Embed Size (px)
Citation preview

Physiologic Status of the Anorectum Following Sphincter-saving Resection for Carcinoma of the Rectum*
NAOMI IWAI, M.D., KvOZO HASHIMOTO, M.D., TETSURO YAMANE, M.D., OSAMU KOJIMA, M.D., BUNZO NISHIOKA, M.D., YOSHIHIRO FUJITA, M.D., SUSUMU MAJIMA, M.D.
Iwai N, Hashimoto K, Yamane T, Kojima O, Nishioka B, Fujita Y, Majima S. Physiologic status of the anorectum fo l lowing sphincter-saving resection for carcinoma of the rectum. Dis Colon Rectum 1982;25:652-659.
The physiologic status of the anorectum after low anterior resec- tions or pull-through operations of the rectum was evaluated clin- ically and by manometric studies. It was demonstrated that the presence of a normal anal resting pressure and an anorectal re- f lex were important to achieve postoperative continence after sphincter-saving operations. In patients with anastomotic leaks and poor function, a marked high-pressure zone in the anal canal and an anorectal reflex were not found, but as local inflammation resulting from the anastomotic leak disappeared, these paramet- ers returned to normal. A normal anorectal reflex was found in one of three patients after Bacon.type pull-through operations, but the remaining two showed an increase of anal canal pressure during colonic distention. These results indicate that an elevation of anal-canal pressure in response to colonic distention plays a significant role in fecal continence at the time of "a sense of urgency" if internal sphincter function is impaired. [Key words: Anorectum; Manometry, anorectal; Cancer, rectal; Sphincter- saving operations]
THOUGH the t r ea tmen t of carc inomas si tuated in the u p p e r and lower th i rd of the r ec tum is now rea- sonably s tandardized, some cont roversy still exists re- ga rd ing m a n a g e m e n t o f cancers o f the middle third, with the lower edge 7.5 to 11.5 cm f r o m the anal margin . Nevertheless , there is an increasing t endency toward sphincter-saving opera t ions for these tumors because o f increasingly early detect ion o f rectal car- cinoma. However , the efficacy o f the opera t ion in t e r m s o f a n a l f u n c t i o n has n o t b e e n c l e a r l y established.
T h e pu rpose of this s tudy was to evaluate the func- t ion o f the p r e s e r v e d a n o r e c t u m by clinical a n d
* Presented at the 8th Biennial Congress of the International Society of University Colon and Rectal Surgeons, Melbourne, Au- stralia, September 7 to 11, 1980.
Address reprint requests to Dr. Iwai: First Department of Surgery, Kyoto Prefectural University of Medicine, Kamigyo-ku, Kyoto, Japan.
From the First Department of Surgery, Kyoto Prefectural University of Medicine,
Kyoto, Japan
m a n o m e t r i c assessments o f con t inence o f pa t i en t s who have had low an te r io r resect ions or pu l l - th rough opera t ions o f the rec tum.
P a t i e n t s a n d M e t h o d s
Twen ty -one patients were included in this study, 12 m e n and nine women, whose ages r anged f r o m 32 to 78 years and who had u n d e r g o n e sphincter-saving resections for carc inoma o f the rec tum. O f the 21 patients, low an te r ior resection was p e r f o r m e d in 18 and abdomino-ana l pu l l - th rough opera t ion (Bacon 1 technique) in three. T h e height o f the anas tomosis was d e t e r m i n e d by pa lpa t ion or examina t ion with a small s igmoidoscope, and the mean anorecta l s tump was 6.3 cm long in those t rea ted with an te r io r resec- tion. In all patients, a detai led assessment of post- opera t ive bowel funct ion was made on the basis o f interviews and manomet r i c examina t ions at varying intervals r ang ing f rom three months to five years fol- lowing opera t ion . T h e m a n o m e t r i c s tudy was also p e r f o r m e d in seven pat ients who had u n d e r g o n e r ight hemico lec tomy as a control g roup .
