Embed Size (px)
Citation preview

OF THE DIRECTOR OF PUBLIC HEALTH FOR WIRRAL
2011-2012
ANNUAL REPORT

Contents
PUBLIC HEALTH ANNUAL REPORT 2011/122

PUBLIC HEALTH ANNUAL REPORT 2011/12 3
Foreword
Health need versus health service availability
Health and social care delivery must change
Tackling the causes of ill health
A new movement
4
6
10
14
22

PUBLIC HEALTH ANNUAL REPORT 2011/124
Foreword

A central theme this year is the challengeto maintain public health services in theshort term and put in place foundationsfor services that are sustainable in thelong term.
At the time of writing, early results fromthe 2011 Census suggest that there is apositive, upward trend in life expectancyfor Wirral. The population of Wirral hasalso increased in the past decade, whereit was previously predicted to decrease.Health is improving, but the seeminglyintractable differences in health outcomesbetween our most affluent and our leastaffluent communities remain.
Future funding for all public services,including public health services, is underpressure. Unless we intentionally tacklethe years of life our population live in poorhealth, we may be facing a future wherethe population’s need for health servicesconsistently outstrips the resourcesavailable to provide those services.
This highlights for me the need tounderstand within the Borough how ourresources collectively making an impact.Health, social care and preventionservices will have to become moreintegrated and focus on shared objectivesfor health outcomes. We should considerthe services available to our communitiesand look to ensure they work together,building on the strengths of what we haveto offer and making them accessible tothose who need them.
To this end, the establishment of ourshadow Health & Wellbeing Boardprovides an opportunity to strengthencollective leadership across the statutoryand voluntary sectors. It is also a place inwhich to challenge how our collectiveactivities link back to the needs of ourcommunities.
I would like to take this opportunity tothank all those across the Borough, who Ihave worked with and who have helped todeepen my understanding of thecommunity I serve. Most of all, I would liketo say thank you to all those who givetheir time freely to support those whoneed help. I have met some extraordinaryand wonderful people over the last yearand they have enriched my life as aDirector of Public Health.
Finally, I feel very fortunate to have apublic health team who have remainedpassionate and committed to their workduring a difficult year.
I hope there is much in this report thatprompts both interest and discussion aswe embrace both the challenges and theopportunities inherent in improvingWirral’s public health.
Fiona JohnstoneDirector of Public Health
PUBLIC HEALTH ANNUAL REPORT 2011/12 5
Wirral’s 2012 Public Health Annual Report (PHAR) is beingpublished during a time of heightened levels of reform activity, andthe style and content may feel different from recent years. But ouraim remains to highlight issues that impact upon the public’s healthand to recommend action that will improve it.

PUBLIC HEALTH ANNUAL REPORT 2011/126
Health need versus health service availability
PUBLIC HEALTH ANNUAL REPORT 2011/12 7
It is well recognised that the combined successes of healthcare,medicine and the development of social infrastructure in the 20thcentury have led to people living longer now than 100 years ago.In fact, life expectancy has increased from an average 48 years in1901 to 80 years in 20091.
Increased longevity comes at a pricethough. As people live longer, theirlong-term health needs grow accordingly,putting a tremendous strain on resources.Current estimates suggest there arearound 15 million people in England withat least one long-term health condition - acondition that cannot be cured but can bemanaged through medication and/ortherapy2. The most common types oflong-term conditions in the UK are heartdisease, cancers, diabetes, chronicobstructive pulmonary disease (COPD),dementia and arthritis.
Many people live with more than onelong-term condition. In some instancestheir condition can make them morevulnerable to other illness or injury (forexample, heart disease can result inincreased risk of falls, leading to fractures,anxiety and depression). Such conditionsprimarily have a significant impact onpeople’s quality of life, but a knock oneffect is that responsive and, in manycases, more frequent health and socialcare is then required. The Department ofHealth currently estimates that around70% of the current health and social carebudget is spent on long-term conditions3
and that public expenditure on long-termsocial care will rise by 94% to £15.9 billionby 20224. In Wirral, an estimated 15,000people require support with at least one‘activity of daily living’ (for example,feeding, bathing or walking) and this is setto increase to 19,000 by 20205. Althoughmuch of this support is currently provided
by family carers, it is an indication of thegrowing potential demand for more formalcare in the future.
Recent analysis in Wirral shows that heartdisease, stroke and lung and throatcancers were the most common causes ofpremature death between 2005 and 2007in both men and women, accounting for30% of premature death in men and 26%in women. Other important causes werecirrhosis of the liver in men and breastcancer in women, each contributingaround another 6% of premature death6.However, when morbidity (living withillness rather than dying from it) isconsidered, conditions arising fromalcohol use (especially in men), dementia,depression and COPD become the mostfrequently reported diseases. In terms ofthe need for longer-term health and socialservices, these conditions accounted for31% of ‘years lived with disability’ amongboth men and women in 2004, anestimated 7,000 years across the wholepopulation of Wirral.
Since the introduction of the NationalHealth Service in 1948, we have becomeaccustomed to comprehensive healthcarebeing provided whenever we need it. Wehave also become accustomed to thishealthcare keeping in step withdevelopments in technology. However, thepublic sector landscape is changingrapidly and it is likely that demand forservices will outstrip supply at a fasterpace in years to come.

