Embed Size (px)
DESCRIPTION
Pelvic Floor Ultrasound - A Review
Citation preview

GENERAL GYNECOLOGY
Pelvic floor ultrasound: a reviewHans Peter Dietz, MD, PhD
I t has taken more than 2 decades forimaging to develop as a mainstream
diagnostic tool in the investigation of fe-male pelvic organ prolapse, urinary andfecal incontinence, and defecation disor-ders. Physicians have been slow in real-izing that clinical assessment alone is apoor tool to assess pelvic floor functionand anatomy. Our examination skills arequite simply inadequate, focusing onsurface anatomy rather than true struc-tural abnormalities. Because the bestprocedure in the hands of a highly com-petent surgeon will be a failure if per-formed on the wrong patient, it is not atall surprising that recurrence after pelvicreconstructive surgery is common.1 Theproblem is not poor treatment–it is poordiagnostics. Sonography is an acceptedcomponent of any clinical assessment inboth obstetrics and in gynecology–sowhy should it be any different in urogy-necology and female urology?
Imaging techniques can provide im-mediate objective confirmation of find-ings obtained on examination. In someinstances this can lead to markedly en-hanced clinical assessment skills. To givejust one example: the missing link be-tween vaginal childbirth and prolapse(major levator trauma in the form ofavulsion of the anteromedial aspects ofthe puborectalis muscle off the pelvicsidewall2,3) is palpable, but palpation oflevator trauma requires considerableskill and teaching,4-6 preferably with im-aging confirmation. Certainly, diagnosis
by imaging is more reproducible thandiagnosis by palpation,6 and it is easier toteach. After all, vision is our primary sen-sory organ. And suspected levatortrauma or abnormal distensibility (bal-looning) of the hiatus is by no means theonly reason to perform pelvic floor im-aging (Table).
Equipment and examinationtechniqueThis review will be limited to translabial/transperineal ultrasound, and this is re-flected in the following comments onequipment and examination technique.However, many clinical questions can beanswered just as well by what some in-vestigators call “introital ultrasound,” atechnique that is generally understood toinvolve the use of front-firing vaginal en-doprobes placed in the introitus. Al-though such probes can provide higherresolutions, there are obvious downsidesto their use, especially when it comes toassessing the effect of maneuvers and im-aging of the levator ani, and this tech-nique will not be discussed further in thisreview.
Standard requirements for basic 2-di-mensional (2D) translabial pelvic floorultrasound include a B-mode capable 2Dultrasound system with cineloop func-
From the University of Sydney, NepeanClinical School, Penrith, Australia.
Received Dec. 22, 2008; revised Feb. 9, 2009;accepted Aug. 17, 2009.
Reprints: Hans Peter Dietz, MD, PhD,Obstetrics and Gynecology, University ofSydney, Nepean Clinical School, NepeanHospital, Penrith NSW 2750 [email protected].
0002-9378/$36.00© 2010 Published by Mosby, Inc.doi: 10.1016/j.ajog.2009.08.018
TABLEIndications for pelvicfloor ultrasound! Recurrent urinary tract infections! Urgency, frequency, nocturia, and/or
urge urinary incontinence! Stress urinary incontinence! Insensible urine loss! Bladder-related pain! Persistent dysuria! Symptoms of voiding dysfunction! Symptoms of prolapse, ie, sensation of
lump or dragging sensation! Symptoms of obstructed defecation, eg,
straining at stool, chronic constipation,vaginal or perineal digitation, andsensation of incomplete bowel emptying
! Fecal incontinence! Pelvic or vaginal pain after
antiincontinence or prolapse surgery! Vaginal discharge or bleeding after
antiincontinence or prolapse surgery...........................................................................................................Dietz. Pelvic floor ultrasound: a review. Am J ObstetGynecol 2010.
Imaging currently plays a limited role in the investigation of pelvic floor disorders. It isobvious that magnetic resonance imaging has limitations in urogynecology and femaleurology at present due to cost and access limitations and due to the fact that it is generallya static, not a dynamic, method. However, none of those limitations apply to sonography,a diagnostic method that is very much part of general practice in obstetrics and gynecol-ogy. Translabial or transperineal ultrasound is helpful in determining residual urine; de-trusor wall thickness; bladder neck mobility; urethral integrity; anterior, central, and pos-terior compartment prolapse; and levator anatomy and function. It is at least equivalent toother imaging methods in visualizing such diverse conditions as urethral diverticula, rectalintussusception, mesh dislodgment, and avulsion of the puborectalis muscle. Ultrasoundis the only imaging method able to visualize modern mesh slings and implants and maypredict who actually needs such implants. Delivery-related levator trauma is the mostimportant known etiologic factor for pelvic organ prolapse and not difficult to diagnose on3-/4-dimensional and even on 2-dimensional pelvic floor ultrasound. It is likely that this willbe an important driver behind the universal use of this technology. This review gives anoverview of the method and its main current uses in clinical assessment and research.
Key words: female pelvic organ prolapse, levator ani, pelvic floor, 3-dimensionalultrasound, translabial ultrasound
Reviews www.AJOG.org
APRIL 2010 American Journal of Obstetrics & Gynecology 321
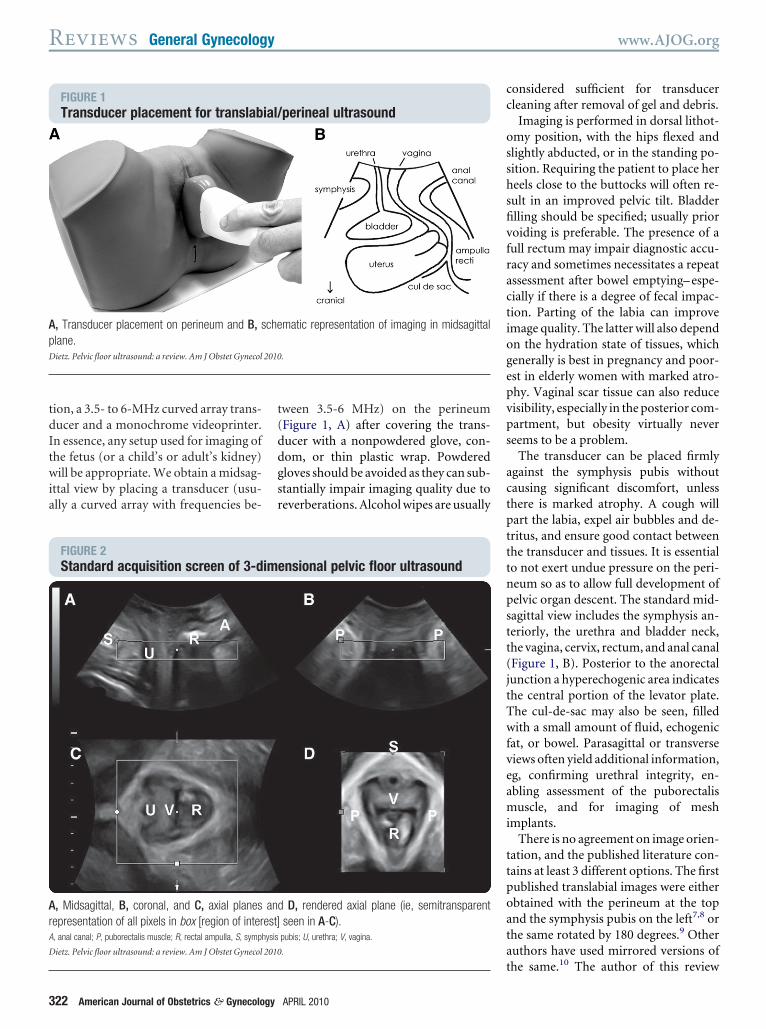
tion, a 3.5- to 6-MHz curved array trans-ducer and a monochrome videoprinter.In essence, any setup used for imaging ofthe fetus (or a child’s or adult’s kidney)will be appropriate. We obtain a midsag-ittal view by placing a transducer (usu-ally a curved array with frequencies be-
tween 3.5-6 MHz) on the perineum(Figure 1, A) after covering the trans-ducer with a nonpowdered glove, con-dom, or thin plastic wrap. Powderedgloves should be avoided as they can sub-stantially impair imaging quality due toreverberations. Alcohol wipes are usually
considered sufficient for transducercleaning after removal of gel and debris.
