It is thought that T-cell-associated L-selectin (CD62L) binds to both MAdCAM-1 and PNAd to tether the lymphocytes to the HEVs to initiate T-cell rolling (Figure 79.7A).204 Although the L-selectin/MAdCAM-1 and L-selectin/PNAd interac-tions are thought to mediate much of the T-cell tethering and rolling in the MLNs, α4β7 may also be used by naive T-cells to tether themselves to MAdCAM-1 thereby pro-viding additional tethering capacity for these cells in both PPs and MLNs (Figure 79.7A).201,202 Interaction of T-cell-associated chemokine receptor CCR7 with secondary lym-phoid tissue chemokine (SLC; CCL21) and/or Epstein Barr virus-induced gene-1 ligand chemokine (ELC; CCL19) presented on the luminal surface of the HEVs activates LFA-1 (CD11a/CD18) and α4β7 on the naive T-cells to bind to ICAM-1 and MAdCAM-1, respectively. These interactions promote firm adhesion and lymphocyte arrest, which ultimately leads to T-cell extravasation into the MLNs and PPs. (Figure 79.7A).200–203 Once naive CD4 T-cells enter the MLNs (and/or PPs), they may encounter their cognate enteric antigens presented on the surface of DCs in association with major histocompatabil-ity complex class II (MHC II). In a process that is not well understood, T-cells move into close proximity of the DCs, ultimately binding to the MHC-Ag complex via its T-cell receptor and initiate cell priming. This antigen-specific

Chapter | 79 Recruitment of Inflammatory and Immune Cells in the Gut: Physiology and Pathophysiology 2115
priming of naive T-cell induces their conversion or polar-ization into a Th1 and/or Th17 effector phenotype as well as promotes clonal expansion of these effector cells within the lymphoid tissue. During this process, the T-cells shed their L-selectin and enhance their surface expres-sion of specific “gut-homing” adhesion molecules such as α4β7 and CCR9 as well as LFA-1, VLA-4 (α4β1), and CD44.200–203
Following the initial priming/activation step within the GALT/MLNs, the antigen-experienced effector T-cells re-enter the systemic circulation via the efferent nodal lymphatics where they will now home to the gut. This new pattern of homing to the small bowel is thought to be mediated by the interaction between α4β7 and CCR9 with post-capillary venular MAdCAM-1 and CCL25, respectively; however, the interactions of lymphocyte-associated PSGL-1, LFA-1, α4β1. and CD44 with venu-lar P/E-selectin, ICAM-1 (and ICAM-2), VCAM-1, and hyaluronate, respectively, are known to be important mediators as well (Figure 79.7B).200–203 The mechanisms responsible for “imprinting” the recruitment of T-cells to the gut following antigen stimulation within the GALT/MLNs are not known with certainty; however, it is thought that effector T-cells are exposed to specific signals/media-tors within the lymphoid tissue that enhances the expres-sion of gut-specific homing receptors.200–203 For example, it is well-appreciated that T-cells activated within PPs and
MLNs express high levels of α4β7 as well as the chemok-ine receptor CCR9, which binds to their respective ligands MAdCAM-1 and CCL25 (TECK), both of which are con-stitutively expressed on intestinal endothelial cells.200–203 Much of what is known regarding the mechanisms by which effector T-cells traffic to intestinal tissue has come from studies focused on the small bowel. However, very little is known regarding the specific T-cell and venular molecular determinants that govern T-cell trafficking to the colon. It is thought that both α4β7 and α4β1 are important for T-cell migration to the inflamed large bowel; however, it remains unclear whether these integrins and/or CCR9/CCL25 interactions are important for T-cell trafficking to the healthy (or inflamed) colon.
Once the effector T-cells enter the gut interstitium, they re-encounter their specific antigen presented on a more diverse population of antigen-presenting cells (APCs), such as macrophages and B-cells as well as DCs (Figure 79.8).204 This secondary, antigen-specific interac-tion results in a more rapid and vigorous response of the effector T-cells, dramatically enhancing the production of IFN-γ, IL-17, TNF-α, LT-α, and IL-2. IL-2 promotes the clonal expansion of T-cells and enhances the function of helper T-cells and B-cells, whereas IFN-γ interacts with and activates APCs and macrophages to produce addi-tional IL-12. IFN-γ, TNF-α, and IL-17 will also activate endothelial cells and enhance endothelial cell adhesion
Tethering and Rolling Activation Arrest
L-Selectin(CD62L) CCR7
CCL19/CCL21
PNAdMAdCAM-1 MAdCAM-1
α4β7α4β7
MAdCAM-1ICAM-2
(activated) (activated)
ICAM-1
LFA-1
Tethering and Rolling Activation
CCR9
CCL25
P-SelectinE-Selectin MAdCAM-1 MAdCAM-1 ICAM-2 ICAM-1
α4β7
α4β7(activated) (activated)
LFA-1
Arrest
PSGL1G protein
(A) (B)
FIGURE 79.7 T-cell trafficking to the MLNs and intestine. (A). MLNs. Naïve T-cell-associated L-selectin binds to both MAdCAM-1 and PNAd to tether these lymphocytes to the high endothelial venules (HEVs) to initiate rolling along the HEVs. Although the L-selectin/MAdCAM-1 and L-selectin/PNAd interactions are thought to mediate much of the T-cell tethering and rolling in the MLNs, α4β7 may also be used by naive T-cells to tether themselves to MAdCAM-1, providing additional tethering capacity for these cells in the MLNs. Interaction of T-cell-associated chemokine receptor CCR7 with SLC (CCL21) and/or ELC (CCL19) presented on the luminal surface of the HEVs activates LFA-1 and α4β7 on the naive T-cells to bind to ICAM-1 (or ICAM-2) and MAdCAM-1, respectively. These interactions promote firm adhesion and lymphocyte arrest, which ultimately lead to T-cell extravasation into the MLNs. (B) Intestine. Initial tethering and rolling of effector T-cells on the post-capillary venular endothelial cells in the gut begins with the interaction between lymphocyte-associated PSGL-1 and venular P-and/or E-selectin. In addition, there is evidence to suggest that VLA-4 (α4β1) also contributes to effector cell rolling via its interaction with MAdCAM-1. Interaction of CCR9 with venular CCL25 promotes the conformational activation of LFA-1 and α4β7, enhancing effector cell binding to ICAM-1 (or ICAM-2) and MAdCAM-1, respectively, and promoting infiltration of these effector cells into the lamina propria. (Modified from 315 with permission.)

SECTION | VI Consequences of Disregulated Physiology2116
molecule expression on the post-capillary venular endothe-lium (Figure 79.8).204 In addition, IFN-γ potently acti-vates macrophages and other myeloid cells produce large amounts of proinflammatory cytokines such as TNF-α, IL-1β, IL-6, IL-8, IL-12, IL-18, and IL-23 as well as reac-tive oxygen (superoxide, hydrogen peroxide) and nitro-gen (NO) metabolites (Figure 79.8). The net result of this concerted interaction following T-cell activation is enhanced killing of ingested pathogenic microbes as well as increased recruitment of additional leukocytes, such as polymorphonuclear leukocyte (PMN), monocytes, and macrophages, into the gut tissue where they engulf and destroy the invading pathogens (Figure 79.8).204
79.5 LEUKOCYTE MOVEMENT THROUGH THE INTERSTITIUM
While leukocyte recruitment is initially mediated by the process of leukocyte adhesion to and transmigration across endothelium, upon completion of leukocyte extravasa-tion another equally important process occurs – migration through interstitial tissues. This process is highly complex and remains poorly understood; however, multiple cellular responses are simultaneously involved including differ-ential regulation of cell adhesion to extracellular matrix, chemosensation to directional chemical and protein gradi-ents, regulation of intracellular cytoskeletal organization, and modulation of various signal transduction pathways. Over several decades, numerous studies have addressed cellular mechanisms necessary for leukocyte migration
through extracellular matrix and the interstitium with adhesion molecules, chemokines, and cytokines serving key molecular functions.
79.5.1 Adhesion Molecule Regulation of Leukocyte Migration
Immune cell migration through tissues, such as that seen during inflammation, involves dynamic leukocyte responses combined with differential activation of several molecular pathways. Numerous environmental signals, such as adhesion molecules, chemoattractants, extracellular matrix proteins, and mechanical forces, are integrated into the cell to generate specific cellular responses. Leukocyte migration occurs through coupling actin-based protrusion and contraction to the dynamic formation and disassem-bly of cell–extracellular matrix adhesions and is highly adhesion dependent. Both the formation of new matrix contacts and the generation of tractional forces are medi-ated through integrins.205–207 Altering the adhesive state of the cell induces a biphasic effect on cell migration, with low levels of adhesion insufficient to support trac-tional forces and high levels of adhesion preventing cel-lular displacement. However, alteration of cell shape and size by intracellular actin network reorganization may also regulate leukocyte migration through integrin-inde-pendent events.208 Together, leukocyte migration through three-dimensional matrices is highly amoeboid like, yet depending on the matrix composition and architecture, mesenchymal-like migration with complex adhesion and
IL-12
IL-12
IL-17 Effector Cell
APC
TNF-α
ROSNO
IFN-Y
IL-1β
MΦ
FIGURE 79.8 Effector T-cells interact with different antigen-presenting cells (APCs) such as DCs, macrophages, and/or B-cells presenting enteric antigen to initiate intestinal inflammation. APC-induced activation of effector cells promotes the production of large amounts of IFN-γ, IL-1β, IL-12, IL-17, and TNF-α. IFN-γ effectively activates macrophages to produce large amounts of proinflammatory cytokines such as TNF-α, IL-1β, IL-12, and IL-17 as well as ROS and NO. In addition, IFN-γ, TNF-α, ROS, and IL-17 activate endothelial cells and enhance endothelial cell adhesion molecule expression on the post-capillary venular endothelium. The net result of this uncontrolled production of Th1/Th17- and macrophage-derived inflammatory cytokines is the recruitment and activation of granulocytes/myeloid cells (e.g., PMNs, monocytes, macrophages) as well as addi-tional T- and B-cells into the gut tissue leading to the induction and perpetuation of chronic gut inflammation. (Modified from 204 with permission.)

Chapter | 79 Recruitment of Inflammatory and Immune Cells in the Gut: Physiology and Pathophysiology 2117
targeting systems are also employed to enable efficient directional migration to injurious or infectious sources.209
Integrin adhesion to extracellular matrix components, such as collagens, fibronectin, and laminins, are prima-rily responsible for neutrophil movement through the interstitium. It has been reported that members of the β1 integrin family very late antigen (VLA)members are pri-marily responsible for neutrophil adhesion to matrix, with no appreciable role for β2 integrins.210,211 Interestingly, β1 expression on circulating leukocyte populations is low in comparison to β2 integrins. However, β2 integrin activa-tion through binding to ligand concomitant with extravasa-tion can quickly upregulate β1 integrin surface localization on neutrophils.211 Consistent with increased expression of β1 integrins, antibody blockade or genetic deletion of β2 integrin does not alter neutrophil migration through inter-stitium or adhesion to matrix proteins, suggesting that additional mechanisms exist to increase β1 expression and function.212,213 Together, these reports suggest that neu-trophil extravasation involves conversion from β2 to β1 integrin-mediated cell motility, which is regulated by β2 integrin–ligand interactions and subsequent engagement of the endothelial cell basement membrane.
