Embed Size (px)
Citation preview

FEATURE
Physiologic effects andmeasurement of carbon dioxideand oxygen levels duringqualitative respirator fit testing
In the United States, two commonly used qualitative respirator fit test methods require the use of a test hoodto be placed over the subject’s head and shoulders. Workers fit tested by this method have commented on thediscomfort of being inside the test hood. This study was designed to quantify some parameters that mightlead to these types of comments. For this study, subjects performed a series of four respirator fit tests. Aquantitative and a qualitative fit test were performed with a full facepiece respirator. Then a quantitative anda qualitative fit test were performed with an N95 filtering facepiece respirator. Parameters measured include:subjects’ height, weight, and age, oxygen and carbon dioxide levels, air temperature, heart rate, arterialoxygen saturation, and Borg Ratio Scale value on breathing exertion. Carbon dioxide levels are significantlyhigher and oxygen levels are significantly lower in the respirator when the test hood is used during thequalitative fit test. This was especially true when fit testing filtering facepieces where mean carbon dioxidelevels rose to 4.2% and mean oxygen levels dropped to 15.5%. Full facepiece respirators had similar changes,but to a lesser magnitude. The temperature inside the test hood rose an average 7.5 8F in the course of thequalitative fit test of the N95 filtering facepiece device. These stressors are not present to such an extentduring a quantitative respirator fit test. Professionals conducting respirator fit tests should be aware of thephysiological burdens that may occur during the qualitative respirator fit test. Some groups may be especiallysensitive to this test such as the elderly, pregnant women, persons with pulmonary and/or cardiac disease, orpersons with psychological disorders such as anxiety, panic disorders, or claustrophobia.
By Edward A. Laferty,Roy T. McKay
INTRODUCTION
When conducting required Occupa-tional Safety and Health Administra-tion (OSHA) respirator qualitative fittests (QLFT) with saccharin and Bitrexsolutions,1 workers often comment theair inside the test hood feels hot and
Edward A. Laferty is associated withDepartment of Environmental Health,Occupational Medicine, The Univer-sity of Cincinnati, Cincinnati, OH,USA (2410 A Challenger Loop,Honolulu, HI 96818, USA; Tel.: 808449-7664 (work)/808 371-2571 (cell);fax: 808 449-7658; e-mail: [email protected]).
Roy T. McKay, Ph.D., is associated withDepartment of Environmental Health,Occupational Medicine, The Universityof Cincinnati, Cincinnati, OH, USA.
22 � Division of Chemical Health and Safety of the
Elsevier Inc. All rights reserved.
uncomfortable. This leads to the ques-tions: What are the actual environ-mental conditions inside the testhood and what influences them?
OSHA has approved quantitative fittest (QNFT) and QLFT methods for fittesting respirators.1 OSHA permits aQLFT to be used to fit test full facepiecerespirators when worn with a positivepressure device, such as a self-contained breathing apparatus. When-ever this is done, the facepiece istemporarily converted to a negativepressure mode of operation for the pur-poses of conducting the fit test, and thenreturned to its original configuration.DuringQLFT withsaccharinandBitrexsolutions a test hood is positioned overa person’s head and shoulderswhilehe/she wears a respirator.1 The challengeagents are then sprayed into the testhood and the worker subjectively indi-cates whether he/she can detect thechallenge agent. Testing conductedwith other methods such as the ambientaerosol condensation nuclei counter2
American Chemical Society
do not require the wearing of a hoodover the head.1
The OSHA Permissible ExposureLimit (PEL)3 and the American Con-ference of Governmental IndustrialHygienists (ACGIH) Threshold LimitValue (TLV)4 for carbon dioxide(CO2) is 5,000 ppm (0.5%). TheACGIH TLV is recommended to mini-mize the potential for asphyxiation andundue metabolic stress.5 The ACGIHshort term exposure limit (STEL) forCO2 is 30,000 ppm (3.0%),4 based onthe short term high CO2 exposure stu-dies that produced increased pulmon-ary ventilation rates.5 The NationalInstitute of Safety and Health (NIOSH)immediately dangerous to life andhealth (IDLH) value for CO2 is40,000 ppm (4.0%), for up to 30 min-utes for egress.6,7