PUBLIC HEALTH ANNUAL REPORT 2011/128
The situation is made worse by economicuncertainty. With pressure on publicbudgets, the NHS Chief Executive SirDavid Nicholson estimated in 2009 that upto £20 billion of savings would need to bemade by the NHS in England by 20147.Updated estimates, based on currenteconomic growth forecasts, suggest thatthis saving will in fact need to continueand increase beyond 2014, with cuts tohealth and social care spending requiredup to 20178. The combination of pressureto save money of this magnitude and theever increasing demand for servicesraises the risk of a significant funding gap.Any subsequent growth in NHS or socialcare (to keep pace with national income)would mean a virtual freeze of all otherpublic spending8. A similar gap has beendeveloping in social care for older people,albeit on a smaller scale. Between 2005and 2010, it is estimated that the gapbetween demand and expenditurewas around 9% (around £0.7 billion)and increasing9.
There has been much discussion aboutthe contribution that increasedproductivity and efficient delivery canmake in closing the current gap incapacity and demand for public servicesand current reconfigurations of servicesnationally and locally reflect this. Areaswhere savings can be made includeimproving clinical practice, minimising‘structural support’ costs, improving staffefficiency and redesigning the waypatients are cared for10. However, it isclear that without a significant change inthe way health and social care servicesare used, this gap will not be closed11.
RECOMMENDATIONS• There needs to be much greater awareness in Wirral of the growing imbalance between expectation, demand and resources for public services. Measures/initiatives to engage the local population in the debate should be put in place.
• Modelling of likely future demand for health and social care services is a valuable tool. Such approaches should be employed not only to help set priorities for the health and social care systembut also in regular monitoring and evaluation of service impact through updated data.
PUBLIC HEALTH ANNUAL REPORT 2011/12 9
1. A Century of Change: Trends in UK statistics since 1900, House of Commons Library (accessed June 2012)www.parliament.uk/documents/commons/lib/research/rp99/rp99-111.pdf
2. Department of Health (accessed June 2012) www.dh.gov.uk/health/category/policy-areas/nhs/long-term-conditions/3. Department of Health (accessed June 2012) www.longtermconditions.dh.gov.uk/about/4. Department of Health Improving the health and well-being of people with long term conditions (accessed June 2012)
www.yourpersonalbestcampaign.co.uk/materials/DOH5. English Longitudinal Study of Ageing, 2009 (Wave 4). www.ifs.org.uk/ELSA/reportWave46. NHS Wirral Joint Strategic Needs Assessment (2011). Burden of Disease Assessment (Accessed June 2012)
www.info.wirral.nhs.uk/document_uploads/Health-Profiles/BurdenofDiseaseAssessNov09.pdf 7. 7.1 Nicholson D (2009). The Year: NHS Chief Executive’s Annual Report 2008/09. London: Department of Health (accessed May 2012)
www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_099689 8. 8.2 Crawford R & Emmerson C NHS and social care funding: the outlook to 2021/22. July 2012 Nuffield Trust (accessed July 2012)
www.nuffieldtrust.org.uk/publications/future-NHS-spending 9. Fairer Care Funding. Analysis and evidence supporting the recommendations of the Commission on Funding of Care and Support (July 2011)
(accessed July 2012) www.wp.dh.gov.uk/carecommission/files/2011/07/Volume-II-Evidence-and-Analysis1.pdf10. Appleby J, Ham C, Imison C, Jennings M. 2010 Improving NHS productivity. More with the same not more of the same (accessed May 2012)
www.kingsfund.org.uk/publications/improving_nhs.html11. McKinsey report on the fiscal future of the NHS (2010) (accessed June 2012)
www.dh.gov.uk/en/FreedomOfInformation/Freedomofinformationpublicationschemefeedback/FOIreleases/DH_116520

PUBLIC HEALTH ANNUAL REPORT 2011/1210
Health and social care delivery must change

PUBLIC HEALTH ANNUAL REPORT 2011/12 11
The decade between 1999 and 2009 saw a steady year on yearincrease in the use of hospital and GP care, reflecting the trend ofincreasing demand outlined above12. In particular, emergencyadmissions to hospital have increased and this is mostly accountedfor by short stay admissions and includes a broad range ofconditions12. On average, the number of GP consultations hasincreased from around 4 per person per year in 1995 to 5.5 ayear in 200913.
In 2002, a comprehensive review into thepotential cost of a quality health serviceover the following 20 years was publishedby Sir Derek Wanless. The WanlessReport involved a detailed analysis ofhealth need, public expectation,technological advance and improvingquality. It presented three scenarios offunding for the Government of the timeand highlighted the importance of servicereform alongside the additionalinvestment indicated14. Service reformwas also a theme of the recent review ofsocial care led by Andrew Dilnot. Heconcluded that more joined-up servicesand greater investment in earlyintervention and prevention serviceshad the potential to deliver better valuesocial care15.
Over the past 10-15 years, the NHS hasdeveloped many approaches to servicereform to meet this increasing demand forcare. Examples include the developmentof the 24-hour health phone line, NHSDirect, launched in 1998 to provideclinical information, confidential adviceand reassurance directly to the public.This was followed by the web-based NHSChoices launched in 2008, which not onlyinforms people about NHS services, butalso explains how to manage and improvetheir own health16. Choice of healthprovider was made available in England in
2006 and then enshrined as a right forpatients in the NHS Constitution in 2009.This aimed to encourage furtherengagement by patients in their healthand healthcare.
In 2006, the Government outlined anumber of policies designed to ease thegrowing pressure on hospital services.These included increasing the availabilityof community health services, increasingaccess to primary care through extendedsurgery opening hours and providingbetter support to those with long termconditions (for example, through theExpert Patient Programme)17. There hasbeen an increased provision of minorinjuries units in general practices and inwalk-in centres (premises developedwithin communities to support out ofhours care). In addition, a wider range ofservices is available through high streetpharmacies and community based‘intermediate care’ has been provided forpatients who no longer need hospital carebut are not yet ready to return home. Justone policy example in Wirral is thePrimary Care Assessment Unit atArrowe Park Hospital, set up to treatthose arriving at the hospital’s accidentand emergency department, who could becared for more appropriately in thecommunity through their GP practice.