Additional regulation of neutrophil migration through the interstitium occurs through differential integrin α chains. Different heterodimeric α integrin chain (α1–6) association with the β1 chain significantly alters neutrophil motility through different extracellular matrices. For exam-ple, α2β1 has been reported to play a primary role in neu-trophil chemotaxis through extravascular tissue, such as the mesentery, largely through interactions with collagen.214 Interestingly, neutrophil migration through collagen gels supplemented with fibronectin or tenascin is substantially diminished compared to collagen alone.215,216 Closer examination of this response showed that antibody inhibi-tion of α4β1 and α5β1 integrins restores neutrophil motil-ity through combined matrices similar to collagen alone, suggesting that differential integrin engagement with vari-ous matrix components regulates the overall adhesive state of the neutrophil.210,216 Together, these studies suggest an important role for integrin-regulated haptotaxis that may be involved in controlling neutrophil tissue localization.
T-cell migration through the interstitium can utilize β1 integrins and other unknown mechanisms.206,210,217 However, unique molecular mechanisms regulating T-cell motility also exist.205–207 T-cell engagement of CD3 or CD3/CD2 can significantly enhance β1 integrin-depend-ent matrix adhesion through activation of multiple sig-naling pathways that could alter integrin affinity/avidity and cytoskeletal interactions.217–219 Specifically, CD3-TCR stimulation results in Lck/Zap-70 kinase activation, which increases PI3 kinase activity that enhances Itk tyro-sine kinase membrane localization where it can be phos-phorylated by Lck to alter actin polymerization and thus
modulating β1 integrin function. T-cell migration is further unique because the β2 integrin LFA-1 (αLβ2) is involved in enhancing T-cell motility. LFA-1 is ubiquitously expressed on all T-cells and plays an important role in homing, recruitment, and immunological synapse forma-tion.220,221 However, studies have shown that LFA-1 acti-vation with antibodies or ligand (e.g., ICAM-1) enhances T-cell motility on several extracellular matrix proteins including fibronectin, laminin, and collagen IV.222,223 LFA-1-enhanced T-cell motility also involves activation of intracellular signals including calmodulin/MLCK, PKC-β1, G-protein-coupled receptors, and RhoA/ROCK path-ways.221,223 These reports demonstrate that T-cell motility is highly dynamic and occurs in such a manner as to effec-tively survey tissue for antigen.
Memory T-cell isolated from tissue microenviron-ments rather than peripheral blood also displays differ-ential integrin expression, which alters cell–extracellular matrix adhesion. A study by Krivacic and Levine exam-ined integrin expression profiles and adhesion to native extracellular matrix or its components between lamina pro-pria T-cells or peripheral blood T-cells that were cultured and activated in vitro.224 Several important findings were reported in this study. First, peripheral T-cells showed less adhesion to extracellular matrix compared to lamina pro-pria T-cells. Secondly, peripheral lymphocytes displayed preferential binding to fibronectin while lamina propria lymphocytes preferred collagen. Thirdly, the differential matrix binding was associated with a greater percent of lamina propria T-cells expressing VLA α integrin chains 1, 2, 3, and 5 that was not associated with differences in sub-unit surface expression on an individual cell basis. Lastly, long-term IL-2 expansion of peripheral blood lymphocytes cultured on matrix proteins generated surface integrin expression and adhesion characteristics similar to that of lamina propria lymphocytes. These findings suggest that local tissue matrix environments can further differentiate recruited T-lymphocytes to a highly adhesive phenotype conducive for long-term sequestration in tissue.
Monocyte motility in the interstitium also involves α1β1 (VLA-1). Studies using antibody blockade or gene-targeted ablation of the α1 integrin chain demonstrate significant protection against DSS- or TNBS-induced colitis.225,226 Interestingly, inhibition of α1 function pref-erentially inhibited monocyte infiltration into the intersti-tium that was not associated with decreased immune cell recruitment as determined by intravital microscopy.226 These reports demonstrate that α1β1 expression is impor-tant for monocyte adhesion to extracellular matrix and sub-sequent movement through the interstitium. Together, all of the abovementioned studies suggest that single or mul-tiple inhibition of VLA protein’s association with extracel-lular matrix represents a unique therapeutic approach for inflammatory disorders.

SECTION | VI Consequences of Disregulated Physiology2118
79.5.2 Chemoattractant Regulation of Leukocyte Movement Through the Interstitium
The process of chemosensation of leukocytes during an inflammatory response is essential to ensure optimal recruitment of specific leukocyte types to discreet tissue sites and organs. Numerous molecules have been described that facilitate directional leukocyte migration including chemokines, cytokines, and other biochemical mediators (e.g., fMLP, PAF, complement products, arachidonic acid metabolites, and others). Of these molecules, work over the past several years has yielded important physiological and pathological insight into the critical role of chemok-ines in regulating leukocyte recruitment from the vascula-ture and its subsequent migration through tissue.
Chemokines are small heparin-binding proteins that have been defined based on amino acid composition of a conserved tetra-cysteine motif resulting in two major sub-classes, CXC (separation by a non-conserved amino acid) or CC (adjacent cysteine location), along with three other homologous molecules of differing motifs.227 Forty-three distinct chemokines have been identified to date and bind to 19 receptors in a promiscuous fashion. Chemokine receptors are surface G-protein-coupled receptors that contain seven membrane spanning domains that activate downstream G-protein signal cascades. Chemokines avidly bind glycosaminoglycans associated with cells or matrix proteins and are readily diffusible due to their small size (7–15 kDa). Moreover, chemokines may also be trans-ported through or around microvascular endothelium, thus further identifying discreet regions for leukocyte recruit-ment.228 Collectively, these structural and biochemical features contribute to the chemokines strong ability in mediating directional leukocyte recruitment and migration.
Several chemokines have been implicated in dys-regulated immune responses of the GI system. In patients with active ulcerative colitis or Crohn’s disease increased expression of chemokines CXCL5, CXCL8, CXCL10, CCL2, CCL5, CCL6, and CCL10 have been reported.229,230 Likewise, increased chemokine recep-tor expression of CXCR1 for CXCL8 and CXCR3 for CXCL10 is also observed in colon tissue from patients with inflammatory bowel disease (IBD). An important pathological role for chemokines has further been demon-strated in animal models of experimental colitis. Elevated expression of chemokines CXCL1, CCL2, CCL3, and CCL5 have been reported in different colitis models.229 Consistent with these observations, gene-targeted dele-tion of CCR2, CCR5, or CCR6 attenuates experimental colitis, suggesting that enhanced chemokine expression and release elicits recruitment of leukocytes bearing spe-cific chemokine receptors.231,232 Together these findings
demonstrate an important pathological role for chemokines and their receptors in GI disease.
Chemokines can facilitate leukocyte recruitment and migration through alterations of adhesion molecule func-tion or cellular location. For example, multiple chem-okines including CXCL8, CXCL9, CXCL10, CXCL12, CCL2, CCL11, CCL17, CCL19, CCL21, and CCL22 have all been reported to stimulate rapid integrin-medi-ated leukocyte firm adhesion under hydrodynamic flow conditions.233 Chemokine stimulation enhances integrin-mediated adhesion through changing the state of integrin activation (conversion from a “closed” non-binding con-formation to an “open” high binding state) thus increas-ing its affinity for ligand, or they may alter integrin cell surface location into discreet clusters, thereby increasing avidity for ligand.234,235 Both of these molecular events may also occur simultaneously in the leukocyte, which explains the very rapid and effective nature of chemokine-mediated leukocyte adhesion.236 Chemokine activation of leukocytes also increases adhesion to extracellular matrix proteins through similar mechanisms, and stimulates robust migration through extracellular matrix.216,237–241 However, chemokines are not the only component of the chemoattractant inflammatory milieu, and how these mol-ecules act in concert with other cytokines to stimulate tissue infiltration of leukocytes remains an active area of investigation.
Like chemokines, cytokines may also bind to matrix proteins and establish a “chemoattractant trail” for leu-kocytes to follow.242 For example, TNF-α binds to the N-terminal domain of fibronectin, which enhances T-cell binding to fibronectin in a β1 integrin-dependent man-ner.243 Similarly, TGF-β also modulates leukocyte adhe-sion to and migration through matrix proteins.244,245 Preliminary studies have been recently reported examin-ing how combinatorial gradients of cytokines and chemo-kines affect leukocyte migration through extracellular matrix. Experiments using three-dimensional extracel-lular matrices containing cytokine (e.g., TNF-α or IL-2) to chemokine (e.g., CXCL12 or CCL5) gradients show that cytokine stimulation inhibits lymphocyte chemotaxis due to enhanced integrin adhesion to matrix proteins.246 Importantly, the adhesion response stimulated from com-bined cytokine/chemokine stimulation is substantially greater than cytokine-mediated adhesion alone, suggesting a cooperative effect of these chemoattractants in enhancing cell–matrix interaction. Interestingly, the effects of com-bined chemokine treatment may actually antagonize cel-lular responses from one to another, including decreased chemotactic responses and adhesion to matrix.247 These observations indicate that biophysical regulation of leu-kocyte migration through tissue is multifactorial and sug-gests that differential leukocyte recruitment during various

Chapter | 79 Recruitment of Inflammatory and Immune Cells in the Gut: Physiology and Pathophysiology 2119
inflammatory responses involves several members of the cytokine and chemokine family.
79.6 LEUKOCYTE TRAFFICKING DURING ACUTE INFLAMMATION
Leukocytes have been implicated in the pathogenesis of a variety of GI diseases that are characterized as an acute or chronic inflammatory condition. This section will focus on some acute inflammatory conditions of the GI tract in which the dominant population of recruited leu-kocytes is neutrophils. The trafficking of leukocytes has been characterized using intravital microscopy in several experimental models of acute GI inflammation, including I/R, NSAID-induced ulcers, radiation enteritis, ethanol-induced ulcers, endotoxemia, Helicobacter pylori infec-tion, and Clostridium difficile colitis.154,162,170,175,176 The data collected from these models indicate that they all share features that are characteristic of an inflammatory phenotype, including the rolling firm adhesion and emi-gration of neutrophils, oxidative stress, platelet–leukocyte adhesion/aggregation, increased vascular permeability, and interstitial edema. Furthermore, there is evidence for neutrophil-mediated tissue injury in all of these experi-mental models. The factors that appear to distinguish these models from one another are the inciting events that initi-ate the inflammatory response, and the molecular and bio-chemical mechanisms that underlie the recruitment and/or activation of the tissue injury-inducing leukocytes. The models that are discussed in the following sections exem-plify the diversity of inciting factors and mechanisms that contribute to the trafficking of leukocytes in acute GI inflammation.
