Peritoneal Dialysis in Australia and New Zealand - apsneph.org · Peritoneal Dialysis in Australia...
48
Peritoneal Dialysis in Australia and New Zealand Matthew D. Jose Professor of Medicine The University of Tasmania
Peritoneal Dialysis in Australia and New Zealand - apsneph.org · Peritoneal Dialysis in Australia and New Zealand Matthew D. Jose Professor of Medicine. ... over subcutaneous pathway
ANZDATA Registry Report, chapter 6, 2008. Kavanagh et al. Nephrol Dial Transplant (2004) 19: 2584–2591. Fang et al. NDT 2008; 23[12]: 4021–28. Verger et al. Kid Int Suppl 2006; 103: S12–20. Nakamoto et al. Perit Dial Int 2006; 26(2):136–43. Ho et al. Hong Kong J Nephrol 2005; 7: 38–46.
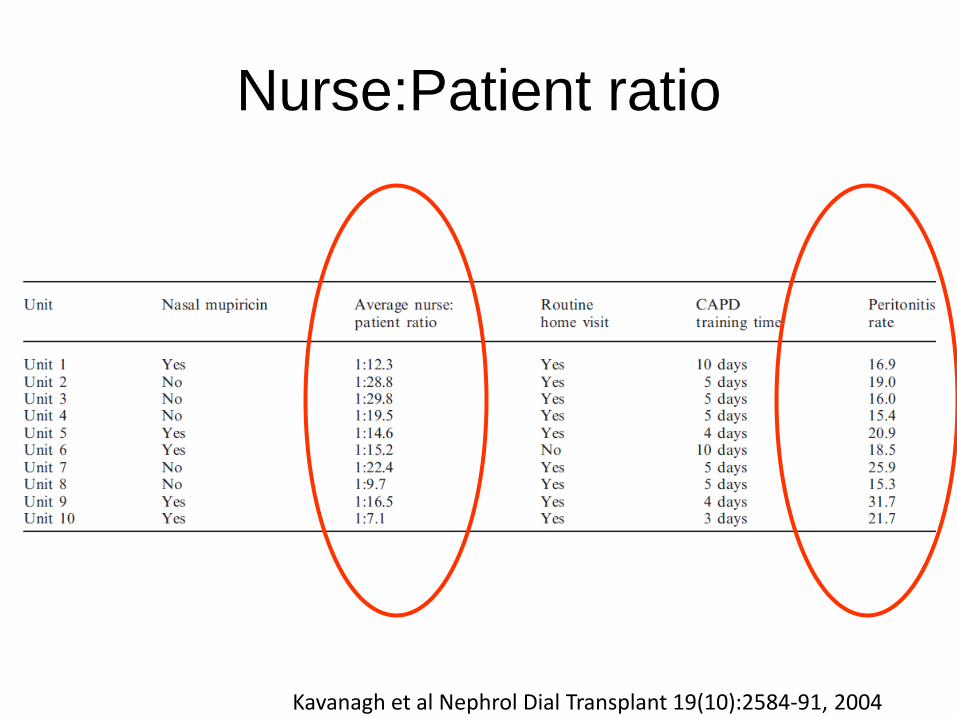
1:15 – 1:73 episodes / patient-month
プレゼンター
プレゼンテーションのノート
Only 35% of~150 countries providing RRT measure infection rates
Causes of PD technique failure
ANZDATA report, www.anzdata.org.au
Infectious complications
050
100150200
Tunnel/ ESI Acuteperitonitis
Recurrentperitonitis
Num
ber
プレゼンター
プレゼンテーションのノート
So we devloped a “Call to Action”, pointing out variation n practice right across ANZ, and suggested areas for improvement.