A n o r e c t a l M a n o m e t r i c S t u d y : T h e p r o b e was made with a Foley ca the te r with a side hole record ing orifice of polyvinyl tubing, 2 m m in d iameter . T h e bal loon for s t imulat ion in the r ec tum was placed at the tip o f the probe, and the side hole o f the pressure recep to r was located 5 cm distal to the lower end o f the balloon. T h e p robe was pe r fused with water at the constant rate o f 10 m l / h o u r with an A t o m automat ic infusion p u m p . This appa ra tus was connec ted to a t r a n s d u c e r ( T o y o B a l d o w i n Co., Ltd . ) , a n d the pressure was r eco rded on a po lyg raph (Sanei L-012). Zero pressure , used t h r o u g h o u t this s tudy, was de-
0012-3706/82/1000/0652/$01.20 �9 American Society of Colon and Rectal Surgeons
6 5 2

Volume 25 Number 7 S P H I N C T E R - S A V I N G R E S E C T I O N 653
TABLE 1. Clinical Assessment and Manometric Study of Anorectal Structures After Low Anterior Resection Without Anastomotic Leak
Rectal Case Stump
Number (cm)
Postoperative Manometric Study
Time of High- Length of Anastomotic Postoperative Clinical pressure High-pressure ARPD*
Leak Investigation Assessment Zone Zone (cm) (cm H~O) Anorectal
Reflex?
1 7.0 2 6.5 3 7.0 4 6.0 5 5.0 6 7.0 7 7.5 8 5.5 9 6.0
10 6.0 11 6.5 12 7.0 13 6.0
Mean_+SE 6.4_+ 0.2
m
m
m
4 mo Good + 4.0 56 5 mo Good + 3.0 42 4 mo Good + 1.5 28 3 mo Good + 2.0 44 4 mo Good + 2.0 58 5 mo Good + 2.5 84 4 mo Good + 4.0 84 3 mo Good + 2.0 74 4 mo Good + 2.5 52 3 mo Good + 2.0 56 5 mo Good + 4.0 78
1 yr, 4 mo Good + 2.5 92 1 yr, 3 mo Good + 3.0 68
2.7 + 0.2 62.8 -+ 5.1
+ + + + + + + + + + + + +
* ARPD = Anorectal pressure difference. ? + = present; - = absent; N = not examined.
1 j j = j l l i i i [ i i l j i i i i i l i l l ) l l l l I I I I I~ I I I1111 I 1~] 11 i I i l i i i ) | 11111 i i i I~ l i I i i i l i i i I1111 ji i i i i i i i i i i1~1 I l l t l I lU
i
" - i
I
cmHzO
. _ I ~ ~ ~
I
7 6 5 4 3 2 -- ' , i I i i
:. �9 ~ ~ i ' ! , - . - - ~ "
i l l - ! 7 1 i i : i .... i " " 7 i ~ i i i i i . . . . i i ~ . . . . . .
losec ( 'A)
I : . . . .
i
. . _ i l �84 . . . . i
i
l ~ i i i i i i ' i ' i ' i i i i i i i i i i i i i i i : i i i ~ i i i i i i i i iii i i i i i i i i i i i i i i i i O i i i i i i i i i i i i l l l l l f i i i l j l i i " ; ~ i i i i i i i i i ~ j i i i i i i i i i i i i i i i i i
7 6 ~ ~ ~ . . . . - ~ - 0 e r a ' . i . ; - _ : . ~_ -t i . Im q :i,~ .~ . . . . . 5 4 3 2 1! ~itl-I.:id-::4~:~-:.l:-.l:~:fl~[.:[~l::~ .~ d - d d ~ h- ld-d- . ' - l -Y- . ; i / i i-~ ~-. I - _ F - h ~ l - l - ~ i h - - ~ - f - ; - ~ t - T [ : : - :
-sOt-l-.: :!-Th:?..o-t'l~?._:.-~-w~'~t~ - ~ ~ . ~ f - l - ~ - ! ~~ ~:-~. t--I ! ~-~..-~:::.~,:,-~,-~~-I~
i . ~ . t - t ~ I
cmH=O :"
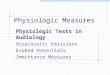
FIG. 1. A. Postoperative anorectal pressure profile of control subject. B. Postoperative anorectal pressure profile after low anterior resection. Distances are in centimeters from the anal margin. A marked high-pressure zone in the anal canal was observed in patients with good anal control after low anterior resection as well as in the control subjects.

