Embed Size (px)
Citation preview

Pediatric Idiopathic Chronic Pain
Disorders
Lucinda M Brown MSN, RN, CNS
Dr. Daniel Lacey MD, PhDJanuary 2015

“ Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage or
described in terms of such damage.”- International Association for the Study of Pain
“Pain is an inherently subjective multi-factorial experience and should be assessed and treated as
such.”- American Academy of Pediatrics and American Pain Society

What is the Purpose of Pain?
Acute pain serves as a protective mechanism against impending tissue injury or death
Chronic pain in contrast serves no such physiologic role and is itself not a symptom, but a disease state.

Acute vs. Chronic Pain
Characteristic Acute Pain Chronic Pain
Cause Generally known Often unknown
Duration of pain Short, well-characterized
Persists after healing, ³3 months
Treatmentapproach
Resolution of underlying cause, usually self-limited
Underlying cause and pain disorder; outcome is often pain control, not cure

Defining Pain
Acute Pain Classification
Somatic Pain: Result of activation of nociceptors (sensory
receptors) sensitive to noxious stimuli in cutaneous or deep
tissues. Experienced locally and described as constant,
aching and gnawing. The most common type in cancer
patients.
Visceral Pain: Mediated by nociceptors. Described as deep,
aching and colicky. Is poorly localized and often is referred
to cutaneous sites, which may be tender. In cancer patients,
results from stretching of viscera by tumor growth.

Defining Pain
Chronic Pain ClassificationNociceptive pain: Visceral or somatic.
stimulation of pain receptors by tissue inflammation, mechanical deformation, ongoing tissue injury. Responds well to common analgesic medications and nondrug strategies.
Neuropathic Pain:Involves the peripheral or central nervous system. Does not respond predictably to conventional analgesics. May respond to adjuvant analgesic drugs. Visceral pain also neuropathic.
Mixed or undetermined pathophysiology:Treatment is unpredictable; requires various approaches.
Psychologically based pain syndromes:Traditional analgesia is not indicated, doesn’t work. Uncommon.

Pediatric Chronic Pain In a large series of 8-16 year-olds, 37.3% had
chronic pain, but only 5.1% had moderate or severe chronic pain; percent increased with age
They had a worse quality of life, missed more days of school, were more likely to miss school
Of those initially reporting chronic pain, 58% still suffered at one year follow-up
Peer relationships are often disrupted, deficient
Huguet A, Miro J. The Severity of Chronic Pediatric Pain: An epidemiological Study. J Pain. 2008;9(3):226-236

Chronic Pain in Children
Pain that lasts at least 1, 3-6, >6 months (contrast chronic from recurrent)
Must be viewed within developmental, ecobiopsychosocial domains
Prematures, neonates fully capable of pain perception and establishing pain “memory”
Objective signs may be absent, in contrast to acute pain
Am Pain Soc Bulletin Jan-Feb. 2001, pp10-12


Misconceptions That Can Lead to Under Treatment of Pain in Children
Children, especially infants do not:– Feel pain the way adults do– Remember pain
Lack of assessment for presence of pain Lack of knowledge of pediatric analgesics
– Use– Dosing– Adverse effects
Preventing pain takes too much time
Pediatrics 2001; 108(3): 793-797

Identifiable Causes of Chronic Pain
Cancer Sickle cell disease HIV, pancreatitis, tumor-related,
neuropathies Cystic fibrosis Cerebral palsy Metabolic disorders Autoimmune/inflammatory disorders (JRA)

Idiopathic Chronic Pain in Children
Headaches, Migraine Recurrent Abdominal Pain (RAP) Musculoskeletal- neck, leg, back, arm,
chest Primary Juvenile Fibromyalgia Neuropathic, CRPS

What’s Causing Chronic Pain?
Idiopathic Pain Syndromes • e.g. fibromyalgia, headaches, irritable bowel• 15 – 20% of population have sx. severe enough to seek medical attention• frequently co-exist with inflammatory and mechanical disorders
Mechanical or “Wear-and-tear” Disorders • e.g. osteoarthritis • prevalence very age-dependant
Autoimmune and Inflammatory Disorders• e.g. rheumatoid arthritis, lupus• 2 – 3 % of population

The “Pain Vulnerable Child”
Both intrinsic and extrinsic factors predispose child to develop more pain than peers under similar circumstances
Whether patient develops “Pain Associated Disability” is influenced by many factors, including family behavior and cultural expectations, access to health care and whether certain kinds of health care are acceptable.

