Embed Size (px)
Citation preview

1
UNIVERSITY OF SIENA SCHOOL OF DENTAL MEDICINE PHD PROGRAM: “DENTAL MATERIALS AND CLINICAL APPLICATIONS” Ph D THESIS OF: Andrea Fabianelli TITLE: A STUDY INTO THE SIGNIFICANCE OF TRACING MICROLEAKAGE BY COLOR DIE INFILTRATION December 18th, 2004

2
Policlinico “le Scotte” Siena Italy Committee: Promoter Prof. Marco Ferrari Co-Promoter Prof. Carel L Davidson Prof. Piero Balleri Prof. Egidio Bertelli Prof. Franklin R Tay Prof. Manuel Toledano TITLE: A STUDY INTO THE SIGNIFICANCE OF TRACING MICROLEAKAGE BY COLOR DIE INFILTRATION CANDIDATE Andrea Fabianelli
December 18th, 2004
3
CONTENTS
Chapter 1 Page 4
Introduction
Chapter 2 Page 21
Efficacy of self-etching primer on sealing margins
of Class II restorations.
Chapter 3 Page 38
In vitro evaluation of wall-to-wall adaptation of self-adhesive resin
cement used for luting gold and ceramic inlays.
Chapter 4 Page 61
Sealing ability of packable resin composites in class II restorations.
Chapter 5 Page 78
Marginal integrity of ceramic inlays luted with a self-curing resin
system.
Chapter 6 Page 97
Influence of tissue characteristics at margins on leakage of Class II
indirect porcelain restorations.
Chapter 7 Page 127
A clinical trial of Empress II porcelain inlays luted to vital
abutments with the self-light-curing adhesive system Excite DSC
and MultiLink.
Chapter 8 Page 147 Leakage and SEM evaluation of in vitro Class V cavities restored
with diverse materials.
Chapter 9 Page 168 General Discussion
Chapter 10 Page 172 Summary and Conclusions
Chapter 11 Page 206 References
Acknowledgments Page 228
Curriculum Vitae Page 230 Publications and abstracts Page 231

4
Chapter 1
Introduction
One of the major requirements of a tooth restoration is protection of the
exposed dentin against bacteria and their toxins (Bränström M et al, 1978).
The interface between restoration and dental substrate is an area of clinical
concern that can result in secondary decay, marginal discoloration, and
pulpits (Bränström M & Vojinovic O; 1976) For that reason, perfect sealing
should be the plan of each clinical performance (Eakle WS & Ito RK, 1990).
In other words: leakage should be prevented.
However, due to inconsistent physical properties between tooth structure
and restorative materials, perfect adaptation is hard to be accomplished.
Clinically, absence of secure adaptation cannot always be detected.
Eventual hidden leakage is usually denoted by microleakage. Microleakage
may be defined as the clinically undetectable passage of bacteria, fluids,
molecules or ions between a cavity wall and the restorative material applied
to it (Kidd EAM, 1976).
One of the most desirable properties that an ideal restorative material should
have is a perfect and complete seal of the restoration’s margin. In fact the
absence of space between dental substrates and restorative materials can
prevent restoration failure and most of the current literature focuses on
elimination of leakage, which is one of the major factors determining the long
term success of restorations. Clinical experiences that are associated to
leakage are staining around the margins of restorations, post-operative
sensitivity, secondary caries, restoration failure, pulpal pathology or pulpal
death, partial or total loss of restoration (Eick JD & Welch FH,1986; Krejci I &
Lutz F,1991).

5
Marginal staining can lead to aesthetic breakdown and consequently to the
need to replace the restoration. The penetration of bacteria and the
presence of a gap can have as early consequence sensitivity when chewing
or when exposed to thermal stimuli. Then secondary decay may occur
(Moreira Jr G et al, 1999). It has to be emphasised that every plaque
retention site is a possible location for secondary decay (Cagidiaco MC et al,
1996). The multiplication of bacteria in the crevice around the filling is
facilitated as they can be acquired in a short time from the oral environment,
tooth surface or smear layer. Subsequently the bacteria and toxic products
are able to diffuse through dentinal troubles and cause pulpal inflammation
(Skogendal O & Erikensen HM,1976).
Fluids along the interface may create hydrolytic breakdown of adhesive resin
and collagen within hybrid layer thereby compromising the stability of resin-
dentin adhesive interface (Finger WJ et al, 1994).
Microleakage of a restoration may vary over time. Resin-based composites in
association with dental adhesives are believed to loose sealing ability over
time, permitting microleakage (Lundin SA & Noren JG, 1991).
On the other side, materials such as amalgam are believed to seal
restoration margins through formation of corrosion products over time (Ben-
Amar A et al, 1995).
Furthermore new marginal gaps may develop during the service life of
restoration due to thermally or mechanically induced stresses (Hakimeh S et
al, 2000).
In addition it has been demonstrated that modern dental adhesives have a
positive influence on preventing leakage that lasts only 6 months and
became in influent after one year of storage (Moore DS et al, 1995).
6
Causes for microleakage
Leakage is related to several factors, such as dimensional changes of
materials due to shrinkage of materials’ polymerisation, thermal contraction,
absorption of water, mechanical stress and also dimensional changes in
tooth structures (Staninec M et al, 1986).
The polymerisation shrinkage of a resin-based composite can create
contraction forces that may disrupt the bond to cavity walls, with marginal
failure and subsequent microleakage (Davidson CL et al, 1984). Modern
composites undergo volumetric contractions ranging between 2.6% to 4.8 %.
(Lösche GM, 1999) and even if modern dentin bonding agents exhibit bond
strengths to dentin higher than 20 MPa (Eick JD et al, 1997), exceeding then
the contraction stress generated by polymerisation stress (13-17 MPa), total
contraction forces may win the adhesive strength to substrates, leading to
open margins.
Also the shape of the cavity can challenge the adaptation: in fact the C-
factor of cavities is firmly related to occurrence of microleakage, especially if
filled with composite and dental adhesive (Davidson CL, 1986; Douvitsas G,
1991; Hakimeh S et al, 2000).
One of the weakest links of Class II composite restorations is leakage at the
gingival margin of proximal boxes. The latter is due to the absence of
enamel at gingival margins implying a less stable and uniform cementum-
dentin substrate for bonding (Carvalho RM et al, 1996). This is sustained by
Cagidiaco et al. who experimentally demonstrated the presence of an outer
layer, partially formed by cementum, of 150-200 microns located below the
cementum enamel junction, that does not allow micro retentions for adhesive
materials (Cagidiaco MC et al, 1995).
Also the orientation of dentinal tubules can negatively affect the quality of
hybridization and thus favor leakage in resin-based restorations placed in
deep inter-proximal boxes (Schubach P et al, 1997).

7
On the other hand it has also been reported that enamel micro-fractures
occurred along the margins in many restorations, immediately after
polymerization of resin composite bonded to etched enamel (Han L et al,
1990).
Furthermore the coefficient of thermal expansion of resin-based composites
differs substantially from that of tooth structure (Yazici AR et al, 2003).
The coefficient of thermal expansion of composite (25 to 60 ppm°C-1) is
several times larger than that of enamel (11,4 ppm°C-1) and dentin ( 8
ppm°C-1)(McCabe JF & Walls AW 1998).
This physical property is also appointed to be responsible of microleakage in
resin-based restorations (Feilzer AJ et al, 1988).
Last but not least, micro-movements of the restoration along the cavity walls
as a result of non-matching moduli of elasticity can contribute to failure of the
mechanical bond and following microleakage (Lundin SA & Noren JG, 1991).
Restricting microleakage
Given that we have to work with the available materials, many attempts to
reduce microleakage are performed by clinicians during restorative
procedures involving application of combinations of different materials, direct
or indirect techniques, different curing strategies etc.
Relying on curing techniques as a means to prevent leakage is controversial:
many authors claimed that incremental placement and curing can generate
less leakage (Cooley R & Barkmeirer W, 1991; Crim GA & Chapman KW,
1986) while other researchers found that both bulk and incremental
techniques have the same substantial leakage at the gingival margin (Coli P
& Brånnstrøm M, 1993; Affleck MS et al, 1999).
The use of a relatively thick layer of a viscous bonding agent, resilient lining
cements and low modulus restorative materials have been advocated to
absorb volumetric changes associated with polymerisation (Kemp-Scholte
CM & Davidson CL, 1990). In the line of applying flexible linings (Davidson
8
CL, 1994) it was in 1996 proposed to minimize polymerisation contraction of
resin-based composites by using flowable composites for restoring Class V
cavities. These restorative materials are micro-hybrid resins which are 60-
70% filled by weight with filler particles ranging in size from 0.7-1.0 micro-
meters. Such composites exhibit a substantially lower modulus of elasticity
that enables increased elastic deformation to flex and absorb polymerization
shrinkage stress (Unterbrink GL & Liebenberg WH, 1999). Moreover the
composition gives to this material a coefficient of thermal expansion similar
to that of tooth structures (Chuang SF et al, 2001).
Undeniably, this operative protocol is able to reduce microleakage, as
reported in literature (Leevailoj C et al, 2001) and reduce stress of 18-50 %
(Kemp-Sholte CM & Davidson CL,1990).
Still this technique could not completely prevent microleakage (Belli S et al,
2001).
Another approach to reduce leakage in Class II restorations is the adaptation
of a slow self curing composite on gingival margin located on cementum as
first step, and then the layering of a photo-cured hybrid composite. Indeed, it
could be demonstrated that light cured resins developed more
polymerisation stresses than chemical cure resins (FusayamaT,1992;
Davidson-Kaban SS et al, 1997).
Also this strategy does not seem to solve the problem completely (Van
Dijken J & Horsted P, 1998).
Another approach is to apply indirect restorations, where eventual bulk
polymerization shrinkage can partly be tackled. Still the luting cement has to
polymerize in situ and will put the seal of the margins at damage. Cement
layer thickness plays a role in stress development (Ausiello P et al, 2002).
To date it is almost impossible to obtain an indirect restoration that perfectly
fits the cavity.
Clinically acceptable margins in metallic restorations have been reported to
be 50 up to 70 microns (Löfstrom LH & Barakat MM, 1989), while for ceramic

9
restorations the gap ranges from 50 to 300 microns (Audenino G et al,
1999).
Certain indirect restorative techniques with soft alloys or gold foil direct
restorations may improve marginal adaptation by burnishing margins
towards dental tissues, thus reducing leakage.
Then there is the need to get a perfect seal with the use of a sealing/luting
agent: In case of wide space between inlays and cavities a thick layer of
viscous resin cements may be the optimum to get sealed margins (Hahn et
al, 2001).
Inlays adhesively luted with resin cements have a small volume of luting
composite that can reduce stress formation caused from polymerisation
shrinkage. (Lutz F et al, 1991), and showing less marginal micro-fracture on
enamel than direct restorations (Iida K et al, 2003), but on the other hand,
the narrower the luting space, the more is the stress occurs (Davidson CL &
De Gee AJ, 1984). In addition this stress is increased by an unfavourable C-
factor, very high in cavities prepared for inlays (Feilzer AJ et al, 1987).
Given the experience that prevention of gap formation is hardly to be
achieved, antibacterial effects of the restoration can be an important
additional safeguard, because the inactivation of bacteria means a direct
strategy to minimize the risk of secondary decay (Imazato S, 2003).
The composites as we have now at our disposition have little or no bacterio-
static or bactericidal effects against oral bacteria. Silica-based filler and resin
monomers such ad TEGDMA, Bis-GMA and UDMA are not antibacterial
against S. Mutans (Kawai K, 1988).
This lack of antibacterial properties means no inhibitory effect against plaque
accumulation that can occur in leakage sites. Indeed it has been
demonstrated that more bacteria accumulation is seen on composites when
compared with other restorative materials (Skjörland KKR, 1973). What is
more, a study demonstrated that composites even promote caries (Kawai K
& Tsuchitani Y, 2000).

10
Glass-ionomer cements exhibit a moderate anti-bacterial effect, in addition
to the presence of fluoride-releasing components that seem to prevent
premature demineralisation and thus protection against secondary caries
(Herrera M et al, 2000). The positive effect of zinc is still a neglected area in
dental literature. Furthermore fluoride releasing materials, such glass-
ionomer and silicate cements, can affect bacterial metabolism with different
mechanisms (Marquis RE, 1995).
In amalgam and other metallic restorations, the presence of metal ions such
as silver or copper can present antibacterial activity (Duguid R, 1983).
Mercury has a long story as an antimicrobial agent effective against
eukaryotic and prokaryotic organisms, even if the basis of this activity is not
well established (Dixit V et al, 2004). In leakage tests, fresh amalgam
restorations usually show total involvement of the cavity’s wall (McCurdy CR,
1974). However it is reported in previous studies that the initial poor seal of
fresh amalgams improves with aging due to the deposition of corrosion
products at the cavity-restoration interface. Indeed it is often reported that
patients only complain about eventual post-operative sensitivity during the
first week after placement, where after the pain disappears. Whether this
effect can be attributed to improved sealing is questionable as it has been
documented that up to 2 years may be required to reduce leakage almost
completely around amalgam restorations (Andrews JT et al, 1980).
It’s reported in literature that over time, water sorption can cause gap
reduction by hygroscopic expansion of resin-based composites (Thonemann
BM et al, 1997). It has to be stressed that it is not seem too realistic to rely
on this mechanism to solve the problem of leakage.
Measuring microleakage
Microleakage usually has been evaluated with in vitro models. A number of
techniques including bacteria-, chemical or radioactive tracer molecules
infiltration are available. Colour dye penetration studies are the most

11
employed tests. Since continuously many new materials are brought on the
market short time laboratory assessments are required because clinical
evaluations are expensive and time consuming and require ethical approval,
in vitro studies such as leakage tests can provide important information on
possible clinical performance of new restorative materials (Mota CS et al,
2003). These are methods of screening dental materials and determining the
eventual presence of microleakage, with the theoretical ability to transfer the
findings in vivo (Roulet JF, 1994).
Microleakage tests are very common in literature (Raskin et al, 2001), even
if these studies have given often contradictory results and were performed
in different procedures and without standardization. Nonetheless it is
reported that microleakage tests may be reliable parameters to predict in
vivo performance (Söderholm KLM, 1991).
Data based on the aetiology of decay lead to the conclusion that every site
of plaque retention has the possibility to be the location of secondary decay
(Olgart L et al, 1974; Cagidiaco MC et al, 1996). The problem with in vitro
studies is, amongst others, that the number of samples is limited to a few. In
literature one finds studies based on ten- twelve cavities for each group
(Hormati AA & Chan KC, 1980; Bauer JG & Henson JL, 1985). Statistical
analysis can only be based on the less powerful ones (Norman GR &
Streiner DL, 1999).
To some extend the oral environment can be mimicked by water storage and
thermo-cycling of the samples. The use of thermo-cycling as simulation of
clinical aging is quite common artificial aging technique. There are
disagreeing opinions about the influence of thermo-cycling on microleakage:
some authors report the absolute absence of any influence of thermo-cycling
on microleakage (Doerr CL et al, 1996), while others show increase of
microleakage at the cementum-dentin-restoration interface after thermal
stressing (Yap AUJ, 1997).
In these studies methylene blue was employed as tracer to evaluate the
degree of infiltration. The small particle size and the permeability of dentinal

12
tubules may lead to overestimate the relevance of this infiltration (Gale MS &
Darvell BW, 1999). The area of methylene blue is calculated to be around
0,52 nm2 , smaller than average bacteria. As bacteria have a diameter of
0,3-1,5 µm or larger, this technique cannot distinguish between too narrow
and sufficiently wide gaps to allow bacteria passage. An interesting finding
was that the use of methylene blue tracer leads to higher leakage scores
than other microscope evaluations (Almeida JB et al 2003). Few data are
available on crevice dimensions: Cooley and Barkmeier founded gaps of 10
microns around Vitrebond restorations (Cooley RL & Barkmeier WW, 1991).
The dwelling time of specimen in methylene blue seems to have no
influence on microleakage scores (Hilton TJ, 1998).
Often the evaluation of penetration scores is done on one or more cuts and
optical microscope observation. This evaluation method may be less
sensitive than three-dimensional evaluation (Gale MS et al, 1994), however
it is reported that also the use of several (eg. three) sections of one tooth
may avoid under-estimation of in vitro microleakage (Raskin A et al, 2003).
This mainly qualitative and to some extend quantitative method of evaluation
is a useful tool to show the pattern of dye penetration and can indicate
where the penetration occurs (Alani AH & Toh CG, 1997).
Based on above discussed measuring methodology it was concluded that
thus far no adhesive restorative technique is available that guarantees a
reliable marginal adaptation when margins are located in cementum-dentin
(Davidson CL & Feilzer AJ, 1997; Van Meerbeek B et al,1998).
Although the contribution of leakage to restoration failure remains
controversial (Camps J et al, 2000; Mior IA & Toffenetti F, 2000), leakage
studies are being carried out at most dental material laboratories.
So it was and is done at our facilities in order to obtain a preliminary idea
about one of the main qualities of a new material or combination of
materials: the potential to seal the cavity. However throughout the present
study, where next to only laboratory studies were carried out, also clinical
assessment of some of the materials was established, not seldom good

13
clinical performance was observed, whilst the in vitro leakage studies
predicted disappointing clinical results.
In the following chapters reports are presented of our initial experimental
findings, whilst in chapter 7 the meant discrepancy between the in vitro
methylene blue leakage findings and the in vivo appreciations will be
discussed. In addition to that some conclusions will be posed in chapter 9.

14
References
Affleck MS, Denehy GE, Vargas MA. Microleakage with incremental vs bulk
placement utilizing condensable composites. J Dent Res 1999; 78: 155.
Alani AH, Toh CG. Detection of microleakage around dental restorations: a
review. Op Dent 1997; 22: 173-185.
Almeida JB, Platt JA, Oshida Y, Moore BK, Cochran MA, Eckert GJ. Three
different methods to evaluate microleakage of packable composites in class
II restorations. Op Dent 2003; 28: 453-460.
Andrews JT, Hembree JH Jr. Marginal leakage of amalgam alloys with high
content of copper: a laboratory study. Oper Dent 1980; 5: 7-10.
Audenino G, Bresciano ME, Bassi F, Carossa S. In vitro evaluation of fit of
adhesively luted ceramic inlays. Int J Prosth 1999; 12: 342-347.
Ausiello P, Apicella A, Davidson CL. Effect of adhesive layer properties on
stress distribution in composite restorations--a 3D finite element analysis.
Dent Mater 2002 (18): 295-3003).
Bauer JG, Henson JL. Microleakage of direct filling materials in class V
restorations using thermal cycling. Quintessence Int 1985; 11: 765-769.
Belli S, Inokoshi S, Ozer F, Pereira PNR, Ogata M, Tagami J. The effect of
additional enamel etching and a flowable composite to the interfacial
integrity of class II adhesive composite restorations. Op Dent 2001; 26: 70-
75.
Ben-Amar A, Cardash HS, Judes H. The sealing of the tooth-amalgam
interface by corrosion products. J Oral Rehabil 1995; 22: 101-104.
Brännström M, Vojinovic O. Response of dental pulp to invasion of bacteria
round three filling materials. J Dent Child 1976; 43: 15-21.
Brännström M, Nordenvall KJ. Bacterial penetration, pulpal reaction and the
inner surface of enamel bond, composite fillings in etched and un etched
cavities. J Dent Res 1978; 57: 3-10.

15
Cagidiaco MC, Vichi A, Ferrari M. SEM evaluation of outside dentin-
cementum layer at cervical margins of Class II restorations. CED-IADR
Congress, Lubliana, September 1995.
Cagidiaco MC, Ferrari M, Garberoglio M. Dentin contamination protection
after mechanical preparation for veneering. Am J Dent 1996; 9: 57-60.
Camps J, Dejou J, Remusat M, About I. Factors influencing pulpal response
to cavity restoration. Dent Mat 2000; 16: 432-444.
Carvalho RM, Pereira JC, Yoshiyama M, Pashley DH. A review of
polymerisation contraction: the influence of stress development versus
stress relief. Op Dent 1996; 21(1): 17-24.
Chuang SF, Liu JK, Chao CC, Liao FP, Chen YH. Effect of flowable
composite lining and operator experience on microleakage and internal
voids in Class II composite restorations. J Prosthet Dent 2001; 85(2): 177-
183.
Coli P, Brannstrom M. The marginal adaptation of four different bonding
agents in Class II composite resin restorations applied in bulk or in two
increments. Quintessence Int 1993; 24: 583-591.
Cooley R, Barkmeirer W. Dental shear bond strength, microleakage and
contraction gap of visible light- polymerised liner/bases. Quintessence Int
1991; 22: 467-474.
Crim GA, Chapman KW. Effect of placement techniques on microleakage of
a dentin bonded composite resin. Quintessence Int 1986; 17: 21-24.
Davidson CL, De Gee AJ, Feilzer A. The competition between the composite
dentin bond strength and the polymerisation contraction stress. J Dent Res
1984; 63(12) :1396-1399.
Davidson CL, De Gee AJ,. Relaxation of polymerisation contraction stresses
by flown in dental composites. J Dent Res 1984; 63: 146-148.
Davidson CL. Resisting the curing contraction with adhesive composites. J
Prosthet Dent 1986; 55(4):446-447.

16
Davidson CL. Glass Ionomer Bases Under Posterior Composites. In: Glass
Ionomers: The Next Generation. Proc. of the 2nd Int. Symp. on Glass
Ionomers. Ed.: P.R. Hunt, Philadelphia PA, USA. June 1994; p. 175-179
Davidson CL, Feilzer AJ. Polymerisation shrinkage and polymerisation
shrinkage stress in polymer based restoratives. J Dent 1997; 25:435-440.
Davidson-Kaban SS; Davidson CL; Feilzer AJ; de Gee AJ; Erdilek N The
effect of curing light variations on bulk curing and wall-to-wall quality of two
types and various shades of resin composites. Dent Mater 1997; 13:344-52.
Dixit V, Bini E, Drozda M, Blum P. Mercury inactivates transcription and the
generalized transcription factor TFB in the archaeon Sulfolobus solfataricus.
Antimic Ag Chem 2004; 48 (6): 1993-1999.
Doerr CL, Hilton TJ, Hermesch CB. Effect of thermocycling on the
microleakage of conventional and resin modified glass ionomer. Am J Dent
1996; 9: 19-21.
Douvitsas G. Effect of cavity design on gap formation in Class II in
composite resin restorations. J Prosthet Dent 1991; 65: 475-479.
Duguid R. Copper-inhibition of the growth of oral streptococci and
actinomyces. Biomat 1983; 4(3):225-227.
Eakle WS, Ito RK. Effect of insertion technique on microleakage in mesio-
occlusodistal composite resin restoration. Quintessence Int 1990; 21: 369-
374.
Eick JD , Welch FH. Polymerisation shrinkage of posterior composite resins
and its possible influence on post operative sensitivity. Quintessence int
1986; 17 (2):103-111.
Eick JD, Gwinnett AJ, Pashley DH, Robinson SJ. Current concepts on
adhesion to dentin. Critical Reviews of Oral Biology and Medicine 1997;
8(3): 306-335.
Feilzer AJ, De Gee J, Davidson CL. Setting stress in composite resin in
relation to configuration of restoration. J Dent Res 1987; 66: 1636- 1639.
Feilzer AJ, de Gee AJ, Davidson CL. Curing contraction of composites and
glass-ionomer cements. J Prosthet Dent 1988; 59(3): 297-300.

17
Finger WJ, Inoue M, Asmussen E. Effect of wettability of adhesive resins on
bonding to dentin. Am J Dent 1994; 7: 35-38.
FusayamaT. Indicationfor self-cured and light-cured adhesive composite
resins. J Prosth Dent 1992; 67: 46-51.
Gale MS, Darvell BW, Cheung GSP. Three-dimensional reconstruction of
microleakage pattern using a sequential grinding technique. J Dent 1994;
22: 370-375.
Gale MS, Darvell BW. Thermal cycling procedures for laboratory testing of
dental restorations. J Dent 1999;27:105-108.
Hahn P, Attin T, Grofke M, Hellwig E. Influence of resin cement viscosity on
microleakage of ceramic inlays. Dent Mat 2001; 17: 191-196.
Hakimeh S, Vaidyanathan J, Houpt ML, Vaidyanathan TK, Von Hagen S.
Microleakage of compomer Class V restorations: effect of load cycling,
thermal cycling and cavity shape differences. J Prosthet Dent 2000; 83: 194-
203.
Han L, Okamoto A, Iwaku M. The effect of various clinical factors on
marginal enamel micro-cracks produced around composite restorations.
Dent Mat 1990; 11: 26-37.
Herrera M, Castillo A, Bravo M, Lièbana J, Carrion P. Antibacterial activity of
resin adhesive, glass ionomer and resin-modified glass ionomer cements
and a compomer in contact with dentin caries samples. Op Dent 2000; 25:
265-269.
Hilton TJ. Can modern restorative procedures and materials reliably seal
cavities? In vitro investigations. Dent Mat Transactions 1998; 12: 21-71.
Hormati AA, Chan KC. Marginal leakage of compacted gold, composite
resin, and high copper amalgam restorations. J Prosthet Dent 1980; 44 (4):
418-422.
Kawai K. Effect of eluate from composite resin on Gtase and growth of
Streptococcus Mutans. Jpn J Conserv Dent 1988; 31: 322-351.

18
Kawai K, Tsuchitani Y. Effects of resin composite components on
glucosyltransferase of cariogenic bacterium. J Biomed Mat Res 2000;51:
123-127.
Kemp-Sholte CM, Davidson CL. Marginal integrity related to bond strength
and strain capacity of composite resin restorative systems. J Prosthet Dent
1990; 64: 658-664.
Kidd EAM. Microleakage: a review. J Dent 1976; 4:199-205.
Krejci I, Lutz F. Marginal adaptation of class V restorations using different
restorative techniques. J Dent 1991; 19: 24-32.
Iida K, Inokoshi S, Kurosaki N. Interfacial gaps following ceramic inlay
cementation vs direct composites. Op Dent 2003; 28: 445-452.
Imazato S. Antibacterial properties of resin composites and bonding
systems. Dent Mat 2003; 19: 449-457.
Leevailoj C, Cochran MA, Matis BA, Moore BK, Platt JA. Microleakage of
posterior packable resin composites with and without flowable liners. Op
Dent 2001; 26(3): 302-307.
Löfstrom LH, Barakat MM. Scanning electron microscopic evaluation of
clinically cemented cast gold restorations. J Prosth Dent 1989;61:664-669
Lösche GM. Marginal adaptation of Class II composite fillings:guided
polymerisation vs reduced light intensity. J Adhes Dent 1999; 1(1): 31-39.
Lundin SA, Noren JG. Marginal leakage in occlusally loaded, etched, Class
II composite resin restorations. Acta Odontol Scand 1991; 49: 247-254.
Lutz F, Krejci I, Barbakow F. Quality and durability of marginal adaptation in
bonded composite restorations. Dent Mater 1991; 7: 107-113.
Marquis RE. Antimicrobial actions of fluoride for oral bacteria. Can J
Microbiol 1995; 41(11): 955-964.
McCabe JF, Walls AW. Properties used to characterize materials. Applied
Dental Materials. 8th ed Oxford: Blackwell Science; 1998: 4-28.
McCurdy CR. A comparison of in vivo and in vitro microleakage of dental
restorations. JADA 1974; 88(3):592-602.

19
Mior IA, Toffenetti F. Secondary caries:a literature review with case reports.
Quint Int 2000; 31: 165-179.
Moore DS, Johnson WW, Kaplan I. A comparison of amalgam microleakage
with a 4-META liner and copal varnish. Int J Prosthodont 1995; 8: 461-466.
Moreira Jr G, Sobrinho APR, Nicoli JR, Bambirra EA, Farinas LM, Carvalho
MAR, Vieira EC. Evaluation of microbial infiltration in restored cavities- an
alternative method. J End 1999; 25:605-608.
Mota CS, Demarco FF, Camacho GB, Powers JM. Microleakage in ceramic
inlays luted with different resin cements. J Adhes Dent 2003; 5: 63-70.
Norman GR, Streiner DL. PDQ statistics. BC Decker inc. Hamilton 1999.
Olgart L, Brännstöm M, Johnson G. Invasion of bacteria into dentinal
tubules: Experiments in vivo and in vitro.Acta Odontol Scand 1974; 32: 61-
70.
Raskin A D’Hoore W, Gonthier S, Degrange M, Dejou J. Reliability of in vitro
microleakage test: a literature review.J Adhesiv Dent 2001; 3: 295-308.
Raskin A, Tassery H, D’Hoore W, Gonthier S, Vreven J, Degrange M, Déjou
J. Influence of the number of section on reliability of in vitro microleakage
evaluations. Am J Dent 2003;16(3):207-210.
Roulet JF. Marginal integrity: clinical significance. J Dent 1994; 22: 9-12.
Schubach P, Krejci I, Lutz F. Dentin bonding: effect of tubule orientation on
hybrid layer formation. Eur J Oral Sci 1997:105: 344-352.
Skjörland KKR. Plaque accumulation on different dental filling materials.
Scand J Dent Res 1973; 81: 538-542.
Skogendal O, Erikensen HM. Effect of composite resin restorations in
monkey’s teeth with experimentally induced pulpitis. Scand J Dent Res
1976; 84(5): 297-303.
Söderholm KLM. Correlation of in vivo and in vitro performance of adhesive
restorative matherials. Dent Mater 1991; 7:74-83.
Staninec M, Mochizuki A, Tanizaki K, Jukuda K, Tsuchitani Y. Interfacial
space, marginal leakage and enamel cracks around composite resins. Op
Dent 1986; 11: 14-24.

20
Thonemann BM, Federlin M, Schmalz G. SEM analysis of marginal
expansionand gap formation in Class II composite restorations. Dent Mater
1997; 13: 192-197.
Unterbrink GL, Liebenberg WH. Flowable resin composites as filled
adhesives; literature review and clinical recommendations. Quintessence Int
1999; 30(4): 249-257.
Van Dijken J, Horsted P. Directed polymerisation shrinkage in Class II
cavities in vivo. J Dent Res 1998; 77: 1326.
Van Meerbeek B, Perdigao J, Lambrechts P,Vanherle G. The clinical
performances of adhesives. J Dent 1998; 26: 1-20.
Yap AUJ. Effects of storage, thermal and load cycling on a new reinforced
glass ionomer cement. J Oral Rehabil 1997; 25: 40-44.
Yazici AR, Baseren M, Dayangaç B. The effect of flowable resin composite
on microleakage in Class V cavities. Op Dent 2003; 28: 42-46.

21
Chapter 2
Efficacy of self-etching primer on sealing margins of Class II restorations.
ABSTRACT: Purpose: To evaluate sealing ability of different types of
restorative-adhesive combinations and to correlate etch patterns with
leakage scores. Materials and Methods: 56 molars were selected and
divided randomly in four groups of 14 specimens each. A standardized
adhesive Class II preparation with the cervical margin placed 1 mm below
the CEJ and an occlusal reduction of 2 mm was performed. No bevels were
utilized in the preparation. Four combinations of bonding system/restorative
material were tested. Group 1: Excite (EX) in combination with Tetric Ceram
(TC) as control; Group 2: Prompt-L-Pop (PP1) applied for 15 seconds in
combination with TC; Group 3: Etch and Prime 3.0 in combination with
Definite restorative material (EP); Group 4: Prompt-L-Pop (PP2) applied for
30 seconds in combination with TC. The bonding systems (Groups 1, 2 and
3) and all restorative materials were used following strictly manufacturers’
instructions. The resin composite was applied following an incremental
technique. Ten specimens of each group were processed for leakage test.
The specimens were sectioned with a diamond saw in three different areas
in mesial-distal direction. Two different operators evaluated the sections
blindly for scoring leakage at cervical and occlusal margins. The highest
score for the sections of each tooth area was selected for scoring and further
statistical analysis. The results of the staining measurements were
statistically evaluated using the Kruskal-Wallis non-parametric analysis of
variance with Bonferroni alpha protection. The level of statistical significance

22
was defined as P< 0.05. The remaining four specimens of each group were
kept in a 37% HCl solution for 48 hours to dissolve the dental structures and
to observe the resin replica of the cavities by SEM. Results: EX showed
less dye penetration at occlusal margins than the other three groups, while
no statistically significant differences were found at the dentin margin. The
SEM observations showed rougher and more uniform enamel etch pattern
when phosphoric acid (EX) was applied than that obtained with self-etching
adhesive systems. Resin tags and adhesive lateral branches were noted in
all groups at the dentin site.
Conclusions: The sealing ability of self-etching priming bonding systems at
the enamel margins was less effective than that obtained using phosphoric
acid bonding systems.

23
Introduction
Patients’ demand for tooth colored restorations rather than amalgam
restorations is increasing day by day (Federation Dentaire Internationale,
1995). Resin-based composite materials are the most common alternative to
amalgam. Resin-based composites have been used for many years but only
recently exhibit improved wear resistance (Hickel R et al, 2000). In fact, the
average annual wear of new composites seems to be equal to that of
amalgam (Roulet JF, 1997). One of the main problems of resin restorations
is microleakage (Eakle WS & Ito RK, 1990). Leakage can be due to the
polymerization shrinkage of resin material that creates a gap between cavity
walls and restoration (Tjan AH et al, 1992). It has become apparent that
even with the development of adhesives that can produce adhesion to dentin
comparable to the adhesion attainable to enamel, leakage cannot be
prevented routinely (Eakle WS & Ito RK, 1990; Tjan AH et al, 1992). Thus,
alterations in the bonding systems and resin-based composites must be
achieved to minimize the deleterious effects of polymerization shrinkage of
the resin material, gap formation and consequent leakage; this will ultimately
make the material easier to use and less sensitive to technical parameters.
Recently, dentin adhesives have been developed with hydrophilic groups
and high wettability: good results on sealing margins of Class II restorations
were achieved (Duncalf WV & Wilson NH, 2000). These newer adhesives
can penetrate into a chemically conditioned dentin and create a mechanical
interlocking based on the formation of a hybrid layer and resin tags
penetrating into opened dentin tubules (Tay FR et al, 1996; Sano H et al,
1998).
Past generations of traditional dental adhesives utilized three steps:
decalcification, infiltration and polymerisation. Acid etching dentin removes
the smear layer and demineralises slightly the underlying dentin, exposing
collagen fibrils. Optimal hybrid layer formation requires the diffusion of a
mixture of hydrophilic resin monomers into the exposed collagen fibrils until

24
undemineralized dentin subsurface is reached (Tay FR et al, 1996;
Nakabayashi N & Pashley DH, 1998).
However, clinical steps of bonding procedures might be technique-sensitive
and lead to ineffective bonding if the operator is not experienced (Sano H et
al, 1998; Peschke A et al, 2000).
In order to simplify handling properties, reduce working time and avoid the
collapse of collagen fibrils, self-etching primers were proposed (Watanabe I
et al, 1994). These bonding systems create a continuum between tooth and
resin by the simultaneous demineralisation and resin penetration of dentin
substrate with acidic molecules that can be polymerised in situ (Watanabe I
et al, 1994) .
This study evaluated the sealing ability of different self-etching adhesives,
correlated etch patterns with leakage scores, and tested the null hypothesis
that there is no difference in the ability of different adhesive systems to seal
Class II restorations.
Materials and Methods
Fifty-six posterior teeth were selected. The teeth were divided randomly in
four groups of 14 specimens each. Extracted human posterior teeth which
had been stored in 1% chloramine between 1-3 months were selected. A
standardized adhesive Class II preparation was made in the mesial and
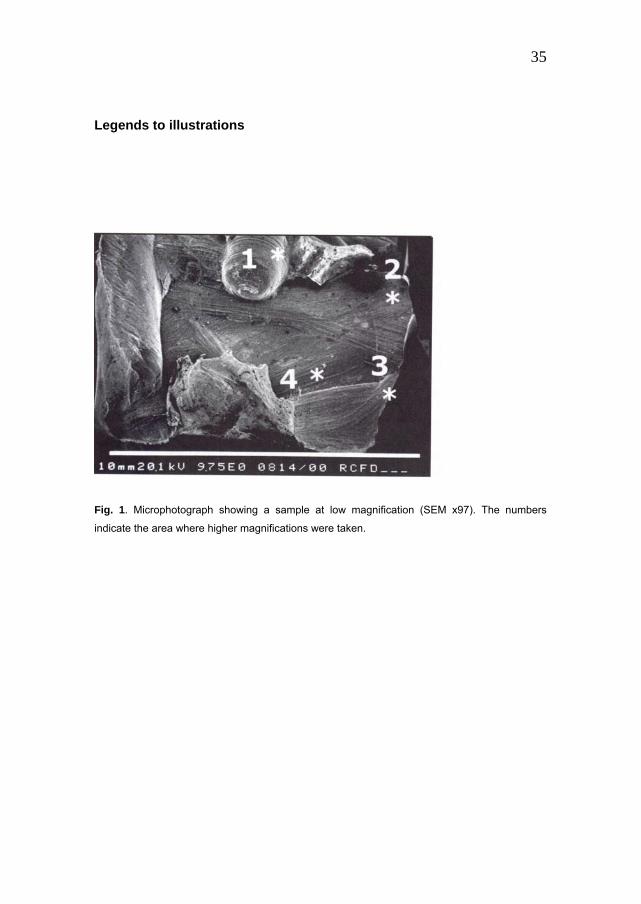
occlusal surface of each tooth (Fig. 1). The cervical margin of the
interproximal box was placed 1 mm below the cementum-enamel junction, in
cementum-dentin. The cavities had an occlusal reduction of 2 mm. The
bucco-lingual width of the proximal boxes was 4 mm, the occlusal width 3
mm and the depth of the pulpal and axial walls 2 mm. A tolerance of 0.3 mm
was used to include preparations in the test. A butt-joint margin preparation
was made at the cervical margin of all samples. The preparations were not
bevelled.

25
The dimensions of prepared cavities were measured with a Boley gauge.
Three combinations of bonding system and restorative material were tested
according to the manufacturer’s instructions, while a fourth group was used
by increasing the application time of one self-etching adhesive (Table 1).
Group 1: Excitea (EX) in combination with Tetric Cerama (TC) as control;
Group 2: Prompt-L-Pop self etching-priming adhesive systemb (PP1) in
combination with TC;
Group 3: Etch and Prime 3.0c in combination with Definitec restorative
material (EP);
Group 4: Prompt-L-Popb (PP2) in combination with TC. The application time
(etching step) was increased to 30 seconds instead of 15 seconds as
recommended by the manufacturer.
The bonding systems and restorative materials were used following
manufacturers’ instructions, except for Group 4. The composites were
applied using an incremental technique. Ten specimens of each group were
randomly selected and processed for the leakage test.
Leakage test After protecting apical foraminas and roots with nail varnish the specimens
were immersed in a dye solution (2% methylene blue) for 24 hours subjected
to 500 cycles of a thermal cycling test with a dwell time of 20 seconds
between 5°C and 55°C.
After the specimens were embedded in acrylic resin, they were sectioned
with a diamond saw (Isometd) in three different sites in a mesio-distal
direction (Fig. 2). The first section was positioned in the middle of the
restoration, while the two others were along the lingual and buccal proximal
walls along the interface between the restoration and the cavity wall.
The sections were evaluated blindly by two different operators for leakage
scores at cervical and occlusal margins and for the presence of voids and
porosities by a stereomicroscope. The highest score for the sections of each
tooth area was selected for scoring and statistical analysis. In case of

26
discrepancy between the two operators, the highest score was selected and
evaluated.
The depth of cervical staining was measured according to the following
parameters: 0= no penetration; 1= leakage not exceeding the middle of
gingival wall; 2= penetration exceeding the middle of gingival wall; 3=
penetration up to the axial wall; 4= penetration up to the axial cervical wall
or into dentin tubules. The extent of occlusal leakage was registered as
depth of dye penetration according to the following scores: 0= no
penetration; 1= leakage not deeper than the enamel-dentin junction; 2=
leakage deeper than the enamel-dentin junction; 3= leakage along the
occlusal and/or axial lateral walls. The results of the staining measurements
were statistically evaluated using the Kruskal-Wallis non-parametric ANOVA
with Bonferroni alpha protection. The level of statistical significance was
defined at P< 0.05.
The remaining four specimens of each group were kept 48 hours in a 37%
HCl solution to completely dissolve the dental structures and to observe the
resin replica of the cavities with a scanning electron microscopee (SEM).
After rinsing extensively with water, the specimens were gently air dried,
sputter-coated with goldf and observed with a SEM at different
magnifications, in order to evaluate the extent and the morphology of etched
dental substrates in three different enamel areas (occlusal, axial and close to
CEJ) and the resin tags formed (Fig. 3).
Results
Leakage test Excite (Group 1) revealed less dye penetration occlusally than the other
groups. Statistical analysis of the scores recorded at occlusal margins
showed significant differences among Group 1 and the other three groups.
In Group 1, 90% of the specimens showed a perfect seal occlusally (Table
2), while only 10-20% of specimens of Groups 2, 3 and 4 showed no

27
leakage. Statistical analysis of the scores recorded at cervical margins did
not show any statistical difference among the four groups (Table 3).
SEM observations
The SEM observation showed rougher and more uniform enamel etch
patterns when phosphoric acid was applied than when self-etching
adhesives were used. At the occlusal site, the enamel prisms were cut along
their long axis and samples etched with phosphoric acid (Group 1) showed a
deeper and more uniform etched pattern than the others groups (Figs. 4,5).
Similarly, the etched pattern at the axial site and close to CEJ was more
uniform and deeper in Group 1 than in the other groups (Figs. 6-9). Resin
tags and adhesive lateral branches were reported in all groups at the dentin
site (Figs. 10-13). The morphology of resin tags and adhesive lateral
branches was similar in all groups.
Discussion
The technique used in this study is a common procedure used for evaluating
sealing ability of bonding/resin composite restorations, allowing observation
of dye that penetrates into gaps between dental substrates and
restorations(Rigsby DF et al, 1990; Ferrari M et al, 1999).
A perfect seal is more difficult to achieve for axial margins(Hilton TJ et al,
1997; Hilton TJ & Ferracane JL, 1998). The sectioning procedure in this
study was selected also for evaluating the leakage at axial walls of cavities
and correlating leakage data with microscopic observations.
Self-etching adhesives which do not require rinsing and perform
simultaneously as primer and adhesive are a simplified approach to
adhesive techniques. The use of self-etching systems does not seem to
produce significant morphological changes in the enamel substrate, while
the dentin substrate was effectively treated by the tested materials.