Imaging is performed in dorsal lithot-omy position, with the hips flexed andslightly abducted, or in the standing po-sition. Requiring the patient to place herheels close to the buttocks will often re-sult in an improved pelvic tilt. Bladderfilling should be specified; usually priorvoiding is preferable. The presence of afull rectum may impair diagnostic accu-racy and sometimes necessitates a repeatassessment after bowel emptying– espe-cially if there is a degree of fecal impac-tion. Parting of the labia can improveimage quality. The latter will also dependon the hydration state of tissues, whichgenerally is best in pregnancy and poor-est in elderly women with marked atro-phy. Vaginal scar tissue can also reducevisibility, especially in the posterior com-partment, but obesity virtually neverseems to be a problem.
The transducer can be placed firmlyagainst the symphysis pubis withoutcausing significant discomfort, unlessthere is marked atrophy. A cough willpart the labia, expel air bubbles and de-tritus, and ensure good contact betweenthe transducer and tissues. It is essentialto not exert undue pressure on the peri-neum so as to allow full development ofpelvic organ descent. The standard mid-sagittal view includes the symphysis an-teriorly, the urethra and bladder neck,the vagina, cervix, rectum, and anal canal(Figure 1, B). Posterior to the anorectaljunction a hyperechogenic area indicatesthe central portion of the levator plate.The cul-de-sac may also be seen, filledwith a small amount of fluid, echogenicfat, or bowel. Parasagittal or transverseviews often yield additional information,eg, confirming urethral integrity, en-abling assessment of the puborectalismuscle, and for imaging of meshimplants.
There is no agreement on image orien-tation, and the published literature con-tains at least 3 different options. The firstpublished translabial images were eitherobtained with the perineum at the topand the symphysis pubis on the left7,8 orthe same rotated by 180 degrees.9 Otherauthors have used mirrored versions ofthe same.10 The author of this review
FIGURE 1Transducer placement for translabial/perineal ultrasound
A, Transducer placement on perineum and B, schematic representation of imaging in midsagittalplane.Dietz. Pelvic floor ultrasound: a review. Am J Obstet Gynecol 2010.
FIGURE 2Standard acquisition screen of 3-dimensional pelvic floor ultrasound
A, Midsagittal, B, coronal, and C, axial planes and D, rendered axial plane (ie, semitransparentrepresentation of all pixels in box [region of interest] seen in A-C).A, anal canal; P, puborectalis muscle; R, rectal ampulla, S, symphysis pubis; U, urethra; V, vagina.
Dietz. Pelvic floor ultrasound: a review. Am J Obstet Gynecol 2010.
Reviews General Gynecology www.AJOG.org
322 American Journal of Obstetrics & Gynecology APRIL 2010

prefers the original orientation as onconventional transvaginal ultrasound(cranioventral aspects to the left, dorso-caudal to the right). This orientation isvery convenient when using 3-dimen-sional (3D)/4-dimensional (4D) systemsas shown in Figure 2, a representation ofa 3D volume of the pelvic floor. The topleft represents the midsagittal plane, withthe bottom left an axial-plane slice, andthe bottom right representing a renderedvolume showing the levator hiatus.
In the following paragraphs, I’ll de-scribe the main clinical applications oftranslabial ultrasound in urogynecologicimaging.
Anterior compartmentAs clinicians, we say “cystocele” when wereally mean “anterior vaginal wall de-scent.” Of course, anterior vaginal walldescent usually implies descent of thebladder, ie, a “cystocele,” but behind thisterm there may hide a number of differ-ent conditions. Ultrasound can be veryhelpful in determining whether it is re-ally the bladder that is descending and inascertaining the configuration of urethraand bladder neck. The original indica-tion for pelvic floor ultrasound, how-ever, is the assessment of bladder neckmobility and funneling of the internalurethral meatus, both of which are im-portant in women with urinary inconti-nence. Figure 3 shows the standard ori-entation used to describe bladder neckmobility.11 The position of the bladderneck is determined relative to the infero-posterior margin of the symphysis pubisor relative to a system of coordinatesbased on the central axis of the symphy-sis pubis.12 Measurements are taken atrest and on maximal Valsalva, and thedifference yields a numerical value forbladder neck descent. Comparativestudies have shown good correlationswith radiological methods.12-16 The re-producibility of measurements of blad-der neck mobility are high.17,18
On Valsalva, the proximal urethra willbe seen to rotate in a posteroinferior di-rection to a greater or lesser degree, dueto the fact that the urethra and anteriorvaginal wall are tethered to the symphy-sis pubis and the pelvic sidewall. Inci-dentally, this rotation markedly changes
the echogenicity of the longitudinalsmooth muscle of the urethra, which be-comes isoechoic and less easy to identify,as evident in Figure 3. Proximal urethralrotation can be measured by comparingthe angle of inclination between theproximal urethra and any other fixedaxis. Some investigators measure the ret-rovesical angle (or posterior urethrovesi-cal angle) between proximal urethra andtrigone, others determine the angle ! be-tween the central axis of the symphysispubis and a line from the inferior sym-physeal margin to the bladder neck.19
There is no definition of normal forbladder neck descent although cutoffsof 20, 25, and 30 mm have been pro-posed to define hypermobility. Bladderfilling, patient position, and catheter-ization all have been shown to influ-ence measurements20 and it can occa-sionally be quite difficult to obtain aneffective Valsalva maneuver, especiallyin nulliparous women who frequentlycoactivate the levator muscle.21 Per-haps not surprisingly, publications todate have presented widely differingreference measurements in nullipa-rous women.18,22-24 I have obtained
measurements of 1.2-40.2 mm (mean,17.3 mm) in a group of 106 stress-con-tinent nulligravid young women of18-23 years of age.17 It is likely thatmethodologic differences account forthe above discrepancies, with allknown confounders tending to reducedescent.
The etiology of increased bladderneck descent is likely to be multifacto-rial. The wide range of values obtainedin young nulliparous women suggests acongenital component. Vaginal child-birth is probably the most significantenvironmental factor,25,26 with a longsecond stage of labor and vaginal oper-ative delivery associated with increasedpostpartum descent. This associationbetween increased bladder descent andvaginal parity is also evident in olderwomen with symptoms of pelvic floordysfunction.27
In patients with stress incontinence, butalso in asymptomatic women,28 funnelingof the internal urethral meatus may be ob-served on Valsalva and sometimes even atrest. Funneling is often (but not necessar-ily) associated with leakage. Marked fun-neling has been shown to be associated
FIGURE 3Determination of bladder neck mobility
Pelvic floor ultrasound, midsagittal plane at rest (left) and maximal Valsalva (right). Arrow identi-fies inferior margin of symphysis pubis, ie, point of reference for measurement of bladder neckposition (*).Reproduced, with permission, from Dietz.11
Dietz. Pelvic floor ultrasound: a review. Am J Obstet Gynecol 2010.
www.AJOG.org General Gynecology Reviews
APRIL 2010 American Journal of Obstetrics & Gynecology 323

with poor urethral closure pressures.29,30
Other indirect signs of urine leakage on B-mode real-time imaging are weak gray-scale echoes (streaming) and the appear-ance of 2 linear (specular) echoes defining
the lumen of a fluid-filled urethra. ColorDoppler ultrasound can directly demon-strate urine leakage on Valsalva maneuveror coughing,31 if this is desired. Agreementbetween color Doppler and fluoroscopy
was high in a controlled group with in-dwelling catheters and identical bladdervolumes.32 Color Doppler imaging mayalso facilitate the documentation of leakpoint pressures.33
Clinical examination is limited tograding anterior compartment prolapse,which we call “cystocele.” In fact, imag-ing will identify a number of anatomicsituations that are difficult, if not impos-sible, to distinguish clinically. There areat least 2 types of cystoceles with very dif-ferent functional implications (Figure4), which were first described in thisJournal in the 1970s.34 A cystourethro-cele is associated with above-averageflow rates and urodynamic stress incon-tinence whereas a cystocele with intactretrovesical angle is generally associatedwith voiding dysfunction and a low like-lihood of stress incontinence.35
Occasionally, a cystocele will turn outto be due to a urethral diverticulum (Fig-ure 5, for a 3D representation of an un-usual anterior urethral diverticulum), aGartner duct cyst, or an anterior entero-cele.36,37 Urethral diverticula are oftenoverlooked for years in women with re-current bladder infections and symp-toms of frequency, urgency, and pain orburning on voiding, until imaging is un-dertaken.38-40 Urethral structure andspatial relationships are much better ap-
FIGURE 4Cysto-urethrocele and custocele with intact retrovesical angle
Two main types of cystocele as imaged on maximal Valsalva in midsagittal plane: cystourethrocele (green type II; B), associated with urinary stressincontinence and good voiding function, and isolated cystocele (green type III; D), associated with prolapse and voiding dysfunction rather than stressincontinence. A and B, Retrovesical angle on Valsalva is at about 180 degrees, and bladder neck is lowest point of bladder. C and D, Retrovesical angleon Valsalva, D, is intact at 90-120 degrees, and bladder base is lower than bladder neck.Dietz. Pelvic floor ultrasound: a review. Am J Obstet Gynecol 2010.
