Embed Size (px)
Citation preview

David F. Kallmes, MD2
Mary E. Jensen, MD
Index terms:Radiology and radiologists, How I
Do ItSpine, fractures, 30.4111, 30.4112Spine, interventional procedures,
30.1269Spine, vertebroplasty, 30.1269
Published online10.1148/radiol.2291020222
Radiology 2003; 229:27–36
Abbreviation:PMMA � polymethylmethacrylate
1 From the Department of Radiology,University of Virginia Health SciencesCenter, PO Box 800170, Charlottes-ville, VA 22908. Received March 26,2002; revision requested June 5; revi-sion received September 26; acceptedNovember 6. Address correspon-dence to M.E.J. (e-mail: [email protected]).
M.E.J. is a paid consultant (co-chair ofthe Scientific Advisory Board) for Par-allax Medical, which makes vertebro-plasty products, and a shareholder inthe company that owns Parallax Med-ical.
Current address:2 Department of Radiology, MayoClinic, Rochester, Minn.© RSNA, 2003
Percutaneous Vertebroplasty1
This review, aimed at current practitioners of vertebroplasty, highlights recentchanges in patient work-up and procedural techniques that have streamlined theauthors’ clinical practice. Preprocedural work-up, including history, physical exam-ination, and adjunctive imaging techniques, are discussed. Technical details arereviewed, including types of equipment, techniques of needle placement, and utilityof venography. Postprocedural issues are noted, including risk of subsequent frac-ture after vertebroplasty, long-term outcome of cement in the vertebral body, andutility of prophylactic vertebroplasty. Finally, the current state of evidence in supportof the efficacy of vertebroplasty are discussed, with particular attention to the needfor ongoing clinical trials.© RSNA, 2003
The first percutaneous vertebroplasty of which we are aware was performed in Europe in1984 and reported in the literature in 1987 (1), and the first vertebroplasty in NorthAmerica was performed in 1993 and reported in 1997 (2). There are currently over 253published reports focused on vertebroplasty. Most of the literature regarding percutaneousvertebroplasty is based on results in early technical reports (2,3) and case series (4), whichinclude methods for patient selection, procedural details, and postprocedural care. Sincethe time these previous studies were published, numerous modifications in patient eval-uation and procedural technique have been made to better define the appropriate patientpopulation, to decrease surgery time, and to optimize overall patient care. Some of thesemodifications have been published in the literature, but many have not.
Our target audience for this review is current practitioners of vertebroplasty who alreadyhave some knowledge of the basic indications, techniques, and vertebroplasty literature.Our goal is to identify specific areas where the approach to vertebroplasty has changedsubstantially over the past several years, with an emphasis on technical changes andclinical research. In addition, the current state of evidence on the efficacy of vertebroplastywill be discussed, with specific focus on the need for future clinical trials.
While this review, by necessity, contains our biases and opinions on the ideal way to runa vertebroplasty service, we do not want to imply that our techniques are the only validones. However, as it will become clear in the following review, we have made substantialefforts recently to justify our methods by careful study of our clinical database, whichcomprises approximately 530 treatment levels in 320 unique patients, and to reportimportant lessons from these studies.
PATIENT EVALUATION AND PREPROCEDURAL WORK-UP
A listing of appropriate clinical features for patients being considered for vertebroplastycan be found in the American College of Radiology Standards 2000–2001 (5). In our practice,by and large, we adhere to clinical indications in the American College of Radiologystandards. However, our approach to patient evaluation has changed substantially since1993. During the early development period of percutaneous vertebroplasty, the typicalpatient presented with subacute or chronic back pain that was unresponsive to medicaltherapy, with a new fracture documented on a conventional radiograph (2). Selectioncriteria included focal discomfort at palpation over the spinous process of the involvedvertebra and absence of radicular symptoms or neurologic deficits. Computed tomography(CT) or magnetic resonance (MR) imaging was often performed to evaluate for nerve rootcompression or retropulsed fragments. While most of these features are still consideredrelevant in the patient work-up, substantial changes in our approach to patient selectionhave been made on the basis of our clinical experience. These revisions involve imagingevaluation, physical examination, and determination of the duration of pain prior to theperformance of vertebroplasty.
27
Ra
dio
logy

Adjunctive Imaging forIdentification of SymptomaticFractures
Although much has been written aboutimaging procedures required prior to ver-tebroplasty, the role of such imaging re-mains largely speculative (empiric) at thispoint. Patients referred to us have oftenundergone a wide array of radiologic stud-ies, including conventional radiography,bone scintigraphy, CT, and/or MR imag-ing. We have tried to determine whichstudies are the most helpful in identifyingwho is most likely to respond to treatment.Patients with a documented new or sub-acute fracture on a conventional radio-graph and who meet the clinical criteriaregarding pain pattern usually proceed tovertebroplasty without undergoing otherimaging. Adjunctive imaging is indicatedin patients with single or multiple fracturesof uncertain age or when serial conven-tional radiographs are unavailable. Resultsfrom physical examination alone may bemisleading in this setting. Either bone scanimaging or MR imaging is potentially use-ful. There is only one published report ofwhich we are aware regarding the use ofscintigraphy in preprocedural evaluationof patients being considered for vertebro-plasty (6). In that small retrospective se-ries, a high percentage of patients (94%)achieved nearly complete pain relief aftervertebroplasty of those vertebral levels thatshowed increased uptake of tracer, even ina challenging patient population with
multiple fractures of uncertain age (Fig 1).In some cases, especially with multiplesevere compression fractures, exact label-ing of vertebrae on bone scans is difficult,although use of a radioactive and ra-diopaque marker helps make identifica-tion possible.