28
Excitea (Group 1) showed less dye penetration at the occlusal margins than
the other three adhesives. When phosphoric acid in combination with Excitea
bonding system was used on cut enamel, the SEM observation of this area
showed rougher and more uniform etch pattern than that obtained withn self-
etching systems (Figs. 4-7).
The leakage score found at cervical margins is in accordance with others
(Thonemann B et al, 1999; Tung FF et al, 2000). Gap-free restorations are
possible to achieve only when margins of small Class II cavities were
located in enamel (Opdam NJM et al, 1998) and shrinkage stress is
counteracted by bonding to etched enamel (Ferrari M & Davidson CL, 1996).
A reason for the high percentage of leakage at the cervical margin noted in
this study might be the presence of an outer layer partially formed by
cementum of 150-200 µm at the cervical margins placed below the CEJ
(Cagidiaco MC et al, 1996). This outer layer is a hypo-mineralised hyper-
organic substrate that, even if etched, does not allow microretention for
adhesive material. Although the hybridisation of the cementum was
demonstrated (Ferrari M et al, 1997), the absence of resin tags in the first
150-200 µm from the cervical margins probably decreases the quality of the
bonding and the durability of adhesion at the cervical margin.
A recent workshop on posterior resin-based composites concluded that the
“quest continues for a more wear-resistant, biologically compatible, and
aesthetic restoration with no marginal leakage” (ADA Council on Scientific
Affairs, 1998). Also, further research in the areas of reducing polymerisation
shrinkage and contact wear, improving bonding and placement techniques,
and developing alternative matrix resins and polymerisation initiators were
encouraged.
Different types of sandwich techniques were evaluated and flowable
composites, glass-ionomer cements or compomer might be placed at the
cervical margin, as first layer of a Class II restoration in order to improve the
seal of the restorations (Ferrari M, 1999; Hilton TJ, 2002b). These materials
should act as stress absorbing layers, reducing the polymerisation

29
contraction stress (Ferrari M, 1999; Hilton TJ, 2002a). However, recent
studies( Labella R et al, 1999; Miguez PA et al, 2001) showed that placement
of a flowable resin-based composite as gingival increment in boxes results in
a moderate to severe leakage. Combinations of different materials and
layering procedures with self-etching systems are in progress in order to
evaluate if the sealing ability of Class II restorations can be improved
(Beznos C, 2001; Chuang SF et al, 2001) .
From this study the following conclusion can be drawn: when gingival
margins are placed below the CEJ, the tested material combinations
performed equally well, while adhesive systems including etching with
phosphoric acid sealed enamel margins significantly better than self-etching
primers and self-etching priming bonding agents.
The results of this study rejected the null hypothesis that was tested.
Different adhesive systems can affect the sealing ability of Class II
restorations.
a. Vivadent, Schaan, Liechtenstein.
b. 3M/ESPE, Seefeld, Germany.
c. Degussa, Hanau, Germany.
d. Buehler, Lake Bluff, IL, USA.
e. Philips Co, Eidhoven, The Netherlands.
f. Edwards Ltd, London, UK.

30
References
ADA Council on Scientific Affairs/ADA Council on Dental Benefit Programs.
Statement on posterior resin-based composites. J Am Dent Assoc 1998;
129: 1627-1628.
Beznos C. Microleakage at the cervical margin of composite Class II cavities
with different restorative techniques. Oper Dent 2001; 26: 60-69.
Cagidiaco MC, Vichi A, Ferrari M. SEM evaluation of outside dentin-
cementum layer at cervical margins of Class II restorations. J Dent Res
1996; 75: 1220 (Abstr 28).
Chuang SF, Liu JK, Jin YT. Microleakage and internal voids in Class II
composite restorations with flowable composite linings. Oper Dent 2001; 26:
193-200.
Duncalf WV, Wilson NH. A comparison of the marginal and internal
adaptation of amalgam and resin composite restorations in small to
moderate-sized Class II preparations of conventional design. Quintessence
Int 2000; 31: 347-352.
Eakle WS, Ito RK. Effects of insertion technique on microleakage in mesio-
occluso-distal composite resin restorations. Quintessence Int 1990; 21: 369-
374.
Federation Dentaire Internationale, World Health Organization, World Dental
Federation, Consensus statement on dental amalgam . FDI World 1995 : 9-
10.
Ferrari M, Davidson CL. Sealing performance of Scotchbond Multi-Purpose-
Z100 in class II restorations. Am J Dent 1996; 9: 145-149.
Ferrari M, Cagidiaco MC, Davidson CL. Resistance of cementum in Class II
and V cavities to penetration by an adhesive system. Dent Mater 1997; 13:
152-162.

31
Ferrari M. Advances in glass-ionomer cements. In: Davidson CL, Mjör IA.
Glass-ionomer cements. Berlin: Quintessence 1999: 137-148.
Ferrari M, Mason PN, Fabianelli A, et al. Influence of tissue characteristics at
margins on leakage of Class II indirect porcelain restorations. Am J Dent
1999; 12: 134-142.
Frankenberger R, Kramer N, Petschelt A. Technique sensitivity of dentin
bonding: Effect of application mistakes on bond strength and marginal
adaptation. Oper Dent 2001;4: 324-330.
Hickel R, Manhart J, García-Godoy F. Clinical results and new developments
of direct posterior restorations. Am J Dent 2000; 13: 41D-54D.
Hilton TJ, Schwartz RS, Ferracane JL. Microleakage of four Class II resin
composite insertion techniques at intraoral temperature. Quintessence Int
1997; 28: 135-144.
Hilton TJ, Ferracane JL. Cavity preparation factors and microleakage of
class II composite restorations filled at intraoral temperatures. Am J Dent
1998; 11: 123-130.
Hilton TJ. Can modern restorative procedures and materials reliably seal
cavities? In vitro investigations. Part 1.Am J Dent 2002;15:198-210.
Hilton TJ. Can modern restorative procedures and materials reliably seal
cavities? In vitro investigations. Part 2.Am J Dent 2002;15:279-289.
Kanca J. Resin bonding to wet substrate. I: Bonding to dentin. Quintessence
Int 1992; 23: 39-41.
Labella R, Lambrechts P, Van Meerbeek B, et al. Polymerization shrinkage
and elasticity of flowable composites and filled adhesives. Dent Mat 1999;
15: 128-137.
Miguez PA, Pereira PNR, Suh IB et al. Gap formation and bond strength of
composites lined with flowable resin. J Dent Res 2001; 80 (Sp. Issue abstr.
n. 1270)194.
Nakabayashi N, Pashley DH. Hybridization of hard dental tissues. Berlin:
Quintessence, 1998; 20-30.

32
Opdam NJM, Roeters JJM, Burgersdijk RCW. Microleakage of Class II box-
type composite restorations. Am J Dent 1998; 11: 160-164.
Peschke A, Blunck U, Roulet JF. Influence of incorrect application of a
water-based adhesive system on the marginal adaptation of Class V
restorations. Am J Dent 2000; 13:239-243.
Rigsby DF, Retief DH, Russell CM, et al. Marginal leakage and marginal gap
dimension of three dentinal bonding system. Am J Dent 1990; 3: 289-294.
Roulet JF. Benefits and disadvantages of tooth-colored alternatives to
amalgama. J Dent 1997; 25: 459-473.
Sano H, Kanemura N, Burrow MF, et al. Effect of operator variability on
dentin adhesion: Students vs. dentists. Dent Mater 1998; 17: 51-58.
Tay FR, Gwinnett AJ, Wei SH. Micromorphological spectrum from overdrying
to overwetting acid-conditioned dentin in water-free, acetone based, single
bottle primer/adhesives. Dent Mater 1996; 12: 236-244.
Thonemann B, Federlin M, Shmalz G, et al. Total bonding vs selective
bonding: adaptation of Class 2 composite restoration. Oper Dent 1999; 24:
261-271.
Tjan AH, Bergh BH, Lidner C. Effect of various incremental techniques on
the marginal adaptation of class II restoration. J Prosthet Dent 1992; 67: 62-
66.
Tung FF, Estafan D, Scherer W. Microleakage of a condensable resin
composite: An in vitro investigation. Quintessence Int 2000; 31: 430-434.
Watanabe I, Nakabayashi N, Pashley DH. Bonding to ground dentin by a
phenyl-P self-etching primer. J Dent Res 1994; 73: 1212-1220.

33
Table 1. Bonding procedures. ______________________________________________________________________________________________
______
Group Bonding system Clinical steps ______________________________________________________________________________________________
______
1 Excite a,b,e,f
2 Prompt-L-Pop c,e,f
3 Etch and Prime 3.0 c,d,e,f*
4 Prompt-L-Pop - applied
for 30 seconds c,e,f ______________________________________________________________________________________________
______
a. Dentin and enamel conditioning with phosphoric acid
b. Primer-adhesive application
c. Self-etching primer application
d. Bonding application
e. Air blowing
f. Light curing

34
Table 2. Leakage scores recorded at occlusal margin. ______________________________________________________________________________________________
______
0 1 2 3 4 ______________________________________________________________________________________________
______
Group 1a 9 1 0 0 0
Group 2b 2 2 3 3 0
Group 3b 1 1 2 1 5
Group 4b 2 3 2 2 1 ______________________________________________________________________________________________
______
Groups with the same letter did not show any statistical significant
difference.
Table 3. Leakage scores recorded at cervical margin. ______________________________________________________________________________________________
______
0 1 2 3 4 ______________________________________________________________________________________________
______
Group 1a 5 1 3 1 0
Group 2 a 6 2 1 0 1
Group 3 a 7 1 0 0 2
Group 4 a 7 1 1 0 1 ______________________________________________________________________________________________
______
Groups with the same letter did not show any statistical significant
difference.
35
Legends to illustrations
Fig. 1. Microphotograph showing a sample at low magnification (SEM x97). The numbers
indicate the area where higher magnifications were taken.

36
Fig. 2. A microphotograph showing the etched pattern at occlusal enamel (area 1 of Fig. 3). The
sample was treated with phosphoric acid (Group 1). The prisms are cut parallely to prisms’
direction and the etch pattern is uniform and deep (SEM x1010).
Fig. 3. Microphotograph showing the etched pattern at axial-occlusal enamel (area 1 of Fig. 3)
of Group 1 sample. The prisms are mainly cut obliquely and the etch pattern is uniform and
rough (SEM x1010).
Figs. 4,5. Microphotographs showing the etched pattern at cervical enamel (area 1 of Fig. 3).
The sample was treated with phosphoric acid (Group 1). The prisms are cut in the less
favourable direction: obliquely (6.) or mainly parallel to their long axis (7.). The etch pattern is
less deep than those observed in Figs. 4 and 5, but rougher and deeper than those noted in
Figs. 7-9 (Groups 2-4) (SEM x1010).
37
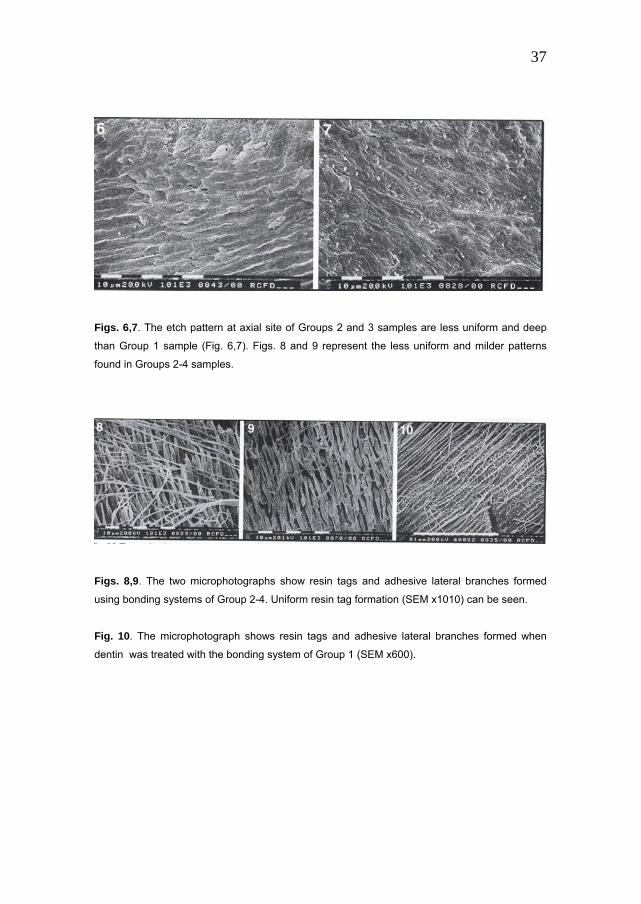
Figs. 6,7. The etch pattern at axial site of Groups 2 and 3 samples are less uniform and deep
than Group 1 sample (Fig. 6,7). Figs. 8 and 9 represent the less uniform and milder patterns
found in Groups 2-4 samples.
Figs. 8,9. The two microphotographs show resin tags and adhesive lateral branches formed
using bonding systems of Group 2-4. Uniform resin tag formation (SEM x1010) can be seen.
Fig. 10. The microphotograph shows resin tags and adhesive lateral branches formed when
dentin was treated with the bonding system of Group 1 (SEM x600).

38
Chapter 3
In vitro evaluation of wall-to-wall adaptation of self-adhesive resin cement used for luting gold and ceramic inlays.
Abstract: Purpose: This in vitro study evaluated the wall-to-wall adaptation
of a new self-adhesive resin-based cement (RelyX Unicem), in comparison
with that of other cements when luting gold and porcelain inlays in
standardized Class II cavities in extracted teeth. Materials and Methods: In
each experimental Group (n=10) a different combination of inlay and luting
material was tested. Group 1: Porcelain Empress II (EII) and RelyX Unicem
(U); Group 2: EII and resin-based cement Variolink II in combination with
primer and bonding Excite DSC; Group 3: Gold inlays (G) and U; Group 4: G
and Harvard zinc-oxy-phosphate cement; Group 4: G and glass-ionomer
cement Fuji Cem. After storage and thermo-cycling, microleakage test was
carried out and dye penetration scoring was performed at the occlusal and
cervical margins of each inlay. The differences in microleakage score were
tested for statistical significance first comparing all Groups, then pooling
together the Groups for inlay material (Kruskal-Wallis Non-Parametric
ANOVA and Mann-Whitney U test, p<0.05). SEM observations of the tooth-
cement-restoration interfaces were also performed in each Group. Results:
Harvard cement had the highest microleakage. The sealing ability exhibited
by RelyX Unicem was satisfactory with both gold and porcelain inlays, and
comparable respectively to that of Fuji Cem and Variolink II. Conclusion:
RelyX Unicem achieved an adequate seal on both enamel and dentin when
used to lute in vitro gold and porcelain inlays.

39
Introduction Notwithstanding the great popularity of resin-based composite restorations
some serious shortcomings of these materials have to be reckoned with.
Disadvantages of the material are polymerization shrinkage, limited color
stability and limited strength, eventually leading to leakage, decreasing
esthetics and premature fracture under stress (Mjör IA, 1992). These
undesirable deficiencies are less likely to occur with indirect porcelain or
gold restorations, which therefore are to be preferred above all for large
restorations, particularly when cuspal coverage is required. A weak link with
indirect restorations is eventual debonding of the luting cement. Moreover,
for the weaker sorts of porcelain, the lute has to guarantee a strong and
reliable bond between the tooth structure and the inlay (Davidson CL, 2001).
Ceramic inlays gain in mechanical characteristics if luted with resin cements
in combination with hydrofluoric acid and silane treatment as introduced by
Horn (Horn , 1983). Adhesives have the potential of eliminating surface flaws
(Sindel J et al,1999; Van Noort R, 2002). Besides luting material and
technique, also substrate conditions represent a critical factor in the quality
of a durable wall-to-wall integrity. As a result of its morphologic variability,
the properties of the organic component, and the changing conditions of
humidity, dentin is the least predictable and undependable substrate for
bonding (Pashley DH et al, 1997; Griffiths BM et al, 1999). To promote
proper adaptation to moist dentin, hydrophilic bi-functional monomers like
HEMA are incorporated in the adhesive (Inoue S et al, 2000). Several
materials are available for luting inlays. Among resin cements, a self-cure,
light-cure or dual-cure material can be chosen, and a simple, quick, and
straightforward handling of the material is usually the practitioner’s desire. In
line with the common trend toward “simplified” application techniques, a new
self-adhesive, single-step universal resin cement, RelyX Unicem (3M ESPE,
Seefeld, Germany)., has recently been introduced The purpose of this study
was to evaluate the wall-to-wall adaptation expressed in sealing ability of

40
RelyX Unicem when used for luting gold and porcelain inlays, in comparison
with cements that have traditionally been used for this purpose. The quality
of the marginal seal achieved with the materials on trial was assessed in
vitro through a microleakage test and scanning electron microscopic
observations of the tooth-cement-restoration interfaces after thermo-cycling.
Materials and Methods
Fifty extracted sound molars were collected for the study. The selected teeth
were hand-scaled, cleaned with slurry of pumice, and stored in distilled
water at room temperature until use in the experiment. The samples were
randomly divided into five Groups of ten specimens each. In each Group a
different combination of inlay and luting material was tested. Standardized
mesio-occlusal Class II cavities were prepared under copious water spray,
with diamond burs in a high-speed handpiece (Fig. 1). On the occlusal
surface of the teeth, the preparation was 3 mm wide bucco-lingually and 2
mm deep. The proximal box of the cavity had a bucco-lingual width of 4mm
and a depth of 2 mm; also the pulpal wall was 2 mm, and the cervical
margins were placed 1mm below the cementum-enamel junction. The
dimensions of the prepared cavities were checked with a Boley gauge. A
±0.3 mm tolerance in the measurements was considered acceptable for
including the specimen in the trial. Butt margins were created in cavities
meant to receive porcelain inlays (Groups 1 and 2), whereas on the teeth to
be restored with gold inlays (Groups 3-5), a 0.5 mm bevel was added at the
preparation margins. Impressions were then taken with a polyether
impression material (Impregum, 3M ESPE, Seefeld, Germany) and sent to
the laboratory. After impression taking the specimens were stored in distilled
water.
In Group 1, Empress II (Ivoclar-Vivadent, Schaan, Liechtenstein) inlays were
cemented with resin-based cement RelyX Unicem (3M ESPE, Seefeld,
Germany). In Group 2 Empress II inlays were cemented with resin-based

41
cement Excite DSC (Ivoclar-Vivadent, Schaan, Liechtenstein) in combination
with bonding system Variolink II (Ivoclar-Vivadent, Schaan, Liechtenstein)
after acid-etching for 20’’and water spray. In Groups 3 through 5 gold inlays
were cemented respectively with RelyX Unicem, Harvard zinc-oxy-
phosphate cement (De Trey, Dentsply, Konstanz, Germany), and glass-
ionomer cement Fuji Cem (GC, Tokyo, Japan). Each luting material was
handled strictly following manufacturer’s instructions (Table I). The inner
surfaces of ceramic inlays were etched with hydrofluoric acid 9,6 %
(Ultradent, South Jordan, UT), rinsed and silanated with Monobond S
(Ivoclar-Vivadent, Schaan, Liechtenstein). Inner surfaces of gold inlay were
only cleaned with gentle sandblasting.
Microleakage evaluation Once the restorations were completed, the specimens’ roots were coated
with two layers of nail varnish up to 2 mm from the cervical margin of the
restoration. After a 24-hour immersion in a 2% methylene blue solution and
submitted to 500 thermo-cyclings, each with a dwell time of 20 s. at 5 and 55 oC. Subsequently, each tooth was embedded in acrylic resin and sectioned
longitudinally with a low-speed diamond saw (Leitz 1600, Munich, Germany)
at three different levels in the mesio-distal direction (Fig. 2). The first cut was
positioned in the middle of the restoration, and the other ones along the
lingual and buccal lateral walls, approximately at the interface between the
restoration and the cavity wall.
The degree of occlusal leakage was quantified according to the following
parameters: 0 = no penetration; 1 = leakage no deeper than the enamel-
dentin junction; 2 = leakage deeper than the enamel-dentin junction; 3 =
leakage along the occlusal and/or axial lateral walls; 4 = leakage into
dentinal tubules (Fig. 3a). Dye penetration at the cervical margin of the
cavity was quantified according to the following score method: 0 = no
penetration; 1 = leakage not exceeding the middle of the cervical wall; 2 =
penetration past the middle of the cervical wall; 3 = penetration to the axial

42
wall; 4 = penetration to and along the axial wall and into the dentinal tubules
(Fig. 3b).
Two operators observed the sections separately by means of an optical
microscope at 20 magnifications (Bausch&Lomb, Rochester, NY, USA). In
case of a disagreement between the two investigators on the score assigned
to a certain specimen, the worst (higher) score was chosen for the statistical
analysis.
Statistical analysis The results of the staining measurements were statistically evaluated using
Kruskal-Wallis Non-Parametric ANOVA by ranks with Bonferroni alpha
protection. The Tukey test was applied for multiple comparisons. All of the
statistical tests were run by the Winks 4.62 software (Texasoft, Cedar Hill,
Texas, USA), setting the level of significance at p<0.05.
SEM evaluation After scoring the specimens for dye penetration, in each Group one section
per tooth was chosen at random to be observed with the scanning electron
microscope (Philips 515, Philips, Eindhoven, Netherlands). The purpose of
the SEM analysis was to assess the integrity and continuity of the tooth-
cement-restoration interfaces, as well as to visualize the structural uniformity
of the cement layer. Specimen preparation for SEM involved a gentle
decalcification with a 37% phosphoric acid solution for 10 s., followed by de-
proteinization with a 2% sodium hypochlorite solution for 1 min. Finally, the
specimens were mounted on an aluminum stub with a colloid silver paint,
and sputter coated with gold-palladium (Edward’s Coater S105B, London,
England).

43
Results Leakage observations Frequency of recording and median value of the microleakage scores for the
different combinations of inlay and luting materials are given in Table III. The
mean ranks of the microleakage scores for each Group are plotted in
Graph1.
When comparing all of the combinations on trial (Graph 1), it appeared that
the Harvard zinc phosphate cement had the worst microleakage score. In
general, RelyX Unicem and Fuji Cem gave a better seal than Variolink II and
Harvard.
The difference in microleakage between Harvard and RelyX Unicem in gold
inlays was statistically significant (p<0.001). Also the difference between
Harvard at the cervical margin and Fuji Cem at the occlusal margin was
statistically significant (p<0.001, Graph 2).
In the comparison among the materials used to lute Empress II inlays
(Graph 2), it is evident that RelyX Unicem performed better than Variolink II
at both the occlusal and the cervical margin. However, the difference was
statistically significant only between occlusal margin with RelyX Unicem and
cervical margin with Variolink II (p=0.03).
As regards using Unicem with Gold or Empress inlays, the results were not
significantly different (p>0.05) at the occlusal as well as at the cervical
margin (Graphs 1-3).
Microscopic observations As expected, the typical features of adhesion, such as the formation of a
hybrid layer at the interface between luting material and dental substrate,
were absent from the SEM views of specimens cemented with Harvard (Fig.
4a). On the other hand, a good adaptation between cement and dental
substrate was visible in the specimens luted with Fuji Cem (Fig. 4b). Also

44
RelyX Unicem was able to establish a good coupling with the dental
substrate. However, voids were often visible within the cement layer (Fig.
4c). In any case, the quality of the seal created by the self-adhesive resin
cement was comparable to that achieved following a standard adhesive
procedure in inlays luted with Variolink II. This appeared from the SEM
observation of specimens restored with porcelain inlays (Fig. 5 a,b).
Discussion Literature is scarce on gold inlay leakage studies. Long-lasting clinical
service is in general expected from gold restorations (Smales RJ &
Hawthorne WS et al, 1996). The fact that these restorations are usually
realized in selective and compliant patients, with a good motivation for oral
hygiene may have an influence on the results of a clinical trial (Mjör IA,
1992). For many years, zinc-oxy-phosphate cements have been the favorite
lute to cement gold inlays and evidence has been presented of the
satisfactory long performance of such restorations (Mjör IA, 1992; Yamashita
J et al, 2000). Once again, factors such as patient selection, oral hygiene,
dimensional matching of the materials involved are likely to play a role in
determining the clinical success of these restorations. Despite this,
restorations luted with this material exhibited in the present study a high
degree of microleakage (Graphs 1, 2). A tentative explanation might be the
generally accepted absence of adhesion. Although the hardening of oxy-
phosphate cements is preceded by the etching action of the cements’ liquid,
no evidence could be found of a form of hybridization at the interface. Grip of
oxy-phosphate cements is merely based on macro-retention and the cements’ excellent dimensional stability (De Gee, A.J, 2004). Inlays luted
with adhesive techniques showed better sealing ability in the laboratory. In
vivo however, these restorations have sometimes failed to produce
satisfactory results, especially when margins were located below the
cementum-enamel junction (Özturk N, & Aykent F, 2003). Some aspects of

45
the luting procedure with resin cements need to be considered. On one
hand, a thin layer of cement would be desirable in order to reduce the stress
generated by the material on curing whilst on the other hand, the smaller the
space available for the polymerizing cement, the higher the stress developed
(Davidson CL, 2001). Accuracy of fit (thicker cement layers) might be less
with ceramic than with gold inlays. Low viscosity of the lute is a prerequisite
for proper seating, thus favoring the achievement of a good marginal seal
(Hahn P et al, 2001). All cements employed in this study showed
comparable, satisfactory flow characteristics with both gold and Empress
inlays. Even with adequate wetting and flow characteristics, it has to be
emphasized that luting with an adhesive techniques is an operator-sensitive
procedure because extreme care has to be given to the condition of the
substrates. With respect to the latter, new resin cements have been
introduced to satisfy the demand for an easy-handling, “user-friendly”
material. Rely-X Unicem is a self-etch, dual-curable resin composite cement,
designed for cementation of crowns, inlays, and fiber posts luting. As a result
of new chemistry (Table III), it is claimed by the manufacturer that this
cement does not require any substrate pretreatment or adhesive application.
As far as the materials’ bond strength is concerned, the data so far collected
are not consistent. In some studies acceptable levels of bond strength have
been reported on both dental substrates (Hecht R et al, 2002) and
restorative materials (Piwowarczyk A et al, 2002). However, these findings
are not confirmed by the results of micro-tensile tests measuring the bond
strength of RelyX Unicem on enamel and dentin (Goracci C et al, 2003).
Strength might be a determining factor in preservation of the sealing ability.
In this part of the study, no mechanical fatiguing of the samples was
considered and thus physical factors other than adaptation and dimensional
stability during thermo-cycling can be used to clarify different sealing ability
of the various luting cements. The fact that Rely-X Unicem is a hydrophilic
resin system, might explain the relatively good sealing. Hydrophilicity will
allow water uptake after setting, which may account for swelling of the

46
material. This seems a positive feature, but it has to be realized that at the
same time, water uptake can accelerate premature degradation of the
cement (El Zohairy AA et al, 2004).
The present microscopic study revealed, as in previous investigations
(Goracci C et al, 2003), that RelyX Unicem is capable of a noticeable
coupling with the dental substrate. However, the formed hybrid layer was
fairly thin. This may explain for the asymmetry between effective sealing
ability and relatively poor bonding potential of this new material. Also, voids
within the cement layer (Fig. 4c) have regularly been observed. These
porosities may result from incomplete mixing of powder and liquid during
vibrating a capsule that contains the two components.
In conclusion, RelyX Unicem showed improved sealing properties to both
enamel and dentin, when used for luting gold and porcelain inlays. With gold
inlays, this resin cement performed significantly better than the zinc
phosphate and comparably to the glass-ionomer cement. In specimens
restored with porcelain inlays, no statistically significant differences in micro-
leakage were found when the restorations were cemented with the new self-
adhesive resin cement, as compared with a standard adhesive procedure
(Excite DSC and Variolink II). Over other adhesive cements, the latter
material offers the advantage of easy handling and, by consequence, of a
reduction in chair-time. The real value of the new cement, both in quality of
persisting adhesion and sealing as well as true reduction of chair time still
has to be established in long-term fatigue studies and clinical trials. Such
studies are under way.
Moreover, the meaning of leakage in restorative dentistry has to be
(re)considered. Laboratory studies seldom show perfect sealing, whilst the
majority of restorations are functioning in an apparently acceptable way. For
sure, leakage should be minimized to prevent post-operative sensitivity and
eventual recurrent caries, but “one leakage is not necessarily the other
leakage”. Here the chemical composition of the luting material may play a

47
significant role e.g. in defending bacteria. In this respect, release of metal
ions and fluorides will play an important role that deserves intensive study.

48
References Davidson CL. Luting Cement, the Stronghold or the Weak Link in Ceramic
Restorations. Advanced Engineering Materials 2001, 3, 10: 763-767).
De Gee, A.J. personal communications, 2004).
El Mowafi OM, Benmergui C, Levinton C. Meta- analysis on long-term
clinical performance of posterior composite restorations. J Dent 1994; 22:
33-43.
El Zohairy AA, De Gee AJ, Hassan FM, Feilzer AJ. The effect of adhesives
with various degrees of hydrophilicity on resin ceramic bond durability. Dent
Mater, 2004 in press.
Feilzer AJ, De Gee AJ, Davidson CL. Increased wall-to wall curing
contraction in thin bonded resin layers. J Dent Res 1989 ; 68 : 48-50.
Ferrari M, Mason PN, Fabianelli A, Cagidiaco MC, Kugel G, Davidson CL.
Influence of tissue characteristics at margins on leakage of class II in direct
porcelain restorations. Am J Dent 1999; 12: 134-142.
Goracci C, Ferrari M, Grandini S, Monticelli F, Tay FR. Bonding of a self-
adhesive resin cement to dental hard tissues. J Adhes Dent 2003 (in press).
Griffiths BM, Watson TF, Sherriff M. The influence of dentine bonding
systems and their handling characteristics on the morphology and micro
permeability of the dentine-adhesive interface. J Dent 1999; 27: 63-71.
Hahn P, Attin T, Grofke M, Hellwig E. Influence of resin cement viscosity on
microleakage of ceramic inlays.Dent Mater 2001; 17: 191-196.
Hecht R, Ludstek M, Raia G. Tensile bond strength of first self adhesive
resin based dental material. J Dent Res 2002; 81: A-75.
Hickel R,. Manhart J. Longevity of dental restorations in posterior teeth and
reasons for failure. J Adhesive Dent 2001; 3:45-64.
Horn HR. Porcelain laminate veneers bonded to etched enamel.
Dent Clin North Am. 1983 Oct;27(4):671-84.

49
Inoue S, Van Meerbeek B, Vargas M, Yoshig’da Y, Lambrechts P, Vanherle
G. Advanced adhesive dentistry, 3rd Int Kuraray Symposium, Como, Italy
2000.
Lutz F, Krejici I, Barbakow F. Quality and durability of marginal adaptation in
bonded composite restorations. Dent Mater 1991; 7: 107-113.
Mjör IA. Long term cost of restorative therapy using different materials.
Scand J Dent Res 1992; 100: 60-65.
Özturk N, Aykent F. Dentin bond strengths of two ceramic inlay systems
after cementation with three different techniques and one bonding system. J
Prosthet dent 2003; 89: 275-281.
Pashley DH, Sano H, Ciucchi B, Yoshiyama M, Carvalho RM. Adhesion
testing of dentin bonding agents: a review. Dent Mater 1995; 11: 117-125.
Piwowarczyk A, Berge HX, Lauer H-Ch, Soresen JA. Shear bond strength of
cements at zirconium and lithium di-silicate ceramics. J Dent Res 2002; 81:
A-401.
Roulet JF Benefits and disadvantages of tooth-colored alternatives to
amalgam. J Dent 1997; 25:459-473.
Sindel J, Frankenberger R, Kramer N, Petschelt A. Crack formation of all
ceramic crowns dependent on different core build-up and luting materials. J
Dent 1999; 27: 175)
Sjögren G, Molin M, van Dijken JWV. A 5-year clinical evaluation of ceramic
inlays cemented with dual-cured or chemically cured resin composite luting
agent. Acta Odontol Scand 1998; 56: 263-267.
Smales RJ, Hawthorne WS. Long-term survival and cost-effectiveness of
five dental restorative materials used in various classes of cavity
preparations. Int Dent J 1996; 46: 126-130.
Van Meerbeek B. Perdigao J, Lambrechts P, Vanherle G. The clinical
performance of adhesives. J Dent 1998; 26: 1-20.
Van Noort R. Introduction to dental materials. Mosby pub 2002: 267)

50
Yamashita J, Takakuda K, Shiozawa I, Nagasawa M, Miyairi H. Fatigue
behavior of the zinc-phosphate cement layer. Int J Prosthodont 2000; 13:
321-326.

51
Legends to illustrations
Fig.1. The standardized Class II cavity prepared for the inlay restoration
Fig. 2. After immersion in a dye solution, each tooth was embedded in acrylic resin and
longitudinally sectioned at three different levels in the mesio-distal direction.

52
Fig. 3a
Fig 3 b
Fig. 3 (a) Dye penetration scores at the occlusal margin. (b) Dye penetration scores at the
cervical margin.

53
Fig. 4a
Fig. 4b

54
Fig. 4c
Fig. 4. SEM images of the tooth-cement-restoration interfaces in gold inlays (D=dentin,
C=cement, G=gold): (a) In specimens luted with Harvard cement, no sign of adhesion could be
detected (X231, bar 0.1 mm). (b) Fuji Cem showed a good adaptation on the dental substrate
(X1620, bar 10 micron). (c) A good coupling was visible also between RelyX Unicem and the
dental substrate. However, voids were often present within the cement layer (X186, bar 0.1
mm).

55
Fig. 5a
Fig. 5b
Fig. 5 SEM images of the tooth-cement-restoration interfaces in porcelain inlays (D=dentin,
C=cement, P=porcelain). The quality of the seal created by the self-adhesive resin cement
RelyX Unicem (a, X710, bar 0.1 mm) was comparable to that achieved following a standard
adhesive procedure in inlays luted with Variolink II (b, X372, bar 0.1 mm).

56
Table I: handling of the luting materials
Preparation of the substrate Material
conditionin
g
priming bondin
g
Handling of the luting material
RelyX
Unicem
Batch
143250
Mix powder and liquid in a
vibrator; light-cure for 20
seconds
Variolink II
Batch
558952bn
37% H3PO4
20’’
+
water rinse
Excite
Mix paste A and paste B; light-
cure for 20 seconds
Fuji Cem
Batch
200310151
Mix paste A and paste B
Harvard Batch
212230201
7
Mix powder and liquid
Table IIa : Chemical composition of the self-adhesive resin cement RelyX Unicem.
Powder Liquid
Radiopaque fluoro-aluminosilicate
glass
Micro-encapsulated potassium per-
sulfate and ascorbic acid catalyst
system
Aqueous solution of a poly-
carboxylic acid modified with
pendant methacrylate Group HEMA
Tartaric acid

57
Table IIb: chemical composition of Variolink II.
BisGMA, UDMA,TEGDMA
silicon dioxide,
self-cure initiators,
light-cure initiators
stabilizers
pigments
Table III: Frequency and median value of the microleakage scores for the different
combinations of inlay and luting materials.
Scores frequency
Material Margin 0 1 2 3 4 Median
occlusa 9 1 0 Gold+Unicem
cervical 6 1 1 2 0
occlusa 5 3 1 1 0.5 Gold+Fuji Cem
cervical 2 1 4 1 2 2
occlusa 9 1 3 Gold+Harvard
cervical 10 4
occlusa 2 2 1 5 3 Empress+VariolinkII
cervical 2 2 6 4
occlusa 8 1 1 0 Empress+Unicem
cervical 4 1 1 3 1 1.5
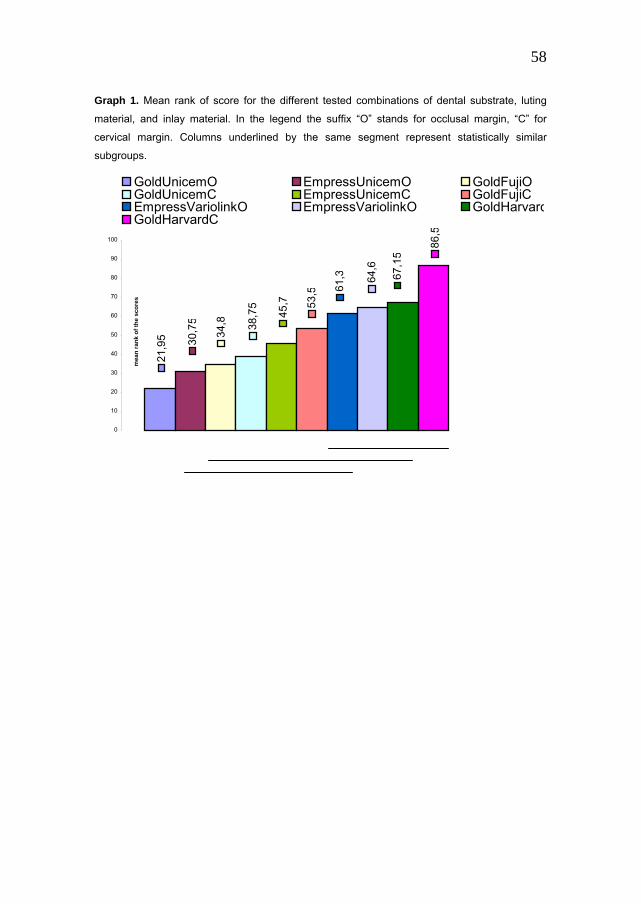
58
Graph 1. Mean rank of score for the different tested combinations of dental substrate, luting
material, and inlay material. In the legend the suffix “O” stands for occlusal margin, “C” for
cervical margin. Columns underlined by the same segment represent statistically similar
subgroups. 21
,95 30
,75
34,8 38
,75
45,7 53
,5 61,3 64
,6
67,1
5
86,5
0
10
20
30
40
50
60
70
80
90
100
mea
n ra
nk o
f the
sco
res
GoldUnicemO EmpressUnicemO GoldFujiOGoldUnicemC EmpressUnicemC GoldFujiCEmpressVariolinkO EmpressVariolinkO GoldHarvardGoldHarvardC

59
Graph 2. Mean rank of scores for the materials used to lute gold inlays. In the legend the suffix “O” stands
for occlusal margin, “C” for cervical margin. Columns underlined by the same segment represent
statistically similar subgroups.
12,9 20
,55
23,2
32,0
5 41,3
53
0
10
20
30
40
50
60
mea
n ra
nk o
f sco
res
UnicemO FujiO UnicemC
FujiC HarvardO HarvardC
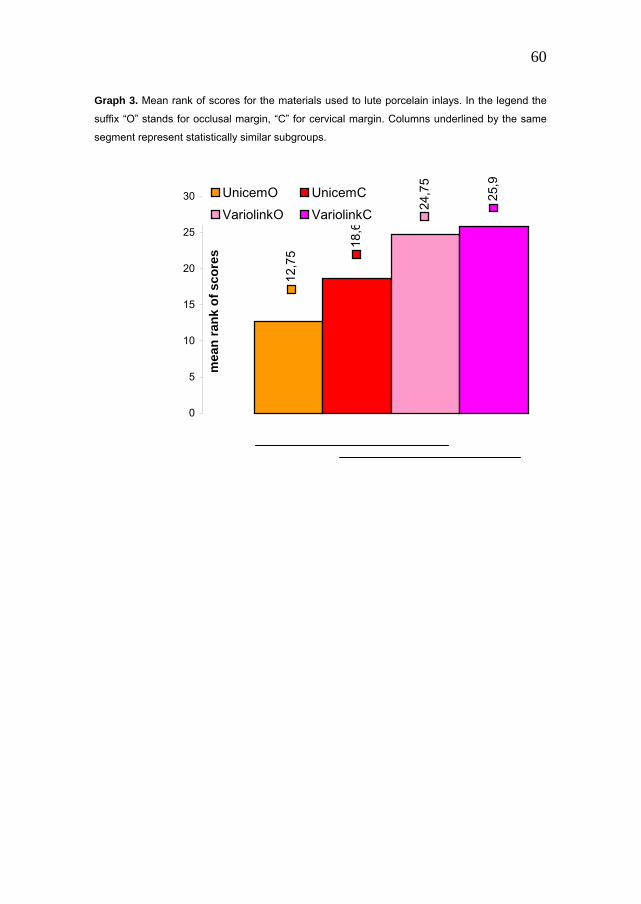
60
Graph 3. Mean rank of scores for the materials used to lute porcelain inlays. In the legend the
suffix “O” stands for occlusal margin, “C” for cervical margin. Columns underlined by the same
segment represent statistically similar subgroups.
12,7
5
18,6
24,7
5
25,9
0
5
10
15
20
25
30
mea
n ra
nk o
f sco
res
UnicemO UnicemCVariolinkO VariolinkC
61
Chapter 4
Sealing ability of packable resin composites in class II restorations.
Abstract: Purpose: To evaluate in Class II restorations the marginal
adaptation of ten packable composite resins in combination with the
proprietary adhesive system.
Materials and Methods: Standard Class II cavities were prepared in 100
extracted molars. The sample was randomly divided into ten Groups. In each
Group one specific packable composite was tested, in association with its
own adhesive: Groups: 1) Scotchbond1/FiltekP60 2) Etch&Prime3.0/Definit
3) Prime & Bond 2.1/SureFil 4) Excite/Tetric Condensable 5) Gluma/Solitaire
6) Kerr Bonding/Prodigy Condensable 7) One-step/Pyramid 8)
Tenure/Virtuoso 9) Syntac/Cavex Packable 10) Excite/Tetric flow/Tetric
Ceram. The restored teeth were sectioned at three levels in the mesio-distal
direction and processed for the microleakage test. On each section the
degree of dye penetration along the margins of the restoration was
assessed, and the differences in the leakage given by the ten materials at either the occlusal or the cervical margin were evaluated for statistical
significance. A statistical analysis was also conducted to assess the
significance of the differences between the scores recorded at the occlusal
margin and those measured at the cervical margin of the restoration. Results and Conclusions: Microleakage was significantly higher at the
cervical than at the occlusal margin of the restorations. The application of a
thin layer of a flowable composite at the cervical margin, as a liner
underneath the packable composite enhanced the marginal adaptation of
the restoration. The use of a self-etching primer to condition the dental
substrate resulted at the occlusal margin in a higher microleakage than
when phosphoric acid was applied.

