Embed Size (px)
Citation preview

Peritoneal Dialysis
Nutritional Considerations in PD

Peritoneal Dialysis
Objectives
1. Discuss risks and importance of poor nutrition
2. How to assess nutritional state
3. How to achieve good nutrition

Peritoneal Dialysis
Nutrition

Peritoneal Dialysis
Alternatives to Avoid

Peritoneal Dialysis
Nutrition in Patients with CRF
Classes of nutrients - carbohydrates - fats - proteins - vitamins - minerals - water
Essential nutrients - amino-acids - essential fatty
acids - vitamins, elements
•Without these, an individualcannot function
•Dietary protein provide amino acids - body proteins
•Without sufficient dietaryprotein and energy, no growthor repair

Peritoneal Dialysis
Recommended Protein & Energy Intakes
# safe for 97.5 % of the population (WHO 1985) CRF patients with GFR 30-20 ml/min reduce protein and energy intake (MDRD study) Protein and energy intake lower than recommended in a large proportion (20-60%?) of HD and CAPD patients
Protein Energy (g/kg BW/day) (kcal/kg BW/day)
Healthy adults > 0.75# >35
CRF patients (non-dialyzed) ? 0.60 (high quality) >35
HD patients > 1.2 >35
CAPD patients > 1.2 >35

Peritoneal Dialysis
Protein-Energy Malnutrition
A state of deficiency resulting from inadequate intake of protein and/or energy relative to physiological needs leading to progressive changes in body composition and function and nutrition

Peritoneal Dialysis
B O D YS T O R E
IN T A K E L O S S E S
S U P P L Y D E M A N D
Nutrition is a balance between supply and demand

Peritoneal Dialysis
Negative Feedback Loop
Loss of renal function
Low protein andenergy intake
Anorexa nauseavomiting
Accumulation of uremic toxins
Low serumurea
MALNUTRITiON
J Bergström ASN -94

Peritoneal Dialysis
Major Metabolic Steps in Nutritional Deficiency Disease
Mortality
Morbid ity
Clin ical sym ptom s
Deterioration in capacityto function norm ally
Altered b io logical and physiologicalFunctions
Depletion of T issueLevels and Body Stores
Inadequate in takeIm paired absorption
Increased nutrient loss from body
Well nourishedindividual
Individual at risk
Malnourishedindividual
Dietary surveyNutrient intake
Biochem and physiol studies
Signs & symptoms
Vital statistic

Peritoneal Dialysis
Patients at Risk of Developing Malnutrition
Elderly Socially isolated Diabetes mellitus Recurrent peritonitis Active comorbid conditions Loss of RRF Inadequate solute removal

Peritoneal Dialysis
Risk Factors for Poor Nutrition
Late start of dialysis - Use of low protein diet
Poor appetite Social factors Protein loss through peritoneum
- Increased with peritonitis Catabolic state

Peritoneal Dialysis
Effects of Renal Insufficiency
Protein and Amino Acid Metabolism• Altered metabolism of proteins & amino acids• Intravascular alb pool may be reduced, even
though serum albumin is normal• Transferrin levels low• Increased catabolism (higher levels of
glucagon, PTH, toxins, acidosis)• Changes in amino-acid profiles• Increased risk of developing protein
malnutrition• Major cause of morbidity and mortality
DPI also diminishes with declining GFR

Peritoneal Dialysis
Protein-Calorie Malnutrition in CRF
Catabolic Factors Comorbid illness Physical inactivity Infections Metabolic acidosis Abnormal energy metabolism

Peritoneal Dialysis
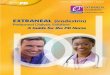
Protein intake and GFR
>50 25-50 24-10 <100.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
1.1
1.2
1.3
GFR
DPI
10ml / minGFR = 4.4g in DPI
Ikizler, JASN 1995

Peritoneal Dialysis
Protein Intake in Pre-dialysis
GFR (mls / min)
N = 1687
70 45 25 90.0
0.2
0.4
0.6
0.8
1.0
1.2
DPI
MDRD study ; JASN 1994

Peritoneal Dialysis
CAPD HD
Loss of amino acids
2-4 g/day
14-28 g/week
9-13 g/dialysis
27-39 g/week
Loss of glucose uptake ~25 g/dialysis(glucose free dialysate)
Loss of protein 5-15 g/day(higher with peritonitis)
0
Inflammatory stimuli
Low grade inflammation (particles chemicals)
Cytokine release
Blood membrane contact
Cytokine release
Catabolic Effects of Dialysis