Typical room air consists of 20.9%oxygen (O2), 79% nitrogen, and 0.1%CO2, water vapor, and other inertgases.8 The concentration of CO2 inalveolar air is 5%.8 CO2 is formed by
1871-5532/$32.00
doi:10.1016/j.jchas.2005.11.015

cellular respiration and is removed bypulmonary ventilation.8 If the concen-tration of the inspired CO2 is increased,it will alter the normal diffusion gradi-ents of the alveolar blood.8 An increasein alveolar CO2 will result in hypercap-nia (elevated levels of CO2 in the bloodresult from inadequate ventilation orfrom mismatches between ventilationand perfusion of the blood) and sys-temic acidosis.8 The effects of inhaledCO2 are several fold.9 First, the stimula-tion of respiration adds to the burden ofthe work of breathing, and coulddecrease the ability to produce physicalwork if the work was performed at closeto the maximum level.9 Second, CO2
directly causes a feeling of discomfortand unease, and may cause sufficientanxiety to affect work performance.9
Third, CO2 has local vasodilator effects,and may affect the ability to work byshunting blood from other workingmuscles.9 Fourth, high inhaled CO2
levels tend to increase the ventilationrate, thus increasing the effect of breath-ing resistance since a greater air volumecreates higher pressure differences.10
CO2 is the principal regulator ofrespiration, acid–base balance, andbehavioral state arousal in humans.11
In normal individuals, hypercapnia ismildly to moderately anxiogenic, butindividuals with panic disorders aresusceptible to more intense anxiety oreven panic attacks.11 This has beendemonstrated fromprolongedexposureto low levels of CO2.
11 Unconscious-ness and death can occur as the con-centration of inhaled CO2 reaches10%.8 Other symptoms reported atexposures of 7.5% CO2 for 15 minuteswere dyspnea, headache, restlessness,visual color distortions, vertigo, sweat-ing, numbness, irritability, and mentaldisorientation.12 Cardiac rhythmchanges were noted when 6% CO2
was administered for 6–8 minutes.11
Exposure to CO2 at 5% for 30 minutescan cause decreased vascular resistanceand increased renal blood flow; withcontinuous exposure to 3% CO2 theonly observed changes are limited torenal and respiratory compensatorymechanisms without any apparentadverse symptoms.11 Acclimatization,or the development of tolerance toCO2 has been demonstrated.11 Dimin-ished respiratory response to a subse-
Journal of Chemical Health & Safety, Septe
quent challenge of 5% CO2 has beendemonstrated after prolonged expo-sures at CO2 concentrations of 1.5–3%.11 The increased ventilatoryresponse produced by chronic CO2
exposures returns to normal after 2–3days of exposure at 1.5–3%.11 The bodycompensates to the exposure byincreasing respiratory efficiency evi-denced by improved O2 intake andCO2 excretion.11
OSHA defines O2 deficiency as anatmosphere that contains less than19.5% O2 by volume and O2 enrichedas any atmosphere that contains morethan 22% O2 by volume.13 A minimumvalue of 19.5% O2 has been widelyaccepted as the criterion for identifyinga space as O2 deficient.14 An O2 level of16% at standard temperature and pres-sure (STP) can result in increased heartrate, increased breathing rate, somedecrease in coordination, increasedbreathing volume, impaired attention,and impaired thought processes.14 Atconcentrations less than 14% at STP,health effects include: abnormal fatigueon exertion, emotional upset, faultycoordination, and impaired judg-ment.14 A 10% O2 content at STPmay cause nausea, vomiting, lethargy,and inability to perform vigorous move-ments, possible unconsciousness, fol-lowed by death.14 At concentrationsless than 4% at STP unconsciousnesswithin 1 or 2 breaths followed by deathmayoccur.14 Thehumanbodyrespondsto the alveolar partial pressure of O2
rather than the percentage of O2 inrespired air.14 Therefore, a substantiallack of agreement exists as to whatactually constitutes an O2 deficientIDLH atmosphere.14