FIGURE 5Anterior urethral diverticulum on 3-dimensional pelvic floor ultrasound
A-C, Orthogonal planes clearly illustrate location and extent of diverticulum.Reproduced, with permission, from Dietz.11
Dietz. Pelvic floor ultrasound: a review. Am J Obstet Gynecol 2010.
Reviews General Gynecology www.AJOG.org
324 American Journal of Obstetrics & Gynecology APRIL 2010

preciated in the axial plane (Figure 5),which is particularly useful in the differ-ential diagnosis of Gartner cyst and ure-thral diverticulum.
Finally, translabial ultrasound maydetect foreign bodies or bladder tu-mors20,37 and can be used to determineresidual urine,41 using a formula origi-nally developed for transvaginal ultra-sound.42 Although detrusor wall thick-ness has probably been overrated as adiagnostic tool in the context of detru-sor overactivity,43,44 increased detru-sor wall thickness seems associatedwith symptoms of the overactive blad-der,45-48 and may be a predictor ofpostoperative de novo urge inconti-nence and/or detrusor overactivity af-ter anti-incontinence procedures. Asopposed to the situation in men, detru-sor wall thickness in women is not pre-dictive of voiding dysfunction.49
Central compartmentGenerally, uterine prolapse is obvious clin-ically, as is vault descent. Having said that,ultrasound can graphically show the effectof an anteriorized cervix in women with anenlarged, retroverted uterus, explainingsymptoms of voiding dysfunction andsupporting surgical intervention to im-prove voiding in someone with a retro-
verted fibroid uterus.50 On the other hand,mild descent of an acutely anteverteduterus can result in compression of theanorectum, explaining symptoms of ob-
structed defecation–a situation that is de-scribed as a “colpocele” on defecationproctography. The uterus can be difficultto identify due to its isoechoic nature, sim-
FIGURE 6Rectocele, perineal hypermobility, and rectal intussusception
Distinction among true rectocele, ie, defect of rectovaginal septum (left); perineal hypermobility, ie, descent of rectal ampulla without fascial defect(middle); and rectal intussusception (right). All 3 conditions can manifest as clinical rectocele and are impossible to distinguish on examination.Reproduced, with permission, from Dietz.36
Dietz. Pelvic floor ultrasound: a review. Am J Obstet Gynecol 2010.
FIGURE 7Rectocele on 3D translabial ultrasound
True rectocele (*) as imaged in A, midsagittal, B, coronal, and C, axial planes and in D, axial plane renderedvolume. Images A and B show rectocele to be typically located at anorectal junction and symmetrical, C and,even more clearly, D, illustrate that it occupies a very substantial part of levator hiatus.Dietz. Pelvic floor ultrasound: a review. Am J Obstet Gynecol 2010.
www.AJOG.org General Gynecology Reviews
APRIL 2010 American Journal of Obstetrics & Gynecology 325

ilar in echotexture to the vaginal wall, es-pecially in postmenopausal women withsmall, atrophic uteri. In premenopausalwomen the uterus is often quite obvious,especially if anteverted. Sometimes Nabo-thian follicles help identify the cervix.
Posterior compartmentPelvic floor ultrasound is particularlyuseful in the posterior compartment, al-though we have in no way realized its po-tential benefits for clinical practice. Wesee descent of the posterior vaginal walland diagnose a rectocele, usually quiteunaware that at least 5 different anatom-ically distinct conditions can cause thisappearance. A stage II rectocele could bedue to a true rectocele, ie, a defect ofthe rectovaginal septum (most com-mon, and associated with symptoms ofprolapse, incomplete bowel emptying,
and straining at stool);51 an abnor-mally distensible, intact rectovaginalseptum (common and associated onlywith prolapse symptoms); perineal hy-permobility, ie abnormal candad dis-placement of the levator plate; a com-bined recto-enterocele (common); andan isolated enterocele (uncommon);or just a deficient perineum giving theimpression of a bulge.52 Occasionally arectocele turns out to be a rectal intus-susception, an early stage of rectal pro-lapse, where the wall of the rectal am-pulla is inverted and enters the analcanal on Valsalva; see Figure 6 for acomparison of 3 of those conditions.Figure 7 shows a simple true rectocelein the 3 orthogonal planes and in a ren-dered volume. Images in the coronaland axial plane demonstrate that this
rectocele, as most others, is symmetri-cal, suggesting a high transverse defectof the rectovaginal septum.
It is not surprising that colorectal sur-geons have started using this techniquein the initial investigation of womenwith defecatory disorders, although theytend to use ultrasound gel as a contrastmedium.53-55 Several studies have re-cently shown that ultrasound is muchbetter tolerated than defecation proctog-raphy,56,57 and of course it is muchcheaper. If there is a rectocele or a rectalintussusception/prolapse on ultrasound,this condition is very likely to be found onx-ray imaging.57,58 Consequently, it islikely that ultrasound will replace radio-logic techniques in the initial investigationof women with defecatory symptoms.
Although it is not always clear whatkind of therapeutic consequences oneshould draw from imaging findings, onewould not expect a rectocele repair to al-leviate symptoms caused by rectal intus-susception. If there is a defect of the rec-tovaginal septum then the patient is anobvious candidate for a defect-specificrectocele repair as first popularized byCullen Richardson.59 If a clinical recto-cele is due to a hyperdistensible fascia orlevator hiatus (perineal hypermobility)then one should not be too surprised ifon surgical dissection one does not findany defect to close–which is what hasprevented the universal acceptance ofdefect-specific rectocele repair. Such pa-tients probably respond best to fascialplication or even a levatorplasty. Need-less to say, it makes no sense whatsoeverto remove rectal wall in someone whohas a herniation of that rectal wallthrough a defect in the rectovaginal sep-tum as with transanal methods such asthe stapled transanal rectal resectionprocedure.60
Assessment of the anal sphincter willnot be discussed in any detail here. Theanal sphincter is generally imaged by en-doanal ultrasound. This method isfirmly established as one of the corner-stones of a colorectal diagnostic workupfor anal incontinence and is beyond thescope of this review. Due to the limitedavailability of such probes in gynecology,obstetricians and gynecologists haveused high-frequency curved array or en-
FIGURE 8Suburethral slings as seen on translabial ultrasound
A and C, In midsagittal plane 2 slings, 1 a transretzius (A), the other transobturator sling (C), areessentially indistinguishable. Both are hyperechogenic and located dorsal to midurethra. B and D, Inaxial plane, distinction is quite obvious: B, a tension-free vaginal tape (TVT) is curving ventrally towardsymphysis pubis, whereas D, a Monarc tracks laterally toward insertion of puborectalis muscle andobturator foramen.Dietz. Pelvic floor ultrasound: a review. Am J Obstet Gynecol 2010.
Reviews General Gynecology www.AJOG.org
326 American Journal of Obstetrics & Gynecology APRIL 2010

dovaginal probes placed exoanally, ie,transperineally, in the coronal ratherthan the midsagittal plane.61-63 There areadvantages to this approach–not justfrom the point of view of the patient.Exoanal imaging reduces distortion ofthe anal canal and allows dynamic eval-uation of the anal sphincter and mucosaat rest and on sphincter contraction,which seems to enhance the definition ofmuscular defects. However, resolutionsare quite likely to be inferior64 to thoseobtained by endoanal ultrasound, andgood comparative studies are lacking atpresent.
