Embed Size (px)
Citation preview

8/9/2019 Pharmacoeconomics Principles, Methods and Economic Evaluation of Drug Therapies
http://slidepdf.com/reader/full/pharmacoeconomics-principles-methods-and-economic-evaluation-of-drug-therapies 1/8
Vol-2/Issue-5/Sept-Oct 2013 PhTechMed
ISSN: 2278-1099
www.pharmtechmedica.com
362
Pharmacoeconomics: Principles, Methods and Economic Evaluation of Drug Therapies
Sumit Kumar, Ashish Baldi*
*Department of Quality Assurance, I.S.F. College of Pharmacy, Moga, (Punjab), India
AbstractPharmacoeconomics identifies, measures, and compares the costs and consequences of drug therapy to healthcare systems and society.
Due to the high pricing of drug, it is very essential in pharmaceutical industry, government, and in the private sector for comparing
various cost consequences. This branch of health care economics offers important guidance for the management of limited
health care resources and medical practice. As a consequence of limited financial resources, health economics, and particularlypharmacoeconomic analyses, are becoming a frequently used criterion for decision making in modern health care policy. The purpose
of this article is to provide an introduction of pharmacoeconomics, its various methods of evaluations such as cost
minimization analysis, cost benefit analysis, cost utility analysis, cost effectiveness analysis and guidelines to deliver quality care
cost effectively and also discuss challenges, limitations and applications of pharmacoeconomics.
Key Words: Cost minimization analysis, Cost benefit analysis, Cost utility analysis, Cost effectiveness analysis, Health careeconomics, Pharmacoeconomics
Introduction Pharmacoeconomics can be defined as the branch of
economics that uses cost-benefit, cost-effectiveness, cost-
minimization, cost-of-illness and cost-utility analyses tocompare pharmaceutical products and treatment strategies
(Brinsmead 2003). Pharmacoeconomics and health outcomes
research are playing an increasingly important role in
informing clinical development and market access decisions of
new innovative medicines. It mainly works on the healtheconomics which particularly focuses upon the costs and
benefits of drug therapy.
It is the part of health economics that focuses on the economic
evaluation of pharmaceuticals. Health outcomes research, and
patient-reported outcomes (PRO) in particular, aim at
understanding patient value in terms of impact of disease andits treatment on physical functioning and psychosocial
wellbeing, known also as “health-related quality of life”(HRQL). Components of pharmacoeconomics are given as
Fig.1. It is the description and analysis of the costs of drug
therapy to healthcare systems and society. The importance of
pharmacoeconomic information to healthcare decision makerswill depend upon the viewpoint from which the analysis is
conducted. Pharmacoeconomic research in the managed care
system is growing. It is currently being used to make
formulary decisions (complementing clinical data), design
disease management programs and measuring the cost-
effectiveness of interventions and programs in managed care
(Lopert 2003). The demand for and the cost of health care
are increasing in all countries as the improvement in and
sophistication of health technologies. The increase in healthcare spending is mainly because of increased life expectance,
increased technology, increased standard of living and
increased demand in health care quality and services.
Medicines form a small but significant proportion of total
health care cost. The writing of a prescription is the most
common therapeutic intervention in medicine. Cost of
medicines are growing constantly as new medicines are
marketed and are under patent law, preference of drug therapy
over invasive therapy, discovering various off label uses of
existing drugs and the irrational drug prescription.
Pharmaceutical companies have to spend a lot of money and
Address for CorrespondenceEmail ID: [email protected]
Tel No.: +91-896842384
Received: 10/08/2013
Accepted: 18/10/2013
time to market any new chemical entity as a drug to fulfill
various research requirements
(Newdy 2003). Since 1961,
pharmaceuticals are fallen under price regulation in India. Atotal of 343 drugs accounting for, 85% of the drug market was
under price control in 1979. With successive polices, the
number diminished and now a mere 15 - 20% of the drug
market is under price control. Therefore drug prices are
quickly spinning out of reach of the common man.Pharmacoeconomics adopts and applies the principles and
methodology of health economics to the field of
pharmaceutical policy (Basskin 1998). Pharmacoeconomic
evaluation therefore makes use of the broad range of
techniques used in health economics evaluation to the specific
context of medicines management.
Figure 1: Components of pharmacoeconomics
Pharmacoeconomics: Needs and Challenges
Multi-factorial Variability of Drug Pricing
Enumerable factors affect the prices of drug; some of them are
as follows:i.
The sector in which medicines are purchased: The price is
often higher in the private sector due to distilentor’s costs
and profiteering.ii.
The types of procurement agent: e.g. different prices may
be paid for the same product by a public sector purchaser,
such as Ministry of Health (Garber 2004).
iii.
The distribution route. A patient who purchases a medicine
at a hospital pharmacy may have to pay more if the hospital
pharmacy purchased the product from a local wholesalerthan if it has been purchased by tender and supplied
through public health sector distribution system10
. Many
times hospital pharmacy may have limited stock of the
generic drugs which one is cheaper than the branded drugsprescribed to the patient on routine basis and patient has to
purchase the branded drugs in the emergency condition.

8/9/2019 Pharmacoeconomics Principles, Methods and Economic Evaluation of Drug Therapies
http://slidepdf.com/reader/full/pharmacoeconomics-principles-methods-and-economic-evaluation-of-drug-therapies 2/8
Vol-2/Issue-5/Sept-Oct 2013 Baldi et al.,
www.pharmtechmedica.com 363
iv.