Respiratory inspiratory resistanceinduces hypoventilation with lowerminute volumes and lower O2 con-sumption values at higher resis-tances.15,16 Average O2 consumptionrates and minute ventilation alsodecrease linearly with increased ex-piratory resistances, indicating thatincreases in expiratory resistance resultin a considerable level of hypoventila-tion.17 Hypoventilation while wearingrespirators causes higher amounts ofblood lactate.16 The respirator wearerdecreases O2 consumption relative tothe unmasked person.16 The result isthat body metabolism is more anaero-
mber/October 2006
bic and blood lactate builds up morequickly for the respirator wearer.16 Inorder to supply the O2 requirements ofthebody, ahypoventilating personmustextract more O2 from each breath.16
Respiration rates with the full facepiecerespirator are lower than without.16
Inhalation times are longer due toincreased inhalation resistance.16
Increased inhalation resistance leadsto hypoventilation, which leads tohigher CO2 and lower O2 levels inexhaled air.16 Metabolic processes ofthe respirator wearer do not changewhen a respirator is worn, but therespirator adds a respiratory burdendue largely to increased breathing resis-tance, for which compensatory adjust-ments are not complete.16 Thus,anaerobicmetabolismoccursatahigherrate, andmaximumO2 deficit is reachedsooner with the respirator than with-out.16 It has been shown that exerciseperformance time was decreased due tohypoventilation, or the inability of ven-tilation to keep pace with O2 consump-tion.18 In another study, it was shownthat respirator exhalation resistancesare better tolerated than inhalationresistances for individuals engaged inrelatively hard physical activities.17
O2 consumption and CO2 produc-tion are elevated at rest during preg-nancy.19 Increased O2 utilizationtogether with decreased O2 reservesmake pregnant women particularly sus-ceptible to hypoxia during hypoventila-tion or apnea.20 In some pregnantwomen, a higher sensitivity to CO2
and hypoxia may induce excessive ven-tilation upon metabolic demand, whichwould contribute to dyspnea.21 Dys-pnea is a common and normal physio-logic response during pregnancy,occurring in 60–70% of pregnantwomen.21
MATERIALS AND METHODS
Apparatus
The CO2 and O2 concentrations weremeasured with a Landtec LandfillControl Technologies GEM-500 infra-red gas analyzer. The analyzer wascalibrated according to the manufac-ture’s instructions using Gasco Affili-ates certified gas. The manufacturer’sliterature listed an accuracy of �0.3%
23

for CO2 and �1.0% for O2. Tempera-tures were recorded with a GeneralElectric 5805WS5 wireless digitalindoor/outdoor thermometer with anaccuracy of�1.88 Fahrenheit (F). Heartrate and arterial O2 saturation weremeasured with a Nellcor CorporationN200 Pulse Oximeter and a DS-100ADurasensor. This pulse oximeter has anaccuracy of saturation without motionof (70–100)%� 2% and pulse ratewithout motion of (20–250) bpm � 3bpm. An IBM ThinkPad Pentium lap-top computer with TSI Inc. softwarecontrolled the 8020A TSI Portacountduring QNFT. The TSI model8095 N95Companion was used to conduct aQNFT with the N95 respirator. TheTSI software was also used to measurethe time of the exercises during QLFT.During the QLFT a standard size 3Mhood was used. The TSI Fit Test ProbeKit was also used to connect the N95respirator to the Portacount during theQNFT.
Subject Testing Procedure
Fit tests were conducted with twotypes of respirators, a Scott O-Vistafull facepiece respirator equipped withhigh efficiency filters and an MSA Affi-nity Pro N95 filtering facepiecerespirator. These two styles wereselected since they represent theextremes of negative pressure air pur-ifying respirators. The filtering face-piece respirator was typical, in that itdid not have an exhalation valve. Onthe day of testing, height, weight,demographic data and smoking statuswere collected. Twenty subjects (10male and 10 female) accomplished aseries of four respirator fit tests. Eachtest subject completed four fit tests inthe following order: first a QNFT fol-lowed by a QLFT with the full face-piece, then a QNFT followed by aQLFT with the filtering facepiecerespirator. Fit testing was conductedusing the standard set of exercisesrecommended by OSHA.1 QNFT wasused in this study for two principlereasons. One was to ensure the respira-tors to be worn provided an acceptablelevel of fit to the wearer. Second, themeasured levels of CO2 and O2 duringthe QNFT provided a baseline withwhich to compare the effects of wearingthe hood during subsequent QLFT.
