Embed Size (px)
Citation preview

Review
2002 © Ashley Publications Ltd ISSN 1465-6566 39
Ashley Publicationswww.ashley-pub.com
1. Introduction
2. Goal of therapy
3. Available compounds
4. Current best practice
5. Other factors influencing choice
of therapy
6. Conclusions
7. Expert opinion
Pharmacotherapy of primary CNS lymphomaDeric Minwoo Park & Lauren E. AbreyDepartment of Neurology, Memorial Sloan-Kettering Cancer Center New York, USA
Primary CNS lymphoma (PCNSL) is distinguished from other brain tumours byits striking response to chemotherapy. Surgery has little role (if any) in thetreatment of PCNSL. Radiation therapy has been proven to prolong survivalbut its use is complicated by delayed neurological toxicity, particularly amongthe elderly. Progress in understanding the physiology of the blood-brain bar-rier (BBB) and the pharmacology of chemotherapeutic agents has substan-tially improved the treatment and prognosis of this disease. The single mosteffective agent is methotrexate (MTX). The goal of delivering an adequatedose of MTX to the brain and the cerebrospinal fluid (CSF) has been achievedby a variety of strategies, including systemic high dose, intra-arterial injectionfollowing pharmacological disruption of the BBB and intrathecal (it.) admin-istration. MTX-based combination chemotherapy has yielded the best resultsto date but the prognosis of patients with PCNSL remains significantly worsethan comparable patients with systemic non-Hodgkin’s lymphoma (NHL).Ongoing trials continue to test novel combinations of agents, doses andimproved routes of delivery with the hope of improving disease control anddiminishing treatment-related neurotoxicity.
Keywords: brain lymphoma, chemotherapy, CNS, primary CNS lymphoma
Expert Opin. Pharmacother. (2001) 3(1):39-49
1. Introduction
PCNSL is a high- or intermediate-grade lymphoma arising in and usually confinedto the CNS. The first description of this entity is credited to Bailey’s report of a‘perivascular sarcomatous tumour’ in 1929 [1]. Difficulty in identifying the cell oforigin is illustrated by numerous subsequent designations, such as reticulum cell sar-coma, histiocytic sarcoma, adventitial sarcoma, reticulohistiocytic encephalitis,malignant reticulo-endotheliosis and microglioma [2]. The development of refinedimmunohistochemical methods definitively identified PCNSL as a NHL, usually ofthe B-cell type [3].
PCNSL has traditionally been considered rare, comprising ~ 1% of all primarybrain tumours and often seen in the context of immunosuppression. However,recent epidemiological analyses suggest an increased incidence of this disease withinthe immunocompetent population, the rising rate of which exceeds that of systemicNHL [4-6]. Some experts have suggested the ‘epidemic’ may eventually rival glialtumours, although the incidence of PCNSL remains much lower than gliomas [7].The pathogenesis of PCNSL remains a puzzle, since the CNS lacks lymph nodes orlymphatic vessels [8]. Proposed hypotheses are unproven, including neoplastic trans-formation of inflammatory lymphocytes that traffic in and out of the CNS, sincethese are primarily T-cells while the cell of origin in > 90% of PCNSLs is the B-lym-phocyte [7]. AIDS-related PCNSL is often associated with latent Epstein-Barr virus(EBV) infection of the malignant clone [9]. After primary infection with EBV, asmall population of B-cells develop a latent EBV infection which immortalises thecells; the growth of this population is controlled by suppressor T-cells. This popula-

Pharmacotherapy of primary CNS lymphoma
40 Expert Opin. Pharmacother. (2002) 3(1)
tion is permitted to proliferate when suppressor T-cell activityis impaired by immunosuppression.
The variable macroscopic appearance of PCNSL precludesuniform description. Tumours may range from well-demar-cated homogeneous lesions to diffuse infiltration of brainparenchyma [10]. Necrosis and haemorrhage may occasionallybe present, mimicking glioblastoma. Under the microscope,the borders of the tumour extend beyond gross appearance.Sheets of uniform lymphoid cells with perivascular orienta-tion are interrupted by the presence of reactive T-lymphocytesand astrocytes. Widespread availability of immunohistochem-ical staining has facilitated diagnosis. With few exceptions,most PCNSLs can be labelled with an antibody directedagainst the cluster differentiation antigen (CD) 45, alsoknown as leukocyte common antigen. Cytological subtypingmay be performed with antibodies specific for B-cells (CD20)and T-cells (CD3). Definitive proof of clonality can be dem-onstrated by T-cell receptor gene rearrangement analysis andmay be particularly useful in discriminating T-cell lymphomafrom an inflammatory response [11,12].
The majority of patients with PCNSL are aged 55 - 70,although patients with AIDS-related disease are younger byseveral decades. There is a slight male preponderance [13]. Spe-cific clinical manifestations of PCNSL follow location of dis-ease burden; however, headache and changes in cognition andpersonality are the most common symptoms. More than 40%demonstrate involvement of the leptomeninges and oculardissemination is seen in ~ 15% [14]. Symptoms progressquickly, reflecting the rapid growth of the neoplastic lym-phocytes, and seizures are less frequent compared to othertypes of brain tumours, perhaps due to the deep location ofmost PCNSL lesions. Staging evaluation should include gado-linium-enhanced cranial magnetic resonance imaging (MRI),cytological examination of the CSF, slit lamp ophthalmologicexamination, bone marrow biopsy, body imaging by compu-terised tomography (CT) and some suggest testicular ultra-sound in the elderly. HIV serology should also be obtained.Spinal MRI with gadolinium should be performed when spi-nal symptoms are present.
The management of PCNSL is distinct from that of otherprimary brain tumours, so accurate diagnosis is essential.Most are moderately hyperdense on non-enhanced CT scanswith homogeneous enhancement following infusion of a con-trast medium [15]. MRI images are iso-intense to hypointenseon T1-weighted studies and iso-intense to slightly hyperin-tense on T2-weighted studies; administration of gadoliniumtypically results in homogeneous enhancement, althoughexceptions exist [15,16]. The lack of distinctive clinical featuresand its relative rarity makes a high index of suspicion neces-sary to consider the diagnosis on the basis of these radio-graphic features. Suspicion of PCNSL should promptwithholding corticosteroids until histopathological diagnosishas been obtained, since their oncolytic effect may obscurethe diagnosis [17,18]. Histological diagnosis may be obtained
from examination of the CSF by lumbar puncture, brainbiopsy or vitrectomy.
The aggressive nature of PCNSL is illustrated by the shortmedian survival of 3.3 months in those receiving supportivecare only [13]. Surgery serves no therapeutic role in PCNSLexcept in the rare instance that urgent decompression is neces-sary to prevent herniation. Tumour resection may result inneurological deficits and does not improve survival whencompared to biopsy [19]. Corticosteroids are effective oncolyticagents and once the diagnosis has been confirmed, corticos-teroids may be administered to stabilise deteriorating neuro-logical symptoms. However, chronic use is limited by toxicity.