PUBLIC HEALTH ANNUAL REPORT 2011/1212
12. Blunt I, Bardsley M, Dixon J (2010) Trends in emergency admissions in England 2004–2009 (accessed June 2012)www.nuffieldtrust.org.uk/sites/files/nuffield/publication/Trends_in_emergency_admissions_BRIEFING.pdf
13. Hippisley-Cox J, Vinogradova Y (2009) Trends in Consultation Rates in General Practice 1995/1996 to 2008/2009 www.ic.nhs.uk/webfiles/publications/gp/Trends_in_Consultation_Rates_in_General_Practice_1995_96_to_2008_09.pdf
14. Wanless D (2002) Securing Our Future Health: Taking a Long-Term View (accessed June 2012) webarchive.nationalarchives.gov.uk/+/http://www.hm-treasury.gov.uk/consult_wanless_final.htm
15. Fairer Care Funding. Analysis and evidence supporting the recommendations of the Commission on Funding of Care and Support (July 2011)www.wp.dh.gov.uk/carecommission/files/2011/07/Volume-II-Evidence-and-Analysis1.pdf
16. www.nhs.uk/aboutNHSChoices/aboutnhschoices/Aboutus/Pages/Introduction.aspx17. DH, (2006) Our Health, Our Care, Our Say: a new direction for community services
www.webarchive.nationalarchives.gov.uk/+/www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_412745318. Wanless D, Appleby J, Harrison T, Patel D (2007) (accessed June 2012) www.kingsfund.org.uk/publications/our_future.html

PUBLIC HEALTH ANNUAL REPORT 2011/12 13
Similarly, there have been developmentswithin social care to prolong olderpeople’s independence and their ability tolive in their own homes (delaying the needfor long-term residential or nursing care).‘Re-ablement’ seeks to acceleraterecovery from illness or accident,including the use of assistive technologiesor by adapting the patient’s home.A range of community services have alsobeen developed in Wirral to help thosewith long term conditions manage theirconditions better. Examples include thechronic obstructive pulmonary disease(COPD) service at Albert Lodge inWallasey, and the chronic heart failurecentre at St Catherine’s Hospital inTranmere. Current policy changes withinthe NHS seek to further increase theprominence and impact of primary care aspart of the solution to the growing gapin capacity.
However, a five-year review of his originalreport (completed in 2007) led Sir DerekWanless to conclude that:
‘even with higher productivity andgreater engagement by individuals intheir own health, funding for healthservices will need to increasesubstantially… without significantimprovements in NHS productivity, andefforts to tackle key determinants of illhealth, such as obesity, even higherlevels of funding will be needed overthe next two decades to deliver thehigh-quality services envisaged by the2002 Wanless review’.18
The Dilnot Commission also called forincreased investment in adult social careto ensure that future services remainviable and effective. With the currentpressure on public service funding, incontrast to the further increases in fundingadvocated for in these and other reports,tackling the determinants of ill healthbecomes all the more important, not onlyfor improving the health of the populationbut also for sustaining a high qualityhealth and social care system.
RECOMMENDATIONS• Awareness and promotion of early intervention services across health and social care should be maintained and increased through this period of system change in Wirral. An integrated approach to promotion and use of these services must be adopted by all organisations to relieve pressure on hospital and residential care.

PUBLIC HEALTH ANNUAL REPORT 2011/1214
Tackling the causes of ill health

PUBLIC HEALTH ANNUAL REPORT 2011/12 15
Tackling the causes of ill health can redirect individuals, familiesand communities from paths that inevitably lead to disease and theneed for treatment onto a path that maintains or improves existinghealth. A wide range of physical, sociological and environmentalinfluences contribute to ill health. Wherever possible, individuals,families and communities should be supported to improve theirlifestyle, for example, by doing more physical activity, eatinghealthily and stopping smoking. Enabling and empowering peopleto change is a core function of public health.
The Government will measure the successof public health using a new PublicHealth Outcomes Framework, publishedthis year19. This framework sets out thepublic health function in four areas,referred to as domains:
• Improving the wider determinants of health - including impacts on health such as wealth, education, employment,housing and crime;
• Health improvement - including stopping smoking, safe alcohol consumption, physical activity, healthy diet, sexual health, mental wellbeing, freedom from drug dependence;
• Health protection - including screening, vaccination, control of infectious disease and environmental hazards;
• Healthcare public health and preventing premature mortality - including mortality from preventable disease, accident or mental ill-health.
These areas will be the responsibility ofthe new public health system thatincludes national bodies and local teamsworking within Local Authorities. As wellas benefiting people’s health, achievingthe targets within each of these domains
would reduce or at least delay the needfor health and social care. For example,alcohol misuse and binge drinking havebeen key drivers for emergencyadmissions to hospital, whether throughaccident, violent assault or alcohol-relateddisease. Smoking is a major contributornot only to lung cancer but also COPDand heart disease. Obesity increases therisk of people developing Type 2 diabetesand heart disease. Injecting drug usersrisk blood borne infections such ashepatitis and HIV. Low levels of wellbeingcan lead to more serious mental healthdisorders and psychological conditions.
Although the published framework is new,the challenges are not and Public HealthWirral has been working in these areas forseveral years. A full description of publichealth services (as they apply across thelife course from birth to death) can befound in the 2011 Public Health AnnualReport20. This year, we are focusing onhow current initiatives are contributing tothe capacity challenge outlined inprevious sections. Evaluating the impactof programmes both in terms of healthoutcome and also in terms of the costbenefit of early intervention andprevention are on-going responsibilities ofthe public health workforce.