The patient status: The price of patented medicine is often
higher than that of their generic equivalent at least whilethe patient is in force (Moayyedi et al 2004).
Many other factors influence the total cost of drugs is as
follows:
• Prices of patented, non-patented and generic drugs;
• Retail and wholesale mark-ups,
• Pharmacists' professional fees,
• Changes in the composition of total population, e.g.
proportion of older persons,
• Changes in prescribing habits of physicians,
• Changes in the utilization of drugs, i.e. number of drugs
used per patient,
• Trends towards using newer drug therapy instead of other
treatments,
Need of Pharmacoeconomics
Pharmacoeconomics identifies measures and compares the
cost and consequences of pharmaceutical products and
services and describe the economic relationship involving drugresearch, drug production distribution, storage, pricing and
used by the people (Rawlins et al 2004). It runs through the
thread of our socioeconomic system, which regulates andinfluences all the sectors involved in pharmaceuticals.
The demand for and the cost of health care are increasing in all
countries as the improvement of health technologies. All overthe world, patients are affected by high price of medicines. In a
developing country like India, 85% of total health expenditure
is financed by house-hold out of pocket expenditure. Many
poor people frequently face a choice between buying
medicines or buying food or other necessities due to limited
resources and high pricing of drug (Russell 1996). So medicine
prices do matter. Pharmacoeconomics has become more
important over the past 20 years, due to an increases emphasis
on efficient drug therapies for disease, which increase health
cost etc.Pharmacoeconomics is a subdivision of health economics and
results from that discipline coming of age through
consolidation to diversification (Siegel 1996). Health
economics, as a branch of economics is itself relatively young.
Basically the pharmacoeconomics is needful in following
manner:
• In Industry- Deciding among specific research anddevelopment alternatives.
• In Government- Determining program benefits and prices
paid.
• In Private Sector- Designing insurance benefit coverage.
Pharmacoeconomic Challenges
This is a challenging time for the pharmaceutical industry,with blockbuster drugs going off-patent, generics competition
and a pressing need for innovative medicines, associated with
rising drug development costs (Vermeulen et al 2000). The
role for pharmacoeconomics could not be timelier.
Pharmacoeconomic evaluations will be able to assist in the
development of performance based pricing and reimbursement
agreements.
The main challenges for pharmacoeconomics continue to be:
1. Establishing guidelines or standards of practice.
2. Creating a cadre of trained producers and consumers of
pharmacoeconomic work.3. Continuing education on the relevant features of this
discipline for practitioners, government officials, private sectorexecutives.
4. Stable funding to support applied pharmacoeconomic
research.
Pharmacoeconomic Evaluations
Components
Pharmacoeconomic analysis will play a central role in futureassessments of new technologies and the guidance of pediatric
care (Weinstein 1996). The components of pharmacoeconomic
analysis are given in Figure 2.
Figure 2: Components of pharmacoeconomics analysisIt is implicitly understood that reducing costs and rationing
resources is not compatible with the achievement of optimal
health outcomes. Decisions on resource allocation must be
based on comparisons of cost and benefits as much as possible
(Sackett et al 2000). In an era when resources for health and
health care are scarce, the costs of clinical decisions must be
recognized and accommodated. Pharmacoeconomic analysis is
a powerful tool for such adaptation. In this, the movement
toward outcomes research has been fueled by a number
of factors, including increasing prevalence of chronic
disease among children, the desire of patients (and their
parents) to participate in decision making, the limited
generalizability or external validity of clinical trial data(particularly for a pediatric population), evidence of wide
variation in clinical practice norms that cannot be
accounted for on the basis of evidence, growing interest
in cost containment and acceptance of the need for
accountability on the part of clinical decision makers
(Abarca 2005) and the perceived threat of cost containment
to the overall quality of patient care. The target sector and
assessment methodology adopted for pharmacoeconomic
evaluation is given as Figure 3 and Figure 4.
Figure 3: Target health care sector for pharmacoeconomic
evaluation
Aims and Objectives of Pharmacoeconomic Evaluation
Implementation of pharmacoeconomic evaluation will help to
reduce monetary burden on the consumers (by insuring
global pricing strategy) for the effective management of health
care system as the principle of pharmacoeconomic evaluation
is to make more efficient use of limited resources for
maximization of health care benefit at lower cost (Sculpher et
al 2005). In this way, it can be applied in practice to take
decisions about drug therapies.

8/9/2019 Pharmacoeconomics Principles, Methods and Economic Evaluation of Drug Therapies
http://slidepdf.com/reader/full/pharmacoeconomics-principles-methods-and-economic-evaluation-of-drug-therapies 3/8
Vol-2/Issue-5/Sept-Oct 2013 Baldi et al.,
www.pharmtechmedica.com 364
Figure 4: Nature of pharmacoeconomic assessments
The Fundamentals
Types of Cost Costs involved in pharmacoeconomic evaluation can bemainly divided into financial cost (mandatory cost) and
economic cost (resource for which no mandatory payment is
made) opportunity cost is the benefit foregone when selecting
one therapy alternative over the next best alternative (Doubilet
et al 1986). Several costs can be measured when weighing up
the cost of any invention. The first step in any cost analysis isidentification of the various costs. These can be direct, indirect
and intangible.
