Embed Size (px)
Citation preview

Pediatric TBI Rescuing the Injured Brain
Dr. Nina Hardcastle Society of Pediatric Anesthesia Meeting
October 23, 2015

Disclosures
Nothing to disclose!

Outline
Background – Pediatric TBI Guidelines
Mechanisms of injury and why they matter
TBI Interventions – physiology and targets
TBI Interventions – tiered strategies

Pediatric TBI Guidelines
! First guidelines published in 2003, then updated in 2012
! Significant changes in level of evidence between documents
! 2003 - mostly level 3 evidence
! 2012 - more level 2 evidence, with RCTs on many major issues

Primary and Secondary Injury
! Primary Injury - physical damage
! Secondary Injury - many contributors
! Cerebral ischemia
! Cerebral hypoxia
! Cerebral edema and elevated ICP
! Hypotension, hypercapnia, acidosis, hyperthermia
! = therapeutic targets in TBI management

First Tier Strategies

Second Tier Strategies

Elevated ICP… why does it matter?
Elevated ICP… why does it matter?
CPP = MAP – ICP
• CPP determines blood flow and oxygen delivery
• Elevated ICP compromises CPP

Minimal CPP
! Source: Guidelines for the acute medical management of severe TBI in infants, children, and adolescents. Pediatric Critical Care Medicine (2012). Volume 13, No. 1 (Supplement)

How can we lower ICP?

Physiology Review
! Adapted from Cottrell’s Neuroanesthesia, Coexisting Disease, 5th edition
2. Carbon dioxide and oxygen
Figure 2. Relationship between CBF and PaC02.
At normotension, the relationship between partial pressure of carbon dioxide in arterial
blood (PaCO2) and CBF is almost linear and at a PaCO2 80mmHg (10.6kPa) CBF is
approximately doubled. No further increase in flow is possible at this point as the
arterioles are maximally dilated. Conversely at 20mmHg (2.7kPa) flow is almost halved
and again cannot fall further as the arterioles are maximally vasoconstricted (Fig. 2).
These effects are regulated by a complex and interrelated system of mediators. The
initial stimulus is a decrease in brain extracellular pH bought about by the change in
PaCO2, further mediated by nitric oxide, prostanoids, cyclic nucleotides, potassium
channels, and a decrease in intracellular calcium concentration as a final common
mediator.
Arteriolar tone has an important influence on how PaCO2 affects CBF. Moderate
hypotension impairs the response of the cerebral circulation to changes in PaCO2, and
severe hypotension abolishes it altogether.
The response of the cerebral vessels to CO2 can be utilised to help manage patients with
raised intracranial pressure, for example after traumatic brain injury. Hyperventilation
reduces the PaCO2 and causes vasoconstriction of the cerebral vessels (reduces their
radius) and therefore reduces cerebral blood volume and ICP. However if PaCO2 is
reduced too much, the resulting vasoconstriction can reduce CBF to the point of causing
or worsening cerebral ischaemia. Clearly hypercapnia and the resulting vasodilatation
and increase in ICP must be avoided. PaCO2 is therefore best maintained at low-normal