PUBLIC HEALTH ANNUAL REPORT 2011/1216
PUBLIC HEALTH OUTCOMES FRAMEWORK
VisionTo improve and protect the nation’s health and wellbeing,
and improve the health of the poorest fastest.
Outcome 1Increased health life expectancy
Taking account of the health quality as well as the length of life
(Note: This measure uses a self-reported health assessment, applied to life expectancy).
Outcome 2Reduced differences in life expectancy and healthy life expectancy
between communities.Through greater improvements in more disadvantaged comunities.
(Note: These two measures would work as a package covering both morbidity andmortality, addressing within-area differences and between area differences).
DOMAIN 1
Improving thewider
determinants ofhealth
OBJECTIVE:Improvementsagainst wider
factors that affecthealth and
wellbeing, andhealth inequalities
DOMAIN 2
Health Improvement
OBJECTIVE:People are helpedto live healthylifestyles, makehealthy choicesand reduce health
inequalities
DOMAIN 3
Health Protection
OBJECTIVE:The population’shealth is protected
from majorincidents andother threats,while reducing
health inequalities
DOMAIN 4
Healthcarepublic healthand preventingprematuremortality
OBJECTIVE:Reduced numbersof people livingwith preventableill health andpeople dying
prematurely, whilereducing thegap betweencommunities
DOMAINS
OUTCOMES

PUBLIC HEALTH ANNUAL REPORT 2011/12 17
Encouraging healthy behaviour
The concept of wellness services (keepingpeople healthy) in contrast to illnessservices (treating people’s illness) hascontinued to grow within Wirral in the pastyear. We have an established CommunityProgramme of activities21 for, amongstother things, improving mental health,developing new skills for healthy livingand supporting individuals to makepositive changes in lifestyle that keepthem healthy. Clinicians can use theprogramme to ‘prescribe’ a healthyactivity for their patients to minimise theeffects of current illness and, hopefully,prevent future illness. The introduction ofhealth trainers22 also supports individualsto make lifestyle changes that bothimprove health but also lessen theirdependence on healthcare and treatment.Here is what one client had to say afterteaming up with a local health trainer onthe advice of his GP - and losing morethan 10 kilograms in weight.
“We talked of various activities which mayhelp in my fight against obesity. After alengthy discussion I myself decided whichactivities suited me the best and they areOver 40’s 5-a-side Football, CircuitTraining and Weight Training.
Circuit Training I took to like a duck towater as it felt good and comfortable.The instructor Ron King is a very goodmotivator. The actual class is mixed and
are really friendly people, you train at yourown pace. If you need a rest or waterbreak you take one. It’s all about you. It’snot a race. Whilst attending the circuitclasses I’ve made some really nice friendswhich really help with my motivation. Myhealthy eating advisor is Claire whomonitors my weight loss and records it.Claire also advises me about my diet,nutrition and portioning. We also discussany worries I may have about eating in/outand she comes up with some very helpfulstrategies to help with my weight loss.
I now walk around Birkenhead Park, 2circuits of the inner park road … 3 times aweek and I’ve also purchased a bicycle tocycle around the park and various cycleroutes around the Wirral. At the start ofthis I was 139.6kg and waist measurementof 149cm and that was on 3rd June 2011.I am now 128.8kg and a waistmeasurement of 139 cm and that was onthe 5th September 2011. This means todate I’ve lost in weight 10.8kg and 10cmoff my waist measurement.”
This year, Wirral is building on thissuccess by bringing together a wide rangeof healthy lifestyle services into onesingle, seamless service. This will make iteasier for people to get the help andsupport they need to improve and sustaintheir lifestyle.

PUBLIC HEALTH ANNUAL REPORT 2011/1218
Smoking in pregnancy
Many Wirral women continue to smokeduring their pregnancy (up to 30% in themost deprived parts of the borough).Smoking is linked to economicdeprivation, low self-esteem and stress. Anew, dedicated group-based course waslaunched this year to help pregnantsmokers quit by addressing barriers -such as low self-esteem - that preventthem from stopping. As well asencouraging smoking cessation, sessionsalso incorporate support to maintainhealthy weight and levels of exercisethrough pregnancy and include one-to-one follow up on completion of thecourse. Creating the kind of environmentthat empowers people to make a lastingchange in behaviour is often as importantas providing health information. In thisexample, healthy outcomes not onlybenefit the mother but also lay vitalhealthy foundations for the unborn child.
Drug and substance misuse
Public Health Wirral seeks to shift peoplefrom being treated for drug addictiontowards enabling them to becomecompletely drug-free, in ‘recovery’.A pioneering drug and alcohol project,The Quays, has been opened this year23.The initiative offers peer-led support topeople who are struggling to overcome
their addiction. Early evidence suggeststhat this is a popular and effectiveapproach, with many addicts beinghelped to join job clubs and to accesssupport services that can help them movefrom dependence (whether social orphysiological) to better health and a morepositive future.
In addition, an outreach service has beenlaunched to reduce the number ofproblem drinkers making inappropriateuse of health care services - notably A&Eemergency care. Replicating similarprogrammes for heroin users, this latestdevelopment works in partnership withother agencies to address the kind oflifestyle issues, such as poor livingconditions, that may contribute to adrinker’s chaotic lifestyle. The aim is tosupport people to manage their own liveseffectively and to take greaterresponsibility for their own health andwellbeing before reaching crisis point.
Another initiative redirecting individualsaway from crisis healthcare is the AlcoholShared Care scheme. Developed withCheshire and Wirral Partnership NHSFoundation Trust, the scheme ensuresthat every general practice in Wirral hasaccess to an alcohol treatmentpractitioner who can fast track clients intocommunity and residential detoxificationbefore a crisis point is reached.

