Embed Size (px)
Citation preview

IntroductionThe addition of the VVI antibradycardia pac-
ing capability to the implantable cardioverter de-fibrillator (ICD) represented a significant ad-vance.1 Postshock bradyarrhythmias2 became lessof a concern, and sudden death due to asystole3
could be prevented. However, because of hemo-dynamic limitations imposed by fixed rate VVImode4 and significant current drain, it has beencommon practice to use separate physiologicpacemakers in ICD patients requiring more thanoccasional backup pacing.
ICDs capable of dual chamber, rate respon-sive pacing promise to largely eliminate the needfor a separate pacemaker.5 Potential advantagesinclude fewer intravascular leads, elimination ofdevice-device interactions,6,7 better cosmetic re-sults, and simplified follow-up. Early experiencewith these systems has been favorable.8 Im-proved tachyarrhythmia discrimination9,10 andrelief of pacemaker syndrome following upgradefrom single to dual chamber ICDs11 have been re-ported. Addition of full-featured pacing is tech-nically complex, and the resultant product is notsimply the sum of a DDDR pacemaker and atiered-therapy ICD. As clinical experience ex-pands, device shortcomings and idiosyncrasiesare becoming apparent. Compromises have beenmade between pacing versatility and safe defib-rillator function. The emphasis on defibrillationsafety may, at times, result in suboptimal pace-maker function. In this article, we describe po-tential problems and provide guidelines for theirprevention at the time of implant (and initial pro-gramming) and during follow-up. Problems oc-curring with single chamber ICDs are discussedwhen anticipated with dual chamber units ofsimilar operation.
Need for Antibradycardia Pacing in ICDRecipients
In the past, 15%–20% of patients with ICDsrequired a separate pacemaker. Geelen et al.11 re-ported that permanent pacing was required in 25(18%) of 139 consecutive ICD patients. This in-cluded 10 patients with a preexistent pacemaker,10 patients in whom the indication for pacing be-came evident at the time of ICD implantation, and5 patients who became pacemaker dependent dur-ing follow-up. Iskos et al.12 analyzed the need fora subsequent dual chamber pacemaker in 224 pa-tients with ICDs capable of VVI pacing. Twenty-two (10%) patients received dual chamber pace-makers (mean interval from ICD to pacemakerimplant of 2.5 years). A history of atrial tach-yarrhythmia and treatment with antiarrhythmicdrugs before ICD implantation were significantpredictors of a subsequent need for physiologicpacing. Higgins et al.13 reviewed 122 consecutivepatients undergoing ICD implantation or replace-ment and concluded that a dual-chamber ICDcould have been of value in 55% of patients. Strictcriteria for dual chamber pacing were present in29%. A Mayo Clinic review of 253 patients re-vealed that a dual chamber ICD would have beendefinitely indicated in 11% of patients, probablyindicated in 28%, and possibly indicated in14%.14 Candidacy rates will increase greatly ifbiventricular pacing proves beneficial for patientswith heart failure.15 Jung and Lüderitz16 observedthat the frequent need to add drugs with negativechronotropic effects (e.g., amiodarone, sotalol) inpatients with ICDs implanted for ventriculartachycardia (VT) may justify use of a dual cham-ber ICD system in some patients without brady-cardia documented at baseline. Industry surveysestimate that, in 1999, 50% of the ICDs implantedin the U.S. and 30% of those implanted in Europehad dual chamber pacing capabilities.16
Limitations of ICDs as PacemakersLong-Term Lead Reliability
The incidence, causes, and prevention of pac-ing lead failure (conductor fracture, insulationbreakdown) have been the subject of intense in-vestigation. Leads differ in their long-term relia-
REVIEW
Permanent Pacing via Implantable DefibrillatorsSERGIO L. PINSKI and RICHARD G. TROHMANFrom the Section of Cardiology, Rush Medical College and Rush-Presbyterian-St. Luke’s MedicalCenter, Chicago, Illinois
PACE, Vol. 23 November 2000, Part I 1667
Address for reprints: Sergio L. Pinski, M.D., Rush-Presbyte-rian-St. Luke’s Medical Center, 1750 W. Harrison St., JS-1091,Chicago, IL 60612. Fax: (312) 942-5862; e-mail: spinski6rush.edu
Received December 14, 2000; revised March 1, 2000; acceptedMarch 16, 2000.
Reprinted with permission fromJOURNAL OF PACING AND CLINICAL ELECTROPHYSIOLOGY , Volume 23, No. 11, Part I, November 2000
Copyright © 2000 by Futura Publishing Company, Inc., Armonk, NY 10504-0418.

bility.17 The best are associated with . 95% 10-year survival, while several models with a failurerate $10% at 5 years have been identified.18 Thereis much less information on long-term perfor-mance of transvenous defibrillator leads. Designfeatures, including larger size and complex multi-electrode configurations make defibrillator leadsmore susceptible to structural failure. Failure ofthe pacing and sensing components of a defibril-lator lead can be associated with severe symptoms(or death) in pacemaker dependent patients.19
Nondependent patients usually present with in-appropriate aborted or delivered shocks.20
The rapid evolution in transvenous ICD leaddesign makes assessment of long-term perfor-mance difficult.21 Current leads have been avail-able for , 5 years. Ongoing surveillance is crucialbecause excellent performance during the first fewyears postimplant does not guarantee long-term re-liability.18 Table I summarizes available informa-tion on medium-term performance of early leaddesigns.22–25 Recent technological changes may re-sult in reduced failure rates.26 As with pacemakerleads, it appears that lead breakdown at the level ofthe thoracic inlet is less common with insertionthrough the cephalic vein cutdown compared tosubclavian puncture.27 Modern ICD leads can beimplanted via a small cephalic vein . 90% of thetime using a modified Seldinger technique.28 Me-dial subclavian punctures should be avoided.Abrasion of lead insulation inside the pocket hasalso been a common mechanism of ICD lead fail-ure, particularly with abdominal devices.29 Abra-sions seem less frequent with shorter leads andsmaller generators implanted pectorally.30
Uncertainties about the long-term perfor-mance of defibrillation leads should be taken intoaccount for pacemaker dependent patients. Al-though automatic capacitor reformation permits
widely spaced clinic visits, these patients shouldbe seen more often (probably every 3–4 months).Abnormalities in electrical parameters, includinglead impedance, can be an early sign of lead fail-ure.31 Routine radiological surveillance is lowyield.32 Newer systems perform daily automaticmeasurements of lead impedance and can warnpatients with an alarm tone if the measurement isout of range (Fig. 1).33 Enabling the alarm shouldbe considered in pacemaker dependent patients.However, there is no long-term data on the effec-tiveness of this measure. More complex leads ca-pable of shocking, pacing, and sensing the atriumand ventricle are under clinical investigation.34,35
It may be prudent to avoid using those leads inpacemaker dependent patients until their long-term reliability is established.
Increased Current Drain
Estimation of pulse generator longevity ismore complex in ICDs than standard pacemakersbecause it depends on the capacity and efficiencyof power source(s), frequency and energy ofshocks, static current drain, frequency and effi-ciency of pacing, and ancillary functions (e.g.,electrogram storage).36 There are no standard crite-ria to predict device longevity. Different manufac-turers’ estimates are not comparable. Their scenar-ios may be constructed to amplify strengths andminimize weaknesses.36 Although not all manu-facturers provide estimates of battery longevitywith 100% pacing, it can be assumed to decreasebattery longevity by 20%–40%. For example,when a Medtronic (Minneapolis, MN, USA) GEMDR ICD delivers quarterly 35 J shocks, 100% atri-oventricular (AV) sequential pacing at 60beats/min (4 V at 0.4-ms pulse width, pacing load510 V) would decrease expected longevity by 38%(from 10.6 years with 100% sensing to 6.6 years).37
PINSKI, ET AL.
1668 November 2000, Part I PACE, Vol. 23
Table I.
Failure Rate of Defibrillator Leads
Failure Rate* Follow-UpStudy Lead(s) Number (%) (months)
Lawton et al.2 0 Endotak (60 and 70 series) 348 2.8 15 6 11Degeratu et al.22 Endotak (60 and 70 series) 140 4.3 26 6 14Mewis et al.23 Endotak (60 and 70 series) 41 24 49 6 19Jones et al.24 Transvene 6996 159 1.3 21 6 10Medtronic Chronic Transvene 6936, 6996, 6884 1297 4.5 60
Lead Study25
Luria et al.26 Various 406 46Abdominal ICD 33Pectoral ICD 11
* Indicates proportion of leads that failed during follow-up except for reference 25 which reported actuarial rateof failure at 60 months, and reference 26 which reported actuarial rate of failure at 46 months.

