Embed Size (px)
Citation preview
utaneous in Evolvin
sluminal oronary ngioplas
ute Myocard’ial Infarction
XAVIER E. PRIDA, MD, J. PATRICK HOLLAND, MD, ROBERT L. FELDMAN, JAMES A. HILL, MD, ROBERT G. MacDONALD, MD, C. RICHARD CONTI,
and CARL J. PEPINE, MD
In 29 patients with evolving acute myocardial in- farction, acute reperfusion of the infarct-related cor- onary artery was attempted using percutaneous transluminal coronary angioplasty (PTCA) . Before
TCA, angiography showed 23 totally occluded and severely stenotic infarct-related coronary arteries.
PTCA was initially successful in 25 of 29 patients (88% ). Reocclusion occurred in 4 patients within 12 hours after successful PTCA and was associate with new electrocardiographic changes or recur- rence of symptoms. In 17 patients the infarct-relat- ed coronary artery remained patent at early follow-
up; late stenosis occurred in patients. Recurrence of stenosis was accompanied by development of angina. No clinical or an&graphic features distin- guished those with ultimate vessel patency, occlu- sion or recurrence of stenosis. On follow-up, ven- tricular function appeared better preserved or improved in those with a patent infarct-related coro- nary artery than in those with an occluded infarct- related Coronary artery. Further studies are warrant- ed to compare PTCA and streptokinase as primary reperfusion modalities in evolving acute myocardial infarction. (Am J Cardiol 1986;57:1069-1074)
T he focus of treatment and management of the pa- tient with evolving acute myocardial infarction (AMI) is being directed toward limiting the amount of myo- cardial necrosis. Jeopardized myocardium could be salvaged by methods intended to decrease myocardial oxygen demand or increase coronary blood flow. In numerous studies the feasibility and effects of throm- bolytic therapy or coronary artery bypass surgery in patients with evolving AM1 have been evaluated.1-4 Attention has recently been directed toward the appli- cability of percutaneous transluminal coronary angio- plasty (PTCA) in this situation.5-g PTCA appears par- ticularly attractive. After thrombolytic therapy, residual severe stenosis is frequent&present and may continue to serve as a nidus for thrombogenesis and reocclusion, or for continued symptoms without recur- rence of thrombosislo Additionally, residual severe ______-.----- ______---.------ From the Division of Cardiology, Department of Medicine, LJni- versity of Florida, and the Veterans Administration Medical Center, Gainesville, Florida. Manuscript received February 1, 1985; revised manuscript received October 21, 1985, accepted December 2,1985.
Address for reprints: Robert L. Feldman, MD, Department of Medicine, Division of Cardiology, 1. Hillis Miller Health Center, Box J-277, Gainesville, Florida 32610.