79.6.1 Oxidative Stress-dependent Models of Inflammation
I/R and abdominal irradiation are two distinct incit-ing factors that can produce an acute intense inflamma-tory response in the GI tract. A major component of the inflammatory response elicited by both stimuli results from an increased production of reactive oxygen metabo-lites (ROS), which are the resultant effects of the oxi-dative stress on leukocyte recruitment and activation. The enhanced ROS production occurs in microvascu-lar endothelial cells, particularly in venules, suggesting that these cells assume an activated state. The increased endothelial cell ROS production induced by I/R occurs within seconds to minutes following the restoration of blood flow to an ischemic tissue and is largely generated by the enzyme xanthine oxidase.248,249 As neutrophils are recruited into venules of the post-ischemic tissue, a second, more intense oxidative stress results from the
ROS production by adherent and emigrating leukocytes. Neutrophil adhesion in post-ischemic venules can occur within a few minutes after the onset of reperfusion, but this accumulation of adherent cells increases over the next few hours, which accounts for the slow progressive increase in the intensity of the oxidative stress experienced by the ves-sel walls. With abdominal radiation, however, the oxidative stress exhibited by intestinal venules appears to parallel the accumulation of adherent and emigrating leukocytes, as well as adherent platelets.250–253 The leukocyte dependency of the accelerated ROS production is most pronounced at 6 hours after irradiation, and the oxidative stress detected at 2 hours is only partially dependent on adherent leuko-cytes. This is supported by the fact that inhibition of the later leukocyte adhesion response with an anti-CD18 mAb eliminates the corresponding oxidative stress, while the oxidative stress is only partially blunted at 2 hours. In con-trast to what is seen following I/R, neither the leukocyte-independent nor -dependent components of the oxidative stress are attenuated by the xanthine oxidase inhibitor allopurinol.252,253
Both I/R and abdominal radiation elicit the recruit-ment of rolling leukocytes in venules that can be blocked by P-selectin immunoneutralization. Similarly, both mod-els have been shown to result in an increased expression of P-selectin in the gut microvasculature. Increased E-selectin expression and a blunted neutrophil recruitment response following E-selectin immunoblockade have been dem-onstrated in the gut after I/R, but the contribution of this adhesion molecule to radiation-induced inflammation has not yet been evaluated. The firm adhesion of leukocytes in both models appears to involve an interaction between CD11/CD18 on leukocytes with constitutively expressed ICAM-1 on endothelial cells.2 If this firm adhesion is blocked by treatment with a CD18- or an ICAM-1-specific mAb, the increased vascular permeability that results from I/R or abdominal irradiation is prevented. While a genetic deficiency or immunoblockade of P-selectin has been shown to protect the intestine against histological mucosal damage after I/R, no such protection is observed after abdominal radiation.251,254
While oxidative stress appears to be a major factor in the initiation and progression of leukocyte recruitment in I/R- and abdominal irradiation-induced inflammation, the involvement of ROS has been more clearly delineated when I/R is the inciting stimulus. A variety of ROS-directed inter-ventions have been shown to significantly diminish the leu-kocyte trafficking that occurs in the intestinal vasculature after I/R.248,249 Antioxidant enzymes such as SOD and cata-lase, iron-chelators such as desferrioxamine, and xanthine oxidase inhibitors such as allopurinol are all capable of blunt-ing the leukocyte recruitment response whether administered prior to or immediately following the onset of reperfusion.

SECTION | VI Consequences of Disregulated Physiology2120
SOD1 transgenic mice (that overexpress CuZnSOD) show an attenuated I/R-induced upregulation of P- and E-selectin. A similar attenuation of I/R-induced E-selectin expression is noted in mice treated with an inhibitor of NF-kB activa-tion, supporting a role for this transcription factor as the link between oxidative stress and the increased biosynthesis/expression of E-selectin after I/R.170,254
There are several lines of evidence that support a role for NO in I/R-induced leukocyte trafficking.255 NO donors appear to be as effective as SOD in attenuating I/R-induced leukocyte rolling and adhesion. Non-selective inhibitors of NOS (e.g., L-NAME) induce a similar endothelial cell phenotype as seen following I/R, includ-ing oxidative stress and leukocyte–endothelial cell adhe-sion. The observation that NOS inhibition does not induce further increases in leukocyte adhesion following I/R is consistent with the view that the bioavailability of NO fol-lowing reperfusion in untreated animals is already limited to inactivation by the large fluxes of superoxide produced in the post-ischemic vasculature. Hence, I/R (and possibly abdominal irradiation) appears to be an excellent exam-ple of increased leukocyte trafficking that results from an imbalance between superoxide and NO fluxes through mechanisms depicted in Figure 79.4.
79.6.2 Bacterial Toxins
Translocation of enteric bacteria and/or bacterial products (e.g., LPS) from the gut lumen to the mucosal interstitium is a potential mechanism for the initiation of leukocyte trafficking in the GI tract. LPS or other bacterial prod-ucts that gain access into the interstitium can interact with receptors on mucosal macrophages to stimulate the pro-duction and release of cytokines that can act on vascular endothelium to enhance CAM expression and promote leukocyte adhesion. It was recently demonstrated that the constitutive expression of ICAM-1 in the GI vascula-ture of germ-free mice is significantly lower than in their conventional counterparts, suggesting that indigenous GI microflora are responsible for a significant proportion of the basal ICAM-1 expression detected in the GI tract.256 This raises the possibility that enteric bacteria may also contribute to the elevated CAM expression and leuko-cyte recruitment that is observed in GI diseases accompa-nied by mucosal injury. In a murine model of I/R injury, this does not appear to be the case, since the I/R-induced increase in E-selectin expression does not differ between LPS-sensitive and -insensitive mice.257 A similar finding has been reported for mice that are subjected to cecal liga-tion and puncture (a model of sepsis), where no differences in the E-selectin upregulation responses are noted between LPS-sensitive and -insensitive mice.258
Two models of GI inflammation for which there is clear evidence of bacterial toxin involvement in the
initiation of leukocyte activation and recruitment are H. pylori gastritis and C. difficile colitis. Soluble extracts of both can elicit an inflammatory response when applied directly to the mesenteric microcirculation.259,260 Both low molecular weight non-protein substances and high molecular weight protein fractions of water-soluble extracts of H. pylori have been shown to elicit an increased expression of different CAMs on monolayers of cultured endothelial cells and in vivo.259,261 The same water extract of H. pylori as well as a neutrophil-activating protein pro-duced by it has been shown to increase the adhesion and emigration of leukocytes, promote leukocyte-platelet aggregation, increase vascular permeability in mesenteric venules, and to elicit the degranulation of perivenular mast cells.176,260,262 Gastrin has also been implicated in the leu-kocyte–endothelial cell adhesion induced by H. pylori.263 Both in vitro and in vivo models of H. pylori-induced inflammation implicate CD11/CD18 interactions with ICAM-1 in the neutrophil adhesion response, while the leukocyte-platelet aggregation appears to be largely medi-ated by P-selectin expressed on the activated platelets interacting with PSGL-1 on neutrophils. Immunoblockade of CD18 or ICAM-1 diminishes the H. pylori-induced vascular permeability response, suggesting that the adher-ent leukocytes are responsible for this manifestation of endothelial cell dysfunction.176,260
C. difficile is the principal agent responsible for antibiotic-associated pseudomembranous colitis in humans and experimental animals. This bacteria produces two protein exotoxins (A and B) that have different biologi-cal properties, but only one (toxin A) of which is respon-sible for the inflammatory responses.259 Exposure of the mesenteric microcirculation to C. difficile toxin A elic-its an inflammatory response that is nearly identical to that observed with the water extract of H. pylori, that is, leukocyte adhesion and emigration, increased vascular permeability, leukocyte-platelet aggregation, and mast cell degranulation. Furthermore, the leukocyte adhesion response is mediated by CD11/CD18:ICAM-1 interac-tions.259 A shared feature of the microvascular responses to the products of H. pylori and C. difficile toxin is degranulation of perivenular mast cells. In both models of inflammation, this mast cell response makes an important contribution to the overall inflammatory response, since mast stabilizers not only blunt the leukocyte recruitment, but also protect against the endothelial barrier dysfunc-tion (increased vascular permeability).259,260 While mast cell degranulation appears to be a critical early step in both inflammatory responses, the mast cell-derived sub-stances that mediate these effects appear to differ between the two stimuli. In C. difficile toxin A-mediated leukocyte recruitment and microvascular dysfunction, histamine appears to play a major role since treatment with diamine oxidase (histaminase) or an H1-receptor antagonist is as

Chapter | 79 Recruitment of Inflammatory and Immune Cells in the Gut: Physiology and Pathophysiology 2121
effective as lodoxamide (a mast cell stabilizer). However, PAF appears to be the major mast cell-derived product that contributes to the H. pylori-induced leukocyte adhe-sion and increased vascular permeability. Support for this contention is provided by the observation that PAF recep-tor antagonists are as effective in blunting the H. pylori-induced responses as the mast cell stabilizer ketotifen. PAF is known to be a potent inducer of leukocyte adhesion and can increase vascular permeability in both a leukocyte-dependent and -independent manner.172,176,259,260
79.7 LEUKOCYTE TRAFFICKING DURING CHRONIC GUT INFLAMMATION
The potential for the immune system to produce local and systemic tissue injury suggests that the immune system has ways to efficiently regulate immune responses to both pathogenic and harmless antigens. This regulatory activity is accomplished by a variety of different leukocyte popu-lations. The best characterized of these populations are naturally occurring regulatory T-cells (nTregs) express-ing the phenotype CD4CD25Foxp3. These nTregs are known to suppress a wide range of immune responses via several different mechanisms including production of regulatory cytokines, competition for essential cytokines, and contact-dependent mechanisms These Tregs are capa-ble of inhibiting a variety of experimental autoimmune diseases including chronic colitis.264 In addition to CD4 nTregs, studies have identified certain CD8 T-cells that are part of the intraepithelial lymphocyte compartment in the gut and are capable of attenuating chronic colitis in vivo.265,266 Furthermore, specific subsets of B-cells have been shown to function as regulatory cells in mice.267 It is becoming increasingly appreciated that IL-10 and TGF-β are required for the regulatory function of nTregs and B-cells in vivo and that both of these regulatory cytokines play important roles in continuously regulat-ing immune responses to enteric bacteria such that the gut is maintained in a state of immunological “tolerance” to commensal microorganisms.264 A large body of experi-mental data has been generated over the past 10 years to suggest that a break in tolerance to enteric antigens may be responsible for the induction of the chronic intestinal inflammation that is observed in patients who suffer from inflammatory bowel diseases (Crohn’s disease; ulcerative colitis).264,268–272 Indeed, the role of commensal bacteria in the pathogenesis of experimental IBD has been well characterized in a number of different animal models of chronic gut inflammation.268,269,271 Although the etiology of these chronic inflammatory disorders in humans has not been definitively elucidated, there is good evidence to suggest that chronic gut inflammation arises from a com-plex interaction among genetic, immune, and environ-mental factors.269,271,273 Experimental and clinical data
have implicated T-cells as important mediators of disease and suggest that chronic intestinal inflammation arises from a dysregulated immune response to enteric bacterial antigens.