.3.4
.5.6
.7E
piso
des
per y
ear
2004 2006 2008 2010 2012 2014
Australia 2004-2013PD peritonitis rate
SAVICNSW
QLDTAS
ACTWA
NT
.4.6
.81
Epi
sode
s pe
r yea
r
By state, Australia 2004-2013PD peritonitis rate
Aboriginal population
プレゼンター
プレゼンテーションのノート
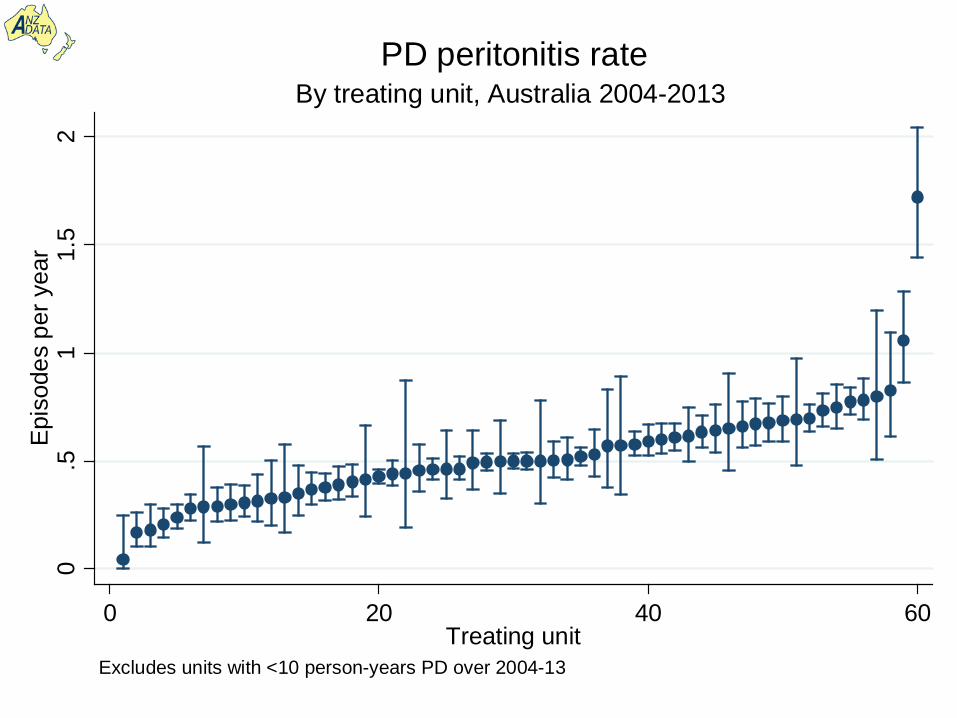
But there is still considerable variability
0.5
11.
52
Epi
sode
s pe
r yea
r
0 20 40 60Treating unit
Excludes units with <10 person-years PD over 2004-13
By treating unit, Australia 2004-2013PD peritonitis rate
ObesitySmokingLiving distantly from PD unitDepressionHypoalbuminemiaHypokalemiaMedical procedures (eg colonoscopy)Absence of vitamin D supplementationBiocompatible fluidsNasal S. aureus carrier statusPrevious exit site infectionPD against patient’s choicePrior hemodialysisPets Patient training
プレゼンター
プレゼンテーションのノート
Support of the person, avoiding infection and addressing modifiable risk factors are ciritical to sustaining someone on PD
• Exit site infection– Purulent drainage ± erythema
• Tunnel infection– Erythema, oedema or tenderness
over subcutaneous pathway– May require USS confirmation
Peritonitis Outcomes in ANZOrganism Cure Relapse Hospitalisation Catheter
RemovalInterim HD Permanent
HDDeath
Streptococci 87% 3% 74% 10% 3% 9% 1.4%
CoNS 77% 17% 61% 10% 2% 9% 1.0%
Culture negative
77% 14% 60% 12% 3% 10% 0.9%
Corynebact 67% 18% 70% 21% 7% 15% 2.4%
S. Aureus (all) 67% 20% 67% 23% 4% 18% 2.2%
NPGN 60% 11% 81% 31% 4% 26% 4.2%
MRSA 54% 19% 75% 31% 6% 25% 4.6%
Polymicrobial 52% 10% 83% 43% 5% 38% 3.9%
Enterococci 51% 15% 78% 37% 6% 32% 3.4%
Pseudomonas 50% 9% 79% 44% 11% 35% 3.1%
Fungal 9% 9% 98% 88% 12% 74% 8.6%
Overall 68% 14% 70% 22% 4% 18% 2.3%
Siva et al CJASN 4:957-64, 2009; Miles et al Kidney Int Jun 10 2009 [Epub ahead of print]; Barraclough et al NDT 2009; doi: 10.1093/ndt/gfp322; Govindarajulu et al Perit Dial Int [In press]; O’Shea et al BMC Nephrol 10:19, 2009; Barraclough et al Am J Kidney Dis [In press]