stenosis may limit the potential for salvage of jeopar- dized myocardium. l1 We evaluated PTCA in patients with evolving AMI, both as a means of primary reper- fusion of totally occluded infarct-related coronary ar- teries and as an adjunct to thrombolytic therapy to reduce residual coronary stenosis after thrombolytic therapy in infarct-related coronary arteries.
ethods Between June 1983 and July 1985, 39 consecutive
patients with suspected evolving AM1 were admitted to the University of Florida or the Veterans Admin- istration Medical Centers and were taken to the car- diac catheterization laboratory to establish reperfu- sion (Fig. 1). PTCA was attempted in 29 patients an was not attempted in 10. In 3 patients, coronary an- giographic findings were normal and t clinical course did not document AMI analysis showed noncardiac chest pain and early repo- larization changes on the electrocardiogram. The other 7 patients did not undergo PTCA because the infarct- related coronary artery was tortuous in 5 patients, because of multivessel coronary artery disease in 1 patient in whom emergency bypass surgery was per- formed, and because the infarct-related artery was only mildly narrowed (30%) after intracoronary strep-
1070 ANGIOPLASTY IN ACUTE MYOCARDIAL INFARCTION
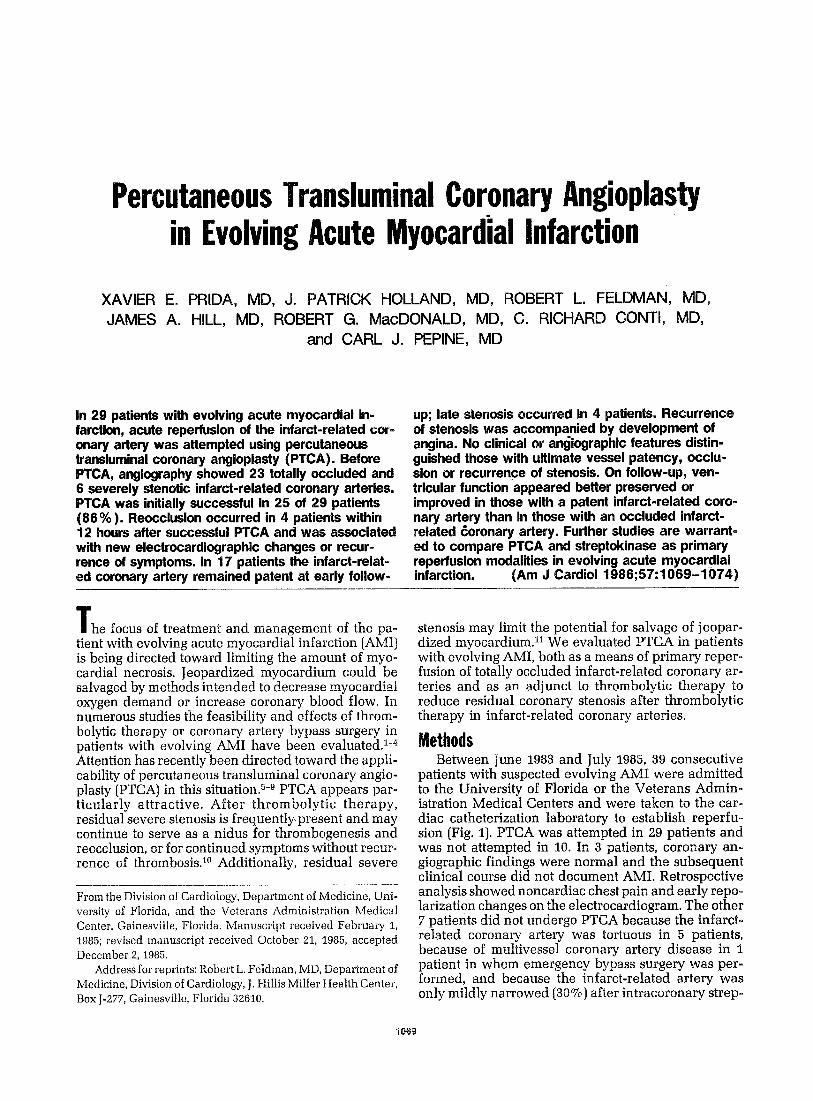
TABLE I Clinical and Angiographic Data in Patients with Evolving Infarction in Whom Angloplasty Was Attempted
SK Infarct-Related Coronary Angiographic Findings Units (X 10s) (% Diameter Reduction)
Age Wr) Infarct Pt & Sex Location IV IC Artery Initial After SKlPre PTCA After PTCA Restudy
1 50F Inferior 0 1.5 Right 100 2 58F Anterior 0 1.5 LAD 100 3 56M Inferior 15 0 Right 60 4 56M Anterior 15 1.0 LAD 100 5 48M Anterior 0 0.75’ LAD 100 6 39F Inferior 0 0.50” Right 100 7 57M Inferior 0 1.27’ Right 100 8 66M Inferior 7.5 0.45 LC 100 9 64M Anterior 0 1.5” LAD 100
10 36M Anterior 0 1.05’ LAD 100 11 32M Anterior 15 0 LAD 100 12 58M Anterior a.5 0.60’ LAD 90 13 72F Inferior 0 0 Right 100 14 58M Anterior 15 0 LAD 100 15 66M Anterior 0 1.5’ LAD 100 16 54M Anterior 0 0 LAD 95 17 55M Anterior 0 0.30’ LAD 100 18 40M Inferior 0 0 LC 100 19 62M Inferior 0 1.5” Right 100 20 54M Anterior 15 0 LAD 100 21 60M Anterior 5 0 LAD 100 22 60M Anterior 0 1.0” LAD 100 23 54F Inferior 0 0 Right 100 24 48M Inferior 0 1.2 Right (SVBG) 100 25 63M Anterior 0 0 LAD 95 26 39M Anterior 0 0 LAD 100 27 68M Inferior 15 0 Right 100 28 73M Anterior 0 1.85’ LAD 100 29 73M Anterior 0 0 LAD 90
90 100 60
100 . . .
. 100 . . . . 100
90
100
. .
. . .
. 100 100 . .
100
100 100 .
40 50 25 30 20 30 40
100 30 20 20 20 20 30
100 30 10 30
100 50 40 30 20 50 20 50
100 20 10
80 50 25 30 20
100 40
died 100
20 20
100 90 30
100 .