Direct i.e. costs from the perspective of the healthcare funder:
including staff costs, capital costs, drug acquisition costs. It
includes physicians’ fees, cost of administering the
medication, costs of treating an adverse drug reaction, etc.Indirect i.e. costs from the perspective of society as a whole:
for example, these might include loss of earnings, loss of
productivity, loss of leisure time, due to the illness, and cost of
travel to hospital etc (Drummond et al 1997). This would
include not just the patient themselves but also their family
and society as a whole.Intangible i.e. the pain, worry or other distress; which a
patient or their family might suffer. These may be impossible
to measure in monetary terms, but are sometimes captured in
measures of quality of life.
The cost can be measured in following ways:
• Cost / unit
• Cost / treatment
• Cost / person
• Cost / person / year
• Cost / case prevented
• Cost / life saved
• Cost / DALY (disability-adjusted life year)
Outcomes
The second fundamental component of a pharmacoeconomic
study is outcomes or benefits. A cost-benefit analysis
compares the costs and outcomes of alternative therapies and
the outcome is then expressed in monetary terms (Brien et al
1997). Cost-benefit analysis allows researchers to make
comparisons across a wide variety of alternatives. It compares
the costs involved in implementing a programme with the
value of the outcome. Since the endpoints are measured in
monetary terms, different endpoints can be studied, such as a
surgical procedure compared with a pharmaceutical
interventionThe expected benefits from an intervention might be
measured in:
A. “Natural” units e.g. years of life saved, strokes prevented,
peptic ulcers healed etc.
B. “Utility” units - Utility is an economist’s word for
satisfaction, or sense of well being, and is an attempt toevaluate the quality of a state of health, and not just its
quantity (Sanchez 1999). Utility estimates can be obtained
through direct measurement (using techniques such as time
trade off or standard gambles, or by imputing them from the
literature or expert opinion. They are often informed by
measures of quality of life in different disease states.
The Approach
A pharmacoeconomic evaluation may be conducted as aneconomic assessment incorporated into clinical trials
(Sanchez
1999). It is difficult to justify a pharmacoeconomic trial as a
separate, independent trial primarily due to the increase in
costs (Weinstein et al 2003). The evaluation may be done at
any time during phase I or II of the clinical trials.
The reasons for conducting a pharmacoeconomic trial include:
1. Pricing of a new drug;
2. Repricing of an old drug;
3. Convincing a drug formulatory;
4. Generation of data for promotional material; and5. Mandatory legislative requirement for drug licensing and
medical reimbursement (in some countries).
An ideal approach of economic evaluation in health café sectoris given in Figure 5.
Figure 5: An ideal approach of pharmacoeconomic evaluation
Methods of Pharmacoeconomic Evaluation
Pharmacoeconomic evaluations include any study designed to
assess the costs (resources consumed) and consequences
(clinical, humanistic) of alternative therapies The evaluation
mechanisms delineated were often helpful in demonstratingthe cost impact of innovative treatments, therefore grantingthem greater acceptance by healthcare providers,
administrators, and the public.
There are basically four types of pharmacoeconomic studies.
• Cost-minimization analysis (CMA)
• Cost-effectiveness analysis (CEA)
• Cost-utility analysis (CUA)
• Cost-benefit analysis (CBA)
Cost-Minimization Analysis (CMA)
Cost-minimization is a tool used in pharmacoeconomics and is
applied when comparing multiple drugs of equal efficacy and
equal tolerability. This is done when the outcomes are thesame for the two interventions. In this, only the input, i.e. the
cost, is considered. The option that has the least cost is
selected, e.g. if a hospital decides to introduce compulsory
prescribing of generic names of drugs instead of their brand
names, then the pharmacoeconomic evaluation of this would

8/9/2019 Pharmacoeconomics Principles, Methods and Economic Evaluation of Drug Therapies
http://slidepdf.com/reader/full/pharmacoeconomics-principles-methods-and-economic-evaluation-of-drug-therapies 4/8
Vol-2/Issue-5/Sept-Oct 2013 Baldi et al.,
www.pharmtechmedica.com 365
be done by CMA (Rawlins 1999). The objective of this method
is to select the least costly among multiple equivalentinterventions. It cannot be used to evaluate programmes or
therapies that lead to different outcomes.
CMA is a relatively straightforward and simple method for
comparing competing programs or treatment alternatives as
long as the therapeutic equivalence of the alternatives being
compared has been established. If no evidence exists tosupport this, then a more comprehensive method such as cost-
effectiveness analysis should be employed. However, CMAshows only a “cost savings” of one program or treatment over
another. Employing CMA is appropriate when comparing two
or more therapeutically equivalent agents or alternate dosing
regimens of the same agent (Tan et al 2006).
Cost Effective Analysis (CEA)
CEA is a technique designed to assist a decision-maker in
identifying a preferred choice among possible alternatives.
Generally, cost-effectiveness is defined as a series of analytical
and mathematical procedure that aid in the selection of a
course of action from various alternative approaches.CEA evaluates multiple drug treatments for the same
condition. The cost of the drug treatments are weighed against
the effectiveness of the drug (Thwaits et al 1998). The costs ofdrug treatments include acquisition costs, physician
involvement, and nursing costs for administration of the drug.
The effectiveness of drug treatment is measured in tangible
measures such as length of hospital stay, duration of treatment
required, and mortality rate. The results of a CEA are
expressed as cost/outcome for both therapies.