The importance of T-cells in the pathogenesis of IBD has prompted numerous investigations into identify-ing which of the many different T-cell- and endothelial cell-associated adhesion molecules are important for the induction and/or perpetuation of intestinal inflamma-tion. Several different adhesion molecules have been sug-gested as important cellular determinants for induction of colonic inflammation using erosive (chemically induced), self-limiting models of acute colitis. However, few if any of these molecules have been shown to be required for the pathogenesis of chronic gut inflammation. For exam-ple, T-cell-associated CD62L (L-selectin) and PSGL-1 have been identified as important cellular determinants in the pathogenesis of colonic inflammation using short-term hypersensitivity or erosive self-limiting models of acute colitis.59,274–277 Our laboratory has failed to dem-onstrate a requirement for either of these adhesion mol-ecules in a T-cell-dependent mouse model of chronic gut inflammation.100 Several T-cell-associated integrins (e.g., LFA-1, α4β1, α4β7) have been suggested to be important determinants for induction of gut inflammation. We have found that LFA-1(CD11a/CD18) plays an important role in acute colitis as CD11a (LFA-1)-deficient mice develop significantly less colitis in response to short-term, oral administration of the erosive polymer DSS.278 In addition, we have demonstrated a critical role for T-cell-associated LFA-1 in the development of chronic colitis induced by adoptive transfer of naive T-cells. We found that transfer of CD11a/(LFA-1/) CD4CD45RBhigh T-cells into immunodeficient recombinase activating gene-1 (RAG/) recipients induces very little colitis when compared to the robust disease produced by the transfer of wild-type T-cells.279
In addition to the β2 integrins, investigators have also been actively exploring the roles of leukocyte-associated α4β1 and α4β7 in different animal models of chronic intes-tinal inflammation with conflicting results. For example, Sydora et al. reported that adoptive transfer of β7-deficient CD4CD45RBhigh T-cells into immunodeficient-recipient mice delayed the onset of colitis, but did not attenuate the incidence and severity of the disease, suggesting that αEβ7 and α4β7 were not required for full expression of chronic colitis.280 This study is in agreement with Rivera-Nieves and co-workers who demonstrated that monoclonal anti-body (mAb) blockade of α4β1 or α4β7 individually did not attenuate chronic ileitis in SAMP1/Yit mice, whereas immunoneutralization of both or their endothelial ligands significantly attenuated disease.281 Interestingly, it has been reported that long-term administration of anti-α4 integrin mAb actually exacerbates the colonic inflammation

SECTION | VI Consequences of Disregulated Physiology2122
observed in a model of spontaneous colitis in mice.282 The reasons for these conflicting results are not clear, however, they may be explained in part by the fact that these stud-ies relied on the administration of mAbs that may affect several different cell types. For example, α4β7 is found on T-cells as well as natural killer cells and monocytes, whereas α4β1 is expressed by different myeloid cells (e.g., PMNs, monocytes).283–286 Although clinical studies have demonstrated the efficacy of mAbs directed against the α4 integrin (e.g., natalizumab) in patients with Crohn’s dis-ease, is not clear whether α4β7 and/or α4β1 is the impor-tant molecular determinants for this protective effect or whether the identity of various α4-expressing leukocyte populations involved in disease pathogenesis has been identified.287,288 Concern has been raised over the past few years as several cases of progressive multifocal leukoen-cephalopathy (PML) have occurred in patients treated with natalizumab either alone or in combination with immuno-suppressive therapy for multiple sclerosis, Crohn’s disease or rheumatoid arthritis.288,289 This potentially fatal disease results from the reactivation of the normally dormant JC polyomavirus in immunosuppressed inviduals.288,289
The multistep paradigm for leukocyte trafficking states that endothelial cell-associated selectins are very important for tethering the leukocyte to the microvascular surface to initiate cell rolling. It has been demonstrated E-selectin is significantly upregulated on endothelial cells in mucosal biopsies obtained from patients with active (but not qui-escent) ulcerative colitis or Crohn’s disease.290,291 We have demonstrated that colonic microvascular E-selectin expression is significantly enhanced with the onset of chronic colitis in SCID mice that have been reconsti-tuted with naive T-cells or in colons of IL-10-deficient (IL-10/) mice with colitis.292–295 Intervention studies using two different antibodies to E-selectin were not effec-tive at attenuating the spontaneous colitis that develops in the non-human primates cotton-top tamarins, suggest-ing that E-selectin-dependent leukocyte adhesion may not represent an important interaction to sustain the inflam-matory response in this model of colitis.296 In other stud-ies, P-selectin was found to be upregulated in venules of mucosal biopsies obtained from patients with active IBD.291,297 As with the earlier work using antibodies to E-selectin, studies addressing the importance of P- and E-selectin in experimental colitis using mice genetically deficient in these adhesion molecules have proven rather disappointing.298 In these studies investigators found that colitis induced by acetic acid or TNBS in ethanol was either not attenuated or enhanced in mice deficient in P-selectin and/or E-selectin.298 Interpretation of these stud-ies in the context of human IBD is difficult since neither the acetic acid nor the TNBS/ethanol model are T-cell dependent models and thus are not chronic in nature, which makes their clinical relevance questionable.
In addition to the selectins, T-cells, PMNs, and mono-cytes adhere to venular endothelium by virtue of the strong adhesive interactions between their β2 integrins (CD11a/CD18, CD11b/CD18) and ICAM-1 and/or ICAM-2 expressed on the surface of endothelial cells. Several dif-ferent reports have demonstrated enhanced staining for ICAM-1 on mucosal mononuclear or endothelial cells in biopsies obtained from patients with active ulcerative colitis and Crohn’s disease.291,299,300 We have shown that colonic ICAM-1 (but not ICAM-2) expression is signifi-cantly enhanced in colitic SCID mice reconstituted with CD45RBhigh T-cells and in the colons of IL-10/ mice with active enterocolitis.292–295 It has been shown that infu-sion of an anti-sense oligonucleotide or antibodies directed against ICAM-1 produces clinical improvement in mouse models of colitis or ileitis and in steroid-resistant Crohn’s disease patients, respectively.301–303 However, larger, pla-cebo controlled clinical trials were negative.304,305 The inef-fectiveness of ICAM-1 blockade in the abovementioned studies would appear to rule out a major role for LFA-1 (or CD11b/CD18) in the pathogenesis of IBD. However, LFA-1 also interacts with other ligands such as ICAM-2.306 This counter-receptor for LFA-1 is actually a trun-cated form of ICAM-1 that is constitutively expressed at a 10-fold higher level on venular endothelium than ICAM-1.62,306 In addition, ICAM-2 expression does not change upon stimulation of the endothelium, and expression is constitutive in models of IBD.292,293,307 Furthermore, lym-phocyte adhesion to HUVECs has been shown to be medi-ated by ICAM-2 to a greater extent than by ICAM-1.306 Although the abovementioned studies suggest that β2 integrins as well as ICAM-1 and/or ICAM-2 may play a more important role in the pathogenesis, two case reports have prompted a reevaluation of this hypothesis.308,309 These studies reported a case of CD18 deficiency in which the patient presented with chronic ileocolitis. Bone marrow transplantation completely resolved the intestinal inflam-mation, suggesting that marrow-derived leukocyte dys-function may contribute to disease. These data are similar to those recently reported demonstrating that 4 out of 5 Crohn’s disease patients given allogenic marrow transplan-tation remained disease free for several years post trans-plantation,310 and support the concept that Crohn’s disease may arise from alterations in leukocyte function.
The endothelial ligands for α4β7 (MAdCAM-1) and α4β1 (VCAM-1) have also been suggested to play impor-tant roles in regulating the infiltration of leukocytes into gut tissue and thus may represent important targets for treating chronic gut inflammation. Indeed, we have demonstrated enhanced endothelial cell expression of VCAM-1 with the onset of chronic colitis in the SCID/CD45RBhigh or IL-10/ models of chronic colitis.75,292–294,307,311 Few stud-ies have attempted to ascertain the importance of VCAM-1 in the pathogenesis of chronic gut inflammation.281

Chapter | 79 Recruitment of Inflammatory and Immune Cells in the Gut: Physiology and Pathophysiology 2123
In addition to VCAM-1, MAdCAM-1 has been suggested to be important for T-cell trafficking and thus may play an important role in disease pathogenesis. This endothelial cell adhesion molecule is expressed on GI mucosal endothe-lial cells and high endothelial cells in MLNs and PPs and is involved in the selective homing of lymphocytes to mucosal tissue.74,76,77 Surface expression of MAdCAM-1 is induced by certain Th1 or macrophage-derived cytokines and bacterial products and may last for several days.75 Its lymphocyte-associated counter-receptor, α4β7, is found primarily on a subpopulation of memory/activated CD4 T-lymphocytes involved in mucosal immunity. Briskin et al. reported that MAdCAM-1 expression on venular endothe-lial cells in the lamina propria of the gut is enhanced in inflammatory foci in biopsies obtained from patients with active ulcerative colitis or Crohn’s disease.74 Colonic and cecal (but not ileal) MAdCAM-1 expression increases dra-matically (11-fold) with the onset of colitis in the SCID/CD45RBhigh and IL-10/ models of colitis.75,292,293,295 We have demonstrated that immunoneutralization of MAdCAM-1 (but not ICAM-1 or VCAM-1) profoundly reduced the adhesion of CD4 T-cells in inflamed post-capillary venules of mice with chronic colitis.81 Several additional studies using low molecular weight antagonists or immunoneutralizing monoclonal antibodies to α4β7 or MAdCAM-1 show that the α4β7/MAdCAM-1 interaction plays an important role in the pathophysiology of three dif-ferent experimental models of colitis.79,312–314 MAdCAM-1 represents a potentially important therapeutic target for the treatment of IBD. Indeed, the clinical efficacy of antibodies to α4 in patients with CD would appear to indirectly impli-cate a role for MAdCAM-1 in disease pathogenesis.287,288
PECAM-1, which is preferentially distributed between endothelial cells (intercellular junctions), appears to play an important role in the extravasation of leukocytes. A report by Schurmann et al. demonstrated a significant increase in PECAM expression on venules in mucosal biopsies obtained from patients with active ulcerative coli-tis.297 In other studies, JAM-1 has been found to be critical for both PMN and T-cell transendothelial cell migration.86 The extracellular matrix-rich environment of perivascular tissue is thought to be an important sight where certain human leukocytes undergo differentiation (e.g., mono-cytes) and activation (neutrophils, monocytes, and T-cells) upon extravascular migration. The α1β1 integrin is a major cell surface receptor for collagens with a preference for type IV collagen. The presumed role of the extracellular matrix environment in the inflammatory process, and the fact that chronically activated immune cells can express α1β1, led to the hypothesis that the α1β1 integrin may contribute to the pathophysiology of intestinal inflamma-tion. In a recent series of studies, we have found that treat-ment of mice with acute self-limiting colitis induced by DSS with a blocking anti-α1 mAb resulted in significant
attenuation of colitis, and that similar protection was con-ferred to DSS-exposed mice lacking the α1β1 integrin.226 Blockade of α1β1 was also associated with decreased mucosal inflammatory cell infiltrate and cytokine produc-tion. It was shown that both the induction of DSS-induced colitis and α1-mediated inhibition of colitis occurred inde-pendently of lymphocytes, and identified the monocyte as a key α1β1-expressing cell involved in the develop-ment of colitis in this model. Given that α1β1 represents a major collagen-binding integrin expressed on leukocytes, these findings highlight the important role of extracellular matrix–leukocyte interactions in the pathogenesis of coli-tis, with particular relevance to monocytes.
