Embed Size (px)
Citation preview

Pharmacokinetic and Pharmacodynamic Sciences in Oncology Drug Development: Enabling Rational Dose Selection from Translational to Global Drug Development
Karthik Venkatakrishnan, Ph.D., FCPQuantitative Clinical PharmacologyTakeda Pharmaceuticals International Co.Cambridge, MA, USA
3rd Annual Conference of Society for the Study of Xenobiotics (SSX), India
October 13, 2018Bangalore, India
1

Outline of Presentation
Translational PK/PD Considerations
Dose Selection in Early Drug Development
Case Study: Alisertib Single Agent and Combination with Paclitaxel
Population Pharmacokinetics and Exposure-Response
Case Study: Ixazomib in Relapsed/ Refractory Multiple Myeloma
Enabling Global Drug Development
Case Study: Alisertib in East Asian Patient Populations
Concluding Remarks
2

Quantitative Pharmacology Across the Continuum ofOncology Drug Development: Challenges and Opportunities
Venkatakrishnan K et al., Clinical Pharmacology and Therapeutics 97(1): 37-54, 20153

PK/PD Scientific Considerations are Crucial to EnhanceTranslational Utility of Mouse Xenograft Models
PK/E Model-estimated Potency
Clin
ical
Exp
osur
eat
Effe
ctiv
e D
ose
Rocchetti M et al., European Journal of Cancer 43: 1862-1868, 2007Wong H et al., Clinical Cancer Research 18:3846-3855, 2012
4

Translational PK/Efficacy Modeling and Simulationto Guide Clinical Dosing Schedules
Venkatakrishnan K et al., Clinical Pharmacology and Therapeutics 97(1): 37-54, 2015 5

Clinical Tumor Pharmacodynamic Studies –Are they Adding Value as Designed and Analyzed?
Sweis RF et al., Journal of Clinical Oncology 34(4):369-74, 2016
Only 17% of Ph 1’s with Tumor PD assessments demonstrated
positive PD effects!
6
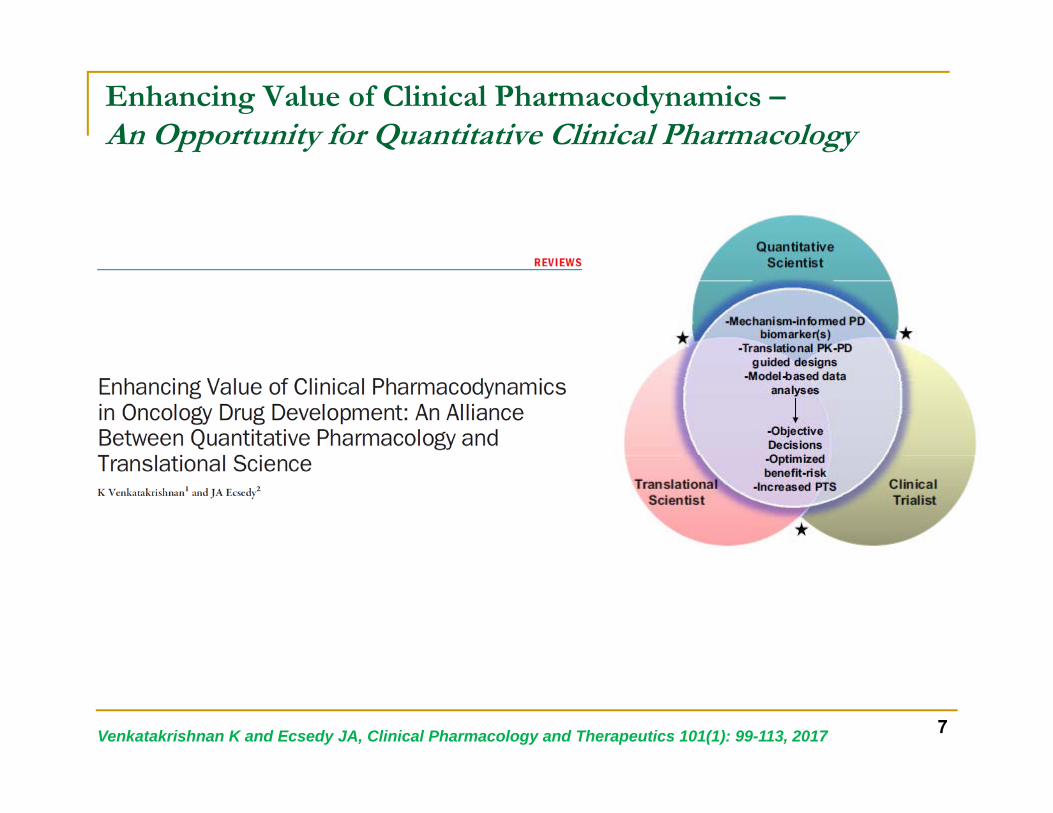
Enhancing Value of Clinical Pharmacodynamics –An Opportunity for Quantitative Clinical Pharmacology
Venkatakrishnan K and Ecsedy JA, Clinical Pharmacology and Therapeutics 101(1): 99-113, 2017 7