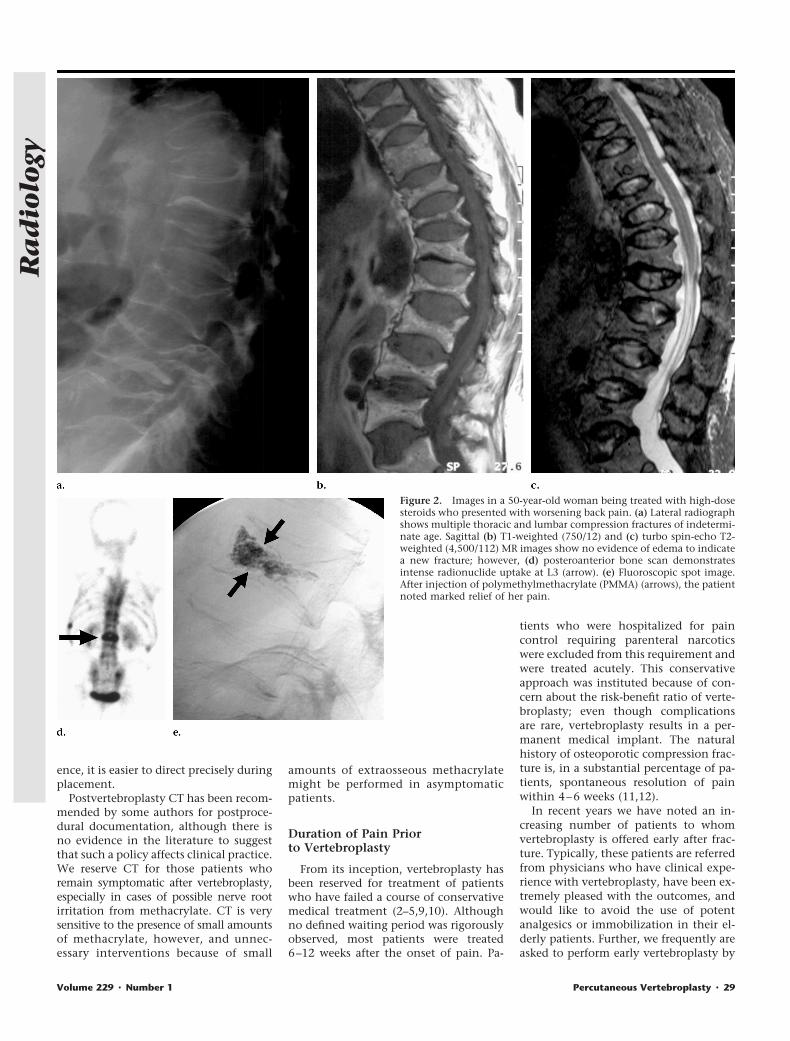
To our knowledge, there currently ex-ist no data regarding the use of MR im-aging in the evaluation of patients forconsideration of vertebroplasty, althoughsome investigators (7) have suggested thatedema seen on MR images is predictive ofa favorable response to vertebroplasty.Whereas MR imaging is sensitive for thedetection of acute compression fractures,we have noted a number of cases whereMR imaging has demonstrated normal(fatty) marrow signal intensity on T1- andT2-weighted images, while the bone scanwas abnormal. After treatment of the ver-tebrae that demonstrated increased activ-ity, a good clinical response was noted inthese patients (Fig 2). However, we havenot evaluated the use of imaging tech-niques such as short-tau inversion-recov-ery or contrast material–enhanced fat sat-urated MR imaging. What remains unclearis the appropriateness of these imagingmodalities with regard to age of fracture.
Role of CT in Vertebroplasty
The primary indication for CT prior tovertebroplasty is to evaluate the integrityof the posterior wall of the vertebral bodyand to assess posterior displacement of
fragments. Canal compromise from ret-ropulsed bone is not considered an abso-lute contraindication, provided there isno cord or nerve root compression orneurologic symptoms. To our knowl-edge, there are no written reports of im-mediate or delayed movement of thefracture fragment; however, if substantialretropulsion is present, we will proceedwith vertebroplasty but are careful tokeep the acrylic within the ventral aspectof the vertebral body and away from thefracture lines.
CT provides information about frac-ture involvement of the pedicles and pos-terior elements, which may help deter-mine the appropriate needle path. CTallows measurement of the pedicular di-ameter, which may influence the size ofthe needle chosen for puncture, particu-larly in the more gracile thoracic vertebralpedicles. However, we recently reviewedour series of thoracic vertebroplasties andfound that the size of the needle used didnot result in a difference in complicationrate (8). Forty-seven vertebral bodies weretreated in 34 patients. Eleven-gauge nee-dles were used in 40 (85%) of 47 treat-ments, while 13-gauge needles were usedin seven (15%) treatments. Postvertebro-plasty fracture involving the pedicle usedfor needle access was noted in one (2%) of47 treatments; this pedicle had been tra-versed by using a 13-gauge needle. Wefavor the larger-gauge needle over thesmaller needle because, in our experi-
Figure 1. Images in an elderly woman with low back pain. (a) Lateral radiograph shows multiple lumbar compression fractures of indeterminateage. Clinical examination demonstrated nonfocal tenderness over the lower back. (b) Posteroanterior and oblique bone scan images show markeduptake at L1 (arrows). After treatment of this single vertebra, the patient’s pain was relieved.
28 � Radiology � October 2003 Kallmes and Jensen
Ra
dio
logy
ence, it is easier to direct precisely duringplacement.
Postvertebroplasty CT has been recom-mended by some authors for postproce-dural documentation, although there isno evidence in the literature to suggestthat such a policy affects clinical practice.We reserve CT for those patients whoremain symptomatic after vertebroplasty,especially in cases of possible nerve rootirritation from methacrylate. CT is verysensitive to the presence of small amountsof methacrylate, however, and unnec-essary interventions because of small
amounts of extraosseous methacrylatemight be performed in asymptomaticpatients.
Duration of Pain Priorto Vertebroplasty
From its inception, vertebroplasty hasbeen reserved for treatment of patientswho have failed a course of conservativemedical treatment (2–5,9,10). Althoughno defined waiting period was rigorouslyobserved, most patients were treated6–12 weeks after the onset of pain. Pa-
tients who were hospitalized for paincontrol requiring parenteral narcoticswere excluded from this requirement andwere treated acutely. This conservativeapproach was instituted because of con-cern about the risk-benefit ratio of verte-broplasty; even though complicationsare rare, vertebroplasty results in a per-manent medical implant. The naturalhistory of osteoporotic compression frac-ture is, in a substantial percentage of pa-tients, spontaneous resolution of painwithin 4–6 weeks (11,12).
In recent years we have noted an in-creasing number of patients to whomvertebroplasty is offered early after frac-ture. Typically, these patients are referredfrom physicians who have clinical expe-rience with vertebroplasty, have been ex-tremely pleased with the outcomes, andwould like to avoid the use of potentanalgesics or immobilization in their el-derly patients. Further, we frequently areasked to perform early vertebroplasty by
Figure 2. Images in a 50-year-old woman being treated with high-dosesteroids who presented with worsening back pain. (a) Lateral radiographshows multiple thoracic and lumbar compression fractures of indetermi-nate age. Sagittal (b) T1-weighted (750/12) and (c) turbo spin-echo T2-weighted (4,500/112) MR images show no evidence of edema to indicatea new fracture; however, (d) posteroanterior bone scan demonstratesintense radionuclide uptake at L3 (arrow). (e) Fluoroscopic spot image.After injection of polymethylmethacrylate (PMMA) (arrows), the patientnoted marked relief of her pain.
Volume 229 � Number 1 Percutaneous Vertebroplasty � 29
Ra
dio
logy
patients who have previously beentreated successfully and have sustained asubsequent fracture. In most cases, wewill proceed with early vertebroplasty inthese patients. We recently have ana-lyzed our patient outcomes as a functionof fracture age (13). Even though subjec-tive pain relief was reported as excellentregardless of fracture age, patients withmore chronic fractures failed to improvewith regard to use of analgesics. This lackof decrease in medication requirementnoted in patients with more chronic frac-tures may have resulted from chemicaldependency, which suggests some disad-vantage to delaying vertebroplasty. Weno longer require a failure of medicaltherapy prior to our offer to perform ver-tebroplasty; however, adopting such acourse may result in nonpayment byMedicare. In addition, adoption of earlyvertebroplasty might result in substantialincreases in the number of such proce-dures performed, with resultant increasesin societal costs for treatment of painfulcompression fractures.
Physical Examination andVertebroplasty
In the past, focal pain elicited by pal-pation over the spinous process of thefractured vertebra has been used as a pa-tient-selection criterion. Patients havebeen excluded from treatment whentheir point tenderness has been locatedremote to the affected vertebra. The pres-ence of radicular pain involving thelower extremities or low back pain thatradiates to the hip may disqualify a pa-tient or lead to a different intervention,such as facet injections.