ICDs are inefficient pacemakers. Constantpacing will reduce longevity twofold compared tobradycardia pacemakers of similar battery size.This results, in part, from differences in batterychemistry. The deliverable energy density of thelithium-iodine battery used in pacemakers isabout 10% greater than a similar-sized lithium-sil-ver vanadium oxide battery used in ICDs. Pace-maker batteries are optimized to generate 1–10 mJpulses needed for cardiac stimulation, whereasICD batteries are optimized to deliver up to 40 J, acurrent drain 100,000 times greater. Fundamen-tally different internal designs result in more ICDbattery waste space, and hence, a much lower de-liverable energy density, a prime determinant of
device longevity. The use of separate batteries forshocking (silver vanadium oxide) and pacing(lithium iodine) could further extend ICD longev-ity in patients with frequent pacing.
Current drain increases with lower pacingimpedance. In “integrated” bipolar defibrillationleads, pacing occurs between the distal tip and thelarge surface right ventricular coil. The pacingimpedance of these leads is in the 500–700 Vrange (lower than average for standard bipolarpacing leads). For example, during clinical trialsthe mean pacing impedance for the Medtronic6945 lead (integrated bipolar) was 692 V, versus1,169 V for the otherwise similar 6943 (“dedi-cated” bipolar).38 Guidant (St. Paul, MN, USA) has
ICDS AS PACEMAKERS
PACE, Vol. 23 November 2000, Part I 1669
Figure 1. Implantable cardioverter defibrillator (ICD) interrogation from a boy who receivedspurious shocks for a lead related problem from a single chamber ICD capable of rate responsivepacing. (Panel A) The alerts were set up to ring every morning at 9:30 AM upon detection of a highpacing lead impedance during daily automated testing (arrow). (Panel B) A single abnormalimpedance determination (. 2000 V) occurred on November 13, 1999. Impedance measurementswere normal before and afterwards (not logged in the report). The alarm sounded every morningfor 30 seconds for the next 5 days, but the patient and parents did not recognize its origin. (PanelC) Representative stored electrograms (S 5 shocking patches; V 5 bipolar epicardial) from a clusterof inappropriate shocks that occurred on November 17, 1999. Note the make-and-break signals(arrows) suggestive of intermittent electrical continuity on the V electrogram. A loose-set screw ina Y adapter was confirmed intraoperatively.

introduced a higher impedance integrated bipolardefibrillation lead (Endotak Endurance models0134/0135/0136) with a smaller active tip elec-trode surface area. This lead has similar pacingand sensing parameters with a nearly 50% higherpacing impedance than the standard DSP lead(model 0125).39 This design should be useful indecreasing current drain associated with pacingvia integrated bipolar leads.
The impact of continuous pacing on ICD cost-effectiveness is difficult to ascertain. Cost consid-erations alone should not prevent the use of ICDsas permanent pacemakers. Thoughtful program-ming of pacing parameters (mode, rates, AV de-lays, and outputs) will be more critical to optimizebattery longevity for ICDs than for standard pace-makers.40 In patients with sinus node dysfunctionand intact AV conduction, pacing in the AAIRmode may provide excellent results41 with lowercurrent drain than the DDDR mode. Postshockventricular pacing should always be enabled for ashort period because of the risk of arrhythmia in-duced or shock induced AV block.
Noncapture Due to Increased PostshockThresholds
Early reports that describe epicardial shocksleading to transient ventricular noncapture oc-curred in the presence of separate ICD and pace-maker leads.42 It is unclear if the severity of thisphenomenon in current systems (which includebiphasic waveforms and multipurpose leads usedfor pacing, sensing, and defibrillation) depends onthe type of lead involved. Kudenchuk et al.43 stud-ied 57 patients with Medtronic Transvene dedi-cated bipolar leads and found that pacing at apulse width three times the preshock threshold al-ways achieved ventricular capture within 1 sec-ond of defibrillation. Small changes in thresholdwere not related to defibrillation energy, numberof shocks, lead chronicity, shock orientation, orclinical factors. In contrast, Welch et al.44 ob-served failure to capture at twice preshock voltagethreshold 2.5 seconds following a shock in 8 of 20patients with dedicated bipolar, steroid-elutingMedtronic Sprint leads, which persisted in threepatients when the output was increased threefoldover threshold. Kessler et al.45 found an increasein pacing threshold (1.5- to 4-fold) in six (60%) often patients 2.5 seconds after biphasic endocardialshocks via Endotak integrated bipolar leads.
Current ICDs allow independent program-ming of higher pacing outputs immediately aftershock delivery. The longest reported instances ofnoncapture after internal shocks have been . 50seconds,46,47 but there was no significant increasein pacing thresholds measured 1 minute after de-fibrillation in seven patients with a prototype En-
dotak lead.48 Programming higher pacing outputsfor ; 1 minute after shocks is recommended to en-sure consistent capture. In Medtronic GEM gener-ators, the duration of postshock higher output pac-ing is fixed. Higher output pulses are delivereduntil the episode is terminated (eight consecutiveV-V intervals below the lowest tachycardia detec-tion interval) or a total of 25 events have occurred.Transient loss of capture could occur because ofthe short duration of postshock bradycardia pac-ing parameters.
The temporal course of pacing thresholds inICD systems has not been well studied. A patho-logic study of eight hearts from patients with en-docardial defibrillation leads showed consistent,intense endocardial fibrosis at the electrode/my-ocardial interface.49 Each lead was encased by fi-broelastic tissue with adjacent fibrosis of the rightventricular myocardium. Microscopically, inter-stitial fibrosis was present in the current path ofdefibrillation shocks. Epstein et al.50 prospec-tively studied 17 patients with ICDs and Endotaktined leads. After a 1-year follow-up, the ventricu-lar pacing threshold at 2.5 V gradually increasedfrom 0.08 6 0.08 ms to 0.5 6 0.3 ms (P # 0.01).The plateau in pacing threshold typically seenwith standard pacing leads was not observed. Allpatients had received shocks, and the possibilitythat shock induced inflammation (and scarring)were responsible for the steady increase in thresh-olds could not be ruled out. The increase in pac-ing thresholds did not, however, correlate withthe amount of shocking energy delivered via theleads. Steroid-eluting defibrillation leads are asso-ciated with an important decrease in chronic pac-ing thresholds51 and are preferable in patients re-quiring frequent ICD pacing.
Oversensing Resulting in Pacing Inhibition andPotential Asystole
A basic requirement of ICDs is reliable sens-ing of low amplitude ventricular depolarizationsignals during ventricular fibrillation (VF), whilesimultaneously avoiding T wave sensing and ex-tracardiac noise. This technically challenging pro-cess is accomplished by an automatic adjustmentof the gain or sensing threshold.52,53 Generally,these autoadjusting algorithms function ade-quately. Life-threatening tachyarrhythmias arecorrectly detected, while spurious device activa-tions due to oversensing are infrequent.
The addition of bradycardia pacing to the ICDpresents a dilemma. In the absence of sensed com-plexes, two potentially life-threatening diagnosesmust be considered: asystole (requiring pacing) andfine VF (requiring amplifier gain adjustments forproper detection). To ensure VF detection, pacingonset triggers a rapid increase in sensitivity in most
PINSKI, ET AL.
1670 November 2000, Part I PACE, Vol. 23

