Embed Size (px)
Citation preview

INHERITED METABOLIC EPILEPSIES
PHILLIP L PEARL
Second Edition
- -
+ +
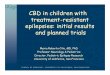
Focal Seizure
Multiple neurons with PDS
E gt I
PDS
R
L
EEG 3 Hz spike-wave
EEG Spike
Intracellular recording 1
2
3
nRT
+
Generalized Seizure
-
+
+
TR
Disrupted thalamocortical
network function
E or I
A B
SPRINGER PUBLISHING
See Code Inside
DIGITALACCESS
INHERITED METABOLIC EPILEPSIES
PHILLIP L PEARL
An Imprint of Springer Publishing
Second Edition
INHERITED METABOLIC EPILEPSIESPhillip L Pearl MD
ldquoThis book fills an important and unique niche in pediatric neurology and will be a frequently referenced textbookfor all clinicians caring for children with epilepsy It is well-organized and readable and provides essentialand up-to-date clinical data on these individually rare but collectively more common disordersrdquo-Elaine Wirrell MD Neurology
ldquoSpecialists in pediatric neurology epilepsy and biochemical genetics will find this volume to be indispensable for their daily practice The organized approach to an incredibly complex set of disorders will also benefit trainees trying to make sense of the complex field and developing their own clinical approach as knowledge about metabolic epilepsies continues to growrdquo-Carl E Stafstrom MD PhD Journal of Pediatric Epilepsy
The continued explosion of information in neurogenetics and metabolism mandates increasing awareness of current diagnostic and therapeutic strategies in disease settings where prompt identification and intervention is crucial for a positive outcome This thoroughly revised and greatly expanded new edition of the first book to bridge clinical epilepsy with inherited metabolic diseases brings together leading authorities to present state-of-the-art clinical reviews covering the science recognition and treatment of the inherited metabolic epilepsies and related disorders
Inherited Metabolic Epilepsies Second Edition contains 15 new chapters and all existing chapters have been updated to reflect the latest science and clinical advances in this fast-moving field New sections on basic and clinical sciencemdashcovering energetics metabolomics pathways the use of novel investigations like transcranial magnetic stimulation neuropathology and genomic technologiesmdashsupplement the disease-focused sections Dedicated chapters focus on recently recognized disorders having novel therapeutic implications pyridoxal-5-phosphate dependency Menkesrsquo disease and thiamine transporter deficiency The book also includes new clinical applications of genomics and advanced generation gene sequencing in the diagnosis of inherited metabolic epilepsies This readable well-illustrated reference concludes with an updated clinical algorithm to aid physicians in screening and identifying suspected metabolic disorders and a collection of resources for families
n Synthesizes cutting-edge diagnostic clinical and scientific information on epilepsy and inborn errors of metabolism
n Completely updated and expanded second edition contains the latest knowledge and 15 entirely new chapters
n Authored and edited by international experts in neurology metabolic disorders and genetics
n A readable and well-illustrated reference for clinicians
n Essential coverage of the new generation of genetic tests which were not widely available or utilized when the first edition was published
n New chapter on inherited metabolic epilepsies in adults
Features
9 780826 168634
11 W 42nd Street New York NY 10036 wwwspringerpubcom
An Imprint of Springer Publishing
Recommended Shelving CategoryNeurology
Praise for the Previous Edition
Second Edition
INH
ERITED M
ETABOLIC EPILEPSIESPEA
RL
Inherited Metabolic Epilepsies
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Inherited Metabolic Epilepsies
Second Edition
Editor
Phillip L Pearl MDDirector of Epilepsy and Clinical Neurophysiology
William G Lennox Chair Boston Childrenrsquos HospitalProfessor of Neurology
Harvard Medical SchoolBoston Massachusetts
An Imprint of Springer Publishing
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Visit our website at wwwspringerpubcom
ISBN 9780826168634e-book ISBN 9780826168641
Acquisitions Editor Beth BarryCompositor Exeter Premedia Services Private Ltd
Copyright copy 2018 Springer Publishing CompanyDemos Medical Publishing is an imprint of Springer Publishing Company LLC
All rights reserved This book is protected by copyright No part of it may be reproduced stored in a retrieval system or transmitted in any form or by any means electronic mechanical photocopying recording or otherwise without the prior written permission of the publisher
Medicine is an ever-changing science Research and clinical experience are continually expanding our knowledge in particular our understanding of proper treatment and drug therapy The authors editors and publisher have made every effort to ensure that all information in this book is in accordance with the state of knowledge at the time of pro-duction of the book Nevertheless the authors editors and publisher are not responsible for errors or omissions or for any consequences from application of the information in this book and make no warranty expressed or implied with respect to the contents of the publication Every reader should examine carefully the package inserts accompanying each drug and should carefully check whether the dosage schedules mentioned therein or the contraindications stated by the manufacturer differ from the statements made in this book Such examination is particularly important with drugs that are either rarely used or have been newly released on the market
Library of Congress Cataloging-in-Publication Data
Names Pearl Phillip L editorTitle Inherited metabolic epilepsies editor Phillip L PearlDescription Second edition | New York Demos [2018] | Includes bibliographical references and indexIdentifi ers LCCN 2017031804| ISBN 9780826168634 | ISBN 9780826168641 (e-book)Subjects | MESH Epilepsymdashetiology | Brain Diseases Metabolic Inbornmdashcomplications | Epilepsymdashdiagnosis | Brain Diseases Metabolic Inbornmdashdiagnosis | Epilepsymdashtherapy | Brain Diseases Metabolic InbornmdashtherapyClassifi cation LCC RC372 | NLM WL 385 | DDC 616853mdashdc23LC record available at httpslccnlocgov2017031804
Contact us to receive discount rates on bulk purchases We can also customize our books to meet your needs
For more information please contact salesspringerpubcom
Printed in the United States of America by Sheridan Books Inc17 18 19 20 21 5 4 3 2 1
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This book is dedicated to my wife Maria Tartaglia Pearl MD whose sacrifi ces for my work are fortunately outmatched
by our mutual love for medicine
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Contents
Contributors xiPreface xvii
Acknowledgments xix
PART I GENERAL PRINCIPLES 1 Recognition Scope and Implications of Inherited Metabolic Epilepsies 2
Phillip L Pearl
2 Overview of Inherited Metabolic Disease 16Lance H Rodan and Gerard T Berry
3 Treatable Inherited Metabolic Epilepsies Diagnoses Not to Miss 40Phillip L Pearl and Mohammed Almuqbil
PART II BASIC SCIENCE IN METABOLIC EPILEPSIES 4 Metabolic Epilepsies Principles and Mechanisms 56
Carl E Stafstrom and Jong M Rho
5 Metabolic Energetics in Epilepsy 74Ashwini Sri Hari and Manisha Patel
6 Pathways Dysregulation of mTOR and Epilepsy 86Darius Ebrahimi-Fakhari Jonathan Lipton and Mustafa Sahin
7 Protein Anchoring as an Important Mechanism in Early Onset Epilepsy Glycosylphosphatidylinositol (GPI) Defi ciency Syndromes 98Gali Heimer Bruria Ben-Zeev and Yair Anikster
PART III CLINICAL SCIENCE IN METABOLIC EPILEPSIES 8 Neuroimaging in the Metabolic Epilepsies 110
Robert A Zimmerman and Zarir P Khademian
9 Advances in MR Spectroscopy for Inherited Epilepsies 125Andrew Breeden Morgan J Prust Stanley T Fricke Matthew Whitehead and Andrea L Gropman
10 Neuropathology of Metabolic Epilepsies Novel Aspects in Children and the Diagnostic Role of Skin Biopsy 135Harvey B Sarnat
11 Electroencephalography in the Metabolic Epilepsies 149Samata Singhi Mona Alduligan and Phillip L Pearl
Share Inherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
viii
12 Genomic Technologies in Clinical Practice 187Christina Y Hung and Olaf A Bodamer
13 Measures of Cortical Excitability by Transcranial Magnetic Stimulation 201Alexander Rotenberg
14 Ketogenic Diet in Metabolic Epilepsies 207Susan L Fong and Eric H Kossoff
PART IV SMALL MOLECULE DISEASES 15 Amino and Organic Acid Disorders and Epilepsy 218
Kimberly A Chapman and Jamie L Fraser
16 Fatty Acid Oxidation Disorders and Epilepsy 237Dimitar Gavrilov and Dietrich Matern
17 Urea Cycle Disorders and Epilepsy 257Debra S Regier Brendan Lanpher and Marshall L Summar
18 Mitochondrial Diseases and Epilepsy 267Sumit Parikh Lynne A Wolfe and Andrea L Gropman
19 Pyridoxine-Dependent Epilepsy 275Sidney M Gospe Jr
20 Pyridoxamine 5acute-Phosphate Oxidase (PNPO) Defi ciency 287Barbara Plecko-Startinig
21 Tetrahydrobiopterin Defi ciencies and Epilepsy 293Nenad Blau and Thomas Opladen
22 Disorders of GABA Metabolism and Epilepsy 301Phillip L Pearl Kara Vogel and K Michael Gibson
23 Glucose Transporter Type 1 Defi ciency Syndrome 313Cigdem I Akman and Darryl C De Vivo
24 Thiamine Transporter Defi ciency and Epilepsy 326Brahim Tabarki
25 DEND Syndrome Developmental Delay Epilepsy and Neonatal Diabetes a Potassium Channelopathy 333Carolina Lahmann and Frances Ashcroft
26 HyperammonemiaHyperinsulinism Syndrome and Epilepsy 345Nicholas S Abend and Andrea Kelly
27 Glycine Encephalopathy and Epilepsy 353Julia B Hennermann Johan L K Van Hove and Curtis R Coughlin II
28 Serine Synthesis Disorders and Epilepsy 364T J de Koning
29 LeschndashNyhan Disease and Epilepsy 371Beth A Leeman-Markowski and Hyder A Jinnah
30 Sulfi te Oxidase Defi ciencyMolybdenum Cofactor Defi ciency and Epilepsy 394Joumlrn Oliver Sass and Barbara Plecko-Startinig
31 Creatine Disorders and Epilepsy 401Ton de Grauw
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
32 Cerebral Folate Defi ciency and Epilepsy 407Robert Steinfeld
33 Menkesrsquo Disease and Infantile Epilepsy 415Asuri N Prasad
PART V LARGE MOLECULE DISEASES 34 Congenital Disorders of Glycosylation and Epilepsy 428
Susan E Sparks
35 Lysosomal Storage Diseases and Epilepsy 445Pranoot Tanpaiboon and Grisel Lopez
36 Peroxisomal Diseases and Epilepsy 473Parastoo Jangouk Kristin W Barantildeano and Gerald V Raymond
37 Leukodystrophies and Epilepsy 483Davide Tonduti and Adeline Vanderver
PART VI CONCLUSIONS 38 Diagnostic Approaches to Genetic Epilepsies 490
Erika Takle Axeen Christelle El Achkar and Annapurna Poduri
39 Therapeutic Approaches to Inherited Metabolic Epilepsies 497Brandy Verhalen and Berge A Minassian
40 Inherited Metabolic Epilepsies in Adults 503Phillip L Pearl
41 Genetic Counseling in Metabolic Epilepsies 508Jodie M Vento
42 Support and Resources for Patients and Families With Inherited Metabolic Epilepsies 518Christopher Ryan and Jennifer Jeffs
43 Clinical Approach to Inherited Metabolic Epilepsies 525Scott Demarest Anna Lecticia Pinto and Phillip L Pearl
Index 529
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Contributors
Nicholas S Abend MD MSCEAssociate Professor of Neurology and PediatricsDepartments of Neurology and PediatricsChildrenrsquos Hospital of Philadelphia and the University
of PennsylvaniaPhiladelphia Pennsylvania
Christelle El Achkar MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Cigdem I Akman MDAssociate Professor of Clinical Neurology and PediatricsDepartments of Neurology and PediatricsDivision of Pediatric NeurologyInterim ChiefChild NeurologyDirectorPediatric EpilepsyColumbia University College of Physicians and SurgeonsNew York New York
Mona Alduligan MDPhysicianDivision of Clinical NeurophysiologyChildrenrsquos National Medical CenterWashington DC
Mohammed Almuqbil MD FRCP (C)King Abdullah Specialist Childrenrsquos Hospital (KASCH)King Saud bin Abdulaziz University for Health Sciences
(KSAU-HS)Pediatric Neurology DivisionRiyadh Saudi ArabiaKing Abdullah International Medical Research Center
(KAIMRC)National Guard MinistryRiyadh Saudi ArabiaDivision of Genetics and GenomicsBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Yair Anikster MD PhDDirectorMetabolic Disease UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
Frances Ashcroft PhD ScDGlaxoSmithKline Royal Society Research ProfessorDepartment of Physiology Anatomy and GeneticsFellow of Trinity CollegeDirector OXIONUniversity of OxfordOxford England
Erika Takle Axeen MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Minnesota
Kristin W Barantildeano MD PhDClinical AssociatePediatric NeurologyDepartment of NeurologyJohns Hopkins HospitalAssistant Professor of NeurologyJohns Hopkins School of MedicineBaltimore Maryland
Bruria Ben-Zeev MDDirectorPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xii
Gerard T Berry MDDirector Metabolism ProgramProfessor of PediatricsBoston Childrenrsquos HospitalBoston Massachusetts
Nenad Blau PhDSenior Consultant in Biochemical GeneticsProfessor Emeritus of Clinical Biochemistry (UZH)Dietmar-Hopp Metabolic CenterUniversity Childrenrsquos HospitalHeidelberg Germany
Olaf A Bodamer MD PhDAssociate Chief of Genetics and GenomicsBoston Childrenrsquos HospitalPark Gerald Chair in Genetics and GenomicsHarvard Medical SchoolBoston Massachusetts
Andrew Breeden PhDProgram AnalystHealth Program SpecialistNational Institute of Neurological Disorders and
Stroke (NINDS)Bethesda Maryland
Kimberly A Chapman MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National
Health SystemWashington DC
Curtis R Coughlin II MS MBe CGCAssistant Professor of PediatricsSection of Clinical Genetics and MetabolismDepartment of PediatricsUniversity of ColoradoAurora Colorado
Ton de Grauw MD PhDChiefNeurosciencesChildrenrsquos Healthcare of AtlantaDirectorPediatric NeurologyEmory University School of MedicineAtlanta Georgia
T J de Koning MD PhDPaediatrician for Inborn Errors of MetabolismDepartment of Genetics and PaediatricsUniversity Medical Centre GroningenUniversity of GroningenGroningen The Netherlands
Darryl C De Vivo MDSidney Carter Professor of NeurologyProfessor of PediatricsPediatric Neurology ServiceFounding DirectorColleen Giblin Research Laboratories for Pediatric
NeurologyAssociate ChairmanPediatric Neurosciences and Developmental
NeurobiologyCo-DirectorMotor Neuron CenterDirectorSpinal Muscular Atrophy (SMA) CenterChief EmeritusPediatric NeurologyColumbia University Medical CenterNew York New York
Scott Demarest MDAssistant Professor of Pediatrics and NeurologyChildrenrsquos Hospital ColoradoUniversity of ColoradoAurora Colorado
Darius Ebrahimi-Fakhari MD DrmedResident PhysicianDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Susan L Fong MD PhDAssistant ResidentPediatric NeurologyJohns Hopkins HospitalBaltimore Maryland
Jamie L Fraser MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National Health
SystemWashington DC
Stanley T Fricke PhDPhysicistChildrenrsquos National Medical CenterWashington DC
Dimitar Gavrilov MD PhDAssistant ProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
K Michael Gibson PhDAllen I White Distinguished Professor and ChairDepartment of PharmacotherapyWashington State University College of PharmacySpokane Washington
Sidney M Gospe Jr MD PhDHerman and Faye Sarkowsky Endowed ChairProfessor and HeadDivision of Pediatric NeurologyDepartments of Neurology and PediatricsUniversity of WashingtonDivision of NeurologySeattle Childrenrsquos Hospital and Seattle Childrenrsquos
Research InstituteSeattle Washington
Andrea L Gropman MDChief Neurogenetics and Neurodevelopmental
PediatricsChildrenrsquos National Medical CenterAssociate Professor of Neurology and PediatricsGeorge Washington School of Medicine and Health
SciencesWashington DC
Ashwini Sri Hari PhD CandidateDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Gali Heimer MD PhDSenior Physician and Director of the Angelman ClinicPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical Center Tel-Hashomer Israel Sackler Faculty of MedicineTel-Aviv UniversityTel-Aviv IsraelMember of the Dr Pinchas Borenstein Talpiot Medical
Leadership ProgramSheba Medical CenterTel-Hashomer Israel
Julia B Hennermann MDProfessor of Metabolic DiseasesUniversity Medical Center MainzVilla Metabolica Department of Pediatric and
Adolescent MedicineMainz Germany
Christina Y Hung MDResearch AssociateHMS Instructor in PediatricsDivision for Human Genetics and GenomicsBoston Childrenrsquos HospitalBoston Massachusetts
Parastoo Jangouk MDGastroenterology and Hepatology FellowYale-New Haven HospitalNew Haven Connecticut
Jennifer Jeffs LICSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Hyder A Jinnah MD PhDProfessorDepartments of Neurology Human Genetics and
PediatricsEmory University School of MedicineAtlanta Georgia
Andrea Kelly MD MSCEAssociate Professor of Pediatrics CEDepartment of PediatricsChildrenrsquos Hospital of Philadelphia and Perelman School
of Medicine of the University of PennsylvaniaPhiladelphia Pennsylvania
Zarir P Khademian MD PhDAssistant Professor of Radiology and PediatricsStaff Neurologist Division of Diagnostic Imaging and
RadiologyChildrenrsquos National Medical CenterWashington DC
Eric H Kossoff MDProfessorNeurology and PediatricsJohns Hopkins HospitalBaltimore Maryland
Carolina Lahmann PhDPostdoctoral FellowHarvard Medical SchoolBoston Massachusetts
Brendan Lanpher MDAssistant Professor of Medical GeneticsDepartment of Clinical GenomicsMayo ClinicRochester Minnesota
Beth A Leeman-Markowski MD MA MMScAssistant ProfessorDepartment of NeurologyNew York UniversityInvestigatorResearch ServiceVA New York Harbor Healthcare SystemmdashManhattan
CampusNew York New York
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xiv
Jonathan Lipton MD PhDAssistant Professor of NeurologyDepartment of Neurology and F M Kirby Center for
NeuroscienceBoston Childrenrsquos Hospital Harvard Medical SchoolBoston Massachusetts
Grisel Lopez MDSenior Staff ClinicianNational Human Genome Research InstituteNational Institutes of HealthBethesda Maryland
Dietrich Matern MD PhDProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
Berge A Minassian MDDivision ChiefPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas TexasUniversity of TorontoToronto Ontario Canada
Thomas Opladen MDDivision of Child Neurology and Metabolic DiseasesUniversity Childrenlsquos Hospital Heidelberg Germany
Sumit Parikh MDDirector of Cleveland Clinic Neurogenetics Metabolic
amp Mitochondrial Disease ProgramCleveland ClinicAssociate ProfessorDepartment of PediatricsCase Western Reserve University School of MedicineCleveland Ohio
Manisha Patel PhDProfessorDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Phillip L Pearl MDDirector of Epilepsy and Clinical NeurophysiologyWilliam G Lennox ChairBoston Childrenrsquos HospitalProfessor of NeurologyHarvard Medical SchoolBoston Massachusetts
Anna Lecticia Pinto MDAssistant in Neurology and Co-DirectorSturge Weber Clinic Boston Childrenrsquos HospitalLecturer of NeurologyHarvard Medical SchoolBoston Massachusetts
Barbara Plecko-Startinig MDHeadDivision of Child NeurologyChildrenrsquos Hospital ZurichProfessor of Child NeurologyUniversity of ZurichZurich Switzerland
Annapurna Poduri MD MPHEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Asuri N Prasad MBBS MD FRCPC FRCPEProfessor in Pediatrics and Clinical NeurosciencesDivision of Pediatric NeurologyDepartment of PediatricsSchulich School of Medicine and DentistryChildrenrsquos Hospital London Health Sciences CentreWestern UniversityLondon Ontario Canada
Morgan J Prust MDClinical Fellow in NeurologyDepartment of NeurologyMassachusetts General HospitalBrigham amp Womenrsquos HospitalBoston Massachusetts
Gerald V Raymond MDProfessorDepartment of NeurologyUniversity of Minnesota Medical SchoolMinneapolis Minnesota
Debra S Regier MD PhDDirector of Genetic and Genomic Education Medical
GeneticistRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Jong M Rho MDProfessor of Pediatrics Clinical Neurosciences
Physiology and PharmacologyDr Robert Haslam Chair in Child NeurologySection of Paediatric NeurologyCumming School of Medicine University of CalgaryAlberta Childrenrsquos HospitalCalgary Alberta Canada
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Lance H Rodan MDStaff PhysicianBoston Childrenrsquos HospitalBoston Massachusetts
Alexander Rotenberg MD PhDDirector Neuromodulation ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalAssociate Professor of NeurologyHarvard Medical SchoolBoston Massachusetts
Christopher Ryan LCSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Mustafa Sahin MD PhDProfessor of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Harvey B Sarnat MS MD FRCPCProfessor Departments of Paediatrics Pathology
(Neuropathology) and Clinical NeurosciencesUniversity of Calgary Cumming School of Medicine
and Alberta Childrenrsquos Hospital Research InstituteCalgary Alberta Canada
Joumlrn Oliver Sass Dr rer natProfessor of Bioanalytics and BiochemistryDepartment of Natural SciencesBonn-Rhein-Sieg University of Applied SciencesSankt Augustin Germany
Samata Singhi MDClinical Fellow in NeurologyDepartment of NeurologyBoston Childrenrsquos HospitalBoston Massachusetts
Susan E Sparks MD PhDMedical DirectorNA Medical AffairsRare DiseasesSanofi GenzymeCambridge Massachusetts
Carl E Stafstrom MD PhDProfessor of Neurology and PediatricsLederer Chair in Pediatric EpilepsyDirector Division of Pediatric NeurologyJohns Hopkins University School of MedicineBaltimore Maryland
Robert Steinfeld MD PhDProfessor of Neurometabolic and Neurodegenerative
Diseases in Childhood and AdolescenceDepartment of Pediatrics and Pediatric NeurologyUniversity Medical Center GoumlttingenGoumlttingen Germany
Marshall L Summar MDChief Division of Genetics and MetabolismMargaret OrsquoMalley Chair of Genetic MedicineRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Brahim Tabarki MDDivision of Pediatric NeurologyPrince Sultan Military Medical CityRiyadh Saudi ArabiaAssociate Professor of Neurology and PediatricsThe Ibn El Jazzar University School of MedicineSousse Tunisia
Pranoot Tanpaiboon MDAssociate Professor of PediatricsDivision of Genetics and MetabolismThe George Washington University School of Medicine
and Health SciencesChildrenrsquos National Health System Childrenrsquos National
Rare Disease InstituteWashington DC
Davide Tonduti MDChild NeurologistDepartment of Child NeurologyFondazione IRCCS Istituto Neurologico Carlo BestaMilano Italy
Johan L K Van Hove MD PhDProfessor of PediatricsSection of Clinical Genetics and Metabolism
Department of PediatricsUniversity of ColoradoAurora Colorado
Adeline Vanderver MDAttending PhysicianDivision of NeurologyProgram DirectorLeukodystrophy CenterJacob A Kamens Endowed Chair in Neurologic
Disorders and Translational NeurotherapeuticsChildrenrsquos Hospital of PhiladelphiaAssociate Professor of NeurologyPerelman School of Medicine at the University of
PennsylvaniaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xvi
Jodie M Vento MGC LCGCManagerCenter for Rare Disease TherapyManagerBrain Care InstituteManagerLaboratory Genetic Counseling ServicesChildrenrsquos Hospital of Pittsburgh of UPMCPittsburgh Pennsylvania
Brandy Verhalen PhDLab ManagerPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas Texas
Kara Vogel PhDPostdoctoral Research AssociateUniversity of WisconsinndashMadisonMadison Wisconsin
Matthew Whitehead MDRadiologistChildrenrsquos National Medical CenterWashington DC
Lynne A Wolfe MS CRNPSenior Nurse PractitionerUndiagnosed Disorders ProgramNational Human Genome Research Institute National
Institutes of HealthBethesda Maryland
Robert A Zimmerman MDProfessor of RadiologyRaymond and Ruth Perelman School of Medicine at the
University of PennsylvaniaChiefDivision of Neuroradiology and MRIThe Childrenrsquos Hospital of PhiladelphiaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Preface
This edition of Inherited Metabolic Epilepsies is a greatly expanded and updated version of the fi rst Following a rousing response to the fi rst edition far beyond any anticipated measure it was clear that a reexamination of the material taking into account many helpful sug-gestions that I received from readers far and wide was in order Despite my own misgivings that books are no longer fashionable and are largely replaced by journals and online sources that lend themselves to periodic if not continual updating there remains an appetite and clamor for books that accomplish what I had hoped to do originally and aim to achieve to a greater extent in this edition to encapsulate a burgeoning fi eld suf-fi ciently that a student practitioner or investigator can turn to the source with confi dence that the neces-sary background as well as detail will be available to reward the search for information and also move the fi eld forward
The fi rst edition of this monograph was born follow-ing the organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the annual meeting of the American Epilepsy Society in Boston in 2009 At the time of proposing the topic I was wrestling with a chasmic gap between the fascinat-ing disorders being discussed at the geneticndashmetabolic meetings and the advancing wave in epilepsy classifi ca-tion diagnosis and treatment occupying the meetings attended by members of the societies associated with neurology and epilepsy At that time a storybook series of investigations elucidated not only the surprising antiq-uitin defect in pyridoxine-dependent epilepsy but also the highly charged requirement that physicians consider a pivotal role for folinic acid and pyridoxal-5-phosphate in patients with virtually the same clinical presentation I also perceived a relative lack of awareness of disorders such as glucose transporter 1 defi ciency serine synthetic defects developmental delay epilepsy and neonatal dia-betes (DEND) and hyperinsulinismndashhyperammonemia (HIndashHA) that had very specifi c therapeutic implications with potential for dramatically improving outcome but with an even greater likelihood that they were escaping diagnosis
Overall the inherited metabolic epilepsies repre-sent a group of disorders that is rare individually but
in aggregate represents a substantial clinical burden as well as a vexing area for physicians investigators and students to master The sheer amount and complexity of information are overwhelming and require the physician to synthesize key concepts in neurology genetics and epilepsy As a pediatric epileptologist and medical edu-cator I have found this area among the most challenging and rewarding in practice and research The fi rst edition organized the disorders in a traditional approach under the roof of metabolism by dividing them into small- and large-molecule disorders In the Preface to that edition there was an explanation of various ways of organizing these disorders some more user friendly to the neurol-ogist than the small- versus large-molecule divide but this was an opportunity to present that way of thinking to the neurologist which brings this clinical specialty closer to that of genetics metabolism
In this second edition there is an expansion from four sections (General Principles Small Molecule Diseases Large Molecule Diseases and Conclusions) to six sec-tions with the addition of chapters in basic science and clinical science of the metabolic epilepsies The book has been expanded from 28 to 43 chapters with new chapters including overviews of metabolic disease and the basic science of metabolic epilepsy plus new topics such as metabolic energetics and implications of vital pathways A full chapter is devoted to the mechanistic target of rapamycin (mTOR) pathway that regulates cell replica-tion and so much of homeostasis and new pathophysi-ologic mechanisms such as protein anchoring disorders There are new chapters on neurotransmitter transmission measurement using transcranial magnetic stimulation genomic technologies and approaches to diagnosis and therapy referable to this group of disorders The clinical science section now includes a marvelous and refl ective chapter on neuropathology by Harvey B Sarnat There are new chapters devoted to specifi c disorders such as pyridoxal-5-phosphate dependency and Menkesrsquo disease There are chapters with completely new vantage points from community and family resources to an emphasis on adult patients the latter being the most commonly requested area to cover that I receive after giving talks on the subject In addition the prior chapters from the fi rst edition have been revised and updated
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xviii
Hence what began as a quest to increase awareness of treatable metabolic epilepsies fi rst became a mono-graph to give some form to this arena and has now been enlarged and updated to a second edition It is hoped that this will provide a resource to in some way lead the fi eld and carry it forward It is truly hoped that this book will educate if not enlighten physicians particularly
specialists and trainees in pediatric and adult neurology neurodevelopmental disabilities epilepsy and genetics while caring for patients with inherited metabolic epi-lepsies as well as spur further research into basic mecha-nisms and clinical trials in this group of maladies
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Acknowledgments
This book was fi rst suggested to me by Beth Barry from Demos Medical Publishers following my organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the American Epilepsy Society 2009 meeting Beth was a driving force for the creation of this second edition and she and Young Kim at Demos now aligned with Springer are gratefully acknowledged for unmatched hard work and persever-ance in seeing this through to completion
My education in child neurology and epilepsy is grounded by great mentors including Ralph D Feigin MD in pediatrics and Marvin A Fishman MD in pediat-ric neurology of Baylor College of Medicine in Houston and Gregory L Holmes MD in epilepsy and clinical neurophysiology then at Childrenrsquos Hospital Harvard Medical School in Boston I wish to take this opportunity to acknowledge these teachers of mine
My foray into metabolic disorders has been made pos-sible by the always helpful brilliant and steadfast work of Mike Gibson PhD whose collaboration in the area of gamma-amino butyric acid (GABA) disorders specifi -cally succinic-semialdehyde dehydrogenase (SSADH) defi ciency has been a constant source of intellectual
nourishment and encouragement My career during the two editions of this book has now spanned two great childrenrsquos hospitals Childrenrsquos National and Boston Childrenrsquos and the insight and support of colleagues at both institutions have been fundamental to this work Ongoing collaborations with Mike Gibson as well as William H Theodore MD chief of the Clinical Epilepsy Section at the NINDS have been critical to the ongoing investigative work on metabolic epilepsies
I thank each of the contributors to the fi rst edition of this book for revising and updating their chapters and each of the authors of the new chapters resulting in a signifi cant expansion The outstanding assistance of Alisa Marino is gratefully acknowledged given the enormous complexity of the project and the organiza-tional skills needed to accomplish this and a myriad of other tasks As a group I thank the many patients and families as well as students residents and fellows who inspire our work I thank my own family who as with all of us shoulder the largest burden of personal sacrifi ce and inspire us the most
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