100 30 90 95 40 30 20
95. 50 .
l Streptokinase given after attempted PTCA. IC = intracoronary; IV = intravenous; LAD = left anterior descending coronary artery; LC = left circumflex artery; PTCA = percutaneous transluminal
coronary angioplasty; SK = streptokinase; SVBG = saphenous vein bypass graft.
tokinase administration in the other. All patients who underwent PTCA did have evolving AMI as shown by standard electrocardigraphic (ECG) and enzymatic criteria. Twenty-six patients came directly to the emer- gency room or from referral hospitals, and AM1 devel- oped in 3 patients who were in our hospitals for other reasons. The age range was 32 to 73 years (mean 56). Pertinent clinical characteristics and angiographic findings are described in Table I.
Symptoms began no earlier than 6 hours before admission to the hospital. Morphine sulfate was ad-
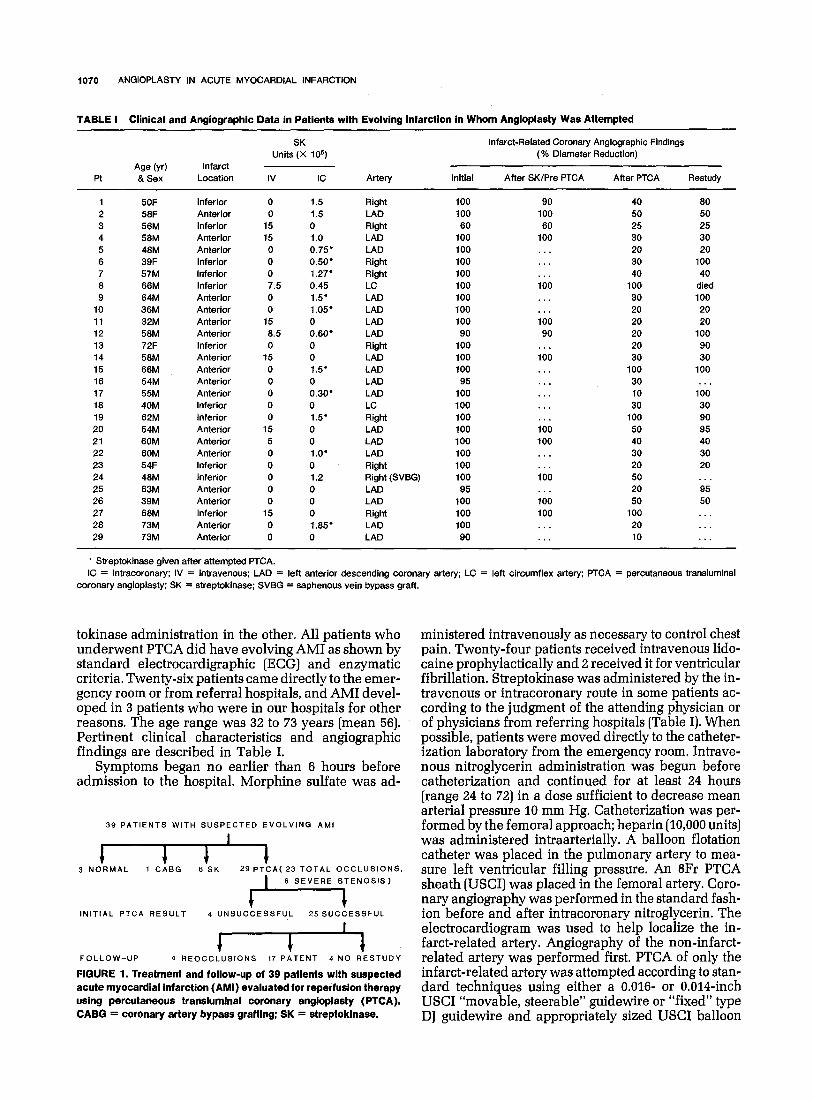
39 PATIENTS WITH SUSPECTED EVOLVING AMI
I
i 1 4 I 3 NORMAL 1 CABG 6 SK 29 PTCA( 23 TOTAL OCCLUSIONS.