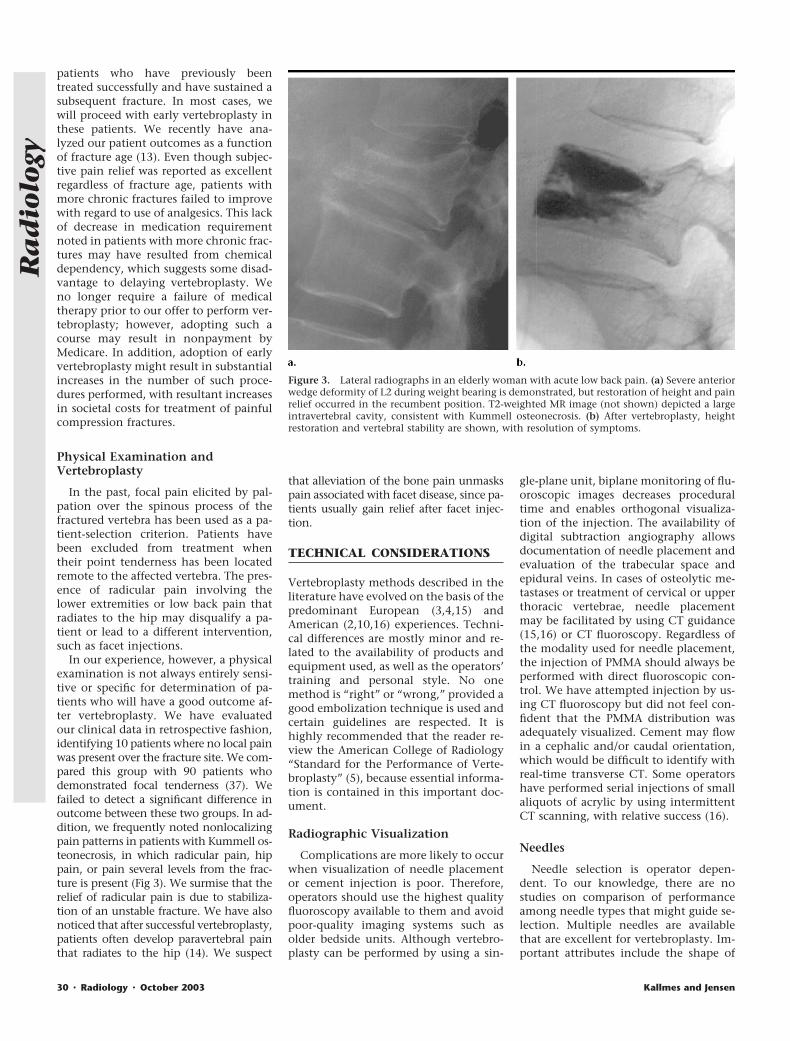
In our experience, however, a physicalexamination is not always entirely sensi-tive or specific for determination of pa-tients who will have a good outcome af-ter vertebroplasty. We have evaluatedour clinical data in retrospective fashion,identifying 10 patients where no local painwas present over the fracture site. We com-pared this group with 90 patients whodemonstrated focal tenderness (37). Wefailed to detect a significant difference inoutcome between these two groups. In ad-dition, we frequently noted nonlocalizingpain patterns in patients with Kummell os-teonecrosis, in which radicular pain, hippain, or pain several levels from the frac-ture is present (Fig 3). We surmise that therelief of radicular pain is due to stabiliza-tion of an unstable fracture. We have alsonoticed that after successful vertebroplasty,patients often develop paravertebral painthat radiates to the hip (14). We suspect
that alleviation of the bone pain unmaskspain associated with facet disease, since pa-tients usually gain relief after facet injec-tion.
TECHNICAL CONSIDERATIONS
Vertebroplasty methods described in theliterature have evolved on the basis of thepredominant European (3,4,15) andAmerican (2,10,16) experiences. Techni-cal differences are mostly minor and re-lated to the availability of products andequipment used, as well as the operators’training and personal style. No onemethod is “right” or “wrong,” provided agood embolization technique is used andcertain guidelines are respected. It ishighly recommended that the reader re-view the American College of Radiology“Standard for the Performance of Verte-broplasty” (5), because essential informa-tion is contained in this important doc-ument.
Radiographic Visualization
Complications are more likely to occurwhen visualization of needle placementor cement injection is poor. Therefore,operators should use the highest qualityfluoroscopy available to them and avoidpoor-quality imaging systems such asolder bedside units. Although vertebro-plasty can be performed by using a sin-
gle-plane unit, biplane monitoring of flu-oroscopic images decreases proceduraltime and enables orthogonal visualiza-tion of the injection. The availability ofdigital subtraction angiography allowsdocumentation of needle placement andevaluation of the trabecular space andepidural veins. In cases of osteolytic me-tastases or treatment of cervical or upperthoracic vertebrae, needle placementmay be facilitated by using CT guidance(15,16) or CT fluoroscopy. Regardless ofthe modality used for needle placement,the injection of PMMA should always beperformed with direct fluoroscopic con-trol. We have attempted injection by us-ing CT fluoroscopy but did not feel con-fident that the PMMA distribution wasadequately visualized. Cement may flowin a cephalic and/or caudal orientation,which would be difficult to identify withreal-time transverse CT. Some operatorshave performed serial injections of smallaliquots of acrylic by using intermittentCT scanning, with relative success (16).
Needles
Needle selection is operator depen-dent. To our knowledge, there are nostudies on comparison of performanceamong needle types that might guide se-lection. Multiple needles are availablethat are excellent for vertebroplasty. Im-portant attributes include the shape of
Figure 3. Lateral radiographs in an elderly woman with acute low back pain. (a) Severe anteriorwedge deformity of L2 during weight bearing is demonstrated, but restoration of height and painrelief occurred in the recumbent position. T2-weighted MR image (not shown) depicted a largeintravertebral cavity, consistent with Kummell osteonecrosis. (b) After vertebroplasty, heightrestoration and vertebral stability are shown, with resolution of symptoms.
30 � Radiology � October 2003 Kallmes and Jensen
Ra
dio
logy

the tip of the stylet (Fig 4) and the can-nula, as well as the type of handle. Weprefer to use a system that includes twotypes of stylets. The first stylet has a sharpmultibeveled or “diamond-shaped” tipand facilitates entry into the pedicle. Inour experience, single-beveled styletstend to slide off the pedicle. Once wehave traversed the pedicle, we typicallyremove the multibeveled stylet and placea single-beveled stylet. Although thereare no data to support this, we believethat the single bevel allows one to steerthe needle tip slightly (Fig 5).
Also available is a coaxial system with acurved nitinol cannula (Cook, Blooming-ton, Ind) for facilitating cross-midline ac-cess or specific placement (Fig 6). Withthis device, care should be used to avoidpuncture of the lateral wall of the verte-bral body. While most needle cannulashave a square distal shape, one availablecannula has a beveled distal end (Cook)that may allow one to direct cement in agiven direction. Multiple handle shapesare available, including standard grip de-signs (Cook; Manan Medical Products,Wheeling, Ill), whereas other manufac-turers offer novel designs such as an awlhandle (Parallax Medical, Scotts Valley,Calif). Last, we use 10-cm-long needles inmost patients but favor 15-cm-long nee-dles when treating lower lumbar verte-brae in larger patients.