ACKNOWLEDGMENTSSome the of work reported in this manuscript was supported by a grant from the NIH (PO1-DK43785, Projects 1, 3, and 4 and Animal Models and Histopathology Core).
REFERENCES 1. Bevilacqua MP, Pober JS, Mendrick DL, Cotran RS, Gimbrone
Jr. MA. Proc Natl Acad Sci USA. 1987;84:9238–9242. 2. Gallatin WM, Weissman IL, Butcher EC. Nature. 1983;304:30–34. 3. Hsu-Lin S, Berman CL, Furie BC, August D, Furie B. J Biol Chem.
1984;259:9121–9126. 4. McEver RP, Beckstead JH, Moore KL, Marshall-Carlson L, Bainton
DF. J Clin Invest. 1989;84:92–99. 5. Frenette PS, Johnson RC, Hynes RO, Wagner DD. Proc Natl Acad
Sci USA. 1995;92:7450–7454. 6. Frenette PS, Wagner DD. Thromb Haemost. 1997;78:60–64. 7. Frenette PS, Moyna C, Hartwell DW, Lowe JB, Hynes RO, Wagner
DD. Blood. 1998;91:1318–1324. 8. Jung U, Bullard DC, Tedder TF, Ley K. Am J Physiol.
1996;271:H2740–H2747. 9. Mayadas TN, Johnson RC, Rayburn H, Hynes RO, Wagner DD. Cell.
1993;74:541–554.10. Hartwell DW, Mayadas TN, Berger G, Frenette PS, Rayburn H,
Hynes RO, et al. J Cell Biol. 1998;143:1129–1141.11. Collins RG, Velji R, Guevara NV, Hicks MJ, Chan L, Beaudet AL.
J Exp Med. 2000;191:189–194.12. Dong ZM, Chapman SM, Brown AA, Frenette PS, Hynes RO,
Wagner DD. J Clin Invest. 1998;102:145–152.13. Dong ZM, Brown AA, Wagner DD. Circulation. 2000;
101:2290–2295.14. Johnson RC, Mayadas TN, Frenette PS, Mebius RE, Subramaniam
M, Lacasce A, et al. Blood. 1995;86:1106–1114.15. Johnson RC, Chapman SM, Dong ZM, Ordovas JM, Mayadas TN,
Herz J, et al. J Clin Invest. 1997;99:1037–1043.16. Jones SP, Trocha SD, Strange MB, Granger DN, Kevil CG, Bullard
DC, et al. Am J Physiol Heart Circ Physiol. 2000;279:H2196–H2201.17. Kanwar S, Bullard DC, Hickey MJ, Smith CW, Beaudet AL,
Wolitzky BA, et al. J Exp Med. 1997;185:1077–1087.18. Singbartl K, Green SA, Ley K. Faseb J. 2000;14:48–54.19. Subramaniam M, Saffaripour S, Watson SR, Mayadas TN, Hynes
RO, Wagner DD. J Exp Med. 1995;181:2277–2282.

SECTION | VI Consequences of Disregulated Physiology2124
20. Wickel DJ, Mercer-Jones M, Peyton JC, Shrotri MS, Cheadle WG. Shock (Augusta, Ga). 1998;10:265–269.
21. Mizgerd JP, Meek BB, Kutkoski GJ, Bullard DC, Beaudet AL, Doerschuk CM. J Exp Med. 1996;184:639–645.
22. Soriano SG, Wang YF, Wagner DD, Frenette PS. Brain Res. 1999;835:360–364.
23. Wong J, Johnston B, Lee SS, Bullard DC, Smith CW, Beaudet AL, et al. J Clin Invest. 1997;99:2782–2790.
24. Barkalow FJ, Goodman MJ, Gerritsen ME, Mayadas TN. Blood. 1996;88:4585–4593.
25. Homeister JW, Zhang M, Frenette PS, Hynes RO, Wagner DD, Lowe JB, et al. Blood. 1998;92:2345–2352.
26. Kunkel EJ, Ley K. Circ Res. 1996;79:1196–1204.27. Ley K, Allietta M, Bullard DC, Morgan S. Circ Res.
1998;83:287–294.28. Lorenzon P, Vecile E, Nardon E, Ferrero E, Harlan JM, Tedesco F,
et al. J Cell Biol. 1998;142:1381–1391.29. Arbones ML, Ord DC, Ley K, Ratech H, Maynard-Curry C, Otten G,
et al. Immunity. 1994;1:247–260.30. Bargatze RF, Jutila MA, Butcher EC. Immunity. 1995;3:99–108.31. Bradley LM, Watson SR, Swain SL. J Exp Med. 1994;
180:2401–2406.32. Simon SI, Burns AR, Taylor AD, Gopalan PK, Lynam EB, Sklar LA,
et al. J Immunol. 1995;155:1502–1514.33. Smolen JE, Petersen TK, Koch C, O’Keefe SJ, Hanlon WA, Seo S,
et al. J Biol Chem. 2000;275:15876–15884.34. Tsang YT, Neelamegham S, Hu Y, Berg EL, Burns AR, Smith CW,
et al. J Immunol. 1997;159:4566–4577.35. Jung TM, Gallatin WM, Weissman IL, Dailey MO. J Immunol.
1988;141:4110–4117.36. Kishimoto TK, Jutila MA, Berg EL, Butcher EC. Science (New York,
NY). 1989;245:1238–1241.37. Rothlein R, Dustin ML, Marlin SD, Springer TA. J Immunol.
1986;137:1270–1274.38. Lawson C, Ainsworth M, Yacoub M, Rose M. J Immunol.
1999;162:2990–2996.39. Pattillo CB, Pardue S, Shen X, Fang K, Langston W, Jourd’heuil D,
et al. ICAM-1 cytoplasmic tail regulates endothelial glutathione syn-thesis through NOX4/P13-kinase-dependent pathway. Free Radic Biol Med. 2010;49(6):1119–1128.
40. Pluskota E, Chen Y, D’Souza SE. J Biol Chem. 2000;275:30029–30036.
41. Pluskota E, D’Souza SE. Eur J Biochem. 2000;267:4693–4704.42. Kevil CG, Pruitt H, Kavanagh TJ, Wilkerson J, Farin F, Moellering
D, et al. Faseb J. 2004;18:1321–1323.43. Langston W, Chidlow Jr. JH, Booth BA, Barlow SC, Lefer DJ, Patel
RP, et al. Free Radic Biol Med. 2007;42:720–729.44. Connolly Jr. ES, Winfree CJ, Springer TA, Naka Y, Liao H, Yan SD,
et al. J Clin Invest. 1996;97:209–216.45. Kelly KJ, Williams Jr. WW, Colvin RB, Meehan SM, Springer TA,
Gutierrez-Ramos JC, et al. J Clin Invest. 1996;97:1056–1063.46. Kitagawa K, Matsumoto M, Mabuchi T, Yagita Y, Ohtsuki T, Hori M,
et al. J Cereb Blood Flow Metab. 1998;18:1336–1345.47. Palazzo AJ, Jones SP, Girod WG, Anderson DC, Granger DN, Lefer
DJ. Am J Physiol. 1998;275:H2300–H2307.48. Bendjelloul F, Maly P, Mandys V, Jirkovska M, Prokesova L,
Tuckova L, et al. Clin Exp Immunol. 2000;119:57–63.49. Bullard DC, Hurley LA, Lorenzo I, Sly LM, Beaudet AL, Staite ND.
J Immunol. 1996;157:3153–3158.
50. Bullard DC, King PD, Hicks MJ, Dupont B, Beaudet AL, Elkon KB. J Immunol. 1997;159:2058–2067.
51. Broide DH, Humber D, Sullivan S, Sriramarao P. Blood. 1998;91:2847–2856.
52. Broide DH, Sullivan S, Gifford T, Sriramarao P. Am J Respir Cell Mol Biol. 1998;18:218–225.
53. Foy DS, Ley K. Microvasc Res. 2000;60:249–260.54. Kevil CG, Bullard DC. Acta Physiol Scand. 2001;173:151–157.55. Kevil CG, Patel RP, Bullard DC. Am J Physiol. 2001;281:C1442–C1447.56. Reiss Y, Hoch G, Deutsch U, Engelhardt B. Eur J Immunol.
1998;28:3086–3099.57. Reiss Y, Engelhardt B. Int Immunol. 1999;11:1527–1539.58. Kevil CG, Chidlow JH, Bullard DC, Kucik DF. Am J Physiol.
2003;285:C112–C118.59. Steeber DA, Campbell MA, Basit A, Ley K, Tedder TF. Proc Natl
Acad Sci USA. 1998;95:7562–7567.60. Phillipson M, Heit B, Colarusso P, Liu L, Ballantyne CM, Kubes P.
J Exp Med. 2006;203:2569–2575.61. Ryschich E, Kerkadze V, Lizdenis P, Paskauskas S, Knaebel HP,
Gross W, et al. J Surg Res. 2006;135:291–296.62. De Fougerolles AR, Stacker SA, Schwarting R, Springer TA. J Exp
Med. 1991;174:253–267.63. Gerwin N, Gonzalo JA, Lloyd C, Coyle AJ, Reiss Y, Banu N, et al.
Immunity. 1999;10:9–19.64. De Fougerolles AR, Qin X, Springer TA. J Exp Med.
1994;179:619–629.65. Vazeux R, Hoffman PA, Tomita JK, Dickinson ES, Jasman St RL,
John T, et al. Nature. 1992;360:485–488.66. Butini L, De Fougerolles AR, Vaccarezza M, Graziosi C, Cohen DI,
Montroni M, et al. Eur J Immunol. 1994;24:2191–2195.67. Carlos TM, Schwartz BR, Kovach NL, Yee E, Rosa M, Osborn L,
et al. Blood. 1990;76:965–970.68. Elices MJ, Osborn L, Takada Y, Crouse C, Luhowskyj S, Hemler
ME, et al. Cell. 1990;60:577–584.69. Osborn L, Hession C, Tizard R, Vassallo C, Luhowskyj S, Chi-Rosso
G, et al. Cell. 1989;59:1203–1211.70. Taooka Y, Chen J, Yednock T, Sheppard D. J Cell Biol.
