Embed Size (px)
Citation preview

Inflammatory Stress and Idiosyncratic Hepatotoxicity:Hints from Animal Models
XIAOMIN DENG, JAMES P. LUYENDYK, PATRICIA E. GANEY, AND ROBERT A. ROTH
Departments of Biochemistry and Molecular Biology (X.D.) and Pharmacology and Toxicology (P.E.G., R.A.R.), Center for IntegrativeToxicology, Michigan State University, East Lansing, Michigan; and Department of Pharmacology, Toxicology and Therapeutics, the
University of Kansas Medical Center, Kansas City, Kansas (J.P.L.)
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 262I. Drug-induced idiosyncratic hepatotoxicity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 263
A. Overview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 263B. Example: troglitazone. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 264C. Episodic inflammation and the potential for interactions during drug therapy . . . . . . . . . . . . . . 265D. Inflammatory stress and idiosyncratic adverse drug reactions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 266
II. Inflammation and the liver . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 266A. Overview of inflammation as a contributor to tissue injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 266B. Tumor necrosis factor � . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 267C. Neutrophils . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 268D. The hemostatic system and hypoxia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 269E. Summary of lipopolysaccharide-induced inflammatory responses . . . . . . . . . . . . . . . . . . . . . . . . . . 269
III. Mechanisms of liver injury in models of inflammation-drug interaction: ranitidine anddiclofenac as examples . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 270A. Ranitidine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 270
1. Ranitidine-induced idiosyncratic hepatotoxicity in human patients . . . . . . . . . . . . . . . . . . . . . 2702. Inflammation-ranitidine interaction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2703. Involvement of hemostasis, neutrophils, and tumor necrosis factor �. . . . . . . . . . . . . . . . . . . . 272
a. Hemostasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 272b. Neutrophils . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 272c. Tumor necrosis factor �. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 272
4. Interaction of hemostasis and neutrophils and tumor necrosis factor � . . . . . . . . . . . . . . . . . . 273B. Diclofenac-induced idiosyncratic hepatotoxicity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 275
IV. Summary and conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 277Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 278References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 278
Abstract——Adverse drug reactions (ADRs) presenta serious human health problem. They are major con-tributors to hospitalization and mortality throughoutthe world (Lazarou et al., 1998; Pirmohamed et al.,2004). A small fraction (less than 5%) of ADRs can beclassified as “idiosyncratic.” Idiosyncratic ADRs(IADRs) are caused by drugs with diverse pharma-cological effects and occur at various times duringdrug therapy. Although IADRs affect a number oforgans, liver toxicity occurs frequently and is the
primary focus of this review. Because of the incon-sistency of clinical data and the lack of experimentalanimal models, how IADRs arise is largely unde-fined. Generation of toxic drug metabolites and in-duction of specific immunity are frequently cited ascauses of IADRs, but definitive evidence supportingeither mechanism is lacking for most drugs. Amongthe more recent hypotheses for causation of IADRsis that inflammatory stress induced by exogenous orendogenous inflammagens is a susceptibility factor.In this review, we give a brief overview of idiosyn-cratic hepatotoxicity and the inflammatory re-sponse induced by bacterial lipopolysaccharide. Wediscuss the inflammatory stress hypothesis and useas examples two drugs that have caused IADRs inhuman patients: ranitidine and diclofenac. The re-view focuses on experimental animal models that
Address correspondence to: Dr. Robert A. Roth, Department ofPharmacology and Toxicology, 221 Food Safety and Toxicology Build-ing, Michigan State University, East Lansing, MI 48824. E-mail:[email protected]
This article is available online at http://pharmrev.aspetjournals.org.doi:10.1124/pr.109.001727.
0031-6997/09/6103-262–282$20.00PHARMACOLOGICAL REVIEWS Vol. 61, No. 3Copyright © 2009 by The American Society for Pharmacology and Experimental Therapeutics 1727/3521935Pharmacol Rev 61:262–282, 2009 Printed in U.S.A.
262
by guest on May 4, 2018
Dow
nloaded from

support the inflammatory stress hypothesis and onthe mechanisms of hepatotoxic response in thesemodels. The need for design of epidemiological stud-
ies and the potential for implementation of inflam-mation interaction studies in preclinical toxicityscreening are also discussed briefly.
I. Drug-Induced Idiosyncratic Hepatotoxicity
A. Overview
Drug-induced toxicity is an important human healthproblem. A recent study in the United Kingdom foundthat adverse drug reactions (ADRs)1 targeting severalorgans are responsible for more than 6% of hospitaladmissions, and the mortality rate is approximately 2%(Pirmohamed et al., 2004). Underreporting is suspected,however, and the real incidence might be greater thanestimated by current methods (Bagheri et al., 2000; Sgroet al., 2002). An immediate outcome of ADRs is thewithdrawal or restricted usage of otherwise efficaciousdrugs, leading to deficits in therapy. An example of thisis felbamate (Pellock, 1999; Dieckhaus et al., 2002),which was effective in treating severe cases of epilepsy.Unfortunately, its usage was markedly reduced becauseof its association with aplastic anemia and hepatotoxic-ity in some patients. In addition to posing issues forhuman health, the curtailed use of a drug represents forpharmaceutical companies a loss of financial investmentand of committed scientific effort and profit. Moreover,the occurrence of ADRs presents the likelihood of fur-ther financial loss from lawsuits.
Idiosyncratic ADRs that target the liver are a commoncause of acute liver failure in the United States, account-ing for more than 10% of cases. The results of a 5-yearprospective study indicated that many dietary supple-ments and drugs with different pharmacological targetsare associated with idiosyncratic, hepatotoxic ADRs(Chalasani et al., 2008). The reactions lead to his-topathological and clinical features of acute hepatocel-lular necrosis, biliary injury, or a combination of the two(Zimmerman, 1993, 2000). The main culprits are anti-infective, central nervous system, musculoskeletal, andgastrointestinal drugs (Andrade et al., 2005, 2006).
ADRs can be classified as predictable (type A reac-tions) or idiosyncratic (type B reactions). Type A reac-tions are dose-dependent and occur in a relatively con-
sistent time frame; all individuals are susceptible. Atypical example is acetaminophen-induced hepatotoxic-ity (Larson et al., 2005; Amar and Schiff, 2007). Incontrast, idiosyncratic ADRs (IADRs) occur in a minor-ity of patients during drug therapy and are unrelated tothe pharmacological action of the drug (Senior, 2008).IADRs are currently unpredictable and difficult to diag-nose, and they occur at doses that do not cause toxicityin most people. They typically display a variable onsettime after the beginning of drug therapy, and they havenot been reproducible in animal models (Kaplowitz,2005; Waring and Anderson, 2005; Uetrecht, 2007,2008). These features make IADRs more insidious thantype A reactions, difficult to understand, and more dif-ficult to predict by use of current preclinical testingparadigms or during clinical trials that use relativelyfew volunteers. Better prediction of idiosyncratic drug-induced liver injury will require an understanding of themodes and mechanisms of the reactions.
Drug properties, genetic variation, and environmentalfactors probably contribute to IADRs (Kaplowitz, 2001;Boelsterli, 2003a). Two hypotheses to explain IADRshave become widely accepted in the past few decades.One of them is that the reactions are based on drugmetabolism polymorphisms among patients that resultin different levels of toxic drug metabolites (Williamsand Park, 2003). The other argues that the reactionsarise from an adaptive immune response to proteinsbound to the drug or its metabolites (Park et al., 2001;Ju and Uetrecht, 2002). These two hypotheses are notmutually exclusive, in that a drug metabolism polymor-phism might contribute to reactive metabolite formationand consequently to the production of hapten needed fora harmful adaptive immune response. An extension ofthe latter is the “danger hypothesis” (Pirmohamed et al.,2002; Seguin and Uetrecht, 2003), which suggests that,in addition to immunization and challenge, a second“danger signal” is needed to precipitate an adaptive im-mune response that becomes hepatotoxic. This signalmight be any of a number of factors including some formof cellular stress, underlying disease, or environmentalfactors.
Despite the popularity of these two hypotheses, evi-dence for them is incomplete or lacking for the vastmajority of drugs that have caused IADRs in humanpatients. One drug that has caused considerable concernbecause of its link to severe, hepatotoxic IADRs is tro-glitazone. The next section uses troglitazone as an ex-ample to illustrate the progress, knowledge gaps, andalternative thinking regarding mechanisms of idiosyn-cratic hepatotoxicity.
1 Abbreviations: ABC, ATP-binding-cassette; ADR, adverse drugreaction; COX, cyclooxygenase; P450, cytochrome P450; DCLF, di-clofenac; FAM, famotidine; GI, gastrointestinal; HOCl, hypochlorousacid; H2, histamine 2; IADRs, idiosyncratic ADRs; IL, interleukin;JNK, Jun-N-terminal kinase; KCs, Kupffer cells; LPS, lipopolysac-charide; MAPK, mitogen-activated protein kinase; MIP-2, macro-phage inflammatory protein-2; MPO, myeloperoxidase; NSAID, non-steroidal anti-inflammatory drug; PAI-1, plasminogen activatorinhibitor-1; PAR-1, protease-activated receptor-1; PMNs, neutro-phils; PPAR�, peroxisome proliferator-activated receptor-�; RAN,ranitidine; ROS, reactive oxygen species; SECs, sinusoidal endothe-lial cells; SNPs, single-nucleotide polymorphisms; TACE, TNF�-con-verting enzyme; TF, tissue factor; TGZ, troglitazone; TLR4, toll-likereceptor 4; TNF�, tumor necrosis factor �; TVX, trovafloxacin.
INFLAMMATORY STRESS AND IDIOSYNCRATIC HEPATOTOXICITY 263

B. Example: Troglitazone
Troglitazone (TGZ) was initially marketed in 1997and is one of several thiazolidinediones that have beenused for treatment of type 2 diabetes. It acts pharmaco-logically as a peroxisome proliferator-activated recep-tor-� (PPAR�) agonist and reduces insulin resistance.During clinical trials, 1.9% of patients taking the drugexperienced elevated serum alanine aminotransferaseactivity more than 3 times the upper limit of normal,suggesting mild or moderate hepatocellular injury(Watkins and Whitcomb, 1998). After TGZ was mar-keted, rarer but more severe liver injury also occurred insome patients, and this serious idiosyncratic hepatotox-icity from TGZ led to its withdrawal from the market in2000 (Graham et al., 2003). Liver biopsies from affectedpatients revealed predominantly hepatocellular necrosiswith occasional bridging fibrosis. The time frame of hep-atotoxicity occurrence varied from within a month toseveral years after initiation of maintenance therapy.IADRs induced by TGZ are most probably independentof its pharmacological target, because other thiazo-lidinediones, such as rosiglitazone and pioglitazone, alsoact as PPAR� agonists, yet lack the same hepatotoxicpotential in patients with diabetes (Scheen, 2001a,b).
Since its withdrawal from the market, a large amountof effort has been devoted to elucidating the mechanismof TGZ-induced hepatotoxicity. A variety of hypotheseswere proposed, including reactive metabolite formationand accumulation, mitochondrial dysfunction and oxida-tive stress, inhibition of bile salt exporter pump, andapoptosis (Chojkier, 2005; Masubuchi, 2006). The majorTGZ metabolites (sulfate, glucuronide, quinone) havebeen identified in cultured cells, experimental animals,and human patients (Kawai et al., 1997; Loi et al., 1999;Yoshigae et al., 2000; Honma et al., 2002; Watanabe etal., 2002). However, TGZ metabolite-protein adductshave only been demonstrated in liver microsomal prep-arations from rats with various cytochrome P450 (P450)inducers or in “supersomes” (cDNA-expressed humanP450) (He et al., 2004). Furthermore, although TGZ iscytotoxic to human HepG2 cells and to rat and humanhepatocytes in vitro, inhibitors of enzymes responsiblefor TGZ metabolism do not protect against TGZ-inducedcytotoxicity (Kostrubsky et al., 2000; Yamamoto et al.,2001; Tirmenstein et al., 2002). HepG2 cells transfectedwith CYP3A4 or incubated with microsomes containingcDNA-expressed CYP3A4 metabolized TGZ, leading toincreased cytotoxicity (Vignati et al., 2005). However,the TGZ quinone metabolite formed by CYP3A4 is lesscytotoxic than TGZ itself, both in rat hepatocytes andHepG2 cells (Tettey et al., 2001). In addition, in normalhuman hepatocytes, these CYP3A4-related metabolitesare unlikely to be generated or to accumulate in anamount large enough to exert toxic effects. Studies in-vestigating TGZ-induced cytotoxicity were performedwith cultured cell lines or primary cells using concentra-
tions of TGZ 1 to 2 orders of magnitude greater thanthose likely to occur in patients. Thus, these studies ofmetabolism in vitro have not provided an explanationfor the infrequent TGZ hepatotoxicity that occurs inpatients, and the role of reactive metabolites in TGZcytoxicity remains unclear.
The role of metabolism in TGZ toxicity in vivo is notclear either. The hepatic expression and activity ofCYP3A4 vary significantly among individuals (Eichel-baum and Burk, 2001). This might occur, in part, as aconsequence of single-nucleotide polymorphisms (SNPs)in the CYP3A4 gene or its promoter. SNPs have beenfound in three genes important for CYP3A activity(Kuehl et al., 2001). SNPs of the CYP3A gene familymembers affect various ethnic groups, occurring withrelatively high frequency in Europeans and Americansof European descent (Hustert et al., 2001; Kuehl et al.,2001). TGZ quinone (metabolite M3) is the putative re-active metabolite formed by CYP3A4 (Rothwell et al.,2002). However, treatment of primates with doses ofTGZ sufficient to cause exposure to the TGZ M3 metab-olite (i.e., up to 1.2 g/kg) did not cause hepatotoxicity(Rothwell et al., 2002).
In human patients, M3-derived reactive intermedi-ates were found to bind covalently to microsomal proteinand glutathione (Tettey et al., 2001; He et al., 2004), butthe importance of these adducts to TGZ-associated hep-atotoxicity has not been established. In a cohort study of4079 patients, combined genetic polymorphisms fromseveral genes were associated with increased suscepti-bility to TGZ-induced liver injury. These includedCYP1A1, NAD(P)H dehydrogenase, quinone 1, glucosetransporter type 1, PPAR�-892, and PPAR�-1431 (de laIglesia FA. et al., 2003). In another study, a strongcorrelation was also observed in patients between TGZ-induced liver injury and the combined glutathione trans-ferase-�1–glutathione transferase M1 null genotype(Watanabe et al., 2003). However, none of these studiesestablished a functional relationship between theseSNPs and TGZ-induced liver injury.
Several case reports described histological evidenceconsistent with an adaptive immune-mediated reaction(Arioglu et al., 2000; Kohlroser et al., 2000; Murphy etal., 2000), and responses from some patients were re-duced by corticosteroids (Prendergast et al., 2000; Bonk-ovsky et al., 2002). One of these patients developed asimilar cholestatic hepatitis when switched to rosiglita-zone after TGZ treatment, consistent with an adaptiveimmune-mediated reaction and suggesting a class effectrelated to the drugs’ pharmacophore (Bonkovsky et al.,2002). Although eosinophils and granulomatous inflam-matory infiltrates have been observed in the livers ofpatients with TGZ hepatotoxicity, this alone does notconstitute conclusive evidence that these cells played arole in the hepatotoxic response or that an adaptiveimmune reaction was responsible. Animal models that
264 DENG ET AL.

recapitulate TGZ hepatotoxicity, in particular, an im-mune hypersensitivity component, have not emerged.
A study by Ong et al., (2007) showed that TGZ inducesmild hepatocellular injury after 4 weeks of treatment ofmice heterozygous for the mitochondrial antioxidant en-zyme, superoxide dismutase 2. Hepatic mitochondriaisolated from TGZ-treated mice exhibited enhanced ox-idative stress. Furthermore, in hepatocytes isolatedfrom untreated superoxide dismutase 2(�/�) mice, butnot wild-type mice, TGZ caused a concentration-depen-dent increase in superoxide anion production. TGZ-in-duced superoxide generation was shown to induce injuryto hepatocytes by activating apoptosis signal-regulatingkinase 1 (Lim et al., 2008). This was the first publisheddemonstration in an animal model that TGZ treatmentcould cause hepatocellular injury, even though the tox-icity was mild. In agreement with other studies, wild-type animals tolerated the drug without adverse effects.The results support the general concept that subclinicalstresses from prolonged drug treatment superimposedon a genetic deficiency in the same organism can lead tocell injury and organ damage. The use of the SOD het-erozygous mouse as a model to study mitochondrialmechanisms of drug-induced liver injury has recentlybeen reviewed (Boelsterli and Hsiao, 2008).
The findings of Boelsterli and colleagues suggestedthat healthy experimental animals are resistant to TGZhepatotoxicity because they lack some undefined stres-sor required to produce hepatotoxicity (Boelsterli andHsiao, 2008). By extension, differences in such stressorsin human patients, either genetic or environmental,might constitute susceptibility factors to TGZ-inducedhepatotoxicity. Moreover, the unpredictable temporaland dose relationships that characterize IADRs fromTGZ and other drugs could be explained if stressor ex-pression was episodic and its effects unnoticed in theabsence of drug treatment.
C. Episodic Inflammation and the Potential forInteractions during Drug Therapy
It may not be mere coincidence that antibiotics andnonsteroidal anti-inflammatory drugs (NSAIDs) thatare used in clinical conditions associated with inflam-mation are also the most common causes of hepaticIADRs (Hussaini and Farrington, 2007; Chalasani et al.,2008). Likewise, the presence of viral hepatitis (i.e., he-patic inflammation) is a risk factor for idiosyncratic hep-atotoxicity from antiretroviral drugs in patients infectedwith HIV (Hussaini and Farrington, 2007). Such obser-vations suggest the possibility that inflammatory stressduring drug therapy could contribute causally to hepa-totoxic IADRs.
An inflammatory response can be considered a collageof stresses originating from numerous inflammatorycells and the various mediators that they produce (seesection II, below). Such stresses are capable of alteringtissue homeostasis and may thereby set the stage for
tissue injury. Systemic or localized inflammation is com-monplace and can be caused by infection, concurrentdisease, or other factors. Inflammation is a feature ofnumerous diseases and in some cases participates indisease pathogenesis. Anti-inflammatory therapy has beensuccessful in the treatment of arthritis, inflammatorybowel disease, asthma, and other disease entities. Further-more, inflammation plays a key role in chronic conditionssuch as diabetes (Tracy, 2003), obesity (Cottam et al.,2004), cardiovascular disease (Willerson and Ridker,2004), and cancer (Whitcomb, 2004; De Marzo et al., 2007).Adaptive immune responses (allergic reactions) to specificantigens usually have an inflammatory component. Acti-vation of the innate immune system by exposure to exog-enous bacteria, viruses, and their molecular constituentsalso results in inflammation. It is noteworthy that micro-organisms indigenous to the gastrointestinal (GI) tract ofhumans are responsible for periodic inflammation. Forexample, liver and GI diseases are associated with in-creased blood levels of endotoxin (lipopolysaccharide, LPS),a cell wall component of Gram-negative bacteria (Gardineret al., 1995), and LPS is a well characterized inducer ofinflammation. Surgery can elevate plasma LPS concentra-tion, as can changes in diet, alcohol consumption, or anti-biotic treatment (Roth et al., 1997; Lepper et al., 2002).Drugs known to produce GI injury, such as NSAIDs, cancause translocation of LPS from the GI tract to blood (Kimet al., 2005; Deng et al., 2006). These and other factorsresult in inflammatory stress in humans that is episodicand common and can occur under numerous conditions inthe absence of overt tissue injury.
Concurrent inflammation could precipitate IADRs bya variety of mechanisms. Minor hepatic injury elicitedby some drugs might progress to more serious injury asdamaging inflammatory mediators are generated andreleased. In addition to exacerbating the hepatotoxicresponse, inflammation might inhibit or delay liver re-generation and repair. Conversely, inflammatory stressmight also initiate hepatotoxicity that could be exacer-bated by certain drugs. Increased sensitivity of the livermight occur as a consequence of altered cellular signal-ing, accumulation and activation of extrahepatic cells, orother factors. Inflammation can inhibit expression ofdrug-metabolizing enzymes (e.g., P450s). This could re-sult in accumulation of parent compound in the liver andimpaired drug clearance, which could pose a significantrisk for patients taking these drugs (Renton, 2005; Mor-gan et al., 2008). Furthermore, concurrent inflammationmight modify the intrahepatic distribution of drugs byaltering expression of drug transporters including theATP-binding-cassette (ABC) transporters in hepatocytes(Renton, 2005; Petrovic et al., 2007). Thus, there aremany ways in which drugs might interact with an in-flammatory response to cause liver injury. The effects ofinflammation on sensitivity of the liver to drug-inducedinjury and the diverse factors and mechanisms involvedwill be the focus of the remainder of this review.
INFLAMMATORY STRESS AND IDIOSYNCRATIC HEPATOTOXICITY 265