devices (Table II; Fig. 2). These very high sensitiv-ity levels can promote oversensing of intra- or ex-tracardiac signals. Oversensing can lead to spuri-ous ICD discharges (with associated psychologicalmorbidity,54 battery consumption, and occasionalproarrhythmia46) and to potentially catastrophicinhibition of pacing. If the patient is pacemaker de-pendent, oversensing perpetuates because the ab-sence of spontaneous large amplitude escape beatsmaintains the high operating sensitivity.
Oversensing of Diaphragmatic Myopotentials
Oversensing of intermittent high frequency,large amplitude signals during ventricular pacingin patients with Ventritex Cadence (Sunnyvale,CA, USA) defibrillators (persisting after lead re-placement) was originally felt to represent randomamplifier noise.55,56 However, subsequent demon-strations that deep breathing or the Valsalva ma-
ICDS AS PACEMAKERS
PACE, Vol. 23 November 2000, Part I 1671
Table II.
Ventricular Sensing Algorithms of Some Commercially Available Dual Chamber ICDs
Ventricular Sensitivity During Pacing atDevice Nominal Settings Programmability
Ventak AV series
Prizm AV
Medtronic Gem DRseries
ELA Defender II
Biotronik Phylax AV
Set at 2.3 mV after the pacing artifact.Gain starts to automatically increase 27 ms
before the expiration of the ventricularpace blanking to ensure that sensitivityreaches 0.28 mV 200 ms before the end ofthe ventricular escape interval.
Set at 3.5 mV after the pacing artifact.Gain starts to automatically increase 27 ms
before the expiration of the ventricularpace blanking to ensure that sensitivityreaches 0.44 mV 200 ms before the end ofthe ventricular escape interval.
Set at 1.35 mV at the end of the postpaceblanking.
Decays toward 0.3 mV with a 450 msconstant (Fig. 1).
Set at 0.4 mV at the end of the postpaceventricular blanking (maximum 219 ms).
Set to 50% of postpace amplitude afterpostpace refractory period or to 2 mV,whichever is less. Decays to 25% ofpostpace activity (or 1 mV if initial settingwas 2 mV) after 125 ms. Continues tostep-down toward 0.5 mV every 125 ms.
Programmable maximum sensitivity:“nominal” 5 0.19 mV“less sensitive” 5 0.27 mV“least sensitive” 5 0.43 mV
Programmable maximum sensitivity:“most sensitive” 5 0.18 mV“nominal” 5 0.27 mV“least sensitive” 5 0.43 mV
Programmable maximum sensitivity 0.15 mV to1.2 mV in 0.15 mV steps (nominal 0.3 mV).
Sensitivity is set at 4.5 times maximum at theend of the postpace blanking (but only up to1.8 mV)
Programmable maximum sensitivity from 0.4 mVto 2.0 mV in 0.2 mV steps
Programmable ventricular postpacing sensitivitymargin (0 to 2.0 mV in 0.2 steps; nominal 0mV). Sets the ventricular sensitivity to theprogrammed value 1 sensitivity margin for thefirst 500 ms after pulse, before returning to theprogrammed value.
Programmable maximum sensitivity from 0.25mV to 3.0 mV in 0.125 mV steps.
Figure 2. Autoadjusting sensitivity thresholds in theMedtronic GEM DR ICD. After a ventricular paced (VP)event, the sensitivity is increased to 4.5x theprogrammed value (up to a maximum of 1.8 mV; 1.35mV at the nominal sensitivity of 0.3 mV). After a sensedevent (VS) the device is less sensitive, starting to decayfrom a level of 75% of the electrogram (EGM) peak (upto a maximum of 8x the programmed value; 2.4 mV atthe nominal sensitivity of 0.3 mV).
neuver could elicit oversensing during ventricularpacing in most patients with Cadence-Endotaksystems identified diaphragmatic myopotentialsas the cause.56 Although a study by Mann et al.57
suggested that Ventritex devices may be particu-larly prone to this phenomenon, similar instancesof clinical oversensing with single and dual cham-ber ICDs from other vendors are well documented(Fig. 3).58–61 Sweeney et al.62 evaluated oversens-ing of diaphragmatic myopotentials with provoca-tive maneuvers during intrinsic rhythm and ven-tricular pacing in 100 consecutive ICD patients (52with Guidant and 48 with Medtronic devices).The incidence of provoked oversensing was 5%
during intrinsic rhythm and 14% during pacing.Oversensing was not associated with sensing leadconfiguration (i.e., dedicated vs integrated bipo-lar) or sensing algorithms (i.e., Guidant vsMedtronic), and could be eliminated by reducingthe sensitivity in all cases. Spontaneous clinicaloversensing (always during pacing), occurred infour (4%) patients, three of whom also had pro-vokable oversensing.
It appears prudent to perform provocativetesting during implant (especially in patients ex-pected to use the pacing function assiduously),and in follow-up when noise has triggered ar-rhythmia detection. Testing is performed after dis-
PINSKI, ET AL.
1672 November 2000, Part I PACE, Vol. 23
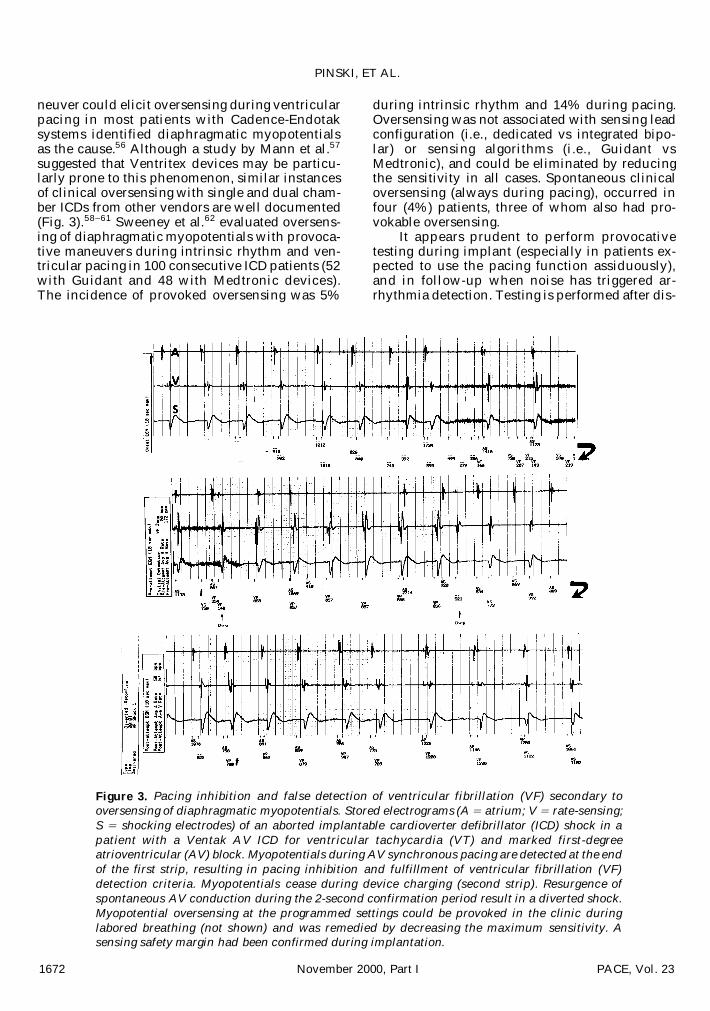
Figure 3. Pacing inhibition and false detection of ventricular fibrillation (VF) secondary tooversensing of diaphragmatic myopotentials. Stored electrograms (A 5 atrium; V 5 rate-sensing;S 5 shocking electrodes) of an aborted implantable cardioverter defibrillator (ICD) shock in apatient with a Ventak AV ICD for ventricular tachycardia (VT) and marked first-degreeatrioventricular (AV) block. Myopotentials during AV synchronous pacing are detected at the endof the first strip, resulting in pacing inhibition and fulfillment of ventricular fibrillation (VF)detection criteria. Myopotentials cease during device charging (second strip). Resurgence ofspontaneous AV conduction during the 2-second confirmation period result in a diverted shock.Myopotential oversensing at the programmed settings could be provoked in the clinic duringlabored breathing (not shown) and was remedied by decreasing the maximum sensitivity. Asensing safety margin had been confirmed during implantation.

abling tachyarrhythmia therapies and elicitingventricular pacing (by increasing the pacing rateabove the intrinsic rate or shortening the AV de-lay). Real-time electrograms and event markers aremonitored during deep inspiration, forced exhala-tion, cough, and the Valsalva maneuver. Some in-vestigators have suggested that an active-fixationlead in the right ventricular outflow tract mini-mizes myopotential oversensing58,60 without com-promising defibrillation efficiency.63,64 This leadlocation should be considered in patients whowill rely intensively on the ICD for pacing.
Oversensing of Intracardiac Signals
ICD oversensing of intracardiac signals is alsomore likely when the sensitivity is automaticallyincreased during pacing. Oversensing of T wavesfalling outside the postpace ventricular blankingperiod is common.65 It results in inhibition of thenext pacing stimulus, consequently lengtheningthe effective pacing escape interval. Most in-stances are of little clinical consequence, but theresulting bradycardia may become symptomatic.Oversensing of paced T waves can invoke “rate-stabilization” algorithms and perpetuate pacing inpatients without bradycardia.66
Programming a longer postpace blanking pe-riod usually circumvents T wave oversensing. Atthe default blanking of 350 ms, oversensing of Twaves during pacing at 10 beats/min above the in-trinsic rate occurred in 35 (70%) of 50 patientswith Ventritex devices.67 The mean postpaceblanking period needed to eliminate oversensingwas 386 6 32 ms. However, a long postpace blank-ing period during the fast rates, achievable withdual chamber or rate adaptive pacing, may delaytachyarrhythmia detection. Programming a lowersensitivity may also eliminate T wave oversens-ing. With the Medtronic Jewel,65 T wave over-sensing was observed in 84% of patients duringpacing at maximum output (8.4 V, 1.5 ms) withmaximum sensitivity (0.15 mV) and nominal post-pace blanking of 320 ms. Oversensing decreasedto 35%, 15%, and 3.7% when the sensitivity wasreduced to 0.3, 0.45, and 0.6 mV, respectively.
Oversensing of paced T waves may be diffi-cult to eliminate in patients with QT prolongation.Their T wave may fall outside the maximum pro-grammable ventricular blanking period. The re-sulting slower paced rate further prolongs the QTinterval, may perpetuate oversensing,68,69 andlead to development of torsades de pointes. InVentritex devices, paced T wave oversensingcould result in pauses longer than those expectedfrom simple resetting of the bradycardia pacing in-terval (and equal to twice the programmed pacingcycle length), if the “lower threshold crossing”feature is invoked.70
Oversensing of the far-field atrial activation isuncommon (Fig. 4), but can be life-threateningwhen it results in prolonged inhibition of pacing.Several investigators71–73 have reported cases ofinappropriate sensing of atrial depolarizationsduring atrial flutter with continuous or intermit-tent ventricular pacing. Oversensing resulted inspurious shocks and (in one case) prolonged asys-tole. Ensuring that the distal coil of integratedbipolar leads lies entirely within the right ventric-ular chamber can minimize oversensing of atrialsignals. In current Ventak AV devices (CardiacPacemakers, Inc., St. Paul, MN, USA), ventricularoversensing of the atrial pacing artifact during theblanking period is frequent. It has no clinical con-sequences, but can complicate device follow-up(Fig. 5).
Oversensing of Electromagnetic Interference
The increased sensitivity of ICDs could makethem more vulnerable to electromagnetic interfer-ence (EMI) than permanent pacemakers, espe-cially for patients at the fringe of an electromag-netic field. Studies of the interactions betweensources of EMI and ICDs should create a “worst-case scenario” by ensuring maximum sensitivityduring pacing. Isolated reports have described ICDinterference with slot machines, toy remote con-trols, transcutaneous electric nerve stimulators,
ICDS AS PACEMAKERS
PACE, Vol. 23 November 2000, Part I 1673
Figure 4. Inhibition of ventricular pacing secondary tooversensing of the atrial depolarization in a patient withcomplete heart block, slow intratrial conduction, and aVentak AV implantable cardioverter defibrillator (ICD)coupled to an integrated bipolar lead. Real-time atrial(A) and ventricular (V) electrograms during DDD pacingat 70 beats/min show intermittent oversensing of theatrial signal in the ventricular channel (VS, arrows) 130ms after the atrial pacing artifact with inhibition ofventricular pacing. An escape beat falling in thepostatrial pace blanking period is detected as noise (VN).Decreasing the maximum sensitivity of the ICD solvedthe oversensing. (Courtesy of Andrea Natale, M.D.)