I’
6 SEVERE STENOSIS)
1 INITIAL PTCA RESULT 4 UNSUCCESSFUL 25 SUCCESSFUL
I
I 4 FOLLOW-UP 4 AEOCCLUSIONS 17 PATENT 4 NO RESTUDY
FIGURE 1. Treatment and follow-up of 39 patlents wlth suspected acute myocardlal Infarction (AMI) evaluated for reperfuslon therapy using percutaneous translumlnal coronary angloplasty (PTCA). CABG = coronary artery bypass grafting; SK = streptoklnase.
ministered intravenously as necessary to control chest pain, Twenty-four patients received intravenous lido- Caine prophylactically and 2 received it for ventricular fibrillation. Streptokinase was administered by the in- travenous or intracoronary route in some patients ac- cording to the judgment of the attending physician or of physicians from referring hospitals (Table I). When possible, patients were moved directly to the catheter- ization laboratory from the emergency room. Intrave- nous nitroglycerin administration was begun before catheterization and continued for at least 24 hours [range 24 to 72) in a dose sufficient to decrease mean arterial pressure 10 mm Hg. Catheterization was per- formed by the femoral approach; heparin (10,000 units) was administered intraarterially. A balloon flotation catheter was placed in the pulmonary artery to mea- sure left ventricular filling pressure. An 8Fr PTCA sheath (USCI) was placed in the femoral artery. Coro- nary angiography was performed in the standard fash- ion before and after intracoronary nitroglycerin. The electrocardiogram was used to help localize the in- farct-related artery. Angiography of the non-infarct- related artery was performed first. PTCA of only the infarct-related artery was attempted according to stan- dard techniques using either a 0.016- or 0.014-inch USC1 “movable, steerable” guidewire or “fixed” type DJ guidewire and appropriately sized USC1 balloon
May 1, 1986 THE AMERICAN JOURNAL OF CARDIOLOGY Volume 67 1071
dilation catheters. Within 10 minutes after attempted PTCA, left ventriculography (right anterior oblique projection) was performed in 23 patients. The femoral arterial and venous sheaths were left in place. Hepa- rin was continued for a minimum of 1 day (range 1 to 6). Aspirin (325 or 650 mg) was administered orally before or within 2.5 hours of PTCA and was continued as a once-daily dose. Follow-up catheterization was performed in 23 patients at a mean of 3.2 weeks (range 1 day to 16 weeks). Acute and late ventriculography were available for comparison in 17 patients.
Coronary anatomy was evaluated from cineangi- ography performed in multiple views. Two angiog- raphers measured the percent coronary diameter ste- nosis from the view showing maximal reduction of diameter, and the average was determined. Presence or absence of collateral vessels before and after PTCA was noted. Analysis of left ventriculograms was per- formed by 2 independent observers who assessed the difference in global ejection fraction and regional area change between initial and follow-up study. End-dia- stolic and end-systolic frames of normally conducted beats (none following a premature ventricular con- traction) were traced using a digital planimeter. Cal- culations were performed by a PDP 11/02 computer interfaced with a Honeywell Electronics for Medi- cine recorder. Regional area change in 5 segments was generated to determine averages of the jeopar- dized and nonjeopardized regions. The observer de- fined the jeopardized regions as that portion of the ventriculogram perfused by the infarct-related artery.
Time to reperfusion was defined by angiographic visualization of the distal coronary artery in patients with total occlusion and a best estimate was assessed by symptoms and ECG findings (reperfusion ectopy and reduction of ST-segment elevation) in patients with severe stenosis.
TABLE II Follow-Up of Patients with Initial Successful Angioplasty Procedure
Infarct Artery at Follow-Up
Patent Occluded
No. of pts Location of infarcted vessel
LAD LC Right
Average percent stenosis of infarcted vessel Initial Before PTCA After PTCA
SK administration (no. of pts) Before PTCA After PTCA
Aspirin administration (no. of pts) Before PTCA After PTCA
Time to reperfusion (hr) Mean Range
17 4
11 3 1 0 5 1
97 98 97 98 31 23
8 2 4 2
12 3 5 1
5.9 9.3 2-11 4-22
LAD = left anterior descending coronary artery; LC = left circumflex artery; PTCA = percutaneous transluminal coronary angioplasty.