D. Inflammatory Stress and Idiosyncratic AdverseDrug Reactions
As described above, episodic exposures to inflamma-tory stimuli are common in people, although most causeno obvious tissue injury. Moreover, they occur irregu-larly and often go unnoticed. These observations led usto hypothesize that an episode of inflammation duringdrug therapy might decrease the threshold for drug tox-icity and thereby render an individual susceptible to anadverse drug reaction. This hypothesis could explainmany of the characteristics of IADRs. The irregular fre-quency of inflammatory episodes is consistent with theerratic temporal relationship to onset of therapy. Fur-thermore, an inflammation-mediated increase in sensi-tivity to hepatic toxicity from a drug could explain theapparent lack of dose-toxicity relationship for these re-actions. Accordingly, this hypothesis is an attractiveexplanation for the basis of some IADRs.
Small doses of LPS precipitate modest inflammatoryresponses in mammals, resulting in increased suscepti-bility to toxicity from numerous hepatotoxic chemicals(Roth et al., 1997; Ganey and Roth, 2001). For example,exposing rats to a nonhepatotoxic dose of LPS resultedin a significant decrease in the dose of allyl alcoholrequired to produce liver injury (Sneed et al., 1997). Thisincrease in sensitivity depended on an LPS-stimulatedinflammatory response involving resident hepatic mac-rophages (Kupffer cells, KCs), cyclooxygenase (COX)-2-derived eicosanoids, neutrophils (PMNs), and the coag-ulation cascade (Sneed et al., 1997; Ganey et al., 2001;Kinser et al., 2002, 2004). Such observations with agentsthat cause type A hepatotoxic reactions provide furthersupport for the possibility that inflammation can alterthe sensitivity of liver to injury and for the hypothesisthat some idiosyncratic reactions might arise from drug-inflammation interaction.
Evidence is growing that mild inflammation from ex-posure to LPS interacts with drugs that cause humanIADRs to cause liver injury in experimental animals(Table 1). For example, coadministration of nonhepato-toxic doses of LPS and the antipsychotic drug chlorprom-azine to rats results in liver damage that resembleshuman chlorpromazine idiosyncrasy (Buchweitz et al.,2002). Trovafloxacin (TVX), a fluoroquinolone antibioticassociated with idiosyncratic reactions, also interacts
with LPS, resulting in hepatotoxicity both in rats andmice (Waring et al., 2006; Shaw et al., 2007). In contrast,levofloxacin, another quinolone antibiotic without thetendency for causing idiosyncratic liver injury in people,does not share this capacity for hepatotoxic interactionwith inflammatory stress in rodents. Thus, this model ofdrug-inflammation interaction is able to distinguish adrug that causes IADRs from one in the same pharma-cological class that does not. Besides LPS, Gram-positivebacterial components (i.e., peptidoglycan and lipotei-choic acid) also interact with nontoxic doses of TVX toprecipitate liver injury in mice (Shaw et al., 2008). Re-sults of recent studies show that three other drugs as-sociated with IADRs, sulindac, amiodarone, and halo-thane, also induce liver injury at otherwise nontoxicdoses when coadministered with LPS (Dugan et al.,2008; Lu et al., 2009; Zou et al., 2009). A recent studyindicated that activation of the innate immune responseby viral RNA mimetic poly(I:C) also exaggerated halo-thane hepatotoxicity (Cheng et al., 2009), supporting thehypothesis that inflammation contributes to IADRs(Roth et al., 2003). Such inflammatory stress-drug inter-action models in animals that mimic IADRs in humanpatients could provide useful tools for mechanisticstudy, which in turn might lead to novel biomarkers andmethods to prevent or treat IADRs. Because much workto date has focused on models in which rats are treatedwith LPS and either ranitidine (RAN) or diclofenac(DCLF), these IADR-associated drugs will be empha-sized in the remainder of this review.
II. Inflammation and the Liver
A. Overview of Inflammation as a Contributor toTissue Injury
Inflammation is traditionally defined as a local reac-tion of tissue to irritation, injury, or infection character-ized as “redness, swelling, pain, heat and loss of func-tion.” However, it is now viewed in terms of theactivation of cells of the innate immune system, thecoordinated actions of the mediators they produce, andaltered inflammatory gene expression and cell signaling.Inflammation participates in host defense against mi-crobial pathogens but also has the potential to injuretissues. Indeed, as mentioned above, it has become clearthat inflammation plays a role in the pathogenesis ofmany diseases, can cause tissue injury by itself, and canincrease sensitivity of tissues to the toxic effects of xe-nobiotic agents.
Inflammation encompasses not only traditional in-flammatory cells (e.g., PMNs, macrophages) and themediators they produce (e.g., cytokines/chemokines, co-agulation and complement proteins, lipid mediators),but also endothelial cells and parenchymal cells in thetissue (Ganey et al., 2004). The inflammatory cells canattack and damage tissues directly by releasing toxicfactors such as reactive oxygen species (ROS), proteases,
TABLE 1Similarity in ability of drugs to cause hepatotoxic IADRs in human
patients and liver injury in LPS/drug models in rodents
Drug Human IADRs? LPS � Drug Hepatotoxicityin Rodents?
Diclofenac Yes YesSulindac Yes YesHalothane Yes YesChlorpromazine Yes YesTrovafloxacin Yes YesLevofloxacin No NoRanitidine Yes YesFamotidine No No
266 DENG ET AL.

etc., or they can release cytokines, eicosanoids, or othermediators that lead indirectly to damaging events. Thehemostatic and complement systems are also activatedin inflammatory responses and can participate in tissueinjury. Various transcription factors [e.g., nuclear factor�B, activator protein-1, early growth response-1] inducethe expression of gene products integral to the inflam-matory response. Transcriptional regulators not onlycontrol the production of inflammatory mediators butalso play an important role indirectly in the activation ofvarious cells involved.
LPS is an important example of an inflammagen thatelicits the expression of a broad range of proinflamma-tory genes. Monocytes/macrophages are the primary in-nate immune cells that orchestrate LPS-induced inflam-mation. LPS-binding protein presents LPS to CD14 onthe plasma membrane of these and other cells. Theinteraction of this complex with the pattern recognitionreceptor, Toll-like receptor 4 (TLR4), activates a complexintracellular signaling network. TLR signaling has beenwell studied and is described in detail elsewhere (Guhaand Mackman, 2001; Oda and Kitano, 2006). LPS acti-vates several proinflammatory intracellular signalingcascades [e.g., the mitogen activated protein kinases(MAPKs) p38, extracellular-regulated kinase 1/2, andJun-N-terminal kinase (JNK)1/2, and I�B kinase] andanti-inflammatory signaling cascades (e.g., PI3K-Aktsignaling pathway). These intracellular signaling path-ways coordinate activation of transcription factors andthe induction of gene expression. The response elicitedby exposure to large amounts of LPS, such as duringGram-negative bacterial sepsis, can result in damage toseveral organs including the liver, as well as death(Hewett and Roth, 1993). Of importance, inflammatorycells such as KCs, endothelial cells, stellate cells, andbile duct epithelial cells in the liver recognize LPS andcontribute to inflammation. KCs also remove LPS fromthe sinusoidal blood, thereby acting as an active “filter”for bacterial products inappropriately released into theportal circulation. This can reduce the exposure of otherorgans to LPS, but LPS originating from the GI tract canelicit a localized, and potentially damaging inflamma-tory response in the liver. The next section discusses therole of some inflammatory mediators in the pathogene-sis of liver injury induced by systemic endotoxemia. Par-ticular emphasis is placed on the contribution of hepaticparenchymal and nonparenchymal cells in the inflam-matory response. The involvement of these mediators inliver toxicity from selected xenobiotic agents will also bementioned.
B. Tumor Necrosis Factor �
Tumor necrosis factor � (TNF�) is critically importantin inflammatory responses. Production of this cytokineis triggered by LPS mainly in monocytes/macrophages(Michalek et al., 1980), including KCs in the liver
(Hewett and Roth, 1993). Hepatic expression of TNF�mRNA increases shortly after systemic exposure to LPS,and the concentration of TNF� protein in blood riseswithin a few minutes (Hewett and Roth, 1993). TNF�production can be regulated at a post-transcriptionallevel. For example, TNF� mRNA stabilization andtranslation are regulated by p38 MAPK (Neininger etal., 2002; Hitti et al., 2006). Furthermore, TNF� con-verting enzyme (TACE) cleaves the 26-kDa membrane-bound pro-TNF� protein to generate the secreted, 17-kDa mature TNF� (Aggarwal et al., 1985; Mullberg etal., 2000). The release of TNF� from cells in vitro and invivo can be selectively blocked by hydroxamate-basedmetalloprotease inhibitors that inhibit TACE activity(Gearing et al., 1994; McGeehan et al., 1994; Mohler etal., 1994).
TNF� activates two cellular receptors (TNFR1 [p55]and TNFR2 [p75]) to initiate cell death signaling, pro-mote inflammatory mediator release, increase expres-sion of nitric oxide synthase 2, activate the hemostaticsystem, and induce cell proliferation (Vassalli, 1992;Hehlgans and Pfeffer, 2005). TNF� has been identifiedas a critical proinflammatory cytokine of the acute in-flammatory response, as well as a major component inthe pathogenesis of the septic shock syndrome (Tarta-glia et al., 1993; Rietschel et al., 1996). The expression ofTNF� and its role in liver damage have been reviewedelsewhere (Schwabe and Brenner, 2006; Tacke et al.,2009). Indeed, TNF� infusion into the circulation leadsto a sepsis-like syndrome in rats (Tracey et al., 1986).Administration of TNF�-neutralizing antibodies to ba-boons protects them from lethal bacteremia triggered byinfusion of live Escherichia coli (Tracey et al., 1987). Inthese models, TNFR1 is essential in mediating TNF�signaling, because TNFR1-deficient mice are protectedfrom septic shock induced by LPS/D-galactosamine orStaphylococcus aureus superantigen/D-galactosamine(Pfeffer et al., 1993). However, in experimental modelsusing concanavalin A or Pseudomonas exotoxin A-in-duced hepatitis, TNFR2 signaling seems to be importantfor the host-damaging effects (Kusters et al., 1997; Schu-mann et al., 1998). Administration of TNF�-neutralizingantibodies or inhibition of TNF� biosynthesis signifi-cantly attenuates liver injury from large doses of LPS inrodents (Hewett and Roth, 1993; Mohler et al., 1994).Moreover, inhibitors of TACE protect against endotoxin-mediated lethality, in which TNF� plays a critical role(Mohler et al., 1994).
TNF� not only promotes tissue injury, but it alsohas beneficial effects. Activation of TNFR2 by endog-enous TNF� is important for the development of LPS-induced resistance to bacterial infection (Echtenacherand Mannel, 2002). The cecal ligation and puncturemodel generates invasion of gut-derived bacteria intothe blood stream and into organs, causing a sepsis-likesyndrome. In this model, TNF� is important for recov-ery and survival from septic peritonitis (Echtenacher
INFLAMMATORY STRESS AND IDIOSYNCRATIC HEPATOTOXICITY 267

et al., 1990, 1995). A state of immunoparalysis char-acterized by a reduced production of TNF� developsafter cecal ligation and puncture, which results inbacterial superinfection and subsequent lethality.TNF� administration during this phase of immunopa-ralysis can be beneficial or deleterious, depending onthe location of TNF� activity, timing of TNF� admin-istration, and the type of infection (Echtenacher et al.,2003). From these results, it is clear that TNF� hasmultiple, sometimes opposing actions, and under-standing of the role of TNF� in both defense againstpathogens and host damage is currently incomplete.
C. Neutrophils
PMNs are involved in producing liver injury inducedby large, hepatotoxic doses of LPS (Hewett et al., 1992).After exposure of rodents to LPS, the mRNAs encodingvarious PMN chemoattractants, such as cytokine-in-duced neutrophil chemoattractant-1, interleukin (IL)-8,or KC/Gro, and macrophage inflammatory protein-2(MIP-2) increase in the liver, and these proteins aredetectable in the plasma. The cellular source of thesechemokines in the livers of endotoxemic mice has notbeen definitively identified, although Kupffer cell deple-tion does not affect hepatic MIP-2 and KC/Gro expres-sion in LPS-treated mice (Kopydlowski et al., 1999).Adhesion molecules become up-regulated on the sur-faces of sinusoidal endothelial cells (SECs), PMNs, andhepatocytes (Jaeschke et al., 1996). The up-regulation ofthese chemokines and adhesion molecules facilitatesPMN transmigration across the endothelial cell layerand promotes subsequent localization of PMNs close tohepatocytes (Butcher, 1991; Springer, 1994). This trans-migration and activation process involves rolling along,binding to, and migrating across the endothelium. Themigration of PMNs from the liver microvasculature isregulated by at least three distinct types of moleculesinteracting with their respective receptors: selectins, in-tegrins, and chemokines. A key feature is that theseligand-receptor interactions act in sequence, not in par-allel (Ley et al., 2007). Selectins initiate the rolling ofPMNs across the endothelium, whereas integrins causefirm adhesion. Integrins and chemokines comprise thedriving force for transmigration into the liver paren-chyma (Kobayashi, 2008). This concept of sequentialaction has been confirmed by the observation that inhi-bition of any one of these steps gives essentially com-plete, rather than partial inhibition of PMN emigrationfrom blood vessels.
PMNs are critical mediators of injury in models ofLPS-potentiated hepatotoxicity, such as from aflatoxinB1, monocrotaline, and TVX (Barton et al., 2000; Yee etal., 2003b; Waring et al., 2006). There are several likelymechanisms by which these cells contribute to tissuedamage. When activated, PMNs release numerous cyto-toxic factors, including ROS and proteases (Ganey et al.,1994; Jaeschke et al., 2002), such as cathepsin G and
elastase (Ho et al., 1996). ROS and proteases mediatetissue injury in several pathological conditions such asacute lung injury, endotoxemia, and ischemia-reperfu-sion injury (Jaeschke et al., 1990, 1991; Kawabata et al.,2002).
There is no consensus on the relative contributions ofROS and proteases to PMN-induced hepatocyte injury.PMN-mediated hepatocellular death can occur within1 h in vivo and coincides with the appearance of intra-cellular oxidant stress and the formation of hypochlo-rite-mediated chlorotyrosine protein adducts (Jaeschkeet al., 2002; Gujral et al., 2004; Hasegawa et al., 2005).A selective inhibitor of PMN NADPH oxidase, the en-zyme that catalyzes production of ROS, significantlydelayed liver injury in galactosamine-sensitized micegiven LPS (Gujral et al., 2004). Mice deficient in gluta-thione peroxidase-1 also showed enhanced susceptibilityto PMN-mediated liver injury (Jaeschke et al., 1999).These results suggest a crucial role for the PMN-depen-dent oxidative burst and ROS generation in the patho-genesis of liver injury. On the other hand, in experi-ments using activated PMNs cocultured withhepatocytes, protease inhibitors, but not antioxidant en-zymes, prevented PMN-mediated cell injury, and cellkilling could be reproduced by substituting cathepsin Gor elastase for PMNs (Mavier et al., 1988; Harbrecht etal., 1993; Ganey et al., 1994).
PMNs stimulated to release proteases and ROS killhepatocytes with a time course similar to that of pro-teases alone (Ganey et al., 1994). This time frame (15–20h) is much longer than that by which hepatocellularinjury develops in LPS-treated rats, suggesting, how-ever, that PMN proteases might act in concert withother factors to damage hepatocytes in vivo. It is alsopossible that isolated, primary hepatocytes lack key fea-tures of hepatocytes altered by an inflammatory re-sponse in vivo (Gujral et al., 2004). Such features couldinclude increased sensitivity of hepatocytes to PMN-derived proteases. For example, when isolated hepato-cytes were exposed to PMN proteases in a hypoxic envi-ronment, damage occurred more rapidly than in anoxygen-replete environment (Luyendyk et al., 2005).Moreover, PMN protease inhibitors protected the liverfrom injury caused by ischemia-reperfusion, althoughthis attenuation was accompanied by a decrease in cir-culating chemokines and hepatic PMN accumulation(Yamaguchi et al., 1997). Thus, PMN proteases mightcontribute to hepatocellular injury by mechanisms inde-pendent of direct hepatocyte killing (Yamaguchi et al.,1997, 1999; Soejima et al., 1999). It is possible that PMNproteases induce intracellular oxidative stress in hepa-tocytes, which could be exacerbated by glutathione per-oxidase deficiency. Thus, the composite of all inflamma-tory mediators and additional cellular stressors areprobably necessary for the complete manifestation ofPMN-dependent hepatocyte killing in vivo.
268 DENG ET AL.