Vertebroplasty with PMMA
Currently, the only biomaterial usedfor vertebroplasty in the United States is,to our knowledge, PMMA. PMMA is ap-proved for surgical implantation in mul-tiple bone locations. However, there is nocommercially available cement approvedfor percutaneous vertebroplasty. Use ofPMMA in vertebroplasty is performed in
an “off-label” manner. In most instances,approved devices can be used in routineclinical practice without the need for aninvestigational device exemption (IDE)from the FDA. If in doubt, however, it issuggested that practitioners check withlocal institutional review boards prior tostarting a vertebroplasty practice. In ad-dition, it is suggested that practitionersdiscuss the regulatory status of PMMAwith patients as part of the consent pro-cess. Finally, if vertebroplasty is to be per-formed as part of a clinical trial, then anIDE is required.
There are at least four PMMA productscurrently available, including Secour(Parallax Medical), Codman Cranioplas-tic (Johnson and Johnson, Bracknell,England), Osteobond (Zimmer, Warsaw,Ind) and Surgical Simplex P (Stryker-Howmedica, Limerick, Ireland). Impor-tant differences are seen among theseproducts with regard to polymerizationtime. The Stryker-Howmedica and Zim-mer products have relatively rapid poly-merization, wherein the cement becomestoo viscous to inject within 5–7 minutes.This polymerization time can be pro-longed by refrigerating the powderedpolymer pack and liquid monomer vialprior to use or by placing syringes filledwith the acrylic in an ice bath. The rapidpolymerization of the cement may limitthe ability to inject multiple levels with asingle mix. If using the Codman product,we recommend the slow-polymerizationtype, which allows 17–20 minutes ofworking time (unpublished data, 1999).Because it takes time for the powderedPMMA component to dissolve in the liq-uid monomer, the manufacturer of Sec-our recommends addition of a “solvationtime” of approximately 2–3 minutes aftermixing and before injection. This added
time allows the powder to dissolve intothe liquid, preventing their separationduring injection. Such separation maylead to the formation of a powder plugwithin the needle.
Opacification
Perhaps the most critical attribute thatfacilitates safe vertebroplasty is excellentopacification of cement. Authors of earlyreports (1–4) suggested use of either bar-ium sulfate and powdered tungsten ortantalum. We have observed that idealvisualization of cement is achieved byusing relatively large particles of barium,on the order of 1 mm in diameter, whichcan be tracked easily during slow injec-tion of cement. Smaller particles or finelysifted opacifiers provide a gray back-ground to the cement, but this gray back-ground is difficult to discern against theoverlying tissues. As such, we have aban-doned the use of tungsten powder. Trac-ers (Parallax Medical) is composed of var-ious sizes of barium sulfate particles andhas been approved by the U.S. Food andDrug Administration for cement opacifi-cation. Another barium product is of-fered by Bryan (Woburn, Mass). Barium isalready present in the Stryker-HowmedicaPMMA product, but it is not a sufficientamount for opacification, and use of addi-tional barium is recommended.
Antibiotics
We routinely add tobramycin (Nebcin;Eli Lilly, Indianapolis, Ind) to the cementmixture, on the basis of information inthe surgical literature supporting thispractice (17). Other practitioners advo-cate use of intravenously administeredantibiotics (7), but we reserve use of thesefor patients who are substantially immu-nocompromised. We have encounteredone case of iatrogenic infection, withStaphylococcus epidermidis, among 250consecutive patients treated with verte-broplasty (unpublished data, 2002). Thissingle patient was taking multiple immu-nosuppressive medications and thus wasat high risk. In similar situations in thefuture, we will use intravenous antibiot-ics in addition to antibiotics placed intothe cement.
Injection Devices
Although various methods have beenproposed for cement injection, the ma-jority of our experience has been gainedby using 1-mL syringes. The 1-mL sy-ringes are inexpensive, require minimalstorage space, and allow exquisite tactile
Figure 4. Needles suitable for vertebroplasty are supplied with avariety of stylets: A, single bevel; B, multibevel point; C, diamondpoint; D, threaded stylet. (Image courtesy of Parallax Medical.)
Volume 229 � Number 1 Percutaneous Vertebroplasty � 31
Ra
dio
logy

feedback during injection, which we con-sider to be important to prevent largeamounts of cement extravasation. Thereare several commercially available injec-tion devices (from Parallax Medical,Cook, and Stryker-Howmedica) for thedelivery of cement. These injection de-vices increase the distance between theoperator and the x-ray tube; facilitate an-teroposterior fluoroscopy during injec-tion, because the operator’s hands areout of the field; and allow a single con-nection of the injector to the needle. Useof 1-mL syringes rather than an injectiondevice is largely determined by operatorpreference.
VERTEBROPLASTY TECHNIQUE
Vertebral Venography
Some practitioners (2,18) of percutane-ous vertebroplasty described the use ofintraosseous venography prior to cementinfusion, to map the venous outlets fromthe vertebral body (Fig 7). On the basis ofthe venographic findings, the operatorwould gain confidence in his or her abilityto prevent extraosseous cement extravasa-tion, since the outlets would be knownalready. Alternatively, the needle could berepositioned if injection showed a large di-rect venous connection. Some practitio-ners even suggested protective venous em-bolization with gelatin foam sponges orother embolic agents prior to cement injec-tion.
Although we routinely used venogra-phy for several years during the develop-ment of vertebroplasty (2), we have aban-doned its use over the past 2 years.Because of our extensive experience withthe technique, we gained a reliable un-derstanding of the most likely routes forvenous extravasation, including epiduraland paravertebral routes. We have re-
cently performed a retrospective reviewin which we compared vertebroplastyperformed with and that performedwithout venography (18). We demon-strated no significant differences in fre-quency or amount of venous extravasa-tion and no difference in clinicaloutcome between patients in whomvenography was performed versus that inpatients in whom no venography wasperformed. Furthermore, in cases of apreexisting cavity or endplate fracture,contrast medium injected during venog-raphy may be impossible to wash outprior to cement injection, rendering itdifficult to visualize the barium-opacifiedcement.
Although we no longer consider it nec-essary to perform venography prior tocement infusion, some operators mayfind the venogram to be comforting, as itdefines the exact point where the basiver-tebral plexus exits the vertebral body andoutlines the paraspinal venous system.Previously, authors (19) have reportedthe use of venography to help detect di-rect venous communications and predictPMMA flow characteristics and potentialsites of egress.
Needle Placement
Unipedicular versus bipedicular vertebro-plasty.—Authors of early reports (1–4) ofvertebroplasty described bipedicular ver-tebroplasty with separate cement infu-sions into both hemivertebra with theuse of two needles. Bipedicular injectionswere performed in an effort to maximizevolume of cement placed into the verte-bra. However, two needle placementsand two injections result in relativelylong procedures. Further, monitoring ofthe second injection is often problem-atic, given that the indwelling barium-
opacified cement from the initial injec-tion obscures visualization.
To speed procedure time and eliminatethe need for separate injections, manypractitioners have adopted a unipedicu-lar technique for vertebroplasty. Thistechnique involves placement of the nee-dle tip in the midline of the ventral as-pect of the vertebral body by using atranspedicular approach, with the expec-tation that the central portion of the ver-tebra can be filled (20). The technique isslightly different when comparing lum-bar to thoracic vertebra. In the lumbarregion, the appropriate oblique approachcan be found by angling the anteropos-terior tube laterally until the “scotty-dog” profile is seen over the pedicle, withapproximately 20° of lateral angulation.