Dis. Col, & Rect, 654 IWAI, ET AL. Octobe r 1982
~'T~, i : . . . . [ ! i i , i , i l i i i I I I i i i i i i i i i i i i i ] ; i , ] ; l l l , ~ : l i , i i I h i l i ~ i i i i i i l i l l l i l l l l i l i l i ~ l [ J ] l i i l l l i i i i i l i , i i l l l l l i
R e c t a l distension
,Pressure in A n a l C a n a l -
50
~ o ; i - . . . . . ~ . . . . . . . . . . . . . . . . . . . . . . . . . . . - l O s e c ~-
=mH,O (A)
iiiiiiii~liiiilliJiii~_ .Jiiiiiiiiiilllllillllllilllllliillll~_
Rectal distension
~ i . - ~ _ ~ ~ ~ , ' . i - ; t - :~_ , ,__ .:_Z~ ~-.4~ - ; ' ~ . . - - ' ~ : ~ _ , _ ' _ _ _ _ _ ~ ' . ~ 1 _ ... ' ~ v s = i ~ : l : ~ - v - ~ - ; q / t . . ,
T ~--:Pressure in Anal Canal!2~ ~i . l -G-w,k.~-~ci_!._ ~ ; - . - - = - 7 - -! - - i ~----~ = i-: - ~ - ~ - f = T=h-l-~ -i--~--)-l-
i ~ , , - r - - = - = ~ = t - r - - r - . , ,---r-v-. ~. .............. lOs~ '-'~ , ~--r~,-I , ,-- ~ t , 1~ ,,
c, mH,O (B)
, l i { l l i i l l 1 1 1 | i f i l l l l i l i l l l ~ _ l l i J i J J i i l i l i i J
FIG. 2. A. Postoperative anorectal reflex o f control subject. B. All pat ients with good anal control af ter low anter ior resect ion showed a typical decrease in anal-canal p ressure in response to rectal dis tent ion, as did the control subjects�9
TABLE 2 . Clinical Assessment and Manometric Stud)' q[-Anorectal Structures After Low Anterior Resection lVitk Anastonu~tic Leak
Rectal T i m e o f Case S tump Anas tomot ic Postoperat ive Clinical
N u m b e r (cm) Leak Invest igat ion Asses smen t
Postoperat ive Manomet r i c Study
High- Leng th o f p res su re H igh -p re s su re ARPD* Anorectal
Zone Zone (cm) (cm H20) Ref lex t
3 me Poor 14 6.0 + 1 1
7 m e Fair
3 m e Poor 15 7.0 + 1
7 m e Fair
6 me Poor 16 7.0 + 1 1
4 yr Fair
3 ) r Fair 17 5.0 ~- 1 1
4 vr 6 m e Good
3 m e Fair 18 5.0 + ~
1 yr, 10 rno Good
- 1 6 -
+ 2.0 76 -
- 1 8 -
+ 3.0 34 +
N N N
+ 3.0 26 -
+ 2.0 50 -
+ 2.5 92 +
+ 1.5 60 -
+ 2.5 76 +
* ARPD = Anorecta l p re s su re difference. % + = present ; - = absent ; N = not examined .

Vol ..... 25 SPHINCTER-SAVING RESECTION 655 Number 7
t e rmined by record ing a tmospher ic pressure at the anal margin .