and antitheft surveillance equipment.74 Interac-tions with cellular phones and antitheft devicesare of particular concern because they are ubiqui-tous in modern society.
Our group75 highlighted the potential risk ofEMI in patients who depend on their ICD forbradycardia pacing. A patient with complete heartblock and a Ventak AV ICD developed multipleshocks and near fatal inhibition of pacing upon ex-posure to EMI from an antitheft device. Provoca-tive testing with similar equipment in a controlledenvironment reproduced the interaction. Themaximum distance at which ventricular oversens-ing occurred was 30 cm. When sensitivity was re-programmed from “nominal” to “least sensitive,”the interaction only occurred at a closer proximity.McIvor et al.76 exposed 25 volunteers with a vari-ety of ICDs to fields from different types of an-titheft devices and did not find instances of falsetachyarrhythmia detection, but the ICDs were notprogrammed to pace during the testing. Groh etal.77 studied the interaction between ICDs andthree models of antitheft devices (two electromag-netic and one acoustomagnetic) in 169 patients.No spurious detections occurred during a 10- to15-second walk through the gates. False VF detec-tion occurred in three patients (one Medtronic7219 and two CPI 1746) during a 2-minute expo-sure to the acoustomagnetic system. The incidenceof oversensing was much higher (19 [15%] of 126patients), when the 2-minute exposure was re-peated during continuous pacing. Oversensingwas severe (complete or prolonged pacing inhibi-
tion) in 7 (6%) patients, including the same threepatients who had spurious tachyarrhythmia detec-tion at baseline and four additional patients withVentritex ICDs during exposure to an electromag-netic system. In 12 (9%) patients, intermittent de-layed pacing (compatible with noise-augmented Twave oversensing) was seen. All the patients withserious interactions had an abdominal implant,but by multivariate analysis, diminished R waveamplitude and a Ventritex ICD were the only pre-dictors of interactions. It seems prudent to recom-mend that ICD recipients not linger in close prox-imity to antitheft devices. Cellular phones appearsafe for patients with ICDs. During in vitro testing,interference only occurred with some devices veryclose to the source.78,79 In vivo worst-case scenariotesting has not disclosed instances of significantoversensing.78,80
Prevention of OversensingSeveral measures can minimize the likeli-
hood of oversensing. The larger length and surfacearea of the right ventricular coil electrode com-pared to a ring could, in theory, increase the op-portunity for oversensing with integrated bipolarleads. Many implanters prefer integrated bipolarleads because they incorporate two defibrillationcoils in the same lead and increase defibrillationefficiency.81 However, a dedicated bipolar leadshould be considered in pacemaker dependent pa-tients. A dual coil lead with dedicated bipolarsensing would be a valuable option. This type oflead (Biotronik Kainox SL, Berlin, Germany) hasbecome available outside the United States.
Current ICDs allow some programming ofmaximum sensitivity (Table II). Although the cor-relation between the electrogram in sinus rhythmand VF is not perfect, the risk of undersensing VFdecreases when the ventricular electrogram is . 5mV during sinus rhythm.82,83 A search for a largeamplitude ventricular electrogram during implantmay be worthwhile, anticipating a need to de-crease sensitivity during follow-up. Programminga less sensitive setting during device-based defib-rillation testing provides information about the“safety margin” for VF detection.
The immediate reproducibility of the ventric-ular electrogram characteristics during inducedVF is fair-to-good for dedicated and integratedbipolar sensing configurations.84 The relation be-tween induced and spontaneous VF has not beeninvestigated extensively. The cycle length of in-duced VF in the same patient is reproducible, butmay not correlate with the cycle length of sponta-neous VF. However, spontaneous fibrillation issignificantly slower, suggesting that (at least interms of cycle length), VF induced during testingmay represent a worst-case scenario.85 Program-
PINSKI, ET AL.
1674 November 2000, Part I PACE, Vol. 23
Figure 5. Cross-talk without inhibition in a patient witha Ventak AV implantable cardioverter defibrillator (ICD).Real-time atrial (A) and ventricular (V) electrogramsshow consistent oversensing of the atrial artifact duringthe ventricular blanking (marked as noise [VN]).Repeated attempts at measuring the ventricular leadimpedance during this rhythm were unsuccessful. Theimpedance could only be measured after decreasing theventricular sensitivity or during pacing in the VVI mode.

ming of maximum sensitivity to values . 0.3 mVcould hinder the speed and accuracy of VF detec-tion. When this is done to avoid oversensing, re-producible prompt detection of induced VF mustbe verified.
It may be difficult to differentiate oversensingsecondary to normal automatic gain control algo-rithms from oversensing secondary to structurallead failure requiring operative lead replacement.Oversensing exclusively during deep breathing fa-vors the former. Reproduction of oversensing bypocket manipulation and measurement of abnor-mal or changing lead parameters (impedance, pac-ing threshold, electrogram amplitude) suggestslead failure. In unclear cases, frequent follow-upmay elucidate the cause. It may be necessary toreposition the defibrillation lead away from thediaphragm (e.g., in the right ventricular outflowtract) or to add a separate bipolar lead for pacingand sensing when chronic lead oversensing of di-aphragmatic signals cannot be adequately reducedor eliminated by reprogramming sensitivity.58,60
Undersensing Resulting in Asynchronous Pacingand Tachyarrhythmia Induction
Competition between asynchronous pacingand the spontaneous rhythm may induce ventric-ular tachyarrhythmias if the pacemaker stimuluscaptures the ventricle during its vulnerable pe-riod.86 This is extremely uncommon with an-tibradycardia pacemakers (attested to by the rou-tine magnet use to check pacemaker function).ICD patients may have a more vulnerable sub-strate. Saeed et al.87 studied stored electrogramsfrom 268 episodes of monomorphic VT, and foundthat 12 (4.5%) were induced by asynchronousventricular pacing after undersensing the previ-ous beat.
Spontaneous variation in signal amplitude, attimes exacerbated by the autoadjusting amplifiermechanism, makes transient undersensing rela-tively common in patients with ICDs. The electro-gram amplitude of a sinus beat following a prema-ture beat is often significantly lower than thepreceding beat.88 Depending on the coupling in-terval and the time constant of the autoadjustingmechanism (200–400 ms in different devices), thesensitivity may not be sufficiently high to sensethe postpause beat. Implementing a “dual-sensinglevel” reduces this problem. In the ELA Lyra ICD(ELA Medical, Plymouth, MN, USA), the auto-matic threshold control system uses a large timeconstant for the period immediately after detec-tion (to “hop” over T waves) and a shorter timeconstant afterwards.89 Changes in the amplifiergain setting have a more prominent role in thegenesis of undersensing with Ventritex ICDs.90
Their software-implemented automatic gain re-sponse is relatively slow, requiring a fixed numberof signals of different amplitude before changingits settings.65 There are no commercially availabledual chamber ICDs with this type of software-con-trolled automatic gain response.
To prevent cross-talk inhibition, Ventak AVdevices have a nonprogrammable 66-ms ventricu-lar blanking period after atrial paced events with-out “safety pacing” options. If the AV delay is pro-grammed long (i.e., $ 200 ms), undersensing of alate-coupled ventricular premature depolarization(VPD) falling in this long blanking period fol-lowed by ventricular capture in the vulnerable pe-riod could result in arrhythmia induction. Wehave seen a patient with a Ventak AV ICD inwhom “committed” ventricular pacing after a VPDfalling in the postatrial blanking period resulted inconsistent capture and triggered VT twice (Fig. 6).Proarrhythmia was solved by shortening thepaced AV delay to 150 ms to ensure delivery ofcommitted ventricular pacing during the myocar-dial effective refractory period. In the VentakPrizm ICD, the ventricular blanking after atrialpace is now programmable between 45 ms and 85ms (nominal 65 ms). In other dual chamber ICDs,the postatrial pacing ventricular blanking isshorter (Gem DR: 30 ms; ELA Defender II: 47 ms).Ventricular sensing during the AV delay (but afterthe blanking) invokes ventricular safety pacing.
Tachyarrhythmia Induction by AppropriatePacing After a Pause
Several investigators reported ventriculartachyarrhythmias occurring after a pause termi-nated by appropriate ventricular paced beats inICD patients.91,92 Although this has been consid-ered a form of ICD proarrhythmia, it is difficult todetermine if the tachyarrhythmias occurred be-cause of or despite ventricular pacing. Inductionof ventricular tachyarrhythmias by a prematurebeat after a pause (a long-short sequence) is wellestablished in the setting of QT prolongation93
and in patients with monomorphic VT.94
It has been hypothesized that the different ac-tivation wavefronts initiated by pacing or the highcurrent of the pacing pulse could promote reentry.Absence of arrhythmias after a similar or longerpause culminating in a conducted beat favors thishypothesis. Vlay and Vlay92 reported a patientwhose episodes of VF (always occurring after aventricular paced beat aborting a postectopic com-pensatory pause) were completely suppressed af-ter disabling antibradycardia pacing from the ICD.In pacemaker dependent patients, increasing thepacing rate91 or enabling rate-smoothing95 or rate-stabilization algorithms may be beneficial.
ICDS AS PACEMAKERS
PACE, Vol. 23 November 2000, Part I 1675