Results At the time of catheterization, 28 of 29 patients had
ongoing chest pain. Patient 16 had new-onset chest pain and experienced “sudden death” but was resus- citated just before study. All 29 patients had Q waves with acute ST elevation in the corresponding region of AM1 (18 anterior, 11 inferior]. The mean of elapsed time between onset of pain and arrival at our hospital was 2.4 hours (range 1.0 to 6.0). Reperfusion was at- tained at 6.5 hours (range 1.5 to 221 after the onset of symptoms. In patient 9, chest pain increased and di- minished both before and during hospitalization, and reperfusion occurred at 22 hours after onset of the first
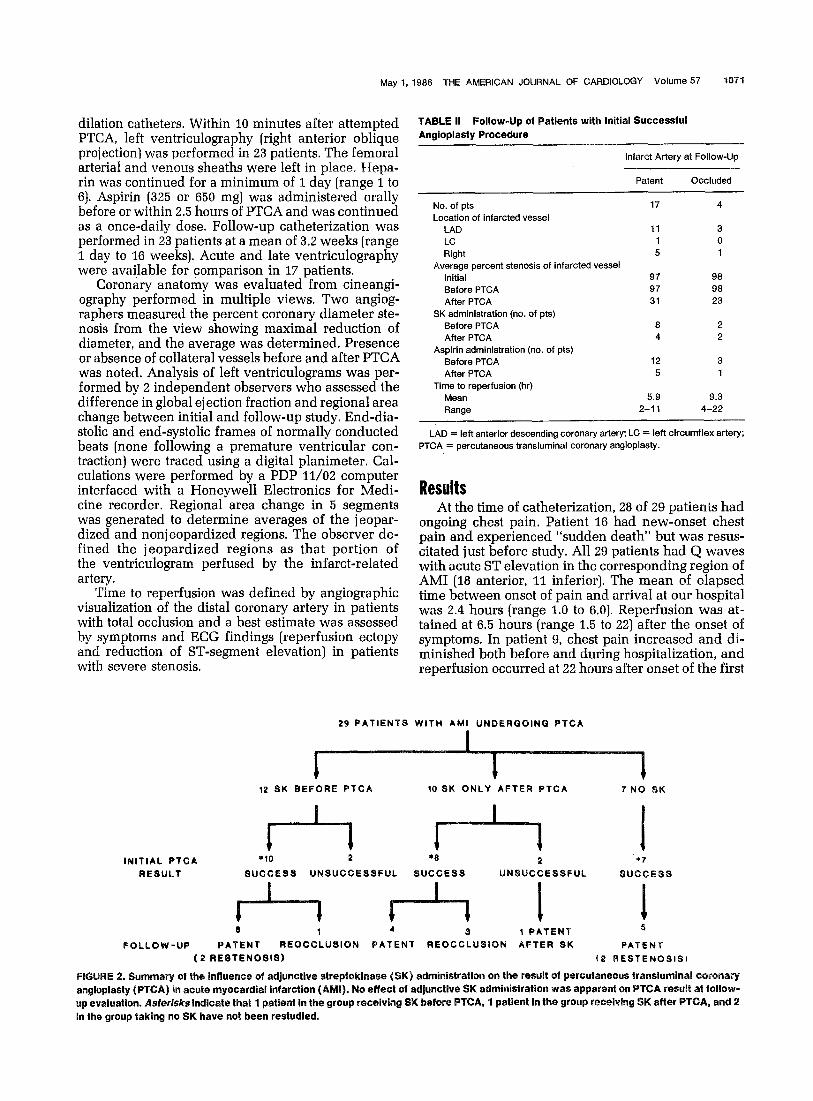
29 PATIENTS WITH AMI UNDERQOING PTCA
iz SK BEFORE PTCA 10 SK ONLY AFTER PTCA 7 NO SK
lNlTlAL PTCA *to 2 *e 2 +7
RESULT SUCCESS UNSUCCESSFUL SUCCESS UNSUCCESSFUL SUCCESS
8 1 4 3 1 PATENT s
FOLLCW-UP PATENT REOCCLUSION PATENT REOCCLUSION AFTER SK PATENT (2 RESTENOSIS) (2 BESTENOSISI
FI 2. summary of the influence of adjunctiwe streptoki~ase (SK) administration on the result of percutaneous tra~slumtnal coronary angioplasty (PTCA) in acute myocardial infarction (AM). No effect of ad/uncttve SK administration was apparent on PTCA result at follow- up evaluation. Asfer~s~sindicate that 1 patient In the group receiving SK before PTCA, 1 pattent in the group receiving SK after PTCA, and 2 in the group taking no SK have not been restudied.

1072 ANGIOPLASTY IN MYOCARDIAL INFARCTION
symptoms. With exclusion of data from this patient, mean time to reperfusion was 5.7 hours.
CAD affected 1 vessel in 13 patients, 2 vessels in 11 patients and 3 vessels in 5 patients. At least 1 hour after intravenous streptokinase (500,000 to 1.5 million U) was administered, 7 of 9 patients had totally occluded infarct-related arteries (Fig. 1 and 2). Before PTCA, intracoronary streptokinase was administered as pri- mary therapy in 5 patients; recanalization was success- ful only in patient 1.