Inherited Metabolic Epilepsies
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Inherited Metabolic Epilepsies
Second Edition
Editor
Phillip L Pearl MDDirector of Epilepsy and Clinical Neurophysiology
William G Lennox Chair Boston Childrenrsquos HospitalProfessor of Neurology
Harvard Medical SchoolBoston Massachusetts
An Imprint of Springer Publishing
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Visit our website at wwwspringerpubcom
ISBN 9780826168634e-book ISBN 9780826168641
Acquisitions Editor Beth BarryCompositor Exeter Premedia Services Private Ltd
Copyright copy 2018 Springer Publishing CompanyDemos Medical Publishing is an imprint of Springer Publishing Company LLC
All rights reserved This book is protected by copyright No part of it may be reproduced stored in a retrieval system or transmitted in any form or by any means electronic mechanical photocopying recording or otherwise without the prior written permission of the publisher
Medicine is an ever-changing science Research and clinical experience are continually expanding our knowledge in particular our understanding of proper treatment and drug therapy The authors editors and publisher have made every effort to ensure that all information in this book is in accordance with the state of knowledge at the time of pro-duction of the book Nevertheless the authors editors and publisher are not responsible for errors or omissions or for any consequences from application of the information in this book and make no warranty expressed or implied with respect to the contents of the publication Every reader should examine carefully the package inserts accompanying each drug and should carefully check whether the dosage schedules mentioned therein or the contraindications stated by the manufacturer differ from the statements made in this book Such examination is particularly important with drugs that are either rarely used or have been newly released on the market
Library of Congress Cataloging-in-Publication Data
Names Pearl Phillip L editorTitle Inherited metabolic epilepsies editor Phillip L PearlDescription Second edition | New York Demos [2018] | Includes bibliographical references and indexIdentifi ers LCCN 2017031804| ISBN 9780826168634 | ISBN 9780826168641 (e-book)Subjects | MESH Epilepsymdashetiology | Brain Diseases Metabolic Inbornmdashcomplications | Epilepsymdashdiagnosis | Brain Diseases Metabolic Inbornmdashdiagnosis | Epilepsymdashtherapy | Brain Diseases Metabolic InbornmdashtherapyClassifi cation LCC RC372 | NLM WL 385 | DDC 616853mdashdc23LC record available at httpslccnlocgov2017031804
Contact us to receive discount rates on bulk purchases We can also customize our books to meet your needs
For more information please contact salesspringerpubcom
Printed in the United States of America by Sheridan Books Inc17 18 19 20 21 5 4 3 2 1
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This book is dedicated to my wife Maria Tartaglia Pearl MD whose sacrifi ces for my work are fortunately outmatched
by our mutual love for medicine
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Contents
Contributors xiPreface xvii
Acknowledgments xix
PART I GENERAL PRINCIPLES 1 Recognition Scope and Implications of Inherited Metabolic Epilepsies 2
Phillip L Pearl
2 Overview of Inherited Metabolic Disease 16Lance H Rodan and Gerard T Berry
3 Treatable Inherited Metabolic Epilepsies Diagnoses Not to Miss 40Phillip L Pearl and Mohammed Almuqbil
PART II BASIC SCIENCE IN METABOLIC EPILEPSIES 4 Metabolic Epilepsies Principles and Mechanisms 56
Carl E Stafstrom and Jong M Rho
5 Metabolic Energetics in Epilepsy 74Ashwini Sri Hari and Manisha Patel
6 Pathways Dysregulation of mTOR and Epilepsy 86Darius Ebrahimi-Fakhari Jonathan Lipton and Mustafa Sahin
7 Protein Anchoring as an Important Mechanism in Early Onset Epilepsy Glycosylphosphatidylinositol (GPI) Defi ciency Syndromes 98Gali Heimer Bruria Ben-Zeev and Yair Anikster
PART III CLINICAL SCIENCE IN METABOLIC EPILEPSIES 8 Neuroimaging in the Metabolic Epilepsies 110
Robert A Zimmerman and Zarir P Khademian
9 Advances in MR Spectroscopy for Inherited Epilepsies 125Andrew Breeden Morgan J Prust Stanley T Fricke Matthew Whitehead and Andrea L Gropman
10 Neuropathology of Metabolic Epilepsies Novel Aspects in Children and the Diagnostic Role of Skin Biopsy 135Harvey B Sarnat
11 Electroencephalography in the Metabolic Epilepsies 149Samata Singhi Mona Alduligan and Phillip L Pearl
Share Inherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
viii
12 Genomic Technologies in Clinical Practice 187Christina Y Hung and Olaf A Bodamer
13 Measures of Cortical Excitability by Transcranial Magnetic Stimulation 201Alexander Rotenberg
14 Ketogenic Diet in Metabolic Epilepsies 207Susan L Fong and Eric H Kossoff
PART IV SMALL MOLECULE DISEASES 15 Amino and Organic Acid Disorders and Epilepsy 218
Kimberly A Chapman and Jamie L Fraser
16 Fatty Acid Oxidation Disorders and Epilepsy 237Dimitar Gavrilov and Dietrich Matern
17 Urea Cycle Disorders and Epilepsy 257Debra S Regier Brendan Lanpher and Marshall L Summar
18 Mitochondrial Diseases and Epilepsy 267Sumit Parikh Lynne A Wolfe and Andrea L Gropman
19 Pyridoxine-Dependent Epilepsy 275Sidney M Gospe Jr
20 Pyridoxamine 5acute-Phosphate Oxidase (PNPO) Defi ciency 287Barbara Plecko-Startinig
21 Tetrahydrobiopterin Defi ciencies and Epilepsy 293Nenad Blau and Thomas Opladen
22 Disorders of GABA Metabolism and Epilepsy 301Phillip L Pearl Kara Vogel and K Michael Gibson
23 Glucose Transporter Type 1 Defi ciency Syndrome 313Cigdem I Akman and Darryl C De Vivo
24 Thiamine Transporter Defi ciency and Epilepsy 326Brahim Tabarki
25 DEND Syndrome Developmental Delay Epilepsy and Neonatal Diabetes a Potassium Channelopathy 333Carolina Lahmann and Frances Ashcroft
26 HyperammonemiaHyperinsulinism Syndrome and Epilepsy 345Nicholas S Abend and Andrea Kelly
27 Glycine Encephalopathy and Epilepsy 353Julia B Hennermann Johan L K Van Hove and Curtis R Coughlin II
28 Serine Synthesis Disorders and Epilepsy 364T J de Koning
29 LeschndashNyhan Disease and Epilepsy 371Beth A Leeman-Markowski and Hyder A Jinnah
30 Sulfi te Oxidase Defi ciencyMolybdenum Cofactor Defi ciency and Epilepsy 394Joumlrn Oliver Sass and Barbara Plecko-Startinig
31 Creatine Disorders and Epilepsy 401Ton de Grauw
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
32 Cerebral Folate Defi ciency and Epilepsy 407Robert Steinfeld
33 Menkesrsquo Disease and Infantile Epilepsy 415Asuri N Prasad
PART V LARGE MOLECULE DISEASES 34 Congenital Disorders of Glycosylation and Epilepsy 428
Susan E Sparks
35 Lysosomal Storage Diseases and Epilepsy 445Pranoot Tanpaiboon and Grisel Lopez
36 Peroxisomal Diseases and Epilepsy 473Parastoo Jangouk Kristin W Barantildeano and Gerald V Raymond
37 Leukodystrophies and Epilepsy 483Davide Tonduti and Adeline Vanderver
PART VI CONCLUSIONS 38 Diagnostic Approaches to Genetic Epilepsies 490
Erika Takle Axeen Christelle El Achkar and Annapurna Poduri
39 Therapeutic Approaches to Inherited Metabolic Epilepsies 497Brandy Verhalen and Berge A Minassian
40 Inherited Metabolic Epilepsies in Adults 503Phillip L Pearl
41 Genetic Counseling in Metabolic Epilepsies 508Jodie M Vento
42 Support and Resources for Patients and Families With Inherited Metabolic Epilepsies 518Christopher Ryan and Jennifer Jeffs
43 Clinical Approach to Inherited Metabolic Epilepsies 525Scott Demarest Anna Lecticia Pinto and Phillip L Pearl
Index 529
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Contributors
Nicholas S Abend MD MSCEAssociate Professor of Neurology and PediatricsDepartments of Neurology and PediatricsChildrenrsquos Hospital of Philadelphia and the University
of PennsylvaniaPhiladelphia Pennsylvania
Christelle El Achkar MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Cigdem I Akman MDAssociate Professor of Clinical Neurology and PediatricsDepartments of Neurology and PediatricsDivision of Pediatric NeurologyInterim ChiefChild NeurologyDirectorPediatric EpilepsyColumbia University College of Physicians and SurgeonsNew York New York
Mona Alduligan MDPhysicianDivision of Clinical NeurophysiologyChildrenrsquos National Medical CenterWashington DC
Mohammed Almuqbil MD FRCP (C)King Abdullah Specialist Childrenrsquos Hospital (KASCH)King Saud bin Abdulaziz University for Health Sciences
(KSAU-HS)Pediatric Neurology DivisionRiyadh Saudi ArabiaKing Abdullah International Medical Research Center
(KAIMRC)National Guard MinistryRiyadh Saudi ArabiaDivision of Genetics and GenomicsBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Yair Anikster MD PhDDirectorMetabolic Disease UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
Frances Ashcroft PhD ScDGlaxoSmithKline Royal Society Research ProfessorDepartment of Physiology Anatomy and GeneticsFellow of Trinity CollegeDirector OXIONUniversity of OxfordOxford England
Erika Takle Axeen MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Minnesota
Kristin W Barantildeano MD PhDClinical AssociatePediatric NeurologyDepartment of NeurologyJohns Hopkins HospitalAssistant Professor of NeurologyJohns Hopkins School of MedicineBaltimore Maryland
Bruria Ben-Zeev MDDirectorPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xii
Gerard T Berry MDDirector Metabolism ProgramProfessor of PediatricsBoston Childrenrsquos HospitalBoston Massachusetts
Nenad Blau PhDSenior Consultant in Biochemical GeneticsProfessor Emeritus of Clinical Biochemistry (UZH)Dietmar-Hopp Metabolic CenterUniversity Childrenrsquos HospitalHeidelberg Germany
Olaf A Bodamer MD PhDAssociate Chief of Genetics and GenomicsBoston Childrenrsquos HospitalPark Gerald Chair in Genetics and GenomicsHarvard Medical SchoolBoston Massachusetts
Andrew Breeden PhDProgram AnalystHealth Program SpecialistNational Institute of Neurological Disorders and
Stroke (NINDS)Bethesda Maryland
Kimberly A Chapman MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National
Health SystemWashington DC
Curtis R Coughlin II MS MBe CGCAssistant Professor of PediatricsSection of Clinical Genetics and MetabolismDepartment of PediatricsUniversity of ColoradoAurora Colorado
Ton de Grauw MD PhDChiefNeurosciencesChildrenrsquos Healthcare of AtlantaDirectorPediatric NeurologyEmory University School of MedicineAtlanta Georgia
T J de Koning MD PhDPaediatrician for Inborn Errors of MetabolismDepartment of Genetics and PaediatricsUniversity Medical Centre GroningenUniversity of GroningenGroningen The Netherlands
Darryl C De Vivo MDSidney Carter Professor of NeurologyProfessor of PediatricsPediatric Neurology ServiceFounding DirectorColleen Giblin Research Laboratories for Pediatric
NeurologyAssociate ChairmanPediatric Neurosciences and Developmental
NeurobiologyCo-DirectorMotor Neuron CenterDirectorSpinal Muscular Atrophy (SMA) CenterChief EmeritusPediatric NeurologyColumbia University Medical CenterNew York New York
Scott Demarest MDAssistant Professor of Pediatrics and NeurologyChildrenrsquos Hospital ColoradoUniversity of ColoradoAurora Colorado
Darius Ebrahimi-Fakhari MD DrmedResident PhysicianDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Susan L Fong MD PhDAssistant ResidentPediatric NeurologyJohns Hopkins HospitalBaltimore Maryland
Jamie L Fraser MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National Health
SystemWashington DC
Stanley T Fricke PhDPhysicistChildrenrsquos National Medical CenterWashington DC
Dimitar Gavrilov MD PhDAssistant ProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
K Michael Gibson PhDAllen I White Distinguished Professor and ChairDepartment of PharmacotherapyWashington State University College of PharmacySpokane Washington
Sidney M Gospe Jr MD PhDHerman and Faye Sarkowsky Endowed ChairProfessor and HeadDivision of Pediatric NeurologyDepartments of Neurology and PediatricsUniversity of WashingtonDivision of NeurologySeattle Childrenrsquos Hospital and Seattle Childrenrsquos
Research InstituteSeattle Washington
Andrea L Gropman MDChief Neurogenetics and Neurodevelopmental
PediatricsChildrenrsquos National Medical CenterAssociate Professor of Neurology and PediatricsGeorge Washington School of Medicine and Health
SciencesWashington DC
Ashwini Sri Hari PhD CandidateDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Gali Heimer MD PhDSenior Physician and Director of the Angelman ClinicPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical Center Tel-Hashomer Israel Sackler Faculty of MedicineTel-Aviv UniversityTel-Aviv IsraelMember of the Dr Pinchas Borenstein Talpiot Medical
Leadership ProgramSheba Medical CenterTel-Hashomer Israel
Julia B Hennermann MDProfessor of Metabolic DiseasesUniversity Medical Center MainzVilla Metabolica Department of Pediatric and
Adolescent MedicineMainz Germany
Christina Y Hung MDResearch AssociateHMS Instructor in PediatricsDivision for Human Genetics and GenomicsBoston Childrenrsquos HospitalBoston Massachusetts
Parastoo Jangouk MDGastroenterology and Hepatology FellowYale-New Haven HospitalNew Haven Connecticut
Jennifer Jeffs LICSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Hyder A Jinnah MD PhDProfessorDepartments of Neurology Human Genetics and
PediatricsEmory University School of MedicineAtlanta Georgia
Andrea Kelly MD MSCEAssociate Professor of Pediatrics CEDepartment of PediatricsChildrenrsquos Hospital of Philadelphia and Perelman School
of Medicine of the University of PennsylvaniaPhiladelphia Pennsylvania
Zarir P Khademian MD PhDAssistant Professor of Radiology and PediatricsStaff Neurologist Division of Diagnostic Imaging and
RadiologyChildrenrsquos National Medical CenterWashington DC
Eric H Kossoff MDProfessorNeurology and PediatricsJohns Hopkins HospitalBaltimore Maryland
Carolina Lahmann PhDPostdoctoral FellowHarvard Medical SchoolBoston Massachusetts
Brendan Lanpher MDAssistant Professor of Medical GeneticsDepartment of Clinical GenomicsMayo ClinicRochester Minnesota
Beth A Leeman-Markowski MD MA MMScAssistant ProfessorDepartment of NeurologyNew York UniversityInvestigatorResearch ServiceVA New York Harbor Healthcare SystemmdashManhattan
CampusNew York New York
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xiv
Jonathan Lipton MD PhDAssistant Professor of NeurologyDepartment of Neurology and F M Kirby Center for
NeuroscienceBoston Childrenrsquos Hospital Harvard Medical SchoolBoston Massachusetts
Grisel Lopez MDSenior Staff ClinicianNational Human Genome Research InstituteNational Institutes of HealthBethesda Maryland
Dietrich Matern MD PhDProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
Berge A Minassian MDDivision ChiefPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas TexasUniversity of TorontoToronto Ontario Canada
Thomas Opladen MDDivision of Child Neurology and Metabolic DiseasesUniversity Childrenlsquos Hospital Heidelberg Germany
Sumit Parikh MDDirector of Cleveland Clinic Neurogenetics Metabolic
amp Mitochondrial Disease ProgramCleveland ClinicAssociate ProfessorDepartment of PediatricsCase Western Reserve University School of MedicineCleveland Ohio
Manisha Patel PhDProfessorDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Phillip L Pearl MDDirector of Epilepsy and Clinical NeurophysiologyWilliam G Lennox ChairBoston Childrenrsquos HospitalProfessor of NeurologyHarvard Medical SchoolBoston Massachusetts
Anna Lecticia Pinto MDAssistant in Neurology and Co-DirectorSturge Weber Clinic Boston Childrenrsquos HospitalLecturer of NeurologyHarvard Medical SchoolBoston Massachusetts
Barbara Plecko-Startinig MDHeadDivision of Child NeurologyChildrenrsquos Hospital ZurichProfessor of Child NeurologyUniversity of ZurichZurich Switzerland
Annapurna Poduri MD MPHEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Asuri N Prasad MBBS MD FRCPC FRCPEProfessor in Pediatrics and Clinical NeurosciencesDivision of Pediatric NeurologyDepartment of PediatricsSchulich School of Medicine and DentistryChildrenrsquos Hospital London Health Sciences CentreWestern UniversityLondon Ontario Canada
Morgan J Prust MDClinical Fellow in NeurologyDepartment of NeurologyMassachusetts General HospitalBrigham amp Womenrsquos HospitalBoston Massachusetts
Gerald V Raymond MDProfessorDepartment of NeurologyUniversity of Minnesota Medical SchoolMinneapolis Minnesota
Debra S Regier MD PhDDirector of Genetic and Genomic Education Medical
GeneticistRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Jong M Rho MDProfessor of Pediatrics Clinical Neurosciences
Physiology and PharmacologyDr Robert Haslam Chair in Child NeurologySection of Paediatric NeurologyCumming School of Medicine University of CalgaryAlberta Childrenrsquos HospitalCalgary Alberta Canada
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Lance H Rodan MDStaff PhysicianBoston Childrenrsquos HospitalBoston Massachusetts
Alexander Rotenberg MD PhDDirector Neuromodulation ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalAssociate Professor of NeurologyHarvard Medical SchoolBoston Massachusetts
Christopher Ryan LCSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Mustafa Sahin MD PhDProfessor of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Harvey B Sarnat MS MD FRCPCProfessor Departments of Paediatrics Pathology
(Neuropathology) and Clinical NeurosciencesUniversity of Calgary Cumming School of Medicine
and Alberta Childrenrsquos Hospital Research InstituteCalgary Alberta Canada
Joumlrn Oliver Sass Dr rer natProfessor of Bioanalytics and BiochemistryDepartment of Natural SciencesBonn-Rhein-Sieg University of Applied SciencesSankt Augustin Germany
Samata Singhi MDClinical Fellow in NeurologyDepartment of NeurologyBoston Childrenrsquos HospitalBoston Massachusetts
Susan E Sparks MD PhDMedical DirectorNA Medical AffairsRare DiseasesSanofi GenzymeCambridge Massachusetts
Carl E Stafstrom MD PhDProfessor of Neurology and PediatricsLederer Chair in Pediatric EpilepsyDirector Division of Pediatric NeurologyJohns Hopkins University School of MedicineBaltimore Maryland
Robert Steinfeld MD PhDProfessor of Neurometabolic and Neurodegenerative
Diseases in Childhood and AdolescenceDepartment of Pediatrics and Pediatric NeurologyUniversity Medical Center GoumlttingenGoumlttingen Germany
Marshall L Summar MDChief Division of Genetics and MetabolismMargaret OrsquoMalley Chair of Genetic MedicineRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Brahim Tabarki MDDivision of Pediatric NeurologyPrince Sultan Military Medical CityRiyadh Saudi ArabiaAssociate Professor of Neurology and PediatricsThe Ibn El Jazzar University School of MedicineSousse Tunisia
Pranoot Tanpaiboon MDAssociate Professor of PediatricsDivision of Genetics and MetabolismThe George Washington University School of Medicine
and Health SciencesChildrenrsquos National Health System Childrenrsquos National
Rare Disease InstituteWashington DC
Davide Tonduti MDChild NeurologistDepartment of Child NeurologyFondazione IRCCS Istituto Neurologico Carlo BestaMilano Italy
Johan L K Van Hove MD PhDProfessor of PediatricsSection of Clinical Genetics and Metabolism
Department of PediatricsUniversity of ColoradoAurora Colorado
Adeline Vanderver MDAttending PhysicianDivision of NeurologyProgram DirectorLeukodystrophy CenterJacob A Kamens Endowed Chair in Neurologic
Disorders and Translational NeurotherapeuticsChildrenrsquos Hospital of PhiladelphiaAssociate Professor of NeurologyPerelman School of Medicine at the University of
PennsylvaniaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xvi
Jodie M Vento MGC LCGCManagerCenter for Rare Disease TherapyManagerBrain Care InstituteManagerLaboratory Genetic Counseling ServicesChildrenrsquos Hospital of Pittsburgh of UPMCPittsburgh Pennsylvania
Brandy Verhalen PhDLab ManagerPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas Texas
Kara Vogel PhDPostdoctoral Research AssociateUniversity of WisconsinndashMadisonMadison Wisconsin
Matthew Whitehead MDRadiologistChildrenrsquos National Medical CenterWashington DC
Lynne A Wolfe MS CRNPSenior Nurse PractitionerUndiagnosed Disorders ProgramNational Human Genome Research Institute National
Institutes of HealthBethesda Maryland
Robert A Zimmerman MDProfessor of RadiologyRaymond and Ruth Perelman School of Medicine at the
University of PennsylvaniaChiefDivision of Neuroradiology and MRIThe Childrenrsquos Hospital of PhiladelphiaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Preface
This edition of Inherited Metabolic Epilepsies is a greatly expanded and updated version of the fi rst Following a rousing response to the fi rst edition far beyond any anticipated measure it was clear that a reexamination of the material taking into account many helpful sug-gestions that I received from readers far and wide was in order Despite my own misgivings that books are no longer fashionable and are largely replaced by journals and online sources that lend themselves to periodic if not continual updating there remains an appetite and clamor for books that accomplish what I had hoped to do originally and aim to achieve to a greater extent in this edition to encapsulate a burgeoning fi eld suf-fi ciently that a student practitioner or investigator can turn to the source with confi dence that the neces-sary background as well as detail will be available to reward the search for information and also move the fi eld forward
The fi rst edition of this monograph was born follow-ing the organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the annual meeting of the American Epilepsy Society in Boston in 2009 At the time of proposing the topic I was wrestling with a chasmic gap between the fascinat-ing disorders being discussed at the geneticndashmetabolic meetings and the advancing wave in epilepsy classifi ca-tion diagnosis and treatment occupying the meetings attended by members of the societies associated with neurology and epilepsy At that time a storybook series of investigations elucidated not only the surprising antiq-uitin defect in pyridoxine-dependent epilepsy but also the highly charged requirement that physicians consider a pivotal role for folinic acid and pyridoxal-5-phosphate in patients with virtually the same clinical presentation I also perceived a relative lack of awareness of disorders such as glucose transporter 1 defi ciency serine synthetic defects developmental delay epilepsy and neonatal dia-betes (DEND) and hyperinsulinismndashhyperammonemia (HIndashHA) that had very specifi c therapeutic implications with potential for dramatically improving outcome but with an even greater likelihood that they were escaping diagnosis
Overall the inherited metabolic epilepsies repre-sent a group of disorders that is rare individually but
in aggregate represents a substantial clinical burden as well as a vexing area for physicians investigators and students to master The sheer amount and complexity of information are overwhelming and require the physician to synthesize key concepts in neurology genetics and epilepsy As a pediatric epileptologist and medical edu-cator I have found this area among the most challenging and rewarding in practice and research The fi rst edition organized the disorders in a traditional approach under the roof of metabolism by dividing them into small- and large-molecule disorders In the Preface to that edition there was an explanation of various ways of organizing these disorders some more user friendly to the neurol-ogist than the small- versus large-molecule divide but this was an opportunity to present that way of thinking to the neurologist which brings this clinical specialty closer to that of genetics metabolism
In this second edition there is an expansion from four sections (General Principles Small Molecule Diseases Large Molecule Diseases and Conclusions) to six sec-tions with the addition of chapters in basic science and clinical science of the metabolic epilepsies The book has been expanded from 28 to 43 chapters with new chapters including overviews of metabolic disease and the basic science of metabolic epilepsy plus new topics such as metabolic energetics and implications of vital pathways A full chapter is devoted to the mechanistic target of rapamycin (mTOR) pathway that regulates cell replica-tion and so much of homeostasis and new pathophysi-ologic mechanisms such as protein anchoring disorders There are new chapters on neurotransmitter transmission measurement using transcranial magnetic stimulation genomic technologies and approaches to diagnosis and therapy referable to this group of disorders The clinical science section now includes a marvelous and refl ective chapter on neuropathology by Harvey B Sarnat There are new chapters devoted to specifi c disorders such as pyridoxal-5-phosphate dependency and Menkesrsquo disease There are chapters with completely new vantage points from community and family resources to an emphasis on adult patients the latter being the most commonly requested area to cover that I receive after giving talks on the subject In addition the prior chapters from the fi rst edition have been revised and updated
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xviii
Hence what began as a quest to increase awareness of treatable metabolic epilepsies fi rst became a mono-graph to give some form to this arena and has now been enlarged and updated to a second edition It is hoped that this will provide a resource to in some way lead the fi eld and carry it forward It is truly hoped that this book will educate if not enlighten physicians particularly
specialists and trainees in pediatric and adult neurology neurodevelopmental disabilities epilepsy and genetics while caring for patients with inherited metabolic epi-lepsies as well as spur further research into basic mecha-nisms and clinical trials in this group of maladies
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Acknowledgments
This book was fi rst suggested to me by Beth Barry from Demos Medical Publishers following my organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the American Epilepsy Society 2009 meeting Beth was a driving force for the creation of this second edition and she and Young Kim at Demos now aligned with Springer are gratefully acknowledged for unmatched hard work and persever-ance in seeing this through to completion
My education in child neurology and epilepsy is grounded by great mentors including Ralph D Feigin MD in pediatrics and Marvin A Fishman MD in pediat-ric neurology of Baylor College of Medicine in Houston and Gregory L Holmes MD in epilepsy and clinical neurophysiology then at Childrenrsquos Hospital Harvard Medical School in Boston I wish to take this opportunity to acknowledge these teachers of mine
My foray into metabolic disorders has been made pos-sible by the always helpful brilliant and steadfast work of Mike Gibson PhD whose collaboration in the area of gamma-amino butyric acid (GABA) disorders specifi -cally succinic-semialdehyde dehydrogenase (SSADH) defi ciency has been a constant source of intellectual
nourishment and encouragement My career during the two editions of this book has now spanned two great childrenrsquos hospitals Childrenrsquos National and Boston Childrenrsquos and the insight and support of colleagues at both institutions have been fundamental to this work Ongoing collaborations with Mike Gibson as well as William H Theodore MD chief of the Clinical Epilepsy Section at the NINDS have been critical to the ongoing investigative work on metabolic epilepsies
I thank each of the contributors to the fi rst edition of this book for revising and updating their chapters and each of the authors of the new chapters resulting in a signifi cant expansion The outstanding assistance of Alisa Marino is gratefully acknowledged given the enormous complexity of the project and the organiza-tional skills needed to accomplish this and a myriad of other tasks As a group I thank the many patients and families as well as students residents and fellows who inspire our work I thank my own family who as with all of us shoulder the largest burden of personal sacrifi ce and inspire us the most
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Inherited Metabolic Epilepsies
Second Edition
Editor
Phillip L Pearl MDDirector of Epilepsy and Clinical Neurophysiology
William G Lennox Chair Boston Childrenrsquos HospitalProfessor of Neurology
Harvard Medical SchoolBoston Massachusetts
An Imprint of Springer Publishing
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Visit our website at wwwspringerpubcom
ISBN 9780826168634e-book ISBN 9780826168641
Acquisitions Editor Beth BarryCompositor Exeter Premedia Services Private Ltd
Copyright copy 2018 Springer Publishing CompanyDemos Medical Publishing is an imprint of Springer Publishing Company LLC
All rights reserved This book is protected by copyright No part of it may be reproduced stored in a retrieval system or transmitted in any form or by any means electronic mechanical photocopying recording or otherwise without the prior written permission of the publisher
Medicine is an ever-changing science Research and clinical experience are continually expanding our knowledge in particular our understanding of proper treatment and drug therapy The authors editors and publisher have made every effort to ensure that all information in this book is in accordance with the state of knowledge at the time of pro-duction of the book Nevertheless the authors editors and publisher are not responsible for errors or omissions or for any consequences from application of the information in this book and make no warranty expressed or implied with respect to the contents of the publication Every reader should examine carefully the package inserts accompanying each drug and should carefully check whether the dosage schedules mentioned therein or the contraindications stated by the manufacturer differ from the statements made in this book Such examination is particularly important with drugs that are either rarely used or have been newly released on the market
Library of Congress Cataloging-in-Publication Data
Names Pearl Phillip L editorTitle Inherited metabolic epilepsies editor Phillip L PearlDescription Second edition | New York Demos [2018] | Includes bibliographical references and indexIdentifi ers LCCN 2017031804| ISBN 9780826168634 | ISBN 9780826168641 (e-book)Subjects | MESH Epilepsymdashetiology | Brain Diseases Metabolic Inbornmdashcomplications | Epilepsymdashdiagnosis | Brain Diseases Metabolic Inbornmdashdiagnosis | Epilepsymdashtherapy | Brain Diseases Metabolic InbornmdashtherapyClassifi cation LCC RC372 | NLM WL 385 | DDC 616853mdashdc23LC record available at httpslccnlocgov2017031804
Contact us to receive discount rates on bulk purchases We can also customize our books to meet your needs
For more information please contact salesspringerpubcom
Printed in the United States of America by Sheridan Books Inc17 18 19 20 21 5 4 3 2 1
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This book is dedicated to my wife Maria Tartaglia Pearl MD whose sacrifi ces for my work are fortunately outmatched
by our mutual love for medicine
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Contents
Contributors xiPreface xvii
Acknowledgments xix
PART I GENERAL PRINCIPLES 1 Recognition Scope and Implications of Inherited Metabolic Epilepsies 2
Phillip L Pearl
2 Overview of Inherited Metabolic Disease 16Lance H Rodan and Gerard T Berry
3 Treatable Inherited Metabolic Epilepsies Diagnoses Not to Miss 40Phillip L Pearl and Mohammed Almuqbil
PART II BASIC SCIENCE IN METABOLIC EPILEPSIES 4 Metabolic Epilepsies Principles and Mechanisms 56
Carl E Stafstrom and Jong M Rho
5 Metabolic Energetics in Epilepsy 74Ashwini Sri Hari and Manisha Patel
6 Pathways Dysregulation of mTOR and Epilepsy 86Darius Ebrahimi-Fakhari Jonathan Lipton and Mustafa Sahin
7 Protein Anchoring as an Important Mechanism in Early Onset Epilepsy Glycosylphosphatidylinositol (GPI) Defi ciency Syndromes 98Gali Heimer Bruria Ben-Zeev and Yair Anikster
PART III CLINICAL SCIENCE IN METABOLIC EPILEPSIES 8 Neuroimaging in the Metabolic Epilepsies 110
Robert A Zimmerman and Zarir P Khademian
9 Advances in MR Spectroscopy for Inherited Epilepsies 125Andrew Breeden Morgan J Prust Stanley T Fricke Matthew Whitehead and Andrea L Gropman
10 Neuropathology of Metabolic Epilepsies Novel Aspects in Children and the Diagnostic Role of Skin Biopsy 135Harvey B Sarnat
11 Electroencephalography in the Metabolic Epilepsies 149Samata Singhi Mona Alduligan and Phillip L Pearl
Share Inherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
viii
12 Genomic Technologies in Clinical Practice 187Christina Y Hung and Olaf A Bodamer
13 Measures of Cortical Excitability by Transcranial Magnetic Stimulation 201Alexander Rotenberg
14 Ketogenic Diet in Metabolic Epilepsies 207Susan L Fong and Eric H Kossoff
PART IV SMALL MOLECULE DISEASES 15 Amino and Organic Acid Disorders and Epilepsy 218
Kimberly A Chapman and Jamie L Fraser
16 Fatty Acid Oxidation Disorders and Epilepsy 237Dimitar Gavrilov and Dietrich Matern
17 Urea Cycle Disorders and Epilepsy 257Debra S Regier Brendan Lanpher and Marshall L Summar
18 Mitochondrial Diseases and Epilepsy 267Sumit Parikh Lynne A Wolfe and Andrea L Gropman
19 Pyridoxine-Dependent Epilepsy 275Sidney M Gospe Jr
20 Pyridoxamine 5acute-Phosphate Oxidase (PNPO) Defi ciency 287Barbara Plecko-Startinig
21 Tetrahydrobiopterin Defi ciencies and Epilepsy 293Nenad Blau and Thomas Opladen
22 Disorders of GABA Metabolism and Epilepsy 301Phillip L Pearl Kara Vogel and K Michael Gibson
23 Glucose Transporter Type 1 Defi ciency Syndrome 313Cigdem I Akman and Darryl C De Vivo
24 Thiamine Transporter Defi ciency and Epilepsy 326Brahim Tabarki
25 DEND Syndrome Developmental Delay Epilepsy and Neonatal Diabetes a Potassium Channelopathy 333Carolina Lahmann and Frances Ashcroft
26 HyperammonemiaHyperinsulinism Syndrome and Epilepsy 345Nicholas S Abend and Andrea Kelly
27 Glycine Encephalopathy and Epilepsy 353Julia B Hennermann Johan L K Van Hove and Curtis R Coughlin II
28 Serine Synthesis Disorders and Epilepsy 364T J de Koning
29 LeschndashNyhan Disease and Epilepsy 371Beth A Leeman-Markowski and Hyder A Jinnah
30 Sulfi te Oxidase Defi ciencyMolybdenum Cofactor Defi ciency and Epilepsy 394Joumlrn Oliver Sass and Barbara Plecko-Startinig
31 Creatine Disorders and Epilepsy 401Ton de Grauw
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
32 Cerebral Folate Defi ciency and Epilepsy 407Robert Steinfeld
33 Menkesrsquo Disease and Infantile Epilepsy 415Asuri N Prasad
PART V LARGE MOLECULE DISEASES 34 Congenital Disorders of Glycosylation and Epilepsy 428
Susan E Sparks
35 Lysosomal Storage Diseases and Epilepsy 445Pranoot Tanpaiboon and Grisel Lopez
36 Peroxisomal Diseases and Epilepsy 473Parastoo Jangouk Kristin W Barantildeano and Gerald V Raymond
37 Leukodystrophies and Epilepsy 483Davide Tonduti and Adeline Vanderver
PART VI CONCLUSIONS 38 Diagnostic Approaches to Genetic Epilepsies 490
Erika Takle Axeen Christelle El Achkar and Annapurna Poduri
39 Therapeutic Approaches to Inherited Metabolic Epilepsies 497Brandy Verhalen and Berge A Minassian
40 Inherited Metabolic Epilepsies in Adults 503Phillip L Pearl
41 Genetic Counseling in Metabolic Epilepsies 508Jodie M Vento
42 Support and Resources for Patients and Families With Inherited Metabolic Epilepsies 518Christopher Ryan and Jennifer Jeffs
43 Clinical Approach to Inherited Metabolic Epilepsies 525Scott Demarest Anna Lecticia Pinto and Phillip L Pearl
Index 529
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Contributors
Nicholas S Abend MD MSCEAssociate Professor of Neurology and PediatricsDepartments of Neurology and PediatricsChildrenrsquos Hospital of Philadelphia and the University
of PennsylvaniaPhiladelphia Pennsylvania
Christelle El Achkar MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Cigdem I Akman MDAssociate Professor of Clinical Neurology and PediatricsDepartments of Neurology and PediatricsDivision of Pediatric NeurologyInterim ChiefChild NeurologyDirectorPediatric EpilepsyColumbia University College of Physicians and SurgeonsNew York New York
Mona Alduligan MDPhysicianDivision of Clinical NeurophysiologyChildrenrsquos National Medical CenterWashington DC
Mohammed Almuqbil MD FRCP (C)King Abdullah Specialist Childrenrsquos Hospital (KASCH)King Saud bin Abdulaziz University for Health Sciences
(KSAU-HS)Pediatric Neurology DivisionRiyadh Saudi ArabiaKing Abdullah International Medical Research Center
(KAIMRC)National Guard MinistryRiyadh Saudi ArabiaDivision of Genetics and GenomicsBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Yair Anikster MD PhDDirectorMetabolic Disease UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
Frances Ashcroft PhD ScDGlaxoSmithKline Royal Society Research ProfessorDepartment of Physiology Anatomy and GeneticsFellow of Trinity CollegeDirector OXIONUniversity of OxfordOxford England
Erika Takle Axeen MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Minnesota
Kristin W Barantildeano MD PhDClinical AssociatePediatric NeurologyDepartment of NeurologyJohns Hopkins HospitalAssistant Professor of NeurologyJohns Hopkins School of MedicineBaltimore Maryland
Bruria Ben-Zeev MDDirectorPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xii
Gerard T Berry MDDirector Metabolism ProgramProfessor of PediatricsBoston Childrenrsquos HospitalBoston Massachusetts
Nenad Blau PhDSenior Consultant in Biochemical GeneticsProfessor Emeritus of Clinical Biochemistry (UZH)Dietmar-Hopp Metabolic CenterUniversity Childrenrsquos HospitalHeidelberg Germany
Olaf A Bodamer MD PhDAssociate Chief of Genetics and GenomicsBoston Childrenrsquos HospitalPark Gerald Chair in Genetics and GenomicsHarvard Medical SchoolBoston Massachusetts
Andrew Breeden PhDProgram AnalystHealth Program SpecialistNational Institute of Neurological Disorders and
Stroke (NINDS)Bethesda Maryland
Kimberly A Chapman MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National
Health SystemWashington DC
Curtis R Coughlin II MS MBe CGCAssistant Professor of PediatricsSection of Clinical Genetics and MetabolismDepartment of PediatricsUniversity of ColoradoAurora Colorado
Ton de Grauw MD PhDChiefNeurosciencesChildrenrsquos Healthcare of AtlantaDirectorPediatric NeurologyEmory University School of MedicineAtlanta Georgia
T J de Koning MD PhDPaediatrician for Inborn Errors of MetabolismDepartment of Genetics and PaediatricsUniversity Medical Centre GroningenUniversity of GroningenGroningen The Netherlands
Darryl C De Vivo MDSidney Carter Professor of NeurologyProfessor of PediatricsPediatric Neurology ServiceFounding DirectorColleen Giblin Research Laboratories for Pediatric
NeurologyAssociate ChairmanPediatric Neurosciences and Developmental
NeurobiologyCo-DirectorMotor Neuron CenterDirectorSpinal Muscular Atrophy (SMA) CenterChief EmeritusPediatric NeurologyColumbia University Medical CenterNew York New York
Scott Demarest MDAssistant Professor of Pediatrics and NeurologyChildrenrsquos Hospital ColoradoUniversity of ColoradoAurora Colorado
Darius Ebrahimi-Fakhari MD DrmedResident PhysicianDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Susan L Fong MD PhDAssistant ResidentPediatric NeurologyJohns Hopkins HospitalBaltimore Maryland
Jamie L Fraser MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National Health
SystemWashington DC
Stanley T Fricke PhDPhysicistChildrenrsquos National Medical CenterWashington DC
Dimitar Gavrilov MD PhDAssistant ProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
K Michael Gibson PhDAllen I White Distinguished Professor and ChairDepartment of PharmacotherapyWashington State University College of PharmacySpokane Washington
Sidney M Gospe Jr MD PhDHerman and Faye Sarkowsky Endowed ChairProfessor and HeadDivision of Pediatric NeurologyDepartments of Neurology and PediatricsUniversity of WashingtonDivision of NeurologySeattle Childrenrsquos Hospital and Seattle Childrenrsquos
Research InstituteSeattle Washington
Andrea L Gropman MDChief Neurogenetics and Neurodevelopmental
PediatricsChildrenrsquos National Medical CenterAssociate Professor of Neurology and PediatricsGeorge Washington School of Medicine and Health
SciencesWashington DC
Ashwini Sri Hari PhD CandidateDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Gali Heimer MD PhDSenior Physician and Director of the Angelman ClinicPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical Center Tel-Hashomer Israel Sackler Faculty of MedicineTel-Aviv UniversityTel-Aviv IsraelMember of the Dr Pinchas Borenstein Talpiot Medical
Leadership ProgramSheba Medical CenterTel-Hashomer Israel
Julia B Hennermann MDProfessor of Metabolic DiseasesUniversity Medical Center MainzVilla Metabolica Department of Pediatric and
Adolescent MedicineMainz Germany
Christina Y Hung MDResearch AssociateHMS Instructor in PediatricsDivision for Human Genetics and GenomicsBoston Childrenrsquos HospitalBoston Massachusetts
Parastoo Jangouk MDGastroenterology and Hepatology FellowYale-New Haven HospitalNew Haven Connecticut
Jennifer Jeffs LICSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Hyder A Jinnah MD PhDProfessorDepartments of Neurology Human Genetics and
PediatricsEmory University School of MedicineAtlanta Georgia
Andrea Kelly MD MSCEAssociate Professor of Pediatrics CEDepartment of PediatricsChildrenrsquos Hospital of Philadelphia and Perelman School
of Medicine of the University of PennsylvaniaPhiladelphia Pennsylvania
Zarir P Khademian MD PhDAssistant Professor of Radiology and PediatricsStaff Neurologist Division of Diagnostic Imaging and
RadiologyChildrenrsquos National Medical CenterWashington DC
Eric H Kossoff MDProfessorNeurology and PediatricsJohns Hopkins HospitalBaltimore Maryland
Carolina Lahmann PhDPostdoctoral FellowHarvard Medical SchoolBoston Massachusetts
Brendan Lanpher MDAssistant Professor of Medical GeneticsDepartment of Clinical GenomicsMayo ClinicRochester Minnesota
Beth A Leeman-Markowski MD MA MMScAssistant ProfessorDepartment of NeurologyNew York UniversityInvestigatorResearch ServiceVA New York Harbor Healthcare SystemmdashManhattan
CampusNew York New York
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xiv
Jonathan Lipton MD PhDAssistant Professor of NeurologyDepartment of Neurology and F M Kirby Center for
NeuroscienceBoston Childrenrsquos Hospital Harvard Medical SchoolBoston Massachusetts
Grisel Lopez MDSenior Staff ClinicianNational Human Genome Research InstituteNational Institutes of HealthBethesda Maryland
Dietrich Matern MD PhDProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
Berge A Minassian MDDivision ChiefPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas TexasUniversity of TorontoToronto Ontario Canada
Thomas Opladen MDDivision of Child Neurology and Metabolic DiseasesUniversity Childrenlsquos Hospital Heidelberg Germany
Sumit Parikh MDDirector of Cleveland Clinic Neurogenetics Metabolic
amp Mitochondrial Disease ProgramCleveland ClinicAssociate ProfessorDepartment of PediatricsCase Western Reserve University School of MedicineCleveland Ohio
Manisha Patel PhDProfessorDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Phillip L Pearl MDDirector of Epilepsy and Clinical NeurophysiologyWilliam G Lennox ChairBoston Childrenrsquos HospitalProfessor of NeurologyHarvard Medical SchoolBoston Massachusetts
Anna Lecticia Pinto MDAssistant in Neurology and Co-DirectorSturge Weber Clinic Boston Childrenrsquos HospitalLecturer of NeurologyHarvard Medical SchoolBoston Massachusetts
Barbara Plecko-Startinig MDHeadDivision of Child NeurologyChildrenrsquos Hospital ZurichProfessor of Child NeurologyUniversity of ZurichZurich Switzerland
Annapurna Poduri MD MPHEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Asuri N Prasad MBBS MD FRCPC FRCPEProfessor in Pediatrics and Clinical NeurosciencesDivision of Pediatric NeurologyDepartment of PediatricsSchulich School of Medicine and DentistryChildrenrsquos Hospital London Health Sciences CentreWestern UniversityLondon Ontario Canada
Morgan J Prust MDClinical Fellow in NeurologyDepartment of NeurologyMassachusetts General HospitalBrigham amp Womenrsquos HospitalBoston Massachusetts
Gerald V Raymond MDProfessorDepartment of NeurologyUniversity of Minnesota Medical SchoolMinneapolis Minnesota
Debra S Regier MD PhDDirector of Genetic and Genomic Education Medical
GeneticistRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Jong M Rho MDProfessor of Pediatrics Clinical Neurosciences
Physiology and PharmacologyDr Robert Haslam Chair in Child NeurologySection of Paediatric NeurologyCumming School of Medicine University of CalgaryAlberta Childrenrsquos HospitalCalgary Alberta Canada
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Lance H Rodan MDStaff PhysicianBoston Childrenrsquos HospitalBoston Massachusetts
Alexander Rotenberg MD PhDDirector Neuromodulation ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalAssociate Professor of NeurologyHarvard Medical SchoolBoston Massachusetts
Christopher Ryan LCSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Mustafa Sahin MD PhDProfessor of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Harvey B Sarnat MS MD FRCPCProfessor Departments of Paediatrics Pathology
(Neuropathology) and Clinical NeurosciencesUniversity of Calgary Cumming School of Medicine
and Alberta Childrenrsquos Hospital Research InstituteCalgary Alberta Canada
Joumlrn Oliver Sass Dr rer natProfessor of Bioanalytics and BiochemistryDepartment of Natural SciencesBonn-Rhein-Sieg University of Applied SciencesSankt Augustin Germany
Samata Singhi MDClinical Fellow in NeurologyDepartment of NeurologyBoston Childrenrsquos HospitalBoston Massachusetts
Susan E Sparks MD PhDMedical DirectorNA Medical AffairsRare DiseasesSanofi GenzymeCambridge Massachusetts
Carl E Stafstrom MD PhDProfessor of Neurology and PediatricsLederer Chair in Pediatric EpilepsyDirector Division of Pediatric NeurologyJohns Hopkins University School of MedicineBaltimore Maryland
Robert Steinfeld MD PhDProfessor of Neurometabolic and Neurodegenerative
Diseases in Childhood and AdolescenceDepartment of Pediatrics and Pediatric NeurologyUniversity Medical Center GoumlttingenGoumlttingen Germany
Marshall L Summar MDChief Division of Genetics and MetabolismMargaret OrsquoMalley Chair of Genetic MedicineRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Brahim Tabarki MDDivision of Pediatric NeurologyPrince Sultan Military Medical CityRiyadh Saudi ArabiaAssociate Professor of Neurology and PediatricsThe Ibn El Jazzar University School of MedicineSousse Tunisia
Pranoot Tanpaiboon MDAssociate Professor of PediatricsDivision of Genetics and MetabolismThe George Washington University School of Medicine
and Health SciencesChildrenrsquos National Health System Childrenrsquos National
Rare Disease InstituteWashington DC
Davide Tonduti MDChild NeurologistDepartment of Child NeurologyFondazione IRCCS Istituto Neurologico Carlo BestaMilano Italy
Johan L K Van Hove MD PhDProfessor of PediatricsSection of Clinical Genetics and Metabolism
Department of PediatricsUniversity of ColoradoAurora Colorado
Adeline Vanderver MDAttending PhysicianDivision of NeurologyProgram DirectorLeukodystrophy CenterJacob A Kamens Endowed Chair in Neurologic
Disorders and Translational NeurotherapeuticsChildrenrsquos Hospital of PhiladelphiaAssociate Professor of NeurologyPerelman School of Medicine at the University of
PennsylvaniaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xvi
Jodie M Vento MGC LCGCManagerCenter for Rare Disease TherapyManagerBrain Care InstituteManagerLaboratory Genetic Counseling ServicesChildrenrsquos Hospital of Pittsburgh of UPMCPittsburgh Pennsylvania
Brandy Verhalen PhDLab ManagerPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas Texas
Kara Vogel PhDPostdoctoral Research AssociateUniversity of WisconsinndashMadisonMadison Wisconsin
Matthew Whitehead MDRadiologistChildrenrsquos National Medical CenterWashington DC
Lynne A Wolfe MS CRNPSenior Nurse PractitionerUndiagnosed Disorders ProgramNational Human Genome Research Institute National
Institutes of HealthBethesda Maryland
Robert A Zimmerman MDProfessor of RadiologyRaymond and Ruth Perelman School of Medicine at the
University of PennsylvaniaChiefDivision of Neuroradiology and MRIThe Childrenrsquos Hospital of PhiladelphiaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Preface
This edition of Inherited Metabolic Epilepsies is a greatly expanded and updated version of the fi rst Following a rousing response to the fi rst edition far beyond any anticipated measure it was clear that a reexamination of the material taking into account many helpful sug-gestions that I received from readers far and wide was in order Despite my own misgivings that books are no longer fashionable and are largely replaced by journals and online sources that lend themselves to periodic if not continual updating there remains an appetite and clamor for books that accomplish what I had hoped to do originally and aim to achieve to a greater extent in this edition to encapsulate a burgeoning fi eld suf-fi ciently that a student practitioner or investigator can turn to the source with confi dence that the neces-sary background as well as detail will be available to reward the search for information and also move the fi eld forward
The fi rst edition of this monograph was born follow-ing the organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the annual meeting of the American Epilepsy Society in Boston in 2009 At the time of proposing the topic I was wrestling with a chasmic gap between the fascinat-ing disorders being discussed at the geneticndashmetabolic meetings and the advancing wave in epilepsy classifi ca-tion diagnosis and treatment occupying the meetings attended by members of the societies associated with neurology and epilepsy At that time a storybook series of investigations elucidated not only the surprising antiq-uitin defect in pyridoxine-dependent epilepsy but also the highly charged requirement that physicians consider a pivotal role for folinic acid and pyridoxal-5-phosphate in patients with virtually the same clinical presentation I also perceived a relative lack of awareness of disorders such as glucose transporter 1 defi ciency serine synthetic defects developmental delay epilepsy and neonatal dia-betes (DEND) and hyperinsulinismndashhyperammonemia (HIndashHA) that had very specifi c therapeutic implications with potential for dramatically improving outcome but with an even greater likelihood that they were escaping diagnosis
Overall the inherited metabolic epilepsies repre-sent a group of disorders that is rare individually but
in aggregate represents a substantial clinical burden as well as a vexing area for physicians investigators and students to master The sheer amount and complexity of information are overwhelming and require the physician to synthesize key concepts in neurology genetics and epilepsy As a pediatric epileptologist and medical edu-cator I have found this area among the most challenging and rewarding in practice and research The fi rst edition organized the disorders in a traditional approach under the roof of metabolism by dividing them into small- and large-molecule disorders In the Preface to that edition there was an explanation of various ways of organizing these disorders some more user friendly to the neurol-ogist than the small- versus large-molecule divide but this was an opportunity to present that way of thinking to the neurologist which brings this clinical specialty closer to that of genetics metabolism
In this second edition there is an expansion from four sections (General Principles Small Molecule Diseases Large Molecule Diseases and Conclusions) to six sec-tions with the addition of chapters in basic science and clinical science of the metabolic epilepsies The book has been expanded from 28 to 43 chapters with new chapters including overviews of metabolic disease and the basic science of metabolic epilepsy plus new topics such as metabolic energetics and implications of vital pathways A full chapter is devoted to the mechanistic target of rapamycin (mTOR) pathway that regulates cell replica-tion and so much of homeostasis and new pathophysi-ologic mechanisms such as protein anchoring disorders There are new chapters on neurotransmitter transmission measurement using transcranial magnetic stimulation genomic technologies and approaches to diagnosis and therapy referable to this group of disorders The clinical science section now includes a marvelous and refl ective chapter on neuropathology by Harvey B Sarnat There are new chapters devoted to specifi c disorders such as pyridoxal-5-phosphate dependency and Menkesrsquo disease There are chapters with completely new vantage points from community and family resources to an emphasis on adult patients the latter being the most commonly requested area to cover that I receive after giving talks on the subject In addition the prior chapters from the fi rst edition have been revised and updated
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xviii
Hence what began as a quest to increase awareness of treatable metabolic epilepsies fi rst became a mono-graph to give some form to this arena and has now been enlarged and updated to a second edition It is hoped that this will provide a resource to in some way lead the fi eld and carry it forward It is truly hoped that this book will educate if not enlighten physicians particularly
specialists and trainees in pediatric and adult neurology neurodevelopmental disabilities epilepsy and genetics while caring for patients with inherited metabolic epi-lepsies as well as spur further research into basic mecha-nisms and clinical trials in this group of maladies
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Acknowledgments
This book was fi rst suggested to me by Beth Barry from Demos Medical Publishers following my organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the American Epilepsy Society 2009 meeting Beth was a driving force for the creation of this second edition and she and Young Kim at Demos now aligned with Springer are gratefully acknowledged for unmatched hard work and persever-ance in seeing this through to completion
My education in child neurology and epilepsy is grounded by great mentors including Ralph D Feigin MD in pediatrics and Marvin A Fishman MD in pediat-ric neurology of Baylor College of Medicine in Houston and Gregory L Holmes MD in epilepsy and clinical neurophysiology then at Childrenrsquos Hospital Harvard Medical School in Boston I wish to take this opportunity to acknowledge these teachers of mine
My foray into metabolic disorders has been made pos-sible by the always helpful brilliant and steadfast work of Mike Gibson PhD whose collaboration in the area of gamma-amino butyric acid (GABA) disorders specifi -cally succinic-semialdehyde dehydrogenase (SSADH) defi ciency has been a constant source of intellectual
nourishment and encouragement My career during the two editions of this book has now spanned two great childrenrsquos hospitals Childrenrsquos National and Boston Childrenrsquos and the insight and support of colleagues at both institutions have been fundamental to this work Ongoing collaborations with Mike Gibson as well as William H Theodore MD chief of the Clinical Epilepsy Section at the NINDS have been critical to the ongoing investigative work on metabolic epilepsies
I thank each of the contributors to the fi rst edition of this book for revising and updating their chapters and each of the authors of the new chapters resulting in a signifi cant expansion The outstanding assistance of Alisa Marino is gratefully acknowledged given the enormous complexity of the project and the organiza-tional skills needed to accomplish this and a myriad of other tasks As a group I thank the many patients and families as well as students residents and fellows who inspire our work I thank my own family who as with all of us shoulder the largest burden of personal sacrifi ce and inspire us the most
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

Inherited Metabolic Epilepsies
Second Edition
Editor
Phillip L Pearl MDDirector of Epilepsy and Clinical Neurophysiology
William G Lennox Chair Boston Childrenrsquos HospitalProfessor of Neurology
Harvard Medical SchoolBoston Massachusetts
An Imprint of Springer Publishing
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Visit our website at wwwspringerpubcom
ISBN 9780826168634e-book ISBN 9780826168641
Acquisitions Editor Beth BarryCompositor Exeter Premedia Services Private Ltd
Copyright copy 2018 Springer Publishing CompanyDemos Medical Publishing is an imprint of Springer Publishing Company LLC
All rights reserved This book is protected by copyright No part of it may be reproduced stored in a retrieval system or transmitted in any form or by any means electronic mechanical photocopying recording or otherwise without the prior written permission of the publisher
Medicine is an ever-changing science Research and clinical experience are continually expanding our knowledge in particular our understanding of proper treatment and drug therapy The authors editors and publisher have made every effort to ensure that all information in this book is in accordance with the state of knowledge at the time of pro-duction of the book Nevertheless the authors editors and publisher are not responsible for errors or omissions or for any consequences from application of the information in this book and make no warranty expressed or implied with respect to the contents of the publication Every reader should examine carefully the package inserts accompanying each drug and should carefully check whether the dosage schedules mentioned therein or the contraindications stated by the manufacturer differ from the statements made in this book Such examination is particularly important with drugs that are either rarely used or have been newly released on the market
Library of Congress Cataloging-in-Publication Data
Names Pearl Phillip L editorTitle Inherited metabolic epilepsies editor Phillip L PearlDescription Second edition | New York Demos [2018] | Includes bibliographical references and indexIdentifi ers LCCN 2017031804| ISBN 9780826168634 | ISBN 9780826168641 (e-book)Subjects | MESH Epilepsymdashetiology | Brain Diseases Metabolic Inbornmdashcomplications | Epilepsymdashdiagnosis | Brain Diseases Metabolic Inbornmdashdiagnosis | Epilepsymdashtherapy | Brain Diseases Metabolic InbornmdashtherapyClassifi cation LCC RC372 | NLM WL 385 | DDC 616853mdashdc23LC record available at httpslccnlocgov2017031804
Contact us to receive discount rates on bulk purchases We can also customize our books to meet your needs
For more information please contact salesspringerpubcom
Printed in the United States of America by Sheridan Books Inc17 18 19 20 21 5 4 3 2 1
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This book is dedicated to my wife Maria Tartaglia Pearl MD whose sacrifi ces for my work are fortunately outmatched
by our mutual love for medicine
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Contents
Contributors xiPreface xvii
Acknowledgments xix
PART I GENERAL PRINCIPLES 1 Recognition Scope and Implications of Inherited Metabolic Epilepsies 2
Phillip L Pearl
2 Overview of Inherited Metabolic Disease 16Lance H Rodan and Gerard T Berry
3 Treatable Inherited Metabolic Epilepsies Diagnoses Not to Miss 40Phillip L Pearl and Mohammed Almuqbil
PART II BASIC SCIENCE IN METABOLIC EPILEPSIES 4 Metabolic Epilepsies Principles and Mechanisms 56
Carl E Stafstrom and Jong M Rho
5 Metabolic Energetics in Epilepsy 74Ashwini Sri Hari and Manisha Patel
6 Pathways Dysregulation of mTOR and Epilepsy 86Darius Ebrahimi-Fakhari Jonathan Lipton and Mustafa Sahin
7 Protein Anchoring as an Important Mechanism in Early Onset Epilepsy Glycosylphosphatidylinositol (GPI) Defi ciency Syndromes 98Gali Heimer Bruria Ben-Zeev and Yair Anikster
PART III CLINICAL SCIENCE IN METABOLIC EPILEPSIES 8 Neuroimaging in the Metabolic Epilepsies 110
Robert A Zimmerman and Zarir P Khademian
9 Advances in MR Spectroscopy for Inherited Epilepsies 125Andrew Breeden Morgan J Prust Stanley T Fricke Matthew Whitehead and Andrea L Gropman
10 Neuropathology of Metabolic Epilepsies Novel Aspects in Children and the Diagnostic Role of Skin Biopsy 135Harvey B Sarnat
11 Electroencephalography in the Metabolic Epilepsies 149Samata Singhi Mona Alduligan and Phillip L Pearl
Share Inherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
viii
12 Genomic Technologies in Clinical Practice 187Christina Y Hung and Olaf A Bodamer
13 Measures of Cortical Excitability by Transcranial Magnetic Stimulation 201Alexander Rotenberg
14 Ketogenic Diet in Metabolic Epilepsies 207Susan L Fong and Eric H Kossoff
PART IV SMALL MOLECULE DISEASES 15 Amino and Organic Acid Disorders and Epilepsy 218
Kimberly A Chapman and Jamie L Fraser
16 Fatty Acid Oxidation Disorders and Epilepsy 237Dimitar Gavrilov and Dietrich Matern
17 Urea Cycle Disorders and Epilepsy 257Debra S Regier Brendan Lanpher and Marshall L Summar
18 Mitochondrial Diseases and Epilepsy 267Sumit Parikh Lynne A Wolfe and Andrea L Gropman
19 Pyridoxine-Dependent Epilepsy 275Sidney M Gospe Jr
20 Pyridoxamine 5acute-Phosphate Oxidase (PNPO) Defi ciency 287Barbara Plecko-Startinig
21 Tetrahydrobiopterin Defi ciencies and Epilepsy 293Nenad Blau and Thomas Opladen
22 Disorders of GABA Metabolism and Epilepsy 301Phillip L Pearl Kara Vogel and K Michael Gibson
23 Glucose Transporter Type 1 Defi ciency Syndrome 313Cigdem I Akman and Darryl C De Vivo
24 Thiamine Transporter Defi ciency and Epilepsy 326Brahim Tabarki
25 DEND Syndrome Developmental Delay Epilepsy and Neonatal Diabetes a Potassium Channelopathy 333Carolina Lahmann and Frances Ashcroft
26 HyperammonemiaHyperinsulinism Syndrome and Epilepsy 345Nicholas S Abend and Andrea Kelly
27 Glycine Encephalopathy and Epilepsy 353Julia B Hennermann Johan L K Van Hove and Curtis R Coughlin II
28 Serine Synthesis Disorders and Epilepsy 364T J de Koning
29 LeschndashNyhan Disease and Epilepsy 371Beth A Leeman-Markowski and Hyder A Jinnah
30 Sulfi te Oxidase Defi ciencyMolybdenum Cofactor Defi ciency and Epilepsy 394Joumlrn Oliver Sass and Barbara Plecko-Startinig
31 Creatine Disorders and Epilepsy 401Ton de Grauw
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
32 Cerebral Folate Defi ciency and Epilepsy 407Robert Steinfeld
33 Menkesrsquo Disease and Infantile Epilepsy 415Asuri N Prasad
PART V LARGE MOLECULE DISEASES 34 Congenital Disorders of Glycosylation and Epilepsy 428
Susan E Sparks
35 Lysosomal Storage Diseases and Epilepsy 445Pranoot Tanpaiboon and Grisel Lopez
36 Peroxisomal Diseases and Epilepsy 473Parastoo Jangouk Kristin W Barantildeano and Gerald V Raymond
37 Leukodystrophies and Epilepsy 483Davide Tonduti and Adeline Vanderver
PART VI CONCLUSIONS 38 Diagnostic Approaches to Genetic Epilepsies 490
Erika Takle Axeen Christelle El Achkar and Annapurna Poduri
39 Therapeutic Approaches to Inherited Metabolic Epilepsies 497Brandy Verhalen and Berge A Minassian
40 Inherited Metabolic Epilepsies in Adults 503Phillip L Pearl
41 Genetic Counseling in Metabolic Epilepsies 508Jodie M Vento
42 Support and Resources for Patients and Families With Inherited Metabolic Epilepsies 518Christopher Ryan and Jennifer Jeffs
43 Clinical Approach to Inherited Metabolic Epilepsies 525Scott Demarest Anna Lecticia Pinto and Phillip L Pearl
Index 529
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Contributors
Nicholas S Abend MD MSCEAssociate Professor of Neurology and PediatricsDepartments of Neurology and PediatricsChildrenrsquos Hospital of Philadelphia and the University
of PennsylvaniaPhiladelphia Pennsylvania
Christelle El Achkar MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Cigdem I Akman MDAssociate Professor of Clinical Neurology and PediatricsDepartments of Neurology and PediatricsDivision of Pediatric NeurologyInterim ChiefChild NeurologyDirectorPediatric EpilepsyColumbia University College of Physicians and SurgeonsNew York New York
Mona Alduligan MDPhysicianDivision of Clinical NeurophysiologyChildrenrsquos National Medical CenterWashington DC
Mohammed Almuqbil MD FRCP (C)King Abdullah Specialist Childrenrsquos Hospital (KASCH)King Saud bin Abdulaziz University for Health Sciences
(KSAU-HS)Pediatric Neurology DivisionRiyadh Saudi ArabiaKing Abdullah International Medical Research Center
(KAIMRC)National Guard MinistryRiyadh Saudi ArabiaDivision of Genetics and GenomicsBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Yair Anikster MD PhDDirectorMetabolic Disease UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
Frances Ashcroft PhD ScDGlaxoSmithKline Royal Society Research ProfessorDepartment of Physiology Anatomy and GeneticsFellow of Trinity CollegeDirector OXIONUniversity of OxfordOxford England
Erika Takle Axeen MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Minnesota
Kristin W Barantildeano MD PhDClinical AssociatePediatric NeurologyDepartment of NeurologyJohns Hopkins HospitalAssistant Professor of NeurologyJohns Hopkins School of MedicineBaltimore Maryland
Bruria Ben-Zeev MDDirectorPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xii
Gerard T Berry MDDirector Metabolism ProgramProfessor of PediatricsBoston Childrenrsquos HospitalBoston Massachusetts
Nenad Blau PhDSenior Consultant in Biochemical GeneticsProfessor Emeritus of Clinical Biochemistry (UZH)Dietmar-Hopp Metabolic CenterUniversity Childrenrsquos HospitalHeidelberg Germany
Olaf A Bodamer MD PhDAssociate Chief of Genetics and GenomicsBoston Childrenrsquos HospitalPark Gerald Chair in Genetics and GenomicsHarvard Medical SchoolBoston Massachusetts
Andrew Breeden PhDProgram AnalystHealth Program SpecialistNational Institute of Neurological Disorders and
Stroke (NINDS)Bethesda Maryland
Kimberly A Chapman MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National
Health SystemWashington DC
Curtis R Coughlin II MS MBe CGCAssistant Professor of PediatricsSection of Clinical Genetics and MetabolismDepartment of PediatricsUniversity of ColoradoAurora Colorado
Ton de Grauw MD PhDChiefNeurosciencesChildrenrsquos Healthcare of AtlantaDirectorPediatric NeurologyEmory University School of MedicineAtlanta Georgia
T J de Koning MD PhDPaediatrician for Inborn Errors of MetabolismDepartment of Genetics and PaediatricsUniversity Medical Centre GroningenUniversity of GroningenGroningen The Netherlands
Darryl C De Vivo MDSidney Carter Professor of NeurologyProfessor of PediatricsPediatric Neurology ServiceFounding DirectorColleen Giblin Research Laboratories for Pediatric
NeurologyAssociate ChairmanPediatric Neurosciences and Developmental
NeurobiologyCo-DirectorMotor Neuron CenterDirectorSpinal Muscular Atrophy (SMA) CenterChief EmeritusPediatric NeurologyColumbia University Medical CenterNew York New York
Scott Demarest MDAssistant Professor of Pediatrics and NeurologyChildrenrsquos Hospital ColoradoUniversity of ColoradoAurora Colorado
Darius Ebrahimi-Fakhari MD DrmedResident PhysicianDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Susan L Fong MD PhDAssistant ResidentPediatric NeurologyJohns Hopkins HospitalBaltimore Maryland
Jamie L Fraser MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National Health
SystemWashington DC
Stanley T Fricke PhDPhysicistChildrenrsquos National Medical CenterWashington DC
Dimitar Gavrilov MD PhDAssistant ProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
K Michael Gibson PhDAllen I White Distinguished Professor and ChairDepartment of PharmacotherapyWashington State University College of PharmacySpokane Washington
Sidney M Gospe Jr MD PhDHerman and Faye Sarkowsky Endowed ChairProfessor and HeadDivision of Pediatric NeurologyDepartments of Neurology and PediatricsUniversity of WashingtonDivision of NeurologySeattle Childrenrsquos Hospital and Seattle Childrenrsquos
Research InstituteSeattle Washington
Andrea L Gropman MDChief Neurogenetics and Neurodevelopmental
PediatricsChildrenrsquos National Medical CenterAssociate Professor of Neurology and PediatricsGeorge Washington School of Medicine and Health
SciencesWashington DC
Ashwini Sri Hari PhD CandidateDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Gali Heimer MD PhDSenior Physician and Director of the Angelman ClinicPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical Center Tel-Hashomer Israel Sackler Faculty of MedicineTel-Aviv UniversityTel-Aviv IsraelMember of the Dr Pinchas Borenstein Talpiot Medical
Leadership ProgramSheba Medical CenterTel-Hashomer Israel
Julia B Hennermann MDProfessor of Metabolic DiseasesUniversity Medical Center MainzVilla Metabolica Department of Pediatric and
Adolescent MedicineMainz Germany
Christina Y Hung MDResearch AssociateHMS Instructor in PediatricsDivision for Human Genetics and GenomicsBoston Childrenrsquos HospitalBoston Massachusetts
Parastoo Jangouk MDGastroenterology and Hepatology FellowYale-New Haven HospitalNew Haven Connecticut
Jennifer Jeffs LICSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Hyder A Jinnah MD PhDProfessorDepartments of Neurology Human Genetics and
PediatricsEmory University School of MedicineAtlanta Georgia
Andrea Kelly MD MSCEAssociate Professor of Pediatrics CEDepartment of PediatricsChildrenrsquos Hospital of Philadelphia and Perelman School
of Medicine of the University of PennsylvaniaPhiladelphia Pennsylvania
Zarir P Khademian MD PhDAssistant Professor of Radiology and PediatricsStaff Neurologist Division of Diagnostic Imaging and
RadiologyChildrenrsquos National Medical CenterWashington DC
Eric H Kossoff MDProfessorNeurology and PediatricsJohns Hopkins HospitalBaltimore Maryland
Carolina Lahmann PhDPostdoctoral FellowHarvard Medical SchoolBoston Massachusetts
Brendan Lanpher MDAssistant Professor of Medical GeneticsDepartment of Clinical GenomicsMayo ClinicRochester Minnesota
Beth A Leeman-Markowski MD MA MMScAssistant ProfessorDepartment of NeurologyNew York UniversityInvestigatorResearch ServiceVA New York Harbor Healthcare SystemmdashManhattan
CampusNew York New York
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xiv
Jonathan Lipton MD PhDAssistant Professor of NeurologyDepartment of Neurology and F M Kirby Center for
NeuroscienceBoston Childrenrsquos Hospital Harvard Medical SchoolBoston Massachusetts
Grisel Lopez MDSenior Staff ClinicianNational Human Genome Research InstituteNational Institutes of HealthBethesda Maryland
Dietrich Matern MD PhDProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
Berge A Minassian MDDivision ChiefPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas TexasUniversity of TorontoToronto Ontario Canada
Thomas Opladen MDDivision of Child Neurology and Metabolic DiseasesUniversity Childrenlsquos Hospital Heidelberg Germany
Sumit Parikh MDDirector of Cleveland Clinic Neurogenetics Metabolic
amp Mitochondrial Disease ProgramCleveland ClinicAssociate ProfessorDepartment of PediatricsCase Western Reserve University School of MedicineCleveland Ohio
Manisha Patel PhDProfessorDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Phillip L Pearl MDDirector of Epilepsy and Clinical NeurophysiologyWilliam G Lennox ChairBoston Childrenrsquos HospitalProfessor of NeurologyHarvard Medical SchoolBoston Massachusetts
Anna Lecticia Pinto MDAssistant in Neurology and Co-DirectorSturge Weber Clinic Boston Childrenrsquos HospitalLecturer of NeurologyHarvard Medical SchoolBoston Massachusetts
Barbara Plecko-Startinig MDHeadDivision of Child NeurologyChildrenrsquos Hospital ZurichProfessor of Child NeurologyUniversity of ZurichZurich Switzerland
Annapurna Poduri MD MPHEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Asuri N Prasad MBBS MD FRCPC FRCPEProfessor in Pediatrics and Clinical NeurosciencesDivision of Pediatric NeurologyDepartment of PediatricsSchulich School of Medicine and DentistryChildrenrsquos Hospital London Health Sciences CentreWestern UniversityLondon Ontario Canada
Morgan J Prust MDClinical Fellow in NeurologyDepartment of NeurologyMassachusetts General HospitalBrigham amp Womenrsquos HospitalBoston Massachusetts
Gerald V Raymond MDProfessorDepartment of NeurologyUniversity of Minnesota Medical SchoolMinneapolis Minnesota
Debra S Regier MD PhDDirector of Genetic and Genomic Education Medical
GeneticistRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Jong M Rho MDProfessor of Pediatrics Clinical Neurosciences
Physiology and PharmacologyDr Robert Haslam Chair in Child NeurologySection of Paediatric NeurologyCumming School of Medicine University of CalgaryAlberta Childrenrsquos HospitalCalgary Alberta Canada
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Lance H Rodan MDStaff PhysicianBoston Childrenrsquos HospitalBoston Massachusetts
Alexander Rotenberg MD PhDDirector Neuromodulation ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalAssociate Professor of NeurologyHarvard Medical SchoolBoston Massachusetts
Christopher Ryan LCSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Mustafa Sahin MD PhDProfessor of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Harvey B Sarnat MS MD FRCPCProfessor Departments of Paediatrics Pathology
(Neuropathology) and Clinical NeurosciencesUniversity of Calgary Cumming School of Medicine
and Alberta Childrenrsquos Hospital Research InstituteCalgary Alberta Canada
Joumlrn Oliver Sass Dr rer natProfessor of Bioanalytics and BiochemistryDepartment of Natural SciencesBonn-Rhein-Sieg University of Applied SciencesSankt Augustin Germany
Samata Singhi MDClinical Fellow in NeurologyDepartment of NeurologyBoston Childrenrsquos HospitalBoston Massachusetts
Susan E Sparks MD PhDMedical DirectorNA Medical AffairsRare DiseasesSanofi GenzymeCambridge Massachusetts
Carl E Stafstrom MD PhDProfessor of Neurology and PediatricsLederer Chair in Pediatric EpilepsyDirector Division of Pediatric NeurologyJohns Hopkins University School of MedicineBaltimore Maryland
Robert Steinfeld MD PhDProfessor of Neurometabolic and Neurodegenerative
Diseases in Childhood and AdolescenceDepartment of Pediatrics and Pediatric NeurologyUniversity Medical Center GoumlttingenGoumlttingen Germany
Marshall L Summar MDChief Division of Genetics and MetabolismMargaret OrsquoMalley Chair of Genetic MedicineRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Brahim Tabarki MDDivision of Pediatric NeurologyPrince Sultan Military Medical CityRiyadh Saudi ArabiaAssociate Professor of Neurology and PediatricsThe Ibn El Jazzar University School of MedicineSousse Tunisia
Pranoot Tanpaiboon MDAssociate Professor of PediatricsDivision of Genetics and MetabolismThe George Washington University School of Medicine
and Health SciencesChildrenrsquos National Health System Childrenrsquos National
Rare Disease InstituteWashington DC
Davide Tonduti MDChild NeurologistDepartment of Child NeurologyFondazione IRCCS Istituto Neurologico Carlo BestaMilano Italy
Johan L K Van Hove MD PhDProfessor of PediatricsSection of Clinical Genetics and Metabolism
Department of PediatricsUniversity of ColoradoAurora Colorado
Adeline Vanderver MDAttending PhysicianDivision of NeurologyProgram DirectorLeukodystrophy CenterJacob A Kamens Endowed Chair in Neurologic
Disorders and Translational NeurotherapeuticsChildrenrsquos Hospital of PhiladelphiaAssociate Professor of NeurologyPerelman School of Medicine at the University of
PennsylvaniaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xvi
Jodie M Vento MGC LCGCManagerCenter for Rare Disease TherapyManagerBrain Care InstituteManagerLaboratory Genetic Counseling ServicesChildrenrsquos Hospital of Pittsburgh of UPMCPittsburgh Pennsylvania
Brandy Verhalen PhDLab ManagerPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas Texas
Kara Vogel PhDPostdoctoral Research AssociateUniversity of WisconsinndashMadisonMadison Wisconsin
Matthew Whitehead MDRadiologistChildrenrsquos National Medical CenterWashington DC
Lynne A Wolfe MS CRNPSenior Nurse PractitionerUndiagnosed Disorders ProgramNational Human Genome Research Institute National
Institutes of HealthBethesda Maryland
Robert A Zimmerman MDProfessor of RadiologyRaymond and Ruth Perelman School of Medicine at the
University of PennsylvaniaChiefDivision of Neuroradiology and MRIThe Childrenrsquos Hospital of PhiladelphiaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Preface
This edition of Inherited Metabolic Epilepsies is a greatly expanded and updated version of the fi rst Following a rousing response to the fi rst edition far beyond any anticipated measure it was clear that a reexamination of the material taking into account many helpful sug-gestions that I received from readers far and wide was in order Despite my own misgivings that books are no longer fashionable and are largely replaced by journals and online sources that lend themselves to periodic if not continual updating there remains an appetite and clamor for books that accomplish what I had hoped to do originally and aim to achieve to a greater extent in this edition to encapsulate a burgeoning fi eld suf-fi ciently that a student practitioner or investigator can turn to the source with confi dence that the neces-sary background as well as detail will be available to reward the search for information and also move the fi eld forward
The fi rst edition of this monograph was born follow-ing the organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the annual meeting of the American Epilepsy Society in Boston in 2009 At the time of proposing the topic I was wrestling with a chasmic gap between the fascinat-ing disorders being discussed at the geneticndashmetabolic meetings and the advancing wave in epilepsy classifi ca-tion diagnosis and treatment occupying the meetings attended by members of the societies associated with neurology and epilepsy At that time a storybook series of investigations elucidated not only the surprising antiq-uitin defect in pyridoxine-dependent epilepsy but also the highly charged requirement that physicians consider a pivotal role for folinic acid and pyridoxal-5-phosphate in patients with virtually the same clinical presentation I also perceived a relative lack of awareness of disorders such as glucose transporter 1 defi ciency serine synthetic defects developmental delay epilepsy and neonatal dia-betes (DEND) and hyperinsulinismndashhyperammonemia (HIndashHA) that had very specifi c therapeutic implications with potential for dramatically improving outcome but with an even greater likelihood that they were escaping diagnosis
Overall the inherited metabolic epilepsies repre-sent a group of disorders that is rare individually but
in aggregate represents a substantial clinical burden as well as a vexing area for physicians investigators and students to master The sheer amount and complexity of information are overwhelming and require the physician to synthesize key concepts in neurology genetics and epilepsy As a pediatric epileptologist and medical edu-cator I have found this area among the most challenging and rewarding in practice and research The fi rst edition organized the disorders in a traditional approach under the roof of metabolism by dividing them into small- and large-molecule disorders In the Preface to that edition there was an explanation of various ways of organizing these disorders some more user friendly to the neurol-ogist than the small- versus large-molecule divide but this was an opportunity to present that way of thinking to the neurologist which brings this clinical specialty closer to that of genetics metabolism
In this second edition there is an expansion from four sections (General Principles Small Molecule Diseases Large Molecule Diseases and Conclusions) to six sec-tions with the addition of chapters in basic science and clinical science of the metabolic epilepsies The book has been expanded from 28 to 43 chapters with new chapters including overviews of metabolic disease and the basic science of metabolic epilepsy plus new topics such as metabolic energetics and implications of vital pathways A full chapter is devoted to the mechanistic target of rapamycin (mTOR) pathway that regulates cell replica-tion and so much of homeostasis and new pathophysi-ologic mechanisms such as protein anchoring disorders There are new chapters on neurotransmitter transmission measurement using transcranial magnetic stimulation genomic technologies and approaches to diagnosis and therapy referable to this group of disorders The clinical science section now includes a marvelous and refl ective chapter on neuropathology by Harvey B Sarnat There are new chapters devoted to specifi c disorders such as pyridoxal-5-phosphate dependency and Menkesrsquo disease There are chapters with completely new vantage points from community and family resources to an emphasis on adult patients the latter being the most commonly requested area to cover that I receive after giving talks on the subject In addition the prior chapters from the fi rst edition have been revised and updated
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xviii
Hence what began as a quest to increase awareness of treatable metabolic epilepsies fi rst became a mono-graph to give some form to this arena and has now been enlarged and updated to a second edition It is hoped that this will provide a resource to in some way lead the fi eld and carry it forward It is truly hoped that this book will educate if not enlighten physicians particularly
specialists and trainees in pediatric and adult neurology neurodevelopmental disabilities epilepsy and genetics while caring for patients with inherited metabolic epi-lepsies as well as spur further research into basic mecha-nisms and clinical trials in this group of maladies
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Acknowledgments
This book was fi rst suggested to me by Beth Barry from Demos Medical Publishers following my organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the American Epilepsy Society 2009 meeting Beth was a driving force for the creation of this second edition and she and Young Kim at Demos now aligned with Springer are gratefully acknowledged for unmatched hard work and persever-ance in seeing this through to completion
My education in child neurology and epilepsy is grounded by great mentors including Ralph D Feigin MD in pediatrics and Marvin A Fishman MD in pediat-ric neurology of Baylor College of Medicine in Houston and Gregory L Holmes MD in epilepsy and clinical neurophysiology then at Childrenrsquos Hospital Harvard Medical School in Boston I wish to take this opportunity to acknowledge these teachers of mine
My foray into metabolic disorders has been made pos-sible by the always helpful brilliant and steadfast work of Mike Gibson PhD whose collaboration in the area of gamma-amino butyric acid (GABA) disorders specifi -cally succinic-semialdehyde dehydrogenase (SSADH) defi ciency has been a constant source of intellectual
nourishment and encouragement My career during the two editions of this book has now spanned two great childrenrsquos hospitals Childrenrsquos National and Boston Childrenrsquos and the insight and support of colleagues at both institutions have been fundamental to this work Ongoing collaborations with Mike Gibson as well as William H Theodore MD chief of the Clinical Epilepsy Section at the NINDS have been critical to the ongoing investigative work on metabolic epilepsies
I thank each of the contributors to the fi rst edition of this book for revising and updating their chapters and each of the authors of the new chapters resulting in a signifi cant expansion The outstanding assistance of Alisa Marino is gratefully acknowledged given the enormous complexity of the project and the organiza-tional skills needed to accomplish this and a myriad of other tasks As a group I thank the many patients and families as well as students residents and fellows who inspire our work I thank my own family who as with all of us shoulder the largest burden of personal sacrifi ce and inspire us the most
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

