Embed Size (px)
Citation preview
Pediatric & Neonatal Advanced Life Support
Intensive Review of Pediatric Anesthesia Dr. Jim Fehr, Washington University
March 2015
Intensive Review of Pediatric Anesthesiology 2015 1
Disclosures
No financial conflicts
Intensive Review of Pediatric Anesthesiology 2015 2

Learning Objectives • Causes of perioperative cardiac arrest 2010 Updates: • Basic Life Support [BLS] • Neonatal Resuscitation Program [NRP] • Pediatric Advanced Life Support [PALS]
• Team Training & Crisis Resource Management
Intensive Review of Pediatric Anesthesiology 2015 3

4 ASA Refresher 2007 Domino

Pediatric vs Adult Closed Claims
5 Anes 1993 Morray

Pediatric Closed Claims
6 2007 A&A Jimenez

Causes of anesthesia-related cardiac arrest
7 CPR, Ch38, Smith's Ped Anes, 2011

8 CPR, Ch38, Smith's Ped Anes, 2011

9 CPR, Ch38, Smith's Ped Anes, 2011

CPR, Ch38, Smith's Ped Anes, 2011 10

The Frequency of Cardiac Arrests in Patients with Congenital Heart Disease Undergoing Cardiac Catheterization
Odegard A&A 2013 11

Death or Neurologic Injury After Tonsillectomy in Children with a Focus on Obstructive Sleep Apnea
12 Coté A&A 2013

Postoperative Mortality in Children After 101,885 Anesthetics at a Tertiary Pediatric Hospital
13 A&A 2011 Van der Griend

14 PEDS 2012

15

CPR Changes in 2010
ABCs changed to CAB Removed:
“Look-Listen-Feel” & “Give two rescue breaths”
40th American President as lifeguard
16
CAB: Circulation-Airway-Breathing
1. “Are you all right?” Look for breathing 2. Activate emergency response & get AED 3. Check for a carotid pulse
– (no more than 10 seconds)
4. Defibrillation Early defibrillation & chest compressions
High-Quality CPR = ROSC (ROSC=return of spontaneous circulation)
17

• Start compressions within 10 seconds • Push hard, push fast • Allow complete chest recoil • Minimize interruptions • Give effective breaths • Avoid excessive ventilation
18

Pediatric BLS • Age 1 to Puberty • Puberty: underarm/chest hair in males, any
breast development in females
• If you are alone & event was unwitnessed: do 5 cycles before activating emergency response
19

Infant BLS: 1 rescuer
• Check for response & breathing • Call for help & AED • Check for pulse (brachial) for 5-10 seconds • If HR<60 or no pulse: assure adequate oxygenation • If oxygenation OK: Start Chest compressions • Two fingers for chest compressions • One third the depth of the chest (1.5 inches=4 cm)
@ rate of at least 100 bpm • Rate 30 compressions per 2 breaths 20

Infant BLS: 2 rescuer
• Check for response & breathing • Call for help & AED • Check for pulse (brachial) for 5-10 seconds • If HR<60 or no pulse: assure adequate oxygenation • If oxygenation OK: Start Chest compressions • Two thumb encircling hands for 2 rescuers • One third the depth of the chest (1.5 inches=4 cm)
@ rate of at least 100 bpm • Rate 15 compressions per 2 breaths 21

High-Quality CPR
High quality CPR increases the likelihood of survival
22

2014 Feb CPR Update
• Chest compression fraction >80% of the time • Switch roles every 5 cycles in less than 5 seconds
• Chest compression rate 100-120/min • Chest compression depth
• 50 mm or greater in adults • At least 1/3rd of the AP diameter in infants & kids
• Complete chest recoil • Avoid excessive ventilation:
• Rate of 12 or less breaths per minute
23

Capnography Correlates with ROSC
Return of Spontaneous Circulation
EtCO2<10 mmHg correlated with worse outcome EtCO2<20 mmHg potentially inadequate coronary perfusion
24