T h e manome t r i c study was p e r f o r m e d without spe- cial bowel p repara t ion , with the pat ient in the left lateral position. T h e anorecta l pressure profi le was first r e c o r d e d in cen t ime te r s by wi thd rawing the p robe which was in t roduced 8 cm above the anal verge. To examine the anorecta l reflex, the p robe was set to locate the p r e s s u r e r e c e p t o r in the h igh- p r e s su re zone a f t e r e x a m i n a t i o n o f the anorec ta l pressure profile. In this position, the presence or ab- sence o f an anorecta l ref lex was d e t e r m i n e d by dis- t end ing the balloon in the r ec tum for 10 seconds with 20 to 30 ml o f air.
Clinical Assessment : All pa t ients were in te r ro- gated with r ega rd to their bowel habits and anal con- trol. Par t icular a t tent ion was paid to the presence or absence o f fecal soiling, the ability o f the pat ient to recognize and dist inguish between flatus and solid or liquid feces, and the occur rence of inadver ten t e r rors in the passage o f flatus and feces. In addit ion, any dietetic, domestic, or social restruct ions as a resul t o f funct ional imper fec t ions a f t e r the o p e r a t i o n were documen ted . On the basis o f these p a r a m e t e r s o f bowel function, the results were classified as good, fair, or poor , as de f ined below. Good consisted of excellent results with funct ion indist inguishable f rom no rma l and no e r rors in the passage o f feces and no soiling. Fair consisted o f occasional mild soiling and t e n e s m u s , bu t d i f f e r e n t i a t i o n be tween f la tus and feces possible, and a few errors in control; however , these deficiencies do not in ter fere with the patient 's social life. Poor mean t unsat isfactory bowel function,
with f r equen t soiling, inability to d i f fe ren t ia te be- tween flatus and feces, and f r equen t e r rors in control , and social activities dis turbed.
Results
1. Patients with Low Anterior Resect ion: O f the 18 pat ients t rea ted by low an te r io r resection, 13 could be r ega rded as having good anal control at the first interview, which was held three to 16 m o n t h s af ter opera t ion . A s u m m a r y o f the clinical and m a n o m e t r i c studies o f these patients is p resen ted in Tab le 1. None o f these patients had anas tomot ic leaks. T h e anorecta l s tumps were 5.0 to 7.5 cm long (mean 6.4 -+ 0.2 cm). It was notable that the m a x i m u m re tu rn o f anal func- tion was achieved within three months af ter ope ra t ion for all patients, including one who was interviewed 16 months af ter resection. In the m a n o m e t r i c s tudy, the patients with good anal control exhibi ted the same anorecta l pressure profile, with a h igh-pressure zone in the anal canal, as did the control subjects (Fig 1), and their anorecta l pressure d i f ferences r anged f r o m 28 to 92 cm H 2 0 (mean 62.8 +- 5.1 cm H~O), which was not significantly d i f fe ren t f rom those of the con- trol g r o u p (60.1 _+ 7.9 cm H20) . With r ega rd to the anorectal reflex, all pat ients showed a typical decrease in anal-canal pressure , co r r e spond ing to rectal disten- tion (Fig. 2).
T h e remain ing five patients with low an te r io r re- section were cons idered to have fair or p o o r anal con- trol at the t ime of the first review, usually th ree mon ths af ter opera t ion , but by the t ime o f the second examinat ion , four mon ths to th ree and one -ha l f years
~ T J JJ J J I I T T F T " H T I T [ l q T r ~[ FT-[T'FI~H'q'- " T F V I T 1 - F I ' q T [ I + F F F F r q T I q q q q q - F ' ~ r l ; [ Tlql~-, F T T F F ~ fT1~'T ; H H T F !
& ~, 6 5 4
FIG. 3. Anorectal pressure profile of Case 14. A. No marked high-pressure zone was noted three months postopera- tively. B. Anorectal pressure profile with a high-pressure zone, observed seven months postoperatively, was similar to profile of control subjects.