24
Each subject was instructed on theproper procedure for conducting userseal checks. Inall cases, user seal checkswere satisfactory before a fit test wasconducted. The subject removed therespirator for at least 2 minutesbetween each fit test to ensure an accu-mulation of gas was not present for thenext fit test. The gas analyzer was con-nected to the sampling port used for theQNFT when recording gas measure-ments inside the facepiece. In facepiecemeasurements of CO2 and O2 wererecorded 30 seconds after the end ofthe test. The value of 30 seconds waschosen to allow for adequate sampletimeandtoreduceobserver bias.Valuesfor heart rate, arterial O2 saturation,and breathing exertion were recordedbefore and after each fit test. Breathingexertion values were obtained using theBorg Ratio Scale.22 The temperaturesensor was located inside the test hoodon the anterior lower plastic rim was onthe subject’s right side. No challengeagents were used during this mockQLFT procedure to avoid potentialinterference with gas analyzer measure-ments. The sampling hose was insertedinto the test hood and placed next to afilter inlet of the respirator whenobtain-ing inside the hood gas measurement.
Data Analysis
A one-sample t-test was performedwhen comparing CO2 levels in eachrespirator type with the STEL and O2
levels in each respirator type with theO2 deficient level. Hypothesis testingwas performed using the two samplet-test assuming population variancesare equal when comparing gas levelsof each respirator type. A p value<0.05 was considered statistically sig-nificant. A regression analysis was con-ducted on the height, weight, body massindex (BMI), and levels of CO2 and O2.Thecoefficient of determination, r2, wasused to determine if a correlationexisted. The independent variableswere height, weight, and BMI and thedependent variables were CO2 and O2.
RESULTS
All subjects passed medical clearanceand had no facial hair. One subject wasa smoker but had not smoked within
Journal of Chemical Hea
30 minutes of starting the fit tests.Instructions on donning a respiratorwere provided to subjects and all hadworn a respirator prior to fit testing.Subject characteristics were as follows(mean� SD (range)): age, 30 � 6.2years (23–43); height, 67.25 � 3.0inches (62–72); weight, 176� 39.3pounds (126–250); BMI, 27.2 � 5.6(20.3–38.9).
Fit Factors
Nineteen participants had fit factorsexceeding the OSHA minimum of500 for the full facepiece QNFT. Dur-ing the N95 filtering facepiece QNFT,only two subjects did not achieve theOSHA minimum passing score of 100.
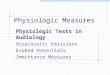
Carbon Dioxide Levels
The mean level of CO2 inside the testhood at the end of the QLFT was 2.2%for the N95 Filtering Facepiece and1.4% for the full facepiece respirator.At the end of the QLFT, the mean CO2
level inside the N95 Filtering Face-piece respirator was 4.2% and for thefull facepiece respirator was 3.2%. Incontrast after the QNFT, the meanCO2 level inside the N95 FilteringFacepiece was 2.8% and full facepiecerespirator was 2.1%. The mean level ofCO2 was higher after the QLFT thanthe QNFT for both types of respirators.Figure 1 illustrates the results of CO2
levels present inside the respirator andtest hood during fit testing. AverageCO2 levels by respirator type and fittest method are shown in Table 1.
A comparison of the mean CO2 levelinside the respirator during fit testingwith the STEL was conducted and theresults are presented in Table 2. A com-parison was conducted on the CO2
levels present in the two types ofrespirators. The mean level of CO2
was significantly higher in the N95 fil-tering facepiece than the full facepiecerespirator after the QNFT, QLFT, andinside the test hood (p < 0.0001). Afterthe QLFT, the CO2 level inside both thefull facepiece and N95 Filtering Face-piece was significantly higher than theSTEL.
Oxygen Levels
The mean level of O2 inside the testhood at the end of the QLFT was18.0% for the N95 Filtering Facepiece
lth & Safety, September/October 2006

Figure 1. Percent CO2 Levels Measured Inside the Respirator and Test Hood. Theboxplot shows the following: horizontal lines from the bottom, 10th, 25th, 50th,75th, 90th percentiles; * – shows the range of data.