PUBLIC HEALTH ANNUAL REPORT 2011/12 19
Immunisation and screening
Immunisation and screening are two ofthe safest and most effective ways ofprotecting people’s health. One of thelatest national immunisation campaigns isfor Human Papilloma Virus (HPV), toprotect young women from future risk ofcervical cancer. A recommendation in lastyear’s Public Health Annual Report wasfor close working between schools andGPs to maximise HPV vaccinationuptake24. Last year, 93.6% of 12-13 yearold girls in Wirral received all three dosesof HPV vaccine, making Wirral the sixthmost successful Primary Care Trust inEngland in terms of vaccine coverage.
Similarly, the Cervical ScreeningProgramme aims to protect women byoffering regular screening between theages of 25 and 64. Regular screeningenables the identification and earlytreatment of conditions that mightotherwise develop into cervical cancer,thereby reducing the risk of medicalintervention later in life. In 2011,Improving Outcomes: a Strategy forCancer committed the Government torolling out HPV testing as part of theCervical Screening Programme acrossEngland. As well as detecting problemsearly, HPV testing reduces the number ofunnecessary hospital referrals for those atvery low risk of cervical cancer.Systematic testing also results in morewomen getting the medical help they needmore quickly.
Helping vulnerable children andyoung people
Health Challenge Champions is aprogramme of healthy behaviour andhealth promotion sessions for childrenwho are at risk of going into long-termcare. These children are more likely tosuffer mental and physical healthproblems than their peers. An evaluationsuggested that the initiative was verypopular, resulting in some specific positivechanges in this group’s approach tolooking after their own health25. The aim isthat in rolling out this programme to alarger group, these children can supportothers in a similar position. Developingindividual responsibility for aspects oftheir lives can enable children to live moreindependently in the future and to avoidlong-term social care.

PUBLIC HEALTH ANNUAL REPORT 2011/1220
A decade of wellbeing
Wellbeing denotes a state of healthinessthat can delay or prevent serious ill healthand includes aspects of physical andmental health. Merseyside has designated2010-20 a decade of wellbeing, basedaround the 5 ways to wellbeingconceptualised by the New EconomicsFoundation. This year, the promotion ofreading is an example of a simpleintervention which has the potential toboost wellbeing in a variety of ways. Thishas included an initiative called ReadYourself Well, a collection of self-helpresources including DVDs,autobiographies and books to supportspecific conditions, supported by a locallibrarian who is also trained as a healthchampion. Get Into Reading is anotherinitiative, commissioned to deliversessions that use group reading topromote social inclusion and mentalwellbeing in various community settings,including libraries. A specific application isthe delivery of group reading sessions inresidential care settings for peoplesuffering from dementia. Of the 89residents involved in these groups thisyear, over 85% experienced less agitation,
improved mood and better concentrationas a result. A recent evaluation ofthis initiative included the followingcase study:
‘B and D often sit next to each other inthe lounge, but outside of the poetrysession they rarely speak to each other.They both are from Wirral and are ableto reminisce easily about their lives.They are really eloquent and often wittyin the way they express things. Whathas been striking to witness is the waythat during the session they interactwith each other in a way that theyrarely do outside of it. The poetryseems to spark discussion about familylife, memories (both happy and sad),love, marriage, and their fathers’ jobsworking at the docks. They also use thethemes of the poetry to express theirfeelings about their lives now - and thepoetry can enable them to have aframework to express how they arefeeling about living in the residentialhome. B recently described the groupas “out of the ordinary.”
RECOMMENDATIONS• Developing integrated services where any point of access opens up a wide diversity of interventions is a model which can bring both improved efficiency as well as effectiveness and improved user engagement. This model should be considered across the system and co-ordinated for maximum impact;
• Wellbeing is a well recognised factor promoting improved health. Health and social care services should increasingly consider their impact on wellbeing as an additional measure of performance.

PUBLIC HEALTH ANNUAL REPORT 2011/12 21
19. www.info.wirral.nhs.uk/document_uploads/Annually-Produced-Reports/PHARAnnualReport2011.pdf20. Annual Report of the Director of Public Health for Wirral 2010-2011
www.info.wirral.nhs.uk/document_uploads/Annually-Produced-Reports/PHARAnnualReport2011.pdf21. Wirral Community NHS Trust, Community Programme (accessed June 2012)
www.wirralct.nhs.uk/index.php/our-services/services/community-programme22. Wirral Community NHS Trust, Health Trainers www.wirralct.nhs.uk/index.php/our-services/services/health-trainers23. NHS Wirral News (accessed June 2012) www.wirral.nhs.uk/news.aspx?storyID=505224. Annual Report of the Director of Public Health for Wirral 2010-2011
www.info.wirral.nhs.uk/document_uploads/Annually-Produced-Reports/PHARAnnualReport2011.pdf

