Embed Size (px)
Citation preview
Pheochromocytoma and Paraganglioma:
Progress in Therapeutics
Camilo Jimenez, MDAssociate Professor
The University of Texas MD Anderson Cancer Center
Outline
• Introduction: anatomical definitions, clinical manifestations, biochemical diagnosis, genetics, imaging.
• Therapeutics:– Preoperative management
– Catecholamine crisis
– Constipation
– Clinical predictors of malignancy
– Systemic therapy
Anatomical definitions

Paraganglia
• Group of neuro-
endocrine cells that
migrate during
embryonic
development with
components of the
parasympathetic and
sympathetic ganglia.
Pheochromocytomas
• Chromaffin (+) tumors originated in the adrenal medulla. They may produce catecholamines such as epinephrine and/or norepinephrine predisposing to cardiovascular disease and other complications.
WHO 2004

Paragangliomas
• Paragangliomas are tumors that arise from extra-adrenal chromaffin cells and can originate either in the parasympathetic or sympathetic ganglia.
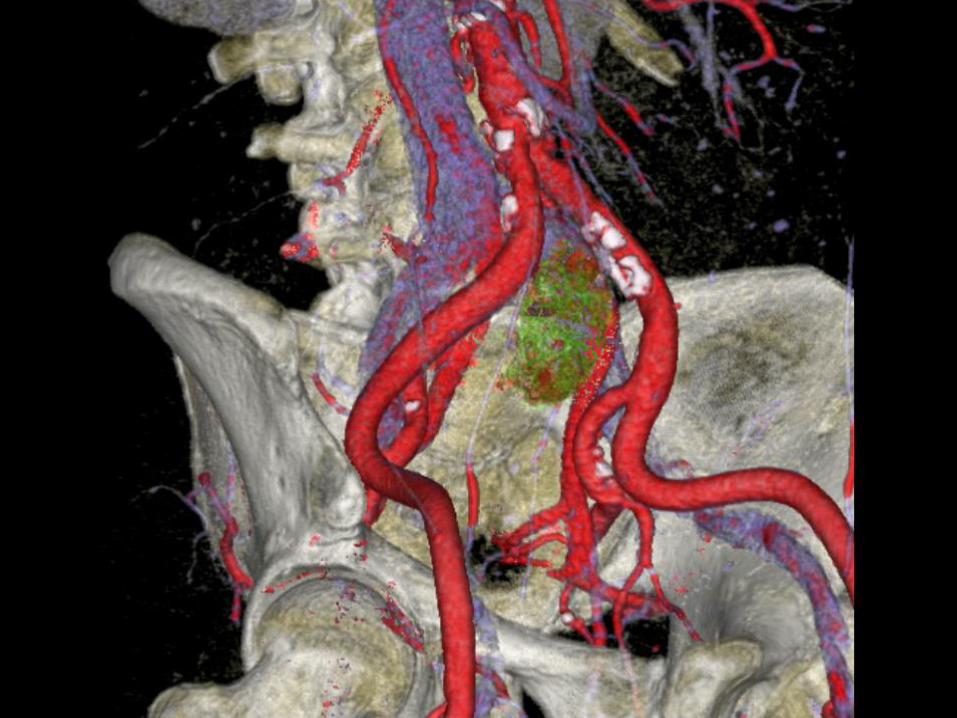
– Parasympathetic: chemodectomas, carotid body tumors, glomusjugular tumors, etc.
– Sympathetic: thoracic, abdominal, and pelvic tumors. They may produce norepinephrine and/or dopamine predisposing to cardiovascular disease and other endocrine complications
WHO 2004
Clinical Manifestations
• More than 100 symptoms and signs have been described in association with these tumors. Hypertension, headaches, palpitations, and diaphoresis are the most common ones.
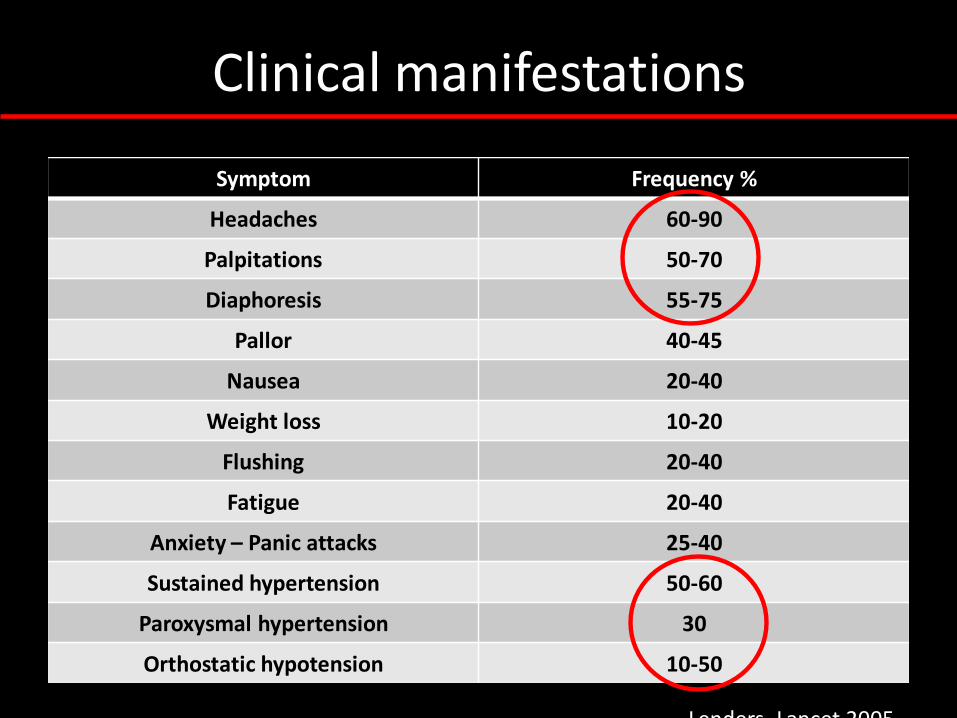
Clinical manifestations
Symptom Frequency %
Headaches 60-90
Palpitations 50-70
Diaphoresis 55-75
Pallor 40-45
Nausea 20-40
Weight loss 10-20
Flushing 20-40
Fatigue 20-40
Anxiety – Panic attacks 25-40
Sustained hypertension 50-60
Paroxysmal hypertension 30
Orthostatic hypotension 10-50
Lenders, Lancet 2005
Clinical manifestations
• The clinical presentation of these tumors is highly variable and can overlap with the signs and symptoms associated with numerous other non-related clinical conditions.
• The critical first step in making the diagnosis is to suspect the presence of a tumor.