62
Introduction
Patients’ demand for tooth colored restorations in the place of amalgam
restorations is constantly increasing (FDI World 1995). Composite resins are
the materials clinicians most commonly turn to as an alternative to amalgam
in Class II restorations. Highly filled composite resins, with a wear resistance
comparable to that of amalgam(Leinefelder KF, 1995 and 1997), especially
meant for posterior restorations have lately been developed. The viscosity of
these composites is so high, in comparison with other resin-based materials,
that they require an application technique similar to that of amalgam. Hence
the name “packable”, by which this class of resin composites has been
called (Leinefelder KF et al, 1999).
The availability of a material with an handling similar to that of amalgam has
appeared to be a decisive factor in convincing many practitioners to move
from amalgam to direct composites also for posterior restorations. However,
packable composites have not yet given proof of mechanical properties far
superior to conventional composites (Manhart J et al, 2000). In addition,
some further light should be shed on the polymerization stress of these
highly-filled resins, which is a factor of crucial importance clinically, as it can
directly affect the quality of marginal seal in the restoration (Eakle WS & Ito
RK, 1990). Recently it has been reported (Chen et al, 2001) that packable
composites develop a quite high contraction stress in the early stages of
curing. This stress, if transmitted to the adhesive interface, can become
responsible for the failure of the bond, followed by the opening of a gap
between cavity walls and restoration, through which microleakage can occur
(Eakle WS & Ito RK, 1990; Tjan AH ,1992). It has been shown that even with
the latest generation adhesive systems, able to achieve on dentin levels of
bond strength similar to those reached on enamel, microleakage can not be
completely eliminated in vivo (Eakle WS & Ito RK, 1990; Tjan AH ,1992). It
therefore becomes imperative to do whatever possible to limit the
occurrence of this phenomenon. At this objective have aimed the recent

63
advancements of research in the field of bonding. These have led to the
introduction of more hydrophilic adhesives, which have proved able to
improve the quality of marginal seal in Class II restorations (Duncalf WV,
Wilson NA, 2000). A parallel front of the research activity has been working
on the development of bonding systems with simplified handling, in the
attempt to control as much as possible the influence of the operating and
operator’s conditions on the properties expressed by the material (Kanca J,
1992; Sano H & Ciucchi B, 1995; Tay FR et al, 1996).
The aim of this study was to assess the ability of different combinations of
latest-generation adhesive systems and packable composites in creating a
valid seal on the margins of Class II restorations. The quality of marginal
adaptation was evaluated through microleakage tests. The null hypothesis
that the type of bonding system and packable composite used does not
significantly affect the quality of seal was tested.
Materials and Methods
Specimen Preparation One hundred human extracted molars were selected as being sound and
free from caries and/or restorations. The teeth were stored in a 1%
chloramine solution until used for the experiment, in any case no longer than
three month. A standardized adhesive Class II preparation was made in the
mesial and occlusal surface (Fig. 1). The cervical margin of the interproximal
box was placed 1mm below the cementum-enamel junction, in cementum-
dentin. Occlusally the tooth was reduced by 2 mm, and the cavity was 3 mm
wide. The proximal box was 4 mm wide bucco-lingually, whereas the pulpal
and axial walls measured 2 mm in depth. The dimensions of the prepared
cavities were checked with a Boley gauge. A ±0.3 mm tolerance in the
measurements was considered acceptable for including the specimen in the
trial. No bevels were added at any margin of the preparation.

64
The sample of teeth was randomly divided into ten groups of ten specimens
each. All of the specimens in each group were restored with the same
composite, used in combination with the proprietary adhesive system:
Group 1. Scotchbond1 and Filtek P60 (3M, St. Paul, MN, USA)
Group 2. Etch&Prime 3.0 and Definit (Dentsply Degussa, Bloomfield, CT,
USA)
Group 3. Prime & Bond 2.1 and SureFil (Dentsply/Caulk, Milford, DE, USA).
Group 4. Excite and Tetric Condensable (3 layers) (Ivoclar Vivadent, Schaan,
Liechtenstein).
Group 5. Gluma and Solitaire (Haereus Kulzer, Hanau, Germany).
Group 6. Kerr Bonding and Prodigy Condensable (Kerr, Orange, CA, USA).
Group 7. One-step and Pyramid (Bisco, Schaumburg, IL, USA).
Group 8. Tenure and Virtuoso Packable (DenMat, Santa Maria, CA, USA).
Group 9. Syntac Single Component (Ivoclar Vivadent, Schaan, Liechtenstein)
and Cavex Packable (Kuraray, Japan).
Group 10. Excite, Tetric flow, and Tetric Ceram (Ivoclar Vivadent, Schaan,
Liechtenstein).
In Groups 1-9 packable composites were tested. In Group 10, on the other
hand, a flowable composite was applied as a 1-2 mm thick base, which
remained exposed at the cervical margin, according to the “open-sandwich”
technique. On top of the flowable, a hybrid resin composite was stratified,
filling up the cavity. This group served as control, as the restoration
technique followed has provided quite satisfactory results in terms of quality
of the marginal seal.
All of the restorations were finished with a fine-grit diamond bur, polished
with abrasive disks, and stored in tap water for twenty-four hours.
Microleakage test After coating the roots and blocking the canal foramina with nail varnish, the
specimens were immersed in a dye solution (2% methylene blue) for twenty-

65
four hours, and subjected to 500 thermal cycling tests, each with a dwell time
of twenty seconds at 5 C° and 55 C°.
The specimens were then embedded in acrylic resin, and longitudinally
sectioned with a diamond saw (Isomet, Buehler, Lake Bluff, IL, USA) at three
different levels in the mesio-distal direction. The first cut was positioned in
the center of the restorations, whereas other two sections were made along
the lingual and buccal lateral walls, approximately at the interface between
the restoration and the cavity's wall (Fig. 2).
The extent of staining was measured at both the occlusal and cervical
margins. The depth of dye penetration at the occlusal level was scored as: 0
= no penetration; 1 = leakage no deeper than the enamel-dentin junction; 2 =
leakage deeper than the enamel-dentin junction; 3 = leakage along the
occlusal and/or axial lateral walls; 4 = leakage into dentinal tubules (Fig. 3).
The extent of cervical leakage was assessed according to the following score
method: 0 = no penetration; 1 = leakage not exceeding the middle of the
cervical wall; 2 = penetration past the middle of the cervical wall; 3 =
penetration to the axial wall; 4 = penetration to and along the axial wall or
into the dentinal tubules (Fig. 4).
The sections were observed under a stereomicroscope in double blind by
two different operators. In case of a disagreement between the two
investigators on the score assigned to a certain specimen, the worse score
was chosen for the statistical analysis.
Statistical analysis The differences in the microleakage data recorded for all of the groups at
either the occlusal or the cervical margin of the restorations were tested for
statistical significance using Kruskal-Wallis Non-Parametric ANOVA by
ranks, with Bonferroni alpha protection. In order to compare all of the scores
measured at the cervical margin with all the pooled data from the occlusal
margin, the Mann-Whitney-U test was performed. The level of statistical
significance was set at p=0.05.

66
Results In general, the scores recorded at the cervical margin were significantly
higher than those measured at the occlusal margin (p<0.05).
When all of the groups were compared for microleakage at the occlusal
margin, the only significant difference revealed by the statistical analysis was
that the specimens treated with Etch&Prime 3.0 and Definit (Group 2)
exhibited a marginal adaptation significantly worse than that seen in Groups
1, 3, 4, 6, 8, 10.
When the comparison was made among all groups for the scores at the
cervical margin, Group 5 restorations (Gluma/Solitaire) were revealed to
have leaked significantly more than Groups 1, 4, 8, 10 restorations. Also, the
difference between Group 9 (Syntac/Cavex Packable) and Group 1
(Scotchbond 1/Filtek P60) at the cervical margin was significant, with
Syntac/Cavex Packable giving a higher microleakage.
Discussion In order to be considered as a valid alternative to amalgam and indirect
restorations for Class II cavities, packable composites have to give proof not
only of adequate mechanical properties, but also of the ability to efficiently
seal the cavity margins.
In this investigation, the method of microleakage was chosen to assess the
quality of the marginal adaptation achieved by ten commercially available
packable composites. Measurements were taken at both the occlusal and
the cervical margins of the cavity, and not only in the middle of the
restoration, but also in the vicinity of the axial walls, along which gaps
between tooth substrate and material are more likely to develop (Rigsby DF
et al, 1990; Ferrari M et al, 1999).

67
The outcome of this trial, in agreement with the results of previous studies,
confirms that the cervical level remains the weakest point of the adhesive
restorations, as far as marginal integrity is concerned (Thonemann B et al,
1999; Tung FF et al, 2000). It has indeed been shown that when the margin
is placed below the cemento-enamel junction, an outer layer of cement 150-
200 microns thick is present, which provides a hypomineralized and
hyperorganic substrate to bonding (Cagidiaco MC et al, 1996). This tissue,
even after etching, does not provide the adequate conditions for the
micromechanical retention of an adhesive material. Although the
hybridization of the cementum has been demonstrated (Ferrari M et al,
1997), however the absence of resin tags in the first 150-200 microns from
the cervical margin testifies the relatively poor quality of the bonding that can
be achieved at this level.
Another factor that challenges the marginal integrity of an adhesive
restoration is the contraction stress of the composite resin. It is known that
the shrinkage of resin-based materials is inevitable, as related to the
chemistry of the polymerization reaction itself, that involves the conversion of
intermolecular distances in the order of 0.4 nm into covalent bonds 0.15 nm
long (Peutzfeld A, 1997). It has also been proved that some of the
contraction shrinkage can be absorbed through the material if its molecules
are free to flow at the exposed surfaces of the restoration (Feilzer AJ et al,
1990). When the material is in a more rigid state, most of the polymerization
shrinkage can not be absorbed, and is indeed transmitted to the adhesive
interface. Here the contraction stress can become responsible of the
opening of marginal gaps or of microfractures within the dental substrate
(Davidson CL & Feilzer AJ, 1997).
The polymerization stress transmitted by a resin-based material is directly
related to its modulus of elasticity (Feilzer AJ et al,1990; Davidson CL &
Feilzer AJ, 1997). It follows that packable composites, being relatively rigid
materials, can intensely stress the adhesive interface (Chen HY et al, 2001).
Under these conditions, if the bond is not strong enough, the marginal seal

68
can be violated, and microleakage can occur as a consequence. It has
earlier been proposed to incorporate an “elastic” layer at the restoration base
to act as a stress absorber not only of the functional loads, but also of the
internal tensions induced by composite polymerisation (Kemp-Scholte CM &
Davidson CL, 1990; Hilton TJ, 1998; Ferrari M, 1999; Hilton TJ & Ferracane
JL, 1999; Dietschi D et al, 2002). The insertion of an elastic liner is especially
advisable underneath packable composites restorations.
In a recent investigation (Dietschi D et al, 2002) it was found advantageous,
for the purposes of marginal adaptation, the application of a 1-1.5mm thick
layer of a compomer at the cervical margin of Class II cavities, then filled
with a hybrid composite. The compomer was applied following both the
“open-“ and the “closed-sandwich” technique, and a significant improvement
in the quality of marginal seal was obtained in particular when the layer of
low-modulus material was covered by the composite at the gingival margin
(closed-sandwich).
In this study, the “open-sandwich” technique was followed in the restoration
of the control group’s specimens (Group 10), where a layer of flowable
composite was applied at the cervical margin as a liner, on top of which a
hybrid composite was then stratified. In this Group relatively low
microleakage scores were recorded at the cervical margin, confirming that
the insertion of an elastic layer at this level definitely adds to the quality of
marginal adaptation.
As regards the results of the test at the occlusal level, it should be noted that
a significantly higher microleakage was reported in the only one group where
a self-etching primer was used to treat the substrate (Group 2). It can
therefore be inferred that the conditioning action of the self-etching primer
has failed to create the adequate conditions for the establishment of a
micromechanical bonding to enamel. To similar conclusions regarding the
efficacy of self-ecthing primers on the enamel substrate have led the results
of some previously published studies (Hara AT et al, 1999).

69
It should finally be pointed out that the same Group 2 specimens scored
relatively low for microleakage at the cervical margin, indicating that the
conditioning action of the self-ecthing primer was on dentin comparable to
that of the phosphoric acid used in the other experimental groups. Also this
finding is in line with the results of some previous trials, investigating the
performance of self-etching primers on dentin substrates (Pashley DH & Tay
FR, 2001).
In conclusion, in a Class II cavity restored with a packable composite:
1. Microleakage is significantly more noticeable at the cervical than at
the occlusal margin.
2. The application of a thin layer of a flowable composite at the cervical
margin, as a liner underneath the more rigid composite filling up the
cavity, enhances the marginal adaptation of the restoration.
3. The use of a self-etching primer to condition the dental substrate
results at the occlusal margin in a higher microleakage than if
phosphoric acid is applied as an etchant.

70
References
Cagidiaco MC, Vichi A, Ferrari M. SEM evaluation of outside dentin-
cementum layer at cervical margins of Class II restorations. J Dent Res
1996; 75 (Abstr 28) 1220.
Chen HY, Manhart J, Hickel R, Kunzelmann KH. Polymerization contraction
stress in light cured packable composite resins. Dent Mater 2001; 17: 253-
259.
Davidson CL, Feilzer AJ. Polymerization shrinkage and polymerization
shrinkage stress in polymer-based restorative. J Dent 1997; 25: 435-440.
Dietschi D, Bindi G, Krejci I, Davidson C. Marginal and internal adaptation of
stratified compomer-composite Class II restorations. Oper Dent 2002; 27:
500-509.
Duncalf WV, Wilson NA. A comparison of the marginal and internal
adaptation of amalgam and resin composite restorations in small to
moderate-sized Class II preparations of conventional design. Quint Int 2000;
31: 347-352.
Eakle WS, Ito RK. Effects of insertion technique on microleakage in mesio-
occluso-distal composite resin restorations. Quintessence Int 1990; 21: 369-
374.
Federation Dentaire Internationale, World Health Organization, World Dental
Federation, Consensus statement on dental amalgam. FDI World 1995 : 9-
10.
Feilzer AJ, de Gee AJ, Davidson CL.Quantitative determination of stress
reduction by flow in composite restorations. Dent Mater 1990; 6: 167-171.
Ferrari M, Cagidiaco MC, Davidson CL. Resistance of cementum in Class II
and V cavities to penetration by an adhesive system. Dental Mater 1997; 13:
152-162.
Ferrari M, Mason PN, Fabianelli A, Cagidiaco MC, Kugel G, Davidson CL.
Influence of tissue characteristics at margins on leakage of Class II indirect
porcelain restorations. Am J Dent 1999; 12: 134-142.
71
Ferrari M. “Advances in Glass-Ionomer Cements” in Davidson CL and Mjor
IA: Glass-Ionomer Cements. Quintessence Int, Berlin 1999: 137-148.
Hara AT, Amaral CM, Pimenta LA, Sinhoreti MA. Shear bond strength of
hydrophilic adhesive systems to enamel. Am J Dent 1999; 12: 181-184.
Hilton TJ, Ferracane JL. Cavity preparation factors and microleakage of
Class II composite restorations filled at intraoral temperatures. Am J Dent
1999; 12: 123-130.
Hilton TJ. Can modern restorative procedures and materials reliably seal
cavities? In vitro investigation. Transaction of Academy of Dental Materials
Meeting, Banff, 1998; vol 12: 21-74.
Kanca J. Resin bonding to wet substrate. Quint Int 1992; 23: 39-41.
Kemp-Scholte CM, Davidson CL. Complete marginal seal of class V resin
composite restorations effected by increased flexibility. J Dent Res 1990; 69:
1240-1243.
Leinefelder KF, Bayne SC, Swift Jr EJ. Packable composites: overview and
technical considerations. J Esthet Dent 1999; 11: 234-249.
Leinefelder KF. New developments in resins restorative systems. J Am Dent
Assoc 1997; 58: 484-487.
Leinefelder KF. Posterior composite resins: the materials and their clinical
performance. J Am Dent Assoc 1995; 126: 663-676.
Manhart J, Kunzelmann KH, Chen HY, Hickel R. Mechanical properties and
wear behaviour of light-cured packable composite resins. Dent Mater 2000;
16: 33-40.
Pashley DH, Tay FR. Aggressiveness of contemporary self-etching
adhesives. Part I: Depth of penetration beyond dentin smear layers. Dent
Mater 2001; 17: 296-308.
Peutzfeld A. Resin composites in dentistry : the monomer systems. Eur J
Oral Sci 1997; 105: 97-116.
Rigsby DF, Retief DH, Russel CM, Denys FR. Marginal leakage and
marginal gap dimension of three dentinal bonding system. Am J Dent 1990;
3: 289-294.
72
Sano H, Ciucchi B. Nanoleakage: leakage within the hybrid layer. Oper Dent
1995; 20: 18-25.
Tay FR, Gwynnet AJ, Wei SH. Micromorphological spectrum from overdrying
to overwetting acid-conditioned dentin in water-free, acetone-based, single-
bottle primer/adhesives. Dent Mater 1996; 12: 236-244.
Thonemann B, Federlin M, Shmalz G, Grundler W. Total bonding vs
selective bonding: marginal adaptation of Class II composite restorations.
Oper Dent 1999; 24: 261-271.
Tjan AH, Bergh BH, Linder C. Effect of various incremental techniques on
the marginal adaptation of class II restoration. J Prosthet Dent 1992; 67: 62-
66.
Tung FF, Estafan D, Scherer W. Microleakage of a condensable resin
composite: an in vitro investigation. Quintessence Int 2000; 31: 430-434.

73
Table I Bonding procedures
Bonding system Clinical procedures
Conditioning
with
phosphoric
acid
Primer-
adhesive
application
Self-etching
primer
application
Bonding
application
Air
blowing
Light
curing
Scotchbond1 x x x x
Etch&Prime3.0 x x x
Prime&Bond2.1 x x x x
Excite x x x x
Gluma x x x x x
Kerr Bonding x x x x x
One Step x x x x
Tenure x x x x x
Syntac x x x x
Excite x x x x
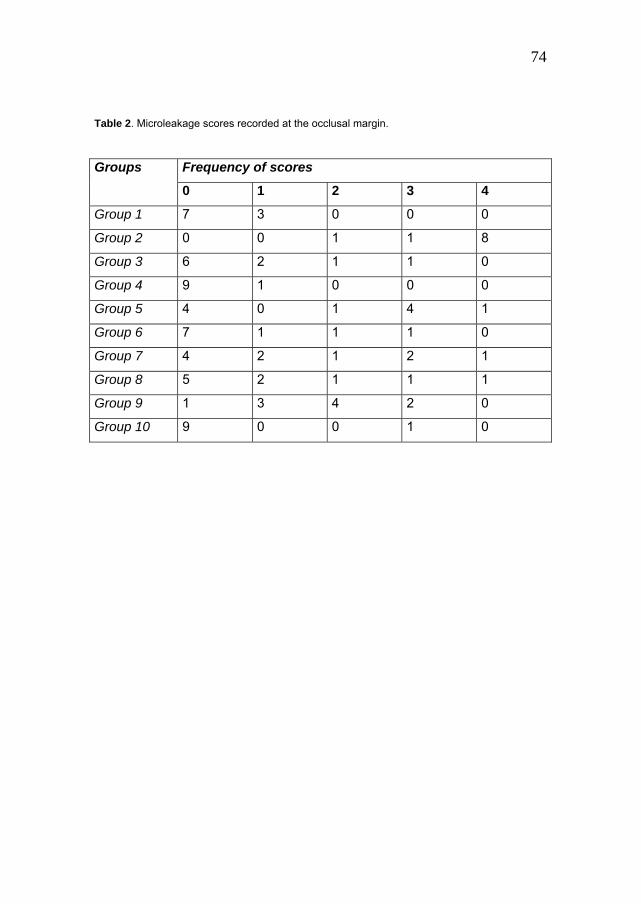
74
Table 2. Microleakage scores recorded at the occlusal margin.
Frequency of scores Groups
0 1 2 3 4
Group 1 7 3 0 0 0
Group 2 0 0 1 1 8
Group 3 6 2 1 1 0
Group 4 9 1 0 0 0
Group 5 4 0 1 4 1
Group 6 7 1 1 1 0
Group 7 4 2 1 2 1
Group 8 5 2 1 1 1
Group 9 1 3 4 2 0
Group 10 9 0 0 1 0

75
Table 3. Microleakage scores recorded at the cervical margin.
Frequency of scores Groups
0 1 2 3 4
Group 1 7 2 1 0 0
Group 2 7 1 0 0 2
Group 3 1 2 2 5 0
Group 4 3 3 3 1 0
Group 5 0 0 0 2 8
Group 6 3 1 1 3 2
Group 7 3 2 1 2 2
Group 8 3 2 3 1 1
Group 9 1 0 0 8 1
Group 10 6 1 1 1 1

76
Legends to illustrations
Fig. 1. The standardized Class II cavity prepared for the resin composite restoration.
Fig. 2. Each sample was longitudinally sectioned at three different levels in the mesio-
distal direction.

77
Fig. 3. Scores of dye penetration at the occlusal margin.
Fig. 4. Scores of dye penetration at the cervical margin
.
78
Chapter 5
Marginal integrity of ceramic inlays luted with a self-curing resin system. Abstract: Purpose: Aim of this study was to observe the efficacy of two
different composite cements on the prevention of marginal deterioration
around adhesive ceramic inlay restorations, under laboratory conditions, and
to test the null hypothesis that different luting procedures cannot affect
sealing ability of luted inlays. Methods. Twenty-six standardized mesio-
occlusal Class II cavities were prepared in extracted posterior teeth. Class II
inlays were fabricated with IPS Empress II system following the
manufacturer's instructions. The samples were divided into two groups of 13
teeth each at random. Group 1: The ceramic inlays of Group 1 were luted
using Excite DSC and an experimental self-curing resin cement (Multilink,
Vivadent); in this group, Excite DSC was self-activated and not light-cured.
Group 2: Excite DSC in combination with a dual-curing resin cement
(Variolink II, Vivadent) was used (as control). In this group Excite DSC was
light-cured for 20 s separately, before resin cement application. The ‘wet’
bonding technique was followed. Three samples of each group were
selected at random for SEM observations, while the other 10 samples were
processed for marginal leakage. The bonding mechanism to dentin and resin
cement thickness was evaluated. Results: Samples of both groups showed
resin tag and adhesive lateral branch formation. In Group 1 the hybrid layer
was mainly uniform along the interface between dental substrates and
adhesive material, and resin cement thickness was between 20 and 85 µm.
At the cervical margin no gap was detected. In Group 2 the cement
thickness was between 30 and 110 µm and hybrid layer formation was
observed along the interface but at the cervical margin it was not always
uniform and continuous. Resin tag formation was uniform in both groups. At

79
cervical margins, 80% of Group 1 samples showed a perfect seal at the
dentin–cementum margins, and 90% at enamel margins. Group 2 samples
showed only 50% of cervical margins free from leakage and 80% at the
occlusal enamel margins. Statistically significant differences were found at
cervical margins between the two groups, while no significant differences
were found at enamel site. Conclusions: It can be concluded that the self-
curing adhesive-resin cement combination can properly seal Class II
porcelain inlays.

80
Introduction
During recent years, increasing demand for aesthetics in dentistry resulted in
the development of restorative materials. Composite materials are
acceptable for restoring anterior teeth but it is possible to have problems
with their usage in stress bearing areas of the mouth (Vanherle G et al,
1985). The use of ceramic materials for aesthetic dental restorations has
increased substantially. This trend is attributed mainly to improvements in
the properties of ceramics and porcelain bonding systems.
A number of ceramic inlays techniques have been developed, e.g. castable
and pressed glass ceramic inlays which have excellent aesthetic properties.
They have satisfactory physic-mechanical properties and abrasion
resistance(Binns D, 1983). They are also resistant to wear (Krejci I et al,
1993), their plaque retention behaviour is lower than enamel (Savitt ED et al,
1987), they are biocompatible with the periodontal tissues and pulp (Cavel
WT et al, 1988), and transfer less heat (Adair PJ & Grossman DG , 1984;
Grossman DG , 1985) compared to metallic restorations.
However, a number of unsolved problems are associated with the fit of
ceramic inlays: the marginal adaptation and the resistance to fracture of
ceramic inlays seem to be probably the most important features that could
influence the durability of these restorations (Cavel WT et al, 1988;
Malament KA & Grossman DG, 1987; Bessing C & M. Molin, 1990; Van
Meerbeek BV et al, 1992; Krejci I et al, 1993; Thordrup M et al, 1994).
Different investigations have shown that inlays cemented with adhesive
materials exhibited superior fracture resistance compared to those cemented
with conventional cements (Dietschi D et al, 1990; Jensen ME et al, 1987).
Thus, the thickness of the layer of the luting cement may influence the risk of
disintegration of it, as well as microleakage along the inlay margins
(Leinfelder KF et al, 1989; Reich E et al, 1990).
The aim of this study was to observe the efficacy of two adhesive/resin
composite combinations on the prevention of marginal deterioration around

81
adhesive ceramic inlay restorations, under laboratory conditions, and to test
the null hypothesis that different luting procedures cannot affect the sealing
ability of luted inlays.
Method and materials
Preparation design Twenty-six recently extracted posterior molars, all free from previous
restoration and decay, were selected for this study. Mesio-occlusal Class II
cavities, designed according to manufacturer's instructions for making
porcelain inlays, were prepared under a copious water spray with medium-
grit diamond point burs, mounted in a high-speed handpiece. The proximal
boxes were extended 1 mm below the cementum–enamel junction (CEJ), to
place cervical margins in cementum–dentin (Fig. 1). An occlusal reduction of
2 mm was made, the bucco-lingual width of the proximal boxes was 4 mm,
the occlusal width 3 mm and the depth of the pulpal and axial walls 2 mm. A
tolerance of 0.3 mm was used to include preparations in the test. A butt-joint
margin preparation was made at the cervical margins of all samples. No
bevels were utilized in the preparation.
Restoration placement An impression for each tooth was made using polyether impression material
(Permadyne, Espe, Seefeld, Germany). Impressions were cast in type IV
stone (Fuji Rock, GC Dental, Tokyo, Japan). The inlays were fabricated with
IPS Empress II system (Ivoclar, Schaan, Liechtenstein) following
manufacturer's instructions. Before the luting procedure, Empress II inlays
were inspected under optical microscope at ×24 (Nikon 102, Tokyo, Japan):
when a marginal discrepancy higher than 25 µm was registered, the ceramic
inlays were remade; three inlays were remade.
The samples were randomly divided into two groups of 13 teeth each.
Adhesive-luting procedures are listed in Table 1.

82
Group 1. The ceramic inlays of Group 1 were luted to the corresponding
abutments using an experimental bonding system (Excite DSC, Vivadent,
Schaan Liechtenstein) and an experimental self-curing resin cement
(Multilink, Vivadent). In this group, Excite DSC was self-activated and not
light-cured.
Group 2. Excite DSC in combination with a dual-curing resin cement
(Variolink II, Vivadent) was used (as control). In this group Excite DSC was
light-cured for 20 s separately, before resin cement application.
Luting procedures The enamel margins of the teeth were acid-etched with 37% phosphoric acid
gel for 15 s. Then, the dentin and enamel were simultaneously etched for
another 15 s. The cavities were then thoroughly rinsed with water for 20 s
and gently air-dried for 1–2 s to remove the excess of water but leave the
cavity surfaces ‘wet’ (Kanca J, 1996). Then, the cementing procedures were
completed following manufacturers' instructions. The samples were
submitted to 500 thermal cycles (5 and 55°) and then stored for 24–48 h in
saline solution at room temperature before being processed for leakage.
Microscopic evaluation Three samples of each group were selected at random and split-fractured
along the long axis of the teeth, through the center of the restoration (Leitz
1600, Munchen, Germany). Then, one section of each tooth was gently
decalcified with 36% phosphoric acid for 10 s and deproteinized with 2%
sodium hypochlorite for 60 s at the interface site between the resin and
dentin layer. The other sections of each sample were kept in 30%
hydrochloric acid solution for 2 days in order to completely dissolve the
dental structures and to expose the resin replica of the interface (Cagidiaco
MC, 1995). Finally, all the sections and the resin replicas were mounted on
aluminum stubs, sputter-coated with gold using an Edwards Coater S150B
device, and observed under a Philips 515 scanning electron microscope.

83
Two different operators evaluated the samples in double blind. For each
sample of the two groups, observations and microphotographs of hybrid
layer, resin tags and adhesive lateral branches were detected to show the
most significant features. Also resin cement thickness was evaluated at
three different sites (at the cervical margin, along the axial wall and
occlusally); the media of each sample was recorded and evaluated
statistically.
Microleakage evaluation The other 10 samples of both groups, after being kept in 2% methylene blue
solution for 1 day, were embedded in resin (Technovit 2 100, Kuler,
Werheim, Germany). Each specimen was longitudinally sectioned into three
facio-lingual sections (Fig. 2) using a slow-speed diamond saw (Leitz 1600).
Dye penetration was evaluated according to the following parameters: 0, no
leakage; 1, microleakage at shoulder area; 2, microleakage at half of axial
wall(s); 3, microleakage at all of axial wall(s); 4, microleakage at occlusal
area. Two different operators scored the dye penetration in double blind,
using a binocular microscope (Nikon) at ×20. The worst score for the
sections of each tooth was used for scoring and further statistical analysis. In
case of discrepancy between the two evaluators, the worst score was
recorded. The leakage scores were evaluated statistically using the Kruskal–
Wallis multiple comparison test.
Results
Microscopic observations Samples of both groups in which dental substrates were completely
dissolved (Fig. 3) showed resin tag and adhesive lateral branch formation. At
the cervical margins short resin tags were noted (Fig. 4) while the occlusal
wall showed a high density of long resin tags (Fig. 5). Along the axial walls,
short resin tags were noted (Fig. 6). The morphology and density of resin

84
tags was directly related to tubule direction and density. In both groups, the
formation of resin tags, adhesive lateral branches and a hybrid layer were
evidenced. Also at the interface between enamel substrate and adhesive
resin, no gap was observed (Fig. 7). Resin cement thickness data are
reported in Table 2.
In Group 1 the hybrid layer was mainly uniform along the interface between
dental substrates and adhesive material (Fig. 8). The resin cement showed
very small voids/bubbles and its medium thickness was 62 µm, while
readings were between 20 and 85 µm. At the cervical margin, which was
placed below the CEJ, in cementum–dentin, the adhesion between adhesive
material and dental substrate was uniform and continuous (Fig. 8). No gap
was detected.
In Group 2 the medium cement thickness was 82 µm (readings between 30
and 110 µm). The hybrid layer formation was observed along the interface
(Fig. 9 and Fig. 10) but at the cervical margin, it was not always uniform and
continuous. No statistically significant difference was found between the
cement thickness of the two luting materials (Table 2).
Microleakage scores The results of this part of the study are summarized in Table 3.
Group 1: at cervical margins, 80% of specimens showed a perfect seal,
while 20% of them scored 1 as leakage. 90% of samples showed no dye
penetration at enamel–resin–porcelain interface and 10% of them had
scored 1.
Group 2: only 50% of samples were free from leakage at cervical margins.
Eight percent of specimens showed a perfect seal at the occlusal enamel
margins.
When the leakage scores of Groups 1 and 2 were evaluated, statistically
significant differences were found at cervical margins, while no significant
differences were found at the enamel (occlusal/axial) site.

85
Discussion
As it has been pointed out by several authors, marginal leakage is one of the
major drawbacks of a tooth-colored inlay (Torstensen B and Brännström M,
!988; Hofmann N et al, 1990).
Marginal fit of cemented restorations may be estimated by invasive or non-
invasive techniques. A non-invasive method leaving the tooth intact, may be
a quantitative SEM analysis, describing the whole margin of the area from
replicas and microphotographs (Remer R et al, 1989; Roulet JF et al, 1989)
or a microscopic assessment of the width of the luting cement at selected
points along the inlay margin (Hung SH et al, 1990; Thierfelder C et al,
1991; Dietschi D et al, 1992; Hass M et al, 1992; Inokoshi S et al, 1992).
The quantitative SEM analysis provides information of the surface area, but
not of the overall fit of the inlay.
The invasive methods are based on sections. The multiple sectioning
technique used in this study offers an advantage over the more simple
procedure of one-sectioned samples. According to Hung et al. (Hung SH et
al, 1990), the multiple-section technique can be more precise than the non-
invasive method, also from a statistical point of view. A possible explanation
might be that the absolute marginal discrepancy appears more well defined
on a section compared to an intact surface, and thus easier to determine.
The present investigation confirms these hypotheses.
It might also be possible to correlate the presence of a gap in several
samples of Group 2 and the absence of the gap at the interface between
conditioned dentin and adhesive material in Group 1 sample with the
leakage results: where a gap was present, dye penetration was deeper and
the score higher.
The clinical success of a tooth-colored inlay is correlated to the resin luting
cement properties. According to Leinfelder et al. (Leinfelder BP et al, 1989),
the maximum width of exposed luting cement should not exceed 100 ųm
86
occlusally due to the risk of abrasion. Disintegration caused by chemical
attack may present another problem for exposed resin luting cement (Larsen
IB & Munksgaard EC, 1991). Moreover, if the cement layer is too thick,
complete seating of inlay cannot be accomplished and the aesthetic
restoration will probably fail. In the present study, the average values of
occlusal thickness of the luting cements were below 100 ųm and the
experimental self-curing resin cement showed the lowest values.
In this study, microscopic evaluation of resin tag and adhesive lateral branch
formation was performed. In fact, the acid etching of dentin permits hybrid
layer, resin tags and adhesive lateral branch formation, thus creating a site
for micro mechanical retention of the resin into the demineralised substrate
(Nakabayashi N et al, 1991; Titley K et al, 1994; Perdigão J, 1995; Kanca J,
1996; Van Meerbek B et al, 1998) . Also, resin tags formed at the first part
of the tubule orifices can seal the tubules, avoiding any fluid movement and,
consequently, post-operative sensitivity(Nakabayashi N et al, 1991; Titley K
et al, 1994; Perdigão J, 1995; Kanca J, 1996; Van Meerbek B et al, 1998).
The efficacy of Excite DSC on forming resin tags, adhesive lateral branches
and a hybrid layer was already evaluated under laboratory and clinical
conditions (Dagostin A & Ferrari M, 2001; Ferrari M et al, 2001; Dagostin A &
Ferrari M, 2002). The uniformity of the bonding mechanism (hybrid layer,
resin tag and adhesive lateral branch formation) obtained using Excite DSC
might be correlated with the presence of the self-activating particles
(Dagostin A & Ferrari M, 2001; Ferrari M et al, 2001; Dagostin A & Ferrari M,
2002). In fact, the small particles of catalyst placed into the bristles of a very
thin microbrush included in the system, can carry the primer-adhesive
solution into the deepest area of the preparation and simultaneously also
self-activate it in the area that cannot be perfectly reached by the light
(Dagostin A & Ferrari M, 2001; Ferrari M et al, 2001; Dagostin A & Ferrari M,
2002).The difficulty of the light curing source to reach deep proximal areas
has also created the potential for marginal percolation and bacterial
penetration at the partially cured resin–dentin interface. This often leads to

87
marginal discoloration, secondary decay, and postoperative sensitivity (Eick
JD and Welch FH, 1986; Stangel I et al, 1987). The use of a self-curing
adhesive system in combination with self-curing resin cement like the
experimental one seems also to minimize these risks at cervical margins.
The results of this study rejected the null hypothesis that was tested.
Different luting material combinations and procedures can affect the sealing
ability of luted inlays.

88
References
Adair PJ, Grossman DG. The castable ceramic crown. Int J Period Rest
Dent 1984; 4: 32–38.
Bessing C, Molin M. An in vivo study of glass ceramic (Dicor) inlays. Acta
Odont Scand 1990; 48: 351–356.
Binns D. The chemical and physical properties of porcelain. In: J.W.
McLean, Editor, Dental Ceramics: Proceeding of the First International
Symposium on Ceramics, Quintessence, Chicago 1983:,41–83.
Cagidiaco MC. Bonding to dentin: mechanism, morphology and efficacy of
bonding resin composites to dentin in vitro and in vivo, De Batte ed., PhD
Thesis. Amsterdam, University of Amsterdam; 1995.
Cavel WT, Kelsey WP, Barkmeier WW , Blankenau RJ. A pilot study of the
clinical evaluation of castable ceramic inlays and a dual cure resin cement.
Quintessence Int 1988; 19: 247–252.
Dagostin A, Ferrari M. In vivo bonding mechanism of an experimental
bonding system. Am J Dent 2001; 14: 103–108.
Dagostin A, M Ferrari, Effect of dual bonding technique on the bond strength
of ceramic restorations. Dent Mater 2002; 18: 304–310.
Dietschi D, Maeder M, Meyer J-M. In vitro resistance to fracture of porcelain
bonded to tooth. Quintessence Int 1990; 21: 823–831.
Dietschi D, Maeder M, Holz J. In vitro evaluation of marginal fit and
morphology of fired ceramic inlays. Quintessence Int 1992; 23: 271–278.
Eick JD, Welch FH. Polymerization shrinkage of posterior composite resins
and its possible influence on postoperative sensitivity. Quintessence Int
1986 ; 17: 103–111.
Ferrari M, Vichi A, Grandini S, Goracci C. Efficacy of a self-curing
adhesive/resin cement system on luting Vectris fiber posts into root canals: a
SEM investigation. Int J Prosthodont 2001; 14: 543–549.
Grossman DG. Cast glass ceramics. Dent Clin North Am 1985; 29: 275.

89
Hass M, Arnetzl G, Wegscheider WA, König K, Bratschko RO. Klinische und
Werkstoffkundliche Erfahrungen mit Komposit, Keramik und Gold inlays.
Dtsch Zahnärzt Z 1992; 47: 18–22.
Hofmann N, Klaiber B, Heners M. Okklusale Randschlussqualität von Cerec-
Inlays nach mehrmonatiger Tragedauer. Dtsch Zahnärztl Z 1990; 45: 289–
292.
Hung SH, Hung KS, Eick JD, Chappel RP. Marginal fit of porcelain-fused-to-
metal and two types of ceramic crown. J Prosthet Dent 1990; 63: 26–31.
Inokoshi S., Van Meerbeck B, Willems G, Lambrechts P, Braem M,
VanherleG. Marginal accuracy of CAD/CAM inlays made with the original
and the updated software. J Dent 1992; 20: 171–177.
Jensen ME, Redford AD, Wilson BT. Posterior etched porcelain restorations.
an in vitro study. Compen Contin Edu Dent 1987; 8: 615–621.
Kanca J. Wet bonding: effect of drying time and distance. Am J Dent 1996;
9: 273-276
Krejci I, Lutz F, Reimer M. Marginal adaptation and fit of adhesive ceramic
inlays. J Dent 1993; 21: 39–45.
Krejci I, Lutz F, Reimer M, Heinzmann JL. Wear of ceramic inlays, their
enamel antagonists, and luting cements. J Prosthet Dent 1993; 69: 225–229.
Larsen IB,. Munksgaard EC. Effect of human saliva on surface degradation
of composite resins. Scand J Dent Res 1991; 99: 254–261.
Leinfelder KF, Isenberg BP, Essig ME. A new method for generating ceramic
restorations: a Cad–Cam system. J Am Dent Assoc 1989; 118: 703–708.
Malament KA, Grossman DG. The cast glass-ceramic restoration. J Prosthet
Dent 1987; 57: 674–681.
Nakabayashi N, Nakamura M, Yasuda N. Hybrid layer as dentin bonding
mechanism. J Esthet Dent 1991; 3: 133-138.
Perdigão J. An ultra-morphological study of human dentine exposed to
adhesive systems. Thesis. Leuven, Belgium: Catholic University of Leuven;
1995.

90
Reich E, Schmalz G, Federlin M. Randspaltverhalten von Keramik- und
Konpositinlays in vitri. Dstch Zahnärztl Z 1990; 45: 656–660.
Roulet J.F., Reich T, Blunck T, Noack M. Quantitative margin analysis in the
scanning electron microscope. Scan Elect Microsc 1989; 3: 147–159.
Savitt ED, Malement KA, Socransky SS, Melcer AJ, Backmann KJ. Effect of
colonization of oral microbiota by a cast Glass ceramic restoration. Int J
Period Rest Dent 1987; 7: 23–30.
Stangel I, Nathanson D, Hsu CS. Shear strength of the composite bond to
etched porcelain. J Dent Res 1987; 66: 1460–1465.
Thierfelder C, Fuhrmann I, Knappe M. Vergleichende Untersuchung zur
Passgenauigkeit des Kompositinlays Estilux posterior CVS. Die Quintessenz
1991; 9: 1399–1407.
Thordrup M, Isidor F, Hörsted-Bindslev P. Comparison of marginal fit and
microleakage of ceramic and composite inlays: an in vivo study. J Dent
1994; 22: 147–154.
Titley K, Chernecky R, Maric B. Penetration of a dentin bonding agent into
dentin. Am J Dent 1994; 7: 190–194.
Torstensen B, Brännström M. Composite resin contraction gaps measured
with a fluorescent resin technique. Dent Mater 1988; 4 : 238–245.
Van Meerbeek BV, Inokoshi S, Willems G. Marginal adaptation of four tooth-
coloured inlay systems in vivo. J Dent 1992; 20: 18–29.
Van Meerbek B., Y. Yoshida and P. Lambrechts, A TEM study of two water-
based adhesive systems bonded to dry and wet dentin. J Dent Res 1998;
77: 50–59.
Vanherle G, Lambrechts P, Braem M. Overview of the clinical requirements
for posterior composites. In: G. Vanherle and D.C. Smith, Editors, Posterior
composite resin dental restorative materials, 3M Co, St Paul, MN 1985: 21–
40.
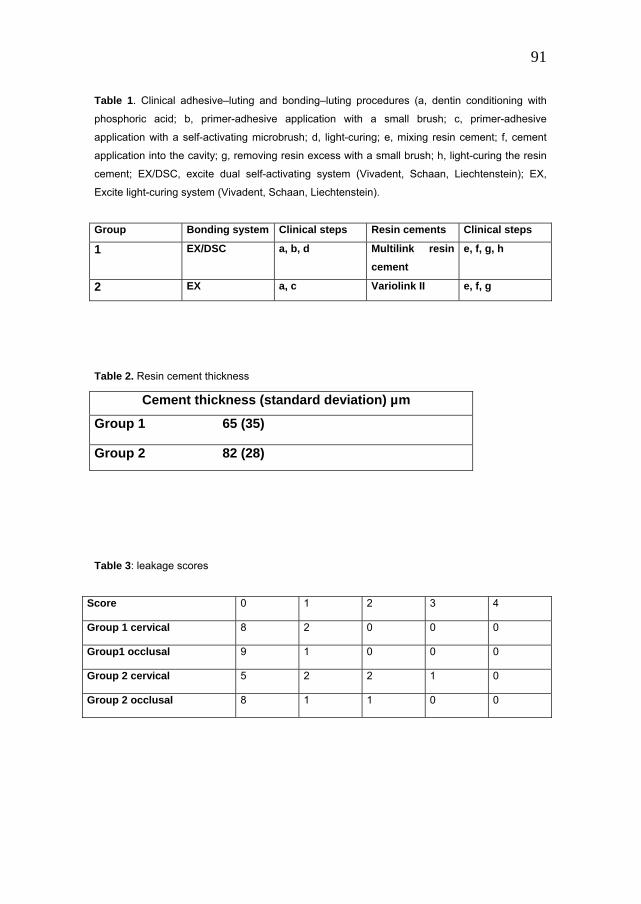
91
Table 1. Clinical adhesive–luting and bonding–luting procedures (a, dentin conditioning with
phosphoric acid; b, primer-adhesive application with a small brush; c, primer-adhesive
application with a self-activating microbrush; d, light-curing; e, mixing resin cement; f, cement
application into the cavity; g, removing resin excess with a small brush; h, light-curing the resin
cement; EX/DSC, excite dual self-activating system (Vivadent, Schaan, Liechtenstein); EX,
Excite light-curing system (Vivadent, Schaan, Liechtenstein).
Group Bonding system Clinical steps Resin cements Clinical steps 1 EX/DSC a, b, d Multilink resin
cement e, f, g, h
2 EX a, c Variolink II e, f, g
Table 2. Resin cement thickness
Cement thickness (standard deviation) µm
Group 1 65 (35)
Group 2 82 (28)
Table 3: leakage scores
Score 0 1 2 3 4
Group 1 cervical 8 2 0 0 0
Group1 occlusal 9 1 0 0 0
Group 2 cervical 5 2 2 1 0
Group 2 occlusal 8 1 1 0 0

92
Legends to illustrations
Fig. 1. Picture of standardized Class II cavity preparation
Fig. 2. Picture of sectioning procedure for evaluating dye penetration.