Peritoneal Dialysis
Causes of Anorexia
Underdialysis particularly with loss of residual renal function
Sensation of abdominal fullness- Poor gastric emptying particularly in diabetics
Hyperglycaemia and glucose absorption from excessive use of hypertonic dextrose
Depression

Peritoneal Dialysis
Risk Factors for Obesity
Use of hypertonic dialysate, particularly 3.86% dextrose, to maintain fluid balance
High caloric intake, but low protein intake
Lack of physical activity

Peritoneal Dialysis
Causes of Low Plasma Albumin (Malnutrition vs. Malnourished)
True malnutrition Co-morbid conditions
- Infection
- Generalised vascular disease
- Chronic inflammation
- Proteinuria
- Malignancy
Old age Dietary preference

Peritoneal Dialysis
Assessment of Nutritional Status
History and physical examination looking for loss of weight and muscle wasting
Dietary history Plasma creatinine, urea, albumin, transferrin
- creatinine can mean muscle mass and not dialysis clearance
- creatinine can mean muscle mass and not dialysis clearance
Anthropometry SGA (Subjective Global Assessment) Biochemical / laboratory tests

Peritoneal Dialysis
Anthropometry
Mainly used as research tool
Wolfson 1984

Peritoneal Dialysis
Subjective Global Assessment
Four items assessed over 7 point scale
Weight change - What was weight change over last 6 months?
Anorexia- Has dietary intake changed?
Subcutaneous tissue- Fat and muscle wasting e.g., under eyes or shoulders- Muscle mass and wasting- Examining temporalis muscle, prominence of clavicles,
contour of shoulders etc

Peritoneal Dialysis
Subjective Global Assessment
1. Weight Change - in last 6 mths
- % (<5, 5-10,>10)
- in last 2 weeks
2. Dietary Intake - overall
- pattern
- duration
- type
3. GIT Symptoms - > 6weeks
4. Functional Capacity - overall +change
1. Loss of subcutaneous fat
2. Loss of muscle mass
3. Oedema
History
PE

Peritoneal Dialysis
Subjective Global Assessment
Severe malnutrition - ‘1 or 2’ ratings in most categories
Mild to moderate - ‘3, 4 or 5’ ratings in most categories
Mild to Well Nourished - ‘6 or 7’ ratings in most categories or continued improvement
A - Well nourished
B - Mild-Mod malnourished
C - Severely malnourished

Peritoneal Dialysis
There is No Single Magic Nutritional Index
Each has limitations
Use of combinations gives corroborating information

Peritoneal Dialysis
Non-Nutritional Factors Affecting Albumin
Fluid balance
Infection/inflammation
Urinary losses
High dialysate losses

Peritoneal Dialysis
Non-Nutritional Factors Affecting Albumin
Analytical method Gender Age Pregnancy Fluid balance
Infection/inflammation Cardiac disease Malignancy Protein losses
(urine, dialysate)
•Infection/inflammation related albumin is like an ‘negative’ acute phase protein•Association between cardiac disease and hypoalbuminaemia (Foley 1996)

Peritoneal Dialysis
Albumin as a Negative Acute Phase Reactant
Qureshi et al., 1995

Peritoneal Dialysis
Albumin as a Predictor
Strong predictor of morbidity and mortality (CANUSA study)
Albumin may be affected by protein intake
Albumin is affected by non-nutritional factors
Albumin may not increase in response to nutritional intervention
However,

Peritoneal Dialysis
Serum albumin alone is neither necessary nor sufficient to indicate
malnutrition

Peritoneal Dialysis
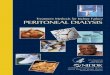
<=2.5 2.5-3.0 3.0-3.5 3.5-4.0 4.0-4.5 >4.50
10
20
Serum Albumin (mg/dl)
Rel
ativ
e D
eath
Ris
k
Lowrie et al, 1990
Serum Albumin and Death RiskHaemodialysis Patients

Peritoneal Dialysis
Target Protein Intake for PD
Nitrogen balance is the reference method for determining adequacy of protein intake
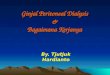
N Balance studies by Blumenkrantz and Bergstrom indicate that at 1.2 g protein/kg/day no patients were in negative nitrogen balance

Peritoneal Dialysis
Malnutrition in ESRDTarget Intake for PD
Blumenkrantz et al, KI 1982
4
5
3
2
1
1
0
2
0.9 1.0 1.1 1.2 1.3 1.4 1.5
Protein intake, g/kg body wt/day
Nit
roge
n b
alan
ce, g
/day

Peritoneal Dialysis
How Can This Target Be Achieved?