NEJM 1997 Levine 25
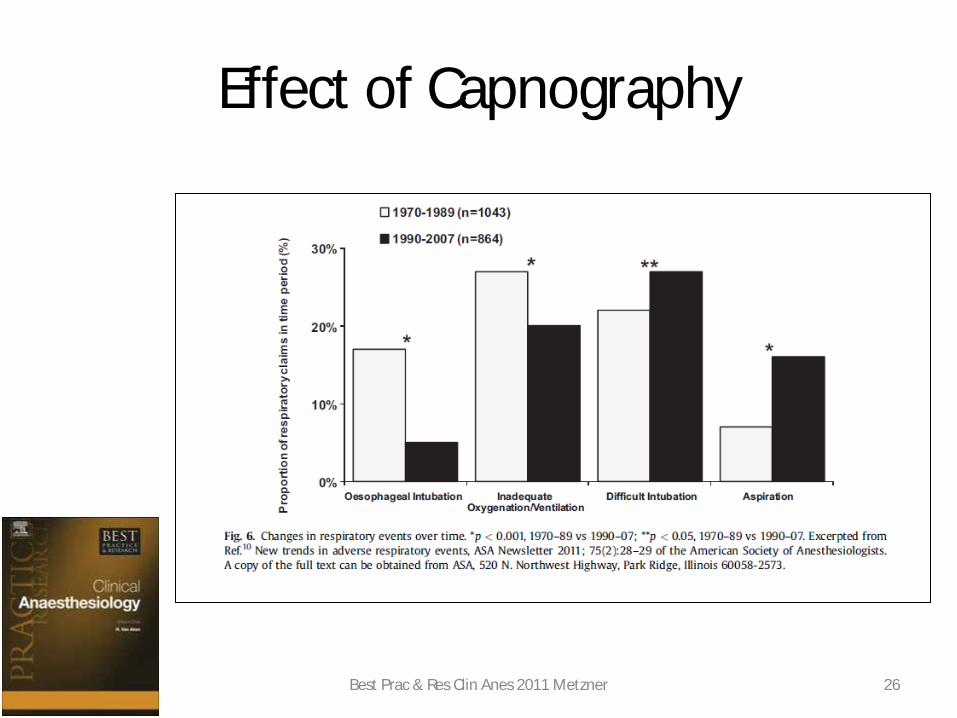
Effect of Capnography
26 Best Prac & Res Clin Anes 2011 Metzner
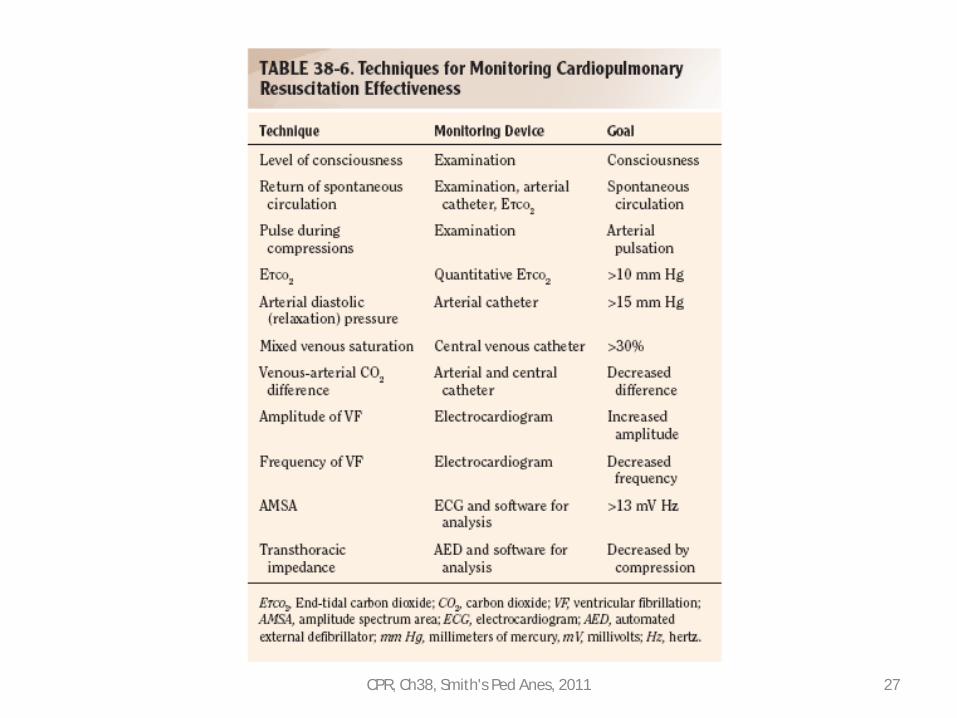
27 CPR, Ch38, Smith's Ped Anes, 2011

Vascular Access
If a peripheral intravenous line cannot be placed
expeditiously, obtain intraosseous (IO) access
Any medication that can be given intravenously can be given via an IO as can fluids including
crystalloid, colloid and blood products
28

Vascular Access
CPR, Ch38, Smith's Ped Anes, 2011 29

NRP & PALS
NRP ≈ NALS PALS ≠ NRP
PALS is sponsored by the AHA, NRP is supported by the American Academy of Pediatrics in conjunction with the AHA.
30

