Embed Size (px)
Citation preview

4 Hospital Physician Board Review Manual www.turner-white.com
OrthOpaedic Surgery BOard review Manual
Statement of editorial PurPoSe
The Hospital Physician Orthopaedic Surgery Board Review Manual is a study guide for trainees and practicing physicians preparing for board examinations in orthopaedic surgery. Each manual reviews a topic essential to the current practice of orthopaedic surgery.
PuBliSHinG Staff
PRESIDENT, GRouP PuBLISHERBruce M. White
SENIoR EDIToRRobert Litchkofski
ExEcuTIvE vIcE PRESIDENTBarbara T. White
ExEcuTIvE DIREcToR of oPERaTIoNS
Jean M. Gaul
NoTE fRoM THE PuBLISHER:This publication has been developed without involvement of or review by the American Board of Orthopaedic Surgery.
Pediatric Cervical Spine InstabilityEditor:Pedro K. Beredjiklian, MDAssociate Professor of Orthopaedic Surgery, Thomas Jefferson University Hospital, Chief, Division of Hand Surgery, The Rothman Institute, Philadelphia, PA
Harish S. Hosalkar MD, MBMS (Orth), FCPS (Orth),DN B (Orth)Attending Orthopedic Surgeon, Clinical Associate Professor of Orthopedic Surgery, School of Medicine, University of California–San Diego; Co-Director of International Center for Pediatric and Adolescent Hip Disorders, Director Hip Research Program, Pediatric Hip and Trauma Specialist, AONA Faculty for Pediatric Orthopedic Trauma, Rady Children’s Hospital, University of California–San Diego
Denis S. Drummond, MDAttending Surgeon and Emeritus Chief, Department of OrthopaedicSurgery, Children’s Hospital of Philadelphia; Professor of Orthopaedic Surgery, University of Pennsylvania School of Medicine, Philadelphia, PA
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5 Anatomy and Biomechanics. . . . . . . . . . . . . . . . .5 Evaluation of Cervical Instability. . . . . . . . . . . . .7 Causes of Cervical Instability. . . . . . . . . . . . . . . .9 Management of Cervical Spine Instability . . . . .15 Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .18 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . .18
Table of Contents

P e d i a t r i c C e r v i c a l S p i n e I n s t a b i l i t y
www.turner-white.com Orthopaedic Surgery Volume 8, Part 1 5
ORTHOPAEDIC SuRgERy BOARD REvIEw MANuAl
ORTPediatric Cervical Spine Instability
Harish S. Hosalkar MD, MBMS (Orth), FCPS (Orth), DN B (Orth), and Denis S. Drummond, MD
introduCtion
Most pediatric spine injuries occur in the cervi-cal spine, the majority of which involve the upper cervical spine. Although cervical spine trauma accounts for only about 1% of traumatic injuries in children,1,2
it can be life-threatening. Knowledge of the unique anatomy and biomechanics of the pe-diatric cervical spine forms the basis for accurate diagnosis and appropriate treatment.
anatomY and BiomeCHaniCS
The pediatric cervical spine differs significantly from that of adults, and many of these unique features un-favorably affect spinal stability. The combination of an immature skeleton, ligamentous laxity, and a relatively large head size in children has a detrimental effect on cervical spine stability. Differences are notable in terms of injury as well: the effects of any cervical injury are magnified, particularly in the upper cervical spine, where the relatively large head of younger children increases acceleration forces applied to the spine.
anatOMy
The cervical spine in children can be divided into the upper cervical spine, which extends from the
occiput to the C2–C3 disk space, and the lower cervical spine, which extends caudally from the same disk space. The embryology, development, and anatomy of the upper cervical spine differ from the lower cervical spine, which develops similarly to the rest of the spine. Compared with the lower cervical spine, the upper cervical spine has a greater dependence on the ligament complexes to provide stability. Also, the relatively larger head size of younger children negatively impacts stability and response to injury. This combination of factors creates a setting for ligament failure in the proximal cervical spine when large mechanical loads occur in high-impact injury. In addition, the dynamic sta-bility of the pediatric cervical spine is challenged by weaker support from adjacent muscles that are smaller and less developed than in the adolescent or adult.3
The anatomy of the pediatric cervical spine is constantly changing because of the growth, matu-ration, and ongoing ossification of vertebral bodies. The presence of the polar growth centers adjacent to the vertebral end plates and the many synchon-droses of the immature skeleton determine the sites where vertebral injury is likely to occur. For example, the basilar synchondrosis caudal to the base of the dens is a common site of fracture displacement
copyright 2011, Turner White communications, Inc., Strafford avenue, Suite 220, Wayne, Pa 19087-3391, www.turner-white.com. all rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, mechanical, electronic, photocopying, recording, or otherwise, without the prior written permission of Turner White communications. The preparation and distribution of this publication are supported by spon-sorship subject to written agreements that stipulate and ensure the editorial independence of Turner White communications. Turner White communications retains full control over the design and production of all published materials, including selection of topics and preparation of editorial content. The authors are solely responsible for substantive content. Statements expressed reflect the views of the authors and not necessarily the opinions or policies of Turner White communications. Turner White communications accepts no responsibility for statements made by authors and will not be liable for any errors of omission or inaccuracies. Information contained within this publication should not be used as a substitute for clinical judgment.

