Embed Size (px)
Citation preview

Pharmacogenetics and
Thienopyridines
Sandra Close Kirkwood, PhD
Eli Lilly and Company
May 14, 2010

Conflict of Interest
Sandra Close Kirkwood is employed by and
owns stock in Eli Lilly and Company. Eli Lilly
and Company developed and markets
prasugrel.
The views and opinions expressed in the
following PowerPoint slides are those of the
individual presenter.
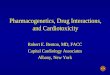
Adapted from Cannon CP. J Thrombolysis 1995:2:205-218
UA/NSTEMI STEMIStable Angina
Acute Coronary Syndromes
JJ
UA=Unstable angina; NSTEMI=Non–ST-elevation myocardial infarction; STEMI=ST-elevation myocardial infarction
Continuum of Severity
* Heart Disease and Stroke Statistics – 2007 Update. Circulation 2007; 115:69–171
1.57 Million Hospital Admissions in the US*

Antiplatelet Therapy in ACS
0
108
Placebo APTC CURE
Reduction in
Ischemic Events
Increase in
Major Bleeds
Single
Antiplatelet Rx
Dual
Antiplatelet Rx
ASA
- 22%
ASA + Clopidogrel
- 20%
+ 60% + 38%

Platelet Activation Mechanisms
Thrombin
Thromboxane
A2
5HT
P2Y12
ADP ADPADP
5HT
PLATELET
ACTIVATION
P2Y15HT2A
PAR1
PAR4
Dense
granule
Thrombin
generation
Shape
change
aIIbb3
aIIbb3
FibrinogenaIIbb3
Aggregation
AmplificationAlpha
granule
Coagulation factors
Inflammatory mediators
TPa
Coagulation
GPVI
Collagen
ATPATP
P2X1
ASPIRIN
x TICLOPIDINE
CLOPIDOGREL
PRASUGREL
ACTIVE
METABOLITE
x AZD6140
CANGRELOR
GP IIb/IIIa ANTAGONISTS
xx
Storey RF. Curr Pharm Des. 2006;12:1255-59.

Benefit
Harm
Adapted from presentation by Dr. Barbara Evans, ASCPT Annual Meeting (2010)
Frequency of various responses in the RCT treated population
Mixed Benefit and Harm
Small benefit
Neither harm or benefit --
Nonresponders(
Harm Without Benefit
Large Benefit with little harm
Ma
gnitude
Green = Benefit
Red = Harm
Yellow = Mixed Benefit and Risk
Silver = Neither Benefit or Risk
Distribution of Individual Response Rates To
Medicines

Variable Response to Clopidogrel
24 hrs after 300 mg Clopidogrel
Gurbel PA et al. Circulation 2003; 107: 2908-2913
10
20
≤ -30
(-30,-20)
(-20,-10)
(-10,0)
(0,10)
(10,20)
(20,30)
(30,40)
(40,50)
(50,60)
>60
Platelet aggregation before and after Clopidogrel (%)
Patients
(%
)
“Resistance” = 31% N = 96, Elective PCI
“Resistance” = ≤ 10% platelet aggregation

Persistent Variability in Platelet Inhibition
(MPA) With High Dose Clopidogrel
von Beckerath N, et al. Circulation 2005;112(19):2946-2950
AD
P (
20
µm
ol/L
)-In
duced
Ag
gre
ga
tio
n (
%)
12
0
10
0
8
0
6
0
4
0
2
00
300 mg 600 mg 900 mg
P=0.004 P=0.39
P=0.001
MPA 4 Hours after dosing
MPA=Maximum Platelet Aggregation
Clopidogrel Dose
150 mg/day 75 mg/day0
20
40
60
80
100
120P < 0.001