D. The Hemostatic System and Hypoxia
The coagulation and fibrinolytic systems are impor-tant controllers of vascular hemostasis (Levi et al., 2003)and act to limit hemorrhage after vascular injury (Mack-man, 2007). On the other hand, the coagulation cascadecontributes to thrombosis (e.g., myocardial infarction,stroke, deep vein thrombosis, pulmonary embolism) andto the pathogenesis of numerous diseases including ath-erosclerosis, cancer, and sepsis (Levi et al., 2003; Spek,2004; Levi, 2005). Components of the coagulation andfibrinolytic systems also participate in the liver damageinduced by LPS-mediated inflammation.
The hemostatic system has been the subject of numer-ous excellent reviews (e.g., (Mackman et al., 2007; Rauet al., 2007), and only elements germane to the studiesbelow will be described briefly here. LPS induces theexpression of tissue factor (TF; coagulation factor 3,thromboplastin) by hematopoietic cells (e.g., monocytes/macrophages, platelets) (Pawlinski et al., 2004), and thisactivates the coagulation cascade in mice. The formationof a complex between TF and coagulation factor VIIaactivates a cascade of coagulation factors, ultimatelygenerating the serine protease thrombin. Thrombincleaves circulating fibrinogen into fibrin. Fibrin, uponcross-linking and polymerization, is a major componentof clots in blood vessels. The coagulation cascade is neg-atively regulated by several proteins, such as protein C,TF pathway inhibitor, and antithrombin. Likewise, fi-brin deposition in blood vessels is tightly regulated bythe fibrinolytic system. Plasminogen activators, includ-ing urokinase PA and tissue-specific PA, cleave plasmin-ogen into its active form, plasmin. Plasmin can cleaveand dissolve cross-linked fibrin. The activity of the plas-minogen activators is negatively regulated by plasmin-ogen activator inhibitor-1 (PAI-1).
Inhibition of thrombin significantly attenuated LPS-induced liver injury in rats (Hewett and Roth, 1995;Moulin et al., 2001), although the injury was indepen-dent of circulating fibrinogen (Hewett and Roth, 1995).This suggests that thrombin activity, but not fibrin clots,is required for LPS-induced liver injury. Indeed, throm-bin activation of the tethered-ligand receptor, proteaseactivated receptor-1 (PAR-1), seems to play a criticalrole in LPS-induced liver injury. Perfusion of livers fromLPS-treated rats with thrombin or a PAR-1 agonistcaused hepatocellular injury in a PMN-dependent man-ner (Moulin et al., 2001; Copple et al., 2003). Moreover,thrombin inhibition impaired PMN activation in LPS-treated rats (Pearson et al., 1996a,b; Copple et al., 2003).These results suggest that thrombin activation of PAR-1is important for PMN activation in endotoxemia andthat both of these events are sufficient for causing in-flammatory liver injury in rats given a large, hepato-toxic dose of LPS.
Although fibrin deposition does not seem to be impor-tant for liver injury caused by large doses of LPS, it
might be important in animals cotreated with smallerdoses of LPS and another xenobiotic agent (Luyendyk etal., 2004; Beier et al., 2009). One of the possible conse-quences of fibrin deposition in liver sinusoids is tissuehypoxia caused by impaired blood flow. Hypoxia candeplete cellular ATP and interfere with intracellular pHand homeostasis of ions such as Na� and Ca2�, whichcould subsequently cause cell death (Carini et al., 1997,2000). In addition, hypoxia can cause the production ofROS (Lluis et al., 2005, 2007). It can also activate nu-merous intracellular signaling pathways related to cellstress and stabilize hypoxia inducible factor-1�, an im-portant transcription factor (Piret et al., 2002). Breath-ing a low O2 atmosphere enhanced the liver lesions inrats caused by a large, hepatotoxic dose of LPS(Shibayama, 1987). This suggests that hypoxia mightinteract with LPS-induced inflammatory mediators tocause hepatocellular injury in vivo.
As mentioned above, PAI-1 is the major endogenousdown-regulator of fibrinolysis. PAI-1 is synthesized by avariety of cells in culture (e.g., hepatocytes, adipocytes,endothelial cells, cardiac myocytes) (Macfelda et al.,2002; Westrick and Eitzman, 2007), although the cellu-lar source of PAI-1 in vivo is probably model- and dis-ease-dependent. A PAI-1 pool is also found in the gran-ules of platelets, where it is stored and can be releasedafter vessel damage (Hoekstra et al., 2004). PAI-1 ispresent in three forms in the circulation: active, inactive,and latent forms. The active form converts spontane-ously into the latent form with a half-life of 1 h (Hoek-stra et al., 2004). The latent form is more stable and canbe reconverted into the active form. PAI-1 is removedfrom the circulation by the liver and is also inactivatedby endothelium (Hekman and Loskutoff, 1985; Owensbyet al., 1991). Endothelium- or platelet-derived PAI-1 isnormally complexed to vitronectin, resulting in an in-creased half-life of PAI-1 in the circulation.
Experiments in vitro have demonstrated that expres-sion of PAI-1 can be induced by a variety of factorsinvolved in inflammatory responses, including TNF�,IL-1, transforming growth factor-�, LPS, glucocorti-coids, and insulin. The transcriptional induction ofPAI-1 is mediated through an Sp1 element, hypoxia-responsive element, and/or Sma- and Mad-related pro-tein 3/4 (SMAD 3/4) binding sites in the PAI-1-promoter(Fink et al., 2002; Hou et al., 2004). Up-regulation ofPAI-1 is associated with disseminated intravascular co-agulation and other thrombotic diseases (Padro et al.,1995, 1997). PAI-1 also plays a role in models of acuteand chronic liver injury (Bergheim et al., 2006; Arteel,2008).
E. Summary of Lipopolysaccharide-InducedInflammatory Responses
As discussed above, LPS affects numerous inflammatorypathways through activation of TLR4. These include intra-cellular signaling pathways and transcription factors (e.g.,
INFLAMMATORY STRESS AND IDIOSYNCRATIC HEPATOTOXICITY 269

nuclear factor �B, p38) and inflammatory mediators (e.g.,TNF�). The coordination of these mediators leads to theactivation of innate immune cells (e.g., monocytes, PMNs),coagulation, and complement systems, etc., the conse-quence of which can be tissue injury (Table 2). In thecontext of hepatotoxic LPS-drug interaction, it is possiblethat numerous inflammatory mediators are critical, andthese mediators might vary among drugs.
III. Mechanisms of Liver Injury in Models ofInflammation-Drug Interaction: Ranitidine and
Diclofenac as Examples
Given the scarcity and inconsistency of clinical data,animal models of LPS-drug interaction could be helpfulin understanding IADRs. Mechanistic studies usingsuch models could provide biomarkers to predict thesereactions. This section discusses two potential IADRanimal models resulting from LPS-drug interaction:LPS-RAN and LPS-DCLF models.
A. Ranitidine
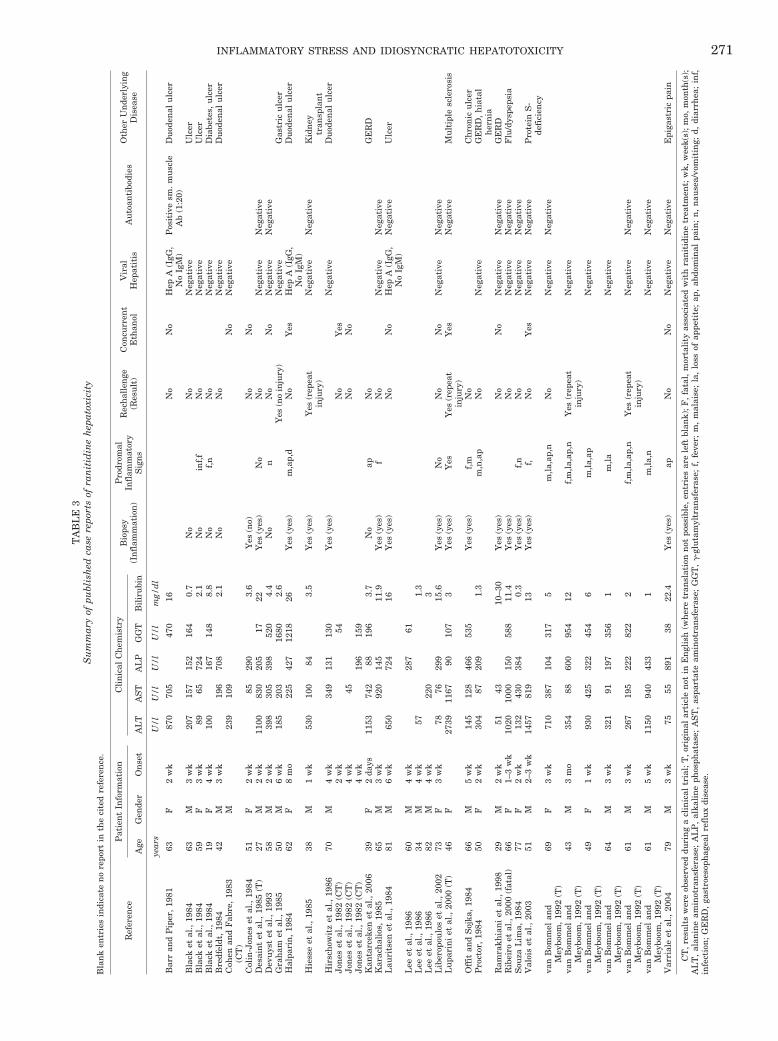
1. Ranitidine-Induced Idiosyncratic Hepatotoxicity inHuman Patients. A widely used drug associated withidiosyncratic hepatotoxicity is the histamine 2 (H2)-re-ceptor antagonist, RAN. RAN is available over thecounter for oral administration or by prescription forparenteral administration for treatment of duodenal ul-cers, gastric hypersecretory diseases, and gastroesopha-geal reflux disease. Idiosyncratic hepatotoxicity occursin less than 0.1% of people taking RAN (Vial et al.,1991). A summary of numerous published case reportsappears in Table 3. The capacity of RAN to cause IADRsis not related to its pharmacological action, because fa-motidine (FAM), a H2 receptor antagonist also in long-term use, does not share this liability. Most liver reac-tions from RAN are mild and reversible; however,extensive liver damage and death have occurred in someindividuals (Ribeiro et al., 2000). RAN hepatotoxicitytypically manifests as elevations in serum markers ofhepatocellular injury with more modest increases in in-dicators of cholestatic injury. The reactions are typical ofIADRs, because the time of onset of hepatotoxicity rela-tive to initiation of therapy varies greatly (Table 3).Rechallenge with RAN does not necessarily result in areoccurrence of toxicity (Graham et al., 1985). Indeed, in
some cases the adverse response resolved despite con-tinued therapy (Barr and Piper, 1981). These character-istics do not seem consistent with an adaptive immuneresponse as the cause of RAN IADRs.
RAN is minimally converted into three metabolites inboth humans and rats: N-oxide, S-oxide, and desmethylmetabolites (Carey et al., 1981; Chung et al., 2000). RANis excreted mostly unchanged in urine in humans asopposed to through bile in rats (Carey et al., 1981;Huang et al., 2005). No known RAN metabolite has beenreported to be toxic to liver either in humans or rodentsto our knowledge. Accordingly, it seems unlikely thatIADRs caused by RAN are due to metabolic bioactiva-tion of this drug.
Although direct evidence implicating inflammation asa contributing factor to these idiosyncratic reactions islacking, it is interesting that several human case reportsof RAN idiosyncratic hepatotoxicity mentioned prodro-mal signs consistent with endotoxemia or inflammation(e.g., diarrhea, fever, nausea/vomiting, and/or abdomi-nal pain; Table 3). In several of the cases, the patientshad GI ulceration, which could increase translocation ofbacterial products like LPS into the portal circulation.Thus, it is possible that some RAN-induced IADRs re-sult from episodes of mild inflammation occurring dur-ing drug therapy. However, it is important to note thatthese clinical observations do not constitute definitiveevidence of an inflammatory response in the patientswith RAN hepatotoxicity and could also be related toensuing liver damage. Results in an animal model sug-gest that concurrent inflammation increases susceptibil-ity to RAN hepatotoxicity. The discussion below willsummarize this model and what is known about theinflammatory cascade that results in liver injury.
2. Inflammation-Ranitidine Interaction. AlthoughRAN alone is not hepatotoxic in rats, modest underlyinginflammation induced by a small, nontoxic dose of LPSprecipitates IADR-like liver injury from RAN (Luyendyket al., 2003). This was not the case with FAM, whichdoes not share RAN�s propensity to cause IADRs inhuman patients. This indicated that the pharmacologi-cal target (H2 receptor) cannot be solely responsible forthe hepatotoxic inflammation-RAN interaction. Whengiven to rats 2 h after a nonhepatotoxic dose of LPS,RAN caused acute, midzonal, suppurative, necrotizinghepatitis that resembled lesions in animals treated witha hepatotoxic dose of LPS alone (Luyendyk et al., 2003),suggesting that RAN might increase hepatic sensitivityto this inflammagen. The liver injury in LPS/RAN-co-treated rats began 2 to 3 h after intravenous RAN injec-tion, was maximal at 6 h, and was sustained for at least24 h.
Hepatic inflammatory infiltrates in LPS/RAN-treatedrats comprised predominantly PMNs, suggesting thepossibility of a role for these cells in the liver injury(Luyendyk et al., 2005). In addition, the expression ofseveral genes involved in hemostasis or the response to
TABLE 2Examples of inflammatory mediators important in the pathogenesis of
LPS-induced liver injury
Mediator Reference Demonstrating Contributionto Liver Injury
TNF Hewett et al., 1993PMN chemokines Li et al., 2004PMNs Hewett et al., 1992; Ishii et al., 2002;
Gujral et al., 2004Platelets Pearson et al., 1996aThrombin Hewett and Roth, 1995; Moulin et al., 2001Kupffer cells Vollmar et al., 1996; Brown et al., 1997
270 DENG ET AL.
TA
BL
E3
Su
mm
ary
ofpu
blis
hed
case
repo
rts
ofra
nit
idin
eh
epat
oxic
ity
Bla
nk
entr
ies
indi
cate
no
repo
rtin
the
cite
dre
fere
nce
.
Ref
eren
ceP
atie
nt
Info
rmat
ion
Cli
nic
alC
hem
istr
yB
iops
y(I
nfl
amm
atio
n)
Pro
drom
alIn
flam
mat
ory
Sig
ns
Rec
hal
len
ge(R
esu
lt)
Con
curr
ent
Eth
anol
Vir
alH
epat
itis
Au
toan
tibo
dies
Oth
erU
nde
rlyi
ng
Dis
ease
Age
Gen
der
On
set
AL
TA
ST
AL
PG
GT
Bil
iru
bin
year
sU
/l
U/
lU
/l
U/
lm
g/d
l
Bar
ran
dP
iper
,19
8163
F2
wk
870
705
470
16N
oN
oH
epA
(IgG
,N
oIg
M)
Pos
itiv
esm
.m
usc
leA
b(1
:20)
Du
oden
alu
lcer
Bla
cket
al.,
1984
63M
3w
k20
715
715
216
40.
7N
oN
oN
egat
ive
Ulc
erB
lack
etal
.,19
8459
F3
wk
8965
724
2.1
No
inf,
fN
oN
egat
ive
Ulc
erB
lack
etal
.,19
8419
F4
wk
100
167
148
8.8
No
f,n
No
Neg
ativ
eD
iabe
tes,
ulc
erB
redf
eldt
,19
8442
M3
wk
196
708
2.1
No
No
Neg
ativ
eD
uod
enal
ulc
erC
ohen
and
Fab
re,
1983
(CT
)M
239
109
No
Neg
ativ
e
Col
in-J
ones
etal
.,19
8451
F2
wk
8529
03.
6Y
es(n
o)N
oN
oD
esai
nt
etal
.,19
85(T
)27
M2
wk
1100
830
205
1722
Yes
(yes
)N
oN
oN
egat
ive
Neg
ativ
eD
evu
yst
etal
.,19
9358
M2
wk
398
305
398
520
4.4
No
nN
oN
oN
egat
ive
Neg
ativ
eG
rah
amet
al.,
1985
50M
6w
k18
520
316
802.
6Y
es(n
oin
jury
)N
egat
ive
Gas
tric
ulc
erH
alpa
rin
,19
8462
F8
mo
225
427
1218
26Y
es(y
es)
m,a
p,d
No
Yes
Hep
A(I
gG,
No
IgM
)D
uod
enal
ulc
er
Hie
sse
etal
.,19
8538
M1
wk
530
100
843.
5Y
es(y
es)
Yes
(rep
eat
inju
ry)
Neg
ativ
eN
egat
ive
Kid
ney
tran
spla
nt
Hir
sch
owit
zet
al.,
1986
70M
4w
k34
913
113
0Y
es(y
es)
Neg
ativ
eD
uod
enal
ulc
erJo
nes
etal
.,19
82(C
T)
2w
k54
No
Yes
Jon
eset
al.,
1982
(CT
)4
wk
45N
oN
oJo
nes
etal
.,19
82(C
T)
4w
k19
615
9K
anta
rcek
enet
al.,
2006
39F
2da
ys11
5374
288
196
3.7
No
apN
oG
ER
DK
arac
hal
ios,
1985
65M
3w
k92
014
511
.9Y
es(y
es)
fN
oN
egat
ive
Neg
ativ
eL
auri
tsen
etal
.,19
8481
M6
wk
650
724
16Y
es(y
es)
No
No
Hep
A(I
gG,
No
IgM
)N
egat
ive
Ulc
er
Lee
etal
.,19
8660
M4
wk
287
61L
eeet
al.,
1986
34M
4w
k57
1.3
Lee
etal
.,19
8682
M4
wk
220
3L
iber
opou
los
etal
.,20
0273
F3
wk
7876
299
15.6
Yes
(yes
)N
oN
oN
oN
egat
ive
Neg
ativ
eL
upa
rin
iet
al.,
2000
(T)
46F
2739
1167
9010
73
Yes
(yes
)Y
esY
es(r
epea
tin
jury
)Y
esN
egat
ive
Mu
ltip
lesc
lero
sis
Off
itan
dS
ojka
,19
8466
M5
wk
145
128
466
535
Yes
(yes
)f,
mN
oC
hro
nic
ulc
erP
roct
or,
1984
50F
2w
k30
487
209
1.3
m,n
,ap
No
Neg
ativ
eG
ER
D,
hia
tal
her
nia
Ram
rakh
ian
iet
al.,
1998
29M
2w
k51
4310
–30
Yes
(yes
)N
oN
oN
egat
ive
Neg
ativ
eG
ER
DR
ibei
roet
al.,
2000
(fat
al)
66F
1–3
wk
1020
1000
150
588
11.4
Yes
(yes
)N
oN
egat
ive
Neg
ativ
eF
lu/d
yspe
psia
Sou
zaL
ima,
1984
77F
2w
k13
243
038
40.
3Y
es(y
es)
f,n
No
Neg
ativ
eN
egat
ive
Val
ois
etal
.,20
0351
M2–
3w
k14
5781
913
Yes
(yes
)f,
No
Yes
Neg
ativ
eN
egat
ive
Pro
tein
S-
defi
cien
cyva
nB
omm
elan
dM
eybo
om,
1992
(T)
69F
3w
k71
038
710
431
75
m,la
,ap,
nN
oN
egat
ive
Neg
ativ
e
van
Bom
mel
and
Mey
boom
,19
92(T
)43
M3
mo
354
8860
095
412
f,m
,la,a
p,n
Yes
(rep
eat
inju
ry)
Neg
ativ
e
van
Bom
mel
and
Mey
boom
,19
92(T
)49
F1
wk
930
425
322
454
6m
,la,a
pN
egat
ive
van
Bom
mel
and
Mey
boom
,19
92(T
)64
M3
wk
321
9119
735
61
m,la
Neg
ativ
e
van
Bom
mel
and
Mey
boom
,19
92(T
)61
M3
wk
267
195
222
822
2f,
m,la
,ap,
nY
es(r
epea
tin
jury
)N
egat
ive
Neg
ativ
e
van
Bom
mel
and
Mey
boom
,19
92(T
)61
M5
wk
1150
940
433
1m
,la,n
Neg
ativ
eN
egat
ive
Var
rial
eet
al.,
2004
79M
3w
k75
5589
138
22.4
Yes
(yes
)ap
No
No
Neg
ativ
eN
egat
ive
Epi
gast
ric
pain
CT
,res
ult
sw
ere
obse
rved
duri
ng
acl
inic
altr
ial;
T,o
rigi
nal
arti
cle
not
inE
ngl
ish
(wh
ere
tran
slat
ion
not
poss
ible
,en
trie
sar
ele
ftbl
ank)
;F,f
atal
,mor
tali
tyas
soci
ated
wit
hra
nit
idin
etr
eatm
ent;
wk,
wee
k(s)
;mo,
mon
th(s
);A
LT
,al
anin
eam
inot
ran
sfer
ase;
AL
P,
alka
lin
eph
osph
atas
e;A
ST
,as
part
ate
amin
otra
nsf
eras
e;G
GT
,�
-glu
tam
yltr
ansf
eras
e;f,
feve
r;m
,m
alai
se;
la,
loss
ofap
peti
te;
ap,
abdo
min
alpa
in;
n,
nau
sea/
vom
itin
g;d,
diar
rhea
;in
f,in
fect
ion
;G
ER
D,
gast
roes
oph
agea
lre
flu
xdi
seas
e.
INFLAMMATORY STRESS AND IDIOSYNCRATIC HEPATOTOXICITY 271