Hyperventilation
! Source: Guidelines for the acute medical management of severe TBI in infants, children, and adolescents. Pediatric Critical Care Medicine (2012). Volume 13, No. 1 (Supplement)
Table 1. Changes in recommendations from the first edition to the second edition
Chapter First Edition Second Edition
Cerebral PerfusionPressure
Level II—A CPP !40 mm Hg in children with TBIshould be maintained
Level III—A CPP between 40 and 65 mm Hg probablyrepresents an age-related continuum for the optimaltreatment threshold; there may be exceptions to thisrange in some infants and neonates
Level III—Advanced cerebral physiological monitoringmay be useful to define the optimal CPP in individualinstances
Level III—Hypotension should be avoided
Level III—A minimum CPP of 40 mm Hg may beconsidered in children with TBI
Level III—A CPP threshold 40–50 mm Hg may beconsidered; there may be age-specific thresholdswith infants at the lower end and adolescents atthe upper end of this range
Hyperosmolar Therapy Level III—Hypertonic saline is effective for control ofincreased ICP after severe head injury; effective dosesas a continuous infusion of 3% saline range between0.1 and 1.0 mL/kg of body weight per hour,administered on a sliding scale; the minimum doseneeded to maintain ICP "20 mm Hg should be used
Level III—Mannitol is effective for control of increasedICP after severe TBI; effective bolus doses range from0.25 g/kg of body weight to 1 g/kg of body weight
Level III—Euvolemia should be maintained by fluidreplacement; a Foley catheter is recommended inthese patients to avoid bladder rupture
Level III—Serum osmolarity should be maintainedbelow 320 mOsm/L with mannitol use, whereas alevel of 360 mOsm/L appears to be tolerated withhypertonic saline, even when used in combinationwith mannitol
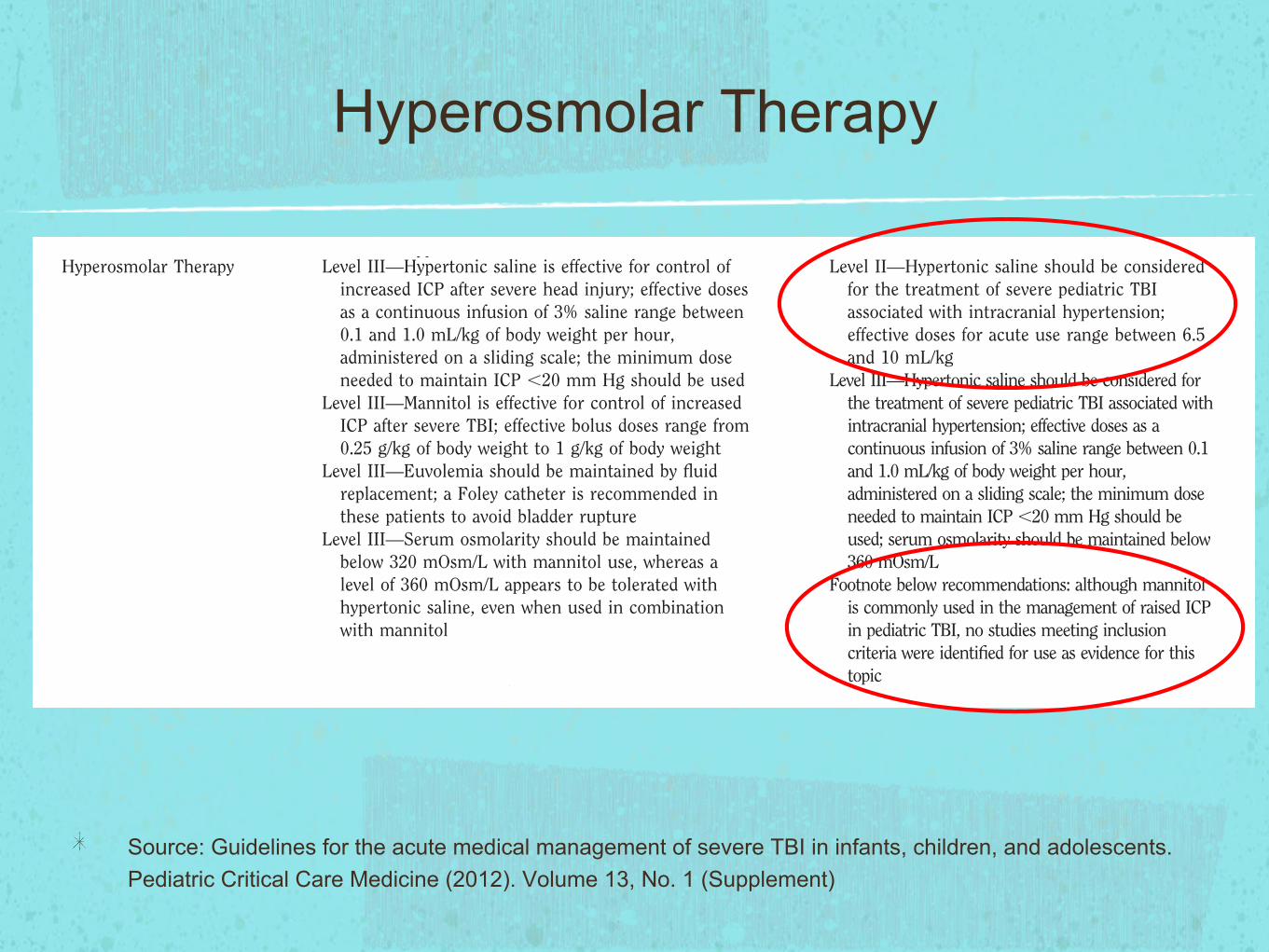
Level II—Hypertonic saline should be consideredfor the treatment of severe pediatric TBIassociated with intracranial hypertension;effective doses for acute use range between 6.5and 10 mL/kg
Level III—Hypertonic saline should be considered forthe treatment of severe pediatric TBI associated withintracranial hypertension; effective doses as acontinuous infusion of 3% saline range between 0.1and 1.0 mL/kg of body weight per hour,administered on a sliding scale; the minimum doseneeded to maintain ICP "20 mm Hg should beused; serum osmolarity should be maintained below360 mOsm/L
Footnote below recommendations: although mannitolis commonly used in the management of raised ICPin pediatric TBI, no studies meeting inclusioncriteria were identified for use as evidence for thistopic
Temperature Control Level III—Extrapolated from the adult data,hyperthermia should be avoided in children withsevere TBI
Level III—Despite the lack of clinical data in children,hypothermia may be considered in the setting ofrefractory intracranial hypertension
Level II—Moderate hypothermia (32–33°C)beginning early after severe TBI for only 24 hrsduration should be avoided
Level II—Moderate hypothermia (32–33°C)beginning within 8 hrs after severe TBI for upto 48 hrs’ duration should be considered toreduce intracranial hypertension
Level II—If hypothermia is induced for anyindication, rewarming at a rate of !0.5°C perhour should be avoided
Level III—Moderate hypothermia (32–33°C)beginning early after severe TBI for 48 hrsduration may be considered
Hyperventilation Level III—Mild or prophylactic hyperventilation (PaCO2
"35 mm Hg) in children should be avoidedLevel III—Mild hyperventilation (PaCO2 30–35 mm Hg)
may be considered for longer periods for intracranialhypertension refractory to sedation and analgesia,neuromuscular blockade, cerebrospinal fluiddrainage, and hyperosmolar therapy
Level III—Aggressive hyperventilation (PaCO2 "30 mmHg) may be considered as a second-tier option in thesetting of refractory hypertension; cerebral bloodflow, jugular venous oxygen saturation, or braintissue oxygen monitoring is suggested to helpidentify cerebral ischemia in this setting
Level III—Aggressive hyperventilation therapy titratedto clinical effect may be necessary for brief periods incases of cerebral herniation or acute neurologicdeterioration
Level III—Avoidance of prophylactic severehyperventilation to a PaCO2 "30 mm Hg may beconsidered in the initial 48 hrs after injury
Level III—If hyperventilation is used in themanagement of refractory intracranialhypertension, advanced neuromonitoring forevaluation of cerebral ischemia may beconsidered
S4 Pediatr Crit Care Med 2012 Vol. 13, No. 1 (Suppl.)
Table 1. Changes in recommendations from the first edition to the second edition
Chapter First Edition Second Edition
Cerebral PerfusionPressure
Level II—A CPP !40 mm Hg in children with TBIshould be maintained
Level III—A CPP between 40 and 65 mm Hg probablyrepresents an age-related continuum for the optimaltreatment threshold; there may be exceptions to thisrange in some infants and neonates
Level III—Advanced cerebral physiological monitoringmay be useful to define the optimal CPP in individualinstances
Level III—Hypotension should be avoided
Level III—A minimum CPP of 40 mm Hg may beconsidered in children with TBI
Level III—A CPP threshold 40–50 mm Hg may beconsidered; there may be age-specific thresholdswith infants at the lower end and adolescents atthe upper end of this range
Hyperosmolar Therapy Level III—Hypertonic saline is effective for control ofincreased ICP after severe head injury; effective dosesas a continuous infusion of 3% saline range between0.1 and 1.0 mL/kg of body weight per hour,administered on a sliding scale; the minimum doseneeded to maintain ICP "20 mm Hg should be used
Level III—Mannitol is effective for control of increasedICP after severe TBI; effective bolus doses range from0.25 g/kg of body weight to 1 g/kg of body weight
Level III—Euvolemia should be maintained by fluidreplacement; a Foley catheter is recommended inthese patients to avoid bladder rupture
Level III—Serum osmolarity should be maintainedbelow 320 mOsm/L with mannitol use, whereas alevel of 360 mOsm/L appears to be tolerated withhypertonic saline, even when used in combinationwith mannitol
Level II—Hypertonic saline should be consideredfor the treatment of severe pediatric TBIassociated with intracranial hypertension;effective doses for acute use range between 6.5and 10 mL/kg
Level III—Hypertonic saline should be considered forthe treatment of severe pediatric TBI associated withintracranial hypertension; effective doses as acontinuous infusion of 3% saline range between 0.1and 1.0 mL/kg of body weight per hour,administered on a sliding scale; the minimum doseneeded to maintain ICP "20 mm Hg should beused; serum osmolarity should be maintained below360 mOsm/L