Visit our website at wwwspringerpubcom
ISBN 9780826168634e-book ISBN 9780826168641
Acquisitions Editor Beth BarryCompositor Exeter Premedia Services Private Ltd
Copyright copy 2018 Springer Publishing CompanyDemos Medical Publishing is an imprint of Springer Publishing Company LLC
All rights reserved This book is protected by copyright No part of it may be reproduced stored in a retrieval system or transmitted in any form or by any means electronic mechanical photocopying recording or otherwise without the prior written permission of the publisher
Medicine is an ever-changing science Research and clinical experience are continually expanding our knowledge in particular our understanding of proper treatment and drug therapy The authors editors and publisher have made every effort to ensure that all information in this book is in accordance with the state of knowledge at the time of pro-duction of the book Nevertheless the authors editors and publisher are not responsible for errors or omissions or for any consequences from application of the information in this book and make no warranty expressed or implied with respect to the contents of the publication Every reader should examine carefully the package inserts accompanying each drug and should carefully check whether the dosage schedules mentioned therein or the contraindications stated by the manufacturer differ from the statements made in this book Such examination is particularly important with drugs that are either rarely used or have been newly released on the market
Library of Congress Cataloging-in-Publication Data
Names Pearl Phillip L editorTitle Inherited metabolic epilepsies editor Phillip L PearlDescription Second edition | New York Demos [2018] | Includes bibliographical references and indexIdentifi ers LCCN 2017031804| ISBN 9780826168634 | ISBN 9780826168641 (e-book)Subjects | MESH Epilepsymdashetiology | Brain Diseases Metabolic Inbornmdashcomplications | Epilepsymdashdiagnosis | Brain Diseases Metabolic Inbornmdashdiagnosis | Epilepsymdashtherapy | Brain Diseases Metabolic InbornmdashtherapyClassifi cation LCC RC372 | NLM WL 385 | DDC 616853mdashdc23LC record available at httpslccnlocgov2017031804
Contact us to receive discount rates on bulk purchases We can also customize our books to meet your needs
For more information please contact salesspringerpubcom
Printed in the United States of America by Sheridan Books Inc17 18 19 20 21 5 4 3 2 1
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This book is dedicated to my wife Maria Tartaglia Pearl MD whose sacrifi ces for my work are fortunately outmatched
by our mutual love for medicine
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Contents
Contributors xiPreface xvii
Acknowledgments xix
PART I GENERAL PRINCIPLES 1 Recognition Scope and Implications of Inherited Metabolic Epilepsies 2
Phillip L Pearl
2 Overview of Inherited Metabolic Disease 16Lance H Rodan and Gerard T Berry
3 Treatable Inherited Metabolic Epilepsies Diagnoses Not to Miss 40Phillip L Pearl and Mohammed Almuqbil
PART II BASIC SCIENCE IN METABOLIC EPILEPSIES 4 Metabolic Epilepsies Principles and Mechanisms 56
Carl E Stafstrom and Jong M Rho
5 Metabolic Energetics in Epilepsy 74Ashwini Sri Hari and Manisha Patel
6 Pathways Dysregulation of mTOR and Epilepsy 86Darius Ebrahimi-Fakhari Jonathan Lipton and Mustafa Sahin
7 Protein Anchoring as an Important Mechanism in Early Onset Epilepsy Glycosylphosphatidylinositol (GPI) Defi ciency Syndromes 98Gali Heimer Bruria Ben-Zeev and Yair Anikster
PART III CLINICAL SCIENCE IN METABOLIC EPILEPSIES 8 Neuroimaging in the Metabolic Epilepsies 110
Robert A Zimmerman and Zarir P Khademian
9 Advances in MR Spectroscopy for Inherited Epilepsies 125Andrew Breeden Morgan J Prust Stanley T Fricke Matthew Whitehead and Andrea L Gropman
10 Neuropathology of Metabolic Epilepsies Novel Aspects in Children and the Diagnostic Role of Skin Biopsy 135Harvey B Sarnat
11 Electroencephalography in the Metabolic Epilepsies 149Samata Singhi Mona Alduligan and Phillip L Pearl
Share Inherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
viii
12 Genomic Technologies in Clinical Practice 187Christina Y Hung and Olaf A Bodamer
13 Measures of Cortical Excitability by Transcranial Magnetic Stimulation 201Alexander Rotenberg
14 Ketogenic Diet in Metabolic Epilepsies 207Susan L Fong and Eric H Kossoff
PART IV SMALL MOLECULE DISEASES 15 Amino and Organic Acid Disorders and Epilepsy 218
Kimberly A Chapman and Jamie L Fraser
16 Fatty Acid Oxidation Disorders and Epilepsy 237Dimitar Gavrilov and Dietrich Matern
17 Urea Cycle Disorders and Epilepsy 257Debra S Regier Brendan Lanpher and Marshall L Summar
18 Mitochondrial Diseases and Epilepsy 267Sumit Parikh Lynne A Wolfe and Andrea L Gropman
19 Pyridoxine-Dependent Epilepsy 275Sidney M Gospe Jr
20 Pyridoxamine 5acute-Phosphate Oxidase (PNPO) Defi ciency 287Barbara Plecko-Startinig
21 Tetrahydrobiopterin Defi ciencies and Epilepsy 293Nenad Blau and Thomas Opladen
22 Disorders of GABA Metabolism and Epilepsy 301Phillip L Pearl Kara Vogel and K Michael Gibson
23 Glucose Transporter Type 1 Defi ciency Syndrome 313Cigdem I Akman and Darryl C De Vivo
24 Thiamine Transporter Defi ciency and Epilepsy 326Brahim Tabarki
25 DEND Syndrome Developmental Delay Epilepsy and Neonatal Diabetes a Potassium Channelopathy 333Carolina Lahmann and Frances Ashcroft
26 HyperammonemiaHyperinsulinism Syndrome and Epilepsy 345Nicholas S Abend and Andrea Kelly
27 Glycine Encephalopathy and Epilepsy 353Julia B Hennermann Johan L K Van Hove and Curtis R Coughlin II
28 Serine Synthesis Disorders and Epilepsy 364T J de Koning
29 LeschndashNyhan Disease and Epilepsy 371Beth A Leeman-Markowski and Hyder A Jinnah
30 Sulfi te Oxidase Defi ciencyMolybdenum Cofactor Defi ciency and Epilepsy 394Joumlrn Oliver Sass and Barbara Plecko-Startinig
31 Creatine Disorders and Epilepsy 401Ton de Grauw
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
32 Cerebral Folate Defi ciency and Epilepsy 407Robert Steinfeld
33 Menkesrsquo Disease and Infantile Epilepsy 415Asuri N Prasad
PART V LARGE MOLECULE DISEASES 34 Congenital Disorders of Glycosylation and Epilepsy 428
Susan E Sparks
35 Lysosomal Storage Diseases and Epilepsy 445Pranoot Tanpaiboon and Grisel Lopez
36 Peroxisomal Diseases and Epilepsy 473Parastoo Jangouk Kristin W Barantildeano and Gerald V Raymond
37 Leukodystrophies and Epilepsy 483Davide Tonduti and Adeline Vanderver
PART VI CONCLUSIONS 38 Diagnostic Approaches to Genetic Epilepsies 490
Erika Takle Axeen Christelle El Achkar and Annapurna Poduri
39 Therapeutic Approaches to Inherited Metabolic Epilepsies 497Brandy Verhalen and Berge A Minassian
40 Inherited Metabolic Epilepsies in Adults 503Phillip L Pearl
41 Genetic Counseling in Metabolic Epilepsies 508Jodie M Vento
42 Support and Resources for Patients and Families With Inherited Metabolic Epilepsies 518Christopher Ryan and Jennifer Jeffs
43 Clinical Approach to Inherited Metabolic Epilepsies 525Scott Demarest Anna Lecticia Pinto and Phillip L Pearl
Index 529
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Contributors
Nicholas S Abend MD MSCEAssociate Professor of Neurology and PediatricsDepartments of Neurology and PediatricsChildrenrsquos Hospital of Philadelphia and the University
of PennsylvaniaPhiladelphia Pennsylvania
Christelle El Achkar MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Cigdem I Akman MDAssociate Professor of Clinical Neurology and PediatricsDepartments of Neurology and PediatricsDivision of Pediatric NeurologyInterim ChiefChild NeurologyDirectorPediatric EpilepsyColumbia University College of Physicians and SurgeonsNew York New York
Mona Alduligan MDPhysicianDivision of Clinical NeurophysiologyChildrenrsquos National Medical CenterWashington DC
Mohammed Almuqbil MD FRCP (C)King Abdullah Specialist Childrenrsquos Hospital (KASCH)King Saud bin Abdulaziz University for Health Sciences
(KSAU-HS)Pediatric Neurology DivisionRiyadh Saudi ArabiaKing Abdullah International Medical Research Center
(KAIMRC)National Guard MinistryRiyadh Saudi ArabiaDivision of Genetics and GenomicsBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Yair Anikster MD PhDDirectorMetabolic Disease UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
Frances Ashcroft PhD ScDGlaxoSmithKline Royal Society Research ProfessorDepartment of Physiology Anatomy and GeneticsFellow of Trinity CollegeDirector OXIONUniversity of OxfordOxford England
Erika Takle Axeen MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Minnesota
Kristin W Barantildeano MD PhDClinical AssociatePediatric NeurologyDepartment of NeurologyJohns Hopkins HospitalAssistant Professor of NeurologyJohns Hopkins School of MedicineBaltimore Maryland
Bruria Ben-Zeev MDDirectorPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xii
Gerard T Berry MDDirector Metabolism ProgramProfessor of PediatricsBoston Childrenrsquos HospitalBoston Massachusetts
Nenad Blau PhDSenior Consultant in Biochemical GeneticsProfessor Emeritus of Clinical Biochemistry (UZH)Dietmar-Hopp Metabolic CenterUniversity Childrenrsquos HospitalHeidelberg Germany
Olaf A Bodamer MD PhDAssociate Chief of Genetics and GenomicsBoston Childrenrsquos HospitalPark Gerald Chair in Genetics and GenomicsHarvard Medical SchoolBoston Massachusetts
Andrew Breeden PhDProgram AnalystHealth Program SpecialistNational Institute of Neurological Disorders and
Stroke (NINDS)Bethesda Maryland
Kimberly A Chapman MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National
Health SystemWashington DC
Curtis R Coughlin II MS MBe CGCAssistant Professor of PediatricsSection of Clinical Genetics and MetabolismDepartment of PediatricsUniversity of ColoradoAurora Colorado
Ton de Grauw MD PhDChiefNeurosciencesChildrenrsquos Healthcare of AtlantaDirectorPediatric NeurologyEmory University School of MedicineAtlanta Georgia
T J de Koning MD PhDPaediatrician for Inborn Errors of MetabolismDepartment of Genetics and PaediatricsUniversity Medical Centre GroningenUniversity of GroningenGroningen The Netherlands
Darryl C De Vivo MDSidney Carter Professor of NeurologyProfessor of PediatricsPediatric Neurology ServiceFounding DirectorColleen Giblin Research Laboratories for Pediatric
NeurologyAssociate ChairmanPediatric Neurosciences and Developmental
NeurobiologyCo-DirectorMotor Neuron CenterDirectorSpinal Muscular Atrophy (SMA) CenterChief EmeritusPediatric NeurologyColumbia University Medical CenterNew York New York
Scott Demarest MDAssistant Professor of Pediatrics and NeurologyChildrenrsquos Hospital ColoradoUniversity of ColoradoAurora Colorado
Darius Ebrahimi-Fakhari MD DrmedResident PhysicianDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Susan L Fong MD PhDAssistant ResidentPediatric NeurologyJohns Hopkins HospitalBaltimore Maryland
Jamie L Fraser MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National Health
SystemWashington DC
Stanley T Fricke PhDPhysicistChildrenrsquos National Medical CenterWashington DC
Dimitar Gavrilov MD PhDAssistant ProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
K Michael Gibson PhDAllen I White Distinguished Professor and ChairDepartment of PharmacotherapyWashington State University College of PharmacySpokane Washington
Sidney M Gospe Jr MD PhDHerman and Faye Sarkowsky Endowed ChairProfessor and HeadDivision of Pediatric NeurologyDepartments of Neurology and PediatricsUniversity of WashingtonDivision of NeurologySeattle Childrenrsquos Hospital and Seattle Childrenrsquos
Research InstituteSeattle Washington
Andrea L Gropman MDChief Neurogenetics and Neurodevelopmental
PediatricsChildrenrsquos National Medical CenterAssociate Professor of Neurology and PediatricsGeorge Washington School of Medicine and Health
SciencesWashington DC
Ashwini Sri Hari PhD CandidateDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Gali Heimer MD PhDSenior Physician and Director of the Angelman ClinicPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical Center Tel-Hashomer Israel Sackler Faculty of MedicineTel-Aviv UniversityTel-Aviv IsraelMember of the Dr Pinchas Borenstein Talpiot Medical
Leadership ProgramSheba Medical CenterTel-Hashomer Israel
Julia B Hennermann MDProfessor of Metabolic DiseasesUniversity Medical Center MainzVilla Metabolica Department of Pediatric and
Adolescent MedicineMainz Germany
Christina Y Hung MDResearch AssociateHMS Instructor in PediatricsDivision for Human Genetics and GenomicsBoston Childrenrsquos HospitalBoston Massachusetts
Parastoo Jangouk MDGastroenterology and Hepatology FellowYale-New Haven HospitalNew Haven Connecticut
Jennifer Jeffs LICSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Hyder A Jinnah MD PhDProfessorDepartments of Neurology Human Genetics and
PediatricsEmory University School of MedicineAtlanta Georgia
Andrea Kelly MD MSCEAssociate Professor of Pediatrics CEDepartment of PediatricsChildrenrsquos Hospital of Philadelphia and Perelman School
of Medicine of the University of PennsylvaniaPhiladelphia Pennsylvania
Zarir P Khademian MD PhDAssistant Professor of Radiology and PediatricsStaff Neurologist Division of Diagnostic Imaging and
RadiologyChildrenrsquos National Medical CenterWashington DC
Eric H Kossoff MDProfessorNeurology and PediatricsJohns Hopkins HospitalBaltimore Maryland
Carolina Lahmann PhDPostdoctoral FellowHarvard Medical SchoolBoston Massachusetts
Brendan Lanpher MDAssistant Professor of Medical GeneticsDepartment of Clinical GenomicsMayo ClinicRochester Minnesota
Beth A Leeman-Markowski MD MA MMScAssistant ProfessorDepartment of NeurologyNew York UniversityInvestigatorResearch ServiceVA New York Harbor Healthcare SystemmdashManhattan
CampusNew York New York
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xiv
Jonathan Lipton MD PhDAssistant Professor of NeurologyDepartment of Neurology and F M Kirby Center for
NeuroscienceBoston Childrenrsquos Hospital Harvard Medical SchoolBoston Massachusetts
Grisel Lopez MDSenior Staff ClinicianNational Human Genome Research InstituteNational Institutes of HealthBethesda Maryland
Dietrich Matern MD PhDProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
Berge A Minassian MDDivision ChiefPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas TexasUniversity of TorontoToronto Ontario Canada
Thomas Opladen MDDivision of Child Neurology and Metabolic DiseasesUniversity Childrenlsquos Hospital Heidelberg Germany
Sumit Parikh MDDirector of Cleveland Clinic Neurogenetics Metabolic
amp Mitochondrial Disease ProgramCleveland ClinicAssociate ProfessorDepartment of PediatricsCase Western Reserve University School of MedicineCleveland Ohio
Manisha Patel PhDProfessorDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Phillip L Pearl MDDirector of Epilepsy and Clinical NeurophysiologyWilliam G Lennox ChairBoston Childrenrsquos HospitalProfessor of NeurologyHarvard Medical SchoolBoston Massachusetts
Anna Lecticia Pinto MDAssistant in Neurology and Co-DirectorSturge Weber Clinic Boston Childrenrsquos HospitalLecturer of NeurologyHarvard Medical SchoolBoston Massachusetts
Barbara Plecko-Startinig MDHeadDivision of Child NeurologyChildrenrsquos Hospital ZurichProfessor of Child NeurologyUniversity of ZurichZurich Switzerland
Annapurna Poduri MD MPHEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Asuri N Prasad MBBS MD FRCPC FRCPEProfessor in Pediatrics and Clinical NeurosciencesDivision of Pediatric NeurologyDepartment of PediatricsSchulich School of Medicine and DentistryChildrenrsquos Hospital London Health Sciences CentreWestern UniversityLondon Ontario Canada
Morgan J Prust MDClinical Fellow in NeurologyDepartment of NeurologyMassachusetts General HospitalBrigham amp Womenrsquos HospitalBoston Massachusetts
Gerald V Raymond MDProfessorDepartment of NeurologyUniversity of Minnesota Medical SchoolMinneapolis Minnesota
Debra S Regier MD PhDDirector of Genetic and Genomic Education Medical
GeneticistRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Jong M Rho MDProfessor of Pediatrics Clinical Neurosciences
Physiology and PharmacologyDr Robert Haslam Chair in Child NeurologySection of Paediatric NeurologyCumming School of Medicine University of CalgaryAlberta Childrenrsquos HospitalCalgary Alberta Canada
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Lance H Rodan MDStaff PhysicianBoston Childrenrsquos HospitalBoston Massachusetts
Alexander Rotenberg MD PhDDirector Neuromodulation ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalAssociate Professor of NeurologyHarvard Medical SchoolBoston Massachusetts
Christopher Ryan LCSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Mustafa Sahin MD PhDProfessor of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Harvey B Sarnat MS MD FRCPCProfessor Departments of Paediatrics Pathology
(Neuropathology) and Clinical NeurosciencesUniversity of Calgary Cumming School of Medicine
and Alberta Childrenrsquos Hospital Research InstituteCalgary Alberta Canada
Joumlrn Oliver Sass Dr rer natProfessor of Bioanalytics and BiochemistryDepartment of Natural SciencesBonn-Rhein-Sieg University of Applied SciencesSankt Augustin Germany
Samata Singhi MDClinical Fellow in NeurologyDepartment of NeurologyBoston Childrenrsquos HospitalBoston Massachusetts
Susan E Sparks MD PhDMedical DirectorNA Medical AffairsRare DiseasesSanofi GenzymeCambridge Massachusetts
Carl E Stafstrom MD PhDProfessor of Neurology and PediatricsLederer Chair in Pediatric EpilepsyDirector Division of Pediatric NeurologyJohns Hopkins University School of MedicineBaltimore Maryland
Robert Steinfeld MD PhDProfessor of Neurometabolic and Neurodegenerative
Diseases in Childhood and AdolescenceDepartment of Pediatrics and Pediatric NeurologyUniversity Medical Center GoumlttingenGoumlttingen Germany
Marshall L Summar MDChief Division of Genetics and MetabolismMargaret OrsquoMalley Chair of Genetic MedicineRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Brahim Tabarki MDDivision of Pediatric NeurologyPrince Sultan Military Medical CityRiyadh Saudi ArabiaAssociate Professor of Neurology and PediatricsThe Ibn El Jazzar University School of MedicineSousse Tunisia
Pranoot Tanpaiboon MDAssociate Professor of PediatricsDivision of Genetics and MetabolismThe George Washington University School of Medicine
and Health SciencesChildrenrsquos National Health System Childrenrsquos National
Rare Disease InstituteWashington DC
Davide Tonduti MDChild NeurologistDepartment of Child NeurologyFondazione IRCCS Istituto Neurologico Carlo BestaMilano Italy
Johan L K Van Hove MD PhDProfessor of PediatricsSection of Clinical Genetics and Metabolism
Department of PediatricsUniversity of ColoradoAurora Colorado
Adeline Vanderver MDAttending PhysicianDivision of NeurologyProgram DirectorLeukodystrophy CenterJacob A Kamens Endowed Chair in Neurologic
Disorders and Translational NeurotherapeuticsChildrenrsquos Hospital of PhiladelphiaAssociate Professor of NeurologyPerelman School of Medicine at the University of
PennsylvaniaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xvi
Jodie M Vento MGC LCGCManagerCenter for Rare Disease TherapyManagerBrain Care InstituteManagerLaboratory Genetic Counseling ServicesChildrenrsquos Hospital of Pittsburgh of UPMCPittsburgh Pennsylvania
Brandy Verhalen PhDLab ManagerPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas Texas
Kara Vogel PhDPostdoctoral Research AssociateUniversity of WisconsinndashMadisonMadison Wisconsin
Matthew Whitehead MDRadiologistChildrenrsquos National Medical CenterWashington DC
Lynne A Wolfe MS CRNPSenior Nurse PractitionerUndiagnosed Disorders ProgramNational Human Genome Research Institute National
Institutes of HealthBethesda Maryland
Robert A Zimmerman MDProfessor of RadiologyRaymond and Ruth Perelman School of Medicine at the
University of PennsylvaniaChiefDivision of Neuroradiology and MRIThe Childrenrsquos Hospital of PhiladelphiaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Preface
This edition of Inherited Metabolic Epilepsies is a greatly expanded and updated version of the fi rst Following a rousing response to the fi rst edition far beyond any anticipated measure it was clear that a reexamination of the material taking into account many helpful sug-gestions that I received from readers far and wide was in order Despite my own misgivings that books are no longer fashionable and are largely replaced by journals and online sources that lend themselves to periodic if not continual updating there remains an appetite and clamor for books that accomplish what I had hoped to do originally and aim to achieve to a greater extent in this edition to encapsulate a burgeoning fi eld suf-fi ciently that a student practitioner or investigator can turn to the source with confi dence that the neces-sary background as well as detail will be available to reward the search for information and also move the fi eld forward
The fi rst edition of this monograph was born follow-ing the organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the annual meeting of the American Epilepsy Society in Boston in 2009 At the time of proposing the topic I was wrestling with a chasmic gap between the fascinat-ing disorders being discussed at the geneticndashmetabolic meetings and the advancing wave in epilepsy classifi ca-tion diagnosis and treatment occupying the meetings attended by members of the societies associated with neurology and epilepsy At that time a storybook series of investigations elucidated not only the surprising antiq-uitin defect in pyridoxine-dependent epilepsy but also the highly charged requirement that physicians consider a pivotal role for folinic acid and pyridoxal-5-phosphate in patients with virtually the same clinical presentation I also perceived a relative lack of awareness of disorders such as glucose transporter 1 defi ciency serine synthetic defects developmental delay epilepsy and neonatal dia-betes (DEND) and hyperinsulinismndashhyperammonemia (HIndashHA) that had very specifi c therapeutic implications with potential for dramatically improving outcome but with an even greater likelihood that they were escaping diagnosis
Overall the inherited metabolic epilepsies repre-sent a group of disorders that is rare individually but
in aggregate represents a substantial clinical burden as well as a vexing area for physicians investigators and students to master The sheer amount and complexity of information are overwhelming and require the physician to synthesize key concepts in neurology genetics and epilepsy As a pediatric epileptologist and medical edu-cator I have found this area among the most challenging and rewarding in practice and research The fi rst edition organized the disorders in a traditional approach under the roof of metabolism by dividing them into small- and large-molecule disorders In the Preface to that edition there was an explanation of various ways of organizing these disorders some more user friendly to the neurol-ogist than the small- versus large-molecule divide but this was an opportunity to present that way of thinking to the neurologist which brings this clinical specialty closer to that of genetics metabolism
In this second edition there is an expansion from four sections (General Principles Small Molecule Diseases Large Molecule Diseases and Conclusions) to six sec-tions with the addition of chapters in basic science and clinical science of the metabolic epilepsies The book has been expanded from 28 to 43 chapters with new chapters including overviews of metabolic disease and the basic science of metabolic epilepsy plus new topics such as metabolic energetics and implications of vital pathways A full chapter is devoted to the mechanistic target of rapamycin (mTOR) pathway that regulates cell replica-tion and so much of homeostasis and new pathophysi-ologic mechanisms such as protein anchoring disorders There are new chapters on neurotransmitter transmission measurement using transcranial magnetic stimulation genomic technologies and approaches to diagnosis and therapy referable to this group of disorders The clinical science section now includes a marvelous and refl ective chapter on neuropathology by Harvey B Sarnat There are new chapters devoted to specifi c disorders such as pyridoxal-5-phosphate dependency and Menkesrsquo disease There are chapters with completely new vantage points from community and family resources to an emphasis on adult patients the latter being the most commonly requested area to cover that I receive after giving talks on the subject In addition the prior chapters from the fi rst edition have been revised and updated
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xviii
Hence what began as a quest to increase awareness of treatable metabolic epilepsies fi rst became a mono-graph to give some form to this arena and has now been enlarged and updated to a second edition It is hoped that this will provide a resource to in some way lead the fi eld and carry it forward It is truly hoped that this book will educate if not enlighten physicians particularly
specialists and trainees in pediatric and adult neurology neurodevelopmental disabilities epilepsy and genetics while caring for patients with inherited metabolic epi-lepsies as well as spur further research into basic mecha-nisms and clinical trials in this group of maladies
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Acknowledgments
This book was fi rst suggested to me by Beth Barry from Demos Medical Publishers following my organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the American Epilepsy Society 2009 meeting Beth was a driving force for the creation of this second edition and she and Young Kim at Demos now aligned with Springer are gratefully acknowledged for unmatched hard work and persever-ance in seeing this through to completion
My education in child neurology and epilepsy is grounded by great mentors including Ralph D Feigin MD in pediatrics and Marvin A Fishman MD in pediat-ric neurology of Baylor College of Medicine in Houston and Gregory L Holmes MD in epilepsy and clinical neurophysiology then at Childrenrsquos Hospital Harvard Medical School in Boston I wish to take this opportunity to acknowledge these teachers of mine
My foray into metabolic disorders has been made pos-sible by the always helpful brilliant and steadfast work of Mike Gibson PhD whose collaboration in the area of gamma-amino butyric acid (GABA) disorders specifi -cally succinic-semialdehyde dehydrogenase (SSADH) defi ciency has been a constant source of intellectual
nourishment and encouragement My career during the two editions of this book has now spanned two great childrenrsquos hospitals Childrenrsquos National and Boston Childrenrsquos and the insight and support of colleagues at both institutions have been fundamental to this work Ongoing collaborations with Mike Gibson as well as William H Theodore MD chief of the Clinical Epilepsy Section at the NINDS have been critical to the ongoing investigative work on metabolic epilepsies
I thank each of the contributors to the fi rst edition of this book for revising and updating their chapters and each of the authors of the new chapters resulting in a signifi cant expansion The outstanding assistance of Alisa Marino is gratefully acknowledged given the enormous complexity of the project and the organiza-tional skills needed to accomplish this and a myriad of other tasks As a group I thank the many patients and families as well as students residents and fellows who inspire our work I thank my own family who as with all of us shoulder the largest burden of personal sacrifi ce and inspire us the most
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