Pharmacodynamic Non-response to Clopidogrel is Associated With an Increase in Ischemic Events
MYONECROSIS/ELEVATED ENZYME
MYOCARDIAL INFARCTION
CARDIOVASCULAR DEATH
STENT THROMBOSIS
Hochholzer 2006COMPOSITE ISCHEMIC ENDPOINTS
◄
1 10 100
3.3802 0.5Buonamici 2007 10.5804 2.7Trenk 2008 6.0765 2.0Geisler 2006 22.7363 5.6Suh 2006 7.3348 1.9Cuisset JACC 2006 31.0292 3.0Patti 2008 30.0160 10.0Angiolillo 2008 37.8173 13.2Cuisset JTH 2006 39.0106 4.0Bliden 2007 72.0100 9.0Matetzky 2004 47.060 2.0
Trenk 2008 1.3765 4.6Gori 2008 2.6746 13.3Buonamici 2007 2.3804 8.6Wenewaser 2005 31.273 25.0Klamroth 2004 36.740 90.0
Buonamici 2007 1.4804 8.6Geisler 2006 2.9363 18.2
Geisler 2006 1.2363 4.5
Lev 2006 17.3150 32.4
N Responders Non-respondersEvent rate
Favors Non-responders Favors Responders
Odds Ratio (95% CI)
►
►

Criteria for Clinical Biomarkers
• Strategic
– Clear Objective/Deliverable
• Biologic understanding
• Technologic Capabilities
• Clinical Relevance
• Regulatory
• Implementation
??

Criteria Clinical Biomarkers: Clear Strategy
Prodrug Conversion
to active
metabolite
(PK)
Platelet
response
(PD)
Clinical
response
CYP
Genotypes
• Does CYP variation effect generation of AM? PD?
• If so, does this affect clinical outcome rates?
•Efficacy: increased cardiovascular event rate in those unable to
effectively generate active metabolite.
• Bleeding: decreased bleeding in those unable to generate AM.

Criteria for Clinical Biomarkers: Biology
Active Metabolite Formation
Farid NA et al. Drug Metab Dispos 2007;35(7):1096-1104Rehmel JL et al. Drug Metab Dispos 2006;34(4):600-607Williams ET et al. Drug Metab Dispos 2008;36(7):1227-1232
Plavix® package insert, 2008Kurihara A et al. Drug Metab Rev 2005;37(S2):99 Tang M et.al. J Pharmacol Exp Ther 2006;319(3):1467-1476
Prasugrel
S
N
F
O
OCH3
O
N
F
O
HS
HOOC
Gut CYPs
(3A, 2C9, 2C19)
Clopidogrel
S
N
Cl
OCH3O
Prodrug
Thiolactone
metaboliteCl
N
OCH3O
S
O
Liver CYPs
(2C19, 1A2, 2B6)
Active
metaboliteN
Cl
OCH3O
HS
HOOC
Liver CYPs
(3A, 2B6, 2C19, 2C9)
EsterasesOHO
N hCE1
(mainly liver)
S
N
F
O
O
Esterases hCE2 (mainly gut)
Liver CYPs
(3A, 2B6, 2C9, 2C19)
hCE1
Inactive
Acid
Metabolite
(85% of
parent)

Translation into Star Allele Nomenclature
eg. CYP2C19 *2
54 Different Allele Calls (“normal” by default)
48 DNA Variants
Daly TM et al. Clin Chem 2007;53(7):1222-1230
Criteria for Clinical Biomarkers:
Technological Capabilities6 Genes: CYP 3A4/5, 2B6, 2C19, 2C9, 1A2
Genetic Variation: SNPs, in/del, STR
Predicted Genetic Functional Group
Extensive
Metabolizers
(EM)
Reduced
Metabolizers
(RM)
For 3A5 EM = EM + IM and RM = PM
For 2C19 the *17 necessitated a UM group for *1/*17. EM = UM + EM
Intermedite
Metabolizers
(IM)
Poor
Metabolizers
(PM)
Extensive
Metabolizers
(EM)
Close SL et al. Eur Heart J 2008;29(S1):759
Comparison by
predicted
metabolic function