Enhancing Value of PharmacodynamicsAn Analytical Framework Enabled by a Totality of Evidence Mindset
Venkatakrishnan K and Ecsedy JA, Clinical Pharmacology and Therapeutics 101(1): 99-113, 2017 8

Case Study: Investigational Aurora A Kinase Inhibitor Alisertib
Selecting RP2D Leveraging Clinical Exposure-Tumor PD and Exposure-Safety Relationships
9

Exposure- Tumor PD Relationships for the InvestigationalAurora A Kinase Inhibitor Alisertib to Guide RP2D/ Schedule Selection
Venkatakrishnan K et al., Journal of Clinical Pharmacology 55(3): 336-347, 2015
Aligned chromosomesBipolar spindle
Unaligned chromosomesBipolar spindle
Unaligned chromosomesNon‐bipolar spindle
Steady-state AUC(0-24hr) (nM.hr)
0 20000 40000 60000 80000 100000 120000 140000 160000
Chr
omos
ome
Alig
nmen
t(P
erce
nt o
f Bas
elin
e V
alue
)
0
10
20
30
40
50
60
70
80
90
100
110130
135
Steady-state AUC(0-24hr) (nM.hr)
0 20000 40000 60000 80000 100000 120000 140000 160000
Spi
ndle
Bip
olar
ity(P
erce
nt o
f Bas
elin
e V
alue
)
0
10
20
30
40
50
60
70
80
90
100
110130
135Chromosome Alignment Spindle Bipolarity
Schedule MTD Dose density(mg/day)
AUC0-24h,ss(M.hr)
IQR
Tumor PD(% in CA/SB)
IQR7on/ 14off 50 mg BID 33.3 33-63 68-80 / 55-70
21on/ 14off 50 mg QD 30.0 17-31 52-67 / 38-53
10

Therapeutic Index Understanding for the Investigational Agent Alisertib Informed by Population PK, Exposure-PD and Exposure-Safety Analyses
Venkatakrishnan K et al., Journal of Clinical Pharmacology 55(3): 336-347, 2015 11

Tota
l Cyc
le U
nbou
nd P
aclit
axel
AU
C (n
g.hr
/mL)
0 1000 2000 3000 4000 5000 6000 7000 8000 9000 100000
200
400
600
800
1000
60P80P60P/40A80P/10A
857565
352515
555
Total cycle unbound AUC of investigational agent
Translational Exposure-Efficacy Modeling for Drug Combinations:RP2D Selection for Alisertib-Paclitaxel
Two MTDs determined in Phase 1b MTD1: Full weekly paclitaxel dose (80 mg/m2) plus 10 mg BID alisertib MTD2: Level -1 weekly paclitaxel dose (60 mg/m2) plus 40 mg BID alisertib
MTD2 selected as RP2D based on translational PK/PD considerations
Huck JJ et al., Molecular Cancer Therapeutics 13(9):2170-83, 2014
Isobologram
MTD1
MTD2
TGI Response Surface
12

Case Study: Ixazomib for Relapsed/ Refractory Multiple Myeloma
Population PK and Exposure-Response Applications in Support of the Approved Dose in Combination with Lenalidomide and Dexamethasone (Len-Dex)
13