31 Kleinman Circulation 2010;122:S876-S908
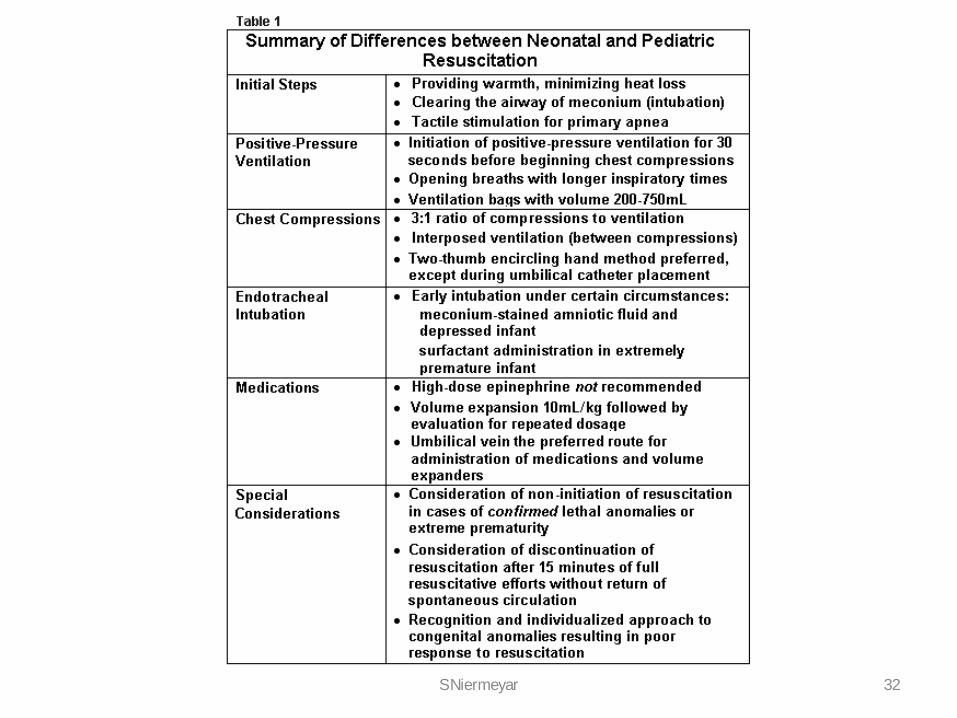
32 S Niermeyar

Fetal Circulation
33
Figure 1. The fetal pattern of circulation is characterized by right-to-left shunts at the level of the patent foramen ovale and the ductus arteriosus. These shunts close after birth with successful transition to the neonatal circulatory pattern.
Kattwinkel (ed) Textbook of Neonatal Resuscitation, AHA/AAP

Neonatal Resuscitation Program [NRP] The critical first minute
• Warm, Dry & Stimulate • Clear airway if necessary • Assess heart rate
– If >100: consider CPAP • Or if labored breathing, cyanosis, grunting) but patient
has respiratory effort
– If <100: PPV • Or apnea / ineffective respirations
• Pulse oximeter on right hand 34 A Vaccharajani & S Julian pc

Kattwinkel Circ 2010;122:S909-S919

Titrating FiO2 delivery
• Titrate with good judgment • CPAP with room air • Blend in FiO2 to achieve target SpO2 • Increase FiO2 to 100% until HR>100
36 A Vaccharajani & S Julian pc

Suctioning • Do not routinely suction airway • Suction if obvious airway obstruction to
spontaneous breathing • Suction if positive-pressure ventilation
or CPAP required • If meconium, intubation and immediate
suctioning may remove meconium – Done prior to warm/dry/stimulate – But no evidence it will reduce
meconium aspiration syndrome
37 S Julian pc

2009 Arch Dis Child, Dawson 38
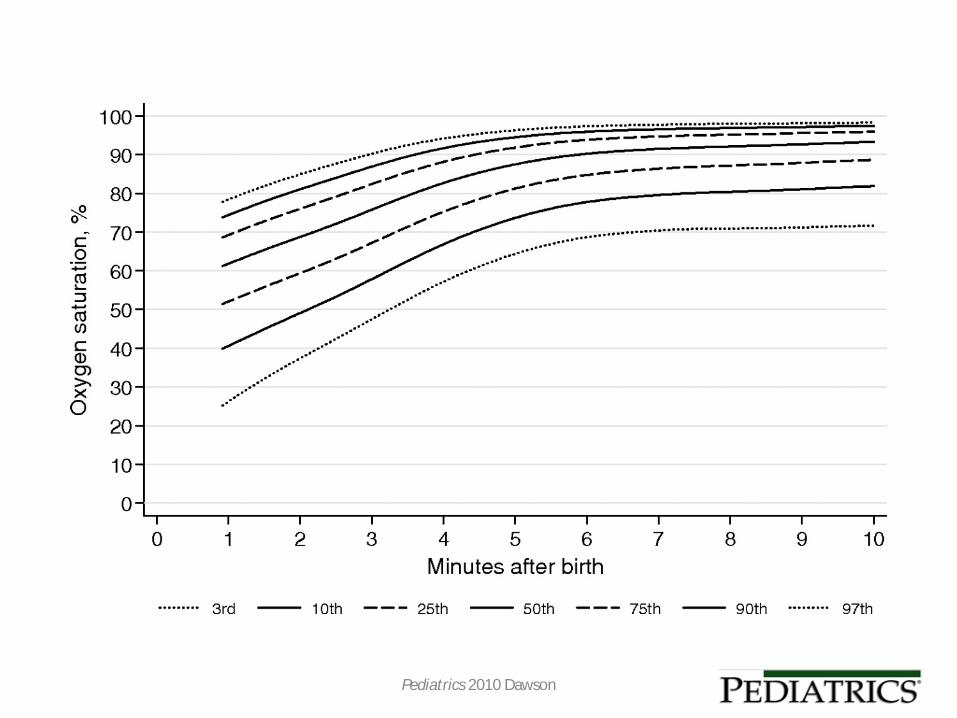
Pediatrics 2010 Dawson

Healthy Term Neonate Saturations
J Ped 2007 Mariani

Bag Mask Ventilation
• Apnea • Ineffective CPAP • Grunting with HR<100 • Agonal or gasping respirations
41