93
Fig. 3. Picture of a sample prepared for SEM observation after completely dissolving dental
substrates in an acid solution (SEM ×19) (1: cervical area; 2: occlusal area; 3: axial area).
Fig. 4. Picture at the cervical margin (area 1 of Fig. 3), placed 1 mm below the
cementum–enamel junction. Short resin tags and adhesive lateral branches are
visible (SEM ×710).

94
Fig. 5. Picture at the occlusal area (area 2 of Fig. 3). Long resin tags are noted (SEM
×710).
Fig. 6. Picture at the axial wall (area 3 of Fig. 3). Short resin tags are visible (SEM
×710).

95
Fig. 7. Picture at the enamel margin. Resin tags are formed (T: resin tags) (SEM
×1250).
Fig. 8. Picture at the interface between conditioned dentin and adhesive materials of
Group 1 sample. Hybrid layer formation is evident and no gaps are detected between
the different substrates (R: resin cement; D: dentin; H: hybrid layer) (SEM ×406).

96
Fig. 9. Picture of Group 2 sample. At the cervical margin this sample does not show
any gap interface between conditioned dentin and adhesive material (SEM ×1310) (H:
hybrid layer; D: dentin; R: resin cement).
Fig. 10. Picture of Group 2 sample. In this sample, at the cervical margin a gap (G)
was detectable at the interface between conditioned dentin and adhesive system
(SEM ×1250).

97
Chapter 6
Influence of tissue characteristics at margins on leakage of Class II indirect porcelain restorations.
Abstract: Purpose: to evaluate the sealing ability in class II porcelain inlays
with margins placed in cementum-dentin and enamel, luted by two new
different cementing materials. Materials and Methods: Thirty extracted
molars, free from caries and restorations were selected. The sample cavities
were prepared in a standardized manner and then were divided in three
groups (n=10) at random. Group 1: the cervical marginwas located 1 mm
below the CEJ and the inlays were luted EBS Multi (Espe) bonding system
in combination with Compolute 1.0 Aplicap (CLA 1.0 Espe) experimental
resin cement. Group 2: The cervical margin was placed 1 mm below the CEJ
and Syntac bonding system (Vivadent) and Variolink II resin cement
(Vivadent) were used. Group 3: The cervical margin was placed 0.5 mm
above the CEJ and the same matherials selected for Group 1 were used.
IPS-Empress (Ivoclar) inlays were made following manufacturer’s
instructions. After luting procedures and 2500 thermal cycles (5° and 55° C),
the samples were processed and evaluated for marginal leakage at cervical
and occlusal site. Samples of Group 3 were first selectioned in the center of
restorations as in Group 1 and 2 and scored (Group 3A) and then two other
cuts were made along the buccal and lingual areas (group 3B) and also
scored. After scoring dye penetration of Group 1 and 2 samples, half of the
sections were randomly selected to evaluate: (1) resin cement thickness, (2)
Hybrid layer formation at the interface between adhesive material and dental
substrate and (3) to observe the morphology of the class II cavity margins.
The leakage data were statistically evaluated with the Mann-Whitney U test
(P < 0.5). Results: statistically significant differences were found between
Groups 3A and 3B at the occlusal site, and not the cervical site. Samples of

98
Group 1 showed a cement thickness of 92 µm, 68 µm in Group 2. Hybrid
layer and resin tag formation was evident in Group 1. In Group 2 samples,
the hybrid layer formation was less evident and thinner than Group 1. At
cervical margins, an outer layer, not identifiable as sound dentin, of 200-300
µm thick, was noted. This layer was present in all three groups between
outer margin and sound dentin. The margins located both cervically and
axially in enamel mainly showed prisms cut along their long axis and low
level of structured etch pattern.
Conclusions : The results of this study suggest that an enamel thickness of
0.5 mm at the cervical margin of Class II indirect restorations in unable to
seal them completely. The two combinations of bonding-cement materials
performed similarly. The enamel axial margins of Class II inlays must be
considered one of the weakest margin of the cervical area.

99
Introduction
Knowledge on the aetiology of caries (Thylstrup A et al, 1986) and
observation of caries location lead to the conclusion that every plaque
retention site is a possible secondary caries zone (Anusavice KJ, 1989).
Defective wall-to-wall continuity between material and cavity walls facilitates
bacterial or toxin invasion, marginal staining, secondary caries and adverse
pulpal reactions (Branstrom M, 1982; Branstrom M, 1988). Therefore
marginal integrity of restorations in an important factor on preventing
leakage.
Unless the new developments on bonding to dentin (Nakabayashi N et al,
1991; Kanca J, 1992; Gwinnet AJ & Kanca J, 1992) improve marginal seal
and clinical performance of aesthetic restorations (Van Merbeeck B et al,
1994; Tyas MJ, 1996), poor adaptation and micro-leakage will still produce
problems at the gingival margins of Class II restoration (Donly KJ & Jensen
ME, 1990; Hilton TJ et al, 1997). Robinson et al (1987) and Dietschi et al
(1995) noted that marginal adaptation of indirect restorations was better than
that of direct restorations in Class II cavities. Dietschi et al (1995) also
pointed out that when residual enamel was less than 1mm in height or 0.5 in
thickness, indirect restorations had superior marginal quality. Less leakage
was found with indirect Class II restorations (inlays) compared to direct
aesthetic restorations. This is probably because aesthetic inlays reduce
polymerisation shrinkage, except for the small amount associated with a
layer of composite resin luting cement (Feilzer AJ et al, 1989), and
minimizes the variables of clinical procedures. The presence of leakage at
margins of Class II restorations was correlated with the type of dental
substrate at margins, etching procedures and type of bonding system used
(Cagidiaco MC, 1995; Ferrari M & Davidson CL, 1996). Hilton et al (1997)
pointed out an extensive leakage along the facial and lingual enamel walls of
Class II resin composite restorations. A variety of polymer-based resin
cement are now available. The ideal resin cement must be dual cured and

100
should demonstrate a film thickness of no more than 50 µm (Picard B et al,
1997). If the cement is too thick complete seating will not be accomplished
and the aesthetic crown will probably fail. The cement thickness is also
related to resin viscosity, its handling characteristics, clinical procedures and
experience of practitioners.
Recently two new combinations of bonding and resin cements were
proposed (Syntaca and Variolink II, a EBS Multib and CLA 1.0b) to increase
predictable clinical results. This study evaluated the marginal adaptation and
leakage of porcelain inlays luted with two different bonding resin cement
systems under laboratory conditions and correlated the dye penetration
depth with the morphology of dental substrates present at margins of the
preparations.
Materials and Methods
Thirty recently extracted posterior molars, all free from caries, cracks and
previous restorations on visual inspection, were selected for this study. The
average age of patients was 61 (range: 49-72). Tissue remnants on the
roots were removed by hand scaling. The teeth were stored in a saline
solution at room temperature (±22°C) for no longer than 4 weeks prior to
further preparation.
Preparations design
The selected molars were randomly ivied in three groups of 10 samples
each. Mesio-occlusal Class II cavities were prepared under a copious water
spray with medium-grit diamond-point burs, mounted in a high speed
handpiece. Twenty cavities for inlays were prepared with the proximal boxes
extending 1 mm below the cementum-enamel junction to place cervical
margins in cementum-dentin (groups 1 and 2). The last 10 samples were
prepared with the proximal boxes extending 0.5 mm above the CEJ to place
their margins in enamel (Group 3). Table 1 summarizes the three

101
experimental groups, variables, location of margins and materials of the
study.
The abutments were prepared according to manufacturer’s for making
single-unit all-porcelain inlay (Fig.1) with an occlusal reduction of 2 mm. The
bucco-lingual width of the proximal boxes was 4 mm, the occlusal width 3
mm and the depth of the pulpal and axial walls 2 mm. A tolerance of 0.3 mm
was used to include preparation in the test. A button-joint margin preparation
was made at the cervical margin of all samples. No bevels were utilized in
preparation. The dimensions of the cavity after preparation was confirmed
with a Boley gauge.
Although the mesio-distal and bucco-lingual dimensions of the preparations
were closely controlled, the length of the preparation was dependent on the
anatomy of the individual tooth. After all the preparations were completed
and dimensions recorded, the occlusal-gengival length of preparation varied
from 4.5 to 6.5 mm. The teeth were divided in two groups: short in which the
average length was 5.0 mm (range 5.6-6.5); and long in which the average
length was 6.1 mm (range 5.6-6.5). In addition, each experimental group had
an equal randomized number of teeth from the short and long occlusal-
gingival preparation categories.
Restoration placement Polyether impression (Permadyneb) of prepared teeth was madefor each
abutment, poured in type IV stone. The porcelain inlays (IPS-Empressc)
were fabricated strictly following manufacturer’s instructions. All porcelain
inlays were checked on the corresponding dies under optical microscope at
x20 (Nikon 102d). The inlays were made were made when a marginal
discrepancy greater than x20 µm was detected.
After making the inlays, sample teeth with cervical margins located below
the CEJ were randomly assigned to Groups1 and2 respectively (Table 1).

102
Group 1: EBS Multib enamel dentin bonding system and CLA 1.0
(Compolute 1.0 Aplicapb) experimental resin cement were used to lute the
porcelain inlays into the cavities.
Group 2: Syntaca enamel dentin bonding system in combination with
Variolink IIa resin cement was used.
Group 3: In the group of samples in which the cervical margins were located
above the CEJ (in the enamel), the same materials selected in Group 1 were
used.
The enamel margins of the teeth were acid-etched with 37% phosphoric acid
gel for 15 seconds. Then, the dentin and enamel were simultaneously
etched for another 15 seconds. The cavity was than thoroughly rinsed with
water for 20 seconds and gently air dried for 1-2 seconds to remove the
water but leave the cavity surface “wet”. Then, the cementing procedures
were completed following manufacturers’ instructions.
The inlay was seated and a small brush was used to remove the cement
excess from the margins. The complete removal of resin cement around the
margins was checked at x3 with loupes. To avoid oxygen inhibition of the
superficial layer of resin cement, a glycerine gel was applied along the
margins with a syringe. The composite resin luting material, protected by a
glycerine gel was finally light cured for 40 seconds from the lingual, gingival,
buccal and occlusal directions (total of 160 seconds). Table 2 summarizes
the two cementing procedures.
The samples werestored for 24-48 hours in saline solution at room
temperature (±22°C) before they were subjected to 2500 complete thermal
cycles in of 1-minute water baths alternatively at 5°C and 55°C.
Microleakage evaluation To visualize possible leakage, all samples were dried and apices of the roots
sealed with sticky wax. The surfaces of the tooth were coated with two
layers of fingernail polish, so that only the restorations and a surrounding
band of tooth structure approximately 1 mm wide were exposed. The

103
samples were immersed in 2 % methylene blue solution at room
temperature for 24 hours, washed, dried with compressed air and embedded
in slow-curing epoxyresin, prior to sectioning with a low speed diamond
blade saw through the center of the restorations in a mesial distal direction
(Groups 1-3). The samples of Group 3 were first sectioned in the center of
the restoration as those of Groups 1 and 2 (Group 3a). Then, two other cuts
were made in a medial distal direction along the buccal and lingual areas
between enamel and porcelain restoration to evaluate possible leakage
coming from these interfaces (Group 3b) (Fig. 2).
Dye penetration was observed with a binocular microscope (Nikond) at x 20.
Two different operators evaluated double-blind the sectioned samples for
leakage score. The amount of leakage viewed with the microscope was
scored. The worst score for the sections of each tooth area was used for
scoring and further statistical analysis. In case of discrepancy between the
two examiners, the worst score was used for evaluation.
The dept of cervical staining was measured according to the following
parameters (Fig. 3): 0= no penetration; 1= leakage not exceeding the middle
of the gingival wall; 2= penetration past the middle of gingival wall; 3=
penetration to the axial wall; 4= penetration to and along the axial cervical
wall or into dentin tubules.
The extent of the occlusal leakage was registered as the depth of dye
penetration according to the following scores (Fig. 4): 0= no penetration; 1=
leakage no deeper than the enamel-dentin junction; 2= leakage deeper than
the enamel-dentin junction; 3= leakage along the occlusal (Group 3a) and/or
axial walls (Group 3b).
The results of the staining measurements were statistically evaluated using
the Kruskal-Wallis non-parametric ANOVA by ranks with Bonferroni alpha
protection. The level of statistical significance was defined P= 0.05.

104
Microscopic evaluation Three different protocols were performed to evaluate: (1) resin cement
thickness, (2) hybrid layer formation at the interface between resin cement
and dental substrate, and (3) to observe the morphology of the cavity
margins.
After scoring for dye penetration of Group 1 and 2 samples, half of the
sections were randomly selected to observe hybrid layer formation and resin
cement thickness. To detect hybrid layer and resin tags formation, each
section was gently decalcified (with 37% phosphoric acid for 10 seconds)
and deproteinized (2% sodium hypochlorite solution for1 minute). Finally,
the sections were prepared for scanning electron microscope (SEM)
observations. The samples were critical-point dried (Blazer device). All
samples were gold coated, mounted on stubs and inspected by SEM (Joel
JXA-840f). The resin infiltration of cervical margins was studied at different
magnifications. Simultaneously, the same specimens were evaluated
regarding the resin cement thickness along the interface and the presence of
air bubbles along the cervical wall and at the angle between cervical and
axial wall of each abutment. The resin cement thickness was evaluated at
the cervical margin of Groups1, 2 and 3a, approximately 500 µm from the
margin toward the axial wall. With SEM, the resin cement thickness was
calculated for both the halves of each sample, and than the average score
was registered. To observe the morphology of the conditioned cavity
margins, 16 extracted posterior teeth were selected for the microscopic part
of the study. The selected teeth were randomly divided in two groups of
eight samples each. Group 4: Eight Class II cavities were prepared as
already described, for groups 1 and 2 (with cervical margins located below
the CEJ) and Group 5, another eight teeth were prepared as Groups 3a and
b (with cervical margins located above the CEJ).
Five samples each group (Groups 4a and 5a) were prepared to be directly
observed under SEM. The enamel margins of cavity preparations were
conditioned with 37% phosphoric acid for 15 seconds and then for another

105
15 seconds in the entire cavity surface, then washed for 20 seconds and
gently air-dried. This procedure was carried out to completely remove the
smear layer and open the dentin tubules as well as demineralise the inter-
tubular dentin at the interface and etch enamel. The samples were critical
point dried, gold coated and inspected by SEM.f Photographs were taken of
enamel sites along occlusal, lingual and buccal margins to document
significant aspects. Photographs were also taken at different sites
approximately every 200 µm on the abutments at different magnifications ,
starting at the cervical margin and moving towards the axial wall. The
appearance of the abutments was described close to the cervical margins
over a range of 100-500 µm along the interface between abutment and
bonding-cement system, and at the axial and occlusal areas.
The remaining three samples of each group (Groups 4b and 5b) were
restored as Groups 1-3 with an indirect porcelain restoration. After luting
procedures, the samples were stored for 24 hours in saline solution,
immersed in a 30% hydrochloric acid solution for 48 hours, and washed in a
2% sodium hypochlorite solution for 60 seconds to thoroughly demineralise
and deproteinize the tooth structure and to expose the resin replica of the
interface. In this way, it is possible to directly observe the resin tag formation
in the different areas of cavity walls. The resin specimens were gold coated,
mounted in metallic stubs and inspected by SEM.f Photographs were taken
of different sites along cavity margins to show significant aspects.
Results Microleakage data
Table 3 summarize the dye penetration depths by site for the three first
groups. In the samples of Group 1, 90% of samples showed no leakage at
the occlusal enamel margins, while only 40% of them showed no dye
penetration cervically. In the samples of Group 2, only 30% of specimens

106
presented a perfect seal at the cervical site and no leakage was observed at
the enamel site in 70% of the sections.
The samples of Group 3a showed 80% of samples without leakage at
enamel site after one section and 40% of the samples without leakage after
three seconds (Group 3b). In Group 3b, the dye mainly penetrated from axial
walls buccally or lingually. At the cervical site, the samples of Group 3a
showed 50% leakage after one section and 60% after three sections (Group
3b).
Statistical analysis of the data showed no significant differences between
occlusal sites of the same three groups.
When the leakage scores of Groups 3a and 3b, in which scoring after one
section and three sections were made, were compared, no statistically
significant differences were found at the cervical site, while they were found
at the enamel (occlusal/axial) site.
Microleakage observations
The thickness of resin cement, which represents the post cementation
marginal discrepancy, was higher in samples of Group 1 (92 µm) than in
those observed in Group 2 (68 µm) and a higher frequency of bubbles in the
resin cement was noted in the samples of Group 1 than in Group 2. In three
samples of Group 1, a cement thickness of 200 µm was noted. In another
five samples of the same group, the cement thickness was 50-70 µm.
However, no statistically significant difference was found between resin
cement thickness of the two groups.
The microscopic observation also showed hybrid layer formation at the
interface between resin and dentin of Group1 samples (Fig. 5). The hybrid
layer was 4-7 µm thick and many resin tags penetrating into the dentin
tubules were observed. The hybrid layer thickness clearly increased in each
sample moving from the cervical margin toward the axial wall (Fig. 6).
In the samples of Group 2 the hybrid layer was thinner than Group 1
between 0.5-4 µm (Fig. 7). In the cervical area, the hybrid layer thickness

107
was very thin (0.5 µm) or not detectable. Resin tag formation was also noted
(Fig. 8).
In both groups, close to the cervical margin, resin tag formation was rarely
seen. Only 200-300 µm from the cervical margin and moving towards the
inner dentin, resin tags were detectable.
Seldom, gap formation was noted between dentin substrate and bonding
system in the samples of Group 2 (Fig. 8) and between resin cement and
bonding system Group1.
At the enamel sites of the first groups, resin tags penetrating into the etched
enamel surface were observed (Fig. 9). The resin tags length was 5-8 µm.
At the cervical margin, all specimens of Group 4a, with margin located 1 mm
below the CEJ, presented an outer layer which was not identifiable as dentin
(Fig. 10). No open tubules were detectable in this area. The outer layer was
approximately 200-300 µm thick and consisted of a relatively thick inner
layer covered by a thin layer of cementum along the entire length of the
cervical margin. Moving inwards across the entire width of the gingival floor
of the proximal box, tubules cut in cross section were clearly visible. In the
samples of Group 5a, in which the cervical margin was located
approximately 0.5 mm above the CEJ, a thin enamel layer was visible. The
enamel prisms tented to be cut along their long axes (Fig. 11). The etched
patterns of the enamel layer was not uniform and frequently, areas without
characteristic enamel morphology were noted both at cervical (Fig. 11) and
axial margins (Fig. 12). Moving inwards across the entire width of the
gingival box, an outer dentin layer of 100-250 µm, similar to that observed in
Group 4 was also observed before finding dentin with cross-sectioned
tubules (Fig. 11). At the buccal and ligual margins, the enamel prisms were
mainly cut along their long axes and only close to the most occlusal area of
the buccal or lingual wall; prisms cut perpendicularly to their long axes were
noted and showed typical etch patterns.
The resin replica (Groups 4b and 5b) reproduced the morphology observed
in the micrographs taken on the empty cavities (Fig. 13). At the cervical

108
margin, it was very rare to observe resin tag formation. At the least after
200-300 µm from the cervical margin and towards the inner dentin, resin
tags were detected. At the edge of margins (cervically, buccally and
lingually) the resin reproduced the thin enamel layer (group 4a and 5a). The
enamel prisms at the margins presented a low level of structured
arrangement. The prisms, reproduced by the resin, were cut approximately
parallel to their long axis, both at cervical and lateral/occlusal margins.
Discussion Technical difficulties associated with the placement of the inlays has to be a
serious point of consideration in marginal integrity studies (Roulet JF, 1997).
In this study, the restorations of Group 1 free of leakage at the cervical
margins were of those inlays showing the thinnest resin cement thickness.
The presence of air bubbles within the material corresponded to the thickest
resin cement thickness and always to the highest leakage score. The
presence of bubbles may suggest that handling difficulties existed in mixing
the resin cement, placing and setting the inlays into the cavity during
cementing procedures. The thickness of resin cement and the presence of
bubbles can be also related to several properties of resin cement as its
viscosity and composition (Picard B et al, 1997).
The dye penetration was particularly observed at the cervical margins of
Groups 1 and 2: in this areas (Figs. 10, 13) the presence of an outer layer,
partially formed by cementum of 150-300 µm may affect the quality of
bonding when the margin is located below the CEJ (Cagidiaco MC, 1995;
Ferrari M & Davidson CL, 1996; Cagidiaco MC et al 1997). Although the
hybridisation of the cementum-dentin margins was demonstrated (Ferrari M
et al, 1997) and also showed in this study (Fig. 5), the absence of resin tags
in the first 200-300 µm from the cervical margin, determines no peritubular
dentin demineralisation and therefore, a limited increase of intertubular
surface area after conditioning (Pashley DH et al, 1995 ; Cagidiaco MC et al

109
1997) this can be responsible for a decrease of bond strength and,
consequently, of durability of the bonding to cavity margin. The outer layer is
partially formed by cementum, which is a hypo-mineralized hyperorganic
dentin matrix which has lost its tubular aspect. This outer layer is composed
of two different layers, the so called Tomes’ granular layer and hyaline layer
of Hopewell-Smith (Bradford EW, 1967) and by the outer part of dentin.
Blackwood (1957) pointed out that sound dentin can be separated from
cementum through a zone known as the “intermeditate cementum layer”,
which has not exhibit the characteristic features of either dentin or
cementum, and its formation is still unclear. The thickness of this layer
increases considerably in the apical direction (Vacel JS & Gher ME, 1993;
Bosshardt DD & Selving KA, 1997) . In the samples of Group 3b of this
study, the presence an “intermediate layer” or “outer layer” between sound
dentin and thin enamel cervical margin was also demonstrated.
A recent study performed with finite element analysis demonstrated that the
highest stresses are concentrated in the most external areas of cervical
walls of the Class II cavity (Apicella A et al, 1997). This stress concentration,
with values exceeding the strength of the materials, can contribute to
disruption of the seal at the cervical margin of Class II restorations.
From a clinical point of view, it seems that, if the bonding between adhesive
resin and the thin enamel layer at the cervical margin at the most external
area is broken and consequently infiltrated by bacteria, the “intermediate
layer” cannot stop the leakage of fluid and bacteria, causing post operative
sensitivity and secondary caries (Eick JD & Welch FH, 1986; Cox CF, 1994).
Resin replica technique also made it possible to study the cementum layer
(Cagidiaco MC, 1995). Replicas of Class II restoration done in this study
confirm the anatomical observations made directly on empty cavities. The
results of this investigation, which demonstrate the absence of resin tags in
the cervical area, reinforce the consideration that the cervical margins are
the weakest bonding area of Class II restorations (Ferrari M & Davidson CL,
1996). However, the superior sealing capacity of restoration which use the

110
latest dentin bonding systems, in comparison with the results obtained by
using the oldest systems, can be attributed to the hybridisation of the
conditioned substrate (Bayne SC et al, 1996). Many weak points on hybrid
layer formation were pointed out (Sano H et al 1995; Tay FR et al 1995; Tay
FR et al, 1997). Although it was demonstrated that from a quantitative view-
point the interfacial bond strength is not per se due to the infiltration of the
collagen rich zone (Wakabayashi Y et al, 1994; Gwinnett AJ, 1994; Kanca J,
1997), the qualitative role of hybrid layer on the marginal seal of Class V
restorations placed under clinical conditions was recently demonstrated
(Ferrari M et al, 1997; Vichi A et al, 1997).
Further research is needed to determine which bonding procedures, related
to different substrates, can be ideal for obtaining a perfect and durable seal
of Class II indirect aesthetic restorations.
In this study two bonding-cementing systems were evaluated. The
experimental bonding system used in Group 1 (EBS Multi and CLA 1.0b)
showed hybrid layer and resin tag formation along the interface between
adhesive material and conditioned dentin (Fig. 5). Because of vacuum
pressure during the procedures for preparing samples for microscopic
examination, and the negative pressure in the chamber of SEM, a gap
between hybrid layer and resin cement was sometimes noted. However, in
this area where gap formation was observed, the dentin tubules remained
sealed by resin tags. Recent investigations concluded that the most
important feature of resin tag formation in demineralised dentin is the resin’s
ability to plug the dentin tubules to the depth of funnelling produced by the
etching agent (Nakabayashi N et al, 1992; Pashley DH et al, 1993; Titley K
et al, 1995).
Probably because of these same reasons, a gap formation was also noted in
Group 2 samples (Figs. 8, 9) in which porcelain restorations were luted with
Syntaca bonding system and Variolink IIa resin cement. In the latest group,
the gap was mainly located between demineralised dentin and adhesive
system. This fact can be correlated with the thin hybrid layer probably due to

111
the high wettability of this enamel-dentin bonding system (Moello FS-TC et
al, 1996). For that reason, the bonding system of Group 1 may be
considered superior to that used in Group 2.
At the occlusal margins of Group 1, 2 and 3a samples, which were located in
the enamel, 70%-90% of restorations showed a perfect seal. Apparently, the
total etch technique using phosphoric acid etched tooth enamel sufficiently.
At the occlusal site of Groups 1, 2 and 3a, the thickness of the enamel was
between 1.0 and 1.8 mm and the prisms orientation probably permitted a
high bond level. When the enamel site of buccal and lingual cavity walls
were evaluated (Group 3b) the dye penetration considerably increased. This
is in agreement with the study by Hilton et al (1997). The high leakage score
was probably due to the fact that the enamel thickness ranged between 0.3
mm, more cervically, to 0.8-1.0 mm occlusally. Also, the enamel prisms were
mainly cut along their long axes, creating an etch enamel pattern less
retentive than when cut perpendicular to their long axes (Attal JP &
Degrange M, 1996 ; Dietschi D & Sperafico R, 1997). The interdependency
between enamel thickness and prisms orientation was noted, in such a way
that in thinner cervical enamel the prisms predominantly run straight, while in
thicker cuspal enamel they show a wavy path and their orientation towards
the enamel surface is predominantly oblique (Radlanski RJ et al, 1990;
Radlanski RJ, 1995). A higher bond strength to transverse cut enamel
prisms than to longitudinal sectioned prisms was found (Munecika T et al,
1984) and, for that, the wavy path of the prisms in human enamel is
assumed to lead to higher strength than a parallel structural pattern
(Fernandes CP, Chevitarese O, 1991; Martin T, 1997; Pfrentzschner HU,
1997). These facts may explain the higher dye penetration found at the
cervical (Group 3a), lingual and buccal (Group 3b) sitesthan that at occlusal
site (Groups 1,2).
The technique used in the present study of sectioning the leakage samples
of Group 1-3a allowed standardized visualization of the dye penetration
along the cervical and occlusal margins. While this is the most common

112
sectioning procedure for leakage test, which allows visualization of leakage
that penetrates down dentin tubules in a pulp ward direction, it does not
permit a three dimensional assessment of the leakage pattern. To evaluate
the leakage at axial walls of cavities, Group 3 samples were sectioned
approximately along the interface between buccal, lingual walls and indirect
restorations. Because the dye penetration was staining the axial cavity walls
mainly in an occlusal-pulpal direction, the leakage scores registered in this
areas were compared with the occlusal data of the first score of the same
samples. The dye penetration resulted more evident at the axial walls than
occlusally, and statistically significant differences were found between the
two groups. To ameliorate the dye infiltration reading, the demineralisation
was and clearing procedure advocated by Gwinnet et al (1995) can be
useful. However, the sample process performed in this study also permitted
the SEM evaluation of the same specimens after leakage scoring, the
possibility to correlate the leakage data with the morphological appearance
of the dental substrates and with bonding material behaviour. The statistical
evaluation of scores obtained in Group 3b at axial/occlusal site and cervical
margins of Groups1, 2, 3a and 3b showed no significant differences. For
that, the enamel axial walls of Class II cavities must be considered, from
clinical viewpoint, as one of the weakest margins in the cervical area of
Class II restorations.
This would seem to be in favour of placement of conservative bevels on the
enamel of the facial, lingual and cervical walls of Class II restorations
(Dietschi D et al, 1995;Hilton TJ et al, 1997). Unfortunately, with indirect
porcelain inlays, if a bevel is placed at the margins, it can produce unstable
margins, can fail at the margins and a bevelled ceramic inlays would be
difficult to fabricate. Clinical conditions cannot permit the bevel placement at
this margins without mechanically damaging the adjacent tooth and or the
root of the tooth interproximally. Beside the difficulties in making porcelains
restorations with bevelled margins, clinical experience has demonstrated the
low risk of marginal fracture when a butt-joint is made at the margin.

113
However, further long term assessment of Class II restorations is required to
determine their success addition to their excellent aesthetic qualities.
a. Vivadent, Schaan, Liechtenstein.
b. Espe, Seefeld, Germany.
c. Ivoclar, Schaan, Liechtenstein.
d. Nikon Ltd, Tokyo, Japan.
e. Balzer Ltd, London England.
f. Jeol Ltd, Tokyo, Japan.
This study was partially supported by ESPE GmbH and Research Center for
Dentistry/Tufts University, Boston, USA.
114
References
Anusavice KJ. Quality evaluation of dental restorations. Chicago:
Quintessance, 1989.
Apicella A, Raddi S, Ausiello P, et al. FEM study of shrinkage stress build-up
on adhesive restorations. J Dent Res 1997; 76: 49 (Abstr 435).
Attal JP, Degrange M. Influence de l’orientation des prismes et du traitment
de surface sur l’adhesion et l’adherence a l’email. J Biomater Dent 1996 ;
11 : 41-57.
Bayne SC, Heymann HO, Wilder AD, et al. Clinical performance of bonding
systems with and without hybrid layers. J Dent Res 1996; 75: 23 (Abstr 47).
Blackwood HJJ. Intermediate cementum. Br Dent J 1957; 102: 345-350.
Bosshardt DD, Selving KA. Dental cementum: The dynamic tissue covering
the root. Periodontal 2000 1997; 13: 41-75.
Bradford EW. Microanatomy and histochemistry of dentin. In: Miles AEW.
Structural and chemical organization of teeth. New York: Academic Press,
1967; Vol II, 49.
Branstrom M. Dentin and pulp in restorative dentistry. London: Wolfe
Medical Publ., 1982.
Branstrom M. Etiology of dentin Hypersensivity. Proc Finn Dent So 1992; 88
(Suppl. 1): 7-13.
Cagidiaco MC, Ferrari M, Vichi A, et al. Mapping of tubule and intertubule
surface areas available for bonding in Class V and Class II preparations. J
Dent 1997; 25: 379-389.
Cagidiaco MC. Bonding to dentin: Mechanism morphology and efficacy of
bonding resin composites to dentin in vitro and in vivo. Amsterdam,
University of Amsterdam, Ph D Thesis, De Batte Ed. 1995.
Cox CF. Evaluation and treatment of bacterial microleakage. AM J Dent
1994; 7: 293-295.

115
Dietschi D, Scampa G, Campanile U, et al. Marginal adaptation and seal of
direct and indirect Class II composite restorations: An in vitro evaluation.
Quint int 1995; 26: 127- 138.
Dietschi D, Sperafico R, Adesive metal-free restorations. Current concepts
for the esthetic treatment of posterior teeth. Berlin: Quintessence 1997.
Donly KJ, Jensen ME. Posterior composite Class II restorations: In vitro
comparison of preparation designs and restorations techniques. Dent Mater
1990; 6: 88-93.
Eick JD, Welch FH. Polimerization shrinkage of posterior composite resins
and its possible influence on postoperative sensitivity. Quit Int 1986; 17: 103-
111.
Feilzer AJ De Gee AJ, Davidson CL. Increased wall-to-wall curing
contraction in thin bonded resin inlays. J Dent Res 1989; 68: 48-50.
Fernandes CP, Chevitarese o. The orientation and directions of the rods in
dental enamel. J Prosthet Dent 1991; 65 : 793-800.
Ferrari M, Cagidiaco MC, Davidson CL. Resistence of cementum in Class II
and V cavities to penetration an adhesive system Dental Mater 1997; 13:
152-162.
Ferrari M, Davidson CL. Sealing performance of Scotchbond Multi-Purpose-
Z100 in Class II restorations. Am J Dent 1996; 9: 145-149.
Gwinnet AJ, Kanca J. Micromorphological relationship between resin and
dentin in vivo and in vitro. Am J Dent 1992; 5: 19-23
Gwinnett AJ, Tay FR, Pang KM, et al. Comparison of three methods of
critical evaluation of microleakage along restorative interfaces. J Prosthet
Dent 1995; 74: 575-585.
Gwinnett AJ. Chemically conditioned dentin: A comparison of conventional
and environment scanning electron microscopy findings. Dent Mater 1994;
10: 150-155.
Hilton TJ, Schwartz RS, Ferracane JL. Microleakage of four Class II resin
composite insertion techniques at intraoral temperature. Quit int 1997; 28:
135-144.
116
Kanca J Resin Bonding to wet substrate. I. Bonding to dentin. Quit int 1992;
23: 39-41
Kanca J. Investigation into dentin adhesion mechanism. J Dent Res 1997;
76: 277 (Abstr 2111).
Kanca J. Wet bonding: effect of drying time and distance. Am J Dent 1996;
9: 273-276.
Martin T. Schmeltzmikrostrukturen bei Saugetieren. In: Alt KW, Tucrp J. Die
evolution der zahne. Philogenie –ontogenie variation. Berlin: Quintessenz,
1997.
Moello FS-TC, Feiltzer AJ, De Gee AJ, et al. The influence of the presence
of a bonding layer on marginal sealing of resin composite Class II
restorations. J Dent Res 1996; 75: 26 (Abstr 224).
Munecika T, Suzuki K, Nishiyama M, et al. A comparison of the tensile bond
strengths of composite resins to longitudinal and transverse sections of
enamel prisms in human teeth. J Dent Res 1984; 63: 1079-1082.
Nakabayashi N, Ashizawa M, Nakamura M. Identification of a resin dentin
hybrid layer in vital human dentin created in vivo: Durable bonding to vital
dentin. Quit int 1992; 23: 135-141.
Nakabayashi N, Nakamura M, Yasuda N. Hybrid layer as dentin bonding
mechanism. J Esthet Dent 1991; 3: 133-138.
Pashley DH, Ciucchi B, Sano H, et al. Bond strenght versus dentine
structure: A modelling approach. Archs Oral Biol 1995; 40: 1109-1118.
Pashley DH, Ciucchi B, Sano H, et al. Permeability o dentin to adesive
agents. Quint int 1993; 24: 618-631
Pfrentzschner HU. Biomechanik des zanhschmelzes. In: Alt KW, Tucrp J.
Die evolution der zahne. Phylogenie-Ontogenie variation. Berlin Quintessenz
1997.
Picard B, Jardel V, Tirlat G. Ceramic bonding: Reliability. In Degrange M,
Roulet JF. Minimally invasive restoration with bonding. Chicago
Qiuntessence 1997; 103-127.

117
Radlanski RJ, Jager A, Seidi W, et al. Uber die ausrichtung der prismen im
zahnschmelz menschlicher permanenter zahne. Anat Anz 1990; 170: 329-
337.
Radlanski RJ. Prism arrangement in early layers in human fetal enamel. In :
Radlanski RJ, Renz H. Proceeding of the 10th international symposium on
dental morphology. Berlin: C & M Brunne, 1995.
Robinson PB, Moore BK, Swartz ML. Comparison of microleakage in direct
and indirect composite resin restorations in vitro. Oper Dent 1987;12: 113-
116.
Roulet JF. Longevity of glass ceramic inlays and amalgam-results up to 6
years. Clin Oral Invest 1997; 1: 40 -46.
Sano H, Takatsu T, Ciucchi B, et al. Nanoleakage within the hybrid layer.
Oper Dent 1995; 20 : 18-25.
Tay FR, Gwinnett AJ Pang KM, et al. Variability in microleakage observed in
a total-etch wet-bonding technique under different handling conditions. J
Dent Res 1995; 74: 1168-1178.
Tay FR, Gwinnett AJ, Wei Shy. Ultrastructure of the resin-dentin interface
following reversible and irreversible rewetting. Am J Dent 1997; 10: 77-82.
Thylstrup A, Bille J, Qvist V. Radiographic and observed tissue in approximal
carious lesions at the time of operative treatment. Caries Res 1986; 20: 75-
84.
Titley K, Chernecky R, Chan A, et al. The composition and ultrastructure of
resin tags in etched dentine. Am J Dent 1995; 8: 224-230.
Tyas MJ. Clinical performance of two dentin adhesives: 2-year results. Aust
Dent 1996; 41: 324-7.
Vacel JS, Gher ME. Cementum anomalies of the dentogigngival junction. Int
J Perio Dent 1993; 5: 443-449.
Van Merbeeck B, Peumans M, Verschueren M, et al. Clinical status of ten
dentin adhesive systems. J Dent Res 1994; 73: 1690-1702

118
Vichi A, Ferrari M, Davidson CL. In vivo leakage of an adhesive system with
and without NaOCl as preatreatment. J Dent Res 1997; 76: 398 (Abstr
3077).
Wakabayashi Y, Kondou Y, Suzuki K, et al. Effect of dissolution of collagen
on adhesion to dentin. Int J Prosthodont 1994; 7: 302-306.

119
Table 1. Experimental groups.
Group # Materials Margin
Location
No of
sections
Type of
investigation
1 ESPE 1 mm below
CEJ
1 ML/RCT/HLF
2 Vivadent 1 mm below
CEJ
1 ML/RCT/HLF
3a ESPE 0.5 mm
above CEJ
1 ML/RCT/HLF
3b ESPE 0.5 mm
above CEJ
3 ML/RCT/HLF
4a / 1 mm below
CEJ
/ MDO
4b ESPE 1 mm below
CEJ
1 Resin replica
5a / 0.5 mm
above CEJ
/ MDO
5b ESPE 0.5 mm
above CEJ
1 Resin replica
ML: Microleakage; RCT: resin cement thickness; HLF: hybrid layer formation; MDO:
Microscopic direct observation by SEM; Resin replica observation by SEM;

120
Table 2. Cementing procedures.
Product Bonding
System
Clinical
steps
Resin
cement
Clinical
steps
ESPEb
VivadentaEBS Multi
Syntac
a b c d
a b c d e
CLA 1.0
Variolink II
f g h i k l m n
f g h j k l m n a Enamel etching with phosphoric acid
b Dentin conditioning with phosphoric acid
c Primer application
d Adhesive application
e Heliobonda application
f Inlay etching with fluoridric acid
g Silanization of etched porcelain surface
h Heliobonda application
i Aplicap capsule application
j Mixing of resin cement
l Removing cement access
m Margins isolation with glycerine
n Light-curing
Table 3. Leakage scores, resin cement thickness at the cervical margins and the presence of
bubbles in cement of the three experimental groups (n=10).
Group1
0 1 2 3 4
Group 2
0 1 2 3 4
Group 3a
0 1 2 3 4
Group 3b
0 1 2 3 4
Occlusal 9 1 - - - 7 3 - - - 8 2 - - - 4 2 3 1 -
Cervical 4 2 1 2 1 3 3 2 1 1 5 1 2 2 - 4 1 2 3 1
Cement
thickness
92 µm
(SD:40)
68 µm
(SD:25)
Not
evaluated
Not
evaluated
Bubbles 2 at occlusal
area
3 at cervical
area
1 at occlusal
area
1 at cervical
area
Not
evaluated
Not
evaluated

121
Legends to illustrations
Fig. 1. Preparation characteristics of standard Class II cavity
Fig. 2. One section was made on Groups 1, 2 and 3a, and three sections were made on Group 3b

122
Fig. 3. Scale of cervical interfacial dye penetration.
Fig. 4. Scale of occlusal interfacial dye penetration.

123
Fig. 5. Hybrid layer formation at interface between resin cement and dentin (Group 1: EBS Multi, Espe). The hybrid layer thickness was 4-7µm. ( SEM x 2000; bar = 10 µm) (hybrid layer between arrows).
Fig. 6. Hybrid layer thickness increases from the cervical margin towards the pulpal wall (Group 1 EBS Multi, Espe) (SEM x 1000; bar = 10 µm) ( HL= Hybrid Layer; M= cervical Margin; T= resin Tags).

124
Fig. 7. Hybrid layer formed in a sample of Group 2 (Syntac, Vivadent). The thickness of the layer is of 3-4 µm ( SEM x 3500; bar= 10 µm) (Hybrid layer between arrows).
Fig. 8. Resin tag formation in a Group 2 sample ( Syntac, Vivadent) (SEM x 2000; bar= 10 µm).
Fig. 9. Resin tag penetration into the etched enamel of Group 1 sample (EBS Multi, Espe) (SEM x 2000; bar= 10 µm).

125
Fig. 10. At cervical margin located 1 mm below the CEJ, an outer layer not identifiable as sound dentin was detectable (SEM x 500; bar = 100 µm) (C= Cementum; D= Dentin; OL= Outer Layer).
Fig. 11. Cervical margin located 0,5 mm above the CEJ. The etched pattern was not uniform and the prisms tended to be cut along their long axes. Moving towards the pulpal wall, an outer layer of 250-300 µm was observed (SEM x 500; bar= 100 µm) (E= Etched Enamel; OL= Outer Layer; D= Dentin).

126
Fig. 12. Axial margin of a Class II cavity. The enamel prisms are cut along their long axes and the etched pattern is not uniform (SEM x 1000; bar = 20 µm) (UE= unprepared Enamel; E= Etched Enamel; CW= dentin Cavity Wall).
Fig. 13. Resin replica showing an empty cavity. The section goes from outer enamel to outer layer to dentin in a mesial-distal direction. Resin tags were not observed close to the cervical margin. (SEM x 500; bar= 100 µm) (E= Enamel; OL= Outer Layer; T= resin Tags formed on dentin).
127
Chapter 7
A clinical trial of Empress II porcelain inlays luted to vital abutments with the self-light-curing adhesive system Excite DSC and MultiLink. Abstract: Purpose: The aim of the study was to evaluate the quality
expressed in marginal integrity and sealing of Empress II inlays cemented
under clinical conditions with the self/light-curing Excite DSC and MultiLink
adhesive luting system. Materials and methods: Forty patients were
selected and each received one Empress II inlay. Empress II is a heat
pressed glass ceramic and contains lithium di-silicate and lithium ortho-
phosphate crystals, from which higher stress resistance and improved
strength is claimed. The restorations were placed within the time span March
2000 until May 2000. Recalls were performed after 6, 12, 24 and 36 months.
At the 3-year recall, seven patients were lost for this study. Inlays were
evaluated for postoperative sensitivity, marginal integrity, marginal leakage,
color stability, surface staining, retention, surface crazing (micro-cracks).
Results: At the 3-year recall, all restorations were still in place, no fracture of
any inlay was observed and only one restoration showed post-op sensitivity
(at the first recall, 1 week after placement). Only few inlays showed slight
marginal staining and gaps, with little surface staining and crazing, but no
inlay needed replacement. Conclusions: No inlay came loose or fractured
during the whole period of observation and all the inlays were still clinically in
service.
Patient‘s satisfaction was high and no hypersensitivity was present at three-
year recall.