Transient Inhibition of Pacing after ShockDelivery
Initiation of pacing after shock delivery canbe transiently delayed in devices from Guidant(postshock pacing delay; nominal 3 s) and Ventri-tex (suppressed events/maximum post-therapypause; nominal two suppressed events). The ratio-nale for this delay is that (particularly in patientswithout “clean” arrhythmia conversion), transientafter-shock undersensing could result in asyn-chronous pacing and proarrhythmia. In pace-maker dependent patients, the additional 3 sec-onds of asystole following the tachyarrhythmiacould result in syncope (Fig. 7). In these patients,the programmable postshock pacing delay shouldbe minimized (i.e., 1.5 s in Ventak ICDs).
Failure to Abort Shocks after NonsustainedArrhythmias
Adding reconfirmation capabilities to ICDsdramatically decreased shock delivery for nonsus-tained ventricular arrhythmias.96 However, in somedevices, ventricular pacing interferes with the re-confirmation algorithm. Conservative reconfirma-tion algorithms aim to avoid withholding therapyfor low amplitude VF at the expense of promotingshock delivery after self-terminating ventricular ar-rhythmias in pacemaker dependent patients.
Current Ventak defibrillators function defacto as committed in pacemaker dependent pa-tients.97 Upon detection of tachyarrhythmias, thedual chamber devices switch their pacing mode toVVI at the programmed fallback lower rate (nomi-nal 70 beats/min). During capacitor charge, shock
diversion for nonsustained arrhythmias requiresthe presence of four ventricular “sensed” events ata rate below the tachycardia cut-off rate, but ven-tricular paced events count as tachycardia beats.The shock can also be aborted after completion ofcapacitor charge if two spontaneous ventricularevents below the rate cutoff are sensed during the2 seconds in which the pacing function is sus-pended (Fig. 8). However, if two spontaneous ven-tricular beats do not occur (a likely scenario inpacemaker dependent patients), the shock is de-livered upon expiration of the 2-second timer (Fig.9). The Biotronik Phylax AV also suppresses pac-ing after capacitor charge and delivers a shock ifasystole is present. The “shock confirmation pe-riod” during which the device looks for sponta-neous beats is short (twice the slowest pro-grammed tachycardia zone as default; four timesthe slowest programmed zone if the “extendedconfirmation period” feature is selected). This al-gorithm can result in delivery of committedshocks in patients with even mild or transientbradycardia. Programming strategies aimed ateliminating this problem are limited. The durationparameter can be extended to decrease the likeli-hood of capacitor charging for nonsustained VT.However, this could result in syncope beforeshock delivery if the tachyarrhythmia sustains. Itmay be necessary to pharmacologically suppressthe nonsustained VT or implant a separate pace-maker. In GEM devices, paced events occurringduring the reconfirmation period after capacitorcharge count as normal intervals and result in ap-propriately aborted shocks.
PINSKI, ET AL.
1676 November 2000, Part I PACE, Vol. 23
Figure 6. Induction of ventricular tachycardia (VT) by asynchronous pacing secondary tofunctional undersensing of ventricular premature depolarization (VPD). Stored atrial (A),ventricular (V), and shocking (S) electrograms show ventricular trigeminy with late ventricularextrasystoles (VE) falling 40 ms after the atrial artifact (ventricular blanking period). There isconsistent ventricular capture by the “committed” pulses (small arrows). The AV delay wasprogrammed at 200 ms and rate smoothing was enabled at 9%. The last asynchronous pulse (largearrow) triggers a run of rapid monomorphic VT (cycle length 260 ms), that the implantablecardioverter defibrillator (ICD) appropriately detects and terminates (not shown).

ICDS AS PACEMAKERS
PACE, Vol. 23 November 2000, Part I 1677
Figure 7. Transient postshock inhibition of pacing due to nominal settings in a patient with aVentak AV implantable cardioverter defibrillator (ICD) and complete heart block. Stored atrial(A), ventricular (V), and shocking (S) electrograms show an episode of ventricular fibrillation (VF)appropriately terminated by a 17-J shock. Three seconds elapsed between the shock and thedelivery of the first ventricular pacing pulse.
Figure 8. Confirmation algorithm in a Ventak AV implantable cardioverter defibrillator (ICD)after a nonsustained arrhythmia episode. Rapid ventricular tachycardia (VT) is detected, andcapacitor charge starts at the white arrow. Almost simultaneously, the arrhythmia self-terminates,and VVI pacing at 70 beats/min (857 ms) ensues. (This rate is faster than the intrinsic sinus rate.)Because 4 sensed events are not seen by the device, capacitor charge is completed (solid arrow).Pacing is then suspended for 2 seconds, allowing emergence of the spontaneous rhythm and theshock is appropriately diverted.

Delayed Tachyarrhythmia Detection Secondaryto a Short Detection Window
As stated previously, it is often necessary toprogram a relatively long (. 250 ms) postpaceventricular blanking period to avoid oversensingthe pacing-evoked repolarization response. Ven-tricular tachyarrhythmias that emerge during pac-ing may be temporarily masked by a lengthyblanking period, thereby delaying detection.When the postpaced blanking is fixed, the upperrate limit(s) may need to be lowered to ensuremaintenance of a tachycardia detection windowduring ventricular pacing.98 In the GEM DR de-vice, the maximum programmable pacing rate is120 beats/min. The GEM II DR allows program-ming of the upper tracking rate up to 150beats/min and of the upper sensor rate up to 130beats/min. However, the maximum achievable
pacing rate can be still limited by a series of pa-rameter interlocks to ensure that (1) the minimumpaced V-V interval is 60 ms longer than the tachy-cardia detection interval, (2) in dual chamber pac-ing modes, the shortest V-A interval must begreater than or equal to the tachycardia detectioninterval, and (3) no more than 50% of the ventric-ular pacing interval is blanked. If ventricularsafety pacing is enabled, the minimum ventricularpacing interval must be $ 2 3 (ventricular paceblanking 1 50 ms). Although, disabling ventricu-lar safety pacing is a possible way to resolve a pa-rameter interlock,99 it is risky in patients withcomplete heart block in view of the short posta-trial pace ventricular blanking.
The QT interval shortens at faster paced rates.Ventak AV devices take advantage of this phe-nomenon via a programmable dynamic ventricu-
PINSKI, ET AL.
1678 November 2000, Part I PACE, Vol. 23
Figure 9. Spurious shock for a nonsustained arrhythmia in a pacemaker dependent patient witha Ventak AV implantable cardioverter defibrillator (ICD). Stored atrial (A), ventricular (V) andshocking (S) electrograms show a rapid ventricular tachycardia (VT) (detected in the ventricularfibrillation [VF] zone) that terminates during capacitor charge. VVI pacing at 70 beats/min ensuesfor 2 beats. Upon completion of charge, pacing is suspended for 2 seconds with consequent asystolesecondary to complete heart block. A shock is delivered with no detrimental consequences, andafter a 2-second programmable postshock bradycardia pacing delay, atrioventricular (AV)sequential pacing is restored.