Newborn Resuscitation Algorithm
Copyright © American Heart Association, Inc. All rights reserved. 42 Kattwinkel Circ 2010;122:S909-S919

Newborn Airway: MRSOPA
MRSOPA: Corrective actions for ineffective BMV
• M - reposition mask • R - reposition airway, sniffing position • S - suction • O - open mouth • P - increase pressure used • A - consider ETT / LMA
43 A Vaccharajani & S Julian pc

Newborn Airway
• Laryngeal Mask Airways: Limited data on newborns <2000 gram or <34 weeks gestation
• Endotracheal Intubation: – Nonvigorous meconium-stained newborns – Ineffective bag-mask ventilation – Chest compressions – Special circumstances: e.g. Diaphragmatic hernia
44

Thermoregulation
• Warm baby but avoid hyperthermia • Can wrap in plastic to prevent hypothermia • Pay attention to warming when transporting
infant
45
Virginia Apgar MD (1909-1974)
• Columbia ‘33 medical school • Trained as a surgeon Columbia ‘35 • Encouraged by Allen Whipple, surgical
chair at Columbia, to study anesthesiology • Became the first director of anesthesiology
at Columbia in 1937 46

NRP: Apgars
A þ Appearance (Color) P þ Pulse (Heart Rate) G þ Grimace (Response to Stimulation) A þ Activity (Muscle Tone) R þ Respiration (Respiration)
47

48 Laptook, PEDS 2009
• Associated the 10-min Apgar with outcomes in infants with HIE
• Death or severe disability common in infants with Apgar score <7 at 10 min
• Outcome of 10 minute Apgar score of 0, 1 & 2 are comparable

Discontinuation of newborn CPR
• If no heart rate develops in a newborn within
10 minutes of appropriate resuscitation • Longer resuscitation than 10 minutes should
be guided by presumed etiology, gestation, complications and parent’s feelings
49 Kattwinkel Circ 2010;122:S909-S919

PALS
• Bradycardic Arrest • Tachyarrhythmias
– Narrow Complex – Wide Complex
• Asystole/Pulseless Electrical Activity [PEA] 50

Incidence of out-of-hospital arrest in Dutch children
51 Bardai 2011 JACC

Shock States
Compensated Shock
• Tachycardia • Cool & pale distal extremities • Prolonged (>2 sec) capillary refill • Weak peripheral pulses • Normal systolic blood pressure
Worsening Shock
• Depressed mental status • Decreased urine output • Metabolic acidosis • Tachypnea • Weak central pulses • Deterioration in color (mottling)
52 Kleinman 2010;122:S876-S908

Shock States
Compensated Shock
• Tachycardia • Cool & pale distal extremities • Prolonged (>2 sec) capillary refill • Weak peripheral pulses • Normal systolic blood pressure
Decompensated Shock
• Depressed mental status • Decreased urine output • Metabolic acidosis • Tachypnea • Weak central pulses • Deterioration in color (mottling) • Pallor • Peripheral cyanosis • Hypotension
53 Kleinman Circulation 2010;122:S876-S908