ImplantsSince the late 1990s, synthetic subure-thral slings have become very popular.Ultrasound can confirm the presence ofsuch a sling, distinguish between trans-obturator and trans-Retzius implants,especially when examining the axialplane (Figure 8), and even allow an edu-cated guess regarding the type of im-plant.65 As these meshes are highly echo-genic, ultrasound is superior to magneticresonance (MR) in identifying im-plants66 and has helped elucidate theirmode of action.67 It is also very helpfulwhen assessing women with complica-tions of suburethral slings such as void-ing dysfunction and de novo symptomsof urgency, helping the surgeon to decidewhether to cut a sling. Sling division usu-ally results in a 5- to 10-mm gap betweenmesh arms (Figure 9).
There is a worldwide trend toward theuse of permanent vaginal wall meshes,especially for recurrent prolapse, andcomplications such as support failure,mesh erosion, and chronic pain are notthat uncommon. Polypropylene meshessuch as the Perigee (American MedicalSystems, Minnetonka, MI), Prolift(Ethicon Gynecare, Somerville, NJ), andApogee (American Medical Systems,Minnetonka, MI) are highly echogenic(Figure 10), and their visibility is lim-ited only by persistent prolapse anddistance from the transducer. Three-dimensional translabial ultrasound hasdemonstrated that the implanted meshoften is nowhere near as wide as it issupposed to be, and this finding hasbeen interpreted as evidence of mesh
FIGURE 9Patient after TVT division due to de novo urgency,urge incontinence, and chronic mild obstruction
A, Midsagittal plane. Arrow indicates most likely tape location, but tape is invisible in midsagittal plane.B and C, Coronal and axial views, with 2 free tape ends (arrows). Gap between 2 tape ends is alsoevident in D, axial plane rendered volume.A, anal canal; B, bladder; R, rectal ampulla; S, symphysis pubis; U, urethra.
Dietz. Pelvic floor ultrasound: a review. Am J Obstet Gynecol 2010.
FIGURE 10Anterior and posterior compartment mesh implants
A, Midsagittal view and B, axial plane rendered volume in patient after successful Perigee (P) andApogee (A) implantation. A, Midsagittal plane demonstrates absence of prolapse on Valsalva, despitesevere levator ballooning evident in B, axial plane in this patient with bilateral avulsion injury.B, bladder; R, rectal ampulla; S, symphysis pubis; U, urethra.
Dietz. Pelvic floor ultrasound: a review. Am J Obstet Gynecol 2010.
www.AJOG.org General Gynecology Reviews
APRIL 2010 American Journal of Obstetrics & Gynecology 327

shrinkage, contraction, or retraction.68
In the view of the author, the phenom-enon of mesh retraction remains un-proven to date. A more likely explana-tion is that the mesh did not remain flat
but folded up on itself, either duringthe implantation or immediately afterclosure. Surgical technique seems toplay a role here as fixation of mesh tounderlying tissues results in a flatter,more even appearance. The position, ex-tent, and mobility of vaginal wall mesh canbe determined, helping with the assess-ment of individual technique, and ultra-sound may uncover complications such asdislodgment of anchoring arms.69
Clearly, translabial 4D ultrasoundwill be useful in determining func-tional outcome and location of im-plants, and will help in optimizingboth implant design and surgical tech-nique. Finally, although this is notmuch more than an afterthought inthis age of minimally invasive slings,most of the injectables used in antiin-continence surgery are also highlyechogenic and can be visualized as ahyperechoic donut shape surroundingthe urethra.20 Sometimes the materialturns out in unexpected locations,such as underneath the bladder neck,protruding into the bladder itself, inthe space of Retzius, or even trackingtoward the obturator foramen.
The axial planeAccess to the axial plane, previouslythe domain of cross-sectional imaging,has markedly increased the usefullnessof ultrasound in the assessment of pel-vic floor disorders. Although side-fir-ing vaginal transducers can image theaxial plane on 2D, such instrumentswere never very common and have ma-jor disadvantages. In the mid-1990s,such systems were used in clinical re-search,70,71 but the most significant ab-normality visible in the axial plane,levator avulsion, was overlooked. Inconsequence, results of such studieswere published only 10 years later,72
well after the “rediscovery” of levatortrauma by translabial 3D imaging.
Clearly, the translabial use of abdom-inal 4D probes has major advantagesover endosonography, even if resolu-tions are potentially lower. A single vol-ume obtained at rest with an acquisitionangle of 70° or higher will include theentire levator hiatus with symphysis pu-bis, urethra, paravaginal tissues, the va-gina, anorectum, and puborectalis mus-cle, from the pelvic sidewall in the area ofthe arcus tendineus of the levator ani to
FIGURE 11Rendered volume (axial plane)of typical unilateral avulsion
Prior insertion of muscle (long arrow), now com-pletely devoid of any hyperechogenic tissue, andretracted puborectalis muscle (short arrow).P, puborectalis muscle; R, rectum; S, symphysis pubis; V, vagina.
Dietz. Pelvic floor ultrasound: a review. Am J ObstetGynecol 2010.
FIGURE 12Right-sided avulsion of the puborectalis muscle
Delivery-related levator trauma as seen on exploration of large vaginal tear after vaginal delivery (left), as imaged on translabial 4-dimensional ultrasound(middle), and on magnetic resonance (MR) (right).Reproduced, with permission, from Dietz.11
Dietz. Pelvic floor ultrasound: a review. Am J Obstet Gynecol 2010.
Reviews General Gynecology www.AJOG.org
328 American Journal of Obstetrics & Gynecology APRIL 2010

the posterior aspect of the anorectaljunction. A Valsalva maneuver, how-ever, may result in lateral or posteriorparts of the puborectalis being displacedoutside the field of vision, especially inwomen with significant prolapse. Forthis reason higher acquisition angles of80° or 85° are preferable in pelvic floorimaging. Further technical details onvolume data acquisition are available in arecent review article.73
Display modesFigure 2 demonstrates the 2 basic dis-play modes on 3D pelvic floor ultra-sound. The orthogonal display mode
shows cross-sectional planes throughthe volume in question, each plane atright angles to the 2 others. For pelvicfloor imaging, this means the midsag-ittal, the coronal, and the axial plane.Contrary to the situation on MR, im-aging planes on 3D ultrasound can bevaried in arbitrary fashion to enhancethe visibility of a given anatomicalstructure, either in real time during theexamination or offline at a later time.The levator ani, for example, usuallyrequires an axial plane that is slightlytilted in a dorsocaudal to ventrocaudaldirection, and the required tilt may
change substantially with maneuvers.This is what makes it so difficult to ob-tain predictable axial planes on dy-namic MR imaging (MRI), with a con-sequent reduction in accuracy.74
The 3 orthogonal images are comple-mented by a rendered image, ie, a semi-transparent representation of all voxelsin an arbitrarily definable region of in-terest. Figure 2 shows a standard ren-dered image of the levator hiatus, withthe rendering direction set from caudallyto cranially. The result is an image thatcorresponds to observing the patient’spelvic floor from below, that is, from the
FIGURE 13Quantification of trauma on multislice/tomographic ultrasound imaging
Typical right-sided levator defect (*) measuring about 2 cm in (dorsoventral) width and at least 1.75 cm in (craniocaudal) depth as it is apparent in all 8slices.Reproduced, with permission, from Dietz.36
Dietz. Pelvic floor ultrasound: a review. Am J Obstet Gynecol 2010.
www.AJOG.org General Gynecology Reviews
APRIL 2010 American Journal of Obstetrics & Gynecology 329
perspective of the examining clinician.In some instances, rendering greatly en-hances the visibility of a given structureand helps patients and caregivers under-stand anatomic relationships much bet-ter (see Figure 7 for an orthogonal andrendered representation of a rectocele).
4D imagingFour-dimensional, as opposed to 3D,imaging implies the real-time acquisi-tion of volume ultrasound data, that is, asuccession of volumes over time, not justa single volume. Typically, modern sys-tems acquire anywhere between 0.5-20volumes per second, depending on ac-quisition angle and quality settings. Forpelvic floor imaging, that is, with acqui-sition angles of 70-85°, 4 volumes persecond can usually be achieved withoutcompromising quality. The resultingcineloops of volume data are particularly
useful for the evaluation of functionalanatomy, that is, for observing morpho-logic changes during maneuvers such asa pelvic floor contraction or a Valsalva.Even on 2D single-plane imaging, a staticassessment at rest gives little informationcompared with the evaluation of maneu-vers to assess levator function and delin-eate levator or fascial trauma.