128
Introduction Concern about the potential toxicity of amalgam fillings and their limited
anaesthetic aspect motivates a call for substitute restorative materials also
for the posterior area (Roulet JF, 1997). Resin-based composite, glass-
ionomer, and compomer direct restorations, as well as composite, porcelain
and gold inlays form the wide spectrum of options for more aesthetic and
biocompatible alternatives to amalgam. Disadvantages of above listed direct
restorative materials are setting shrinkage, limited color stability and limited
strength, eventually leading to leakage, decreasing esthetics and premature
fracture under stress. These undesirable deficiencies are less likely to arise
with indirect composite or porcelain restorations, which therefore are to be
preferred above the others, when aesthetics is a prerequisite. Other
advantages of the utilization of inlays in large cavities are enhanced
mechanical properties, better occlusal and inter-proximal morphology.
However, also these restorations have their limitations. Possible causes of
failure for indirect esthetic restorations are debonding (Sjögren G et al, 1998)
and bulk fracture of the chosen material (Banks RG, 1990).
There are many reason used to explain premature fractures of all ceramic
restorations (Kelly JR et al, 1996), such as uncorrect indications, limited
strength of the specific ceramic or, more often, insufficient thickness of the
inlay (Pallesen U, 1996) . The intrinsic weakness of ceramics is brittleness
due to the per se existence of numerous internal micro-cracks that, with time,
can propagate into connecting networks of cracks and consequently
fracture(Chen HY et al, 1999). Such premature failures represent a major
problem as they require replacement of restorations and constitutes
undesired additional workload in the dental office: in fact it represents around
60% of our daily work (Mjör IA, 1989).
Empress II, a lithium di-silicate and lithium orthophosphate reinforced glass
ceramic is proposed in order to extend the use of resin bonded ceramic
restoration even for bridges. Empress II derives its additional strength from

129
the microstructure that consists of many little interlocking needle-like crystals
randomly oriented, meant to arrest the propagation of micro-cracks through
the material.
Prerequisite for application of full porcelain inlays is perfect bonding, which
has to integrate all parts into one coherent structure (Davidson CL, 2001).
Therefore the luting material and technique, as well as the substrate
characteristics form success determining factors.
The aim of the study was to evaluate the sealing ability of Empress II inlays
cemented under clinical conditions with the self/light-curing adhesive system
Excite DSC and MultiLink resin cement.
Materials and methods
Forty patients were selected and each received one Empress 2 (Vivadent,
Schaan, Liechtenstein) inlay each. The selection of the patients followed the
next parameters:
1. Need for a Class II inlay, 2. Informed written consent of the patients.
Inclusion criteria Selection of male and female subjects was restricted to those aged 18-60
years and in good general and periodontal health.
Exclusion criteria Patients with the following factors were excluded from the clinical trial: 1)
Patients receiving drugs that modify pain perception, 2) pregnancy or breast
feeding, 3) eating disorders, 4) periodontal surgery, 5) orthodontic therapy in
the preceding three months, 6) teeth with carious lesions (after clinical and
radiographic examination) or restored in the preceding three months, 7)
extensively restored teeth (excessively wide Class II and/or Class V), 8)
allergy to drugs or chemicals used in the study materials, 9) active
periodontal disease, 10) patients spontaneously sensitive.

130
Test stimuli and assessment Before applying the adhesive material, pain measurement was performed
utilizing a simple pain scale based on the response method. Response was
determined to a one second application of air from a dental unit syringe (at
40-65 p.s.i. at approximately 20 oC) directed perpendicular to the root
surface at a distance of 2 cm and by tactile stimuli with a sharp #5 explorer.
The subject was asked to rate the perception of the sensitivity experienced
during this thermal/evaporative stimulation by providing mark on a visual
analog scale or line beginning at 0 and ending at 10 (where 0=no pain and
10=excruciating pain). In order to translate these scores to easily understood
pain levels a score of 0 was defined as no pain, 1-4 as mild sensitivity (which
was provoked by the dentists’ air blast) and 5-10 as strong sensitivity (which
was spontaneously reported by the patient during drinking, eating, etc.).
At baseline all patients were tested for dentin sensitivity. The same
measurement was performed again at each recall. The status of the gingival
tissues adjacent to the test sites was observed at baseline and at each
recall.
Clinical Procedure After suitable teeth have been chosen, clinical photographs were taken and
set aside for later use. After anesthesia, the preparation was made. All
carious structures were excavated, any restorative material was removed.
Inlay preparation was achieved using conventional diamond burs in a high-
speed hand-piece; preparation was dictated by extent of decay, extent of
pre-existing restoration. At the end of preparation all cervical margins of the
cavities were located below the cementum-enamel junction (approximately
1.0 mm below the CEJ). The Residual Dentin Thickness (RDT) was
evaluated by x-ray and abutments with RDT thinner than 0.5 mm were
excluded.

131
After preparation, impression was taken with a poly-vinyl-siloxane material
(Virtual, Vivadent, Schaan, Liechtenstein) and sent to the technician .
Lab works were performed strictly following manufacturer’s instructions. At
the moment of cementation no liner was applied; dentine and enamel
surfaces were conditioned with 37% phosphoric acid gel for 20 seconds ,
washed with water and then gently dried; Excite DSC (Vivadent, Schaan,
Liechtenstein) self-curing was applied in one layer; MultiLink (Vivadent,
Schaan, Liechtenstein) resin cement was used following manufacturer’s
instructions; Empress 2 (Vivadent, Schaan, Liechtenstein) inlays was made
of glazed core material (Staining technique). The internal surface of
Empress 2 (Vivadent, Schaan, Liechtenstein) was etched with fluoridric acid,
rinsed,dried and silanated (Monobond, Vivadent, Schaan, Liechtenstein)
.The restorations were placed within the time span March 2000 until May
2000. The inlays were next examined by the same operator at different
periods. The patients were recalled before the end of November 2000 in
order to complete the data on post-operative sensitivity. The post-operative
sensitivity was evaluated after 1, 7 and 30 days.
Then, they were recalled after 6 and 12, 24 and 36 months. During the
recalls, it was attempted to collect data on post-operative sensitivity, stability
and longevity by assessing the restorations regarding the following aspects:
postoperative sensitivity, marginal leakage, marginal integrity, color stability,
surface staining, retention, surface crazing (micro-cracks).
The following methodology was utilized in the evaluation process:
1. Postoperative Sensitivity (assessed both with sharp #5 explorer and
with cold and warm stimuli): a) Absent; b) Present.
2. Color stability: a) No mismatch; b) Slight discoloration not requiring
replacement; c) Discoloration requiring replacement.
3. Marginal integrity (assessed both digitally with sharp #5 explorers and
visually): margins a) Excellent continuity at the restorative/tooth
interface; b) Slight ledge or ditch at the interface: c) Visible marginal
ditch or ledge or actual separation of interface.

132
4. Marginal leakage: a) Excellent continuity at the restorative/tooth
interface, no discoloration; b) Slight discoloration at the interface; c)
Moderate discoloration at the interface measuring 1 mm or greater or
recurrent decay at margins.
5. Surface staining: a) Absent; b) Present.
6. Retention: a) Present; b) Partial loss; c) Absent
7. Surface crazing (Micro-cracks): a) Absent; b) Slight crazing not
requiring replacement; c) Crazing requiring replacement
Results
The results at 3-year recall are summarized in table 1. The ceramic
restorations were made and placed following manufacturer’s instructions.
Experimental temporary resin cement was used (Fermit with chlorhexidine.,
Vivadent, Schaan, Liechtenstein). No particular discomfort was noted by the
patients. The temporary restorations remained approximately 1 week in the
mouth of the patients. The materials were a little too sticky (when used with
metallic hand instruments). In order to keep in place the temporary
restorations for, at least few days, in wide cavities the temporary material
was light cured, removed, refined and finally cemented with temporary no-
eugenol cement. It was possible to recall the patients in order to collect 1-
month data. The use of self-activating microbrush and MultiLink dual-curing
resin cement (Vivadent, Schaan, Liechstenstein) was very useful. The
setting time of the resin cement was directly correlated to room temperature,
glass plate temperature and, of course, mouth temperature. The setting time
is probably a little too fast for common practitioner (the material sets within
1.30 - 2 min.).
After 3 years all the restorations were still in place so the survival rate was of
100%.

133
At 3-year recall, seven patients did not come back to the office (the same of
the 2-year recall plus 3 other). For that, the results are based on 33
restorations instead 40.
Only one restoration showed post-op sensitivity at the first recall (1 week).
The patient referred immediately after cementing procedure post-op
sensitivity, which disappeared after 3 weeks. No post-op sensitivity was
present in the patients rechecked.
All the restorations were still in place at the 3-year recall.
Only four restoration scored C about marginal leakage, which means they
had moderate discoloration at the restorative-tooth interface measuring 1
mm or greater or recurrent decay at margins.
Also marginal integrity was good and only 3 inlays showed visible marginal
ditch or ledge and interface between the restoration and tooth. The color
stability was excellent, while only 3 restorations had little surface staining.
About surface crazing at 3 year recall 2 inlays presented slight crazing not
requiring replacement.
All the data are reported and summarized on Table 2.
Discussion It is hard to compare longevity of different types of restorations, mainly
because of differences in clinical procedures, different study designs and non
comparable materials. However even with these limitations it is possible to
get certain indications from the comparison of all the clinical studies
available. A first extrapolation learns that ceramic inlays are considered as a
safe kind of restoration and that they are reported to last longer than any
other esthetic indirect restoration (Manhart J et al, 2000). Yet,
notwithstanding the inlay material, debonding and thus microleakage at the
gingival margins, particularly where the outline is located under the
cementum- enamel junction cannot completely be prevented (Alavi AA &

134
Kianimanesh N, 2002). All these factors are related to three subjects: patient,
dentist and material(Hickel R & Manhart J, 2001).
In the present study, a new glass ceramic containing a high volume of
lithium di-silicate and lithium-ortho-phosphate crystals, which claims higher
stress resistance and in improved strength, marketed as Empress II
(Vivadent, Schaan, Liechstenstein) was used.
During this study no restoration fractured, confirming the enhanced strength
of this material and its good performance in comparison with data of other
ceramics as reported in other studies (Molin MK & Karlsson SL, 2000) .
Another aspect of this new ceramic system was the observed accurate fitting
of the inlay, even if this property was not explicitly measured. Ideal values of
all porcelain fit still has to be defined (Davidson CL, 2001) but this aspect
requires attention. In several studies it had been reported (Kawai K et al,
1994, Guzman AF et al, 1997) that the marginal wear of composite luting
cement can undermine the mechanical support. To prevent excessive
marginal wear, it is therefore mandatory to have the narrowest gap between
cavity preparation and ceramic restoration. Optimal fit (ranging from 50 to
100 µm) is to be preferred (Audenino G et al, 1999), particularly if the inlay
extends under the cementum-enamel junction (Hahn P et al, 2001). The
post-op sensitivity with this system was satisfactory: only a patient reported
sensitivity at baseline that disappeared after few days. No patient referred
pain or sensitivity in the next recalls.
This observation is in contrast with a study that reports hypersensitivity to be
the most common post-op complication (Millediing P et al,1995).
The utilization of a correct bonding technique is mandatory to achieve good
clinical results on luting ceramic inlay (Frankenberger R et al, 2000). The
dual cure dental adhesive application allows a good polymerisation even
under a thick layer of ceramic. In fact incomplete transmission of the curing
light through the ceramic restoration can compromise polymerisation of the
only light-curing adhesive system (Lee IB & Um CM, 2001). In direct resin
restorations, light curing the bonding agent prior to insertion of the

135
composite is routine. In ceramic luting procedures this pre-curing of the
resin-based adhesive is also considered as an important step, but can lead
to interfere with complete seating of the ceramic inlay (Hahn P et al, 2000)
and therefore clinicians might wrongly choose to cure bonding agent and
cement in one step. So it can be helpful to use a dentin bonding agent that
does not need any pre-polymerisation. To prevent these problems, in the
present study a dual-curing cement was chosen for luting the inlays. Dual-
cure cements offer a safe and a good degree of conversion also at sites
where light-curing might be hindered as is the case with thick inlays. In
recent studies it was reported that inlays luted with chemical-cure cements
performed better than inlays luted with dual-cure ones (Studer S et al,
1996; Van Dijken JWV et al, 1998). However it has to be emphasized that
when inlay margins are in cementum, perfect margins and perfect seal is
still very difficult to achieve (Haller B et al, 2003). In addition, the absence
of any coming loose of the observed inlays confirmed acceptable adhesion
of the system.
At three years recall, 4 restorations scored C for marginal leakage and 3
scored C for marginal integrity. This observation that reveals decreasing
marginal quality with aging due to either marginal wear of the luting cement
or other forms of degradation was for us not a reason for replacement in
accordance with literature (Molin MK & Karlsson SL, 1996). Another
compromising factor for perfect seal was that cavity extension was in all
cases in areas with high probability of micro- infiltration so a marginal
leakage was possible to occur (Ferrari M et al, 1999). These restorations are
still in place and capable of further clinical service and do not require
replacement.
A further aspect to evaluate was color stability and surface staining. In
general, the high chemical stability of ceramics guarantees good color
stability and eventually only mild surface staining. In this respect ceramics
are far superior to composite direct or indirect restorations (Wassell RW et
al, 2000) .

136
At three years recall all Empress II inlays perform clinically satisfactory,
which agrees with literature (Felden A et al, 1998; Kramer N et al, 1999;
Manhart J et al, 2001).
Conclusions After 3-year period of service, the following conclusions can be drawn:
Seven out of 40 patients were lost.
No inlay came loose during the whole period of observation and all the
inlays were still clinically in service.
No fracture was observed.
After 3 years moderate discoloration and visible marginal ditching were
present in some of the restorations that were still rated satisfactory. Slight
crazing and little surface staining were also reported after 3 years. Patient‘s
satisfaction was very high whilst no hypersensitivity was present. The results
of this three-year study are in accordance with the other lately published
prospective studies and exhibit good clinical performance of the Excite
DSC/Multilink/Empress II system over a 3 years survey period.
137
References Alavi AA, Kianimanesh N. Microleakage of direct and indirect composite
restorations with three dentin bonding agents. Op Dent 2002; 27: 19-24.
Audenino G, Bresciano ME, Bassi F, Carossa S. In vitro evaluation of fit of
adhesively luted ceramic inlays. Int J Prosthodont 1999; 12: 342-347.
Banks RG. Conservative posterior ceramic restorations: a literature review. J
Prosthet dent 1990; 63(6): 619-626).
Chen HY, Hickel R, Setcos JC, Kunzelmann KH. Effects of surface finish and
fatigue testing on the fracture strength of CAD/CAM and pressed ceramic
crowns J Prosthet Dent 1999; 82: 468-475.)
Davidson CL. Luting Cement, the Stronghold or the Weak Link in Ceramic
Restorations. Advanced Engineering Materials 2001, 3, 10: 763-767.
Felden A, Schmalz G, Federlin M, Hiller KA. Retrospective clinical
investigation and survival analysis on ceramic inlays and partial ceramic
crowns: results up to 7 years. Clin Oral Invest 1998; 2: 161-167.
Ferrari M, Mason PN, Fabianelli A, Cagidiaco MC, Kugel G, Davidson CL.
Influence of tissue characteristics at margins on leakage of class II indirect
porcelain restorations. Am J Dent 1999; 12: 134-142.
Frankenberger R, Kramer N, Petschelt A: Technique sensitivity of dentin
bonding: effect of application mistakes on bond strength and marginal
adaptation. Oper Dent 2000; 25: 324-330.
Guzman AF, Moore BK, Andres CJ. Wear resistance of four luting agents as
a function of marginal gap distance, cement type and restorative material. Int
J Prosthodont 1997; 10:25-30.
Hahn P, Attin T, Gröfke E, Hellwig E. Influence of resin cement viscosity on
microleakage of ceramic inlays. Dent Mat 2001; 17: 191-196.
Hahn P, Schaller HG, Hafner P, Hellwig E. Effect of different luting
procedures on the seating of ceramic inlays. J Oral Rehabil 2000; 27: 1-8.

138
Haller B, Häßner K, Moll K. Marginal adaptation of dentin bonded ceramic
inlays: effect of bonding systems and luting resin composites. Op Dent 2003;
28-5: 574-584.
Hickel R, Manhart J. Longevity of dental restorations in posterior teeth and
reasons for failure. J Adhesive Dent 2001; 3:45-64.
Kawai K, Isemberg PD, Leinfelder KF. Effect of gap dimension on composite
cement wear. Quintessence Int 1994; 25: 53-58.
Kelly JR, Nishimura I, Campbell SD. Ceramics in dentistry: historical roots
and current prospectives. J Prosthet Dent 1996; 75: 18-32.
Kramer N, Frankenberger R, Pelka M, Petschelt A. IPS Empress inlays and
onlays after four years- a clinical study. J Dent 1999; 28: 325-331.
Lee IB, Um CM. Thermal analysis on the cure speed of dual cured resin
cements under porcelain inlays. J Oral Rehabil 2001; 28: 186-197.
Manhart J, Chen HY, Neuerer P, Scheibenbogen-Fuchsbrunner A, Hickel R.
Three-year clinical evaluation of composite and ceramic inlays. Am J Dent.
2001;14(2): 95-99.
Manhart J, Scheibenbogen-Fuchsbrunner A, Chen HY, Hickel R. A 2-year
clinical study of composite and ceramic inlays. Clin Oral invest 2000; 4: 192-
198.
Millediing P, Örtengren U, Karlsson S. Ceramic inlay systems: some clinical
aspect. J Oral Rehabil 1995; 22: 571-580.
Mjör IA. Amalgam and composite resin restorations: longevity and reasons
for replacement. In: Anusavice K, Quality evaluation of dental restorations,
Chicago Quintessence 1989: 61-80.
Molin MK, Karlsson SL. A 3- year clinical follow-up study of a ceramic
(Optec) inlay system Acta Odontol Scand 1996; 54: 145-149.
Molin MK, Karlsson SL. A randomized 5-year clinical evaluation of 3 ceramic
inlay systems. Int J Prosthodont 2000; 13: 194-200.
Pallesen U. Clinical evaluation of CAD/CAM ceramic restorations: 6-years
report in CAD/CAM esthetic dentistry. Cerec 10 year anniversary
symposium. (Ed Mormann) Quintessenz Berlin 1996: 241-253.

139
Roulet JF Benefits and disadvantages of tooth-coloured alternatives to
amalgam J Dent 1997; 25:459-473.
Sjögren G, Molin M, van Dijken JWV. A 5-year clinical evaluation of ceramic
inlays cemented with dual-cured or chemically cured resin composite luting
agent. Acta Odontol Scand 1998; 56: 263-267.
Studer S, Lehner C, Brodbeck U, Shärer P. Short-term results of IPS
Empress inlays and onlays. J Prosthodont 1996; 5: 277-287.
Van Dijken JWV, Höglund-Åberg C, Olofsson AL. Fired ceramic inlays: a 6-
year follow up. J Dent 1998; 26: 219-225.
Wassell RW, Walls AWG, McCabe JF. Direct composite inlays vs
conventional composite restorations: 5-year follow-up. J Dent 2000; 28: 375-
382.
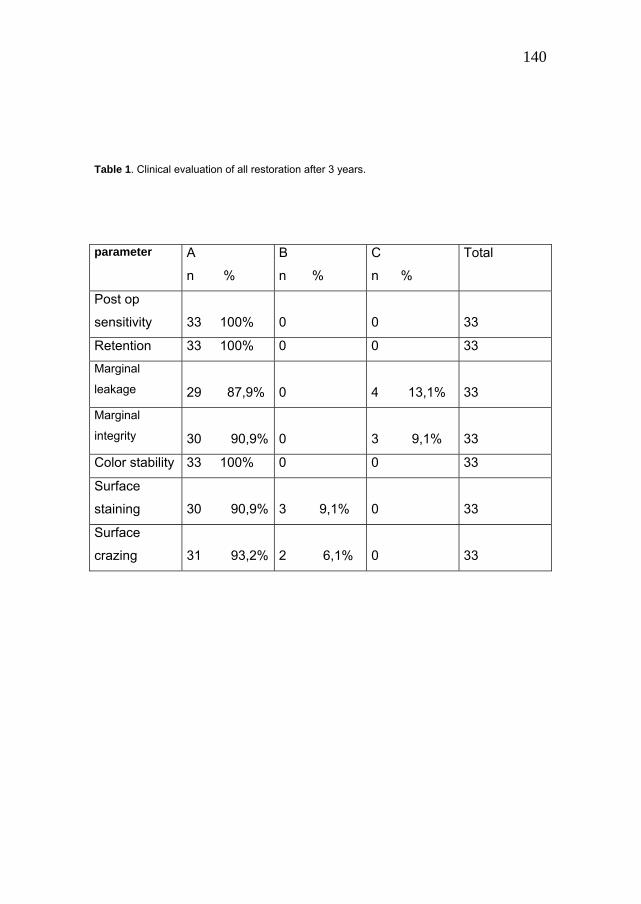
140
Table 1. Clinical evaluation of all restoration after 3 years.
parameter A
n %
B
n %
C
n %
Total
Post op
sensitivity
33 100%
0
0
33
Retention 33 100% 0 0 33
Marginal
leakage
29 87,9%
0
4 13,1%
33
Marginal
integrity
30 90,9%
0
3 9,1%
33
Color stability 33 100% 0 0 33
Surface
staining
30 90,9%
3 9,1%
0
33
Surface
crazing
31 93,2%
2 6,1%
0
33

141
Table 2. Clinical evaluation of all restorations at each recall
Post-operative sensitivity (n=40)
Absent A Present B Not recalled
Baseline 39 (96 %) 1 (4%)
1 week 40 (100 %)
1 month recall 40 (100 %)
5-6 month recall 40 (100 %)
12 month recall 38 (100%) 2
24 month recall 36 (100%) 4
36 month recall 33 (100%) 7
Retention (n=40)
Present A Partial loss B Completely loss C
Baseline 40 (100%)
1 month 40 (100%)
5-6 month recall 40 (100%)
12 month recall 38 (100%)
24 month recall 36(100%)
36 month recall 33(100%)

142
Marginal leakage (n=40)
A B C
Baseline 40 (100%)
1 month 40 (100%)
5-6 month recall 40 (100%)
12 month recall 36 (92.4%) 2 (7.6%)
24 month recall 34 (94,4%) 2 (5,6%)
36 month recall 29 ( 87,9%) 4(12,1%)
Legends: A= excellent continuity at the restorative-tooth interface, no
discoloration; B= Slight discoloration at the interface; C= Moderate
discoloration at the restorative-tooth interface measuring 1 mm or greater or
recurrent decay at margins.
Marginal Integrity (n=40)
A B C
Baseline 40 (100 %)
1 month 40 (100 %)
5-6 month recall 40 (100%)
12 month recall 37 (96.2%) 1 (3.8%)
24 month recall 34 (94,4%) 2 (5,6%)
36 month recall 30 (90,9%) 3( 9,1%)
Legends: A= excellent continuity at the restorative-tooth interface, no ledge,
no discoloration; B= Slight ledge or ditch at the interface detectable with
explorer; C= Visible marginal ditch or ledge or actual separation of interface
between the restoration and tooth.

143
Color stability (n=40)
A B C
Baseline 40 (100 %)
1 month 40 (100 %)
5-6 month recall 40 (100%)
12 month recall 38 (100%)
24 month recall 36 (100%)
36 month recall 33 (100%)
Legends: a) No mismatch; b) Slight discoloration not requiring replacement;
c) Discoloration requiring replacement
Surface staining (n=40)
A B
Baseline 40 (100 %)
1 month 40 (100 %)
5-6 month recall 40 (100%)
12 month recall 37 (96%) 1 (3.8%)
24 month recall 35 (97,2%) 1 (2,8%)
36 month recall 30 (90,9%) 3( 9,1%) Legends: a) Absent; b) Present.
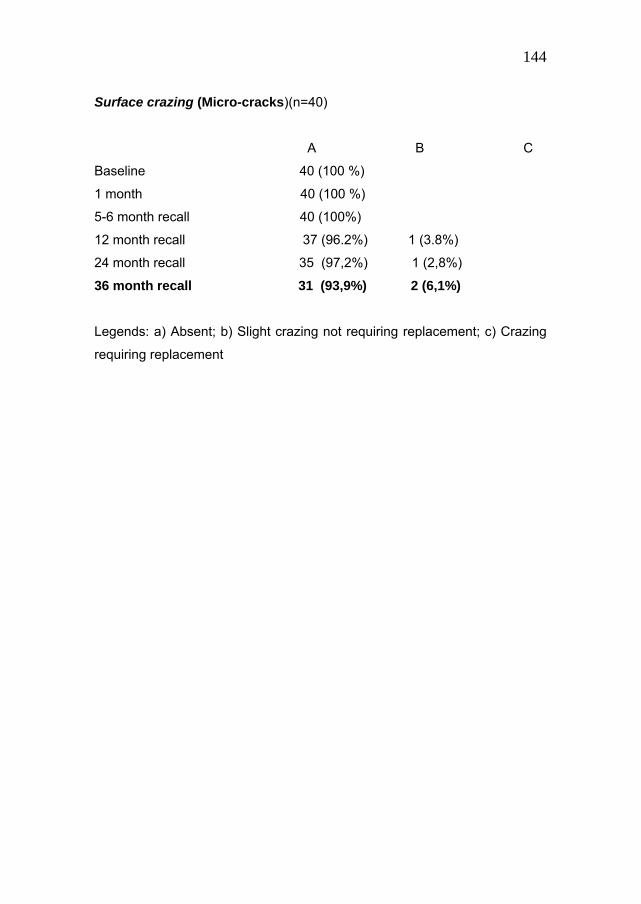
144
Surface crazing (Micro-cracks)(n=40)
A B C
Baseline 40 (100 %)
1 month 40 (100 %)
5-6 month recall 40 (100%)
12 month recall 37 (96.2%) 1 (3.8%)
24 month recall 35 (97,2%) 1 (2,8%)
36 month recall 31 (93,9%) 2 (6,1%)
Legends: a) Absent; b) Slight crazing not requiring replacement; c) Crazing
requiring replacement

145
Legends to illustrations Fig 1: Pre-op : a mod inlay will be prepared on tooth 15 for a mesial and distal decay
Fig 2: inlay preparation
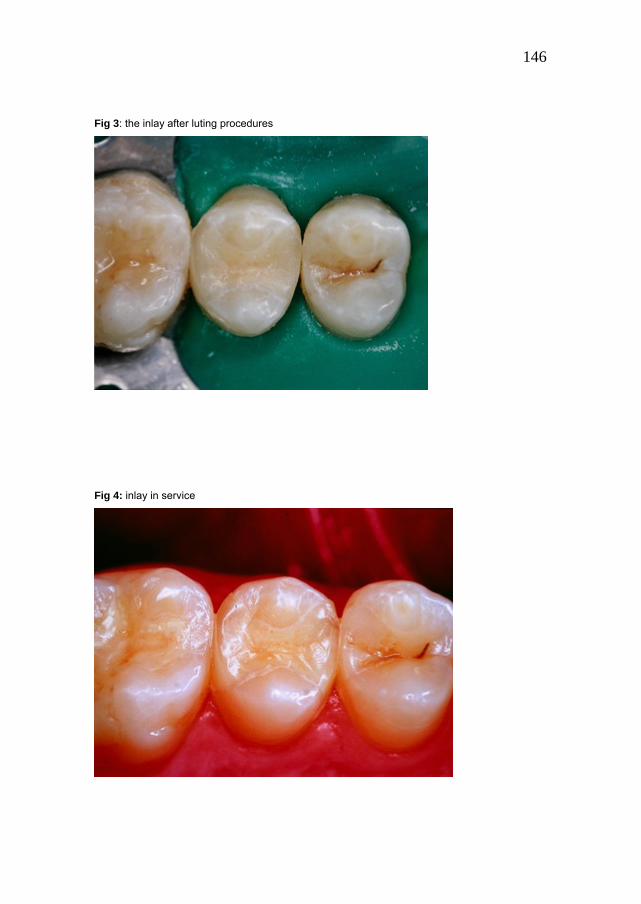
146
Fig 3: the inlay after luting procedures
Fig 4: inlay in service

147
Chapter 8
Leakage and SEM evaluation of in vitro Class V cavities restored with diverse materials.
Abstract: Purpose: This in vitro study evaluated the marginal integrity of
standardized Class V cavities, restored with 3 different sorts of filling
materials. Materials and Methods: In each experimental Group (n=12) a
different restorative material was employed. Group 1: gold foil; Group 2:
amalgam; Group 3: resin-based composite in addition with a three steps
dentin bonding system. After storage and thermo-cycling, a leakage test was
carried out and dye penetration scoring was performed at the cervical
margins of each specimen. The differences in microleakage score were
tested for statistical significance comparing all Groups, (Kruskal-Wallis Non-
Parametric ANOVA and Tukey test, p<0.05). SEM observations of the tooth-
restoration interfaces were also performed in each Group. Results:
Amalgam had the worst marginal integrity. The sealing ability exhibited by
gold foil and composite resin was satisfactory and statistically superior to
amalgam. Conclusion: Gold foil and composite resin perform equally regard
to microleakage and achieve better sealing ability than amalgam.

148
Introduction
Improved dental care, preventive programs and longer life have changed the
disease pattern of decay processes (Krejci I & Lutz F, 1991).
Also gingival recessions, occlusal inhabits, inappropriate tooth brushing and
several scaling and root planning may lead to promote cervical loosening of
substance where root caries may develop (Rees JS, 1998 ; Schüpbach P et
al, 1989).
The gingival area may be affect by carious and non-carious lesions.
Cervical non-carious lesions may develop as loss of dental substance at
cementum-enamel level for erosive and abrasive reasons (Ibbetson R &
Eder A, 2000).
Also cuspal flexure due to occlusal loads may generate stresses at
cementum-enamel margins, with disruption of hydroxyapatite crystals and
loss of enamel (Lee WC & Eakle WS, 1984).
While little non-carious cervical lesions, without any symptom, can be
treated only with occlusal adjustment, oral hygiene instructions and dietary
suggestions, deep sensitive defects and caries affected lesions have to be
treated, in order to stop progression, solve symptomatology and avoid pulp-
disease (Hickel R, 1994).
To restore this kind of lesion many restorative materials were proposed
through dental history: amalgam (Wood R et al, 1993), gold (Stibbs GD,
1980; Medina J, 1969), resins based composite (Ianzano JA & Gwinnett AJ,
1993), glass ionomer cements (Powell LV et al, 1992), compomer (Sjodin L
et al, 1996).
Demand for tooth-coloured restorations rather than anaesthetic metallic
fillings is increasing day by day (Federatin Dentaire Internationale, 1995).

149
Resin-based composite materials are the most common alternatives to
amalgam or gold and the use of resin based composite in Class V cavities is
an actively developing technology.
In this study we wanted to compare the quality of resin-based composites in
the Class V cavity with the established materials amalgam and gold.
Gold foil restorations are known as high quality and most lasting dental
provisions. It is remarkable that literature is scarce on successful treatments
and abundant on failures. Although we know by experience about the
success of compacted gold restorations in Class V situations and composite
in Class IV we cannot find too much reference on this, whilst there are
countless articles on the problems with composites in the Class V situation.
The cervical gold foil restoration it is time consuming, expensive, requires an
extensive non conservative preparation, needs a very skilled operator and,
above all, in our society, it’s absolutely not aesthetic. On the other hand gold
foil needs one chair session only, is biocompatible, has a thermal expansion
coefficient similar to enamel and has an excellent stability with time.
Amalgam used to be the standard material for Class V fillings for its
effectiveness, low cost, easy to use. Drawbacks are poor aesthetics, non
conservative preparation, need of macro mechanical retentions, and a still
questionable biocompatibility (Dodes JE, 2001).
Resin-based composites are nowadays the most common materials to
restore Class V lesions.
Their utilization in association with minimal invasive treatment, conservative,
adhesion with dentin bonding systems, permits to have highly aesthetic and
quite reliable restorations (McCoy RB et al, 1998; Manhart J et al, 2001),
however the complex morphology of this type of cavity and dentin leads
unpredictable preservation of the cervical sealing (Dietrich T et al, 1999;
Ferrari M & Davidson C, 1996; Schuckar M & Geurtsen W, 1997; Cagidiaco
MC & Ferrari M, 1995; Van Meerbeck B et al, 1994).

150
In box like Class V cavities the relation between bonded and free surfaces is
unfavourable (high C factor) whereby flow is restrained, which raises
shrinkage stresses (Davidson CL, 1986; Feilzer AJ et al, 1987).
Another problem related to Class V restorations is the location of its apical
margin. If it is positioned near the gingiva, serious control of saliva and
bleeding is essential and application of rubber dam becomes obligatory
(Penschke A et al, 2000).
The interface between restoration and dental substrate is an area of clinical
concern that can result in gap formation, marginal discoloration, leakage,
post-operative sensitivity, pulpits, recurrent decay and loss of retention
(Bränström M &Vojinovic, 1976; Sparrius O & Grossman ES 1989).
The aim of this study was to convey a quality of Class V restorations by
qualitative SEM observations along the margins and quantitatively
evaluating the sealing capacity of the various materials expressed in degree
of dye penetration at the restoration-tooth interface.
Materials and methods
Thirty six extracted sound molars and premolars were collected for this
study. The selected teeth were hand-scaled, cleaned with slurry of pumice,
and stored in distilled water at room temperature until use in the experiment.
Teeth were randomly divided into three Groups of twelve specimens each.
Standardized Class V cavities were prepared under copious water spray,
with diamond burs in a high-speed hand-piece, with upper margins in
enamel and lower margins in cementum. The occlusal margins of the cavity
had 4 mm length, the gingival margins had 3 mm length, with a traditional
trapezoid aspect of the cavity. The dept of the cavities was 2 mm.
The dimensions of the prepared cavities were checked with a Boley gauge.
A ±0.3 mm tolerance in the measurements was considered acceptable for
including the specimen in the trial. Butt margins were created in cavities
meant to receive gold foil restorations and amalgam restorations (Groups 1

151
and 2), whereas on the teeth to be restored with composite resins (Group3),
a bevel was added at the preparation margins on enamel; all the specimens
were stored in distilled water.
In Group 1 cavities were filled with gold foil only( Williams Gold Foil, Ivoclar,
Amherst, NY, USA, lot 98397B090696): no base was added to protect the
cavity, and all the specimens were prepared by the same operator. After the
complete filling of the cavity the outer face of the restorations were
burnished with a Spratley burnisher , finished with Moore discs (E C Moore
Company, Inc. Dearborn, 48126 MI) of decreasing abrasiveness and
polished with pumice and tin oxide.
The instruments used are listed in table I.
In Group 2 cavities were filled with a non-gamma 2 (Phasalloy, Wykle
Research ,Larson City NV, USA; lot 1194): no base was added and a very
accurate polishing was performed. Even in this group there was only one
operator performing the fillings. In Groups 3 cavities were filled with
composite resins. After 20 seconds of total etch, rinsing and gentile drying,
a three steps dental adhesive (Scotchbond MPS,3MESPE St Paul, MN
55144, USA, 7540 S) was employed (table II) and a flowable composite
resin (Filtek Flow, 3MESPE St Paul, MN 55144, USA, 3700 A3 3FB) was
used as elastic base.
The outer composite material was a hybrid composite resin (Filtek 250,
3MESPE St Paul, MN 55144, USA, 6020 A3 3CF).
All photo-curing materials were light-cured with a light-curing unit (3MESPE
St Paul, MN 55144, USA) for the required time.
The bonding systems and restorative materials were used following strictly
manufacturers' instructions. Once the restorations were completed and
submitted to 500 thermo-cycling each with a dwell time of 20 s. at 5 and 55
Co , the specimens were coated with two layers of nail varnish up to 2 mm
from the margin of the restorations. After a 24-hour immersion in a 2%
methylene blue solution each tooth was embedded in acrylic resin and
sectioned longitudinally with a low-speed diamond saw (Leitz 1600, Munich,

152
Germany) at three different levels perpendicular to the restoration in a
bucco-lingual direction (Fig. 1). The first cut was positioned in the middle of
the restoration, and the other ones mesial and distal.
Dye penetration at the cervical margin of the cavity was quantified according
to the following score method: 0 = no penetration; 1 = leakage not exceeding
the middle of the cervical wall; 2 = penetration past the middle of the cervical
wall; 3 = penetration to the axial wall; 4 = penetration to and along the axial
wall and into the dentinal tubules (Fig 2). Two operators observed the
sections separately by means of an optical microscope at 20 magnifications
(Bausch&Lomb, Rochester, NY, USA). In case of a disagreement between
the two investigators on the score assigned to a certain specimen, the worst
(higher) score was chosen for the statistical analysis.
Statistical analysis The results of the staining measurements were statistically evaluated using
Kruskal-Wallis Non-Parametric ANOVA by ranks with Bonferroni alpha
protection. The Tukey test was applied for multiple comparisons. All of the
statistical tests were run by the Winks 4.62 software (Texasoft, Cedar Hill,
Texas, USA), setting the level of significance at p<0.05.
SEM evaluation After scoring the specimens for dye penetration, in each Group one section
per tooth was chosen at random to be observed with the scanning electron
microscope (Philips 515, Philips, Eindhoven, Netherlands). The purpose of
the SEM analysis was to assess the integrity and continuity of the tooth-
restoration interfaces. Specimen preparation for SEM involved a gentle
decalcification with a 37% phosphoric acid solution for 10 s., followed by de-
proteinization with a 2% sodium hypo chlorite solution for 1 minute. Finally,
the specimens were mounted on an aluminum stub with a colloid silver paint,
and sputter coated with gold-palladium (Edward’s Coater S105B, London,
England).

153
Results
Leakage observations Frequency of recording of the microleakage scores for the different
combinations of restorative materials are given in Table III.
When comparing all of the combinations on trial (Graph 1), it appeared that
the amalgam Group had the worst microleakage score. In general, gold foil
Group and composite restoration Group gave a better seal than amalgam
Group.
The difference in microleakage between gold foil and composite restoration
Groups and amalgam Group were statistically significant (p<0.001).
As regards using gold foil or resin restoration, the results were not
significantly different (p>0.05) at the cervical margin and also at the occlusal
one.
Microscopic observations As expected, the typical features of adhesion, such as the formation of a
hybrid layer at the interface between restoration material and dental
substrate, were absent from the SEM views of specimens with amalgam and
gold foil. On the other hand, an excellent adaptation between gold foil and
dental substrate was visible in the specimens. (Fig. 3 a,b).
The typical features of adhesion, with the formation of a hybrid layer and
resin plugs at the interface between restorative material and dental
substrate, were present in all the specimens filled with resin composite in
association to dentin bonding agent. ( Fig 4).
Discussion
Data based on aetiology of decay lead to the conclusion that every site of
plaque retention has the possibility to be the location of secondary
decay.(Olgart L et al, 1974;Cagidiaco MC et al, 1996). For this reason

154
marginal integrity is very important to prevent secondary caries and pulp
inflammation (Roulet JF, 1994).
With the rapid turn-over of new composite materials it is very difficult to have
long term clinical test . The functioning of the composite in the present study
was not chosen to be compared with previous composites, but with
completely other materials that have an established value for clinical
dentistry.
In vitro tests are a very useful for screening dental material (Ferrari M &
Garcia-Godoy F, 2002). One of these, to valuate the presence of micro-
leakage or not, encompasses the theoretical ability to transport these dates
reliably to in vivo conditions (Söderholm KLM, 1991; Roulet JF, 1994).
Microleakage may be defined as “the clinically undetectable passage of
bacteria, fluids, molecules or ions between a cavity wall and the restorative
material applied to it” (Kidd EAM, 1976).
Based on above reasoning, in vitro micro-leakage tests were chosen for this
study as a reliable indicator for clinical performance. In fact micro-leakage
tests are very common in literature (Raskin A et al, 2001).
The shape of the cavities (high C factor) in this study was most challenging
as spherical and rounded cavities have less microleakage than box shaped
ones, specially if adhesively filled with resin-based composite (Douvitsas G,
1991; Hakimeh S et al, 2000).
In addition to the critical cavity shape, the restored teeth submitted to
thermo-cycling in order to get the most serious performance conditions.
The use of thermo-cycling as simulation of clinical aging is quite common
artificial aging technique. There are different opinions about the influence of
thermo-cycling on microleakage: some authors report the absolute absence
of influence of thermo-cycling on microleakage (Doerr CL et al, 1996), while
others show increase of microleakage at cementum-dentin-restoration
interface after thermal stress (Yap AUJ, 1997).
In this study methylene blue was the tracer employed to evaluate the degree
of infiltration. The small particle size and the permeability of dentinal tubules

155
may lead to the overestimation of the penetration (Gale MS & Darvell BW,
1999): bacteria have diameter of 0,3-1,5 µm or larger and this technique
cannot discern smaller gaps not enough wide for bacteria’s penetration.
The dwelling time of specimens in methylene blue seems to have no
influence on microleakage scores (Hilton TJ, 1998).
In this study the number of specimens, twelve cavities for each group, is in
accord with other studies (Hormati AA & Chan KC, 1980; Bauer JG &
Henson JL, 1985), even if this small number of specimens limits the choice
of statistical tests, permitting the use of less powerful ones (Norman GR &
Streiner DL, 1999).
The evaluation of penetration was scored after three cuts and optical
microscope observation.
This evaluation method may be less sensitive than three-dimensional
evaluation (Gale MS et al, 1994), however it is reported that the use of three
section may avoid under-estimation of in vitro microleakage (Raskin A et al,
2003).
This qualitative part of the method of evaluation can show the pattern of dye
penetration and can indicate where the penetration occurs (Alani AH & Toh
CG, 1997).
Regarding microleakage gold foil demonstrated a good sealing ability, in
accord with other studies (Thye RP, 1967; Martin DW, 1981).
The statistically equal ability to seal of gold foil and composite is very
interesting.
In fact the good scores achieved by gold foil, a very old non adhesive
technique, is very surprising in comparison to the modern adhesive resin-
based restorations. It has to be emphasized that gold foil techniques is
operator sensitive, and good results may only be achieved by very skilled
operators and with a lot of chair time. The absence of adhesion may very
well be compensated by gold’s dimensional and chemical stability and
thermal expansion coefficient similar to dental tissues.