PUBLIC HEALTH ANNUAL REPORT 2011/1222
A new movement

PUBLIC HEALTH ANNUAL REPORT 2011/12 23
If we are to maintain and develop population-wide health servicesalongside treatment and response services and if we are to tip thebalance from health and social care systems that mostly treat in acrisis to ones that prevent the crisis arising, new relationships andnew ways of approaching health services in Wirral are required.
If the Wirral public health system (in itswidest sense) is to successfully deliver thefour domains of outcomes describedacross the whole population, a new, morewidespread health movement is calledfor. Such a movement will include fundingagencies, public sector, voluntary sector,individuals and communities working instronger partnership.
This year we have been developing theseapproaches, some of which we havealready described in the previous projectexamples. Over the next three years weneed to build on our foundations for asustainable approach to preventing illhealth across Wirral, whilst maintaining asafe transition of the public health serviceinto Wirral Borough Council.
Such a movement requires:
• Strategic alliances - widening thepotential input into design and delivery of services in recognition that health andwellbeing are commonly held priorities;
• New settings - opportunities for improved healthy behaviour and access to health services in the ‘everyday’ context;
• New perspectives - developing a betterunderstanding of population and individual health states and needs.
Strategic alliances
Health and social care leadership is arequirement of a number of statutoryagencies. Although this responsibility isnot (in most cases) new, the way in whichthis leadership is applied must change.The recognition of a wider andinterconnected health and social careeconomy is more important than ever.Leadership must go beyond traditionalbarriers of culture and funding that canexist between, for example, socialservices and hospital care or betweenhealth improvement and clinical services.
Decisions about prioritising whichservices need to be developed, howservices should be configured and how afinite workforce should be deployed willoften need to be made acrossprofessional groups and organisations.Such decisions can have an impactbeyond their immediate scope and theinformation that can inform them isinvariably a shared resource betweenmany distinct groups. Three majordevelopments this year aim to developnew leadership from the perspective ofstatutory agencies: the formation of theHealth and Wellbeing Board (H&WB), thelaunch of Wirral Clinical CommissioningGroup (CCG) and the transfer ofthe public health service into theLocal Authority.
PUBLIC HEALTH ANNUAL REPORT 2011/1224
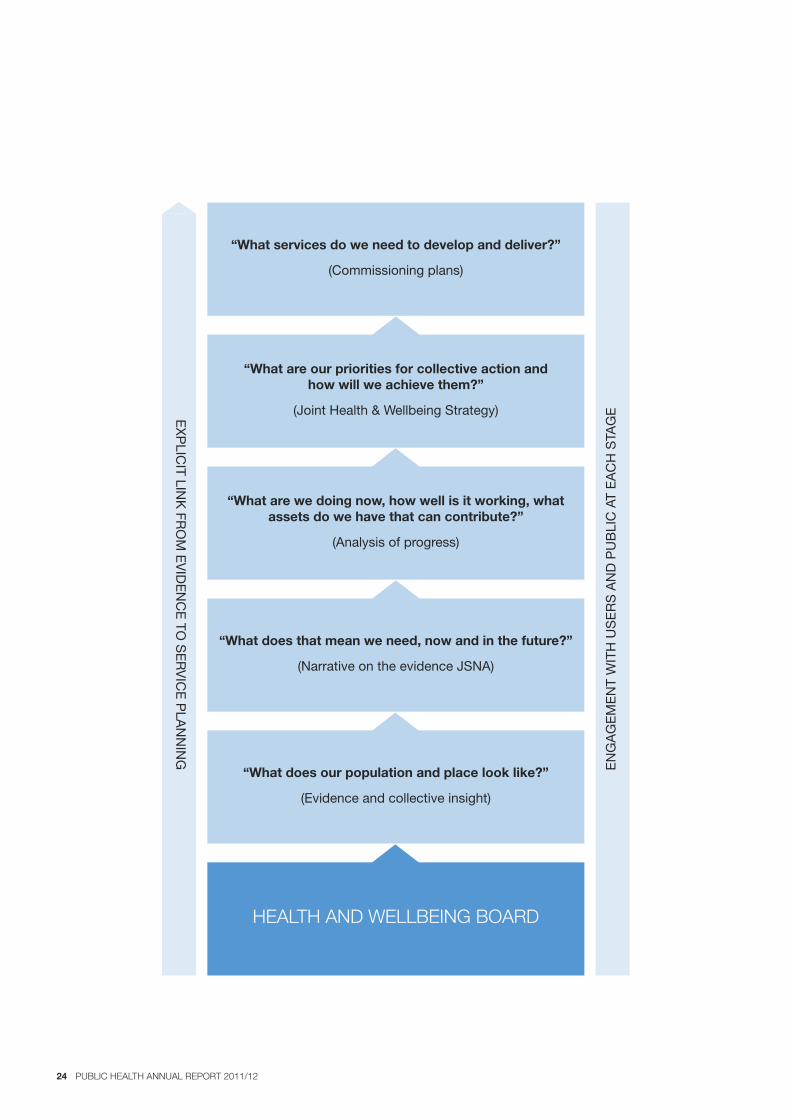
HEALTH AND WELLBEING BOARD
“What does our population and place look like?”
(Evidence and collective insight)
“What does that mean we need, now and in the future?”
(Narrative on the evidence JSNA)
“What are we doing now, how well is it working, whatassets do we have that can contribute?”
(Analysis of progress)
“What are our priorities for collective action andhow will we achieve them?”
(Joint Health & Wellbeing Strategy)
“What services do we need to develop and deliver?”
(Commissioning plans)
ENGAGEMENT WITH USERS AND PUBLIC AT EACH STAGEE
XPLIC
IT LINK FR
OM EVIDENCE TO
SERVICE PLANNING

PUBLIC HEALTH ANNUAL REPORT 2011/12 25
The development of the Wirral H&WBrecognises the need to devise healthapproaches as a whole system, withcommon aims and common ownership.This is why the H&WB includes not only allthe new commissioners of health servicesbut also the providers, includingcommunity and voluntary sectorrepresentation. Because of itsmembership and profile, the Board,through a number of work streams, willbe better able to maintain an overview ofpopulation health and social care needand opportunity, develop a joint strategyaround which suitable services can bedeveloped and assess progress in a farmore integrated way.
The official launch of the Wirral CCG asthe main commissioner for health care in2013 aims to bring the development ofcare pathways and appropriate healthservices closer to the communities theyserve. With its greater involvement ofGeneral Practitioners and practice teams(in most cases the first point of contactfor the public), the CCG aims to develophealthcare systems that are moreresponsive to the health care needs ofthe Wirral population, and therebymore effective.
The transfer of Wirral’s public healthservice to the Local Authority in 2013 isintended to strengthen the impact ofpreventative approaches, not only byaligning the relevant expertise withinpublic health, social care and communitydevelopment but also by developinggreater synergy in achieving economicand social growth in Wirral. One suchexample is the impact that improvedpopulation health has on the numbersof people able to gain and retainemployment.
However, strategic alliances are not justabout statutory organisations. Formalhealth services are limited in what theycan offer a diverse community like Wirral.With increasing demand and decreasingresources, an open and frank discussionabout priorities and the means by whichto address them becomes more and moreimportant at every level.
Third sector charitable, voluntary andcommunity organisations (whether faith-based, cultural, geographical or topic-based) are key to developing moreeffective, efficient and sustainable publichealth services. They are often in contactwith individuals, families and communitiesthat rarely use, but often need, health orsocial care services. Where appropriate,existing links with these invaluablepartners should be developedand nurtured.
One such example was thecommissioning this year of public healthprojects through Voluntary & CommunityAction Wirral (VCAW). VCAW was askedto administer a Public Health InnovationFund set up for local third sectororganisations. It meant that theorganisations could bid for fundingunhindered by the constraints andcomplexities of public sectorprocurement. It was also felt that VCAW’sclose links with the community wouldencourage a greater involvement atgrassroots level.
More than 30 proposals were submittedand of these 12 were approved to share atotal of £132,270. Projects included skillstraining to improve people’s jobprospects; the setting up of self-helpgroups for those with poor mental healthand some gentle but structured activity forpeople recovering from serious illness.