4. Patient Training
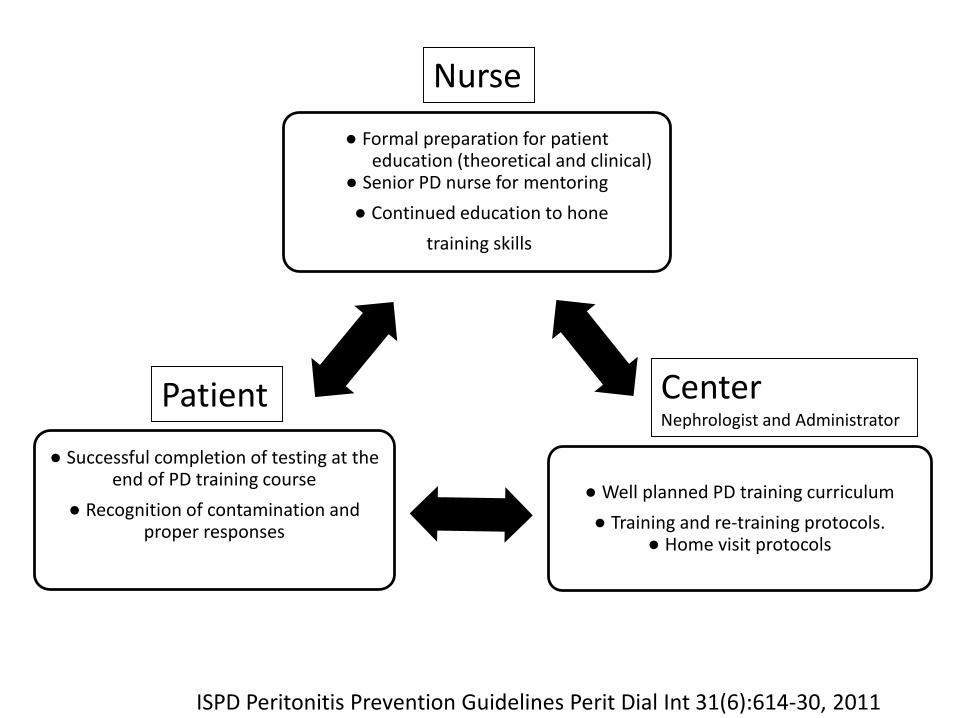
● Formal preparation for patient education (theoretical and clinical)
● Senior PD nurse for mentoring ● Continued education to hone
training skills
● Well planned PD training curriculum● Training and re-training protocols.
● Home visit protocols
● Successful completion of testing at the end of PD training course
● Recognition of contamination and proper responses
Nurse
Patient CenterNephrologist and Administrator
ISPD Peritonitis Prevention Guidelines Perit Dial Int 31(6):614-30, 2011
ISPD Training Guidelines• Nurse trainer, whenever possible• 1:1 trainer to patient ratio• Dedicated qualified trainers with training expertise (adult learning)• Continuous education of trainers• Multidisciplinary team involvement• Centralised and standardised training practices - adult learning
principles• Private, quiet, well-lit training space with adequate hygiene• Training tailored to individual’s learning capacity, language• Practical training - preferably with home-based instruction• No recommendations re duration of training • At end of training, patients need to meet minimum objectives:
– Safely perform all procedures– Recognise contamination and infection– Able to list appropriate responses
• Re-training of patients important• Home visits recommended
Bernardini et al Perit Dial Int 26:625-32, 2006
Nurse:Patient ratio
Kavanagh et al Nephrol Dial Transplant 19(10):2584-91, 2004
Influence of trainers’ experience in PD
200 PD patients in a single center in HK, 81 episodes of G+ peritonitis.
Chow et al Clin J Am Soc Nephrol 2(4):647-652, 2007
プレゼンター
プレゼンテーションのノート
“The finding of negative association between the trainers’ length of time in practice and peritonitis incidence reminds us that active continued learning and applying principles of adult learning might be the answers for the nurses to teach the patients.”