The ability to perform a real-time 3D(or 4D) assessment of pelvic floor struc-tures makes pelvic floor ultrasoundsuperior to MRI for this application.Prolapse assessment by MR requires ul-trafast acquisition,75 which is of limitedavailability and does not allow optimalresolutions. Alternatively, some systemsallow imaging of the sitting or erect pa-tient, but again accessibility will be lim-ited for the foreseeable future. The sheerphysical characteristics of MR equip-ment make it much harder for the oper-
ator to ensure efficient maneuvers as!50% of all women will not perform aproper pelvic floor contraction whenasked,76 and a Valsalva is often con-founded by concomitant levator activa-tion.21 Without real-time imaging, it isimpossible to control for these con-founders. Therefore, ultrasound has ma-jor potential advantages when it comesto describing prolapse, especially whenassociated with fascial or muscular de-fects, and in terms of defining functionalanatomy. In addition, the offline analysispackages marketed by manufacturers ofsuch equipment allow distance, area, andvolume measurements in any user-de-fined plane (oblique or orthogonal),which is much superior to what is cur-rently possible with DICOM (DigitalImaging and Communications in Medi-cine) viewer software on a standard set ofsingle-plane MRI.
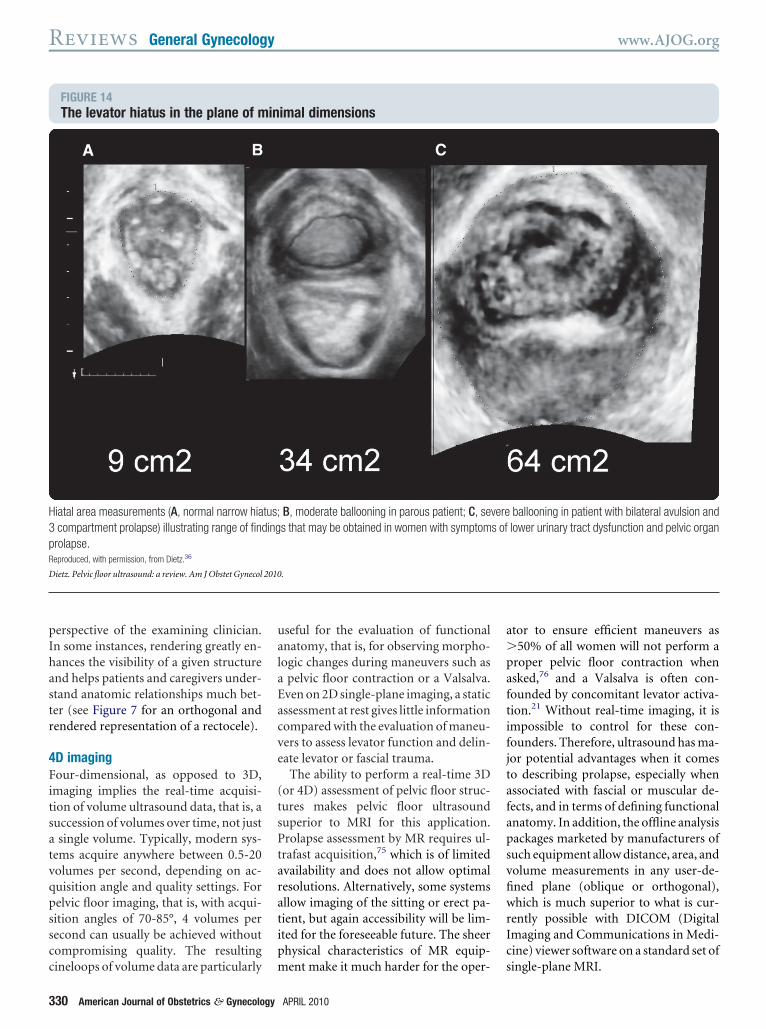
FIGURE 14The levator hiatus in the plane of minimal dimensions
Hiatal area measurements (A, normal narrow hiatus; B, moderate ballooning in parous patient; C, severe ballooning in patient with bilateral avulsion and3 compartment prolapse) illustrating range of findings that may be obtained in women with symptoms of lower urinary tract dysfunction and pelvic organprolapse.Reproduced, with permission, from Dietz.36
Dietz. Pelvic floor ultrasound: a review. Am J Obstet Gynecol 2010.
Reviews General Gynecology www.AJOG.org
330 American Journal of Obstetrics & Gynecology APRIL 2010

Clinical applicationsAxial-plane imaging is particularlysuited to the assessment of the levator animuscle, extending to paraurethral tissuesin patients with diverticula or strictures.Translabial ultrasound has vindicated60-year-old clinical data77 and con-firmed MRI studies78 showing that ma-jor morphologic abnormalities of levatorstructure and function are common invaginally parous women.79 AlthoughMR images showing morphologic ab-normalities of the levator ani were usu-ally considered to be the result of puden-dal nerve trauma, this interpretationbecame untenable on considering find-ings on rendered volumes. Clearly, ap-pearances (as in Figure 11) suggesttrauma rather than atrophy, with themuscle completely removed from thepelvic sidewall.
It can now be regarded as proven thatsuch morphologic abnormalities areusually due to traumatic avulsion of themuscle at the time of vaginal delivery(see Figure 12 for a comparison of MR,ultrasound, and clinical findings in pa-tients with unilateral levator avul-sion).2,80 Such trauma can be docu-mented on 2D ultrasound– either with aside-firing endocavitary probe72 or witha parasagittal probe orientation.81 How-ever, the most convenient and reproduc-ible approach is by using an abdominal3D/4D probe–the technology that isused to image the face of a fetus in utero.Just as in that situation, a rendered vol-ume, with the rendering direction setfrom distally to proximally, results invery graphic, impressive images, butfor the reproducible diagnosis of leva-tor trauma multislice or tomographicimaging (Figure 13) is preferred.82,83
Major delivery-related levator trauma,affecting the inferomedial aspects of thepuborectalis muscle, seems to be part ofthe missing link between vaginal child-birth and prolapse. Although there arebound to be other factors, including mi-crotrauma or altered biomechanics ofotherwise intact muscle, and fascialtrauma, levator avulsion enlarges the hi-atus84,85 and results in anterior and cen-tral compartment prolapse.79,86 Thelarger the defect, the higher is the likeli-
hood of prolapse,83 as quantified onmultislice or tomographic ultrasound(Figure 13). Levator defects seem to beassociated with cystocele recurrence af-ter anterior repair,87 hysterectomy andantiincontinence and prolapse surgery88
substantially increase the likelihood ofanterior and central compartment pro-lapse,86 and are associated with reducedcontractile strength.89,90 These defectsare palpable, but palpation requires sig-nificant teaching4,5 and is clearly less re-peatable (kappa " 0.41)91 than identifi-cation by ultrasound (kappa " 0.83 onanalysis of whole volumes and kappa" 0.61 for single slices in owndata).82,92 There seems to be a high prev-alence of levator defects in women withanal sphincter defects, which is not really
surprising given the overlap in risk fac-tors.93,94 Bilateral defects are more diffi-cult to detect because there is no normalside to compare with, but they have aparticularly severe impact on pelvic floorfunction85 and organ support.
Another factor only apparent on axial-plane imaging is the degree of hiatal dis-tension on Valsalva. Figure 14 gives animpression of the range of hiatal areameasurements in patients attending apelvic floor clinic. Measures of hiatal di-mensions seem highly repeatable95-99
and correlate well with findings onMRI.73 Hiatal enlargement to !25 cm2
on Valsalva is defined as “ballooning” onthe basis of receiver operator character-istic statistics and normative data inyoung nulliparous women.95,100 It can
FIGURE 15Surgical audit with translabial ultrasound
A and B, Patient with A, large cystocele who developed B, rectocele 6 months after successful Perigeeanterior compartment mesh (which is invisible due to shadowing from air-filled rectocele). C and D,Patient with large rectocele (C, imaged here before full development of rectocele to improve visual-ization) who developed D, cystocele 6 months after successful defect-specific rectocele repair.A, anal canal; B, bladder/cystocele; R, rectal ampulla/rectocele; S, symphysis pubis; U, urethra.