Footnote below recommendations: although mannitolis commonly used in the management of raised ICPin pediatric TBI, no studies meeting inclusioncriteria were identified for use as evidence for thistopic
Temperature Control Level III—Extrapolated from the adult data,hyperthermia should be avoided in children withsevere TBI
Level III—Despite the lack of clinical data in children,hypothermia may be considered in the setting ofrefractory intracranial hypertension
Level II—Moderate hypothermia (32–33°C)beginning early after severe TBI for only 24 hrsduration should be avoided
Level II—Moderate hypothermia (32–33°C)beginning within 8 hrs after severe TBI for upto 48 hrs’ duration should be considered toreduce intracranial hypertension
Level II—If hypothermia is induced for anyindication, rewarming at a rate of !0.5°C perhour should be avoided
Level III—Moderate hypothermia (32–33°C)beginning early after severe TBI for 48 hrsduration may be considered
Hyperventilation Level III—Mild or prophylactic hyperventilation (PaCO2
"35 mm Hg) in children should be avoidedLevel III—Mild hyperventilation (PaCO2 30–35 mm Hg)
may be considered for longer periods for intracranialhypertension refractory to sedation and analgesia,neuromuscular blockade, cerebrospinal fluiddrainage, and hyperosmolar therapy
Level III—Aggressive hyperventilation (PaCO2 "30 mmHg) may be considered as a second-tier option in thesetting of refractory hypertension; cerebral bloodflow, jugular venous oxygen saturation, or braintissue oxygen monitoring is suggested to helpidentify cerebral ischemia in this setting
Level III—Aggressive hyperventilation therapy titratedto clinical effect may be necessary for brief periods incases of cerebral herniation or acute neurologicdeterioration
Level III—Avoidance of prophylactic severehyperventilation to a PaCO2 "30 mm Hg may beconsidered in the initial 48 hrs after injury
Level III—If hyperventilation is used in themanagement of refractory intracranialhypertension, advanced neuromonitoring forevaluation of cerebral ischemia may beconsidered
S4 Pediatr Crit Care Med 2012 Vol. 13, No. 1 (Suppl.)
Table 1. Changes in recommendations from the first edition to the second edition
Chapter First Edition Second Edition
Cerebral PerfusionPressure
Level II—A CPP !40 mm Hg in children with TBIshould be maintained
Level III—A CPP between 40 and 65 mm Hg probablyrepresents an age-related continuum for the optimaltreatment threshold; there may be exceptions to thisrange in some infants and neonates
Level III—Advanced cerebral physiological monitoringmay be useful to define the optimal CPP in individualinstances
Level III—Hypotension should be avoided
Level III—A minimum CPP of 40 mm Hg may beconsidered in children with TBI
Level III—A CPP threshold 40–50 mm Hg may beconsidered; there may be age-specific thresholdswith infants at the lower end and adolescents atthe upper end of this range
Hyperosmolar Therapy Level III—Hypertonic saline is effective for control ofincreased ICP after severe head injury; effective dosesas a continuous infusion of 3% saline range between0.1 and 1.0 mL/kg of body weight per hour,administered on a sliding scale; the minimum doseneeded to maintain ICP "20 mm Hg should be used
Level III—Mannitol is effective for control of increasedICP after severe TBI; effective bolus doses range from0.25 g/kg of body weight to 1 g/kg of body weight
Level III—Euvolemia should be maintained by fluidreplacement; a Foley catheter is recommended inthese patients to avoid bladder rupture
Level III—Serum osmolarity should be maintainedbelow 320 mOsm/L with mannitol use, whereas alevel of 360 mOsm/L appears to be tolerated withhypertonic saline, even when used in combinationwith mannitol
Level II—Hypertonic saline should be consideredfor the treatment of severe pediatric TBIassociated with intracranial hypertension;effective doses for acute use range between 6.5and 10 mL/kg
Level III—Hypertonic saline should be considered forthe treatment of severe pediatric TBI associated withintracranial hypertension; effective doses as acontinuous infusion of 3% saline range between 0.1and 1.0 mL/kg of body weight per hour,administered on a sliding scale; the minimum doseneeded to maintain ICP "20 mm Hg should beused; serum osmolarity should be maintained below360 mOsm/L
Footnote below recommendations: although mannitolis commonly used in the management of raised ICPin pediatric TBI, no studies meeting inclusioncriteria were identified for use as evidence for thistopic
Temperature Control Level III—Extrapolated from the adult data,hyperthermia should be avoided in children withsevere TBI
Level III—Despite the lack of clinical data in children,hypothermia may be considered in the setting ofrefractory intracranial hypertension
Level II—Moderate hypothermia (32–33°C)beginning early after severe TBI for only 24 hrsduration should be avoided
Level II—Moderate hypothermia (32–33°C)beginning within 8 hrs after severe TBI for upto 48 hrs’ duration should be considered toreduce intracranial hypertension
Level II—If hypothermia is induced for anyindication, rewarming at a rate of !0.5°C perhour should be avoided
Level III—Moderate hypothermia (32–33°C)beginning early after severe TBI for 48 hrsduration may be considered
Hyperventilation Level III—Mild or prophylactic hyperventilation (PaCO2
"35 mm Hg) in children should be avoidedLevel III—Mild hyperventilation (PaCO2 30–35 mm Hg)
may be considered for longer periods for intracranialhypertension refractory to sedation and analgesia,neuromuscular blockade, cerebrospinal fluiddrainage, and hyperosmolar therapy
Level III—Aggressive hyperventilation (PaCO2 "30 mmHg) may be considered as a second-tier option in thesetting of refractory hypertension; cerebral bloodflow, jugular venous oxygen saturation, or braintissue oxygen monitoring is suggested to helpidentify cerebral ischemia in this setting
Level III—Aggressive hyperventilation therapy titratedto clinical effect may be necessary for brief periods incases of cerebral herniation or acute neurologicdeterioration
Level III—Avoidance of prophylactic severehyperventilation to a PaCO2 "30 mm Hg may beconsidered in the initial 48 hrs after injury
Level III—If hyperventilation is used in themanagement of refractory intracranialhypertension, advanced neuromonitoring forevaluation of cerebral ischemia may beconsidered
S4 Pediatr Crit Care Med 2012 Vol. 13, No. 1 (Suppl.)