Figure 5. (a) Lateral radiograph shows initial trajectory (arrow) of the needle, which places the tip anteriorly at the midportion of the vertebralbody. However, use of a beveled stylet, with bevel face pointing upward, deflects the tip downward. (b) Lateral radiograph shows that final positionof the cannula approximates the anterior inferior corner of the vertebral body (arrow).
Figure 6. Lateral radiograph shows curvedstylet, which allows the operator to depositPMMA precisely at superior (arrowheads) andinferior (arrows) endplates. The referring phy-sician specifically requested that reinforce-ment of these locations be performed prior to asurgical procedure.
32 � Radiology � October 2003 Kallmes and Jensen
Ra
dio
logy

The pedicle is punctured in its midpor-tion, with the needle tip placed in theupper one-third of the pedicle, just me-dial to the lateral pedicular border. Sub-stantial angulation is more difficult inthoracic vertebrae, because the pediclesare oriented in the straight anteroposte-rior direction. The pedicular outline maybecome difficult to visualize with mini-mal angulation. In our experience, theproper obliquity is achieved by anglingthe anteroposterior tube laterally untilthe pedicle projects over the medial one-fifth of the vertebral body (19).
We have performed a retrospective re-view of cases performed with a unipe-dicular versus a bipedicular technique(20). We were unable to demonstrate anydifference in clinical outcome betweenthe two groups, even though there was asmall statistically significant difference inpercentage of vertebral body filling whencomparing unipedicular and bipedicularprocedure results. On the basis of theseconsiderations, we use the unipedicularapproach in essentially all cases.
Volume of cement.—The amount of ce-ment required for good clinical outcomehas never been systematically studied, toour knowledge. Testing of cadavericspines suggests that up to 8 mL of cementis required to achieve biomechanical in-tegrity (21). However, the risk of ex-traosseous extravasation of cement in-creases with increasing volumes ofcement injected (22). To minimize therisk for such extravasation, we tend toplace relatively small amounts of cementinto a given vertebral body.
We have recently reviewed our experi-
ence when performing “high-volume”vertebroplasty, defined as injection into avertebral body of more than 3 mL, versus“low-volume” vertebroplasty, defined asinjection of less than 3 mL (unpublisheddata, 2002). Although we have not yetcorrelated such volumes to vertebral levelor percentage of collapse, we did not de-tect clinically important differences inoutcome between the low- and high-vol-ume groups. These data may offer com-fort to inexperienced practitioners whowant to minimize risk for extraosseouscement extravasation by “underfilling”the vertebral body.
Potential cardiovascular changes withPMMA administration.—Authors of re-ports in the orthopedic literature (23–25)have shown cardiovascular compromisedue to instillation of large amounts ofPMMA during hip arthroplasty. We havestudied a large cohort, including 142 ver-tebroplasties in 78 patients, where de-tailed cardiovascular data were docu-mented before, during, and after PMMAinjection (26). We noted no change inmean arterial blood pressure or heart rateat any point in time. There was a statis-tically significant decrease in percentageof oxygen saturation 10 minutes afterPMMA injection; however, this differ-ence was very small, with mean prepro-cedure saturation of 98.0% and meanpostprocedural saturation of 97.4%, andwas considered clinically irrelevant.
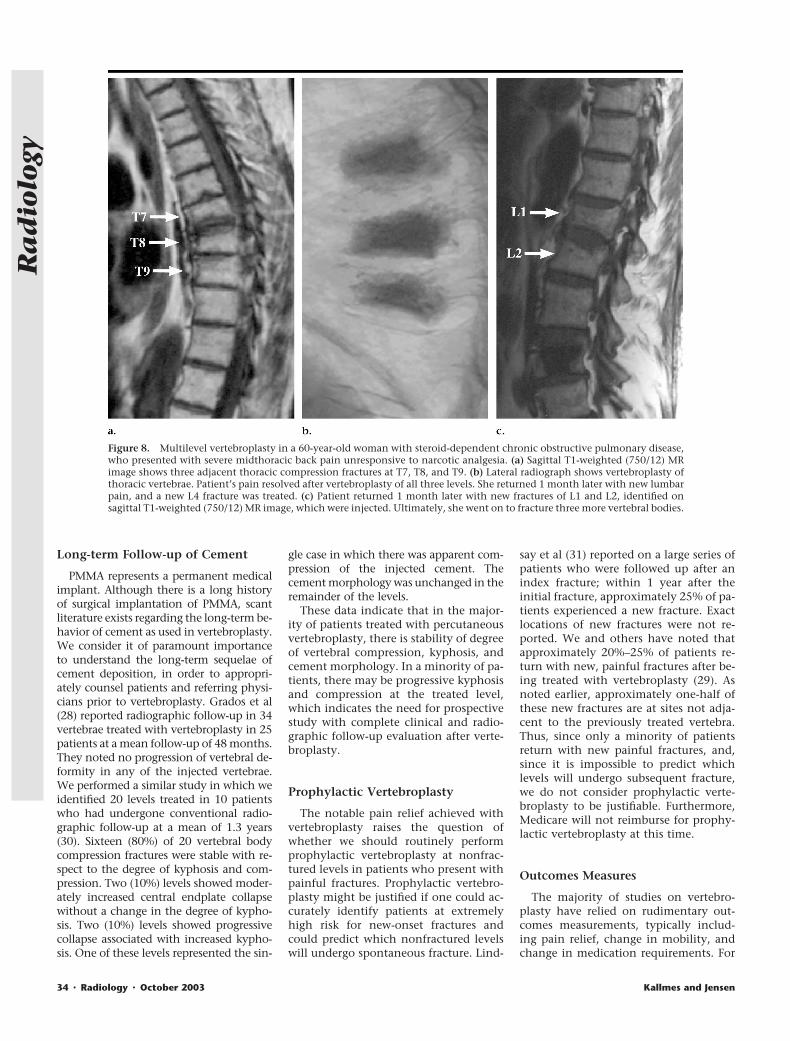
Multilevel vertebroplasty.—Currently, manypractitioners routinely treat multiple frac-tures at a single session. Not uncommonly,we will treat two to three levels at onesession (Fig 8) and have treated up to five
vertebrae at a single session. We know ofno published study in which the safety ofmultilevel vertebroplasty has been investi-gated. We have studied the relative efficacyof single- versus multilevel vertebroplasty(unpublished data, 2002). Three groupswere studied, including patients treated ata single level at one session, patientstreated at multiple levels at a single session,and patients treated at multiple levels atmultiple sessions. When performing mul-tilevel vertebroplasty, we routinely placemultiple needles at once before preparingthe cement. We then inject multiplepedicles sequentially, using the same batchof cement. In this retrospective review,we demonstrated equivalent pain reliefamong the three groups. To our surprise,however, we noted that mobility was sig-nificantly more impaired for the single-level group than for the other groups. Thereason for this difference between groups isunknown.