The infarct-related artery was readily entered with the guidewire and balloon catheter in all but 4 patients (nos. 8,15,19 and 27). In 1 of the 4, the wire could not be guided into a totally occluded circumflex artery. This patient (no. 8) was in cardiogenic shock and had re- ceived streptokinase and intraaortic balloon pump support, but died. In the other 3 patients, the guidewire would not cross the totally occluded infarct-related artery. In patients 15 and 27, an uncomplicated AM1 evolved. In patient 19, intracoronary streptokinase opened the infarct-related artery after PTCA was un- successful. In the other 25 patients, PTCA was initially successful, resulting in reduction of the stenosis to 50% or less and prompt opacification of the distal vessel.
After PTCA, 11 patients received intracoronary streptokinase for reocclusion after initial opening, per-
FIGURE 3. Patient with patent Infarct-related coronary artery at follow-up. A, lnltlal coronary anglogram showing totally occluded left anterior descending artery with stalnlng of thrombus (arrow). B, guldewlre of angloplasty catheter system through previous totally occluded left anterior descending artery. C, coronary anglogram lmmedlalely after successful percutaneous transluminal anglo- plasty. D, coronary angiogram 10 days after percutaneous translu- mlnal coronary angloplasty.
sistent intraluminal filling defect at the site of PTCA, coronary emboli in the distal infarct-related artery, and unsuccessful PTCA. When intracoronary strepto- kinase was administered after PTCA, it did not estab- lish reperfusion or alter the angiographic appearance of the infarct-related artery, except in patient 19.
Of the 29 patients, 25 left the catheterization labora- tory with patent infarct-related arteries. Reocclusion subsequently occurred in 4. Two of the 4 [patients 9 and 12) had immediate reocclusion in the catheteriza- tion laboratory after initially successful PTCA. Repeat PTCA was initially successful in both. Initial angio- graphic appearances were indistinguishable between the 4 patients with reocclusion and those with patent infarct-related arteries at follow-up (Table II, Fig. 3 and 4). These 4 patients had recurrence of chest pain or ECG changes within 12 hours of PTCA despite antico- agulation with intravenous heparin and adjunctive therapy with aspirin and intravenous nitroglycerin. All who had reocclusion had received streptokinase.
Catheterization has not been repeated in patients 16, 24, 28 and 29. The other 17 patients who left the catheterization laboratory with patent infarct-related arteries were studied again at an average of 15 days (range 11 to 60) after AMI. Thirteen had a patent in- farct-related artery with residual stenosis similar (& 10%) to that in the acute stage; each was asymptomatic. Four had recurrence of stable angina and restenosis at or near the site of previous total or subtotal occlusion.
FIGURE 4. Patient with occluded Infarct-related coronary artery at follow-up. A, initial coronary anglogram showing totally occluded artery with stalning of thrombus. 6, angloplasty catheter system through prevlously totally occluded left anterlor descending artery. C, coronary anglogram immediately after successful percutaneous transluminal coronary angioplasly. D, coronary anglogram al fol- low-up 1 day after percutaneous translumlnal coronary angioplasty.