Pharmacoeconomic analysis should be incorporated in the
clinical trial itself. However, for the majority of drugs, CEA is
done on the basis of pre-existing data available in the medical
literature.
CEA is the most commonly applied form of economic analysis
in the literature, and especially in drug therapy (Lee et al
1991). It does not allow comparisons to be made between twototally different areas of medicine with different outcomes.
The key measure of these evaluations is the incremental cost
effectiveness ratio (ICER), which can be determined as
follows:
Incremental cost effectiveness ratio=
Cost of drug A -
Cost of drug B
Benefits of drug A -
Benefits of drug B
Cost Utility Analysis (CUA) CUA is a type of evaluation in which drugs/interventions with
different outcomes can be compared. CUA is the most
appropriate method to use when comparing programs and
treatment alternatives that are life extending with serious side
effects (e.g., cancer chemotherapy), those which produce
reductions in morbidity rather than mortality (e.g., medical
treatment of arthritis), and when HRQOL is the most
important health outcome being examined (Bootman 1995).
CUA is employed less frequently than other economic
evaluation methods because of a lack of agreement on
measuring utilities, difficulty comparing QALYs (quality
adjusted life years) across patients and populations, and
difficulty quantifying patient preferences.
Pharmacoeconomists sometimes want to include a measure of
patient preference or quality of life when comparing
competing treatment alternatives. CUA is a method for
comparing treatment alternatives that integrates patient
preferences and HRQOL. CUA can compare cost, quality, and
the quantity of patient-years. Cost is measured in dollars, and
therapeutic outcome is measured in patient-weighted utilities
rather than in physical units (Hepler et al 1990).Often the
utility measurement used is a quality-adjusted life year
(QALY) gained. QALY is a common measure of health statusused in CUA, combining morbidity and mortality data. Results
of CUA are also expressed in a ratio, a cost-utility ratio (C:U
ratio). Most often this ratio is translated as the cost per QALY
gained or some other health-state utility measurement. The
preferred treatment alternative is that with the lowest cost per
QALY (or other health-status utility). QALYs represent thenumber of full years at full health that are valued equivalently
to the number of years as experienced. For example, a full yearof health in a disease free patient would equal 1.0 QALY,
whereas a year spent with a specific disease might be valued
significantly lower, perhaps as 0.5 QALY, depending on the
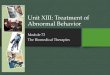
disease (Eisenberg 1989). An example of QALY measurement
for two different treatment approaches is given in Figure 6
.
Figure 6: Calculating QALYs - A simple example
Cost Benefit Analysis (CBA)
CBA is the most comprehensive and the most difficult of all
economic evaluation techniques. In this technique, the benefits
are also assigned a monetary value so that costs and benefits
can be easily compared. Thus, totally different interventions
can be compared, making it a useful tool (like CUA) forresource allocation by policy-makers. It is a basic tool thatallows for the identification, measurement, and comparison of
the benefits and costs of a program or treatment alternative.
CBA should be employed when comparing treatment
alternatives in which the costs and benefits do not occur
simultaneously. CBA also can be used when comparing
programs with different objectives because all benefits are
converted into dollars and to evaluate a single program or
compare multiple programs.
The benefits realized from a program or treatment alternative
are compared with the costs of providing it. Both the costs and
the benefits are measured and converted into equivalent dollars
in the year in which they will occur. Future costs and benefitsare discounted or reduced to their current value. These costs
and benefits are expressed as a ratio (a benefit-to-cost ratio), a
net benefit, or a net cost (Bootman et al 2005). The most
difficult and challenging part of CBA lies in calculating the
benefits in economic terms. Some benefits are easy to convert,
others need subjective judgment. CBA may ignore intangible
benefits (pain, anxiety, stress) that are difficult to express in
monetary terms (Freund et al 1992).
Analysis of Results in Pharmacoeconomic Evaluation Health economics, and particularly its branch precision healtheconomics, help us choose between two alternatives, which we
compare with regard to their clinical benefit on one hand and
their cost on the other. The users of pharmacoeconomicevaluations are not interested in the results themselves but in
where and how these results can help them for a better care of
their patients (Barner et al 2003).

8/9/2019 Pharmacoeconomics Principles, Methods and Economic Evaluation of Drug Therapies
http://slidepdf.com/reader/full/pharmacoeconomics-principles-methods-and-economic-evaluation-of-drug-therapies 5/8
Vol-2/Issue-5/Sept-Oct 2013 Baldi et al.,
www.pharmtechmedica.com 366
Health benefits and costs can be accessed from a different
viewpoint called "perspective". There are three common typesof perspectives in economic studies: a producer's perspective, a
payer's perspective and a social perspective. The perspective of
an economic assessment is important. In general, the social
perspective is the broadest and most appropriate for making
financial decision because it leads to optimal decisions but
other perspectives are also valid (Blumenschein et al 1999).
Consider the four possible results arising in a CEA given in
Fig.7. First, if costs are lower and health benefits higher forone drug relative to another, the former is said to dominate and
would be the preferred treatment. Second, the opposite applies,
i.e. the new drug is more expensive and less effective, and thus
is considered inferior and not recommended. The third andmost common case is where the new drug is both more
effective and more expensive than the standard; on the basis of
ICERs, a judgment must be made regarding whether the
additional benefits are worth the extra costs of the new drug
and, therefore, whether it is ‘cost-effective’. This might be
defined by a previously agreed ICER threshold value (Thar
1992). The fourth case is similar to the third, with the roles of
the new therapy and the standard reversed; the question now is
whether the extra benefits provided by the standard justify theadditional costs of retaining it as the preferred treatment when
the option of a new, cheaper but less effective drug exists.