Dietz. Pelvic floor ultrasound: a review. Am J Obstet Gynecol 2010.
www.AJOG.org General Gynecology Reviews
APRIL 2010 American Journal of Obstetrics & Gynecology 331

be measured in axial-plane slices at theplane of minimal hiatal dimensions or inrendered volumes, and because the hia-tal plane is non-Euclidean (warpedrather than flat), measurements ob-tained in rendered volumes may be morevalid and more reproducible as well aseasier to obtain.101 The degree of disten-sion is strongly associated with prolapseand symptoms of prolapse,100 and bothavulsion and ballooning seem to be inde-pendent risk factors.102 It seems that bal-looning is associated with prolapse re-currence after rectocele repair,103 andthe same probably holds for other formsof prolapse surgery.
If delivery-related trauma and exces-sive distensibility of the levator are in-deed risk factors for female pelvic organprolapse and recurrence after recon-structive surgery, then these conditionsneed to be diagnosed preoperatively, andin future we will have to adjust our sur-gical approach accordingly. Some formsof prolapse are probably impossible tocure surgically unless one uses mesh im-plants. We should aim to develop surgi-cal methods that reduce the size and dis-tensibility of the hiatus or reconnect thedetached muscle in an attempt to pre-vent recurrence–and in 2009 this is nolonger a hypothetical goal.80,104 As al-ways, proper diagnosis has to come be-fore treatment, and ultrasound imagingis now an indispensable part of a com-plete preoperative workup.
Finally, but most important in clinicalpractice, another major advantage of thenew technology is the ease with whichpreoperative and postoperative data canbe compared using stored volume datasets and postprocessing software (seeFigure 15 for a comparison of preopera-tive and postoperative findings in 2 pa-tients with recurrent prolapse). Thiscapability is already enhancing postop-erative audit and our understanding ofhow certain procedures work (or do notwork). In future it very likely will influ-ence surgical development and teaching.
ConclusionEven before the widespread introductionof 3D/4D imaging, pelvic floor ultra-sound was a highly useful diagnostic toolfor physicians dealing with pelvic floor
disorders. As of 2009, this includes notjust gynecologists, urologists, urogyne-cologists, and radiologists, but also colo-rectal surgeons and gastroenterologists.Current trends, ie, the near universal in-troduction of 4D ultrasound, new soft-ware options, and increasing availabilityof training, will likely lead to more gen-eral acceptance of ultrasound as a stan-dard diagnostic option in pelvic floormedicine. The issue of levator trauma,one of the most significant develop-ments in clinical obstetrics since theintroduction of fetal monitoring, willtake pelvic floor ultrasound from aniche application into the mainstreamand speed the convergence of clinicalspecialties dealing with pelvic floor dis-orders. The crucial issue, as always, isteaching and the provision of up-to-date resources, and it may still be an-other decade or 2 before this methodtruly becomes a fully accepted part ofthe diagnostic workup in women withpelvic floor disorders.
For further information see my WorldWide Web site at http://www.medfac.usyd.edu.au/people/academics/profiles/pdietz.php and the Atlas of Pelvic FloorUltrasound.105 f
REFERENCES1. DeLancey J. The hidden epidemic of pelvicfloor dysfunction: achievable goals for improvedprevention and treatment. Am J Obstet Gynecol2005;192:1488-95.2. Dietz H, Lanzarone V. Levator trauma aftervaginal delivery. Obstet Gynecol 2005;106:707-12.3. Kearney R, Miller J, Ashton-Miller J, DelanceyJ. Obstetric factors associated with levator animuscle injury after vaginal birth. Obstet Gynecol2006;107:144-9.4. Dietz HP, Hyland G, Hay-Smith J. The as-sessment of levator trauma: a comparison be-tween palpation and 4D pelvic floor ultrasound.Neurourol Urodyn 2006;25:424-7.5. Kearney R, Miller JM, Delancey JO. Interraterreliability and physical examination of the pubo-visceral portion of the levator ani muscle, validitycomparisons using MR imaging. NeurourolUrodyn 2006;25:50-4.6. Dietz HP, Shek KL. Validity and reproducibil-ity of the digital detection of levator trauma. IntUrogynecol J Pelvic Floor Dysfunct 2008;19:1097-101.7. Kohorn EI, Scioscia AL, Jeanty P, HobbinsJC. Ultrasound cystourethrography by perinealscanning for the assessment of female stress
urinary incontinence. Obstet Gynecol 1986;68:269-72.8. Grischke EM, Dietz HP, Jeanty P, SchmidtW. A new study method: the perineal scan inobstetrics and gynecology [German]. Ultra-schall Med 1986;7:154-61.9. Koelbl H, Bernaschek G, Wolf G. A compar-ative study of perineal ultrasound scanning andurethrocystography in patients with genuinestress incontinence. Arch Gynecol Obstet1988;244:39-45.10. Gordon D, Pearce M, Norton P, Stanton SL.Comparison of ultrasound and lateral chain ure-throcystography in the determination of bladderneck descent. Am J Obstet Gynecol 1989;160:182-5.11. Dietz HP. Pelvic floor ultrasound. ASUM Ul-trasound Bulletin 2007;10:17-23.12. Schaer GN, Koechli OR, Schuessler B,Haller U. Perineal ultrasound for evaluating thebladder neck in urinary stress incontinence. Ob-stet Gynecol 1995;85:220-4.13. Ammann ME, Winkelbauer F, Fitzal P. Theurethrocystogram and perineal sonographycompared [German]. Rofo Fortschr Geb Ront-genstr Neuen Bildgeb Verfahr 1992;156:309-12.14. Dietz HP, Wilson PD. Anatomical assess-ment of the bladder outlet and proximal urethrausing ultrasound and videocystourethrography.Int Urogynecol J Pelvic Floor Dysfunct1998;9:365-9.15. Voigt R, Halaska M, Michels W, Martan A,Starker K, Voigt P. Examination of the ure-throvesical junction using perineal sonographycompared to urethrocystography using a beadchain. Int Urogynecol J 1994;5:212-4.16. Grischke EM, Anton HW, Dietz P, SchmidtW. Perineal sonography and roentgenologicprocedures within the scope of diagnosisof female urinary incontinence [German]. Ge-burtshilfe Frauenheilkd 1989;49:733-6.17. Dietz H, Eldridge A, Grace M, Clarke B. Pel-vic organ descent in young nulliparous women.Am J Obstet Gynecol 2004;191:95-9.18. Schaer GN, Koechli OR, Schuessler B,Haller U. Perineal ultrasound: determination ofreliable examination procedures. UltrasoundObstet Gynecol 1996;7:347-52.19. Martan A, Masata J, Halaska M, Voigt R.Ultrasound imaging of the lower urinary systemin women after Burch colposuspension. Ultra-sound Obstet Gynecol 2001;17:58-64.20. Dietz H. Ultrasound imaging of the pelvicfloor, part 1: 2D aspects. Ultrasound Obstet Gy-necol 2004;23:80-92.21. Oerno A, Dietz H. Levator co-activation is asignificant confounder of pelvic organ descenton Valsalva maneuver. Ultrasound Obstet Gy-necol 2007;30:346-50.22. Reed H, Waterfield A, Freeman RM, Adek-anmi OA. Bladder neck mobility in continentnulliparous women: normal references. IntUrogynecol J Pelvic Floor Dysfunct 2002;13(Suppl):S4.23. Brandt FT, Albuquerque CD, Lorenzato FR,Amaral FJ. Perineal assessment of urethrovesi-
Reviews General Gynecology www.AJOG.org
332 American Journal of Obstetrics & Gynecology APRIL 2010