Training Protocols
• No RCTs• No trials comparing different training
schedules covering same content and curriculum
• Length of training does not correlate with outcomes
Objective Structured Assessment
Gadola et al Perit Dial Int 33(1):38-45 , 2013
Objective Structured
Assessment
Gadola et al Perit Dial Int 33(1):38-45 , 2013
OSA Score and Peritonitis
* *
Gadola et al Perit Dial Int 33(1):38-45 , 2013
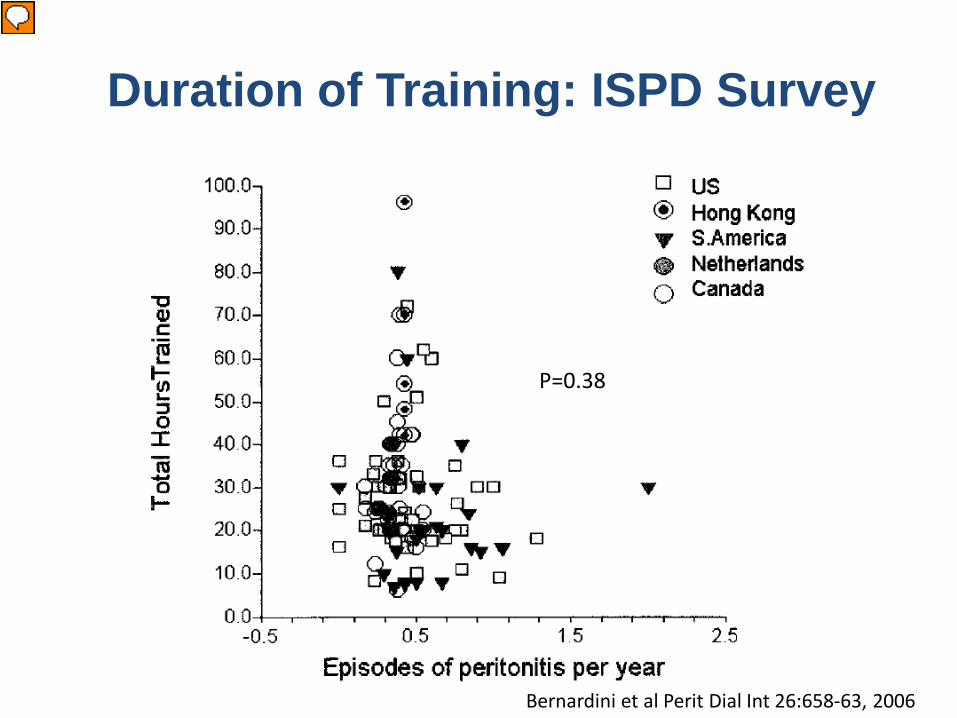
Duration of Training: ISPD Survey
Bernardini et al Perit Dial Int 26:658-63, 2006
P=0.38
プレゼンター
プレゼンテーションのノート
♦ Objective: To survey nurses around the world about current practices for peritoneal dialysis (PD) home training programs. ♦ Design: Random sampling of nurses to complete a written survey from the International Society for Peritoneal Dialysis Nursing Liaison Committee. ♦ Settings: United States, Canada, South America (Brazil, Columbia), The Netherlands, Hong Kong. ♦ Methods: Surveys and responses were sent by fax whenever possible, or by regular mail, or hand carried, or conducted by telephone. Results were stratified by geographic areas as well as by cumulative responses and were expressed as medians with ranges. Kruskal-Wallis was used to evaluate differences in responses. Associations between variables were tested with Pearson correlation. Univariate regression analysis was used to evaluate the impact of variables on peritonitis rates. Variables with p < 0.10 were included in a multivariate analysis. ♦ Results: A total of 317 nurses responded: 88 in the United States, 46 in Canada, 58 in South America, 58 in Hong Kong, and 67 in The Netherlands. This represented 37% of all surveys distributed. Respondents had a median of 12 years' experience in nephrology (range 1-35 years), but only 31% had a formal background in adult education. Nearly half received their guidance to patient training from a nurse colleague, 11% were guided by a corporate colleague, and 8% were simply self-taught. Clinics responding had a median of 30 PD patients (range 1-400) and reported they trained a median of 8 patients per year (range 0-86). Reported peritonitis rates were a median 0.46 per year or 1 episode every 26 months. Peritonitis rates, however, were not known by 53% of respondents. Total training time per patient had a very wide range of hours, from 6 to 96. There was no correlation between training time and peritonitis rates among the study respondents (p = 0.38), nor with any other variables. ♦ Conclusions: There is wide variation in practices for PD patient training programs within countries and around the world. Training time did not appear to be related to peritonitis rates. Randomized trials of training practices are needed to determine which approaches produce the best outcomes for patients.