PUBLIC HEALTH ANNUAL REPORT 2011/1226
In October 2011, NHS Wirral alsocommissioned VCAW to identify andrecruit volunteers to receive training in theearly detection and screening of cancer.VCAW is currently working closely withtargeted organisations in two phases:those with a direct link to cancerawareness and those with a broaderinterest in health and wellbeing. Flexibletraining sessions will be offered in asmany community venues as possible toensure that a wide variety of volunteers(including those with caringresponsibilities, for example) are able toparticipate. The Social Partnership andAdvocacy in Wirral are two of theorganisations taking part in the training.
Initiatives to increase smokers’ success inquitting have increasingly includedmembers of third sector organisations.Individuals are being trained to deliverrobust smoking cessation programmescloser to users’ homes and without theneed for appointments. There are now sixorganisations delivering smokingcessation and five more are being trainedto do so. This approach complements themore intensive NHS-based service,improving both choice and accessto support.
A final element of health leadership is atan individual level. Generally, people areresponsible for their lifestyle choices anddecisions about health services. Thisresponsibility can be encouraged andsupported through information and skillsdevelopment, but it can also beundermined when individuals have limitedcontrol over health and social caredecisions. This is where the developmentof peer approaches to healthimprovement can be effective. Forexample, in 2010 Wirral developed apeer-led approach to encouragebreastfeeding. During 2010-11, 769women received support from thisprogramme and this increased last year to
1,257. Of these, 44% were stillbreastfeeding at the crucial 6-8 weeksstage, compared with an average (acrossall Wirral) of 30%, suggesting theeffectiveness of peer leadership insupporting healthy behaviour.
New settings
Last year’s Public Health Annual Reportdescribed in some detail the varioussettings for public health work beingdeveloped in Wirral, with a focus ontraining frontline health and social carestaff to deliver brief interventions andsignpost individuals to existing services.This year we are building on thissignposting by extending the rangeof health services that are delivered inother settings.
The school environment is one of thefastest growing of these settings. HealthServices in Schools (HSIS) is nowestablished in all but one of Wirral’ssecondary schools as an invaluable andvery accessible source of health adviceand support for young people. HSIS is apartnership in the true sense of the word,with a provider network managed bymembers of the Wirral School NursingService, Response, Bridgewater, WirralBrook, Merseyside Youth Alliance andTranmere Community Project.
The concept of early intervention isexemplified by smoking cessationsessions introduced into HSIS this year.The younger a person starts smoking, thegreater the lifelong risk of developingsmoking-related cancers, because youngsmokers are more likely to becomeaddicted. By providing specially tailoredstop smoking support in schools there is afar greater opportunity for young smokersto quit early. In the past 12 months, morethan 150 young people have quit as aresult of this initiative.

PUBLIC HEALTH ANNUAL REPORT 2011/12 27

PUBLIC HEALTH ANNUAL REPORT 2011/1228
Alongside support to quit there is A StopSmoking in Schools Trial (ASSIST),which promotes non-smoking behaviouras the norm among secondary students.The programme recruits and trainsinfluential students as peer educators whoare able to discuss with their friends andfellow students the risks of smoking andthe benefits of being smoke-free. Theinitiative is being introduced into 20 Wirralschools over the next two years.If smoking prevention is successful, nearlyall disease associated with it will beavoided - along with the expense of anyfuture treatment.
Last year’s Public Health Annual Report26
made a specific recommendation toincrease the reach of Chlamydia screeningand to focus on young men, a grouptraditionally harder to engage in theestablished screening programme. Anovel and effective approach this yearwas a campaign that did not rely onaccessing NHS services. Developed by alocal social marketing company, Screenfor a Screen offered a free cinemavoucher to any young person completinga brief intervention (this included a shortsurvey on sexual behaviour and a urinesample for screening). NHS staff fromWirral Community Trust were involved inthe training to ensure that screeningprotocols were observed. For maximumimpact, the intervention was delivered atnight in established social settings.Between December 2011 and March 2012an additional 3,200 Chlamydia tests wereachieved. The campaign also resulted in ahigher proportion of males over the age of18 being tested.
Other important settings for public healthin Wirral are Children’s Centres. A pilotinvolving three Wirral centres is underwayto support the Government’s effortsto tackle the growing problem of VitaminD deficiency.
The Government is encouraging pregnantand breast-feeding women and infantsaged between six months and five yearsto take a daily supplement of vitamin D,which is essential for good health, growthand strong bones. Free vitamins areavailable for those eligible for the nationalHealthy Start programme through avoucher exchange scheme at most Wirralhealth clinics. However, by December2011, only 2.5% of vouchers for children’svitamin D drops had been redeemed inWirral (and only 3.1% of vouchers forwomen’s vitamin D tablets). To improveuptake by increasing access to thescheme, a variety of non-NHS venues -including Children’s Centres - are beingconsidered.
New perspectives
People relate to health improvement andhealthcare initiatives in different ways andservices need to respond/reactaccordingly if they are to be effective. Thefindings of a recent survey (Redesigningservices to meet users’ needs in adifferent way) involving 202 senior publicsector leaders from local government andhealth sectors concluded that thisapproach represented the best wayforward for organisations seeking todeliver better services in the nextfive years27.
In healthcare, the concept of shareddecision-making is becoming increasinglyimportant. This goes beyond simplechoices of where to be treated and seeksto change the relationship between apatient and health professional, with theaim of sharing the health decision-making.This should lead to better-informedpatients who have the skills to discusscomplex health decisions and theconfidence to direct the agenda of theircare on more equal terms with theirdoctor. In social care, the Personalisation