Hyperventilation
! Frequency of regional ischemia in TBI
! 28.9% with normocapnia
! 59.4% with PaCO2 of 25-35 mmHg
! 73.1% with PaCO2 of <25mmHg

Hyperventilation
! Prolonged hyperventilation has been shown to exacerbate secondary injury and may worsen outcome
Hyperosmolar Therapy
! Source: Guidelines for the acute medical management of severe TBI in infants, children, and adolescents. Pediatric Critical Care Medicine (2012). Volume 13, No. 1 (Supplement)
Table 1. Changes in recommendations from the first edition to the second edition
Chapter First Edition Second Edition
Cerebral PerfusionPressure
Level II—A CPP !40 mm Hg in children with TBIshould be maintained
Level III—A CPP between 40 and 65 mm Hg probablyrepresents an age-related continuum for the optimaltreatment threshold; there may be exceptions to thisrange in some infants and neonates
Level III—Advanced cerebral physiological monitoringmay be useful to define the optimal CPP in individualinstances
Level III—Hypotension should be avoided
Level III—A minimum CPP of 40 mm Hg may beconsidered in children with TBI
Level III—A CPP threshold 40–50 mm Hg may beconsidered; there may be age-specific thresholdswith infants at the lower end and adolescents atthe upper end of this range
Hyperosmolar Therapy Level III—Hypertonic saline is effective for control ofincreased ICP after severe head injury; effective dosesas a continuous infusion of 3% saline range between0.1 and 1.0 mL/kg of body weight per hour,administered on a sliding scale; the minimum doseneeded to maintain ICP "20 mm Hg should be used
Level III—Mannitol is effective for control of increasedICP after severe TBI; effective bolus doses range from0.25 g/kg of body weight to 1 g/kg of body weight
Level III—Euvolemia should be maintained by fluidreplacement; a Foley catheter is recommended inthese patients to avoid bladder rupture
Level III—Serum osmolarity should be maintainedbelow 320 mOsm/L with mannitol use, whereas alevel of 360 mOsm/L appears to be tolerated withhypertonic saline, even when used in combinationwith mannitol
Level II—Hypertonic saline should be consideredfor the treatment of severe pediatric TBIassociated with intracranial hypertension;effective doses for acute use range between 6.5and 10 mL/kg
Level III—Hypertonic saline should be considered forthe treatment of severe pediatric TBI associated withintracranial hypertension; effective doses as acontinuous infusion of 3% saline range between 0.1and 1.0 mL/kg of body weight per hour,administered on a sliding scale; the minimum doseneeded to maintain ICP "20 mm Hg should beused; serum osmolarity should be maintained below360 mOsm/L
Footnote below recommendations: although mannitolis commonly used in the management of raised ICPin pediatric TBI, no studies meeting inclusioncriteria were identified for use as evidence for thistopic
Temperature Control Level III—Extrapolated from the adult data,hyperthermia should be avoided in children withsevere TBI
Level III—Despite the lack of clinical data in children,hypothermia may be considered in the setting ofrefractory intracranial hypertension
Level II—Moderate hypothermia (32–33°C)beginning early after severe TBI for only 24 hrsduration should be avoided
Level II—Moderate hypothermia (32–33°C)beginning within 8 hrs after severe TBI for upto 48 hrs’ duration should be considered toreduce intracranial hypertension
Level II—If hypothermia is induced for anyindication, rewarming at a rate of !0.5°C perhour should be avoided
Level III—Moderate hypothermia (32–33°C)beginning early after severe TBI for 48 hrsduration may be considered
Hyperventilation Level III—Mild or prophylactic hyperventilation (PaCO2
"35 mm Hg) in children should be avoidedLevel III—Mild hyperventilation (PaCO2 30–35 mm Hg)
may be considered for longer periods for intracranialhypertension refractory to sedation and analgesia,neuromuscular blockade, cerebrospinal fluiddrainage, and hyperosmolar therapy
Level III—Aggressive hyperventilation (PaCO2 "30 mmHg) may be considered as a second-tier option in thesetting of refractory hypertension; cerebral bloodflow, jugular venous oxygen saturation, or braintissue oxygen monitoring is suggested to helpidentify cerebral ischemia in this setting
Level III—Aggressive hyperventilation therapy titratedto clinical effect may be necessary for brief periods incases of cerebral herniation or acute neurologicdeterioration
Level III—Avoidance of prophylactic severehyperventilation to a PaCO2 "30 mm Hg may beconsidered in the initial 48 hrs after injury
Level III—If hyperventilation is used in themanagement of refractory intracranialhypertension, advanced neuromonitoring forevaluation of cerebral ischemia may beconsidered
S4 Pediatr Crit Care Med 2012 Vol. 13, No. 1 (Suppl.)
Table 1. Changes in recommendations from the first edition to the second edition
Chapter First Edition Second Edition
Cerebral PerfusionPressure
Level II—A CPP !40 mm Hg in children with TBIshould be maintained
Level III—A CPP between 40 and 65 mm Hg probablyrepresents an age-related continuum for the optimaltreatment threshold; there may be exceptions to thisrange in some infants and neonates
Level III—Advanced cerebral physiological monitoringmay be useful to define the optimal CPP in individualinstances
Level III—Hypotension should be avoided
Level III—A minimum CPP of 40 mm Hg may beconsidered in children with TBI
Level III—A CPP threshold 40–50 mm Hg may beconsidered; there may be age-specific thresholdswith infants at the lower end and adolescents atthe upper end of this range
Hyperosmolar Therapy Level III—Hypertonic saline is effective for control ofincreased ICP after severe head injury; effective dosesas a continuous infusion of 3% saline range between0.1 and 1.0 mL/kg of body weight per hour,administered on a sliding scale; the minimum doseneeded to maintain ICP "20 mm Hg should be used
Level III—Mannitol is effective for control of increasedICP after severe TBI; effective bolus doses range from0.25 g/kg of body weight to 1 g/kg of body weight
Level III—Euvolemia should be maintained by fluidreplacement; a Foley catheter is recommended inthese patients to avoid bladder rupture
Level III—Serum osmolarity should be maintainedbelow 320 mOsm/L with mannitol use, whereas alevel of 360 mOsm/L appears to be tolerated withhypertonic saline, even when used in combinationwith mannitol
Level II—Hypertonic saline should be consideredfor the treatment of severe pediatric TBIassociated with intracranial hypertension;effective doses for acute use range between 6.5and 10 mL/kg
Level III—Hypertonic saline should be considered forthe treatment of severe pediatric TBI associated withintracranial hypertension; effective doses as acontinuous infusion of 3% saline range between 0.1and 1.0 mL/kg of body weight per hour,administered on a sliding scale; the minimum doseneeded to maintain ICP "20 mm Hg should beused; serum osmolarity should be maintained below360 mOsm/L
Footnote below recommendations: although mannitolis commonly used in the management of raised ICPin pediatric TBI, no studies meeting inclusioncriteria were identified for use as evidence for thistopic
Temperature Control Level III—Extrapolated from the adult data,hyperthermia should be avoided in children withsevere TBI
Level III—Despite the lack of clinical data in children,hypothermia may be considered in the setting ofrefractory intracranial hypertension
Level II—Moderate hypothermia (32–33°C)beginning early after severe TBI for only 24 hrsduration should be avoided
Level II—Moderate hypothermia (32–33°C)beginning within 8 hrs after severe TBI for upto 48 hrs’ duration should be considered toreduce intracranial hypertension
Level II—If hypothermia is induced for anyindication, rewarming at a rate of !0.5°C perhour should be avoided
Level III—Moderate hypothermia (32–33°C)beginning early after severe TBI for 48 hrsduration may be considered
Hyperventilation Level III—Mild or prophylactic hyperventilation (PaCO2
"35 mm Hg) in children should be avoidedLevel III—Mild hyperventilation (PaCO2 30–35 mm Hg)
may be considered for longer periods for intracranialhypertension refractory to sedation and analgesia,neuromuscular blockade, cerebrospinal fluiddrainage, and hyperosmolar therapy
Level III—Aggressive hyperventilation (PaCO2 "30 mmHg) may be considered as a second-tier option in thesetting of refractory hypertension; cerebral bloodflow, jugular venous oxygen saturation, or braintissue oxygen monitoring is suggested to helpidentify cerebral ischemia in this setting
Level III—Aggressive hyperventilation therapy titratedto clinical effect may be necessary for brief periods incases of cerebral herniation or acute neurologicdeterioration
Level III—Avoidance of prophylactic severehyperventilation to a PaCO2 "30 mm Hg may beconsidered in the initial 48 hrs after injury
Level III—If hyperventilation is used in themanagement of refractory intracranialhypertension, advanced neuromonitoring forevaluation of cerebral ischemia may beconsidered
S4 Pediatr Crit Care Med 2012 Vol. 13, No. 1 (Suppl.)
Table 1. Changes in recommendations from the first edition to the second edition
Chapter First Edition Second Edition
Cerebral PerfusionPressure
Level II—A CPP !40 mm Hg in children with TBIshould be maintained
Level III—A CPP between 40 and 65 mm Hg probablyrepresents an age-related continuum for the optimaltreatment threshold; there may be exceptions to thisrange in some infants and neonates
Level III—Advanced cerebral physiological monitoringmay be useful to define the optimal CPP in individualinstances
Level III—Hypotension should be avoided
Level III—A minimum CPP of 40 mm Hg may beconsidered in children with TBI
Level III—A CPP threshold 40–50 mm Hg may beconsidered; there may be age-specific thresholdswith infants at the lower end and adolescents atthe upper end of this range
Hyperosmolar Therapy Level III—Hypertonic saline is effective for control ofincreased ICP after severe head injury; effective dosesas a continuous infusion of 3% saline range between0.1 and 1.0 mL/kg of body weight per hour,administered on a sliding scale; the minimum doseneeded to maintain ICP "20 mm Hg should be used
Level III—Mannitol is effective for control of increasedICP after severe TBI; effective bolus doses range from0.25 g/kg of body weight to 1 g/kg of body weight
Level III—Euvolemia should be maintained by fluidreplacement; a Foley catheter is recommended inthese patients to avoid bladder rupture
Level III—Serum osmolarity should be maintainedbelow 320 mOsm/L with mannitol use, whereas alevel of 360 mOsm/L appears to be tolerated withhypertonic saline, even when used in combinationwith mannitol
Level II—Hypertonic saline should be consideredfor the treatment of severe pediatric TBIassociated with intracranial hypertension;effective doses for acute use range between 6.5and 10 mL/kg
Level III—Hypertonic saline should be considered forthe treatment of severe pediatric TBI associated withintracranial hypertension; effective doses as acontinuous infusion of 3% saline range between 0.1and 1.0 mL/kg of body weight per hour,administered on a sliding scale; the minimum doseneeded to maintain ICP "20 mm Hg should beused; serum osmolarity should be maintained below360 mOsm/L
Footnote below recommendations: although mannitolis commonly used in the management of raised ICPin pediatric TBI, no studies meeting inclusioncriteria were identified for use as evidence for thistopic
Temperature Control Level III—Extrapolated from the adult data,hyperthermia should be avoided in children withsevere TBI
Level III—Despite the lack of clinical data in children,hypothermia may be considered in the setting ofrefractory intracranial hypertension
Level II—Moderate hypothermia (32–33°C)beginning early after severe TBI for only 24 hrsduration should be avoided
Level II—Moderate hypothermia (32–33°C)beginning within 8 hrs after severe TBI for upto 48 hrs’ duration should be considered toreduce intracranial hypertension
Level II—If hypothermia is induced for anyindication, rewarming at a rate of !0.5°C perhour should be avoided
Level III—Moderate hypothermia (32–33°C)beginning early after severe TBI for 48 hrsduration may be considered
Hyperventilation Level III—Mild or prophylactic hyperventilation (PaCO2
"35 mm Hg) in children should be avoidedLevel III—Mild hyperventilation (PaCO2 30–35 mm Hg)
may be considered for longer periods for intracranialhypertension refractory to sedation and analgesia,neuromuscular blockade, cerebrospinal fluiddrainage, and hyperosmolar therapy
Level III—Aggressive hyperventilation (PaCO2 "30 mmHg) may be considered as a second-tier option in thesetting of refractory hypertension; cerebral bloodflow, jugular venous oxygen saturation, or braintissue oxygen monitoring is suggested to helpidentify cerebral ischemia in this setting
Level III—Aggressive hyperventilation therapy titratedto clinical effect may be necessary for brief periods incases of cerebral herniation or acute neurologicdeterioration
Level III—Avoidance of prophylactic severehyperventilation to a PaCO2 "30 mm Hg may beconsidered in the initial 48 hrs after injury
Level III—If hyperventilation is used in themanagement of refractory intracranialhypertension, advanced neuromonitoring forevaluation of cerebral ischemia may beconsidered
S4 Pediatr Crit Care Med 2012 Vol. 13, No. 1 (Suppl.)