Observations of conspicuous radiosensitivity initially estab-lished whole brain radiotherapy (RT) as the standard treat-ment. Median survival improves dramatically to 10 -18 months upon irradiation of the brain [20,21]. The optimaldose is unknown but experience suggests a range of 40 -50 Gy. Those treated with a lower dose fared worse and deliv-ery of a higher dose or a boost failed to improve survival[5,19,22-24]. Higher RT dose may also result in greater incidenceof neurological toxicity [25]. From these observations, the cur-rent standard at our institution is 45 Gy whole brain RT.Craniospinal RT has been proposed to treat diffuse CSF dis-semination but its role remains dubious and is often pre-cluded by considerable associated morbidity [21,22,26,27].
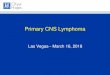
Patients treated with a combination of chemotherapy andRT have substantially better survival rates than those reportedpreviously for patients treated with RT alone, with medianreported survivals ranging between 30 - 60 months [28] (Table1). The chemosensitivity of PCNSL is clearly demonstratedby the dramatic radiographic response observed followingmultiple pre-RT chemotherapy regimens [29] (Figure 1). How-ever, durable responses are seen only in conjunction withagents able to cross an intact BBB, presumably because of theimportance of treating microscopic tumour deposits.
2. Goal of therapy
The primary goal of therapy is disease control, as measuredby patient survival and rate of relapse. While significantimprovements have been made in the past decade, at leasthalf of patients who achieve a complete remission willrelapse. In contrast, cure can be expected in most patientswith limited stage (stage I and non-bulky stage II) high gradesystemic NHL and in approximately one-third with dissemi-nated disease [30]. The major ongoing challenge in the treat-ment of PCNSL is to improve disease control whileminimising the attendant treatment-related neurotoxicity.While the combination of MTX-based chemotherapy andcranial RT is effective, it is clearly associated with significantneurological morbidity, particularly in patients > 60 years ofage. Therefore, the development of newer treatment strate-gies should include prospective neurocognitive assessment asan outcome measure [31-33].

Park & Abrey
Expert Opin. Pharmacother. (2002) 3(1) 41
3. Available compounds
3.1 MTX
MTX, a potent competitive antagonist of dihydrofolatereductase, is effective in a variety of rapidly growing tumours.Both normal and neoplastic cells require tetrahydrofolate(FH4) to serve as a single-carbon donor essential in the syn-thesis of purines and thymidylate. The enzyme dihydrofolatereductase (DHFR), which is required for the reduction ofdihydrofolate to FH4, is inhibited by MTX, resulting in criti-cal intracellular depletion of necessary substrates for the sur-vival and accumulation of toxic dihydrofolate polyglutamate[34]. Pharmacokinetic analysis after intravenous (iv.) deliveryrevealed a triphasic clearance with ~ 50% bound to plasmaproteins [35]. Immediate distribution is followed by renalclearance with a half-life of 2 - 3 h. Final phase has a half-lifeof 8 - 10 h and may be delayed in the setting of renal insuffi-ciency. Oncolytic effects exercised during the S-phase of thecell cycle also extend to rapidly-dividing normal cells. Within5 - 10 days the antimetabolic effect on the bone marrow andthe GI epithelium causes mucositis, thrombocytopenia andmyelosuppression. Caution should be observed when using
certain drugs, such as phenytoin, salicylates and sulfonamides,that are capable of displacing the protein-bound MTX. A bio-chemical basis for the clinical observation of drug resistancehas been investigated in mammalian cell cultures. The mutantcells demonstrate defective intracellular transport of the drug,decreased affinity for DHFR (induced by changes in theactive site of the enzyme) and amplification of the DHFRgene resulting in overproduction of the enzyme [36].
Experience with high-dose iv. administration of MTX fol-lowed by leucovorin (folinic acid) rescue therapy stems fromtreatment of systemic high-grade NHL, leukaemia and osteo-genic sarcoma [37]. A dose > 1 g/m2 is capable of producing acytotoxic concentration in the brain parenchyma but demandsleucovorin rescue and close observation. Vigorous hydrationand alkalisation of the urine is necessary to prevent precipita-tion of the drug in the renal tubules. Although side effects,including behavioural abnormalities, seizures and alternatingfocal findings are rarely seen with high-dose iv. MTX, theseusually occur within 6 days of treatment and are transient [38].Leucovorin is available in oral and parenteral formulations. Itbypasses the inhibition of DHFR by MTX and permits use ofhigh-dose MTX. We use an iv. dose of 25 mg every 6 h untilthe concentration of MTX is < 100 nM.
Table 1. Chemotherapy regimens for PCNSL§.
Type N Regimen RT Result Other Ref.
Series 10 DHAP ± 70% response40% prolonged remission
4 newly diagnosed6 recurrentseveral did not receive RT
[53]
Series 10 PCV + 100% response30-month median survival
PCV given post-RT1 patient received carmustine
[104]
Series 13 MTX 3.5 g/m2 + 92% response9-month median survival
Survival up to 54 months [28]
Series 25 MTX 3.5 g/m2 + 88% response33-month median survival
59% relapse rate [29]
Series 74 MTX BBBD - 65% complete response40.7-month median survival
[47]
Series 31 MTX 1 g/m2 + 64% response41-month survival
[105]
Phase II 14 MTX it. Ara-C - 100% response16.5-month median PFS
68.8% alive at 54 months [95]
Prospective 19 BOMES + 84% response rate6-month median PFS
5 patients with concurrent systemic lymphoma
[103]
Series 19 MTX-based3.5 - 8 g/m2
- 94% response rate [109]
Phase II 102 MPV Ara-C + 94% response rate30-month median survival
[29]
Prospective 52 MPV Ara-C ± 60-month median survival 22 older patients did not receive RT
[14]
Ara-C: Cytarabine; BBBD: Blood brain barrier disruption; BOMES: Carmustine, vincristine, methotrexate, etoposide and methylprednisolone; DHAP: Dexamethasone, high-dose cytarabine and cisplatin; it.: Intrathecal; MPV: Methotrexate, procarbazine and vincristine; MTV: Methotrexate, thiotepa and vincristine; PCV: Procarbazine, chloroethylcyclo-hexylnitrosourea and vincristine; PFS: Progression-free survival; RT: Radiotherapy.§Reproduced with permission from ABREY LE: Primary Central Nervous System Lymphoma. Neurologist (2000) 6:245-254. © Lippincott, Williams & Wilkins (2000).