lar paced blanking period. Enabling this featureresults in automatic linear shortening of the ven-tricular blanking period from the programmedbaseline value (at the lower rate limit) down to the“dynamic” value (minimum allowed 150 ms) atthe upper rate limit. Worst-case scenario testing(maximum pacing output and ventricular sensi-tivity, shortest blanking period of 150 ms, maxi-mum rate of 120 beats/min) suggests that this fea-ture prevents oversensing of paced T waves whilemaintaining a wide tachyarrhythmia detectionwindow.100 Safe detection of VF occurring in thesetting of rapid paced rates in devices with a dy-namic postpace ventricular blanking was con-firmed by Ellenbogen et al.101 They compared thedetection time for induced VF during DDD pacingat 150 beats/min and DDDR pacing at 175beats/min in 26 patients with Ventak AV ICDs. AllVF episodes were detected with mean times of2.35 and 2.85 seconds, respectively. The mini-mum dynamic ventricular blanking was pro-grammed at 150 ms in all patients except the firsttwo. In a patient with minimum ventricular blank-ing programmed at 240 ms, detection of a slowerepisode of polymorphic VT induced during pac-ing at 175 beats/min was delayed up to 10.5 sec-onds due to a combination of intermittent under-sensing plus tachycardia beats falling in theblanking period. There is little safety informationon tachyarrhythmia detection during rapid pacingby ICDs with fixed postpace ventricular blanking.
Lack of Magnet-Triggered and ProgrammableAsynchronous Pacing Modes
ICD magnet responses generally inhibit tach-yarrhythmia therapy without effecting bradycar-dia pacing. Thus, pacemaker-mediated tachycar-dia will not terminate with magnet application indual chamber ICDs.98 Tachycardia termination re-quires reprogramming or pharmacological block-ade of VA conduction.
Current ICDs lack programmable asyn-chronous pacing modes (DOO, VOO) that are use-ful in pacemaker dependent patients during pro-cedures involving sources of EMI. (Ventak ICDshave temporary asynchronous pacing modes, butthey require a continuous telemetry link with theprogrammer.) In Ventak devices, a noise responsemode can be programmed to the DOO, VOO (nom-inal), or OOO. Programming an asynchronousmode in pacemaker dependent patients shouldprevent asystole in response to external interfer-ence. A 40-ms retriggerable noise reversion win-dow starts early after each sensed event. Recurrentnoise activity in this window would result inasynchronous pacing at the end of the escape in-terval. However, reversion may not occur reliably
in response to common sources of interferencesuch as electrocautery (Fig. 10). Ventritex ICDs,the Biotronik Phylax AV, and the Defender II alsoallow programming of an asynchronous pacingnoise reversion mode, but they differ in the re-quired frequency and duration of the signals.Medtronic devices do not incorporate a noise re-version mode. The manufacturers’ reluctance toprovide asynchronous pacing in patients with thesubstrate for sustained ventricular tachyarrhyth-mias is understandable. However, as these ICDsgain popularity in pacemaker dependent patients,the inability to program asynchronous pacingmodes (under strict monitoring) may become clin-ically detrimental.
Increased Incidence of Hardware and SoftwareDesign Problems
Although this has not been rigorously docu-mented, it appears that the increased complexityof ICDs makes them more prone than pacemakersto flaws in hardware or software design that canresult in (at times unheralded) pacing failure. Re-cent examples include an idiosyncratic form ofcross-talk inhibition with the original Ventak AVdevice due to an inadvertent , 2-ms hiatus duringthe nonprogrammable 66-ms ventricular blanking
ICDS AS PACEMAKERS
PACE, Vol. 23 November 2000, Part I 1679
Figure 10. Inappropriate inhibition of pacing duringapplication of electrocautery in a patient with a VentakAV defibrillator. This patient with complete heart blockand no reliable escape rhythm required thoracic surgery.The implantable cardioverter defibrillator (ICD) wasprogrammed in the “monitor only” mode. The stripshows the stored atrial (A), ventricular (V), and shocking(S) electrograms during a false detection of ventricularfibrillation (VF) secondary to electrocautery. Oversensingdoes not invoke the noise reversion mode (programmedDOO), instead resulting in pacing inhibition. The pausesare aborted by the paced beats from a separate temporaryventricular pacemaker (arrows) inserted preoperativelyin anticipation of this problem.

make “prophylactic” ICD implantation untenablein patients with indications for pacing alone. Thelimitations of these complex devices can be par-tially countered by heightened awareness and un-derstanding. In patients likely to use frequent ICDpacing, the type of device, sensing lead configura-tion, and lead position are crucial to avoid adverseoutcomes. Pacemaker dependent patients are es-pecially vulnerable. De facto committed devicesshould be avoided in them. A dedicated bipolarconfiguration is preferable. Worst-case scenariotesting at implant and during follow-up can en-sure necessary sensing safety margins. For pace-maker dependent patients, we recommend pro-gramming the minimum sensitivity to less thannominal after testing confirms reproducible VFdetection. Periodic clinic follow-up and promptdevice interrogation after shocks can identifyproblems and suggest appropriate reprogrammingmaneuvers.
PINSKI, ET AL.
1680 November 2000, Part I PACE, Vol. 23
period after atrial pacing.102 In Ventak AV II andIII, sudden failure of the ICDs to pace for up to 24hours could occur due to an interaction of the de-vices’ internal timing sequences.103 The observedfrequency of the problem was 0.035% permonth.104 A manufacturing flaw in someMedtronic GEM VR defibrillators could result insudden device failure after high voltage cathodalshocks delivered via integrated bipolar leads.105
Although these malfunctions were rapidly cor-rected (with software upgrades or appropriate re-programming), they highlight the possibility ofunexpected interactions between different com-ponents in dual chamber or rate responsive ICDs.
ConclusionsNewer ICDs capable of dual chamber, rate re-
sponsive pacing provide state-of-the-art therapyfor patients prone to tachy- and bradyarrhythmias.Their shortcomings, cost considerations aside,
References1. Saksena S, Poczobutt-Johanos M, Castle LW, et al. Long-term mul-
ticenter experience with a second-generation implantable pace-maker-defibrillator in patients with malignant ventricular tach-yarrhythmias. The Guardian Multicenter Investigators Group. JAm Coll Cardiol 1992; 19:490–499.
2. Niazi I, Kadri N, Mahmud R, et al. Absence of significant postde-fibrillation arrhythmias in patients with automatic implantabledefibrillators. Am Heart J 1988; 115:830–836.
3. Khastgir T, Aarons D, Veltri E. Sudden bradyarrhythmic death inpatients with the implantable cardioverter-defibrillator: Report oftwo cases. PACE 1991; 14:395–398.
4. Hayes DL, Rasmussen MJ, Friedman PA, et al. Pacemaker syn-drome in patients receiving ICDs. (abstract) PACE 1998; 21:891.
5. Elliott L, Gilkerson J. Advances in dual chamber implantable car-dioverter/defibrillators. J Interven Cardiol 1998; 11:187–196.
6. Brode SE, Schwartzman D, Callans DJ, et al. ICD-antiarrhythmicdrug and ICD-pacemaker interactions. J Cardiovasc Electrophys-iol 1997; 8:830–842.
7. Geiger MJ, O’Neill P, Sharma A, et al. Interactions betweentransvenous nonthoracotomy cardioverter defibrillator systemsand permanent transvenous endocardial pacemakers. PACE 1997;20:624–630.
8. Lavergne T, Daubert JC, Chauvin M, et al. Preliminary clinical ex-perience with the first dual chamber pacemaker defibrillator.PACE 1997; 20:182–188.
9. Nair M, Saoudi N, Kroiss D, et al. Automatic arrhythmia identifi-cation using analysis of the atrioventricular association: Applica-tion to a new generation of implantable defibrillators. Circulation1997; 95:967–973.
10. Dorian P, Newman D, Thibault B, et al. A randomized clinicaltrial of a standardized protocol for the prevention of inappropri-ate therapy using a dual chamber implantable cardioverter-defib-rillator. (abstract) Circulation 1999; 100:I-766.
11. Geelen P, Lorga Filho A, Chauvin M, et al. The value of DDD pac-ing in patients with an implantable cardioverter defibrillator.PACE 1997; 20:177–181.
12. Iskos D, Fahy GJ, Lurie KG, et al. Physiologic cardiac pacing in pa-tients with contemporary implantable cardioverter-defibrillators.Am J Cardiol 1998; 82:66–71.
13. Higgins SL, Williams SK, Pak JP, et al. Indications for implanta-tion of a dual-chamber pacemaker combined with an implantablecardioverter-defibrillator. Am J Cardiol 1998; 81:1360–1362.
14. Best PJM, Hayes DL, Stanton MS. The potential usage of dualchamber pacing in patients with implantable cardioverter-defib-rillators. PACE 1999; 22:79–85.
15. Stellbrink C, Auricchio A, Diem B, et al. Potential benefit ofbiventricular pacing in patients with congestive heart failure andventricular tachyarrhythmia. Am J Cardiol 1999; 83:143D-150D.
16. Jung W, Lüderitz B. Should all candidates for ICD therapy receive
a dual-chamber system? J Interven Cardiol Electrophysiol 1999;3:203–206.
17. Helguera ME, Maloney JD, Pinski SL, et al. Long-term perfor-mance of endocardial pacing leads. PACE 1994; 17:56–64.
18. Maloney JD, Hayes DL, Timmis GC, et al. Report of the policyconference of NASPE on device/lead performance and the devel-opment of a postmarket surveillance database. PACE 1991; 16:1945–1952.
19. Helguera ME, Maloney JD, Fahy GJ, et al. Clinical presentation ofendocardial pacing lead malfunction. Am J Cardiol 1996; 78:1297–1299.
20. Lawton JS, Ellenbogen KA, Wood MA, et al. Sensing-lead relatedcomplications in patients with transvenous implantable car-dioverter-defibrillators. Am J Cardiol 1996; 78:647–651.
21. Lawton JS, Wood MA, Gilligan DM, et al. Implantable car-dioverter-defibrillator leads: The dark side. PACE 1996; 19:1273–1278.
22. Degeratu FT, Khalighi K, Peters RW, et al. Sensing lead failure inimplantable defibrillators: A comparison of two commonly usedleads. J Cardiovasc Electrophysiol 2000; 11:21–24.
23. Mewis C, Kühlkamp V, Dörnberger V, et al. Poor long term per-formance of Endotak C-lead in patients with implantable defib-rillators. (abstract) PACE 1999; 22:806.
24. Jones GK, Bardy GH, Kudenchuk PJ, et al. Mechanical complica-tions after implantation of multiple-lead nonthoracotomy defib-rillator systems: Implications for management and future systemdesign. Am Heart J 1995; 130:327–333.
25. Tachyarrhythmia product performance report, number 4, Novem-ber 1998. Minneapolis, MN, Medtronic, Inc., 1998.
26. Luria DM, Chugh SS, Lexvold NY, et al. High rate of long-term en-dovascular lead failure with abdominally placed implantable de-fibrillators. (abstract) Circulation 1999; 100:I-568.
27. Gallik DM, Ben-Zur UM, Gross JN, et al. Lead fracture in cephalicversus subclavian approach with transvenous implantable car-dioverter-defibrillator systems. PACE 1996; 19:1089–1094.
28. Ong LS, Barold SS, Lederman M, et al. Cephalic vein guide wiretechnique for implantation of permanent pacemakers. Am Heart J1987; 114:753–756.
29. De Lurgio DB, Sathavorn C, Mera F, et al. Incidence and implica-tion of abrasion of implantable cardioverter-defibrillator leads.Am J Cardiol 1997; 79:1409–1411.
30. Mehta D, Nayak HM, Singson M, et al. Late complications in pa-tients with pectoral defibrillator implants with transvenous de-fibrillator lead systems: High incidence of insulation breakdown.PACE 1998; 21:1893–1900.
31. Schibgilla V, Diem B, Mahmout O, et al. Impedance rise, onlyclue to severe insulation damage in a transvenous single-leadAICD-system. PACE 1998; 21:1322–1324.
32. Gupta A, Zegel HG, Dravid VS, et al. Value of radiography in di-