P e d i a t r i c C e r v i c a l S p i n e I n s t a b i l i t y
6 Hospital Physician Board Review Manual www.turner-white.com
of the odontoid process in younger children. The facets and articulations of the spine of the younger child are shallow, making them less resistant to high loads and more susceptible to failure and instability. In addition to affecting cervical spine stability, the immature and changing anatomy complicates radio-graphic evaluation of children with traumatic injury or congenital vertebral anomalies.
BiOMechanicS
The comparative ligamentous laxity in children has an adverse effect on stability of facet joints as well as on atlanto-occipital and atlanto-axial joint competency. Furthermore, the facet joints and con-dylar development of the atlanto-occipital articulation are relatively shallow in children. Accordingly, when acceleration and deceleration forces occur, children are more vulnerable to injury primarily to the spinal column and, secondarily, to the spinal cord, which
is at risk for serious traction injury. Even when the spine appears normal on plain radiographs, with failure of supporting soft tissues the stability of the disks, facet joints, and synchondroses may fail.4 Al-though the pediatric spine can tolerate subluxation and distraction, the pediatric spinal cord cannot. When stretched beyond tolerance, myelopathy en-sues. This phenomenon is termed spinal cord injury without radiographic abnormality (SCIWORA).
definitiOn Of inStaBility
The parameters commonly used to define normal spine stability are slightly greater for children than for adults. Further, an acceptable increase of any measurement that defines stability is dependent not only on the measurement itself but also on the space available for the spinal cord. The measurement method and established normal value as observed on lateral flexion–extension radiographs follow:
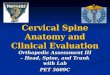
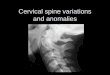
• Atlanto-occipital motion. Instability in transla-tion is best observed on the lateral extension view. Of the 3 commonly used parameters, the Powers ratio (figure 1) and Harris technique best measure horizontal translation, whereas the Kauffmann method measures vertical dis-placement (figure 2). The upper limit of normal for horizontal translation in children is 2 mm (versus 1 mm in adults); vertical displacement should not exceed 5 mm in both adults and children (> 5 mm is defined as atlanto-occipital dislocation [AOD]).
• Atlanto-axial motion. Atlanto-axial instability is best observed in flexion on the lateral radio-graph, and the atlanto-dens interval is accepted as the standard method of measurement (see Figure 2). The accepted upper limit of nor-mal for this index is usually 5 mm in children (versus 4 mm in adults).5
figure 1. Use of Power’s ratio to determine atlanto-occipital sub-luxation. In patients without subluxation, BC ≤ AO ≤ 1. A = an-terior arch of the atlas; B = basion; C = posterior arch of atlas; O = opisthion. (Adapted with permission from Drummond DS. Pediatric cervical instability: diagnosis and treatment concepts. Semin Spine Surg 1996:8:296.)

P e d i a t r i c C e r v i c a l S p i n e I n s t a b i l i t y
www.turner-white.com Orthopaedic Surgery Volume 8, Part 1 7
• Subaxial motion. There is no accepted norm for subaxial translation to define instability in chil-dren, although some consider more than 2 mm as abnormal (versus 3.5 mm in adults).5 Subaxial translation is best appreciated radio-graphically on the lateral flexion view. Again, the available spinal cord space is an important con-sideration when evaluating children who have more than 2 mm of subaxial translation.
eValuation of CerViCal inStaBilitY
In the acute trauma situation, great care must be taken during evaluation, particularly in cases of head injury or with signs of neurologic impairment. With the alert and cooperative patient who shows no signs of spinal cord injury, stability can be confirmed with dynamic lateral flexion–extension radiography. For unconscious or obtunded patients, flexion– extension examination is unsafe. Neck immobiliza-tion by a firm fitted collar is critical, and computed
tomography (CT) or magnetic resonance imaging (MRI) is used to evaluate the stability status.