Biochemical Diagnosis
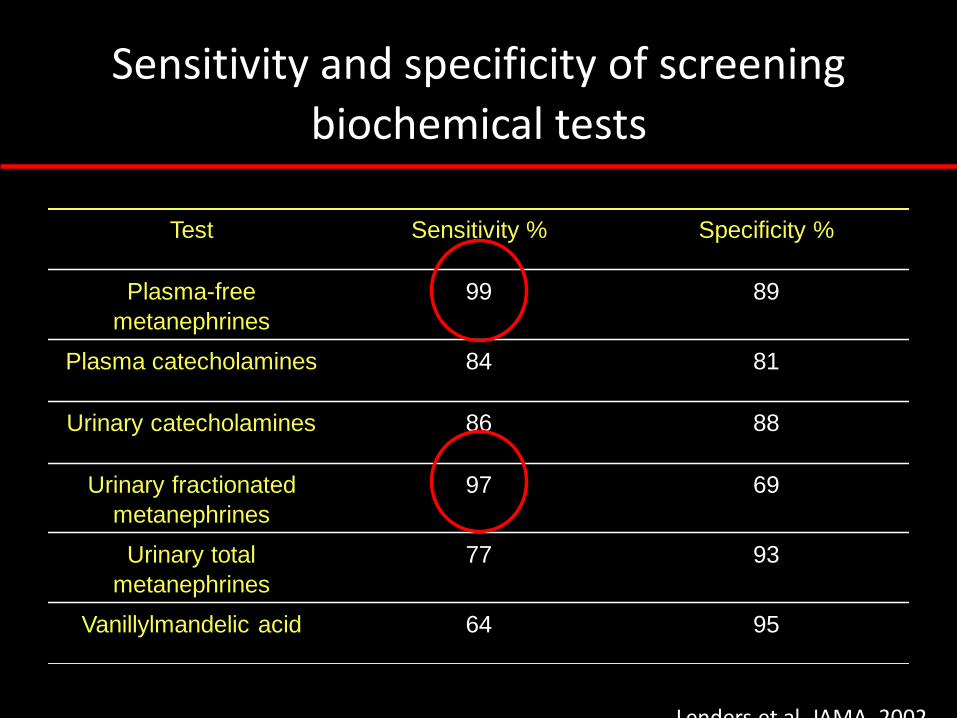
Sensitivity and specificity of screening
biochemical tests
Test Sensitivity % Specificity %
Plasma-free
metanephrines
99 89
Plasma catecholamines 84 81
Urinary catecholamines 86 88
Urinary fractionated
metanephrines
97 69
Urinary total
metanephrines
77 93
Vanillylmandelic acid 64 95
Lenders et al, JAMA, 2002
Drugs that may cause false positive elevations of plasma metanephrines
• Tricyclic antidepressants
• Alpha-blockers
• Beta-blockers
• Calcium channel
blockers
• Vasodilators
• Monoamine oxidase
inhibitors
• Sympathomimetics
• Stimulants
• Levodopa and
carbidopa
• Cocaine
Lenders, Lancet 2005
Imaging
• CT/MRI scans are sensitive tests for the localization of these tumors (>95%)
• Complimentary studies include MIBG, octreotide, FDG-PET, dopamine scans, etc
• 83-87% of these tumors are not malignant
Brito, Endocrine, 2015
Genetics
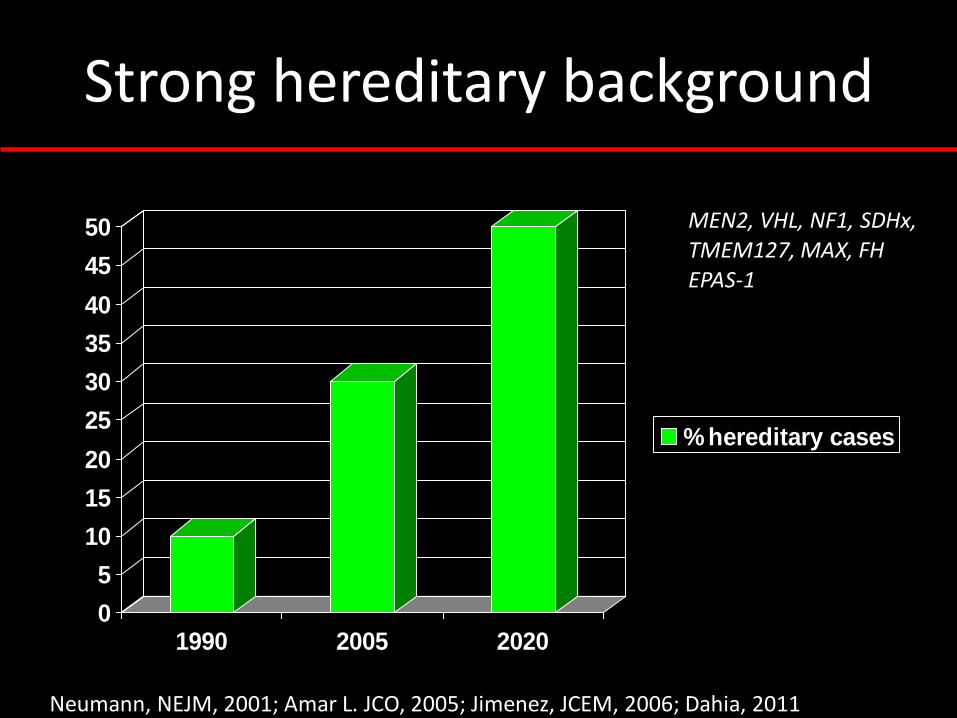
Strong hereditary background
0
5
10
15
20
25
30
35
40
45
50
1990 2005 2020
% hereditary cases
Neumann, NEJM, 2001; Amar L. JCO, 2005; Jimenez, JCEM, 2006; Dahia, 2011
MEN2, VHL, NF1, SDHx,TMEM127, MAX, FHEPAS-1

Therapeutics
Therapeutic challenges
• Patients with pheochromocytomas and paragangliomas are uncommon; thus, the clinicians experience on treating these patients is limited
• Treatment for acute and chronic complications is not well-recognized
• There are no expert guidelines on the follow-up and treatment of patients with malignant disease
• Therapeutic options for patients with malignancy are very limited

Preoperative Management
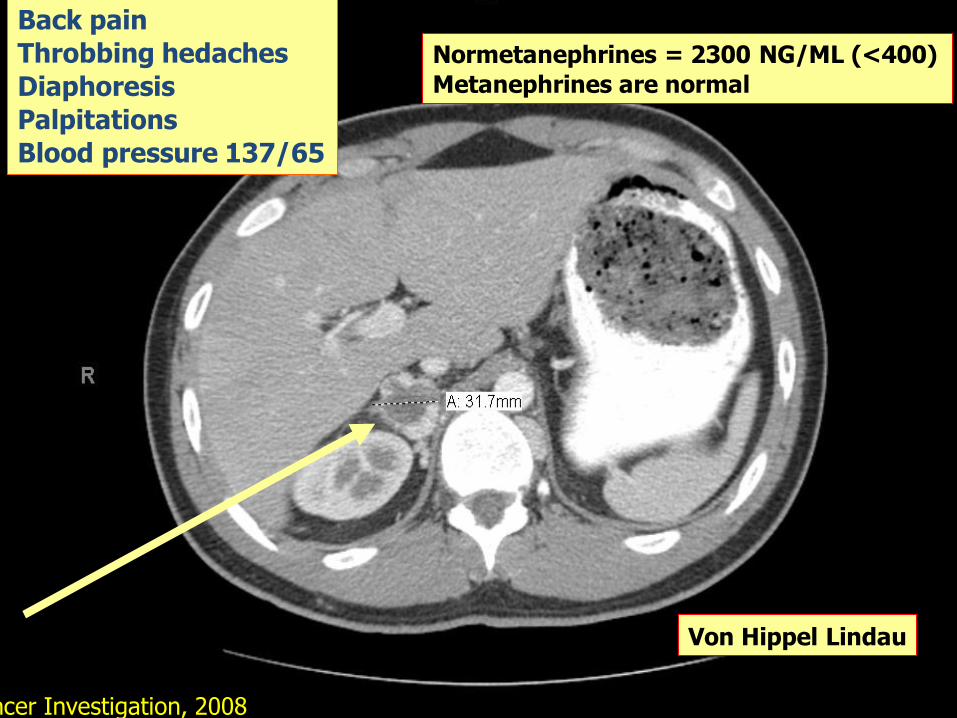
Back pain
Throbbing hedaches
Diaphoresis
Palpitations
Blood pressure 137/65
Normetanephrines = 2300 NG/ML (<400)
Metanephrines are normal
Von Hippel Lindau
Rich, Cancer Investigation, 2008
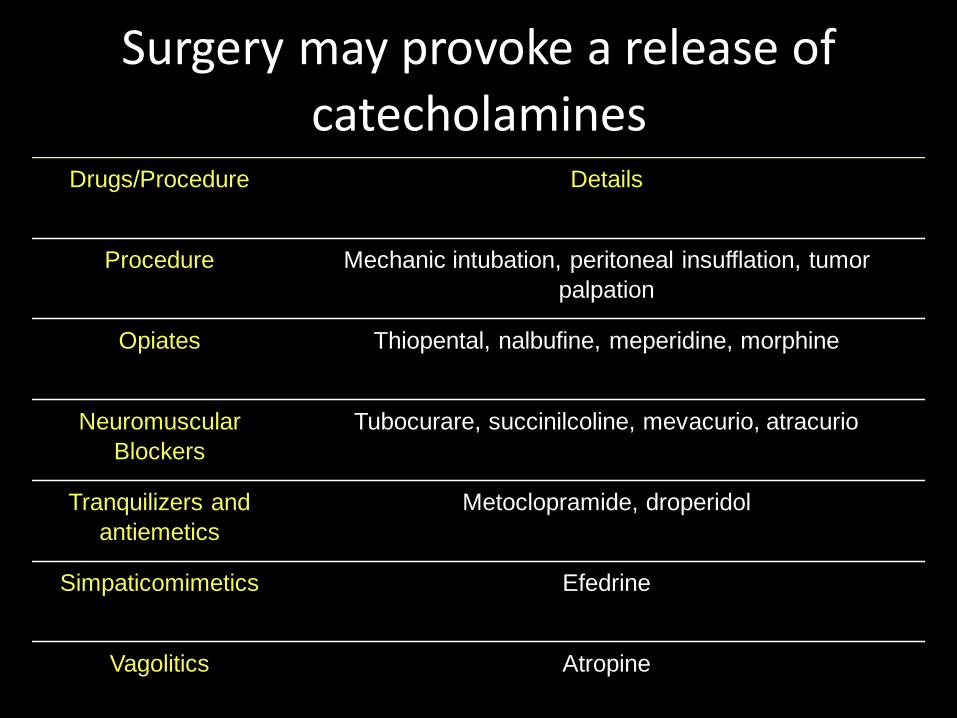
Surgery may provoke a release of
catecholaminesDrugs/Procedure Details
Procedure Mechanic intubation, peritoneal insufflation, tumor