Investigation in Healthy Subjects

• Model-based mean estimates and 95% confidence intervals for genetic effects in carriers vs. non-carriers of reduced function alleles
on the PK and PD parameters of clopidogrel and prasugrel in 346 healthy subjects (includes LD and MD data)
P value
-32.4 0.00003
-6.8 0.30
-15.7 0.017
5.6 0.70
11.2 0.78
-6.1 0.031
-5.3 0.14
-0.4 0.45
-0.8 0.41
-3.5 0.23
CLOPIDOGREL
CYP Gene
2C19
2C9
2B6
3A5
1A2
PRASUGREL
CYP Gene
2C19
2C9
2B6
3A5
1A2
-15
Pharmacokinetics (PK) Pharmacodynamics (PD)
-10 -5 0 5 10 15-40 -20 200-50 -30 -10 3010
P value
-9.0 0.00027
-0.6 0.43
-5.7 0.006
7.5 0.99
0.5 0.55
-1.3 0.31
-1.7 0.21
-0.6 0.33
1.3 0.81
-1.6 0.18
% Difference
In AUC0-t
Absolute
difference
in ∆MPA
Relative Percent Difference in AUC0-t Absolute Difference in ∆MPA
Genetic Effects on Pharmacokinetic and
Pharmacodynamic Parameters

Does the effect look dominant? Additive?
Is the genetic effect observed for both
loading doses and maintenance doses?
.

CYP2C19 Effect on Exposure and Platelet Aggregation Following Clopidogrel LD and MD
Percent Reduction in AUC0-t
CYP2C19 LD 300mg LD 600mg MD 75mg
IM vs EM
PM vs EM
P Value
-26.1
-55.2
<0.001 (n= 89)
-29.9
NA
0.047 (n = 42)
-30.7
-45.6
0.0023 (n = 87)
Absolute Decrease in ΔMPA
CYP2C19 LD 300mg LD 600mg MD 75mg
IM vs EM
PM vs EM
P Value
-10.6
-19.3
0.011 (n = 180)
-6.3
NA
0.024 (n = 155)
-9.1
-28.7
<0.001 (n = 197)
EM=extensive metabolizer; IM=intermediate metabolizer; PM=poor metabolizer
Mega J et al. NEJM 2009;360(4):354-362
Investigations in Patients

Is the genetic effect consistently
observed?
In patients with coronary artery disease
In those receiving a 600 mg loading doses

-40 -20 0 20 40
Difference in VASP-PRI
(EM - RM)
Loading Dose
24 ± 4 hr
-40 -20 0 20 40
Difference in VASP-PRI
(EM - RM)
Maintenance Dose
Day 14 ± 3 day
-40 -20 0 20 40
Difference in VASP-PRI
(EM - RM)
Maintenance Dose
Day 29 ± 3 day
Ratio of AUC
(RM/EM)
0.4 0.8 1.2 1.6
Loading Dose
24 ± 4 hr
CYP2C19
CYP2B6
CYP2C9
CYP3A5
CYP2C19
CYP2B6
CYP2C9
CYP3A5
Prasugrel
Clopidogrel
AUC=area under the concentration-time curve
EM=extensive metabolizer; RM=reduced metabolizer
PRI=platelet reactivity index; VASP=vasodilator-stimulated phosphoprotein
Pharmacokinetic and Pharmacodynamic
Responses for Other Cytochrome P450 Genes
Varenhorst C et al. Eur Heart J 2009;30(14):1744-1752

-2.5
-2.0
-1.5
-1.0
-0.5
0.0
0.5
EM EMRM RM
Prasugrel Clopidogrel
Lo
g A
UC
(0-∞
)(m
M●h
)
*
**
*p=0.6361 vs. prasugrel EM
**p=0.0015 vs. clopidogrel EM
AUC=area under the concentration-time curve;
EM=extensive metabolizer; LD=loading dose;
RM = reduced metabolizer
Box represents median, 25th, and 75th
percentiles
Whiskers represent the
most extreme values within
1.5 times inter-quartile range of the box
Clopidogrel - Significantly
lower exposure to active
metabolite in CYP2C19 RM
Prasugrel - No relationship
between exposure and
CYP2C19 metabolizer status
Exposure to prasugrel’s active
metabolite was higher when
compared to clopidogrel
Varenhorst C et al. Eur Heart J 2009;30(14):1744-1752
Active Metabolite Exposure to Prasugrel 60 mg and
Clopidogrel 600 mg LD by CYP2C19 Function