Extrinsic Factors for Chronic Pain
Previous pain experiences Social deprivation Physical or sexual abuse Parental modeling of chronic pain behaviors Sleep disturbances Decreased fitness, limited exercise Stressors- school difficulties, poor test taking,
bereavement

Intrinsic Factors for Chronic Pain Low pain thresholds Female gender Hypermobility of joints Poor perceived control over pain Maladaptive coping strategies Difficult temperament Many of these are genetic
Malleson PN, Connell H, Bennett SM, Eccleston C. Chronic musculoskeletal and other idiopathic pain syndromes. Arch Dis Child. 2001;84:189-192

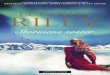
Physiology of Pain Perception
Transduction Transmission Modulation Perception Interpretation Behavior
Injury
Descending Pathway
PeripheralNerve
Dorsal RootGanglion
C-Fiber
A-beta Fiber
A-delta Fiber
AscendingPathways
Dorsal Horn
Brain
Spinal Cord
Adapted with permission from WebMD Scientific American® Medicine.17

Volume
+
Volume
Brain and Spinal Influences on Pain Processing
• Substance P• Glutamate and EAA • Serotonin (5HT2a, 3a)
• Neurotensin• Nerve growth factor
• Descending analgesic pathways – Norepinephrine –
serotonin (5HT1a,b)
– Opioids• GABA• Cannabanoids• Adenosine

Central Sensitization
Nociceptive neurons in CNS develop lowered thresholds and increase in suprathreshold responses. This also results from dysfunction of endogenous descending pain control systems. Initially protective, thresholds should return to baseline if tissue injury is absent. Instead, they respond more to non-nocuous stimuli and outlast an initiating trigger.
Hyperalgesia- excessive sensitivity to a normally painful stimulus
Allodynia- painful sensation to a normally non-painful stimulus. This is an easy clinical sign of sensitization.
Expansion of the receptive field- pain beyond the area of peripheral nerve supply. After-stimulus unpleasant quality of pain- burning, throbbing, tingling, numbness, etc.
Chronicity- pain is no longer coupled to tissue injury, a sensory “illusion”.


Idiopathic CS Syndromes “Family”• Fibromyalgia syndromes
(FMS)• Chronic headaches• Irritable bowel syndrome
(IBS), RAP• Chronic fatigue
syndromes (CFS)• Orthostatic Intolerance
(OI), POTS• Myofascial pain
syndromes (MPS)• Posttraumatic stress
disorder (PTSD)• Depression, anxiety• Neuropathic, central pain• Noncardiac chest pain
• Restless legs syndromes (RLS)
• Periodic limb movement disorder (PLMD)
• Temporomandibular disorder (TMD)
• Multiple chemical sensitivity (MCS) ?
• Female urethral syndromes (FUS)
• Interstitial cystitis• Primary dysmenorrhea
(PD), pelvic pain, vulvodynia
• Sleep disorders
Daniel Lacey, MD

CSS Symptoms That Overlap
The neurologist sees chronic headache; the gastroenterologist sees IBS; the dentist sees TMD; the cardiologist sees chest pain/syncope; the rheumatologist sees fibromyalgia; the gynecologist sees pelvic pain; the orthopod sees…etc…..