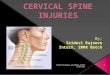
Instability is frequently overdiagnosed in children younger than age 3 years because the incompletely ossified vertebrae may be perceived as translation or pseudosubluxation. table 1 lists the normal ver-tebral observations unique to the immature cervical spine that can be mistaken for spinal pathology. By applying the spinolaminar line, the correct diagnosis of stability can be appreciated (figure 3).
iMMOBiliZatiOn and phySical eXaMinatiOn
Patients with cervical spine trauma or suspected spinal cord injury should be immobilized in the neu-tral position to prevent possible further neurologic damage. Younger children (age < 8 years) have disproportionately large heads compared with the
table 1. Unique Features of the Normal Pediatric Cervical Spine
general features involving the entire cervical spineSecondary centers of ossification of the spinous processes may
mimic fracturesRounding of anterior vertebral body may give the appearance of a
wedge compression fractureHorizontal facets and ligamentous laxity allow greater intersegment
mobilityCervical lordosis is decreasedWider prevertebral soft tissues that may mimic swelling
features of specific anatomic levelsC1 multiple ossification centers may mimic fracturesAbsent ossification of anterior arch of C1 may be mistaken for
C1–C2 instabilityC1–C2 atlanto-dens interval may be up to 4.5 mmC2 posterior angulation of odontoid (4% of children) may mimic fractureOssiculum terminale may mimic fractureBasilar synchondrosis may mimic fractureC2–C3 and C3–C4 pseudosubluxation may be mistaken for instability
Adapted from Drummond DS, Hosalkar HS. Instabilidade da coluna cervicalem criancas. In: Vialle LR, editor. Clinica ortopedica: a coluna da criancae do adolescente. Rio de Janeiro, Brazil: Guanabara Koogan; 2005:27–44.
figure 2. Schematic illustration of the Kaufman method, which speci-fies that the width of the atlanto-occipital junction at all points (large arrows) should not exceed 5 mm. This method is useful for determin-ing vertical displacement on flexion–extension films. The atlas-dens interval is indicated by the small arrow. (Adapted with permission from Hosalkar HS, Cain EL, Horn D, et al. Traumatic atlanto-occipital dislocation in children. J Bone Joint Surg Am 2005;87:2482.)

P e d i a t r i c C e r v i c a l S p i n e I n s t a b i l i t y
8 Hospital Physician Board Review Manual www.turner-white.com
torso, and improper positioning onto a spinal im-mobilization board may place the child’s neck into flexion. A neutral position can be achieved by plac-ing blankets underneath the shoulders and trunk or by using a half-spine board with occipital recess. Current approaches to immobilizing the pediatric cervical spine include using a half-spine board with occipital recess (with the external auditory meatus in line with the shoulder to avoid placing the neck into kyphosis) or a rigid collar and, possibly, placing tape across the torso in patients without respiratory problems.6
After the patient has been safely immobilized and Advanced Trauma Life Support measures taken, a detailed physical examination should be conducted. Findings that correlate with cervical spine injury in-clude head injury, neurologic deficit, torticollis, neck guarding, tenderness, palpable step-off between contiguous spinous processes, and multiple trau-ma. Skin abrasions over the neck area (shoulder-
belt sign) may suggest underlying cervical spine or vertebral artery injury. Serial assessments may be necessary in children who have difficulty cooperat-ing with the physical examination.
radiOgraphic eXaMinatiOn fOr StaBility
With a high index of suspicion of a cervical spine injury, an anteroposterior (AP), lateral, and open-mouth odontoid view of the cervical spine should be obtained. In conscious and alert patients, voluntary flexion and extension views of the cervical spine may be performed to assess spine stability, provid-ed that no abnormalities are seen on static films.
CT may serve as an adjunct to the radiographic evaluation of the bony cervical spine to reduce the risk of missing a fracture on plain radiographic evaluation alone. Helical CT is recommended in high-risk older children or adults who have sustained multisystem trauma after significant blunt injuries. Viccellio et al,7
in a prospective multicenter study of cervical spine injury in 3065 patients younger than 18 years, found that advanced cervical spine imaging may not be necessary in adolescents (age > 9 years) in the ab-sence of high-risk criteria that include: midline cervical tenderness, altered level of alertness, evidence of intoxication, neurologic abnormality, and presence of painful distracting injury.