Figure 7: Difference in costs
Applications of Pharmacoeconomics I.
One of the primary applications of pharmacoeconomics in
clinical practice today is to aid clinical and policy decision
making. Through the appropriate application of
pharmacoeconomics, practitioners and administrators can
make better, more informed decisions regarding the
products and services they provide (Detsky et al 1990).
Complete pharmacotherapy decisions should contain
assessments of three basic outcome areas whenever
appropriate: economic, clinical, and humanistic outcomes(ECHO). Traditionally, most drug therapy decisions were
based solely on the clinical outcomes (e.g., safety and
efficacy) associated with a treatment alternative (Kozma et
al 1993).
II.
Pharmacoeconomic data can be a powerful tool to supportvarious clinical decisions, ranging from the level of the
patient to the level of an entire healthcare system. Fig. 8
shows various decisions that can be supported using
pharmacoeconomics, including effective formulary
management, individual patient treatment, medication
policy, and resource allocation (Bungay et al 2003). Fordiscussion purposes, the application of pharmacoeconomics
to decision making is divided into two basic areas: drugtherapy evaluation and clinical pharmacy service
evaluation.
III. While the proper output of pharmacoeconomics is
information needed for making decisions on selection of
pharmaceuticals and medical devices as viewed from the
standpoint of cost-effectiveness, the techniques areapplicable in a diversity of domains (Druglis et al 1989).
IV.
Pharmacoeconomics provides precious input in studies of
product portfolios by pharmaceutical firms and
manufacturers of medical devices. Because QALYs may be
equated to pharmaceutical value per se, the aggregate
QALYs of a firm's products may be equated to its corporatevalue (Drummond at al 1997).
V.
Healthcare practitioners, regardless of practice setting, canbenefit from applying the principles and methods of
pharmacoeconomics to their daily practice settings.
Applied pharmacoeconomics is defined as putting
pharmacoeconomic principles, methods, and theories intopractice to quantify the value of pharmacy products and
pharmaceutical care services used in real-world
environments
(Cox 2003).Today’s practitioners
increasingly are required to justify the value of the products
and services they provide. Applied pharmacoeconomics
can provide the means or tools for this valuation.VI.
Pharmacoeconomic analysis is important since payers such
as third-party payers or government/private health plans
utilise them when determining whether to reimburse aclaim. These results in decreased adherence, lack of
prescription filling, decreased physician visits and
increased emergency room care (Sanchez 1994).
Figure 8: Decisions for pharmacoeconomic applications
Guidelines for Pharmacoeconomics Evaluations
In 1999, the Health Care Insurance Board published the
‘Dutch Guidelines for Pharmacoeconomic Research’. TheseGuidelines were updated in 2005 and published in the report
‘Guidelines for Pharmacoeconomic Research; Evaluation and
Actualisation. The guidelines are intended for designing,
conducting and reporting pharmacoeconomic research, but areapplicable to economic evaluations in general within the field
of health care (Schrand et al 2001).
Guideline 1 - The perspective of the evaluationThe pharmacoeconomic evaluation should be performed and
reported from a societal perspective, in which all costs and
benefits are included, irrespective of who actually bears the
costs or receives the benefits (Armstrong et al 2003).
Guideline 2 - Choice of comparative treatment/ indicationThe drug for a certain indication should be compared with the
standard treatment, or if that does not exist, the usual
treatment. This can either be a medicinal or a non-medicinal
treatment. The standard treatment is the treatment regarded in
daily practice as first-choice, for which effectiveness has beenproven.
Guideline 3 - Analytical techniqueIf the improvement in quality of life forms an important effect
of the drug being assessed, then it is necessary to carry out a

8/9/2019 Pharmacoeconomics Principles, Methods and Economic Evaluation of Drug Therapies
http://slidepdf.com/reader/full/pharmacoeconomics-principles-methods-and-economic-evaluation-of-drug-therapies 6/8
Vol-2/Issue-5/Sept-Oct 2013 Baldi et al.,
www.pharmtechmedica.com 367
CUA. If this is not the case, then CEA has to be carried out. If
the manufacturer does not expect the drug to have an addedtherapeutic value, nor that it will be mutually replaceable with
(a) different drug(s), then a CMA can be carried out.
Guideline 4 - Time horizonThe time horizon of a pharmacoeconomic evaluation must be
such that it enables valid and reliable statements to be made
regarding the effects and costs of the treatments beingcompared. This includes both intended and unintended effects
and costs e.g. side effects (Milne 1994).Guideline 5 - Cost identification, measurement and
evaluationWhere possible, the Health Care Insurance Board’s ‘Manual
for cost research’ should be applied for the identification,measurement and evaluation of costs. The aim of using this
manual is to promote the uniformity and the standardization of
cost measurement and evaluation in pharmacoeconomic
evaluations.
Guideline 6 - Assessing quality of life and QALYsIf improvement in the quality of life is an important effect ofthe drug being assessed, then a CUA should be performed.
When carrying out a cost-utility analysis, assessments for
health states of patients need to be determined in order tocalculate the number of 'quality-adjusted life-years’ (QALYs).