May 1, 1986 THE AMERICAN JOURNAL OF CARDIOLOGY Volume 57 1073
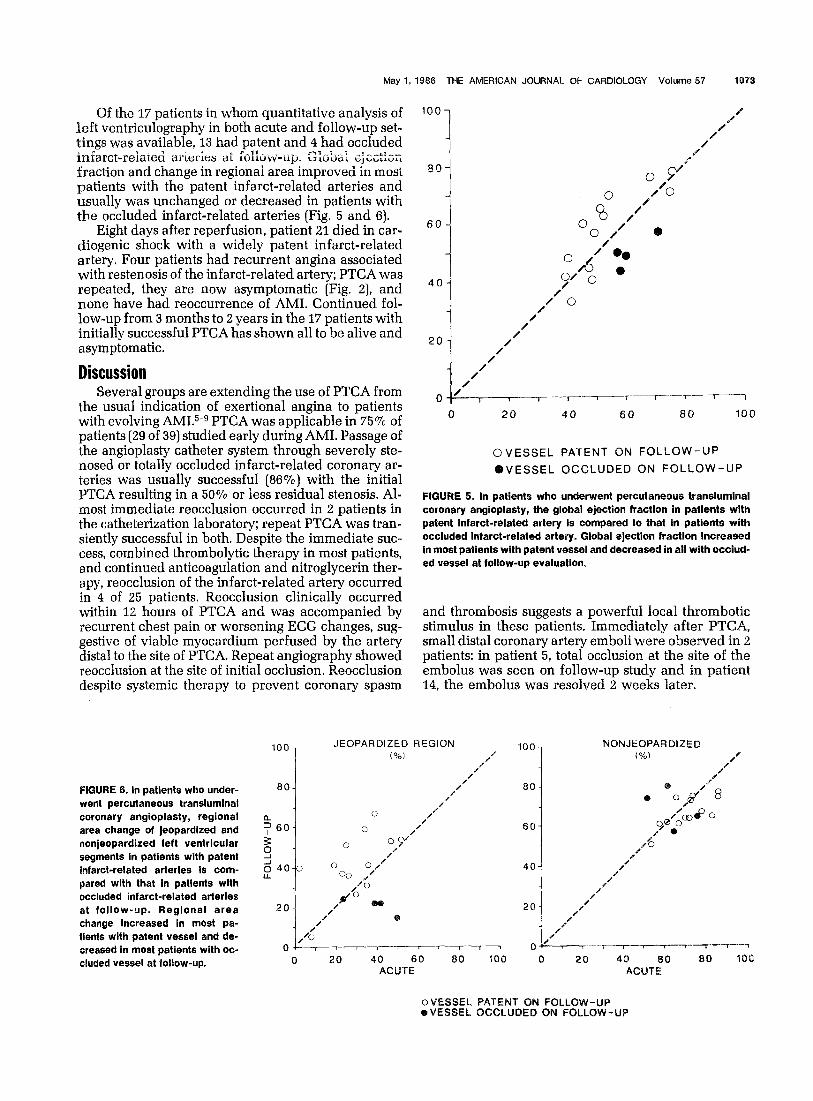
Of the 17 patients in whom quantitative analysis of left ventriculography in both acute and follow-up set- tings was available, 13 had patent and 4 had occluded
c 11 -. “._ inlarct-related arier~es ai I~I~UVV-up. Gk’dd ;jix:t;;;
fraction and change in regional area improved in rrwst
patients with the patent infarct-related arteries and usually was unchanged or decreased in patients with the occluded infarct-related arteries (Fig. 5 and 6).
Eight days after reperfusion, patient 21 died in car- diogenic shock with a widely patent infarct-related artery. Four patients had recurrent angina associated with restenosis of the infarct-related artery; PTCA was repeated, they are now asymptomatic (Fig. 2), and none have had reoccurrence of AMI. Continued fol- low-up from 3 months to 2 years in the 17 patients with initially successful PTCA has shown all to be alive and asymptomatic.
Discussion Several groups are extending the use of PTCA from
the usual indication of exertional angina to patients with evolving AMI.5-g PTCA was applicable in 75% of patients (29 of 39) studied early during AMI. Passage of the angioplasty catheter system through severely ste- nosed or totally occluded infarct-related coronary ar- teries was usually successful (86%) with the initial PTCA resulting in a 50% or less residual stenosis. Al- most immediate reocclusion occurred in 2 patients in the catheterization laboratory; repeat PTCA was tran- siently successful in both. Despite the immediate suc- cess, combined thrombolytic therapy in most patients, and continued anticoagulation and nitroglycerin ther- apy, reocclusion of the infarct-related artery occurred in 4 of 25 patients. Reocclusion clinically occurred within 12 hours of PTCA and was accompanied by recurrent chest pain or worsening ECG changes, sug- gestive of viable myocardium perfused by the artery distal to the site of PTCA. Repeat angiography showed reocclusion at the site of initial occlusion. Reocclusion despite systemic therapy to prevent coronary spasm
T-- 7--
0 20 40 60 80 100
OVESSEL PATENT ON FOLLOW-UP
~VE~SEL OCCLUDED ON FOLLOW-UP
FIGURE 5. In patients who underwent percutaneous translumlnal coronary angioplasty, the global ejection fraction in patlents with patent infarct-related artery is compared to that in patients with occluded infarct-related artery. Global ejection fraction increased in most patients with patent vessel and decreased in all with occlud- ed vessel at follow-up evaluation.
and thrombosis suggests a powerful local thrombotic stimulus in these patients. Immediately after PTCA, small distal coronary artery emboli were observed in 2 patients: in patient 5, total occlusion at the site of the embolus was seen on follow-up study and in patient 14. the embolus was resolved 2 weeks later.
NONJEOPARDIZED
FIGURE 8. In patients who under- went percutaneous transluminal coronary angioplasty, regional area change of jeopardized and nonjeopardized left ventricular segments in patients with patent infarct-related arteries is com- pared with that in patients wlth occluded infarct-related arteries at follow-up. Regional area change increased In most pa- tients with patent vessel and de- creased in most patients with oc- cluded vessel at follow-up.