Peritoneal Dialysis
Methods for Nutritional Support in PD
Nutritional counseling Pharmacologic appetite stimulation Oral supplements Enteral formulas (nasogastric, PEG) Intravenous Intraperitoneal (nutritional dialysis)

Peritoneal Dialysis
Prevalence of Malnutrition is Similar in HD and PD*
Mode #Studies #Pts % Malnourished
HD 3 502 21-53 (28%)
PD 3 401 26-56 (36%)
* Evaluated by the same method

Peritoneal Dialysis
Nutrition: Guidelines 2002
All patients should undergo regular screening for undernutrition using as a minimum SGA, height weight and albumin
Diagnosis of undernutrition should be considered if any of following are met:- BMI < 18.5
- unintentional loss of oedema free weight of > 10% in last 6 mths
- plasma albumin below normal (value depends on assay)
- Low SGA scores

Peritoneal Dialysis
Nutrition: Guidelines 2002
If undernutrition suspected- refer to dietitian to assess dietary intake- measure CRP, plasma bicarbonate, dialysis adequacy
and residual renal function
Correct low dietary intake
If intake adequate, look for infection if CRP high, and other catabolic factors such as acidosis, thyrotoxicosis and poorly controlled diabetes

Peritoneal Dialysis
What is Nutrineal™?
Nutrineal™ is a peritoneal dialysis solution with
amino acids instead of glucose which integrates
dialysis and nutritional supplementation

Peritoneal Dialysis
Nutrineal™ Characteristics
Amino acids as osmotic agent
No glucose
No change in dialysis procedures
More physiologic pH
Osmolality equivalent to 1.5% glucose
Clearance equivalent to 1.5% glucose
40 mEq/L lactate

Peritoneal Dialysis
Amino Acid Content of Nutrineal™ (2.0 L)
Essential Nonessential
Histidine AlanineIsoleucine ArginineLeucine GlycineLysine ProlineMethionine SerinePhenylalanine TyrosineThreonineTryptophanValine
14.1g (64%) 7.9 g (36%)
Conditionally essential in renal patients

Peritoneal Dialysis
Bioavailability and Utilization Nutrineal™
• How much is absorbed?
• How is it utilized (Anabolic?)- Nitrogen balance- IGF-1

Peritoneal Dialysis
In just one exchange Nutrineal can deliver 25% of the target Daily Protein Intake*
Delivering 25% of daily protein intake
Jones MR, et al., PDI, 1998;18(2):210-216
With an absorption rate of 70-80% over 4-6 hours, one exchange of 2L Nutrineal provides approximately 18g of AAs to an average, stable, 60kg patient: that is 0.3 g/kg body weight/day, which represents 25% of the 1.2 g/kg body weight/day target intake1
* Recommended dosage for adults: one 2L or 2.5L bag/day
25%
Target DPI

Peritoneal Dialysis
0.16g/kg 0.3 g/kg
Bioavailability
AAsFor 60 kg
patient
Day 1 Protein and AA Losses
Day 2 AA gains
Jones et al, PDI 1998;18:210-216

Peritoneal Dialysis
The Therapy
Before Prescription:
1. Check adequacy (Kt/V > 2; Cr.Cl. > 50 L./week)
2. Correct possible acidosis (bicarbonate > 23 mmol/L.)
3. Verify protein intake
4. Review comorbid conditions
5. Assess nutritional status
Therapeutic Target:
Protein intake of around 1.2 g/kg/day

Peritoneal Dialysis
Nutrineal® : an efficient and compliant way of delivering AA’s whilst providing dialysis

Peritoneal Dialysis
Managing Protein Needs with Nutrineal
Target protein intake* = 1.2 g/kg/day
One exchange with Nutrineal contributes the equivalent of 0.3 g/kg in an average patient (20-25% of daily target)
*Kopple, 1997

Peritoneal Dialysis
Conclusion
Poor nutrition common in PD patients and is adverse risk factor
Important to assess nutritional status In malnourished patients
- correct identifiable comorbidities - assess dialysis adequacy and increase dose if near or
below target- maximise oral intake
Nutrineal