agnosing complications of cardioverter-defibrillators implantedwithout thoracotomy in 437 patients. Am J Roentgenol 1997; 168:105–108.
33. GEM Implantable Cardioverter-Defibrillator System ReferenceGuide. Minneapolis, MN, Medtronic, Inc., 1998, p. 11–12.
34. Butter C, Auricchio A, Schwarz T, et al. Clinical evaluation of aprototype passive fixation dual chamber single pass lead for dualchamber ICD systems. PACE 1999; 22:169–173.
35. Niehaus M, Schuchert A, Thamasett S, et al. A new single leadelectrode for dual chamber ICD systems in the acute human clin-ical evaluation. (abstract) J Am Coll Cardiol 1999; 33:112A.
36. Crossley GH, Fitzgerald DM. Estimating defibrillator longevity: Aneed for an objective comparison. PACE 1997; 20:1897–1901.
37. GEM DR system reference guide. Minneapolis, MN, Medtronic,Inc., 1997, pp. 1–5.
38. Model 6945 RV-SVC lead. Clinical report. Minneapolis, MN,Medtronic, Inc., 1998.
39. Physician’s Manual. Endotakw EnduranceTM Models 0134/0135/0136 endocardial defibrillation leads. St. Paul, MN, CardiacPacemakers, Inc., 1998.
40. Crossley GH, Gayle DD, Simmons TW, et al. Reprogrammingpacemakers enhances longevity and is cost-effective. Circulation1996; 94:II245–247.
41. Andersen HR, Nielsen JC, Thomsen PE, et al. Long-term follow-up of patients from a randomised trial of atrial versus ventricularpacing for sick-sinus syndrome. Lancet 1997; 350:1210–1216.
42. Guarnieri T, Datorre SD, Bondke H, et al. Increased pacing thresh-old after an automatic defibrillator shock in dogs: Effects of classI and class II antiarrhythmic drugs. PACE 1988; 11:1324–1330.
43. Kudenchuk PJ, Poole JE, Dolack GL, et al. Prospective evaluationof the effect of biphasic waveform defibrillation on ventricularpacing thresholds. J Cardiovasc Electrophysiol 1997; 8:485–495.
44. Welch PJ, Joglar JA, Hamdan MH, et al. The effect of biphasic de-fibrillation on the immediate pacing threshold of a dedicatedbipolar, steroid-eluting lead. PACE 1999; 22:1229–1233.
45. Kessler DJ, Canby RC, Horton RP, et al. Effect of biphasic endo-cardial countershock on pacing thresholds in humans. Am J Car-diol 1996; 77:527–528.
46. Pinski SL, Fahy GJ. The proarrhythmic potential of implantabledefibrillators. Circulation 1995; 92:1651–1664.
47. Calkins H, Brinker J, Veltri EP, et al. Clinical interactions betweenpacemakers and automatic implantable cardioverter-defibrilla-tors. J Am Coll Cardiol 1990; 16:666–673.
48. Winkle RA, Bach Jr SM, Mead RH, et al. Comparison of defibril-lation efficacy in humans using a new catheter and superior venacava spring-left ventricular patch electrodes. J Am Coll Cardiol1988; 11:365–370.
49. Epstein AE, Kay GN, Plumb VJ, et al. Gross and microscopicpathological changes associated with nonthoracotomy im-plantable defibrillator leads. Circulation 1998; 98:1517–1524.
50. Epstein AE, Plumb VJ, Kirk KA, et al. Pacing threshold increasein nonthoracotomy implantable defibrillator leads: Implicationsfor battery longevity and margin of safety. J Interven Cardiol Elec-trophysiol 1997; 1:131–134.
51. Ehrlich S, Rashtian M, Kwasney J, et al. Improved sensing andpacing characteristics utilizing steroid eluting active fixationtransvenous defibrillator leads: A randomized trial. (abstract)PACE 1999; 22:869.
52. Jones GK, Bardy GH. Considerations for ventricular fibrillationdetection by implantable cardioverter defibrillators. Am Heart J1994; 127:1107–1110.
53. Brumwell DA, Kroll K, Lehmann MH. The amplifier: Sensing thedepolarization. In MW Kroll, MH Lehmann (eds.): ImplantableCardioverter-Defibrillator Therapy: The Engineering-Clinical In-terface. Norwell, Massachusetts, Kluwer Academical Publishers,1996, pp. 275–302.
54. Dunbar SB, Warner CD, Purcell JA. Internal cardioverter defibril-lator device discharge: Experiences of patients and family mem-bers. Heart Lung 1993; 22:494–501.
55. Kelly PA, Mann DE, Damle RS, et al. Oversensing during ventric-ular pacing in patients with a third-generation implantable car-dioverter-defibrillator. J Am Coll Cardiol 1994; 23:1531–1534.
56. Rosenthal ME, Paskman C. Noise detection during bradycardiapacing with a hybrid nonthoracotomy implantable cardioverter-defibrillator system: Incidence and clinical significance. PACE1998; 21:1380–1386.
57. Mann DE, Otto L, Kelly PA, et al. Effect of sensing system on theincidence of myopotential oversensing during bradycardia pac-ing in implantable cardioverter-defibrillators. Am J Cardiol 2000;85:1380–1382.
58. Swygman CA, Sloan SB, Homoud MK, et al. Oversensing of di-aphragmatic myopotentials by implantable cardioverter-defibril-lators: A unique cause of inappropriate therapy and inhibition ofpacing. (abstract) PACE 1998; 21:810.
59. Deshmukh P, Anderson K. Myopotential sensing by a dual cham-ber implantable cardioverter-defibrillator: Two case reports. JCardiovasc Electrophysiol 1998; 9:767–772.
60. Peters RW, Cooklin M, Brockman R, et al. Inappropriate shocksfrom implanted cardioverter defibrillators caused by sensing ofdiaphragmatic myopotentials. J Interven Cardiol Electrophysiol1998; 2:367–370.
61. Babuty D, Fauchier L, Cosnay P. Inappropriate shocks deliveredby implantable cardioverter-defibrillators during oversensing ofactivity of diaphragmatic muscle. Heart 1999; 81:94–96.
62. Sweeney MO, Ellison KE, Shea JB. Spontaneous and provoked di-aphragmatic myopotential oversensing in patients with ICDs: In-cidence and relationship to clinical variables, sensing lead con-figuration and sensing algorithms. (abstract) J Am Coll Cardiol1999; 33:142A.
63. Wolfhard UF, Jäger HP, Knocks M, et al. Alternative lead posi-tioning in the right ventricular outflow tract in transvenous im-plantation of ICDs. PACE 1995; 18:179–181.
64. Giudici MC, Paul DL, VanWhy KJ. Permanent right ventricularoutflow septal placement of active-fixation pacing-defibrillationleads: Safety and efficacy for pacing and defibrillation. (abstract)PACE 1999; 22:801.
65. Reiter MJ, Mann DE. Sensing and tachyarrhythmia detectionproblems in implantable cardioverter defibrillators. J CardiovascElectrophysiol 1996; 7:542–558.
66. Pinski SL. Inappropriate pacing due to autoperpetuation of theventricular rate stabilization algorithm: A manifestation of T-wave oversensing by ICDs. PACE 2000; 23:1446–1447.
67. Mann DE, Damle RS, Kelly PA, et al. Comparison of oversensingduring bradycardia pacing in two types of implantable car-dioverter-defibrillator systems. Am Heart J 1998; 136:658–663.
68. Perry GY, Kosar EM. Problems in managing patients with long QTsyndrome and implantable cardioverter-defibrillators: A report oftwo cases. PACE 1996; 19:863–867.
69. Böhm A, Pintér A, Préda I. QT dependent T wave sensing. PACE1998; 21:1290–1291.
70. Cossu SF, Hsia HH, Simson MB, et al. Inappropriate pauses dur-ing bradycardia pacing in a third-generation implantable car-dioverter defibrillator. PACE 1997; 20:2271–2274.
71. Curwin JH, Roelke M, Ruskin JN. Inhibition of bradycardia pac-ing caused by far-field atrial sensing in a third-generation car-dioverter defibrillator with an automatic gain feature. PACE 1996;19:124–126.
72. Schecter SO, Greenberg SM, Hoch DH, et al. Inappropriate dis-charges of an implantable cardioverter defibrillator secondary toautomatic adjustable gain of atrial tachycardia. PACE 1997;20:1721–1722.
73. Peters W, Kowallik P, Wittenberg G, et al. Inappropriate dischargeof an implantable cardioverter-defibrillator during atrial flutterand intermittent ventricular antibradycardia pacing. J CardiovascElectrophysiol 1997; 8:1167–1174.
74. Pinski SL, Trohman RG. Interference with cardiac pacing. CardiolClin 2000; 18:219–239.
75. Santucci PA, Haw J, Trohman RG, et al. Interference with an im-plantable defibrillator by an electronic antitheft-surveillance de-vice. N Engl J Med 1998; 339:1371–1374.
76. McIvor ME, Reddinger J, Floden E, et al. Study of pacemakerand implantable cardioverter-defibrillator triggering by elec-tronic article surveillance devices (SPICED TEAS). PACE 1998;21:1847–1861.
77. Groh W, Boschee S, Engelstein E, et al. Interactions between elec-tronic article surveillance systems and implantable cardioverter-defibrillators. Circulation 1999; 100:387–392.
78. Fetter JG, Ivans V, Benditt DG, et al. Digital cellular telephone in-teraction with implantable cardioverter-defibrillators. J Am CollCardiol 1998; 31:623–628.
79. Bassen HI, Moore HJ, Ruggera PS. Cellular phone interferencetesting of implantable cardiac defibrillators in vitro. PACE 1998;21:1709–1715.
80. Sanmartín M, Feranández Lozano I, Márquez J, et al. Ausencia deinterferencia entre teléfonos móviles GSM y desfibriladores im-plantables: Estudio in vivo. Rev Esp Cardiol 1997; 50:715–719.
81. Gold MR, Olsovsky MR, Pelini MA, et al. Comparison of single-and dual-coil active pectoral defibrillation lead systems. J AmColl Cardiol 1998; 31:1391–1394.
82. Ellenbogen KA, Wood MA, Stambler BS, et al. Measurement of
ICDS AS PACEMAKERS
PACE, Vol. 23 November 2000, Part I 1681