Headaches in Children
Acute- trauma, infectionAcute, recurrent- migraine or equivalents in
younger childrenChronic, progressive- increased intracranial
pressure, degenerative disease, vascular, hydrocephalus
Chronic, stable- tension, medication overuse, new daily persistent headaches (NDPH), transformed migraine, pseudotumor cerebri

Teens with Chronic Headaches
Often not diagnosed and treated for many years!Are at a significantly greater risk for suicideTeens who have migraines with aura are 6 times more likely to
have a high suicide risk than those without aura.Are 3.5 times more likely to have a psychiatric disorder than
those without migraineHave at least a 50% chance of having at least one psychiatric
disorder if their headaches are daily. Abut 20% have major depression and/or panic and anxiety disorders.
Have a higher frequency of previous physical and/or sexual abuse (30%)

CDH/Migraine TreatmentsUrgency and aggressiveness depends on whether
child is going to school, participating in normal activities of daily living.
May need inpatient admission for IV meds if has been in “status migrainosus”, to ED many times. Unfortunately, a common occurrence.
Often a mixture of acute, abortive and preventive medications and non-medical treatments is the most successful regimen.
Long-term headache freedom rate: 30%, many CDH patients return to being episodic migraneurs

CDH/Migraine Treatment (2)
1. Amitriptyline, start 0.5-1mg/kg @ bedtime
(25mg maximum), increase to 1-3mg/kg
2. Topiramate, start 0.5mg/kg @ bedtime
(25mg maximum), increase to 50-100mg BID
3. Propranolol, start 1mg/kg divided BID
4. Consider valproate, tizanidine, gabapentin,
clonidine, venlafaxine, BOTOX, fluoxetine, ? opioids
5. “Alternatives”, riboflavin, Coenzyme Q10,
magnesium, butterbur, massage, Vitamin D
6. Biobehavioral, relaxation, imaging, SLEEP!


The current status of Recurrent (RAP)Abdominal Pain

Definition of RAP • Derives from the seminal description by Apley of
children between the ages of 4 and 16 years that persists for more than 3 months and affects normal activity.
• RAP is not a diagnosis !!!!! • It may be the predominant clinical manifestation
of a large number of precisely defined organic disorders, but in the majority of cases, RAP is due to a ‘functional’ bowel disorder. Often see IBS in patients with inflammatory bowel diseases.

Prognosis of RAP in Children
• Pain resolves completely in 30% to 50% of patients by 2 to 6 weeks after diagnosis.
• This suggests that child and parent accept reassurance that the pain is not organic and that environmental modification is effective.
• Nevertheless, more long-term studies suggest that 30% to 50% of children who have functional abdominal pain in childhood experience pain as adults, especially IBS.
• Thirty percent of patients who have functional abdominal pain develop other chronic complaints as adults.

Treatment of RAP
Reassure the family and patient that we believe the pain is real and will treat accordingly
Reassure that the appropriate medical evaluations have been done, we will not keep “fishing” or “shot- gunning” unless symptoms change
Behavioral- relaxation, hypnosis, encourage “well” behaviors, ignore and discourage “sick” behaviors (PADS), biofeedback
Medication- tricyclics, pregabalin; specific GI meds +/-

Pediatric Low Back Pain40% of teens report low back pain (LBP)LBP plus other pain 46%LBP plus whole body pain 9%Boys more common if LBP onlyGirls more common if LBP plus other
painFunction better if only have LBP, worse
if have LBP plus other pain, worst if have LBP plus widespread pain
Pellise F, Balague F, Rajmil L, Cedraschi C, Aguirre M, Fontacha CG. Prevalence of Low Back Pain and its Effect on Health-Related Quality of Life in Adolescents. Arch Pediatr Adolesc Med. 2009;163(1):65-71

Red Flags Young age (particularly younger than
4 years) Fever Weight loss Severe or constant pain Nocturnal pain Progression over the course of time Hx of acute or repetitive trauma Hx of malignancy Bowel or bladder dysfunction Interference with activity (self
limitation)

Chronic Pediatric Chest Pain
• Musculoskeletal 86%• Infectious (costochondritis) 9%• Asthma 3%• Gastrointestinal 0.6%• Cardiac 0.6%- more likely if occurs during
exertion
Rx- Effexor, NSAIDs
Reddy SRV, Singh HR. Chest Pain in Children and Adolescents. Pediatrics in Review. 2010;33(1)e1-e9