palpation
Opiates Thiopental, nalbufine, meperidine, morphine
Neuromuscular
Blockers
Tubocurare, succinilcoline, mevacurio, atracurio
Tranquilizers and
antiemetics
Metoclopramide, droperidol
Simpaticomimetics Efedrine
Vagolitics Atropine
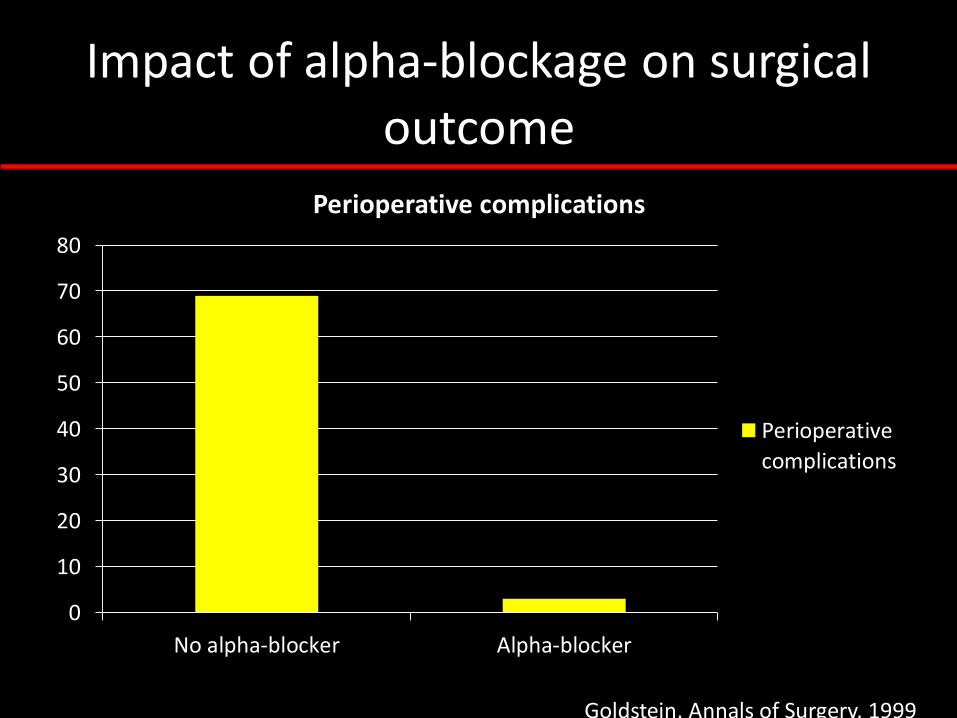
Impact of alpha-blockage on surgical
outcome
0
10
20
30
40
50
60
70
80
No alpha-blocker Alpha-blocker
Perioperative complications
Perioperative
complications
Goldstein, Annals of Surgery, 1999
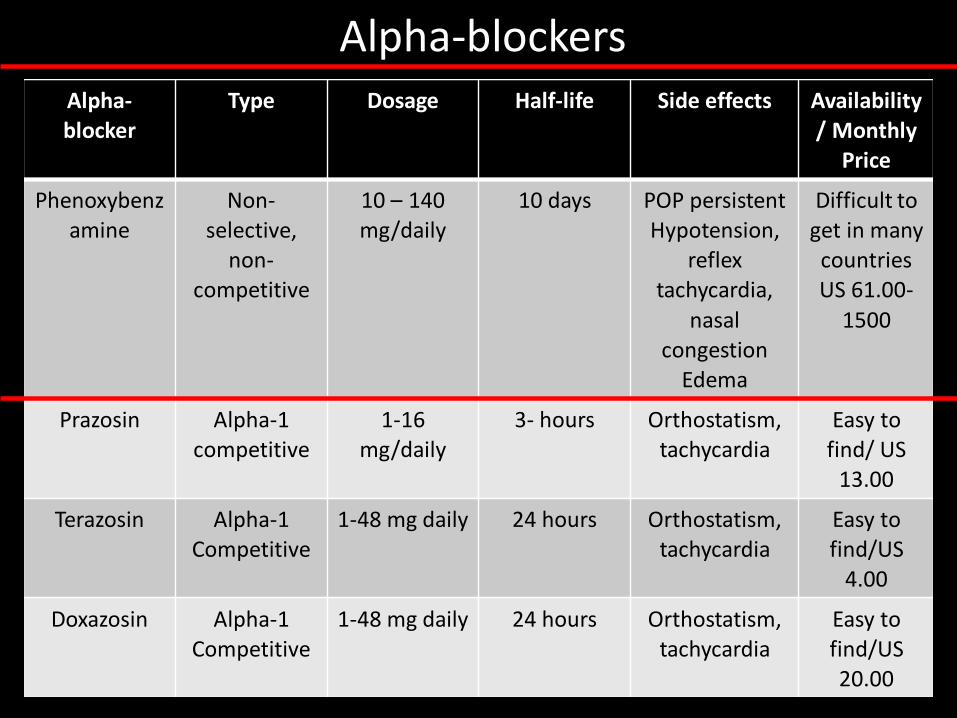
Alpha-blocker
Type Dosage Half-life Side effects Availability/ Monthly
Price
Phenoxybenzamine
Non-selective,
non-competitive
10 – 140 mg/daily
10 days POP persistentHypotension,
reflex tachycardia,
nasal congestion
Edema
Difficult to get in many countriesUS 61.00-
1500
Prazosin Alpha-1 competitive
1-16 mg/daily
3- hours Orthostatism,tachycardia
Easy to find/ US
13.00
Terazosin Alpha-1Competitive
1-48 mg daily 24 hours Orthostatism,tachycardia
Easy to find/US
4.00
Doxazosin Alpha-1Competitive
1-48 mg daily 24 hours Orthostatism,tachycardia
Easy to find/US 20.00
Alpha-blockers
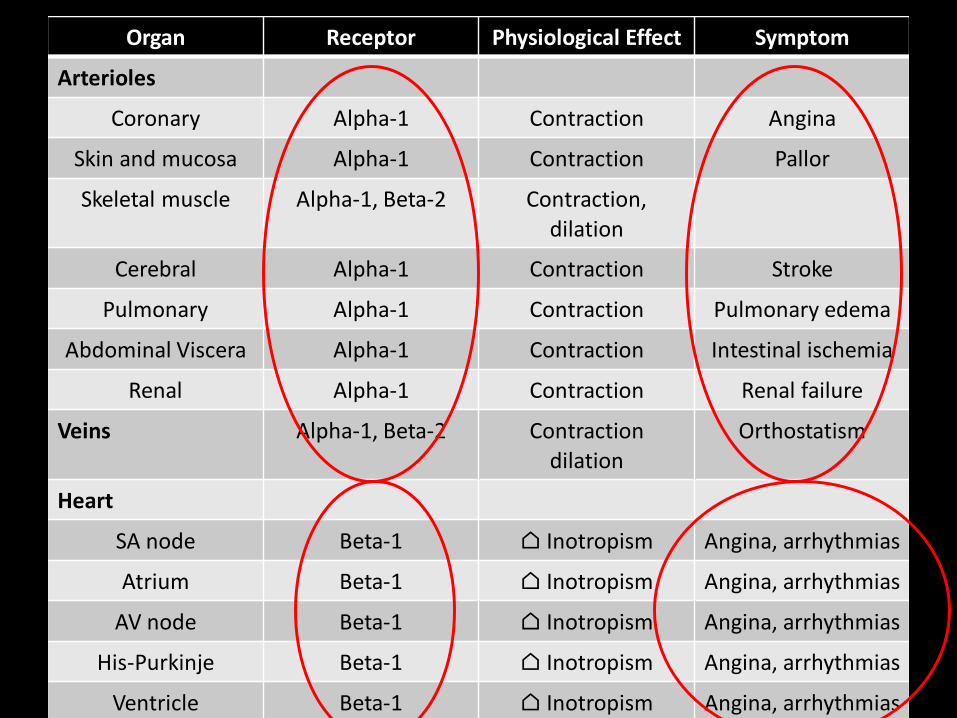
Organ Receptor Physiological Effect Symptom
Arterioles
Coronary Alpha-1 Contraction Angina
Skin and mucosa Alpha-1 Contraction Pallor
Skeletal muscle Alpha-1, Beta-2 Contraction,dilation
Cerebral Alpha-1 Contraction Stroke
Pulmonary Alpha-1 Contraction Pulmonary edema
Abdominal Viscera Alpha-1 Contraction Intestinal ischemia
Renal Alpha-1 Contraction Renal failure
Veins Alpha-1, Beta-2 Contractiondilation
Orthostatism
Heart
SA node Beta-1 ⌂ Inotropism Angina, arrhythmias
Atrium Beta-1 ⌂ Inotropism Angina, arrhythmias
AV node Beta-1 ⌂ Inotropism Angina, arrhythmias
His-Purkinje Beta-1 ⌂ Inotropism Angina, arrhythmias
Ventricle Beta-1 ⌂ Inotropism Angina, arrhythmias
Beta-blockers
• They should be initiated once the patient develops orthostatism and/or reflex tachycardia which indicate that alpha blockage has been obtained.