ventricular electrogram amplitude during intraoperative induc-tion of ventricular tachyarrhythmias. Am J Cardiol 1992; 70:1017–1022.
83. Michelson BI, Igel DA, Wilkoff BL. Adequacy of implantable car-dioverter-defibrillator lead placement of tachyarrhythmia detec-tion by sinus rhythm electrogram amplitude. Am J Cardiol 1995;76:1162–1166.
84. Taneja T, Goldberger J, Parker MA, et al. Reproducibility of ven-tricular fibrillation characteristics in patients undergoing im-plantable cardioverter-defibrillator implantation. J CardiovascElectrophysiol 1997; 8:1209–1217.
85. Bollmann A, Langberg JJ. The relationship between induced andspontaneous ventricular fibrillation. (abstract) Circulation 1997;96:I-529.
86. Bilitch M, Cosby RS, Cafferky EA. Ventricular fibrillation andcompetitive pacing. N Engl J Med 1967; 276:598–604.
87. Saeed M, Mahapatra S, Mouded M, et al. Initiation of ventriculartachycardia: Analysis of intracardiac electrograms in patientswith internal cardioverter defibrillator. (abstract) J Am Coll Car-diol 1999; 33:118A.
88. Callans DJ, Hook BG, Marchlinski FE. Effect of rate and couplinginterval on endocardial R wave amplitude variability in perma-nent ventricular sensing lead systems. J Am Coll Cardiol 1993;22:746–750.
89. Brewer JE, Perttu JS, Kroll MW, et al. Dual level sensing signifi-cantly improves automatic threshold control for R wave sensingin implantable defibrillators. PACE 1996; 19:2051–2059.
90. Callans DJ, Hook BG, Marchlinski FE. Paced beats following sin-gle nonsensed complexes in a “codependent” cardioverter defib-rillator and bradycardia pacing system: Potential for ventriculartachycardia induction. PACE 1991; 14:1281–1287.
91. Roelke M, O’Nunain S, Osswald S, et al. Ventricular pacing in-duced ventricular tachycardia in patients with implantable car-dioverter-defibrillators. PACE 1995; 18:486–491.
92. Vlay LC, Vlay SC. Pacing induced ventricular fibrillation in in-ternal cardioverter defibrillator patients: A new form of proar-rhythmia. PACE 1997; 20:132–133.
93. Locati EH, Maison-Blanche P, Dejode P, et al. Spontaneous se-quences of onset of torsades de pointes in patients with acquiredprolonged repolarization: Quantitative analysis of Holter record-ings. J Am Coll Cardiol 1995; 25:1564–1575.
94. Roelke M, Garan H, McGovern BA, et al. Analysis of the initiationof spontaneous monomorphic ventricular tachycardia by storedintracardiac electrograms. J Am Coll Cardiol 1995; 23:117–122.
95. Viskin S, Fish R, Roth A, et al. Prevention of torsade de pointes inthe congenital long QT syndrome: Use of a pause prevention pac-ing algorithm. Heart 1998; 79:417–419.
96. Hurwitz JL, Hook BG, Flores BT, et al. Importance of abortiveshock capability with electrogram storage in cardioverter-defib-rillator devices. J Am Coll Cardiol 1993; 21:895–900.
97. Mann DE, Kelly PA, Reiter MJ. Inappropriate shock therapy fornonsustained ventricular tachycardia in a dual chamber pace-maker defibrillator. PACE 1998; 21:2005–2006.
98. Kopp DE, Lin AC, Burke MC, et al. Adverse events with dual-chamber implantable cardioverter-defibrillators. (abstract) PACE1999; 22:896.
99. GEM II DR system reference guide. Minneapolis, MN, Medtronic,Inc., 1999, p. B-8.
100. Pinski SL, Haw J, Trohman RG. Usefulness of a dynamic post-pace ventricular blanking period in dual-chamber, rate-respon-sive implantable defibrillators. (abstract) PACE 1999; 22:897.
101. Ellenbogen KA, Edel T, Moore S, et al. A prospective random-ized-controlled trial of ventricular fibrillation detection time in aDDDR ventricular defibrillator. PACE 2000; 23:1268–1272.
102. Wilkoff BL, Ching EA, Chung MK, et al. Dual chamber pacemakerdefibrillators: A unique form of crosstalk inhibition. (abstract)PACE 1998; 21:847.
103. Coppess MA, Miller JM, Zipes DP, et al. Software error resultingin malfunction of an implantable cardioverter-defibrillator. J Car-diovasc Electrophysiol 1999; 10:871–873.
104. De Vries DW. Medical device safety alert. Guidant Corporation,December 4, 1998.
105. Tremmel J. Important patient management information.Medtronic, Inc., October 15, 1999.
PINSKI, ET AL.
1682 November 2000, Part I PACE, Vol. 23





