Pharmacotherapy of primary CNS lymphoma
42 Expert Opin. Pharmacother. (2002) 3(1)
3.1.1 Current standard high-dose MTXAt standard dose the polar structure of MTX prevents pene-tration of the BBB but iv. delivery of a high-dose (≥ 1 g/m2)permits entry into the CNS compartment. The optimal doseis not defined but prior experiences provide guidance. Deliv-ery of 3 g/m2 over a 3-hour period given as nervous systemprophylaxis in patients with systemic NHL without CNSdisease achieves cytotoxic CSF concentration (10-6 M) lastingup to 8 h [39]. The rate of infusion is also critical since the
non-protein-bound serum MTX directly correlates with theCSF concentration [40]. Hiraga et al. compared tumour vol-ume reduction in patients with PCNSL receiving high doseMTX (~ 3.8 g/m2) with different rates of infusion. Thegroup receiving rapid (3 h) infusion had higher CSF concen-tration and improved radiographic response [41]. Pharmaco-logical data suggesting increased CSF concentration of MTXwith very high systemic dose have prompted trials exploring8 g/m2 in PCNSL [42,43]. Direct intravitreal administration of
A
B
C
D
Figure 1. T-1 weighted post-gadolinium and FLAIR sequences, before and after administration of high-dose MTX. A and B arepre-treatment images (FLAIR and contrast-enhanced, respectively), while C and D are post-treatment images (FLAIR and contrast-enhanced, respectively).

Park & Abrey
Expert Opin. Pharmacother. (2002) 3(1) 43
MTX has been reported to successfully treat intra-ocularlymphoma [44,45].
3.1.2 Intra-arterial MTX with BBB disruptionStrategies allowing for pharmacological breakdown of theBBB permit the use of a variety of hydrophilic compoundsincapable of penetrating the endothelial tight junctions inordinary circumstances. Hyperosmolar disruption mediatedby intra-arterial mannitol, the technique preferred by mostinvestigators, produces a temporary period of barrier disrup-tion; the transient nature of the barrier disruption allows thedelivery of increased concentrations of water-soluble agentsinto the interstitial space of the CNS by creating a ‘trap’ [46].The application of this approach to PCNSL has successfullyextended survival without RT [31,32,47]. Dahlborg et al. treated39 patients with non-AIDS-related PCNSL with intra-arterialmannitol followed by MTX in conjunction with systemiccyclophosphamide, procarbazine and corticosteroids. Theyobserved a complete response in 29 patients, with overallmedian survival of 40 months [32]. This method of therapyavoided delayed neurological toxicity but 31% required RTfor relapse. Furthermore, intra-arterial infusion resulted inacute toxicities such as focal seizures, cerebral oedema andlocal arterial trauma not seen with conventional methods.
3.1.3 Intrathecal MTXDirect administration of MTX into the subarachnoid space,ensures tumouricidal concentrations in the CSF but does nottreat parenchymal tumours. The drug may be given via lum-bar puncture or by the use of an intraventricular Ommaya res-ervoir. The latter approach is preferred since injection into thelumbar cistern may distribute poorly over the cerebral convex-ities. Age-dependent pharmacokinetic studies suggest a doseof 12 mg for those > 3 years old. [48]. Toxicity associated withit. MTX includes acute aseptic meningitis, paraplegia and sei-zures [49-51]. Leucovorin does not cross the BBB and thereforeis not useful in the treatment of neurotoxicity; however, itmay be helpful in preventing systemic side effects during it.MTX therapy [52].
3.2 CytarabineHigh-dose cytarabine (> 2 g/m2) is often used in concert withother agents in the treatment of PCNSL [23,53]. The arabinosenucleoside, which derives from the sponge Cryptothethyacrypta, is crucial in the therapy of acute myelogenous leukae-mia [34]. Similar to MTX, cytarabine is an antimetaboliteactive during the S-phase of the cell cycle. Upon entry into thecell the drug is converted into the active form, ara-cytidinemonophosphate by deoxycytidine kinase [37]. Diphosphateand triphosphate forms of the ara-cytidine interrupt DNAsynthesis by inhibiting DNA elongation [54]. Intravenousadministration of high-dose cytarabine achieves cytotoxic con-centrations of the drug in the CSF. Absence of cytidine deam-inase in the CSF prolongs time of activity in the subarachnoidspace [55]. Concurrent administration of cytarabine with MTX
results in suboptimal levels of the MTX [56]. Systemic toxicityof high-dose cytarabine consists of myelosuppression with anadir at 7 - 14 days and GI symptoms [57]. Well-characterisedneurological side effects, including seizures, peripheral neu-ropathy, cognitive abnormalities and cerebellar dysfunction,are uncommon [57]. In addition to its role in treatment ofbrain lesions, high-dose cytarabine can be effective in ocularlymphoma by penetrating the vitreous [58,59].
3.3 ProcarbazineProcarbazine is a methylhydrazine derivative initially synthe-sised in search of monoamine oxidase inhibition [60,61]. Thisdrug is metabolised to a DNA-methylating agent by anincompletely understood mechanism, which causes an antitu-mour effect [62]. In PCNSL, procarbazine is generally given inconjunction with high-dose MTX or in combination withlomustine and vincristine [33]. The use of procarbazine asmonotherapy has not been tested by prospective trials. GIabsorption is efficient and the lipophilic nature of the drugpromotes entry into the CNS compartments [63,64]. Moderatemyelosuppression is common and occasional patients developrash, encephalopathy and/or reversible peripheral neuropathy[63,65]. Similar to other alkylating agents, procarbazine is a car-cinogen, teratogen and mutagen [66]. All patients should betreated with prophylactic anti-emetics.
3.4 VincristineVincristine is a member of the vinca alkaloid family of antine-oplastic agents and acts by disrupting the polymerisation oftubulin into microtubules [67]. Affected cells are arrested inmetaphase, leading to apoptosis. In addition to its role in sys-temic haematopoietic malignancies, vincristine has beenincorporated into treatment of PCNSL although no formalprospective monotherapy studies exist. Intravenous adminis-tration follows a complex triphasic clearance with a final half-life of 23 - 85 h [68]. Toxicity includes paralytic ileus andperipheral neuropathy. The peripheral neuropathy is cumula-tive and warrants discontinuation upon development of sig-nificant motor deficit [69]. Poor entry into the CNS accountsfor the paucity of reports relating to vincristine-induced cen-tral neurotoxicity but the syndrome of inappropriate secretionof antidiuretic hormone, confusion, hallucinations, seizuresand coma have been described [60,65,70,71]. Intrathecal admin-istration of vincristine results in devastating neurological tox-icity and death [72-74].
3.5 CorticosteroidsSimilar to systemic lymphoma, PCNSL responds dramaticallyto the administration of corticosteroids with regression oflesions in up to 50% of patients [7,75]. The oncolytic responseis mediated by activation of the endogenous steroid receptor,which triggers the apoptosis cascade. O’Neill et al. reportedlong-term survival in a few patients treated with high-dosemethylprednisolone alone [76]; however, the therapeutic effectis short-lived in most cases and chronic use is associated with

Pharmacotherapy of primary CNS lymphoma
44 Expert Opin. Pharmacother. (2002) 3(1)
significant complications, including GI bleeding and perfora-tion, avascular osteonecrosis, opportunistic infections, myop-athy and psychosis. In spite of these potential side effects,short-term administration of corticosteroids can result in dra-matic resolution of neurological symptoms. Corticosteroidsshould be avoided prior to biopsy of a suspected PCNSL sincethe lympholytic effect may result in non-diagnostic histology.