• Selective: Metoprolol, Atenolol
• Non-selective: Propranolol
• Labetalol and Carvedilol
Calcium Channel Blockers and ACE
inhibitors
• Indications:– Mild cases (e.g. small tumors identified by
radiographic screening in patient with hereditary predisposition) or unable to tolerate alpha-blockers
– As a supplement to alpha- and beta-blockers when BP is still difficult to control
– As a supplement to alpha- and beta-blockers in order to prevent toxicity associated with higher doses
Metyrosine
• Tyrosine hydroxilase inhibitor
• It decreases catecholamine secretion
• It has side effects that frequently prevent the use of effective doses: fatigue, depression, anxiety, diarrhea
• Price > US 1000

How long it takes to prepare someone
for surgery?
• 7-14 days
• At MDACC the average time is 8 days thanks to communication with the patient daily and frequent drug adjustments
• There is no need to admit the patient to the hospital or to use metyrosine.
• The patient should have a normal salt diet and free water intake. IV fluids may be necessary before surgery.

Catecholamine Crisis
Case Presentation
• 40 year old man with a history of a malignant paraganglioma presents to the ER with chest pain, shortness of breath, nausea, vomiting, headaches (“his head is about to explode”), and palpitations.
• Blood pressure is 230/140 mmHg, Pulse 124 pmn
• EKG shows sinus tachycardia. Troponin is normal. BNP is elevated at 2118.
• The patient is not compliant with his antihypertensive treatment

Medication Preparation Dose Details
Nitroprusside: dilator (arterial > vein); rapid action 30 seconds, peak at two
minutes
50 mg in 250 cc of D5W. Should be protected from the light
0.5-5 ug/kg/minNo used for more than 24 hours.
Cyanide toxicity/lactic acidosis; tachycardia, hypotension
Nicardapine calcium channel blocker; vasodilator
25 mg in 250 cc of D5W
Loading 1-2.5 mg/1-2 min; Infusion 5-15 mg/h
Reflex mild tachycardia, prevents coronary spasm
Magnesium Sulfate, vasodilator, antiarrhytmic,decreases
catecholamine secretion
40 g in 500 cc of Ringer solution
Loading 1-2 g; infusion 1-3 g/h
Muscular weakness, high magnesium
Fenoldopam 10 mg in 250 cc of NS
0.1-1.6 ug/kg/min Renoprotective, causes tachycardia
Phentolamine alpha-blocker
100 mg in 500 cc of D5W
Bolus 5-15 mg; infusion 0.2-2mg/min
Half-life 19 minutesTachycardia
Urapidil 12.5 g in 250 cc of NS CNS effects
Esmolol
• B1-blocker
• Short half-life of 9 minutes
• Very fast action
• Excellent to control tachycardia once a vasodilator has been started