OUTCOMES
Risk of Subsequent Fracture
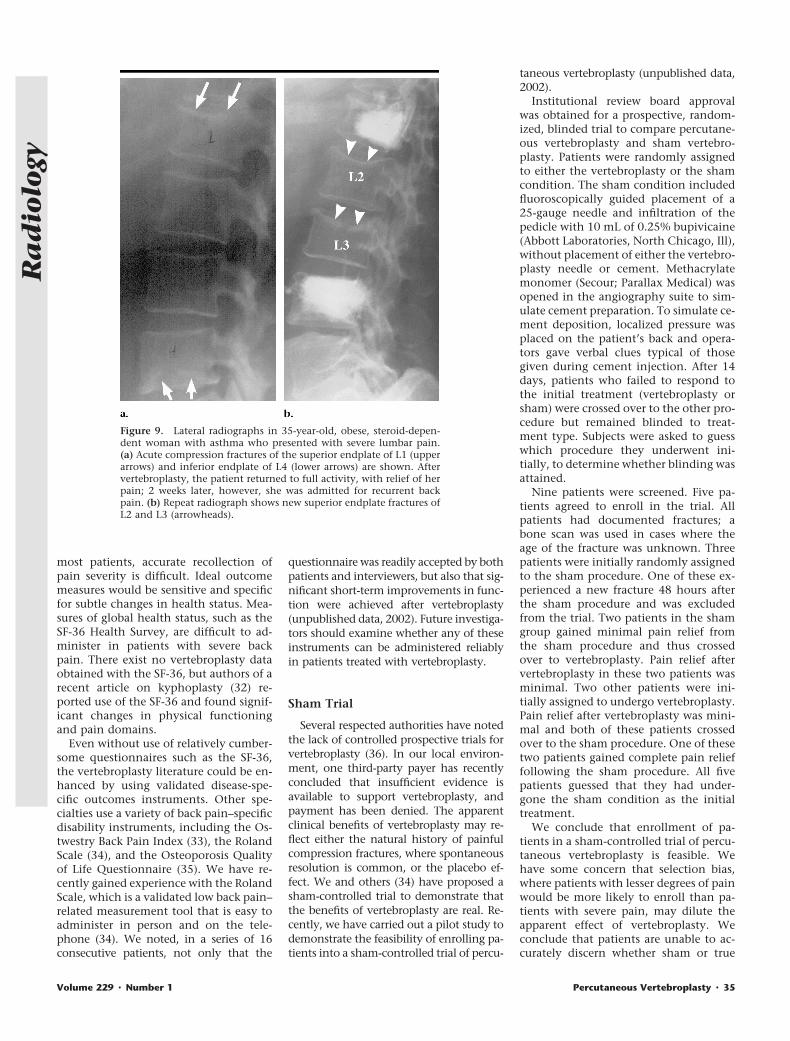
The effect of cement deposition intoan osteoporotic fracture on the risk forsubsequent fractures at other levels re-mains unclear. There is theoretical con-cern that diminishment of the compli-ance of one vertebra by means of cementinjection may place the remainder of theaxial skeleton at greater risk for collapse.Previously, authors (28) have noted asmall increased risk of new-onset frac-tures in the vicinity of the treated levelbut did not identify specific levels in re-lation to treated vertebrae. We have ret-rospectively reviewed our data to identify58 patients who returned with new frac-tures following vertebroplasty. One-halfof these new fractures were adjacent tothe initial vertebroplasty level (Fig 9). Wereviewed a separate series of patients pre-senting with multiple osteoporotic frac-tures prior to vertebroplasty and foundthat 68% of fractures were at contiguouslevels (Fig 8) (29). These latter data sug-gest a strong trend toward “clustering” offractures as part of the natural history ofosteoporosis. As such, a finding that 50%of new postvertebroplasty fractures occurat adjacent levels may simply representthe normal distribution of new-onsetfractures. We conclude that, at this time,there remains no compelling evidence tosuggest that vertebroplasty results inhigher risk of subsequent fracture as com-pared with the risk in untreated patientsand that proof of such a claim will re-quire large-scale, prospective studies.
Figure 7. Prone intraosseous venograms obtained during (a) anteroposterior and (b) lateralinjections of contrast material prior to vertebroplasty shows rapid filling of intraosseous venouscomplex followed by egress into paravertebral veins (PVV) and basivertebral plexus (BVP). Fillingof inferior vena cava (IVC) demonstrates how cement migration into the venous system mayresult in pulmonary embolization.
Volume 229 � Number 1 Percutaneous Vertebroplasty � 33
Ra
dio
logy
Long-term Follow-up of Cement
PMMA represents a permanent medicalimplant. Although there is a long historyof surgical implantation of PMMA, scantliterature exists regarding the long-term be-havior of cement as used in vertebroplasty.We consider it of paramount importanceto understand the long-term sequelae ofcement deposition, in order to appropri-ately counsel patients and referring physi-cians prior to vertebroplasty. Grados et al(28) reported radiographic follow-up in 34vertebrae treated with vertebroplasty in 25patients at a mean follow-up of 48 months.They noted no progression of vertebral de-formity in any of the injected vertebrae.We performed a similar study in which weidentified 20 levels treated in 10 patientswho had undergone conventional radio-graphic follow-up at a mean of 1.3 years(30). Sixteen (80%) of 20 vertebral bodycompression fractures were stable with re-spect to the degree of kyphosis and com-pression. Two (10%) levels showed moder-ately increased central endplate collapsewithout a change in the degree of kypho-sis. Two (10%) levels showed progressivecollapse associated with increased kypho-sis. One of these levels represented the sin-
gle case in which there was apparent com-pression of the injected cement. Thecement morphology was unchanged in theremainder of the levels.
These data indicate that in the major-ity of patients treated with percutaneousvertebroplasty, there is stability of degreeof vertebral compression, kyphosis, andcement morphology. In a minority of pa-tients, there may be progressive kyphosisand compression at the treated level,which indicates the need for prospectivestudy with complete clinical and radio-graphic follow-up evaluation after verte-broplasty.
Prophylactic Vertebroplasty
The notable pain relief achieved withvertebroplasty raises the question ofwhether we should routinely performprophylactic vertebroplasty at nonfrac-tured levels in patients who present withpainful fractures. Prophylactic vertebro-plasty might be justified if one could ac-curately identify patients at extremelyhigh risk for new-onset fractures andcould predict which nonfractured levelswill undergo spontaneous fracture. Lind-
say et al (31) reported on a large series ofpatients who were followed up after anindex fracture; within 1 year after theinitial fracture, approximately 25% of pa-tients experienced a new fracture. Exactlocations of new fractures were not re-ported. We and others have noted thatapproximately 20%–25% of patients re-turn with new, painful fractures after be-ing treated with vertebroplasty (29). Asnoted earlier, approximately one-half ofthese new fractures are at sites not adja-cent to the previously treated vertebra.Thus, since only a minority of patientsreturn with new painful fractures, and,since it is impossible to predict whichlevels will undergo subsequent fracture,we do not consider prophylactic verte-broplasty to be justifiable. Furthermore,Medicare will not reimburse for prophy-lactic vertebroplasty at this time.
Outcomes Measures
The majority of studies on vertebro-plasty have relied on rudimentary out-comes measurements, typically includ-ing pain relief, change in mobility, andchange in medication requirements. For
Figure 8. Multilevel vertebroplasty in a 60-year-old woman with steroid-dependent chronic obstructive pulmonary disease,who presented with severe midthoracic back pain unresponsive to narcotic analgesia. (a) Sagittal T1-weighted (750/12) MRimage shows three adjacent thoracic compression fractures at T7, T8, and T9. (b) Lateral radiograph shows vertebroplasty ofthoracic vertebrae. Patient’s pain resolved after vertebroplasty of all three levels. She returned 1 month later with new lumbarpain, and a new L4 fracture was treated. (c) Patient returned 1 month later with new fractures of L1 and L2, identified onsagittal T1-weighted (750/12) MR image, which were injected. Ultimately, she went on to fracture three more vertebral bodies.