hypoxia was greatly enhanced in LPS/RAN-cotreatedrats. One of these genes encodes PAI-1 (Luyendyk et al.,2004). Because PAI-1 is an important negative regulatorof fibrinolysis, its enhanced gene expression suggestedthat fibrin clots might be involved in the injury. Fur-thermore, the crucial role of TNF� and other cytokinesin liver toxicity from large doses of LPS raised the pos-sibility of the importance of inflammatory cytokines inthis model. The next sections review the evidence thatsupports the roles of these inflammatory factors anddiscuss how they interact with each other to contributeto the liver injury caused by LPS/RAN cotreatment.
3. Involvement of Hemostasis, Neutrophils, andTumor Necrosis Factor �.
a. Hemostasis. In rats, a small, nonhepatotoxic doseof LPS alone caused a mild and transient increase inplasma thrombin-antithrombin concentration, indicat-ing activation of coagulation, and an increase in plasmaPAI-1 concentration, suggesting impaired fibrinolysis.RAN cotreatment augmented and prolonged the in-creases in plasma thrombin-antithrombin and PAI-1(Luyendyk et al., 2004). Activation of the coagulationsystem and the production of PAI-1 in LPS/RAN-co-treated rats was more pronounced than that in LPS/FAM-cotreated rats, which did not develop liver injury(Luyendyk et al., 2006a). Consistent with enhanced co-agulation and impaired fibrinolysis, significant sinusoi-dal fibrin deposition occurred selectively in livers ofLPS/RAN-treated rats. Cotreatment with either antico-agulant heparin, the fibrinolytic agent streptokinase, ora PAI-1 inhibitor decreased the hepatocellular injuryinduced by LPS/RAN, suggesting a role for the hemo-static system (Luyendyk et al., 2004). Hepatic hypoxiaoccurred in LPS/RAN-treated rats, and heparin reducedthe tissue hypoxia and fibrin deposition (Luyendyk etal., 2005). RAN seems to selectively augment coagula-tion and PAI-1 production triggered by LPS, and this inturn causes fibrin deposition that leads to tissue hypoxiaand hepatocyte death. SEC dysfunction probably con-tributes to coagulation system activation and PAI-1 pro-duction in LPS/RAN-treated rats (Luyendyk et al.,2004).
b. Neutrophils. In the LPS/RAN model, PMNs accu-mulate in livers early in response to LPS, and pretreat-ment with either a PMN-depleting antiserum or an an-tiserum to CD18 integrin reduced the hepatocellularinjury (Luyendyk et al., 2005; Deng et al., 2007). Be-cause the PMN antiserum selectively reduced both cir-culating and hepatic PMNs, and the CD18 antiserumreduced hepatic PMN activation, the protection affordedby these two antisera indicates a crucial role for PMNsin the pathogenesis.
The absence of liver injury after treatment with LPSalone, despite PMN accumulation, suggested that PMNsare not extravasated and activated in liver after expo-sure to the noninjurious LPS dose used in these studies.This was confirmed by the observation that LPS alone
did not cause an increase in immunostaining for hypo-chlorous acid (HOCl) adducted to liver proteins, amarker of PMN activation (Deng et al., 2007). In con-trast, LPS/RAN cotreatment did cause hepatic PMNactivation. Accordingly, PMNs require a secondary sig-nal provided by RAN treatment to be activated andcause damage. RAN itself does not activate PMNs di-rectly; in fact, it inhibits PMN activation both in vitroand in vivo (Okajima et al., 2000, 2002). This suggeststhat RAN acts indirectly through other inflammatorymediators produced during LPS exposure. These medi-ators might be PMN chemokines (i.e., MIP-2) or hemo-static factors like PAI-1, because both can promote PMNactivation (Maher et al., 1997; Lentsch et al., 1998; Li etal., 2004). In fact, PAI-1 can potentiate LPS-inducedPMN activation in vitro (Kwak et al., 2006). mRNA andserum protein concentration of both MIP-2 and PAI-1were increased to a greater extent after treatment withLPS/RAN than after LPS alone at a time before liverinjury onset (Luyendyk et al., 2006b), and this increasewas unique to RAN compared with FAM. This raises thepossibility that MIP-2 and/or PAI-1 act as signals toactivate PMNs in this model. In this regard, a PAI-1inhibitor reduced PMN activation in LPS/RAN-co-treated rats (Deng et al., 2008).
c. Tumor Necrosis Factor �. Because TNF� is a crit-ical cytokine involved in liver injury from large doses ofLPS, the effect of LPS/RAN treatment on TNF� produc-tion was examined. At the nontoxic doses used in thisanimal model, LPS rapidly induced TNF� release intothe serum; the serum TNF� concentration peaked atapproximately 2 h and rapidly decreased after that,returning toward basal levels by 8 h (Tukov et al., 2007).RAN cotreatment caused the serum TNF� concentrationincrease to last longer than in rats given LPS alone, andLPS/RAN-cotreated rats developed hepatotoxicity. Incontrast, FAM neither enhanced TNF� production norcaused liver injury when administered with LPS. Thus,the prolongation of LPS-stimulated TNF� productiondistinguished a drug that causes human IADRs fromone that does not. Some TNF�-dependent cytokines/che-mokines, such as IL-6, IL-1�, and MIP-2 also had thesame pattern of prolonged increase after RAN cotreat-ment (Tukov et al., 2007).
To explore the role of TNF� in LPS/RAN-induced hep-atotoxicity, pentoxifylline or etanercept was used to re-duce or neutralize TNF�, respectively. Pentoxifylline isa methylxanthine that inhibits the synthesis of TNF�(Dezube et al., 1993; Barton et al., 2001; Yee et al.,2003a), but it also has several other pharmacologicaleffects (Banfi et al., 2004). Etanercept is a dimeric fusionprotein that contains a soluble TNF� receptor capable ofselectively neutralizing TNF� in serum. Treatment witheither pentoxifylline or etanercept significantly reducedserum TNF� concentration and activity, respectively,and both reduced hepatocellular injury in LPS/RAN-cotreated rats (Tukov et al., 2007). These results indi-
272 DENG ET AL.
cate that TNF� is critically involved in LPS/RAN-in-duced liver injury. To investigate more specifically therole of the RAN-induced prolongation of the TNF� re-sponse, a TACE inhibitor was administered immedi-ately before RAN so that the inhibitor did not affect theinitial, LPS-induced increase in serum TNF� concentra-tion (Deng et al., 2008). This treatment regimen de-creased hepatocellular injury, suggesting that the RAN-induced prolongation of the TNF� response wasimportant for the pathogenesis.
Many of the cytokines/chemokines that are selectivelyup-regulated in LPS/RAN-treated rats (Luyendyk et al.,2006b; Tukov et al., 2007) are regulated by p38 and itsdownstream MAPK-activated protein kinase-2 (Nein-inger et al., 2002; Numahata et al., 2003; Hitti et al.,2006). Thus, it seemed possible that p38 MAPK activa-tion might be an upstream signal leading to the patho-genic cascade. Indeed, RAN, but not FAM, selectivelyaugmented p38 activation early after LPS treatment. Ap38 inhibitor given at the same time as RAN reduced thehepatotoxicity (Deng et al., 2008). This suggests thatp38 activation is critical for the liver injury after RANcotreatment of LPS-treated rats.
Despite the increase in serum TNF�, RAN did notincrease TNF� mRNA in liver after LPS treatment(Deng et al., 2008). Moreover, the reduction in serumTNF� protein concentration after p38 inhibition was notaccompanied by diminished hepatic TNF� mRNA.These results suggested the importance of post-tran-scriptional events in the up-regulation of TNF� and itsregulation by p38. Indeed, p38 and MAPK-activated pro-tein kinase-2 can regulate TNF� production in macro-phages mostly by increasing mRNA translation (Nein-inger et al., 2002; Hitti et al., 2006). As mentioned above,an increase in TNF� protein can arise from the cleavageof cell-bound pro-TNF� by TACE (Aggarwal et al., 1985;Mullberg et al., 2000); accordingly, another possibility isthat p38 activated TACE, leading to increased TNF�protein release into the circulation. LPS/RAN treatmentcaused greater hepatic TACE activation than LPS/vehi-cle treatment (Deng et al., 2008). Moreover, a p38 inhib-itor (SB 239603) reduced hepatic TACE activity afterLPS/RAN treatment to the same level as LPS/vehicletreatment. Furthermore, a TACE inhibitor (BMS-561392; Luo et al., 2007) similarly reduced serum TNF�concentration and liver injury. All of these results sug-gest that RAN prolonged TNF� production after LPStreatment through augmented p38-dependent TACEactivity.
4. Interaction of Hemostasis and Neutrophils and Tu-mor Necrosis Factor �. Several interactions among in-flammatory factors seem to be at play in the pathogen-esis of LPS/RAN-induced liver injury. Some of those forwhich evidence exists are depicted in Fig. 1. In LPS/RAN-cotreated rats, TNF� inhibition led to decreases inPMN chemokines such as MIP-2 and in plasma markersof coagulation activation and impaired fibrinolysis
(Tukov et al., 2007). This suggests that TNF� is a prox-imal inflammatory mediator relative to the hemostaticsystem or PMNs. This is supported by the observationthat inhibition of coagulation did not reduce serumTNF� concentration (unpublished results). How TNF�contributes to hemostatic system activation in thismodel remains unknown, but it might act on vascularendothelial cells or on macrophages in an autocrinefashion to induce TF expression (Schwager and Jungi,1994; Bierhaus et al., 1995; Parry and Mackman, 1995).In addition, in the presence of PMNs, TNF� exposuredamages SECs in vitro (Smedly et al., 1986; Takei et al.,1995), and such damage can activate the coagulationsystem. TNF� and IL-1 also stimulate the expressionand release of PAI-1 by endothelial cells in vitro (Schleefet al., 1988). The contribution of TNF� to TF productionand inhibition of fibrinolysis has been demonstratedin vivo in a model of lung hemorrhagic shock (Fan etal., 2000). Thus, TNF� could promote coagulation andimpair fibrinolysis by inducing TF and/or PAI-1expression.
TNF� prompts the accumulation of PMNs in tissuesby activating endothelial cells (Vassalli, 1992; Bradhamet al., 1998) and primes PMNs for activation (Schleiffen-baum and Fehr, 1990; Nagaki et al., 1991; Vassalli,1992; Kushimoto et al., 1996). In LPS/RAN-cotreatedrats, neutralization of TNF� did not affect hepatic PMNaccumulation but did reduce serum MIP-2 and PAI-1concentrations (Tukov et al., 2007). These results sug-gest that the signal for PMN extravasation and activa-tion might depend on TNF�, whereas PMN accumula-tion does not. Heparin similarly reduced serum MIP-2and PAI-1 concentrations but had no effect on hepaticPMN accumulation (Luyendyk et al., 2006a). Thus,TNF�-mediated activation of coagulation induces theexpression of MIP-2 and PAI-1, and these mediatorsmay activate PMNs accumulated in the liver.
Mechanisms by which these events lead to activationof PMNs are diverse. One possibility is that coagulationactivation causes activation of PAR-1 on KCs, endothe-lial cells, and/or hepatic stellate cells (Copple et al.,2003). PAR-1 can contribute to PMN activation but in anindirect manner, because this receptor is not present onPMNs (Copple et al., 2003). Fibrin clots can also modifythe accumulation and activation of PMNs. For example,fibrin(ogen) interacts with adhesion molecules on ratPMNs, and this contributes to the innate immune re-sponse (Flick et al., 2004a,b). Another possibility is thathypoxia caused by occlusive fibrin clots in liver sinusoidspromotes PMN activation by altering expression of che-mokines and adhesion molecules. Hypoxia can inducechemokines such as MIP-2 or adhesion molecules suchas intercellular adhesion molecule-1 and P-selectin onendothelial cells and/or hepatocytes (Shreeniwas et al.,1992; Pinsky et al., 1996; Xu et al., 1999; Laurens et al.,2005). These actions would favor the adhesion, transmi-gration, and activation of PMNs. Indeed, PMNs isolated
INFLAMMATORY STRESS AND IDIOSYNCRATIC HEPATOTOXICITY 273

from humans after acute exposure to a hypoxic atmo-sphere released more superoxide anion and elastasecompared with PMNs from people who breathed air(Tamura et al., 2002).
In addition to modulating fibrin levels, PAI-1 mighthave direct effects on PMN activation. As noted above, aPAI-1 inhibitor decreased PMN activation in LPS/RAN-cotreated rats, whereas it did not affect hepatic PMNaccumulation or serum PMN chemokine concentration(Deng et al., 2008), suggesting a direct effect of PAI-1 onPMN activation. A recent study showed that PAI-1 di-rectly potentiated LPS-induced PMN activation througha JNK-dependent pathway (Kwak et al., 2006). Theseresults suggest that RAN might induce activation ofPMNs accumulated in the liver after LPS exposure in-directly by augmenting PAI-1 production.
In the LPS/RAN model, both PMN antiserum andCD18 antiserum reduced hepatic fibrin deposition at 6 hafter RAN treatment, even though PMN depletion didnot affect fibrin deposition at an earlier time at the onsetof injury (Deng et al., 2007). PMNs express functionalTF upon stimulation and can promote thrombin activa-tion and fibrin deposition (Goel and Diamond, 2003,2004; Maugeri et al., 2006). Although either PMN deple-tion or administration of PMN protease inhibitor (eglinC), decreased fibrin deposition, neither influenced
plasma thrombin-antithrombin concentration, suggest-ing that the contribution of PMNs to fibrin is indepen-dent of coagulation cascade activation (Deng et al.,2007).
PMN lysosomal proteases cathepsin B, D, and G in-creased PAI-1 activity in the medium of human umbili-cal vein endothelial cells by cleaving PAI-1 from extra-cellular matrix (Pintucci et al., 1992, 1993; Kimura andYokoi-Hayashi, 1996). Accordingly, PMNs could contrib-ute to deposition of fibrin through inhibition of fibrino-lysis by increasing active PAI-1. Indeed, PMN depletionand eglin C each reduced active PAI-1 at 6 h after RAN(Deng et al., 2007). This suggests that PMNs contributeto fibrin deposition during injury progression by releas-ing proteases to activate PAI-1 and thereby inhibit fibri-nolysis. The lack of effect of PMNs on active PAI-1 at anearlier time (i.e., 2 h) is consistent with the observationthat these cells are not activated until 3 h after LPS/RAN treatment. In this regard, the shedding of PAI-1from endothelial matrix by PMN proteases might play amore dominant role at later times (i.e., 6 h). This couldrepresent a feed-forward mechanism to cause morePMN protease release, because PAI-1 can cause PMNactivation directly as mentioned above.
PMN depletion reduced liver hypoxia 2 h after LPS/RAN treatment (Deng et al., 2007). This early contribu-
FIG. 1. Proposed mechanism of LPS/RAN-induced liver injury. RAN augments TNF� production after LPS treatment in a post-transcriptionalmanner by enhancing p38 activation. The increase in TNF� protein occurs through the p38-dependent activation of TACE. The prolongation ofLPS-induced TNF-� production by RAN seems to be crucial for liver injury. TNF� leads to coagulation system activation and PAI-1 production, bothof which cause hepatic fibrin deposition. PAI-1 might also contribute to the activation of hepatic PMNs accumulated after LPS exposure. The hypoxiaresulting from hepatic fibrin deposition and perhaps other factors could act synergistically with toxic proteases released from activated PMNs to killhepatocytes. PMN proteases are also involved in enhancing PAI-1 production and fibrin deposition. HPC, hepatic parenchymal cell; STC, hepaticstellate cell; Trans-factor(s), transcription factor(s).
274 DENG ET AL.