• Loading 500 ug/kg over one minute
• Infusion 50-300 ug/kg/min

Gastrointestinal disease
Case presentation
• 46 year-old man with history of malignant paraganglioma presents with hypertension, palpitations, headaches, sweats, and constipation for longer than 1 year (last bowel movement was hard and happened 8 days ago). The patient noticed fever, nausea, and lack of appetite. On physical examination bowel sounds are decreased.
• Creatinine and WBC are elevated
• Plasma normetanephrines 49.5 nmol/L (<0.90)
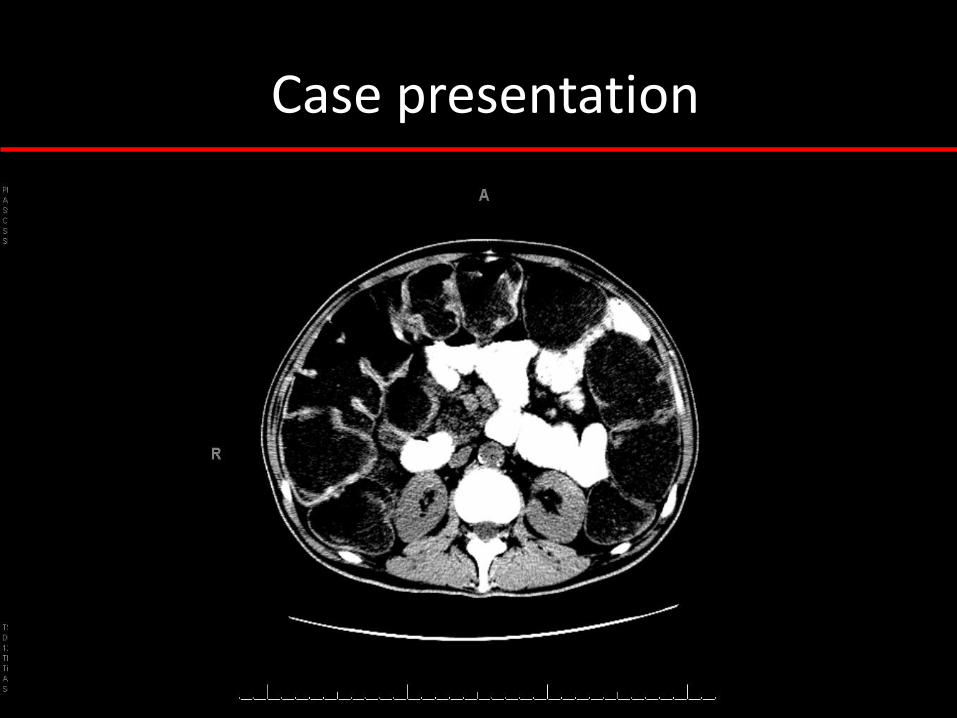
Case presentation
Constipation
• It happens in 6% of patients
• It is usually mild but occasional cases are severe
• It may predispose to hemorrhoids, stercoral ulcers, toxic megacolon, bleeding, perforation, and obstruction.
• Alpha- and beta-blockers do not treat constipation. Laxatives are required and their chose depends on the severity.
• It is preventable with diet rich in fiber and liquids
Thosani, EJE, 2015
Treatment of Metastatic Disease.
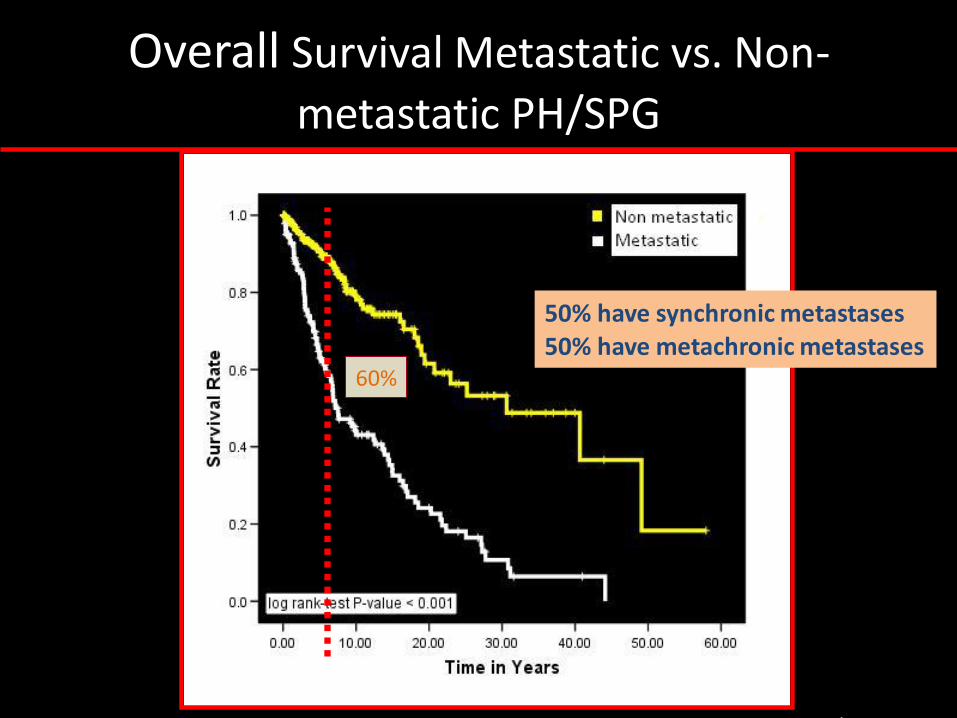
Overall Survival Metastatic vs. Non-
metastatic PH/SPG
60%
Jimenez C, Curr Oncol Rep, 2013
50% have synchronic metastases50% have metachronic metastases
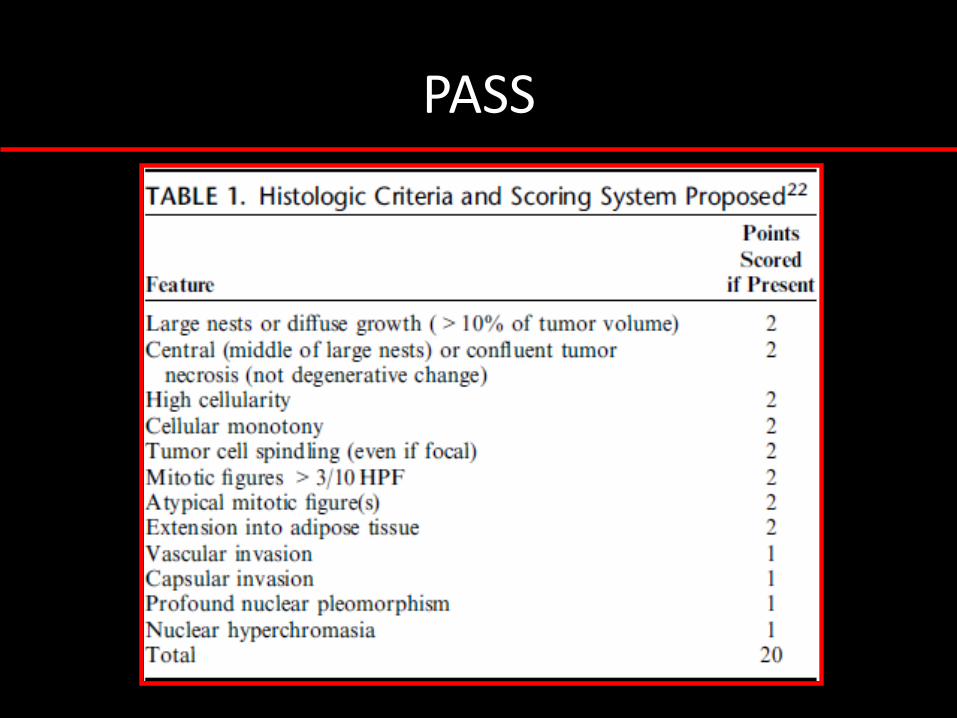
PASS
Thomson, Am J Surg Pathol, 2002
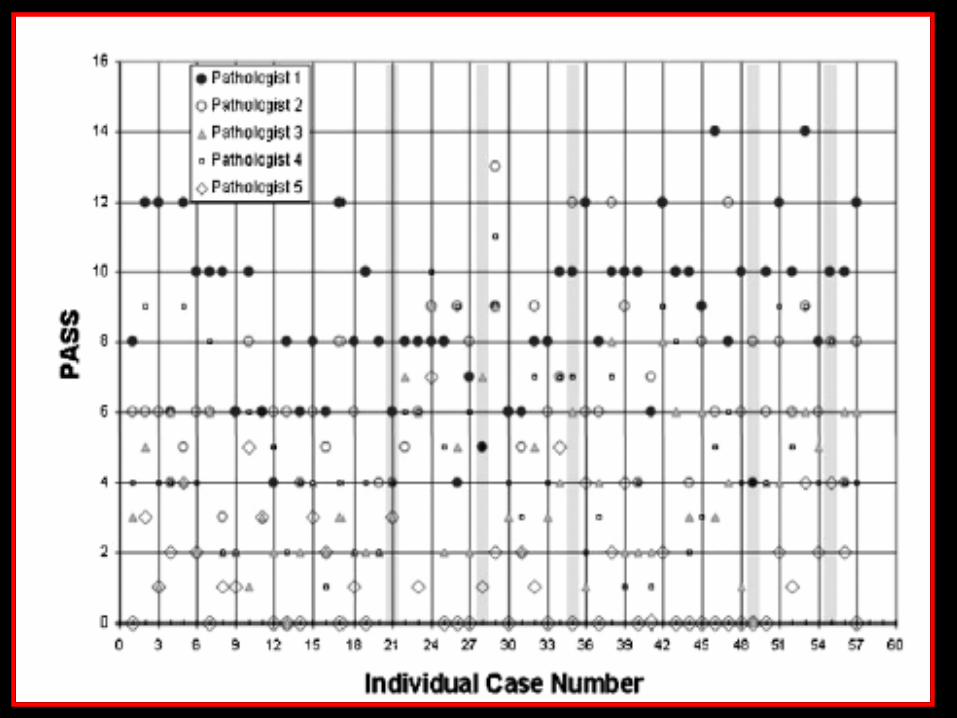
Wu, Am J Surg Pathol, 2009

MIBG

Meta-Iodobenzylguanidine (MIBG)
• Described by Wieland et al in 1979 at the University of Michigan
• Iodination in the meta position
– Stable and highly resistant to in vivo metabolism
• ~90% excreted intact in the urine
– 40-50% within 24 hours
• MIBG is not a norepinephrine analog
– Substrate for norepinephrine transporter (NET)
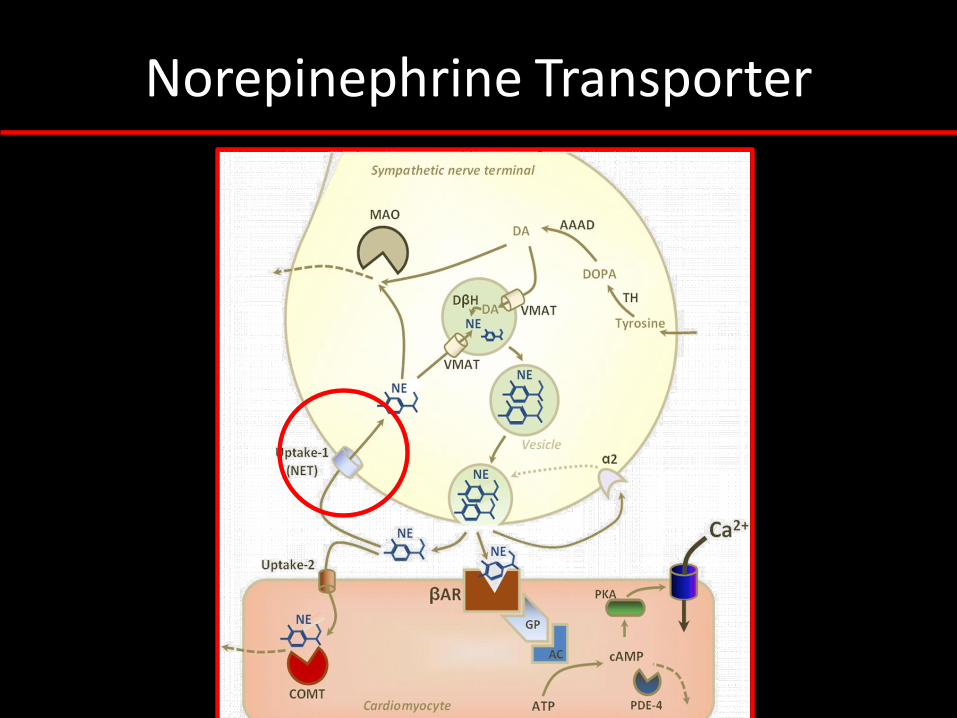
Norepinephrine Transporter
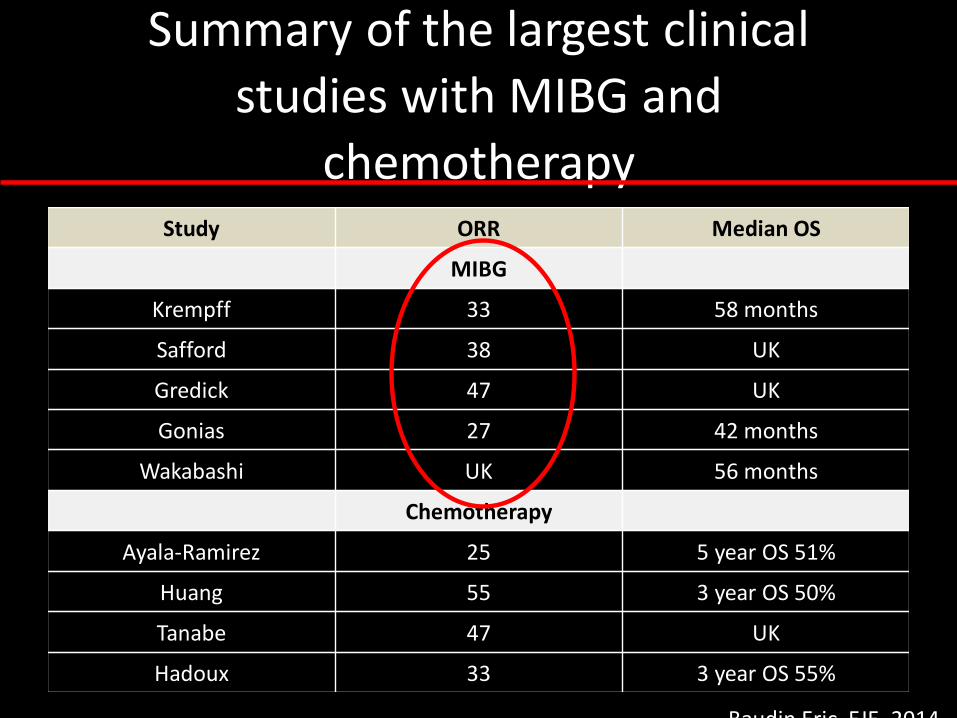
Summary of the largest clinical
studies with MIBG and
chemotherapyStudy ORR Median OS
MIBG
Krempff 33 58 months
Safford 38 UK
Gredick 47 UK
Gonias 27 42 months
Wakabashi UK 56 months
Chemotherapy
Ayala-Ramirez 25 5 year OS 51%
Huang 55 3 year OS 50%
Tanabe 47 UK
Hadoux 33 3 year OS 55%
Baudin Eric, EJE, 2014

Azedra®
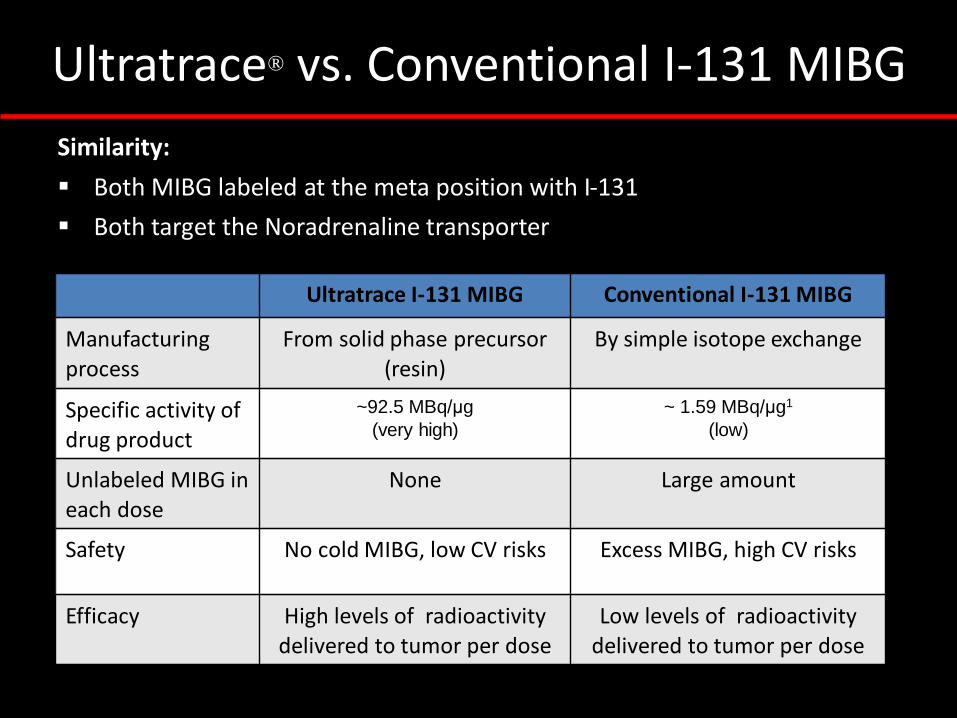
Similarity:
▪ Both MIBG labeled at the meta position with I-131
▪ Both target the Noradrenaline transporter
Differences: Ultratrace I-131 MIBG Conventional I-131 MIBG
Manufacturing process
From solid phase precursor (resin)
By simple isotope exchange
Specific activity of drug product
~92.5 MBq/μg
(very high)