In unconscious patients, plain radiographs should be obtained but advanced imaging may be neces-sary to reduce the incidence of missed fractures. It is critical to note that lateral flexion–extension radiogra-phy is unsafe in the unconscious or very young child (age < 3 years). The relative ligamentous laxity in children may allow the cervical spine to deform more than the spinal cord can tolerate, and SCIWORA may occur. The flexion–extension maneuvers can also potentially lead to spontaneous reduction, and significant pathology could be missed. MRI is recom-mended in this situation. MRI can be highly effective
figure 3. Four-line analysis of cervical spine radiographs: 1 = tips of the spinous processes, 2 = spinolaminar line, 3 = posteri-or margins, and 4 = anterior margins of the vertebral bodies. All lines should follow a smooth, even contour. (Adapted with per-mission from Copley LA, Dormans JP. Cervical spine disorders in infants and children. J Am Acad Orthop Surg 1998;6:207.)

P e d i a t r i c C e r v i c a l S p i n e I n s t a b i l i t y
www.turner-white.com Orthopaedic Surgery Volume 8, Part 1 9
in ruling out injury to the cervical spine in patients who are obtunded and intubated, as well as in alert children with persistent pain or neurologic symptoms without radiographic abnormalities.
CauSeS of CerViCal inStaBilitY
The causes of pediatric cervical instability are classified in table 2. The following discussion
focuses on some of the most common conditions leading to instability.
trauMatic cauSeS
table 3 outlines common cervical spine injuries in children. Children younger than 8 years of age usually have upper cervical injuries, whereas older children, whose biomechanics more closely resemble those of adults, are prone to lower cervical injuries. Neonatal high cervical spinal cord injury may result from rota-tional forceps delivery exerting torsional forces that can cause quadriparesis, areflexia, and diaphragmatic pa-ralysis. Other neonatal risk factors include breech posi-tion, which can place traction forces on the spine and cause injury, typically at the cervicothoracic junction.6
Cervical spine trauma in children is more likely to be associated with concomitant head trauma,
table 3. Common Types of Pediatric Cervical Spine Trauma
atlanto-occipital traumaAtlanto-occipital dislocationJefferson’s fractureOdontoid fracture
atlanto-axial traumaHangman’s fractureTraumatic spondylolisthesisAtlanto-axial subluxationAtlanto-axial rotational dislocation
Subaxial traumaTraumatic subluxation with or without fractureTraumatic fracture dislocationsAnterior/ posterior/ lateral element fractures in isolation or
combination
Spinal cord injury without radiographic abnormality(SciwOra)
Adapted from Drummond DS, Hosalkar HS. Instabilidade da coluna cervicalem criancas. In: Vialle LR, editor. Clinica ortopedica: a coluna da crianca e do adolescente. Rio de Janeiro, Brazil: Guanabara Koogan; 2005:27–44.
table 2. Causes and Subtypes of Cervical Instability
congenital causesVertebral (bony anomalies)
Cranio-occipital defects (occipital vertebrae, basilar impression, occipital dysplasias, condylar hypoplasia, occipitalized atlas)
Atlanto-axial defects (aplasia of the atlas arch, aplasia of odontoid process)
Subaxial anomalies (failure of segmentation and/or fusion, spina bifida, spondylolisthesis)
LigamentousOsteochondrodysplasias (achondroplasia, spondyloepiphyseal
dysplasia)Storage disorders (mucopolysaccharidoses)Combined anomalies (at birth as an element of somatogenic
aberration)Syndromic disorders/developmental dysplasias
Down syndromeKlippel-Feil syndrome22q11.2 deletion syndromeMarfan syndromeEhlers-Danlos syndrome
acquired causesTrauma (Hangman fracture, odontoid fracture, atlanto-occipital dislo-
cation)Iatrogenic (cervical laminectomy)Infection (pyogenic/granulomatous)Tumor (osteoid osteoma, osteoblastoma, aneurysmal bone cyst,
Langerhans cell histiocytosis)Inflammatory conditions (juvenile rheumatoid arthritis)
Adapted from Drummond DS, Hosalkar HS. Instabilidade da coluna cervicalem criancas. In: Vialle LR, editor. Clinica ortopedica: a coluna da criancae do adolescente. Rio de Janeiro, Brazil: Guanabara Koogan; 2005:27–44.