Neuropathic Pain is Different from Muscle/skeletal Pain
Neuropathic Pain Muscle/Skeletal Pain
Chronic pain (months/years) Acute pain (hours or days)
Caused by injury or disease to nerves Caused by injury or inflammation that affects both the muscles and joints
Mild to excruciating pain that can last indefinitely
Moderate to severe pain that disappears when the injury heals
Causes extreme sensitivity to touch –simply wearing light clothing is
painful
Causes sore, achy muscles
Sufferers can become depressed or socially withdrawn because they see no relief in sight and may experience
sleep problems
Sufferers can become anxious and distressed but optimistic about relief
from pain
Wall PD. Textbook of Pain. 4th ed; 1999; Jude EB. Clin in Pod Med and Surg.1999;16:81-97; Price SA. Pathophysiology: Clinical Concepts of Disease Processes. 5th ed; 1997: Goldman L. Cecil Textbook of Medicine. 21st ed; 2000

Complex Regional Pain Syndrome
• COMPLEX- A combination of neuropathic and sensory/neurovascular abnormalities required
• REGIONAL- Often involves one or more limbs, generalizes distally, contralateral spread is also possible
• PAIN- Can be spontaneous and/or provoked, not dermatomal in distribution

CRPS Symptoms Spontaneous burning or stinging pain (81%). Electrical sensations or shooting pain Allodynia, hyperalgesia, hyperesthesia Vasomotor autonomic disturbance (87%
color, 79% temperature). Sudomotor symptoms : sweating asymmetry
(53%). Trophic changes (altered skin, nail, or hair
growth patterns) Notable limb edema (80%) and associated
stiffness. Differences often present between “warm”
and “cold” Often a prior and/or family history of
migraine

Pediatric CRPS 90% in girls, mean age 11.8 years Lower limbs 85%, especially the foot (75% of all cases)
whereas in adults, uppers twice as frequent Frequently initiated by minor trauma, pain can occur
immediately or weeks to months after injury Mean time to diagnosis 13.6 weeks 70% required adjuvant medication (amitriptyline,
gabapentin) Early mobilization and physical therapy are the mainstays
of treatment, kids respond better to non-invasive treatment Most recover completely, 40% need inpatient stay, 20%
relapse
Low AK, Ward K, Wines AP. Pediatric Complex Regional Pain Syndrome. J Ped Ortho. 2007;27(5):567-572
Wilder TR. Management of Pediatric patients with Complex Regional Pain Syndrome. Clinical J Pain. 2006;22(5):443-448

Screening for Neuropathic Pain
Give one point each, if yes, for: 1. Pain feels like pins and needles 2. Pain feels hot and burning 3. Pain feels numb 4. Pain is like an electric shock 5. Pain is worse if touched by clothes or
bed linen Pain is limited to joints (subtract one
point if yes)If score is three or higher, pain is likely
neuropathic

CRPS FACTS
When not caught early, CRPS can be progressive (70% of cases)
NEED to find single diagnostic test, not yetEarly recognition through educationEarly diagnosis equals BETTER prognosis Need more effective treatments for CRPSResearch is desperately needed In 40-60% of patients, pain is unrelieved
Cherny NI. The treatment of neuropathic pain: From hubris to humility. Pain. 2007;132:225-226

EARLY DIAGNOSIS CRITICAL
Early diagnosis ( <3 mo.) with PROPER treatment, success rate is highest, the best prognosis
If left untreated, can lead to lifetime of severe, intractable, chronic pain
First 3-6 months after onset: 80-90% recovery rate6 months to 2 years 70-80%, after 2 years: 20%
PREVENT PADS!!!

BRAIN
PNS
SPINALCORD

Treatment Goals for Chronic Pain
Minimize physical pain and
discomfort
Alleviate anxiety
Prevent potentially deleterious
physiologic responses due to
pain
PREVENT PADS!!!!!