How can we lower ICP?

Hyperosmolar Therapy
! Hypertonic Saline
! Low penetration across BBB - lowers ICP
! Positive side effects
! Negative side effects
Hyperosmolar Therapy

Hyperosmolar Therapy
! 2012 Guidelines –
! Level 2 evidence for hypertonic saline bolus therapy
! Level 3 evidence for hypertonic saline infusion therapy
! What about mannitol??

Hyperosmolar Therapy
! Mannitol
! Widespread use
! Limited pediatric data
! Concern: accumulation in injured brain tissue

Hyperosmolar Therapy
! “One must thus weigh the value of longstanding clinical acceptance and safety of mannitol, which has no evidence to support its efficacy... against hypertonic saline, for which there is less clinical experience but reasonably good performance in contemporary clinical trials”

Decompressive Craniectomy
! 2012 Guidelines – consider craniectomy in patients:
! Showing early signs of neurologic deterioration or herniation
! Developing ICH refractory to medical therapies

How can we lower ICP?
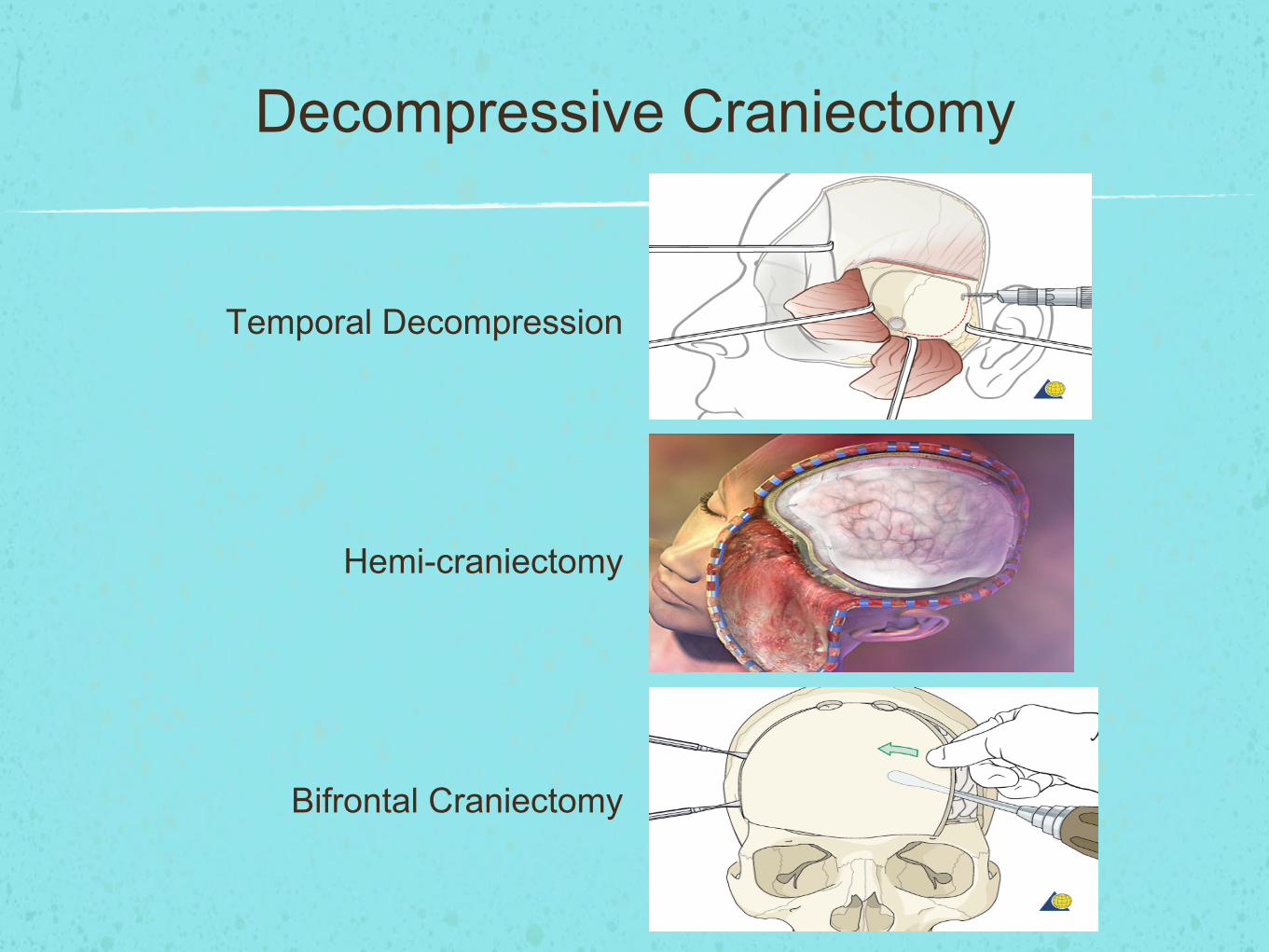
Decompressive Craniectomy
Temporal Decompression
Hemi-craniectomy
Bifrontal Craniectomy

Decompressive Craniectomy
Questions:
Early versus late?
Rescue vs solo intervention?

Decompressive Craniectomy

CSF Drainage
! Level 3 evidence only
! CSF drainage with EVD may be considered for elevated ICP in severe TBI
! Addition of a lumbar drain may be considered for refractory elevated ICP

How can we lower ICP?

CSF Drainage

Third Tier Strategies
Barbiturate Coma

Temperature Control
! Hypothermia
! Decreases CMRO2 & CBF
! At 27C, CBF = 50%
! At 20C, CBF =10%
! Risks?

How can we lower ICP?