cal junction mobility in young continent females.Int Urogynecol J Pelvic Floor Dysfunct2000;11:18-22.24. Peschers UM, Fanger G, Schaer GN, Vo-dusek DB, DeLancey JO, Schuessler B. Blad-der neck mobility in continent nulliparouswomen. BJOG 2001;108:320-4.25. Peschers U, Schaer G, Anthuber C, De-Lancey JO, Schuessler B. Changes in vesicalneck mobility following vaginal delivery. ObstetGynecol 1996;88:1001-6.26. Dietz HP, Bennett MJ. The effect of child-birth on pelvic organ mobility [comment]. Ob-stet Gynecol 2003;102:223-8.27. Dietz HP, Clarke B, Vancaillie TG. Vaginalchildbirth and bladder neck mobility. Aust N Z JObstet Gynaecol 2002;42:522-5.28. Schaer GN, Perucchini D, Munz E,Peschers U, Koechli OR, DeLancey JO. Sono-graphic evaluation of the bladder neck in conti-nent and stress-incontinent women. Obstet Gy-necol 1999;93:412-6.29. Dietz HP, Clarke B. The urethral pressureprofile and ultrasound imaging of the lower uri-nary tract. Int Urogynecol J Pelvic Floor Dys-funct 2001;12:38-41.30. Huang WC, Yang JM. Bladder neck funnel-ing on ultrasound cystourethrography in pri-mary stress urinary incontinence: a sign asso-ciated with urethral hypermobility and intrinsicsphincter deficiency. Urology 2003;61:936-41.31. Dietz HP, McKnoulty L, Clarke B. Transla-bial color Doppler for imaging in urogynecology:a preliminary report. Ultrasound Obstet Gynecol1999;14:144-7.32. Dietz HP, Clarke B. Translabial color Dopp-ler urodynamics. Int Urogynecol J Pelvic FloorDysfunct 2001;12:304-7.33. Masata J, Martan A, Halaska M, KasikovaE, Otcenasek M, Voigt R. Detection of Valsalvaleak point pressure with color Doppler–newmethod for routine use. Neurourol Urodyn2001;20:494-6.34. Green TH. Urinary stress incontinence: dif-ferential diagnosis, pathophysiology, and man-agement. Am J Obstet Gynecol 1975;122:378-400.35. Dietz HP, Haylen BT, Vancaillie TG. Femalepelvic organ prolapse and voiding function. IntUrogynecol J Pelvic Floor Dysfunct 2002;13:284-8.36. Dietz HP. Pelvic floor ultrasound. In: StokerJ, Taylor S, De Lancey JOL, eds. Imaging pelvicfloor disorders, 2nd ed. London, UK: SpringerVerlag; 2008:115-30.37. Tunn R, Petri E. Introital and transvaginalultrasound as the main tool in the assessment ofurogenital and pelvic floor dysfunction: an im-aging panel and practical approach. UltrasoundObstet Gynecol 2003;22:205-13.38. Mouritsen L, Bernstein I. Vaginal ultra-sonography: a diagnostic tool for urethral diver-ticulum. Acta Obstet Gynecol Scand 1996;75:188-90.39. Romanzi LJ, Groutz A, Blaivas JG. Urethraldiverticulum in women: diverse presentations re-
sulting in diagnostic delay and mismanagement.J Urol 2000;164:428-33.40. Siegel CL, Middleton WD, Teefey SA, Wain-stein MA, McDougall EM, Klutke CG. Sonogra-phy of the female urethra. AJR 1998;170:1269-74.41. Haylen BT. Verification of the accuracy andrange of transvaginal ultrasound in measuringbladder volumes in women. Br J Urol 1989;64:350-2.42. Haylen BT, Frazer MI, Sutherst JR, WestCR. Transvaginal ultrasound in the assessmentof bladder volumes in women: preliminary re-port. Br J Urol 1989;63:149-51.43. Yang JM, Huang WC. Bladder wall thick-ness on ultrasonographic cystourethrography:affecting factors and their implications. J Ultra-sound Med 2003;22:777-82.44. Lekskulchai O, Dietz H. Detrusor wall thick-ness as a test for detrusor overactivity inwomen. Ultrasound Obstet Gynecol 2008;32:535-9.45. Khullar V, Cardozo LD, Salvatore S, Hill S.Ultrasound: a noninvasive screening test for de-trusor instability. Br J Obstet Gynaecol 1996;103:904-8.46. Khullar V, Salvatore M, Cardozo L, BourneT, Abbott D, Kelleher C. A novel technique formeasuring bladder wall thickness in women us-ing transvaginal ultrasound. Ultrasound ObstetGynecol 1994;4:220-3.47. Robinson D, Anders K, Cardozo L, Bid-mead J, Toozs-Hobson P, Khullar V. Can ultra-sound replace ambulatory urodynamics wheninvestigating women with irritative urinary symp-toms? BJOG 2002;109:145-8.48. Robinson D, Khullar V, Cardozo L. Canbladder wall thickness predict postoperativedetrusor overactivity? Int Urogynecol J PelvicFloor Dysfunct 2005;16:S106.49. Lekskulchai O, Dietz HP. Is detrusor hyper-trophy in women associated with symptomsand signs of voiding dysfunction? ICS AnnualScientific Meeting 2006.50. Haylen BT. Voiding difficulty in women [re-view]. Int Urogynecol J Pelvic Floor Dysfunct2000;11:1-3.51. Dietz HP, Korda A. Which bowel symptomsare most strongly associated with a true recto-cele? Aust N Z J Obstet Gynaecol 2005;45:505-8.52. Dietz HP, Steensma AB. Posterior com-partment prolapse on two-dimensional andthree-dimensional pelvic floor ultrasound: thedistinction between true rectocele, perineal hy-permobility and enterocele. Ultrasound ObstetGynecol 2005;26:73-7.53. Beer-Gabel M, Teshler M, Barzilai N, et al.Dynamic transperineal ultrasound in the diag-nosis of pelvic floor disorders: pilot study. DisColon Rectum 2002;45:239-45.54. Beer-Gabel M, Teshler M, Schechtman E,Zbar AP. Dynamic transperineal ultrasound vsdefecography in patients with evacuatory diffi-culty: a pilot study. Int J Colorectal Dis2004;19:60-7.
55. Brusciano L, Limongelli P, Pescatori M, etal. Ultrasonographic patterns in patients withobstructed defecation. Int J Colorectal Dis2007;22:969-77.56. Perniola G, Shek K, Chong C, Chew S,Cartmill J, Dietz H. Defecation proctographyand translabial ultrasound in the investigation ofdefecatory disorders. Ultrasound Obstet Gy-necol 2008;31:567-71.57. Steensma AB, Oom DMJ, Burger CW,Schouten WR. Comparison of defecographyand 3D/4D translabial ultrasound in patientswith pelvic organ prolapse and/or evacuationdisorders. Ultrasound Obstet Gynecol 2007;30:447.58. Konstantinovic ML, Steensma AB, DomaliE, et al. Correlation between 3D/4D translabialultrasound and colpocystodefecography in di-agnosis of posterior compartment prolapse. Ul-trasound Obstet Gynecol 2007;30:448.59. Richardson AC. The rectovaginal septumrevisited: its relationship to rectocele and its im-portance in rectocele repair. Clinical Ob Gyn1993;36:976-83.60. Boccasanta P, Venturi M, Salamina G, Ce-sana B, Bernasconi F, Roviaro G. New trends inthe surgical treatment of outlet obstruction: clin-ical and functional results of two novel transanalstapled techniques from a randomized con-trolled trial. Int J Colorectal Dis 2005;19:359-69.61. Peschers UM, DeLancey JO, Schaer GN,Schuessler B. Exoanal ultrasound of the analsphincter: normal anatomy and sphincter de-fects. Br J Obstet Gynaecol 1997;104:999-1003.62. Kleinubing H Jr, Jannini JF, Malafaia O,Brenner S, Pinho TM. Transperineal ultrasonog-raphy: new method to image the anorectal re-gion. Dis Colon Rectum 2000;43:1572-4.63. Yagel S, Valsky DV. Three-dimensionaltransperineal sonography for evaluation of theanal sphincter complex: another dimension inunderstanding peripartum sphincter trauma.Ultrasound Obstet Gynecol 2006;27:119-23.64. Cornelia L, Stephan B, Michel B, Antoine W,Felix K. Trans-perineal versus endo-anal ultra-sound in the detection of anal sphincter tears.Eur J Obstet Gynecol Reprod Biol 2002;103:79-82.65. Dietz HP, Barry C, Lim YN, Rane A. Two-dimensional and three-dimensional ultrasoundimaging of suburethral slings. Ultrasound Ob-stet Gynecol 2005;26:175-9.66. Schuettoff S, Beyersdorff D, Gauruder-Bur-mester A, Tunn R. Visibility of the polypropylenetape after TVT (tension-free vaginal tape) proce-dure in women with stress urinary inconti-nence–a comparison of introital ultrasound andMRI in vitro and in patients. Ultrasound ObstetGynecol 2006;27:687-92.67. Dietz HP, Wilson PD. The ‘iris effect’: howtwo-dimensional and three-dimensional ultra-sound can help us understand anti-inconti-nence procedures. Ultrasound Obstet Gynecol2004;23:267-71.