156
Although composite restorations also are operator sensitive, they still are
easier to make in less time.
Unfortunately the coefficient of linear thermal expansion of resin composite
is 3-4 times that of tooth structure (Yazici AR et al, 2003).
This physical property in association with polymerization shrinkage may be
responsible of microleakage in resin restorations (Feilzer AJ et al, 1988;
Davidson CL & Feilzer AJ, 1997).
Partly to reduce the polymerization shrinkage stress, a layer of a low module
flowable composite was applied under the hybrid restorative material to
restore the cavities of Group 3 of this study (Davidson CL & Davidson-Kaban
SS, 1998; Unterbrink GL & Liebenberg WH, 1999; Chuang SF et al, 2001).
In agreement with these findings, a layer of flowable composite was applied
under the hybrid restorative material to restore the cavities of Group 3 of this
study . This operative protocol is able to reduce microleakage, as reported in
literature (Leevailoj C et al, 2001).
The results of the amalgam group are the poorest of this study.
The amalgam specimens showed total leakage involvement of the cavity’s
wall, notwithstanding it is reported in earlier studies that the initial poor seal
of fresh amalgam fillings improves with aging due to deposition of corrosion
products at the cavity-restoration interface (McCurdy CR,. 1974).
Amalgam restorations have been used for more than 150 years (Peyton FA
& Craig RG. 1971) and in clinical longevity surveys perform very satisfactory
(Hickel R & Manhart J, 2001; Ben-Amar A et al, 1995).
The SEM analysis revealed the quality of the restoration-cavity interface, with
the well-known morphological aspects of resin-bonding-dentin area. A very
intimate contact between gold and dental substrate was also confirmed with
SEM.
In this in vitro study only marginal integrity and seal was studied. It has to be
stressed that one leakage is not the other one. As important is to know
whether the materials alongside the eventual gap exhibit any bacteriostatic

157
effect. In this respect leakage in metal restorations is hard to compare with
leakage in resin restorations. This problem requires further study.
Conclusions
Gold and composite show a better seal than amalgam in Class V
restorations.
Surprisingly, an old, non adhesive restorative technique as compacted gold
foil still shows satisfactory results.
The quality of seal is related to dimensional and chemical stability and to
thermal expansion coefficient that is similar to dental tissues.
Close adaptation of restorative materials to the cavity wall is operator
dependant.

158
References
Alani AH, Toh CG. Detection of microleakage around dental restorations: a
review. Op Dent 1997; 22(4): 173-185.
Bauer JG, Henson JL. Microleakage of direct filling materials in class V
restorations using thermal cycling. Quintessence Int 1985;16(11): 765-769.
Ben-Amar A, Cardash HS, Judes H. The sealing of the tooth-amalgam
interface by corrosion products. J Oral Rehab 1995; 22(2): 101-104.
Bränström M, Vojinovic O. Response of dental pulp to invasion of bacteria
round threefilling materials. J Dent r Child 1976; 43: 15-21.
Cagidiaco MC, Ferrari M. Bonding to dentin: Mechanism morphology and
efficacy of bonding resin composites to dentin in vitro and in vivo.
Amsterdam, University of Amsterdam, Ph D Thesis, De Batte Ed. 1995.
Cagidiaco MC, Ferrari M, Garberoglio R. Dentin contamination protection
after mechanical preparation for veneering. Am J Dent 1996;9(2): 57-60.
Chuang SF, Liu JK, Chao CC, Liao FP, Chen YH. Effect of flowable
composite lining and operator experience on microleakage and internal
voids in Class II composite restorations. J Prosthet Dent 2001; 85(2): 177-
183.
Davidson CL. Resisting the curing contraction with adhesive composites. J
Prosthet Dent 1986; 55(4): 446-447.
Davidson CL, Feilzer AJ. Polymerization shrinkage and polymerization
shrinkage stress in polymer-based restoratives. J Dent 1997; 25: 435-440.
Davidson CL, Davidson-Kaban SS. Handling of mechanical stresses in
composite restorations. Dent Update 1998; 25: 274-279.
Dietrich T, Lösche AC, Lösche GM. Marginal adaptation of direct composite
and sandwich restorations in Class II cavities with cervical margins in
dentine. J Dent 1999; 27(6): 119-128.
Dodes JE. The amalgam controversy: an evidence-based analysis. J Am
Dent Association 2001; 132(3): 348-355.

159
Doerr CL, Hilton TJ, Hermesch CB. Effect of thermocycling on the
microleakage of conventional and resin modified glass ionomer. Am J Dent
1996; 9(1): 19-21.
Douvitsas G. Effect of cavity design on gap formation in Class II in
composite resin restorations. J Prosthet Dent 1991; 65(4): 475-479.
Federation Dentaire Internationale, World Health Organization, World Dental
Federation, Consensus statement on dental amalgam. FDI World 1995 : 9-
10.
Feilzer AJ, De Gee AJ, Davidson CL. Setting stress in composite resin in
relation to configuration of the restoratives. J Dent Res 1987; 66(11): 1636-
1639.
Feilzer AJ, de Gee AJ, Davidson CL. Curing contraction of composites and
glass-ionomer cements. J Prosthet Dent 1988; 59(3): 297-300.
Ferrari M, Davidson CL. Sealing performance of Scotchbond Multi-Purpose-
Z100 in Class II restorations. Am J Dent 1996; 9: 145-149.
Ferrari M, Garcia-Godoy F. Sealing ability of new generation adhesive-
restorative materials placed on vital teeth. Am J Dent 2002: 15(2): 117-28.
Gale MS, Darvell BW, Cheung GSP. Three-dimensional reconstruction of
microleakage pattern using a sequential grinding technique. J Dent 1994;
22(6): 370-375.
Gale MS, Darvell BW. Thermal cycling procedures for laboratory testing of
dental restorations. J Dent 1999; 27(2): 105-108.
Hakimeh S, Vaidyanathan J, Houpt ML, Vaidyanathan TK, Von Hagen S.
Microleakage of compomer Class V restorations: effect of load cycling,
thermal cycling and cavity shape differences. J Prosthet Dent 2000; 83: 194-
203.
Hickel R. Die zervikale füllung. Dtsch Zahnärzt Z 1994; 49(11): 13-19.
Hickel R, Manhart J. Longevity of dental restorations in posterior teeth and
reasons for failure. J Adhesive Dent 2001; 3:45-64.
160
Hilton TJ. Can modern restorative procedures and materials reliably seal
cavities? In vitro investigations. Part 1.Am J Dent 2002;15:198-210.
Hilton TJ. Can modern restorative procedures and materials reliably seal
cavities? In vitro investigations. Part 2.Am J Dent 2002;15:279-289.
Hormati AA, Chan KC. Marginal leakage of compacted gold, composite
resin, and high copper amalgam restorations. J Prosthet Dent 1980; 44 (4):
418-422.
Ianzano JA, Gwinnett AJ. Clinical evaluation of Class V restorations using a
total etch technique: 1 year results. Am J Dent 1993; 6(4): 207-210.
Ibbetson R, Eder A. Tooth surface loss. BDJbooks 2000: 3-8.
Kidd EAM. Microleakage: a review. J Dent 1976; 4: 199-205.
Krejci I, Lutz F. Marginal adaptation of class V restorations using different
restorative techniques. J Dent 1991; 19: 24-32.
Lee WC, Eakle WS. Possible role of tensile stresses in the aetiology of
cervical erosive lesions of teeth. J Prosthet Dent 1984, 52(3): 374-380.
Leevailoj C, Cochran MA, Matis BA, Moore BK, Platt JA. Microleakage of
posterior packable resin composites with and without flowable liners. Op
Dent 2001; 26(3): 302-307.
Manhart J, Chen HY, Mehl A, Weber K, Hickel R. Marginal quality and
microleakage of adhesive Class V restorations. J Dent 2001; 29(2): 123-130.
Martin DW. Interface leakage in microfilled composites, amalgam,
conventional composites and gold foil: a comparative in vitro study. J Calif
Dent Association 1981; 1(1) : 33-39.
McCoy RB, Anderson MH, Lepe X, Johnson GH. Clinical success of class V
composite resin restorations without mechanical retention. J Am Dent
Association 1998; 129 (5): 593-599.
McCurdy CR. A comparison of in vivo and in vitro microleakage of dental
restorations. J Am Dent Association 1974;88(3): 592-602.
Medina J. Matt gold-gold foil restoration. Journal of the American
Association of Gold Foil Operators 1969; 12-1: 13-26.

161
Norman GR, Streiner DL . PDQ statistics. BC Decker inc 1999. Hamilton.
Olgart L, Brännstöm M, Johnson G. Invasion of bacteria into dentinal
tubules: Experiments in vivo and in vitro. Act Odontol Scand 1974 ; 32(1):
61-70.
Penschke A, Blunck U, Roulet JF. Influence of incorrect application of
Optibond FL on the marginal adaptation of Class V restorations. Am J Dent
2000; 13(5): 239-244.
Peyton FA, Craig RG (1971) Restorative Dental Materials ,Mosby 4th
edition, St Luis: 358-397.
Powell LV, Gordon GE, Johnson GH. Clinical comparison of Class V resin
composite and glass ionomer restorations. Am J Dent 1992; 5(5): 249-252.
Raskin A D’Hoore W, Gonthier S, Degrange M, Dejou J. Reliability of in vitro
microleakage test: a literature review.J Adhesiv Dent 2001; 3: 295-308.
Raskin A, Tassery H, D’Hoore W, Gonthier S, Vreven J, Degrange M, Déjou
J. Influence of the number of section on reliability of in vitro microleakage
evaluations. Am J Dent 2003; 16(3): 207-210 .
Rees JS. The role of cuspal flexure in the development of abfraction lesions:
a finite element study. Euro J Oral Sci 1998; 106(6): 1028-1032.
Roulet JF. Marginal integrity: clinical significance. J Dent 1994; 22: 9-12.
Schuckar M, Geurtsen W. Proximo-cervical adaptation of Class II composite
restorations after thermo cycling: a quantitative and qualitative study. J Oral
Rehab 1997 ; 24(10) : 766-775.
Schüpbach P, Guggenheim B, Lutz F. Human root caries. Oral Path Med
1989; 18(3): 146-156.
Sjodin L, Uunsitalo M, van Dijken J. Resin modified glass ionomer cements.
In vitro microleakage. Swed Dent J 1996; 20(3): 77-86.
Söderholm KLM. Correlation of in vivo and in vitro performance of adhesive
restorative matherials. Dent Mater 1991; 7:74-83.
Sparrius O, Grossman ES. Marginal leakage of composite resin restorations
in combination with dentinal and enamel bonding agents. J Prosthet Dent
1989; 61(6): 678-684.

162
Stibbs GD. Direct golds in dental restorative therapy. Op Dent 1980; 5(3):
107-114.
Thye RP. A comparison of the marginal penetration of direct filling golds
using Ca45. J Am Acad Gold Foil Op 1967; 34 (4): 12-16.
Unterbrink GL, Liebenberg WH. Flowable resin composites as filled
adhesives; literature review and clinical recommendations. Quintessence Int
1999; 30(4): 249-257.
Van Meerbeck B, Braem M, Lambrechts P, Vanherle G. Morphological
characterization of the interface between resin and sclerotic dentine. J Dent
1994; 22(3): 141-146.
Wood RE, Maxymiw WG, McComb D. A clinical comparison of glass
ionomer and silver amalgam restorations in the treatment of Class V caries
in xerostomic head and neck cancer patients. Op Dent 1993; 18(3): 94-102.
Yap AUJ. Effects of storage, thermal and load cycling on a new reinforced
glass ionomer cement. J Oral Rehab 1997; 25(1): 40-44.
Yazici AR, Baseren M, Dayangaç B. The effect of flowable resin composite
on microleakage in Class V cavities. Op Dent 2003; 28: 42-46.

163
Table I
BBuurrss ((ffoorr hhiigghh--ssppeeeedd aanndd llooww--ssppeeeedd hhaannddppiieeccee))
CChhiieesseellss
GGoolldd
PPlluuggggeerrss
BBuunnsseenn bbuurrnneerr
CCaarrvveerrss//kknniivveess
RRuubbbbeerr ccuuppss aanndd ddiisskkss
Table II: Composition of Scotchbond MPS
Primer: 40%HEMA, 15% polyalkenoic acid copolymer, water
Adhesive: 40%HEMA, 70% bis-GMA, photoinitiator

164
Table III: Leakage scores recorded at cervical margin and median
0 1 2 3 4 median
Group 1 8 1 3 0 0 0
Group 2 2 0 0 10 0 3
Group 3 8 4 0 0 0 0
Graph 1
0123456789
10
0 1 2 3 4
goldamalgamcomposite

165
Legends to illustrations
Fig. 1. After immersion in a dye solution, each tooth was embedded in acrylic resin and
longitudinally sectioned at three different levels in the bucco-lingual direction.
.
Fig. 2. Dye penetration scores at the cervical margin

166
Fig. 3a. SEM image of the tooth- restoration interfaces in gold foil restorations that shows a
good adaptation on the dental substrate
Fig. 3b. SEM image of the enamel-restoration interface in gold foil a higher magnification

167
Fig. 4. Typical aspect of resin-bonding-dentin interface achieved in composite resins restoration

168
Chapter 9
Discussion
Since the introduction of resin-based materials in dentistry around the early
fifties of last century, increased concern and research was generated. There
are various reasons for this. One is that research and particularly dental
research underwent considerable upgrading, not at least because of improved
technical possibilities. Another one is that in that post-war period polymers
were introduced on a wide scale and application was accordingly.
Unfortunately, the early “plastics” were usually of questionable quality and so
were the resin-based dental materials. In contrast to their ease of handling,
these materials were mechanically inferior to the established ones such as
amalgam or casting alloys. One particular mediocre property of polymer
materials was their dimensional instability. Thermal expansion and water
swelling were huge and the polymerisation is still accompanied by substantial
volume reduction.
Since, exciting development brought about more stable, bondable, good
looking and easy applicable restorative materials that by now almost replaced
the established metal materials.
Parallel to the technical developments, enlarged interest in cosmetics
conquered the world and thus, also dentistry. With the need of new aesthetic
treatments in restorative dentistry a great interest has developed on the
prediction of the reliability and longevity of restorations. Paramount interest
was given to colour and colour stability and, because, for a great deal, resin-
based material had to do the job, attention had and has to be paid to
dimensional stability. The absence of the latter particularly affects marginal

169
integrity. Even the option of bonding cannot prevent gap formation and
consequently leakage.
To study marginal integrity, several in vitro and in vivo tests are available. In
this thesis the use of a dye, 2% methylene blue was the chosen as the
laboratory method for the study of leakage, whilst marginal staining was used
as an indication for clinical malfunction, both in agreement with the literature.
The in vitro project encompassed dye penetration measurements on several
types of restorations, restored in various ways, ranging from traditional non-
adhesive restorative materials such as gold foils, gold inlays, amalgams, to the
newest adhesive restorative techniques, direct fillings, combined use of
different composite resins, use of aesthetic inlays and self-adhesive luting
cements. Also the influence of different substrates was investigated; in
particular attention was given to the more risky sites where the margins are
placed in cementum-dentin.
A most striking finding was that almost all restorations demonstrated more or
less staining along the restoration-cavity interface, even if the restoration was
placed in theoretically ideal conditions. Taken that staining is indicative for
leakage, leaking restorations were consistently found in practically all our
specimens, though of course there were statistically significant differences
among the various experimental Groups. Moreover, adhesion showed not to be
the guarantee for perfect sealing. This was dramatically shown by the
frequently observed marginal dying of adhesive restorations, whilst the non-
adhesive gold foil fillings showed hardly any leakage. The latter comparative
experiment on straight-forward Class V restorations was carried out because
during the course of the project, doubt arose about the real meaning of the
colour dye penetration experiment as indicative for true leakage. It has to be
emphasized that if one desires to screen new materials, it is impossible to
perform the clinical screening at the same speed as the laboratory tests. Apart
from more complicated sample selection and making, clinical trials take at least
1 – 2 years, whilst the laboratory test can be done within one week. It was
therefore inevitable that there grows a significant time lag between laboratory

170
and clinical experience about a new material or procedure. As our results were
in conformity with literature where laboratory studies show many defects, whilst
the materials perform clinically relatively satisfactory, in vitro leakage should be
regarded as a theoretical maximum amount of leakage that may or may not
occur in vivo. Pashley (1990) stated that results of in vitro studies are often
presumed to be more negative than in vivo ones. (Pashley DH, 1990), but
possibly such a general statement should be differentiated with regard to the
specific in vitro test. Moreover, to date there are no accepted scientific methods
to correlate leakage results and clinical findings (Camps J et al, 2000; Mior IA
& Toffenetti F, 2000).
Based on the present study, it has to be questioned whether the widely
accepted methylene blue dying technique has a reliable clinical implication.
Apart from some sources (Gale MS & Darvell BW, 1999), there are no data
available on an eventual correlation between dye penetration and bacterial
invasion along the interface between restoration and cavity wall.
Another matter that has to be considered is that an eventual perfect initial seal
might be lost with time. It is reported in the literature (Lundin SA & Noren JG,
1991; Hakimeh S et al, 2000 ). that a breakdown of seal happens with aging of
the adhesive interface between resin composite and dental substrate. On the
other hand, corrosion and hygroscopic expansion may improve the sealing
ability of certain restorative materials.
In vitro leakage studies on adhesive constructions can also function as
indication whether the wall-to-wall integrity is persisting. Preliminary studies
(Fabianelli et al. 2004) indicated that the methylene blue staining does not per
se mean loss of adhesion as determined in a micro-tensile bond strength
measurement. Probably the dye penetration, especially the one labelled with a
low score, is a rather a diffusion of small molecules rather than a true stream of
liquid.

171
References Camps J, Dejou J, Remusat M, About I. Factors influencing pulpal response
to cavity restoration. Dent Mat 2000; 16: 432-444.
Gale MS, Darvell BW. Thermal cycling procedures for laboratory testing of
dental restorations. J Dent 1999;27:105-108.
Hakimeh S, Vaidyanathan J, Houpt ML, Vaidyanathan TK, Von Hagen S.
Microleakage of compomer Class V restorations: effect of load cycling,
thermal cycling and cavity shape differences. J Prosthet Dent 2000; 83: 194-
203.
Lundin SA, Noren JG. Marginal leakage in occlusally loaded, etched, Class
II composite resin restorations. Acta Odontol Scand 1991; 49: 247-254.
Mior IA, Toffenetti F. Secondary caries:a literature review with case reports.
Quint Int 2000; 31: 165-179.
Pashley DH. Clinical considerations of microleakage. J Endodont 1990; 16: 70-
77.

172
Chapter 10
Summary and Conclusions One of the most important needs of a restoration is to protect exposed
dentin against the infiltration of bacteria and their toxins along the interface
between restoration and dental substrate. For that reason, perfect sealing
should be the plan of each clinical performance and the ideal restorative
material should have a perfect and complete seal of the restoration’s margin.
In this thesis the aim was to measure the quantity and the quality of leakage
in relation to different dental materials, different luting agents, different
restorative techniques and , if possible, to explain the eventual discrepancy
between the in vitro methylene blue leakage findings and the in vivo
appreciations of our restorations.
After a review on leakage and its aspects in chapter 1, in chapter 2 sealing
ability of different types of restorative-adhesive combinations was measured
and etch patterns were correlated with leakage scores. Four combinations
of bonding system/restorative material were tested. Specimens of each
group were processed for leakage test, scored on dye penetration and resin
replicas were observed by SEM. The results of the staining measurements
were statistically evaluated. Our conclusions were that when gingival
margins are placed below the CEJ, the tested material-combinations
performed equally well; Adhesive systems that include etching with
phosphoric acid, sealed enamel margins significantly better than self-etching
primers and self-etching priming bonding agents.
In chapter 3 the in vitro wall-to-wall adaptation of a new self-adhesive resin-
based cement, Relyx Unicem 3M Espe, was evaluated, in comparison with
that of other cements when luting inlays in standardized Class II cavities in
extracted teeth. As a result of new chemistry, it is claimed by the

173
manufacturer that this cement does not require any substrate pretreatment
or adhesive application. Powder is a radiopaque fluoro-aluminosilicate glass,
potassium per-sulfate and ascorbic acid catalyst system mixed with an
aqueous solution of a poly-carboxylic acid modified with pendant
methacrylate Group HEMA and Tartaric acid.
Different combinations of inlay and luting material were tested: porcelain and
gold inlays, resin-based, zinc-oxy-phosphate, glass-ionomer cements. Zinc-
oxy-phosphate cement showed the highest microleakage and the sealing
ability exhibited by the new self-adhesive resin-based cement was
satisfactory with both gold and porcelain inlays, and comparable respectively
to that of resin-based and glass-ionomer cements. Conclusions were that
this new self-adhesive resin-based cement achieved an adequate seal,
similar to a standard adhesive procedure on both enamel and dentin when
used to lute in vitro gold and porcelain inlays.
In chapter 4 the purpose was to evaluate in Class II restorations the
marginal adaptation of 10 different packable composite resins in combination
with the proprietary adhesive system in one hundred human extracted
molars. The quality of marginal adaptation was evaluated through
microleakage tests. Microleakage was significantly higher at the cervical than
at the occlusal margin of the restorations, and the application of a thin layer
of a flowable composite at the cervical margin, as a liner underneath the
packable composite enhanced the marginal adaptation of the restoration.
The use of a self-etching primer to condition the dental substrate resulted at
the occlusal margin in a higher microleakage than when phosphoric acid was
applied.
Chapter 5 describes the observations on the in vitro efficacy of two different
composite luting cements on the prevention of marginal deterioration around
adhesive ceramic inlay restorations, testing whether different luting
procedures can affect sealing ability of luted inlays. Specimens were
selected at random for SEM observations, while others were processed for
marginal leakage. The bonding mechanism to dentin and resin cement

174
thickness was evaluated. The conclusion was that with the use of a self-
curing adhesive system in combination with self-curing resin cement like the
experimental one it seems possible to minimize risks of micro infiltration at
cervical margins.
In chapter 6 attention was given to the evaluation of the in vitro sealing
ability of Class II porcelain inlays with margins placed in cementum-dentin
and enamel, luted with two different cementing materials, correlating the dye
penetration depth with the morphology of dental substrates present at
margins of the preparations. Also in this study a SEM evaluation was
performed to assess with three different protocols: (1) variation of resin
cement thickness, (2) hybrid layer formation at the interface between resin
cement and dental substrate, and (3) to observe the morphology of the
cavity margins. The results of this study suggest that an enamel thickness of
0.5 mm at the cervical margin of Class II indirect restorations in unable to
seal them completely. The two combinations of bonding-cement materials
involved on the protocol performed similarly. The axial enamel margins of
Class II inlays have to be considered as one of the weakest margin of the
cervical area.
Chapter 7 presents a clinical trial, based on the quality expressed in
marginal integrity and sealing of Empress II inlays cemented under clinical
conditions with the self/light-curing Excite DSC and MultiLink adhesive luting
system. All patients received one Empress II inlay with the same clinical
protocol and were recalled after 6 and 12, 24 and 36 months. After 3-year
period of service no inlay came loose during the whole period of observation
and all the inlays were still clinically in service. No fracture was observed and
only moderate discoloration and visible marginal ditching were present in
some of the restorations that were still rated satisfactory. Slight crazing and
little surface staining were also reported. The results suggest that all the
restorations leak, notwithstanding satisfactory clinical performance are
achieved.

175
Chapter 8 was meant to obtain more insight in the discrepancy between
clinical positive appreciation and apparent in vitro leakage. It was evaluated
marginal integrity of standardized Class V cavities, restored with 3 different
sorts of filling materials, each of them generally accepted in the dental
profession. The restorative materials were: gold foil, amalgam and resin-
based composite in addition with a three steps dentin bonding system.
Dye penetration scoring was performed at the cervical margins, whilst also
each specimen was evaluated by SEM observations. Gold and composite
showed a better seal than amalgam in Class V restorations, bearing in mind
that even an non adhesive restorative technique as compacted gold foil still
shows satisfactory results.
General conclusions:
At the end of this thesis several conclusions can be drawn on occurrence of
leakage as demonstrated by methylene blue staining:
Microleakage was significantly higher at the cervical than at the occlusal
margin of restorations.
The application of a thin layer of a flowable composite at the cervical
margin, as a liner underneath the packable composite enhanced the
marginal adaptation of the restoration.
The use of a self-etching primer to condition the dental substrate resulted
at the occlusal margin in a higher microleakage than when phosphoric acid
was applied.
When we evaluated sealing ability of different types of restorative-adhesive
combinations, the tested material combinations performed equally well,
although adhesive systems including etching with phosphoric acid sealed
enamel margins significantly better than self-etching primers and self-etching
priming bonding agents.

176
Luting material combinations and handling procedures can affect the sealing
ability of luted inlays and enamel with a thickness of 0.5 mm at the cervical
margin of Class II indirect restorations was unable to guarantee the seal .
The sealing ability exhibited by RelyX Unicem, Fuji Cem and Variolink II
was satisfactory with both gold and porcelain inlays and an adequate seal
was achieved both on enamel and dentin.
Gold foil and composite resin perform equally with regard to microleakage
and achieve better sealing ability than amalgam.
In the clinical study where Empress II and Variolink were employed no
inlay came loose during the whole period of observation and all the inlays
were still clinically in service.
Discrepancy between observed in vitro staining of at the interface of
restorations and clinical acceptability requires further investigation.
Appendix In vitro leakage studies on adhesive reconstructions are widely accepted as an
indication whether the wall-to-wall integrity is persisting. In a preliminary study
it was indicated that methylene blue staining does not per se mean loss of
adhesion as determined in a micro-tensile bond strength measurement. After
preparing specimens (composite resin bonded to dentin with a Prime and
Bond dental adhesive) for microtensile test, half of the specimens were left for
two hours in methylene blue, where after the microtensile test were performed
( Fig 1 and Fig 2). The scores were the same for the two group, and the group
dipped in methylene blue presented stained surface where the failure occurred
( adhesive interface).
Probably the dye penetration, especially the one labelled with a low score in
leakage tests, is a diffusion of the small methylene blue molecules rather than
a true stream of liquid and doesn’t interfere with adhesion. Another clue might
be that staining indicated only partial conversion of the resin and not true
leakage. In another preliminary study a mass of dentin bonding agent

177
polimerized in a cut needle cap was dipped in methylene blue. After four days,
the specimens were washed. It was observed that the specimen was mainly
stained on the surface, but also staining was found inside the bulk material.
Apart from staining incompletely cured resin, the hydrophilicity of the
monomers in dentin bonding agents is responsible for uptake of the methylene
blue ( Fig.3, Fig.4 and Fig 5).
Staining vs. leakage will be subject for further investigation of the relevance of
color dying as a means to study marginal integrity of restorations.
A second approach will be the study of the narrowest space in which
Streptococcus Mutans can colonize with the use of calibrated micro-pipes and
living bacteria.
References
De Gee AJ, Ten Harkel-Hagenaar E, Davidson CL. Color dye for identification
of incompletely cured composite resins. J Prosthet Dent. 1984 Nov;52(5):626-
31.
178
Riassunto e conclusioni
Uno degli scopi più importanti di un restauro è quello di proteggere la
dentina esposta dall’aggressione dei batteri e delle loro tossine a livello
dell’interfaccia substrato dentale-materiale da restauro. Per questa ragione
un sigillo perfetto dovrebbe essere il fine di ogni attività clinica ed il materiale
ideale da restauro dovrebbe essere in grado di ottenere un sigillo marginale
perfetto. Lo scopo di questa tesi e’ di misurare la quantità e la qualità della
infiltrazione in relazione all’utilizzo di diversi materiali da restauro, diversi
cementi, diverse tecniche di restauro e , se possibile, capire il perché esista
una discrepanza tra le infiltrazioni misurate con il blu di metilene in vitro e il
reale buon funzionamento dei nostri restauri in vivo.
Dopo una review sulla infiltrazione ed i suoi aspetti nel capitolo 1, nel
capitolo 2 si è misurato la capacità di sigillo di diverse combinazioni
materiale da restauro-adesivo, e si sono paragonate diverse strategie di
mordenzatura in rapporto al grado di infiltrazione. Quattro combinazioni di
adesivi dentinali e materiali da restauro sono state sperimentate. I campioni
di ciascun gruppo venivano trattati per essere sottoposti a test di
microinfiltrazione, ne venivano misurate le infiltrazioni, e venivano fatte
repliche da osservare al SEM. I risultati delle misurazioni delle penetrazioni
di colorante venivano poi valutati statisticamente. Le nostre conclusioni
erano che, quando i gradini cervicali erano piazzati sotto la giunzione amelo-
cementizia, le combinazioni di materiali testate funzionavano ugualmente
bene, mentre i sistemi che includevano un passaggio con acido ortofosforico
sigillavano lo smalto significativamente meglio dei self-etching primers e
degli adesivi all-in-one.
Nel capitolo 3 si è valutato in vitro l’ adattamento parete-parete di un nuovo
cemento resinoso auto adesivo, Relyx Unicem 3M Espe, comparandolo con
altri cementi per la cementazione di intarsi in cavità standardizzate di II
Classe su denti estratti. Dotato di una innovativa chimica, secondo le
intenzioni del produttore, questo cemento resinoso non richiederebbe alcun
179
trattamento acido o passaggio di primer per effettuare cementazione
adesiva. La polvere è costituita da vetro fluoro-amino-silicato, potassio pre-
solfato ed un sistema catalitico in base acido ascorbico, mentre il liquido è
una soluzione acquosa di acido policarbossilico modificato con gruppi
metacrilici, HEMA e acido tartarico.
Varie combinazioni di inlays e cementi sono state testate: ceramica ed oro
come materiali per inlays e cementi a base resinosa, all’ossifosfato e vetro-
ionomerici come agenti cementanti. Il cemento all’ossifosfato è stato quello
che ha mostrato i peggiori risultati all’infiltrazione, mentre la capacità di
sigillo del nuovo cemento auto-adesivo si è dimostrata soddisfacente a
prescindere dal materiale utilizzato per gli intarsi, e comparabile ai risultati
ottenuti con le cementazioni adesive classiche. Le conclusioni tratte sono
state che questo nuovo cemento è riuscito ad ottenere un sigillo adeguato e
simile a quello ottenibile con procedure adesive standard, sia a livello di
smalto che di dentina radicolare quando utilizzato per cementare inlays in
oro o ceramica in vitro.
Nel capitolo 4 si è studiata la capacità di adattamento marginale in restauri
di Classe II di 10 diversi compositi compattabili associati ai loro rispettivi
sistemi adesivi. Tale adattamento marginale veniva studiato attraverso tests
di infiltrazione. Tale infiltrazione era maggiormente riscontrabile a livello del
gradino cervicale rispetto al margine occlusale. L’applicazione di un sottile
strato di composito fluido riusciva a diminuire, ma non ad azzerare, il grado
di infiltrazione a livello del gradino cervicale. L’utilizzo di sistemi auto-
mordenzanti dava risultati di infiltrazione peggiori a livello della superficie
occlusale rispetto all’applicazione di mordenzatura acida.
Il capitolo 5 descrive la efficacia in vitro di due diversi agenti cementanti nel
prevenire l’infiltrazione attorno a restauri adesivi in ceramica, valutando se
diverse procedure di cementazione possono dare risultati differenti al test di
infiltrazione. Alcuni campioni venivano scelti a caso per l’osservazione al
SEM, mentre altri venivano avviati al test di micro-infiltrazione. Venivano
analizzati anche I meccanismi di adesione e gli spessori dei cementi

180
resinosi. La conclusione era che l’utilizzo di un sistema adesivo auto-
polimerizzante associato ad un cemento resinoso anch’esso auto-
polimerizzante si riusciva a minimizzare il rischio di infiltrazione a livello del
margine cervicale.
Nel capitolo 6 si è posta l’attenzione alla capacità di sigillo in vitro di intarsi
in ceramica con gradino cervicale posto in cemento-dentina e smalto,
cementati con due diversi sistemi di cementazione, correlando grado di
infiltrazione alla morfologia tissutale presente a livello del margine di
preparazione. Anche in questo studio sono state fatte osservazioni al SEM
con tre diverse analisi: (1) variazione di spessore del cemento, (2)
formazione di strato ibrido a livello dell’interfaccia cemento-dentina, (3)
morfologia dei margini di cavità. I risultati di questo studio sembrano
suggerire che a livello del gradino cervicale in presenza di smalto sottile 0,5
mm non si riesca ad ottenere un adeguato sigillo. I due sistemi di
cementazione hanno dato risultati simili. I margini assiali degli inlays di
Classe II devono essere considerati come margini a rischio, similarmente
all’area del gradino cervicale.
Il capitolo 7 presenta un trial clinico basato sulla qualità della integrità
marginale e del sigillo di inlays in Empress II cementati in vivo utilizzando
come sistema adesivo Excite DSC e come cemento resinoso il Multilink. Tutti
I pazienti di questo studio avevano ricevuto un restauro di questo tipo con lo
stesso protocollo e sono stati richiamati dopo 6, 12, 24 e 36 mesi. Dopo un
periodo di osservazione di 3 anni nessun intarsio è andato perso e tutti i
restauri erano ancora in servizio. Nessuna frattura è stata registrata e solo
una moderata discolorazione marginale e una modesta determinabilità dei
bordi era presente su alcuni inlays. Piccole incrinature e pigmentazioni superficiali erano anche riscontrabili. Tali risultati suggeriscono che anche se
in vitro non riusciamo ad ottenere un sigillo assoluto, clinicamente possiamo
riscontrare buone performances. Il capitolo 8 si propone di meglio
approfondire la dicotomia tra I risultati clinici positivi dei nostri restauri e
l’apparente infiltrazione in vitro. si è valutato la integrità marginale di cavità di

181
Classe V trattate con 3 diverse tipologie di restauro diretto, ciascuna
generalmente accettata dai clinici. I materiali da restauro utilizzati sono stai
oro coesivo, amalgama e composito associato a sistema adesivo. Si è
misurato il grado di infiltrazione a livello del gradino cervicale, oltre ad una
osservazione al SEM.
Oro coesivo e composito hanno dato risultati simili, mentre l’amalgama
sigillava significativamente peggio. Una tecnica non adesiva come quella
dell’ oro coesivo sembra dare risultati soddisfacenti a questo tipo di test.
Conclusioni generali Alla fine di questa tesi diverse conclusioni possono essere tratte sulla
determinazione dell’infiltrazione dimostrata con l’impiego del blu di metilene.
La infiltrazione si presenta maggiormente a livello cervicale rispetto al livello
occlusale
L’utilizzo di uno strato sottile di composito fluido a livello del gradino
cervicale migliora l’adattamento marginale e diminuisce la penetrazione del
blu di metilene.
L’applicazione di un self-etching primer a livello occlusale da come risultato
maggiore infiltrazione rispetto ad adesivi che prevedono l’impiego di
mordenzatura con acido ortofosforico.
Diverse combinazioni di sistemi adesivi e rispettivi compositi danno risultati
positivi ai tests di infiltrazione, sebbene i sistemi che prevedano una
mordenzatura acida diano risultati migliori comparati a quelli che
impiegano dei self-etching primers.
Diversi materiali da cementazione e diverse procedure possono influenzare
la capacità di sigillo degli inlays.
Uno spessore di 0,5 mm di smalto a livello del gradino cervicale non
garantisce un adeguato sigillo.

182
La capacità di sigillo dimostrata da RelyX Unicem, Fuji Cem e Variolink II è
soddisfacente sia se si impiegano inlays in oro o in ceramica.
Gold foil e composito danno risultati simili riguardo l’infiltrazione e superiori a
quelli forniti dai restauri di Classe V in amalgama.
Nel clinical trial dove abbiamo Empress II e Variolink, non si è perso nessun
restauro nel periodo di osservazione e tutti I restauri sono ancora
clinicamente in servizio, con ottima soddisfazione dei pazienti.
La discrepanza tra la penetrazione a livello delle interfacce della sostanza
tracciante e la accettabilità clinica dei nostri restauri deve essere
ulteriormente approfondita.
Appendice
Gli studi sulla micro-infiltrazione dei restauri adesivi sono generalmente
accettati come indicatori della esistenza di integrità tra le pareti del restauro
e del substrato dentale. In uno studio preliminare si è evidenziato che la
colorazione della sostanza tracciante non vuol dire perdita di adesione,
come si è evidenziato con il test micro-tensile per la forza di adesione. Dopo
aver preparato i campioni da sottoporre al micro-tensile test ( composito e
dentina con utilizzo di un adesivo prime and bond dopo mordenzatura
acida), metà campioni sono stati immediatamente processati, mentre gli altri
sono stati lasciati in soluzione di blu di metilene per due ore e poi anch’essi
testati ( Fig 1 and Fig 2). I risultati sono stati gli stessi per i due gruppi, ed il
gruppo blu di metilene presentava pigmentazione a livello della zona di
frattura (interfaccia adesiva).
Probabilmente la penetrazione della sostanza tracciante, specialmente
quella che dava punteggi bassi a livello dei test di infiltrazione, è una
diffusione delle piccole molecole di blu di metilene piuttosto che un vero
flusso di liquido e non interferisce con l’adesione. Un’ altra indicazione
potrebbe essere che la colorazione indica solamente la parziale conversione
del monomero resinoso e non la vera infiltrazione (De Gee AJ et al, 1984) .
183
In un altro studio in fieri si è polimerizzata stratificando una massa di adesivo
dentinale in una punta di un copriago e poi si è immerso il campione in
bagno di blu di metilene al 2% per 4 giorni.
Successivamente I campioni venivano lavati ed osservati con l’utilizzo di
sistemi ottici ingrandenti. Si è osservato che i campioni erano
particolarmente pigmentati in superficie, ma si è reperito anche colorante
all’interno del materiale.
Oltre quindi a pigmentare il monomero resinoso non polimerizzato, il blu di
metilene potrebbe essere assorbito dalla idrofilicità dei monomeri presenti
negli adesivi dentinali. ( Fig.3, Fig.4 and Fig 5).
Il paragonare pigmentazione e infiltrazione sarà il soggetto di ulteriori studi
sulla importanza della penetrazione del colorante come mezzo per valutare la
qualità del sigillo marginale nei restauri.
Un altro approccio sarà lo studio sulla capacità di colonizzazione dello
Streptococcus Mutans di spazi sempre più piccoli con l’utilizzo di
micropipette disponibili nei laboratori di microbiologia.
Referenze
De Gee AJ, Ten Harkel-Hagenaar E, Davidson CL. Color dye for
identification of incompletely cured composite resins. J Prosthet Dent. 1984
Nov;52(5):626-31.
Fig. 1. Campioni pronti al test microtensile
Fig. 2. Campioni dopo test microtensile: notere la presenza di colorante a
livello della interfaccia.
Fig. 3. Campioni di adesivi dentali polimerizzati in un copriago.
Fig. 4. Campioni di adesivi dentali dopo bagno in soluzione di blu di
metilene.
Fig. 5. Sezione del campione dopo bagno in blu di metilene.

184
Résumé et Conclusions Un des principaux objectifs de la restauration est de protéger la dentine
exposée contre l’infiltration des bactéries et de leurs toxines sur l’interface
entre la restauration et le substrat dentaire. Pour cette raison toute
intervention clinique devrait avoir comme but un scellage parfait et le
matériau de restauration idéal devrait permettre de sceller parfaitement et
complètement les bords de la restauration. Notre thèse a comme but de
mesurer la quantité et la qualité des fuites concernant les différents
matériaux dentaires, ciments et techniques employées et dans la mesure du
possible d’expliquer les différences éventuelles qui auraient pu être
remarquées entre les fuites de bleu de méthylène observées in vitro et les
appréciations in vivo de nos restaurations.
Après avoir passé en revue les fuites et leurs différents aspects dans le
1.ier chapitre, nous avons mesuré dans le 2.ième chapitre les propriétés
de scellage des différentes combinaisons restauratrices – adhésives et nous
avons corrélé les schémas de mordançage avec les performances de
fuites. Nous avons soumis à épreuve quatre combinaisons de systèmes
adhésifs et de matériaux de restauration. Des éprouvettes de chaque
groupe ont été soumises à des essais de fuite, on a mesuré la pénétration
de colorant et les répliques en résine ont été observées sous le SEM. Les
résultats des colorations ont été évalués statistiquement. Nos conclusions
montrent que quand les bords gingivaux sont placés en dessous de la
limite CEJ, les combinaisons de matériaux testés ont des performances
égales. Les systèmes adhésifs comprenant le mordançage à l’acide
phosphorique ont scellé les bords significativement mieux que les primers
auto-corrosifs et les adhésifs avec primer auto-corrosif.
L’adaptation in vitro aux parois (wall-to-wall) d’un nouveau ciment
autoadhésif sur base de résine, RelyX Unicem 3M Espe, fait l’objet de
l’examen du chapitre 3 , suivie par une comparaison avec d’autres types de
ciment avec inlay à cimentation dans les cavités de classe II de dents

185
extraites. Nous avons analysé différentes combinaisons d’inlays et de
produits à cimentation : inlays en porcelaine et or, produits à base de résine,
zinc-oxy-phosphate, ciments en verre ionomère. Le ciment zinc-oxy-
phosphate présentait le taux les plus élevé de micro-fuites et les propriétés
de scellage du nouveau ciment autoadhésif sur base de résine étaient
satisfaisantes avec les inlays en porcelaine tout comme avec ceux en or, et
comparables respectivement avec les ciments à base de résine et de verre
ionomère. Nous avons conclu que ce nouveau ciment autoadhésif à base de
résine permettait d’obtenir un scellage approprié et sur l’émail et sur la
dentine lors de l’utilisation in vitro pour cimenter les inlays en or et en
porcelaine.
Le chapitre 4 s’occupe de l’évaluation de l’adaptation marginale de
restaurations de Classe II de 10 types différents de résines composites
condensables en combinaison avec le système adhésif propriétaire sur cent
molaires humaines extraites. La qualité de l’adaptation marginale a été
évaluée par des essais de micro-fuites. Les micro-fuites étaient
significativement plus élevées sur le bord cervical que sur le bord occlusal
des restaurations. Notamment l’application d’une fine couche d’un composite
fluide sur le bord cervical, posée en dessous du composite condensable, a
permis d’améliorer l’adaptation marginale de la restauration. L’emploi d’un
primer auto-corrosif pour la préparation du substrat dentaire a donné lieu a
un nombre plus élevé de micro-fuites sur le bord occlusal, par rapport aux
cas où l’acide phosphorique a été utilisé.
Le Chapitre 5 décrit nos observations de l’efficacité in vitro de deux produits
composites de cimentation pour la prévention de la détérioration marginale
sur le contour des restaurations avec inlays adhésifs en céramique : Nous
avons testé si différentes procédures de cimentation peuvent influencer les
propriétés du scellage des inlays cimentés. Les éprouvettes ont été choisies
de manière randomisée pour l’observation par SEM, tandis que d’autres ont
été examinées pour relever les micro-fuites. On a évalué le mécanisme de
collage à la dentine et l’épaisseur du ciment en résine . Les conclusions

186
montrent que l’emploi d’un système adhésif autorenforçant combiné avec un
ciment en résine auto-renforçante , comme les produits expérimentaux,
semble effectivement minimiser les risques de micro-infiltration sur les bords
cervicaux.
Dans le chapitre 6 nous avons examiné les propriétés de scellage in vitro
des inlays en porcelaine de Classe II avec les bords placés dans le cément
– dentine et dans l’émail, cimentés avec deux produits de cimentation
différents, en établissant une corrélation entre la profondeur de pénétration
du colorant et la morphologie des substrats dentaires qui se trouvaient sur
le contour des préparations. Dans cette étude nous avons également fait
recours à l’observation par SEM avec trois protocoles différents d’évaluation:
(1) la variation de l’épaisseur du ciment résine, (2) la formation d’une couche
hybride sur l’interface entre le ciment résine et le substrat dentaire et (3)
l’observation de la morphologie des bords de la cavité.
Les résultats de cette étude font penser qu’une épaisseur de l’émail de 0,5
mm sur le bord cervical des restaurations indirectes de Classe II empèche le
scellage complet.
Les deux combinaisons de matériaux adhésifs et de ciment prévues par le
protocole ont eu des performances semblables. Les bords axiaux de l’émail
des inlays de Classe II sont à considérer comme les plus faibles de la zone
cervicale.
Dans le Chapitre 7 nous présentons un essai clinique basé sur la qualité en
termes d’intégrité marginale et du scellage des inlays Empress II cimentés
sous conditions cliniques avec un système adhésif de cimentation
autorenforçant à la lumière Excite DSC et MultiLink. Les résultats montrent
que toutes les restaurations présentent des fuites, malgré les performances
cliniques satisfaisantes. Tous les patients ont eu un inlay Empress II en
suivant le même protocole clinique et ont été réexaminés après 6, 12, 24 et
36 mois. Après une mise en place d’une durée de 3 ans aucun inlay ne s’est
détaché pendant toute la période d’observation et tous les inlays étaient
encore cliniquement en service. Nous n’avons observé aucun cas de

187
fracture et il n’y avait qu’une décoloration modérée et des sillons marginaux
visibles dans certaines restaurations qui étaient toutefois considérées
satisfaisantes. On a également signalé de légères craquelures et quelques
taches superficielles.
Avec le Chapitre 8 nous nous sommes proposé de mieux connaître les
différences entre l’appréciation clinique positive et des pertes apparentes in
vitro : l’intégrité marginale des cavités de Classe V standardisées, restaurées
avec trois matériaux d’obturation différents qui sont généralement acceptés
par les dentistes. Les matériaux de restauration étaient : la feuille d’or,
l’amalgame et les composites à base de résine ensemble avec un système
à trois phases d’adhésion à la dentine.
Nous avons évalué la pénétration du colorant sur les bords cervicaux, mais
chaque éprouvette a également été évaluée par SEM. L’or et le matériau
composite ont donné lieu à un meilleur scellage que l’amalgame dans les
restaurations de Classe V, tout en sachant que même une technique de
restauration non adhésive comme la feuille d’or compacté donne encore des
résultats satisfaisants.
Conclusions générales: A la fin de notre thèse plusieurs conclusions peuvent être tirées concernant
la fréquence des fuites comme nous avons pu prouver à l’aide de la
coloration au bleu de méthylène:
Les micro-fuites étaient significativement plus élevées sur les bords
cervicaux que sur les bords occlusaux des restaurations.
L’application d’une fine couche de composite fluide sur le bord cervical,
comme revêtement en dessous du composite condensable, a amélioré
l’adaptation marginale de la restauration.
L’emploi des primers autocorrosifs pour préparer le substrat dentaire a
donné lieu a plus de micro-fuites sur le bord occlusal que l’emploi de l’acide
phosphorique.