3.6 RituximabRituximab is a chimeric anti-CD20 monoclonal antibodyeffective in the treatment of low-grade systemic NHL and wasthe first antibody-based therapy to receive FDA approval fortreatment of neoplasm [77,78]. Although effective alone, addi-tion of conventional chemotherapeutic agents to Rituximabproduces a synergistic antitumour effect without added toxic-ity [79,80]. The role of Rituximab in the treatment of PCNSLis unknown but preliminary reports indicate that furtherstudy is warranted [81-83]. Some patients treated with Rituxi-mab have had demonstrable clinical or radiographic improve-ment [82]. Direct it. administration or combination withsystemic chemotherapy may further improve efficacy [84,85].
3.7 TopotecanTopotecan, a semi-synthetic derivative of camptothecin, is atopoisomerase I inhibitor [86]. The agent can be administerediv. or orally and effectively enters the CSF [87]. Apart fromdose-limiting myelosuppression, topotecan is generally well-tolerated. Activity against systemic haematological malignan-cies prompted a small trial for PCNSL. Patients (n = 7) whowere failing MTX were treated with an iv. dose of 1.5 mg/m2/day for 5 days; complete response was seen in three, partialresponse in one and one patient progressed [88]. Etoposide, atopoisomerase II inhibitor, has also been used in combinationwith other agents [89,90]. Due to limited experience, its role inthe treatment of PCNSL is unclear.
3.8 TemozolomideTemozolomide is a second-generation imidazotetrazine deriva-tive recently approved for use in malignant gliomas [91]. Thedose of this oral methylating agent is limited by non-cumula-tive myelosuppression. Formal studies are lacking but anecdotalexperience suggests activity against PCNSL. Reni et al. treateda 65 year-old man with recurrent PCNSL using temozolomideand observed a complete response after two cycles [92].
3.9 ThiotepaThiotepa is an aziridine analogue of nitrogen mustard and isused in conjunction with other alkylating agents to treat avariety of systemic solid and haematopoietic tumours [66,93,94].Myelosuppression is the major toxic effect, although somepatients experience mucositis. The role of thiotepa in PCNSLis unclear but it has been used in combination with otheragents and as monotherapy to treat recurrent PCNSL. It hasbeen used with MTX, cytarabine, vincristine, procarbazine,bulsulfan and stem cell rescue in both immunocompetent and
AIDS-related PCNSL [95-98,89]. Intravitreal injection of thi-otepa in combination with MTX has been reported for thecontrol of ocular disease [99].
3.10 CyclophosphamideCyclophosphamide is a nitrogen mustard important in thetreatment of systemic NHL as part of the cyclophosphamide,adriamycin, vincristine, prednisone (CHOP) regimen [100]. Aswith other alkylating agents, myelosuppression is common.Other potential toxicities include nausea, vomiting, alopeciaand haemorrhagic cystitis. The use of a cyclophosphamide-based regimen, such as CHOP, in PCNSL is marked by atransient initial response followed by tumour recurrence,reflecting the inability of the drug to reach tumours residingbehind an intact BBB [101]. Based on three clinical trials ofPCNSL patients, CHOP does not improve survival ofpatients with PCNSL and should be avoided in the treatmentof this disease [101-103].
3.11 LomustineLomustine is a member of the nitrosourea family of alkylatingagents used in malignant gliomas. Oral administration resultsin reliable bioavailability and rapid penetration into the CNS.Commonly encountered side effects are myelosuppression,nausea and vomiting; pulmonary fibrosis and renal failureassociated with high cumulative doses are uncommon but seri-ous. Lomustine has been used in combination with procar-bazine and vincristine (PCV regimen) and with other drugs ina limited number of patients with PCNSL [104]. Chamberlainand Levin reported a tolerable side effect profile with a mediansurvival of 41 months when combined with RT [33,105].
4. Current best practice
The current standard of care for PCNSL was established bythe completion of a Radiation Therapy Oncology Group(RTOG) study 93-10 in conjunction with a number of othersingle-institution studies [106]. Based on these results patientsshould be treated with pre-RT MTX-based chemotherapy.We use a combination of MTX plus procarbazine and vincris-tine. Standard whole-brain RT, including the upper cervicalspinal cord, should be dosed at 45 Gy [19,22,107]. The use of aboost is not warranted [19,23]. Our experience suggests thatsurvival is not compromised in older patients by eliminatingRT in those who achieve a complete response with initialchemotherapy; however, neurotoxicity is eliminated whenchemotherapy is used alone, thus patients have a higher qual-ity of function. Adjuvant high-dose cytarabine should begiven following RT or the MTX-based regimen.
5. Other factors influencing choice of therapy
The age of the patient is an important consideration in plan-ning treatment. It seems clear that the combination of MTXand whole-brain RT results in an unacceptably high risk of

Park & Abrey
Expert Opin. Pharmacother. (2002) 3(1) 45
neurotoxicity for long-term survivors aged > 60. Therefore, thebest recommendation is to use chemotherapy alone for thetreatment of older patients [98,108]. The more difficult decisionarises when treating younger patients aged 50 - 60, where therisk of treatment-related neurotoxicity is less well defined.
Advanced age or poor performance status are often cited asreasons to avoid the use of chemotherapy; however, manyelderly patients can be safely treated with high-dose systemicMTX provided that adequate attention is paid to renal func-tion, hydration and other metabolic parameters. The same istrue for patients with poor performance status on the basis ofneurological disability, many of whom will have dramaticimprovement in their cognitive status and focal neurologicaldeficits following the first treatments with MTX-basedchemotherapy.
The incidence of HIV-related PCNSL is declining follow-ing the advent and widespread use of highly active antiretrovi-ral therapy. Furthermore, those HIV patients who developPCNSL despite treatment with HAART are often in betterclinical condition and able to tolerate more aggressive inter-ventions with chemotherapy. The greatest challenge in treat-ing HIV-related PCNSL is obtaining an accurate diagnosis ina prompt enough fashion to allow aggressive treatment. Non-invasive techniques such as single photon emission CT scan-ning and polymerase chain reaction analysis of the CSF forEBV may be definitive, eliminating the need for brain biopsyin many patients.
Impaired renal function is an important factor to considerbefore treating any patient with high-dose systemic MTX. Allpatients should have a 24 h urine collection for creatinineclearance with a target value of 50 cc/h in order to treat themsafely. Patients with a value < 50 cc/h may require a differentchoice of drug since the adjusted lower dose of the MTX isunlikely to effectively penetrate the CNS. It is equally impor-tant to maintain adequate renal function in those patientsbeing treated; all patients should receive systemic leucovorinand appropriate hydration. Urine should be alkalinised andserum MTX levels, blood urea nitrogen and creatinine shouldbe followed closely.