TREATMENT MODALITIES
EDUCATIONPHARMACOLOGICALPHYSICALBEHAVIORALPSYCHOLOGICALCOMPLEMENTARY THERAPIES

EDUCATION Reassurance: pain is real and biological Reason for pain: dysregulation in pain
neural signaling system (ascending/descending)
Reason for failure of medical tests: looking in the wrong places
Avoid mind-body split Review how other factors influence pain:
anxiety, depression, beliefs, attention, memory; hypervigilance, catastrophizing

PHYSICAL THERAPY
Especially for patients who have chronic musculoskeletal pain complex regional pain syndrome become deconditioned due to inactivity
Requires specific expertise by PT Exercise has specific benefits related to muscle
strengthening/functioning & posture, and generalized benefits related to improved body image, body mechanics, somatic self-efficacy, sleep, and mood

PSYCHOLOGICAL INTERVENTIONS
Cognitive-Behavioral Therapy (CBT) Social Skills Training Psychotherapy: child or family or both Academic interventions Treatment aimed at PTSD or unresolved
grief or trauma

FAMILY THERAPY
To observe and alter family contributors to pain perception
To participate in development & implementation of behavioral plan (e.g. how to get child to go to school)
To address family stress& problems
To improve family communication To provide support& improve
family coping

CAM and OTHER PAIN TREATMENTS
Acupuncture Distraction Muscle Relaxation/Breathing Meditation Hypnotherapy Iyengar Yoga Biofeedback Massage Therapy Art Therapy

PAIN-ASSOCIATED DISABILITY SYNDROME
“PADS”
DOWNWARD SPIRAL OF INCREASING
SYMPTOMS AND DISABILITY

Pain-Associated Disability Syndrome (PADS)
Described in 1998 as “a spiral of increasing pain-related disruption of function” in children
Seen in all types of pediatric chronic pain disorders, head, visceral, musculoskeletal, etc.
Preventing or addressing this should be the primary goal of early pediatric pain management
Zeltzer LK, Tsao JC, Bursch B, Myers CD. Introduction to the Special Issue on Pain: From Pain to Pain-Associated Disability Syndrome. J Pediatr Psychol. 2006;31(7):661-666

PADS Prevention Must assess functional limitations at home,
school, etc., not just focus on pain as the only dimension
Sole treatment focus on medications often does not result in functional restoration
Best treatment program is multimodal with emphasis on non-medical therapies, including cognitive behavioral
Functional improvement always precedes pain reduction!!

Chronic Pain Treatment Impediments
CatastrophizationHypervigilanceFocusing only on pain severity (0-10) and
reductionFocusing only on mediation treatmentNot focusing on function!!!Not emphasizing that restoration of normal
function almost always precedes pain reduction, not the other way round
For some patients, accepting that they may always have pain will actually result in less pain (ACT)

Chronic Pain Service at Dayton Children’s
Consult team includes Dr. Lacey, Cindy Brown MSN, RN, CNS, Rehab therapist, Massage therapist by referral, Psychologist, Dietician. A pharmacist is consulted by the team as needed.
Goal-To use a coordinated team approach to reduce pain(NOT pain free) and to restore activities of daily living.
Available by referral through the Neurology Clinic

Treatment Goals
Medications alone will not relieve the pain.Strategies that include exercise(up and out of
bed ambulating on a regular basis), massage, discussing emotions, improving sleep, using relaxation and deep breathing techniques/guided imaging and distraction are utilized daily.

Important Do’s for our pain patients
Do not re enforce the “sick role.”
Be empathetic but firm regarding exercise, activities of daily living.
Do not use pain scales to “rate” pain(they were developed for acute pain), instead focus on function and daily activities.

Follow-up
Patients continue to follow with Dr. Lacey and the chronic pain team on an outpatient basis. Other alternative therapies such as hydrotherapy, acupuncture/acupressure, hypnosis may be initiated.
Patients need to also follow a regular schedule at home. School attendance may be limited during acute exacerbations but school/activity involvement is essential.
Ongoing psychological counseling which focuses on managing pain is crucial.

Follow-up
Working with parents and other caregivers on an outpatient basis is an important part of the plan-parents need to be coaches and not enablers.
Goal to successful treatment is outpatient care; repeat admissions should be limited.
Key is to focus on multi-modal interventions and again, to attend school/work and activities as much as possible.

What’s new in 2014-15
“Start Talking” Opioid Consent Requirement and the use of OARRS.
Support group for patients with chronic pain
Education for the community providers and schools regarding chronic pain

Questions
Contact-
Cindy Brown MSN, RN, [email protected] X8934
Thanks for your interest in pain management!