ISPD PD Patient Training Guidelines
Bernardini et alPerit Dial Int 26:625-32, 2006
Home Training
P not reported
Castro et al EDTNA-ERCA J 28:36-9, 2002
N=84
プレゼンター
プレゼンテーションのノート
The objective of nursing is to increase health and well being, prevent morbidity and obtain the best physical and social rehabilitation. The nurse's role in Peritoneal Dialysis (PD) consists of promoting and supporting patients to perform self-care. In the'Text Book of Peritoneal Dialysis, published in 2000,the chapter dedicated to the nurses' role says:"Regular home visits are an important part of follow-up care, as the family and patient need to realize that continuing support is available... It is advisable that the first exchange after discharge from hospital is in the presence of a nurse... Early recognition and management of problems will assist in keeping the patient healthy and well rehabilitated, and will hopefully reduce hospital visits and inpatient stays" (1). Home care in Hospital Universitario La Paz has been developed with varying dedication over the years. Firstly, it was offered if significant problems appeared (1979-1990), later, home visits were started for some new PD patients (1990-1994) and follow up visits then ensued (1995-1996). In 1997, a project was undertaken which included home training for the first time in our unit, as well as periodic follow up visits. This project was shown to the Hospital Nurse Direction, and approved immediately. It started during the first term of 1997. There were several reasons which led us to undertake this project including the importance of providing PD at home and making it lifelong and it was felt that the hospital was an unfriendly environment in which to learn PD. The main objective was to establish early on, the patient's social environment and psychological status, and to assess how these influenced aspects of learning and adapting to PD. Most patients expressed a very good opinion about the home training. Only one patient rejected the presence of the nurse at home. The nursing team was very satisfied because early knowledge about the patient's psychosocial conditions and family environment was established. The incidence of peritonitis decreased.
Note presence of “false memory” The aim of this multicenter, quantitative, observational study was to analyze compliance and re-training needs of patients on peritoneal dialysis (PD) through the assessment of patient knowledge (with a Patient Questionnaire; phase 1) and patient behavior (home visit with a Score Card; phase 2). A total of 353 patients from 11 Italian centers participated in the first phase and 191 patients from nine centers in the second phase. Overall, 66% of questions on the Patient Questionnaire were answered correctly. Correct answers were more frequent in females than males, in patients under 55 years of age, and in those with higher education. The lowest rate of correct answers involved questions related to diet and physical activity (67% and 51%, respectively). Data collected during the home visit showed that 25% of patients were partially compliant with their drug therapy. Twenty-three percent of patients were non-compliant with the exchange protocol procedures, with a significant association between compliance and the incidence of peritonitis, and 11% were non-compliant with the exit-site protocol procedures without a statistically significant correlation to peritonitis. By combining the two evaluations, we found that approximately one-third (29%) of patients needed reinforcement of knowledge and ability to correctly perform PD as related to infection control and 27% for the correct use of drugs. Looking at the combined evaluation of infection control and drug use, results showed that 47% of patients needed re-training. This need for re-training was greater for younger patients (less than 55 years old), patients with lower education degree and patients in the early or late phase of PD therapy (less than 18 months or more than 36 months). Gender and degree of autonomy had no effect on the need for re-training.