6. Conclusions
PCNSL, an aggressive NHL arising within the CNS, isobserved with increasing incidence. Particular clinical symp-tomatology is dependent on tumour location but cognitivedysfunction is common. Unlike other brain tumours, surgeryfunctions only to establish the diagnosis and corticosteroidsshould be withheld until a histological diagnosis has beenobtained. The best outcome to date has been seen in patientstreated with a combination of MTX-based chemotherapy andwhole-brain RT. Concerns about treatment-related neurotox-icity have prompted the development of alternative strategiesto improve disease control while minimising treatment relatedtoxicity. Additional studies, particularly Phase II investigations,will be necessary to define the role of other agents alone or incombination with MTX in treating this aggressive disease.
7. Expert opinion
The treatment of PCNSL is both rewarding and challenging.The dramatic improvement in prognosis that has accompa-nied new treatment strategies over the past decade and theresponse of individual patients to treatment is gratifying. Atthe same time, concerns about treatment-related neurotoxic-ity and numerous unanswered questions present an ongoingdilemma. Can RT be deferred or delayed without sacrificingdisease control? What is the best dose or route of administra-tion for MTX? Does it. MTX significantly improve diseasecontrol or contribute to treatment-related neurotoxicity? Canwe better characterise the molecular characteristics of PCNSLin a way that will improve treatment strategies? Is there a rolefor newer immunotherapies or biological therapies in thetreatment of PCNSL?
In order to further improve on the studies made in thetreatment of PCNSL, it is imperative that newly diagnosedpatients be enrolled in carefully designed clinical trials if at allpossible. Ideally, all trials should assess standard measures,including radiographic response, disease control, survival,prospective neurocognitive testing and molecular and radio-graphic markers of biological activity.
Bibliography
1. BAILEY P: Intracranial sarcomatous tumors of leptomeningeal origin. Arch. Surg. (1929) 18:1359-1402.
2. RUBINSTEIN LJ: Tumors of the central nervous system. In: Atlas of Tumor Pathology. Fascicle 6. Armed Forces Institute of Pathology Washington DC, USA (1972) 215-234.
3. LENNERT K: Morphology and classification of malignant lymphomas and
so-called reticulosis. Acta Neuropathologica (1975) (Suppl. 6):1-16.
4. EBY NL, GRUFFERMAN S, FLANNELLY CM, SCHOLD SC JR, VOGEL FS, BURGER PC: Increasing incidence of primary brain lymphoma in the US. Cancer (1988) 62:2461-2465.
5. LUTZ JM, COLEMAN MP: Trends in primary cerebral lymphoma. Br. J. Cancer (1994) 70:716-718.
6. O’NEILL BP, JANNEY CA, OLSON JE et
al.: The continuing increase in primary central nervous system non-Hodgkin’s lymphoma (PCNSL): a surveillance, epidemiology, and end results (SEER) analysis. Proc. Am. Soc. Clin. Oncol. (2001) 20:53a. Abstract.
7. HOCHBERG FH, MILLER DC: Primary central nervous system lymphoma. J. Neurosurg. (1988) 68:835-853.
8. VELASQUEZ WS: Primary central nervous system lymphoma. J. Neurooncol. (1994) 20:177-185.

Pharmacotherapy of primary CNS lymphoma
46 Expert Opin. Pharmacother. (2002) 3(1)
9. MACMAHON EM, GLASS JD, HAYWARD SD et al.: Epstein-Barr virus in AIDS-related primary central nervous system lymphoma. Lancet (1991) 338:969-973.
10. TRAWEEK ST: Nervous system involvement by lymphoma, leukemia and other hematopoietic cell proliferations. In: Russell and Rubinstein’s Pathology of Tumors of the Nervous System. Bigner D, McLendon R, Bruner J (Eds.), Oxford University Press (1998).
11. KUMANISHI T, WASHIYAMA K, NISHIYAMA A, ABE S, SAITO T, ICHIKAWA T: Primary malignant lymphoma of the brain: demonstration of immunoglobulin gene rearrangements in four cases by the Southern blot hybridization technique. Acta Neuropathol (Berl.) (1989) 79:23-26.
12. TSUJINO S: [Immunoglobulin and T-cell receptor gene rearrangements as markers of lineage and clonality in malignant lymphoma]. Nippon Rinsho (2000) 58:612-617.
13. HENRY JM, HEFFNER RR, JR, DILLARD SH, EARLE KM, DAVIS RL: Primary malignant lymphomas of the central nervous system. Cancer (1974) 34: 1293-1302.
14. ABREY LE: Primary central nervous system lymphoma. Neurologist (2000) 6:245-254.
15. OSBORN A: Meningiomas and other nonglial neoplasms. In: Diagnostic Neuroradiology. Mosby (1994).
16. DEANGELIS LM: Cerebral lymphoma presenting as a nonenhancing lesion on computed tomographic/magnetic resonance scan. Ann Neurol (1993) 33:308-311.
17. SINGH A, STROBOS RJ, SINGH BM et al.: Steroid-induced remissions in CNS lymphoma. Neurology (1982) 32:1267-1271.
18. PIROTTE B, LEVIVIER M, GOLDMAN S, BRUCHER JM, BROTCHI J, HILDEBRAND J: Glucocorticoid-induced long-term remission in primary cerebral lymphoma: case report and review of the literature. J. Neurooncol. (1997) 32:63-69.
19. NELSON DF, MARTZ KL, BONNER H et al.: Non-Hodgkin’s lymphoma of the brain: can high dose, large volume radiation therapy improve survival? Report on a prospective trial by the Radiation Therapy Oncology Group (RTOG): RTOG 8315. Int. J. Radiat. Oncol. Biol. Phys. (1992) 23:9-17.
20. DEANGELIS LM: Current management of primary central nervous system lymphoma. Oncology (Huntingt.) (1995) 9:63-71.
21. RAMPEN FH, VAN ANDEL JG, SIZOO W, VAN UNNIK JA: Radiation therapy in primary non-Hodgkin’s lymphomas of the CNS. Eur. J. Cancer (1980) 16:177-184.
22. POLLACK IF, LUNSFORD LD, FLICKINGER JC, DAMESHEK HL: Prognostic factors in the diagnosis and treatment of primary central nervous system lymphoma. Cancer (1989) 63:939-947.
23. ABREY LE, YAHALOM J, DEANGELIS LM: Treatment for primary CNS lymphoma: the next step. J. Clin. Oncol. (2000) 18:3144-3150.
•• Older patients may be treated successfully with RT.
24. DEANGELIS LM, YAHALOM J, THALER HT, KHER U: Combined modality therapy for primary CNS lymphoma. J. Clin. Oncol. (1992) 10:635-643.