1999;145:413–420.71. Newman PJ. J Clin Invest. 1997;100:S25–S29.72. Muller WA, Randolph GJ. J Leukoc Biol. 1999;66:698–704.73. Schenkel AR, Chew TW, Muller WA. J Immunol. 2004;
173:6403–6408.74. Briskin M, Winsor-Hines D, Shyjan A, Cochran N, Bloom S, Wilson
J, et al. Am J Pathol. 1997;151:97–110.75. Connor EM, Eppihimer MJ, Morise Z, Granger DN, Grisham MB.
J Leukoc Biol. 1999;65:349–355.76. Briskin MJ, McEvoy LM, Butcher EC. Nature. 1993;363:461–464.77. Briskin MJ, Rott L, Butcher EC. J Immunol. 1996;156:719–726.78. Arihiro S, Ohtani H, Suzuki M, Murata M, Ejima C, Oki M, et al.
Pathol Int. 2002;52:367–374.79. Hokari R, Kato S, Matsuzaki K, Iwai A, Kawaguchi A, Nagao S,
et al. Clin Exp Immunol. 2001;126:259–265.80. Kato S, Hokari R, Matsuzaki K, Iwai A, Kawaguchi A, Nagao S,
et al. J Pharmacol Exp Ther. 2000;295:183–189.81. Shigematsu T, Specian RD, Wolf RE, Grisham MB, Granger DN. Am
J Physiol Gastrointest Liver Physiol. 2001;281:G1309–G1315.82. Bazzoni G. Curr Opin Cell Biol. 2003;15:525–530.83. Ebnet K, Suzuki A, Ohno S, Vestweber D. J Cell Sci. 2004;
117:19–29.

Chapter | 79 Recruitment of Inflammatory and Immune Cells in the Gut: Physiology and Pathophysiology 2125
84. Martin-Padura I, Lostaglio S, Schneemann M, Williams L, Romano M, Fruscella P, et al. J Cell Biol. 1998;142:117–127.
85. Liu Y, Nusrat A, Schnell FJ, Reaves TA, Walsh S, Pochet M, et al. J Cell Sci. 2000;113(Pt 13):2363–2374.
86. Ostermann G, Weber KS, Zernecke A, Schroder A, Weber C. Nat Immunol. 2002;3:151–158.
87. Zen K, Parkos CA. Curr Opin Cell Biol. 2003;15:557–564. 88. Bradfield PF, Nourshargh S, Aurrand-Lions M, Imhof BA.
Arterioscler Thromb Vasc Biol. 2007;27:2104–2112. 89. Nourshargh S, Krombach F, Dejana E. J Leukoc Biol.
2006;80:714–718. 90. Scheiermann C, Colom B, Meda P, Patel NS, Voisin MB, Marrelli
A, et al. Arterioscler Thromb Vasc Biol. 2009;29:1509–1515. 91. Weber C, Fraemohs L, Dejana E. Nat Rev Immunol. 2007;7:467–477. 92. Laukoetter MG, Nava P, Lee WY, Severson EA, Capaldo CT,
Babbin BA, et al. J Exp Med. 2007;204:3067–3076. 93. Harris ES, McIntyre TM, Prescott SM, Zimmerman GA. J Biol
Chem. 2000;275:23409–23412. 94. Kevil CG, Bullard DC. Am J Med. 1999;106:677–687. 95. Bullard DC. Immunol Res. 2002;26:27–33. 96. Abdelbaqi M, Chidlow JH, Matthews KM, Pavlick KP, Barlow SC,
Linscott AJ, et al. Lab Invest. 2006;86:380–390. 97. Barlow SC, Langston W, Matthews KM, Chidlow Jr. JH, Kevil CG.
Am J Pathol. 2004;165:1849–1852. 98. Glawe JD, Patrick DR, Huang M, Sharp CD, Barlow SC, Kevil CG.
Diabetes. 2009;58:1292–1301. 99. Kevil CG, Hicks MJ, He X, Zhang J, Ballantyne CM, Raman C,
et al. Am J Pathol. 2004;165:609–616.100. Ostanin DV, Furr KL, Pavlick KP, Gray L, Kevil CG, Shukla D, et al.
Am J Physiol Gastrointest Liver Physiol. 2007;292:G1706–G1714.101. Titova E, Ostrowski RP, Kevil CG, Tong W, Rojas H, Sowers LC,
et al. J Neurosci Res. 2008;86:3240–3245.102. Pavlick KP, Ostanin DV, Furr KL, Laroux FS, Brown CM, Gray L,
et al. Int Immunol. 2006;18:389–398.103. Berlin C, Bargatze RF, Campbell JJ, von Andrian UH, Szabo MC,
Hasslen SR, et al. Cell. 1995;80:413–422.104. Osborn L, Vassallo C, Browning BG, Tizard R, Haskard DO,
Benjamin CD, et al. J Cell Biol. 1994;124:601–608.105. Castanedo GM, Sailes FC, Dubree NJ, Nicholas JB, Caris L, Clark
K, et al. Bioorg Med Chem Lett. 2002;12:2913–2917.106. Jackson DY. Curr Pharm Des. 2002;8:1229–1253.107. Yusuf-Makagiansar H, Anderson ME, Yakovleva TV, Murray JS,
Siahaan TJ. Med Res Rev. 2002;22:146–167.108. Patel SD, Chen CP, Bahna F, Honig B, Shapiro L. Curr Opin Struct
Biol. 2003;13:690–698.109. Wheelock MJ, Johnson KR. Curr Opin Cell Biol. 2003;15:509–514.110. Gooding JM, Yap KL, Ikura M. Bioessays. 2004;26:497–511.111. Nelson WJ, Nusse R. Science (New York, NY). 2004;303:1483–1487.112. Gessner R, Tauber R. Ann NY Acad Sci. 2000;915:136–143.113. Karayiannakis AJ, Syrigos KN, Efstathiou J, Valizadeh A, Noda M,
Playford RJ, et al. J Pathol. 1998;185:413–418.114. Zbar AP, Simopoulos C, Karayiannakis AJ. J Gastroenterol.
2004;39:413–421.115. Johnson KR, Lewis JE, Li D, Wahl J, Soler AP, Knudsen KA, et al.
Exp Cell Res. 1993;207:252–260.116. Higgins JM, Mandlebrot DA, Shaw SK, Russell GJ, Murphy EA,
Chen YT, et al. J Cell Biol. 1998;140:197–210.117. Taraszka KS, Higgins JM, Tan K, Mandelbrot DA, Wang JH,
Brenner MB. J Exp Med. 2000;191:1555–1567.
118. Sydora BC, Wagner N, Lohler J, Yakoub G, Kronenberg M, Muller W, et al. Clin Exp Immunol. 2002;129:35–42.
119. Dejana E, Spagnuolo R, Bazzoni G. Thromb Haemost. 2001;86:308–315.
120. Alexander JS, Alexander BC, Eppihimer LA, Goodyear N, Haque R, Davis CP, et al. Inflammation. 2000;24:99–113.
121. Gavard J. FEBS Lett. 2009;583:1–6.122. Kevil CG, Ohno N, Gute DC, Okayama N, Robinson SA, Chaney
E, et al. Free Radic Biol Med. 1998;24:1015–1022.123. Kevil CG, Payne DK, Mire E, Alexander JS. J Biol Chem.
1998;273:15099–15103.124. Alcaide P, Auerbach S, Luscinskas FW. Microcirculation.
2009;16:43–57.125. Andrews RK, Berndt MC. Thromb Res. 2004;114:447–453.126. Bussel JB, Kunicki TJ, Michelson AD. Hematology/the education
program of the American Society of Hematology. Am Soc Hematol. 2000:222–240.
127. Andre P, Denis CV, Ware J, Saffaripour S, Hynes RO, Ruggeri ZM, et al. Blood. 2000;96:3322–3328.
128. Gralnick HR, Kramer WS, McKeown LP, Garfinkel L, Pinot A, Williams SB, et al. Thromb Res. 1996;81:113–119.
129. Katayama T, Ikeda Y, Handa M, Tamatani T, Sakamoto S, Ito M, et al. Circ Res. 2000;86:1031–1037.
130. Ross JM, McIntire LV, Moake JL, Rand JH. Blood. 1995;85:1826–1835.
131. Khandoga A, Biberthaler P, Enders G, Axmann S, Hutter J, Messmer K, et al. Transplantation. 2002;74:681–688.
132. Massberg S, Enders G, Matos FC, Tomic LI, Leiderer R, Eisenmenger S, et al. Blood. 1999;94:3829–3838.
133. Savage B, Saldivar E, Ruggeri ZM. Cell. 1996;84:289–297.134. Burns AR, Bowden RA, MacDonell SD, Walker DC, Odebunmi
TO, Donnachie EM, et al. J Cell Sci. 2000;113(Pt 1):45–57.135. Luscinskas FW, Ma S, Nusrat A, Parkos CA, Shaw SK. Immunol
Rev. 2002;186:57–67.136. Furuse M, Hirase T, Itoh M, Nagafuchi A, Yonemura S, Tsukita S,
et al. J Cell Biol. 1993;123:1777–1788.137. Hartsock A, Nelson WJ. Biochim Biophys Acta. 2008;1778:660–669.138. Blaschuk OW, Oshima T, Gour BJ, Symonds JM, Park JH, Kevil
CG, et al. Inflammation. 2002;26:193–198.139. Huber D, Balda MS, Matter K. J Biol Chem. 2000;275:5773–5778.140. Kevil CG, Oshima T, Alexander B, Coe LL, Alexander JS. Am J
Physiol. 2000;279:C21–C30.141. Kucharzik T, Walsh SV, Chen J, Parkos CA, Nusrat A. Am J Pathol.
2001;159:2001–2009.142. Oshima T, Blaschuk O, Gour B, Symonds M, Elrod JW, Sasaki M,
et al. Life Sci. 2003;73:1729–1740.143. Stamatovic SM, Keep RF, Kunkel SL, Andjelkovic AV. J Cell Sci.
2003;116:4615–4628.144. Xu H, Dawson R, Crane IJ, Liversidge J. Invest Ophthalmol Vis Sci.
2005;46:2487–2494.145. Saitou M, Furuse M, Sasaki H, Schulzke JD, Fromm M, Takano H,
et al. Mol Biol Cell. 2000;11:4131–4142.146. Alexander JS, Jackson SA, Chaney E, Kevil CG, Haselton FR.
Inflammation. 1998;22:419–433.147. Inagaki-Ohara K, Sawaguchi A, Suganuma T, Matsuzaki G, Nawa
Y. Biochem Biophys Res Commun. 2005;331:977–983.148. Lal-Nag M, Morin PJ. Genome Biol. 2009;10:235.149. Krause G, Winkler L, Mueller SL, Haseloff RF, Piontek J, Blasig
IE. Biochim Biophys Acta. 2008;1778:631–645.