-50 T
0 K _ _ q crnH zO lOsec (A)
�9 �9 ~ . . . . . . . "~ . . . . . ; T ; ' Z ; ~ T T ' [ ' ; ; , ; ; T T F I I ; ~ T T ~ r . ~ I ~ F I T T T U F H . T I q T 1 q T , T T ~ T T T T T f q q - T T T T T ' F T ~ , F F F ~ T 1-/ ~, ~ . . . . . . . ; ' " ,
-i 50 ~
c.mH 20
_5 4 3 2 1 0 ~ i
( B ) ,

Dis. Col. & Rect.
656 IWAI, ET AL. October 1982
FIG. 4. Anorectal reflex of Case i4. A. A pressure decrease in response to rectal distention was not found three months postoperatively. B. Rectal distention caused a pressure decrease in the anal canal seven months postoperatively, with functional improvement.
l a t e r , t h e y h a d a c h i e v e d f a i r o r g o o d a n a l c o n t r o l .
R e s u l t s o f t h e t e s t s o f t h e s e f ive p a t i e n t s a r e l i s t e d i n
d e t a i l i n T a b l e 2. A n a s t o m o t i c l e a k s w e r e p r e s e n t in
all f ive p a t i e n t s ; t h e a n o r e c t a l s t u m p s w e r e 5 .0 to 7 .0
c m l o n g ( m e a n 6 .0 - - 0 . 4 c m ) l ike i n t h e p a t i e n t s w i t h
g o o d a n a l c o n t r o l . M a n o m e t r i c s t u d i e s s h o w e d o n l y
m i n o r p r e s s u r e r e l a x a t i o n i n t h e a n a l c a n a l i n t h o s e
w i t h p o o r a n o r e c t a l f u n c t i o n , a n d t h e i r a n o r e c t a l
p r e s s u r e d i f f e r e n c e s r a n g e d f r o m 16 to 18 c m H 2 0 ,
c o n s i d e r a b l y l o w e r t h a n t h o s e o f t h e p a t i e n t s w i t h
TABLE 3. Clinical Assessment and Manometric Study of Anorectal Structures After Pull-through Operation
Time of Case Postoperative Clinical
Number Investigation Assessment
Postoperative Manometric Study
High- Length of pressure High-pressure ARPD* Anorectal
Zone Zone (cm) (cm H20) Reflext
3 yr Fair 19
5 yr Fair
1 yr, 2 mo Fair 20
2 yr, 1 mo Good
6 mo Poor 21
1 yr, 6 mo Fair
+ 2.0 62 -
+ 2.5 74 -
+ 1.5 34 -
+ 2.5 84 +
N N N
+ 2.0 30 -
* ARPD = Anorectal pressure difference. t + = present; - = absent; N = not examined.

Volume 25 Number 7 S P H I N C T E R - S A V I N G R E S E C T I O N 657
good anal control. As functional improvemen t oc- curred, however, a high-pressure zone such as that seen in the control subjects was observed again, and anorectal pressure differences ranged f rom 26 to 92 cm H 2 0 (mean 60.8 --- 11.6 cm H=O) (Fig. 3). T h e anorectal reflex, on the o the r hand, was absent in patients with poo r control, but when funct ion im- proved, relaxation o f the anal-canal pressure corre- sponding to rectal distention was observed again in four o f the five patients at the t ime o f the second examinat ion (Fig. 4).
2. Patients with Abdomino-anal Pull-through Operation: T h e results o f three patients t rea ted by a b d o m i n o - a n a l p u l l - t h r o u g h o p e r a t i o n (Bacon technique) are presented in Table 3. Clinical assess- men t showed p o o r anorec ta l func t ion du r ing six mon ths a f t e r ope ra t ion , but acceptable anorec ta l funct ion was rega ined by one year, and social ac- tivities were not restr ic ted, a l though the patients sometimes complained o f soiling. Anorectal funct ion was finally classified as fair for two patients and good for one.