The assessments of the health states and the survival data need
to be reported separately. The combination of these two
elements into a QALY should be presented clearly (Barr et al
1996).
Guideline 7 – ModelingIn order to be able to support decision-making, the model must
be transparent: preferably based on 'peer-reviewed'
publications and with a user-friendly electronic version. In
order to make a model transparent, the model must be as
simple as possible, and obviously it must include all the most
important processes. Modelling should be supplementary, and
in line with pharmacoeconomic analysis of the clinical studies(preferably ones that have already been published).
Guideline 8 - Incremental analysis
The cost effectiveness of the treatments to be compared is
presented by reporting the incremental effects and costs
between the treatments.
Guideline 9 - Discounting future effects and costsIf data on effects and costs are collected over a period longer
than one year, then the effects and costs need to be discounted
after the first year (Touchette et al 2003). In the primary
analysis the costs should be discounted at a constant discount
rate of 4%. Future effects should be discounted at a constant
discount rate of 1.5%.
Guideline 10 - Uncertainty analysisDefinitive estimate of the costs, effects and a cost-
effectiveness ratio, a number of methodological choices have
been made and a number of parameters have been estimated.
In a sensitivity analysis it is preferred to first formulate an
upper and a lower limit for each estimate reflecting the
uncertainty margins
(Bennett et al 1997). A multivariate
sensitivity analysis examines the effect of simultaneous
alterations in various variables thereby taking into account the
correlation between these variables. When the chance
distribution within these values is known, as well as the
extreme values of the parameters, then simultaneous ‘random’
draws can be used to determine a new estimate of each
parameter.
Guideline 11 - Use of expert panelIn the pharmacoeconomic evaluation, the manufacturer first
needs to demonstrate that the study data are missing. TheHealth Care Insurance Board needs to have access to this
information relating to the expert panel in order to determine
the composition and independence of the expert panel.Furthermore, this information provides insight into the way in
which consensus is reached within the expert panel. Finally,
the data used in the pharmacoeconomic evaluation provided by
the expert panel should be clearly documented in the
reimbursement file (Kim et al 1997).
Conclusion
In the era of rising medical costs, the science focuses on ‘value
for money’. For this, there is an urgent need to develop ascience based on study of cost and consequences of drug
therapy to healthcare system and society (Younossi et al 1990).
Pharmacoeconomics is that science, although still testing its
methodologies which provide the mean to qualify the value ofpharmacotheraphy through balancing costs and outcomes. By
understanding the principal, methods and applications of
pharmacoeconomics, healthcare professionals will be prepared
to make better, motre informed decisions the ultimately
represent ther interest of the patient, the healthcare system, and
society. Hence pharmacoeconomics is also relevantsocioeconomics as it relates patients, society and economy, to
drug therapy. In today’s healthcare settings, various
pharmacoeconomic methods can be applied for effectiveformulary management, individual patient treatment,
medication policy determination, and resource allocation.
Economic, humanistic, and clinical outcomes should be
considered and valued using pharmacoeconomic methods, to
inform local decision making whenever possible.
The perspective of a pharmacoeconomic evaluation is
paramount because the study results will be highly dependent
on the perspective selected. When evaluating published
pharmacoeconomic studies, factors should to be considered are
study objective, study perspective, pharmacoeconomic
method, study design, choice of interventions, costs and
consequences, discounting, study results, sensitivity analysis
and study conclusions (Schecter 1993).Majority of pharmacoeconomic guidelines provide only
general and vague recommendation in many areas may be
because of no consensus among the developers and challenge
of sustenance for relatively young science of
pharmacoeconomics. Therefore strict guidelines having
uniform global standards should be formulated by an
independent body comprising of people from academia,
industry and health authorities. Upon implementation it would
be helpful towards prescribing a rational drug therapy and
pharmacist, the bridge between patients and doctors, will
dispense as well as help in purchasing drugs for hospital
pharmacies. This would also help in reducing the monetary
burden on institutions and public.
Acknowledgements: Authors are grateful to Mr. Praveen
Garg, ISFCP for provides necessary facilities and support.
References 1. Armstrong EP, Grauer D, Lee J, Odom T. (2003):
Sensitivity analysis. Pharmacoeconomics and Outcomes,
2nd Ed. Kansas City, MO: American College of Clinical
Pharmacy, pp.231–245.
2. Abarca J (2005): Assessing Principles of
Pharmacoeconomics. Int. Jour. Pharm. Tech, 23(3):76-89.
3. Akehurst R, Anderson P, Brazier J. (2000): Consensus
Conference on Guidelines on Economic Modeling in
Health Technology Assessment. Decision analytic
modeling in economic evaluation of health technologies: A
consensus statement. Pharmacoeconomics, 17: 443–444.

8/9/2019 Pharmacoeconomics Principles, Methods and Economic Evaluation of Drug Therapies
http://slidepdf.com/reader/full/pharmacoeconomics-principles-methods-and-economic-evaluation-of-drug-therapies 7/8
Vol-2/Issue-5/Sept-Oct 2013 Baldi et al.,
www.pharmtechmedica.com 368
4.
Blumenschein K, Johannesson M (1999): Use of contingent
valuation to place a monetary value on pharmacy services:An overview and review of the literature. Clin Ther
21:1402–1417.