tion of PMNs to hypoxia did not depend on sinusoidalfibrin deposition, because PMN depletion did not affectliver fibrin at this time. Furthermore, PMNs that haveaccumulated in liver are not activated at 2 h, suggestingthat enhancement of hypoxia by PMNs at this time doesnot require their activation and might be mediated di-rectly by plugging of sinusoids by these cells. LPS-RANcotreatment caused a greater degree of tissue hypoxiathan LPS given alone (Luyendyk et al., 2004), althoughthese two treatments had a similar effect on PMN accu-mulation (Luyendyk et al., 2005). Thus, it is possiblethat RAN cotreatment causes PMNs to adhere morefirmly to sinusoidal endothelium and/or to undergo ashape change that results in reduced sinusoidal perfu-sion and consequent hypoxia.
In addition to their role in hemostasis, activatedPMNs release toxic products such as ROS and proteasesthat can damage hepatocytes directly. As noted above, aPMN-protease inhibitor diminished LPS/RAN-inducedhepatocellular injury (Deng et al., 2007). The killing ofhepatocytes in vitro by PMN elastase is enhanced by ahypoxic environment (Luyendyk et al., 2005). The timecourse over which elastase caused hepatocyte death dur-ing hypoxia in vitro (i.e., 2 h) is consistent with the onsetof liver injury in LPS/RAN-treated rats. Taken togetherwith the evidence that fibrin deposition and hypoxia arecritical to liver injury in LPS/RAN-treated rats, it seemspossible that PMNs contribute to the pathogenesis byreleasing proteases that kill hepatocytes in an environ-ment made hypoxic by fibrin deposition or other events.
The proposed pathogenic mechanism of LPS/RAN-in-duced liver injury is summarized in Fig. 1. RAN aug-ments TNF� production after LPS treatment in a post-transcriptional manner by enhancing p38 activation,which in turn activates TACE. The prolongation of LPS-induced TNF� production by RAN seems to be crucial forthe liver injury. TNF� leads to coagulation system acti-vation and PAI-1 production, both of which cause he-patic fibrin deposition. PAI-1 might also contribute tothe activation of hepatic PMNs accumulated after LPSexposure. The hypoxia resulting from hepatic fibrin dep-osition acts synergistically with toxic proteases releasedfrom activated PMNs to kill hepatocytes. PMN proteasesare also involved in enhancing PAI-1 production andfibrin deposition.
In the LPS/RAN model, the initial molecular target ofRAN remains unknown. The lack of liver injury aftercotreatment of LPS with FAM at a dose pharmacologi-cally comparable with RAN rules out H2 receptor antag-onism as the only mechanism of RAN/LPS interaction.Because RAN, but not FAM, augmented hepatic p38activation induced by LPS, and because p38 is crucial forthe downstream cascade of TNF� production, coagula-tion activation, and PMN activation, it is possible thatactivation of the p38 pathway is the point at which RANexerts its initial effect. RAN itself did not activate p38,whereas it enhanced the p38 activation after LPS expo-
sure. Thus, RAN might perturb one or more of the sig-naling molecules in the pathway of LPS-induced p38activation.
B. Diclofenac-Induced Idiosyncratic Hepatotoxicity
NSAIDs inhibit COX-1 and/or COX-2. Many drugs inthis class cause hepatic IADRs. For example, DCLF hascaused rare but sometimes serious hepatotoxicity in hu-mans (Boelsterli, 2003b). In an analysis of 180 patientswith DCLF hepatotoxicity, the latent period to onset ofliver injury was quite variable, ranging from less thanone month to greater than a year (Banks et al., 1995).The hepatotoxicity was predominantly hepatocellular,appeared most frequently in women with osteoarthritis,and was not accompanied by signs typically associatedwith an adaptive immune reaction. Although the appar-ent incidence of severe DCLF-induced hepatic adversereactions is quite low (one to two cases per million pre-scriptions or 6–18 cases/100,000 person-years), the largenumber of patients treated with DCLF makes the abso-lute number of cases impressive (Walker, 1997). In ad-dition, severe injury leading to liver transplantation oc-curred in a large proportion of the reported cases ofDCLF-induced hepatotoxicity (Lewis, 2003). The scarce-ness of liver biopsies from patients and the diverse his-topathlogical presentations in available samples make itdifficult to draw clues about mechanisms from humanliver pathology alone (Zimmerman, 1999).
Several mechanisms of DCLF-induced hepatotoxicityhave been proposed, including metabolic and kineticfactors (Seitz et al., 1998; Aithal and Day, 2007; Daly etal., 2007), oxidative stress (Cantoni et al., 2003), andmitochondrial injury (Masubuchi et al., 2002; Lim et al.,2006; Lim et al., 2008; Siu et al., 2008). However, addi-tional studies are required to determine the relevance ofthese mechanisms in vivo. For instance, DCLF or itsmetabolites are cytotoxic to hepatocytes in vitro only atlarge concentrations that are not achieved in vivo (Bortet al., 1999; Masubuchi et al., 2002; Gomez-Lechon et al.,2003). In patients who developed hepatotoxicity afterDCLF treatment, associations have been identified withpolymorphisms in enzymes that metabolize DCLF, suchas UGT2B7 and CYP2C8, and in the DCLF glucuronidetransporter ABCC2 (Daly et al., 2007). These could leadto increased exposure to hydroxylated and/or glucu-ronidated DCLF metabolites. However, there is cur-rently no evidence to support a causal relationship be-tween these DCLF metabolites and hepatotoxicity invivo, although there are reports that DCLF acyl gluc-uronide is directly involved in small intestinal injury inrats (Seitz and Boelsterli, 1998).
There is some evidence suggesting an adaptive im-mune-mediated hypersensitivity in DCLF-induced hep-atotoxicity. For example, a 53-year-old female developedfulminant hepatic failure after inadvertent rechallengewith DCLF (Greaves et al., 2001). DCLF conjugated tomouse serum albumin or keyhole limpet hemocyanin is
INFLAMMATORY STRESS AND IDIOSYNCRATIC HEPATOTOXICITY 275

immunogenic in mice (Kretz-Rommel and Boelsterli,1995). Furthermore, T cells isolated from DCLF-keyholelimpet hemocyanin conjugate-treated mice killed hepa-tocytes previously exposed in vitro to noncytotoxic con-centrations of DCLF. However, there are no animalmodels that have reproduced hepatotoxic DCLF-inducedimmunoallergic reactions in the liver. In fact, the T cellpopliteal lymph node reaction was attenuated if animalswere treated with DCLF orally compared with injectioninto the footpad (Gutting et al., 2002, 2003). BecauseDCLF is normally given orally to human patients, thisraises a question about the likelihood that immunoaller-gic reactions contribute to DCLF-induced IADRs. DCLFautoantibodies have been found in human patients, buttheir relevance to idiosyncratic hepatotoxicity is un-known (Aithal et al., 2004). Thus, the lack of a demon-strable connection between an immunoallergic responseto DCLF and overt hepatotoxicity raises a question as towhether DCLF IADRs occur by this mechanism.
As observed for RAN, a small, nontoxic dose of LPSgiven to rats rendered a nontoxic dose of DCLF injuriousto the liver (Deng et al., 2006), suggesting inflammatorystress as a susceptibility factor for DCLF-inducedIADRs. This merits special attention because mostNSAIDs, including DCLF, have been associated in hu-mans with GI injury, and the latter can promote LPSand/or bacterial translocation from the intestine into thecirculation. In laboratory rodents a single, small dose ofDCLF (1.5 mg/kg) induced intestinal ulceration (Seitzand Boelsterli, 1998; Atchison et al., 2000). Moreover,DCLF is normally prescribed to patients with inflamma-tory conditions, in which inflammatory mediators areusually present. The role of inflammatory stress inDCLF hepatotoxicity is further suggested by the clinicalfindings that IL-4 and IL-10 polymorphisms have beenfound in human patients who developed hepatotoxicityafter DCLF treatment (Aithal et al., 2004). These poly-morphisms would lead to less IL-10 and more IL-4 pro-duction. Because IL-10 is an anti-inflammatory cytokineand IL-4 can promote PMN activation (Bober et al.,1995), these changes could result in hepatotoxic inter-action between DCLF and endotoxin or other inflamma-gens to which patients are exposed during drug therapy.
The mechanism by which LPS-DCLF interactioncauses hepatocellular injury remains unknown. Antiser-um-induced PMN depletion in LPS/DCLF-cotreated ratsprotected against liver injury, demonstrating a role forPMNs in the pathogenesis (Deng et al., 2006). PMNscause cytotoxicity through the release of ROS and othertoxic factors as described above. It is interesting in thisregard that the addition of noncytotoxic concentrationsof peroxidase/H2O2 to hepatocyte cultures markedly in-creased DCLF cytotoxicity (Tafazoli et al., 2005). In fact,several novel reactive metabolites of DCLF appearedwhen the drug was incubated with PMN-derived myelo-peroxidase (MPO) (Zuurbier et al., 1990; Miyamoto etal., 1997). Thus, PMNs that accumulate in liver after
LPS exposure might render DCLF more cytotoxic byforming MPO-derived metabolites.
Unlike RAN, DCLF causes hepatotoxicity in ratswhen given alone at larger doses than were used inLPS/DCLF cotreatment studies. Liver injury from alarge dose of DCLF was associated with a marked in-crease in bacteria in the liver, consistent with increasedintestinal permeability (Deng et al., 2006). Under theseconditions, prior treatment with nonabsorbable antibi-otics to sterilize the GI tract attenuated liver damage.These results support the hypothesis that DCLF-medi-ated GI disturbance leads to increased hepatic exposureto bacterial products that can induce inflammatorystress and increase susceptibility to hepatotoxicity. Mi-croarray analysis of gene expression changes suggestedthat DCLF might interact with bacteria/LPS throughinducing oxidative stress, apoptotic signaling, orchanges in fatty acid metabolism in liver (Deng et al.,2008). In addition, hypoxia occurred in the livers ofDCLF-treated rats and rendered hepatocytes sensitiveto DCLF-induced cytotoxicity in vitro (Deng et al., 2008).These results suggest that hypoxia might be a secondaryfactor that interacts with DCLF to kill hepatocytes.
In summary, as depicted in Fig. 2, inflammation in-duced by a small dose of LPS interacts with a nontoxicdose of DCLF to produce hepatocellular injury in ratsthrough a PMN-dependent mechanism. Furthermore,results from animal models are consistent with large,toxic doses of DCLF causing hepatotoxicity through amechanism that involves gut-derived, inflammatorystimuli that probably induce oxidative stress and apo-ptotic signaling or alter lipid metabolism.
FIG. 2. Working hypothesis for DCLF-induced hepatocellular injury.DCLF could cause hepatocellular injury through different modes depend-ing on the dose. A nontoxic dose of DCLF interacts with an independentlygenerated inflammatory stress (e.g., from LPS translocation) to producehepatocellular injury in rats through a PMN-dependent mechanism.Large, toxic doses of DCLF cause hepatotoxicity through a mechanismthat depends on gut-derived bacteria/LPS and probably do so by inducingoxidative stress and apoptotic signaling or altering lipid metabolism.Mito, mitochondrial.
276 DENG ET AL.

IV. Summary and Conclusions
There is evidence, especially in experimental animals,suggesting that inflammatory stress could be a suscep-tibility factor for IADRs. In this review, rodent models ofhuman hepatic IADRs were discussed that involve in-teraction between inflammatory stress and RAN orDCLF. It would be helpful to have more informationabout the role of inflammatory stress in IADRs fromthese two drugs in humans. In the case of RAN, epide-miological study evaluating the connection between in-flammation and liver injury has not been conducted. ForDCLF, the type of arthritis might be important in deter-mining sensitivity to DCLF-induced liver injury; a ret-rospective study showed that patients with osteoarthri-tis were at greater risk for DCLF-induced liver injurythan those with rheumatoid arthritis (Banks et al.,1995). This difference might relate to differences in pat-terns of inflammation in the two conditions. Further-more, as mentioned above, polymorphisms in genes en-coding cytokines that would favor a proinflammatorystate have been identified in patients developing DCLF-induced liver injury. However, epidemiological studiesdesigned to explore the role of inflammatory stress inhuman IADRs caused by DCLF are lacking. Thus, inhuman patients, the connection between inflammatorystress and IADRs has not been established with cer-tainty, although results in animals render this connec-tion plausible. It seems likely from the results in ani-mals that an acute inflammatory response (rather thanchronic inflammation) during drug therapy might beneeded to evoke an IADR. Because many inflammatory
responses such as cytokine production are short-livedevents, the lack of such connection in available clinicaldata might be related to the fact that clinical samplesare invariably taken after hepatotoxicity develops (i.e.,at a time when the peak of potentially pathological in-flammatory responses has passed).
The inflammatory stress-drug interaction mechanismfor IADRs is not necessarily inconsistent with otherhypotheses regarding underlying causes of these reac-tions (Fig. 3). For example, exposure to LPS can de-crease hepatic P450 expression, and could therefore re-sult in parent drug accumulation, potentially with toxicconsequences. Conversely, activated leukocytes and theproducts they release (ie., MPO) can metabolize drugs toreactive metabolites (Uetrecht, 1991). Inflammationmight also be an important factor in adaptive immune-mediated hepatotoxicity. For example, in one model ofallergic hepatitis, cotreatment with LPS markedly in-creased the hepatotoxicity (Mizoguchi et al., 1990).Thus, inflammation might act as a sufficient dangersignal to promote hepatotoxicity after drug challenge ina sensitized individual.
In describing the “multiple determinant hypothesis,”Li and colleagues suggested that the probability of anidiosyncratic reaction occurring from a drug is related tothe product of the probabilities of several factors includ-ing, but not limited to, drug exposure, environmentalfactors, genetic polymorphisms, altered metabolism, for-mation of antigens, and inadequate liver repair (Li,2002). One important environmental factor might beexposure to inflammagens. However, one mechanism is
FIG. 3. Integration of the “inflammation hypothesis” with other hypotheses for etiology of idiosyncratic hepatotoxicity. Inflammation can influencea drug’s propensity to cause idiosyncratic toxicity by several modes. For example, inflammatory cytokines can increase the concentration of a drug byinhibiting P450 expression. Activated leukocytes have also been implicated in metabolism of drugs to reactive species. Modification of proteins by thesemetabolites could result in hapten formation and, upon rechallenge, precipitation of an adaptive immune response, which during a concurrentinflammatory stress (i.e., as a danger signal) might cause hepatotoxicity. Finally, the ability of a drug to alter hepatocellular homeostasis might renderthe liver sensitive to injury from normally noninjurious activation of inflammatory mediators.
INFLAMMATORY STRESS AND IDIOSYNCRATIC HEPATOTOXICITY 277

unlikely to account for all idiosyncratic reactions, andnumerous factors should be considered in future devel-opment of animal models.
It has been suggested that many drugs might causestress to the liver at therapeutic doses, often resulting inmild injury (e.g., modest serum alanine aminotransfer-ase increases) to which most patients adapt during con-tinued therapy. It is hypothesized that failure to adaptin some patients could permit progression to liver dam-age and that this could be a mode by which IADRs occur(Watkins, 2005). If so, it could be that inflammatorystress is one of the factors that prevents adaptation andenables a liver homeostatically altered by drug exposureto progress to frank injury (Fig. 3).
One reason for continued occurrence of hepatic IADRsis that drugs with the propensity to cause these reac-tions are not identified under current preclinical safetytesting paradigms. It is possible that this inflammation-drug interaction model could provide a basis for preclin-ical drug safety screening models to identify new drugcandidates that might have this propensity. The concor-dance between IADRs in humans and inflammation-drug interaction in animals with certain known drugs(Table 1) largely supports this idea. This list is smallrelative to the number of drugs responsible for humanhepatic IADRs, however, and the hypothesis requiresvalidation with more drugs. Furthermore, the animalmodel is cumbersome as a screening tool. Nonetheless,the information gleaned regarding interaction of drugsand inflammatory mediators that result in hepatotoxic-ity in these animal models could be valuable for devel-opment of more streamlined, predictive models.
Another utility of these models is in the identificationof early biomarkers that portend serious reactions inhuman patients. In the LPS/RAN rat model, severalinflammatory mediators (e.g., TNF�, PAI-1, thrombin)are selectively up-regulated before liver injury, andthese proved crucial for the pathogenesis. These or otherinflammatory mediators might serve as early bio-markers for IADRs resulting from inflammation-druginteraction.
Acknowledgments.This work was supported by the National Insti-tutes of Health National Institute of Environmental Health Sciences[Grant ES004139]; National Institutes of Health National Instituteof General Medicine [Grant GM075865]; and the National Institutesof Health National Institute of Diabetes and Digestive and KidneyDiseases [Grant DK061315].
REFERENCES
Aggarwal BB, Kohr WJ, Hass PE, Moffat B, Spencer SA, Henzel WJ, Bringman TS,Nedwin GE, Goeddel DV, and Harkins RN (1985) Human tumor necrosis factor.Production, purification, and characterization. J Biol Chem 260:2345–2354.
Aithal GP and Day CP (2007) Nonsteroidal anti-inflammatory drug-induced hepa-totoxicity. Clin Liver Dis 11:563–575, vi–vii.
Aithal GP, Ramsay L, Daly AK, Sonchit N, Leathart JB, Alexander G, Kenna JG,Caldwell J, and Day CP (2004) Hepatic adducts, circulating antibodies, and cyto-kine polymorphisms in patients with diclofenac hepatotoxicity. Hepatology 39:1430–1440.
Amar PJ and Schiff ER (2007) Acetaminophen safety and hepatotoxicity—where dowe go from here? Expert Opin Drug Saf 6:341–355.
Andrade RJ, Lucena MI, Fernandez MC, Pelaez G, Pachkoria K, García-Ruiz E,García-Munoz B, Gonzalez-Grande R, Pizarro A, Duran JA, et al. (2005) Drug-
induced liver injury: an analysis of 461 incidences submitted to the Spanishregistry over a 10-year period. Gastroenterology 129:512–521.
Andrade RJ, Lucena MI, Kaplowitz N, García-Munoz B, Borraz Y, Pachkoria K,García-Cortes M, Fernandez MC, Pelaez G, Rodrigo L, et al. (2006) Outcome ofacute idiosyncratic drug-induced liver injury: long-term follow-up in a hepatotox-icity registry. Hepatology 44:1581–1588.
Arioglu E, Duncan-Morin J, Sebring N, Rother KI, Gottlieb N, Lieberman J, HerionD, Kleiner DE, Reynolds J, Premkumar A, et al. (2000) Efficacy and safety oftroglitazone in the treatment of lipodystrophy syndromes. Ann Intern Med 133:263–274.
Arteel GE (2008) New role of plasminogen activator inhibitor-1 in alcohol-inducedliver injury. J Gastroenterol Hepatol 23 (Suppl 1):S54–S59.
Atchison CR, West AB, Balakumaran A, Hargus SJ, Pohl LR, Daiker DH, AronsonJF, Hoffmann WE, Shipp BK, and Treinen-Moslen M (2000) Drug enterocyteadducts: possible causal factor for diclofenac enteropathy in rats. Gastroenterology119:1537–1547.
Bagheri H, Michel F, Lapeyre-Mestre M, Lagier E, Cambus JP, Valdiguie P, andMontastruc JL (2000) Detection and incidence of drug-induced liver injuries inhospital: a prospective analysis from laboratory signals. Br J Clin Pharmacol50:479–484.
Banfi C, Sironi L, De Simoni G, Gelosa P, Barcella S, Perego C, Gianazza E, GuerriniU, Tremoli E, and Mussoni L (2004) Pentoxifylline prevents spontaneous brainischemia in stroke-prone rats. J Pharmacol Exp Ther 310:890–895.
Banks AT, Zimmerman HJ, Ishak KG, and Harter JG (1995) Diclofenac-associatedhepatotoxicity: analysis of 180 cases reported to the Food and Drug Administrationas adverse reactions. Hepatology 22:820–827.
Barr GD and Piper DW (1981) Possible ranitidine hepatitis. Med J Aust 2:421.Barton CC, Barton EX, Ganey PE, Kunkel SL, and Roth RA (2001) Bacterial
lipopolysaccharide enhances aflatoxin B1 hepatotoxicity in rats by a mechanismthat depends on tumor necrosis factor �. Hepatology 33:66–73.
Barton CC, Ganey PE, and Roth RA (2000) Lipopolysaccharide augments aflatoxinB(1)-induced liver injury through neutrophil-dependent and -independent mech-anisms. Toxicol Sci 58:208–215.
Beier JI, Luyendyk JP, Guo L, von Montfort C, Staunton DE, and Arteel GE (2009)Fibrin accumulation plays a critical role in the sensitization to lipopolysaccharide-induced liver injury caused by ethanol in mice. Hepatology 49:1545–1553.
Bergheim I, Guo L, Davis MA, Lambert JC, Beier JI, Duveau I, Luyendyk JP, RothRA, and Arteel GE (2006) Metformin prevents alcohol-induced liver injury in themouse: critical role of plasminogen activator inhibitor-1. Gastroenterology 130:2099–2112.
Bierhaus A, Zhang Y, Deng Y, Mackman N, Quehenberger P, Haase M, Luther T,Muller M, Bohrer H, and Greten J (1995) Mechanism of the tumor necrosis factor�-mediated induction of endothelial tissue factor. J Biol Chem 270:26419–26432.
Black M, Scott WE Jr, and Kanter R (1984) Possible ranitidine hepatotoxicity. AnnIntern Med 101:208–210.
Bober LA, Waters TA, Pugliese-Sivo CC, Sullivan LM, Narula SK, and Grace MJ(1995) IL-4 induces neutrophilic maturation of HL-60 cells and activation ofhuman peripheral blood neutrophils. Clin Exp Immunol 99:129–136.
Boelsterli UA (2003a) Disease-related determinants of susceptibility to drug-inducedidiosyncratic hepatotoxicity. Curr Opin Drug Discov Devel 6:81–91.
Boelsterli UA (2003b) Diclofenac-induced liver injury: a paradigm of idiosyncraticdrug toxicity. Toxicol Appl Pharmacol 192:307–322.
Boelsterli UA and Hsiao CJ (2008) The heterozygous Sod2(�/�) mouse: modeling themitochondrial role in drug toxicity. Drug Discov Today 13:982–988.
Bonkovsky HL, Azar R, Bird S, Szabo G, and Banner B (2002) Severe cholestatichepatitis caused by thiazolidinediones: risks associated with substituting rosigli-tazone for troglitazone. Dig Dis Sci 47:1632–1637.
Bort R, Ponsoda X, Jover R, Gomez-Lechon MJ, and Castell JV (1999) Diclofenactoxicity to hepatocytes: a role for drug metabolism in cell toxicity. J Pharmacol ExpTher 288:65–72.
Bradham CA, Plumpe J, Manns MP, Brenner DA, and Trautwein C (1998) Mecha-nisms of hepatic toxicity. I. TNF-induced liver injury. Am J Physiol 275:G387–G392.
Bredfeldt JE and von Huene C (1984) Ranitidine, acetaminophen, and hepatotoxic-ity. Ann Intern Med 101:719.
Brown AP, Harkema JR, Schultze AE, Roth RA, and Ganey PE (1997) Gadoliniumchloride pretreatment protects against hepatic injury but predisposes the lungs toalveolitis after lipopolysaccharide administration. Shock 7:186–192.
Buchweitz JP, Ganey PE, Bursian SJ, and Roth RA (2002) Underlying endotoxemiaaugments toxic responses to chlorpromazine: is there a relationship to drug idio-syncrasy? J Pharmacol Exp Ther 300:460–467.
Butcher EC (1991) Leukocyte-endothelial cell recognition: three (or more) steps tospecificity and diversity. Cell 67:1033–1036.
Cantoni L, Valaperta R, Ponsoda X, Castell JV, Barelli D, Rizzardini M, MangoliniA, Hauri L, and Villa P (2003) Induction of hepatic heme oxygenase-1 by diclofenacin rodents: role of oxidative stress and cytochrome P-450 activity. J Hepatol38:776–783.
Carey PF, Martin LE, and Owen PE (1981) Determination of ranitidine and itsmetabolites in human urine by reversed-phase ion-pair high-performance liquidchromatography. J Chromatogr 225:161–168.
Carini R, de Cesaris MG, Bellomo G, and Albano E (1997) Role of Na�/Ca2�exchanger in preventing Na� overload and hepatocyte injury: opposite effects ofextracellular and intracellular Ca2� chelation. Biochem Biophys Res Commun232:107–110.
Carini R, De Cesaris MG, Splendore R, Bagnati M, and Albano E (2000) Ischemicpreconditioning reduces Na(�) accumulation and cell killing in isolated rat hepa-tocytes exposed to hypoxia. Hepatology 31:166–172.
Chalasani N, Fontana RJ, Bonkovsky HL, Watkins PB, Davern T, Serrano J, YangH, Rochon J, and Drug Induced Liver Injury Network (DILIN) (2008) Causes,clinical features, and outcomes from a prospective study of drug-induced liverinjury in the United States. Gastroenterology 135:1924–1934.
278 DENG ET AL.