Table 3. Mean and Standard Deviationof O2 Levels Inside the Respirator andTest Hood
Mean(%)
SD(%)
Full FacepieceQNFT 18.3 0.5QLFT 16.7 0.6
N95 Filtering FacepieceQNFT 17.1 0.5QLFT 15.5 0.6
Inside Test Hood, Outside RespiratorAfter QLFTFull Facepiece 19.0 0.5N95 Filtering
Facepiece18.0 0.8
Table 1. Mean and Standard Deviationof CO2 Levels Inside the Respirator andTest Hood
Mean(%)
SD(%)
Full FacepieceQNFT 2.1 0.4QLFT 3.2 0.4
N95 Filtering FacepieceQNFT 2.8 0.5QLFT 4.2 0.4
Inside Test Hood, Outside RespiratorAfter QLFTFull Facepiece 1.4 0.4N95 Filtering
Facepiece2.2 0.7
and 19.0% for the full facepiecerespirator. At the end of the QLFT,the mean O2 level inside the N95 Fil-tering Facepiece was 15.5% and insidethe full facepiece respirator was 16.7%.In contrast after the QNFT, the mean
Table 2. Comparison of Mean CO2 Level aQLFT
Journal of Chemical Health & Safety, Septe
O2 level inside the N95 Filtering Face-piece was 17.7% and for the full face-piece respirator was 18.3%. The meanlevel of O2 was lower after the QLFTthan theQNFTforboth typesof respira-tors. Figure 2 illustrates the results of O2
levels present inside the respirator andtest hood during fit testing. Average O2
levels by respirator type and fit test areshown in Table 3.
The mean level of O2 inside therespirator after each of the four fit testsand the level in the test hood was sig-nificantly lower than the level consid-eredO2 deficient of19.5%(p < 0.0001).
A comparison was made of the O2
levels present in the two types ofrespirators. The mean level of O2 wassignificantly lower in the N95 filteringfacepiece than the full facepiecerespirator in the QNFT, QLFT, andinside the test hood (p < 0.0001).
A regression analysis was conductedfor CO2 and O2 levels on the height,weight, and BMI of subjects. The lar-gest coefficient of determination, r2
nd the STEL (3.0%) During QNFT and
mber/October 2006
was 0.17. This indicates less than17% of the total variation in the datapoints can be explained by the regres-sion equation. Consequently, the lin-ear relationship with height, weight,and BMI to gas levels in our studypopulation was weakly related.
Test Hood Temperature
The mean increase of temperatureinside the test hood during qualitativefit testing was 5.3 8F for the full face-piece respirator and 7.5 8F for the N95filtering facepiece respirator (Table 4).The mean temperature increase insidethe test hood with the filtering facepiecewas significantly higher than the fullfacepiece respirator (p < 0.0007). Tem-perature characteristics were as follows(mean� SD (range)): pre-test roomtemperature, 66.4 8F � 1.4 8F (64.4–68.9 8F); inside the test hood afterthe full facepiece respirator QLFT,71.8 8F � 2.7 8F (67.5–77.4 8F); insidethe test hood after the N95 respiratorQLFT, 74.0 8F � 2.8 8F (69.3–80.6 8F).
Table 4. Temperature Increase Meanand Standard Deviation Levels Insidethe Test Hood
MeanTemperatureIncrease (8F)
SD(8F)
QLFT FullFacepiece
5.3 1.6
QLFT N95FilteringFacepiece
7.5 2.1
25

Figure 2. Percent O2 Levels Measured Inside the Respirator and Test Hood. Theboxplot shows the following: horizontal lines from bottom, 10th, 25th, 50th, 75th,90th percentiles; * – shows the range of data.
Borg Ratio Scale, Heart Rate Data, andO2 Saturation
The overall mean change in Borg RatioScale, heart rate, and arterial O2
saturation was less than 1% through-out testing and not statistically differ-ent than pre-test conditions.
DISCUSSION
This study found significantly elevatedlevels of CO2 and significantly loweredlevels of O2 inside two types of respira-tors when subjects wore a test hood toperform QLFTs. These results are con-sistent with those reported by NIOSHwith nonhuman subjects. The NIOSHstudies used a breathing machine withrespirators of similar styles to thosereported here.23 NIOSH reported thatthe N95 filtering facepiece respiratorshad the highest inhaled CO2 concen-trations (3.6%) and the lowest meaninhaled O2 concentration (16.8%).23
The NIOSH study concluded thathigher levels of CO2 and lower levelsof O2 were present inside the respiratorin conjunction with lower ventilationrates.23 We found very similar findings,but of greater magnitude when humansubjects wear a test hood during QLFT.