SECTION | VI Consequences of Disregulated Physiology2126
150. Morita K, Sasaki H, Furuse M, Tsukita S. J Cell Biol. 1999;147:185–194.
151. Nitta T, Hata M, Gotoh S, Seo Y, Sasaki H, Hashimoto N, et al. J Cell Biol. 2003;161:653–660.
152. Williams MR, Kataoka N, Sakurai Y, Powers CM, Eskin SG, McIntire LV. Endothelium. 2008;15:73–165.
153. Granger DN, Kubes P. J Leukoc Biol. 1994;55:662–675.154. Panes J, Granger DN. Gastroenterology. 1998;114:1066–1090.155. Eppihimer MJ, Wolitzky B, Anderson DC, Labow MA, Granger
DN. Circ Res. 1996;79:560–569.156. Keelan ET, Licence ST, Peters AM, Binns RM, Haskard DO. Am J
Physiol. 1994;266:H278–H290.157. Panes J, Perry MA, Anderson DC, Manning A, Leone B, Cepinskas
G, et al. Am J Physiol. 1995;269:1955–1964.158. Henninger DD, Panes J, Eppihimer M, Russell J, Gerritsen M,
Anderson DC, et al. J Immunol. 1997;158:1825–1832.159. Eppihimer MJ, Russell J, Langley R, Vallien G, Anderson DC,
Granger DN. Microcirculation. 1998;5:179–188.160. Langley RR, Russell J, Eppihimer MJ, Alexander SJ, Gerritsen M,
Specian RD, et al. Am J Physiol. 1999;277:1156–1166.161. Sklak R, Skalak T. In: Schmid-Schonbein GW, GD, ed., Physiology
and Pathophysiology of Leukocyte Adhesion. New York: Oxford University Press; 1995. p. 97–115.
162. Granger DN, Korthuis RJ. Annu Rev Physiol. 1995;57:311–332.163. Atherton A, Born GV. J Physiol. 1973;233:157–165.164. Bienvenu K, Granger DN, Perry M.. In: Schmid-Schonbein GW,
GD, ed., Physiology and Pathophysiology of Leukocyte Adhesion. New York: Oxford University Press; 1995. p. 278–293.
165. Perry MA, Granger DN. J Clin Invest. 1991;87:1798–1804.166. Nazziola E, House SD. Microvasc Res. 1992;44:127–142.167. Iigo Y, Suematsu M, Higashida T, Oheda J, Matsumoto K,
Wakabayashi Y, et al. Am J Physiol. 1997;273:138–147.168. Steinhoff G, Behrend M, Schrader B, Duijvestijn AM, Wonigeit K.
Am J Pathol. 1993;142:481–488.169. Watanabe K, Suematsu M, Iida M, Takaishi K, Iizuka Y, Suzuki H,
et al. Exp Mol Pathol. 1992;56:60–69.170. Cooper D, Stokes KY, Tailor A, Granger DN. Cardiovasc Toxicol.
2002;2:165–180.171. Kokura S, Rhoads CA, Wolf RE, Yoshikawa T, Granger DN, Aw TY.
J Vasc Res. 2001;38:47–58.172. Panes J, Perry M, Granger DN. Br J Pharmacol. 1999;126:537–550.173. Jourd’heuil D, Grisham MB, Granger DN. Curr Gastroenterol Rep.
1999;1:384–388.174. Ignarro LJ. Nitric Oxide: Biology and Pathobiology. San Diego:
Academic Press; 2010.175. Stokes KY, Cooper D, Tailor A, Granger DN. Free Radic Biol Med.
2002;33:1026–1036.176. Kubes P, Granger DN. Cardiovasc Res. 1996;32:699–708.177. Granger DN. Am J Physiol. 1997;273:G982–G986.178. Tailor A, Cooper D, Granger DN. Microcirculation. 2005;12:275–285.179. Cooper D, Russell J, Chitman KD, Williams MC, Wolf RE, Granger
DN. Am J Physiol Heart Circ Physiol. 2004;286:1895–1900.180. Mori M, Salter JW, Vowinkel T, Krieglstein CF, Stokes KY, Granger
DN. Am J Physiol Gastrointest Liver Physiol. 2005;288:920–926.181. Vowinkel T, Wood KC, Stokes KY, Russell J, Tailor A, Anthoni C,
et al. Am J Physiol Gastrointest Liver Physiol. 2007;293:1054–1060.182. Clark SR, Ma AC, Tavener SA, McDonald B, Goodarzi Z, Kelly
MM, et al. Nat Med. 2007;13:463–469.
183. Fuchs T, Brill A, Durschmied D, Schatzberg D, Hartwig JH, Myers D, et al. Neutrophil extracellular traps induce platelet adhesion and thrombus formation. Blood. 2009;114:1345.
184. Cerwinka WH, Cooper D, Krieglstein CF, Ross CR, McCord JM, Granger DN. Am J Physiol Heart Circ Physiol. 2003;284:535–541.
185. Ley RE, Peterson DA, Gordon JI. Cell. 2006;124:837–848.186. Qin J, Li R, Raes J, Arumugam M, Burgdorf KS, Manichanh C,
et al. Nature. 2010;464:59–65.187. Maynard CL, Weaver CT. Immunity. 2009;31:389–400.188. Macpherson AJ, Uhr T. Ann NY Acad Sci. 2004;1029:36–43.189. Macpherson AJ, Smith K. J Exp Med. 2006;203:497–500.190. Mowat AM. Nat Rev Immunol. 2003;3:331–341.191. Mowat AM, Millington OR, Chirdo FG. J Pediatr Gastroenterol
Nutr. 2004;39(suppl 3):S723–S724.192. Worbs T, Bode U, Yan S, Hoffmann MW, Hintzen G, Bernhardt G,
et al. J Exp Med. 2006;203:519–527.193. Coombes JL, Powrie F. Nat Rev Immunol. 2008;8:435–446.194. Forster R, Pabst O, Bernhardt G. Semin Immunol. 2008;20:171–180.195. Malmstrom V, Shipton D, Singh B, Al-Shamkhani A, Puklavec MJ,
Barclay AN, et al. J Immunol. 2001;166:6972–6981.196. Weaver CT, Hatton RD, Mangan PR, Harrington LE. Annu Rev
Immunol. 2007;25:821–852.197. Yen D, Cheung J, Scheerens H, Poulet F, McClanahan T, McKenzie
B, et al. J Clin Invest. 2006;116:1310–1316.198. Rescigno M, Di SA. J Clin Invest. 2009;119:2441–2450.199. Agace WW. Trends Immunol. 2008;29:514–522.200. Luster AD, Alon R, von Andrian UH. Nat Immunol. 2005;6:1182–1190.201. Mora JR. Inflamm Bowel Dis. 2008;14:275–289.202. von Andrian UH, KA . In: Schmid-Schonbein GW, GD, ed.,
Molecular Basis for Microcirculatory Disorders. Paris: Springer; 2004. p. 101–137.
203. von Andrian UH, Mempel TR. Nat Rev Immunol. 2003;3:867–878.204. Koboziev I, Karlsson F, Grisham MB. Ann NY Acad Sci. 2010:1–8.
In Press205. Friedl P, Noble PB, Zanker KS. J Immunol. 1995;154:4973–4985.206. Friedl P, Entschladen F, Conrad C, Niggemann B, Zanker KS. Eur J
Immunol. 1998;28:2331–2343.207. Friedl P, Zanker KS, Brocker EB. Microsc Res Tech. 1998;43:369–378.208. Lammermann T, Bader BL, Monkley SJ, Worbs T, Wedlich-Soldner
R, Hirsch K, et al. Nature. 2008;453:51–55.209. Van Goethem E, Poincloux R, Gauffre F, Maridonneau-Parini I, Le
Cabec V J. Immunol. 184:1049–1061.210. Lindbom L, Werr J. Semin Immunol. 2002;14:115–121.211. Werr J, Johansson J, Eriksson EE, Hedqvist P, Ruoslahti E,
Lindbom L. Blood. 2000;95:1804–1809.212. Bienvenu K, Harris N, Granger DN. Am J Physiol.
1994;267:H1573–H1577.213. Sixt M, Hallmann R, Wendler O, Scharffetter-Kochanek K, Sorokin
LM. J Biol Chem. 2001;276:18878–18887.214. Werr J, Eriksson EE, Hedqvist P, Lindbom L. J Leukoc Biol.
2000;68:553–560.215. Kuntz RM, Saltzman WM. Biophys J. 1997;72:1472–1480.216. Loike JD, Cao L, Budhu S, Hoffman S, Silverstein SC. J Immunol.
2001;166:7534–7542.217. Woods ML, Shimizu Y. J Leukoc Biol. 2001;69:874–880.218. Nikolai G, Niggemann B, Werner M, Zanker KS, Friedl P.
Immunology. 1998;95:62–68.

Chapter | 79 Recruitment of Inflammatory and Immune Cells in the Gut: Physiology and Pathophysiology 2127
219. Serrador JM, Nieto M, Sanchez-Madrid F. Trends Cell Biol. 1999;9:228–233.
220. Hogg N, Laschinger M, Giles K, McDowall A. J Cell Sci. 2003;116:4695–4705.
221. Hogg N, Smith A, McDowall A, Giles K, Stanley P, Laschinger M, et al. Immunol Lett. 2004;92:51–54.
222. Hauzenberger D, Klominek J, Holgersson J, Bergstrom SE, Sundqvist KG. J Immunol. 1997;158:76–84.
223. Smith A, Bracke M, Leitinger B, Porter JC, Hogg N. J Cell Sci. 2003;116:3123–3133.
224. Krivacic KA, Levine AD. J Immunol. 2003;170:5034–5044.225. Fiorucci S, Mencarelli A, Palazzetti B, Sprague AG, Distrutti E,
Morelli A, et al. Immunity. 2002;17:769–780.226. Krieglstein CF, Cerwinka WH, Sprague AG, Laroux FS, Grisham
MB, Koteliansky VE, et al. J Clin Invest. 2002;110:1773–1782.227. Rot A, von Andrian UH. Annu Rev Immunol. 2004;22:891–928.228. Middleton J, Neil S, Wintle J, Clark-Lewis I, Moore H, Lam C,
et al. Cell. 1997;91:385–395.229. Ajuebor MN, Swain MG. Immunology. 2002;105:137–143.230. Ajuebor MN, Swain MG, Perretti M. Biochem Pharmacol.
2002;63:1191–1196.231. Andres PG, Beck PL, Mizoguchi E, Mizoguchi A, Bhan AK,
Dawson T, et al. J Immunol. 2000;164:6303–6312.232. Varona R, Cadenas V, Flores J, Martinez AC, Marquez G. Eur J
Immunol. 2003;33:2937–2946.233. Laudanna C, Kim JY, Constantin G, Butcher E. Immunol Rev.
2002;186:37–46.234. Chan JR, Hyduk SJ, Cybulsky MI. J Exp Med. 2001;193:1149–1158.235. Grabovsky V, Feigelson S, Chen C, Bleijs DA, Peled A, Cinamon
G, et al. J Exp Med. 2000;192:495–506.236. Constantin G, Majeed M, Giagulli C, Piccio L, Kim JY, Butcher
EC, et al. Immunity. 2000;13:759–769.237. Gilat D, Hershkoviz R, Mekori YA, Vlodavsky I, Lider O. J
Immunol. 1994;153:4899–4906.238. Hershkoviz R, Schor H, Ariel A, Hecht I, Cohen IR, Lider O, et al.