34 � Radiology � October 2003 Kallmes and Jensen
Ra
dio
logy
most patients, accurate recollection ofpain severity is difficult. Ideal outcomemeasures would be sensitive and specificfor subtle changes in health status. Mea-sures of global health status, such as theSF-36 Health Survey, are difficult to ad-minister in patients with severe backpain. There exist no vertebroplasty dataobtained with the SF-36, but authors of arecent article on kyphoplasty (32) re-ported use of the SF-36 and found signif-icant changes in physical functioningand pain domains.
Even without use of relatively cumber-some questionnaires such as the SF-36,the vertebroplasty literature could be en-hanced by using validated disease-spe-cific outcomes instruments. Other spe-cialties use a variety of back pain–specificdisability instruments, including the Os-twestry Back Pain Index (33), the RolandScale (34), and the Osteoporosis Qualityof Life Questionnaire (35). We have re-cently gained experience with the RolandScale, which is a validated low back pain–related measurement tool that is easy toadminister in person and on the tele-phone (34). We noted, in a series of 16consecutive patients, not only that the
questionnaire was readily accepted by bothpatients and interviewers, but also that sig-nificant short-term improvements in func-tion were achieved after vertebroplasty(unpublished data, 2002). Future investiga-tors should examine whether any of theseinstruments can be administered reliablyin patients treated with vertebroplasty.
Sham Trial
Several respected authorities have notedthe lack of controlled prospective trials forvertebroplasty (36). In our local environ-ment, one third-party payer has recentlyconcluded that insufficient evidence isavailable to support vertebroplasty, andpayment has been denied. The apparentclinical benefits of vertebroplasty may re-flect either the natural history of painfulcompression fractures, where spontaneousresolution is common, or the placebo ef-fect. We and others (34) have proposed asham-controlled trial to demonstrate thatthe benefits of vertebroplasty are real. Re-cently, we have carried out a pilot study todemonstrate the feasibility of enrolling pa-tients into a sham-controlled trial of percu-
taneous vertebroplasty (unpublished data,2002).
Institutional review board approvalwas obtained for a prospective, random-ized, blinded trial to compare percutane-ous vertebroplasty and sham vertebro-plasty. Patients were randomly assignedto either the vertebroplasty or the shamcondition. The sham condition includedfluoroscopically guided placement of a25-gauge needle and infiltration of thepedicle with 10 mL of 0.25% bupivicaine(Abbott Laboratories, North Chicago, Ill),without placement of either the vertebro-plasty needle or cement. Methacrylatemonomer (Secour; Parallax Medical) wasopened in the angiography suite to sim-ulate cement preparation. To simulate ce-ment deposition, localized pressure wasplaced on the patient’s back and opera-tors gave verbal clues typical of thosegiven during cement injection. After 14days, patients who failed to respond tothe initial treatment (vertebroplasty orsham) were crossed over to the other pro-cedure but remained blinded to treat-ment type. Subjects were asked to guesswhich procedure they underwent ini-tially, to determine whether blinding wasattained.
Nine patients were screened. Five pa-tients agreed to enroll in the trial. Allpatients had documented fractures; abone scan was used in cases where theage of the fracture was unknown. Threepatients were initially randomly assignedto the sham procedure. One of these ex-perienced a new fracture 48 hours afterthe sham procedure and was excludedfrom the trial. Two patients in the shamgroup gained minimal pain relief fromthe sham procedure and thus crossedover to vertebroplasty. Pain relief aftervertebroplasty in these two patients wasminimal. Two other patients were ini-tially assigned to undergo vertebroplasty.Pain relief after vertebroplasty was mini-mal and both of these patients crossedover to the sham procedure. One of thesetwo patients gained complete pain relieffollowing the sham procedure. All fivepatients guessed that they had under-gone the sham condition as the initialtreatment.
We conclude that enrollment of pa-tients in a sham-controlled trial of percu-taneous vertebroplasty is feasible. Wehave some concern that selection bias,where patients with lesser degrees of painwould be more likely to enroll than pa-tients with severe pain, may dilute theapparent effect of vertebroplasty. Weconclude that patients are unable to ac-curately discern whether sham or true
Figure 9. Lateral radiographs in 35-year-old, obese, steroid-depen-dent woman with asthma who presented with severe lumbar pain.(a) Acute compression fractures of the superior endplate of L1 (upperarrows) and inferior endplate of L4 (lower arrows) are shown. Aftervertebroplasty, the patient returned to full activity, with relief of herpain; 2 weeks later, however, she was admitted for recurrent backpain. (b) Repeat radiograph shows new superior endplate fractures ofL2 and L3 (arrowheads).
Volume 229 � Number 1 Percutaneous Vertebroplasty � 35
Ra
dio
logy

vertebroplasty is being performed. Com-plete pain relief can be achieved with thesham procedure, even after failure of ver-tebroplasty. The placebo effect may playan important role in determining theoutcome of vertebroplasty.
CONCLUSION
Percutaneous vertebroplasty has beenembraced by the North American radiol-ogy community within the past decade.Although the basic principles behind ver-tebroplasty remain unchanged, the tech-nical aspects have been dramatically af-fected by operator experience, productdevelopment, and critical evaluation oflarge series of patients. Although ques-tions concerning the safety of vertebro-plasty have been answered, its efficacyand durability remain clouded owing tothe lack of randomized controlled trialsand uncertainty over the role of the pla-cebo effect. Radiologists have spear-headed the effort behind the validationof vertebroplasty. It remains incumbenton us to silence any doubts about the rolevertebroplasty should play in patient carethrough our continued thoughtful ques-tioning evaluation of this procedure.
References1. Galibert P, Deramond H, Rosat P, Le Gars
D. Preliminary note on the treatment ofvertebral angioma by percutaneousacrylic vertebroplasty. Neurochirurgie1987; 33:166–168. [French]
2. Jensen ME, Evans AJ, Mathis JM, KallmesDF, Cloft HJ, Dion JE. Percutaneous poly-methylmethacrylate vertebroplasty in thetreatment of osteoporotic vertebral bodycompression fractures: technical aspects.AJNR Am J Neuroradiol 1997; 18:1897–1904.
3. Cotten A, Boutry N, Cortet B, et al. Per-cutaneous vertebroplasty: state of the art.RadioGraphics 1998; 18:311–320.
4. Deramond H, Depriester C, Toussaint P,Galibert P. Percutaneous vertebroplasty.Semin Musculoskelet Radiol 1997; 1:285–296.
5. Barr JD, Mathis JM, Barr MS, et al. Stan-dard for the performance of percutaneousvertebroplasty. In: American College ofRadiology standards 2000–2001. Reston,Va: American College of Radiology, 2000;441–448.
6. Maynard AS, Jensen ME, Schweickert PA,Marx WF, Short JG, Kallmes DF. Value ofbone scan imaging in predicting pain re-lief from percutaneous vertebroplasty inosteoporotic vertebral fractures. AJNRAm J Neuroradiol 2000; 21:1807–1812.