Is the genetic effect consistently
observed?
For clinical outcomes
• Efficacy
• Safety
No significant genetic effect observed for bleeding. The
genetic bleeding analysis was underpowered .
Major bleeds: less than 40% power to detect a HR of 2.0
Maj/Min: 60% to detect a HR of 2.0

N=1,455Reduced n=407 (28%) Extensive n=1,048 (72%)
Hazard Ratio 0.89
(95% CI 0.60 - 1.31)
P=0.27
9.8%
8.5%
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
0 30 90 180 270 360 450
Days After Randomization
CV
Dea
th, N
on
fata
l MI,
or
Non
fata
l S
troke
(%
)
Extensive
Reduced
Days After Randomization
1.0%
0.5%
0
1
2
3
4
0 30 90 180 270 360 450
Definite
or
Pro
ba
ble
Ste
nt T
hro
mb
osis
(%
)
Hazard Ratio 0.58
(95% CI 0.13 - 2.69)
P=0.48
Extensive
Reduced
N=1,379Reduced n=379 (27%) Extensive n=1,000 (73%)
No Increased Rate of Primary Endpoint or Stent Thrombosis
in ACS Patients With Reduced Metabolism Variant of
CYP2C19 Treated with Prasugrel – TRITON-TIMI 38
Mega et al. Circulation. 2009;119:2553-2560.

Mega JL, et al. New Engl J Med 2009;360(4):354-362
N=1,389Reduced n=375 (27%) Extensive n=1,014 (73%)
N=1,459Reduced n=395 (27%) Extensive n=1,064 (73%)
Higher Rate of Primary Endpoint and Stent Thrombosis
in ACS Patients with Reduced Metabolism Variant of
CYP2C19 Treated With Clopidogrel – TRITON-TIMI 38
Days After Randomization
0.8%
2.6%
0
1
2
3
4
0 30 90 180 270 360 450
Hazard Ratio 3.09
(95% CI 1.19 - 8.00)
P=0.02
Definite
or
Pro
ba
ble
Ste
nt T
hro
mb
osis
(%
)
Extensive
Reduced8.0%
12.1%
Days After Randomization
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
0 30 90 180 270 360 450
Hazard Ratio 1.53
(95% CI 1.07 - 2.19)
P=0.01
Extensive
Reduced
CV
Dea
th, N
on
fata
l MI,
or
Non
fata
l S
troke
(%
)

26
Primary Clinical Outcome by CYP2C19 for
Clopidogrel: TRITON-TIMI 38
4266.01
EM = Extensive Metabolizer, IM = Intermediate Metabolizer, PM = Poor Metabolizer
30 90 180 270 360 450
Hazard Ratio: PM vs. EM, 1.35
(95% CI, 0.49-3.69)
Hazard Ratio: IM vs. EM, 1.55
(95% CI, 1.07-2.25)
P=0.017
P=0.029 P=0.038
Days from Randomization
0
2
4
6
8
10
12
14
0
CV
De
ath
, N
on
fata
l M
I,or
Nonfa
tal S
troke (
%) IM
EM
PM