Immunology. 2000;99:87–93.239. Lloyd AR, Oppenheim JJ, Kelvin DJ, Taub DD. J Immunol.
1996;156:932–938.240. Loike JD, Cao L, Budhu S, Marcantonio EE, El Khoury J, Hoffman
S, et al. J Cell Biol. 1999;144:1047–1056.241. Vaday GG, Lider O. J Leukoc Biol. 2000;67:149–159.242. Moghe PV, Nelson RD, Tranquillo RT. J Immunol Methods.
1995;180:193–211.243. Alon R, Cahalon L, Hershkoviz R, Elbaz D, Reizis B, Wallach D,
et al. J Immunol. 1994;152:1304–1313.244. Bauvois B, Van Weyenbergh J, Rouillard D, Wietzerbin J. Exp Cell
Res. 1996;222:209–217.245. Letterio JJ, Roberts AB. Annu Rev Immunol. 1998;16:137–161.246. Franitza S, Hershkoviz R, Kam N, Lichtenstein N, Vaday GG, Alon
R, et al. J Immunol. 2000;165:2738–2747.247. Vaday GG, Franitza S, Schor H, Hecht I, Brill A, Cahalon L, et al. J
Leukoc Biol. 2001;69:885–892.248. Carden DL, Granger DN. J Pathol. 2000;190:255–266.249. Granger DN. Microcirculation. 1999;6:167–178.250. Mihaescu A, Santen S, Jeppsson B, Thorlacius H. Br J Surg.
2010;97:226–234.251. Molla M, Gironella M, Salas A, Miquel R, Perez-del-Pulgar S,
Conill C, et al. Int J Cancer. 2001;96:99–9109.
252. Panes J, Anderson DC, Miyasaka M, Granger DN. Gastroenterology. 1995;108:1761–1769.
253. Panes J, Granger DN. Gastroenterology. 1996;111:981–989.254. Granger DN, Stokes KY, Shigematsu T, Cerwinka WH, Tailor A,
Krieglstein CF. Acta Physiol Scand. 2001;173:83–91.255. Granger DN, Kubes P. Methods Enzymol. 1996;269:434–442.256. Komatsu S, Berg RD, Russell JM, Nimura Y, Granger DN. Am J
Physiol Gastrointest Liver Physiol. 2000;279:186–191.257. Bauer P, Russell JM, Granger DN. Am J Physiol. 1999;276:G479–G484.258. Bauer P, Lush CW, Kvietys PR, Russell JM, Granger DN. Am J
Physiol Regul Integr Comp Physiol. 2000;278:1140–1147.259. Kurose I, Pothoulakis C, LaMont JT, Anderson DC, Paulson JC,
Miyasaka M, et al. J Clin Invest. 1994;94:1919–1926.260. Kurose I, Granger DN, Evans DJ, Evans DG, Graham DY,
Miyasaka M, et al. Gastroenterology. 1994;107:70–79.261. Yoshida N, Granger DN, Evans DJ, Evans DG, Graham DY,
Anderson DC, et al. Gastroenterology. 1993;105:1431–1440.262. Polenghi A, Bossi F, Fischetti F, Durigutto P, Cabrelle A, Tamassia
N, et al. J Immunol. 2007;178:1312–1320.263. Alvarez A, Ibiza S, Hernandez C, Alvarez-Barrientos A, Esplugues
JV, Calatayud S. Faseb J. 2006;20:2396–2398.264. Izcue A, Coombes JL, Powrie F. Annu Rev Immunol.
2009;27:313–338.265. Laroux FS, Norris HH, Houghton J, Pavlick KP, Bharwani S,
Merrill DM, et al. Int Immunol. 2004;16:77–89.266. Poussier P, Ning T, Banerjee D, Julius M. J Exp Med.
2002;195:1491–1497.267. Mizoguchi A, Bhan AK. J Immunol. 2006;176:705–710.268. Elson CO, Cong Y, McCracken VJ, Dimmitt RA, Lorenz RG,
Weaver CT. Immunol Rev. 2005;206:260–276.269. Kaser A, Zeissig S, Blumberg RS. Annu Rev Immunol. 2010270. Powrie F, Read S, Mottet C, Uhlig H, Maloy K. Novartis Found
Symp. 2003;252:92–98.271. Strober W, Fuss I, Mannon P. J Clin Invest. 2007;117:514–521.272. Uhlig HH, Powrie F. Springer Semin Immunopathol. 2005;
27:167–180.273. Bamias G, Nyce MR, De La Rue SA, Cominelli F. Ann Intern Med.
2005;143:895–904.274. Sans M, Salas A, Soriano A, Prats N, Gironella M, Pizcueta P, et al.
Gastroenterology. 2001;120:1162–1172.275. Steeber DA, Tang ML, Zhang XQ, Muller W, Wagner N, Tedder TF.
J Immunol. 1998;161:6638–6647.276. Tang ML, Hale LP, Steeber DA, Tedder TF. J Immunol.
1997;158:5191–5199.277. Zhang XW, Liu Q, Thorlacius H. Scand J Gastroenterol.
2001;36:270–275.278. Abdelbaqi M, Chidlow JH, Matthews KM, Pavlick KP, Barlow SC,
Linscott AJ, et al. Lab Invest. 2006;86:380–390.279. Pavlick KP, Ostanin DV, Furr KL, Laroux FS, Brown CM, Gray L,
et al. Int Immunol. 2006;18:389–398.280. Sydora BC, Wagner N, Lohler J, Yakoub G, Kronenberg M, Muller
W, et al. Clin Exp Immunol. 2002;129:35–42.281. Rivera-Nieves J, Olson T, Bamias G, Bruce A, Solga M, Knight RF,
et al. J Immunol. 2005;174:2343–2352.282. Bjursten M, Bland PW, Willen R, Hornquist EH. Eur J Immunol.
2005;35:2274–2283.283. Bowden RA, Ding ZM, Donnachie EM, Petersen TK, Michael LH,
Ballantyne CM, et al. Circ Res. 2002;90:562–569.

SECTION | VI Consequences of Disregulated Physiology2128
284. Podolsky DK, Lobb R, King N, Benjamin CD, Pepinsky B, Sehgal P, et al. J Clin Invest. 1993;92:372–380.
285. Podolsky DK. N Engl J Med. 2005;353:1965–1968.286. Schneider MK, Strasser M, Gilli UO, Kocher M, Moser R, Seebach
JD. Transplantation. 2002;73:789–796.287. Rutgeerts P, van Deventer S, Schreiber S. Aliment Pharmacol Ther.
2003;17:1435–1450.288. Rutgeerts P, Vermeire S, Van Assche G. Gastroenterology.
2009;136:1182–1197.289. Yousry TA, Major EO, Ryschkewitsch C, Fahle G, Fischer S, Hou J,
et al. N Engl J Med. 2006;354:924–933.290. Koizumi M, King N, Lobb R, Benjamin C, Podolsky DK.
Gastroenterology. 1992;103:840–847.291. Nakamura S, Ohtani H, Watanabe Y, Fukushima K, Matsumoto T,
Kitano A, et al. Lab Invest. 1993;69:77–85.292. Kawachi S, Morise Z, Jennings SR, Conner E, Cockrell A, Laroux
FS, et al. Inflamm Bowel Dis. 2000;6:171–180.293. Kawachi S, Jennings S, Panes J, Cockrell A, Laroux FS,
Gray L, et al. Am J Physiol Gastrointest Liver Physiol. 2000;278:G734–G743.
294. Kawachi S, Morise Z, Conner E, Laroux FS, Gray L, Fuseler J, et al. Biochem Biophys Res Commun. 2000;268:547–552.
295. Morise Z, Eppihimer M, Granger DN, Anderson DC, Grisham MB. Inflammation. 1999;23:99–110.
296. Podolsky DK, Lobb R, King N, Benjamin CD, Pepinsky B, Sehgal P, et al. J Clin Invest. 1993;92:372–380.
297. Schurmann GM, Bishop AE, Facer P, Vecchio M, Lee JC, Rampton DS, et al. Gut. 1995;36:411–418.
298. McCafferty DM, Smith CW, Granger DN, Kubes P. J Leukoc Biol. 1999;66:67–74.
299. Jones SC, Banks RE, Haidar A, Gearing AJ, Hemingway IK, Ibbotson SH, et al. Gut. 1995;36:724–730.
300. Oshitani N, Campbell A, Bloom S, Kitano A, Kobayashi K, Jewell DP. Scand J Gastroenterol. 1995;30:915–920.
301. Bennett CF, Kornbrust D, Henry S, Stecker K, Howard R, Cooper S, et al. J Pharmacol Exp Ther. 1997;280:988–1000.
302. Burns RC, Rivera-Nieves J, Moskaluk CA, Matsumoto S, Cominelli F, Ley K. Gastroenterology. 2001;121:1428–1436.
303. Yacyshyn BR, Bowen-Yacyshyn MB, Jewell L, Tami JA, Bennett CF, Kisner DL, et al. Gastroenterology. 1998;114:1133–1142.
304. Schreiber S, Nikolaus S, Malchow H, Kruis W, Lochs H, Raedler A, et al. Gastroenterology. 2001;120:1339–1346.
305. Yacyshyn BR, Chey WY, Goff J, Salzberg B, Baerg R, Buchman AL, et al. Gut. 2002;51:30–36.
306. Xu H, Gonzalo St JA, Williams PY, Kupper IR, Cotran TS, Springer RS, et al. J Exp Med. 1994;180:95–109.
307. Kawachi S, Cockrell A, Laroux FS, Gray L, Granger DN, van der Heyde HC, et al. Am J Physiol. 1999;277:G572–G576.
308. D’Agata ID, Paradis K, Chad Z, Bonny Y, Seidman E. Gut. 1996;39:605–608.
309. Uzel G, Kleiner DE, Kuhns DB, Holland SM. Gastroenterology. 2001;121:958–964.
310. Lopez-Cubero SO, Sullivan KM, McDonald GB. Gastroenterology. 1998;114:433–440.
311. Conner EM, Brand S, Davis JM, Laroux FS, Palombella VJ, Fuseler JW, et al. J Pharmacol Exp Ther. 1997;282:1615–1622.
312. Hesterberg PE, Winsor-Hines D, Briskin MJ, Soler-Ferran D, Merrill C, Mackay CR, et al. Gastroenterology. 1996;111:1373–1380.
313. Picarella D, Hurlbut P, Rottman J, Shi X, Butcher E, Ringler DJ. J Immunol. 1997;158:2099–2106.
314. Viney JL, Jones S, Chiu HH, Lagrimas B, Renz ME, Presta LG, et al. J Immunol. 1996;157:2488–2497.
315. von Andrian UH, Mackay CR. N Engl J Med. 2000;343:1020–1034.