Wearing respiratory protectioninside a test hood significantly elevatedthe levels of inhaled CO2. The level ofinhaled CO2 was found to differ withrespirator style (full versus filteringfacepiece). For example, the levels ofCO2 in the full facepiece respirator sig-
26
nificantly exceeded the STEL duringQLFT (p < 0.01), such as would occurwith Bitrex or sweetener. Results whilewearing a filtering facepiece were evenmore dramatic. The mean level of CO2
inside the N95 filtering facepiece respi-rator measured during QLFT was 4.2%.As expected, CO2 levels inside bothfacepieces were lower when the testhood was not worn. Thus, the combina-tion of the test hood and the respiratorincreased CO2 levels. This finding isconsistent with the expectation thatplacing an unventilated enclosure overthe head, even for short periods of timeelevates the level of CO2 and reducesthe level of available O2.
The literature reports cardiac eventsoccur at exposure levels of 6% CO2 for6–8 minutes.12 Signs of intoxicationwere produced by a 30 minute expo-sure at 5%.5 CO2 is weakly narcotic at3%, giving rise to reduced acuity ofhearing and increasing blood pressureand pulse. Takahashi et al.10 reportedthat increased levels of inhaled CO2
significantly affected ventilation rate,end-tidal O2 and CO2 concentrations,and breathing pressures. The increasein end-tidal CO2 concentration wascaused by the increase in inhaledCO2, and the increases in end-tidalO2 concentration and pressure levelwere induced by the increased ventila-tion rate which was accelerated by theincrease in CO2.10 Breathing resis-tance tended to decrease breathing fre-quency and volume, and to increasepressure.10 The resistance decreased
Journal of Chemical Hea
end-tidal O2 concentrations andincreased end-tidal CO2 signifi-cantly.10 Kaye et al.11 demonstratedthat acute exposure to CO2, tradition-ally used in psychiatry to stimulateanxiety, can produce mood disordersand the increased frequency of cardi-ovascular complications associatedwith chronic stress. The principal psy-chological changes seen by Kayeet al.11 were a dose-dependent increasein subjective feelings of anxiety,breathlessness, and a few specificsomatic symptoms of fear (i.e., diffi-culty concentrating, dizziness/light-headedness, blurred or narrowedvision and feeling hot or flushed). Ananxious individual’s condition may beaggravated by respirator wear alone.The anxiety may be further exacer-bated by the higher levels of CO2 insidethe test hood during QLFT. To ourknowledge, no published studies haveevaluated health symptoms from ele-vated CO2 exposure inside the testhood during QLFT. Measured valuesof CO2 during this study reached amaximum of 4.8%. This level may besufficient to induce health symptomsamong susceptible individuals whenconducting QFLTs.
Our results are not inconsistent withthe hypothesis that inhaled O2 levels ineither style respirator are considered tobe O2 deficient (<19.5%). Even moresignificant changes are observed whenwearing a test hood. The mean O2 levelof the N95 filtering facepiece respira-tor was 17.1% but decreased to 15.5%when worn inside the test hood. Atlowered O2 levels potential adversehealth effects include increased heartrate, some decrease in coordination,increased breathing volume, andimpaired thought processes.14
There is little information regardingthe safe use of a respirator during preg-nancy and no guidance regardingsafety while being placed inside thetest hood during QLFT. In the absenceof a respirator, CO2 production is sig-nificantly higher in pregnant womenthan it is in nonpregnant woman atrest.19 Given the elevated levels ofCO2 inside the test hood (and lowlevels of O2), persons who conductQLFTs may need to be aware of poten-tial signs of dyspnea (shortness ofbreath on exertion) and/or signs of
lth & Safety, September/October 2006

hypoxia (a state of O2 deficiency in thebody which is sufficient to cause animpairment of function). Testing per-sonnel may need to be adequatelytrained on monitoring for these signs.Alternatively, QNFT may be the pre-ferred method to fit test pregnantwomen to avoid potential health risks.
Although a mean temperatureincrease of 7 8F was observed duringthe QLFT with the test hood, our sub-jects did not complain of high tempera-tures. This may have been due to therelatively cool temperature of our test-ing room. The temperature increaseinside the test hood might have beengreater if the mean room temperaturewas higher. This temperature rise mayhave more of an impact on the heatstress of an individual if starting from ahigher ambient temperature that maybe present in some workplaces.