This book is dedicated to my wife Maria Tartaglia Pearl MD whose sacrifi ces for my work are fortunately outmatched
by our mutual love for medicine
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Contents
Contributors xiPreface xvii
Acknowledgments xix
PART I GENERAL PRINCIPLES 1 Recognition Scope and Implications of Inherited Metabolic Epilepsies 2
Phillip L Pearl
2 Overview of Inherited Metabolic Disease 16Lance H Rodan and Gerard T Berry
3 Treatable Inherited Metabolic Epilepsies Diagnoses Not to Miss 40Phillip L Pearl and Mohammed Almuqbil
PART II BASIC SCIENCE IN METABOLIC EPILEPSIES 4 Metabolic Epilepsies Principles and Mechanisms 56
Carl E Stafstrom and Jong M Rho
5 Metabolic Energetics in Epilepsy 74Ashwini Sri Hari and Manisha Patel
6 Pathways Dysregulation of mTOR and Epilepsy 86Darius Ebrahimi-Fakhari Jonathan Lipton and Mustafa Sahin
7 Protein Anchoring as an Important Mechanism in Early Onset Epilepsy Glycosylphosphatidylinositol (GPI) Defi ciency Syndromes 98Gali Heimer Bruria Ben-Zeev and Yair Anikster
PART III CLINICAL SCIENCE IN METABOLIC EPILEPSIES 8 Neuroimaging in the Metabolic Epilepsies 110
Robert A Zimmerman and Zarir P Khademian
9 Advances in MR Spectroscopy for Inherited Epilepsies 125Andrew Breeden Morgan J Prust Stanley T Fricke Matthew Whitehead and Andrea L Gropman
10 Neuropathology of Metabolic Epilepsies Novel Aspects in Children and the Diagnostic Role of Skin Biopsy 135Harvey B Sarnat
11 Electroencephalography in the Metabolic Epilepsies 149Samata Singhi Mona Alduligan and Phillip L Pearl
Share Inherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
viii
12 Genomic Technologies in Clinical Practice 187Christina Y Hung and Olaf A Bodamer
13 Measures of Cortical Excitability by Transcranial Magnetic Stimulation 201Alexander Rotenberg
14 Ketogenic Diet in Metabolic Epilepsies 207Susan L Fong and Eric H Kossoff
PART IV SMALL MOLECULE DISEASES 15 Amino and Organic Acid Disorders and Epilepsy 218
Kimberly A Chapman and Jamie L Fraser
16 Fatty Acid Oxidation Disorders and Epilepsy 237Dimitar Gavrilov and Dietrich Matern
17 Urea Cycle Disorders and Epilepsy 257Debra S Regier Brendan Lanpher and Marshall L Summar
18 Mitochondrial Diseases and Epilepsy 267Sumit Parikh Lynne A Wolfe and Andrea L Gropman
19 Pyridoxine-Dependent Epilepsy 275Sidney M Gospe Jr
20 Pyridoxamine 5acute-Phosphate Oxidase (PNPO) Defi ciency 287Barbara Plecko-Startinig
21 Tetrahydrobiopterin Defi ciencies and Epilepsy 293Nenad Blau and Thomas Opladen
22 Disorders of GABA Metabolism and Epilepsy 301Phillip L Pearl Kara Vogel and K Michael Gibson
23 Glucose Transporter Type 1 Defi ciency Syndrome 313Cigdem I Akman and Darryl C De Vivo
24 Thiamine Transporter Defi ciency and Epilepsy 326Brahim Tabarki
25 DEND Syndrome Developmental Delay Epilepsy and Neonatal Diabetes a Potassium Channelopathy 333Carolina Lahmann and Frances Ashcroft
26 HyperammonemiaHyperinsulinism Syndrome and Epilepsy 345Nicholas S Abend and Andrea Kelly
27 Glycine Encephalopathy and Epilepsy 353Julia B Hennermann Johan L K Van Hove and Curtis R Coughlin II
28 Serine Synthesis Disorders and Epilepsy 364T J de Koning
29 LeschndashNyhan Disease and Epilepsy 371Beth A Leeman-Markowski and Hyder A Jinnah
30 Sulfi te Oxidase Defi ciencyMolybdenum Cofactor Defi ciency and Epilepsy 394Joumlrn Oliver Sass and Barbara Plecko-Startinig
31 Creatine Disorders and Epilepsy 401Ton de Grauw
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
32 Cerebral Folate Defi ciency and Epilepsy 407Robert Steinfeld
33 Menkesrsquo Disease and Infantile Epilepsy 415Asuri N Prasad
PART V LARGE MOLECULE DISEASES 34 Congenital Disorders of Glycosylation and Epilepsy 428
Susan E Sparks
35 Lysosomal Storage Diseases and Epilepsy 445Pranoot Tanpaiboon and Grisel Lopez
36 Peroxisomal Diseases and Epilepsy 473Parastoo Jangouk Kristin W Barantildeano and Gerald V Raymond
37 Leukodystrophies and Epilepsy 483Davide Tonduti and Adeline Vanderver
PART VI CONCLUSIONS 38 Diagnostic Approaches to Genetic Epilepsies 490
Erika Takle Axeen Christelle El Achkar and Annapurna Poduri
39 Therapeutic Approaches to Inherited Metabolic Epilepsies 497Brandy Verhalen and Berge A Minassian
40 Inherited Metabolic Epilepsies in Adults 503Phillip L Pearl
41 Genetic Counseling in Metabolic Epilepsies 508Jodie M Vento
42 Support and Resources for Patients and Families With Inherited Metabolic Epilepsies 518Christopher Ryan and Jennifer Jeffs
43 Clinical Approach to Inherited Metabolic Epilepsies 525Scott Demarest Anna Lecticia Pinto and Phillip L Pearl
Index 529
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Contributors
Nicholas S Abend MD MSCEAssociate Professor of Neurology and PediatricsDepartments of Neurology and PediatricsChildrenrsquos Hospital of Philadelphia and the University
of PennsylvaniaPhiladelphia Pennsylvania
Christelle El Achkar MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Cigdem I Akman MDAssociate Professor of Clinical Neurology and PediatricsDepartments of Neurology and PediatricsDivision of Pediatric NeurologyInterim ChiefChild NeurologyDirectorPediatric EpilepsyColumbia University College of Physicians and SurgeonsNew York New York
Mona Alduligan MDPhysicianDivision of Clinical NeurophysiologyChildrenrsquos National Medical CenterWashington DC
Mohammed Almuqbil MD FRCP (C)King Abdullah Specialist Childrenrsquos Hospital (KASCH)King Saud bin Abdulaziz University for Health Sciences
(KSAU-HS)Pediatric Neurology DivisionRiyadh Saudi ArabiaKing Abdullah International Medical Research Center
(KAIMRC)National Guard MinistryRiyadh Saudi ArabiaDivision of Genetics and GenomicsBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Yair Anikster MD PhDDirectorMetabolic Disease UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
Frances Ashcroft PhD ScDGlaxoSmithKline Royal Society Research ProfessorDepartment of Physiology Anatomy and GeneticsFellow of Trinity CollegeDirector OXIONUniversity of OxfordOxford England
Erika Takle Axeen MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Minnesota
Kristin W Barantildeano MD PhDClinical AssociatePediatric NeurologyDepartment of NeurologyJohns Hopkins HospitalAssistant Professor of NeurologyJohns Hopkins School of MedicineBaltimore Maryland
Bruria Ben-Zeev MDDirectorPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xii
Gerard T Berry MDDirector Metabolism ProgramProfessor of PediatricsBoston Childrenrsquos HospitalBoston Massachusetts
Nenad Blau PhDSenior Consultant in Biochemical GeneticsProfessor Emeritus of Clinical Biochemistry (UZH)Dietmar-Hopp Metabolic CenterUniversity Childrenrsquos HospitalHeidelberg Germany
Olaf A Bodamer MD PhDAssociate Chief of Genetics and GenomicsBoston Childrenrsquos HospitalPark Gerald Chair in Genetics and GenomicsHarvard Medical SchoolBoston Massachusetts
Andrew Breeden PhDProgram AnalystHealth Program SpecialistNational Institute of Neurological Disorders and
Stroke (NINDS)Bethesda Maryland
Kimberly A Chapman MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National
Health SystemWashington DC
Curtis R Coughlin II MS MBe CGCAssistant Professor of PediatricsSection of Clinical Genetics and MetabolismDepartment of PediatricsUniversity of ColoradoAurora Colorado
Ton de Grauw MD PhDChiefNeurosciencesChildrenrsquos Healthcare of AtlantaDirectorPediatric NeurologyEmory University School of MedicineAtlanta Georgia
T J de Koning MD PhDPaediatrician for Inborn Errors of MetabolismDepartment of Genetics and PaediatricsUniversity Medical Centre GroningenUniversity of GroningenGroningen The Netherlands
Darryl C De Vivo MDSidney Carter Professor of NeurologyProfessor of PediatricsPediatric Neurology ServiceFounding DirectorColleen Giblin Research Laboratories for Pediatric
NeurologyAssociate ChairmanPediatric Neurosciences and Developmental
NeurobiologyCo-DirectorMotor Neuron CenterDirectorSpinal Muscular Atrophy (SMA) CenterChief EmeritusPediatric NeurologyColumbia University Medical CenterNew York New York
Scott Demarest MDAssistant Professor of Pediatrics and NeurologyChildrenrsquos Hospital ColoradoUniversity of ColoradoAurora Colorado
Darius Ebrahimi-Fakhari MD DrmedResident PhysicianDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Susan L Fong MD PhDAssistant ResidentPediatric NeurologyJohns Hopkins HospitalBaltimore Maryland
Jamie L Fraser MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National Health
SystemWashington DC
Stanley T Fricke PhDPhysicistChildrenrsquos National Medical CenterWashington DC
Dimitar Gavrilov MD PhDAssistant ProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
K Michael Gibson PhDAllen I White Distinguished Professor and ChairDepartment of PharmacotherapyWashington State University College of PharmacySpokane Washington
Sidney M Gospe Jr MD PhDHerman and Faye Sarkowsky Endowed ChairProfessor and HeadDivision of Pediatric NeurologyDepartments of Neurology and PediatricsUniversity of WashingtonDivision of NeurologySeattle Childrenrsquos Hospital and Seattle Childrenrsquos
Research InstituteSeattle Washington
Andrea L Gropman MDChief Neurogenetics and Neurodevelopmental
PediatricsChildrenrsquos National Medical CenterAssociate Professor of Neurology and PediatricsGeorge Washington School of Medicine and Health
SciencesWashington DC
Ashwini Sri Hari PhD CandidateDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Gali Heimer MD PhDSenior Physician and Director of the Angelman ClinicPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical Center Tel-Hashomer Israel Sackler Faculty of MedicineTel-Aviv UniversityTel-Aviv IsraelMember of the Dr Pinchas Borenstein Talpiot Medical
Leadership ProgramSheba Medical CenterTel-Hashomer Israel
Julia B Hennermann MDProfessor of Metabolic DiseasesUniversity Medical Center MainzVilla Metabolica Department of Pediatric and
Adolescent MedicineMainz Germany
Christina Y Hung MDResearch AssociateHMS Instructor in PediatricsDivision for Human Genetics and GenomicsBoston Childrenrsquos HospitalBoston Massachusetts
Parastoo Jangouk MDGastroenterology and Hepatology FellowYale-New Haven HospitalNew Haven Connecticut
Jennifer Jeffs LICSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Hyder A Jinnah MD PhDProfessorDepartments of Neurology Human Genetics and
PediatricsEmory University School of MedicineAtlanta Georgia
Andrea Kelly MD MSCEAssociate Professor of Pediatrics CEDepartment of PediatricsChildrenrsquos Hospital of Philadelphia and Perelman School
of Medicine of the University of PennsylvaniaPhiladelphia Pennsylvania
Zarir P Khademian MD PhDAssistant Professor of Radiology and PediatricsStaff Neurologist Division of Diagnostic Imaging and
RadiologyChildrenrsquos National Medical CenterWashington DC
Eric H Kossoff MDProfessorNeurology and PediatricsJohns Hopkins HospitalBaltimore Maryland
Carolina Lahmann PhDPostdoctoral FellowHarvard Medical SchoolBoston Massachusetts
Brendan Lanpher MDAssistant Professor of Medical GeneticsDepartment of Clinical GenomicsMayo ClinicRochester Minnesota
Beth A Leeman-Markowski MD MA MMScAssistant ProfessorDepartment of NeurologyNew York UniversityInvestigatorResearch ServiceVA New York Harbor Healthcare SystemmdashManhattan
CampusNew York New York
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xiv
Jonathan Lipton MD PhDAssistant Professor of NeurologyDepartment of Neurology and F M Kirby Center for
NeuroscienceBoston Childrenrsquos Hospital Harvard Medical SchoolBoston Massachusetts
Grisel Lopez MDSenior Staff ClinicianNational Human Genome Research InstituteNational Institutes of HealthBethesda Maryland
Dietrich Matern MD PhDProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
Berge A Minassian MDDivision ChiefPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas TexasUniversity of TorontoToronto Ontario Canada
Thomas Opladen MDDivision of Child Neurology and Metabolic DiseasesUniversity Childrenlsquos Hospital Heidelberg Germany
Sumit Parikh MDDirector of Cleveland Clinic Neurogenetics Metabolic
amp Mitochondrial Disease ProgramCleveland ClinicAssociate ProfessorDepartment of PediatricsCase Western Reserve University School of MedicineCleveland Ohio
Manisha Patel PhDProfessorDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Phillip L Pearl MDDirector of Epilepsy and Clinical NeurophysiologyWilliam G Lennox ChairBoston Childrenrsquos HospitalProfessor of NeurologyHarvard Medical SchoolBoston Massachusetts
Anna Lecticia Pinto MDAssistant in Neurology and Co-DirectorSturge Weber Clinic Boston Childrenrsquos HospitalLecturer of NeurologyHarvard Medical SchoolBoston Massachusetts
Barbara Plecko-Startinig MDHeadDivision of Child NeurologyChildrenrsquos Hospital ZurichProfessor of Child NeurologyUniversity of ZurichZurich Switzerland
Annapurna Poduri MD MPHEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Asuri N Prasad MBBS MD FRCPC FRCPEProfessor in Pediatrics and Clinical NeurosciencesDivision of Pediatric NeurologyDepartment of PediatricsSchulich School of Medicine and DentistryChildrenrsquos Hospital London Health Sciences CentreWestern UniversityLondon Ontario Canada
Morgan J Prust MDClinical Fellow in NeurologyDepartment of NeurologyMassachusetts General HospitalBrigham amp Womenrsquos HospitalBoston Massachusetts
Gerald V Raymond MDProfessorDepartment of NeurologyUniversity of Minnesota Medical SchoolMinneapolis Minnesota
Debra S Regier MD PhDDirector of Genetic and Genomic Education Medical
GeneticistRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Jong M Rho MDProfessor of Pediatrics Clinical Neurosciences
Physiology and PharmacologyDr Robert Haslam Chair in Child NeurologySection of Paediatric NeurologyCumming School of Medicine University of CalgaryAlberta Childrenrsquos HospitalCalgary Alberta Canada
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Lance H Rodan MDStaff PhysicianBoston Childrenrsquos HospitalBoston Massachusetts
Alexander Rotenberg MD PhDDirector Neuromodulation ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalAssociate Professor of NeurologyHarvard Medical SchoolBoston Massachusetts
Christopher Ryan LCSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Mustafa Sahin MD PhDProfessor of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Harvey B Sarnat MS MD FRCPCProfessor Departments of Paediatrics Pathology
(Neuropathology) and Clinical NeurosciencesUniversity of Calgary Cumming School of Medicine
and Alberta Childrenrsquos Hospital Research InstituteCalgary Alberta Canada
Joumlrn Oliver Sass Dr rer natProfessor of Bioanalytics and BiochemistryDepartment of Natural SciencesBonn-Rhein-Sieg University of Applied SciencesSankt Augustin Germany
Samata Singhi MDClinical Fellow in NeurologyDepartment of NeurologyBoston Childrenrsquos HospitalBoston Massachusetts
Susan E Sparks MD PhDMedical DirectorNA Medical AffairsRare DiseasesSanofi GenzymeCambridge Massachusetts
Carl E Stafstrom MD PhDProfessor of Neurology and PediatricsLederer Chair in Pediatric EpilepsyDirector Division of Pediatric NeurologyJohns Hopkins University School of MedicineBaltimore Maryland
Robert Steinfeld MD PhDProfessor of Neurometabolic and Neurodegenerative
Diseases in Childhood and AdolescenceDepartment of Pediatrics and Pediatric NeurologyUniversity Medical Center GoumlttingenGoumlttingen Germany
Marshall L Summar MDChief Division of Genetics and MetabolismMargaret OrsquoMalley Chair of Genetic MedicineRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Brahim Tabarki MDDivision of Pediatric NeurologyPrince Sultan Military Medical CityRiyadh Saudi ArabiaAssociate Professor of Neurology and PediatricsThe Ibn El Jazzar University School of MedicineSousse Tunisia
Pranoot Tanpaiboon MDAssociate Professor of PediatricsDivision of Genetics and MetabolismThe George Washington University School of Medicine
and Health SciencesChildrenrsquos National Health System Childrenrsquos National
Rare Disease InstituteWashington DC
Davide Tonduti MDChild NeurologistDepartment of Child NeurologyFondazione IRCCS Istituto Neurologico Carlo BestaMilano Italy
Johan L K Van Hove MD PhDProfessor of PediatricsSection of Clinical Genetics and Metabolism
Department of PediatricsUniversity of ColoradoAurora Colorado
Adeline Vanderver MDAttending PhysicianDivision of NeurologyProgram DirectorLeukodystrophy CenterJacob A Kamens Endowed Chair in Neurologic
Disorders and Translational NeurotherapeuticsChildrenrsquos Hospital of PhiladelphiaAssociate Professor of NeurologyPerelman School of Medicine at the University of
PennsylvaniaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xvi
Jodie M Vento MGC LCGCManagerCenter for Rare Disease TherapyManagerBrain Care InstituteManagerLaboratory Genetic Counseling ServicesChildrenrsquos Hospital of Pittsburgh of UPMCPittsburgh Pennsylvania
Brandy Verhalen PhDLab ManagerPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas Texas
Kara Vogel PhDPostdoctoral Research AssociateUniversity of WisconsinndashMadisonMadison Wisconsin
Matthew Whitehead MDRadiologistChildrenrsquos National Medical CenterWashington DC
Lynne A Wolfe MS CRNPSenior Nurse PractitionerUndiagnosed Disorders ProgramNational Human Genome Research Institute National
Institutes of HealthBethesda Maryland
Robert A Zimmerman MDProfessor of RadiologyRaymond and Ruth Perelman School of Medicine at the
University of PennsylvaniaChiefDivision of Neuroradiology and MRIThe Childrenrsquos Hospital of PhiladelphiaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Preface
This edition of Inherited Metabolic Epilepsies is a greatly expanded and updated version of the fi rst Following a rousing response to the fi rst edition far beyond any anticipated measure it was clear that a reexamination of the material taking into account many helpful sug-gestions that I received from readers far and wide was in order Despite my own misgivings that books are no longer fashionable and are largely replaced by journals and online sources that lend themselves to periodic if not continual updating there remains an appetite and clamor for books that accomplish what I had hoped to do originally and aim to achieve to a greater extent in this edition to encapsulate a burgeoning fi eld suf-fi ciently that a student practitioner or investigator can turn to the source with confi dence that the neces-sary background as well as detail will be available to reward the search for information and also move the fi eld forward
The fi rst edition of this monograph was born follow-ing the organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the annual meeting of the American Epilepsy Society in Boston in 2009 At the time of proposing the topic I was wrestling with a chasmic gap between the fascinat-ing disorders being discussed at the geneticndashmetabolic meetings and the advancing wave in epilepsy classifi ca-tion diagnosis and treatment occupying the meetings attended by members of the societies associated with neurology and epilepsy At that time a storybook series of investigations elucidated not only the surprising antiq-uitin defect in pyridoxine-dependent epilepsy but also the highly charged requirement that physicians consider a pivotal role for folinic acid and pyridoxal-5-phosphate in patients with virtually the same clinical presentation I also perceived a relative lack of awareness of disorders such as glucose transporter 1 defi ciency serine synthetic defects developmental delay epilepsy and neonatal dia-betes (DEND) and hyperinsulinismndashhyperammonemia (HIndashHA) that had very specifi c therapeutic implications with potential for dramatically improving outcome but with an even greater likelihood that they were escaping diagnosis
Overall the inherited metabolic epilepsies repre-sent a group of disorders that is rare individually but
in aggregate represents a substantial clinical burden as well as a vexing area for physicians investigators and students to master The sheer amount and complexity of information are overwhelming and require the physician to synthesize key concepts in neurology genetics and epilepsy As a pediatric epileptologist and medical edu-cator I have found this area among the most challenging and rewarding in practice and research The fi rst edition organized the disorders in a traditional approach under the roof of metabolism by dividing them into small- and large-molecule disorders In the Preface to that edition there was an explanation of various ways of organizing these disorders some more user friendly to the neurol-ogist than the small- versus large-molecule divide but this was an opportunity to present that way of thinking to the neurologist which brings this clinical specialty closer to that of genetics metabolism
In this second edition there is an expansion from four sections (General Principles Small Molecule Diseases Large Molecule Diseases and Conclusions) to six sec-tions with the addition of chapters in basic science and clinical science of the metabolic epilepsies The book has been expanded from 28 to 43 chapters with new chapters including overviews of metabolic disease and the basic science of metabolic epilepsy plus new topics such as metabolic energetics and implications of vital pathways A full chapter is devoted to the mechanistic target of rapamycin (mTOR) pathway that regulates cell replica-tion and so much of homeostasis and new pathophysi-ologic mechanisms such as protein anchoring disorders There are new chapters on neurotransmitter transmission measurement using transcranial magnetic stimulation genomic technologies and approaches to diagnosis and therapy referable to this group of disorders The clinical science section now includes a marvelous and refl ective chapter on neuropathology by Harvey B Sarnat There are new chapters devoted to specifi c disorders such as pyridoxal-5-phosphate dependency and Menkesrsquo disease There are chapters with completely new vantage points from community and family resources to an emphasis on adult patients the latter being the most commonly requested area to cover that I receive after giving talks on the subject In addition the prior chapters from the fi rst edition have been revised and updated
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xviii
Hence what began as a quest to increase awareness of treatable metabolic epilepsies fi rst became a mono-graph to give some form to this arena and has now been enlarged and updated to a second edition It is hoped that this will provide a resource to in some way lead the fi eld and carry it forward It is truly hoped that this book will educate if not enlighten physicians particularly
specialists and trainees in pediatric and adult neurology neurodevelopmental disabilities epilepsy and genetics while caring for patients with inherited metabolic epi-lepsies as well as spur further research into basic mecha-nisms and clinical trials in this group of maladies
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Acknowledgments
This book was fi rst suggested to me by Beth Barry from Demos Medical Publishers following my organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the American Epilepsy Society 2009 meeting Beth was a driving force for the creation of this second edition and she and Young Kim at Demos now aligned with Springer are gratefully acknowledged for unmatched hard work and persever-ance in seeing this through to completion
My education in child neurology and epilepsy is grounded by great mentors including Ralph D Feigin MD in pediatrics and Marvin A Fishman MD in pediat-ric neurology of Baylor College of Medicine in Houston and Gregory L Holmes MD in epilepsy and clinical neurophysiology then at Childrenrsquos Hospital Harvard Medical School in Boston I wish to take this opportunity to acknowledge these teachers of mine
My foray into metabolic disorders has been made pos-sible by the always helpful brilliant and steadfast work of Mike Gibson PhD whose collaboration in the area of gamma-amino butyric acid (GABA) disorders specifi -cally succinic-semialdehyde dehydrogenase (SSADH) defi ciency has been a constant source of intellectual
nourishment and encouragement My career during the two editions of this book has now spanned two great childrenrsquos hospitals Childrenrsquos National and Boston Childrenrsquos and the insight and support of colleagues at both institutions have been fundamental to this work Ongoing collaborations with Mike Gibson as well as William H Theodore MD chief of the Clinical Epilepsy Section at the NINDS have been critical to the ongoing investigative work on metabolic epilepsies
I thank each of the contributors to the fi rst edition of this book for revising and updating their chapters and each of the authors of the new chapters resulting in a signifi cant expansion The outstanding assistance of Alisa Marino is gratefully acknowledged given the enormous complexity of the project and the organiza-tional skills needed to accomplish this and a myriad of other tasks As a group I thank the many patients and families as well as students residents and fellows who inspire our work I thank my own family who as with all of us shoulder the largest burden of personal sacrifi ce and inspire us the most
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Contents
Contributors xiPreface xvii
Acknowledgments xix
PART I GENERAL PRINCIPLES 1 Recognition Scope and Implications of Inherited Metabolic Epilepsies 2
Phillip L Pearl
2 Overview of Inherited Metabolic Disease 16Lance H Rodan and Gerard T Berry
3 Treatable Inherited Metabolic Epilepsies Diagnoses Not to Miss 40Phillip L Pearl and Mohammed Almuqbil
PART II BASIC SCIENCE IN METABOLIC EPILEPSIES 4 Metabolic Epilepsies Principles and Mechanisms 56
Carl E Stafstrom and Jong M Rho
5 Metabolic Energetics in Epilepsy 74Ashwini Sri Hari and Manisha Patel
6 Pathways Dysregulation of mTOR and Epilepsy 86Darius Ebrahimi-Fakhari Jonathan Lipton and Mustafa Sahin
7 Protein Anchoring as an Important Mechanism in Early Onset Epilepsy Glycosylphosphatidylinositol (GPI) Defi ciency Syndromes 98Gali Heimer Bruria Ben-Zeev and Yair Anikster
PART III CLINICAL SCIENCE IN METABOLIC EPILEPSIES 8 Neuroimaging in the Metabolic Epilepsies 110
Robert A Zimmerman and Zarir P Khademian
9 Advances in MR Spectroscopy for Inherited Epilepsies 125Andrew Breeden Morgan J Prust Stanley T Fricke Matthew Whitehead and Andrea L Gropman
10 Neuropathology of Metabolic Epilepsies Novel Aspects in Children and the Diagnostic Role of Skin Biopsy 135Harvey B Sarnat
11 Electroencephalography in the Metabolic Epilepsies 149Samata Singhi Mona Alduligan and Phillip L Pearl
Share Inherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
viii
12 Genomic Technologies in Clinical Practice 187Christina Y Hung and Olaf A Bodamer
13 Measures of Cortical Excitability by Transcranial Magnetic Stimulation 201Alexander Rotenberg
14 Ketogenic Diet in Metabolic Epilepsies 207Susan L Fong and Eric H Kossoff
PART IV SMALL MOLECULE DISEASES 15 Amino and Organic Acid Disorders and Epilepsy 218
Kimberly A Chapman and Jamie L Fraser
16 Fatty Acid Oxidation Disorders and Epilepsy 237Dimitar Gavrilov and Dietrich Matern
17 Urea Cycle Disorders and Epilepsy 257Debra S Regier Brendan Lanpher and Marshall L Summar
18 Mitochondrial Diseases and Epilepsy 267Sumit Parikh Lynne A Wolfe and Andrea L Gropman
19 Pyridoxine-Dependent Epilepsy 275Sidney M Gospe Jr
20 Pyridoxamine 5acute-Phosphate Oxidase (PNPO) Defi ciency 287Barbara Plecko-Startinig
21 Tetrahydrobiopterin Defi ciencies and Epilepsy 293Nenad Blau and Thomas Opladen
22 Disorders of GABA Metabolism and Epilepsy 301Phillip L Pearl Kara Vogel and K Michael Gibson
23 Glucose Transporter Type 1 Defi ciency Syndrome 313Cigdem I Akman and Darryl C De Vivo
24 Thiamine Transporter Defi ciency and Epilepsy 326Brahim Tabarki
25 DEND Syndrome Developmental Delay Epilepsy and Neonatal Diabetes a Potassium Channelopathy 333Carolina Lahmann and Frances Ashcroft
26 HyperammonemiaHyperinsulinism Syndrome and Epilepsy 345Nicholas S Abend and Andrea Kelly
27 Glycine Encephalopathy and Epilepsy 353Julia B Hennermann Johan L K Van Hove and Curtis R Coughlin II
28 Serine Synthesis Disorders and Epilepsy 364T J de Koning
29 LeschndashNyhan Disease and Epilepsy 371Beth A Leeman-Markowski and Hyder A Jinnah
30 Sulfi te Oxidase Defi ciencyMolybdenum Cofactor Defi ciency and Epilepsy 394Joumlrn Oliver Sass and Barbara Plecko-Startinig
31 Creatine Disorders and Epilepsy 401Ton de Grauw
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
32 Cerebral Folate Defi ciency and Epilepsy 407Robert Steinfeld
33 Menkesrsquo Disease and Infantile Epilepsy 415Asuri N Prasad
PART V LARGE MOLECULE DISEASES 34 Congenital Disorders of Glycosylation and Epilepsy 428
Susan E Sparks
35 Lysosomal Storage Diseases and Epilepsy 445Pranoot Tanpaiboon and Grisel Lopez
36 Peroxisomal Diseases and Epilepsy 473Parastoo Jangouk Kristin W Barantildeano and Gerald V Raymond
37 Leukodystrophies and Epilepsy 483Davide Tonduti and Adeline Vanderver
PART VI CONCLUSIONS 38 Diagnostic Approaches to Genetic Epilepsies 490
Erika Takle Axeen Christelle El Achkar and Annapurna Poduri
39 Therapeutic Approaches to Inherited Metabolic Epilepsies 497Brandy Verhalen and Berge A Minassian
40 Inherited Metabolic Epilepsies in Adults 503Phillip L Pearl
41 Genetic Counseling in Metabolic Epilepsies 508Jodie M Vento
42 Support and Resources for Patients and Families With Inherited Metabolic Epilepsies 518Christopher Ryan and Jennifer Jeffs
43 Clinical Approach to Inherited Metabolic Epilepsies 525Scott Demarest Anna Lecticia Pinto and Phillip L Pearl
Index 529
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Contributors
Nicholas S Abend MD MSCEAssociate Professor of Neurology and PediatricsDepartments of Neurology and PediatricsChildrenrsquos Hospital of Philadelphia and the University
of PennsylvaniaPhiladelphia Pennsylvania
Christelle El Achkar MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Cigdem I Akman MDAssociate Professor of Clinical Neurology and PediatricsDepartments of Neurology and PediatricsDivision of Pediatric NeurologyInterim ChiefChild NeurologyDirectorPediatric EpilepsyColumbia University College of Physicians and SurgeonsNew York New York
Mona Alduligan MDPhysicianDivision of Clinical NeurophysiologyChildrenrsquos National Medical CenterWashington DC
Mohammed Almuqbil MD FRCP (C)King Abdullah Specialist Childrenrsquos Hospital (KASCH)King Saud bin Abdulaziz University for Health Sciences
(KSAU-HS)Pediatric Neurology DivisionRiyadh Saudi ArabiaKing Abdullah International Medical Research Center
(KAIMRC)National Guard MinistryRiyadh Saudi ArabiaDivision of Genetics and GenomicsBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Yair Anikster MD PhDDirectorMetabolic Disease UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
Frances Ashcroft PhD ScDGlaxoSmithKline Royal Society Research ProfessorDepartment of Physiology Anatomy and GeneticsFellow of Trinity CollegeDirector OXIONUniversity of OxfordOxford England
Erika Takle Axeen MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Minnesota
Kristin W Barantildeano MD PhDClinical AssociatePediatric NeurologyDepartment of NeurologyJohns Hopkins HospitalAssistant Professor of NeurologyJohns Hopkins School of MedicineBaltimore Maryland
Bruria Ben-Zeev MDDirectorPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xii
Gerard T Berry MDDirector Metabolism ProgramProfessor of PediatricsBoston Childrenrsquos HospitalBoston Massachusetts
Nenad Blau PhDSenior Consultant in Biochemical GeneticsProfessor Emeritus of Clinical Biochemistry (UZH)Dietmar-Hopp Metabolic CenterUniversity Childrenrsquos HospitalHeidelberg Germany
Olaf A Bodamer MD PhDAssociate Chief of Genetics and GenomicsBoston Childrenrsquos HospitalPark Gerald Chair in Genetics and GenomicsHarvard Medical SchoolBoston Massachusetts
Andrew Breeden PhDProgram AnalystHealth Program SpecialistNational Institute of Neurological Disorders and
Stroke (NINDS)Bethesda Maryland
Kimberly A Chapman MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National
Health SystemWashington DC
Curtis R Coughlin II MS MBe CGCAssistant Professor of PediatricsSection of Clinical Genetics and MetabolismDepartment of PediatricsUniversity of ColoradoAurora Colorado
Ton de Grauw MD PhDChiefNeurosciencesChildrenrsquos Healthcare of AtlantaDirectorPediatric NeurologyEmory University School of MedicineAtlanta Georgia
T J de Koning MD PhDPaediatrician for Inborn Errors of MetabolismDepartment of Genetics and PaediatricsUniversity Medical Centre GroningenUniversity of GroningenGroningen The Netherlands
Darryl C De Vivo MDSidney Carter Professor of NeurologyProfessor of PediatricsPediatric Neurology ServiceFounding DirectorColleen Giblin Research Laboratories for Pediatric
NeurologyAssociate ChairmanPediatric Neurosciences and Developmental
NeurobiologyCo-DirectorMotor Neuron CenterDirectorSpinal Muscular Atrophy (SMA) CenterChief EmeritusPediatric NeurologyColumbia University Medical CenterNew York New York
Scott Demarest MDAssistant Professor of Pediatrics and NeurologyChildrenrsquos Hospital ColoradoUniversity of ColoradoAurora Colorado
Darius Ebrahimi-Fakhari MD DrmedResident PhysicianDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Susan L Fong MD PhDAssistant ResidentPediatric NeurologyJohns Hopkins HospitalBaltimore Maryland
Jamie L Fraser MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National Health
SystemWashington DC
Stanley T Fricke PhDPhysicistChildrenrsquos National Medical CenterWashington DC
Dimitar Gavrilov MD PhDAssistant ProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
K Michael Gibson PhDAllen I White Distinguished Professor and ChairDepartment of PharmacotherapyWashington State University College of PharmacySpokane Washington
Sidney M Gospe Jr MD PhDHerman and Faye Sarkowsky Endowed ChairProfessor and HeadDivision of Pediatric NeurologyDepartments of Neurology and PediatricsUniversity of WashingtonDivision of NeurologySeattle Childrenrsquos Hospital and Seattle Childrenrsquos
Research InstituteSeattle Washington
Andrea L Gropman MDChief Neurogenetics and Neurodevelopmental
PediatricsChildrenrsquos National Medical CenterAssociate Professor of Neurology and PediatricsGeorge Washington School of Medicine and Health
SciencesWashington DC
Ashwini Sri Hari PhD CandidateDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Gali Heimer MD PhDSenior Physician and Director of the Angelman ClinicPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical Center Tel-Hashomer Israel Sackler Faculty of MedicineTel-Aviv UniversityTel-Aviv IsraelMember of the Dr Pinchas Borenstein Talpiot Medical
Leadership ProgramSheba Medical CenterTel-Hashomer Israel
Julia B Hennermann MDProfessor of Metabolic DiseasesUniversity Medical Center MainzVilla Metabolica Department of Pediatric and
Adolescent MedicineMainz Germany
Christina Y Hung MDResearch AssociateHMS Instructor in PediatricsDivision for Human Genetics and GenomicsBoston Childrenrsquos HospitalBoston Massachusetts
Parastoo Jangouk MDGastroenterology and Hepatology FellowYale-New Haven HospitalNew Haven Connecticut
Jennifer Jeffs LICSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Hyder A Jinnah MD PhDProfessorDepartments of Neurology Human Genetics and
PediatricsEmory University School of MedicineAtlanta Georgia
Andrea Kelly MD MSCEAssociate Professor of Pediatrics CEDepartment of PediatricsChildrenrsquos Hospital of Philadelphia and Perelman School
of Medicine of the University of PennsylvaniaPhiladelphia Pennsylvania
Zarir P Khademian MD PhDAssistant Professor of Radiology and PediatricsStaff Neurologist Division of Diagnostic Imaging and
RadiologyChildrenrsquos National Medical CenterWashington DC
Eric H Kossoff MDProfessorNeurology and PediatricsJohns Hopkins HospitalBaltimore Maryland
Carolina Lahmann PhDPostdoctoral FellowHarvard Medical SchoolBoston Massachusetts
Brendan Lanpher MDAssistant Professor of Medical GeneticsDepartment of Clinical GenomicsMayo ClinicRochester Minnesota
Beth A Leeman-Markowski MD MA MMScAssistant ProfessorDepartment of NeurologyNew York UniversityInvestigatorResearch ServiceVA New York Harbor Healthcare SystemmdashManhattan
CampusNew York New York
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xiv
Jonathan Lipton MD PhDAssistant Professor of NeurologyDepartment of Neurology and F M Kirby Center for
NeuroscienceBoston Childrenrsquos Hospital Harvard Medical SchoolBoston Massachusetts
Grisel Lopez MDSenior Staff ClinicianNational Human Genome Research InstituteNational Institutes of HealthBethesda Maryland
Dietrich Matern MD PhDProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
Berge A Minassian MDDivision ChiefPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas TexasUniversity of TorontoToronto Ontario Canada
Thomas Opladen MDDivision of Child Neurology and Metabolic DiseasesUniversity Childrenlsquos Hospital Heidelberg Germany
Sumit Parikh MDDirector of Cleveland Clinic Neurogenetics Metabolic
amp Mitochondrial Disease ProgramCleveland ClinicAssociate ProfessorDepartment of PediatricsCase Western Reserve University School of MedicineCleveland Ohio
Manisha Patel PhDProfessorDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Phillip L Pearl MDDirector of Epilepsy and Clinical NeurophysiologyWilliam G Lennox ChairBoston Childrenrsquos HospitalProfessor of NeurologyHarvard Medical SchoolBoston Massachusetts
Anna Lecticia Pinto MDAssistant in Neurology and Co-DirectorSturge Weber Clinic Boston Childrenrsquos HospitalLecturer of NeurologyHarvard Medical SchoolBoston Massachusetts
Barbara Plecko-Startinig MDHeadDivision of Child NeurologyChildrenrsquos Hospital ZurichProfessor of Child NeurologyUniversity of ZurichZurich Switzerland
Annapurna Poduri MD MPHEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Asuri N Prasad MBBS MD FRCPC FRCPEProfessor in Pediatrics and Clinical NeurosciencesDivision of Pediatric NeurologyDepartment of PediatricsSchulich School of Medicine and DentistryChildrenrsquos Hospital London Health Sciences CentreWestern UniversityLondon Ontario Canada
Morgan J Prust MDClinical Fellow in NeurologyDepartment of NeurologyMassachusetts General HospitalBrigham amp Womenrsquos HospitalBoston Massachusetts
Gerald V Raymond MDProfessorDepartment of NeurologyUniversity of Minnesota Medical SchoolMinneapolis Minnesota
Debra S Regier MD PhDDirector of Genetic and Genomic Education Medical
GeneticistRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Jong M Rho MDProfessor of Pediatrics Clinical Neurosciences
Physiology and PharmacologyDr Robert Haslam Chair in Child NeurologySection of Paediatric NeurologyCumming School of Medicine University of CalgaryAlberta Childrenrsquos HospitalCalgary Alberta Canada
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Lance H Rodan MDStaff PhysicianBoston Childrenrsquos HospitalBoston Massachusetts
Alexander Rotenberg MD PhDDirector Neuromodulation ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalAssociate Professor of NeurologyHarvard Medical SchoolBoston Massachusetts
Christopher Ryan LCSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Mustafa Sahin MD PhDProfessor of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Harvey B Sarnat MS MD FRCPCProfessor Departments of Paediatrics Pathology
(Neuropathology) and Clinical NeurosciencesUniversity of Calgary Cumming School of Medicine
and Alberta Childrenrsquos Hospital Research InstituteCalgary Alberta Canada
Joumlrn Oliver Sass Dr rer natProfessor of Bioanalytics and BiochemistryDepartment of Natural SciencesBonn-Rhein-Sieg University of Applied SciencesSankt Augustin Germany
Samata Singhi MDClinical Fellow in NeurologyDepartment of NeurologyBoston Childrenrsquos HospitalBoston Massachusetts
Susan E Sparks MD PhDMedical DirectorNA Medical AffairsRare DiseasesSanofi GenzymeCambridge Massachusetts
Carl E Stafstrom MD PhDProfessor of Neurology and PediatricsLederer Chair in Pediatric EpilepsyDirector Division of Pediatric NeurologyJohns Hopkins University School of MedicineBaltimore Maryland
Robert Steinfeld MD PhDProfessor of Neurometabolic and Neurodegenerative
Diseases in Childhood and AdolescenceDepartment of Pediatrics and Pediatric NeurologyUniversity Medical Center GoumlttingenGoumlttingen Germany
Marshall L Summar MDChief Division of Genetics and MetabolismMargaret OrsquoMalley Chair of Genetic MedicineRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Brahim Tabarki MDDivision of Pediatric NeurologyPrince Sultan Military Medical CityRiyadh Saudi ArabiaAssociate Professor of Neurology and PediatricsThe Ibn El Jazzar University School of MedicineSousse Tunisia
Pranoot Tanpaiboon MDAssociate Professor of PediatricsDivision of Genetics and MetabolismThe George Washington University School of Medicine
and Health SciencesChildrenrsquos National Health System Childrenrsquos National
Rare Disease InstituteWashington DC
Davide Tonduti MDChild NeurologistDepartment of Child NeurologyFondazione IRCCS Istituto Neurologico Carlo BestaMilano Italy
Johan L K Van Hove MD PhDProfessor of PediatricsSection of Clinical Genetics and Metabolism
Department of PediatricsUniversity of ColoradoAurora Colorado
Adeline Vanderver MDAttending PhysicianDivision of NeurologyProgram DirectorLeukodystrophy CenterJacob A Kamens Endowed Chair in Neurologic
Disorders and Translational NeurotherapeuticsChildrenrsquos Hospital of PhiladelphiaAssociate Professor of NeurologyPerelman School of Medicine at the University of
PennsylvaniaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xvi
Jodie M Vento MGC LCGCManagerCenter for Rare Disease TherapyManagerBrain Care InstituteManagerLaboratory Genetic Counseling ServicesChildrenrsquos Hospital of Pittsburgh of UPMCPittsburgh Pennsylvania
Brandy Verhalen PhDLab ManagerPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas Texas
Kara Vogel PhDPostdoctoral Research AssociateUniversity of WisconsinndashMadisonMadison Wisconsin
Matthew Whitehead MDRadiologistChildrenrsquos National Medical CenterWashington DC
Lynne A Wolfe MS CRNPSenior Nurse PractitionerUndiagnosed Disorders ProgramNational Human Genome Research Institute National
Institutes of HealthBethesda Maryland
Robert A Zimmerman MDProfessor of RadiologyRaymond and Ruth Perelman School of Medicine at the
University of PennsylvaniaChiefDivision of Neuroradiology and MRIThe Childrenrsquos Hospital of PhiladelphiaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Preface
This edition of Inherited Metabolic Epilepsies is a greatly expanded and updated version of the fi rst Following a rousing response to the fi rst edition far beyond any anticipated measure it was clear that a reexamination of the material taking into account many helpful sug-gestions that I received from readers far and wide was in order Despite my own misgivings that books are no longer fashionable and are largely replaced by journals and online sources that lend themselves to periodic if not continual updating there remains an appetite and clamor for books that accomplish what I had hoped to do originally and aim to achieve to a greater extent in this edition to encapsulate a burgeoning fi eld suf-fi ciently that a student practitioner or investigator can turn to the source with confi dence that the neces-sary background as well as detail will be available to reward the search for information and also move the fi eld forward
The fi rst edition of this monograph was born follow-ing the organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the annual meeting of the American Epilepsy Society in Boston in 2009 At the time of proposing the topic I was wrestling with a chasmic gap between the fascinat-ing disorders being discussed at the geneticndashmetabolic meetings and the advancing wave in epilepsy classifi ca-tion diagnosis and treatment occupying the meetings attended by members of the societies associated with neurology and epilepsy At that time a storybook series of investigations elucidated not only the surprising antiq-uitin defect in pyridoxine-dependent epilepsy but also the highly charged requirement that physicians consider a pivotal role for folinic acid and pyridoxal-5-phosphate in patients with virtually the same clinical presentation I also perceived a relative lack of awareness of disorders such as glucose transporter 1 defi ciency serine synthetic defects developmental delay epilepsy and neonatal dia-betes (DEND) and hyperinsulinismndashhyperammonemia (HIndashHA) that had very specifi c therapeutic implications with potential for dramatically improving outcome but with an even greater likelihood that they were escaping diagnosis
Overall the inherited metabolic epilepsies repre-sent a group of disorders that is rare individually but
in aggregate represents a substantial clinical burden as well as a vexing area for physicians investigators and students to master The sheer amount and complexity of information are overwhelming and require the physician to synthesize key concepts in neurology genetics and epilepsy As a pediatric epileptologist and medical edu-cator I have found this area among the most challenging and rewarding in practice and research The fi rst edition organized the disorders in a traditional approach under the roof of metabolism by dividing them into small- and large-molecule disorders In the Preface to that edition there was an explanation of various ways of organizing these disorders some more user friendly to the neurol-ogist than the small- versus large-molecule divide but this was an opportunity to present that way of thinking to the neurologist which brings this clinical specialty closer to that of genetics metabolism
In this second edition there is an expansion from four sections (General Principles Small Molecule Diseases Large Molecule Diseases and Conclusions) to six sec-tions with the addition of chapters in basic science and clinical science of the metabolic epilepsies The book has been expanded from 28 to 43 chapters with new chapters including overviews of metabolic disease and the basic science of metabolic epilepsy plus new topics such as metabolic energetics and implications of vital pathways A full chapter is devoted to the mechanistic target of rapamycin (mTOR) pathway that regulates cell replica-tion and so much of homeostasis and new pathophysi-ologic mechanisms such as protein anchoring disorders There are new chapters on neurotransmitter transmission measurement using transcranial magnetic stimulation genomic technologies and approaches to diagnosis and therapy referable to this group of disorders The clinical science section now includes a marvelous and refl ective chapter on neuropathology by Harvey B Sarnat There are new chapters devoted to specifi c disorders such as pyridoxal-5-phosphate dependency and Menkesrsquo disease There are chapters with completely new vantage points from community and family resources to an emphasis on adult patients the latter being the most commonly requested area to cover that I receive after giving talks on the subject In addition the prior chapters from the fi rst edition have been revised and updated
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xviii
Hence what began as a quest to increase awareness of treatable metabolic epilepsies fi rst became a mono-graph to give some form to this arena and has now been enlarged and updated to a second edition It is hoped that this will provide a resource to in some way lead the fi eld and carry it forward It is truly hoped that this book will educate if not enlighten physicians particularly
specialists and trainees in pediatric and adult neurology neurodevelopmental disabilities epilepsy and genetics while caring for patients with inherited metabolic epi-lepsies as well as spur further research into basic mecha-nisms and clinical trials in this group of maladies
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Acknowledgments
This book was fi rst suggested to me by Beth Barry from Demos Medical Publishers following my organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the American Epilepsy Society 2009 meeting Beth was a driving force for the creation of this second edition and she and Young Kim at Demos now aligned with Springer are gratefully acknowledged for unmatched hard work and persever-ance in seeing this through to completion
My education in child neurology and epilepsy is grounded by great mentors including Ralph D Feigin MD in pediatrics and Marvin A Fishman MD in pediat-ric neurology of Baylor College of Medicine in Houston and Gregory L Holmes MD in epilepsy and clinical neurophysiology then at Childrenrsquos Hospital Harvard Medical School in Boston I wish to take this opportunity to acknowledge these teachers of mine
My foray into metabolic disorders has been made pos-sible by the always helpful brilliant and steadfast work of Mike Gibson PhD whose collaboration in the area of gamma-amino butyric acid (GABA) disorders specifi -cally succinic-semialdehyde dehydrogenase (SSADH) defi ciency has been a constant source of intellectual
nourishment and encouragement My career during the two editions of this book has now spanned two great childrenrsquos hospitals Childrenrsquos National and Boston Childrenrsquos and the insight and support of colleagues at both institutions have been fundamental to this work Ongoing collaborations with Mike Gibson as well as William H Theodore MD chief of the Clinical Epilepsy Section at the NINDS have been critical to the ongoing investigative work on metabolic epilepsies
I thank each of the contributors to the fi rst edition of this book for revising and updating their chapters and each of the authors of the new chapters resulting in a signifi cant expansion The outstanding assistance of Alisa Marino is gratefully acknowledged given the enormous complexity of the project and the organiza-tional skills needed to accomplish this and a myriad of other tasks As a group I thank the many patients and families as well as students residents and fellows who inspire our work I thank my own family who as with all of us shoulder the largest burden of personal sacrifi ce and inspire us the most
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

