Embed Size (px)
Citation preview

PERFORMANCE OF THE BELGIUM
HEALTH SYSTEM IN INTERNATIONAL
COMPARISON
Academic session: “Looking back with an eye on the future”13 January 2017
Mark Pearson - Deputy DirectorEmployment, Labour and Social Affairs

BELGIUM HAS A HIGH PERFORMING HEALTH
SYSTEM
2

Some indicators of health status and quality of
care are amongst the best in the OECD
Life expectancy at birth
Ischemic heart disease
mortality rates
CHD hospital admission in
adults
Belgium OCDE
81.4 year
244.4 / 100 000 hab182.7 / 100 000 hab
80.6 year
114 / 100 000 hab.78.4 / 100 000 hab.
In-hospital case-fatality
rates for stroke 7.3 / 100 admissions 8.0 /100 admissions
Health expenditure as a %
of GDP10.4 % 9.0 %
Colorectal cancer five-year
relative survival62.4 %66.9 %
Source: OECD Health Statistics 2016.3

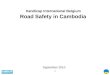
Most patients are positive about their
experience with ambulatory care
4Source: Commonwealth Fund International Health Policy Survey 2013 and other national sources.
D
Doctor spending enough time with patient in
consultation, 2013 (or latest year)
Doctor providing easy-to-understand explanations,
2013 (or latest year)
1. National sources. 2. Data refer to patient experiences with regular
doctor.
1. National sources. 2. Data refer to patient experiences with regular
doctor.
Note: 95% confidence intervals represented by H. Note: 95% confidence intervals represented by H.
59.6
78.3
79.3
79.6
80.0
80.9
81.8
83.6
84.9
85.1
86.3
86.5
86.9
88.2
89.6
92.6
95.6
97.2
97.5
0 20 40 60 80 100
Poland 1, 2
Sweden 2
Canada 2
Norway 2
France 2
United States 2
Israel 1
Switzerland 2
OECD18
Netherlands 2
United Kingdom 2
Australia 1
Estonia 1
Germany 2
Portugal 1, 2
New Zealand 1
Luxembourg 1
Czech Republic 1
Belgium 1
A Age-standardised rates per 100 patients
69.5
81.8
81.9
83.2
83.7
84.1
85.4
85.9
86.3
86.8
87.4
87.9
89.5
90.7
90.9
96.2
96.3
96.3
97.5
97.8
0 20 40 60 80 100
Poland 1, 2
Sweden 2
Switzerland 2
Israel 1
France 2
Norway 2
Canada 2
Australia 2
United States 2
Netherlands 2
Estonia 1, 2
OECD19
United Kingdom 2
Germany 2
New Zealand 1
Czech Republic 1
Japan 1
Portugal 1, 2
Luxembourg 1
Belgium 1
Age-standardised rates per 100 patients

But 3 important challenges do lie ahead for
Belgium
Inequalities in health and
access to care
Low spending on pre-
vention and rising risk
factors
Waste in clinical care
Direct impact on
population health
Direct or indirect
impact on health
care costs
Social and economic
consequences
1
2
3
5

REDUCING INEQUALITIES IN HEALTH AND ACCESS
TO CARE
6

Inequality in longevity by education groups is
among the highest in Belgium
B. 65 year-olds
35
40
45
50
55
60
65
ES
T²H
UN
LVA
CZ
EP
OL
SV
K²
CH
LO
EC
D³
SV
NB
EL
FIN
ME
XU
SA
DN
KTU
RN
OR
AU
TFR
AN
ZL
PR
T²A
US
SW
EIS
RIT
A²
GB
R
Low education High education
Men
35
40
45
50
55
60
65
LVA
ES
T²H
UN
PO
LC
HL
BE
LS
VK
²M
EX
CZ
ED
NK
US
AO
EC
D³
FIN
TUR
NO
RS
WE
NZ
LG
BR
SV
NIS
RA
UT
AU
SP
RT²
ITA
²FR
A
Women
Life expectancy by gender and educational attainment at age
25 (2012 or closest year)
Source: Fabrice Murtin (2016), "Annex: Inequalities in Longevity by Education in OECD countries:
Insights from New OECD Estimates
7

The burden of unmet needs for medical
examination fell heaviest on low income groups
Percentage of people with unmet needs
for medical examination, 2014
Source: Eurostat Database, based on EU-SILC. 8
Belgium EU

STRENGTHENING PREVENTION AND
PRIMARY CARE
9

Spending on prevention represents only
2.1% of current health spending
Source: OECD Health Statistics 2016.10

Risk factors are worsening, having social
and economic consequences
2nd highest rate
across the EU
(increased by 16%
from 2000 to 2014)
Less than 1 adult
in 5 is obese, but
on the rise in
recent years
At age 15, less
than 1 in 10 girls
report daily
physical activity
Risk factors are associated with numerous chronic diseases,
having large employment and productivity impacts
Alcohol
consumptionObesity rates Physical activity
High social disparities in risk factors
(eg. smoking prevalence is twice among low education groups)
Source: OECD Health Statistics 2016. 11

The total cost of mental health amounts
to 3.4% of GDP in Belgium
• Suicide mortality rates are 1.5 times
higher the EU average
• The indirect costs are larger than
direct medical costs of mental ill-
health
• People with mental disorders
underperform in the labor market :
• Employment rates are 15
percentage points lower
• Unemployment rates are 10
percentage points higher
• Higher risk of living in poverty
and social marginalisation
7%
12%
17%
36%
UnitedKingdom
EU 28 Belgium Lithuania
Suicide mortality rates, 2013Age-standardised rates of suicides, per 100 000
population
Source: Eurostat Database.12

REDUCING WASTE IN CLINICAL CARE
13

Prescribing patterns in primary care raise
concerns about appropriateness of care
Overall volume of antibiotics prescribed, 2014 (or nearest year)
Source: European Centre for Disease Prevention and Control 2016; OECD Health Statistics 2016.14

Adverse events are often preventable, while
devastating for patients
Percentage of hospitalised patients with at least one healthcare-
associated infection, 2011-12
Source: ECDC 2013 Point prevalence survey.
15

Collecting more patient-reported measures will
improve both health system policy and practice
Outcome of treatments
that people care about
People's experience of
care
• levels of pain;
• Ability to live
independently,
• quality of life, …
• Good communication;
• Being involved in
decisions about care,
• Convenience, …
In Sweden, patient-reported
outcomes were used to identify
brands of hip prosthesis that did
little to improve mobility and pain
Source: OECD (2013), OECD Reviews of Health Care Quality: Sweden 2013
It has improved patient outcomes,
and saved the Swedish health care
system an estimated SEK 1 billion
(EUR 100 million) over seven years.
16

Key policy challenges
17
More prevention and
strengthen primary
care
Tackle waste
2
3
• Reduce risk factors and postpone chronic
diseases
• Better manage chronic diseases
• Reduce the detrimental labour market
impacts of ill-health
• Ensure patients get care that is aligned
with the outcomes that matter to them
• PaRIS will standardise international
benchmarcking and develop new patient
reported indicators
Reduce inequalities1• Tackle financial and non-financial barriers
to improve access to care for
socioeconomically disadvantaged

Read more about OECD work Follow us on Twitter: @OECD_Social
Website: www.oecd.org/health
Newsletter: http://www.oecd.org/health/update
Thank you
OECD Health Ministerial
and
Policy Forum on the
Future of Health
Paris, 16-17 January 2017
18