80 -
60-
Cl 20 40 60 80 100 0 20 40 60 60 10 ACUTE ACUTE
oVESSEL PATENT ON FOLLOW-UP @VESSEL OCCLUQED ON FOLLOW-UP

1074 ANGIOPLASTY IN MYOCARDIAL INFARCTION
Thus, at follow-up the infarct-related artery was open in 81% (17 of 21) of these patients. Most patients have remained asymptomatic and the infarct-related arteries were widely patent. Angina developed in only 4 patients, all of whom had recurrent severe stenosis at the site of previous coronary occlusion. Repeat PTCA was successful and all have been asymptomatic for more than 6 months. Unfortunately, no clinical, labo- ratory or angiographic features in this small group pre- dicted reocclusion or restenosis after initially success- ful PTCA. The frequency of sudden reocclusion was much greater in these patients with AM1 than in the other patient groups undergoing PTCA. However, fre- quent sudden reocclusion also occurs with thromboly- tic therapy. The frequency of restenosis in patients who did not have sudden reocclusion was similar to the frequency of restenosis in other patient groups un- dergoing PTCA. The results suggest that PTCA is a feasible alternative approach for acute reperfusion of the patient with evolving AMI, even in those in whom streptokinase therapy failed.
References 1. Ganz W, Buchbinder N, Marcus H, Mondkar A, Maddahi 1, Charuzi Y, O’Connor L, Shell W, Fishbein MC, Kass R, Miyamoto A, Swan HJC. Intra- coronary thrombolysis in evolving myocardiol infarction. Am Heart J 1981;101:4-18.
2. Rentrou P. Blanke H. Karsch KR. Rutsch W. Schartl M. Merx W. Dorr R. Mathey D’, K&k K. Changes in left bentricular function after intracoronar; streptokinase infusion in clinically evolving myocardial infarction. Am Heart J 1~81;102:1188-1193.
_
3. Mathey DG, Kuck KH, Tilsner V, Krebber HJ, Bleifeld W. Nonsurgical coronary artery recanalization in acute transmural myocordial infarction. Circdotion 1981;63:489-497. 4. Markis JE, Malagold M, Parker JA, Silverman KJ. Barry WH, Als AV, Paulin S, Grossman W, Braunwald E. Myocardial salvage after intracoronary thrombolysis with streptokinase in acute myocardial infarction. Assessment by introcoronary thallium-291. N Engl J Med 1981;305:777-782. 5. Hartzler GO, Rutherford BD, McConahay DR, Johnson WL Jr, McCallister BD, Gura GM Jr, Conn RC, Crockett JE. Percutaneous transluminal coronary angioplasty with and without thrombolytic therapy for treatment of acute myocardial infarction. Am Heart J 1983;106:965-973. 6. Hartzler GO, Rutherford BD, McConahay DR. Percutaneous transluminal coronary angioplasty: application for acute myocardial infarction. Am J Car- dial 1984;53:117C-12fC. 7. Gold HK, Cowley MJ, Palacios IF, Vetrovec GW, Akins CW, Block PC, Leinbach RC. Combined intracoronary streptokinase infusion and coronary angioplasty during acute myocardial infarction. Am J Cardiol 1984;53:122C-
6. Meyer J, Mere W, Schmitz H, Erbel R, Kiesslich T, Dorr R, Lambertz H, Bethge C, Krebs W, Bardos P, Minale C, Messmer BJ, Effert S. Percutaneous transluminal coronary angioplasty immediately after intracoronary strepto- Jvsis of transmural mvocardial infarction. Circulation 1982X36:905-913. 6. Papapietro SE, M&Lean WA& Stanley AWH Jr, Hess RG, Corley N, Arciniegas JG, Cooper TB. Percutaneous transluminal coronary angioplasty after intracoronary streptokinase in evolving acute myocardiol infarction. Am J Cardiol 1985;55:48-53. 10. Terrosu P, Ibba GV, Contini GM, Franceschino V. Angiographic features of the coronary arteries during intracoronary thrombolysis. Br Heart J 1984;52:154-163. 11. Sheehan FH, Mathey DG, Schafer J. Dodge HT, Bolson EL. Factors that determine recovery of left ventricular function after thromboiysis in patients with acute myocardial infarction. CircuIation 1985;71:1121-1128.





