Contents
Contributors xiPreface xvii
Acknowledgments xix
PART I GENERAL PRINCIPLES 1 Recognition Scope and Implications of Inherited Metabolic Epilepsies 2
Phillip L Pearl
2 Overview of Inherited Metabolic Disease 16Lance H Rodan and Gerard T Berry
3 Treatable Inherited Metabolic Epilepsies Diagnoses Not to Miss 40Phillip L Pearl and Mohammed Almuqbil
PART II BASIC SCIENCE IN METABOLIC EPILEPSIES 4 Metabolic Epilepsies Principles and Mechanisms 56
Carl E Stafstrom and Jong M Rho
5 Metabolic Energetics in Epilepsy 74Ashwini Sri Hari and Manisha Patel
6 Pathways Dysregulation of mTOR and Epilepsy 86Darius Ebrahimi-Fakhari Jonathan Lipton and Mustafa Sahin
7 Protein Anchoring as an Important Mechanism in Early Onset Epilepsy Glycosylphosphatidylinositol (GPI) Defi ciency Syndromes 98Gali Heimer Bruria Ben-Zeev and Yair Anikster
PART III CLINICAL SCIENCE IN METABOLIC EPILEPSIES 8 Neuroimaging in the Metabolic Epilepsies 110
Robert A Zimmerman and Zarir P Khademian
9 Advances in MR Spectroscopy for Inherited Epilepsies 125Andrew Breeden Morgan J Prust Stanley T Fricke Matthew Whitehead and Andrea L Gropman
10 Neuropathology of Metabolic Epilepsies Novel Aspects in Children and the Diagnostic Role of Skin Biopsy 135Harvey B Sarnat
11 Electroencephalography in the Metabolic Epilepsies 149Samata Singhi Mona Alduligan and Phillip L Pearl
Share Inherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
viii
12 Genomic Technologies in Clinical Practice 187Christina Y Hung and Olaf A Bodamer
13 Measures of Cortical Excitability by Transcranial Magnetic Stimulation 201Alexander Rotenberg
14 Ketogenic Diet in Metabolic Epilepsies 207Susan L Fong and Eric H Kossoff
PART IV SMALL MOLECULE DISEASES 15 Amino and Organic Acid Disorders and Epilepsy 218
Kimberly A Chapman and Jamie L Fraser
16 Fatty Acid Oxidation Disorders and Epilepsy 237Dimitar Gavrilov and Dietrich Matern
17 Urea Cycle Disorders and Epilepsy 257Debra S Regier Brendan Lanpher and Marshall L Summar
18 Mitochondrial Diseases and Epilepsy 267Sumit Parikh Lynne A Wolfe and Andrea L Gropman
19 Pyridoxine-Dependent Epilepsy 275Sidney M Gospe Jr
20 Pyridoxamine 5acute-Phosphate Oxidase (PNPO) Defi ciency 287Barbara Plecko-Startinig
21 Tetrahydrobiopterin Defi ciencies and Epilepsy 293Nenad Blau and Thomas Opladen
22 Disorders of GABA Metabolism and Epilepsy 301Phillip L Pearl Kara Vogel and K Michael Gibson
23 Glucose Transporter Type 1 Defi ciency Syndrome 313Cigdem I Akman and Darryl C De Vivo
24 Thiamine Transporter Defi ciency and Epilepsy 326Brahim Tabarki
25 DEND Syndrome Developmental Delay Epilepsy and Neonatal Diabetes a Potassium Channelopathy 333Carolina Lahmann and Frances Ashcroft
26 HyperammonemiaHyperinsulinism Syndrome and Epilepsy 345Nicholas S Abend and Andrea Kelly
27 Glycine Encephalopathy and Epilepsy 353Julia B Hennermann Johan L K Van Hove and Curtis R Coughlin II
28 Serine Synthesis Disorders and Epilepsy 364T J de Koning
29 LeschndashNyhan Disease and Epilepsy 371Beth A Leeman-Markowski and Hyder A Jinnah
30 Sulfi te Oxidase Defi ciencyMolybdenum Cofactor Defi ciency and Epilepsy 394Joumlrn Oliver Sass and Barbara Plecko-Startinig
31 Creatine Disorders and Epilepsy 401Ton de Grauw
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
32 Cerebral Folate Defi ciency and Epilepsy 407Robert Steinfeld
33 Menkesrsquo Disease and Infantile Epilepsy 415Asuri N Prasad
PART V LARGE MOLECULE DISEASES 34 Congenital Disorders of Glycosylation and Epilepsy 428
Susan E Sparks
35 Lysosomal Storage Diseases and Epilepsy 445Pranoot Tanpaiboon and Grisel Lopez
36 Peroxisomal Diseases and Epilepsy 473Parastoo Jangouk Kristin W Barantildeano and Gerald V Raymond
37 Leukodystrophies and Epilepsy 483Davide Tonduti and Adeline Vanderver
PART VI CONCLUSIONS 38 Diagnostic Approaches to Genetic Epilepsies 490
Erika Takle Axeen Christelle El Achkar and Annapurna Poduri
39 Therapeutic Approaches to Inherited Metabolic Epilepsies 497Brandy Verhalen and Berge A Minassian
40 Inherited Metabolic Epilepsies in Adults 503Phillip L Pearl
41 Genetic Counseling in Metabolic Epilepsies 508Jodie M Vento
42 Support and Resources for Patients and Families With Inherited Metabolic Epilepsies 518Christopher Ryan and Jennifer Jeffs
43 Clinical Approach to Inherited Metabolic Epilepsies 525Scott Demarest Anna Lecticia Pinto and Phillip L Pearl
Index 529
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Contributors
Nicholas S Abend MD MSCEAssociate Professor of Neurology and PediatricsDepartments of Neurology and PediatricsChildrenrsquos Hospital of Philadelphia and the University
of PennsylvaniaPhiladelphia Pennsylvania
Christelle El Achkar MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Cigdem I Akman MDAssociate Professor of Clinical Neurology and PediatricsDepartments of Neurology and PediatricsDivision of Pediatric NeurologyInterim ChiefChild NeurologyDirectorPediatric EpilepsyColumbia University College of Physicians and SurgeonsNew York New York
Mona Alduligan MDPhysicianDivision of Clinical NeurophysiologyChildrenrsquos National Medical CenterWashington DC
Mohammed Almuqbil MD FRCP (C)King Abdullah Specialist Childrenrsquos Hospital (KASCH)King Saud bin Abdulaziz University for Health Sciences
(KSAU-HS)Pediatric Neurology DivisionRiyadh Saudi ArabiaKing Abdullah International Medical Research Center
(KAIMRC)National Guard MinistryRiyadh Saudi ArabiaDivision of Genetics and GenomicsBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Yair Anikster MD PhDDirectorMetabolic Disease UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
Frances Ashcroft PhD ScDGlaxoSmithKline Royal Society Research ProfessorDepartment of Physiology Anatomy and GeneticsFellow of Trinity CollegeDirector OXIONUniversity of OxfordOxford England
Erika Takle Axeen MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Minnesota
Kristin W Barantildeano MD PhDClinical AssociatePediatric NeurologyDepartment of NeurologyJohns Hopkins HospitalAssistant Professor of NeurologyJohns Hopkins School of MedicineBaltimore Maryland
Bruria Ben-Zeev MDDirectorPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xii
Gerard T Berry MDDirector Metabolism ProgramProfessor of PediatricsBoston Childrenrsquos HospitalBoston Massachusetts
Nenad Blau PhDSenior Consultant in Biochemical GeneticsProfessor Emeritus of Clinical Biochemistry (UZH)Dietmar-Hopp Metabolic CenterUniversity Childrenrsquos HospitalHeidelberg Germany
Olaf A Bodamer MD PhDAssociate Chief of Genetics and GenomicsBoston Childrenrsquos HospitalPark Gerald Chair in Genetics and GenomicsHarvard Medical SchoolBoston Massachusetts
Andrew Breeden PhDProgram AnalystHealth Program SpecialistNational Institute of Neurological Disorders and
Stroke (NINDS)Bethesda Maryland
Kimberly A Chapman MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National
Health SystemWashington DC
Curtis R Coughlin II MS MBe CGCAssistant Professor of PediatricsSection of Clinical Genetics and MetabolismDepartment of PediatricsUniversity of ColoradoAurora Colorado
Ton de Grauw MD PhDChiefNeurosciencesChildrenrsquos Healthcare of AtlantaDirectorPediatric NeurologyEmory University School of MedicineAtlanta Georgia
T J de Koning MD PhDPaediatrician for Inborn Errors of MetabolismDepartment of Genetics and PaediatricsUniversity Medical Centre GroningenUniversity of GroningenGroningen The Netherlands
Darryl C De Vivo MDSidney Carter Professor of NeurologyProfessor of PediatricsPediatric Neurology ServiceFounding DirectorColleen Giblin Research Laboratories for Pediatric
NeurologyAssociate ChairmanPediatric Neurosciences and Developmental
NeurobiologyCo-DirectorMotor Neuron CenterDirectorSpinal Muscular Atrophy (SMA) CenterChief EmeritusPediatric NeurologyColumbia University Medical CenterNew York New York
Scott Demarest MDAssistant Professor of Pediatrics and NeurologyChildrenrsquos Hospital ColoradoUniversity of ColoradoAurora Colorado
Darius Ebrahimi-Fakhari MD DrmedResident PhysicianDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Susan L Fong MD PhDAssistant ResidentPediatric NeurologyJohns Hopkins HospitalBaltimore Maryland
Jamie L Fraser MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National Health
SystemWashington DC
Stanley T Fricke PhDPhysicistChildrenrsquos National Medical CenterWashington DC
Dimitar Gavrilov MD PhDAssistant ProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
K Michael Gibson PhDAllen I White Distinguished Professor and ChairDepartment of PharmacotherapyWashington State University College of PharmacySpokane Washington
Sidney M Gospe Jr MD PhDHerman and Faye Sarkowsky Endowed ChairProfessor and HeadDivision of Pediatric NeurologyDepartments of Neurology and PediatricsUniversity of WashingtonDivision of NeurologySeattle Childrenrsquos Hospital and Seattle Childrenrsquos
Research InstituteSeattle Washington
Andrea L Gropman MDChief Neurogenetics and Neurodevelopmental
PediatricsChildrenrsquos National Medical CenterAssociate Professor of Neurology and PediatricsGeorge Washington School of Medicine and Health
SciencesWashington DC
Ashwini Sri Hari PhD CandidateDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Gali Heimer MD PhDSenior Physician and Director of the Angelman ClinicPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical Center Tel-Hashomer Israel Sackler Faculty of MedicineTel-Aviv UniversityTel-Aviv IsraelMember of the Dr Pinchas Borenstein Talpiot Medical
Leadership ProgramSheba Medical CenterTel-Hashomer Israel
Julia B Hennermann MDProfessor of Metabolic DiseasesUniversity Medical Center MainzVilla Metabolica Department of Pediatric and
Adolescent MedicineMainz Germany
Christina Y Hung MDResearch AssociateHMS Instructor in PediatricsDivision for Human Genetics and GenomicsBoston Childrenrsquos HospitalBoston Massachusetts
Parastoo Jangouk MDGastroenterology and Hepatology FellowYale-New Haven HospitalNew Haven Connecticut
Jennifer Jeffs LICSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Hyder A Jinnah MD PhDProfessorDepartments of Neurology Human Genetics and
PediatricsEmory University School of MedicineAtlanta Georgia
Andrea Kelly MD MSCEAssociate Professor of Pediatrics CEDepartment of PediatricsChildrenrsquos Hospital of Philadelphia and Perelman School
of Medicine of the University of PennsylvaniaPhiladelphia Pennsylvania
Zarir P Khademian MD PhDAssistant Professor of Radiology and PediatricsStaff Neurologist Division of Diagnostic Imaging and
RadiologyChildrenrsquos National Medical CenterWashington DC
Eric H Kossoff MDProfessorNeurology and PediatricsJohns Hopkins HospitalBaltimore Maryland
Carolina Lahmann PhDPostdoctoral FellowHarvard Medical SchoolBoston Massachusetts
Brendan Lanpher MDAssistant Professor of Medical GeneticsDepartment of Clinical GenomicsMayo ClinicRochester Minnesota
Beth A Leeman-Markowski MD MA MMScAssistant ProfessorDepartment of NeurologyNew York UniversityInvestigatorResearch ServiceVA New York Harbor Healthcare SystemmdashManhattan
CampusNew York New York
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xiv
Jonathan Lipton MD PhDAssistant Professor of NeurologyDepartment of Neurology and F M Kirby Center for
NeuroscienceBoston Childrenrsquos Hospital Harvard Medical SchoolBoston Massachusetts
Grisel Lopez MDSenior Staff ClinicianNational Human Genome Research InstituteNational Institutes of HealthBethesda Maryland
Dietrich Matern MD PhDProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
Berge A Minassian MDDivision ChiefPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas TexasUniversity of TorontoToronto Ontario Canada
Thomas Opladen MDDivision of Child Neurology and Metabolic DiseasesUniversity Childrenlsquos Hospital Heidelberg Germany
Sumit Parikh MDDirector of Cleveland Clinic Neurogenetics Metabolic
amp Mitochondrial Disease ProgramCleveland ClinicAssociate ProfessorDepartment of PediatricsCase Western Reserve University School of MedicineCleveland Ohio
Manisha Patel PhDProfessorDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Phillip L Pearl MDDirector of Epilepsy and Clinical NeurophysiologyWilliam G Lennox ChairBoston Childrenrsquos HospitalProfessor of NeurologyHarvard Medical SchoolBoston Massachusetts
Anna Lecticia Pinto MDAssistant in Neurology and Co-DirectorSturge Weber Clinic Boston Childrenrsquos HospitalLecturer of NeurologyHarvard Medical SchoolBoston Massachusetts
Barbara Plecko-Startinig MDHeadDivision of Child NeurologyChildrenrsquos Hospital ZurichProfessor of Child NeurologyUniversity of ZurichZurich Switzerland
Annapurna Poduri MD MPHEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Asuri N Prasad MBBS MD FRCPC FRCPEProfessor in Pediatrics and Clinical NeurosciencesDivision of Pediatric NeurologyDepartment of PediatricsSchulich School of Medicine and DentistryChildrenrsquos Hospital London Health Sciences CentreWestern UniversityLondon Ontario Canada
Morgan J Prust MDClinical Fellow in NeurologyDepartment of NeurologyMassachusetts General HospitalBrigham amp Womenrsquos HospitalBoston Massachusetts
Gerald V Raymond MDProfessorDepartment of NeurologyUniversity of Minnesota Medical SchoolMinneapolis Minnesota
Debra S Regier MD PhDDirector of Genetic and Genomic Education Medical
GeneticistRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Jong M Rho MDProfessor of Pediatrics Clinical Neurosciences
Physiology and PharmacologyDr Robert Haslam Chair in Child NeurologySection of Paediatric NeurologyCumming School of Medicine University of CalgaryAlberta Childrenrsquos HospitalCalgary Alberta Canada
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Lance H Rodan MDStaff PhysicianBoston Childrenrsquos HospitalBoston Massachusetts
Alexander Rotenberg MD PhDDirector Neuromodulation ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalAssociate Professor of NeurologyHarvard Medical SchoolBoston Massachusetts
Christopher Ryan LCSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Mustafa Sahin MD PhDProfessor of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Harvey B Sarnat MS MD FRCPCProfessor Departments of Paediatrics Pathology
(Neuropathology) and Clinical NeurosciencesUniversity of Calgary Cumming School of Medicine
and Alberta Childrenrsquos Hospital Research InstituteCalgary Alberta Canada
Joumlrn Oliver Sass Dr rer natProfessor of Bioanalytics and BiochemistryDepartment of Natural SciencesBonn-Rhein-Sieg University of Applied SciencesSankt Augustin Germany
Samata Singhi MDClinical Fellow in NeurologyDepartment of NeurologyBoston Childrenrsquos HospitalBoston Massachusetts
Susan E Sparks MD PhDMedical DirectorNA Medical AffairsRare DiseasesSanofi GenzymeCambridge Massachusetts
Carl E Stafstrom MD PhDProfessor of Neurology and PediatricsLederer Chair in Pediatric EpilepsyDirector Division of Pediatric NeurologyJohns Hopkins University School of MedicineBaltimore Maryland
Robert Steinfeld MD PhDProfessor of Neurometabolic and Neurodegenerative
Diseases in Childhood and AdolescenceDepartment of Pediatrics and Pediatric NeurologyUniversity Medical Center GoumlttingenGoumlttingen Germany
Marshall L Summar MDChief Division of Genetics and MetabolismMargaret OrsquoMalley Chair of Genetic MedicineRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Brahim Tabarki MDDivision of Pediatric NeurologyPrince Sultan Military Medical CityRiyadh Saudi ArabiaAssociate Professor of Neurology and PediatricsThe Ibn El Jazzar University School of MedicineSousse Tunisia
Pranoot Tanpaiboon MDAssociate Professor of PediatricsDivision of Genetics and MetabolismThe George Washington University School of Medicine
and Health SciencesChildrenrsquos National Health System Childrenrsquos National
Rare Disease InstituteWashington DC
Davide Tonduti MDChild NeurologistDepartment of Child NeurologyFondazione IRCCS Istituto Neurologico Carlo BestaMilano Italy
Johan L K Van Hove MD PhDProfessor of PediatricsSection of Clinical Genetics and Metabolism
Department of PediatricsUniversity of ColoradoAurora Colorado
Adeline Vanderver MDAttending PhysicianDivision of NeurologyProgram DirectorLeukodystrophy CenterJacob A Kamens Endowed Chair in Neurologic
Disorders and Translational NeurotherapeuticsChildrenrsquos Hospital of PhiladelphiaAssociate Professor of NeurologyPerelman School of Medicine at the University of
PennsylvaniaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xvi
Jodie M Vento MGC LCGCManagerCenter for Rare Disease TherapyManagerBrain Care InstituteManagerLaboratory Genetic Counseling ServicesChildrenrsquos Hospital of Pittsburgh of UPMCPittsburgh Pennsylvania
Brandy Verhalen PhDLab ManagerPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas Texas
Kara Vogel PhDPostdoctoral Research AssociateUniversity of WisconsinndashMadisonMadison Wisconsin
Matthew Whitehead MDRadiologistChildrenrsquos National Medical CenterWashington DC
Lynne A Wolfe MS CRNPSenior Nurse PractitionerUndiagnosed Disorders ProgramNational Human Genome Research Institute National
Institutes of HealthBethesda Maryland
Robert A Zimmerman MDProfessor of RadiologyRaymond and Ruth Perelman School of Medicine at the
University of PennsylvaniaChiefDivision of Neuroradiology and MRIThe Childrenrsquos Hospital of PhiladelphiaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Preface
This edition of Inherited Metabolic Epilepsies is a greatly expanded and updated version of the fi rst Following a rousing response to the fi rst edition far beyond any anticipated measure it was clear that a reexamination of the material taking into account many helpful sug-gestions that I received from readers far and wide was in order Despite my own misgivings that books are no longer fashionable and are largely replaced by journals and online sources that lend themselves to periodic if not continual updating there remains an appetite and clamor for books that accomplish what I had hoped to do originally and aim to achieve to a greater extent in this edition to encapsulate a burgeoning fi eld suf-fi ciently that a student practitioner or investigator can turn to the source with confi dence that the neces-sary background as well as detail will be available to reward the search for information and also move the fi eld forward
The fi rst edition of this monograph was born follow-ing the organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the annual meeting of the American Epilepsy Society in Boston in 2009 At the time of proposing the topic I was wrestling with a chasmic gap between the fascinat-ing disorders being discussed at the geneticndashmetabolic meetings and the advancing wave in epilepsy classifi ca-tion diagnosis and treatment occupying the meetings attended by members of the societies associated with neurology and epilepsy At that time a storybook series of investigations elucidated not only the surprising antiq-uitin defect in pyridoxine-dependent epilepsy but also the highly charged requirement that physicians consider a pivotal role for folinic acid and pyridoxal-5-phosphate in patients with virtually the same clinical presentation I also perceived a relative lack of awareness of disorders such as glucose transporter 1 defi ciency serine synthetic defects developmental delay epilepsy and neonatal dia-betes (DEND) and hyperinsulinismndashhyperammonemia (HIndashHA) that had very specifi c therapeutic implications with potential for dramatically improving outcome but with an even greater likelihood that they were escaping diagnosis
Overall the inherited metabolic epilepsies repre-sent a group of disorders that is rare individually but
in aggregate represents a substantial clinical burden as well as a vexing area for physicians investigators and students to master The sheer amount and complexity of information are overwhelming and require the physician to synthesize key concepts in neurology genetics and epilepsy As a pediatric epileptologist and medical edu-cator I have found this area among the most challenging and rewarding in practice and research The fi rst edition organized the disorders in a traditional approach under the roof of metabolism by dividing them into small- and large-molecule disorders In the Preface to that edition there was an explanation of various ways of organizing these disorders some more user friendly to the neurol-ogist than the small- versus large-molecule divide but this was an opportunity to present that way of thinking to the neurologist which brings this clinical specialty closer to that of genetics metabolism
In this second edition there is an expansion from four sections (General Principles Small Molecule Diseases Large Molecule Diseases and Conclusions) to six sec-tions with the addition of chapters in basic science and clinical science of the metabolic epilepsies The book has been expanded from 28 to 43 chapters with new chapters including overviews of metabolic disease and the basic science of metabolic epilepsy plus new topics such as metabolic energetics and implications of vital pathways A full chapter is devoted to the mechanistic target of rapamycin (mTOR) pathway that regulates cell replica-tion and so much of homeostasis and new pathophysi-ologic mechanisms such as protein anchoring disorders There are new chapters on neurotransmitter transmission measurement using transcranial magnetic stimulation genomic technologies and approaches to diagnosis and therapy referable to this group of disorders The clinical science section now includes a marvelous and refl ective chapter on neuropathology by Harvey B Sarnat There are new chapters devoted to specifi c disorders such as pyridoxal-5-phosphate dependency and Menkesrsquo disease There are chapters with completely new vantage points from community and family resources to an emphasis on adult patients the latter being the most commonly requested area to cover that I receive after giving talks on the subject In addition the prior chapters from the fi rst edition have been revised and updated
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xviii
Hence what began as a quest to increase awareness of treatable metabolic epilepsies fi rst became a mono-graph to give some form to this arena and has now been enlarged and updated to a second edition It is hoped that this will provide a resource to in some way lead the fi eld and carry it forward It is truly hoped that this book will educate if not enlighten physicians particularly
specialists and trainees in pediatric and adult neurology neurodevelopmental disabilities epilepsy and genetics while caring for patients with inherited metabolic epi-lepsies as well as spur further research into basic mecha-nisms and clinical trials in this group of maladies
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Acknowledgments
This book was fi rst suggested to me by Beth Barry from Demos Medical Publishers following my organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the American Epilepsy Society 2009 meeting Beth was a driving force for the creation of this second edition and she and Young Kim at Demos now aligned with Springer are gratefully acknowledged for unmatched hard work and persever-ance in seeing this through to completion
My education in child neurology and epilepsy is grounded by great mentors including Ralph D Feigin MD in pediatrics and Marvin A Fishman MD in pediat-ric neurology of Baylor College of Medicine in Houston and Gregory L Holmes MD in epilepsy and clinical neurophysiology then at Childrenrsquos Hospital Harvard Medical School in Boston I wish to take this opportunity to acknowledge these teachers of mine
My foray into metabolic disorders has been made pos-sible by the always helpful brilliant and steadfast work of Mike Gibson PhD whose collaboration in the area of gamma-amino butyric acid (GABA) disorders specifi -cally succinic-semialdehyde dehydrogenase (SSADH) defi ciency has been a constant source of intellectual
nourishment and encouragement My career during the two editions of this book has now spanned two great childrenrsquos hospitals Childrenrsquos National and Boston Childrenrsquos and the insight and support of colleagues at both institutions have been fundamental to this work Ongoing collaborations with Mike Gibson as well as William H Theodore MD chief of the Clinical Epilepsy Section at the NINDS have been critical to the ongoing investigative work on metabolic epilepsies
I thank each of the contributors to the fi rst edition of this book for revising and updating their chapters and each of the authors of the new chapters resulting in a signifi cant expansion The outstanding assistance of Alisa Marino is gratefully acknowledged given the enormous complexity of the project and the organiza-tional skills needed to accomplish this and a myriad of other tasks As a group I thank the many patients and families as well as students residents and fellows who inspire our work I thank my own family who as with all of us shoulder the largest burden of personal sacrifi ce and inspire us the most
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
viii
12 Genomic Technologies in Clinical Practice 187Christina Y Hung and Olaf A Bodamer
13 Measures of Cortical Excitability by Transcranial Magnetic Stimulation 201Alexander Rotenberg
14 Ketogenic Diet in Metabolic Epilepsies 207Susan L Fong and Eric H Kossoff
PART IV SMALL MOLECULE DISEASES 15 Amino and Organic Acid Disorders and Epilepsy 218
Kimberly A Chapman and Jamie L Fraser
16 Fatty Acid Oxidation Disorders and Epilepsy 237Dimitar Gavrilov and Dietrich Matern
17 Urea Cycle Disorders and Epilepsy 257Debra S Regier Brendan Lanpher and Marshall L Summar
18 Mitochondrial Diseases and Epilepsy 267Sumit Parikh Lynne A Wolfe and Andrea L Gropman
19 Pyridoxine-Dependent Epilepsy 275Sidney M Gospe Jr
20 Pyridoxamine 5acute-Phosphate Oxidase (PNPO) Defi ciency 287Barbara Plecko-Startinig
21 Tetrahydrobiopterin Defi ciencies and Epilepsy 293Nenad Blau and Thomas Opladen
22 Disorders of GABA Metabolism and Epilepsy 301Phillip L Pearl Kara Vogel and K Michael Gibson
23 Glucose Transporter Type 1 Defi ciency Syndrome 313Cigdem I Akman and Darryl C De Vivo
24 Thiamine Transporter Defi ciency and Epilepsy 326Brahim Tabarki
25 DEND Syndrome Developmental Delay Epilepsy and Neonatal Diabetes a Potassium Channelopathy 333Carolina Lahmann and Frances Ashcroft
26 HyperammonemiaHyperinsulinism Syndrome and Epilepsy 345Nicholas S Abend and Andrea Kelly
27 Glycine Encephalopathy and Epilepsy 353Julia B Hennermann Johan L K Van Hove and Curtis R Coughlin II
28 Serine Synthesis Disorders and Epilepsy 364T J de Koning
29 LeschndashNyhan Disease and Epilepsy 371Beth A Leeman-Markowski and Hyder A Jinnah
30 Sulfi te Oxidase Defi ciencyMolybdenum Cofactor Defi ciency and Epilepsy 394Joumlrn Oliver Sass and Barbara Plecko-Startinig
31 Creatine Disorders and Epilepsy 401Ton de Grauw
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
32 Cerebral Folate Defi ciency and Epilepsy 407Robert Steinfeld
33 Menkesrsquo Disease and Infantile Epilepsy 415Asuri N Prasad
PART V LARGE MOLECULE DISEASES 34 Congenital Disorders of Glycosylation and Epilepsy 428
Susan E Sparks
35 Lysosomal Storage Diseases and Epilepsy 445Pranoot Tanpaiboon and Grisel Lopez
36 Peroxisomal Diseases and Epilepsy 473Parastoo Jangouk Kristin W Barantildeano and Gerald V Raymond
37 Leukodystrophies and Epilepsy 483Davide Tonduti and Adeline Vanderver
PART VI CONCLUSIONS 38 Diagnostic Approaches to Genetic Epilepsies 490
Erika Takle Axeen Christelle El Achkar and Annapurna Poduri
39 Therapeutic Approaches to Inherited Metabolic Epilepsies 497Brandy Verhalen and Berge A Minassian
40 Inherited Metabolic Epilepsies in Adults 503Phillip L Pearl
41 Genetic Counseling in Metabolic Epilepsies 508Jodie M Vento
42 Support and Resources for Patients and Families With Inherited Metabolic Epilepsies 518Christopher Ryan and Jennifer Jeffs
43 Clinical Approach to Inherited Metabolic Epilepsies 525Scott Demarest Anna Lecticia Pinto and Phillip L Pearl
Index 529
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Contributors
Nicholas S Abend MD MSCEAssociate Professor of Neurology and PediatricsDepartments of Neurology and PediatricsChildrenrsquos Hospital of Philadelphia and the University
of PennsylvaniaPhiladelphia Pennsylvania
Christelle El Achkar MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Cigdem I Akman MDAssociate Professor of Clinical Neurology and PediatricsDepartments of Neurology and PediatricsDivision of Pediatric NeurologyInterim ChiefChild NeurologyDirectorPediatric EpilepsyColumbia University College of Physicians and SurgeonsNew York New York
Mona Alduligan MDPhysicianDivision of Clinical NeurophysiologyChildrenrsquos National Medical CenterWashington DC
Mohammed Almuqbil MD FRCP (C)King Abdullah Specialist Childrenrsquos Hospital (KASCH)King Saud bin Abdulaziz University for Health Sciences
(KSAU-HS)Pediatric Neurology DivisionRiyadh Saudi ArabiaKing Abdullah International Medical Research Center
(KAIMRC)National Guard MinistryRiyadh Saudi ArabiaDivision of Genetics and GenomicsBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Yair Anikster MD PhDDirectorMetabolic Disease UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
Frances Ashcroft PhD ScDGlaxoSmithKline Royal Society Research ProfessorDepartment of Physiology Anatomy and GeneticsFellow of Trinity CollegeDirector OXIONUniversity of OxfordOxford England
Erika Takle Axeen MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Minnesota
Kristin W Barantildeano MD PhDClinical AssociatePediatric NeurologyDepartment of NeurologyJohns Hopkins HospitalAssistant Professor of NeurologyJohns Hopkins School of MedicineBaltimore Maryland
Bruria Ben-Zeev MDDirectorPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xii
Gerard T Berry MDDirector Metabolism ProgramProfessor of PediatricsBoston Childrenrsquos HospitalBoston Massachusetts
Nenad Blau PhDSenior Consultant in Biochemical GeneticsProfessor Emeritus of Clinical Biochemistry (UZH)Dietmar-Hopp Metabolic CenterUniversity Childrenrsquos HospitalHeidelberg Germany
Olaf A Bodamer MD PhDAssociate Chief of Genetics and GenomicsBoston Childrenrsquos HospitalPark Gerald Chair in Genetics and GenomicsHarvard Medical SchoolBoston Massachusetts
Andrew Breeden PhDProgram AnalystHealth Program SpecialistNational Institute of Neurological Disorders and
Stroke (NINDS)Bethesda Maryland
Kimberly A Chapman MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National
Health SystemWashington DC
Curtis R Coughlin II MS MBe CGCAssistant Professor of PediatricsSection of Clinical Genetics and MetabolismDepartment of PediatricsUniversity of ColoradoAurora Colorado
Ton de Grauw MD PhDChiefNeurosciencesChildrenrsquos Healthcare of AtlantaDirectorPediatric NeurologyEmory University School of MedicineAtlanta Georgia
T J de Koning MD PhDPaediatrician for Inborn Errors of MetabolismDepartment of Genetics and PaediatricsUniversity Medical Centre GroningenUniversity of GroningenGroningen The Netherlands
Darryl C De Vivo MDSidney Carter Professor of NeurologyProfessor of PediatricsPediatric Neurology ServiceFounding DirectorColleen Giblin Research Laboratories for Pediatric
NeurologyAssociate ChairmanPediatric Neurosciences and Developmental
NeurobiologyCo-DirectorMotor Neuron CenterDirectorSpinal Muscular Atrophy (SMA) CenterChief EmeritusPediatric NeurologyColumbia University Medical CenterNew York New York
Scott Demarest MDAssistant Professor of Pediatrics and NeurologyChildrenrsquos Hospital ColoradoUniversity of ColoradoAurora Colorado
Darius Ebrahimi-Fakhari MD DrmedResident PhysicianDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Susan L Fong MD PhDAssistant ResidentPediatric NeurologyJohns Hopkins HospitalBaltimore Maryland
Jamie L Fraser MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National Health
SystemWashington DC
Stanley T Fricke PhDPhysicistChildrenrsquos National Medical CenterWashington DC
Dimitar Gavrilov MD PhDAssistant ProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
K Michael Gibson PhDAllen I White Distinguished Professor and ChairDepartment of PharmacotherapyWashington State University College of PharmacySpokane Washington
Sidney M Gospe Jr MD PhDHerman and Faye Sarkowsky Endowed ChairProfessor and HeadDivision of Pediatric NeurologyDepartments of Neurology and PediatricsUniversity of WashingtonDivision of NeurologySeattle Childrenrsquos Hospital and Seattle Childrenrsquos
Research InstituteSeattle Washington
Andrea L Gropman MDChief Neurogenetics and Neurodevelopmental
PediatricsChildrenrsquos National Medical CenterAssociate Professor of Neurology and PediatricsGeorge Washington School of Medicine and Health
SciencesWashington DC
Ashwini Sri Hari PhD CandidateDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Gali Heimer MD PhDSenior Physician and Director of the Angelman ClinicPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical Center Tel-Hashomer Israel Sackler Faculty of MedicineTel-Aviv UniversityTel-Aviv IsraelMember of the Dr Pinchas Borenstein Talpiot Medical
Leadership ProgramSheba Medical CenterTel-Hashomer Israel
Julia B Hennermann MDProfessor of Metabolic DiseasesUniversity Medical Center MainzVilla Metabolica Department of Pediatric and
Adolescent MedicineMainz Germany
Christina Y Hung MDResearch AssociateHMS Instructor in PediatricsDivision for Human Genetics and GenomicsBoston Childrenrsquos HospitalBoston Massachusetts
Parastoo Jangouk MDGastroenterology and Hepatology FellowYale-New Haven HospitalNew Haven Connecticut
Jennifer Jeffs LICSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Hyder A Jinnah MD PhDProfessorDepartments of Neurology Human Genetics and
PediatricsEmory University School of MedicineAtlanta Georgia
Andrea Kelly MD MSCEAssociate Professor of Pediatrics CEDepartment of PediatricsChildrenrsquos Hospital of Philadelphia and Perelman School
of Medicine of the University of PennsylvaniaPhiladelphia Pennsylvania
Zarir P Khademian MD PhDAssistant Professor of Radiology and PediatricsStaff Neurologist Division of Diagnostic Imaging and
RadiologyChildrenrsquos National Medical CenterWashington DC
Eric H Kossoff MDProfessorNeurology and PediatricsJohns Hopkins HospitalBaltimore Maryland
Carolina Lahmann PhDPostdoctoral FellowHarvard Medical SchoolBoston Massachusetts
Brendan Lanpher MDAssistant Professor of Medical GeneticsDepartment of Clinical GenomicsMayo ClinicRochester Minnesota
Beth A Leeman-Markowski MD MA MMScAssistant ProfessorDepartment of NeurologyNew York UniversityInvestigatorResearch ServiceVA New York Harbor Healthcare SystemmdashManhattan
CampusNew York New York
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xiv
Jonathan Lipton MD PhDAssistant Professor of NeurologyDepartment of Neurology and F M Kirby Center for
NeuroscienceBoston Childrenrsquos Hospital Harvard Medical SchoolBoston Massachusetts
Grisel Lopez MDSenior Staff ClinicianNational Human Genome Research InstituteNational Institutes of HealthBethesda Maryland
Dietrich Matern MD PhDProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
Berge A Minassian MDDivision ChiefPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas TexasUniversity of TorontoToronto Ontario Canada
Thomas Opladen MDDivision of Child Neurology and Metabolic DiseasesUniversity Childrenlsquos Hospital Heidelberg Germany
Sumit Parikh MDDirector of Cleveland Clinic Neurogenetics Metabolic
amp Mitochondrial Disease ProgramCleveland ClinicAssociate ProfessorDepartment of PediatricsCase Western Reserve University School of MedicineCleveland Ohio
Manisha Patel PhDProfessorDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Phillip L Pearl MDDirector of Epilepsy and Clinical NeurophysiologyWilliam G Lennox ChairBoston Childrenrsquos HospitalProfessor of NeurologyHarvard Medical SchoolBoston Massachusetts
Anna Lecticia Pinto MDAssistant in Neurology and Co-DirectorSturge Weber Clinic Boston Childrenrsquos HospitalLecturer of NeurologyHarvard Medical SchoolBoston Massachusetts
Barbara Plecko-Startinig MDHeadDivision of Child NeurologyChildrenrsquos Hospital ZurichProfessor of Child NeurologyUniversity of ZurichZurich Switzerland
Annapurna Poduri MD MPHEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Asuri N Prasad MBBS MD FRCPC FRCPEProfessor in Pediatrics and Clinical NeurosciencesDivision of Pediatric NeurologyDepartment of PediatricsSchulich School of Medicine and DentistryChildrenrsquos Hospital London Health Sciences CentreWestern UniversityLondon Ontario Canada
Morgan J Prust MDClinical Fellow in NeurologyDepartment of NeurologyMassachusetts General HospitalBrigham amp Womenrsquos HospitalBoston Massachusetts
Gerald V Raymond MDProfessorDepartment of NeurologyUniversity of Minnesota Medical SchoolMinneapolis Minnesota
Debra S Regier MD PhDDirector of Genetic and Genomic Education Medical
GeneticistRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Jong M Rho MDProfessor of Pediatrics Clinical Neurosciences
Physiology and PharmacologyDr Robert Haslam Chair in Child NeurologySection of Paediatric NeurologyCumming School of Medicine University of CalgaryAlberta Childrenrsquos HospitalCalgary Alberta Canada
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Lance H Rodan MDStaff PhysicianBoston Childrenrsquos HospitalBoston Massachusetts
Alexander Rotenberg MD PhDDirector Neuromodulation ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalAssociate Professor of NeurologyHarvard Medical SchoolBoston Massachusetts
Christopher Ryan LCSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Mustafa Sahin MD PhDProfessor of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Harvey B Sarnat MS MD FRCPCProfessor Departments of Paediatrics Pathology
(Neuropathology) and Clinical NeurosciencesUniversity of Calgary Cumming School of Medicine
and Alberta Childrenrsquos Hospital Research InstituteCalgary Alberta Canada
Joumlrn Oliver Sass Dr rer natProfessor of Bioanalytics and BiochemistryDepartment of Natural SciencesBonn-Rhein-Sieg University of Applied SciencesSankt Augustin Germany
Samata Singhi MDClinical Fellow in NeurologyDepartment of NeurologyBoston Childrenrsquos HospitalBoston Massachusetts
Susan E Sparks MD PhDMedical DirectorNA Medical AffairsRare DiseasesSanofi GenzymeCambridge Massachusetts
Carl E Stafstrom MD PhDProfessor of Neurology and PediatricsLederer Chair in Pediatric EpilepsyDirector Division of Pediatric NeurologyJohns Hopkins University School of MedicineBaltimore Maryland
Robert Steinfeld MD PhDProfessor of Neurometabolic and Neurodegenerative
Diseases in Childhood and AdolescenceDepartment of Pediatrics and Pediatric NeurologyUniversity Medical Center GoumlttingenGoumlttingen Germany
Marshall L Summar MDChief Division of Genetics and MetabolismMargaret OrsquoMalley Chair of Genetic MedicineRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Brahim Tabarki MDDivision of Pediatric NeurologyPrince Sultan Military Medical CityRiyadh Saudi ArabiaAssociate Professor of Neurology and PediatricsThe Ibn El Jazzar University School of MedicineSousse Tunisia
Pranoot Tanpaiboon MDAssociate Professor of PediatricsDivision of Genetics and MetabolismThe George Washington University School of Medicine
and Health SciencesChildrenrsquos National Health System Childrenrsquos National
Rare Disease InstituteWashington DC
Davide Tonduti MDChild NeurologistDepartment of Child NeurologyFondazione IRCCS Istituto Neurologico Carlo BestaMilano Italy
Johan L K Van Hove MD PhDProfessor of PediatricsSection of Clinical Genetics and Metabolism
Department of PediatricsUniversity of ColoradoAurora Colorado
Adeline Vanderver MDAttending PhysicianDivision of NeurologyProgram DirectorLeukodystrophy CenterJacob A Kamens Endowed Chair in Neurologic
Disorders and Translational NeurotherapeuticsChildrenrsquos Hospital of PhiladelphiaAssociate Professor of NeurologyPerelman School of Medicine at the University of
PennsylvaniaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xvi
Jodie M Vento MGC LCGCManagerCenter for Rare Disease TherapyManagerBrain Care InstituteManagerLaboratory Genetic Counseling ServicesChildrenrsquos Hospital of Pittsburgh of UPMCPittsburgh Pennsylvania
Brandy Verhalen PhDLab ManagerPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas Texas
Kara Vogel PhDPostdoctoral Research AssociateUniversity of WisconsinndashMadisonMadison Wisconsin
Matthew Whitehead MDRadiologistChildrenrsquos National Medical CenterWashington DC
Lynne A Wolfe MS CRNPSenior Nurse PractitionerUndiagnosed Disorders ProgramNational Human Genome Research Institute National
Institutes of HealthBethesda Maryland
Robert A Zimmerman MDProfessor of RadiologyRaymond and Ruth Perelman School of Medicine at the
University of PennsylvaniaChiefDivision of Neuroradiology and MRIThe Childrenrsquos Hospital of PhiladelphiaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Preface
This edition of Inherited Metabolic Epilepsies is a greatly expanded and updated version of the fi rst Following a rousing response to the fi rst edition far beyond any anticipated measure it was clear that a reexamination of the material taking into account many helpful sug-gestions that I received from readers far and wide was in order Despite my own misgivings that books are no longer fashionable and are largely replaced by journals and online sources that lend themselves to periodic if not continual updating there remains an appetite and clamor for books that accomplish what I had hoped to do originally and aim to achieve to a greater extent in this edition to encapsulate a burgeoning fi eld suf-fi ciently that a student practitioner or investigator can turn to the source with confi dence that the neces-sary background as well as detail will be available to reward the search for information and also move the fi eld forward
The fi rst edition of this monograph was born follow-ing the organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the annual meeting of the American Epilepsy Society in Boston in 2009 At the time of proposing the topic I was wrestling with a chasmic gap between the fascinat-ing disorders being discussed at the geneticndashmetabolic meetings and the advancing wave in epilepsy classifi ca-tion diagnosis and treatment occupying the meetings attended by members of the societies associated with neurology and epilepsy At that time a storybook series of investigations elucidated not only the surprising antiq-uitin defect in pyridoxine-dependent epilepsy but also the highly charged requirement that physicians consider a pivotal role for folinic acid and pyridoxal-5-phosphate in patients with virtually the same clinical presentation I also perceived a relative lack of awareness of disorders such as glucose transporter 1 defi ciency serine synthetic defects developmental delay epilepsy and neonatal dia-betes (DEND) and hyperinsulinismndashhyperammonemia (HIndashHA) that had very specifi c therapeutic implications with potential for dramatically improving outcome but with an even greater likelihood that they were escaping diagnosis
Overall the inherited metabolic epilepsies repre-sent a group of disorders that is rare individually but
in aggregate represents a substantial clinical burden as well as a vexing area for physicians investigators and students to master The sheer amount and complexity of information are overwhelming and require the physician to synthesize key concepts in neurology genetics and epilepsy As a pediatric epileptologist and medical edu-cator I have found this area among the most challenging and rewarding in practice and research The fi rst edition organized the disorders in a traditional approach under the roof of metabolism by dividing them into small- and large-molecule disorders In the Preface to that edition there was an explanation of various ways of organizing these disorders some more user friendly to the neurol-ogist than the small- versus large-molecule divide but this was an opportunity to present that way of thinking to the neurologist which brings this clinical specialty closer to that of genetics metabolism
In this second edition there is an expansion from four sections (General Principles Small Molecule Diseases Large Molecule Diseases and Conclusions) to six sec-tions with the addition of chapters in basic science and clinical science of the metabolic epilepsies The book has been expanded from 28 to 43 chapters with new chapters including overviews of metabolic disease and the basic science of metabolic epilepsy plus new topics such as metabolic energetics and implications of vital pathways A full chapter is devoted to the mechanistic target of rapamycin (mTOR) pathway that regulates cell replica-tion and so much of homeostasis and new pathophysi-ologic mechanisms such as protein anchoring disorders There are new chapters on neurotransmitter transmission measurement using transcranial magnetic stimulation genomic technologies and approaches to diagnosis and therapy referable to this group of disorders The clinical science section now includes a marvelous and refl ective chapter on neuropathology by Harvey B Sarnat There are new chapters devoted to specifi c disorders such as pyridoxal-5-phosphate dependency and Menkesrsquo disease There are chapters with completely new vantage points from community and family resources to an emphasis on adult patients the latter being the most commonly requested area to cover that I receive after giving talks on the subject In addition the prior chapters from the fi rst edition have been revised and updated
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xviii
Hence what began as a quest to increase awareness of treatable metabolic epilepsies fi rst became a mono-graph to give some form to this arena and has now been enlarged and updated to a second edition It is hoped that this will provide a resource to in some way lead the fi eld and carry it forward It is truly hoped that this book will educate if not enlighten physicians particularly
specialists and trainees in pediatric and adult neurology neurodevelopmental disabilities epilepsy and genetics while caring for patients with inherited metabolic epi-lepsies as well as spur further research into basic mecha-nisms and clinical trials in this group of maladies
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Acknowledgments
This book was fi rst suggested to me by Beth Barry from Demos Medical Publishers following my organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the American Epilepsy Society 2009 meeting Beth was a driving force for the creation of this second edition and she and Young Kim at Demos now aligned with Springer are gratefully acknowledged for unmatched hard work and persever-ance in seeing this through to completion
My education in child neurology and epilepsy is grounded by great mentors including Ralph D Feigin MD in pediatrics and Marvin A Fishman MD in pediat-ric neurology of Baylor College of Medicine in Houston and Gregory L Holmes MD in epilepsy and clinical neurophysiology then at Childrenrsquos Hospital Harvard Medical School in Boston I wish to take this opportunity to acknowledge these teachers of mine
My foray into metabolic disorders has been made pos-sible by the always helpful brilliant and steadfast work of Mike Gibson PhD whose collaboration in the area of gamma-amino butyric acid (GABA) disorders specifi -cally succinic-semialdehyde dehydrogenase (SSADH) defi ciency has been a constant source of intellectual
nourishment and encouragement My career during the two editions of this book has now spanned two great childrenrsquos hospitals Childrenrsquos National and Boston Childrenrsquos and the insight and support of colleagues at both institutions have been fundamental to this work Ongoing collaborations with Mike Gibson as well as William H Theodore MD chief of the Clinical Epilepsy Section at the NINDS have been critical to the ongoing investigative work on metabolic epilepsies
I thank each of the contributors to the fi rst edition of this book for revising and updating their chapters and each of the authors of the new chapters resulting in a signifi cant expansion The outstanding assistance of Alisa Marino is gratefully acknowledged given the enormous complexity of the project and the organiza-tional skills needed to accomplish this and a myriad of other tasks As a group I thank the many patients and families as well as students residents and fellows who inspire our work I thank my own family who as with all of us shoulder the largest burden of personal sacrifi ce and inspire us the most
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

32 Cerebral Folate Defi ciency and Epilepsy 407Robert Steinfeld
33 Menkesrsquo Disease and Infantile Epilepsy 415Asuri N Prasad
PART V LARGE MOLECULE DISEASES 34 Congenital Disorders of Glycosylation and Epilepsy 428
Susan E Sparks
35 Lysosomal Storage Diseases and Epilepsy 445Pranoot Tanpaiboon and Grisel Lopez
36 Peroxisomal Diseases and Epilepsy 473Parastoo Jangouk Kristin W Barantildeano and Gerald V Raymond
37 Leukodystrophies and Epilepsy 483Davide Tonduti and Adeline Vanderver
PART VI CONCLUSIONS 38 Diagnostic Approaches to Genetic Epilepsies 490
Erika Takle Axeen Christelle El Achkar and Annapurna Poduri
39 Therapeutic Approaches to Inherited Metabolic Epilepsies 497Brandy Verhalen and Berge A Minassian
40 Inherited Metabolic Epilepsies in Adults 503Phillip L Pearl
41 Genetic Counseling in Metabolic Epilepsies 508Jodie M Vento
42 Support and Resources for Patients and Families With Inherited Metabolic Epilepsies 518Christopher Ryan and Jennifer Jeffs
43 Clinical Approach to Inherited Metabolic Epilepsies 525Scott Demarest Anna Lecticia Pinto and Phillip L Pearl
Index 529
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Contributors
Nicholas S Abend MD MSCEAssociate Professor of Neurology and PediatricsDepartments of Neurology and PediatricsChildrenrsquos Hospital of Philadelphia and the University
of PennsylvaniaPhiladelphia Pennsylvania
Christelle El Achkar MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Cigdem I Akman MDAssociate Professor of Clinical Neurology and PediatricsDepartments of Neurology and PediatricsDivision of Pediatric NeurologyInterim ChiefChild NeurologyDirectorPediatric EpilepsyColumbia University College of Physicians and SurgeonsNew York New York
Mona Alduligan MDPhysicianDivision of Clinical NeurophysiologyChildrenrsquos National Medical CenterWashington DC
Mohammed Almuqbil MD FRCP (C)King Abdullah Specialist Childrenrsquos Hospital (KASCH)King Saud bin Abdulaziz University for Health Sciences
(KSAU-HS)Pediatric Neurology DivisionRiyadh Saudi ArabiaKing Abdullah International Medical Research Center
(KAIMRC)National Guard MinistryRiyadh Saudi ArabiaDivision of Genetics and GenomicsBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Yair Anikster MD PhDDirectorMetabolic Disease UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
Frances Ashcroft PhD ScDGlaxoSmithKline Royal Society Research ProfessorDepartment of Physiology Anatomy and GeneticsFellow of Trinity CollegeDirector OXIONUniversity of OxfordOxford England
Erika Takle Axeen MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Minnesota
Kristin W Barantildeano MD PhDClinical AssociatePediatric NeurologyDepartment of NeurologyJohns Hopkins HospitalAssistant Professor of NeurologyJohns Hopkins School of MedicineBaltimore Maryland
Bruria Ben-Zeev MDDirectorPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xii
Gerard T Berry MDDirector Metabolism ProgramProfessor of PediatricsBoston Childrenrsquos HospitalBoston Massachusetts
Nenad Blau PhDSenior Consultant in Biochemical GeneticsProfessor Emeritus of Clinical Biochemistry (UZH)Dietmar-Hopp Metabolic CenterUniversity Childrenrsquos HospitalHeidelberg Germany
Olaf A Bodamer MD PhDAssociate Chief of Genetics and GenomicsBoston Childrenrsquos HospitalPark Gerald Chair in Genetics and GenomicsHarvard Medical SchoolBoston Massachusetts
Andrew Breeden PhDProgram AnalystHealth Program SpecialistNational Institute of Neurological Disorders and
Stroke (NINDS)Bethesda Maryland
Kimberly A Chapman MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National
Health SystemWashington DC
Curtis R Coughlin II MS MBe CGCAssistant Professor of PediatricsSection of Clinical Genetics and MetabolismDepartment of PediatricsUniversity of ColoradoAurora Colorado
Ton de Grauw MD PhDChiefNeurosciencesChildrenrsquos Healthcare of AtlantaDirectorPediatric NeurologyEmory University School of MedicineAtlanta Georgia
T J de Koning MD PhDPaediatrician for Inborn Errors of MetabolismDepartment of Genetics and PaediatricsUniversity Medical Centre GroningenUniversity of GroningenGroningen The Netherlands
Darryl C De Vivo MDSidney Carter Professor of NeurologyProfessor of PediatricsPediatric Neurology ServiceFounding DirectorColleen Giblin Research Laboratories for Pediatric
NeurologyAssociate ChairmanPediatric Neurosciences and Developmental
NeurobiologyCo-DirectorMotor Neuron CenterDirectorSpinal Muscular Atrophy (SMA) CenterChief EmeritusPediatric NeurologyColumbia University Medical CenterNew York New York
Scott Demarest MDAssistant Professor of Pediatrics and NeurologyChildrenrsquos Hospital ColoradoUniversity of ColoradoAurora Colorado
Darius Ebrahimi-Fakhari MD DrmedResident PhysicianDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Susan L Fong MD PhDAssistant ResidentPediatric NeurologyJohns Hopkins HospitalBaltimore Maryland
Jamie L Fraser MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National Health
SystemWashington DC
Stanley T Fricke PhDPhysicistChildrenrsquos National Medical CenterWashington DC
Dimitar Gavrilov MD PhDAssistant ProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
K Michael Gibson PhDAllen I White Distinguished Professor and ChairDepartment of PharmacotherapyWashington State University College of PharmacySpokane Washington
Sidney M Gospe Jr MD PhDHerman and Faye Sarkowsky Endowed ChairProfessor and HeadDivision of Pediatric NeurologyDepartments of Neurology and PediatricsUniversity of WashingtonDivision of NeurologySeattle Childrenrsquos Hospital and Seattle Childrenrsquos
Research InstituteSeattle Washington
Andrea L Gropman MDChief Neurogenetics and Neurodevelopmental
PediatricsChildrenrsquos National Medical CenterAssociate Professor of Neurology and PediatricsGeorge Washington School of Medicine and Health
SciencesWashington DC
Ashwini Sri Hari PhD CandidateDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Gali Heimer MD PhDSenior Physician and Director of the Angelman ClinicPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical Center Tel-Hashomer Israel Sackler Faculty of MedicineTel-Aviv UniversityTel-Aviv IsraelMember of the Dr Pinchas Borenstein Talpiot Medical
Leadership ProgramSheba Medical CenterTel-Hashomer Israel
Julia B Hennermann MDProfessor of Metabolic DiseasesUniversity Medical Center MainzVilla Metabolica Department of Pediatric and
Adolescent MedicineMainz Germany
Christina Y Hung MDResearch AssociateHMS Instructor in PediatricsDivision for Human Genetics and GenomicsBoston Childrenrsquos HospitalBoston Massachusetts
Parastoo Jangouk MDGastroenterology and Hepatology FellowYale-New Haven HospitalNew Haven Connecticut
Jennifer Jeffs LICSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Hyder A Jinnah MD PhDProfessorDepartments of Neurology Human Genetics and
PediatricsEmory University School of MedicineAtlanta Georgia
Andrea Kelly MD MSCEAssociate Professor of Pediatrics CEDepartment of PediatricsChildrenrsquos Hospital of Philadelphia and Perelman School
of Medicine of the University of PennsylvaniaPhiladelphia Pennsylvania
Zarir P Khademian MD PhDAssistant Professor of Radiology and PediatricsStaff Neurologist Division of Diagnostic Imaging and
RadiologyChildrenrsquos National Medical CenterWashington DC
Eric H Kossoff MDProfessorNeurology and PediatricsJohns Hopkins HospitalBaltimore Maryland
Carolina Lahmann PhDPostdoctoral FellowHarvard Medical SchoolBoston Massachusetts
Brendan Lanpher MDAssistant Professor of Medical GeneticsDepartment of Clinical GenomicsMayo ClinicRochester Minnesota
Beth A Leeman-Markowski MD MA MMScAssistant ProfessorDepartment of NeurologyNew York UniversityInvestigatorResearch ServiceVA New York Harbor Healthcare SystemmdashManhattan
CampusNew York New York
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xiv
Jonathan Lipton MD PhDAssistant Professor of NeurologyDepartment of Neurology and F M Kirby Center for
NeuroscienceBoston Childrenrsquos Hospital Harvard Medical SchoolBoston Massachusetts
Grisel Lopez MDSenior Staff ClinicianNational Human Genome Research InstituteNational Institutes of HealthBethesda Maryland
Dietrich Matern MD PhDProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
Berge A Minassian MDDivision ChiefPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas TexasUniversity of TorontoToronto Ontario Canada
Thomas Opladen MDDivision of Child Neurology and Metabolic DiseasesUniversity Childrenlsquos Hospital Heidelberg Germany
Sumit Parikh MDDirector of Cleveland Clinic Neurogenetics Metabolic
amp Mitochondrial Disease ProgramCleveland ClinicAssociate ProfessorDepartment of PediatricsCase Western Reserve University School of MedicineCleveland Ohio
Manisha Patel PhDProfessorDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Phillip L Pearl MDDirector of Epilepsy and Clinical NeurophysiologyWilliam G Lennox ChairBoston Childrenrsquos HospitalProfessor of NeurologyHarvard Medical SchoolBoston Massachusetts
Anna Lecticia Pinto MDAssistant in Neurology and Co-DirectorSturge Weber Clinic Boston Childrenrsquos HospitalLecturer of NeurologyHarvard Medical SchoolBoston Massachusetts
Barbara Plecko-Startinig MDHeadDivision of Child NeurologyChildrenrsquos Hospital ZurichProfessor of Child NeurologyUniversity of ZurichZurich Switzerland
Annapurna Poduri MD MPHEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Asuri N Prasad MBBS MD FRCPC FRCPEProfessor in Pediatrics and Clinical NeurosciencesDivision of Pediatric NeurologyDepartment of PediatricsSchulich School of Medicine and DentistryChildrenrsquos Hospital London Health Sciences CentreWestern UniversityLondon Ontario Canada
Morgan J Prust MDClinical Fellow in NeurologyDepartment of NeurologyMassachusetts General HospitalBrigham amp Womenrsquos HospitalBoston Massachusetts
Gerald V Raymond MDProfessorDepartment of NeurologyUniversity of Minnesota Medical SchoolMinneapolis Minnesota
Debra S Regier MD PhDDirector of Genetic and Genomic Education Medical
GeneticistRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Jong M Rho MDProfessor of Pediatrics Clinical Neurosciences
Physiology and PharmacologyDr Robert Haslam Chair in Child NeurologySection of Paediatric NeurologyCumming School of Medicine University of CalgaryAlberta Childrenrsquos HospitalCalgary Alberta Canada
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Lance H Rodan MDStaff PhysicianBoston Childrenrsquos HospitalBoston Massachusetts
Alexander Rotenberg MD PhDDirector Neuromodulation ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalAssociate Professor of NeurologyHarvard Medical SchoolBoston Massachusetts
Christopher Ryan LCSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Mustafa Sahin MD PhDProfessor of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Harvey B Sarnat MS MD FRCPCProfessor Departments of Paediatrics Pathology
(Neuropathology) and Clinical NeurosciencesUniversity of Calgary Cumming School of Medicine
and Alberta Childrenrsquos Hospital Research InstituteCalgary Alberta Canada
Joumlrn Oliver Sass Dr rer natProfessor of Bioanalytics and BiochemistryDepartment of Natural SciencesBonn-Rhein-Sieg University of Applied SciencesSankt Augustin Germany
Samata Singhi MDClinical Fellow in NeurologyDepartment of NeurologyBoston Childrenrsquos HospitalBoston Massachusetts
Susan E Sparks MD PhDMedical DirectorNA Medical AffairsRare DiseasesSanofi GenzymeCambridge Massachusetts
Carl E Stafstrom MD PhDProfessor of Neurology and PediatricsLederer Chair in Pediatric EpilepsyDirector Division of Pediatric NeurologyJohns Hopkins University School of MedicineBaltimore Maryland
Robert Steinfeld MD PhDProfessor of Neurometabolic and Neurodegenerative
Diseases in Childhood and AdolescenceDepartment of Pediatrics and Pediatric NeurologyUniversity Medical Center GoumlttingenGoumlttingen Germany
Marshall L Summar MDChief Division of Genetics and MetabolismMargaret OrsquoMalley Chair of Genetic MedicineRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Brahim Tabarki MDDivision of Pediatric NeurologyPrince Sultan Military Medical CityRiyadh Saudi ArabiaAssociate Professor of Neurology and PediatricsThe Ibn El Jazzar University School of MedicineSousse Tunisia
Pranoot Tanpaiboon MDAssociate Professor of PediatricsDivision of Genetics and MetabolismThe George Washington University School of Medicine
and Health SciencesChildrenrsquos National Health System Childrenrsquos National
Rare Disease InstituteWashington DC
Davide Tonduti MDChild NeurologistDepartment of Child NeurologyFondazione IRCCS Istituto Neurologico Carlo BestaMilano Italy
Johan L K Van Hove MD PhDProfessor of PediatricsSection of Clinical Genetics and Metabolism
Department of PediatricsUniversity of ColoradoAurora Colorado
Adeline Vanderver MDAttending PhysicianDivision of NeurologyProgram DirectorLeukodystrophy CenterJacob A Kamens Endowed Chair in Neurologic
Disorders and Translational NeurotherapeuticsChildrenrsquos Hospital of PhiladelphiaAssociate Professor of NeurologyPerelman School of Medicine at the University of
PennsylvaniaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xvi
Jodie M Vento MGC LCGCManagerCenter for Rare Disease TherapyManagerBrain Care InstituteManagerLaboratory Genetic Counseling ServicesChildrenrsquos Hospital of Pittsburgh of UPMCPittsburgh Pennsylvania
Brandy Verhalen PhDLab ManagerPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas Texas
Kara Vogel PhDPostdoctoral Research AssociateUniversity of WisconsinndashMadisonMadison Wisconsin
Matthew Whitehead MDRadiologistChildrenrsquos National Medical CenterWashington DC
Lynne A Wolfe MS CRNPSenior Nurse PractitionerUndiagnosed Disorders ProgramNational Human Genome Research Institute National
Institutes of HealthBethesda Maryland
Robert A Zimmerman MDProfessor of RadiologyRaymond and Ruth Perelman School of Medicine at the
University of PennsylvaniaChiefDivision of Neuroradiology and MRIThe Childrenrsquos Hospital of PhiladelphiaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Preface
This edition of Inherited Metabolic Epilepsies is a greatly expanded and updated version of the fi rst Following a rousing response to the fi rst edition far beyond any anticipated measure it was clear that a reexamination of the material taking into account many helpful sug-gestions that I received from readers far and wide was in order Despite my own misgivings that books are no longer fashionable and are largely replaced by journals and online sources that lend themselves to periodic if not continual updating there remains an appetite and clamor for books that accomplish what I had hoped to do originally and aim to achieve to a greater extent in this edition to encapsulate a burgeoning fi eld suf-fi ciently that a student practitioner or investigator can turn to the source with confi dence that the neces-sary background as well as detail will be available to reward the search for information and also move the fi eld forward
The fi rst edition of this monograph was born follow-ing the organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the annual meeting of the American Epilepsy Society in Boston in 2009 At the time of proposing the topic I was wrestling with a chasmic gap between the fascinat-ing disorders being discussed at the geneticndashmetabolic meetings and the advancing wave in epilepsy classifi ca-tion diagnosis and treatment occupying the meetings attended by members of the societies associated with neurology and epilepsy At that time a storybook series of investigations elucidated not only the surprising antiq-uitin defect in pyridoxine-dependent epilepsy but also the highly charged requirement that physicians consider a pivotal role for folinic acid and pyridoxal-5-phosphate in patients with virtually the same clinical presentation I also perceived a relative lack of awareness of disorders such as glucose transporter 1 defi ciency serine synthetic defects developmental delay epilepsy and neonatal dia-betes (DEND) and hyperinsulinismndashhyperammonemia (HIndashHA) that had very specifi c therapeutic implications with potential for dramatically improving outcome but with an even greater likelihood that they were escaping diagnosis
Overall the inherited metabolic epilepsies repre-sent a group of disorders that is rare individually but
in aggregate represents a substantial clinical burden as well as a vexing area for physicians investigators and students to master The sheer amount and complexity of information are overwhelming and require the physician to synthesize key concepts in neurology genetics and epilepsy As a pediatric epileptologist and medical edu-cator I have found this area among the most challenging and rewarding in practice and research The fi rst edition organized the disorders in a traditional approach under the roof of metabolism by dividing them into small- and large-molecule disorders In the Preface to that edition there was an explanation of various ways of organizing these disorders some more user friendly to the neurol-ogist than the small- versus large-molecule divide but this was an opportunity to present that way of thinking to the neurologist which brings this clinical specialty closer to that of genetics metabolism
In this second edition there is an expansion from four sections (General Principles Small Molecule Diseases Large Molecule Diseases and Conclusions) to six sec-tions with the addition of chapters in basic science and clinical science of the metabolic epilepsies The book has been expanded from 28 to 43 chapters with new chapters including overviews of metabolic disease and the basic science of metabolic epilepsy plus new topics such as metabolic energetics and implications of vital pathways A full chapter is devoted to the mechanistic target of rapamycin (mTOR) pathway that regulates cell replica-tion and so much of homeostasis and new pathophysi-ologic mechanisms such as protein anchoring disorders There are new chapters on neurotransmitter transmission measurement using transcranial magnetic stimulation genomic technologies and approaches to diagnosis and therapy referable to this group of disorders The clinical science section now includes a marvelous and refl ective chapter on neuropathology by Harvey B Sarnat There are new chapters devoted to specifi c disorders such as pyridoxal-5-phosphate dependency and Menkesrsquo disease There are chapters with completely new vantage points from community and family resources to an emphasis on adult patients the latter being the most commonly requested area to cover that I receive after giving talks on the subject In addition the prior chapters from the fi rst edition have been revised and updated
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xviii
Hence what began as a quest to increase awareness of treatable metabolic epilepsies fi rst became a mono-graph to give some form to this arena and has now been enlarged and updated to a second edition It is hoped that this will provide a resource to in some way lead the fi eld and carry it forward It is truly hoped that this book will educate if not enlighten physicians particularly
specialists and trainees in pediatric and adult neurology neurodevelopmental disabilities epilepsy and genetics while caring for patients with inherited metabolic epi-lepsies as well as spur further research into basic mecha-nisms and clinical trials in this group of maladies
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Acknowledgments
This book was fi rst suggested to me by Beth Barry from Demos Medical Publishers following my organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the American Epilepsy Society 2009 meeting Beth was a driving force for the creation of this second edition and she and Young Kim at Demos now aligned with Springer are gratefully acknowledged for unmatched hard work and persever-ance in seeing this through to completion
My education in child neurology and epilepsy is grounded by great mentors including Ralph D Feigin MD in pediatrics and Marvin A Fishman MD in pediat-ric neurology of Baylor College of Medicine in Houston and Gregory L Holmes MD in epilepsy and clinical neurophysiology then at Childrenrsquos Hospital Harvard Medical School in Boston I wish to take this opportunity to acknowledge these teachers of mine
My foray into metabolic disorders has been made pos-sible by the always helpful brilliant and steadfast work of Mike Gibson PhD whose collaboration in the area of gamma-amino butyric acid (GABA) disorders specifi -cally succinic-semialdehyde dehydrogenase (SSADH) defi ciency has been a constant source of intellectual
nourishment and encouragement My career during the two editions of this book has now spanned two great childrenrsquos hospitals Childrenrsquos National and Boston Childrenrsquos and the insight and support of colleagues at both institutions have been fundamental to this work Ongoing collaborations with Mike Gibson as well as William H Theodore MD chief of the Clinical Epilepsy Section at the NINDS have been critical to the ongoing investigative work on metabolic epilepsies
I thank each of the contributors to the fi rst edition of this book for revising and updating their chapters and each of the authors of the new chapters resulting in a signifi cant expansion The outstanding assistance of Alisa Marino is gratefully acknowledged given the enormous complexity of the project and the organiza-tional skills needed to accomplish this and a myriad of other tasks As a group I thank the many patients and families as well as students residents and fellows who inspire our work I thank my own family who as with all of us shoulder the largest burden of personal sacrifi ce and inspire us the most
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Contributors
Nicholas S Abend MD MSCEAssociate Professor of Neurology and PediatricsDepartments of Neurology and PediatricsChildrenrsquos Hospital of Philadelphia and the University
of PennsylvaniaPhiladelphia Pennsylvania
Christelle El Achkar MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Cigdem I Akman MDAssociate Professor of Clinical Neurology and PediatricsDepartments of Neurology and PediatricsDivision of Pediatric NeurologyInterim ChiefChild NeurologyDirectorPediatric EpilepsyColumbia University College of Physicians and SurgeonsNew York New York
Mona Alduligan MDPhysicianDivision of Clinical NeurophysiologyChildrenrsquos National Medical CenterWashington DC
Mohammed Almuqbil MD FRCP (C)King Abdullah Specialist Childrenrsquos Hospital (KASCH)King Saud bin Abdulaziz University for Health Sciences
(KSAU-HS)Pediatric Neurology DivisionRiyadh Saudi ArabiaKing Abdullah International Medical Research Center
(KAIMRC)National Guard MinistryRiyadh Saudi ArabiaDivision of Genetics and GenomicsBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Yair Anikster MD PhDDirectorMetabolic Disease UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
Frances Ashcroft PhD ScDGlaxoSmithKline Royal Society Research ProfessorDepartment of Physiology Anatomy and GeneticsFellow of Trinity CollegeDirector OXIONUniversity of OxfordOxford England
Erika Takle Axeen MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Minnesota
Kristin W Barantildeano MD PhDClinical AssociatePediatric NeurologyDepartment of NeurologyJohns Hopkins HospitalAssistant Professor of NeurologyJohns Hopkins School of MedicineBaltimore Maryland
Bruria Ben-Zeev MDDirectorPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xii
Gerard T Berry MDDirector Metabolism ProgramProfessor of PediatricsBoston Childrenrsquos HospitalBoston Massachusetts
Nenad Blau PhDSenior Consultant in Biochemical GeneticsProfessor Emeritus of Clinical Biochemistry (UZH)Dietmar-Hopp Metabolic CenterUniversity Childrenrsquos HospitalHeidelberg Germany
Olaf A Bodamer MD PhDAssociate Chief of Genetics and GenomicsBoston Childrenrsquos HospitalPark Gerald Chair in Genetics and GenomicsHarvard Medical SchoolBoston Massachusetts
Andrew Breeden PhDProgram AnalystHealth Program SpecialistNational Institute of Neurological Disorders and
Stroke (NINDS)Bethesda Maryland
Kimberly A Chapman MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National
Health SystemWashington DC
Curtis R Coughlin II MS MBe CGCAssistant Professor of PediatricsSection of Clinical Genetics and MetabolismDepartment of PediatricsUniversity of ColoradoAurora Colorado
Ton de Grauw MD PhDChiefNeurosciencesChildrenrsquos Healthcare of AtlantaDirectorPediatric NeurologyEmory University School of MedicineAtlanta Georgia
T J de Koning MD PhDPaediatrician for Inborn Errors of MetabolismDepartment of Genetics and PaediatricsUniversity Medical Centre GroningenUniversity of GroningenGroningen The Netherlands
Darryl C De Vivo MDSidney Carter Professor of NeurologyProfessor of PediatricsPediatric Neurology ServiceFounding DirectorColleen Giblin Research Laboratories for Pediatric
NeurologyAssociate ChairmanPediatric Neurosciences and Developmental
NeurobiologyCo-DirectorMotor Neuron CenterDirectorSpinal Muscular Atrophy (SMA) CenterChief EmeritusPediatric NeurologyColumbia University Medical CenterNew York New York
Scott Demarest MDAssistant Professor of Pediatrics and NeurologyChildrenrsquos Hospital ColoradoUniversity of ColoradoAurora Colorado
Darius Ebrahimi-Fakhari MD DrmedResident PhysicianDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Susan L Fong MD PhDAssistant ResidentPediatric NeurologyJohns Hopkins HospitalBaltimore Maryland
Jamie L Fraser MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National Health
SystemWashington DC
Stanley T Fricke PhDPhysicistChildrenrsquos National Medical CenterWashington DC
Dimitar Gavrilov MD PhDAssistant ProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
K Michael Gibson PhDAllen I White Distinguished Professor and ChairDepartment of PharmacotherapyWashington State University College of PharmacySpokane Washington
Sidney M Gospe Jr MD PhDHerman and Faye Sarkowsky Endowed ChairProfessor and HeadDivision of Pediatric NeurologyDepartments of Neurology and PediatricsUniversity of WashingtonDivision of NeurologySeattle Childrenrsquos Hospital and Seattle Childrenrsquos
Research InstituteSeattle Washington
Andrea L Gropman MDChief Neurogenetics and Neurodevelopmental
PediatricsChildrenrsquos National Medical CenterAssociate Professor of Neurology and PediatricsGeorge Washington School of Medicine and Health
SciencesWashington DC
Ashwini Sri Hari PhD CandidateDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Gali Heimer MD PhDSenior Physician and Director of the Angelman ClinicPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical Center Tel-Hashomer Israel Sackler Faculty of MedicineTel-Aviv UniversityTel-Aviv IsraelMember of the Dr Pinchas Borenstein Talpiot Medical
Leadership ProgramSheba Medical CenterTel-Hashomer Israel
Julia B Hennermann MDProfessor of Metabolic DiseasesUniversity Medical Center MainzVilla Metabolica Department of Pediatric and
Adolescent MedicineMainz Germany
Christina Y Hung MDResearch AssociateHMS Instructor in PediatricsDivision for Human Genetics and GenomicsBoston Childrenrsquos HospitalBoston Massachusetts
Parastoo Jangouk MDGastroenterology and Hepatology FellowYale-New Haven HospitalNew Haven Connecticut
Jennifer Jeffs LICSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Hyder A Jinnah MD PhDProfessorDepartments of Neurology Human Genetics and
PediatricsEmory University School of MedicineAtlanta Georgia
Andrea Kelly MD MSCEAssociate Professor of Pediatrics CEDepartment of PediatricsChildrenrsquos Hospital of Philadelphia and Perelman School
of Medicine of the University of PennsylvaniaPhiladelphia Pennsylvania
Zarir P Khademian MD PhDAssistant Professor of Radiology and PediatricsStaff Neurologist Division of Diagnostic Imaging and
RadiologyChildrenrsquos National Medical CenterWashington DC
Eric H Kossoff MDProfessorNeurology and PediatricsJohns Hopkins HospitalBaltimore Maryland
Carolina Lahmann PhDPostdoctoral FellowHarvard Medical SchoolBoston Massachusetts
Brendan Lanpher MDAssistant Professor of Medical GeneticsDepartment of Clinical GenomicsMayo ClinicRochester Minnesota
Beth A Leeman-Markowski MD MA MMScAssistant ProfessorDepartment of NeurologyNew York UniversityInvestigatorResearch ServiceVA New York Harbor Healthcare SystemmdashManhattan
CampusNew York New York
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xiv
Jonathan Lipton MD PhDAssistant Professor of NeurologyDepartment of Neurology and F M Kirby Center for
NeuroscienceBoston Childrenrsquos Hospital Harvard Medical SchoolBoston Massachusetts
Grisel Lopez MDSenior Staff ClinicianNational Human Genome Research InstituteNational Institutes of HealthBethesda Maryland
Dietrich Matern MD PhDProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
Berge A Minassian MDDivision ChiefPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas TexasUniversity of TorontoToronto Ontario Canada
Thomas Opladen MDDivision of Child Neurology and Metabolic DiseasesUniversity Childrenlsquos Hospital Heidelberg Germany
Sumit Parikh MDDirector of Cleveland Clinic Neurogenetics Metabolic
amp Mitochondrial Disease ProgramCleveland ClinicAssociate ProfessorDepartment of PediatricsCase Western Reserve University School of MedicineCleveland Ohio
Manisha Patel PhDProfessorDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Phillip L Pearl MDDirector of Epilepsy and Clinical NeurophysiologyWilliam G Lennox ChairBoston Childrenrsquos HospitalProfessor of NeurologyHarvard Medical SchoolBoston Massachusetts
Anna Lecticia Pinto MDAssistant in Neurology and Co-DirectorSturge Weber Clinic Boston Childrenrsquos HospitalLecturer of NeurologyHarvard Medical SchoolBoston Massachusetts
Barbara Plecko-Startinig MDHeadDivision of Child NeurologyChildrenrsquos Hospital ZurichProfessor of Child NeurologyUniversity of ZurichZurich Switzerland
Annapurna Poduri MD MPHEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Asuri N Prasad MBBS MD FRCPC FRCPEProfessor in Pediatrics and Clinical NeurosciencesDivision of Pediatric NeurologyDepartment of PediatricsSchulich School of Medicine and DentistryChildrenrsquos Hospital London Health Sciences CentreWestern UniversityLondon Ontario Canada
Morgan J Prust MDClinical Fellow in NeurologyDepartment of NeurologyMassachusetts General HospitalBrigham amp Womenrsquos HospitalBoston Massachusetts
Gerald V Raymond MDProfessorDepartment of NeurologyUniversity of Minnesota Medical SchoolMinneapolis Minnesota
Debra S Regier MD PhDDirector of Genetic and Genomic Education Medical
GeneticistRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Jong M Rho MDProfessor of Pediatrics Clinical Neurosciences
Physiology and PharmacologyDr Robert Haslam Chair in Child NeurologySection of Paediatric NeurologyCumming School of Medicine University of CalgaryAlberta Childrenrsquos HospitalCalgary Alberta Canada
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Lance H Rodan MDStaff PhysicianBoston Childrenrsquos HospitalBoston Massachusetts
Alexander Rotenberg MD PhDDirector Neuromodulation ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalAssociate Professor of NeurologyHarvard Medical SchoolBoston Massachusetts
Christopher Ryan LCSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Mustafa Sahin MD PhDProfessor of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Harvey B Sarnat MS MD FRCPCProfessor Departments of Paediatrics Pathology
(Neuropathology) and Clinical NeurosciencesUniversity of Calgary Cumming School of Medicine
and Alberta Childrenrsquos Hospital Research InstituteCalgary Alberta Canada
Joumlrn Oliver Sass Dr rer natProfessor of Bioanalytics and BiochemistryDepartment of Natural SciencesBonn-Rhein-Sieg University of Applied SciencesSankt Augustin Germany
Samata Singhi MDClinical Fellow in NeurologyDepartment of NeurologyBoston Childrenrsquos HospitalBoston Massachusetts
Susan E Sparks MD PhDMedical DirectorNA Medical AffairsRare DiseasesSanofi GenzymeCambridge Massachusetts
Carl E Stafstrom MD PhDProfessor of Neurology and PediatricsLederer Chair in Pediatric EpilepsyDirector Division of Pediatric NeurologyJohns Hopkins University School of MedicineBaltimore Maryland
Robert Steinfeld MD PhDProfessor of Neurometabolic and Neurodegenerative
Diseases in Childhood and AdolescenceDepartment of Pediatrics and Pediatric NeurologyUniversity Medical Center GoumlttingenGoumlttingen Germany
Marshall L Summar MDChief Division of Genetics and MetabolismMargaret OrsquoMalley Chair of Genetic MedicineRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Brahim Tabarki MDDivision of Pediatric NeurologyPrince Sultan Military Medical CityRiyadh Saudi ArabiaAssociate Professor of Neurology and PediatricsThe Ibn El Jazzar University School of MedicineSousse Tunisia
Pranoot Tanpaiboon MDAssociate Professor of PediatricsDivision of Genetics and MetabolismThe George Washington University School of Medicine
and Health SciencesChildrenrsquos National Health System Childrenrsquos National
Rare Disease InstituteWashington DC
Davide Tonduti MDChild NeurologistDepartment of Child NeurologyFondazione IRCCS Istituto Neurologico Carlo BestaMilano Italy
Johan L K Van Hove MD PhDProfessor of PediatricsSection of Clinical Genetics and Metabolism
Department of PediatricsUniversity of ColoradoAurora Colorado
Adeline Vanderver MDAttending PhysicianDivision of NeurologyProgram DirectorLeukodystrophy CenterJacob A Kamens Endowed Chair in Neurologic
Disorders and Translational NeurotherapeuticsChildrenrsquos Hospital of PhiladelphiaAssociate Professor of NeurologyPerelman School of Medicine at the University of
PennsylvaniaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xvi
Jodie M Vento MGC LCGCManagerCenter for Rare Disease TherapyManagerBrain Care InstituteManagerLaboratory Genetic Counseling ServicesChildrenrsquos Hospital of Pittsburgh of UPMCPittsburgh Pennsylvania
Brandy Verhalen PhDLab ManagerPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas Texas
Kara Vogel PhDPostdoctoral Research AssociateUniversity of WisconsinndashMadisonMadison Wisconsin
Matthew Whitehead MDRadiologistChildrenrsquos National Medical CenterWashington DC
Lynne A Wolfe MS CRNPSenior Nurse PractitionerUndiagnosed Disorders ProgramNational Human Genome Research Institute National
Institutes of HealthBethesda Maryland
Robert A Zimmerman MDProfessor of RadiologyRaymond and Ruth Perelman School of Medicine at the
University of PennsylvaniaChiefDivision of Neuroradiology and MRIThe Childrenrsquos Hospital of PhiladelphiaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Preface
This edition of Inherited Metabolic Epilepsies is a greatly expanded and updated version of the fi rst Following a rousing response to the fi rst edition far beyond any anticipated measure it was clear that a reexamination of the material taking into account many helpful sug-gestions that I received from readers far and wide was in order Despite my own misgivings that books are no longer fashionable and are largely replaced by journals and online sources that lend themselves to periodic if not continual updating there remains an appetite and clamor for books that accomplish what I had hoped to do originally and aim to achieve to a greater extent in this edition to encapsulate a burgeoning fi eld suf-fi ciently that a student practitioner or investigator can turn to the source with confi dence that the neces-sary background as well as detail will be available to reward the search for information and also move the fi eld forward
The fi rst edition of this monograph was born follow-ing the organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the annual meeting of the American Epilepsy Society in Boston in 2009 At the time of proposing the topic I was wrestling with a chasmic gap between the fascinat-ing disorders being discussed at the geneticndashmetabolic meetings and the advancing wave in epilepsy classifi ca-tion diagnosis and treatment occupying the meetings attended by members of the societies associated with neurology and epilepsy At that time a storybook series of investigations elucidated not only the surprising antiq-uitin defect in pyridoxine-dependent epilepsy but also the highly charged requirement that physicians consider a pivotal role for folinic acid and pyridoxal-5-phosphate in patients with virtually the same clinical presentation I also perceived a relative lack of awareness of disorders such as glucose transporter 1 defi ciency serine synthetic defects developmental delay epilepsy and neonatal dia-betes (DEND) and hyperinsulinismndashhyperammonemia (HIndashHA) that had very specifi c therapeutic implications with potential for dramatically improving outcome but with an even greater likelihood that they were escaping diagnosis
Overall the inherited metabolic epilepsies repre-sent a group of disorders that is rare individually but
in aggregate represents a substantial clinical burden as well as a vexing area for physicians investigators and students to master The sheer amount and complexity of information are overwhelming and require the physician to synthesize key concepts in neurology genetics and epilepsy As a pediatric epileptologist and medical edu-cator I have found this area among the most challenging and rewarding in practice and research The fi rst edition organized the disorders in a traditional approach under the roof of metabolism by dividing them into small- and large-molecule disorders In the Preface to that edition there was an explanation of various ways of organizing these disorders some more user friendly to the neurol-ogist than the small- versus large-molecule divide but this was an opportunity to present that way of thinking to the neurologist which brings this clinical specialty closer to that of genetics metabolism
In this second edition there is an expansion from four sections (General Principles Small Molecule Diseases Large Molecule Diseases and Conclusions) to six sec-tions with the addition of chapters in basic science and clinical science of the metabolic epilepsies The book has been expanded from 28 to 43 chapters with new chapters including overviews of metabolic disease and the basic science of metabolic epilepsy plus new topics such as metabolic energetics and implications of vital pathways A full chapter is devoted to the mechanistic target of rapamycin (mTOR) pathway that regulates cell replica-tion and so much of homeostasis and new pathophysi-ologic mechanisms such as protein anchoring disorders There are new chapters on neurotransmitter transmission measurement using transcranial magnetic stimulation genomic technologies and approaches to diagnosis and therapy referable to this group of disorders The clinical science section now includes a marvelous and refl ective chapter on neuropathology by Harvey B Sarnat There are new chapters devoted to specifi c disorders such as pyridoxal-5-phosphate dependency and Menkesrsquo disease There are chapters with completely new vantage points from community and family resources to an emphasis on adult patients the latter being the most commonly requested area to cover that I receive after giving talks on the subject In addition the prior chapters from the fi rst edition have been revised and updated
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xviii
Hence what began as a quest to increase awareness of treatable metabolic epilepsies fi rst became a mono-graph to give some form to this arena and has now been enlarged and updated to a second edition It is hoped that this will provide a resource to in some way lead the fi eld and carry it forward It is truly hoped that this book will educate if not enlighten physicians particularly
specialists and trainees in pediatric and adult neurology neurodevelopmental disabilities epilepsy and genetics while caring for patients with inherited metabolic epi-lepsies as well as spur further research into basic mecha-nisms and clinical trials in this group of maladies
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Acknowledgments
This book was fi rst suggested to me by Beth Barry from Demos Medical Publishers following my organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the American Epilepsy Society 2009 meeting Beth was a driving force for the creation of this second edition and she and Young Kim at Demos now aligned with Springer are gratefully acknowledged for unmatched hard work and persever-ance in seeing this through to completion
My education in child neurology and epilepsy is grounded by great mentors including Ralph D Feigin MD in pediatrics and Marvin A Fishman MD in pediat-ric neurology of Baylor College of Medicine in Houston and Gregory L Holmes MD in epilepsy and clinical neurophysiology then at Childrenrsquos Hospital Harvard Medical School in Boston I wish to take this opportunity to acknowledge these teachers of mine
My foray into metabolic disorders has been made pos-sible by the always helpful brilliant and steadfast work of Mike Gibson PhD whose collaboration in the area of gamma-amino butyric acid (GABA) disorders specifi -cally succinic-semialdehyde dehydrogenase (SSADH) defi ciency has been a constant source of intellectual
nourishment and encouragement My career during the two editions of this book has now spanned two great childrenrsquos hospitals Childrenrsquos National and Boston Childrenrsquos and the insight and support of colleagues at both institutions have been fundamental to this work Ongoing collaborations with Mike Gibson as well as William H Theodore MD chief of the Clinical Epilepsy Section at the NINDS have been critical to the ongoing investigative work on metabolic epilepsies
I thank each of the contributors to the fi rst edition of this book for revising and updating their chapters and each of the authors of the new chapters resulting in a signifi cant expansion The outstanding assistance of Alisa Marino is gratefully acknowledged given the enormous complexity of the project and the organiza-tional skills needed to accomplish this and a myriad of other tasks As a group I thank the many patients and families as well as students residents and fellows who inspire our work I thank my own family who as with all of us shoulder the largest burden of personal sacrifi ce and inspire us the most
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