P e d i a t r i c C e r v i c a l S p i n e I n s t a b i l i t y
10 Hospital Physician Board Review Manual www.turner-white.com
a factor contributing to the higher mortality rates in children than in adults. Mortality is higher in patients with upper versus lower cervical spine injuries and is highest in patients with AOD. Chil-dren also more often present with cervical injuries that are ligamentous in nature, and they are more prone to SCIWORA.8
atlanto-Occipital traumaatlanto-occipital dislocation. AOD is a rare but
frequently fatal injury; however, timely and aggres-sive management may lead to survival.9 In a study of pediatric patients with AOD, those who could moan or phonate spontaneously and/or on demand at the time of intubation regained considerable neurologic function.9
This finding is thought to indi-cate incomplete brainstem injury with preservation of neurologic structures that support spontaneous ventilation. In these cases, it is important to stabilize the spine with a halo-vest, establish an airway, and administer intravenous steroids using the spinal cord injury protocol to control spinal cord edema.
Jefferson’s fracture. Atlas fractures are also rare in children and are best observed on CT axial images. When an atlas fracture does occur, only 1 fracture line may be apparent opposite to a plastically deformed synchondrosis. The finding of lateral masses more than 7 mm wide suggests transverse ligament rupture; thus halo-vest immo-bilization is urgently required. If the case is more stable (widening < 6 mm), an orthotic collar may suffice.
Odontoid fracture. Dens fractures are the most common instability-associated fractures of the pe-diatric cervical spine. These fractures occur most frequently in children younger than age 7 years through the basilar synchondrosis situated just dis-tal to the base of the dens. Hosalkar et al10 recently proposed a new classification system for pediatric
odontoid fractures based on location in the dens and degree of displacement. Of the odontoid fracture patterns observed, the type in which the fracture ran through the synchondrosis was most likely to be stable on reduction. In these cases, the anterior periosteum is usually partially intact and thus provides some stability and a hinge for reduction. A gentle reduction maneuver in exten-sion against the anterior periosteal hinge followed by immobilization in a halo-vest usually yields a positive result and healing.
atlanto-axial trauma: hangman’s fractureHangman’s fracture with spondylolisthesis at
C2 is rare in children but should remain in the differential diagnosis following significant trauma, particularly trauma associated with seat belt injury. This fracture is best diagnosed on CT scans with sagittal and frontal formatting.
SciwOra
SCIWORA is a diagnosis that must be consid-ered in all cases of pediatric trauma. Unexplained neurologic signs, major head injury, and seat belt injuries are some of the related pathologies that should alert the physician to this possibility. MRI can confirm this injury. SCIWORA can be man-aged by immobilizing the patient in a halo-vest, stabilizing systemic problems, and administering systemic steroids using the spinal cord injury pro-tocol. Spinal stability through the injured segment should be evaluated.
cOngenital cauSeS
The congenital causes of instability are complex. table 4 lists anomalies classified by the region involved. These conditions are likely the product of a deficiency in embryogenesis that hinders spinal stability. In addition, reduction of the space

P e d i a t r i c C e r v i c a l S p i n e I n s t a b i l i t y
www.turner-white.com Orthopaedic Surgery Volume 8, Part 1 11
available for the spinal cord—caused by associ-ated spinal stenosis at the unstable segments or encroachment on the space by an intrusive mass—can compound the instability. In Chiari type 1 malformation, for example, this encroachment at the brainstem level occurs as a caudal hernia-tion of the cerebellar tonsils through the foramen magnum, which can cause brainstem-centered neurologic deficiency. Chiari type 1 malformation can also interrupt the normal flow of cerebrospinal fluid, leading to hydromyelia and scoliosis. These conditions can compound the associated instabil-ity that is likely in these cases.