Genetics and Cardiovascular Event Rates
0.1 1 10 20
Shuldiner et al, JAMA 2009
Mega et al, N Engl J Med 2009
Simon et al, N Engl J Med 2009 ^
Sibbing et al, Eur Heart J 2009
Anderson et al, J Am Coll Cardiol 2009
Mega et al, Circulation 2009 ^^
429
1477
2208
2485
1250
9684
2.42 (1.18-4.99)
1.53 (1.07-2.19)
1.98 (1.10-3.58)
1.15 (0.082-1.61)
1.50 (1.00-2.24)
1.61 (1.28-2.02)
Hazard Ratios
Collet et al, Lancet 2009
Giusti et al, Am J Cardiol 2009
Bhatt et al, TCT 2009 ^
259
772
4862
3.69 (1.69-8.05)
2.70 (1.00-8.42)
2.38 (1.14-5.00)
0.5 5
Study HRN
^ *2/*2 vs. wt/wt ^^ meta analysis
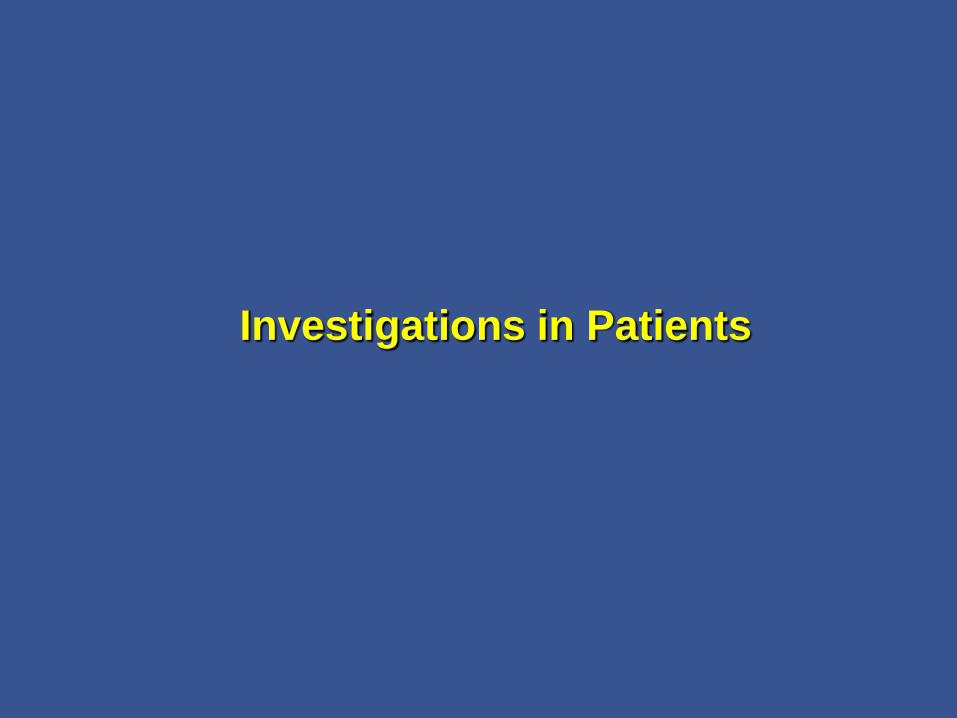
Stent Thrombosis
0.1 1 10 20
Study N
Mega et al, N Engl J Med 2009
Sibbing et al, Eur Heart J 2009
Collet et al, Lancet 2009
Giusti et al, Am J Cardiol 2009
Trenk et al, J Am Coll Cardiol 2008 *
Mega et al, J Am Coll Cardiol 2009 ^^
1477
2485
259
772
797
5772
3.09 (1.19-8.00)
3.81 (1.45-10.02)
6.20 (1.81-20.00)
3.43 (1.01-12.78)
3.70 (1.40-9.60)
2.76 (1.77-4.30)
Hazard Ratios
HR
^^ meta analysis

Criteria for Clinical Biomarkers
• Strategic
– Clear Objective/Deliverable
• Biologic understanding
• Technologic Capabilities
• Clinical Relevance
• Regulatory
• Implementation
??

Criteria for Clinical Biomarkers
Regulatory Decision Making
What constitutes substantive evidence? Obligations for labeling?
• Efficacy, lack of efficacy, safety
• Clinical Studies
Randomized stratified
Prospective
Retrospective
Observational/Community Based
• Biological Plausibility
• Modeling
Genetic labeling both in the European and US labels

Criteria for Clinical Biomarkers
Is this information clinically relevant?
• Factors influencing
Magnitude of Effect
Available treatment options
Clinical condition
Population subgroups
• Patient characteristics such as age, weight, gender
• Co-morbid conditions
• Ethnicity
• etc etc
• Environmental exposures
• Concomitant medications, smoking, etc etc
Will clinical guidelines and practice be influenced?

Applying Clinical Biomarkers• Strategic
– Clear Objective/Deliverable
• Technologic– Information overload
– Platform challenges
• Lack of biologic understanding
• Clinical Relevance
• Regulatory
• Implementation– Medical Infrastructure
– Clinician education, understanding, and acceptance
– Pharmacoeconomic case
??