188
Quand nous avons évalué les propriétés de scellage de différents types de
combinaisons restauratrices – adhésives, les combinaisons testées se sont
comportées de manière semblable, même si les systèmes adhésifs
comprenant le mordançage à l’acide phosphorique scellaient les bords de
l’émail significativement mieux que les primers auto-corrosifs et les agents
adhésifs auto-corrosifs utilisés comme primer.
Les combinaisons des produits de cimentation et les techniques de mise en
oeuvre peuvent influencer les propriétés de scellage des inlays cimentés et
une épaisseur de l’émail de 0,5 mm sur le bord cervical des restaurations
indirectes de Classe II n’était pas en mesure d’assurer le scellage. Les
propriétés de scellage montrées par RelyX Unicem, Fuji Cem et Variolink II
étaient satisfaisantes, avec les inlays en or tout comme avec ceux en
porcelaine et le scellage obtenu était adéquat sur l’émail et sur la dentine.
La feuille d’or et la résine composite se comportent de la même manière en
matière de micro-fuites et ont des propriétés de scellage supérieures à
celles de l’amalgame.
Dans l’étude clinique qui a utilisé Empress II et Variolink aucun inlay ne s’est
détaché pendant toute la période d’observation et tous les inlays étaient
encore cliniquement en service.
Les différences entre les colorations observées in vitro sur l’interface entre
les restauration et l’acceptabilité clinique nécessitent des
approfondissements ultérieurs.
Appendice
Les études in vitro sur les micro-fuites dans les reconstructions adhésives
sont généralement considérées comme une indication de la persistance de
l’intégrité wall-to– wall. Une étude préliminaire avait indiqué que la coloration
au bleu de méthylène ne signifiait pas en tant que telle une perte de
l’adhésion, comme cela a été mesuré lors des essais sur la micro- traction de
l’adhésion. Après avoir préparé les éprouvettes (résine composite liée à la

189
dentine par un Prime et un Bond dentaire adhésif) pour l’essai de micro-
traction, la moitié des éprouvettes ont été laissées pendant deux heures
dans le bleu de méthylène, ensuite les essais de micro-traction ont été
réalisés. (fig. 1 et fig. 2). Les résultats étaient les mêmes dans les deux
groupes. Mais le groupe trempé dans le bleu de méthylène avait des
surfaces tachées au point de rupture (interface adhésive).
Probablement dans le cas de la pénétration du colorant, notamment lorsque
les résultats concernant les fuites étaient faibles, il s’agissait d’une diffusion
de petites molécules de bleu de méthylène et non pas d’une véritable
infiltration de liquide et il n’y avait pas de conséquences sur l’adhésion. Une
autre explication pourrait être que la coloration n’indiquait qu’une conversion
partielle de la résine et non pas une véritable fuite. (De Gee AJ, Ten Harkel-
Hagenaar E, Davidson CL. Color dye for identification of incompletely cured
composite resins. J Prosthet Dent. 1984 Nov;52(5):626-31).
Dans une autre étude préliminaire une masse d’adhésif de dentine
polymérisée dans une tête d’épingle était trempée dans le bleu de
méthylène. Après quatre jours les éprouvettes ont été lavées. On a observé
que l’éprouvette était surtout colorée sur la surface, mais on a trouvé
également des traces de coloration à l’intérieur du matériau. A part le fait
qu’on observe une coloration des résines qui ne sont pas complètement
renforcées, le caractère hydrophile des monomères des adhésifs de la
dentine est responsable de l’absorption du bleu de méthylène. (fig.3, fig.4 et
fig 5).
La coloration en fonction du degré de fuites sera le thème de la recherche
ultérieure sur l’importance de la coloration comme moyen pour étudier
l’intégrité marginale des restaurations.
Dans une deuxième approche nous examinerons les espaces les plus étroits
susceptibles d’être colonisés par le Streptococcus Mutans à l’aide de micro-
tuyaux et de bactéries vivantes.

190
Fig. 1. l’éprouvette prête pour l’essai de micro-traction.
Fig. 2. l’éprouvette après l’essai de micro-traction: à noter la
présence d’agent colorant sur la zone d’interface.
Fig 3. Éprouvettes avec adhésif de la dentine polymérisé dans une tête
d’épingle.
Fig. 4. Une éprouvette restée quatre jours dans une solution de bleu de
méthylène.
Fig. 5. Coupe d’une éprouvette trempée dans du bleu de méthylène.

191
Resumen y conclusiones
Uno de los requisitos más importantes de la restauración consiste en
proteger la dentina expuesta frente a la infiltración de bacterias y de sus
toxinas a lo largo de la interfase de la restauración y de la superficie dental.
Por ese motivo, la finalidad de toda intervención clínica debería ser
conseguir un sellado perfecto, por lo que el material restaurativo ideal ha de
garantizar un sellado perfecto y completo del margen de la restauración. El
objetivo de este estudio es medir la cantidad y la calidad de las filtraciones
de los distintos materiales dentales, de los agentes de sellado y de las
técnicas de restauración, y en la medida de lo posible, explicar la eventual
discrepancia entre las filtraciones de azul de metileno in vitro y las
apreciaciones in vivo de nuestras restauraciones.
En el capítulo 1 se hace un repaso de las filtraciones y de sus aspectos. En
el capítulo 2 se mide la capacidad de sellado de distintos tipos de
combinados adhesivo-restaurativos y se establece una relación entre los
patrones de grabado y los niveles de filtración. En concreto, se han tomado
en consideración cuatro combinaciones de adhesivos/materiales
restaurativos. En primer lugar, se realizó una prueba de hermeticidad con
muestras de cada combinación, con el fin de medir la penetración de tintura
y se observaron las réplicas de resina por Microscopia de Escaneo de
Electrones (SEM). Los resultados de la prueba de hermeticidad se
analizaron estadísticamente. El estudio llega a la conclusión de que cuando
los márgenes gingivales se sitúan por debajo de la unión cemento-esmalte
(CEJ), los combinados de materiales estudiados actúan igual de bien; los
sistemas adhesivos que incluyen grabado con ácido fosfórico sellan los
márgenes de esmalte considerablemente mejor que los sistemas de
autograbado y que el adhesivo total autograbante.
En el capítulo 3 se evalúa la adaptación parietal in vitro de un nuevo
cemento autoadhesivo a base de resina, RelyX Unicem 3M Espe,

192
comparándola con la de otros cementos a la hora de sellar inlays en
cavidades estandarizadas de clase II de piezas extraídas. Se tomaron en
consideración distintas combinaciones de inlays y de material sellante: inlays
de porcelana y oro, inlays a base de resinas, fosfato de zinc y óxido de zinc,
cementos de ionómero de vidrio. El cemento de fosfato /óxido de zinc mostró
los mayores niveles de microfiltración y la capacidad de sellado del nuevo
cemento autoadhesivo a base de resina fue buena, tanto con inlays de oro
como de porcelana, y comparable a la de los cementos a base de resinas y
ionómeros de vidrio. El estudio concluye que este nuevo cemento
autoadhesivo a base de resina ofrece un sellado adecuado tanto del esmalte
como de la dentina, cuando se utiliza para sellar inlays de oro y porcelana in
vitro.
El objetivo del capítulo 4 es evaluar la adaptación marginal de 10 resinas de
composite condensable en restauraciones de clase II combinadas con un
sistema de adhesión comercial en cien molares humanos extraídos. La
calidad de la adaptación marginal se midió a través de pruebas de
microfiltración. Se comprobó que las microfiltraciones eran
considerablemente mayores en el margen cervical que en margen oclusal de
la restauración, y que la aplicación de una fina capa de composite fluido en
el margen cervical, a modo de "liner" del composite consensable, mejoraba
la adaptación marginal de la restauración. La utilización de un adhesivo
autograbante para preparar la superficie dental produjo más microfiltraciones
en el margen oclusal que la utilización de ácido fosfórico.
El capítulo 5 recoge observaciones sobre la eficacia in vitro de dos
cementos de sellado composite a la hora de prevenir el deterioro marginal
en torno a las restauraciones con inlays de cerámica, y comprueba si la
capacidad de sellado de los inlays se ve afectada por el procedimiento de
sellado adoptado. En este estudio se tomaron varias muestras aleatorias
para realizar las observaciones SEM y se prepararon otras muestras para
detectar filtraciones marginales. Se evaluó el mecanismo de adhesión a la
dentina y el grosor del cemento de resina. El estudio llega a la conclusión de

193
que utilizando sistemas adhesivos autocurantes junto a cementos de resina
autocurantes, como el experimental, es posible minimizar el riesgo de que se
produzcan microfiltraciones en los márgenes cervicales.
En el capítulo 6 se evalúa la capacidad de sellado in vitro de inlays de
porcelana clase II con márgenes situados en cemento-dentina y esmalte y
sellados con dos tipos de cemento distintos. Este estudio relaciona la
profundidad de penetración de la tintura con la morfología que presenta la
superficie dental en los márgenes de las preparaciones. Este estudio
también incluye una evaluación SEM basada en tres protocolos distintos
para comprobar: (1) la variación del grosor de los cementos de resina, (2) la
formación de capa híbrida en la interfase entre el cemento de resina y la
superficie dental, y (3) la morfología de los márgenes de la cavidad. Los
resultados de este estudio indican que un grosor de esmalte de 0,5 mm en el
margen cervical impide sellar completamente las restauraciones indirectas
de clase II. Los dos combinados de materiales adhesivos a base de cemento
que se utilizaron en el estudio dieron los mismos resultados. El margen axial
de esmalte de los inlays clase II ha de ser considerado como uno de los
márgenes más débiles de la zona cervical.
El capítulo 7 presenta un ensayo clínico de la calidad (expresada en
integridad marginal y sellado) de los inlays de Empress II cementados en
condiciones clínicas con los sistemas adhesivos autocurante/ligero Excite
DSC y Multilink. Los resultados indican que todas las restauraciones filtran,
independientemente de su buen resultado clínico. Todos los pacientes
recibieron un inlay de Empress II con el mismo protocolo clínico y pasaron
revisiones a los 6, 12, 24 y 36 meses. A los tres años de la restauración no
se había desprendido ni un solo inlay durante todo el período de observación
y todos los inlays funcionaban correctamente desde el punto de vista clínico.
No se apreciaban fracturas y tan sólo se pudo detectar una moderada
descolocación y un surco marginal visible en algunas restauraciones, que
aun así, se calificaron de satisfactorias. También se detectó un ligero
craquelado y pequeñas manchas en la superficie.

194
El capítulo 8 tiene como objetivo ahondar en las diferencias entre el juicio
clínico positivo y a aparente filtración in vitro. La integridad marginal de las
cavidades estandarizadas de clase V, restauradas con tres tipos distintos de
materiales de relleno, todos ellos de uso corriente en la profesión: lámina de
oro, amalgama y composite de resina, además de un sistema de adhesión a
dentina de tres fases.
Se midió la penetración de la tintura en los márgenes cervicales y se
realizaron observaciones SEM de cada muestra. El oro y el composite
mostraron un sellado mejor que la amalgama en las restauraciones de clase
V, teniendo en cuenta que incluso una técnica restauradora no adhesiva
como la lámina compacta de oro sigue dando buenos resultados.
Conclusiones generales Este estudio arroja varias conclusiones en relación a la presencia de
filtraciones detectadas con tintura azul de metileno:
Las microfiltraciones fueron bastante más frecuentes en el margen cervical
que en el margen oclusal de la restauración.
Aplicando una fina capa de composite fluido en el margen cervical, a modo
de "liner" del composite condensable, se consiguió mejorar la adaptación
marginal de la restauración.
La utilización de un adhesivo autograbante para preparar la superficie dental
produjo más microfiltraciones en el margen oclusal que la aplicación de
ácido fosfórico.
Al evaluar la capacidad de sellado de los distintos tipos de combinados
adhesivos-restaurativos, todos los combinados estudiados dieron los
mismos resultados, aunque los sistemas adhesivos con grabado de ácido
fosfórico sellaron los márgenes de esmalte bastante mejor que los primers
autograbantes y los adhesivos totales autograbantes.
Los combinados de material sellante y los procedimientos de manipulación
pueden alterar la capacidad de sellado de los inlays. De igual manera, un

195
grosor de esmalte de 0,5 mm en el margen cervical no garantiza el sellado
de la restauración indirecta de clase II.
La capacidad de sellado de RelyX Unicem, Fuji Cem y Variolink II, tanto con
inlays de oro como de porcelana, fue buena. Estos productos sellaron bien
tanto en esmalte como en dentina.
La lámina de oro y la resina de composite son igual de buenos frente a las
microfiltraciones y poseen más capacidad de sellado que la amalgama.
En el estudio clínico con Empress II y Variolink no se desprendió ningún
inlay durante todo el período de observación y todos los inlays seguían
funcionando bien desde el punto de vista clínico.
Se ha de seguir investigando la discrepancia entre las manchas observadas
in vitro en el interfase de las restauraciones y la aceptabilidad clínica dichas
restauraciones.
Apéndice Los estudios in vitro sobre las filtraciones de las reconstrucciones adhesivas
se consideran como un buen indicador del estado de integridad parietal. En
un estudio anterior se indica que la filtración de azul de metileno no significa
de por sí que se haya producido una pérdida de adhesión, tal como se
determina en una medición de la fuerza de unión microtensil. Para realizar la
prueba microtensil se prepararon una serie de muestras (resina composite
adherida a dentina con un adhesivo dental prime and bond). Seguidamente
se sumergió la mitad de estas muestras en azul de metileno durante dos
horas, al cabo de las cuales se realizó la prueba microtensil ( fig 1 y fig 2).
Ambos grupos obtuvieron la misma puntuación y el grupo sumergido en azul
de metileno presentó manchas en aquellas partes de la superficie en las que
se produjo un fallo (interfase adhesiva).
Probablemente la penetración de la tintura en las muestras, especialmente
en aquellas con baja puntuación en las pruebas de filtración, se debe a la
difusión de pequeñas moléculas de azul de metileno y no a un flujo real de
196
líquido, por lo que no interfieren con la adhesión. Otra señal es que las
manchas indicaban tan sólo una curación parcial de la resina y no una
filtración auténtica (De Gee AJ, Ten Harkel-Hagenaar E, Davidson CL. Color
dye for identification of incompletely cured composite resins. J Prosthet Dent.
1984 Nov;52(5):626-31).
En otro estudio anterior se sumergió en azul de metileno una determinada
cantidad de agente adhesivo a la dentina polimerizado en un capuchón de
aguja cortado. Al cabo de cuatro días se lavó la muestra. Se observó que la
mayoría de las manchas de la muestra eran superficiales, pero también se
encontraron machas en el material interior. Aparte de manchar la resina no
curada totalmente, la hidrofilicidad de los monómeros de los adhesivos a
dentina es la responsable de la absorción de azul de metileno ( Fig.3, Fig.4 y
Fig 5).
Para estudiar la integridad marginal de las restauraciones se deberá
investigar la relevancia de la coloración en las manchas y cotejarla con la de
las filtraciones.
El segundo enfoque de investigación consistirá en estudiar con microtubos y
bacterias vivas el espacio mínimo que el Streptococcus Mutans necesita
para colonizar
Fig. 1. Muestra preparada para la prueba microtensil.
Fig. 2. Muestra tras la realización de la prueba microtensil: notar la presencia
de tintura en la zona interfase.
Fig 3. Muestras de agente adhesivo a la dentina polimerizadas en capuchón
de aguja cortado.
Fig. 4. Aspecto de las muestras tras permanecer cuatro días en una solución
de azul de metileno.
Fig. 5. Sección de muestra sumergida en azul de metileno.
197
Zusammenfassung und Schlussfolgerungen
Eines der wichtigsten Erfordernisse bei der Restauration ist, freiliegendes
Dentin am Übergang zwischen Restauration und natürlicher
Zahnhartsubstanz vor Infiltration von Bakterien und Toxinen zu schützen.
Beim klinischen Eingriff ist daher auf einen einwandfreien Abschluss zu
achten und ein Restaurationsmaterial zu wählen, das den Restaurationsrand
perfekt und vollständig schließt.
Ziel dieser Arbeit ist es Quantität und Qualität der Undichtigkeit bezogen auf
verschiedene Zahnsubstanz, Zemente, verschiedener Füllstoffe,
verschiedene Restaurationstechniken zu messen und wenn möglich die
eventuelle Diskrepanz zu klären zwischen den in vitro Ergebnissen mit
Methylenblau und den in vivo Erkenntnissen bei Restaurationsarbeiten.
Kapitel 1 gibt einen Überblick über Undichtigkeit und ihre Aspekte Kapitel 2 untersucht die Haftfähigkeiten verschiedener Kombinationen von
Füllmitteln und setzt Ätzmodelle in Korrelation zu Messergebnissen der
Undichtigkeit.
Vier Tests mit jeweils verschiedenen Kombinationen von Bonding /
Restaurationsmaterial- Kombinationen wurden durchgeführt.
Die Proben jeder Gruppe wurden auf Undichtigkeit geprüft und nach
Farbstoffeindringung gestuft, die Schaumodelle wurden mit Hilfe von SEM
untersucht. Die Ergebnisse der Verfärbungsmessungen wurden statistisch
ausgewertet. Wir kamen zu folgenden Schluss: bei Gingivallücken unter
dem Schmelzzement (CEJ) erzielen die getesteten Materialkombinationen
gleichgute Ergebnisse; Adhäsivtechniken, die mit Phosphorsäure verätzen,
dichten Zahnschmelzränder besser ab als selbstverätzende Primer und
selbstverätzende Bondingmittel.
Kapitel 3 untersucht den in vitro Wand-zu-Wand Abschluss eines neuen
selbsthaftenden Harzzements im Vergleich zu anderen Zementen und prüft
seine Eignung zur Zementierung von Füllung von Standard II- Kavitäten
nach Zahnextraktion . Getestet wurden verschiedene Verbindungen von
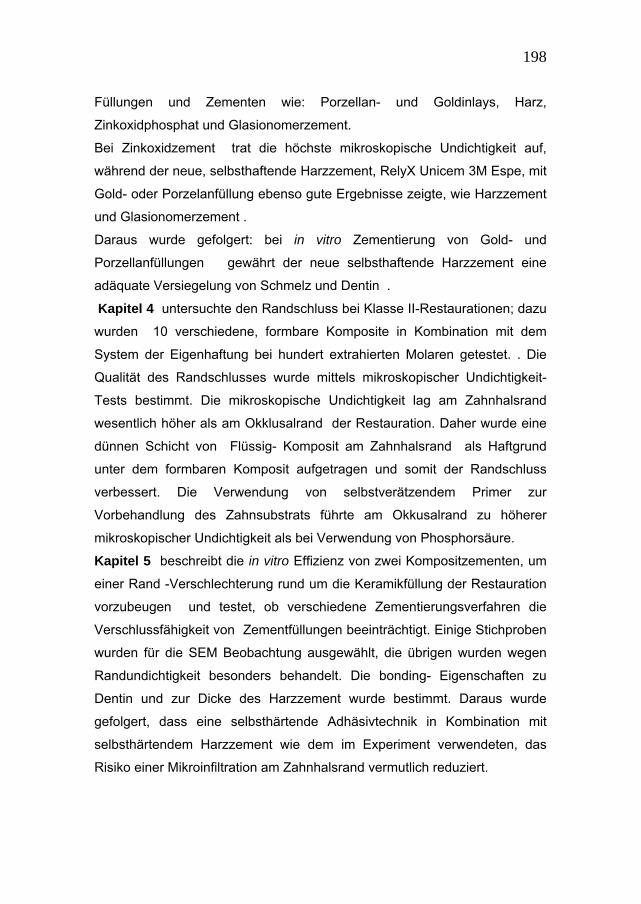
198
Füllungen und Zementen wie: Porzellan- und Goldinlays, Harz,
Zinkoxidphosphat und Glasionomerzement.
Bei Zinkoxidzement trat die höchste mikroskopische Undichtigkeit auf,
während der neue, selbsthaftende Harzzement, RelyX Unicem 3M Espe, mit
Gold- oder Porzelanfüllung ebenso gute Ergebnisse zeigte, wie Harzzement
und Glasionomerzement .
Daraus wurde gefolgert: bei in vitro Zementierung von Gold- und
Porzellanfüllungen gewährt der neue selbsthaftende Harzzement eine
adäquate Versiegelung von Schmelz und Dentin .
Kapitel 4 untersuchte den Randschluss bei Klasse II-Restaurationen; dazu
wurden 10 verschiedene, formbare Komposite in Kombination mit dem
System der Eigenhaftung bei hundert extrahierten Molaren getestet. . Die
Qualität des Randschlusses wurde mittels mikroskopischer Undichtigkeit-
Tests bestimmt. Die mikroskopische Undichtigkeit lag am Zahnhalsrand
wesentlich höher als am Okklusalrand der Restauration. Daher wurde eine
dünnen Schicht von Flüssig- Komposit am Zahnhalsrand als Haftgrund
unter dem formbaren Komposit aufgetragen und somit der Randschluss
verbessert. Die Verwendung von selbstverätzendem Primer zur
Vorbehandlung des Zahnsubstrats führte am Okkusalrand zu höherer
mikroskopischer Undichtigkeit als bei Verwendung von Phosphorsäure.
Kapitel 5 beschreibt die in vitro Effizienz von zwei Kompositzementen, um
einer Rand -Verschlechterung rund um die Keramikfüllung der Restauration
vorzubeugen und testet, ob verschiedene Zementierungsverfahren die
Verschlussfähigkeit von Zementfüllungen beeinträchtigt. Einige Stichproben
wurden für die SEM Beobachtung ausgewählt, die übrigen wurden wegen
Randundichtigkeit besonders behandelt. Die bonding- Eigenschaften zu
Dentin und zur Dicke des Harzzement wurde bestimmt. Daraus wurde
gefolgert, dass eine selbsthärtende Adhäsivtechnik in Kombination mit
selbsthärtendem Harzzement wie dem im Experiment verwendeten, das
Risiko einer Mikroinfiltration am Zahnhalsrand vermutlich reduziert.
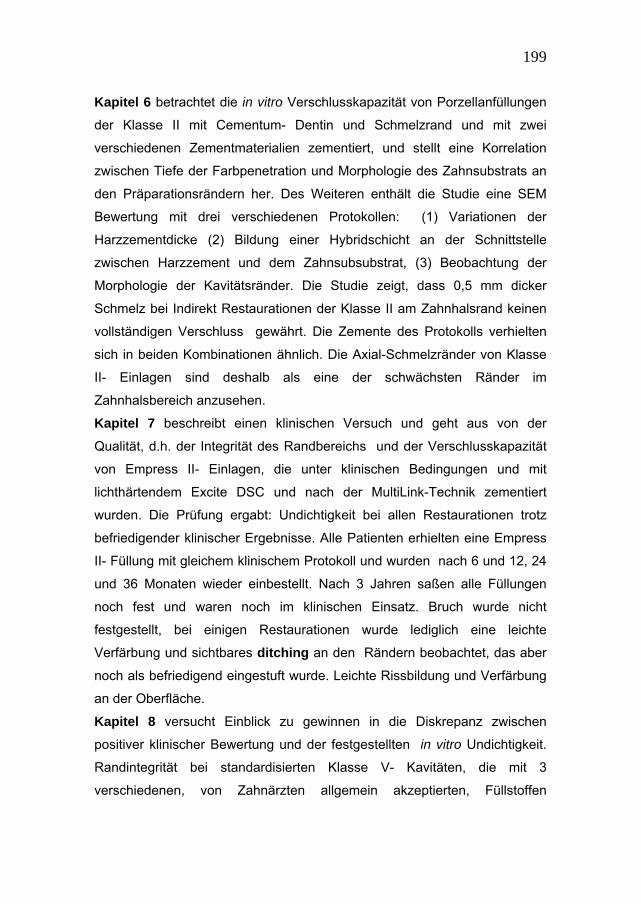
199
Kapitel 6 betrachtet die in vitro Verschlusskapazität von Porzellanfüllungen
der Klasse II mit Cementum- Dentin und Schmelzrand und mit zwei
verschiedenen Zementmaterialien zementiert, und stellt eine Korrelation
zwischen Tiefe der Farbpenetration und Morphologie des Zahnsubstrats an
den Präparationsrändern her. Des Weiteren enthält die Studie eine SEM
Bewertung mit drei verschiedenen Protokollen: (1) Variationen der
Harzzementdicke (2) Bildung einer Hybridschicht an der Schnittstelle
zwischen Harzzement und dem Zahnsubsubstrat, (3) Beobachtung der
Morphologie der Kavitätsränder. Die Studie zeigt, dass 0,5 mm dicker
Schmelz bei Indirekt Restaurationen der Klasse II am Zahnhalsrand keinen
vollständigen Verschluss gewährt. Die Zemente des Protokolls verhielten
sich in beiden Kombinationen ähnlich. Die Axial-Schmelzränder von Klasse
II- Einlagen sind deshalb als eine der schwächsten Ränder im
Zahnhalsbereich anzusehen.
Kapitel 7 beschreibt einen klinischen Versuch und geht aus von der
Qualität, d.h. der Integrität des Randbereichs und der Verschlusskapazität
von Empress II- Einlagen, die unter klinischen Bedingungen und mit
lichthärtendem Excite DSC und nach der MultiLink-Technik zementiert
wurden. Die Prüfung ergabt: Undichtigkeit bei allen Restaurationen trotz
befriedigender klinischer Ergebnisse. Alle Patienten erhielten eine Empress
II- Füllung mit gleichem klinischem Protokoll und wurden nach 6 und 12, 24
und 36 Monaten wieder einbestellt. Nach 3 Jahren saßen alle Füllungen
noch fest und waren noch im klinischen Einsatz. Bruch wurde nicht
festgestellt, bei einigen Restaurationen wurde lediglich eine leichte
Verfärbung und sichtbares ditching an den Rändern beobachtet, das aber
noch als befriedigend eingestuft wurde. Leichte Rissbildung und Verfärbung
an der Oberfläche. Kapitel 8 versucht Einblick zu gewinnen in die Diskrepanz zwischen
positiver klinischer Bewertung und der festgestellten in vitro Undichtigkeit.
Randintegrität bei standardisierten Klasse V- Kavitäten, die mit 3
verschiedenen, von Zahnärzten allgemein akzeptierten, Füllstoffen

200
restauriert wurden, nämlich: Gold, Amalgam, und Komposite sowie einem 3-
Stufen Dentin Bonding-System.
Kerben am Zahnhalsrand wurden Die Farbpenetration am Zahnhalsrand wurde untersucht und jede Probe
wurde nach SEM bewertet. Bei Klasse V- Restaurationen gewährten Gold
und Komposite einen besseren Randschluss als Amalgam, wobei zu
berücksichtigen ist, dass selbst bei nicht adhäsiver Restaurationstechnik
z.B. mit Kompakt- Gold befriedigende Ergebnisse erzielt wurden.
Aus den Beobachtungen von Undichtigkeit bei Methylenblau- Verfärbung
lassen sich folgende Schlussfolgerungen ziehen:
Wesentlich größere mikroskopische Undichtigkeit am Zahnhalsrand als am
Okklusalrand der Restauration. Besserer Randschluss durch Aufstreichen
einer dünnen Schicht Flüssigkomposits am Zahnhalsrand, zur Haftung unter
dem verformbaren Komposit. Die Verwendung eines selbstverätzenden
Primers zur Behandlung des Zahnsubstrats verursachte am Okklusalrand
größere Undichtigkeit als Phosphorsäure.
Bei der Prüfung der Verschlussfähigkeit der einzelnen Haftkombinationen
schlossen die einzelnen Materialkombinationen gleich gut ab, obwohl bei
Verätzen mit Phosphorsäure, die Schmelzränder weit besser verschlossen
wurden als mit Selbst-verätzendem Primer und selbstverätzendem Bonder.
Zementkombinationen und Arbeitsverfahren können Verschlussfähigkeit von
zementierten Füllungen beeinflussen. Zahnschmelz in 0,5 mm Dicke am
Zahnhalsrand von Indirekt-Restaurationen der Klasse II konnte keinen
Verschluss gewährleisten.
Gold- und Porzellanfüllungen wurden mit RelyX Unicem, Fuji und Variolink II
zufrieden stellend verschlossen und gewährleisteten einen adäquaten
Verschluss auf Zahnschmelz und Dentin.
Gold und Kunststoffharz zeigen ein gleiches Verhalten gegenüber
mikroskopischer Undichtigkeit und verschlossen besser als Amalgam.

201
Die klinische Studie verwendete Empress II und Variolink; während der
gesamten Beobachtungszeit löste sich keine Füllung und alle Füllungen
waren noch im klinischen Einsatz.
Die Diskrepanz zwischen in vitro Verfärbung an der Schnittstelle der
Restauration und der klinischen Akzeptanz muss noch weiter untersucht
werden.
Anhang
Untersuchungen der in vitro Undichtigkeit bei Adhäsivrekonstruktionen
werden weitgehend als Hinweis auf eine anhaltende Wand zu Wand-
Integrität verstanden. Eine Preliminar- Studie besagt, dass die
Methylenblaufärbung per se noch nicht auf den Verlust von Haftung
hinweist wie Mikro-Zugfestigkeit-Messungen ergaben. Die Proben wurden
für den Mikro-Zugfestigkeit Test vorbereitet (Kompositharz an Dentin
gebondet mit Hilfe eines Prime and Bond Dentaladhäsivs ), danach wurde
eine Hälfte zwei Stunden in einer Methyklenblau-Bad getaucht und auf
Mikro-Zugfestigkeit getestet.(Abb. 1 und 2). Beide Gruppen erzielten die
gleichen Meßwerte, wobei bei der Gruppe des Methylenblau-Bads an den
Schadstellen Verfärbungen auftraten ( Adäsivschnittstelle).
Die Farbpenetration, insbesondere die mit niedrigerem Undichtigkeits-
Meßwert, entsteht wahrscheinlich durch Diffusion kleiner Methylenblau –
Moleküle, nicht durch austretende Flüssigkeit und beeinträchtigt die Haftung
damit nicht. Die auftretenden Verfärbungen könnten ein weiterr Hinweis auf
eine Teil- Umwandlung des Harzes sein,nicht aber auf tatsächliche
Undichtigkeit. (DeGee AJ, Ten Harkel-Hagenaar E, Davidson CL.Color dye
for identification of completely cured composite resins.J Prosthet Dent. 1984
Nov; 52 (5) 626-31).
In einer anderen Preliminar- Studie wurde eine Klumpen Dentin-Bonding in
einer halbierten Kapsel polymerisiert und in ein Methylenblau- Bad getaucht.
Vier Tage später wurden die Proben gewaschen und nicht nur an der

202
Oberfläche, sondern auch im Inneren waren Verfärbungen aufgetreten.
Gehärtetes Harz verfärbt sich nur unvollständig und die Aufnahme von
Methylenblau ist in erster Linie auf die hydrophilen Monomere des Dentin –
Bondingmittels zurückzuführen. ( Abb. 3,4,5 ).
Die Gegenüberstellung von Verfärbung und Undichtigkeit wird Gegenstand
weiter Untersuchungen sein, um festzustellen, inwiefern Färbung Aufschluss
über die Zahnrandintegrität in Restaurationen gibt.
In einem zweiten Ansatz wird untersucht werden auf welch engem Raum
Streptococcus Mutans mit Hilfe von kalibrierten Mikroröhren und
Lebendbakterien Kolonien bilden können.
Abb. 1 Probestück für die Prüfung der Mikro-Zugfestigkeit
Abb. 2 Probestück nach der Prüfung . Man beachte den Farbstoff an der
Schnittstelle
Abb. 3 polymerisierte Dentin-Bonding Proben in einer offenen Kapsel
Abb. 4 Probe nach 4-tägigem Methylenblau- Bad
Abb. 5 Teil der Probe im Methylenblau-Bad
203
Figures Fig. 1. Specimen ready for micro-tensile test.
Fig. 2. Specimen after micro-tensile test: note the presence of the staining agent at the interface
area.

204
Fig 3. Dentin bonding agent specimens polymerised in needle cap.
Fig. 4. Specimen after four days dwelling in a methylene blue solution.

205
Fig. 5. Section of the specimen dipped in methylene blue
206
Chapter 11
References
ADA Council on Scientific Affairs/ADA Council on Dental Benefit Programs.
Statement on posterior resin-based composites. J Am Dent Assoc 1998;
129: 1627-1628.
Adair PJ, Grossman DG. The castable ceramic crown. Int J Period Rest
Dent 1984; 4: 32–38.
Affleck MS, Denehy GE, Vargas MA. Microleakage with incremental vs bulk
placement utilizing condensable composites. J Dent Res 1999; 78: 155.
Alani AH, Toh CG. Detection of microleakage around dental restorations: a
review. Op Dent 1997; 22(4): 173-185.
Alavi AA, Kianimanesh N. Microleakage of direct and indirect composite
restorations with three dentin bonding agents. Op Dent 2002; 27: 19-24.
Almeida JB, Platt JA, Oshida Y, Moore BK, Cochran MA, Eckert GJ. Three
different methods to evaluate microleakage of packable composites in class
II restorations. Op Dent 2003; 28: 453-460.
Andrews JT, Hembree JH Jr. Marginal leakage of amalgam alloys with high
content of copper: a laboratory study. Op Dent 1980; 5: 7-10.
Anusavice KJ. Quality evaluation of dental restorations. Chicago:
Quintessance, 1989.
Apicella A, Raddi S, Ausiello P, et al. FEM study of shrinkage stress build-up
on adhesive restorations. J Dent Res 1997; 76: 49 (Abstr 435).
Attal JP, Degrange M. Influence de l’orientation des prismes et du traitment
de surface sur l’adhesion et l’adherence a l’email. J Biomater Dent 1996; 11:
41-57.
Audenino G, Bresciano ME, Bassi F, Carossa S. In vitro evaluation of fit of
adhesively luted ceramic inlays. Int J Prosthodont 1999; 12: 342-347.

207
Ausiello P, Apicella A, Davidson CL. Effect of adhesive layer properties on
stress distribution in composite restorations--a 3D finite element analysis.
Dent Mater 2002; 18: 295-3003.
Banks RG. Conservative posterior ceramic restorations: a literature review. J
Prosthet dent 1990; 63(6): 619-626.
Bauer JG, Henson JL. Microleakage of direct filling materials in class V
restorations using thermal cycling. Quintessence Int 1985;16(11): 765-769.
Bayne SC, Heymann HO, Wilder AD, et al. Clinical performance of bonding
systems with and without hybrid layers. J Dent Res 1996; 75: 23 (Abstr 47).
Belli S, Inokoshi S, Ozer F, Pereira PNR, Ogata M, Tagami J. The effect of
additional enamel etching and a flowable composite to the interfacial
integrity of class II adhesive composite restorations. Op Dent 2001; 26: 70-
75.
Ben-Amar A, Cardash HS, Judes H. The sealing of the tooth-amalgam
interface by corrosion products. J Oral Rehab 1995; 22(2): 101-104.
Bessing C, Molin M. An in vivo study of glass ceramic (Dicor) inlays. Acta
Odont Scand 1990; 48: 351–356.
Beznos C. Microleakage at the cervical margin of composite Class II cavities
with different restorative techniques. Oper Dent 2001; 26: 60-69.
Binns D. The chemical and physical properties of porcelain. In: J.W.
McLean, Editor, Dental Ceramics: Proceeding of the First International
Symposium on Ceramics, Quintessence, Chicago 1983:,41–83.
Blackwood HJJ. Intermediate cementum. Br Dent J 1957; 102: 345-350.
Bosshardt DD, Selving KA. Dental cementum: The dynamic tissue covering
the root. Periodontal 2000 1997; 13: 41-75.
Bradford EW. Microanatomy and histochemistry of dentin. In: Miles AEW.
Structural and chemical organization of teeth. New York: Academic Press,
1967; Vol II, 49.
Bränström M, Vojinovic O. Response of dental pulp to invasion of bacteria
round threefilling materials. J Dent r Child 1976; 43: 15-21.
208
Brännström M, Nordenvall KJ. Bacterial penetration, pulpal reaction and the
inner surface of enamel bond, composite fillings in etched and un etched
cavities. J Dent Res 1978; 57: 3-10.
Branstrom M. Dentin and pulp in restorative dentistry. London: Wolfe
Medical Publ., 1982.
Branstrom M. Etiology of dentin Hypersensivity. Proc Finn Dent So 1992; 88
(Suppl. 1): 7-13.
Cagidiaco MC, Ferrari M. Bonding to dentin: Mechanism morphology and
efficacy of bonding resin composites to dentin in vitro and in vivo.
Amsterdam, University of Amsterdam, Ph D Thesis, De Batte Ed. 1995.
Cagidiaco MC, Vichi A, Ferrari M. SEM evaluation of outside dentin-
cementum layer at cervical margins of Class II restorations. CED-IADR
Congress, Lubliana, September 1995.
Cagidiaco MC, Ferrari M, Garberoglio R. Dentin contamination protection
after mechanical preparation for veneering. Am J Dent 1996;9(2): 57-60.
Cagidiaco MC, Ferrari M, Vichi A, et al. Mapping of tubule and intertubule
surface areas available for bonding in Class V and Class II preparations. J
Dent 1997; 25: 379-389.
Cagidiaco MC, Vichi A, Ferrari M. SEM evaluation of outside dentin-
cementum layer at cervical margins of Class II restorations. J Dent Res
1996; 75 (Abstr 28) 1220.
Camps J, Dejou J, Remusat M, About I. Factors influencing pulpal response
to cavity restoration. Dent Mat 2000; 16: 432-444.
Carvalho RM, Pereira JC, Yoshiyama M, Pashley DH. A review of
polymerisation contraction: the influence of stress development versus
stress relief. Op Dent 1996; 21(1): 17-24.
Cavel WT, Kelsey WP, Barkmeier WW , Blankenau RJ. A pilot study of the
clinical evaluation of castable ceramic inlays and a dual cure resin cement.
Quintessence Int 1988; 19: 247–252.

209
Chen HY, Hickel R, Setcos JC, Kunzelmann KH. Effects of surface finish
and fatigue testing on the fracture strength of CAD/CAM and pressed
ceramic crowns. J Prosthet Dent 1999; 82: 468-475.
Chen HY, Manhart J, Hickel R, Kunzelmann KH. Polymerization contraction
stress in light cured packable composite resins. Dent Mater 2001; 17: 253-
259.
Chuang SF, Liu JK, Jin YT. Microleakage and internal voids in Class II
composite restorations with flowable composite linings. Op Dent 2001; 26:
193-200.
Chuang SF, Liu JK, Chao CC, Liao FP, Chen YH. Effect of flowable
composite lining and operator experience on microleakage and internal
voids in Class II composite restorations. J Prosthet Dent 2001; 85(2): 177-
183.
Coli P, Brannstrom M. The marginal adaptation of four different bonding
agents in Class II composite resin restorations applied in bulk or in two
increments. Quintessence Int 1993; 24: 583-591.
Cooley R, Barkmeirer W. Dental shear bond strength, microleakage and
contraction gap of visible light- polymerised liner/bases. Quintessence Int
1991; 22: 467-474.
Cox CF. Evaluation and treatment of bacterial microleakage. AM J Dent
1994; 7: 293-295.
Crim GA, Chapman KW. Effect of placement techniques on microleakage of
a dentin bonded composite resin. Quintessence Int 1986; 17: 21-24.
Dagostin A, Ferrari M. In vivo bonding mechanism of an experimental
bonding system. Am J Dent 2001; 14: 103–108.
Dagostin A, M Ferrari, Effect of dual bonding technique on the bond strength
of ceramic restorations. Dent Mater 2002; 18: 304–310.
Davidson CL, De Gee AJ, Feilzer A. The competition between the composite
dentin bond strength and the polymerisation contraction stress. J Dent Res
1984; 63(12) :1396-1399.