~ 1.59 MBq/μg1
(low)
Unlabeled MIBG ineach dose
None Large amount
Safety No cold MIBG, low CV risks Excess MIBG, high CV risks
Efficacy High levels of radioactivitydelivered to tumor per dose
Low levels of radioactivitydelivered to tumor per dose
Ultratrace® vs. Conventional I-131 MIBG
AZEDRA® (iobenguane I 131) in patients with metastatic and/or recurrent and/or
unresectable pheochromocytoma or paraganglioma: Results of a multicenter,
open-label, pivotal phase 2b study
NCT00874614

Study Design
•Primary endpoint
• Proportion of patients with a reduction
(including discontinuation) of all
antihypertensive medication(s) by at least
50% for ≥ 6 months
•Secondary endpoints
• Objective tumor response by RECIST 1.0
• Biochemical tumor marker response
• Overall survival up to 5 years post- first
therapeutic dose
• Safety
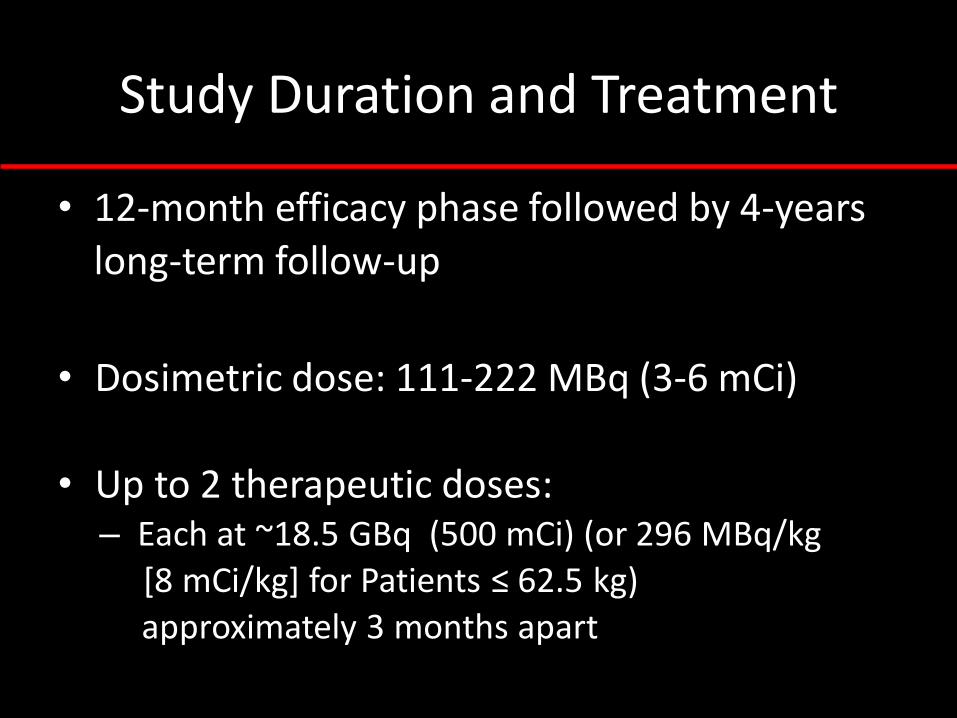
Study Duration and Treatment
• 12-month efficacy phase followed by 4-years long-term follow-up
• Dosimetric dose: 111-222 MBq (3-6 mCi)
• Up to 2 therapeutic doses:– Each at ~18.5 GBq (500 mCi) (or 296 MBq/kg
[8 mCi/kg] for Patients ≤ 62.5 kg)
approximately 3 months apart
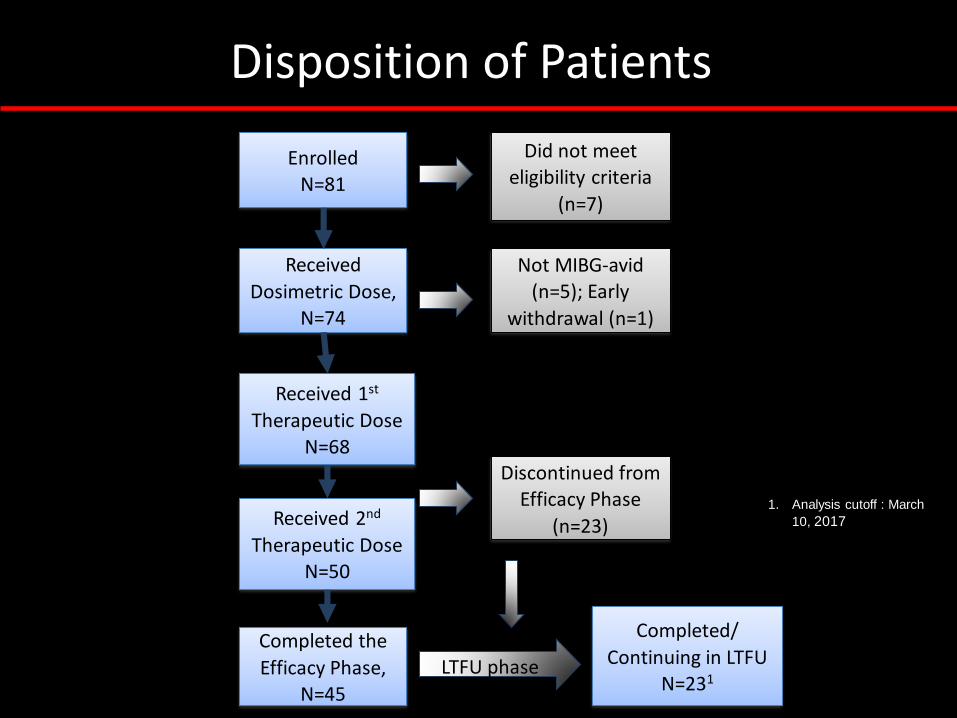
Disposition of Patients
Enrolled N=81
Did not meet
eligibility criteria
(n=7)
Received
Dosimetric Dose, N=74
Not MIBG-avid (n=5); Early
withdrawal (n=1)
Received 1st
Therapeutic DoseN=68
Received 2nd
Therapeutic DoseN=50
Discontinued from Efficacy Phase
(n=23)
Completed the
Efficacy Phase, N=45
1. Analysis cutoff : March
10, 2017
LTFU phase
Completed/
Continuing in LTFUN=231
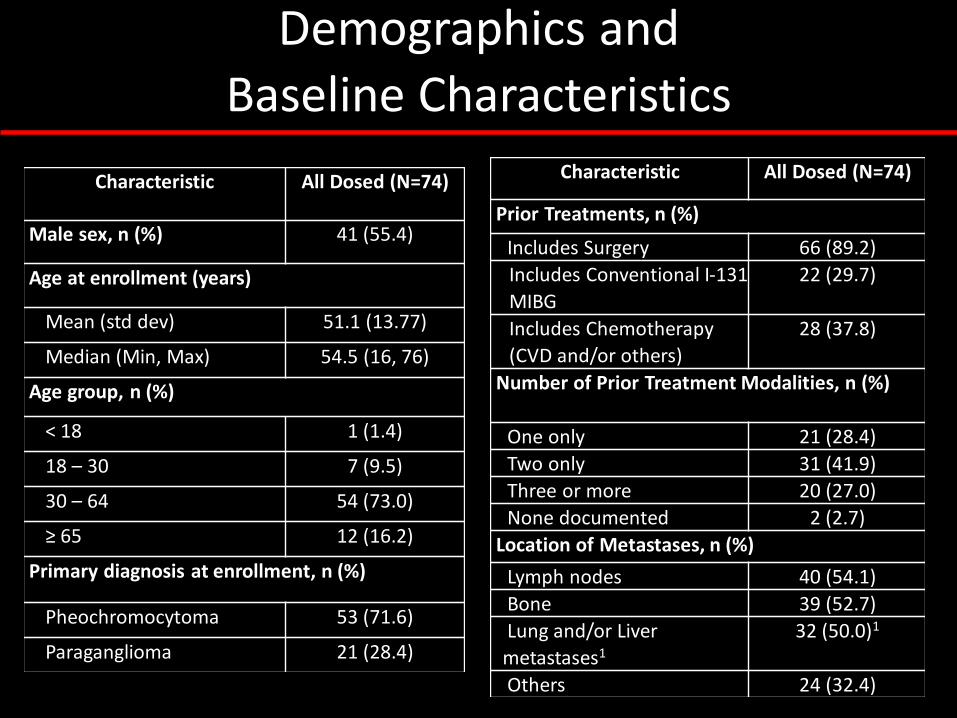
Demographics and
Baseline Characteristics
Characteristic All Dosed (N=74)
Male sex, n (%) 41 (55.4)
Age at enrollment (years)
Mean (std dev) 51.1 (13.77)
Median (Min, Max) 54.5 (16, 76)
Age group, n (%)
< 18 1 (1.4)
18 – 30 7 (9.5)
30 – 64 54 (73.0)
≥ 65 12 (16.2)
Primary diagnosis at enrollment, n (%)
Pheochromocytoma 53 (71.6)
Paraganglioma 21 (28.4)
Characteristic All Dosed (N=74)
Prior Treatments, n (%)
Includes Surgery 66 (89.2)
Includes Conventional I-131
MIBG
22 (29.7)
Includes Chemotherapy
(CVD and/or others)
28 (37.8)
Number of Prior Treatment Modalities, n (%)
One only 21 (28.4)
Two only 31 (41.9)
Three or more 20 (27.0)
None documented 2 (2.7)
Location of Metastases, n (%)
Lymph nodes 40 (54.1)
Bone 39 (52.7)
Lung and/or Liver
metastases1
32 (50.0)1
Others 24 (32.4)
Clinical Benefit (primary
endpoint)
• As of primary analysis data cutoff, the primary endpoint was achieved in 25% (95% CI, 0.16 – 0.37) of all patients