Congenital anomalies of the cervical spine are more often multiple than singular. Therefore, if one anomaly is observed, the physician should search for other anomalies, not only in the cervical spine but in thoracic and lumbar levels as well. In such cases, congenital problems may also exist in other organ systems; thus, collaboration with other pe-diatric specialists for a thorough workup is often needed.5,11
canal encroachmentNarrowing of the bony spinal canal (spinal cord
≤ 13 mm) has been historically described as canal stenosis.12–15
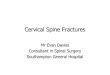
However, this term is inadequate to include all pathologies that decrease available spinal cord space and therefore the concept of canal encroachment is used. Encroachment of the spinal canal or spinal cord may be caused by static and/or dynamic factors (figure 4).16
Static encroachment includes focal bony nar-rowing of the spinal canal (stenosis), a space- occupying mass such as a herniation of the cer-ebellar tonsils with the Chiari type 1 malforma-tion, or odontoid intrusion through the foramen magnum with basilar invagination. Dynamic en-croachment occurs when segmental translational
instability encroaches on available space for the spinal cord or brainstem. Either condition alone can increase risk for neurologic injury; however, together these conditions are associated with a greater risk.16
Finally, with time and degenera-tive changes (by approximately the fourth to fifth decade), canal encroachment may result in a fur-ther neurologic deterioration. In complex patholo-gies of the cervical spine, the concept of canal encroachment enables physicians to better evalu-
table 4. Congenital Anomalies of the Upper Cervical Spine
Bony anomalies of the occipitocervical regionMalformations of occipital bone
Occipital vertebraeBasilar impressionOccipital dysplasiaCondylar hypoplasia
Malformations of atlasOccipitalization of atlasAplasia of the atlas archClefts in the atlas arch
Malformations of axisPersistent os terminaleOs odontoideumDysphasia, hypoplasia, and aplasia of densSpina bifida of the axisFusion of cervical vertebrae 2–3
Bony anomalies of the subaxial regionPrimary failure of embryonic segmentation (Klippel-Feil syndrome
and its variants)Failures of fusionSpina bifidaSpondylolisthesisneurologic anomaliesChiari type 1 malformationSyringomyeliaMeningomyeloceleNeurofibromatosis
Adapted from Drummond DS, Hosalkar HS. Instabilidade da coluna cervical em criancas. In: Vialle LR, editor. Clinica ortopedica: a colu-na da crianca e do adolescente. Rio de Janeiro, Brazil: Guanabara Koogan; 2005:27–44.

P e d i a t r i c C e r v i c a l S p i n e I n s t a b i l i t y
12 Hospital Physician Board Review Manual www.turner-white.com
ate the issues, to establish and explain a prog-nosis, and to develop a management plan. This concept is especially helpful for surgical planning, including decompression and arthrodesis, par-ticularly when static and dynamic encroachments occur simultaneously.
Occipitalization of the atlasOccipitalization is defined as partial or complete
congenital fusion of the occiput and atlas.17 The re-
ported prevalence of occipitalization in the general (adult and pediatric) population ranges from 0.08%
to 2.76%, with males and females equally affected.16
Occipitalization ranges from complete osseous fusion of the atlas and occiput to a partial osseous bridge uniting a focal area of the bones. The clinical spec-trum of occipitalization varies from an asymptomatic condition to a condition causing neck pain and stiff-ness with varying degrees of neurologic deficit.
Pediatric atlas occipitalization is classified into zones based on whether segmentation failure occurs in the anterior arch, the lateral masses, or the posterior arch of the atlas (figure 5).16
Zone 1 occipitalization represents fusion involving the anterior arch; zone 2 occipitalization corre-sponds to fusion involving the lateral masses; and zone 3 occipitalization represents fusion involving the posterior arch. Fusions involving more than 1 atlas zone are classified as a combination of zones. Within each zone, occipitalization can be partial or complete and unilateral or bilateral.
figure 4. (a) Schematic illustration showing the dynamic, static, and combined factors involved in canal encroachment. Some causative factors are outlined. (B) McGregor’s line extends from the superior surface and posterior edge of the hard palate to the most caudal point of the occiput. If the tip of the odon-toid lies more than 4.5 mm above McGregor’s line, this finding is consistent with basilar impression. (Courtesy of Harish Ho-salkar, MD.)
figure 5. The 3 zones of occipitalization of the atlas vertebra. Z1 = anterior arch; Z2 = lateral mass; Z3 = posterior arch. (Adapt-ed with permission from Gholve PA, Hosalkar HS, Ricchetti ET, et al. Occipitalization of the atlas in children. Morphologic clas-sification, associations, and clinical relevance. J Bone Joint Surg Am 2007;89:572.)