www.AJOG.org General Gynecology Reviews
APRIL 2010 American Journal of Obstetrics & Gynecology 333

68. Tunn R, Picot A, Marschke J, Gauruder-Burmester A. Sonomorphological evaluation ofpolypropylene mesh implants after vaginalmesh repair in women with cystocele or recto-cele. Ultrasound Obstet Gynecol 2007;29:449-52.69. Shek C, Rane A, Goh JTW, Dietz HP. Im-aging of the Perigee transobturator mesh andits effect on stress incontinence. UltrasoundObstet Gynecol 2007;30:446.70. Khullar V, Salvatore S, Cardozo LD. Three-dimensional ultrasound of the urethra and ure-thral pressure profiles. Int Urogynecol J1994;5:319.71. Toozs-Hobson P, Khullar V, Cardozo L.Three-dimensional ultrasound: a novel tech-nique for investigating the urethral sphincter inthe third trimester of pregnancy. UltrasoundObstet Gynecol 2001;17:421-4.72. Athanasiou S, Chaliha C, Toozs-Hobson P,Salvatore S, Khullar V, Cardozo L. Direct imag-ing of the pelvic floor muscles using two-dimen-sional ultrasound: a comparison of women withurogenital prolapse versus controls. Br J ObstetGynaecol 2007;114:882-8.73. Dietz H. Ultrasound imaging of the pelvicfloor: 3D aspects. Ultrasound Obstet Gynecol2004;23:615-25.74. Kruger J, Heap X, Murphy B, Dietz H. Pelvicfloor function in nulliparous women using 3-di-mensional ultrasound and magnetic resonanceimaging. Obstet Gynecol 2008;111:631-8.75. Yang A, Mostwin JL, Rosenshein NB, Zer-houni EA. Pelvic floor descent in women: dy-namic evaluation with fast MR imaging and cin-ematic display. Radiology 1991;179:25-33.76. Bo K, Larson S, Oseid S, Kvarstein B, Ha-gen R, Jorgensen J. Knowledge about and abil-ity to do correct pelvic floor muscle exercises inwomen with urinary stress incontinence. Neur-ourol Urodyn 1988;7:261-2.77. Gainey HL. Post-partum observation of pel-vic tissue damage. Am J Obstet Gynecol1943;46:457-66.78. DeLancey JO, Kearney R, Chou Q,Speights S, Binno S. The appearance of levatorani muscle abnormalities in magnetic reso-nance images after vaginal delivery. Obstet Gy-necol 2003;101:46-53.79. Dietz H, Steensma A. The prevalence ofmajor abnormalities of the levator ani in urogy-necological patients. Br J Obstet Gynaecol2006;113:225-30.
80. Dietz H, Gillespie A, Phadke P. Avulsion ofthe pubovisceral muscle associated with largevaginal tear after normal vaginal delivery at term.Aust N Z J Obstet Gynaecol 2007;47:341-4.81. Dietz H, Shek KL. Levator trauma can bediagnosed by 2D translabial ultrasound. Int Uro-gynecol J Pelvic Floor Dysfunct 2009;20:807-11.82. Dietz H. Quantification of major morpholog-ical abnormalities of the levator ani. UltrasoundObstet Gynecol 2007;29:329-34.83. Dietz H. Tomographic ultrasound of the pel-vic floor: which levels matter most? UltrasoundObstet Gynecol 2009;33:698-703.84. Shek K, Dietz HP. The effect of childbirth onhiatal dimensions: a prospective observationalstudy. Obstet Gynecol In Press.85. Abdool Z, Shek K, Dietz HP. The effect oflevator avulsion on hiatal dimensions and func-tion. Am J Obstet Gynecol 2009;201:89.e1-5.86. Dietz H, Simpson J. Levator trauma is as-sociated with pelvic organ prolapse. Br J ObstetGynaecol 2008;115:979-84.87. Dietz HP, Chantarasorn V, Shek KL. Avul-sion of the puborectalis muscle is a risk factorfor recurrence after anterior repair. Int Urogy-necol J Pelvic Floor Dysfunct 2009;20(suppl 2):S172-3.88. Model A, Shek KL, Dietz HP. Do levator de-fects increase the risk of prolapse recurrenceafter pelvic floor surgery? Neurourol Urodyn2009;28(suppl 1):888-9.89. Dietz HP, Shek KL. Levator avulsion andgrading of pelvic floor muscle strength. Int Uro-gynecol J Pelvic Floor Dysfunct 2008;19:633-6.90. DeLancey J, Morgan D, Fenner D, et al.Comparison of levator ani muscle defects andfunction in women with and without pelvic or-gan prolapse. Obstet Gynecol 2007;109:295-302.91. Dietz H, Shek KL. Validity and reproducibil-ity of the digital detection of levator trauma. IntUrogynecol J Pelvic Floor Dysfunct 2008;19:1097-1101.92. Weinstein MM, Pretorius D, Nager CW, Mit-tal R. Inter-rater reliability of pelvic floor muscleimaging abnormalities with 3D ultrasound. Ul-trasound Obstet Gynecol 2007;30:538.93. Weinstein MM, Pretorius D, Jung SY, NagerCW, Mittal R. Anatomic defects in the puborec-talis muscle in women with fecal incontinence.Ultrasound Obstet Gynecol 2007;30:637.
94. Steensma AB, Schweitzer KJ, Burger CW,Schouten WR. Are anal sphincter injuries re-lated to levator abnormalities? Ultrasound Ob-stet Gynecol 2007;30:448.95. Dietz H, Shek K, Clarke B. Biometry of thepubovisceral muscle and levator hiatus bythree-dimensional pelvic floor ultrasound. Ultra-sound Obstet Gynecol 2005;25:580-5.96. Yang J, Yang S, Huang W. Biometry of thepubovisceral muscle and levator hiatus in nul-liparous Chinese women. Ultrasound ObstetGynecol 2006;26:710-6.97. Majida M, Hoff Braekken I, Bo K, Umek W,Dietz H, Ellstrom Engh M. 3D and 4D Ultra-sound of the pelvic floor: an interobserver reli-ability study. Int Urogynecol J Pelvic Floor Dys-funct 2006;17:S136-7.98. Guaderrama N, Liu J, Nager C, et al. Evi-dence for the innervation of pelvic floor musclesby the pudendal nerve. Obstet Gynecol2006;106:774-81.99. Kruger J, Dietz H, Murphy B. Pelvic floorfunction in elite nulliparous athletes and con-trols. Ultrasound Obstet Gynecol 2007;30:81-5.100. De Leon J, Steensma AB, Shek C, DietzHP. Ballooning: how to define abnormal disten-sibility of the levator hiatus. Ultrasound ObstetGynecol 2007;30:447.101. Wong V, Shek KL, Dietz HP. A simplifiedmethod for the determination of levator hiataldimensions. Int Urogynecol J Pelvic Floor Dys-funct 2009;20(suppl 2):S145-6.102. Franco AM, Shek KL, Kirby A, Fynes M,Dietz HP. Avulsion injury and levator hiatal bal-looning: two independent risk factors for pro-lapse? Int Urogynecol J Pelvic Floor Dysfunct2009;20(suppl 2):S145-6.103. Barry C, Dietz H, Lim Y, Rane A. A short-term independent audit of mesh repair for thetreatment of rectocele in women, using 3-di-mensional volume ultrasound: a pilot study.Aust N Z Continence J 2006;12:94-9.104. Shobeiri S, Cimpiri A, Allen AC, Hihira M,Quiroz LH. Surgical reconstruction of a unilater-ally avulsed symptomatic puborectalis muscleusing autologous fascia lata. Obstet Gynecol2009;114(suppl 2):480-2.105. Dietz HP, Steensma AB, Hoyte L, eds. At-las of pelvic floor ultrasound. London: SpringerVerlag; 2007.
Reviews General Gynecology www.AJOG.org
334 American Journal of Obstetrics & Gynecology APRIL 2010





