Population PK Analysis at End of Phase 1:Model-Informed Switch from BSA-Based to Fixed Dosing
Gupta N et al., British Journal of Clinical Pharmacology 79(5):789-800, 2015
BSA‐based dosing
Fixed dosing
AUC (ng*hr/m
L)
020
0040
0060
0080
00
BSA (m2)
AU
C (n
g*hr
/mL)
1.4 1.6 1.8 2.0 2.2 2.4 2.6
050
0010
000
1500
0
Fixed Oral Dosing Simulation (N=1000)
14

Population PK analysis at End of Phase 3:Model-Informed Labeling/ Dosing Recommendations
No dose adjustments for BSA Age Race Sex Mild hepatic impairment Mild/moderate renal
impairment
For BSA and Age, median values are compared 5th and 95th pct
755 patients in 10 clinical studies,
including the phase 3 TOURMALINE-MM1
study
Gupta N et al., Clinical Pharmacokinetics 56(11):1355-1368, 2017 15

Ixazomib-Len-Dex in Relapsed/ Refractory Multiple Myeloma in TOURMALINE-MM1 Phase 3 Trial –
Consistent Efficacy Across Ixazomib Exposure QuartilesSupports 4 mg Weekly Starting Dose
Gupta N et al., Targeted Oncology 12(5):643-654, 2017 16
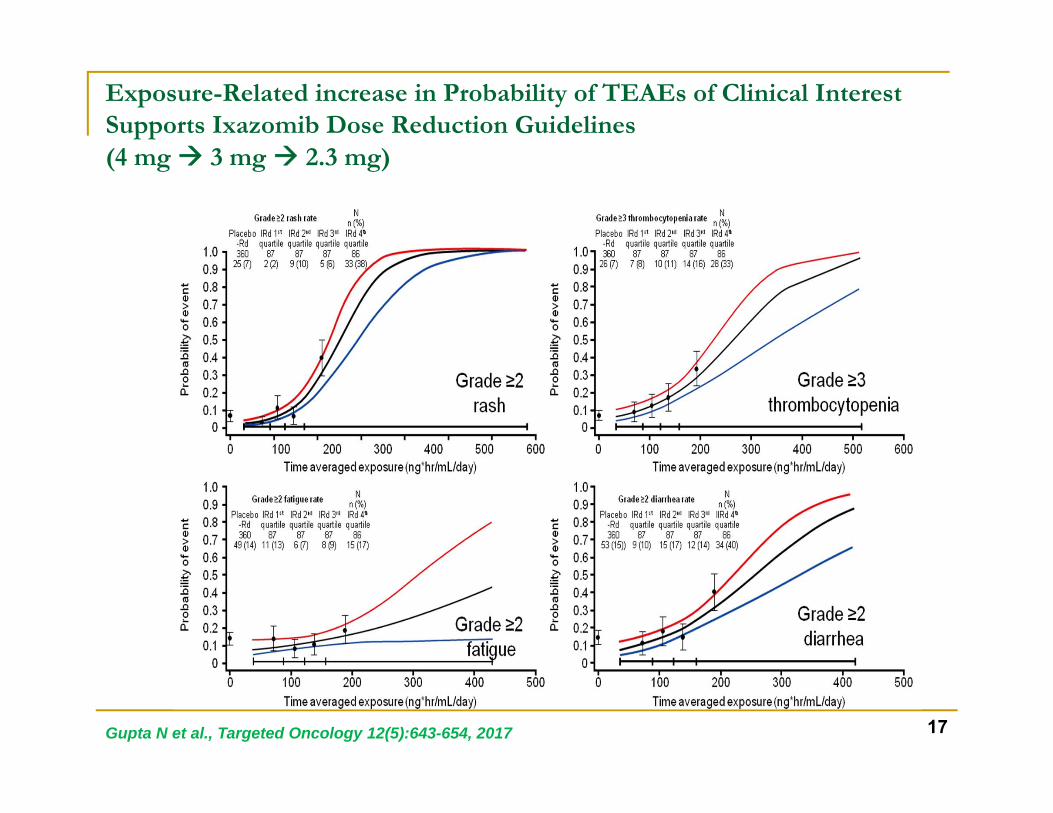
Exposure-Related increase in Probability of TEAEs of Clinical Interest Supports Ixazomib Dose Reduction Guidelines (4 mg 3 mg 2.3 mg)
17Gupta N et al., Targeted Oncology 12(5):643-654, 2017