Cheng L, You Q, Yin H, Holt M, Franklin C, and Ju C (2009) Effect of polyI:Ccotreatment on halothane-induced liver injury in mice. Hepatology 49:215–226.
Chojkier M (2005) Troglitazone and liver injury: in search of answers. Hepatology41:237–246.
Chung WG, Park CS, Roh HK, Lee WK, and Cha YN (2000) Oxidation of ranitidineby isozymes of flavin-containing monooxygenase and cytochrome P450. JpnJ Pharmacol 84:213–220.
Cohen A and Fabre L (1983) Tolerance to repeated intravenous doses of ranitidineHCl and cimetidine HCl in normal volunteers. Curr Ther Res 43:475–482.
Colin-Jones DG, Ireland A, Gear P, Golding PL, Ramage JK, Williams JG, LeicesterRJ, Smith CL, Ross G, and Bamforth J (1984) Reducing overnight secretion of acidto heal duodenal ulcers. Comparison of standard divided dose of ranitidine with asingle dose administered at night. Am J Med 77:116–122.
Copple BL, Moulin F, Hanumegowda UM, Ganey PE, and Roth RA (2003) Thrombinand protease-activated receptor-1 agonists promote lipopolysaccharide-inducedhepatocellular injury in perfused livers. J Pharmacol Exp Ther 305:417–425.
Cottam DR, Mattar SG, Barinas-Mitchell E, Eid G, Kuller L, Kelley DE, and SchauerPR (2004) The chronic inflammatory hypothesis for the morbidity associated withmorbid obesity: implications and effects of weight loss. Obes Surg 14:589–600.
Daly AK, Aithal GP, Leathart JB, Swainsbury RA, Dang TS, and Day CP (2007)Genetic susceptibility to diclofenac-induced hepatotoxicity: contribution ofUGT2B7, CYP2C8, and ABCC2 genotypes. Gastroenterology 132:272–281.
de la Iglesia FA, Haskins JR, and Feuer G (2003) Hepatotoxicity of cardiovascularand antidiabetic drugs, in Drug-Induced Liver Disease (Kaplowitz N, DeLeve LDeds) pp 549–552, Marcel Dekker, New York.
De Marzo AM, Platz EA, Sutcliffe S, Xu J, Gronberg H, Drake CG, Nakai Y, IsaacsWB, and Nelson WG (2007) Inflammation in prostate carcinogenesis. Nat RevCancer 7:256–269.
Deng X, Liguori MJ, Sparkenbaugh EM, Waring JF, Blomme EA, Ganey PE, andRoth RA (2008) Gene expression profiles in livers from diclofenac-treated ratsreveal intestinal bacteria-dependent and -independent pathways associated withliver injury. J Pharmacol Exp Ther 327:634–644.
Deng X, Luyendyk JP, Zou W, Lu J, Malle E, Ganey PE, and Roth RA (2007)Neutrophil interaction with the hemostatic system contributes to liver injury inrats cotreated with lipopolysaccharide and ranitidine. J Pharmacol Exp Ther322:852–861.
Deng X, Stachlewitz RF, Liguori MJ, Blomme EA, Waring JF, Luyendyk JP, MaddoxJF, Ganey PE, and Roth RA (2006) Modest inflammation enhances diclofenachepatotoxicity in rats: role of neutrophils and bacterial translocation. J PharmacolExp Ther 319:1191–1199.
Desaint B, Alperine M, Legendre C, Florent C, and Levy VG (1985) [HepatitisCaused by Ranitidine]. Gastroenterol Clin Biol 9:746–747.
Devuyst O, Lefebvre C, Geubel A, and Coche E (1993) Acute cholestatic hepatitiswith rash and hypereosinophilia associated with ranitidine treatment. Acta ClinBelg 48:109–114.
Dezube BJ, Pardee AB, Chapman B, Beckett LA, Korvick JA, Novick WJ, Chiurco J,Kasdan P, Ahlers CM, and Ecto LT (1993) Pentoxifylline decreases tumor necrosisfactor expression and serum triglycerides in people with AIDS. NIAID AIDSClinical Trials Group. J Acquir Immune Defic Syndr 6:787–794.
Dieckhaus CM, Thompson CD, Roller SG, and Macdonald TL (2002) Mechanisms ofidiosyncratic drug reactions: the case of felbamate. Chem Biol Interact 142:99–117.
Dugan CM, Roth RA, and Ganey PE (2008) Determinants of sensitivity to halothane-induced hepatotoxicity in mice (Abstract). Toxicol Sci 102 (Suppl):174.
Echtenacher B, Falk W, Mannel DN, and Krammer PH (1990) Requirement ofendogenous tumor necrosis factor/cachectin for recovery from experimental peri-tonitis. J Immunol 145:3762–3766.
Echtenacher B, Hultner L, and Mannel DN (1995) Cellular and molecular mecha-nisms of TNF protection in septic peritonitis. J Inflamm 47:85–89.
Echtenacher B and Mannel DN (2002) Requirement of TNF and TNF receptor type2 for LPS-induced protection from lethal septic peritonitis. J Endotoxin Res 8:365–369.
Echtenacher B, Urbaschek R, Weigl K, Freudenberg MA, and Mannel DN (2003)Treatment of experimental sepsis-induced immunoparalysis with TNF. Immuno-biology 208:381–389.
Eichelbaum M and Burk O (2001) CYP3A genetics in drug metabolism. Nat Med7:285–287.
Fan J, Kapus A, Li YH, Rizoli S, Marshall JC, and Rotstein OD (2000) Priming forenhanced alveolar fibrin deposition after hemorrhagic shock: role of tumor necrosisfactor. Am J Respir Cell Mol Biol 22:412–421.
Fink T, Kazlauskas A, Poellinger L, Ebbesen P, and Zachar V (2002) Identificationof a tightly regulated hypoxia-response element in the promoter of human plas-minogen activator inhibitor-1. Blood 99:2077–2083.
Flick MJ, Du X, and Degen JL (2004a) Fibrin(ogen)-� M � 2 interactions regulateleukocyte function and innate immunity in vivo. Exp Biol Med (Maywood) 229:1105–1110.
Flick MJ, Du X, Witte DP, Jirouskova M, Soloviev DA, Busuttil SJ, Plow EF, andDegen JL (2004b) Leukocyte engagement of fibrin(ogen) via the integrin receptoralphaMbeta2/Mac-1 is critical for host inflammatory response in vivo. J Clin Invest113:1596–1606.
Ganey PE, Bailie MB, VanCise S, Colligan ME, Madhukar BV, Robinson JP, andRoth RA (1994) Activated neutrophils from rat injured isolated hepatocytes. LabInvest 70:53–60.
Ganey PE, Barton YW, Kinser S, Sneed RA, Barton CC, and Roth RA (2001)Involvement of cyclooxygenase-2 in the potentiation of allyl alcohol-induced liverinjury by bacterial lipopolysaccharide. Toxicol Appl Pharmacol 174:113–121.
Ganey PE, Luyendyk JP, Maddox JF, and Roth RA (2004) Adverse hepatic drugreactions: inflammatory episodes as consequence and contributor. Chem Biol In-teract 150:35–51.
Ganey PE and Roth RA (2001) Concurrent inflammation as a determinant of sus-ceptibility to toxicity from xenobiotic agents. Toxicology 169:195–208.
Gardiner KR, Halliday MI, Barclay GR, Milne L, Brown D, Stephens S, Maxwell RJ,and Rowlands BJ (1995) Significance of systemic endotoxaemia in inflammatorybowel disease. Gut 36:897–901.
Gearing AJ, Beckett P, Christodoulou M, Churchill M, Clements J, Davidson AH,Drummond AH, Galloway WA, Gilbert R, and Gordon JL (1994) Processing oftumour necrosis factor-� precursor by metalloproteinases. Nature 370:555–557.
Goel MS and Diamond SL (2003) Neutrophil cathepsin G promotes prothrombinaseand fibrin formation under flow conditions by activating fibrinogen-adherentplatelets. J Biol Chem 278:9458–9463.
Goel MS and Diamond SL (2004) Factor VIIa-mediated tenase function on activatedplatelets under flow. J Thromb Haemost 2:1402–1410.
Gomez-Lechon MJ, Ponsoda X, O’Connor E, Donato T, Jover R, and Castell JV (2003)Diclofenac induces apoptosis in hepatocytes. Toxicol In Vitro 17:675–680.
Graham DJ, Green L, Senior JR, and Nourjah P (2003) Troglitazone-induced liverfailure: a case study. Am J Med 114:299–306.
Graham DY, Opekun AR, Smith JL, and Schwartz JT (1985) Ranitidine and hepa-totoxicity. Ann Intern Med 102:416.
Greaves RR, Agarwal A, Patch D, Davies SE, Sherman D, Reynolds N, Rolles K,Davidson BR, and Burroughs AK (2001) Inadvertent diclofenac rechallenge fromgeneric and non-generic prescribing, leading to liver transplantation for fulminantliver failure. Eur J Gastroenterol Hepatol 13:71–73.
Guha M and Mackman N (2001) LPS induction of gene expression in human mono-cytes. Cell Signal 13:85–94.
Gujral JS, Hinson JA, Farhood A, and Jaeschke H (2004) NADPH oxidase-derivedoxidant stress is critical for neutrophil cytotoxicity during endotoxemia. Am JPhysiol Gastrointest Liver Physiol 287:G243–G252.
Gutting BW, Bouzahzah F, Kong PL, Updyke LW, Amacher DE, and Craft J (2003)Oxazolone and diclofenac-induced popliteal lymph node assay reactions are atten-uated in mice orally pretreated with the respective compound: potential role forthe induction of regulatory mechanisms following enteric administration. ToxicolAppl Pharmacol 189:120–133.
Gutting BW, Updyke LW, and Amacher DE (2002) Diclofenac activates T cells in thedirect popliteal lymph node assay and selectively induces IgG(1) and IgE againstco-injected TNP-OVA. Toxicol Lett 131:167–180.
Halparin LS (1984) Adverse effects of ranitidine therapy. Can Med Assoc J 130:668–672.
Harbrecht BG, Billiar TR, Curran RD, Stadler J, and Simmons RL (1993) Hepatocyteinjury by activated neutrophils in vitro is mediated by proteases. Ann Surg218:120–128.
Hasegawa T, Malle E, Farhood A, and Jaeschke H (2005) Generation of hypochlorite-modified proteins by neutrophils during ischemia-reperfusion injury in rat liver:attenuation by ischemic preconditioning. Am J Physiol Gastrointest Liver Physiol289:G760–G767.
He K, Talaat RE, Pool WF, Reily MD, Reed JE, Bridges AJ, and Woolf TF (2004)Metabolic activation of troglitazone: identification of a reactive metabolite andmechanisms involved. Drug Metab Dispos 32:639–646.
Hehlgans T and Pfeffer K (2005) The intriguing biology of the tumour necrosisfactor/tumour necrosis factor receptor superfamily: players, rules and the games.Immunology 115:1–20.
Hekman CM and Loskutoff DJ (1985) Endothelial cells produce a latent inhibitor ofplasminogen activators that can be activated by denaturants. J Biol Chem 260:11581–11587.
Hewett JA and Roth RA (1993) Hepatic and extrahepatic pathobiology of bacteriallipopolysaccharides. Pharmacol Rev 45:382–411.
Hewett JA and Roth RA (1995) The coagulation system, but not circulating fibrin-ogen, contributes to liver injury in rats exposed to lipopolysaccharide from gram-negative bacteria. J Pharmacol Exp Ther 272:53–62.
Hewett JA, Schultze AE, VanCise S, and Roth RA (1992) Neutrophil depletionprotects against liver injury from bacterial endotoxin. Lab Invest 66:347–361.
Hiesse C, Cantarovich M, Santelli C, Francais P, Charpentier B, Fries D, and BuffetC (1985) Ranitidine hepatotoxicity in renal transplant patient. Lancet 1:1280.
Hirschowitz BI, Berenson MM, Berkowitz JM, Bright-Asare P, DeLuca VA Jr,Eshelman FN, Font RG, Griffin JW Jr, Kozarek RA, and McCray RS (1986) Amulticenter study of ranitidine treatment of duodenal ulcers in the United States.J Clin Gastroenterol 8:359–366.
Hitti E, Iakovleva T, Brook M, Deppenmeier S, Gruber AD, Radzioch D, Clark AR,Blackshear PJ, Kotlyarov A, and Gaestel M (2006) Mitogen-activated proteinkinase-activated protein kinase 2 regulates tumor necrosis factor mRNA stabilityand translation mainly by altering tristetraprolin expression, stability, and bind-ing to adenine/uridine-rich element. Mol Cell Biol 26:2399–2407.
Ho JS, Buchweitz JP, Roth RA, and Ganey PE (1996) Identification of factors fromrat neutrophils responsible for cytotoxicity to isolated hepatocytes. J Leukoc Biol59:716–724.
Hoekstra T, Geleijnse JM, Schouten EG, and Kluft C (2004) Plasminogen activatorinhibitor-type 1: its plasma determinants and relation with cardiovascular risk.Thromb Haemost 91:861–872.
Honma W, Shimada M, Sasano H, Ozawa S, Miyata M, Nagata K, Ikeda T, andYamazoe Y (2002) Phenol sulfotransferase, ST1A3, as the main enzyme catalyzingsulfation of troglitazone in human liver. Drug Metab Dispos 30:944–949.
Hou B, Eren M, Painter CA, Covington JW, Dixon JD, Schoenhard JA, and VaughanDE (2004) Tumor necrosis factor � activates the human plasminogen activatorinhibitor-1 gene through a distal nuclear factor �B site. J Biol Chem 279:18127–18136.
Huang SM, Tsai TR, Yeh PH, and Tsai TH (2005) Measurement of unbound raniti-dine in blood and bile of anesthetized rats using microdialysis coupled to liquidchromatography and its pharmacokinetic application. J Chromatogr A 1073:297–302.
Hussaini SH and Farrington EA (2007) Idiosyncratic drug-induced liver injury: anoverview. Expert Opin Drug Saf 6:673–684.
Hustert E, Haberl M, Burk O, Wolbold R, He YQ, Klein K, Nuessler AC, Neuhaus P,
INFLAMMATORY STRESS AND IDIOSYNCRATIC HEPATOTOXICITY 279