who received at least one Tx dose, achieving the pre-specified success criteria. Specifically, it was achieved in
32% (16/50) of patients who received two Tx doses, and
5.6% (1/18) of patients who received only one Tx dose
• Median duration of clinical benefit in primary endpoint responders was 13.3 (range 8.0-60.2) months
• 31.4% (16/51) of patients who were not responders on the
primary endpoint also experienced ≥ 50% reduction of antihypertensive medication(s), albeit for < 6 months
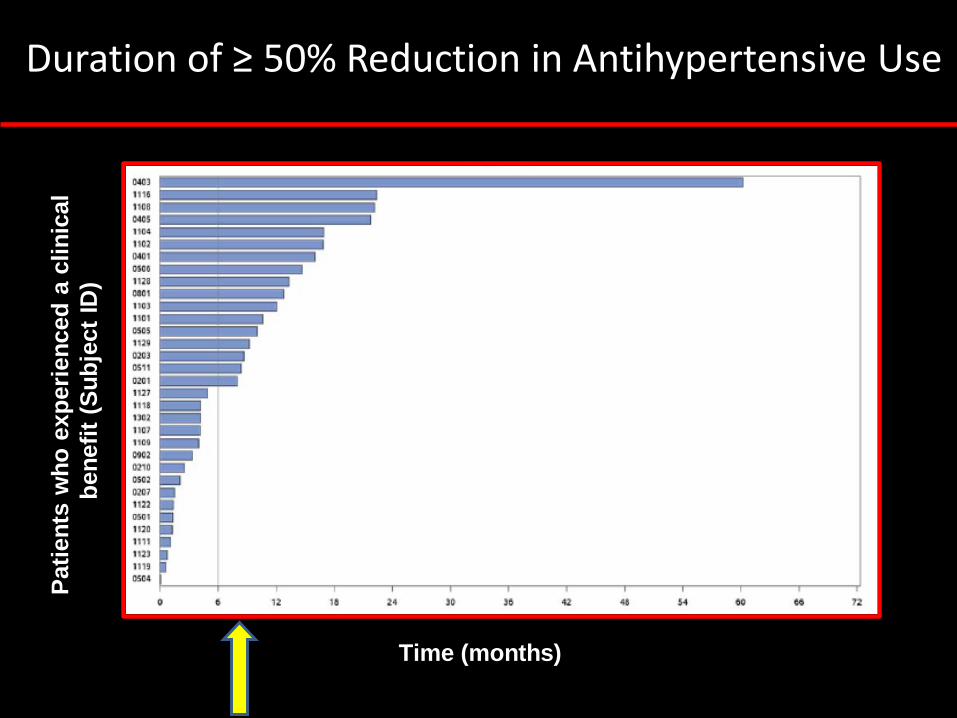
Pati
en
ts w
ho
exp
eri
en
ced
a c
lin
ical
ben
efi
t (S
ub
ject
ID)
Time (months)
Duration of ≥ 50% Reduction in Antihypertensive Use
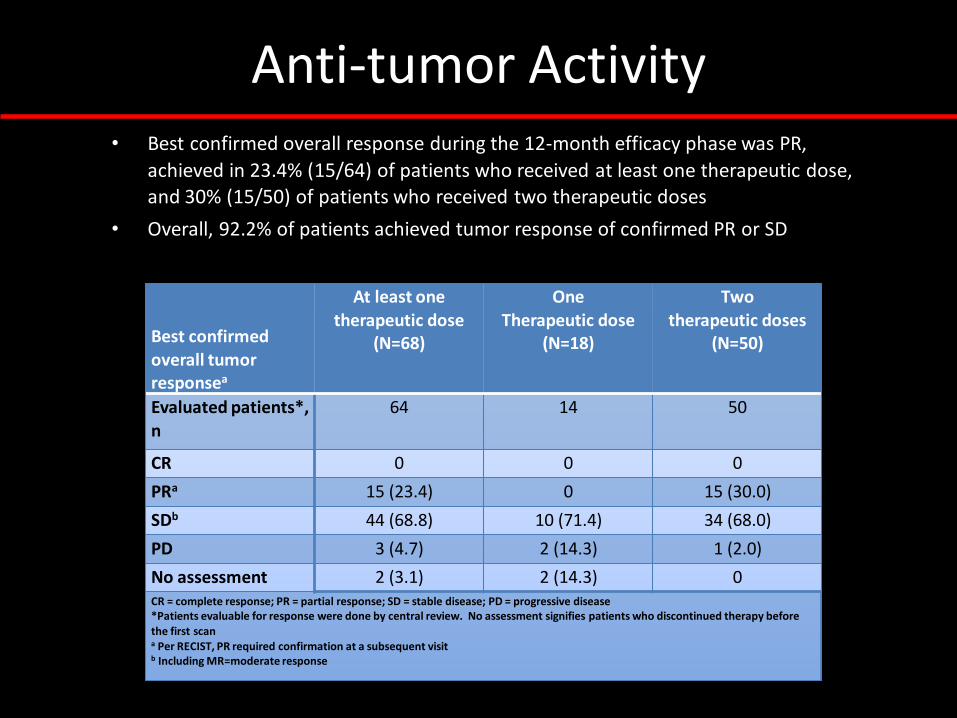
Anti-tumor Activity
Best confirmed overall tumor responsea
At least onetherapeutic dose
(N=68)
One Therapeutic dose
(N=18)
Twotherapeutic doses
(N=50)
Evaluated patients*,
n
64 14 50
CR 0 0 0
PRa 15 (23.4) 0 15 (30.0)
SDb 44 (68.8) 10 (71.4) 34 (68.0)
PD 3 (4.7) 2 (14.3) 1 (2.0)
No assessment 2 (3.1) 2 (14.3) 0CR = complete response; PR = partial response; SD = stable disease; PD = progressive disease*Patients evaluable for response were done by central review. No assessment signifies patients who discontinued therapy before the first scana Per RECIST, PR required confirmation at a subsequent visitb Including MR=moderate response
• Best confirmed overall response during the 12-month efficacy phase was PR,
achieved in 23.4% (15/64) of patients who received at least one therapeutic dose, and 30% (15/50) of patients who received two therapeutic doses
• Overall, 92.2% of patients achieved tumor response of confirmed PR or SD
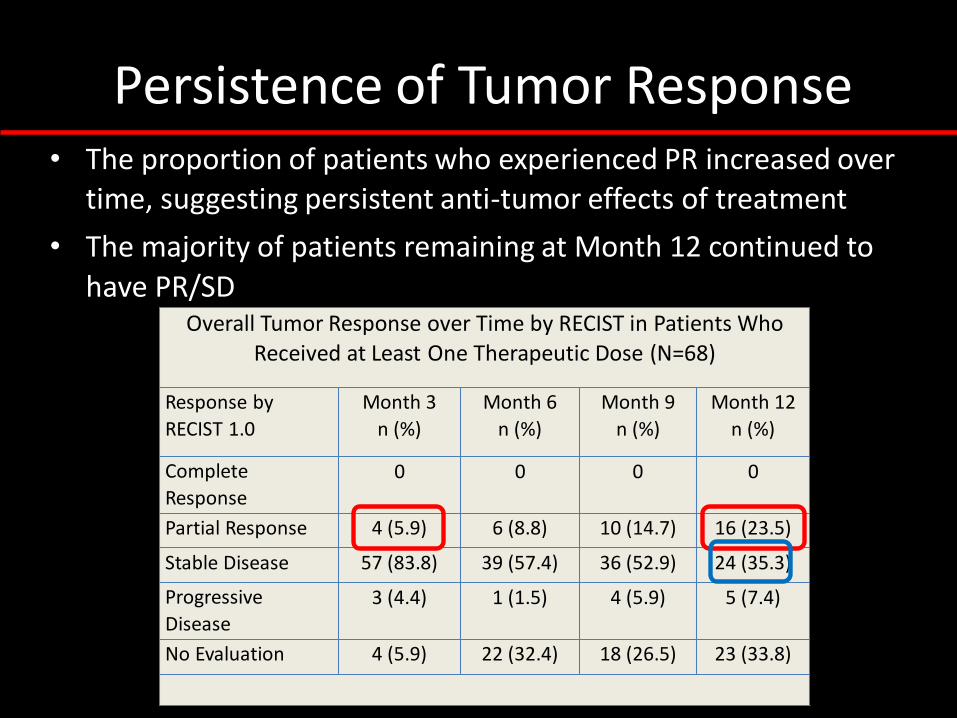
Persistence of Tumor Response• The proportion of patients who experienced PR increased over
time, suggesting persistent anti-tumor effects of treatment
• The majority of patients remaining at Month 12 continued to
have PR/SDOverall Tumor Response over Time by RECIST in Patients Who
Received at Least One Therapeutic Dose (N=68)
Response by
RECIST 1.0
Month 3
n (%)
Month 6
n (%)
Month 9
n (%)
Month 12
n (%)
Complete
Response0 0 0 0
Partial Response 4 (5.9) 6 (8.8) 10 (14.7) 16 (23.5)
Stable Disease 57 (83.8) 39 (57.4) 36 (52.9) 24 (35.3)
Progressive
Disease
3 (4.4) 1 (1.5) 4 (5.9) 5 (7.4)
No Evaluation 4 (5.9) 22 (32.4) 18 (26.5) 23 (33.8)

Tumor Response and
Primary Endpoint• Confirmed PR occurred in 41.2% (7/17) of patients who were considered