5. Brinsmead R (2003): Use of pharmacoeconomics in
prescribing research. J Clin Pharm Ther 28:339-46
6.
Basskin L (1998): Pharmacoeconomics and the Formulary
Decision-Making process. Hospital Formulary.33:459-466.7.
Brien BJ, Heyland, Richardson SW (1997): Users’ Guides
to the Medical Literature. How to Use an Article onEconomic Analysis of Clinical Practice. JAMA,
277(22):1802-6.
8.
Bootman JL. Pharmacoeconomics and outcomes research.
(1995): Am J Health Syst Pharm, 52(3):16–19.9.
Barner J, Rascati K (2003): Pharmacoeconomics and
Outcomes, 2nd Ed. Kansas City, MO: American College of
Clinical Pharmacy, pp.115–132.
10.
Briggs A, Sculpher M (1998): An introduction to Markov
modeling for economic evaluation. Pharmacoeconomics
13:397–409.11.
Barr JT, Schumacher GE (1996): Using decision analysis
to conduct pharmacoeconomic studies. Quality of Life and
Pharmacoeconomics in Clinical Trials, 2nd Ed.Philadelphia: Lippincott-Raven pp.60-75.
12.
Bennett WG, Inoue Y, Beck JR (1997): Estimates of the
cost-effectiveness of a single course of interferon-α2b in
patients with histologically mild chronic hepatitis C. Ann
Intern Med, 127:855–865.
13. Bungay KM, Sanchez LA (2003): Types of economic and
humanistic outcomes assessments. Pharmacoeconomics
and Outcomes, 2nd Ed. Kansas City, MO: American
College of Clinical Pharmacy, pp.18–60.
14.
Bootman JL, Townsend RJ, McGhan WF (2005):
Principles of Pharmacoeconomics, 3rd Ed. Cincinnati, OH:
Harvey Whitney Books, pp.432-459.
15.
Cox E (2003): Cost-minimization analysis.Pharmacoeconomics and Outcomes, 2nd Ed. Kansas City,
MO: American College of Clinical Pharmacy, pp.103–114.
16.
Doubilet P, Weinstein MC, McNeil BJ (1986): Use and
misuse of the term “cost effective” in medicine. New Eng J
Med, 314(4):253-6.
17.
Drummond MF, Richardson SW (1997): Users’ Guides to
the Medical Literature. How to Use an Article on
Economic Analysis of Clinical Practice. 277(19):1552-7.
18.
Drauglis JR, Bootman LJ, Larson LN (1989): Current
Concepts: Pharmacoeconomics Clinical Pharmacy
87(3):45-87-93.
19.
Doubilet P, Weinstein MC, McNeil BJ (1986): Use and
misuse of the term “cost effective” in medicine. New Eng J
Med, 314(4):253-6.
20.
Drummond MF, Richardson SW (1997): Users’ Guides to
the Medical Literature. How to Use an Article on
Economic Analysis of Clinical Practice. 277(19):1552-7.
21.
Drummond MF, Stoddart GL, Torrance GW (1997):
Methods for the Economic Evaluation of Health Care
Programmes, 2nd
Ed. Oxford: Oxford University Press
pp.45-65.
22. Detsky AS, Nagiie IG (1990): A clinician’s guide to cost-
effectiveness analysis. Ann Intern Med, 113:147–154.
23.
Eddy DM. (1992): Clinical decision making: from theory
to practice. Applying cost-effectiveness analysis. The
inside story. 18:2575-82
24.
Eichler HG, Kong SX, Gerth WC (2004): Use of cost-
effectiveness analysis in health-care resource allocation
decision-making: How are the cost-effectiveness thresholdsexpected to emerge? Value Health. 7:518-528.
25.
Eisenberg JM, Glick H, Koffer H (1989):
Pharmacoeconomics: Economic evaluation ofpharmaceuticals. Pharmacoepidemiology. New York:
Churchill-Livingstone,325-350.
26. Eisenberg JM (1989): Clinical economics: A guide to
economic analysis of clinical practices. JAMA, 262:2879–
2886.
27. Freund DA, Dittus RS (1992): Principles ofpharmacoeconomic analysis of drug therapy.
Pharmacoeconomics, 1:20–32.28. Fry RN, Avey SG, Sullivan SD (2003): The academy of
managed care pharmacy format for formulary submissions:
An evolving standard- A Foundation for Managed Care
Pharmacy Task Force report. Value Health. 6:505-21.29.
Garber AM. (2004): Cost-effectiveness and evidence
evaluation as criteria for coverage policy. Health Aff., 4-
284-96.
30.
Hepler CD, Strand LM. (1990): Opportunities and
responsibilities in pharmaceutical care. Am J Hosp Pharm,
47:533–543.31.
Kozma CM, Reeder CE, Schulz RM (1993): Economic,
clinical, and humanistic outcomes: A planning model for
pharmacoeconomic research Clin Ther, 15:1121–1132.32.
Kim WR, Poterucha JJ, Hermans JE (1997): Cost-
effectiveness of 6 and 12 months of interferon-α therapy
for chronic hepatitis C. Ann Intern Med, 127:866–874.
33.
Lopert R (2003): Cost-effectiveness analysis--a technique
for decision-making at the margin. J Clin Pharm Ther
28:243-9.
34.
Lee JT, Sanchez LA. (1991): Interpretation of cost-
effective and soundness of economic evaluations in the
pharmacy literature. Am J Hosp Pharm, 48:2622–2627.