Temperature Control
! Source: Guidelines for the acute medical management of severe TBI in infants, children, and adolescents. Pediatric Critical Care Medicine (2012). Volume 13, No. 1 (Supplement)
Table 1. Changes in recommendations from the first edition to the second edition
Chapter First Edition Second Edition
Cerebral PerfusionPressure
Level II—A CPP !40 mm Hg in children with TBIshould be maintained
Level III—A CPP between 40 and 65 mm Hg probablyrepresents an age-related continuum for the optimaltreatment threshold; there may be exceptions to thisrange in some infants and neonates
Level III—Advanced cerebral physiological monitoringmay be useful to define the optimal CPP in individualinstances
Level III—Hypotension should be avoided
Level III—A minimum CPP of 40 mm Hg may beconsidered in children with TBI
Level III—A CPP threshold 40–50 mm Hg may beconsidered; there may be age-specific thresholdswith infants at the lower end and adolescents atthe upper end of this range
Hyperosmolar Therapy Level III—Hypertonic saline is effective for control ofincreased ICP after severe head injury; effective dosesas a continuous infusion of 3% saline range between0.1 and 1.0 mL/kg of body weight per hour,administered on a sliding scale; the minimum doseneeded to maintain ICP "20 mm Hg should be used
Level III—Mannitol is effective for control of increasedICP after severe TBI; effective bolus doses range from0.25 g/kg of body weight to 1 g/kg of body weight
Level III—Euvolemia should be maintained by fluidreplacement; a Foley catheter is recommended inthese patients to avoid bladder rupture
Level III—Serum osmolarity should be maintainedbelow 320 mOsm/L with mannitol use, whereas alevel of 360 mOsm/L appears to be tolerated withhypertonic saline, even when used in combinationwith mannitol
Level II—Hypertonic saline should be consideredfor the treatment of severe pediatric TBIassociated with intracranial hypertension;effective doses for acute use range between 6.5and 10 mL/kg
Level III—Hypertonic saline should be considered forthe treatment of severe pediatric TBI associated withintracranial hypertension; effective doses as acontinuous infusion of 3% saline range between 0.1and 1.0 mL/kg of body weight per hour,administered on a sliding scale; the minimum doseneeded to maintain ICP "20 mm Hg should beused; serum osmolarity should be maintained below360 mOsm/L
Footnote below recommendations: although mannitolis commonly used in the management of raised ICPin pediatric TBI, no studies meeting inclusioncriteria were identified for use as evidence for thistopic
Temperature Control Level III—Extrapolated from the adult data,hyperthermia should be avoided in children withsevere TBI
Level III—Despite the lack of clinical data in children,hypothermia may be considered in the setting ofrefractory intracranial hypertension
Level II—Moderate hypothermia (32–33°C)beginning early after severe TBI for only 24 hrsduration should be avoided
Level II—Moderate hypothermia (32–33°C)beginning within 8 hrs after severe TBI for upto 48 hrs’ duration should be considered toreduce intracranial hypertension
Level II—If hypothermia is induced for anyindication, rewarming at a rate of !0.5°C perhour should be avoided
Level III—Moderate hypothermia (32–33°C)beginning early after severe TBI for 48 hrsduration may be considered
Hyperventilation Level III—Mild or prophylactic hyperventilation (PaCO2
"35 mm Hg) in children should be avoidedLevel III—Mild hyperventilation (PaCO2 30–35 mm Hg)
may be considered for longer periods for intracranialhypertension refractory to sedation and analgesia,neuromuscular blockade, cerebrospinal fluiddrainage, and hyperosmolar therapy
Level III—Aggressive hyperventilation (PaCO2 "30 mmHg) may be considered as a second-tier option in thesetting of refractory hypertension; cerebral bloodflow, jugular venous oxygen saturation, or braintissue oxygen monitoring is suggested to helpidentify cerebral ischemia in this setting
Level III—Aggressive hyperventilation therapy titratedto clinical effect may be necessary for brief periods incases of cerebral herniation or acute neurologicdeterioration
Level III—Avoidance of prophylactic severehyperventilation to a PaCO2 "30 mm Hg may beconsidered in the initial 48 hrs after injury
Level III—If hyperventilation is used in themanagement of refractory intracranialhypertension, advanced neuromonitoring forevaluation of cerebral ischemia may beconsidered
S4 Pediatr Crit Care Med 2012 Vol. 13, No. 1 (Suppl.)
Table 1. Changes in recommendations from the first edition to the second edition
Chapter First Edition Second Edition
Cerebral PerfusionPressure
Level II—A CPP !40 mm Hg in children with TBIshould be maintained
Level III—A CPP between 40 and 65 mm Hg probablyrepresents an age-related continuum for the optimaltreatment threshold; there may be exceptions to thisrange in some infants and neonates
Level III—Advanced cerebral physiological monitoringmay be useful to define the optimal CPP in individualinstances
Level III—Hypotension should be avoided
Level III—A minimum CPP of 40 mm Hg may beconsidered in children with TBI
Level III—A CPP threshold 40–50 mm Hg may beconsidered; there may be age-specific thresholdswith infants at the lower end and adolescents atthe upper end of this range
Hyperosmolar Therapy Level III—Hypertonic saline is effective for control ofincreased ICP after severe head injury; effective dosesas a continuous infusion of 3% saline range between0.1 and 1.0 mL/kg of body weight per hour,administered on a sliding scale; the minimum doseneeded to maintain ICP "20 mm Hg should be used
Level III—Mannitol is effective for control of increasedICP after severe TBI; effective bolus doses range from0.25 g/kg of body weight to 1 g/kg of body weight
Level III—Euvolemia should be maintained by fluidreplacement; a Foley catheter is recommended inthese patients to avoid bladder rupture
Level III—Serum osmolarity should be maintainedbelow 320 mOsm/L with mannitol use, whereas alevel of 360 mOsm/L appears to be tolerated withhypertonic saline, even when used in combinationwith mannitol
Level II—Hypertonic saline should be consideredfor the treatment of severe pediatric TBIassociated with intracranial hypertension;effective doses for acute use range between 6.5and 10 mL/kg
Level III—Hypertonic saline should be considered forthe treatment of severe pediatric TBI associated withintracranial hypertension; effective doses as acontinuous infusion of 3% saline range between 0.1and 1.0 mL/kg of body weight per hour,administered on a sliding scale; the minimum doseneeded to maintain ICP "20 mm Hg should beused; serum osmolarity should be maintained below360 mOsm/L
Footnote below recommendations: although mannitolis commonly used in the management of raised ICPin pediatric TBI, no studies meeting inclusioncriteria were identified for use as evidence for thistopic
Temperature Control Level III—Extrapolated from the adult data,hyperthermia should be avoided in children withsevere TBI
Level III—Despite the lack of clinical data in children,hypothermia may be considered in the setting ofrefractory intracranial hypertension
Level II—Moderate hypothermia (32–33°C)beginning early after severe TBI for only 24 hrsduration should be avoided
Level II—Moderate hypothermia (32–33°C)beginning within 8 hrs after severe TBI for upto 48 hrs’ duration should be considered toreduce intracranial hypertension
Level II—If hypothermia is induced for anyindication, rewarming at a rate of !0.5°C perhour should be avoided
Level III—Moderate hypothermia (32–33°C)beginning early after severe TBI for 48 hrsduration may be considered
Hyperventilation Level III—Mild or prophylactic hyperventilation (PaCO2
"35 mm Hg) in children should be avoidedLevel III—Mild hyperventilation (PaCO2 30–35 mm Hg)
may be considered for longer periods for intracranialhypertension refractory to sedation and analgesia,neuromuscular blockade, cerebrospinal fluiddrainage, and hyperosmolar therapy
Level III—Aggressive hyperventilation (PaCO2 "30 mmHg) may be considered as a second-tier option in thesetting of refractory hypertension; cerebral bloodflow, jugular venous oxygen saturation, or braintissue oxygen monitoring is suggested to helpidentify cerebral ischemia in this setting
Level III—Aggressive hyperventilation therapy titratedto clinical effect may be necessary for brief periods incases of cerebral herniation or acute neurologicdeterioration
Level III—Avoidance of prophylactic severehyperventilation to a PaCO2 "30 mm Hg may beconsidered in the initial 48 hrs after injury
Level III—If hyperventilation is used in themanagement of refractory intracranialhypertension, advanced neuromonitoring forevaluation of cerebral ischemia may beconsidered
S4 Pediatr Crit Care Med 2012 Vol. 13, No. 1 (Suppl.)
Table 1. Changes in recommendations from the first edition to the second edition
Chapter First Edition Second Edition
Cerebral PerfusionPressure
Level II—A CPP !40 mm Hg in children with TBIshould be maintained
Level III—A CPP between 40 and 65 mm Hg probablyrepresents an age-related continuum for the optimaltreatment threshold; there may be exceptions to thisrange in some infants and neonates
Level III—Advanced cerebral physiological monitoringmay be useful to define the optimal CPP in individualinstances
Level III—Hypotension should be avoided
Level III—A minimum CPP of 40 mm Hg may beconsidered in children with TBI
Level III—A CPP threshold 40–50 mm Hg may beconsidered; there may be age-specific thresholdswith infants at the lower end and adolescents atthe upper end of this range
Hyperosmolar Therapy Level III—Hypertonic saline is effective for control ofincreased ICP after severe head injury; effective dosesas a continuous infusion of 3% saline range between0.1 and 1.0 mL/kg of body weight per hour,administered on a sliding scale; the minimum doseneeded to maintain ICP "20 mm Hg should be used
Level III—Mannitol is effective for control of increasedICP after severe TBI; effective bolus doses range from0.25 g/kg of body weight to 1 g/kg of body weight
Level III—Euvolemia should be maintained by fluidreplacement; a Foley catheter is recommended inthese patients to avoid bladder rupture
Level III—Serum osmolarity should be maintainedbelow 320 mOsm/L with mannitol use, whereas alevel of 360 mOsm/L appears to be tolerated withhypertonic saline, even when used in combinationwith mannitol
Level II—Hypertonic saline should be consideredfor the treatment of severe pediatric TBIassociated with intracranial hypertension;effective doses for acute use range between 6.5and 10 mL/kg
Level III—Hypertonic saline should be considered forthe treatment of severe pediatric TBI associated withintracranial hypertension; effective doses as acontinuous infusion of 3% saline range between 0.1and 1.0 mL/kg of body weight per hour,administered on a sliding scale; the minimum doseneeded to maintain ICP "20 mm Hg should beused; serum osmolarity should be maintained below360 mOsm/L
Footnote below recommendations: although mannitolis commonly used in the management of raised ICPin pediatric TBI, no studies meeting inclusioncriteria were identified for use as evidence for thistopic
Temperature Control Level III—Extrapolated from the adult data,hyperthermia should be avoided in children withsevere TBI
Level III—Despite the lack of clinical data in children,hypothermia may be considered in the setting ofrefractory intracranial hypertension
Level II—Moderate hypothermia (32–33°C)beginning early after severe TBI for only 24 hrsduration should be avoided
Level II—Moderate hypothermia (32–33°C)beginning within 8 hrs after severe TBI for upto 48 hrs’ duration should be considered toreduce intracranial hypertension
Level II—If hypothermia is induced for anyindication, rewarming at a rate of !0.5°C perhour should be avoided
Level III—Moderate hypothermia (32–33°C)beginning early after severe TBI for 48 hrsduration may be considered
Hyperventilation Level III—Mild or prophylactic hyperventilation (PaCO2
"35 mm Hg) in children should be avoidedLevel III—Mild hyperventilation (PaCO2 30–35 mm Hg)
may be considered for longer periods for intracranialhypertension refractory to sedation and analgesia,neuromuscular blockade, cerebrospinal fluiddrainage, and hyperosmolar therapy
Level III—Aggressive hyperventilation (PaCO2 "30 mmHg) may be considered as a second-tier option in thesetting of refractory hypertension; cerebral bloodflow, jugular venous oxygen saturation, or braintissue oxygen monitoring is suggested to helpidentify cerebral ischemia in this setting
Level III—Aggressive hyperventilation therapy titratedto clinical effect may be necessary for brief periods incases of cerebral herniation or acute neurologicdeterioration
Level III—Avoidance of prophylactic severehyperventilation to a PaCO2 "30 mm Hg may beconsidered in the initial 48 hrs after injury
Level III—If hyperventilation is used in themanagement of refractory intracranialhypertension, advanced neuromonitoring forevaluation of cerebral ischemia may beconsidered
S4 Pediatr Crit Care Med 2012 Vol. 13, No. 1 (Suppl.)