ISPD Guidelines: Re-training
Piraino et al Perit Dial Int 31(6):614-30, 2011
5. Clinical Governance and professional standards
Pittsburgh University CQI Program
• Monthly meetings of– Hospital administrator– Nurse manager– Social worker– Dietician– PD nurses– 2 Nephrologists who followed most of the PD patients
• Episodes of peritonitis reviewed → root-cause analysis
• Exit-site infections reviewed• Action plan developed by the team, as needed.
Qamar et al Adv Perit Dial 25:76-9, 2009
Qamar et al Adv Perit Dial 25:76-9, 2009
MupirocinCAD forCyclers Gentamicin
Cream
PeritonitisRetraining
ESI
Peritonitis
Pittsburgh University CQI Program
ISPD 7 Key Infection Prophylaxis Strategies
• Training• Exit site care• Catheter placement• Antibiotic prophylaxis for procedures• Prevention of bowel source peritonitis• Prevention of fungal peritonitis• Connection methods
Mupirocin prophylaxis
プレゼンター
プレゼンテーションのノート
This technique has been employed in some units - Individual units are concentrating their efforts to reduce infection
プレゼンター
プレゼンテーションのノート
In addition all units receive their own technique survival data for PD to be able to compare with ANZ average
プレゼンター
プレゼンテーションのノート
As well as peritonitis rate
1. Preventive antibiotics for catheter insertion2. Preventive antibiotics for procedures3. Use of anti-staph agents to prevent exit site infections4. Training5. Use of biocompatible fluids where appropriate6. Prevention of constipation7. Treatment of acute peritonitis8. Treatment of refractory peritonitis9. Use of anti-fungal agents when on antibiotics
What is happening in the peritoneum?
Davies, AJKD 2014; 64 (6): 978-96
Encapsulating peritoneal sclerosis (EPS)
プレゼンター
プレゼンテーションのノート
Thickening of peritoneal membrane, central gathering of bowel loops and calcification
Davies, AJKD 2014; 64 (6): 978-96
Cho et al, Int J Nephrol 2014;
Clinical causes of inflammation in PD patients
1. Local, but not systemic inflammation is the main determinant of solute transport (PSTR)
Lambie et al, JASN 2013; 24; 2071
2. Systemic, but not local inflammation predicts patient survival
The newer, non-glucose solutions are more expensive. Therefore less than half of PD patients in ANZ use Icodextrin
Li PKT et al. EDEN & IMPENDIA. JASN 2013;24:1889-900
improved metabolic control, but worse fluid overload
プレゼンター
プレゼンテーションのノート
ABSTRACT Glucose-containing peritoneal dialysis solutions may exacerbate metabolic abnormalities and increase cardiovascular risk in diabetic patients. Here, we examined whether a low-glucose regimen improves metabolic control in diabetic patients undergoing peritoneal dialysis. Eligible patients were randomly assigned in a 1:1 manner to the control group (dextrose solutions only) or to the low-glucose intervention group (IMPENDIA trial: combination of dextrose-based solution, icodextrin and amino acids; EDEN trial: a different dextrose-based solution, icodextrin and amino acids) and followed for 6months. Combining both studies, 251 patients were allocated to control (n=127) or intervention (n=124) across 11 countries. The primary endpoint was change in glycated hemoglobin from baseline.Mean glycated hemoglobin at baseline was similar in both groups. In the intention-to-treat population, the mean glycated hemoglobin profile improved in the intervention group but remained unchanged in the control group (0.5% difference between groups; 95% confidence interval, 0.1% to 0.8%; P=0.006). Serum triglyceride, very-low-density lipoprotein, and apolipoprotein B levels also improved in the intervention group. Deaths and serious adverse events, including several related to extracellular fluid volume expansion, increased in the intervention group, however. These data suggest that a low-glucose dialysis regimen improves metabolic indices in diabetic patients receiving peritoneal dialysis but may be associated with an increased risk of extracellular fluid volume expansion. Thus, use of glucose-sparing regimens in peritoneal dialysis patients should be accompanied by close monitoring of fluid volume status.