Implementation: The Clinical Information Problem
Annals of Surgery • Volume 250, Number 4, October 2009
Hypothetical number of
facts potentially
relevant in making a
typical clinical decision.
Ever-increasing accumulation of knowledge promises to rapidly exceed
human cognitive limits in medical decision-making.
The magic number seven, plus or minus two:limits on our capacity for processing information
Miller GA. Psychological Review 1956;63(2):81-97

Information Overload
“I’m sorry. It appears Dr. Mitchell won’t beaccepting any more information today.”
Implementation: The Clinical Information Problem
“As this information overload increases, truly personalized medicine will
only succeed if a multitude of factors can be effectively distilled along
relevant dimensions of clinical decisions.”

Thank you!
The Meeting Organizers
The TIMI Group
DS Colleagues
Lilly
• Prasugrel Team
• PGx and Translational Medicine
• Drug Disposition
• Statistics
• IT
• Regulatory
• GSIC
William Macias
Lei Shen
Brian Moser
Richard Hockett
Michael Man
Kathy Ruiz
Elizabeth Bearby
John Brandt
Nancy Bauer
Hollins Showalter
Baoguang Huang
Lee O’Brien

Regulatory Labels

Prasugrel Summary of Product
Characteristics (FDA and Eur Med Agency)
5.2 Pharmacokinetic properties
Metabolism
In healthy subjects, patients with stable atherosclerosis,
and patients with ACS receiving Efient, there was no
relevant effect of genetic variation in CYP3A5, CYP2B6,
CYP2C9, or CYP2C19 on the pharmacokinetics of
prasugrel or its inhibition of platelet aggregation.

Prasugrel – Boxed Warning
Plavix Label – US Boxed Warning
WARNING: DIMINISHCED EFFECTIVENESS IN POOR METABOLIZERS
See full prescribing information for complete boxed warning
Effectiveness of Plavix depends on activation to active metabolite by the
cytochrome P450 (CYP) system, principally CYP2C19 (5.1)
Poor metabolizers treated with Plavix at recommended doses exhibit
higher cardiovascular event rates following acute coronary syndrome
(ACS) or percutaneous coronary intervention (PCI) than patients with
normal CYP2C19 function (12.5)
Tests are available to identify a patient’s CYP2C19 genotype and can be
used as an aid in determining therapeutic strategy (12.5)
Consider alternative treatment or treatment strategies in patients
identified as CYP2C19 poor metabolizers (2.3, 5.1)
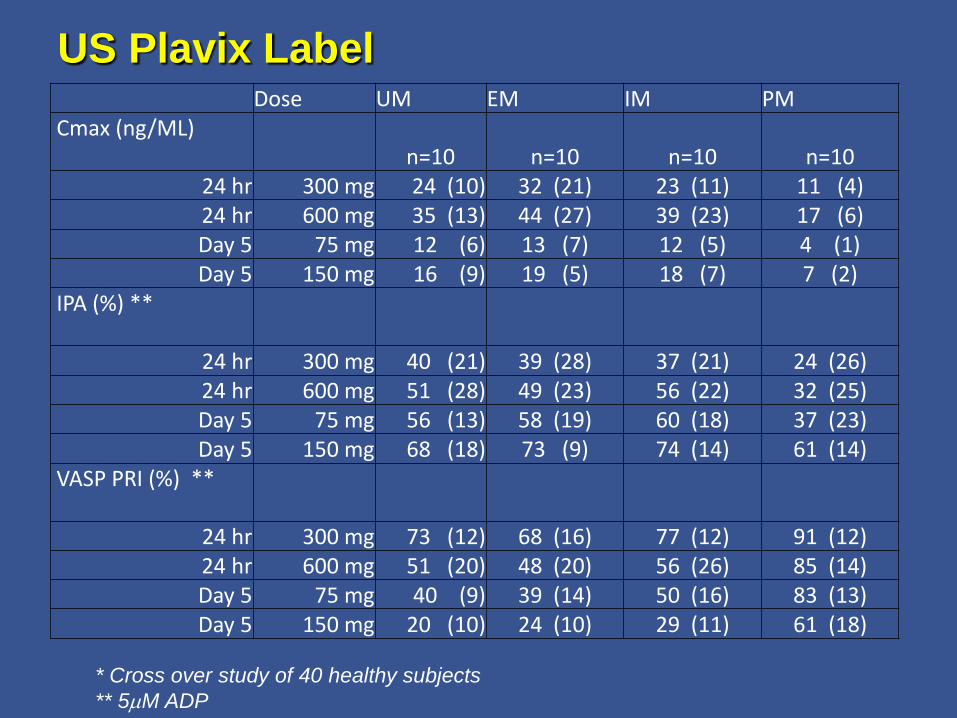
US Plavix LabelDose UM EM IM PM
Cmax (ng/ML)n=10 n=10 n=10 n=10
24 hr 300 mg 24 (10) 32 (21) 23 (11) 11 (4)24 hr 600 mg 35 (13) 44 (27) 39 (23) 17 (6)Day 5 75 mg 12 (6) 13 (7) 12 (5) 4 (1)Day 5 150 mg 16 (9) 19 (5) 18 (7) 7 (2)
IPA (%) **
24 hr 300 mg 40 (21) 39 (28) 37 (21) 24 (26)24 hr 600 mg 51 (28) 49 (23) 56 (22) 32 (25)Day 5 75 mg 56 (13) 58 (19) 60 (18) 37 (23)Day 5 150 mg 68 (18) 73 (9) 74 (14) 61 (14)
VASP PRI (%) **
24 hr 300 mg 73 (12) 68 (16) 77 (12) 91 (12)24 hr 600 mg 51 (20) 48 (20) 56 (26) 85 (14)Day 5 75 mg 40 (9) 39 (14) 50 (16) 83 (13)Day 5 150 mg 20 (10) 24 (10) 29 (11) 61 (18)
* Cross over study of 40 healthy subjects
** 5mM ADP