Contributors
Nicholas S Abend MD MSCEAssociate Professor of Neurology and PediatricsDepartments of Neurology and PediatricsChildrenrsquos Hospital of Philadelphia and the University
of PennsylvaniaPhiladelphia Pennsylvania
Christelle El Achkar MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Cigdem I Akman MDAssociate Professor of Clinical Neurology and PediatricsDepartments of Neurology and PediatricsDivision of Pediatric NeurologyInterim ChiefChild NeurologyDirectorPediatric EpilepsyColumbia University College of Physicians and SurgeonsNew York New York
Mona Alduligan MDPhysicianDivision of Clinical NeurophysiologyChildrenrsquos National Medical CenterWashington DC
Mohammed Almuqbil MD FRCP (C)King Abdullah Specialist Childrenrsquos Hospital (KASCH)King Saud bin Abdulaziz University for Health Sciences
(KSAU-HS)Pediatric Neurology DivisionRiyadh Saudi ArabiaKing Abdullah International Medical Research Center
(KAIMRC)National Guard MinistryRiyadh Saudi ArabiaDivision of Genetics and GenomicsBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Yair Anikster MD PhDDirectorMetabolic Disease UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
Frances Ashcroft PhD ScDGlaxoSmithKline Royal Society Research ProfessorDepartment of Physiology Anatomy and GeneticsFellow of Trinity CollegeDirector OXIONUniversity of OxfordOxford England
Erika Takle Axeen MDEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Minnesota
Kristin W Barantildeano MD PhDClinical AssociatePediatric NeurologyDepartment of NeurologyJohns Hopkins HospitalAssistant Professor of NeurologyJohns Hopkins School of MedicineBaltimore Maryland
Bruria Ben-Zeev MDDirectorPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical CenterTel-Hashomer IsraelProfessorSackler Faculty of MedicineTel-Aviv UniversityTel-Aviv Israel
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xii
Gerard T Berry MDDirector Metabolism ProgramProfessor of PediatricsBoston Childrenrsquos HospitalBoston Massachusetts
Nenad Blau PhDSenior Consultant in Biochemical GeneticsProfessor Emeritus of Clinical Biochemistry (UZH)Dietmar-Hopp Metabolic CenterUniversity Childrenrsquos HospitalHeidelberg Germany
Olaf A Bodamer MD PhDAssociate Chief of Genetics and GenomicsBoston Childrenrsquos HospitalPark Gerald Chair in Genetics and GenomicsHarvard Medical SchoolBoston Massachusetts
Andrew Breeden PhDProgram AnalystHealth Program SpecialistNational Institute of Neurological Disorders and
Stroke (NINDS)Bethesda Maryland
Kimberly A Chapman MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National
Health SystemWashington DC
Curtis R Coughlin II MS MBe CGCAssistant Professor of PediatricsSection of Clinical Genetics and MetabolismDepartment of PediatricsUniversity of ColoradoAurora Colorado
Ton de Grauw MD PhDChiefNeurosciencesChildrenrsquos Healthcare of AtlantaDirectorPediatric NeurologyEmory University School of MedicineAtlanta Georgia
T J de Koning MD PhDPaediatrician for Inborn Errors of MetabolismDepartment of Genetics and PaediatricsUniversity Medical Centre GroningenUniversity of GroningenGroningen The Netherlands
Darryl C De Vivo MDSidney Carter Professor of NeurologyProfessor of PediatricsPediatric Neurology ServiceFounding DirectorColleen Giblin Research Laboratories for Pediatric
NeurologyAssociate ChairmanPediatric Neurosciences and Developmental
NeurobiologyCo-DirectorMotor Neuron CenterDirectorSpinal Muscular Atrophy (SMA) CenterChief EmeritusPediatric NeurologyColumbia University Medical CenterNew York New York
Scott Demarest MDAssistant Professor of Pediatrics and NeurologyChildrenrsquos Hospital ColoradoUniversity of ColoradoAurora Colorado
Darius Ebrahimi-Fakhari MD DrmedResident PhysicianDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Susan L Fong MD PhDAssistant ResidentPediatric NeurologyJohns Hopkins HospitalBaltimore Maryland
Jamie L Fraser MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National Health
SystemWashington DC
Stanley T Fricke PhDPhysicistChildrenrsquos National Medical CenterWashington DC
Dimitar Gavrilov MD PhDAssistant ProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
K Michael Gibson PhDAllen I White Distinguished Professor and ChairDepartment of PharmacotherapyWashington State University College of PharmacySpokane Washington
Sidney M Gospe Jr MD PhDHerman and Faye Sarkowsky Endowed ChairProfessor and HeadDivision of Pediatric NeurologyDepartments of Neurology and PediatricsUniversity of WashingtonDivision of NeurologySeattle Childrenrsquos Hospital and Seattle Childrenrsquos
Research InstituteSeattle Washington
Andrea L Gropman MDChief Neurogenetics and Neurodevelopmental
PediatricsChildrenrsquos National Medical CenterAssociate Professor of Neurology and PediatricsGeorge Washington School of Medicine and Health
SciencesWashington DC
Ashwini Sri Hari PhD CandidateDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Gali Heimer MD PhDSenior Physician and Director of the Angelman ClinicPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical Center Tel-Hashomer Israel Sackler Faculty of MedicineTel-Aviv UniversityTel-Aviv IsraelMember of the Dr Pinchas Borenstein Talpiot Medical
Leadership ProgramSheba Medical CenterTel-Hashomer Israel
Julia B Hennermann MDProfessor of Metabolic DiseasesUniversity Medical Center MainzVilla Metabolica Department of Pediatric and
Adolescent MedicineMainz Germany
Christina Y Hung MDResearch AssociateHMS Instructor in PediatricsDivision for Human Genetics and GenomicsBoston Childrenrsquos HospitalBoston Massachusetts
Parastoo Jangouk MDGastroenterology and Hepatology FellowYale-New Haven HospitalNew Haven Connecticut
Jennifer Jeffs LICSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Hyder A Jinnah MD PhDProfessorDepartments of Neurology Human Genetics and
PediatricsEmory University School of MedicineAtlanta Georgia
Andrea Kelly MD MSCEAssociate Professor of Pediatrics CEDepartment of PediatricsChildrenrsquos Hospital of Philadelphia and Perelman School
of Medicine of the University of PennsylvaniaPhiladelphia Pennsylvania
Zarir P Khademian MD PhDAssistant Professor of Radiology and PediatricsStaff Neurologist Division of Diagnostic Imaging and
RadiologyChildrenrsquos National Medical CenterWashington DC
Eric H Kossoff MDProfessorNeurology and PediatricsJohns Hopkins HospitalBaltimore Maryland
Carolina Lahmann PhDPostdoctoral FellowHarvard Medical SchoolBoston Massachusetts
Brendan Lanpher MDAssistant Professor of Medical GeneticsDepartment of Clinical GenomicsMayo ClinicRochester Minnesota
Beth A Leeman-Markowski MD MA MMScAssistant ProfessorDepartment of NeurologyNew York UniversityInvestigatorResearch ServiceVA New York Harbor Healthcare SystemmdashManhattan
CampusNew York New York
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xiv
Jonathan Lipton MD PhDAssistant Professor of NeurologyDepartment of Neurology and F M Kirby Center for
NeuroscienceBoston Childrenrsquos Hospital Harvard Medical SchoolBoston Massachusetts
Grisel Lopez MDSenior Staff ClinicianNational Human Genome Research InstituteNational Institutes of HealthBethesda Maryland
Dietrich Matern MD PhDProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
Berge A Minassian MDDivision ChiefPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas TexasUniversity of TorontoToronto Ontario Canada
Thomas Opladen MDDivision of Child Neurology and Metabolic DiseasesUniversity Childrenlsquos Hospital Heidelberg Germany
Sumit Parikh MDDirector of Cleveland Clinic Neurogenetics Metabolic
amp Mitochondrial Disease ProgramCleveland ClinicAssociate ProfessorDepartment of PediatricsCase Western Reserve University School of MedicineCleveland Ohio
Manisha Patel PhDProfessorDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Phillip L Pearl MDDirector of Epilepsy and Clinical NeurophysiologyWilliam G Lennox ChairBoston Childrenrsquos HospitalProfessor of NeurologyHarvard Medical SchoolBoston Massachusetts
Anna Lecticia Pinto MDAssistant in Neurology and Co-DirectorSturge Weber Clinic Boston Childrenrsquos HospitalLecturer of NeurologyHarvard Medical SchoolBoston Massachusetts
Barbara Plecko-Startinig MDHeadDivision of Child NeurologyChildrenrsquos Hospital ZurichProfessor of Child NeurologyUniversity of ZurichZurich Switzerland
Annapurna Poduri MD MPHEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Asuri N Prasad MBBS MD FRCPC FRCPEProfessor in Pediatrics and Clinical NeurosciencesDivision of Pediatric NeurologyDepartment of PediatricsSchulich School of Medicine and DentistryChildrenrsquos Hospital London Health Sciences CentreWestern UniversityLondon Ontario Canada
Morgan J Prust MDClinical Fellow in NeurologyDepartment of NeurologyMassachusetts General HospitalBrigham amp Womenrsquos HospitalBoston Massachusetts
Gerald V Raymond MDProfessorDepartment of NeurologyUniversity of Minnesota Medical SchoolMinneapolis Minnesota
Debra S Regier MD PhDDirector of Genetic and Genomic Education Medical
GeneticistRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Jong M Rho MDProfessor of Pediatrics Clinical Neurosciences
Physiology and PharmacologyDr Robert Haslam Chair in Child NeurologySection of Paediatric NeurologyCumming School of Medicine University of CalgaryAlberta Childrenrsquos HospitalCalgary Alberta Canada
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Lance H Rodan MDStaff PhysicianBoston Childrenrsquos HospitalBoston Massachusetts
Alexander Rotenberg MD PhDDirector Neuromodulation ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalAssociate Professor of NeurologyHarvard Medical SchoolBoston Massachusetts
Christopher Ryan LCSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Mustafa Sahin MD PhDProfessor of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Harvey B Sarnat MS MD FRCPCProfessor Departments of Paediatrics Pathology
(Neuropathology) and Clinical NeurosciencesUniversity of Calgary Cumming School of Medicine
and Alberta Childrenrsquos Hospital Research InstituteCalgary Alberta Canada
Joumlrn Oliver Sass Dr rer natProfessor of Bioanalytics and BiochemistryDepartment of Natural SciencesBonn-Rhein-Sieg University of Applied SciencesSankt Augustin Germany
Samata Singhi MDClinical Fellow in NeurologyDepartment of NeurologyBoston Childrenrsquos HospitalBoston Massachusetts
Susan E Sparks MD PhDMedical DirectorNA Medical AffairsRare DiseasesSanofi GenzymeCambridge Massachusetts
Carl E Stafstrom MD PhDProfessor of Neurology and PediatricsLederer Chair in Pediatric EpilepsyDirector Division of Pediatric NeurologyJohns Hopkins University School of MedicineBaltimore Maryland
Robert Steinfeld MD PhDProfessor of Neurometabolic and Neurodegenerative
Diseases in Childhood and AdolescenceDepartment of Pediatrics and Pediatric NeurologyUniversity Medical Center GoumlttingenGoumlttingen Germany
Marshall L Summar MDChief Division of Genetics and MetabolismMargaret OrsquoMalley Chair of Genetic MedicineRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Brahim Tabarki MDDivision of Pediatric NeurologyPrince Sultan Military Medical CityRiyadh Saudi ArabiaAssociate Professor of Neurology and PediatricsThe Ibn El Jazzar University School of MedicineSousse Tunisia
Pranoot Tanpaiboon MDAssociate Professor of PediatricsDivision of Genetics and MetabolismThe George Washington University School of Medicine
and Health SciencesChildrenrsquos National Health System Childrenrsquos National
Rare Disease InstituteWashington DC
Davide Tonduti MDChild NeurologistDepartment of Child NeurologyFondazione IRCCS Istituto Neurologico Carlo BestaMilano Italy
Johan L K Van Hove MD PhDProfessor of PediatricsSection of Clinical Genetics and Metabolism
Department of PediatricsUniversity of ColoradoAurora Colorado
Adeline Vanderver MDAttending PhysicianDivision of NeurologyProgram DirectorLeukodystrophy CenterJacob A Kamens Endowed Chair in Neurologic
Disorders and Translational NeurotherapeuticsChildrenrsquos Hospital of PhiladelphiaAssociate Professor of NeurologyPerelman School of Medicine at the University of
PennsylvaniaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xvi
Jodie M Vento MGC LCGCManagerCenter for Rare Disease TherapyManagerBrain Care InstituteManagerLaboratory Genetic Counseling ServicesChildrenrsquos Hospital of Pittsburgh of UPMCPittsburgh Pennsylvania
Brandy Verhalen PhDLab ManagerPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas Texas
Kara Vogel PhDPostdoctoral Research AssociateUniversity of WisconsinndashMadisonMadison Wisconsin
Matthew Whitehead MDRadiologistChildrenrsquos National Medical CenterWashington DC
Lynne A Wolfe MS CRNPSenior Nurse PractitionerUndiagnosed Disorders ProgramNational Human Genome Research Institute National
Institutes of HealthBethesda Maryland
Robert A Zimmerman MDProfessor of RadiologyRaymond and Ruth Perelman School of Medicine at the
University of PennsylvaniaChiefDivision of Neuroradiology and MRIThe Childrenrsquos Hospital of PhiladelphiaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Preface
This edition of Inherited Metabolic Epilepsies is a greatly expanded and updated version of the fi rst Following a rousing response to the fi rst edition far beyond any anticipated measure it was clear that a reexamination of the material taking into account many helpful sug-gestions that I received from readers far and wide was in order Despite my own misgivings that books are no longer fashionable and are largely replaced by journals and online sources that lend themselves to periodic if not continual updating there remains an appetite and clamor for books that accomplish what I had hoped to do originally and aim to achieve to a greater extent in this edition to encapsulate a burgeoning fi eld suf-fi ciently that a student practitioner or investigator can turn to the source with confi dence that the neces-sary background as well as detail will be available to reward the search for information and also move the fi eld forward
The fi rst edition of this monograph was born follow-ing the organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the annual meeting of the American Epilepsy Society in Boston in 2009 At the time of proposing the topic I was wrestling with a chasmic gap between the fascinat-ing disorders being discussed at the geneticndashmetabolic meetings and the advancing wave in epilepsy classifi ca-tion diagnosis and treatment occupying the meetings attended by members of the societies associated with neurology and epilepsy At that time a storybook series of investigations elucidated not only the surprising antiq-uitin defect in pyridoxine-dependent epilepsy but also the highly charged requirement that physicians consider a pivotal role for folinic acid and pyridoxal-5-phosphate in patients with virtually the same clinical presentation I also perceived a relative lack of awareness of disorders such as glucose transporter 1 defi ciency serine synthetic defects developmental delay epilepsy and neonatal dia-betes (DEND) and hyperinsulinismndashhyperammonemia (HIndashHA) that had very specifi c therapeutic implications with potential for dramatically improving outcome but with an even greater likelihood that they were escaping diagnosis
Overall the inherited metabolic epilepsies repre-sent a group of disorders that is rare individually but
in aggregate represents a substantial clinical burden as well as a vexing area for physicians investigators and students to master The sheer amount and complexity of information are overwhelming and require the physician to synthesize key concepts in neurology genetics and epilepsy As a pediatric epileptologist and medical edu-cator I have found this area among the most challenging and rewarding in practice and research The fi rst edition organized the disorders in a traditional approach under the roof of metabolism by dividing them into small- and large-molecule disorders In the Preface to that edition there was an explanation of various ways of organizing these disorders some more user friendly to the neurol-ogist than the small- versus large-molecule divide but this was an opportunity to present that way of thinking to the neurologist which brings this clinical specialty closer to that of genetics metabolism
In this second edition there is an expansion from four sections (General Principles Small Molecule Diseases Large Molecule Diseases and Conclusions) to six sec-tions with the addition of chapters in basic science and clinical science of the metabolic epilepsies The book has been expanded from 28 to 43 chapters with new chapters including overviews of metabolic disease and the basic science of metabolic epilepsy plus new topics such as metabolic energetics and implications of vital pathways A full chapter is devoted to the mechanistic target of rapamycin (mTOR) pathway that regulates cell replica-tion and so much of homeostasis and new pathophysi-ologic mechanisms such as protein anchoring disorders There are new chapters on neurotransmitter transmission measurement using transcranial magnetic stimulation genomic technologies and approaches to diagnosis and therapy referable to this group of disorders The clinical science section now includes a marvelous and refl ective chapter on neuropathology by Harvey B Sarnat There are new chapters devoted to specifi c disorders such as pyridoxal-5-phosphate dependency and Menkesrsquo disease There are chapters with completely new vantage points from community and family resources to an emphasis on adult patients the latter being the most commonly requested area to cover that I receive after giving talks on the subject In addition the prior chapters from the fi rst edition have been revised and updated
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xviii
Hence what began as a quest to increase awareness of treatable metabolic epilepsies fi rst became a mono-graph to give some form to this arena and has now been enlarged and updated to a second edition It is hoped that this will provide a resource to in some way lead the fi eld and carry it forward It is truly hoped that this book will educate if not enlighten physicians particularly
specialists and trainees in pediatric and adult neurology neurodevelopmental disabilities epilepsy and genetics while caring for patients with inherited metabolic epi-lepsies as well as spur further research into basic mecha-nisms and clinical trials in this group of maladies
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Acknowledgments
This book was fi rst suggested to me by Beth Barry from Demos Medical Publishers following my organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the American Epilepsy Society 2009 meeting Beth was a driving force for the creation of this second edition and she and Young Kim at Demos now aligned with Springer are gratefully acknowledged for unmatched hard work and persever-ance in seeing this through to completion
My education in child neurology and epilepsy is grounded by great mentors including Ralph D Feigin MD in pediatrics and Marvin A Fishman MD in pediat-ric neurology of Baylor College of Medicine in Houston and Gregory L Holmes MD in epilepsy and clinical neurophysiology then at Childrenrsquos Hospital Harvard Medical School in Boston I wish to take this opportunity to acknowledge these teachers of mine
My foray into metabolic disorders has been made pos-sible by the always helpful brilliant and steadfast work of Mike Gibson PhD whose collaboration in the area of gamma-amino butyric acid (GABA) disorders specifi -cally succinic-semialdehyde dehydrogenase (SSADH) defi ciency has been a constant source of intellectual
nourishment and encouragement My career during the two editions of this book has now spanned two great childrenrsquos hospitals Childrenrsquos National and Boston Childrenrsquos and the insight and support of colleagues at both institutions have been fundamental to this work Ongoing collaborations with Mike Gibson as well as William H Theodore MD chief of the Clinical Epilepsy Section at the NINDS have been critical to the ongoing investigative work on metabolic epilepsies
I thank each of the contributors to the fi rst edition of this book for revising and updating their chapters and each of the authors of the new chapters resulting in a signifi cant expansion The outstanding assistance of Alisa Marino is gratefully acknowledged given the enormous complexity of the project and the organiza-tional skills needed to accomplish this and a myriad of other tasks As a group I thank the many patients and families as well as students residents and fellows who inspire our work I thank my own family who as with all of us shoulder the largest burden of personal sacrifi ce and inspire us the most
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

xii
Gerard T Berry MDDirector Metabolism ProgramProfessor of PediatricsBoston Childrenrsquos HospitalBoston Massachusetts
Nenad Blau PhDSenior Consultant in Biochemical GeneticsProfessor Emeritus of Clinical Biochemistry (UZH)Dietmar-Hopp Metabolic CenterUniversity Childrenrsquos HospitalHeidelberg Germany
Olaf A Bodamer MD PhDAssociate Chief of Genetics and GenomicsBoston Childrenrsquos HospitalPark Gerald Chair in Genetics and GenomicsHarvard Medical SchoolBoston Massachusetts
Andrew Breeden PhDProgram AnalystHealth Program SpecialistNational Institute of Neurological Disorders and
Stroke (NINDS)Bethesda Maryland
Kimberly A Chapman MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National
Health SystemWashington DC
Curtis R Coughlin II MS MBe CGCAssistant Professor of PediatricsSection of Clinical Genetics and MetabolismDepartment of PediatricsUniversity of ColoradoAurora Colorado
Ton de Grauw MD PhDChiefNeurosciencesChildrenrsquos Healthcare of AtlantaDirectorPediatric NeurologyEmory University School of MedicineAtlanta Georgia
T J de Koning MD PhDPaediatrician for Inborn Errors of MetabolismDepartment of Genetics and PaediatricsUniversity Medical Centre GroningenUniversity of GroningenGroningen The Netherlands
Darryl C De Vivo MDSidney Carter Professor of NeurologyProfessor of PediatricsPediatric Neurology ServiceFounding DirectorColleen Giblin Research Laboratories for Pediatric
NeurologyAssociate ChairmanPediatric Neurosciences and Developmental
NeurobiologyCo-DirectorMotor Neuron CenterDirectorSpinal Muscular Atrophy (SMA) CenterChief EmeritusPediatric NeurologyColumbia University Medical CenterNew York New York
Scott Demarest MDAssistant Professor of Pediatrics and NeurologyChildrenrsquos Hospital ColoradoUniversity of ColoradoAurora Colorado
Darius Ebrahimi-Fakhari MD DrmedResident PhysicianDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Susan L Fong MD PhDAssistant ResidentPediatric NeurologyJohns Hopkins HospitalBaltimore Maryland
Jamie L Fraser MD PhDAssistant ProfessorGeorge Washington UniversityGenetics and Metabolism Childrenrsquos National Health
SystemWashington DC
Stanley T Fricke PhDPhysicistChildrenrsquos National Medical CenterWashington DC
Dimitar Gavrilov MD PhDAssistant ProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
K Michael Gibson PhDAllen I White Distinguished Professor and ChairDepartment of PharmacotherapyWashington State University College of PharmacySpokane Washington
Sidney M Gospe Jr MD PhDHerman and Faye Sarkowsky Endowed ChairProfessor and HeadDivision of Pediatric NeurologyDepartments of Neurology and PediatricsUniversity of WashingtonDivision of NeurologySeattle Childrenrsquos Hospital and Seattle Childrenrsquos
Research InstituteSeattle Washington
Andrea L Gropman MDChief Neurogenetics and Neurodevelopmental
PediatricsChildrenrsquos National Medical CenterAssociate Professor of Neurology and PediatricsGeorge Washington School of Medicine and Health
SciencesWashington DC
Ashwini Sri Hari PhD CandidateDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Gali Heimer MD PhDSenior Physician and Director of the Angelman ClinicPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical Center Tel-Hashomer Israel Sackler Faculty of MedicineTel-Aviv UniversityTel-Aviv IsraelMember of the Dr Pinchas Borenstein Talpiot Medical
Leadership ProgramSheba Medical CenterTel-Hashomer Israel
Julia B Hennermann MDProfessor of Metabolic DiseasesUniversity Medical Center MainzVilla Metabolica Department of Pediatric and
Adolescent MedicineMainz Germany
Christina Y Hung MDResearch AssociateHMS Instructor in PediatricsDivision for Human Genetics and GenomicsBoston Childrenrsquos HospitalBoston Massachusetts
Parastoo Jangouk MDGastroenterology and Hepatology FellowYale-New Haven HospitalNew Haven Connecticut
Jennifer Jeffs LICSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Hyder A Jinnah MD PhDProfessorDepartments of Neurology Human Genetics and
PediatricsEmory University School of MedicineAtlanta Georgia
Andrea Kelly MD MSCEAssociate Professor of Pediatrics CEDepartment of PediatricsChildrenrsquos Hospital of Philadelphia and Perelman School
of Medicine of the University of PennsylvaniaPhiladelphia Pennsylvania
Zarir P Khademian MD PhDAssistant Professor of Radiology and PediatricsStaff Neurologist Division of Diagnostic Imaging and
RadiologyChildrenrsquos National Medical CenterWashington DC
Eric H Kossoff MDProfessorNeurology and PediatricsJohns Hopkins HospitalBaltimore Maryland
Carolina Lahmann PhDPostdoctoral FellowHarvard Medical SchoolBoston Massachusetts
Brendan Lanpher MDAssistant Professor of Medical GeneticsDepartment of Clinical GenomicsMayo ClinicRochester Minnesota
Beth A Leeman-Markowski MD MA MMScAssistant ProfessorDepartment of NeurologyNew York UniversityInvestigatorResearch ServiceVA New York Harbor Healthcare SystemmdashManhattan
CampusNew York New York
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xiv
Jonathan Lipton MD PhDAssistant Professor of NeurologyDepartment of Neurology and F M Kirby Center for
NeuroscienceBoston Childrenrsquos Hospital Harvard Medical SchoolBoston Massachusetts
Grisel Lopez MDSenior Staff ClinicianNational Human Genome Research InstituteNational Institutes of HealthBethesda Maryland
Dietrich Matern MD PhDProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
Berge A Minassian MDDivision ChiefPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas TexasUniversity of TorontoToronto Ontario Canada
Thomas Opladen MDDivision of Child Neurology and Metabolic DiseasesUniversity Childrenlsquos Hospital Heidelberg Germany
Sumit Parikh MDDirector of Cleveland Clinic Neurogenetics Metabolic
amp Mitochondrial Disease ProgramCleveland ClinicAssociate ProfessorDepartment of PediatricsCase Western Reserve University School of MedicineCleveland Ohio
Manisha Patel PhDProfessorDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Phillip L Pearl MDDirector of Epilepsy and Clinical NeurophysiologyWilliam G Lennox ChairBoston Childrenrsquos HospitalProfessor of NeurologyHarvard Medical SchoolBoston Massachusetts
Anna Lecticia Pinto MDAssistant in Neurology and Co-DirectorSturge Weber Clinic Boston Childrenrsquos HospitalLecturer of NeurologyHarvard Medical SchoolBoston Massachusetts
Barbara Plecko-Startinig MDHeadDivision of Child NeurologyChildrenrsquos Hospital ZurichProfessor of Child NeurologyUniversity of ZurichZurich Switzerland
Annapurna Poduri MD MPHEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Asuri N Prasad MBBS MD FRCPC FRCPEProfessor in Pediatrics and Clinical NeurosciencesDivision of Pediatric NeurologyDepartment of PediatricsSchulich School of Medicine and DentistryChildrenrsquos Hospital London Health Sciences CentreWestern UniversityLondon Ontario Canada
Morgan J Prust MDClinical Fellow in NeurologyDepartment of NeurologyMassachusetts General HospitalBrigham amp Womenrsquos HospitalBoston Massachusetts
Gerald V Raymond MDProfessorDepartment of NeurologyUniversity of Minnesota Medical SchoolMinneapolis Minnesota
Debra S Regier MD PhDDirector of Genetic and Genomic Education Medical
GeneticistRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Jong M Rho MDProfessor of Pediatrics Clinical Neurosciences
Physiology and PharmacologyDr Robert Haslam Chair in Child NeurologySection of Paediatric NeurologyCumming School of Medicine University of CalgaryAlberta Childrenrsquos HospitalCalgary Alberta Canada
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Lance H Rodan MDStaff PhysicianBoston Childrenrsquos HospitalBoston Massachusetts
Alexander Rotenberg MD PhDDirector Neuromodulation ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalAssociate Professor of NeurologyHarvard Medical SchoolBoston Massachusetts
Christopher Ryan LCSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Mustafa Sahin MD PhDProfessor of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Harvey B Sarnat MS MD FRCPCProfessor Departments of Paediatrics Pathology
(Neuropathology) and Clinical NeurosciencesUniversity of Calgary Cumming School of Medicine
and Alberta Childrenrsquos Hospital Research InstituteCalgary Alberta Canada
Joumlrn Oliver Sass Dr rer natProfessor of Bioanalytics and BiochemistryDepartment of Natural SciencesBonn-Rhein-Sieg University of Applied SciencesSankt Augustin Germany
Samata Singhi MDClinical Fellow in NeurologyDepartment of NeurologyBoston Childrenrsquos HospitalBoston Massachusetts
Susan E Sparks MD PhDMedical DirectorNA Medical AffairsRare DiseasesSanofi GenzymeCambridge Massachusetts
Carl E Stafstrom MD PhDProfessor of Neurology and PediatricsLederer Chair in Pediatric EpilepsyDirector Division of Pediatric NeurologyJohns Hopkins University School of MedicineBaltimore Maryland
Robert Steinfeld MD PhDProfessor of Neurometabolic and Neurodegenerative
Diseases in Childhood and AdolescenceDepartment of Pediatrics and Pediatric NeurologyUniversity Medical Center GoumlttingenGoumlttingen Germany
Marshall L Summar MDChief Division of Genetics and MetabolismMargaret OrsquoMalley Chair of Genetic MedicineRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Brahim Tabarki MDDivision of Pediatric NeurologyPrince Sultan Military Medical CityRiyadh Saudi ArabiaAssociate Professor of Neurology and PediatricsThe Ibn El Jazzar University School of MedicineSousse Tunisia
Pranoot Tanpaiboon MDAssociate Professor of PediatricsDivision of Genetics and MetabolismThe George Washington University School of Medicine
and Health SciencesChildrenrsquos National Health System Childrenrsquos National
Rare Disease InstituteWashington DC
Davide Tonduti MDChild NeurologistDepartment of Child NeurologyFondazione IRCCS Istituto Neurologico Carlo BestaMilano Italy
Johan L K Van Hove MD PhDProfessor of PediatricsSection of Clinical Genetics and Metabolism
Department of PediatricsUniversity of ColoradoAurora Colorado
Adeline Vanderver MDAttending PhysicianDivision of NeurologyProgram DirectorLeukodystrophy CenterJacob A Kamens Endowed Chair in Neurologic
Disorders and Translational NeurotherapeuticsChildrenrsquos Hospital of PhiladelphiaAssociate Professor of NeurologyPerelman School of Medicine at the University of
PennsylvaniaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xvi
Jodie M Vento MGC LCGCManagerCenter for Rare Disease TherapyManagerBrain Care InstituteManagerLaboratory Genetic Counseling ServicesChildrenrsquos Hospital of Pittsburgh of UPMCPittsburgh Pennsylvania
Brandy Verhalen PhDLab ManagerPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas Texas
Kara Vogel PhDPostdoctoral Research AssociateUniversity of WisconsinndashMadisonMadison Wisconsin
Matthew Whitehead MDRadiologistChildrenrsquos National Medical CenterWashington DC
Lynne A Wolfe MS CRNPSenior Nurse PractitionerUndiagnosed Disorders ProgramNational Human Genome Research Institute National
Institutes of HealthBethesda Maryland
Robert A Zimmerman MDProfessor of RadiologyRaymond and Ruth Perelman School of Medicine at the
University of PennsylvaniaChiefDivision of Neuroradiology and MRIThe Childrenrsquos Hospital of PhiladelphiaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Preface
This edition of Inherited Metabolic Epilepsies is a greatly expanded and updated version of the fi rst Following a rousing response to the fi rst edition far beyond any anticipated measure it was clear that a reexamination of the material taking into account many helpful sug-gestions that I received from readers far and wide was in order Despite my own misgivings that books are no longer fashionable and are largely replaced by journals and online sources that lend themselves to periodic if not continual updating there remains an appetite and clamor for books that accomplish what I had hoped to do originally and aim to achieve to a greater extent in this edition to encapsulate a burgeoning fi eld suf-fi ciently that a student practitioner or investigator can turn to the source with confi dence that the neces-sary background as well as detail will be available to reward the search for information and also move the fi eld forward
The fi rst edition of this monograph was born follow-ing the organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the annual meeting of the American Epilepsy Society in Boston in 2009 At the time of proposing the topic I was wrestling with a chasmic gap between the fascinat-ing disorders being discussed at the geneticndashmetabolic meetings and the advancing wave in epilepsy classifi ca-tion diagnosis and treatment occupying the meetings attended by members of the societies associated with neurology and epilepsy At that time a storybook series of investigations elucidated not only the surprising antiq-uitin defect in pyridoxine-dependent epilepsy but also the highly charged requirement that physicians consider a pivotal role for folinic acid and pyridoxal-5-phosphate in patients with virtually the same clinical presentation I also perceived a relative lack of awareness of disorders such as glucose transporter 1 defi ciency serine synthetic defects developmental delay epilepsy and neonatal dia-betes (DEND) and hyperinsulinismndashhyperammonemia (HIndashHA) that had very specifi c therapeutic implications with potential for dramatically improving outcome but with an even greater likelihood that they were escaping diagnosis
Overall the inherited metabolic epilepsies repre-sent a group of disorders that is rare individually but
in aggregate represents a substantial clinical burden as well as a vexing area for physicians investigators and students to master The sheer amount and complexity of information are overwhelming and require the physician to synthesize key concepts in neurology genetics and epilepsy As a pediatric epileptologist and medical edu-cator I have found this area among the most challenging and rewarding in practice and research The fi rst edition organized the disorders in a traditional approach under the roof of metabolism by dividing them into small- and large-molecule disorders In the Preface to that edition there was an explanation of various ways of organizing these disorders some more user friendly to the neurol-ogist than the small- versus large-molecule divide but this was an opportunity to present that way of thinking to the neurologist which brings this clinical specialty closer to that of genetics metabolism
In this second edition there is an expansion from four sections (General Principles Small Molecule Diseases Large Molecule Diseases and Conclusions) to six sec-tions with the addition of chapters in basic science and clinical science of the metabolic epilepsies The book has been expanded from 28 to 43 chapters with new chapters including overviews of metabolic disease and the basic science of metabolic epilepsy plus new topics such as metabolic energetics and implications of vital pathways A full chapter is devoted to the mechanistic target of rapamycin (mTOR) pathway that regulates cell replica-tion and so much of homeostasis and new pathophysi-ologic mechanisms such as protein anchoring disorders There are new chapters on neurotransmitter transmission measurement using transcranial magnetic stimulation genomic technologies and approaches to diagnosis and therapy referable to this group of disorders The clinical science section now includes a marvelous and refl ective chapter on neuropathology by Harvey B Sarnat There are new chapters devoted to specifi c disorders such as pyridoxal-5-phosphate dependency and Menkesrsquo disease There are chapters with completely new vantage points from community and family resources to an emphasis on adult patients the latter being the most commonly requested area to cover that I receive after giving talks on the subject In addition the prior chapters from the fi rst edition have been revised and updated
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xviii
Hence what began as a quest to increase awareness of treatable metabolic epilepsies fi rst became a mono-graph to give some form to this arena and has now been enlarged and updated to a second edition It is hoped that this will provide a resource to in some way lead the fi eld and carry it forward It is truly hoped that this book will educate if not enlighten physicians particularly
specialists and trainees in pediatric and adult neurology neurodevelopmental disabilities epilepsy and genetics while caring for patients with inherited metabolic epi-lepsies as well as spur further research into basic mecha-nisms and clinical trials in this group of maladies
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Acknowledgments
This book was fi rst suggested to me by Beth Barry from Demos Medical Publishers following my organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the American Epilepsy Society 2009 meeting Beth was a driving force for the creation of this second edition and she and Young Kim at Demos now aligned with Springer are gratefully acknowledged for unmatched hard work and persever-ance in seeing this through to completion
My education in child neurology and epilepsy is grounded by great mentors including Ralph D Feigin MD in pediatrics and Marvin A Fishman MD in pediat-ric neurology of Baylor College of Medicine in Houston and Gregory L Holmes MD in epilepsy and clinical neurophysiology then at Childrenrsquos Hospital Harvard Medical School in Boston I wish to take this opportunity to acknowledge these teachers of mine
My foray into metabolic disorders has been made pos-sible by the always helpful brilliant and steadfast work of Mike Gibson PhD whose collaboration in the area of gamma-amino butyric acid (GABA) disorders specifi -cally succinic-semialdehyde dehydrogenase (SSADH) defi ciency has been a constant source of intellectual
nourishment and encouragement My career during the two editions of this book has now spanned two great childrenrsquos hospitals Childrenrsquos National and Boston Childrenrsquos and the insight and support of colleagues at both institutions have been fundamental to this work Ongoing collaborations with Mike Gibson as well as William H Theodore MD chief of the Clinical Epilepsy Section at the NINDS have been critical to the ongoing investigative work on metabolic epilepsies
I thank each of the contributors to the fi rst edition of this book for revising and updating their chapters and each of the authors of the new chapters resulting in a signifi cant expansion The outstanding assistance of Alisa Marino is gratefully acknowledged given the enormous complexity of the project and the organiza-tional skills needed to accomplish this and a myriad of other tasks As a group I thank the many patients and families as well as students residents and fellows who inspire our work I thank my own family who as with all of us shoulder the largest burden of personal sacrifi ce and inspire us the most
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