Cho Y et al. NDT 2013;28:1899-907
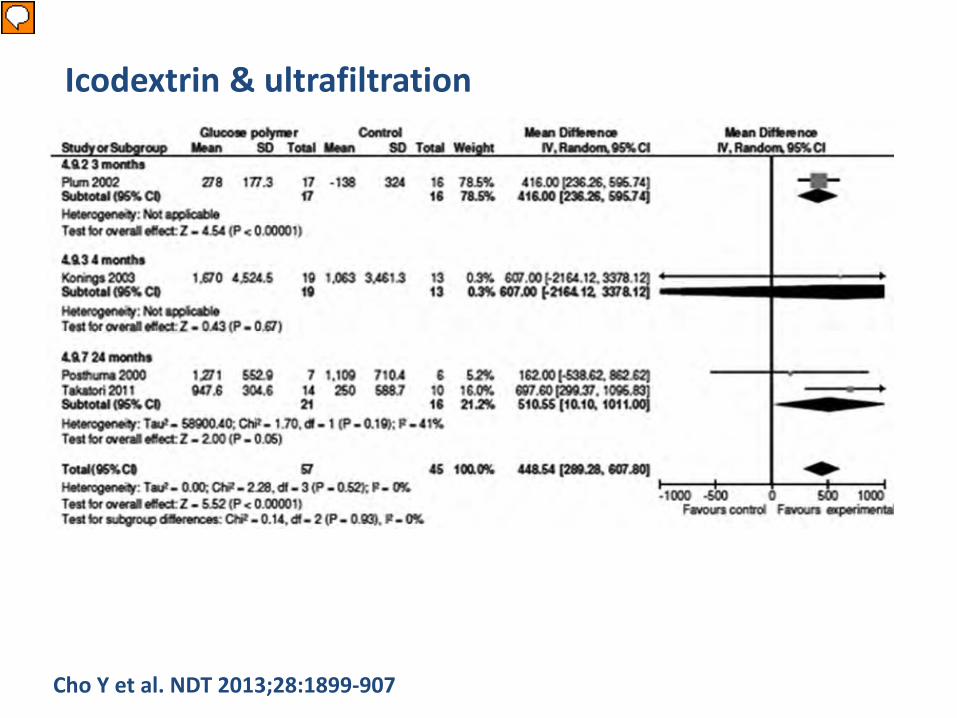
Icodextrin & ultrafiltration
プレゼンター
プレゼンテーションのノート
FIGURE 3 : Effect of glucose polymer PD solution (icodextrin) use on daily peritoneal ultrafiltration (mL/day). Background. Although icodextrin has been shown to augment peritoneal ultrafiltration in peritoneal dialysis (PD) patients, its impact upon other clinical end points, such as technique survival, remains uncertain. This systematic review evaluated the effect of icodextrin use on patient level clinical outcomes. Methods. The Cochrane CENTRAL Registry, MEDLINE, Embase and reference lists were searched (last search 13 September 2012) for randomized controlled trials of icodextrin versus glucose in the long dwell exchange. Summary estimates of effect were obtained using a random effects model. Results. Eleven eligible trials (1222 patients) were identified. There was a significant reduction in episodes of uncontrolled fluid overload [two trials; 100 patients; relative risk (RR) 0.30, 95% confidence interval (CI) 0.15–0.59] and improvement in peritoneal ultrafiltration [four trials; 102 patients; mean difference (MD) 448.54 mL/day, 95% CI 289.28–607.80] without compromising residual renal function [four trials; 114 patients; standardized MD (SMD) 0.12, 95% CI −0.26 to 0.49] or urine output (three trials; 69 patients; MD −88.88, 95% CI −356.88 to 179.12) with icodextrin use for up to 2 years. There was no significant effect on peritonitis incidence (five trials; 607 patients; RR 0.97, 95% CI 0.76–1.23), peritoneal creatinine clearance (three trials; 237 patients; SMD 0.36, 95% CI −0.24 to 0.96), technique failure (three trials; 290 patients; RR 0.58, 95% CI 0.28–1.20), patient survival (six trials; 816 patients; RR 0.82, 95% CI 0.32–2.13) or adverse events. Conclusions. Icodextrin prescription improved peritoneal ultrafiltration, mitigated uncontrolled fluid overload and was not associated with increased risk of adverse events. No effects of icodextrin on technique or patient survival were observed, although trial sample sizes and follow-up durations were limited.