25. BLAY JY, CONROY T, CHEVREAU C et al.: High-dose methotrexate for the treatment of primary cerebral lymphomas: analysis of survival and late neurologic toxicity in a retrospective series. J. Clin. Oncol. (1998) 16:864-871.
• HD-MTX is the single most important chemotherapeutic agent in the treatment of PCNSL.
26. RENI M, FERRERI AJ, GARANCINI MP, VILLA E: Therapeutic management of primary central nervous system lymphoma in immunocompetent patients: results of a critical review of the literature. Ann. Oncol. (1997) 8:227-234.
27. BRADA M, DEARNALEY D, HORWICH A, BLOOM HJ: Management of primary cerebral lymphoma with initial chemotherapy: preliminary results and comparison with patients treated with radiotherapy alone. Int. J. Radiat. Oncol. Biol. Phys. (1990) 18:787-792.
28. GABBAI AA, HOCHBERG FH, LINGGOOD RM, BASHIR R, HOTLEMAN K: High-dose methotrexate for non-AIDS primary central nervous system lymphoma. Report of 13 cases. J. Neurosurg. (1989) 70:190-194.
29. GLASS J, GRUBER ML, CHER L, HOCHBERG FH: Pre-irradiation methotrexate chemotherapy of primary central nervous system lymphoma: long-term outcome. J. Neurosurg. (1994) 81:188-195.
30. KIMBY E, BRANDT L, NYGREN P, GLIMELIUS BL: A systematic overview of chemotherapy effects in aggressive non- Hodgkin’s lymphoma. Acta Oncol. (2001) 40: 198-212.
31. NEUWELT EA, GOLDMAN DL, DAHLBORG SA et al.: Primary CNS lymphoma treated with osmotic blood-brain barrier disruption: prolonged survival and preservation of cognitive function. J. Clin. Oncol. (1991) 9:1580-1590.
32. DAHLBORG SA, HENNER WD, CROSSEN JR et al.: Non-AIDS primary CNS lymphoma: first example of a durable response in a primary brain tumor using enhanced chemotherapy delivery without cognitive loss and without radiotherapy. Cancer J. Sci. Am. (1996) 2:166.
• Chemotherapy after BBB disruption is effective without RT.
33. CHAMBERLAIN MC, LEVIN VA: Primary central nervous system lymphoma: a role for adjuvant chemotherapy. J. Neurooncol. (1992) 14:271-275.
34. CHABNER BA: Cytidine analogues. In: Cancer Chemotherapy and Biotherapy: Principles and Practice. Chabner B, Longo De (Eds.), Lippincott-Raven (1996).
35. SONNEVELD P, SCHULTZ FW, NOOTER K, HAHLEN K: Pharmacokinetics of methotrexate and 7-hydroxy-methotrexate in plasma and bone marrow of children receiving low-dose oral methotrexate. Cancer Chemother. Pharmacol. (1986) 18:111-116.
36. SCHIMKE RT: Methotrexate resistance and gene amplification. Mechanisms and implications. Cancer (1986) 57:1912-1917.
37. CHU E, MOTA A, FOGARASI M: Pharmacology of cancer chemotherapy: antimetabolites. In: Cancer: Principles and Practice of Oncology. DeVita VT, Hellman S, Rosenberg SA (Eds.), Philadelphia: Lippincott Williams and Wilkins (2001).
38. WALKER RW, ALLEN JC, ROSEN G, CAPARROS B: Transient cerebral dysfunction secondary to high-dose methotrexate. J. Clin. Oncol. (1986) 4:1845-1850.
39. VASSAL G, VALTEAU D, BONNAY M, PATTE C, AUBIER F, LEMERLE J: Cerebrospinal fluid and plasma methotrexate levels following high-dose regimen given as a 3-hour intravenous infusion in children with non-Hodgkin’s lymphoma. Pediatr. Hematol. Oncol. (1990) 7:71-77.

Park & Abrey
Expert Opin. Pharmacother. (2002) 3(1) 47
40. EVANS WE, HUTSON PR, STEWART CF et al.: Methotrexate cerebrospinal fluid and serum concentrations after intermediate-dose methotrexate infusion. Clin. Pharmacol. Ther. (1983) 33:301-307.
41. HIRAGA S, ARITA N, OHNISHI T et al.: Rapid infusion of high-dose methotrexate resulting in enhanced penetration into cerebrospinal fluid and intensified tumor response in primary central nervous system lymphomas. J. Neurosurg. (1999) 91:221-230.
42. BORSI JD, MOE PJ: A comparative study on the pharmacokinetics of methotrexate in a dose range of 0.5 g to 33.6 g/m2 in children with acute lymphoblastic leukemia. Cancer (1987) 60:5-13.
43. BORSI JD, SAGEN E, ROMSLO I, SLORDAL L, MOE PJ: 7-Hydroxy-methotrexate concentrations in serum and cerebrospinal fluid of children with acute lymphoblastic leukemia. Cancer Chemother. Pharmacol. (1990) 27:164-167.
44. DE SMET MD: Management of non Hodgkin’s intraocular lymphoma with intravitreal methotrexate. Bull. Soc. Belge. Ophtalmol. (2001):91-95.
45. FISHBURNE BC, WILSON DJ, ROSENBAUM JT, NEUWELT EA: Intravitreal methotrexate as an adjunctive treatment of intraocular lymphoma. Arch. Ophthalmol. (1997) 115:1152-1156.
46. ZUNKELER B, CARSON RE, OLSON J et al.: Quantification and pharmacokinetics of blood-brain barrier disruption in humans. J. Neurosurg. (1996) 85:1056-1065.
47. MCALLISTER LD, DOOLITTLE ND, GUASTADISEGNI PE et al.: Cognitive outcomes and long-term follow-up results after enhanced chemotherapy delivery for primary central nervous system lymphoma. Neurosurgery (2000) 46:51-60.
48. BLEYER AW: Clinical pharmacology of intrathecal methotrexate. II. An improved dosage regimen derived from age-related pharmacokinetics. Cancer Treat. Rep. (1977) 61:1419-1425.
49. SHORE T, BARNETT MJ, PHILLIPS GL: Sudden neurologic death after intrathecal methotrexate. Med. Pediatr. Oncol. (1990) 18:159-161.
50. GEISER CF, BISHOP Y, JAFFE N, FURMAN L, TRAGGIS D, FREI E 3RD: Adverse effects of intrathecal methotrexate in children with acute leukemia in remission. Blood (1975) 45:189-195.
51. POSNER J: Neurologic complications of cancer. FA Davis, Philadelphia, USA (1995a).
52. RAMU A, FUSNER JE: A pharmacokinetic model for predicting the concentration of methotrexate in plasma subsequent to intrathecal injection. Isr. J. Med. Sci. (1979) 15:494-499.