Manometr ic studies were carr ied out at varying intervals ranging f rom 14 months to five years a f te r operat ion, when functional state was ei ther fair or good. All o f these patients had the same anorectal pressure profile, with a high-pressure zone in the anal canal, as did the patients with good anal control af ter low anter ior resection; their anorectal pressure dif- ferences ranged f rom 30 to 84 cm H20 (mean 56.8 + 9.6 cm H20) (Fig. 5). However , they showed a some-
what d i f ferent anorectal ref lex pat tern. When the colon (new rectum) was expanded by inflation o f the balloon with air, the anal-canal pressure increased greatly in two patients with fair control, while the pa- t ient with good anal control had relaxation o f the anal canal (Fig. 6).
Discussion
Sphincter-saving resections have been used for car- cinomas o f the midth i rd o f the rectum, when their size and invasiveness do not requi re more radical surgery. However , d i f ferences of opinion persist in r e g a r d to the qual i ty o f func t ion ach ieved a f t e r sphincter-saving operat ions and to the na ture of the motor mechanisms that subserve cont inence in post- operat ive patients. These varying views 2-4 may well reflect differences in the me thod and time o f post- operat ive funct ional assessments as well as in opera- tive techniques. T h e patients described here had been t reated for carcinoma of the rec tum e i ther by low anter ior resection or Bacon's pul l - through operat ion. Clinical and manomet r ic assessments o f postoperat ive anorectal funct ion were p e r f o r m e d at varying inter- vals (three months to five years) af ter operat ion, and for patients with fecal incontinence at the first as- sessment, a second examinat ion was p e r f o r m e d four months to two years later.
O f the 18 patients t reated by low an te r ior resection, 13 had no anastomotic leaks and achieved good anal control within three months af ter operat ion. T h e re- maining five patients had anastomotic leaks and fre-
FXG. 5. A. Postoperative anorectal pressure profile of Case 19. B. Case 20. C. Case 21. A high-pressure zone in the anal canal was observed in these three cases.

Dis, Col, & Reel 6 5 8 1WAI, ET AL. October 1982
Fro. 6. A, C. A pressure elevation in the anal canal in response to rectal dis- tention was observed in Cases 19 and 21. B. Anorectal reflex of Case 20. A pressure decrease in the anal canal in response to rectal distention was ob- served in a patient with good anal control after pull-through operation.
quent soiling, with 20 to 30 bowel movements a day dur ing the first three months after operation. As the inf lammat ion associated with the anastomotic leak disappeared, however, improvement in fecal conti- nence was noted to occur up to seven months after operation, and the functional state at the time of the second examinat ion was classified as fair, with five to six movements per day and only occasional fecal soil- ing. These results indicate that anastomotic leaks con- tribute to poor funct ion dur ing the first six months after operat ion but that function improves with time, as local i n f l a m m a t i o n d u e to a n a s t o m o t i c leak
disappears. For the t h r e e p a t i e n t s t r e a t e d by Bacon ' s
abdomino-anal pull- through, on the o ther hand, it took more than one year to gain good or fair anal control even without any anastomotic leak. These pa- tients occasionally soiled, even t hough their social life was not severely restricted. I m p r o v e m e n t of clinical function after low anter ior resection was achieved more quickly than after abdomino-anal pul l- through. The inferiority of the latter operat ion seemed to arise f rom the Bacon technique, which requires section o f the levator ani muscle and is associated with some damage o f the internal sphincter muscle resulting from denud ing of the anal mucosa.