Cho Y et al. NDT 2013;28:1899-907
Icodextrin & uncontrolled fluid overload
プレゼンター
プレゼンテーションのノート
FIGURE 4 : Effect of glucose polymer PD solution (icodextrin) use on uncontrolled fluid overload episodes.
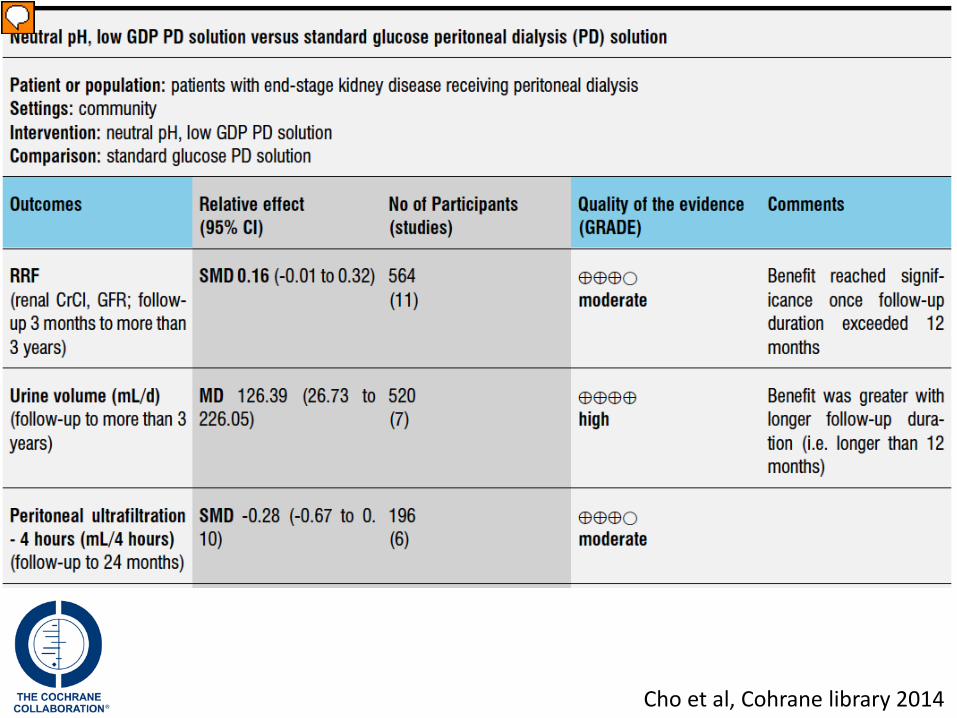
Cho et al, Cohrane library 2014
プレゼンター
プレゼンテーションのノート
Newer solutions led to preserved Residual renal function and better urine volume at >12 months, but note the absolute volume was only 126mls
Cho et al, Cohrane library 2014
プレゼンター
プレゼンテーションのノート
No benefit in pain, peritonitis nor technique failure. Hence in ANZ they have not been adopted widely
Cho et al, Cohrane library 2014
Neutral pH, low GDPgreater UO, higher RRF
Icodextrinbetter Ufless fluid overload
No effects on peritonitis, technique survival, patient survival, harm
Greater cost
プレゼンター
プレゼンテーションのノート
Author’s conclusions suggest some benefit, with no evidence of harm. No comment on cost effectiveness.