54 CPR, Ch38, Smith's Ped Anes, 2011

Copyright © American Heart Association, Inc. All rights reserved. 55 c

PALS Bradycardia
• If at any time patient becomes pulseless,
follow Pulseless Arrest Algorithm • Otherwise, support airway & breathing • Monitor if perfusion adequate • If HR<60 and poor perfusion, begin CPR
56 Kleinman Circulation 2010;122:S876-S908
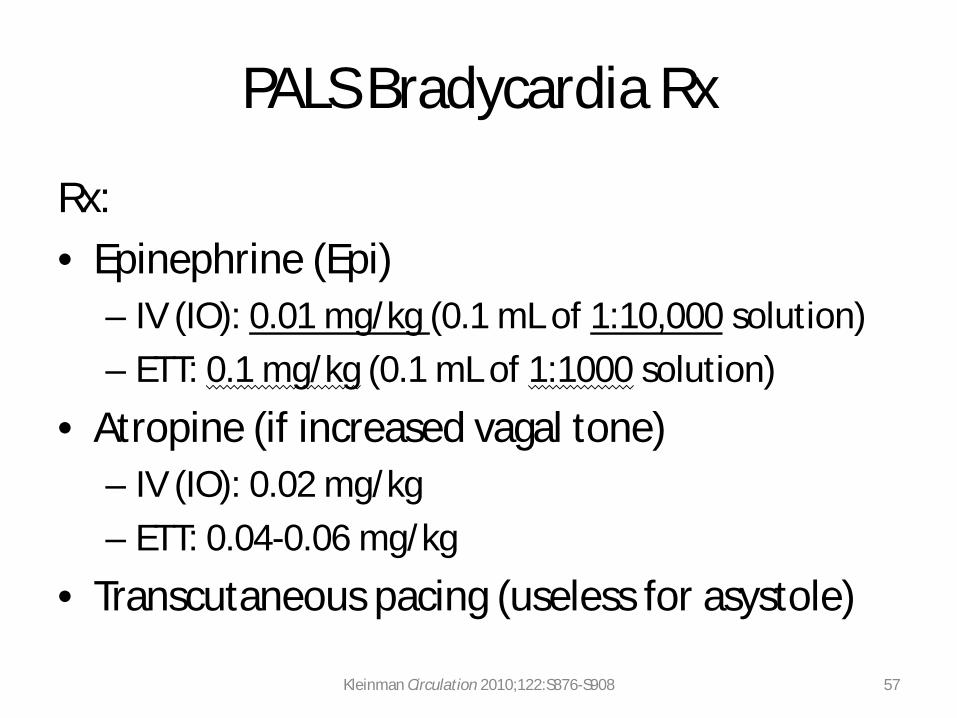
PALS Bradycardia Rx
Rx: • Epinephrine (Epi)
– IV (IO): 0.01 mg/kg (0.1 mL of 1:10,000 solution) – ETT: 0.1 mg/kg (0.1 mL of 1:1000 solution)
• Atropine (if increased vagal tone) – IV (IO): 0.02 mg/kg – ETT: 0.04-0.06 mg/kg
• Transcutaneous pacing (useless for asystole)
57 Kleinman Circulation 2010;122:S876-S908

58 CPR, Ch38, Smith's Ped Anes, 2011

PALS Tachycardia Algorithm.
Copyright © American Heart Association, Inc. All rights reserved. 59 Kleinman Circulation 2010;122:S876-S908

PALS Tachycardia
• If poor perfusion or pulseless, follow Pulseless Arrest Algorithm
• Otherwise, support airway & breathing • Monitor if perfusion adequate • Attach monitor/defibrillator • Obtain vascular access • Evaluate a 12-lead ECG, assess QRS duration
60 Kleinman Circulation 2010;122:S876-S908

PALS Tachycardia
• Narrow-complex (<0.09 sec) tachycardia • Supraventricular tachycardia
– Vagal stimulation – Rx: Adenosine 0.1 mg/kg (flush immediately) – Adenosine should only be used if rhythm is
regular and QRS is monomorphic – Do not use Adenosine in Wolff-Parkinson-White or
Wide-complex tachycardia
• Wide-complex (>0.09 sec) tachycardia 61 Kleinman Circulation 2010;122:S876-S908