35.
Lai LL, Sorkin AL (1998): Cost-benefit analysis of
pharmaceutical care in a Medicaid population: From a
budgetary perspective. J Manage Care Pharm, 4:303–308.
36.
Moayyedi P, Mason J (2004): Cost-Utility and Cost-Benefit Analyses: How Did We Get Here and Where are
We Going? European Journal of Gastroenterology and
Hepatology, 16(6):527-534.
37.
Mullins CD, Flowers LR (2003): Evaluating economic
outcomes literature. Pharmacoeconomics and Outcomes,
2nd Ed. Kansas City, MO: American College of Clinical
Pharmacy, pp.246–273.
38. Mullins CD, Ogilvie S (1998): Emerging standardization in
pharmacoeconomics. Clin Ther, 20(60):1194–1202.
39. Milne RJ (1994): Evaluation of the pharmacoeconomic
literature. Pharmaco-economics, 6:337–345.
40.
Newby D (2003): Cost-minimization analysis--when are
two therapies equal? J Clin Pharm Ther, 28:145-50
41. Neumann PJ, Claxton K, Weinstein MC (2000): The FDA's
regulation of health economic information.” Health Aff.
19:129-37.
42. Rawlins MD, Culyer AJ (2004): National Institute for
Clinical Excellence and its value judgments. BMJ. 24:224-
7.
43. Russell LB (1996): The role of cost-effectiveness analysis
in health and medicine. Panel on Cost-Effectiveness in
Health and Medicine. JAMA, 276(14):1172-7.
44. Rawlins M (1999): In pursuit of quality: The National
Institute for Clinical Excellence. Lancet, 353:1079-1082.
45. Siegel JE (1996): Recommendations for reporting cost-
effectiveness analyses. Panel on Cost-Effectiveness in
Health and Medicine. JAMA, 276(16):1339-41.
46. Sackett D, Straus S (2000): Evidence-Based Medicine:
How to Practice and Teach JAMA, 32(1): 23-87

8/9/2019 Pharmacoeconomics Principles, Methods and Economic Evaluation of Drug Therapies
http://slidepdf.com/reader/full/pharmacoeconomics-principles-methods-and-economic-evaluation-of-drug-therapies 8/8
Vol-2/Issue-5/Sept-Oct 2013 Baldi et al.,
www.pharmtechmedica.com 369
47.
Sculpher MF, Torrance MJ (2005): Critical Assessment of
Economic Evaluation, 3rd
Ed., New York: OxfordUniversity Press, pp.44-87.
48.
Sanchez LA (1994): Pharmacoeconomic principles and
methods: An introduction for hospital pharmacists. Hosp
Pharm, 29:1035–1040.
49.
Schecter CB (1993): Decision analysis in formulary
decision making. Pharmacoeconomics, 3:454–461.50.
Schrand LM, Elliott JM, Ross MB, et al (2001): Cost
benefit analysis of RSV prophylaxis in high-risk infants.Ann Pharmacother, 35:1186–1193.
51.
Schulpher M, Fenwick E, Claxton K (2000): Assessing
quality in decision analytic cost-effectiveness models: A
suggested framework and example of application.Pharmacoeconomics, 17:461–477.
52.
Sanchez LA (1999): Applied Pharmacoeconomics:
Evaluation and Use of Pharmacoeconomic Data from the
Literature. Am J Health-Syst Pharm, 56(16):1630-40.
53.
Sanchez LA, Lee JT (2000): Applied pharmacoeconomics:
Modeling data from internal and external sources. Am JHealth Syst Pharm, 57:146-158.
54.
Touchette D, Hartung D, Grauer D, Lee J, Odom T (2003):
Markov modeling. Pharmacoeconomics and Outcomes, 2nd Ed. Kansas City, MO: American College of Clinical
Pharmacy, pp. 206–230.
55. Tan DA, Michael CY, Regier JM, Esdaile LDL (2006):
Health economic evaluation: A primer for the practicing
rheumatologist. Arthritis Rheum, 55(4): 648-56.
56. Thar A (1992): Glossary of terms used in
pharmacoeconomic and quality of life analysis.
Pharmacoeconomics, 1:151-59
57. Thwaits R, Townsend JR (1998): Pharmaco-economics in
the new millennium: A Pharmaceutical industry
perspective, Pharmacoeconomics, 13(2): 175-180.
58. Vermeulen LC, Beis SJ, Cano SB (2000) Applying
Outcomes Research in Improving the Medication UseProcess. Am J Health Syst Pharm, 57:2277-82.
59. Weinstein MC.(1996): Recommendations of the Panel on
Cost-effectiveness in Health and Medicine. JAMA,
276(15):1253-8.
60. Weinstein MC, O'Brien B, Hornberger J (2003): Principles
of good practice for decision analytic modeling in health-
care evaluation: report of the ISPOR Task Force on Good
Research Practices--Modeling Studies. Value Health,
6(1):9-17.
61. Younossi ZM, Singer ME, McHutchison JG, Shermock
KM (1990): Cost effectiveness of interferon-α2b combined
with ribavirin for the treatment of chronic hepatitis C.
Hepatology, 30:1318–1324.
62. Zupancic JA, Richardson DK, Lee K, McCormick MC
(2000): Economics of prematurity in the era of managed
care. Clin Perinatol, 27:483-497.