Temperature Control

Temperature Control
Sedation and Medications
! Source: Guidelines for the acute medical management of severe TBI in infants, children, and adolescents. Pediatric Critical Care Medicine (2012). Volume 13, No. 1 (Supplement)
rather than diagnosis or prognosis; 3) chap-ters from the first edition which were elim-inated from the second edition includeTrauma Systems, Prehospital Airway Man-agement,b Resuscitation of Blood Pressureand Oxygenation,c Intracranial PressureMonitoring Technology,d and the CriticalPathway for Treatment of Intracranial Hy-pertensione’; 4) broader representation onthe committee of the relevant specialties inthe field, including pediatric anesthesiol-ogy, child neurology, and neuroradiology;and 5) international representation on the
guidelines committee includes Drs.Kissoon and Tasker.
As indicated, some publications in-cluded in the first edition were elimi-nated, because the methods team foundthey did not meet criteria (Appendix A,publications from the first edition notincluded in the second edition).
Table 1 summarizes changes in therecommendations from the first editionto the second edition of these guidelines.
The field is moving forward and it isclear that with advances in neuromoni-toring and imaging and the publication,subsequent to the first edition of theguidelines, of the results of the first ma-jor multicentered randomized controlledtrials in pediatric TBI, we are on the righttrack. Given the importance of severe TBIto the overall burden of childhood mor-bidity and mortality, we hope that thesenew guidelines aid caregivers and stimu-late the pediatric TBI community to gen-erate additional answers.
The authors thank the 14 externalpeer reviewers who further improved thequality of this document through inde-pendent review, including Drs. MarkDias, Richard Ellenbogen, Stuart Friess,Jeffrey Greenfield, Ann-Marie Guergue-rian, Mary Hartman, Mark Helfaer, JohnKuluz, Yi-Chen Lai, Leon Moores, JosePineda, Paul Shore, Kimberley Statler-Bennett, and Michael Whalen. The au-thors also thank Dr. Hector Wong, whoserved as the guest editor of this docu-ment for Pediatric Critical Care Medi-cine. Finally, we are extremely grateful tothe Brain Trauma Foundation for takingon this project and providing the re-sources necessary to ensure its successand for their commitment to improvingthe care of infants, children, and adoles-cents with severe TBI.
REFERENCES1. Adelson PD, Bratton SL, Carney NA, et al:
Guidelines for the acute medical manage-
bPrehospital treatment of pediatric patients withTBI is addressed in the Guidelines for PrehospitalManagement of Severe Traumatic Brain Injury (14).
cThere were no publications that met the inclusioncriteria for this topic.
dThis topic is addressed in the Guidelines for theManagement of Severe Traumatic Brain Injury, ThirdEdition (15).
eThe critical pathway will be developed and pub-lished as a separate document.
Table 1.—Continued
Chapter First Edition Second Edition
Corticosteroids Level III—The use of steroids is not recommended forimproving outcome or reducing ICP in pediatricpatients with severe TBI; despite two class II studiesfailing to show efficacy, the small sample sizespreclude support for a treatment guideline for thistopic
Level II—The use of corticosteroids is notrecommended to improve outcome or reduceICP for children with severe TBI
Analgesics, Sedatives,and NeuromuscularBlockade
Level III—In the absence of outcome data, the choiceof dosing and sedatives, analgesics, andneuromuscular-blocking agents used in themanagement of infants and children with severe TBIshould be left to the treating physician; however, theeffect of individual sedatives and analgesics on ICP ininfants and children with severe TBI can be variableand unpredictable
Level III—Etomidate may be considered to controlsevere intracranial hypertension; however, therisks resulting from adrenal suppression mustbe considered
Level III—Thiopental may be considered tocontrol intracranial hypertension
Footnotes below recommendations:In the absence of outcome data, the specific
indications, choice and dosing of analgesics,sedatives, and neuromuscular-blocking agentsused in the management of infants and childrenwith TBI should be left to the treating physician
As stated by the Food and Drug Administration,continuous infusion of propofol for eithersedation or the management of refractoryintracranial hypertension in infants and childrenwith severe TBI is not recommended)
Glucose and Nutrition Level III—Replace 130% to 160% of resting metabolismexpenditure after TBI in pediatric patients
Level II—The evidence does not support the use ofan immune-modulating diet for the treatmentof severe TBI to improve outcome
Antiseizure Prophylaxis Level II—Prophylactic use of antiseizure therapy is notrecommended for children with severe TBI forpreventing late posttraumatic seizures
Level III—Prophylactic antiseizure therapy may beconsidered as a treatment option to prevent earlyposttraumatic seizure in young pediatric patients andinfants at high risk for seizures after head injury
Level III—Prophylactic treatment with phenytoinmay be considered to reduce the incidence ofearly posttraumatic seizures in pediatric patientswith severe TBI
CPP, cerebral perfusion pressure; TBI, traumatic brain injury; ICP, intracranial pressure.
S5Pediatr Crit Care Med 2012 Vol. 13, No. 1 (Suppl.)
rather than diagnosis or prognosis; 3) chap-ters from the first edition which were elim-inated from the second edition includeTrauma Systems, Prehospital Airway Man-agement,b Resuscitation of Blood Pressureand Oxygenation,c Intracranial PressureMonitoring Technology,d and the CriticalPathway for Treatment of Intracranial Hy-pertensione’; 4) broader representation onthe committee of the relevant specialties inthe field, including pediatric anesthesiol-ogy, child neurology, and neuroradiology;and 5) international representation on the
guidelines committee includes Drs.Kissoon and Tasker.
As indicated, some publications in-cluded in the first edition were elimi-nated, because the methods team foundthey did not meet criteria (Appendix A,publications from the first edition notincluded in the second edition).
Table 1 summarizes changes in therecommendations from the first editionto the second edition of these guidelines.
The field is moving forward and it isclear that with advances in neuromoni-toring and imaging and the publication,subsequent to the first edition of theguidelines, of the results of the first ma-jor multicentered randomized controlledtrials in pediatric TBI, we are on the righttrack. Given the importance of severe TBIto the overall burden of childhood mor-bidity and mortality, we hope that thesenew guidelines aid caregivers and stimu-late the pediatric TBI community to gen-erate additional answers.
The authors thank the 14 externalpeer reviewers who further improved thequality of this document through inde-pendent review, including Drs. MarkDias, Richard Ellenbogen, Stuart Friess,Jeffrey Greenfield, Ann-Marie Guergue-rian, Mary Hartman, Mark Helfaer, JohnKuluz, Yi-Chen Lai, Leon Moores, JosePineda, Paul Shore, Kimberley Statler-Bennett, and Michael Whalen. The au-thors also thank Dr. Hector Wong, whoserved as the guest editor of this docu-ment for Pediatric Critical Care Medi-cine. Finally, we are extremely grateful tothe Brain Trauma Foundation for takingon this project and providing the re-sources necessary to ensure its successand for their commitment to improvingthe care of infants, children, and adoles-cents with severe TBI.
REFERENCES1. Adelson PD, Bratton SL, Carney NA, et al:
Guidelines for the acute medical manage-
bPrehospital treatment of pediatric patients withTBI is addressed in the Guidelines for PrehospitalManagement of Severe Traumatic Brain Injury (14).
cThere were no publications that met the inclusioncriteria for this topic.
dThis topic is addressed in the Guidelines for theManagement of Severe Traumatic Brain Injury, ThirdEdition (15).
eThe critical pathway will be developed and pub-lished as a separate document.
Table 1.—Continued
Chapter First Edition Second Edition
Corticosteroids Level III—The use of steroids is not recommended forimproving outcome or reducing ICP in pediatricpatients with severe TBI; despite two class II studiesfailing to show efficacy, the small sample sizespreclude support for a treatment guideline for thistopic
Level II—The use of corticosteroids is notrecommended to improve outcome or reduceICP for children with severe TBI
Analgesics, Sedatives,and NeuromuscularBlockade
Level III—In the absence of outcome data, the choiceof dosing and sedatives, analgesics, andneuromuscular-blocking agents used in themanagement of infants and children with severe TBIshould be left to the treating physician; however, theeffect of individual sedatives and analgesics on ICP ininfants and children with severe TBI can be variableand unpredictable
Level III—Etomidate may be considered to controlsevere intracranial hypertension; however, therisks resulting from adrenal suppression mustbe considered
Level III—Thiopental may be considered tocontrol intracranial hypertension
Footnotes below recommendations:In the absence of outcome data, the specific
indications, choice and dosing of analgesics,sedatives, and neuromuscular-blocking agentsused in the management of infants and childrenwith TBI should be left to the treating physician
As stated by the Food and Drug Administration,continuous infusion of propofol for eithersedation or the management of refractoryintracranial hypertension in infants and childrenwith severe TBI is not recommended)
Glucose and Nutrition Level III—Replace 130% to 160% of resting metabolismexpenditure after TBI in pediatric patients
Level II—The evidence does not support the use ofan immune-modulating diet for the treatmentof severe TBI to improve outcome
Antiseizure Prophylaxis Level II—Prophylactic use of antiseizure therapy is notrecommended for children with severe TBI forpreventing late posttraumatic seizures
Level III—Prophylactic antiseizure therapy may beconsidered as a treatment option to prevent earlyposttraumatic seizure in young pediatric patients andinfants at high risk for seizures after head injury
Level III—Prophylactic treatment with phenytoinmay be considered to reduce the incidence ofearly posttraumatic seizures in pediatric patientswith severe TBI
CPP, cerebral perfusion pressure; TBI, traumatic brain injury; ICP, intracranial pressure.
S5Pediatr Crit Care Med 2012 Vol. 13, No. 1 (Suppl.)