Wide-complex (>0.09 sec) tachycardia
• If pulseless, follow Pulseless Arrest Algorithm • If hemodynamically stable, consult cardiology • Synchronized cardioversion: 0.5 –1 J/kg
– Double to 2 J/kg if first shock ineffective
• Rx: – Amiodarone (5mg/kg slow IV) – Procainamide (15 mg/kg slow IV)
62 Kleinman Circulation 2010;122:S876-S908
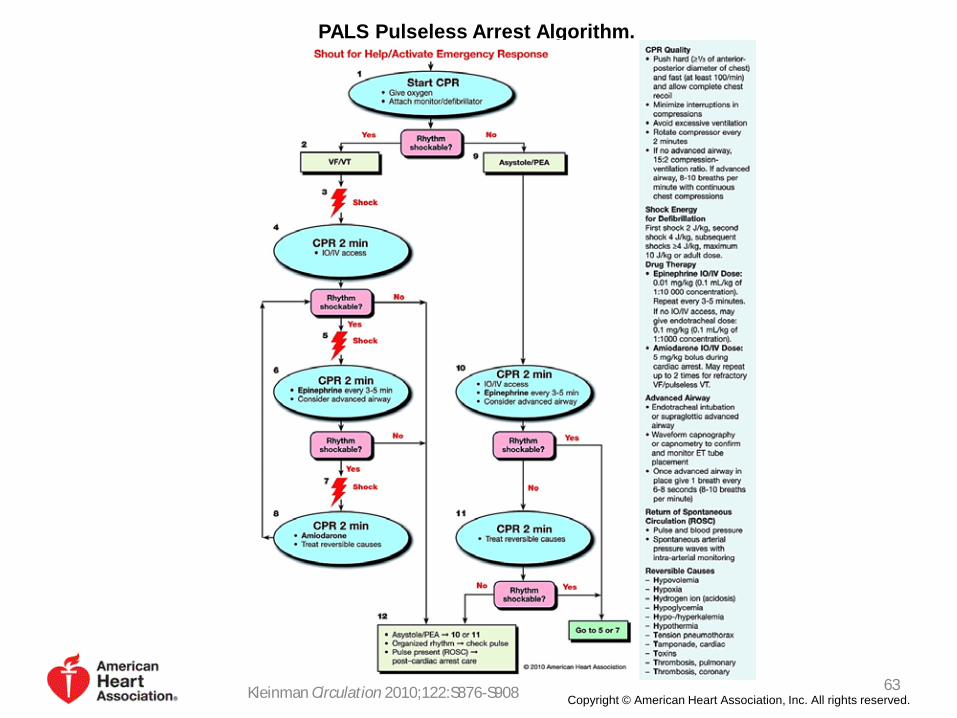
PALS Pulseless Arrest Algorithm.
Copyright © American Heart Association, Inc. All rights reserved. 63 Kleinman Circulation 2010;122:S876-S908
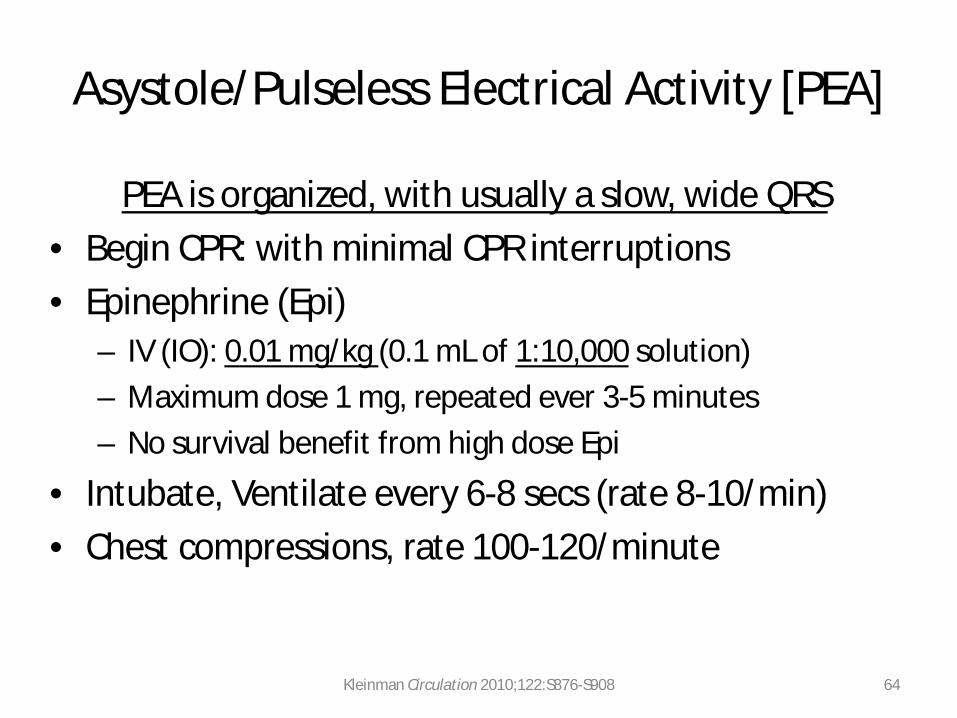
Asystole/Pulseless Electrical Activity [PEA]
PEA is organized, with usually a slow, wide QRS • Begin CPR: with minimal CPR interruptions • Epinephrine (Epi)
– IV (IO): 0.01 mg/kg (0.1 mL of 1:10,000 solution) – Maximum dose 1 mg, repeated ever 3-5 minutes – No survival benefit from high dose Epi
• Intubate, Ventilate every 6-8 secs (rate 8-10/min) • Chest compressions, rate 100-120/minute
64 Kleinman Circulation 2010;122:S876-S908

Asystole/Pulseless Electrical Activity [PEA]
• Check rhythm every 2 minutes with minimal breaks • Rotate compressor role every 2 minutes • If rhythm “Shockable” (VF/pulseless VT): Do it
– Survival 17-20% & declines in adults by 7-10%/min CPR – “Adult” sized pads can be used for children >10 kg – Initial defibrillation dose 2-4 J/kg – Higher energy level not to exceed 10 J/kg or adult max dose
• Torsades de pointes: – Rx: Rapid IV Magnesium sulfate (25-50 mg/kg up to 2G)
65 Kleinman Circulation 2010;122:S876-S908

• Hypovolemia • Hypoxia • Hydrogen ions (acidosis) • Hypoglycemia • Hypo-/Hyper-kalemia • Hypothermia • Pulm Hypertension
• Tension Pneumothorax • Tamponade (Cardiac) • Toxins • Thrombosis (Coronary) • Thrombosis (Pulmonary)
66 CPR, Ch38, Smith's Ped Anes, 2011