210
Davidson CL, De Gee AJ,. Relaxation of polymerisation contraction stresses
by flown in dental composites. J Dent Res 1984; 63: 146-148.
Davidson CL. Resisting the curing contraction with adhesive composites. J
Prosthet Dent 1986; 55(4): 446-447.
Davidson CL. Glass Ionomer Bases Under Posterior Composites. In: Glass
Ionomers: The Next Generation. Proc. of the 2nd Int. Symp. on Glass
Ionomers. Ed.: P.R. Hunt, Philadelphia PA, USA. June 1994; p. 175-179
Davidson CL, Feilzer AJ. Polymerization shrinkage and polymerization
shrinkage stress in polymer-based restoratives. J Dent 1997; 25: 435-440.
Davidson CL, Davidson-Kaban SS. Handling of mechanical stresses in
composite restorations. Dent Update 1998; 25: 274-279.
Davidson CL. Luting Cement, the Stronghold or the Weak Link in Ceramic
Restorations. Advanced Engineering Materials 2001; 3, 10: 763-767.
Davidson-Kaban SS, Davidson CL, Feilzer AJ, de Gee AJ, Erdilek N. The
effect of curing light variations on bulk curing and wall-to-wall quality of two
types and various shades of resin composites. Dent Mater 1997; 13: 344-
352.
De Gee AJ, Ten Harkel-Hagenaar E, Davidson CL. Color dye for identification
of incompletely cured composite resins. J Prosthet Dent. 1984 Nov;52(5):626-
631.
De Gee, A.J. Personal communications, 2004.
Dietrich T, Lösche AC, Lösche GM. Marginal adaptation of direct composite
and sandwich restorations in Class II cavities with cervical margins in
dentine. J Dent 1999; 27(6): 119-128.
Dietschi D, Maeder M, Meyer J-M. In vitro resistance to fracture of porcelain
bonded to tooth. Quintessence Int 1990; 21: 823–831.
Dietschi D, Maeder M, Holz J. In vitro evaluation of marginal fit and
morphology of fired ceramic inlays. Quintessence Int 1992; 23: 271–278.
Dietschi D, Scampa G, Campanile U, et al. Marginal adaptation and seal of
direct and indirect Class II composite restorations: An in vitro evaluation.
Quintessence Int 1995; 26: 127- 138.

211
Dietschi D, Sperafico R. Adesive metal-free restorations. Current concepts
for the esthetic treatment of posterior teeth. Berlin: Quintessence 1997.
Dietschi D, Bindi G, Krejci I, Davidson C. Marginal and internal adaptation of
stratified compomer-composite Class II restorations. Oper Dent 2002; 27:
500-509.
Dixit V, Bini E, Drozda M, Blum P. Mercury inactivates transcription and the
generalized transcription factor TFB in the archaeon Sulfolobus solfataricus.
Antimic Ag Chem 2004; 48 (6): 1993-1999.
Dodes JE. The amalgam controversy: an evidence-based analysis. J Am
Dent Association 2001; 132(3): 348-355.
Doerr CL, Hilton TJ, Hermesch CB. Effect of thermocycling on the
microleakage of conventional and resin modified glass ionomer. Am J Dent
1996; 9(1): 19-21.
Donly KJ, Jensen ME. Posterior composite Class II restorations: In vitro
comparison of preparation designs and restorations techniques. Dent Mater
1990; 6: 88-93.
Douvitsas G. Effect of cavity design on gap formation in Class II in
composite resin restorations. J Prosthet Dent 1991; 65(4): 475-479.
Duguid R. Copper-inhibition of the growth of oral streptococci and
actinomyces. Biomat 1983; 4(3):225-227.
Duncalf WV, Wilson NH. A comparison of the marginal and internal
adaptation of amalgam and resin composite restorations in small to
moderate-sized Class II preparations of conventional design. Quintessence
Int 2000; 31: 347-352.
Eakle WS, Ito RK. Effects of insertion technique on microleakage in mesio-
occluso-distal composite resin restorations. Quintessence Int 1990; 21: 369-
374.
Eick JD, Welch FH. Polymerization shrinkage of posterior composite resins
and its possible influence on postoperative sensitivity. Quintessence Int
1986 ; 17: 103–111.

212
Eick JD, Gwinnett AJ, Pashley DH, Robinson SJ. Current concepts on
adhesion to dentin. Critical Reviews of Oral Biology and Medicine 1997;
8(3): 306-335.
El Mowafi OM, Benmergui C, Levinton C. Meta- analysis on long-term
clinical performance of posterior composite restorations. J Dent 1994; 22:
33-43.
El Zohairy AA, De Gee AJ, Hassan FM, Feilzer AJ. The effect of adhesives
with various degrees of hydrophilicity on resin ceramic bond durability. Dent
Mater, 2004 in press.
Federation Dentaire Internationale, World Health Organization, World Dental
Federation, Consensus statement on dental amalgam. FDI World 1995 : 9-
10.
Feilzer AJ, De Gee AJ, Davidson CL. Setting stress in composite resin in
relation to configuration of the restoratives. J Dent Res 1987; 66(11): 1636-
1639.
Feilzer AJ, de Gee AJ, Davidson CL. Curing contraction of composites and
glass-ionomer cements. J Prosthet Dent 1988; 59(3): 297-300.
Feilzer AJ, De Gee AJ, Davidson CL. Increased wall-to wall curing
contraction in thin bonded resin layers. J Dent Res 1989 ; 68 : 48-50.
Feilzer AJ, de Gee AJ, Davidson CL. Quantitative determination of stress
reduction by flow in composite restorations. Dent Mater 1990; 6: 167-171.
Felden A, Schmalz G, Federlin M, Hiller KA. Retrospective clinical
investigation and survival analysis on ceramic inlays and partial ceramic
crowns: results up to 7 years. Clin Oral Invest 1998; 2: 161-167.
Fernandes CP, Chevitarese O. The orientation and directions of the rods in
dental enamel. J Prosthet Dent 1991; 65 : 793-800.
Ferrari M, Davidson CL. Sealing performance of Scotchbond Multi-Purpose-
Z100 in Class II restorations. Am J Dent 1996; 9: 145-149.
Ferrari M, Cagidiaco MC, Davidson CL. Resistance of cementum in Class II
and V cavities to penetration by an adhesive system. Dental Mater 1997; 13:
152-162.
213
Ferrari M, Mason PN, Fabianelli A, Cagidiaco MC, Kugel G, Davidson CL.
Influence of tissue characteristics at margins on leakage of class II in direct
porcelain restorations. Am J Dent 1999; 12: 134-142.
Ferrari M. “Advances in Glass-Ionomer Cements” in Davidson CL and Mjor
IA: Glass-Ionomer Cements. Quintessence Int, Berlin 1999: 137-148.
Ferrari M, Vichi A, Grandini S, Goracci C. Efficacy of a self-curing
adhesive/resin cement system on luting Vectris fiber posts into root canals: a
SEM investigation. Int J Prosthodont 2001; 14: 543–549.
Ferrari M, Garcia-Godoy F. Sealing ability of new generation adhesive-
restorative materials placed on vital teeth. Am J Dent 2002: 15(2): 117-28.
Finger WJ, Inoue M, Asmussen E. Effect of wettability of adhesive resins on
bonding to dentin. Am J Dent 1994; 7: 35-38.
Frankenberger R, Kramer N, Petschelt A. Technique sensitivity of dentin
bonding: Effect of application mistakes on bond strength and marginal
adaptation. Oper Dent 2001;4: 324-330.
Frankenberger R, Kramer N, Petschelt A: Technique sensitivity of dentin
bonding: effect of application mistakes on bond strength and marginal
adaptation. Oper Dent 2000; 25: 324-330.
FusayamaT. Indicationfor self-cured and light-cured adhesive composite
resins. J Prosth Dent 1992; 67: 46-51.
Gale MS, Darvell BW, Cheung GSP. Three-dimensional reconstruction of
microleakage pattern using a sequential grinding technique. J Dent 1994;
22(6): 370-375.
Gale MS, Darvell BW. Thermal cycling procedures for laboratory testing of
dental restorations. J Dent 1999; 27(2): 105-108.
Goracci C, Ferrari M, Grandini S, Monticelli F, Tay FR. Bonding of a self-
adhesive resin cement to dental hard tissues. J Adhes Dent 2003 (in press).
Griffiths BM, Watson TF, Sherriff M. The influence of dentine bonding
systems and their handling characteristics on the morphology and micro
permeability of the dentine-adhesive interface. J Dent 1999; 27: 63-71.
Grossman DG. Cast glass ceramics. Dent Clin North Am 1985; 29: 275.

214
Guzman AF, Moore BK, Andres CJ. Wear resistance of four luting agents as
a function of marginal gap distance, cement type and restorative material. Int
J Prosthodont 1997; 10:25-30.
Gwinnet AJ, Kanca J. Micromorphological relationship between resin and
dentin in vivo and in vitro. Am J Dent 1992; 5: 19-23
Gwinnett AJ, Tay FR, Pang KM, et al. Comparison of three methods of
critical evaluation of microleakage along restorative interfaces. J Prosthet
Dent 1995; 74: 575-585.
Gwinnett AJ. Chemically conditioned dentin: A comparison of conventional
and environment scanning electron microscopy findings. Dent Mater 1994;
10: 150-155.
Hahn P, Attin T, Gröfke E, Hellwig E. Influence of resin cement viscosity on
microleakage of ceramic inlays. Dent Mat 2001; 17: 191-196.
Hahn P, Schaller HG, Hafner P, Hellwig E. Effect of different luting
procedures on the seating of ceramic inlays. J Oral Rehabil 2000; 27: 1-8.
Hakimeh S, Vaidyanathan J, Houpt ML, Vaidyanathan TK, Von Hagen S.
Microleakage of compomer Class V restorations: effect of load cycling,
thermal cycling and cavity shape differences. J Prosthet Dent 2000; 83: 194-
203.
Haller B, Häßner K, Moll K. Marginal adaptation of dentin bonded ceramic
inlays: effect of bonding systems and luting resin composites. Op Dent 2003;
28-5: 574-584.
Han L, Okamoto A, Iwaku M. The effect of various clinical factors on
marginal enamel micro-cracks produced around composite restorations.
Dent Mat 1990; 11: 26-37.
Hara AT, Amaral CM, Pimenta LA, Sinhoreti MA. Shear bond strength of
hydrophilic adhesive systems to enamel. Am J Dent 1999; 12: 181-184.
Hass M, Arnetzl G, Wegscheider WA, König K, Bratschko RO. Klinische und
Werkstoffkundliche Erfahrungen mit Komposit, Keramik und Gold inlays.
Dtsch Zahnärzt Z 1992; 47: 18–22.

215
Hecht R, Ludstek M, Raia G. Tensile bond strength of first self adhesive
resin based dental material. J Dent Res 2002; 81: A-75.
Herrera M, Castillo A, Bravo M, Lièbana J, Carrion P. Antibacterial activity of
resin adhesive, glass ionomer and resin-modified glass ionomer cements
and a compomer in contact with dentin caries samples. Op Dent 2000; 25:
265-269.
Hickel R. Die zervikale füllung. Dtsch Zahnärzt Z 1994; 49(11): 13-19.
Hickel R, Manhart J, García-Godoy F. Clinical results and new developments
of direct posterior restorations. Am J Dent 2000; 13: 41D-54D.
Hickel R, Manhart J. Longevity of dental restorations in posterior teeth and
reasons for failure. J Adhesive Dent 2001; 3:45-64.
Hilton TJ, Ferracane JL. Cavity preparation factors and microleakage of
Class II composite restorations filled at intraoral temperatures. Am J Dent
1999; 12: 123-130.
Hilton TJ, Schwartz RS, Ferracane JL. Microleakage of four Class II resin
composite insertion techniques at intraoral temperature. Quintessence Int
1997; 28: 135-144.
Hilton TJ. Can modern restorative procedures and materials reliably seal
cavities? In vitro investigation. Transaction of Academy of Dental Materials
Meeting, Banff, 1998; vol 12: 21-74.
Hilton TJ. Can modern restorative procedures and materials reliably seal
cavities? In vitro investigations. Part 1.Am J Dent 2002;15:198-210.
Hilton TJ. Can modern restorative procedures and materials reliably seal
cavities? In vitro investigations. Part 2.Am J Dent 2002;15:279-289.
Hofmann N, Klaiber B, Heners M. Okklusale Randschlussqualität von Cerec-
Inlays nach mehrmonatiger Tragedauer. Dtsch Zahnärztl Z 1990; 45: 289–
292.
Hormati AA, Chan KC. Marginal leakage of compacted gold, composite
resin, and high copper amalgam restorations. J Prosthet Dent 1980; 44 (4):
418-422.

216
Horn HR. Porcelain laminate veneers bonded to etched enamel.
Dent Clin North Am. 1983 Oct;27(4):671-84.
Hung SH, Hung KS, Eick JD, Chappel RP. Marginal fit of porcelain-fused-to-
metal and two types of ceramic crown. J Prosthet Dent 1990; 63: 26–31.
Ianzano JA, Gwinnett AJ. Clinical evaluation of Class V restorations using a
total etch technique: 1 year results. Am J Dent 1993; 6(4): 207-210.
Ibbetson R, Eder A. Tooth surface loss. BDJbooks 2000: 3-8.
Inokoshi S., Van Meerbeck B, Willems G, Lambrechts P, Braem M,
VanherleG. Marginal accuracy of CAD/CAM inlays made with the original
and the updated software. J Dent 1992; 20: 171–177.
Inoue S, Van Meerbeek B, Vargas M, Yoshig’da Y, Lambrechts P, Vanherle
G. Advanced adhesive dentistry, 3rd Int Kuraray Symposium, Como, Italy
2000.
Jensen ME, Redford AD, Wilson BT. Posterior etched porcelain restorations.
an in vitro study. Compen Contin Edu Dent 1987; 8: 615–621.
Kanca J. Resin Bonding to wet substrate. I. Bonding to dentin. Quitessence
int 1992; 23: 39-41.
Kanca J. Wet bonding: effect of drying time and distance. Am J Dent 1996;
9: 273-276
Kanca J. Investigation into dentin adhesion mechanism. J Dent Res 1997;
76: 277 (Abstr 2111).
Kawai K. Effect of eluate from composite resin on Gtase and growth of
Streptococcus Mutans. Jpn J Conserv Dent 1988; 31: 322-351.
Kawai K, Isemberg PD, Leinfelder KF. Effect of gap dimension on composite
cement wear. Quintessence Int 1994; 25: 53-58.
Kawai K, Tsuchitani Y. Effects of resin composite components on
glucosyltransferase of cariogenic bacterium. J Biomed Mat Res 2000;51:
123-127.
217
Kelly JR, Nishimura I, Campbell SD. Ceramics in dentistry: historical roots
and current prospectives. J Prosthet Dent 1996; 75: 18-32.
Kemp-Scholte CM, Davidson CL. Complete marginal seal of class V resin
composite restorations effected by increased flexibility. J Dent Res 1990; 69:
1240-1243.
Kidd EAM. Microleakage: a review. J Dent 1976; 4: 199-205.
Kramer N, Frankenberger R, Pelka M, Petschelt A. IPS Empress inlays and
onlays after four years- a clinical study. J Dent 1999; 28: 325-331.
Krejci I, Lutz F. Marginal adaptation of class V restorations using different
restorative techniques. J Dent 1991; 19: 24-32.
Krejci I, Lutz F, Reimer M. Marginal adaptation and fit of adhesive ceramic
inlays. J Dent 1993; 21: 39–45.
Krejci I, Lutz F, Reimer M, Heinzmann JL. Wear of ceramic inlays, their
enamel antagonists, and luting cements. J Prosthet Dent 1993; 69: 225–229.
Iida K, Inokoshi S, Kurosaki N. Interfacial gaps following ceramic inlay
cementation vs direct composites. Op Dent 2003; 28: 445-452.
Imazato S. Antibacterial properties of resin composites and bonding
systems. Dent Mat 2003; 19: 449-457.
Labella R, Lambrechts P, Van Meerbeek B, et al. Polymerization shrinkage
and elasticity of flowable composites and filled adhesives. Dent Mat 1999;
15: 128-137.
Larsen IB,. Munksgaard EC. Effect of human saliva on surface degradation
of composite resins. Scand J Dent Res 1991; 99: 254–261.
Lee IB, Um CM. Thermal analysis on the cure speed of dual cured resin
cements under porcelain inlays. J Oral Rehabil 2001; 28: 186-197.
Lee WC, Eakle WS. Possible role of tensile stresses in the aetiology of
cervical erosive lesions of teeth. J Prosthet Dent 1984, 52(3): 374-380.
Leevailoj C, Cochran MA, Matis BA, Moore BK, Platt JA. Microleakage of
posterior packable resin composites with and without flowable liners. Op
Dent 2001; 26(3): 302-307.

218
Leinefelder KF, Bayne SC, Swift Jr EJ. Packable composites: overview and
technical considerations. J Esthet Dent 1999; 11: 234-249.
Leinefelder KF. New developments in resins restorative systems. J Am Dent
Assoc 1997; 58: 484-487.
Leinefelder KF. Posterior composite resins: the materials and their clinical
performance. J Am Dent Assoc 1995; 126: 663-676.
Leinfelder KF, Isenberg BP, Essig ME. A new method for generating ceramic
restorations: a Cad–Cam system. J Am Dent Assoc 1989; 118: 703–708.
Löfstrom LH, Barakat MM. Scanning electron microscopic evaluation of
clinically cemented cast gold restorations. J Prosth Dent 1989;61:664-669.
Lösche GM. Marginal adaptation of Class II composite fillings:guided
polymerisation vs reduced light intensity. J Adhes Dent 1999; 1(1): 31-39.
Lundin SA, Noren JG. Marginal leakage in occlusally loaded, etched, Class
II composite resin restorations. Acta Odontol Scand 1991; 49: 247-254.
Lutz F, Krejici I, Barbakow F. Quality and durability of marginal adaptation in
bonded composite restorations. Dent Mater 1991; 7: 107-113.
Malament KA, Grossman DG. The cast glass-ceramic restoration. J Prosthet
Dent 1987; 57: 674–681.
Manhart J, Kunzelmann KH, Chen HY, Hickel R. Mechanical properties and
wear behaviour of light-cured packable composite resins. Dent Mater 2000;
16: 33-40.
Manhart J, Scheibenbogen-Fuchsbrunner A, Chen HY, Hickel R. A 2-year
clinical study of composite and ceramic inlays. Clin Oral invest 2000; 4: 192-
198.
Manhart J, Chen HY, Mehl A, Weber K, Hickel R. Marginal quality and
microleakage of adhesive Class V restorations. J Dent 2001; 29(2): 123-130.
Manhart J, Chen HY, Neuerer P, Scheibenbogen-Fuchsbrunner A, Hickel R.
Three-year clinical evaluation of composite and ceramic inlays. Am J Dent.
2001;14(2): 95-99.
Marquis RE. Antimicrobial actions of fluoride for oral bacteria. Can J
Microbiol 1995; 41(11): 955-964.

219
Martin DW. Interface leakage in microfilled composites, amalgam,
conventional composites and gold foil: a comparative in vitro study. J Calif
Dent Association 1981; 1(1) : 33-39.
Martin T. Schmeltzmikrostrukturen bei Saugetieren. In: Alt KW, Tucrp J. Die
evolution der zahne. Philogenie –ontogenie variation. Berlin: Quintessenz,
1997.
McCabe JF, Walls AW. Properties used to characterize materials. Applied
Dental Materials. 8th ed Oxford: Blackwell Science; 1998: 4-28.
McCoy RB, Anderson MH, Lepe X, Johnson GH. Clinical success of class V
composite resin restorations without mechanical retention. J Am Dent
Association 1998; 129(5): 593-599.
McCurdy CR. A comparison of in vivo and in vitro microleakage of dental
restorations. J Am Dent Association 1974;88(3): 592-602.
Medina J. Matt gold-gold foil restoration. Journal of the American
Association of Gold Foil Operators 1969; 12-1: 13-26.
Miguez PA, Pereira PNR, Suh IB et al. Gap formation and bond strength of
composites lined with flowable resin. J Dent Res 2001; 80 (Sp. Issue abstr.
n. 1270)194.
Millediing P, Örtengren U, Karlsson S. Ceramic inlay systems: some clinical
aspect. J Oral Rehabil 1995; 22: 571-580.
Mjör IA. Amalgam and composite resin restorations: longevity and reasons
for replacement. In: Anusavice K, Quality evaluation of dental restorations,
Chicago Quintessence 1989: 61-80.
Mjör IA. Long term cost of restorative therapy using different materials.
Scand J Dent Res 1992; 100: 60-65.
Mior IA, Toffenetti F. Secondary caries:a literature review with case reports.
Quintessence Int 2000; 31: 165-179.
Moello FS-TC, Feiltzer AJ, De Gee AJ, et al. The influence of the presence
of a bonding layer on marginal sealing of resin composite Class II
restorations. J Dent Res 1996; 75: 26 (Abstr 224).
220
Molin MK, Karlsson SL. A 3- year clinical follow-up study of a ceramic
(Optec) inlay system Acta Odontol Scand 1996; 54: 145-149.
Molin MK, Karlsson SL. A randomized 5-year clinical evaluation of 3 ceramic
inlay systems. Int J Prosthodont 2000; 13: 194-200.
Moore DS, Johnson WW, Kaplan I. A comparison of amalgam microleakage
with a 4-META liner and copal varnish. Int J Prosthodont 1995; 8: 461-466.
Moreira Jr G, Sobrinho APR, Nicoli JR, Bambirra EA, Farinas LM, Carvalho
MAR, Vieira EC. Evaluation of microbial infiltration in restored cavities- an
alternative method. J End 1999; 25:605-608.
Mota CS, Demarco FF, Camacho GB, Powers JM. Microleakage in ceramic
inlays luted with different resin cements. J Adhes Dent 2003; 5: 63-70.
Munecika T, Suzuki K, Nishiyama M, et al. A comparison of the tensile bond
strengths of composite resins to longitudinal and transverse sections of
enamel prisms in human teeth. J Dent Res 1984; 63: 1079-1082.
Nakabayashi N, Nakamura M, Yasuda N. Hybrid layer as dentin bonding
mechanism. J Esthet Dent 1991; 3: 133-138.
Nakabayashi N, Ashizawa M, Nakamura M. Identification of a resin dentin
hybrid layer in vital human dentin created in vivo: Durable bonding to vital
dentin. Quit int 1992; 23: 135-141.
Nakabayashi N, Pashley DH. Hybridization of hard dental tissues. Berlin:
Quintessence, 1998; 20-30.
Norman GR, Streiner DL . PDQ statistics. BC Decker inc 1999. Hamilton.
Olgart L, Brännstöm M, Johnson G. Invasion of bacteria into dentinal
tubules: Experiments in vivo and in vitro. Act Odontol Scand 1974 ; 32(1):
61-70.
Opdam NJM, Roeters JJM, Burgersdijk RCW. Microleakage of Class II box-
type composite restorations. Am J Dent 1998; 11: 160-164.
Özturk N, Aykent F. Dentin bond strengths of two ceramic inlay systems
after cementation with three different techniques and one bonding system. J
Prosthet Dent 2003; 89: 275-281.

221
Pallesen U. Clinical evaluation of CAD/CAM ceramic restorations: 6-years
report in CAD/CAM esthetic dentistry. Cerec 10 year anniversary
symposium. (Ed Mormann) Quintessenz Berlin 1996: 241-253.
Pashley DH. Clinical considerations of microleakage. J Endodont 1990; 16: 70-
77.
Pashley DH, Ciucchi B, Sano H, et al. Permeability o dentin to adesive
agents. Quint int 1993; 24: 618-631
Pashley DH, Ciucchi B, Sano H, et al. Bond strenght versus dentine structure:
A modelling approach. Archs Oral Biol 1995; 40: 1109-1118.
Pashley DH, Sano H, Ciucchi B, Yoshiyama M, Carvalho RM. Adhesion
testing of dentin bonding agents: a review. Dent Mater 1995; 11: 117-125.
Pashley DH, Tay FR. Aggressiveness of contemporary self-etching
adhesives. Part I: Depth of penetration beyond dentin smear layers. Dent
Mater 2001; 17: 296-308.
Penschke A, Blunck U, Roulet JF. Influence of incorrect application of
Optibond FL on the marginal adaptation of Class V restorations. Am J Dent
2000; 13(5): 239-244.
Perdigão J. An ultra-morphological study of human dentine exposed to
adhesive systems. Thesis. Leuven, Belgium: Catholic University of Leuven;
1995.
Peutzfeld A. Resin composites in dentistry : the monomer systems. Eur J
Oral Sci 1997; 105: 97-116.
Peyton FA, Craig RG (1971) Restorative Dental Materials ,Mosby 4th
edition, St Luis: 358-397.
Pfrentzschner HU. Biomechanik des zanhschmelzes. In: Alt KW, Tucrp J.
Die evolution der zahne. Phylogenie-Ontogenie variation. Berlin Quintessenz
1997.
Picard B, Jardel V, Tirlat G. Ceramic bonding: Reliability. In Degrange M,
Roulet JF. Minimally invasive restoration with bonding. Chicago
Qiuntessence 1997; 103-127.

222
Piwowarczyk A, Berge HX, Lauer H-Ch, Soresen JA. Shear bond strength of
cements at zirconium and lithium di-silicate ceramics. J Dent Res 2002; 81:
A-401.
Powell LV, Gordon GE, Johnson GH. Clinical comparison of Class V resin
composite and glass ionomer restorations. Am J Dent 1992; 5(5): 249-252.
Radlanski RJ, Jager A, Seidi W, et al. Uber die ausrichtung der prismen im
zahnschmelz menschlicher permanenter zahne. Anat Anz 1990; 170: 329-
337.
Radlanski RJ. Prism arrangement in early layers in human fetal enamel. In :
Radlanski RJ, Renz H. Proceeding of the 10th international symposium on
dental morphology. Berlin: C & M Brunne, 1995.
Raskin A D’Hoore W, Gonthier S, Degrange M, Dejou J. Reliability of in vitro
microleakage test: a literature review.J Adhesiv Dent 2001; 3: 295-308.
Raskin A, Tassery H, D’Hoore W, Gonthier S, Vreven J, Degrange M, Déjou
J. Influence of the number of section on reliability of in vitro microleakage
evaluations. Am J Dent 2003; 16(3): 207-210 .
Rees JS. The role of cuspal flexure in the development of abfraction lesions:
a finite element study. Euro J Oral Sci 1998; 106(6): 1028-1032.
Reich E, Schmalz G, Federlin M. Randspaltverhalten von Keramik- und
Konpositinlays in vitri. Dstch Zahnärztl Z 1990; 45: 656–660.
Reich E, Schmalz G, Federlin M. Randspaltverhalten von Keramik- und
Konpositinlays in vitri. Dstch Zahnärztl Z 1990; 45: 656–660.
Rigsby DF, Retief DH, Russel CM, Denys FR. Marginal leakage and
marginal gap dimension of three dentinal bonding system. Am J Dent 1990;
3: 289-294.
Robinson PB, Moore BK, Swartz ML. Comparison of microleakage in direct
and indirect composite resin restorations in vitro. Open Dent 1987;12: 113-
116.
Roulet J.F., Reich T, Blunck T, Noack M. Quantitative margin analysis in the
scanning electron microscope. Scan Elect Microsc 1989; 3: 147–159.
Roulet JF. Marginal integrity: clinical significance. J Dent 1994; 22: 9-12.

223
Roulet JF Benefits and disadvantages of tooth-colored alternatives to
amalgam. J Dent 1997; 25:459-473.
Roulet JF. Longevity of glass ceramic inlays and amalgam-results up to 6
years. Clin Oral Invest 1997; 1: 40 -46.
Sano H, Ciucchi B. Nanoleakage: leakage within the hybrid layer. Oper Dent
1995; 20: 18-25.
Sano H, Takatsu T, Ciucchi B, et al. Nanoleakage within the hybrid layer.
Oper Dent 1995; 20 : 18-25.
Sano H, Kanemura N, Burrow MF, et al. Effect of operator variability on
dentin adhesion: Students vs. dentists. Dent Mater 1998; 17: 51-58.
Savitt ED, Malement KA, Socransky SS, Melcer AJ, Backmann KJ. Effect of
colonization of oral microbiota by a cast Glass ceramic restoration. Int J
Period Rest Dent 1987; 7: 23–30.
Schubach P, Krejci I, Lutz F. Dentin bonding: effect of tubule orientation on
hybrid layer formation. Eur J Oral Sci 1997:105: 344-352.
Schuckar M, Geurtsen W. Proximo-cervical adaptation of Class II composite
restorations after thermo cycling: a quantitative and qualitative study. J Oral
Rehab 1997 ; 24(10) : 766-775.
Schüpbach P, Guggenheim B, Lutz F. Human root caries. Oral Path Med
1989; 18(3): 146-156.
Sindel J, Frankenberger R, Kramer N, Petschelt A. Crack formation of all
ceramic crowns dependent on different core build-up and luting materials. J
Dent 1999; 27: 175)
Sjodin L, Uunsitalo M, van Dijken J. Resin modified glass ionomer cements.
In vitro microleakage. Swed Dent J 1996; 20(3): 77-86.
Sjögren G, Molin M, van Dijken JWV. A 5-year clinical evaluation of ceramic
inlays cemented with dual-cured or chemically cured resin composite luting
agent. Acta Odontol Scand 1998; 56: 263-267.
Skjörland KKR. Plaque accumulation on different dental filling materials.
Scand J Dent Res 1973; 81: 538-542.

224
Skogendal O, Erikensen HM. Effect of composite resin restorations in
monkey’s teeth with experimentally induced pulpitis. Scand J Dent Res
1976; 84(5): 297-303.
Smales RJ, Hawthorne WS. Long-term survival and cost-effectiveness of
five dental restorative materials used in various classes of cavity
preparations. Int Dent J 1996; 46: 126-130.
Söderholm KLM. Correlation of in vivo and in vitro performance of adhesive
restorative matherials. Dent Mater 1991; 7:74-83.
Sparrius O, Grossman ES. Marginal leakage of composite resin restorations
in combination with dentinal and enamel bonding agents. J Prosthet Dent
1989; 61(6): 678-684.
Stangel I, Nathanson D, Hsu CS. Shear strength of the composite bond to
etched porcelain. J Dent Res 1987; 66: 1460–1465.
Staninec M, Mochizuki A, Tanizaki K, Jukuda K, Tsuchitani Y. Interfacial
space, marginal leakage and enamel cracks around composite resins. Op
Dent 1986; 11: 14-24.
Stibbs GD. Direct golds in dental restorative therapy. Op Dent 1980; 5(3):
107-114.
Studer S, Lehner C, Brodbeck U, Shärer P. Short-term results of IPS
Empress inlays and onlays. J Prosthodont 1996; 5: 277-287.
Tay FR, Gwinnett AJ Pang KM, et al. Variability in microleakage observed in
a total-etch wet-bonding technique under different handling conditions. J
Dent Res 1995; 74: 1168-1178.
Tay FR, Gwinnett AJ, Wei SH. Micromorphological spectrum from overdrying
to overwetting acid-conditioned dentin in water-free, acetone based, single
bottle primer/adhesives. Dent Mater 1996; 12: 236-244.
Tay FR, Gwinnett AJ, Wei Shy. Ultrastructure of the resin-dentin interface
following reversible and irreversible rewetting. Am J Dent 1997; 10: 77-82.
Thierfelder C, Fuhrmann I, Knappe M. Vergleichende Untersuchung zur
Passgenauigkeit des Kompositinlays Estilux posterior CVS. Die Quintessenz
1991; 9: 1399–1407.

225
Thonemann BM, Federlin M, Schmalz G. SEM analysis of marginal
expansionand gap formation in Class II composite restorations. Dent Mater
1997; 13: 192-197.
Thonemann B, Federlin M, Shmalz G, Grundler W. Total bonding vs
selective bonding: marginal adaptation of Class II composite restorations.
Oper Dent 1999; 24: 261-271.
Thordrup M, Isidor F, Hörsted-Bindslev P. Comparison of marginal fit and
microleakage of ceramic and composite inlays: an in vivo study. J Dent
1994; 22: 147–154.
Thye RP. A comparison of the marginal penetration of direct filling golds
using Ca45. J Am Acad Gold Foil Op 1967; 34 (4): 12-16.
Thylstrup A, Bille J, Qvist V. Radiographic and observed tissue in approximal
carious lesions at the time of operative treatment. Caries Res 1986; 20: 75-
84.
Titley K, Chernecky R, Chan A, et al. The composition and ultrastructure of
resin tags in etched dentine. Am J Dent 1995; 8: 224-230.
Titley K, Chernecky R, Maric B. Penetration of a dentin bonding agent into
dentin. Am J Dent 1994; 7: 190–194.
Tjan AH, Bergh BH, Linder C. Effect of various incremental techniques on
the marginal adaptation of class II restoration. J Prosthet Dent 1992; 67: 62-
66.
Torstensen B, Brännström M. Composite resin contraction gaps measured
with a fluorescent resin technique. Dent Mater 1988; 4 : 238–245.
Tung FF, Estafan D, Scherer W. Microleakage of a condensable resin
composite: an in vitro investigation. Quintessence Int 2000; 31: 430-434.
Tyas MJ. Clinical performance of two dentin adhesives: 2-year results. Aust
Dent 1996; 41: 324-7.
Unterbrink GL, Liebenberg WH. Flowable resin composites as filled
adhesives; literature review and clinical recommendations. Quintessence Int
1999; 30(4): 249-257.

226
Vacel JS, Gher ME. Cementum anomalies of the dentogigngival junction. Int
J Perio Dent 1993; 5: 443-449.
Van Dijken JWV, Höglund-Åberg C, Olofsson AL. Fired ceramic inlays: a 6-
year follow up. J Dent 1998; 26: 219-225.
Van Dijken J, Horsted P. Directed polymerisation shrinkage in Class II
cavities in vivo. J Dent Res 1998; 77: 1326.
Van Meerbeek BV, Inokoshi S, Willems G. Marginal adaptation of four tooth-
coloured inlay systems in vivo. J Dent 1992; 20: 18–29.
Van Meerbeck B, Braem M, Lambrechts P, Vanherle G. Morphological
characterization of the interface between resin and sclerotic dentine. J Dent
1994; 22(3): 141-146.
Van Merbeeck B, Peumans M, Verschueren M, et al. Clinical status of ten
dentin adhesive systems. J Dent Res 1994; 73: 1690-1702
Van Meerbeek B. Perdigao J, Lambrechts P, Vanherle G. The clinical
performance of adhesives. J Dent 1998; 26: 1-20.
Van Meerbek B., Y. Yoshida and P. Lambrechts, A TEM study of two water-
based adhesive systems bonded to dry and wet dentin. J Dent Res 1998;
77: 50–59.
Van Noort R. Introduction to dental materials. Mosby pub 2002: 267.
Vanherle G, Lambrechts P, Braem M. Overview of the clinical requirements
for posterior composites. In: G. Vanherle and D.C. Smith, Editors, Posterior
composite resin dental restorative materials, 3M Co, St Paul, MN 1985: 21–
40.
Vichi A, Ferrari M, Davidson CL. In vivo leakage of an adhesive system with
and without NaOCl as preatreatment. J Dent Res 1997; 76: 398 (Abstr
3077).
Wakabayashi Y, Kondou Y, Suzuki K, et al. Effect of dissolution of collagen
on adhesion to dentin. Int J Prosthodont 1994; 7: 302-306.
Wassell RW, Walls AWG, McCabe JF. Direct composite inlays vs
conventional composite restorations: 5-year follow-up. J Dent 2000; 28: 375-
382.

227
Watanabe I, Nakabayashi N, Pashley DH. Bonding to ground dentin by a
phenyl-P self-etching primer. J Dent Res 1994; 73: 1212-1220.
Wood RE, Maxymiw WG, McComb D. A clinical comparison of glass
ionomer and silver amalgam restorations in the treatment of Class V caries
in xerostomic head and neck cancer patients. Op Dent 1993; 18(3): 94-102.
Yamashita J, Takakuda K, Shiozawa I, Nagasawa M, Miyairi H. Fatigue
behavior of the zinc-phosphate cement layer. Int J Prosthodont 2000; 13:
321-326.
Yap AUJ. Effects of storage, thermal and load cycling on a new reinforced
glass ionomer cement. J Oral Rehab 1997; 25(1): 40-44.
Yazici AR, Baseren M, Dayangaç B. The effect of flowable resin composite
on microleakage in Class V cavities. Op Dent 2003; 28: 42-46.

228
Acknowledgements
The present thesis is respectfully submitted to Prof Piero Tosi of the
University of Siena, to Prof Alberto Auteri, Dean of the Faculty of Medicine,
University of Siena, to Prof Egidio Bertelli, Vice-Dean of the Faculty of
Medicine and Director of the Department of Dental Science and to Prof
Marco Ferrari, Pro-Rector for International Affairs and President of Dental
School, University of Siena. This research has been carried out in the
Dental Materials’ Department at the School of Dentistry at Siena University.
I wish to thank everyone who has been involved in this Project, among
these are:
Prof Marco Ferrari, my Promotor, for the chance he gave me to enter for this
magnificent Program and the precious suggestions and encouragements.
Prof Carel Davidson, my Co-promotor, who provided guidance, scientific
advice and continued encouragement throughout this project and without
whose help, this work would not have come to fulfilment. It was a great
pleasure for me to have his support, be it both on a professional and
friendship level. I’ll never forget his help.
Prof Richard Van Noort, who helped me to focus on my vision of this thesis.
A grateful thank you to many colleagues at the Dental Materials’ Department
at the School of Dentistry at Siena University, especially Cecilia Goracci,
Ornella Raffaelli, Alessandro Vichi and Simone Grandini, whom I worked
together with, forming a team spirit.
In this particular occasion I wish to mention the late Prof Riccardo
Garberoglio, who was the person that initially made me curious about dental
research, through his dedication and stimulation.

229
Finally, a big thank you to my wife, Roberta, who has encouraged and
supported me during this time, to my parents, who were always at my side
and to Tommaso…who is arriving!.

230
CURRICULUM VITAE Date of birth: July, 20th, 1962
Place of birth: Firenze, Italy
Civil status: Married to Roberta Plahuta
Citizenship: Italy
Research activity
2002: Master of Science in Dental Materials.
Professional positions: Institutional
1997-1999- Contract Professor of Dental Materials, School of Dental
Hygenist
1999-2000- Contract Professor of Dental Materials, School of Dentistry,
University of Siena, Italy
2000-2001- Contract Professor of Operative Dentistry, School of Dentistry,
University of Siena, Italy
2002-2003- Clinical Professor of Basic Principles of Dentistry, School of
Dentistry, University of Siena, Italy
Private Office: 42/b via Gramsci, Cortona (AR) 52042, Italy
Telephone and fax: +39(0575)630487
E-mail: [email protected]
Professional Organizations membership 1997 to 2004 International Association for Dental Research
2000 Academy of Operative Dentistry
1993- Academy of R.V. Tucker Gold Inlay Study Club.)

231
List of publications included in the thesis Fabianelli A, Kugel G, Ferrari M. Efficacy of self-etching primer on sealing
margins of Class II restorations. Am J Dent 2003; 16 (1): 37-41.
Fabianelli A, Goracci C, Ferrari M. Sealing ability of packable resin
composites in class II restorations. J Adhes Dent 2003; 5: 217-223.
Fabianelli A, Goracci C, Bertelli E, Monticelli F, Grandini S, Ferrari M. In vitro
evaluation of wall-to-wall adaptation of self-adhesive resin cement used for
luting gold and ceramic inlays. J Adhes Dent; Accepted for publication.
Fabianelli A, Goracci C, Thorbourn D, Davidson CL, Ferrari M. In vitro
microleakage and SEM observations of class V restorations. Submitted.
Fabianelli A, Goracci C, Bertelli E, Ferrari M. A clinical trial of Empress II
porcelain inlays luted to vital abutments with the self-light-curing adhesive
system Excite DSC and MultiLink. Int J Prosthodont; Submitted.
Ferrari M, Mason PN, Fabianelli A, Cagidiaco MC, Kugel G, Davidson CL.
Influence of tissue characteristics at margins on leakage of Class II indirect
porcelain restorations. Am J Dent 1999; 12(3): 134-142.
Ferrari M, Dagostin A, Fabianelli M, Marginal integrity of ceramic inlays luted
with a self-curing resin system. Dent Mat 2003; 19: 270-276.

232
Other publications Goracci C, Tavares AU, Fabianelli A, Monticelli F, Raffaelli O, Cardoso PEC,
Tay F, Ferrari M. The adhesion between fiber posts and root canal walls:
comparison between microtensile and push-out bond strength
measurements.European Journal of Oral Sciences 2004, in press.
Goracci C, Sadek FT, Fabianelli A, Tay FR, Ferrari M. Evaluation of the
adhesion of fiber posts to intraradicular dentin. Submitted for publication on
Operative Dentistry, 2004.
Abstracts Fabianelli A, Ferrari M, Grandini S, Vichi A. Clinical evaluation of Class II
restorations using two enamel-dentin adhesives: 12 months results. J Dent
Res, 1997; 76: Abstract 1375.
Fabianelli A, Mason PN, Kugel G, Ferrari M, Davidson CL. Influence of
different margin substrates on leakage of Class II indirect restorations. J
Dent Res, 1998; 77: Abstract 2248.
Fabianelli A, Grandini S, Vichi A, Ferrari M, Davidson CL. Influence of self-
etching-priming bonding systems on sealing ability of ClassII restorations:
leakage and SEM evaluation. J Dent Res, 2000; 79: Abstract 305.
Ferrari M, Grandini S, Fabianelli A ,Vichi A. Sem study on the efficacy of a
self-activating adhesive system used for bonding fiber posts in root canal. J
37th IADR/CED, Rome, 2001: Abstract 420.

233
Fabianelli A, , Ferrari M, Dagostin A, Grandini S. Operator variability
influence on marginal seal of Class II resin restorations. Dent Mat 2001; vol
15: Abstract P 57.
Borracchini A, Fabianelli A, Grandini S, Ferrari M. Clinical trial of Empress 2,
self curing Excite and Multilink luting materials. J Dent Res, 2002; 81:
Abstract 2634.
Fabianelli A, Grandini S, Bertelli E, Ferrari M. Clinical trial of Gradia in direct
restorations. J Dent Res, 2002; 81: Abstract 2654.
Fabianelli A, Grandini S, Goracci C, Ferrari M. One-year clinical trial of
Gradia Direct Class II restorations. J Dent Res, 2003; 82: Abstract 1472.