rather than diagnosis or prognosis; 3) chap-ters from the first edition which were elim-inated from the second edition includeTrauma Systems, Prehospital Airway Man-agement,b Resuscitation of Blood Pressureand Oxygenation,c Intracranial PressureMonitoring Technology,d and the CriticalPathway for Treatment of Intracranial Hy-pertensione’; 4) broader representation onthe committee of the relevant specialties inthe field, including pediatric anesthesiol-ogy, child neurology, and neuroradiology;and 5) international representation on the
guidelines committee includes Drs.Kissoon and Tasker.
As indicated, some publications in-cluded in the first edition were elimi-nated, because the methods team foundthey did not meet criteria (Appendix A,publications from the first edition notincluded in the second edition).
Table 1 summarizes changes in therecommendations from the first editionto the second edition of these guidelines.
The field is moving forward and it isclear that with advances in neuromoni-toring and imaging and the publication,subsequent to the first edition of theguidelines, of the results of the first ma-jor multicentered randomized controlledtrials in pediatric TBI, we are on the righttrack. Given the importance of severe TBIto the overall burden of childhood mor-bidity and mortality, we hope that thesenew guidelines aid caregivers and stimu-late the pediatric TBI community to gen-erate additional answers.
The authors thank the 14 externalpeer reviewers who further improved thequality of this document through inde-pendent review, including Drs. MarkDias, Richard Ellenbogen, Stuart Friess,Jeffrey Greenfield, Ann-Marie Guergue-rian, Mary Hartman, Mark Helfaer, JohnKuluz, Yi-Chen Lai, Leon Moores, JosePineda, Paul Shore, Kimberley Statler-Bennett, and Michael Whalen. The au-thors also thank Dr. Hector Wong, whoserved as the guest editor of this docu-ment for Pediatric Critical Care Medi-cine. Finally, we are extremely grateful tothe Brain Trauma Foundation for takingon this project and providing the re-sources necessary to ensure its successand for their commitment to improvingthe care of infants, children, and adoles-cents with severe TBI.
REFERENCES1. Adelson PD, Bratton SL, Carney NA, et al:
Guidelines for the acute medical manage-
bPrehospital treatment of pediatric patients withTBI is addressed in the Guidelines for PrehospitalManagement of Severe Traumatic Brain Injury (14).
cThere were no publications that met the inclusioncriteria for this topic.
dThis topic is addressed in the Guidelines for theManagement of Severe Traumatic Brain Injury, ThirdEdition (15).
eThe critical pathway will be developed and pub-lished as a separate document.
Table 1.—Continued
Chapter First Edition Second Edition
Corticosteroids Level III—The use of steroids is not recommended forimproving outcome or reducing ICP in pediatricpatients with severe TBI; despite two class II studiesfailing to show efficacy, the small sample sizespreclude support for a treatment guideline for thistopic
Level II—The use of corticosteroids is notrecommended to improve outcome or reduceICP for children with severe TBI
Analgesics, Sedatives,and NeuromuscularBlockade
Level III—In the absence of outcome data, the choiceof dosing and sedatives, analgesics, andneuromuscular-blocking agents used in themanagement of infants and children with severe TBIshould be left to the treating physician; however, theeffect of individual sedatives and analgesics on ICP ininfants and children with severe TBI can be variableand unpredictable
Level III—Etomidate may be considered to controlsevere intracranial hypertension; however, therisks resulting from adrenal suppression mustbe considered
Level III—Thiopental may be considered tocontrol intracranial hypertension
Footnotes below recommendations:In the absence of outcome data, the specific
indications, choice and dosing of analgesics,sedatives, and neuromuscular-blocking agentsused in the management of infants and childrenwith TBI should be left to the treating physician
As stated by the Food and Drug Administration,continuous infusion of propofol for eithersedation or the management of refractoryintracranial hypertension in infants and childrenwith severe TBI is not recommended)
Glucose and Nutrition Level III—Replace 130% to 160% of resting metabolismexpenditure after TBI in pediatric patients
Level II—The evidence does not support the use ofan immune-modulating diet for the treatmentof severe TBI to improve outcome
Antiseizure Prophylaxis Level II—Prophylactic use of antiseizure therapy is notrecommended for children with severe TBI forpreventing late posttraumatic seizures
Level III—Prophylactic antiseizure therapy may beconsidered as a treatment option to prevent earlyposttraumatic seizure in young pediatric patients andinfants at high risk for seizures after head injury
Level III—Prophylactic treatment with phenytoinmay be considered to reduce the incidence ofearly posttraumatic seizures in pediatric patientswith severe TBI
CPP, cerebral perfusion pressure; TBI, traumatic brain injury; ICP, intracranial pressure.
S5Pediatr Crit Care Med 2012 Vol. 13, No. 1 (Suppl.)rather than diagnosis or prognosis; 3) chap-ters from the first edition which were elim-inated from the second edition includeTrauma Systems, Prehospital Airway Man-agement,b Resuscitation of Blood Pressureand Oxygenation,c Intracranial PressureMonitoring Technology,d and the CriticalPathway for Treatment of Intracranial Hy-pertensione’; 4) broader representation onthe committee of the relevant specialties inthe field, including pediatric anesthesiol-ogy, child neurology, and neuroradiology;and 5) international representation on the
guidelines committee includes Drs.Kissoon and Tasker.
As indicated, some publications in-cluded in the first edition were elimi-nated, because the methods team foundthey did not meet criteria (Appendix A,publications from the first edition notincluded in the second edition).
Table 1 summarizes changes in therecommendations from the first editionto the second edition of these guidelines.
The field is moving forward and it isclear that with advances in neuromoni-toring and imaging and the publication,subsequent to the first edition of theguidelines, of the results of the first ma-jor multicentered randomized controlledtrials in pediatric TBI, we are on the righttrack. Given the importance of severe TBIto the overall burden of childhood mor-bidity and mortality, we hope that thesenew guidelines aid caregivers and stimu-late the pediatric TBI community to gen-erate additional answers.
The authors thank the 14 externalpeer reviewers who further improved thequality of this document through inde-pendent review, including Drs. MarkDias, Richard Ellenbogen, Stuart Friess,Jeffrey Greenfield, Ann-Marie Guergue-rian, Mary Hartman, Mark Helfaer, JohnKuluz, Yi-Chen Lai, Leon Moores, JosePineda, Paul Shore, Kimberley Statler-Bennett, and Michael Whalen. The au-thors also thank Dr. Hector Wong, whoserved as the guest editor of this docu-ment for Pediatric Critical Care Medi-cine. Finally, we are extremely grateful tothe Brain Trauma Foundation for takingon this project and providing the re-sources necessary to ensure its successand for their commitment to improvingthe care of infants, children, and adoles-cents with severe TBI.
REFERENCES1. Adelson PD, Bratton SL, Carney NA, et al:
Guidelines for the acute medical manage-
bPrehospital treatment of pediatric patients withTBI is addressed in the Guidelines for PrehospitalManagement of Severe Traumatic Brain Injury (14).
cThere were no publications that met the inclusioncriteria for this topic.
dThis topic is addressed in the Guidelines for theManagement of Severe Traumatic Brain Injury, ThirdEdition (15).
eThe critical pathway will be developed and pub-lished as a separate document.
Table 1.—Continued
Chapter First Edition Second Edition
Corticosteroids Level III—The use of steroids is not recommended forimproving outcome or reducing ICP in pediatricpatients with severe TBI; despite two class II studiesfailing to show efficacy, the small sample sizespreclude support for a treatment guideline for thistopic
Level II—The use of corticosteroids is notrecommended to improve outcome or reduceICP for children with severe TBI
Analgesics, Sedatives,and NeuromuscularBlockade
Level III—In the absence of outcome data, the choiceof dosing and sedatives, analgesics, andneuromuscular-blocking agents used in themanagement of infants and children with severe TBIshould be left to the treating physician; however, theeffect of individual sedatives and analgesics on ICP ininfants and children with severe TBI can be variableand unpredictable
Level III—Etomidate may be considered to controlsevere intracranial hypertension; however, therisks resulting from adrenal suppression mustbe considered
Level III—Thiopental may be considered tocontrol intracranial hypertension
Footnotes below recommendations:In the absence of outcome data, the specific
indications, choice and dosing of analgesics,sedatives, and neuromuscular-blocking agentsused in the management of infants and childrenwith TBI should be left to the treating physician
As stated by the Food and Drug Administration,continuous infusion of propofol for eithersedation or the management of refractoryintracranial hypertension in infants and childrenwith severe TBI is not recommended)
Glucose and Nutrition Level III—Replace 130% to 160% of resting metabolismexpenditure after TBI in pediatric patients
Level II—The evidence does not support the use ofan immune-modulating diet for the treatmentof severe TBI to improve outcome
Antiseizure Prophylaxis Level II—Prophylactic use of antiseizure therapy is notrecommended for children with severe TBI forpreventing late posttraumatic seizures
Level III—Prophylactic antiseizure therapy may beconsidered as a treatment option to prevent earlyposttraumatic seizure in young pediatric patients andinfants at high risk for seizures after head injury
Level III—Prophylactic treatment with phenytoinmay be considered to reduce the incidence ofearly posttraumatic seizures in pediatric patientswith severe TBI
CPP, cerebral perfusion pressure; TBI, traumatic brain injury; ICP, intracranial pressure.
S5Pediatr Crit Care Med 2012 Vol. 13, No. 1 (Suppl.)

Sedation & Medications
! Etomidate bolus successful as an intervention for elevated ICP, but may cause adrenal suppression (Bramwell et al, 2006)
! No safety concerns with other sedatives
! Propofol: avoid use, as per FDA recommendations in pediatrics
! Clinician preference beyond these statements, as there is no supporting outcome data

What have we learned?
! Optimal CPP is >40mmHg, and up to 60mmHg approaching adult age
! Hyperventilation: significant risk of cerebral ischemia
! Increased usage of 3%NaCl (bolus and infusion) for ICP management
! Decompressive craniectomy and CSF drainage help with ICP control
! Barbiturates: good ICP control, with side effects
! Hypothermia: between 24-48 hours duration, slow rewarming





