K Michael Gibson PhDAllen I White Distinguished Professor and ChairDepartment of PharmacotherapyWashington State University College of PharmacySpokane Washington
Sidney M Gospe Jr MD PhDHerman and Faye Sarkowsky Endowed ChairProfessor and HeadDivision of Pediatric NeurologyDepartments of Neurology and PediatricsUniversity of WashingtonDivision of NeurologySeattle Childrenrsquos Hospital and Seattle Childrenrsquos
Research InstituteSeattle Washington
Andrea L Gropman MDChief Neurogenetics and Neurodevelopmental
PediatricsChildrenrsquos National Medical CenterAssociate Professor of Neurology and PediatricsGeorge Washington School of Medicine and Health
SciencesWashington DC
Ashwini Sri Hari PhD CandidateDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Gali Heimer MD PhDSenior Physician and Director of the Angelman ClinicPediatric Neurology UnitEdmond and Lily Safra Childrenrsquos HospitalSheba Medical Center Tel-Hashomer Israel Sackler Faculty of MedicineTel-Aviv UniversityTel-Aviv IsraelMember of the Dr Pinchas Borenstein Talpiot Medical
Leadership ProgramSheba Medical CenterTel-Hashomer Israel
Julia B Hennermann MDProfessor of Metabolic DiseasesUniversity Medical Center MainzVilla Metabolica Department of Pediatric and
Adolescent MedicineMainz Germany
Christina Y Hung MDResearch AssociateHMS Instructor in PediatricsDivision for Human Genetics and GenomicsBoston Childrenrsquos HospitalBoston Massachusetts
Parastoo Jangouk MDGastroenterology and Hepatology FellowYale-New Haven HospitalNew Haven Connecticut
Jennifer Jeffs LICSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Hyder A Jinnah MD PhDProfessorDepartments of Neurology Human Genetics and
PediatricsEmory University School of MedicineAtlanta Georgia
Andrea Kelly MD MSCEAssociate Professor of Pediatrics CEDepartment of PediatricsChildrenrsquos Hospital of Philadelphia and Perelman School
of Medicine of the University of PennsylvaniaPhiladelphia Pennsylvania
Zarir P Khademian MD PhDAssistant Professor of Radiology and PediatricsStaff Neurologist Division of Diagnostic Imaging and
RadiologyChildrenrsquos National Medical CenterWashington DC
Eric H Kossoff MDProfessorNeurology and PediatricsJohns Hopkins HospitalBaltimore Maryland
Carolina Lahmann PhDPostdoctoral FellowHarvard Medical SchoolBoston Massachusetts
Brendan Lanpher MDAssistant Professor of Medical GeneticsDepartment of Clinical GenomicsMayo ClinicRochester Minnesota
Beth A Leeman-Markowski MD MA MMScAssistant ProfessorDepartment of NeurologyNew York UniversityInvestigatorResearch ServiceVA New York Harbor Healthcare SystemmdashManhattan
CampusNew York New York
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xiv
Jonathan Lipton MD PhDAssistant Professor of NeurologyDepartment of Neurology and F M Kirby Center for
NeuroscienceBoston Childrenrsquos Hospital Harvard Medical SchoolBoston Massachusetts
Grisel Lopez MDSenior Staff ClinicianNational Human Genome Research InstituteNational Institutes of HealthBethesda Maryland
Dietrich Matern MD PhDProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
Berge A Minassian MDDivision ChiefPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas TexasUniversity of TorontoToronto Ontario Canada
Thomas Opladen MDDivision of Child Neurology and Metabolic DiseasesUniversity Childrenlsquos Hospital Heidelberg Germany
Sumit Parikh MDDirector of Cleveland Clinic Neurogenetics Metabolic
amp Mitochondrial Disease ProgramCleveland ClinicAssociate ProfessorDepartment of PediatricsCase Western Reserve University School of MedicineCleveland Ohio
Manisha Patel PhDProfessorDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Phillip L Pearl MDDirector of Epilepsy and Clinical NeurophysiologyWilliam G Lennox ChairBoston Childrenrsquos HospitalProfessor of NeurologyHarvard Medical SchoolBoston Massachusetts
Anna Lecticia Pinto MDAssistant in Neurology and Co-DirectorSturge Weber Clinic Boston Childrenrsquos HospitalLecturer of NeurologyHarvard Medical SchoolBoston Massachusetts
Barbara Plecko-Startinig MDHeadDivision of Child NeurologyChildrenrsquos Hospital ZurichProfessor of Child NeurologyUniversity of ZurichZurich Switzerland
Annapurna Poduri MD MPHEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Asuri N Prasad MBBS MD FRCPC FRCPEProfessor in Pediatrics and Clinical NeurosciencesDivision of Pediatric NeurologyDepartment of PediatricsSchulich School of Medicine and DentistryChildrenrsquos Hospital London Health Sciences CentreWestern UniversityLondon Ontario Canada
Morgan J Prust MDClinical Fellow in NeurologyDepartment of NeurologyMassachusetts General HospitalBrigham amp Womenrsquos HospitalBoston Massachusetts
Gerald V Raymond MDProfessorDepartment of NeurologyUniversity of Minnesota Medical SchoolMinneapolis Minnesota
Debra S Regier MD PhDDirector of Genetic and Genomic Education Medical
GeneticistRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Jong M Rho MDProfessor of Pediatrics Clinical Neurosciences
Physiology and PharmacologyDr Robert Haslam Chair in Child NeurologySection of Paediatric NeurologyCumming School of Medicine University of CalgaryAlberta Childrenrsquos HospitalCalgary Alberta Canada
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Lance H Rodan MDStaff PhysicianBoston Childrenrsquos HospitalBoston Massachusetts
Alexander Rotenberg MD PhDDirector Neuromodulation ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalAssociate Professor of NeurologyHarvard Medical SchoolBoston Massachusetts
Christopher Ryan LCSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Mustafa Sahin MD PhDProfessor of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Harvey B Sarnat MS MD FRCPCProfessor Departments of Paediatrics Pathology
(Neuropathology) and Clinical NeurosciencesUniversity of Calgary Cumming School of Medicine
and Alberta Childrenrsquos Hospital Research InstituteCalgary Alberta Canada
Joumlrn Oliver Sass Dr rer natProfessor of Bioanalytics and BiochemistryDepartment of Natural SciencesBonn-Rhein-Sieg University of Applied SciencesSankt Augustin Germany
Samata Singhi MDClinical Fellow in NeurologyDepartment of NeurologyBoston Childrenrsquos HospitalBoston Massachusetts
Susan E Sparks MD PhDMedical DirectorNA Medical AffairsRare DiseasesSanofi GenzymeCambridge Massachusetts
Carl E Stafstrom MD PhDProfessor of Neurology and PediatricsLederer Chair in Pediatric EpilepsyDirector Division of Pediatric NeurologyJohns Hopkins University School of MedicineBaltimore Maryland
Robert Steinfeld MD PhDProfessor of Neurometabolic and Neurodegenerative
Diseases in Childhood and AdolescenceDepartment of Pediatrics and Pediatric NeurologyUniversity Medical Center GoumlttingenGoumlttingen Germany
Marshall L Summar MDChief Division of Genetics and MetabolismMargaret OrsquoMalley Chair of Genetic MedicineRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Brahim Tabarki MDDivision of Pediatric NeurologyPrince Sultan Military Medical CityRiyadh Saudi ArabiaAssociate Professor of Neurology and PediatricsThe Ibn El Jazzar University School of MedicineSousse Tunisia
Pranoot Tanpaiboon MDAssociate Professor of PediatricsDivision of Genetics and MetabolismThe George Washington University School of Medicine
and Health SciencesChildrenrsquos National Health System Childrenrsquos National
Rare Disease InstituteWashington DC
Davide Tonduti MDChild NeurologistDepartment of Child NeurologyFondazione IRCCS Istituto Neurologico Carlo BestaMilano Italy
Johan L K Van Hove MD PhDProfessor of PediatricsSection of Clinical Genetics and Metabolism
Department of PediatricsUniversity of ColoradoAurora Colorado
Adeline Vanderver MDAttending PhysicianDivision of NeurologyProgram DirectorLeukodystrophy CenterJacob A Kamens Endowed Chair in Neurologic
Disorders and Translational NeurotherapeuticsChildrenrsquos Hospital of PhiladelphiaAssociate Professor of NeurologyPerelman School of Medicine at the University of
PennsylvaniaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xvi
Jodie M Vento MGC LCGCManagerCenter for Rare Disease TherapyManagerBrain Care InstituteManagerLaboratory Genetic Counseling ServicesChildrenrsquos Hospital of Pittsburgh of UPMCPittsburgh Pennsylvania
Brandy Verhalen PhDLab ManagerPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas Texas
Kara Vogel PhDPostdoctoral Research AssociateUniversity of WisconsinndashMadisonMadison Wisconsin
Matthew Whitehead MDRadiologistChildrenrsquos National Medical CenterWashington DC
Lynne A Wolfe MS CRNPSenior Nurse PractitionerUndiagnosed Disorders ProgramNational Human Genome Research Institute National
Institutes of HealthBethesda Maryland
Robert A Zimmerman MDProfessor of RadiologyRaymond and Ruth Perelman School of Medicine at the
University of PennsylvaniaChiefDivision of Neuroradiology and MRIThe Childrenrsquos Hospital of PhiladelphiaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Preface
This edition of Inherited Metabolic Epilepsies is a greatly expanded and updated version of the fi rst Following a rousing response to the fi rst edition far beyond any anticipated measure it was clear that a reexamination of the material taking into account many helpful sug-gestions that I received from readers far and wide was in order Despite my own misgivings that books are no longer fashionable and are largely replaced by journals and online sources that lend themselves to periodic if not continual updating there remains an appetite and clamor for books that accomplish what I had hoped to do originally and aim to achieve to a greater extent in this edition to encapsulate a burgeoning fi eld suf-fi ciently that a student practitioner or investigator can turn to the source with confi dence that the neces-sary background as well as detail will be available to reward the search for information and also move the fi eld forward
The fi rst edition of this monograph was born follow-ing the organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the annual meeting of the American Epilepsy Society in Boston in 2009 At the time of proposing the topic I was wrestling with a chasmic gap between the fascinat-ing disorders being discussed at the geneticndashmetabolic meetings and the advancing wave in epilepsy classifi ca-tion diagnosis and treatment occupying the meetings attended by members of the societies associated with neurology and epilepsy At that time a storybook series of investigations elucidated not only the surprising antiq-uitin defect in pyridoxine-dependent epilepsy but also the highly charged requirement that physicians consider a pivotal role for folinic acid and pyridoxal-5-phosphate in patients with virtually the same clinical presentation I also perceived a relative lack of awareness of disorders such as glucose transporter 1 defi ciency serine synthetic defects developmental delay epilepsy and neonatal dia-betes (DEND) and hyperinsulinismndashhyperammonemia (HIndashHA) that had very specifi c therapeutic implications with potential for dramatically improving outcome but with an even greater likelihood that they were escaping diagnosis
Overall the inherited metabolic epilepsies repre-sent a group of disorders that is rare individually but
in aggregate represents a substantial clinical burden as well as a vexing area for physicians investigators and students to master The sheer amount and complexity of information are overwhelming and require the physician to synthesize key concepts in neurology genetics and epilepsy As a pediatric epileptologist and medical edu-cator I have found this area among the most challenging and rewarding in practice and research The fi rst edition organized the disorders in a traditional approach under the roof of metabolism by dividing them into small- and large-molecule disorders In the Preface to that edition there was an explanation of various ways of organizing these disorders some more user friendly to the neurol-ogist than the small- versus large-molecule divide but this was an opportunity to present that way of thinking to the neurologist which brings this clinical specialty closer to that of genetics metabolism
In this second edition there is an expansion from four sections (General Principles Small Molecule Diseases Large Molecule Diseases and Conclusions) to six sec-tions with the addition of chapters in basic science and clinical science of the metabolic epilepsies The book has been expanded from 28 to 43 chapters with new chapters including overviews of metabolic disease and the basic science of metabolic epilepsy plus new topics such as metabolic energetics and implications of vital pathways A full chapter is devoted to the mechanistic target of rapamycin (mTOR) pathway that regulates cell replica-tion and so much of homeostasis and new pathophysi-ologic mechanisms such as protein anchoring disorders There are new chapters on neurotransmitter transmission measurement using transcranial magnetic stimulation genomic technologies and approaches to diagnosis and therapy referable to this group of disorders The clinical science section now includes a marvelous and refl ective chapter on neuropathology by Harvey B Sarnat There are new chapters devoted to specifi c disorders such as pyridoxal-5-phosphate dependency and Menkesrsquo disease There are chapters with completely new vantage points from community and family resources to an emphasis on adult patients the latter being the most commonly requested area to cover that I receive after giving talks on the subject In addition the prior chapters from the fi rst edition have been revised and updated
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xviii
Hence what began as a quest to increase awareness of treatable metabolic epilepsies fi rst became a mono-graph to give some form to this arena and has now been enlarged and updated to a second edition It is hoped that this will provide a resource to in some way lead the fi eld and carry it forward It is truly hoped that this book will educate if not enlighten physicians particularly
specialists and trainees in pediatric and adult neurology neurodevelopmental disabilities epilepsy and genetics while caring for patients with inherited metabolic epi-lepsies as well as spur further research into basic mecha-nisms and clinical trials in this group of maladies
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Acknowledgments
This book was fi rst suggested to me by Beth Barry from Demos Medical Publishers following my organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the American Epilepsy Society 2009 meeting Beth was a driving force for the creation of this second edition and she and Young Kim at Demos now aligned with Springer are gratefully acknowledged for unmatched hard work and persever-ance in seeing this through to completion
My education in child neurology and epilepsy is grounded by great mentors including Ralph D Feigin MD in pediatrics and Marvin A Fishman MD in pediat-ric neurology of Baylor College of Medicine in Houston and Gregory L Holmes MD in epilepsy and clinical neurophysiology then at Childrenrsquos Hospital Harvard Medical School in Boston I wish to take this opportunity to acknowledge these teachers of mine
My foray into metabolic disorders has been made pos-sible by the always helpful brilliant and steadfast work of Mike Gibson PhD whose collaboration in the area of gamma-amino butyric acid (GABA) disorders specifi -cally succinic-semialdehyde dehydrogenase (SSADH) defi ciency has been a constant source of intellectual
nourishment and encouragement My career during the two editions of this book has now spanned two great childrenrsquos hospitals Childrenrsquos National and Boston Childrenrsquos and the insight and support of colleagues at both institutions have been fundamental to this work Ongoing collaborations with Mike Gibson as well as William H Theodore MD chief of the Clinical Epilepsy Section at the NINDS have been critical to the ongoing investigative work on metabolic epilepsies
I thank each of the contributors to the fi rst edition of this book for revising and updating their chapters and each of the authors of the new chapters resulting in a signifi cant expansion The outstanding assistance of Alisa Marino is gratefully acknowledged given the enormous complexity of the project and the organiza-tional skills needed to accomplish this and a myriad of other tasks As a group I thank the many patients and families as well as students residents and fellows who inspire our work I thank my own family who as with all of us shoulder the largest burden of personal sacrifi ce and inspire us the most
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

xiv
Jonathan Lipton MD PhDAssistant Professor of NeurologyDepartment of Neurology and F M Kirby Center for
NeuroscienceBoston Childrenrsquos Hospital Harvard Medical SchoolBoston Massachusetts
Grisel Lopez MDSenior Staff ClinicianNational Human Genome Research InstituteNational Institutes of HealthBethesda Maryland
Dietrich Matern MD PhDProfessorLaboratory Medicine amp Pathology Medical Genetics
and PediatricsBiochemical Genetics LaboratoryMayo Clinic College of MedicineRochester Minnesota
Berge A Minassian MDDivision ChiefPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas TexasUniversity of TorontoToronto Ontario Canada
Thomas Opladen MDDivision of Child Neurology and Metabolic DiseasesUniversity Childrenlsquos Hospital Heidelberg Germany
Sumit Parikh MDDirector of Cleveland Clinic Neurogenetics Metabolic
amp Mitochondrial Disease ProgramCleveland ClinicAssociate ProfessorDepartment of PediatricsCase Western Reserve University School of MedicineCleveland Ohio
Manisha Patel PhDProfessorDepartment of Pharmaceutical SciencesUniversity of Colorado DenverAurora Colorado
Phillip L Pearl MDDirector of Epilepsy and Clinical NeurophysiologyWilliam G Lennox ChairBoston Childrenrsquos HospitalProfessor of NeurologyHarvard Medical SchoolBoston Massachusetts
Anna Lecticia Pinto MDAssistant in Neurology and Co-DirectorSturge Weber Clinic Boston Childrenrsquos HospitalLecturer of NeurologyHarvard Medical SchoolBoston Massachusetts
Barbara Plecko-Startinig MDHeadDivision of Child NeurologyChildrenrsquos Hospital ZurichProfessor of Child NeurologyUniversity of ZurichZurich Switzerland
Annapurna Poduri MD MPHEpilepsy Genetics ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Asuri N Prasad MBBS MD FRCPC FRCPEProfessor in Pediatrics and Clinical NeurosciencesDivision of Pediatric NeurologyDepartment of PediatricsSchulich School of Medicine and DentistryChildrenrsquos Hospital London Health Sciences CentreWestern UniversityLondon Ontario Canada
Morgan J Prust MDClinical Fellow in NeurologyDepartment of NeurologyMassachusetts General HospitalBrigham amp Womenrsquos HospitalBoston Massachusetts
Gerald V Raymond MDProfessorDepartment of NeurologyUniversity of Minnesota Medical SchoolMinneapolis Minnesota
Debra S Regier MD PhDDirector of Genetic and Genomic Education Medical
GeneticistRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Jong M Rho MDProfessor of Pediatrics Clinical Neurosciences
Physiology and PharmacologyDr Robert Haslam Chair in Child NeurologySection of Paediatric NeurologyCumming School of Medicine University of CalgaryAlberta Childrenrsquos HospitalCalgary Alberta Canada
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Lance H Rodan MDStaff PhysicianBoston Childrenrsquos HospitalBoston Massachusetts
Alexander Rotenberg MD PhDDirector Neuromodulation ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalAssociate Professor of NeurologyHarvard Medical SchoolBoston Massachusetts
Christopher Ryan LCSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Mustafa Sahin MD PhDProfessor of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Harvey B Sarnat MS MD FRCPCProfessor Departments of Paediatrics Pathology
(Neuropathology) and Clinical NeurosciencesUniversity of Calgary Cumming School of Medicine
and Alberta Childrenrsquos Hospital Research InstituteCalgary Alberta Canada
Joumlrn Oliver Sass Dr rer natProfessor of Bioanalytics and BiochemistryDepartment of Natural SciencesBonn-Rhein-Sieg University of Applied SciencesSankt Augustin Germany
Samata Singhi MDClinical Fellow in NeurologyDepartment of NeurologyBoston Childrenrsquos HospitalBoston Massachusetts
Susan E Sparks MD PhDMedical DirectorNA Medical AffairsRare DiseasesSanofi GenzymeCambridge Massachusetts
Carl E Stafstrom MD PhDProfessor of Neurology and PediatricsLederer Chair in Pediatric EpilepsyDirector Division of Pediatric NeurologyJohns Hopkins University School of MedicineBaltimore Maryland
Robert Steinfeld MD PhDProfessor of Neurometabolic and Neurodegenerative
Diseases in Childhood and AdolescenceDepartment of Pediatrics and Pediatric NeurologyUniversity Medical Center GoumlttingenGoumlttingen Germany
Marshall L Summar MDChief Division of Genetics and MetabolismMargaret OrsquoMalley Chair of Genetic MedicineRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Brahim Tabarki MDDivision of Pediatric NeurologyPrince Sultan Military Medical CityRiyadh Saudi ArabiaAssociate Professor of Neurology and PediatricsThe Ibn El Jazzar University School of MedicineSousse Tunisia
Pranoot Tanpaiboon MDAssociate Professor of PediatricsDivision of Genetics and MetabolismThe George Washington University School of Medicine
and Health SciencesChildrenrsquos National Health System Childrenrsquos National
Rare Disease InstituteWashington DC
Davide Tonduti MDChild NeurologistDepartment of Child NeurologyFondazione IRCCS Istituto Neurologico Carlo BestaMilano Italy
Johan L K Van Hove MD PhDProfessor of PediatricsSection of Clinical Genetics and Metabolism
Department of PediatricsUniversity of ColoradoAurora Colorado
Adeline Vanderver MDAttending PhysicianDivision of NeurologyProgram DirectorLeukodystrophy CenterJacob A Kamens Endowed Chair in Neurologic
Disorders and Translational NeurotherapeuticsChildrenrsquos Hospital of PhiladelphiaAssociate Professor of NeurologyPerelman School of Medicine at the University of
PennsylvaniaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xvi
Jodie M Vento MGC LCGCManagerCenter for Rare Disease TherapyManagerBrain Care InstituteManagerLaboratory Genetic Counseling ServicesChildrenrsquos Hospital of Pittsburgh of UPMCPittsburgh Pennsylvania
Brandy Verhalen PhDLab ManagerPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas Texas
Kara Vogel PhDPostdoctoral Research AssociateUniversity of WisconsinndashMadisonMadison Wisconsin
Matthew Whitehead MDRadiologistChildrenrsquos National Medical CenterWashington DC
Lynne A Wolfe MS CRNPSenior Nurse PractitionerUndiagnosed Disorders ProgramNational Human Genome Research Institute National
Institutes of HealthBethesda Maryland
Robert A Zimmerman MDProfessor of RadiologyRaymond and Ruth Perelman School of Medicine at the
University of PennsylvaniaChiefDivision of Neuroradiology and MRIThe Childrenrsquos Hospital of PhiladelphiaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Preface
This edition of Inherited Metabolic Epilepsies is a greatly expanded and updated version of the fi rst Following a rousing response to the fi rst edition far beyond any anticipated measure it was clear that a reexamination of the material taking into account many helpful sug-gestions that I received from readers far and wide was in order Despite my own misgivings that books are no longer fashionable and are largely replaced by journals and online sources that lend themselves to periodic if not continual updating there remains an appetite and clamor for books that accomplish what I had hoped to do originally and aim to achieve to a greater extent in this edition to encapsulate a burgeoning fi eld suf-fi ciently that a student practitioner or investigator can turn to the source with confi dence that the neces-sary background as well as detail will be available to reward the search for information and also move the fi eld forward
The fi rst edition of this monograph was born follow-ing the organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the annual meeting of the American Epilepsy Society in Boston in 2009 At the time of proposing the topic I was wrestling with a chasmic gap between the fascinat-ing disorders being discussed at the geneticndashmetabolic meetings and the advancing wave in epilepsy classifi ca-tion diagnosis and treatment occupying the meetings attended by members of the societies associated with neurology and epilepsy At that time a storybook series of investigations elucidated not only the surprising antiq-uitin defect in pyridoxine-dependent epilepsy but also the highly charged requirement that physicians consider a pivotal role for folinic acid and pyridoxal-5-phosphate in patients with virtually the same clinical presentation I also perceived a relative lack of awareness of disorders such as glucose transporter 1 defi ciency serine synthetic defects developmental delay epilepsy and neonatal dia-betes (DEND) and hyperinsulinismndashhyperammonemia (HIndashHA) that had very specifi c therapeutic implications with potential for dramatically improving outcome but with an even greater likelihood that they were escaping diagnosis
Overall the inherited metabolic epilepsies repre-sent a group of disorders that is rare individually but
in aggregate represents a substantial clinical burden as well as a vexing area for physicians investigators and students to master The sheer amount and complexity of information are overwhelming and require the physician to synthesize key concepts in neurology genetics and epilepsy As a pediatric epileptologist and medical edu-cator I have found this area among the most challenging and rewarding in practice and research The fi rst edition organized the disorders in a traditional approach under the roof of metabolism by dividing them into small- and large-molecule disorders In the Preface to that edition there was an explanation of various ways of organizing these disorders some more user friendly to the neurol-ogist than the small- versus large-molecule divide but this was an opportunity to present that way of thinking to the neurologist which brings this clinical specialty closer to that of genetics metabolism
In this second edition there is an expansion from four sections (General Principles Small Molecule Diseases Large Molecule Diseases and Conclusions) to six sec-tions with the addition of chapters in basic science and clinical science of the metabolic epilepsies The book has been expanded from 28 to 43 chapters with new chapters including overviews of metabolic disease and the basic science of metabolic epilepsy plus new topics such as metabolic energetics and implications of vital pathways A full chapter is devoted to the mechanistic target of rapamycin (mTOR) pathway that regulates cell replica-tion and so much of homeostasis and new pathophysi-ologic mechanisms such as protein anchoring disorders There are new chapters on neurotransmitter transmission measurement using transcranial magnetic stimulation genomic technologies and approaches to diagnosis and therapy referable to this group of disorders The clinical science section now includes a marvelous and refl ective chapter on neuropathology by Harvey B Sarnat There are new chapters devoted to specifi c disorders such as pyridoxal-5-phosphate dependency and Menkesrsquo disease There are chapters with completely new vantage points from community and family resources to an emphasis on adult patients the latter being the most commonly requested area to cover that I receive after giving talks on the subject In addition the prior chapters from the fi rst edition have been revised and updated
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xviii
Hence what began as a quest to increase awareness of treatable metabolic epilepsies fi rst became a mono-graph to give some form to this arena and has now been enlarged and updated to a second edition It is hoped that this will provide a resource to in some way lead the fi eld and carry it forward It is truly hoped that this book will educate if not enlighten physicians particularly
specialists and trainees in pediatric and adult neurology neurodevelopmental disabilities epilepsy and genetics while caring for patients with inherited metabolic epi-lepsies as well as spur further research into basic mecha-nisms and clinical trials in this group of maladies
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Acknowledgments
This book was fi rst suggested to me by Beth Barry from Demos Medical Publishers following my organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the American Epilepsy Society 2009 meeting Beth was a driving force for the creation of this second edition and she and Young Kim at Demos now aligned with Springer are gratefully acknowledged for unmatched hard work and persever-ance in seeing this through to completion
My education in child neurology and epilepsy is grounded by great mentors including Ralph D Feigin MD in pediatrics and Marvin A Fishman MD in pediat-ric neurology of Baylor College of Medicine in Houston and Gregory L Holmes MD in epilepsy and clinical neurophysiology then at Childrenrsquos Hospital Harvard Medical School in Boston I wish to take this opportunity to acknowledge these teachers of mine
My foray into metabolic disorders has been made pos-sible by the always helpful brilliant and steadfast work of Mike Gibson PhD whose collaboration in the area of gamma-amino butyric acid (GABA) disorders specifi -cally succinic-semialdehyde dehydrogenase (SSADH) defi ciency has been a constant source of intellectual
nourishment and encouragement My career during the two editions of this book has now spanned two great childrenrsquos hospitals Childrenrsquos National and Boston Childrenrsquos and the insight and support of colleagues at both institutions have been fundamental to this work Ongoing collaborations with Mike Gibson as well as William H Theodore MD chief of the Clinical Epilepsy Section at the NINDS have been critical to the ongoing investigative work on metabolic epilepsies
I thank each of the contributors to the fi rst edition of this book for revising and updating their chapters and each of the authors of the new chapters resulting in a signifi cant expansion The outstanding assistance of Alisa Marino is gratefully acknowledged given the enormous complexity of the project and the organiza-tional skills needed to accomplish this and a myriad of other tasks As a group I thank the many patients and families as well as students residents and fellows who inspire our work I thank my own family who as with all of us shoulder the largest burden of personal sacrifi ce and inspire us the most
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

Lance H Rodan MDStaff PhysicianBoston Childrenrsquos HospitalBoston Massachusetts
Alexander Rotenberg MD PhDDirector Neuromodulation ProgramDivision of Epilepsy and Clinical NeurophysiologyDepartment of NeurologyBoston Childrenrsquos HospitalAssociate Professor of NeurologyHarvard Medical SchoolBoston Massachusetts
Christopher Ryan LCSWClinical Social WorkerDivision of Epilepsy and Clinical NeurophysiologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Mustafa Sahin MD PhDProfessor of NeurologyBoston Childrenrsquos HospitalHarvard Medical SchoolBoston Massachusetts
Harvey B Sarnat MS MD FRCPCProfessor Departments of Paediatrics Pathology
(Neuropathology) and Clinical NeurosciencesUniversity of Calgary Cumming School of Medicine
and Alberta Childrenrsquos Hospital Research InstituteCalgary Alberta Canada
Joumlrn Oliver Sass Dr rer natProfessor of Bioanalytics and BiochemistryDepartment of Natural SciencesBonn-Rhein-Sieg University of Applied SciencesSankt Augustin Germany
Samata Singhi MDClinical Fellow in NeurologyDepartment of NeurologyBoston Childrenrsquos HospitalBoston Massachusetts
Susan E Sparks MD PhDMedical DirectorNA Medical AffairsRare DiseasesSanofi GenzymeCambridge Massachusetts
Carl E Stafstrom MD PhDProfessor of Neurology and PediatricsLederer Chair in Pediatric EpilepsyDirector Division of Pediatric NeurologyJohns Hopkins University School of MedicineBaltimore Maryland
Robert Steinfeld MD PhDProfessor of Neurometabolic and Neurodegenerative
Diseases in Childhood and AdolescenceDepartment of Pediatrics and Pediatric NeurologyUniversity Medical Center GoumlttingenGoumlttingen Germany
Marshall L Summar MDChief Division of Genetics and MetabolismMargaret OrsquoMalley Chair of Genetic MedicineRare Disease InstituteChildrenrsquos National Medical CenterWashington DC
Brahim Tabarki MDDivision of Pediatric NeurologyPrince Sultan Military Medical CityRiyadh Saudi ArabiaAssociate Professor of Neurology and PediatricsThe Ibn El Jazzar University School of MedicineSousse Tunisia
Pranoot Tanpaiboon MDAssociate Professor of PediatricsDivision of Genetics and MetabolismThe George Washington University School of Medicine
and Health SciencesChildrenrsquos National Health System Childrenrsquos National
Rare Disease InstituteWashington DC
Davide Tonduti MDChild NeurologistDepartment of Child NeurologyFondazione IRCCS Istituto Neurologico Carlo BestaMilano Italy
Johan L K Van Hove MD PhDProfessor of PediatricsSection of Clinical Genetics and Metabolism
Department of PediatricsUniversity of ColoradoAurora Colorado
Adeline Vanderver MDAttending PhysicianDivision of NeurologyProgram DirectorLeukodystrophy CenterJacob A Kamens Endowed Chair in Neurologic
Disorders and Translational NeurotherapeuticsChildrenrsquos Hospital of PhiladelphiaAssociate Professor of NeurologyPerelman School of Medicine at the University of
PennsylvaniaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xvi
Jodie M Vento MGC LCGCManagerCenter for Rare Disease TherapyManagerBrain Care InstituteManagerLaboratory Genetic Counseling ServicesChildrenrsquos Hospital of Pittsburgh of UPMCPittsburgh Pennsylvania
Brandy Verhalen PhDLab ManagerPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas Texas
Kara Vogel PhDPostdoctoral Research AssociateUniversity of WisconsinndashMadisonMadison Wisconsin
Matthew Whitehead MDRadiologistChildrenrsquos National Medical CenterWashington DC
Lynne A Wolfe MS CRNPSenior Nurse PractitionerUndiagnosed Disorders ProgramNational Human Genome Research Institute National
Institutes of HealthBethesda Maryland
Robert A Zimmerman MDProfessor of RadiologyRaymond and Ruth Perelman School of Medicine at the
University of PennsylvaniaChiefDivision of Neuroradiology and MRIThe Childrenrsquos Hospital of PhiladelphiaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Preface
This edition of Inherited Metabolic Epilepsies is a greatly expanded and updated version of the fi rst Following a rousing response to the fi rst edition far beyond any anticipated measure it was clear that a reexamination of the material taking into account many helpful sug-gestions that I received from readers far and wide was in order Despite my own misgivings that books are no longer fashionable and are largely replaced by journals and online sources that lend themselves to periodic if not continual updating there remains an appetite and clamor for books that accomplish what I had hoped to do originally and aim to achieve to a greater extent in this edition to encapsulate a burgeoning fi eld suf-fi ciently that a student practitioner or investigator can turn to the source with confi dence that the neces-sary background as well as detail will be available to reward the search for information and also move the fi eld forward
The fi rst edition of this monograph was born follow-ing the organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the annual meeting of the American Epilepsy Society in Boston in 2009 At the time of proposing the topic I was wrestling with a chasmic gap between the fascinat-ing disorders being discussed at the geneticndashmetabolic meetings and the advancing wave in epilepsy classifi ca-tion diagnosis and treatment occupying the meetings attended by members of the societies associated with neurology and epilepsy At that time a storybook series of investigations elucidated not only the surprising antiq-uitin defect in pyridoxine-dependent epilepsy but also the highly charged requirement that physicians consider a pivotal role for folinic acid and pyridoxal-5-phosphate in patients with virtually the same clinical presentation I also perceived a relative lack of awareness of disorders such as glucose transporter 1 defi ciency serine synthetic defects developmental delay epilepsy and neonatal dia-betes (DEND) and hyperinsulinismndashhyperammonemia (HIndashHA) that had very specifi c therapeutic implications with potential for dramatically improving outcome but with an even greater likelihood that they were escaping diagnosis
Overall the inherited metabolic epilepsies repre-sent a group of disorders that is rare individually but
in aggregate represents a substantial clinical burden as well as a vexing area for physicians investigators and students to master The sheer amount and complexity of information are overwhelming and require the physician to synthesize key concepts in neurology genetics and epilepsy As a pediatric epileptologist and medical edu-cator I have found this area among the most challenging and rewarding in practice and research The fi rst edition organized the disorders in a traditional approach under the roof of metabolism by dividing them into small- and large-molecule disorders In the Preface to that edition there was an explanation of various ways of organizing these disorders some more user friendly to the neurol-ogist than the small- versus large-molecule divide but this was an opportunity to present that way of thinking to the neurologist which brings this clinical specialty closer to that of genetics metabolism
In this second edition there is an expansion from four sections (General Principles Small Molecule Diseases Large Molecule Diseases and Conclusions) to six sec-tions with the addition of chapters in basic science and clinical science of the metabolic epilepsies The book has been expanded from 28 to 43 chapters with new chapters including overviews of metabolic disease and the basic science of metabolic epilepsy plus new topics such as metabolic energetics and implications of vital pathways A full chapter is devoted to the mechanistic target of rapamycin (mTOR) pathway that regulates cell replica-tion and so much of homeostasis and new pathophysi-ologic mechanisms such as protein anchoring disorders There are new chapters on neurotransmitter transmission measurement using transcranial magnetic stimulation genomic technologies and approaches to diagnosis and therapy referable to this group of disorders The clinical science section now includes a marvelous and refl ective chapter on neuropathology by Harvey B Sarnat There are new chapters devoted to specifi c disorders such as pyridoxal-5-phosphate dependency and Menkesrsquo disease There are chapters with completely new vantage points from community and family resources to an emphasis on adult patients the latter being the most commonly requested area to cover that I receive after giving talks on the subject In addition the prior chapters from the fi rst edition have been revised and updated
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xviii
Hence what began as a quest to increase awareness of treatable metabolic epilepsies fi rst became a mono-graph to give some form to this arena and has now been enlarged and updated to a second edition It is hoped that this will provide a resource to in some way lead the fi eld and carry it forward It is truly hoped that this book will educate if not enlighten physicians particularly
specialists and trainees in pediatric and adult neurology neurodevelopmental disabilities epilepsy and genetics while caring for patients with inherited metabolic epi-lepsies as well as spur further research into basic mecha-nisms and clinical trials in this group of maladies
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Acknowledgments
This book was fi rst suggested to me by Beth Barry from Demos Medical Publishers following my organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the American Epilepsy Society 2009 meeting Beth was a driving force for the creation of this second edition and she and Young Kim at Demos now aligned with Springer are gratefully acknowledged for unmatched hard work and persever-ance in seeing this through to completion
My education in child neurology and epilepsy is grounded by great mentors including Ralph D Feigin MD in pediatrics and Marvin A Fishman MD in pediat-ric neurology of Baylor College of Medicine in Houston and Gregory L Holmes MD in epilepsy and clinical neurophysiology then at Childrenrsquos Hospital Harvard Medical School in Boston I wish to take this opportunity to acknowledge these teachers of mine
My foray into metabolic disorders has been made pos-sible by the always helpful brilliant and steadfast work of Mike Gibson PhD whose collaboration in the area of gamma-amino butyric acid (GABA) disorders specifi -cally succinic-semialdehyde dehydrogenase (SSADH) defi ciency has been a constant source of intellectual
nourishment and encouragement My career during the two editions of this book has now spanned two great childrenrsquos hospitals Childrenrsquos National and Boston Childrenrsquos and the insight and support of colleagues at both institutions have been fundamental to this work Ongoing collaborations with Mike Gibson as well as William H Theodore MD chief of the Clinical Epilepsy Section at the NINDS have been critical to the ongoing investigative work on metabolic epilepsies
I thank each of the contributors to the fi rst edition of this book for revising and updating their chapters and each of the authors of the new chapters resulting in a signifi cant expansion The outstanding assistance of Alisa Marino is gratefully acknowledged given the enormous complexity of the project and the organiza-tional skills needed to accomplish this and a myriad of other tasks As a group I thank the many patients and families as well as students residents and fellows who inspire our work I thank my own family who as with all of us shoulder the largest burden of personal sacrifi ce and inspire us the most
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

xvi
Jodie M Vento MGC LCGCManagerCenter for Rare Disease TherapyManagerBrain Care InstituteManagerLaboratory Genetic Counseling ServicesChildrenrsquos Hospital of Pittsburgh of UPMCPittsburgh Pennsylvania
Brandy Verhalen PhDLab ManagerPediatrics NeurologyUniversity of Texas Southwestern Medical CenterDallas Texas
Kara Vogel PhDPostdoctoral Research AssociateUniversity of WisconsinndashMadisonMadison Wisconsin
Matthew Whitehead MDRadiologistChildrenrsquos National Medical CenterWashington DC
Lynne A Wolfe MS CRNPSenior Nurse PractitionerUndiagnosed Disorders ProgramNational Human Genome Research Institute National
Institutes of HealthBethesda Maryland
Robert A Zimmerman MDProfessor of RadiologyRaymond and Ruth Perelman School of Medicine at the
University of PennsylvaniaChiefDivision of Neuroradiology and MRIThe Childrenrsquos Hospital of PhiladelphiaPhiladelphia Pennsylvania
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Preface
This edition of Inherited Metabolic Epilepsies is a greatly expanded and updated version of the fi rst Following a rousing response to the fi rst edition far beyond any anticipated measure it was clear that a reexamination of the material taking into account many helpful sug-gestions that I received from readers far and wide was in order Despite my own misgivings that books are no longer fashionable and are largely replaced by journals and online sources that lend themselves to periodic if not continual updating there remains an appetite and clamor for books that accomplish what I had hoped to do originally and aim to achieve to a greater extent in this edition to encapsulate a burgeoning fi eld suf-fi ciently that a student practitioner or investigator can turn to the source with confi dence that the neces-sary background as well as detail will be available to reward the search for information and also move the fi eld forward
The fi rst edition of this monograph was born follow-ing the organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the annual meeting of the American Epilepsy Society in Boston in 2009 At the time of proposing the topic I was wrestling with a chasmic gap between the fascinat-ing disorders being discussed at the geneticndashmetabolic meetings and the advancing wave in epilepsy classifi ca-tion diagnosis and treatment occupying the meetings attended by members of the societies associated with neurology and epilepsy At that time a storybook series of investigations elucidated not only the surprising antiq-uitin defect in pyridoxine-dependent epilepsy but also the highly charged requirement that physicians consider a pivotal role for folinic acid and pyridoxal-5-phosphate in patients with virtually the same clinical presentation I also perceived a relative lack of awareness of disorders such as glucose transporter 1 defi ciency serine synthetic defects developmental delay epilepsy and neonatal dia-betes (DEND) and hyperinsulinismndashhyperammonemia (HIndashHA) that had very specifi c therapeutic implications with potential for dramatically improving outcome but with an even greater likelihood that they were escaping diagnosis
Overall the inherited metabolic epilepsies repre-sent a group of disorders that is rare individually but
in aggregate represents a substantial clinical burden as well as a vexing area for physicians investigators and students to master The sheer amount and complexity of information are overwhelming and require the physician to synthesize key concepts in neurology genetics and epilepsy As a pediatric epileptologist and medical edu-cator I have found this area among the most challenging and rewarding in practice and research The fi rst edition organized the disorders in a traditional approach under the roof of metabolism by dividing them into small- and large-molecule disorders In the Preface to that edition there was an explanation of various ways of organizing these disorders some more user friendly to the neurol-ogist than the small- versus large-molecule divide but this was an opportunity to present that way of thinking to the neurologist which brings this clinical specialty closer to that of genetics metabolism
In this second edition there is an expansion from four sections (General Principles Small Molecule Diseases Large Molecule Diseases and Conclusions) to six sec-tions with the addition of chapters in basic science and clinical science of the metabolic epilepsies The book has been expanded from 28 to 43 chapters with new chapters including overviews of metabolic disease and the basic science of metabolic epilepsy plus new topics such as metabolic energetics and implications of vital pathways A full chapter is devoted to the mechanistic target of rapamycin (mTOR) pathway that regulates cell replica-tion and so much of homeostasis and new pathophysi-ologic mechanisms such as protein anchoring disorders There are new chapters on neurotransmitter transmission measurement using transcranial magnetic stimulation genomic technologies and approaches to diagnosis and therapy referable to this group of disorders The clinical science section now includes a marvelous and refl ective chapter on neuropathology by Harvey B Sarnat There are new chapters devoted to specifi c disorders such as pyridoxal-5-phosphate dependency and Menkesrsquo disease There are chapters with completely new vantage points from community and family resources to an emphasis on adult patients the latter being the most commonly requested area to cover that I receive after giving talks on the subject In addition the prior chapters from the fi rst edition have been revised and updated
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xviii
Hence what began as a quest to increase awareness of treatable metabolic epilepsies fi rst became a mono-graph to give some form to this arena and has now been enlarged and updated to a second edition It is hoped that this will provide a resource to in some way lead the fi eld and carry it forward It is truly hoped that this book will educate if not enlighten physicians particularly
specialists and trainees in pediatric and adult neurology neurodevelopmental disabilities epilepsy and genetics while caring for patients with inherited metabolic epi-lepsies as well as spur further research into basic mecha-nisms and clinical trials in this group of maladies
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Acknowledgments
This book was fi rst suggested to me by Beth Barry from Demos Medical Publishers following my organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the American Epilepsy Society 2009 meeting Beth was a driving force for the creation of this second edition and she and Young Kim at Demos now aligned with Springer are gratefully acknowledged for unmatched hard work and persever-ance in seeing this through to completion
My education in child neurology and epilepsy is grounded by great mentors including Ralph D Feigin MD in pediatrics and Marvin A Fishman MD in pediat-ric neurology of Baylor College of Medicine in Houston and Gregory L Holmes MD in epilepsy and clinical neurophysiology then at Childrenrsquos Hospital Harvard Medical School in Boston I wish to take this opportunity to acknowledge these teachers of mine
My foray into metabolic disorders has been made pos-sible by the always helpful brilliant and steadfast work of Mike Gibson PhD whose collaboration in the area of gamma-amino butyric acid (GABA) disorders specifi -cally succinic-semialdehyde dehydrogenase (SSADH) defi ciency has been a constant source of intellectual
nourishment and encouragement My career during the two editions of this book has now spanned two great childrenrsquos hospitals Childrenrsquos National and Boston Childrenrsquos and the insight and support of colleagues at both institutions have been fundamental to this work Ongoing collaborations with Mike Gibson as well as William H Theodore MD chief of the Clinical Epilepsy Section at the NINDS have been critical to the ongoing investigative work on metabolic epilepsies
I thank each of the contributors to the fi rst edition of this book for revising and updating their chapters and each of the authors of the new chapters resulting in a signifi cant expansion The outstanding assistance of Alisa Marino is gratefully acknowledged given the enormous complexity of the project and the organiza-tional skills needed to accomplish this and a myriad of other tasks As a group I thank the many patients and families as well as students residents and fellows who inspire our work I thank my own family who as with all of us shoulder the largest burden of personal sacrifi ce and inspire us the most
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

Preface
This edition of Inherited Metabolic Epilepsies is a greatly expanded and updated version of the fi rst Following a rousing response to the fi rst edition far beyond any anticipated measure it was clear that a reexamination of the material taking into account many helpful sug-gestions that I received from readers far and wide was in order Despite my own misgivings that books are no longer fashionable and are largely replaced by journals and online sources that lend themselves to periodic if not continual updating there remains an appetite and clamor for books that accomplish what I had hoped to do originally and aim to achieve to a greater extent in this edition to encapsulate a burgeoning fi eld suf-fi ciently that a student practitioner or investigator can turn to the source with confi dence that the neces-sary background as well as detail will be available to reward the search for information and also move the fi eld forward
The fi rst edition of this monograph was born follow-ing the organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the annual meeting of the American Epilepsy Society in Boston in 2009 At the time of proposing the topic I was wrestling with a chasmic gap between the fascinat-ing disorders being discussed at the geneticndashmetabolic meetings and the advancing wave in epilepsy classifi ca-tion diagnosis and treatment occupying the meetings attended by members of the societies associated with neurology and epilepsy At that time a storybook series of investigations elucidated not only the surprising antiq-uitin defect in pyridoxine-dependent epilepsy but also the highly charged requirement that physicians consider a pivotal role for folinic acid and pyridoxal-5-phosphate in patients with virtually the same clinical presentation I also perceived a relative lack of awareness of disorders such as glucose transporter 1 defi ciency serine synthetic defects developmental delay epilepsy and neonatal dia-betes (DEND) and hyperinsulinismndashhyperammonemia (HIndashHA) that had very specifi c therapeutic implications with potential for dramatically improving outcome but with an even greater likelihood that they were escaping diagnosis
Overall the inherited metabolic epilepsies repre-sent a group of disorders that is rare individually but
in aggregate represents a substantial clinical burden as well as a vexing area for physicians investigators and students to master The sheer amount and complexity of information are overwhelming and require the physician to synthesize key concepts in neurology genetics and epilepsy As a pediatric epileptologist and medical edu-cator I have found this area among the most challenging and rewarding in practice and research The fi rst edition organized the disorders in a traditional approach under the roof of metabolism by dividing them into small- and large-molecule disorders In the Preface to that edition there was an explanation of various ways of organizing these disorders some more user friendly to the neurol-ogist than the small- versus large-molecule divide but this was an opportunity to present that way of thinking to the neurologist which brings this clinical specialty closer to that of genetics metabolism
In this second edition there is an expansion from four sections (General Principles Small Molecule Diseases Large Molecule Diseases and Conclusions) to six sec-tions with the addition of chapters in basic science and clinical science of the metabolic epilepsies The book has been expanded from 28 to 43 chapters with new chapters including overviews of metabolic disease and the basic science of metabolic epilepsy plus new topics such as metabolic energetics and implications of vital pathways A full chapter is devoted to the mechanistic target of rapamycin (mTOR) pathway that regulates cell replica-tion and so much of homeostasis and new pathophysi-ologic mechanisms such as protein anchoring disorders There are new chapters on neurotransmitter transmission measurement using transcranial magnetic stimulation genomic technologies and approaches to diagnosis and therapy referable to this group of disorders The clinical science section now includes a marvelous and refl ective chapter on neuropathology by Harvey B Sarnat There are new chapters devoted to specifi c disorders such as pyridoxal-5-phosphate dependency and Menkesrsquo disease There are chapters with completely new vantage points from community and family resources to an emphasis on adult patients the latter being the most commonly requested area to cover that I receive after giving talks on the subject In addition the prior chapters from the fi rst edition have been revised and updated
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
xviii
Hence what began as a quest to increase awareness of treatable metabolic epilepsies fi rst became a mono-graph to give some form to this arena and has now been enlarged and updated to a second edition It is hoped that this will provide a resource to in some way lead the fi eld and carry it forward It is truly hoped that this book will educate if not enlighten physicians particularly
specialists and trainees in pediatric and adult neurology neurodevelopmental disabilities epilepsy and genetics while caring for patients with inherited metabolic epi-lepsies as well as spur further research into basic mecha-nisms and clinical trials in this group of maladies
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Acknowledgments
This book was fi rst suggested to me by Beth Barry from Demos Medical Publishers following my organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the American Epilepsy Society 2009 meeting Beth was a driving force for the creation of this second edition and she and Young Kim at Demos now aligned with Springer are gratefully acknowledged for unmatched hard work and persever-ance in seeing this through to completion
My education in child neurology and epilepsy is grounded by great mentors including Ralph D Feigin MD in pediatrics and Marvin A Fishman MD in pediat-ric neurology of Baylor College of Medicine in Houston and Gregory L Holmes MD in epilepsy and clinical neurophysiology then at Childrenrsquos Hospital Harvard Medical School in Boston I wish to take this opportunity to acknowledge these teachers of mine
My foray into metabolic disorders has been made pos-sible by the always helpful brilliant and steadfast work of Mike Gibson PhD whose collaboration in the area of gamma-amino butyric acid (GABA) disorders specifi -cally succinic-semialdehyde dehydrogenase (SSADH) defi ciency has been a constant source of intellectual
nourishment and encouragement My career during the two editions of this book has now spanned two great childrenrsquos hospitals Childrenrsquos National and Boston Childrenrsquos and the insight and support of colleagues at both institutions have been fundamental to this work Ongoing collaborations with Mike Gibson as well as William H Theodore MD chief of the Clinical Epilepsy Section at the NINDS have been critical to the ongoing investigative work on metabolic epilepsies
I thank each of the contributors to the fi rst edition of this book for revising and updating their chapters and each of the authors of the new chapters resulting in a signifi cant expansion The outstanding assistance of Alisa Marino is gratefully acknowledged given the enormous complexity of the project and the organiza-tional skills needed to accomplish this and a myriad of other tasks As a group I thank the many patients and families as well as students residents and fellows who inspire our work I thank my own family who as with all of us shoulder the largest burden of personal sacrifi ce and inspire us the most
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

xviii
Hence what began as a quest to increase awareness of treatable metabolic epilepsies fi rst became a mono-graph to give some form to this arena and has now been enlarged and updated to a second edition It is hoped that this will provide a resource to in some way lead the fi eld and carry it forward It is truly hoped that this book will educate if not enlighten physicians particularly
specialists and trainees in pediatric and adult neurology neurodevelopmental disabilities epilepsy and genetics while caring for patients with inherited metabolic epi-lepsies as well as spur further research into basic mecha-nisms and clinical trials in this group of maladies
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Acknowledgments
This book was fi rst suggested to me by Beth Barry from Demos Medical Publishers following my organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the American Epilepsy Society 2009 meeting Beth was a driving force for the creation of this second edition and she and Young Kim at Demos now aligned with Springer are gratefully acknowledged for unmatched hard work and persever-ance in seeing this through to completion
My education in child neurology and epilepsy is grounded by great mentors including Ralph D Feigin MD in pediatrics and Marvin A Fishman MD in pediat-ric neurology of Baylor College of Medicine in Houston and Gregory L Holmes MD in epilepsy and clinical neurophysiology then at Childrenrsquos Hospital Harvard Medical School in Boston I wish to take this opportunity to acknowledge these teachers of mine
My foray into metabolic disorders has been made pos-sible by the always helpful brilliant and steadfast work of Mike Gibson PhD whose collaboration in the area of gamma-amino butyric acid (GABA) disorders specifi -cally succinic-semialdehyde dehydrogenase (SSADH) defi ciency has been a constant source of intellectual
nourishment and encouragement My career during the two editions of this book has now spanned two great childrenrsquos hospitals Childrenrsquos National and Boston Childrenrsquos and the insight and support of colleagues at both institutions have been fundamental to this work Ongoing collaborations with Mike Gibson as well as William H Theodore MD chief of the Clinical Epilepsy Section at the NINDS have been critical to the ongoing investigative work on metabolic epilepsies
I thank each of the contributors to the fi rst edition of this book for revising and updating their chapters and each of the authors of the new chapters resulting in a signifi cant expansion The outstanding assistance of Alisa Marino is gratefully acknowledged given the enormous complexity of the project and the organiza-tional skills needed to accomplish this and a myriad of other tasks As a group I thank the many patients and families as well as students residents and fellows who inspire our work I thank my own family who as with all of us shoulder the largest burden of personal sacrifi ce and inspire us the most
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

Acknowledgments
This book was fi rst suggested to me by Beth Barry from Demos Medical Publishers following my organization of the Pediatric State-of-the-Art Symposium on Treatable Metabolic Epilepsies presented at the American Epilepsy Society 2009 meeting Beth was a driving force for the creation of this second edition and she and Young Kim at Demos now aligned with Springer are gratefully acknowledged for unmatched hard work and persever-ance in seeing this through to completion
My education in child neurology and epilepsy is grounded by great mentors including Ralph D Feigin MD in pediatrics and Marvin A Fishman MD in pediat-ric neurology of Baylor College of Medicine in Houston and Gregory L Holmes MD in epilepsy and clinical neurophysiology then at Childrenrsquos Hospital Harvard Medical School in Boston I wish to take this opportunity to acknowledge these teachers of mine
My foray into metabolic disorders has been made pos-sible by the always helpful brilliant and steadfast work of Mike Gibson PhD whose collaboration in the area of gamma-amino butyric acid (GABA) disorders specifi -cally succinic-semialdehyde dehydrogenase (SSADH) defi ciency has been a constant source of intellectual
nourishment and encouragement My career during the two editions of this book has now spanned two great childrenrsquos hospitals Childrenrsquos National and Boston Childrenrsquos and the insight and support of colleagues at both institutions have been fundamental to this work Ongoing collaborations with Mike Gibson as well as William H Theodore MD chief of the Clinical Epilepsy Section at the NINDS have been critical to the ongoing investigative work on metabolic epilepsies
I thank each of the contributors to the fi rst edition of this book for revising and updating their chapters and each of the authors of the new chapters resulting in a signifi cant expansion The outstanding assistance of Alisa Marino is gratefully acknowledged given the enormous complexity of the project and the organiza-tional skills needed to accomplish this and a myriad of other tasks As a group I thank the many patients and families as well as students residents and fellows who inspire our work I thank my own family who as with all of us shoulder the largest burden of personal sacrifi ce and inspire us the most
Phillip L Pearl MD
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

ShareInherited Metabolic Epilepsies Second Edition
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

Glucose Transporter Type 1 Deficiency Syndrome
Cigdem I Akman and Darryl C De Vivo
23
Brain energy metabolism in the non fasting state is depen-dent primarily on a continuous supply of glucose Glucose transport across the bloodndashbrain barrier is uniquely facil-itated by the glucose transporter type 1 (GLUT1) (1) GLUT1 is highly expressed in the luminal and ablumi-nal membranes of the endothelial cells that comprise the brain microvasculature Additionally the GLUT1 trans-porter facilitates the diffusion of glucose from the brain interstitial compartment across the plasma membranes of astrocytes oligodendrocytes and other glial cells (2)
The metabolic demand of the childrsquos developing brain during the fi rst decade of life far exceeds that of the new-born infant brain and the mature brain hence a dispro-portionately large amount (80) of total body glucose utilization is consumed by the developing brain This high demand for glucose by the developing brain cor-relates with the high synaptic density in early life before pruning occurs during the sculpting and specializa-tion of brain connections and circuits It also correlates with the fact that much of brain energy metabolism is dedicated to synaptic activation balancing the relative infl uences of the excitatory and inhibitory neuronal pop-ulations and preventing epileptic activity (2)
GLUT1 defi ciency was discovered in 1991 when De Vivo and colleagues reported two infants with this con-dition (OMIM 138140) (3) Both children presented with infantile onset refractory seizures delayed neurological development acquired microcephaly and ataxia The unusual fi ndings of low cerebrospinal fl uid (CSF) glucose in the setting of a normal blood glucose coupled with a low to low-normal CSF lactate led De Vivo et al to postu-late a disturbance in the transport of glucose from blood to brain Seven years later this investigative team iden-tifi ed disease-causing mutations in the GLUT1 (SCL2A1) gene to confi rm this initial speculation (4) De Vivo and colleagues proposed to treat the children with the keto-genic diet (KD) thereby providing the only alternate fuel source for brain energy metabolism The high-fat
diet remains the standard of care for these patients and is very effective in controlling the seizure disorder Also the investigative team realized that the GLUT1 trans-porter in the erythrocytes was chemically and immuno-logically identical to the GLUT1 protein located in the brain cells They developed the radiometric RBC glucose uptake assay and demonstrated a decreased uptake in the fi rst patient It has proven to be a diagnostic gold standard for this condition correlating well with phe-notypic severity haploinsuffi ciency and the presence of disease-causing mutations in the GLUT1 gene (5) Both parents typically are used as assay controls because the majority of patients have de novo monoallelic mutations
EPIDEMIOLOGY
Confi rmed cases of GLUT1 defi ciency syndrome (DS) now span the globe having been reported in North and South America Australia China Japan and Europe Collectively these cases usually recapitulate the origi-nally described classic phenotype with infantile-onset seizures described as brief subtle myoclonic limb jerk-ing staring and eyendashhead movements pallor decreased responsiveness disturbed body tone and head bobbing (6ndash11) The eye movements have been called opsoclonus by many authors including ourselves until recently We studied these movements now termed by us as aber-rant gaze saccades and distinguished them from opso-clonus by the presence of associated head movements and intermovement visual fi xation We believe these movements are distinctive and possibly diagnostic of GLUT1 DS (12) The early presentation of GLUT1 DS is paroxysmal in the young infant who otherwise appears to be developing normally Delayed neurolog-ical development then becomes increasingly apparent later in infancy Unfortunately symptomatic treatment
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