responders for the primary endpoint, and 17.0% (8/47) of patients who were not responders for the primary endpoint
• 100% (17/17) of primary endpoint responders achieved PR/SD during the efficacy phase
• 89.3% (41/47) of primary endpoint non-responders achieved PR/SD; 6.4% (3/47) had PD Maximum Percent Change from Baseline in Measurable Target
Lesion
RECIST 1.0, Central
Review
One primary endpoint
responder is not included in the graph because the patient did not have measurable target lesions
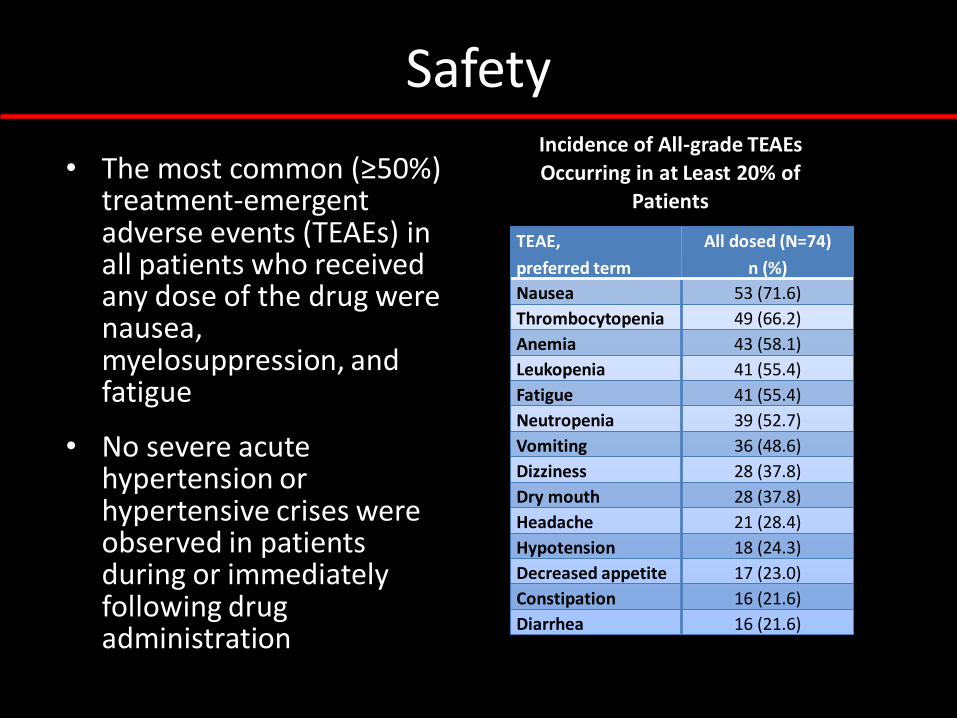
Safety
• The most common (≥50%) treatment-emergent adverse events (TEAEs) in all patients who received any dose of the drug were nausea, myelosuppression, and fatigue
• No severe acute hypertension or hypertensive crises were observed in patients during or immediately following drug administration
Incidence of All-grade TEAEs
Occurring in at Least 20% of
Patients
TEAE,
preferred term
All dosed (N=74)
n (%)
Nausea 53 (71.6)
Thrombocytopenia 49 (66.2)
Anemia 43 (58.1)
Leukopenia 41 (55.4)
Fatigue 41 (55.4)
Neutropenia 39 (52.7)
Vomiting 36 (48.6)
Dizziness 28 (37.8)
Dry mouth 28 (37.8)
Headache 21 (28.4)
Hypotension 18 (24.3)
Decreased appetite 17 (23.0)
Constipation 16 (21.6)
Diarrhea 16 (21.6)
Study Conclusions
• Study IB12B, the largest prospective clinical trial to date, has demonstrated multiple clinical benefits of AZEDRA® (iobenguane I 131) treatment– Control of catecholamine-associated hypertension and sustained
reduction of antihypertensive medications – Majority of patients experienced anti-tumor benefit, both primary
endpoint responders and non-responders– Greater clinical benefits in patients who received two therapeutic
doses
• The most common treatment-emergent adverse events were consistent with expected radiation-related risks of hematologic toxicities, nausea/vomiting, fatigue, and dizziness– Hematological toxicities resolved within 4-8 weeks and without the
need for stem cell transplantation– No severe hypertension, hypertensive crises or acute CV side effects
were observed
Other Therapies
• Clinical trials:
– Cabozantinib
– Hypoxia Inducible Factor Inhibitor
– Luthatera
– Immunotherapy
• Chemotherapy
Conclusions
• Patients with PPG may be prone to metabolic or tumor burden complications that may impact survival.
• Genomic, molecular studies, and clinical observations are very important to identify potential therapies and impulse trial development for this disease
• A brighter future for patients with MPP is at front!