Equipment for Pedi Periop Arrest
67 2013 A&A Shaffner
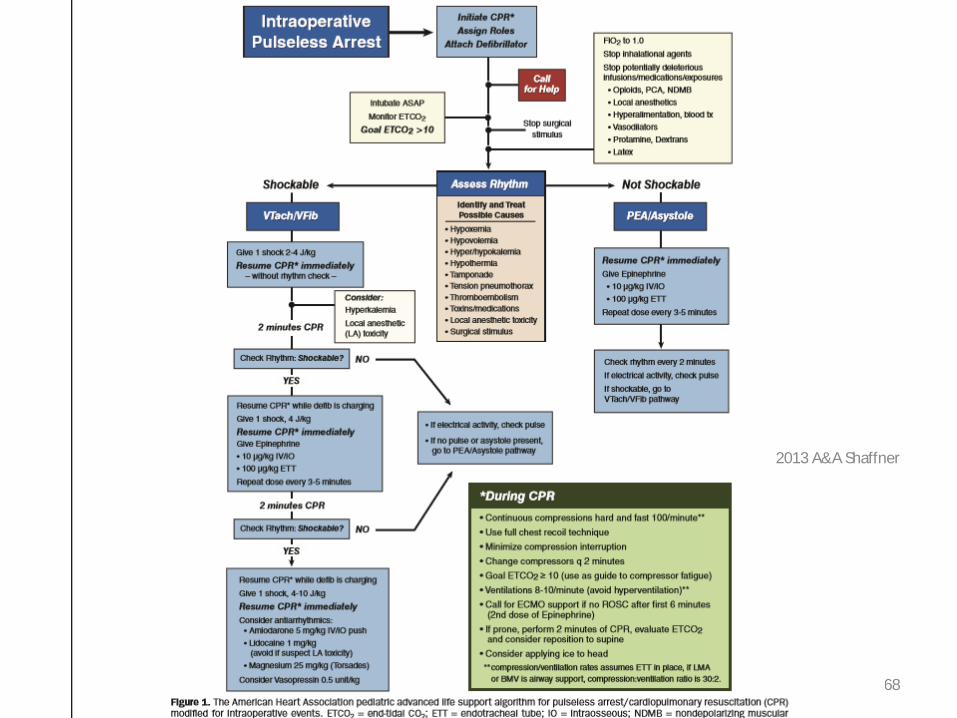
68
2013 A&A Shaffner

69
2013 A&A Shaffner

Post resuscitation care
• Notification of family • Contact intensive care unit • Administration of vasopressors • Preparation to transfer patient to ICU • Transport to ICU: Monitoring including
capnography
70
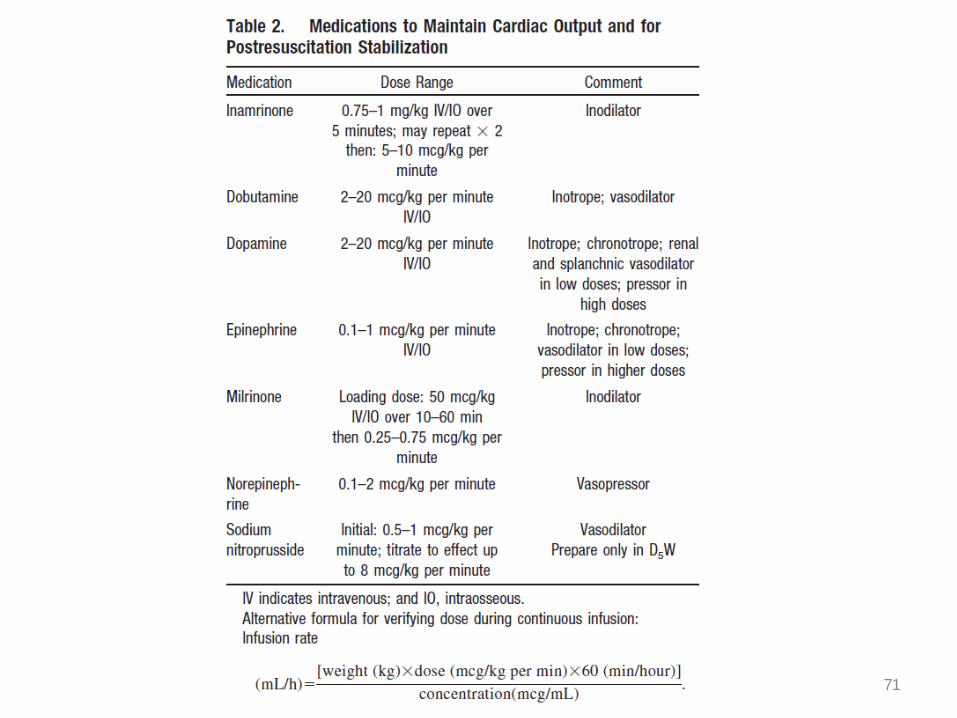
71