53. MCLAUGHLIN P, VELASQUEZ WS, REDMAN JR et al.: Chemotherapy with dexamethasone, high-dose cytarabine, and cisplatin for parenchymal brain lymphoma. J. Natl. Cancer Inst. (1988) 80:1408-1412.
54. MIKITA T, BEARDSLEY GP: Functional consequences of the arabinosylcytosine structural lesion in DNA. Biochemistry (1988) 27:4698-4705.
55. DAMON LE, PLUNKETT W, LINKER CA: Plasma and cerebrospinal fluid pharmacokinetics of 1-beta-D- arabinofuranosylcytosine and 1-beta-D-arabinofuranosyluracil following the repeated intravenous administration of high- and intermediate-dose 1-beta-D-arabinofuranosylcytosine. Cancer Res. (1991) 51:4141-4145.
56. GRAHAM ML, SHUSTER JJ, KAMEN BA et al.: Changes in red blood cell methotrexate pharmacology and their impact on outcome when cytarabine is infused with methotrexate in the treatment of acute lymphocytic leukemia in children: a pediatric Oncology group study. Clin. Cancer Res. (1996) 2:331-337.
57. BAKER WJ, ROYER GL JR, WEISS RB: Cytarabine and neurologic toxicity. J. Clin. Oncol. (1991) 9:679-693.
58. DIETS-OUWEHAND JJ, DE KEIZER RJ, VRENSEN GF, GROEN-JANSEN S, VAN BEST JA: Toxicity of 1-(beta-D-arabinofuranosyl)cytosine after intravitreal injection in the rabbit eye. Graefes Arch. Clin. Exp. Ophthalmol. (1992) 230:488-495.
59. STRAUCHEN JA, DALTON J, FRIEDMAN AH: Chemotherapy in the management of intraocular lymphoma. Cancer (1989) 63:1918-1921.
60. ZELLER P, GUTMANN H, HEGEDUS B et al.: Methylhydrazine derivatives: a new class of cytotoxic agents. Experientia (1963) 19:129.
61. COLVIN O: Pharmacology of cancer chemotherapy: classes of alkylating agents and their properties. In: Cancer: Principles and Practice of Oncology. DeVita VT, Hellman S, Rosenberg SA (Eds.),
Lippincott Williams & Wilkins, Philadelphia, USA (2001).
62. FINK D, AEBI S, HOWELL SB: The role of DNA mismatch repair in drug resistance. Clin. Cancer Res. (1998) 4:1-6.
63. SPIVACK SD: Drugs 5 years later: procarbazine. Ann. Intern. Med. (1974) 81:795-800.
64. OLIVERIO VT, DENHAM C, DEVITA VT et al.: Some pharmacologic properties of a new antitumor agent N-isopropyl-alpha-(2-methyl-hydrazino)-p-toluamide hydrochloride NSC-77213. Cancer Chemother. Rep. (1964) 42:1.
65. POSNER J: Neurologic complications of cancer. FA Davis, Philadelphia (1995b).
66. TEW K, COLVIN M, CHABNER B: Alkylating Agents. In: Cancer Chemotherapy and Biotherapy. Chabner BA, Longo DL (Eds.), Lippincott-Raven, Philadelphia, USA (1996):297-332.
67. GIDDING CE, KELLIE SJ, KAMPS WA, DE GRAAF SS: Vincristine revisited. Crit. Rev. Oncol. Hematol. (1999) 29:267-287.
68. JOEL S: The comparative clinical pharmacology of vincristine and vindesine: does vindesine offer any advantage in clinical use? Cancer Treat. Rev. (1996) 21:513-525.
69. ROSENTHAL S, KAUFMAN S: Vincristine neurotoxicity. Ann. Intern. Med.. (1974) 80:733-737.
70. JACKSON DV JR, SETHI VS, SPURR CL, MCWHORTER JM: Pharmacokinetics of vincristine in the cerebrospinal fluid of humans. Cancer Res. (1981) 41:1466-1468.
71. WHITTAKER JA, PARRY DH, BUNCH C, WEATHERALL DJ: Coma associated with vincristine therapy. Br. Med. J. (1973) 4:335-337.
72. WILLIAMS ME, WALKER AN, BRACIKOWSKI JP, GARNER L, WILSON KD, CARPENTER JT: Ascending myeloencephalopathy due to intrathecal vincristine sulfate. A fatal chemotherapeutic error. Cancer (1983) 51:2041-2047.
73. KWACK EK, KIM DJ, PARK TI, CHO KR, KWON IH, SOHN YK: Neural toxicity induced by accidental intrathecal vincristine administration. J. Korean Med. Sci. (1999) 14:688-692.
74. BERWICK DM: Not again! Br. Med. J. (2001) 322:247-248.
75. WELLER M: Glucocorticoid treatment of

Pharmacotherapy of primary CNS lymphoma
48 Expert Opin. Pharmacother. (2002) 3(1)
primary CNS lymphoma. J. Neurooncol. (1999) 43:237-239.
76. O’NEILL BP, HABERMANN TM, WITZIG TE, RODRIGUEZ M: Prevention of recurrence and prolonged survival in primary central nervous system lymphoma (PCNSL) patients treated with adjuvant high-dose methylprednisolone. Med. Oncol. (1999) 16:211-215.
77. MALONEY DG, GRILLO-LOPEZ AJ, WHITE et al.: IDEC-C2B8 (Rituximab) anti-CD20 monoclonal antibody therapy in patients with relapsed low-grade non-Hodgkin’s lymphoma. Blood (1997) 90:2188-2195.
78. GRILLO-LOPEZ AJ, WHITE CA, DALLAIRE BK et al.: Rituximab: the first monoclonal antibody approved for the treatment of lymphoma. Curr. Pharm. Biotechnol. (2000) 1:1-9.
79. CZUCZMAN MS, GRILLO-LOPEZ AJ, WHITE CA et al.: Treatment of patients with low-grade B-cell lymphoma with the combination of chimeric anti-CD20 monoclonal antibody and CHOP chemotherapy. J. Clin. Oncol. (1999) 17:268-276.
80. DEMIDEM A, LAM T, ALAS S, HARIHARAN K, HANNA N, BONAVIDA B: Chimeric anti-CD20 (IDEC-C2B8) monoclonal antibody sensitizes a B cell lymphoma cell line to cell killing by cytotoxic drugs. Cancer Biother. Radiopharm. (1997) 12:177-186.
81. RUHSTALLER TW, AMSLER U, CERNY T: Rituximab: active treatment of central nervous system involvement by non-Hodgkin’s lymphoma? Ann. Oncol. (2000) 11:374-375.
82. RAIZER JJ, DEANGELIS LM, ZELENETZ AD, ABREY LE: Activity of Rituximab in primary central nervous system lymphoma (PCNSL). Proc. Am. Soc. Clin. Oncol. (2000) 19:166a. Abstract.