A worker may not necessarily sense adifference in breathing exertion whilewearing a respirator. In this study therewas less than a 1% change in mean BorgRatio Scale values. This is in agreementwith other studies where, subjective rat-ing of perceived exertion (RPE) scoresremained unchanged with theincreased breathing load imposed bythe different breathing resistances, indi-cating that subjects perceived that he/she exerted the same level of effort forall test conditions.15,17,18 Even with theincreased burden of breathing higherCO2 and lowered O2 inside the testhood, the subject may not be able toperceive the actual increase in breath-ing exertion brought on by the testhood. Testing monitors may not be ableto depend on feedback from the subjecton the extent of their increased breath-ing difficulty.
Significantly higher levels of CO2
were found in the N95 filtering face-piece when compared to the full face-piece respirator in this study. At firstthis finding was unexpected. However,a review of the literature reveals thatthis is consistent with the physiologicburden of these two respirators. Whilethe N95 filtering facepiece used in thisstudy has a smaller dead space than thefull facepiece respirator, it also has asmaller filter surface area, less filteringmaterial, and no exhalation or inhala-tion valves. Thus, the N95 filteringfacepiece has a higher breathing resis-
Journal of Chemical Health & Safety, Septe
tance compared to the full facepiecerespirator. This was true, even thoughthe full facepiece respirator wasequipped with a higher efficiency filter.CO2 concentrations present in the testhood during QLFT were significantlyhigher for the N95 filtering facepiecethan the full facepiece (p < 0.0001).This is consistent with results foundin the literature.9,15,16,23 Johnsonet al.9 concluded that the physiologicaleffects of resistance on breathing aremuch more pronounced than thosedue to dead space volume. The NIOSHstudy described earlier also confirmshigher CO2 levels with N95 filteringfacepiece respirators, when comparedto the full facepiece. These findingsmay have important implications forthe development of NIOSH certifica-tion standards for CO2 concentrationswithin air purifying respirators.23
The mean heart rate and O2 satura-tion changed less than 1% during test-ing. This is also in agreement with theliterature.17,24 The percentage of arter-ial O2 saturation is not a very sensitivetest when monitoring partial pressureofO2 in the blood system. A more precisemeasurement would have been to inva-sively measure the blood gas levels.
This study utilized high efficiency fil-ters with the full facepiece respirator. Iflower resistance N95 filters had beenused, even larger differences in CO2 andO2 levels may have been demonstratedbetween the full facepiece respiratorand the N95 filtering facepiece.
Another observation that came tolight during testing was the fact thatsubjects could not move their headfully in the OSHA specified test hoodwhile wearing the full facepiecerespirator used in this study. The fullrange of motion necessary to carry outfit test exercises could not be achieved.We suspect this could be a limitationwith other make and/or models of fullfacepiece respirators.
CONCLUSION
When wearing a test hood to conductQLFT, significantly elevated levels ofCO2 occur inside the respirator. Thesechanges were greater for a filtering face-piece respirator than an elastomeric fullfacepiece. Likewise, O2 levels dropped
mber/October 2006
significantly inside the respirator. Therise in CO2 and/or the fall in O2, may beresponsible for many of the subjectivecomplaints that have been heard duringthis type of testing. Professionals con-ducting respirator fit tests should beaware of the physiological burdensbrought on by these tests. There maybe special groups especially sensitive tothe QLFT such as the elderly, pregnantwomen, persons with pulmonary and/or cardiac disease, or persons with psy-chological disorders such as anxiety,panic disorders, or claustrophobia.
ACKNOWLEDGMENTSThis research was supported (in part)by a grant from the University of Cin-cinnati through its Education andResearch Center, supported by Train-ing Grant No. T42/CCT510420 fromthe Centers for Disease Control andPrevention/National Institute forOccupational Safety and Health. Thecontents are solely the responsibility ofthe authors and do not necessarilyrepresent the official views of theNational Institute for OccupationalSafety and Health. The authorsappreciate the help of Dr. Carol Riceand Dr. Rakesh Shukla for their gui-dance and expertise.
REFERENCES1. Respiratory Protection, CFR, Title 29,
Part 1910.134, 1998.2. TSI, Inc. Portacount Plus Model 8020,
Operation and Service Manual, TSI,Inc., Shoreview, MN, 2003.
3. Air Contaminants, CFR, Title 29, Part1910.1000, 2002.
4. ACGIH. Threshold Limit Values forChemical Substances and PhysicalAgents and Biological Exposure In-dices. Cincinnati, OH: ACGIH, 2005.