Team Training & CRM
72

CRM
Communication Briefing
Backup Behavior
Mutual Performance Monitoring
Team Leadership
Decision Making
Task-related Assertiveness
Team Adaptability
Shared Situation
Awareness
73

– Code Leader – Airway – Compressions – Access – Monitor – Recorder
74 CPR, Ch38, Smith's Ped Anes, 2011

CRM: Crisis Resource Management
Core Principles: • Leadership • Communication • Role Clarity • Resource allocation • Personnel support • Situational awareness
CPR, Ch38, Smith's Ped Anes, 2011 75
Elements of Team Dynamics
• Closed-Loop Communication • Clear Messages • Clear Roles & Responsibilities • Know your Limitations • Knowledge Sharing • Constructive Intervention • Summarizing & Reevaluation • Mutual Respect
76

Simulation for CPR training
Assessed the effectiveness of an educational intervention on performance of ED teams in simulated pediatric trauma resuscitations
– 17% of North Carolina EDs – Unannounced simulated pediatric trauma – Educational intervention – ED return 6 months later
77 PEC 2007 Hunt

Simulation for CPR training
78 PEC 2007 Hunt

79 Resus 2010 Donoghue
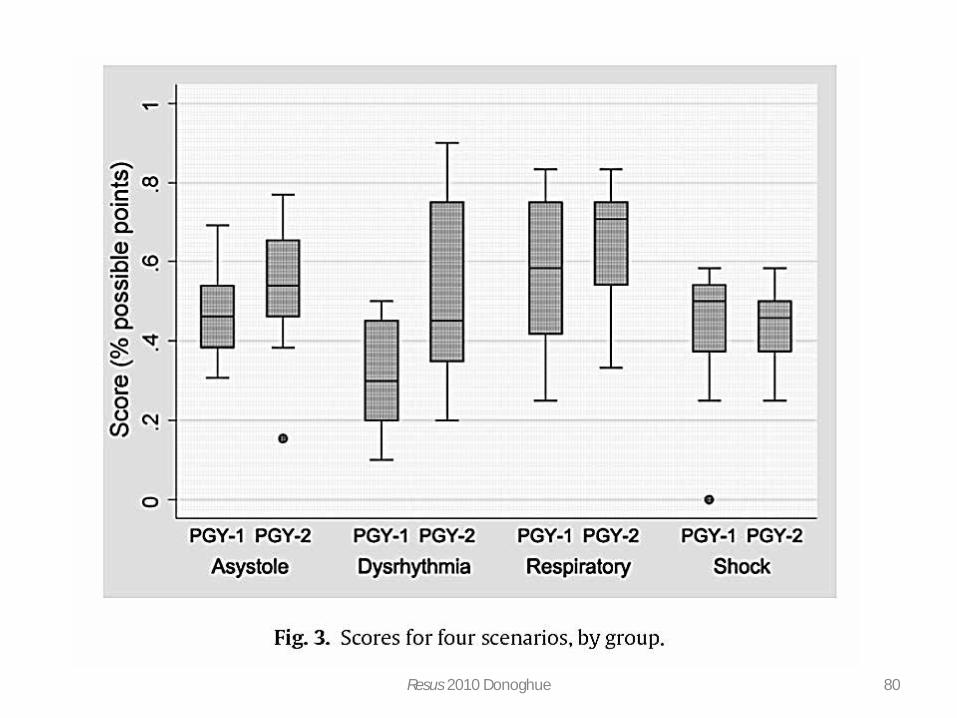
80 Resus 2010 Donoghue

Anesthesiology Howard-Quijano 2010

Anesthesiology April 2010

Simulation-based Assessment to Identify Critical Gaps in Safe Anesthesia Resident Performance
83 Anesthesiology 2014 Blum

84 http://www.pedsanesthesia.org/newnews/Critical_Event_Checklists.pdf

85

86

SPA Critical Events
Checklist App
87

Perioperative death, What to do?
• (Re)Introduce yourself • Create the requisite solemnity • Make a moment sacred • Be compassionate • Provide the family with room to grieve
88
Perioperative death, What to do?
• Emotional and Spiritual support • Encourage family to contact you
– Give your card or cellphone number
• A follow up meeting with the family • Debrief your team
89

Medical-Legal Concerns
• Disclose events • Clear & Timely Documentation • Contact Risk Management
90

Recap
• CAB: Circulation-Airway-Breathing • Early Chest Compressions • Early Defibrillation • Rate 100-120 • Do not ventilate excessively • Minimal interruptions of CPR
91
Nuns Shooting Guns
92

93

References
• CPR, Schwartz et al, Ch 38 Smith's Ped Anes 8th ed, Davis, 2011 • Atlas of Pediatric Physical Diagnosis, Zitelli, 2007 • Pediatric BLS update, Berg et al, Circulation, 2010 • PALS update, Kleinman et al, Circulation, 2010 • NRP update, Kattwinkel et al, Circulation, 2010
Intensive Review of Pediatric Anesthesiology 2015 94





