Klattig J, Eiselt R, et al. (2001) The genetic determinants of the CYP3A5 poly-morphism. Pharmacogenetics 11:773–779.
Jaeschke H, Farhood A, and Smith CW (1990) Neutrophils contribute to ischemia/reperfusion injury in rat liver in vivo. FASEB J 4:3355–3359.
Jaeschke H, Farhood A, and Smith CW (1991) Neutrophil-induced liver cell injury inendotoxin shock is a CD11b/CD18-dependent mechanism. Am J Physiol 261:G1051–G1056.
Jaeschke H, Gores GJ, Cederbaum AI, Hinson JA, Pessayre D, and Lemasters JJ(2002) Mechanisms of hepatotoxicity. Toxicol Sci 65:166–176.
Jaeschke H, Ho YS, Fisher MA, Lawson JA, and Farhood A (1999) Glutathioneperoxidase-deficient mice are more susceptible to neutrophil-mediated hepaticparenchymal cell injury during endotoxemia: importance of an intracellular oxi-dant stress. Hepatology 29:443–450.
Jaeschke H, Smith CW, Clemens MG, Ganey PE, and Roth RA (1996) Mechanismsof inflammatory liver injury: adhesion molecules and cytotoxicity of neutrophils.Toxicol Appl Pharmacol 139:213–226.
Jones DB, Hanson RG, Mihaly GW, Johnson RD, Louis WJ, Yeomans ND, andSmallwood RA (1982) Double-blind controlled trial of ranitidine versus cimetidinein the treatment of duodenal ulceration. Aust N Z J Med 12:547–549.
Ju C and Uetrecht JP (2002) Mechanism of idiosyncratic drug reactions: reactivemetabolite formation, protein binding and the regulation of the immune system.Curr Drug Metab 3:367–377.
Kantarceken B, Cetinkaya A, Bulbuloglu E, Yerhan H, and Ucar MA (2006) Severeliver enzyme elevation due to single-dose ranitidine in a pregnant woman. Turk JGastroenterol 17:242–243.
Kaplowitz N (2001) Drug-induced liver disorders: implications for drug developmentand regulation. Drug Saf 24:483–490.
Kaplowitz N (2005) Idiosyncratic drug hepatotoxicity. Nat Rev Drug Discov 4:489–499.
Karachalios GN (1985) Ranitidine and hepatitis. Ann Intern Med 103:634–635.Kawabata K, Hagio T, and Matsuoka S (2002) The role of neutrophil elastase in
acute lung injury. Eur J Pharmacol 451:1–10.Kawai K, Kawasaki-Tokui Y, Odaka T, Tsuruta F, Kazui M, Iwabuchi H, Nakamura
T, Kinoshita T, Ikeda T, Yoshioka T, et al. (1997) Disposition and metabolism ofthe new oral antidiabetic drug troglitazone in rats, mice and dogs. Arzneimittel-forschung 47:356–368.
Kim JW, Jeon WK, and Kim EJ (2005) Combined effects of bovine colostrum andglutamine in diclofenac-induced bacterial translocation in rat. Clin Nutr 24:785–793.
Kimura Y and Yokoi-Hayashi K (1996) Polymorphonuclear leukocyte lysosomalproteases, cathepsins B and D affect the fibrinolytic system in human umbilicalvein endothelial cells. Biochim Biophys Acta 1310:1–4.
Kinser S, Copple BL, Roth RA, and Ganey PE (2002) Enhancement of allyl alcoholhepatotoxicity by endotoxin requires extrahepatic factors. Toxicol Sci 69:470–481.
Kinser S, Sneed R, Roth R, and Ganey P (2004) Neutrophils contribute to endotoxinenhancement of allyl alcohol hepatotoxicity. J Toxicol Environ Health A 67:911–928.
Kobayashi Y (2008) The role of chemokines in neutrophil biology. Front Biosci13:2400–2407.
Kohlroser J, Mathai J, Reichheld J, Banner BF, and Bonkovsky HL (2000) Hepato-toxicity due to troglitazone: report of two cases and review of adverse eventsreported to the United States Food and Drug Administration. Am J Gastroenterol95:272–276.
Kopydlowski KM, Salkowski CA, Cody MJ, van Rooijen N, Major J, Hamilton TA,and Vogel SN (1999) Regulation of macrophage chemokine expression by lipopoly-saccharide in vitro and in vivo. J Immunol 163:1537–1544.
Kostrubsky VE, Sinclair JF, Ramachandran V, Venkataramanan R, Wen YH, KindtE, Galchev V, Rose K, Sinz M, and Strom SC (2000) The role of conjugation inhepatotoxicity of troglitazone in human and porcine hepatocyte cultures. DrugMetab Dispos 28:1192–1197.
Kretz-Rommel A and Boelsterli UA (1995) Cytotoxic activity of T cells and non-Tcells from diclofenac-immunized mice against cultured syngeneic hepatocytes ex-posed to diclofenac. Hepatology 22:213–222.
Kuehl P, Zhang J, Lin Y, Lamba J, Assem M, Schuetz J, Watkins PB, Daly A,Wrighton SA, Hall SD, et al. (2001) Sequence diversity in CYP3A promoters andcharacterization of the genetic basis of polymorphic CYP3A5 expression. Nat Genet27:383–391.
Kushimoto S, Okajima K, Uchiba M, Murakami K, Harada N, Okabe H, and Takat-suki K (1996) Role of granulocyte elastase in ischemia/reperfusion injury of ratliver. Crit Care Med 24:1908–1912.
Kusters S, Tiegs G, Alexopoulou L, Pasparakis M, Douni E, Kunstle G, BluethmannH, Wendel A, Pfizenmaier K, Kollias G, et al. (1997) In vivo evidence for afunctional role of both tumor necrosis factor (TNF) receptors and transmembraneTNF in experimental hepatitis. Eur J Immunol 27:2870–2875.
Kwak SH, Wang XQ, He Q, Fang WF, Mitra S, Bdeir K, Ploplis VA, Xu Z, Idell S,Cines D, et al. (2006) Plasminogen activator inhibitor-1 potentiates LPS-inducedneutrophil activation through a JNK-mediated pathway. Thromb Haemost 95:829–835.
Larson AM, Polson J, Fontana RJ, Davern TJ, Lalani E, Hynan LS, Reisch JS,Schiødt FV, Ostapowicz G, Shakil AO, et al. (2005) Acetaminophen-induced acuteliver failure: results of a United States multicenter, prospective study. Hepatology42:1364–1372.
Laurens M, Defamie V, Scozzari G, Schmid-Alliana A, Gugenheim J, and CrenesseD (2005) Hypoxia-reoxygenation-induced chemokine transcription is not pre-vented by preconditioning or intermittent hypoxia, in mice hepatocytes. TransplInt 18:444–452.
Lauritsen K, Havelund T, and Rask-Madsen J (1984) Ranitidine and hepatotoxicity.Lancet 2:1471.
Lazarou J, Pomeranz BH, and Corey PN (1998) Incidence of adverse drug reactionsin hospitalized patients: a meta-analysis of prospective studies. JAMA 279:1200–1205.
Lee FI, Reed PI, Crowe JP, McIsaac RL, and Wood JR (1986) Acute treatment ofduodenal ulcer: a multicentre study to compare ranitidine 150 mg twice daily withranitidine 300 mg once at night. Gut 27:1091–1095.
Lentsch AB, Yoshidome H, Cheadle WG, Miller FN, and Edwards MJ (1998) Che-mokine involvement in hepatic ischemia/reperfusion injury in mice: roles formacrophage inflammatory protein-2 and KC. Hepatology 27:1172–1177.
Lepper PM, Held TK, Schneider EM, Bolke E, Gerlach H, and Trautmann M (2002)Clinical implications of antibiotic-induced endotoxin release in septic shock. In-tensive Care Med 28:824–833.
Levi M (2005) Disseminated intravascular coagulation: what’s new? Crit Care Clin21:449–467.
Levi M, Keller TT, van Gorp E, and ten Cate H (2003) Infection and inflammationand the coagulation system. Cardiovasc Res 60:26–39.
Lewis JH (2003) Nonsteroidal anti-inflammatory drugs: pathology and clinical pre-sentation of hepatotoxicity, in Drug-Induced Liver Disease (Kaplowitz N, DeLeveLD eds) pp 377–404, Marcel Dekker, New York.
Ley K, Laudanna C, Cybulsky MI, and Nourshargh S (2007) Getting to the site ofinflammation: the leukocyte adhesion cascade updated. Nat Rev Immunol 7:678–689.
Li AP (2002) A review of the common properties of drugs with idiosyncratic hepato-toxicity and the “multiple determinant hypothesis” for the manifestation of idio-syncratic drug toxicity. Chem Biol Interact 142:7–23.
Li X, Klintman D, Liu Q, Sato T, Jeppsson B, and Thorlacius H (2004) Critical roleof CXC chemokines in endotoxemic liver injury in mice. J Leukoc Biol 75:443–452.
Liberopoulos EN, Nonni AB, Tsianos EV, and Elisaf MS (2002) Possible ranitidine-induced cholestatic jaundice. Ann Pharmacother 36:172.
Lim MS, Lim PL, Gupta R, and Boelsterli UA (2006) Critical role of free cytosoliccalcium, but not uncoupling, in mitochondrial permeability transition and celldeath induced by diclofenac oxidative metabolites in immortalized human hepa-tocytes. Toxicol Appl Pharmacol 217:322–331.
Lim PL, Liu J, Go ML, and Boelsterli UA (2008) The mitochondrial superoxide/thioredoxin-2/Ask1 signaling pathway is critically involved in troglitazone-inducedcell injury to human hepatocytes. Toxicol Sci 101:341–349.
Lluis JM, Buricchi F, Chiarugi P, Morales A, and Fernandez-Checa JC (2007) Dualrole of mitochondrial reactive oxygen species in hypoxia signaling: activation ofnuclear factor-{�}B via c-SRC and oxidant-dependent cell death. Cancer Res 67:7368–7377. �
Lluis JM, Morales A, Blasco C, Colell A, Mari M, Garcia-Ruiz C, and Fernandez-Checa JC (2005) Critical role of mitochondrial glutathione in the survival ofhepatocytes during hypoxia. J Biol Chem 280:3224–3232.
Loi CM, Young M, Randinitis E, Vassos A, and Koup JR (1999) Clinical pharmaco-kinetics of troglitazone. Clin Pharmacokinet 37:91–104.
Lu J, Roth RA, and Ganey PE (2009) Amiodarone exposure during modest inflam-mation induces idiosyncrasy-like liver injury in rats (Abstract). Toxicol Sci, inpress.
Luo G, Garner CE, Xiong H, Hu H, Richards LE, Brouwer KL, Duan J, Decicco CP,Maduskuie T, Shen H, et al. (2007) Effect of DPC 333 [(2R)-2-{(3R)-3-amino-3-[4-(2-methylquinolin-4-ylmethoxy)phenyl]-2-oxopyrrolidin-1-yl}-N-hydroxy-4-methylpentanamide], a human tumor necrosis factor alpha-converting enzymeinhibitor, on the disposition of methotrexate: a transporter-based drug-drug inter-action case study. Drug Metab Dispos 35:835–840.
Luparini RL, Rotundo A, Mattace R, and Marigliano V (2000) [Possibly ranitidine-induced autoimmune hepatitis]. Ann Ital Med Int 15:214–217.
Luyendyk JP, Lehman-McKeeman LD, Nelson DM, Bhaskaran VM, Reilly TP, CarBD, Cantor GH, Deng X, Maddox JF, Ganey PE, et al. (2006a) Coagulation-dependent gene expression and liver injury in rats given lipopolysaccharide withranitidine but not with famotidine. J Pharmacol Exp Ther 317:635–643.
Luyendyk JP, Lehman-McKeeman LD, Nelson DM, Bhaskaran VM, Reilly TP, CarBD, Cantor GH, Maddox JF, Ganey PE, and Roth RA (2006b) Unique geneexpression and hepatocellular injury in the lipopolysaccharide-ranitidine drugidiosyncrasy rat model: comparison with famotidine. Toxicol Sci 90:569–585.
Luyendyk JP, Maddox JF, Cosma GN, Ganey PE, Cockerell GL, and Roth RA (2003)Ranitidine treatment during a modest inflammatory response precipitates idio-syncrasy-like liver injury in rats. J Pharmacol Exp Ther 307:9–16.
Luyendyk JP, Maddox JF, Green CD, Ganey PE, and Roth RA (2004) Role of hepaticfibrin in idiosyncrasy-like liver injury from lipopolysaccharide-ranitidine coexpo-sure in rats. Hepatology 40:1342–1351.
Luyendyk JP, Shaw PJ, Green CD, Maddox JF, Ganey PE, and Roth RA (2005)Coagulation-mediated hypoxia and neutrophil-dependent hepatic injury in ratsgiven lipopolysaccharide and ranitidine. J Pharmacol Exp Ther 314:1023–1031.
Macfelda K, Weiss TW, Kaun C, Breuss JM, Zorn G, Oberndorfer U, Voegele-KadletzM, Huber-Beckmann R, Ullrich R, Binder BR, et al. (2002) Plasminogen activatorinhibitor 1 expression is regulated by the inflammatory mediators interleukin-1[�], tumor necrosis factor-[�], transforming growth factor-[�] and oncostatin m inhuman cardiac myocytes. J Mol Cell Cardiol 34:1681–1691.
Mackman N, Tilley RE, and Key NS (2007) Role of the extrinsic pathway of bloodcoagulation in hemostasis and thrombosis. Arterioscler Thromb Vasc Biol 27:1687–1693.
Maher JJ, Scott MK, Saito JM, and Burton MC (1997) Adenovirus-mediated expres-sion of cytokine-induced neutrophil chemoattractant in rat liver induces a neutro-philic hepatitis. Hepatology 25:624–630.
Masubuchi Y (2006) Metabolic and non-metabolic factors determining troglitazonehepatotoxicity: a review. Drug Metab Pharmacokinet 21:347–356.
Masubuchi Y, Nakayama S, and Horie T (2002) Role of mitochondrial permeabilitytransition in diclofenac-induced hepatocyte injury in rats. Hepatology 35:544–551.
Maugeri N, Brambilla M, Camera M, Carbone A, Tremoli E, Donati MB, de GaetanoG, and Cerletti C (2006) Human polymorphonuclear leukocytes produce and ex-press functional tissue factor upon stimulation. J Thromb Haemost 4:1323–1330.
Mavier P, Preaux AM, Guigui B, Lescs MC, Zafrani ES, and Dhumeaux D (1988) Invitro toxicity of polymorphonuclear neutrophils to rat hepatocytes: evidence for aproteinase-mediated mechanism. Hepatology 8:254–258.
280 DENG ET AL.