5. ACGIH. Documentation of the TLV –Carbon Dioxide, 7th ed.; Cincinnati,OH: ACGIH, 2001.
6. NIOSH. Documentation for Immedi-ately Dangerous to Life and HealthConcentrations (Pub. No. PB-94-195047); Cincinnati, OH: NIOSHDHHS (NTIS), 1994.
7. NIOSH. NIOSH Pocket Guide to Che-mical Hazards (Pub. No. 2002-140).Cincinnati, OH: NIOSH (DHHS),2002.
8. Gill, J. R.; Ely, S. F.; Hau, Z. Environ-mental gas displacement three acciden-tal deaths in the workplace. Am. J.
27

Forensic Med. Pathol. 2002, 23(1), 26–30.
9. Johnson, A. T.; Scott, W. H.; Lausted,C. G. Effect of external dead volume onperformance while wearing a respira-tor. Am. Ind. Hyg. Assoc. J. 2000, 61,678–684.
10. Takahashi, M.; Mano, Y.; Shibayama,M.; Yamami, N. Effects of breathingresistance while inhaling 3% carbondioxide during steady state exercise. J.Occup. Health, 1998, 40, 213–217.
11. Kaye, J.; Buchanan, F.; Kendrick, A.Acute carbon dioxide exposure inhealthy adults: evaluation of a novelmeans of investigating the stress re-sponse. J. Neuroendocrinol. 2004, 16,256–264.
12. NIOSH. Criteria for a RecommendedStandard Occupational Exposure toCarbon Dioxide (Pub. No. 76-194).Cincinnati, OH: NIOSH (DHHS),1976.
13. Permit-required Confined Spaces, CFR,Title 29, Part 1910.146, 2002.
14. DiNardi, S. R. The Occupational En-vironment: Its Evaluation, Control,and Management; AIHA Press; Fair-fax, VA, 2003, pp. 1092.
28
15. Johnson, A. T.; Scott, W. H.; Lausted,C. G. Effect of respirator inspiratoryresistance level on constant load tread-mill work performance. Am. Ind. Hyg.Assoc. J. 1999, 60, 474–479.
16. Johnson, A. T.; Dooly, C. R.; Dotson, C.O. Respirator mask effects on exercisemetabolic measure. Am. Ind. Hyg.Assoc. J. 1995, 56, 467–473.
17. Caretti, D. M.; Scott, W. H.; Johnson,A. T. Work performance when breath-ing through different respirator exhala-tion resistances. Am. Ind. Hyg. Assoc.J. 2001, 62, 411–415.
18. Caretti, D. M.; Whitley, J. A. Exerciseperformance during inspiratory resis-tance breathing under exhaustive con-stant load work. Ergonomics, 1998,41(4), 501–511.
19. Jaque-Fortunato, S. V.; Wiswell, R. A.;Khodiguian, N. A comparison of theventilatory responses to exercise inpregnant, postpartum, and nonpreg-nant women. Semin. Perinatol. 1996,20(4), 263–276.
20. Steinbrook, R. Anesthesia, minimallyinvasive surgery and pregnancy. BestPract. Res. Clin. Anesthesiol. 2002,16(1), 131–143.
Journal of Chemical Hea
21. Garcia-Rio, F.; Pino, J. M.; Gomez, L.Regulation of breathing and percep-tion of dyspnea in healthy pregnantwomen. Chest, 1996, 110(2), 446–453.
22. Grant, S.; Aitchison, T.; Henderson,E.; Christie, J.; Zare, S.; McMurray, J.;Dargie, H. A comparison of thereproducibility and sensitivity tochange of Visual Analogue Scales,Borg Scales, and Likert Scales innormal subjects during submaximalexercise. Chest, 1999, 116(5), 1208–1217.
23. Turner, N.; Sinkule, E.; Hota, S. Auto-mated Breathing and MetabolicSimulator (ABMS/2) CO2 Test for Pow-ered and Non-Powered Air-PurifyingRespirators, Supplied-Air Respirators,and Gas Masks. National Institute forOccupational Safety and Health(NIOSH). Presented at the NationalOccupational Research Agenda(NORA), Symposium, Arlington, VA,June 2003.
24. Gunnar, D. O.; Balldin, U. L. Physiolo-gical effects of pressure demand masksduring heavy exercise. Am. Ind. Hyg.Assoc. J. 1984, 45(3), 177–181.
lth & Safety, September/October 2006