PUBLIC HEALTH ANNUAL REPORT 2011/12 29
Agenda aims to achieve a similarre-balance of power, with individuals ableto make a wider range of care decisionsby becoming the budget holder.
Wirral Public Health routinely uses‘segmentation’ approaches to betterunderstand and identify the groups ofindividuals benefiting from health services.At a basic level, this means geographicalmapping of health status and need andthese maps can be explored onlinethrough the InstantAtlas tool on the WirralJoint Strategic Needs Assessmentwebsite28. However, there is a very widerange of demographic and cultural factorsinfluencing behaviour and health.
Mosaic is a segmentation tool used inWirral to help develop interventions andinformation campaigns that are tailored toparticular communities. This year, ananalysis of smoking prevalence amongstdifferent groups of pregnant women29
highlighted which approaches topromoting awareness and encouragingquit attempts would produce the bestresults. The findings informed the servicethat was subsequently commissioned andits success will be evaluated this year.Another tool to identify an individual’slikely engagement with services is theHealthy Foundations model developed in2006 by the Department of Health30. Suchtools can help target resources effectively.
Although models and analyticalsegmentation can help guide servicedevelopment, people’s personalexperiences and opinions are also crucial.To address the low public involvement inWirral’s Teenage Pregnancy Action Plan,public engagement was included as apriority area for action in this year’s review.Steps are being taken to consult with keyyoung people’s groups, such as YouthParliament, Youth Executive Board andthe Children in Care Council to informstrategy development.
Similarly, when planning and deliveringlocal maternity services, the MaternityServices Liaison Committee (MLSC)has, for the last three years, made a pointof involving those who use these services.The MLSC is currently chaired by aservice user. The committee is key tounderstanding how best to increase thenumber of breastfeeding women in Wirraland in highlighting locally the issue oftongue-tied babies, a birth defect thataffects 3-10% of newborns nationally.
Ongoing efforts to involve the populationin decisions about new services havebeen more formalised this year with theintroduction of the InfrastructureSupport Service (ISS). This is a contractwith VCAW to engage with hard-to reachgroups, such as those from minorityethnic communities, who are often not asinvolved as others in mainstream activity,health or otherwise.
The beliefs and choices of differentcultural or faith communities cansometimes be misunderstood in thedelivery of health improvement orservices. This can result in groupsdisengaging from services aimed atimproving their health. The Wirral EthnicHealth Advisory Group (WEHAG) hasspent many years raising awareness ofhealth issues pertinent to local ethnicpopulations and this year, faith leaderswere involved in developing a valuesframework for the delivery ofRelationships and Sex Education (RSE) inWirral. This ensures that faith schools andparents feel confident about allowing theirchildren to participate in RSE in schools.The guidance document, which includesten value statements, was launched overthe summer as a basis for delivering RSEin Wirral.

A major research project was launched inWirral this year to document the extent towhich community-led projects contributeto the effectiveness of the public healthsystem in achieving its targets. This willsupport a new perspective of whatcommunities contribute, to balance theprevailing view of what they lack or need.Part of this research seeks to measure thesocial value of services alongside moretraditional health or economic value.Developing new ways by which torecognise this contribution can encouragea wider and more inclusive approach topublic health service delivery. It is hopedthat wider perspectives on both the stateof health and how public health can bemore effectively delivered will emergefrom this work; perspectives that can beapplied on a wider scale.
We can all make a difference
The final area of new perspective is withinus, as residents of Wirral. It is clear thathealth services need to adapt and that ourrelationship with them needs to change.The development of more sustainable andequitable health and wellbeing over thecoming three-five years demands ourcontribution as members of thecommunity, as well as the efforts of thosedirectly employed in health andsocial care.
The innovation, vision and energy can befound throughout the Peninsula. We canall take steps to use our precious healthsystem’s resources responsibly andappropriately, to proactively invest in ourown health and wellbeing whereverpossible (by taking more exercise;stopping smoking and eating morehealthily, for starters) and to engage in thewider discussion as to how to meet thehealth priorities on our doorstep.Only then will the true partnershipemerge that is required to make Wirral ahealthier place.
27. Skinner G, Cummings L (2012) Public service reform 2010-2012: a tale of support and scepticism www.ipsos-mori.com/_emails/sri/understandingsociety/july2012/mobile/no2.html
28. www.info.wirral.nhs.uk/instantatlas/ 29. www.info.wirral.nhs.uk/intelligencehub/geodemographicsandsocialmarketing.html 30. www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_086291.pdf
PUBLIC HEALTH ANNUAL REPORT 2011/1230

RECOMMENDATIONS• The described model of communities and community organisations defining how the resource in a particular priority area could be best used is one that should be further developed, as resources allow, within health and social care. This will help to rebalance the complementing priorities of user and provider.
• Peer-led approaches are effective in increasing the reach and influence of public health information and services. There should be ongoing consideration of this approach across health and social careand increased effort to demonstrate successful impact.
• A range of segmentation approaches should be systematically applied to the design of health and social care services to increase their suitability and help monitor their impact.
• Diverse settings, through which health improvement and health protection can be delivered, should continue to be explored.
• The population of Wirral is a central partner in the formation of a new movement for health and wellbeing across the borough. Effective ways to involve communities, families and individuals in debate, design and delivery of initiatives should continue to be improved and expanded by all statutory providers of services.
PUBLIC HEALTH ANNUAL REPORT 2011/12 31

344JUN12GB
Public Health DirectorateNHS Wirral
Old Market House, BirkenheadWirral, CH41 5AL
Tel: 0151 651 0011Email: [email protected]