7. Mathis JM, Barr JD, Belkoff SM, Barr MS,Jensen ME, Deramond H. Percutaneousvertebroplasty: a developing standard ofcare for vertebral compression fractures.AJNR Am J Neuroradiol 2001; 22:373–381.
8. Kallmes DF, Schweickert PA, Marx WF, etal. Vertebroplasty in the mid- and upperthoracic spine. AJNR Am J Neuroradiol2002; 23:1568–1576.
9. Cortet B, Cotten A, Boutry N, Flipo RM,Duquesnoy B, Chastanet P, Delcambre B.Percutaneous vertebroplasty in the treat-ment of osteoporotic vertebral compres-sion fractures: an open prospective study.J Rheumatol 1999; 26:2222–2228.
10. Jensen ME, Dion JE. Percutaneous verte-broplasty in the treatment of osteopo-rotic compression fractures. Neuroimag-ing Clin N Am 2000; 10:547–568.
11. Silverman SL. The clinical consequencesof vertebral compression fracture. Bone1992; 13(suppl 2):S27–S31.
12. Patel UF, Skingle SF, Campbell GAF, CrispAJF, Boyle IT. Clinical profile of acute ver-tebral compression fractures in osteopo-rosis. Br J Rheumatol 1991; 30:418–421.
13. Kaufmann TJ, Jensen ME, SchweickertPA, Marx WF, Kallmes DF. Age of fractureand clinical outcomes of percutaneousvertebroplasty. AJNR Am J Neuroradiol2001; 22:1860–1863.
14. Do HM, Kallmes DF, Marx WF, JensenME. Percutaneous vertebroplasty in thetreatment of patients with vertebral os-teonecrosis (Kummell’s disease). Neuro-surgical Focus/Journal of Neurosurgery1999; 7(1):article 2.
15. Gangi A, Kastler BA, Dietemann JL. Per-cutaneous vertebroplasty guided by acombination of CT and fluoroscopy.AJNR Am J Neuroradiol 1994; 15:83–86.
16. Barr JD, Barr MS, Lemley TJ. CombinedCT and fluoroscopic guidance for percu-taneous vertebroplasty. American Societyof Neuroradiology Annual Meeting 1996.
17. Shapiro SA. Cranioplasty, vertebral bodyreplacement, and spinal fusion with to-bramycin-impregnated methylmethacry-late. Neurosurgery 1991; 28:789–791.
18. Gaughen JR Jr, Jensen ME, SchweickertPA, Kaufmann TJ, Marx W, Kallmes DF.Relevance of antecedent venography inpercutaneous vertebroplasty for the treat-ment of osteoporotic compression frac-tures. AJNR Am J Neuroradiol 2002; 23:594–600.
19. Heatwole EV, McGraw JK, Patzik SB, et al.Predictive value of intraosseous venogra-phy prior to percutaneous vertebroplasty(abstr). J Vasc Interv Radiol 2001; 12:S11.
20. Kim AK, Jensen ME, Dion JE, Schweickert PA,Kaufmann TJ, Kallmes DF. Unilateral trans-pedicular percutaneous vertebroplasty: ini-tial experience. Radiology 2002; 222:737–741.
21. Belkoff SM, Mathis JM, Jasper LE, De-ramond H. The biomechanics of verte-broplasty: the effect of cement volume onmechanical behavior. Spine 2001; 26:1537–1541.
22. Murphy KJF, Deramond H. Percutaneousvertebroplasty in benign and malignantdisease. Neuroimaging Clin N Am 2000;10:535–545.
23. Convery FR, Gunn DR, Hughes JD, Mar-tin WE. The relative safety of polymeth-ylmethacrylate: a controlled clinicalstudy of randomly selected patientstreated with Charnley and ring total hipreplacements. J Bone Joint Surg Am 1975;1:57–64.
24. McLaughlin RE, DiFazio CA, Hakala MF,
et al. Blood clearance and acute pulmo-nary toxicity of methylmethacrylate indogs after simulated arthroplasty and in-travenous injection. J Bone Joint Surg Am1973; 55:1621–1628.
25. Phillips HF, Cole PV, Lettin AW. Cardio-vascular effects of implanted acrylic bonecement. BMJ 1971; 3:460–461.
26. Kaufmann TJ, Jensen ME, Ford G, Gill LL,Marx WF, Kallmes DF. Cardiovascular ef-fects of polymethylmethacrylate use inpercutaneous vertebroplasty. AJNR Am JNeuroradiol 2002; 23:601–604.
27. Kaufmann TJ, Jensen ME, Ford G, Gill LL,Marx WF, Kallmes DF. Cardiovascular ef-fects of polymethylmethacrylate use inpercutaneous vertebroplasty. AJNR Am JNeuroradiol 2002; 23:601–604.
28. Grados F, Depriester C, Cayrolle G, HardyN, Deramond H, Fardellone P. Long-termobservations of vertebral osteoporoticfractures treated by percutaneous verte-broplasty. Rheumatology (Oxford) 2000;39:1410–1414.
29. Jensen ME, Kallmes DF, Short JG, et al.Percutaneous vertebroplasty does not in-crease the risk of adjacent level fracture: aretrospective study (abstr). In: ASNR An-nual Meeting Program. Oak Brook, Ill:American Society of Neuroradiology,2000; 4.
30. Marx WF, Short JG, Kallmes DF, et al.Long term plain film follow-up of pa-tients treated with percutaneous verte-broplasty: evaluation for changes in de-gree of vertebral compression, vertebralkyphosis, and cement morphology. Pre-sented at the ASNR 39th Annual Meeting,Boston, Mass, April 23–27, 2001.
31. Lindsay R, Silverman SL, Cooper C, et al.Risk of new vertebral fracture in the yearfollowing a fracture. JAMA 2001; 285:320–323.
32. Lieberman IH, Dudeney S, Reinhardt MK,Bell G. Initial outcome and efficacy of“kyphoplasty” in the treatment of pain-ful osteoporotic vertebral compressionfractures. Spine 2001; 26:1631–1638.
33. Fairbank JCF, Couper JF, Davies JBF,O’Brien JP. The Oswestry low back paindisability questionnaire. Physiotherapy1980; 66:271–273.
34. Roland MF, Morris R. A study of the nat-ural history of back pain. I. Developmentof a reliable and sensitive measure of dis-ability in low-back pain. Spine 1983;8:141–144.
35. Cook DJ, Guyatt GH, Adachi JD, et al.Development and validation of the mini-osteoporosis quality of life questionnaire(OQLQ) in osteoporotic women withback pain due to vertebral fractures: Os-teoporosis Quality of Life Study Group.Osteoporos Int 1999; 10:207–213.
36. Jarvik JG, Deyo RA. Cementing the evi-dence: time for a randomized trial of ver-tebroplasty. AJNR Am J Neuroradiol 2000;21:1373–1374.
37. Gaughen JR Jr, Jensen ME, SchweickertPA, Kaufmann TJ, Marx WF, Kallmes DF.Lack of preoperative spinous process ten-derness does not affect clinical success ofpercutaneous vertebroplasty. J Vasc In-terv Radiol 2002; 13:1135–1138.
36 � Radiology � October 2003 Kallmes and Jensen
Ra
dio
logy