314
GENETICS
The genetic defect causing GLUT1 DS involves the SLC2A1 gene located on chromosome 1p342 The genomic DNA spans 35 kilobases and contains 10 exons (MIM 138140) By the year 2010 there were over 100 reported pathogenic mutations including missense nonsense deletion insertion and splice site mutations (61617) All reported mutations cause loss of function Most cases result from de novo mutations accounting for the fact that the majority of patients represent single cases within families When transmitted from one gen-eration to the next it behaves as an autosomal domi-nant trait and the phenotype generally is milder often resulting from a missense mutation Rare examples of clinically asymptomatic parents with genetic mosaicism have been described Two families have been described with a pattern of autosomal recessive inheritance (1618) One of these families was consanguineous
Recent work by our group has demonstrated that the pattern of inheritance is determined by the degree of haploinsuffi ciency and the pathogenicity of the muta-tion (19) Compound heterozygotes for example may inherit a recessive mutation from a clinically unaffected parent and suffer a de novo dominant mutation in the other allele resulting in a severe phenotype (19) The erythrocyte 3-O-methyl-D-glucose uptake assay is a functional measure that correlates with phenotypic severity and is a surrogate for the degree of GLUT1 haploinsuffi ciency
GLUT1 DS model mice have recapitulated the human phenotype with acquired microcephaly seizures and disturbed motor function (20) GLUT1 mutations have been shown to account for a monogenic form of dysto-nia and paroxysmal exertion-induced dyskinesia (PED DYT18) with or without epilepsy (21) GLUT1 missense mutations associated with decreased glucose uptake in functional assays also have been identifi ed in family members who suffer from a slowly progressive spastic paraparesis combined with PED (paroxysmal choreo-athetosisspasticity DYT9) (22ndash24)
DIAGNOSTIC GENETIC TESTING
Diagnostic genetic testing for an individual presenting with epilepsy movement disorders or delayed neurolog-ical development in the setting of hypoglycorrhachia is offered on a commercial basis in the United States GLUT1 DS represents one scenario in which identifi cation of a genetic mutation in an epilepsy condition has important and direct impact on treatment choice and ultimately on prognosis With early diagnosis and institution of the KD the progressive symptoms of acquired microcephaly
with phenobarbital and other anti-seizure drugs is often pursued without a careful search for a cause and precious time elapses between clinical presentation in infancy and correct diagnosis of GLUT1 DS in child-hood Although awareness of this syndrome has gradu-ally increased in the medical community the true birth incidence and prevalence of GLUT1 DS are yet to be determined Two studies have estimated the birth inci-dence to be around 180000 to 190000 in all likelihood a conservative underestimate (1314) If accurate this incidence would suggest about 50 new cases per year in the United States and a prevalence of about 3000 to 4000 cases The worldwide prevalence then would be approximately 100000 cases or less
A study in 34 patients diagnosed with early onset absence epilepsy identifi ed SLC2A1 mutations in 12 of the patients (15) Childhood onset epilepsy accounts for approximately 2 to 8 of people with epilepsy Seizure onset is usually between ages 3 and 11 years and most often between ages 5 and 8 years Considering the prevalence of epilepsy as affecting 105 million children worldwide we suspect that GLUT1 DS is signifi cantly underdiagnosed among the children presenting with childhood onset epilepsy Part of this likely underdiag-nosis is related to the reluctance to perform appropriate diagnostic studies including a lumbar puncture when the patient fi rst presents with seizures or other paroxys-mal symptoms
There are a number of barriers to making a GLUT1 DS diagnosis proactively First is the lack of newborn screen-ing which exists for other treatable metabolic conditions of infancy such as phenylketonuria Development of a newborn screen relies on the presence of a high through-put screening test that can be developed from the routine blood spot Currently this test does not exist for GLUT1 DS The promise of molecular genetic screening is com-plicated by the number of reported disease-causing mutations in this condition and further limited by the current cost of technology
Second the main diagnostic procedure the lum-bar puncture is often delayed deferred or inaccu-rately interpreted Low CSF glucose values are often dismissed as a laboratory error or as clinically unim-portant Simultaneous measures of blood and CSF glu-cose and lactate values are an important part of the evaluation CSF lactate values are expected to be low or low-normal (lt 13 mM) In our experience timely performance of the diagnostic lumbar puncture and associated blood studies are the main impediments to early diagnosis and treatment with a KD As a result the developing brain is deprived of suffi cient nutrients to sustain growth and development Recent studies also document a developmental arrest in cerebral angio-genesis likely leading to chronic hypoperfusion of the developed brain (68)
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

small number usually with a milder clinical phenotype now having CSF glucose values in the 40s and 50s In the past signifi cance also has been placed on the ratio of CSF glucose to serum glucose with the cutoff value for GLUT1 DS set at less than 04 and with normal val-ues being greater than 06 (28) In our practice we have placed greater emphasis on the absolute CSF glucose value The ratio can be infl uenced by the glucose value in both body compartments thereby diminishing the spec-ifi city and sensitivity of this marker The measurements are even more reliable if the patient is postabsorptive with nothing to eat or drink for a period of 4 to 8 hours before the blood sample is taken followed immediately by performance of the lumbar puncture As mentioned earlier however this CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS
With the increasing recognition of milder allelic vari-ants higher CSF glucose values of 41 to 52 mgdL are now being described (729ndash32) In our experience the CSF glucose values in 150 cases of GLUT1 DS always have been less than 60 mgdL and the vast majority (greater than 90) of values have been less than 40 mgdL (unpublished observations) (232433) These obser-vations also indicate that the normal range for CSF glu-cose has never been defi ned properly A low CSF glucose concentration can also be found in other neurological conditions such as infectious meningitis hypoglycemic states subarachnoid hemorrhage and meningeal carci-nomatosis and must be ruled out clinically by assessing cell count and imaging fi ndings (34ndash38)
Although not a strict diagnostic requirement brain imaging characteristics in GLUT1 DS deserve attention owing to frequent use of neuroimaging in assessing patients with epilepsy The fi rst GLUT1 DS patient had MRI studies showing mild delay in myelination at age 75 months and subsequent cases have demonstrated normal or minor nonspecifi c abnormalities with slight brain hypotrophy at various ages in childhood (31739) One group has reported a case in which brain hyp-otrophy noted at age 5 years before KD initiation was replaced by normal brain growth at 7 years on the KD a fi nding that underscores the importance of appropriate early diagnosis and treatment (39) Signifi cant specifi c fi ndings on F-fl uoro-deoxyglucose positron emission tomography (FDG-PET) have been reported and include a diffused decrease in cortical uptake of glucose and a striking regional hypometabolism in the cerebellum thalamus frontal parietal and temporal neocortex and relative sparing of the basal ganglia and occipital cortex (4041) (Figure 231) These abnormalities were present in infancy and persistent through adulthood and are not rectifi ed by ketosis In retrospect these immutable fi nd-ings correlate with the developmental arrest of cerebral angiogenesis that has been documented recently in the GLUT1 model mice (68)
brain hypotrophy refractory epilepsy ataxia and devel-opmental regression may be mitigated (2325)
Approximately one third of patients with a clinical phenotype consistent with GLUT1 DS and a confi rmatory CSF biomarker profi le will have negative genetic testing for a GLUT1 disease-causing mutation In general these patients also will have a normal RBC glucose uptake assay suggesting that some other molecular mechanism is responsible Some of these patients also will respond to the KD because this treatment is effective for epilepsy regardless of genetic etiology The key take-home mes-sage is that the CSF biomarker profi le is necessary but not suffi cient for the diagnosis of GLUT1 DS The yield of confi rmatory testing will likely increase as newer molecular genetic diagnostics are developed (26) There is as mentioned earlier no currently available newborn screening method for GLUT1 DS For the moment the diagnostic acumen of the physician at the time of the fi rst clinical event in infancy remains critical and is essential to prognosis With increased surveillance earlier testing and improved treatment outcomes genetic counseling provides an important intervention for affected individu-als as they mature to reproductive ages (27)
CLINICAL DIAGNOSIS
The diagnosis of GLUT1 DS currently depends on clin-ical acumen Confi rmatory genetic testing is available commercially and on a research basis The clinical hall-marks are early onset epilepsy that is refractory to stan-dard anti-seizure medications Diagnosis is facilitated by assessment of cerebrospinal fl uid classically showing hypoglycorrhachia (lt40 mgdL) and low-normal or low CSF lactate values (lt13 mM) in the setting of normo-glycemia (~70ndash110 mgdL) The KD should be started immediately after documenting these clinical and labo-ratory fi ndings and further confi rmatory studies should follow as discussed previously Left untreated patients will develop acquired microcephaly motor and cogni-tive impairments ataxia spasticity dystonia and other paroxysmal disorders GLUT1 DS may cause a myriad of clinical conditions seen in child neurology including epilepsy intellectual disability and learning problems movement disorders behavioral problems such as atten-tion-defi cit hyperactivity disorder and paroxysmal dys-phoria alternating hemiplegia of childhood and familial hemiplegic migraine The presentations may be both par-oxysmal (particularly early) and permanent (later in the course)
The initial cutoff value for diagnosing hypoglycorrha-chia was a CSF glucose concentration of 40 mgdL (22 mM) for suspected GLUT1 defi ciency cases More than 90 of patients still fulfi ll this original criterion with a
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

316
MANAGEMENT
Management of patients with GLUT1 DS should focus on two clinical goals (a) treatment of the cardinal clinical symptoms with a KD in an effort to meet the metabolic energy demands of the growing brain and (b) provi-sion of rehabilitation and nutritional support services to address the needs of children and adults with chronic developmental disabilities
The gold standard for treatment of GLUT1 DS is the KD which provides the only alternative fuel for brain metabolism The response to the KD is rapid and dra-matic and this salutary response permits the weaning of the previously instituted anti-seizure medicines In general the risks of the medicines clearly outweigh any possible benefi ts In our experience better neuro-logical growth and development follow the control of the epilepsy Best results are obtained by maintaining the highest blood beta-hydroxybutyrate (BHB) levels possible We recommend values around 5 mM rather than the standard 2 to 3 mM (28) It is clear that good seizure control can be achieved with the KD at lower blood BHB levels But seizure control is not the primary goal Rather it is nourishment of the ldquostarving brainrdquo that is the primary goal We speculate that brain lactate
values are abnormally low in the untreated patient and we know that brain lactate levels can be elevated in the animal model for the KD Neurons preferentially utilize astrocyte-derived lactate
For this reason we recommend blood BHB measure-ments by fi ngerstick not urine dips (falsely reassuring) Ideally the KD should be maintained at least through adolescence to provide adequate fuel support for the developing brain This recommendation is designed to mitigate structural and functional damage until the brain is mature It also is likely that the mature brain will func-tion better with ketones available for fuel needs This speculation is counterbalanced by issues of lifestyle and compliance
In theory certain medicines may be associated with clinical worsening in GLUT1 DS Common anti-seizure medicines known to inhibit the GLUT1 transporter in vitro specifi cally phenobarbital valproate and benzo-diazepines are relatively contraindicated in GLUT1 DS (4243) Valproate contributes to hypocarnitinemia and also inhibits fatty acid oxidation For these reasons val-proate should not be combined with the KD The KD car-ries with it a risk for kidney stones Drugs that inhibit the enzyme carbonic anhydrase such as acetazolamide topi-ramate and lamotrigine carry a similar risk Combining these antiepileptic drugs (AEDs) with the KD will poten-tiate this risk and generally is ill advised
Finally as hypocarnitinemia develops in patients treated with the KD oral L-carnitine supplementation at a dose of 50 to 100 mgkgd in divided doses up to a maximum of 2 gd should be considered for all GLUT1 DS patients on the KD
Patients with GLUT1 DS require frequent monitor-ing for neurodevelopmental progress and the treatment of epilepsy and movement disorders At our institu-tion we have developed a semiquantitative tool the Columbia Neurological Score to assess 12 domains of neurological function to defi ne a patientrsquos clinical tra-jectory This yields a ldquocentral nervous system (CNS) scorerdquo based on the 12 domains (a) height weight and head circumference (b) general medical exam (c) fun-duscopic exam (d) cranial nerves (e) stance and gait (f) involuntary movements (g) sensation (h) cerebel-lar function (i) muscle bulk tone and strength (j) ten-don refl exes (k) Babinski sign and (l) other fi ndings The CNS score ranges from 0 to 76 (normal) scores of 40 to 49 indicate severe impairment 50 to 59 moder-ate impairment 60 to 69 mild impairment and 70 to 76 minimal impairment and overlapping with normal scores This tool provides a high interrater reliability and has been demonstrated to correlate with other mea-sures of disease severity (44)
Management of GLUT1 DS patients is multifac-eted and often involves a multidisciplinary team approach with neurologists who are conversant with
Figure 231 FDG-PET signature of GLUT1 DS displaying diffuse and regional vulnerabilities decreased glucose uptake in cerebellum thalamus and neocortex with relative sparing of the occipital cortex and basal ganglia
GLUT1 DS glucose transporter type 1 defi ciency syndrome FDG-PET F-fl uoro-deoxyglucose positron emission tomography
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

the management of epilepsy movement disorders and intellectual disability nutritionists familiar with the KD geneticists and genetic counselors and therapists knowledgeable in rehabilitative services The applica-tion of video EEG to determine the nature of the parox-ysmal events and the choice of treatments is essential for optimal long-term management Monitoring of blood and urine parameters while on the KD and anti-seizure drugs if continued after starting the KD is essential to avoid unintended side effects Skillful man-agement of the patient while on the KD can mitigate compliance issues and dietary indiscretions and facil-itate long-term use of the diet as an essential manage-ment strategy for patients with this chronic metabolic encephalopathy
In recent years the modifi ed Atkins diet (MAD) has been introduced as an alternative treatment option to overcome compliance concerns in epilepsy prac-tice MAD is more palatable for patients and practical for caregivers conversely it provides lesser degrees of ketosis compared to the KD A clinical report describing six Japanese patients treated with MAD documented improvement in clinical seizures alertness and back-ground EEG activity and disappearance of epileptic activity (10) However the primary goal in the treatment of the GLUT1 DS patient is nourishment of the ldquostarving brainrdquo not just seizure control
Ketosis provides indispensable fuel for brain energy metabolism therefore the milder ketosis provided by MAD poses a special risk for the growing brain of the child with GLUT1 DS The classical KD should remain the goal standard of treatment for infants and young children to meet the high energy demands of the grow-ing brain MAD can be considered as a management strategy for the teenager or adult GLUT1 DS patients if the classical KD proves to be intolerable
Triheptanoin is an emerging investigational drug cur-rently under study for GLUT1 DS Triheptanoin other-wise known as C7 oil is an odd-chain triglyceride with anapleurotic properties that is the metabolites of this 7-carbon triglyceride can yield acetyl CoA (2 carbons) and propionyl CoA (5 carbons) that will replenish the acetyl CoA and the oxaloacetate pools of the Krebs cycle and optimize the production of citric acid GLUT1 defi -ciency is expected to slow the glycolytic fl ux and the production of pyruvate resulting in decreased lactate oxaloacetate and acetyl CoA
An open-labeled study demonstrated that trihep-tanoin improved EEG fi ndings cerebral metabolic rate and neuropsychological status in 11 patients (45) Another study examined the effectiveness of trihep-tanoin on nonepileptic paroxysmal motor events in eight patients with GLUT1 DS Paroxysmal events sig-nifi cantly improved with triheptanoin treatment and recurred when triheptanoin was withdrawn (4647)
Longitudinal follow-up with a geneticist is important to guide families through diagnosis and family plan-ning and to assist with future reproductive decisions (27) Involvement of physical speech and occupational therapists should be ordered as needed to treat neurode-velopmental delays Long-term quality of life is largely determined by early diagnosis and prompt treatment with a classical KD
MOVEMENT DISORDERS
Two decades since the seminal paper by De Vivo et al the phenotypic spectrum of GLUT1 defi ciency has expanded although the salient clinical features remain the same as originally described (3) All manner of episodic movement disorders have been described in GLUT1 DS including dysarthria ataxia eyendashhead movements choreoathetosis myoclonus spasticity dystonia and weakness indepen-dent of seizure activity (1248) Characteristic exacerbation of these symptoms with fatigue dietary noncompliance with KD and excitement has been noted By 2008 a lit-erature review of 100 published cases revealed 3 cases of ataxia without epilepsy (33) Alternating hemiplegia of childhood (AHC) which is often genetically associated in a small number of cases with mutations in ATP1A2 and CACNA1A is now also a recognized phenotypic pre-sentation of GLUT1 defi ciency (48) As in many cases of AHC these children experience hemiplegic tonic and dystonic episodes starting before 18 months with subse-quent progressive ataxia and cognitive impairment (48) Paroxysmal exertion-induced dyskinesia or DYT18 is yet another new phenotype associated with mutations in SLC2A1 (49) A recent clinical report described the clinical course of 13 individuals recently diagnosed with GLUT1 DS over four generations in a Norwegian family (50) Exercise-induced dyskinesia early-onset epilepsy and mild learning disability were the pertinent clinical symp-toms which improved over time without any treatment Moreover once the GLUT1 DS diagnosis was established the application of dietary treatment even in adulthood improved patient quality of life
EPILEPSY
The most common symptoms across all presentations of GLUT1 DS are seizures affecting approximately 90 of our patient population The seizures often present early in infancy and are refractory to standard anti- seizure medications Accordingly one aim of this chapter is to review the current understanding of the epilepsy com-ponent of this condition highlighting the semiology
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

318
neurophysiology and treatment response aspects of epi-lepsy in GLUT1 DS
The long-recognized wide variation in seizure semiol-ogy seen in GLUT1 DS has led to its designation as ldquothe great mimickerrdquo As with many genetic entities variable penetrance and variable expressivity represent chal-lenges to the diagnostician
The initial two cases described by De Vivo et al epit-omize the key clinical and electrographic characteristics now well described in the GLUT1 DS literature (37) Both patients manifested as early onset or refractory epilepsy at age 2 months characterized by loss of responsiveness and focal myoclonic or horizontal roving eye movements that correlated with seizure activity on the EEG The initial EEG tracings revealed a right frontal focus in one case and progressed from normal to generalized spike and wave in the second Failed medication trials included the typ-ical agents used in infancy including phenobarbital and benzodiazepines and later valproate and carbamazepine Both patients experienced complete resolution on the KD within 4 and 7 days of ketosis followed by weaning of standard medicines As is often the case with newly dis-covered conditions the index cases represent the severe end of the spectrum prior to identifi cation of a gold standard preventive treatment Both children ultimately showed neurological delays despite seizure freedom
Literature review of the subsequent two decades pro-vides 109 cases of GLUT1 DS patients with documented epilepsy and associated clinical features Although the two original index cases presented in early infancy the average age of seizure onset as described in 102 cases was 12 months likely refl ecting identifi cation of milder cases over time (689252951ndash55)
Possible nonepileptic paroxysmal events include peri-odic confusion ataxia weakness headache and sleep changes which may require characterization with EEG (7) Later in childhood mixed seizure types prevail
Our earlier report in 2003 with a special focus on epi-lepsy describes the spectrum of clinical seizures and EEG fi ndings in GLUT1 DS Of the 20 children with confi rmed GLUT1 DS generalized tonic or clonic seizures prevailed (14 of 20) followed by absence (10) focal (9) myoclonic (6) and astatic (4) (25)
In another series of 15 patients followed respectively for 2 to 5 years Klepper et al described absence (7 of 15) myoclonic (7 of 15) generalized tonicndashclonic (GTC) (4 of 15) and tonic (2 of 15) seizures in addition to seizures associated with episodic irregular eye movements (9 of 15) and cyanosis (3 of 15) at the time of the GLUT1 DS diagnosis (51)
A larger cohort of GLUT1 DS from our center also con-fi rms the broad range of seizure semiology The average age of seizure onset was 8 months while the average age at diagnosis was 5 years in the classic phenotype This fi nding highlights the clinical reality that a long delay
still exists between the clinical onset and the diagnosis of GLUT1 DS (24) Absence myoclonic and GTC seizures are the most common seizure types (24) However axial tonic seizures and infantile spasms also are reported but rarely The majority of patients may present with a combination of various seizure types (2425) Myoclonic-absence seizures are also described (56) In contrast convulsive status epilepticus or progressive epileptic encephalopathy have not been reported in GLUT1 DS (24) Focal seizures occur in young age groups partic-ularly in infants while generalized seizures can be seen in any age group Fasting and exertion often trigger sei-zures dystonia and mental status changes
Familial studies of GLUT1 DS have expanded the epi-lepsy spectrum broadly with variable ages of onset and seizure types (52) In two families seizure onset extended in age from early childhood to adulthood and typical absence seizures were the most prevalent seizure type (83) Focal seizures were also reported within the same family Moreover familial GLUT1 DS was associated with a milder clinical course with a variable age of sei-zure onset (8 months to 5 years) and with a more favor-able response to drug treatment Despite infantile-onset seizures seizures abated later in life and freedom from seizures was the general rule in the adult age groups
The potential for misclassifi cation of symptomatic generalized seizures resulting from neuroglycopenia is hardly a new concept In 2003 Leary et al noted that the most common EEG abnormality in their childhood patients was the 25 to 4 Hz generalized spike-wave the hallmark of idiopathic generalized epilepsies (IGE) (25) Shortly after Oguni et al recognized that the infan-tile phenomenon of myoclonic seizures could easily be misinterpreted as benign myoclonic epilepsy in infancy prior to the development of other symptoms (11) An illustrative case was indeed reported by Roulez-Perez in 2008 when a child with occasional myoclonic seizures in infancy and short absences was given a diagnosis of IGE (54) She was treated with valproate ethosuximide and clobazam with only minimal improvement The correct diagnosis was established at age 10 years after identifi -cation of periodic confusion before meals atypical fea-tures on EEG and learning diffi culties She did well on the KD but continues to show mild neurological delays
Newer work has focused on early absence epilepsy in GLUT1 DS yet another syndrome easily misdiag-nosed as IGE Suls et al studied 34 patients with early onset absence epilepsy before 4 years and found 4 of 34 cases with SLC2A1 mutations by direct sequencing (nearly 12) (15) These cases showed inconsistent AED treatment responses ranging from easily controlled to refractory and had normal development prior to seizure onset The authors concluded that seizure phenotype of mutation-positive cases could not be distinguished from mutation-negative early-onset cases or from classic
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

childhood absence epilepsy (CAE) except for the earlier age of onset
Variability of phenotype and particularly variabil-ity of seizure expression within a family may also be seen in GLUT1 DS as evidenced by subsequent work by the same group (52) From the probands with early onset absence Mullen et al identifi ed two families with SLC2A1 mutations and identifi ed 15 patients with muta-tions Of these 12 of 15 were found to have epilepsy with variable seizure types 10 of 12 had absence seizures with onset between 3 and 34 years and 3 of 12 patients had nonconvulsive status epilepticus One sibling pair was reported to have myoclonic astatic epilepsy (MAE) with absence GTC seizures and atonic seizures at age 4 years and intellectual delay Temporal lobe epilepsy and focal dyscognitive seizures with multifocal epileptiform dis-charges on EEG were reported in two patients one diag-nosed with temporal lobe epilepsy (seizure onset at age 15 years) and the other with multifocal epilepsy (seizure onset at age 3 years) Both patients also developed parox-ysmal dyskinesia during the late teens Finally isolated febrile seizures were found in one mutation carrier with-out further development of symptoms or delay Of note seven family members were identifi ed with subtle PED and two mutation carriers were unaffected (52)
Following the discovery of GLUT1 DS in absence epilepsy syndromes two reports examined the preva-lence of GLUT1 DS in 504 patients diagnosed with IGE (5758) SLC2A1 mutations were present in 14 (7 of 504) of patients with IGE three showed the autosomal dominant pattern of inheritance (58) CAE was reported in two juvenile absence epilepsy in three and juvenile myoclonic epilepsy (JME) and generalized epilepsy with GTC seizures in one patient each Furthermore CAE transitioned to JME in one patient
In a familial cohort of IGE (n = 95) an SCL2A1 muta-tion was detected in nine (94) patients All nine patients received the diagnosis of absence epilepsy with variable age of onset ranging from early infancy to adulthood Again one patient initially diagnosed with CAE later developed JME With the exception of one case outcome was excellent and all became seizure free (57)
Myoclonic epilepsy syndromes have been described in several small GLUT1 DS series MAE was reported in familial GLUT1 DS Of 15 patients identifi ed with SLC2A1 mutations in two families two siblings received the diagnosis of MAE Both siblings had mild intellectual disability without any other cardinal signs of GLUT1 DS (1552) A follow-up report specifi cally focused on the frequency of GLUT1 defi ciency in 84 unrelated patients diagnosed with the MAE syndrome (59) The authors found only four patients (5) with a missense mutation in SLC2A1 gene All four patients had mild disability and two later developed paroxysmal dyskinesia Outcome was excellent with ultimate seizure freedom in all four
patients In contrast a newer study failed to replicate the same results Among 150 patients diagnosed with MAE none of the patients harbored an SLC2A1 mutation whereas 10 of CAE (5 of 50) did have a disease-causing mutation in the SLC2A1 gene (14)
Neither LennoxndashGastaut syndrome nor early infantile epileptic encephalopathy syndromes such as Ohtahara syndrome and early myoclonic epilepsy have been reported in association with GLUT1 DS (24)
These clinical reports underline the diagnostic chal-lenges associated with GLUT1 DS in patients presenting with well-recognized generalized epilepsy syndromes The coexistence of GLUT1 DS and childhood epilepsy syndromes suggests causation rather than coincidence GLUT1 DS should be suspected in the presence of dysto-nia dyskinesia or intellectual disability associated with clinical seizures and peculiar EEG fi ndings that are con-sistent with the diagnosis of ldquochildhood onset epilepsy syndromesrdquo
NEUROPHYSIOLOGY
Neurophysiologic features of GLUT1 DS were fi rst stud-ied systemically by Boles et al in 1999 who performed repeated studies on two children prior to and during KD treatment (60) Not surprisingly they found both normal recordings and generalized 2 to 25 Hz paroxysmal spike-wave discharges in both patients One patient had more frequent interictal discharges and absence seizures while not in ketosis suggesting improvement with delivery of ketones across the bloodndashbrain barrier In 2002 Von Moers et al elucidated the relationship between epi-leptiform activity and feeding by increasing the blood glucose concentrations one might facilitate passage of glucose via the defi cient GLUT1 transporter (61) Two children later confi rmed to have GLUT1 mutations were studied with EEG prior to breakfast and 1 and 2 hours thereafter The epileptiform activity at each inter-val was quantifi ed as 48 0 and 0 (patient 1) and 28 13 and 10 (patient 2) at these time points Based on the dra-matic decrease or abolition of epileptiform activity after a normal meal the authors suggested using preprandial and postprandial EEG recordings as a simple screening test for GLUT1 DS Seizures were reported as myoclonic jerks of the shoulders and arms or nodding of the head and corresponded with some of the generalized parox-ysms of spike-waves Subsequently both children were placed on the KD with signifi cant reduction in seizures and improvement in development
Subsequent larger case series have recapitulated the fi ndings of generalized spike-wave on EEG but also demonstrated frequent focal and multifocal ictal and interictal fi ndings Leary et al in their case series of
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

320
20 patients described previously reviewed 24 continu-ous 24-hour EEG recordings and found a mixed picture of background abnormalities generalized 25 to 4 Hz spike-waves (41) generalized slowing or attenuation (34) no abnormalities (34) focal spike-waves (13) and focal slowing or attenuation (9) (25) The authors noted a trend toward increased focal versus generalized abnormalities in those under 2 years of age attributed to immaturity of myelination but this did not reach statis-tical signifi cance (p lt 1) The differences in EEG abnor-malities prior to and after KD were also not statistically signifi cant (p gt 10)
A recent study from our group evaluated moment-to-moment neurophysiological and neuropsychological function in response to hyperglycemia in GLUT1 DS which leads to substrate saturation of the GLUT1 trans-porter (62) Six children were recorded continuously on video EEG starting 2 hours before and continuing for 6 hours after oral glucose loading The tracings revealed continuous background slowing generalized spike-wave discharges and focal frontal and central spike discharges in the preloading state In the fi rst 10 to 180 minutes after oral glucose loading there were marked improvements in background activity with normalization with com-plete disappearance of spike-wave activity and seizures Improvement was also observed in certain neuropsy-chological tasks (coordination and attention) All clinical and EEG abnormalities gradually returned to baseline after 180 minutes These fi ndings underscore the critical minute-to-minute dependence of specifi c neurological functions on glucose transport across the bloodndashbrain barrier GLUT1 transport clearly is a rate-limiting event in this context
Seizure activation with hyperventilation and photic stimulation has also been reported in two cases prior to initiation of KD These children experienced seizures presenting with upward eye deviation behavioral arrest and head drop correlating with less than 3 seconds of generalized spike-wave on EEG (Figure 232) (54) This phenomenon has not yet been replicated on a larger scale
The tendency toward multiple seizure types in indi-viduals with GLUT1 DS is mirrored by the frequent occurrence of mixed EEG fi ndings EEG recordings may range from normal to abnormal with generalized focal or multifocal spike-wave discharges and slowing or attenuation of the background (25) Abnormalities may depend on the neurodevelopmental stage perhaps with increased focal or multifocal fi ndings in infants due to incomplete myelination and have been shown to vary in response to feeding status ketosis or the overall met-abolic state Ultimately GLUT1 DS is a unique genetic condition where the EEG and seizure phenotype is not limited to generalized seizure types or correlative EEG features and importantly variation of clinical and
electrographic expression may be seen in individuals and across affected family members (52)
OUTCOME
The glucose transport defect fortunately does not affect fetal development The intrauterine environment is not metabolically demanding and most metabolic diseases emerge clinically after birth Apgar scores generally are normal at birth The fi rst clinical signs of GLUT1 DS emerge postnatally In fact there is only one longitudinal study in the literature describing the clinical course of 13 patients diagnosed with GLUT1 DS (63) Earliest symp-toms are paroxysmal in an infant who otherwise appears to be developing normally and dominated by seizures and eye movement abnormalities events Other early changes involve muscle strength and tone and breath-ing abnormalities that often overlap with seizures (23) Despite the fact that seizures herald the onset of the con-dition the seizure prognosis is not dismal The seizure frequency declines gradually through late infancy and early childhood and often abates by adolescence or early adulthood Despite normal birthweight and head cir-cumference there is deceleration of head growth in early infancy Ataxia and neurodevelopmental delay become more evident during infancy and early childhood The infantile epileptic phenotype is gradually replaced by a childhood dyskinetic phenotype dominated by dystonia Unfortunately outcome measures and intellectual ability do not improve over time The metabolic encephalopa-thy remains constant and is punctuated by paroxysmal dyskinesias
This longitudinal study of the clinical course suggests that the critical therapeutic window of opportunity is the presymptomatic moment in early infancy or soon after the fi rst clinical event when the infant appears other-wise to be developing normally (Figure 233) In order to diagnose the presymptomatic infant at risk for GLUT1 DS newborn screening will be necessary However diagnosis of the infant immediately after the fi rst clinical event will be an important step in the right direction
FUTURE DIRECTIONS
Our knowledge about the clinical and molecular aspects of GLUT1 DS have evolved rapidly over the past 2 decades since the discovery of this condition in humans Nonetheless many important areas for future research and clinical advances remain largely untapped
The ultimate goal in GLUT1 DS as with all metabolic diseases is to make an early correct diagnosis and to
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

apply this knowledge to institute the best available treat-ment in the hopes of preventing neurodevelopmental defi cits Development of a newborn screen for GLUT1 DS will be an important next step to facilitate this goal Newborn screening will need to evolve into a molecu-lar screen to capture these patients The search for other biomarkers for the condition is moving at a rapid pace including the work by De Vivo et al to develop the eryth-rocyte glucose uptake assay as a gold standard for diag-nosis This functional assay complements the molecular
interrogation of the SLC2A1 gene and helps to assess the relative pathogenicity of the gene variant Further work in this area also will enable the medical community to better understand the disease mechanisms underlying the SLC2A1 gene mutation-negative cases that have a consistent GLUT1 DS phenotype and CSF biomarkers
In the treatment arena we anticipate the develop-ment of further agents to provide fuel for brain metabo-lism An anapleurotic 7-carbon fatty acid 3-heptanone originally developed as a treatment for disorders of
Neonatal
20
0
40
60
80
100
Infancy
Per
cent
of P
atie
nts
Exp
erie
ncin
g S
ympt
om
EarlyChildhood
LateChildhood
Adolescence
SeizureFrequency ge1Week
Microcephaly
Dystonla
Ataxia
Developmental Delay
EarlyAdulthood
Figure 233 Longitudinal clinical course of GLUT1 DS throughout the life cycle prevalence of symptoms during sequential developmental epochs Each patient was treated at some point with the KD thereby possibly altering the natural history of the condition
GLUT1 DS glucose transporter type 1 defi ciency syndrome KD ketogenic diet
Figure 232 EEG fi ndings of absence seizures in a child diagnosed with GLUT1 DS EEG fi ndings are similar to the EEG fi ndings seen in childhood onset absence epilepsy 3Hz spike and slow wave discharges with abrupt onset and offset LFF 1Hz HFF 70Hz sensitivity 7uvmm
GLUT1 DS glucose transporter type 1 defi ciency syndrome
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

322
long-chain fatty acid oxidation is one such agent (64) Clinical trials are presently being conducted to explore the possible benefi t of triheptanoin as a treatment for GLUT1 DS
Thioctic acid (alpha lipoic acid) remains under inves-tigation as an antioxidant agent that facilitates the trans-location of the GLUT1 protein from intracellular pools into the plasma membrane (65) The therapeutic role of other agents transported across the bloodndashbrain barrier by GLUT1 such as vitamin C remains to be determined (6667) Supplemental agents such as acetylcholinester-ase inhibitors have been used anecdotally in an effort to improve cognitive defi cits in GLUT1 DS patients Some patients appeared to benefi t but an appropriate clinical trial will be necessary to evaluate effi cacy Breastfeeding may also be benefi cial or neuroprotective as breast milk is relatively high in fat content Relevant to this point is our observation that the GLUT1 DS model mice do not become symptomatic until after weaning Rodent milk is even higher in fat content A reduction in GLUT1 trans-porter expression by 25 is associated with the emer-gence of brain dysfunction This observation suggests that therapies designed to upregulate GLUT1 expression might be effective in correcting the haploinsuffi ciency
Last but not least a recent study of GLUT1 DS model mice demonstrated that low GLUT1 protein is associated with a developmental arrest of cerebral angiogenesis This arrest results in a profound diminu-tion of the brain microvasculature without compromis-ing the integrity of the bloodndashbrain barrier Repletion of GLUT1 protein using an AAV9 viral vector strategy during early development averts brain microvascula-ture defects and prevents disease (68) Repletion later in life fails to rescue the phenotype indicating a fi xed therapeutic window of opportunity during devel-opment Timely repletion of GLUT1 protein by gene transfer strategies promises in the future to mitigate the symptoms of GLUT1 DS
SUMMARY
GLUT1 DS is a unique treatable metabolic encepha-lopathy associated with various clinical presentations The current standard of care is treatment with a KD which provides the only alternative metabolic fuel for the human brain Most commonly the disorder pres-ents after normal pregnancy and early infancy with refractory epilepsy Seizure types may include focal or multifocal clonic or myoclonic seizures with staring loss of responsiveness head nodding and irregular epi-sodic horizontal eyendashhead movements These eyendashhead movements are distinctive and possibly diagnostic for GLUT1 DS and differ from opsoclonus Untreated
CLINICAL PEARLS
bull GLUT1 DS is a metabolic encephalopathy with broad phenotypic variability over the life cycle Typically it presents as an epileptic phenotype in infancy a dyskinetic phenotype in later childhood and lifelong clumsiness and intellectual disability
patients experience delays in the motor and cognitive domains with acquired microcephaly and spasticity dystonia and ataxia In childhood absence myoclonic tonic or clonic seizures prevail and patients may expe-rience nonconvulsive status epilepticus Variability in phenotype may be explained by GLUT1 haploinsuffi -ciency as measured by the erythrocyte glucose uptake assay MRI fi ndings may be normal initially but show brain hypotrophy over time Neurophysiological stud-ies may also be normal but more often show gener-alized focal or multifocal slowing and epileptiform discharges which may vary over time and improve with glucose loading or treatment with KD FDG-PET shows lifelong decreased cortical metabolic activity in contrast to an apparent relative increase in caudate and lentiform nuclear metabolic activity In the 2 decades since the identifi cation of GLUT1 DS in humans allelic variants with more prominent motor manifestations have been discovered including many cases with-out epilepsy KD remains the standard of care for the nonepileptic forms of GLUT1 DS These individuals may manifest dysarthria ataxia distinctive eyendashhead movements choreoathetosis myoclonus spasticity and weakness These symptoms may be infl uenced by environmental stressors such as fasting fever infection and emotional stress Alternating hemiplegia of child-hood hemiplegic migraine and paroxysmal exertional dyskinesia also have been associated with mutations in the SLC2A1 gene With increasing awareness of this treatable metabolic encephalopathy we anticipate fur-ther discoveries of yet milder phenotypes facilitated by the development of newer genetic testing platforms and novel therapies The primary treatment goal for GLUT1 DS is the nourishment of the immature ldquostarv-ing brainrdquo to allow for the normal sculpting of the devel-oping brain Neuroglycopenia left untreated results in a developmental arrest in cerebral angiogenesis and a permanent limitation of brain function Early diagnosis of the condition and prompt treatment will minimize this prognostic expectation
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

REFERENCES
1 Mueckler M Caruso C Baldwin SA et al Sequence and structure of a human glucose transporter Science 1985229(4717)941ndash945
2 De Vivo DC Wang D Pascual JM et al Glucose transporter protein syndromes Int Rev Neurobiol 200251259ndash288
3 De Vivo DC Trifi letti RR Jacobson RI et al Defective glu-cose transport across the blood brain barrier as a cause of persistent hypoglycorrhachia seizures and developmental delay N Engl J Med 1991325(10)703ndash709
4 Seidner G Alvarez MG Yeh JI et al GLUT-1 defi ciency syn-drome caused by haploinsuffi ciency of the blood-brain bar-rier hexose carrier Nat Genet 199818(2)188ndash191
5 Yang H Wang D Engelstad K et al Glut1 defi ciency syn-drome and erythrocyte glucose uptake assay Ann Neurol 201170(6)996ndash1005
6 Ito Y Gertsen E Oguni H et al Clinical presentation EEG studies and novel mutations in two cases of GLUT1 defi ciency syndrome in Japan Brain Dev 200527(4)311ndash317
7 Brockmann K The expanding phenotype of GLUT1-defi ciency syndrome Brain Dev 200931(7)545ndash552
CLINICAL PEARLS (continued )
bull The clinical condition results from defi cient transport of glucose across the bloodndashbrain barrier causing neuroglycopenia and hypoglycorrhachia
bull Most patients have loss of function mutations in the SLC2A1 gene located on chromosome 1p342 Inheritance pattern is mainly autosomal dominant and rarely autosomal recessive Most patients have de novo mutations Somatic mosaicism and compound heterozygotes have also been described
bull GLUT1 haploinsuffi ciency parallels disease severity and is refl ected in the functional radiometric RBC glucose uptake assay The RBC and the bloodndashbrain barrier GLUT1 proteins are chemically and immunologically identical
bull The classical phenotype begins in infancy with epilepsy distinctive eyendashhead movements acquired microcephaly motor and cognitive delays hypotonia and hyperrefl exia
bull Other phenotypes including children with milder delays and mixed seizure disorders often with early onset absence epilepsy also have been described
bull Movement disorders with paroxysmal ataxia dystonia dysarthria choreoathetosis myoclonus and eyendashhead movement abnormalities have also been identifi ed as allelic variants
bull Ninety percent of identifi ed children have epilepsy usually beginning in infancy
bull Seizure types encompass focal or generalized myoclonic tonic clonic astatic focal dyscognitive absence and nonconvulsive status epilepticus
bull Epilepsy may occur without accompanying motor or cognitive symptoms of GLUT1 DS and without appropriate diagnostic testing or lumbar puncture may be misclassifi ed as IGE
bull Clinical suspicion is based on history neurological examination and diagnostic lumbar puncture Blood samples for glucose and lactate should be obtained immediately before the lumbar puncture Hypoglycorrhachia and low or low-normal CSF lactate are necessary but not suffi cient for diagnostic confi rmation Decreased RBC glucose uptake SLC2A1 gene mutation or both confi rm the clinical diagnosis KD treatment should be started when the condition is suspected and continued if confi rmed
bull EEG fi ndings include normal background features focal or generalized slowing or attenuation or generalized focal
CLINICAL PEARLS (continued )
or multifocal spike-and-wave EEG fi ndings may vary depending on age metabolic status and treatment
bull MRI fi ndings may be normal or nonspecifi c Diffuse hypotrophy may be apparent over time particularly without KD treatment
bull Treatment with KD is the current standard of care for all forms of GLUT1 DS The dietary regimen should be adjusted to achieve blood BHB levels around 5 mM The goal is to provide optimal amounts of metabolic fuel for the developing brain Seizure control can be achieved at lower blood BHB levels
bull Epilepsy in GLUT1 DS is often refractory to standard anti-seizure medicines but responds rapidly and dramatically to the KD
bull KD provides the only alternative metabolic fuel for brain development at this time and promotes brain growth and neurological development
bull Prognosis is determined by early identifi cation of the underlying metabolic condition causing the clinical symptoms and prompt initiation of treatment with KD
bull Genetic counseling for families with an affected child is recommended
(continued )
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

324
8 Fujii T Ho YY Wang D et al Three Japanese patients with glucose transporter type 1 defi ciency syndrome Brain Dev 200729(2)92ndash97
9 Fung EL Ho YY Hui J et al First report of GLUT1 defi ciency syndrome in Chinese patients with novel and hot spot mutations in SLC2A1 gene Brain Dev 201133(2)170ndash173
10 Ito S Oguni H Ito Y et al Modifi ed Atkins diet therapy for a case with glucose transporter type 1 defi ciency syn-drome Brain Dev 200830(3)226ndash228
11 Oguni H Symptomatic epilepsies imitating idiopathic gen-eralized epilepsies Epilepsia 200546(Suppl 9)84ndash90
12 Pearson TS Pons R Engelstad K et al Paroxysmal eyendashhead movements in Glut1 defi ciency syndrome Neurology 201788(17)1666ndash1673
13 Coman DJ Sinclair KG Burke CJ et al Seizures ataxia developmental delay and the general paediatrician glu-cose transporter 1 defi ciency syndrome J Paediatr Child Health 200642(5)263ndash267
14 Larsen J Johannesen KM Ek J et al The role of SLC2A1 mutations in myoclonic astatic epilepsy and absence epi-lepsy and the estimated frequency of GLUT1 defi ciency syndrome Epilepsia 201556(12)e203ndashe208
15 Suls A Mullen SA Weber YG et al Early-onset absence epilepsy caused by mutations in the glucose transporter GLUT1 Ann Neurol 200966(3)415ndash419
16 Wang D Kranz-Eble P De Vivo DC Mutational analysis of GLUT1 (SLC2A1) in Glut-1 defi ciency syndrome Hum Mutat 200016(3)224ndash231
17 Wang D Pascual JM Yang H et al Glut-1 defi ciency syn-drome clinical genetic and therapeutic aspects Ann Neurol 200557(1)111ndash118
18 Klepper J Scheffer H Elsaid MF et al Autosomal recessive inheritance of GLUT1 defi ciency syndrome Neuropediatrics 200940(5)207ndash210
19 Rotstein M De Vivo DC Childhood absence epilepsy as a manifestation of GLUT1 defi ciency Ann Neurol 201067(2)272ndash273
20 Wang D Pascual JM Yang H et al A mouse model for Glut-1 haploinsuffi ciency Hum Mol Genet 200615(7)1169ndash1179
21 Bruumlggemann N Klein C Genetics of primary torsion dys-tonia Curr Neurol Neurosci Rep 201010(3)199ndash206
22 Weber YG Kamm C Suls A et al Paroxysmal choreo-athetosisspasticity (DYT9) is caused by a GLUT1 defect Neurology 201177(10)959ndash964
23 Akman CI Yu J Alter A et al Diagnosing Glucose Transporter 1 defi ciency at initial presentation facilitates early treatment J Pediatr 2016171220ndash226
24 Pong AW Geary BR Engelstad KM et al Glucose trans-porter type I defi ciency syndrome epilepsy phenotypes and outcomes Epilepsia 201253(9)1503ndash1510
25 Leary LD Wang D Nordli DR et al Seizure characteriza-tion and electroencephalographic features in Glut-1 defi -ciency syndrome Epilepsia 200344(5)701ndash707
26 Pong AW Pal DK Chung WK Developments in molecular genetic diagnostics an update for the pediatric epilepsy specialist Pediatr Neurol 201144(5)317ndash327
27 Pal DK Pong AW Chung WK Genetic evaluation and counseling for epilepsy Nat Rev Neurol 20106(8)445ndash453
28 Sedel F Gourfi nkel-An I Lyon-Caen O et al Epilepsy and inborn errors of metabolism in adults a diagnostic approach J Inherit Metab Dis 200730(6)846ndash854
29 Suls A Dedeken P Goffi n K et al Paroxysmal exercise-in-duced dyskinesia and epilepsy is due to mutations in SLC2A1 encoding the glucose transporter GLUT1 Brain 2008131(Pt 7)1831ndash1844
30 Weber YG Storch A Wuttke TV et al GLUT1 mutations are a cause of paroxysmal exertion-induced dyskinesias and induce hemolytic anemia by a cation leak J Clin Invest 2008118(6)2157ndash2168
31 Zorzi G Castellotti B Zibordi F et al Paroxysmal move-ment disorders in GLUT1 defi ciency syndrome Neurology 200871(2)146ndash148
32 De Vivo DC Wang D Glut1 defi ciency CSF glucose How low is too low Rev Neurol 2008164(11)877ndash880
33 Joshi C Greenberg CR de Vivo D et al GLUT1 defi -ciency without epilepsy yet another case J Child Neurol 200823(7)832ndash834
34 Dubos F Moulin F Gajdos V et al Serum procalcitonin and other biologic markers to distinguish between bacterial and aseptic meningitis J Pediatr 2006149(1)72ndash76
35 Javadekar BB Vyas MD Anand IS CSFblood glucose ratio and other prognostic indices in pyogenic meningitis J Indian Med Assoc 199795(1)9ndash11
36 Lindquist L Linneacute T Hansson LO et al Value of cere-brospinal fl uid analysis in the differential diagnosis of meningitis a study in 710 patients with suspected central nervous system infection Eur J Clin Microbiol Infect Dis 19887(3)374ndash380
37 Saacuteez-Llorens X Mccracken GH Bacterial meningitis in children Lancet 2003361(9375)2139ndash2148
38 Silver TS Todd JK Hypoglycorrhachia in pediatric patients Pediatrics 197658(1)67ndash71
39 Peacuterez-Duentildeas B Prior C Ma Q et al Childhood chorea with cerebral hypotrophy a treatable GLUT1 energy fail-ure syndrome Arch Neurol 200966(11)1410ndash1414
40 Akman CI Provenzano F Wang D et al Topography of brain glucose hypometabolism and epileptic net-work in glucose transporter 1 defi ciency Epilepsy Res 2015110206ndash215
41 Pascual JM van Heertum RL Wang D et al Imaging the metabolic footprint of Glut1 defi ciency on the brain Ann Neurol 200252(4)458ndash464
42 Klepper J Voit T Facilitated glucose transporter protein type 1 (GLUT1) defi ciency syndrome impaired glucose transport into brainmdasha review Eur J Pediatr 2002161(6)295ndash304
43 Wong HY Chu TS Lai JC et al Sodium valproate inhib-its glucose transport and exacerbates Glut1-defi ciency in vitro J Cell Biochem 200596(4)775ndash785
44 Kaufmann P Shungu DC Sano MC et al Cerebral lac-tic acidosis correlates with neurological impairment in MELAS Neurology 200462(8)1297ndash1302
45 Pascual JM Liu P Mao D et al Triheptanoin for glu-cose transporter type I defi ciency (G1D) modulation of human ictogenesis cerebral metabolic rate and cognitive indices by a food supplement JAMA Neurol 201471(10)1255ndash1265
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW
46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW

46 Ho YY Yang H Klepper J et al Glucose transporter type 1 defi ciency syndrome (Glut1DS) methylxanthines potentiate GLUT1 haploinsuffi ciency in vitro Pediatr Res 200150(2)254ndash260
47 Mochel F Hainque E Gras D et al Triheptanoin dra-matically reduces paroxysmal motor disorder in patients with GLUT1 defi ciency J Neurol Neurosurg Psychiatry 201687(5)550ndash553
48 Rotstein M Doran J Yang H et al Glut1 defi ciency and alternating hemiplegia of childhood Neurology 200973(23)2042ndash2044
49 Schneider SA Paisan-Ruiz C Garcia-Gorostiaga I et al GLUT1 gene mutations cause sporadic paroxysmal exercise-induced dyskinesias Mov Disord 200924(11)1684ndash1688
50 Ramm-Pettersen A Nakken KO Haavardsholm KC et al GLUT1-defi ciency syndrome Report of a four-generation Norwegian family with a mild phenotype Epilepsy Behav 201770(Pt A)1ndash4
51 Klepper J Scheffer H Leiendecker B et al Seizure control and acceptance of the ketogenic diet in GLUT1 defi ciency syndrome a 2- to 5-year follow-up of 15 children enrolled prospectively Neuropediatrics 200536(5)302ndash308
52 Mullen SA Suls A de Jonghe P et al Absence epilepsies with widely variable onset are a key feature of familial GLUT1 defi ciency Neurology 201075(5)432ndash440
53 Leen WG Klepper J Verbeek MM et al Glucose trans-porter-1 defi ciency syndrome the expanding clinical and genetic spectrum of a treatable disorder Brain 2010133(Pt 3)655ndash670
54 Roulet-Perez E Ballhausen D Bonafeacute L et al Glut-1 defi -ciency syndrome masquerading as idiopathic generalized epilepsy Epilepsia 200849(11)1955ndash1958
55 Takahashi S Ohinata J Suzuki N et al Molecular analy-sis and anticonvulsant therapy in two patients with glu-cose transporter 1 defi ciency syndrome a successful use of zonisamide for controlling the seizures Epilepsy Res 200880(1)18ndash22
56 Goumlkben S Yılmaz S Klepper J et al VideoEEG recording of myoclonic absences in GLUT1 defi ciency syndrome with
a hot-spot R126C mutation in the SLC2A1 gene Epilepsy Behav 201121(2)200ndash202
57 Striano P Weber YG Toliat MR et al EPICURE Consortium GLUT1 mutations are a rare cause of familial idiopathic generalized epilepsy Neurology 201278(8)557ndash562
58 Arsov T Mullen SA Damiano JA et al Early onset absence epilepsy 1 in 10 cases is caused by GLUT1 defi ciency Epilepsia 201253(12)e204ndashe207
59 Mullen SA Marini C Suls A et al Glucose transporter 1 defi ciency as a treatable cause of myoclonic astatic epi-lepsy Arch Neurol 201168(9)1152ndash1155
60 Boles RG Seashore MR Mitchell WG et al Glucose trans-porter type 1 defi ciency a study of two cases with vid-eo-EEG Eur J Pediatr 1999158(12)978ndash983
61 von Moers A Brockmann K Wang D et al EEG features of glut-1 defi ciency syndrome Epilepsia 200243(8)941ndash945
62 Akman CI Engelstad K Hinton VJ et al Acute hypergly-cemia produces transient improvement in glucose trans-porter type 1 defi ciency Ann Neurol 201067(1)31ndash40
63 Alter AS Engelstad K Hinton VJ et al Long-term clini-cal course of Glut1 defi ciency syndrome J Child Neurol 201530(2)160ndash169
64 Roe CR Mochel F Anaplerotic diet therapy in inherited metabolic disease therapeutic potential J Inherit Metab Dis 200629(2ndash3)332ndash340
65 Estrada DE Ewart HS Tsakiridis T et al Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acidthioctic acid participation of elements of the insulin signal-ing pathway Diabetes 199645(12)1798ndash1804
66 Klepper J vera JC de Vivo DC Defi cient transport of dehy-droascorbic acid in the glucose transporter protein syn-drome Ann Neurol 199844(2)286ndash287
67 Klepper J Wang D Fischbarg J et al Defective glucose transport across brain tissue barriers a newly recognized neurological syndrome Neurochem Res 199924(4)587ndash594
68 Tang M Gao G Rueda CB et al Brain microvasculature defects and Glut1 defi ciency syndrome averted by early repletion of the glucose transporter-1 protein Nat Commun 2017814152 doi101038ncomms14152
This is a sample from INHERITED METABOLIC EPILEPSIES SECOND EDITION SECOND EDITION
copy Springer Publishing Company
VISIT THIS BOOKrsquoS WEB PAGE BUY NOW