Case Study: Alisertib in East Asian Patient Populations
Value of Population Pharmacology in Defining Dosage for Global Clinical Development
18

Multi-Regional Clinical Trials and ICH E17 –Opportunities for East Asia-Inclusive Global Clinical Development
Global MRCTs on the rise, notably in oncology and in rare diseases ICH E17 offers opportunities for efficient global drug development
Asano K et al., Clinical and Translational Science 11: 182–188, 2018http://www.ich.org/fileadmin/Public_Web_Site/ICH_Products/Guidelines/Efficacy/E17/E17EWG_Step4_2017_1116.pdf
19

Roadmap for PK/PD/Safety Guided Dose Decisions in East Asia-Inclusive Global Oncology Drug Development
Similar to Western
PK?
NO
YES
(PD, safety)
Clinically relevant
difference?(PD, safety)
• Low risk for differentdose for East Asia
• Base plan to assumecommon global doseWestern
Exposure-safety and Exposure-PD
relationshipNO
YES
DoseAsia ≠ DoseWestEvaluate regional trial versus exposure-matched global registration trial
East Asian Phase 1Assessment of PK/PD/Safety
Western Population PK
Analysis
Venkatakrishnan K et al., Clinical and Translational Science 9: 9-22; 2016 20

Alisertib in East Asia –An example of clinically relevant PK differences
Alisertib Steady-State AUC0-24hr (nM*hr)
0 20000 40000 60000 80000100000
120000140000
Prob
abili
ty o
f DLT
0.0
0.2
0.4
0.6
0.8
1.0
Western AUC Distribution (50 mg BID)
Asian AUC Distribution (50 mg BID - Projected)
Predicted DLT Probability95% Confidence Interval
Asian Geometric Mean AUC (50 mg BID - Projected)
Western Geometric Mean AUC (50 mg BID)
Time (hours)
0 2 4 6 8 10 12
Mea
n D
ose-
Nor
mal
ized
Alis
ertib
Pla
sma
Con
cent
ratio
n (n
M/m
g)
0
20
40
60
80
100
120
140West (n=23)Asia (n=34)
• PK/PD considerations supported a lower (30 mg vs. 50 mg) dosein East Asia
Venkatakrishnan K et al., Investigational New Drugs 33(4):942-53, 2015 22

Dosing Rationale for East Asia-Inclusive Global Development
MATCHINGSYSTEMIC EXPOSURES
22Zhou X et al., British Journal of Clinical Pharmacology 84(1):35-51, 2018

Global Oncology Drug developmentA Multi-Disciplinary Approach
Venkatakrishnan K et al., Clinical and Translational Science 9: 9-22; 2016 23

To conclude…
DOSE OPTIMIZATION IN
ANTICANCER DRUG
DEVELOPMENT
Translational PK/PD/EGuidedDose/
Schedule
Rational PD Design and
Interpretation
Appropriate Control of PK
Variability
RP2D Informed by Long-term Safety and Tolerability
Rational Design of
Combination Dosing
Regimens
Dose-Ranging Phase 2 Studies
Quantitative Benefit-Risk
Understanding
Timely Understanding
of Intrinsic/ Extrinsic
Factor Effects
24

Acknowledgments
Neeraj Gupta, Ph.D., FCP, Quantitative Clinical Pharmacology, Takeda Xiaofei Zhou, Ph.D., Quantitative Clinical Pharmacology, Takeda Michael Hanley, Pharm.D., Ph.D., Quantitative Clinical Pharmacology, Takeda Ajit Suri, Ph.D., MBA, Quantitative Clinical Pharmacology, Takeda Chirag Patel, Ph.D., Quantitative Clinical Pharmacology, Takeda Dean Bottino, Ph.D., Quantitative Clinical Pharmacology, Takeda
Mark Rogge, Ph.D., FCP, Quantitative Clinical Pharmacology, Takeda
Diane R. Mould, Ph.D., FCP, FAAPS, Projections Research Inc. Paul Diderichsen, Ph.D., Certara
Takeda Oncology Program Teams Takeda TREC/ OTAU Leadership
Investigators Patients and their families
25






