Clopidogrel, EU update September 2009
PHARMACOLOGICAL PROPERTIES
Pharmacokinetic properties
Pharmacogenetics
• Added subsection describing involvement of CYP2C19 in metabolic
conversion to clopidogrel active metabolite and the presence of CYP2C19
allelic variation, with CYP2C19*2 and CYP2C19*3 alleles corresponding
to reduced metabolism
• Includes a table from Xie et al1 (not actually cited in the spc) describing
CYP2C19 genotype frequencies conferring extensive, intermediate and
poor metabolism across White, Black and Asian populations
• Describes the association between CYP2C19 genotype and clopidogrel
treatment outcome and cites 2 post-hoc clinical trial analyses and 5
cohort studies
• Adds statement that pharmacogenetic testing can identify genotypes
associated with variability in CYP2C19 activity and that there may be
genetic variants of other CYP450 enzymes with effects on the formation
of clopidogrel active metabolite
• Adds statement that prevalence of CYP2C19 alleles that result in
intermediate and poor CYP2C19 metabolism differs according to
race/ethnicity 1Xie, et al. Annu Rev Pharmacol Toxicol 2001; 41: 815-50

Clopidogrel, EU update September 2009
PHARMACOLOGICAL PROPERTIES
Pharmacodynamic properties
• Added statement “Because the active metabolite is formed by CYP450
enzymes, some of which are polymorphic or subject to inhibition by other
drugs, not all patients will have adequate platelet inhibition.”
CLINICAL PARTICULARS
Posology and method of administration
• Added PGx“CYP2C19 poor metaboliser status is associated with
diminished response to clopidogrel. The optimal dose regimen for poor
metabolisers has yet to be determined.”
Special warnings and precautions for use
• Added text regarding association between genetically reduced
CYP2C19 function and lower systemic exposure to clopidogrel active
metabolite, diminished antiplatelet response, and “generally” higher
cardiovascular event rates following myocardial infarction compared to
patients with normal CYP2C19 function
• Use of drugs that inhibit CYP2C19 is discouraged, stating that
“concomitant use of Proton Pump Inhibitors should be avoided unless
absolutely necessary”