In addit ion to the a forement ioned clinical assess- ment, manometr ic studies have been used by some investigators 5"6 to study the residual motor mecha- nisms capable of providing satisfactory degrees of
postoperative continence. In the present study, man- ometric assessments o f pressures in the anal canal r emnan t and o f the anorectal reflex were made at varying intervals after operat ion because a significant correlation had been demons t ra ted between clinical f ea tu res and m a n o m e t r i c results in ou r previous study on the postoperat ive continence o f patients with imperfora te anus. r It was found that, in patients with carcinoma also treated by sphincter-saving excision o f the rectum, a normal anal resting pressure and an anorectal reflex were impor tan t for the achievement o f postoperat ive continence. Actually, all patients classified as having good func t ion had a m a r k e d high-pressure zone in the anal canal and an anorectal reflex, while all those with poor or fair funct ion had a less marked high-pressure zone in the anal canal or no anorectal reflex, except for two patients with fair functional results after low anter ior resection. The two patients classified as having poor function had no high-pressure zone in the anal canal and no anorectal reflex; their anorectal pressure differences were less than 20 cm H20. However, when anal control became fair, the pressure differences rose to more than 20 cm H20, and the anorectal reflex was observed. On the contrary, it was noted that reflexes were absent in ano ther three patients who had anastomotic leaks after low anter ior resection. These manometr ic data indicate that a marked high-pressure zone and an adequate anorectal pressure difference are more im- por tant than the anorectal reflex in restoring conti-

Volume 25 Number 7 S P H I N C T E R - S A V I N G R E S E C T I O N 659
nence after sphincter-saving resections for carcinoma of the rectum.
Cortesini 6 repor ted a significant decrease in anal- canal pressure after abdomino-anal pu l l - th rough op- erations (Bacon procedure) . On the o ther hand, a high-pressure zone in the anal canal was observed at the time of fair anal control in our three patients t reated by the abdomino-anal pu l l - th rough opera- tion. The internal sphincter muscle was preserved as far as possible in ou r p rocedure af ter resection o f the levator ani muscle. However, removal o f part o f the internal sphincter is inevitable dur ing the Bacon op- eration. Therefore , the normal decrease in anal canal pressure, dur ing colonic balloon distention, was not present when function was fair. However, a normal anorectal reflex was observed in one patient when clinical assessment showed improvement to good anal control. Two o f the three showed increased anal- canal pressure dur ing colonic distention, suggesting anal contraction ra ther than relaxation. This might be explained as follows: resection o f the levator ani mus- cle and a certain degree o f impai rment of the internal sphincter muscle cont r ibute to the absence o f an anorectal reflex. However, the function o f the inter- nal s p h i n c t e r , which main ly c o n t r i b u t e s to the maintenance of anal-canal pressure at rest and to the anorectal reflex, is restored as clinical improvement progresses. Two of the three patients showed in- creased anal-canal pressure instead o f relaxation. It seems likely that this pressure increase was due to
contraction o f the external sphincter, which compen- sates for the resected levator ani muscle. Thus we are in agreement with Cortesini when he states that an elevation o f anal-canal pressure dur ing colonic bal- loon distention plays a significant role in fecal conti- nence at the time of a "sense of urgency." Therefore , in the absence o f l eva tor func t ion , the e x t e r n a l sphincter contributes mainly to anal-canal pressure only when a bolus is delivered into the anal canal.
R e f e r e n c e s
1. Bacon HE. Abdominoperineal proctosigmoidectomy with sphincter preservation: five-year and ten-year survival after "pull-through" operation for cancer of rectum. JAMA 1956;160:628-34.
2. Goligher JC, Duthie HL, Dedombal FT, Watts JM. Abdomino-anal pull-through excision for tumors of the mid-third of the rectum: a comparison with low anterior resection. Br J Surg 1965;52:323-34.
3. Kennedy JT. Mcomish D, Bennett RC, Hughes ESR, Cuthbertson AM. Abdomino-anal pull-through resection of the rectum. BrJ Surg 1970;57:589-96.
4. Bennett RC, Hughes ESR, Cuthbertson AM. Long-term re- view of function following pull-through operations of the rectum. Br J Surg 1972;59:723-5.
5. Bennett RC, Buls J, Kennedy JT, Hughes ESR. The physiologic status of the anorectum after pull-through oper- ations. Surg Gynecol Obstet 1973;136:907-13.
6. Cortesini C. Anorectal reflex following sphincter-saving opera- tions. Dis Colon Rectum 1980;23:320-6.
7. lwai N, Ogita S, Kida M, Fujita Y, Majima S. A clinical and manometric correlation for assessment of postoperative con- tinence in imperforate anus. J Pediatr Surg 1979;14:538- 43.