83. RUBENSTEIN JL, ROSENBERG J, DAMON LE: High dose methotrexate plus Rituximab in the treatment of primary CNS lymphoma. Neurooncology (1999) 1(Suppl. 4):336. Abstract
84. RUBENSTEIN JL, MCDERMOTT M, SHUMAN MA: Intraventricular delivery of rituximab in a nonhuman primate model. Neurooncology (2000) 2(Suppl.4):292. Abstract.
85. SCHULZ H, PELS H, REHWALD U, ROSENBERG J, SCHLEGEL U, DIEHL V: Treatment of a relapsed radio- and
chemotherapy refractory primary CNS lymphoma with the anti-CD20 antibody IDEC-C2B8. Neurology (2001) 56(Suppl. 8):A411. Abstract.
86. TAKIMOTO C, ARBUCK S: Camptothecins. In: Cancer Chemotherapy and Biotherapy. Chabner BA, Longo DL (Eds.), Lippincott-Raven, Philadelphia, USA (1996):463-484.
87. BAKER SD, HEIDEMAN RL, CROM WR, KUTTESCH JF, GAJJAR A, STEWART CF: Cerebrospinal fluid pharmacokinetics and penetration of continuous infusion topotecan in children with central nervous system tumors. Cancer Chemother. Pharmacol. (1996) 37:195-202.
88. CIORDIA R, HOCHBERG F, AND BATCHELOR T: Topotecan as salvage therapy for refractory or relapsed primary central nervous system lymphoma. Proc. Am Soc. Clin. Oncol. (2000) 19. Abstract.
89. SOUSSAIN C, SUZAN F, HOANG-XUAN K et al.: Results of intensive chemotherapy followed by hematopoietic stem-cell rescue in 22 patients with refractory or recurrent primary CNS lymphoma or intraocular lymphoma. J. Clin. Oncol. (2001) 19:742-749.
90. YEH KH, CHENG AL, TIEN HF: Primary T cell leptomeningeal lymphoma--successful treatment with systemic chemotherapy. Oncology (1995) 52:501-504.
91. MILLER JL: Oral temozolomide approved for refractory brain tumor. Am. J. Health Syst. Pharm. (1999) 56:1910.
92. RENI M, FERRERI AJ, LANDONI C, VILLA E: Salvage therapy with temozolomide in an immunocompetent patient with primary brain lymphoma. J. Natl. Cancer Inst. (2000) 92:575-576.
93. GUTIN PH, WEISS HD, WIERNIK PH, WALKER MD: Intrathecal N, N’-triethylenethiophosphoramide [thio-TEPA (NSC 6396)] in the treatment of malignant meningeal disease: Phase I-II study. Cancer (1976) 38:1471-1475.
94. GUTIN PH, LEVI JA, WIERNIK PH, WALKER MD: Treatment of malignant meningeal disease with intrathecal thiotepa: a Phase II study. Cancer Treat. Rep. (1977) 61:885-887.
95. FORSYTH PA, YAHALOM J, DEANGELIS LM: Combined-modality therapy in the treatment of primary central nervous system lymphoma in AIDS. Neurology (1994) 44:1473-1479.
96. SANDOR V, STARK-VANCS V, PEARSON D et al.: Phase II trial of chemotherapy alone for primary CNS and intraocular lymphoma. J. Clin. Oncol. (1998) 16:3000-3006.
•• Chemotherapy alone, without RT, can achieve a high complete response rate.
97. SARAZIN M, AMERI A, MONJOUR A, NIBIO A, POISSON M, DELATTRE JY: Primary central nervous system lymphoma: treatment with chemotherapy and radiotherapy. Eur. J. Cancer (1995) 31A:2003-2007.
98. FREILICH RJ, DELATTRE JY, MONJOUR A, DEANGELIS LM: Chemotherapy without radiation therapy as initial treatment for primary CNS lymphoma in older patients. Neurology (1996) 46:435-439.
99. DE SMET MD, VANCS VS, KOHLER D, SOLOMON D, CHAN CCP: Intravitreal chemotherapy for the treatment of recurrent intraocular lymphoma. Br. J. Ophthalmol. (1999) 83:448-451.
100. FISHER RI: Current therapeutic paradigm for the treatment of non-Hodgkin’s lymphoma. Semin. Oncol. (2000) 27:2-8.
101. LACHANCE DH, BRIZEL DM, GOCKERMAN JP et al.: Cyclophosphamide, doxorubicin, vincristine, and prednisone for primary central nervous system lymphoma: short-duration response and multifocal intracerebral recurrence preceding radiotherapy. Neurology (1994) 44:1721-1727.
102. MEAD GM, BLEEHEN NM, GREGOR A et al.: A medical research council randomized trial in patients with primary cerebral non-Hodgkin lymphoma: cerebral radiotherapy with and without cyclophosphamide, doxorubicin, vincristine, and prednisone chemotherapy. Cancer (2000) 89:1359-1370.
103. SCHULTZ C, SCOTT C, SHERMAN W et al.: Pre-irradiation chemotherapy with cyclophosphamide, doxorubicin, vincristine, and dexamethasone for primary CNS lymphomas: initial report of radiation therapy Oncology group protocol 88-06. J. Clin. Oncol. (1996) 14:556-564.
104. CHENG AL, YEH KH, UEN WC, HUNG RL, LIU MY, WANG CH: Systemic chemotherapy alone for patients with non-Acquired Immunodeficiency Syndrome-related central nervous system lymphoma: a pilot study of the BOMES protocol. Cancer (1998) 82:1946-1951.

Park & Abrey
Expert Opin. Pharmacother. (2002) 3(1) 49
105. CHAMBERLAIN MC, LEVIN VA: Adjuvant chemotherapy for primary lymphoma of the central nervous system. Arch. Neurol. (1990) 47:1113-1116.
106. DEANGELIS LM, SEIFERHELD W, SCHOLD SC, FISHER B, SCHULTZ CJ Combined modality treatment of primary central nervous system lymphoma (PCNSL): RTOG 93-10. Proc. Am. Soc. Clin. Oncol. (1999) 18:140a. Abstract
107. NELSON DF: Radiotherapy in the treatment of primary central nervous system lymphoma (PCNSL). J. Neurooncol. (1999) 43:241-247.
108. ABREY LE, DEANGELIS LM, YAHALOM J: Long-term survival in primary CNS lymphoma. J. Clin. Oncol. (1998) 16:859-863.
109. CHER L, GLASS J, HARSH GR, HOCHBERG FH: Therapy of primary CNS lymphoma with methotrexate-based chemotherapy and deferred radiotherapy: Preliminary results. Neurology (1996) 46:1757-1759.
AffiliationDeric Minwoo Park & Lauren E Abrey†
†Author for correspondence:Department of Neurology, Memorial Sloan-Kettering Cancer Center, 1275 York Avenue, New York, NY 10021, USATel: +1 212 639-5122; Fax: +1 917 432-2310;E-mail: [email protected]