McGeehan GM, Becherer JD, Bast RC Jr, Boyer CM, Champion B, Connolly KM,Conway JG, Furdon P, Karp S, and Kidao S (1994) Regulation of tumour necrosisfactor-� processing by a metalloproteinase inhibitor. Nature 370:558–561.
Michalek SM, Moore RN, McGhee JR, Rosenstreich DL, and Mergenhagen SE (1980)The primary role of lymphoreticular cells in the mediation of host responses tobacterial endotoxin. J Infect Dis 141:55–63.
Miyamoto G, Zahid N, and Uetrecht JP (1997) Oxidation of diclofenac to reactiveintermediates by neutrophils, myeloperoxidase, and hypochlorous acid. Chem ResToxicol 10:414–419.
Mizoguchi Y, Shin T, Mizuno M, Seki S, Kobayashi K, and Morisawa S (1990) Theenhancement of liver injury by lipopolysaccharide in an experimental drug-induced allergic hepatitis model. Gastroenterol Jpn 25:458–462.
Mohler KM, Sleath PR, Fitzner JN, Cerretti DP, Alderson M, Kerwar SS, TorranceDS, Otten-Evans C, Greenstreet T, and Weerawarna K (1994) Protection againsta lethal dose of endotoxin by an inhibitor of tumour necrosis factor processing.Nature 370:218–220.
Morgan ET, Goralski KB, Piquette-Miller M, Renton KW, Robertson GR, ChaluvadiMR, Charles KA, Clarke SJ, Kacevska M, Liddle C, et al. (2008) Regulation ofdrug-metabolizing enzymes and transporters in infection, inflammation, and can-cer. Drug Metab Dispos 36:205–216.
Moulin F, Copple BL, Ganey PE, and Roth RA (2001) Hepatic and extrahepaticfactors critical for liver injury during lipopolysaccharide exposure. Am J PhysiolGastrointest Liver Physiol 281:G1423–G1431.
Mullberg J, Althoff K, Jostock T, and Rose-John S (2000) The importance of sheddingof membrane proteins for cytokine biology. Eur Cytokine Netw 11:27–38.
Murphy EJ, Davern TJ, Shakil AO, Shick L, Masharani U, Chow H, Freise C, LeeWM, and Bass NM (2000) Troglitazone-induced fulminant hepatic failure. AcuteLiver Failure Study Group. Dig Dis Sci 45:549–553.
Nagaki M, Muto Y, Ohnishi H, and Moriwaki H (1991) Significance of tumor necrosisfactor (TNF) and interleukin-1 (IL-1) in the pathogenesis of fulminant hepatitis:possible involvement of serine protease in TNF-mediated liver injury. Gastroen-terol Jpn 26:448–455.
Neininger A, Kontoyiannis D, Kotlyarov A, Winzen R, Eckert R, Volk HD, HoltmannH, Kollias G, and Gaestel M (2002) MK2 targets AU-rich elements and regulatesbiosynthesis of tumor necrosis factor and interleukin-6 independently at differentpost-transcriptional levels. J Biol Chem 277:3065–3068.
Numahata K, Komagata T, Hirasawa N, Someya K, Xiao YQ, and Ohuchi K (2003)Analysis of the mechanism regulating the stability of rat macrophage inflamma-tory protein-2 MRNA in RBL-2H3 Cells. J Cell Biochem 90:976–986.
Oda K and Kitano H (2006) A comprehensive map of the toll-like receptor signalingnetwork. Mol Syst Biol 2:2006.0015.
Offit K and Sojka DA (1984) Ranitidine (Letter). N Engl J Med 310:1603–1604.Okajima K, Harada N, and Uchiba M (2002) Ranitidine reduces ischemia/
reperfusion-induced liver injury in rats by inhibiting neutrophil activation.J Pharmacol Exp Ther 301:1157–1165.
Okajima K, Murakami K, Liu W, and Uchiba M (2000) Inhibition of neutrophilactivation by ranitidine contributes to prevent stress-induced gastric mucosalinjury in rats. Crit Care Med 28:2858–2865.
Ong MM, Latchoumycandane C, and Boelsterli UA (2007) Troglitazone-inducedhepatic necrosis in an animal model of silent genetic mitochondrial abnormalities.Toxicol Sci 97:205–213.
Owensby DA, Morton PA, Wun TC, and Schwartz AL (1991) Binding of plasminogenactivator inhibitor type-1 to extracellular matrix of Hep G2 cells. Evidence that thebinding protein is vitronectin. J Biol Chem 266:4334–4340.
Padro T, Emeis JJ, Steins M, Schmid KW, and Kienast J (1995) Quantification ofplasminogen activators and their inhibitors in the aortic vessel wall in relation tothe presence and severity of atherosclerotic disease. Arterioscler Thromb Vasc Biol15:893–902.
Padro T, Steins M, Li CX, Mesters RM, Hammel D, Scheld HH, and Kienast J (1997)Comparative analysis of plasminogen activator inhibitor-1 expression in differenttypes of atherosclerotic lesions in coronary arteries from human heart explants.Cardiovasc Res 36:28–36.
Park BK, Naisbitt DJ, Gordon SF, Kitteringham NR, and Pirmohamed M (2001)Metabolic activation in drug allergies. Toxicology 158:11–23.
Parry GC and Mackman N (1995) Transcriptional regulation of tissue factor expres-sion in human endothelial cells. Arterioscler Thromb Vasc Biol 15:612–621.
Pawlinski R, Pedersen B, Schabbauer G, Tencati M, Holscher T, Boisvert W, An-drade-Gordon P, Frank RD, and Mackman N (2004) Role of tissue factor andprotease-activated receptors in a mouse model of endotoxemia. Blood 103:1342–1347.
Pearson JM, Brown AP, Schultze AE, Ganey PE, and Roth RA (1996a) Gadoliniumchloride treatment attenuates hepatic platelet accumulation after lipopolysaccha-ride administration. Shock 5:408–415.
Pearson JM, Schultze AE, Schwartz KA, Scott MA, Davis JM, and Roth RA (1996b)The thrombin inhibitor, hirudin, attenuates lipopolysaccharide-induced liver in-jury in the rat. J Pharmacol Exp Ther 278:378–383.
Pellock JM (1999) Felbamate in epilepsy therapy: evaluating the risks. Drug Saf21:225–239.
Petrovic V, Teng S, and Piquette-Miller M (2007) Regulation of drug transportersduring infection and inflammation. Mol Interv 7:99–111.
Pfeffer K, Matsuyama T, Kundig TM, Wakeham A, Kishihara K, Shahinian A,Wiegmann K, Ohashi PS, Kronke M, and Mak TW (1993) Mice deficient for the 55kd tumor necrosis factor receptor are resistant to endotoxic shock, yet succumb toL. monocytogenes infection. Cell 73:457–467.
Pinsky DJ, Naka Y, Liao H, Oz MC, Wagner DD, Mayadas TN, Johnson RC, HynesRO, Heath M, Lawson CA, et al. (1996) Hypoxia-induced exocytosis of endothelialcell Weibel-Palade bodies. A mechanism for rapid neutrophil recruitment aftercardiac preservation. J Clin Invest 97:493–500.
Pintucci G, Iacoviello L, Amore C, Evangelista V, Cerletti C, and Donati MB (1992)Cathepsin G, a polymorphonuclear cell protease, affects the fibrinolytic system by
releasing PAI-1 from endothelial cells and platelets. Ann N Y Acad Sci 667:286–288.
Pintucci G, Iacoviello L, Castelli MP, Amore C, Evangelista V, Cerletti C, and DonatiMB (1993) Cathepsin G-induced release of PAI-1 in the culture medium of endo-thelial cells: a new thrombogenic role for polymorphonuclear leukocytes? J LabClin Med 122:69–79.
Piret JP, Mottet D, Raes M, and Michiels C (2002) Is HIF-1alpha a pro- or ananti-apoptotic protein? Biochem Pharmacol 64:889–892.
Pirmohamed M, James S, Meakin S, Green C, Scott AK, Walley TJ, Farrar K, ParkBK, and Breckenridge AM (2004) Adverse drug reactions as cause of admission tohospital: prospective analysis of 18 820 patients. BMJ 329:15–19.
Pirmohamed M, Naisbitt DJ, Gordon F, and Park BK (2002) The danger hypothesis–potential role in idiosyncratic drug reactions. Toxicology 181–182:55–63.
Prendergast KA, Berg CL, and Wisniewski R (2000) Troglitazone-associated hepa-totoxicity treated successfully with steroids. Ann Intern Med 133:751.
Proctor JD (1984) Hepatitis associated with ranitidine. JAMA 251:1554.Ramrakhiani S, Brunt EM, and Bacon BR (1998) Possible cholestatic injury from
ranitidine with a review of the literature. Am J Gastroenterol 93:822–826.Rau JC, Beaulieu LM, Huntington JA, and Church FC (2007) Serpins in thrombosis,
hemostasis and fibrinolysis. J Thromb Haemost 5 (Suppl 1):102–115.Renton KW (2005) Regulation of drug metabolism and disposition during inflamma-
tion and infection. Expert Opin Drug Metab Toxicol 1:629–640.Ribeiro JM, Lucas M, Baptista A, and Victorino RM (2000) Fatal hepatitis associated
with ranitidine. Am J Gastroenterol 95:559–560.Rietschel ET, Brade H, Holst O, Brade L, Muller-Loennies S, Mamat U, Zahringer U,
Beckmann F, Seydel U, Brandenburg K, et al. (1996) Bacterial endotoxin: Chem-ical constitution, biological recognition, host response, and immunological detoxi-fication. Curr Top Microbiol Immunol 216:39–81.
Roth RA, Harkema JR, Pestka JP, and Ganey PE (1997) Is exposure to bacterialendotoxin a determinant of susceptibility to intoxication from xenobiotic agents?Toxicol Appl Pharmacol 147:300–311.
Roth RA, Luyendyk JP, Maddox JF, and Ganey PE (2003) Inflammation and drugidiosyncrasy—is there a connection? J Pharmacol Exp Ther 307:1–8.
Rothwell C, McGuire EJ, Altrogge DM, Masuda H, and de la Iglesia FA (2002)Chronic toxicity in monkeys with the thiazolidinedione antidiabetic agent trogli-tazone. J Toxicol Sci 27:35–47.
Scheen AJ (2001a) Hepatotoxicity with thiazolidinediones: is it a class effect? DrugSaf 24:873–888.
Scheen AJ (2001b) Thiazolidinediones and liver toxicity. Diabetes Metab 27:305–313.Schleef RR, Bevilacqua MP, Sawdey M, Gimbrone MA Jr, and Loskutoff DJ (1988)
Cytokine activation of vascular endothelium. Effects on tissue-type plasminogenactivator and type 1 plasminogen activator inhibitor. J Biol Chem 263:5797–5803.
Schleiffenbaum B and Fehr J (1990) The tumor necrosis factor receptor and humanneutrophil function. Deactivation and cross-deactivation of tumor necrosis factor-induced neutrophil responses by receptor down-regulation. J Clin Invest 86:184–195.
Schumann J, Angermuller S, Bang R, Lohoff M, and Tiegs G (1998) Acute hepato-toxicity of Pseudomonas aeruginosa exotoxin A in mice depends on T cells andTNF. J Immunol 161:5745–5754.
Schwabe RF and Brenner DA (2006) Mechanisms of liver injury. I. TNF-�-inducedliver injury: role of IKK, JNK, and ROS pathways. Am J Physiol Gastrointest LiverPhysiol 290:G583–G589.
Schwager I and Jungi TW (1994) Effect of human recombinant cytokines on theinduction of macrophage procoagulant activity. Blood 83:152–160.
Seguin B and Uetrecht J (2003) The danger hypothesis applied to idiosyncratic drugreactions. Curr Opin Allergy Clin Immunol 3:235–242.
Seitz S and Boelsterli UA (1998) Diclofenac acyl glucuronide, a major biliary metab-olite, is directly involved in small intestinal injury in rats. Gastroenterology 115:1476–1482.
Seitz S, Kretz-Rommel A, Oude Elferink RP, and Boelsterli UA (1998) Selectiveprotein adduct formation of diclofenac glucuronide is critically dependent on therat canalicular conjugate export pump (Mrp2). Chem Res Toxicol 11:513–519.
Senior JR (2008) What is idiosyncratic hepatotoxicity? What is it not? Hepatology47:1813–1815.
Sgro C, Clinard F, Ouazir K, Chanay H, Allard C, Guilleminet C, Lenoir C, LemoineA, and Hillon P (2002) Incidence of drug-induced hepatic injuries: a Frenchpopulation-based study. Hepatology 36:451–455.
Shaw PJ, Ganey PE, and Roth RA (2009) Trovafloxacin enhances the inflammatoryresponse to a Gram-negative or a Gram-positive stimulus, resulting in neutrophil-dependent liver injury in mice. J Pharmacol Exp Ther 330:72–78.
Shaw PJ, Hopfensperger MJ, Ganey PE, and Roth RA (2007) Lipopolysaccharide andtrovafloxacin coexposure in mice causes idiosyncrasy-like liver injury dependenton tumor necrosis factor-�. Toxicol Sci 100:259–266.
Shibayama Y (1987) Enhanced hepatotoxicity of endotoxin by hypoxia. Pathol ResPract 182:390–395.
Shreeniwas R, Koga S, Karakurum M, Pinsky D, Kaiser E, Brett J, Wolitzky BA,Norton C, Plocinski J, and Benjamin W (1992) Hypoxia-mediated induction ofendothelial cell interleukin-1�. An autocrine mechanism promoting expression ofleukocyte adhesion molecules on the vessel surface. J Clin Invest 90:2333–2339.
Siu WP, Pun PB, Latchoumycandane C, and Boelsterli UA (2008) Bax-mediatedmitochondrial outer membrane permeabilization (MOMP), distinct from the mito-chondrial permeability transition, is a key mechanism in diclofenac-induced he-patocyte injury: multiple protective roles of cyclosporin A. Toxicol Appl Pharmacol227:451–461.
Smedly LA, Tonnesen MG, Sandhaus RA, Haslett C, Guthrie LA, Johnston RB Jr,Henson PM, and Worthen GS (1986) Neutrophil-mediated injury to endothelialcells. Enhancement by endotoxin and essential role of neutrophil elastase. J ClinInvest 77:1233–1243.
Sneed RA, Grimes SD, Schultze AE, Brown AP, and Ganey PE (1997) Bacterialendotoxin enhances the hepatotoxicity of allyl alcohol. Toxicol Appl Pharmacol144:77–87.
INFLAMMATORY STRESS AND IDIOSYNCRATIC HEPATOTOXICITY 281

Soejima Y, Yanaga K, Nishizaki T, Yoshizumi T, Uchiyama H, and Sugimachi K(1999) Effect of specific neutrophil elastase inhibitor on ischemia/reperfusioninjury in rat liver transplantation. J Surg Res 86:150–154.
Souza Lima MA (1984) Hepatitis associated with ranitidine. Ann Intern Med 101:207–208.
Spek CA (2004) Tissue factor: from ‘just one of the coagulation factors’ to a majorplayer in physiology. Blood Coagul Fibrinolysis 15 (Suppl 1):S3–S10.
Springer TA (1994) Traffic signals for lymphocyte recirculation and leukocyte emi-gration: the multistep paradigm. Cell 76:301–314.
Tacke F, Luedde T, and Trautwein C (2009) Inflammatory pathways in liver ho-meostasis and liver injury. Clin Rev Allergy Immunol 36:4–12.
Tafazoli S, Spehar DD, and O’Brien PJ (2005) Oxidative stress mediated idiosyn-cratic drug toxicity. Drug Metab Rev 37:311–325.
Takei Y, Kawano S, Nishimura Y, Goto M, Nagai H, Chen SS, Omae A, Fusamoto H,Kamada T, Ikeda K, et al. (1995) Apoptosis: a new mechanism of endothelial andKupffer cell killing. J Gastroenterol Hepatol 10 (Suppl 1):S65–S67.
Tamura DY, Moore EE, Partrick DA, Johnson JL, Offner PJ, and Silliman CC (2002)Acute hypoxemia in humans enhances the neutrophil inflammatory response.Shock 17:269–273.
Tartaglia LA, Rothe M, Hu YF, and Goeddel DV (1993) Tumor necrosis factor’scytotoxic activity is signaled by the p55 TNF receptor. Cell 73:213–216.
Tettey JN, Maggs JL, Rapeport WG, Pirmohamed M, and Park BK (2001) Enzyme-induction dependent bioactivation of troglitazone and troglitazone quinone in vivo.Chem Res Toxicol 14:965–974.
Tirmenstein MA, Hu CX, Gales TL, Maleeff BE, Narayanan PK, Kurali E, Hart TK,Thomas HC, and Schwartz LW (2002) Effects of troglitazone on HepG2 viabilityand mitochondrial function. Toxicol Sci 69:131–138.
Tracey KJ, Beutler B, Lowry SF, Merryweather J, Wolpe S, Milsark IW, Hariri RJ,Fahey TJ 3rd, Zentella A, and Albert JD (1986) Shock and tissue injury induced byrecombinant human cachectin. Science 234:470–474.
Tracey KJ, Fong Y, Hesse DG, Manogue KR, Lee AT, Kuo GC, Lowry SF, and CeramiA (1987) Anti-cachectin/TNF monoclonal antibodies prevent septic shock duringlethal bacteraemia. Nature 330:662–664.
Tracy RP (2003) Emerging relationships of inflammation, cardiovascular disease andchronic diseases of aging. Int J Obes Relat Metab Disord 27 (Suppl 3):S29–S34.
Tukov FF, Luyendyk JP, Ganey PE, and Roth RA (2007) The role of tumor necrosisfactor � in lipopolysaccharide/ranitidine-induced inflammatory liver injury. Toxi-col Sci 100:267–280.
Uetrecht J (1991) Metabolism of drugs by activated leukocytes: implications fordrug-induced lupus and other drug hypersensitivity reactions. Adv Exp Med Biol283:121–132.
Uetrecht J (2008) Idiosyncratic drug reactions: past, present, and future. Chem ResToxicol 21:84–92.
Uetrecht J (2007) Idiosyncratic drug reactions: current understanding. Annu RevPharmacol Toxicol 47:513–539.
Valois M, Cooper MA, and Shear NH (2003) Clinical pharmacology consultations:consultation requests may be misleading—an organized approach to drug-inducedhepatitis. Can J Clin Pharmacol 10:59–62.
van Bommel EF and Meyboom RH (1992) [Liver damage caused by ranitidine]. NedTijdschr Geneeskd 136:435–437.
Varriale M, Salvio A, Giannattasio F, d’Errico T, Montone L, Borgia F, Gentile I,Reynaud L, Borgia G, Rossiello R, et al. (2004) Intrahepatic cholestatic jaundicerelated to administration of ranitidine. A case report with histologic and ultrami-croscopic study. Minerva Gastroenterol Dietol 50:339–343.
Vassalli P (1992) The pathophysiology of tumor necrosis factors. Annu Rev Immunol10:411–452.
Vial T, Goubier C, Bergeret A, Cabrera F, Evreux JC, and Descotes J (1991) Sideeffects of ranitidine. Drug Saf 6:94–117.
Vignati L, Turlizzi E, Monaci S, Grossi P, Kanter R, and Monshouwer M (2005) Anin vitro approach to detect metabolite toxicity due to CYP3A4-dependent bioacti-vation of xenobiotics. Toxicology 216:154–167.
Vollmar B, Ruttinger D, Wanner GA, Leiderer R, and Menger MD (1996) Modulation
of Kupffer cell activity by gadolinium chloride in endotoxemic rats. Shock 6:434–441.
Walker AM (1997) Quantitative studies of the risk of serious hepatic injury inpersons using nonsteroidal antiinflammatory drugs. Arthritis Rheum 40:201–208.
Waring JF and Anderson MG (2005) Idiosyncratic toxicity: mechanistic insightsgained from analysis of prior compounds. Curr Opin Drug Discov Devel 8:59–65.
Waring JF, Liguori MJ, Luyendyk JP, Maddox JF, Ganey PE, Stachlewitz RF, NorthC, Blomme EA, and Roth RA (2006) Microarray analysis of lipopolysaccharidepotentiation of trovafloxacin-induced liver injury in rats suggests a role for proin-flammatory chemokines and neutrophils. J Pharmacol Exp Ther 316:1080–1087.
Watanabe I, Tomita A, Shimizu M, Sugawara M, Yasumo H, Koishi R, Takahashi T,Miyoshi K, Nakamura K, Izumi T, et al. (2003) A study to survey susceptiblegenetic factors responsible for troglitazone-associated hepatotoxicity in Japanesepatients with type 2 diabetes mellitus. Clin Pharmacol Ther 73:435–455.
Watanabe Y, Nakajima M, and Yokoi T (2002) Troglitazone glucuronidation inhuman liver and intestine microsomes: high catalytic activity of UGT1A8 andUGT1A10. Drug Metab Dispos 30:1462–1469.
Watkins PB (2005) Idiosyncratic liver injury: challenges and approaches. ToxicolPathol 33:1–5.
Watkins PB and Whitcomb RW (1998) Hepatic dysfunction associated with trogli-tazone. N Engl J Med 338:916–917.
Westrick RJ and Eitzman DT (2007) Plasminogen activator inhibitor-1 in vascularthrombosis. Curr Drug Targets 8:966–1002.
Whitcomb DC (2004) Inflammation and Cancer V. Chronic pancreatitis and pancre-atic cancer.. Am J Physiol Gastrointest Liver Physiol 287:G315–G319.
Willerson JT and Ridker PM (2004) Inflammation as a cardiovascular risk factor.Circulation 109:II2–II10.
Williams DP and Park BK (2003) Idiosyncratic toxicity: the role of toxicophores andbioactivation. Drug Discov Today 8:1044–1050.
Xu L, Xie K, Mukaida N, Matsushima K, and Fidler IJ (1999) Hypoxia-inducedelevation in interleukin-8 expression by human ovarian carcinoma cells. CancerRes 59:5822–5829.
Yamaguchi Y, Akizuki E, Ichiguchi O, Matsumura F, Goto M, Miyanari N, Mori K,Yamada S, and Ogawa M (1997) Neutrophil elastase inhibitor reduces neutrophilchemoattractant production after ischemia-reperfusion in rat liver. Gastroenterol-ogy 112:551–560.
Yamaguchi Y, Matsumura F, Liang J, Okabe K, Ohshiro H, Ishihara K, Matsuda T,Mori K, and Ogawa M (1999) Neutrophil elastase and oxygen radicals enhancemonocyte chemoattractant protein- expression after ischemia/reperfusion in ratliver. Transplantation 68:1459–1468.
Yamamoto Y, Nakajima M, Yamazaki H, and Yokoi T (2001) Cytotoxicity andapoptosis produced by troglitazone in human hepatoma cells. Life Sci 70:471–482.
Yee SB, Ganey PE, and Roth RA (2003a) The role of Kupffer cells and TNF-� inmonocrotaline and bacterial lipopolysaccharide-induced liver injury. Toxicol Sci71:124–132.
Yee SB, Hanumegowda UM, Hotchkiss JA, Ganey PE, and Roth RA (2003b) Role ofneutrophils in the synergistic liver injury from monocrotaline and bacterial lipo-polysaccharide exposure. Toxicol Sci 72:43–56.
Yoshigae Y, Konno K, Takasaki W, and Ikeda T (2000) Characterization of UDP-glucuronosyltransferases (UGTS) involved in the metabolism of troglitazone inrats and humans. J Toxicol Sci 25:433–441.
Zimmerman HJ (1993) Hepatotoxicity. Dis Mon 39:675–787.Zimmerman HJ (2000) Drug-induced liver disease. Clin Liver Dis 4:73–96, vi.Zimmerman HJ (1999) Hepatotoxicity: The Adverse Effects of Drugs and Other
Chemicals on the Liver, Lippincott Williams & Wilkins, Philadelphia.Zou W, Devi SS, Sparkenbaugh E, Younis HS, Roth RA, and Ganey PE (2009)
Hepatotoxic interaction of sulindac with lipopolysaccharide: role of the hemostaticsystem. Toxicol Sci 108:184–193.
Zuurbier KW, Bakkenist AR, Fokkens RH, Nibbering NM, Wever R, and MuijsersAO (1990) Interaction of myeloperoxidase with diclofenac. Inhibition of the chlo-rinating activity of myeloperoxidase by diclofenac and oxidation of diclofenac todihydroxyazobenzene by myeloperoxidase. Biochem Pharmacol 40:1801–1808.
282 DENG ET AL.



![INDEX [pharmrev.aspetjournals.org]pharmrev.aspetjournals.org/content/pharmrev/5/4/local/back-matter.pdf · effectonmyasthenia gravis, 64 ... Anemia, effects ofantibiotics on, 406](https://img.dokumen.tips/doc/110x75/5d45af6088c993f1188d864c/index-effectonmyasthenia-gravis-64-anemia-effects-ofantibiotics-on.jpg)

![INDEX [pharmrev.aspetjournals.org]pharmrev.aspetjournals.org/content/pharmrev/7/4/local/... · 2005-07-23 · INDEX 499 Receptor hypothesis, development, 197 theory fornon-competitive](https://img.dokumen.tips/doc/110x75/5f792a265f98132bd25e45a7/index-2005-07-23-index-499-receptor-hypothesis-development-197-theory-fornon-competitive.jpg)

![INDEX [pharmrev.aspetjournals.org]pharmrev.aspetjournals.org/content/pharmrev/6/4/local/back-matter.… · 546 INDEX Drugallergy-Continued dosage ofdrugaffecting, 395 duration of,408](https://img.dokumen.tips/doc/110x75/5e9d1621ae88997f3e7425b1/index-546-index-drugallergy-continued-dosage-ofdrugaffecting-395-duration-of408.jpg)





