P e d i a t r i c C e r v i c a l S p i n e I n s t a b i l i t y
www.turner-white.com Orthopaedic Surgery Volume 8, Part 1 13
The risk of atlanto-axial instability is particularly high in cases of associated congenital C2–C3 fu-sion. Two-dimensional sagittal and coronal refor-matted CT reconstructions and/or MRI can help to establish the diagnosis and allow categorization of occipitalization in 3 zones, each of which may have a different prognostic implication. Patients who are neurologically stable and have high activity level or decreased spinal cord space should undergo careful restoration of the atlanto-axial relationship in extension and occiput-cervical fusion at the ap-propriate level. In cases of neural impairment, de-compression (suboccipital craniectomy and upper cervical laminectomy) with occiput-to-axis arthrod-esis is usually required.
Basilar impressionIn this disorder, the axis is displaced cranially
and the odontoid is displaced through the foramen magnum, resulting in brainstem encroachment. Basilar impression is commonly associated with other anomalies such as atlas occipitalization, hypoplastic atlas, and Klippel-Feil syndrome. Also, basilar impression may accompany systemic disor-ders such as achondroplasia, osteogenesis imper-fecta, and Morquio-Brailsford syndrome. Rheuma-toid arthritis of the upper cervical spine can cause acquired basilar impression.
Most cases of basilar impression remain as-ymptomatic until the second or third decade of life, when patients may present with headache, neck pain, and neurologic compromise. Motor and sen-sory loss are common in symptomatic cases. Cer-ebellar ataxia and lower cranial nerve involvement may occur with dysarthria, dysphagia, nystagmus, and respiratory center compression.
Evaluation should include plain radiographs and MRI. McGregor’s line (see Figure 4), drawn from the upper surface of the posterior edge of the hard
palate to the most caudal point of the occipital curve, is a commonly used radiographic mea-surement. With suspicion of basilar impression on radiography, advanced imaging such as CT is recommended. Treatment may require neurosurgi-cal assistance. Anterior impingement may require fusion in extension or anterior odontoid excision (transoral approach) and stabilization in extension. Posterior impingement may require suboccipital craniectomy and decompression of the posterior ring of C1 and possibly C2, followed by fusion at other appropriate levels.
hemi-atlasCongenital unilateral absence of C1 can present
at birth or later in childhood/adolescence as a sec-ondary torticollis. CT, MRI, and myelography are the best imaging studies to evaluate this anomaly. Magnetic resonance angiography or plain angiog-raphy should be performed prior to surgical inter-vention, because hemi-atlas is commonly associ-ated with vertebral artery anomalies. Management ranges from observation in subtle cases to surgical intervention in the form of decompression (if the spinal cord is inadequate) with posterior fusion, usually between ages 5 and 8 years.
Odontoid anomaliesOdontoid anomalies have a varied spectrum
of presentation from aplasia through different de-grees of hypoplasia. These anomalies may lead to atlanto-axial instability because the odontoid is no longer a stabilizing structure. Os odontoideum, currently thought to be traumatic in origin (missed/unrecognized trauma), has features similar to apla-sia or hypoplasia of odontoid.18 The clinical presen-tation of odontoid anomalies may vary from neck pain and discomfort to frank neural compromise and, occasionally, sudden quadriparesis or death

P e d i a t r i c C e r v i c a l S p i n e I n s t a b i l i t y
14 Hospital Physician Board Review Manual www.turner-white.com
resulting from minor trauma. Surgical stabilization is indicated for patients with neurologic involve-ment, instability on flexion–extension films (super-vised), brainstem or spinal cord encroachment, or persistent neck pain.
Syndromes associated with instabilityThe most common associated syndromes are
Down syndrome, Klippel-Feil syndrome, and 22q11.2 deletion syndrome, all of which can be diagnosed at birth or infancy.
down syndrome. These patients exhibit signifi-cant ligamentous laxity, which in the cervical spine can lead to instability with translation of one spinal segment on the adjacent segment. Typically, insta-bility occurs at the atlanto-occipital joint, the atlanto-axial joint, or both joints. Subaxial instability is less common but also occurs. The degree of translation depends on the severity of ligamentous laxity. The risk for neurologic complications depends on the degree of instability as well as the available space for the spinal cord. The translation at the atlanto- occipital and atlanto-axial joints may be signifi-cant in these patients, and the spinal cord should beevaluated with MRI in cases of cervical spine instability (> 5 mm translation of the atlanto-occipital articulation or > 7 mm translation of the atlanto-axial joint).
Klippel-feil syndrome. Patients with Klippel-Feil syndrome can present with multiple congenital fu-sions of the vertebral bodies of the cervical spine. The classic presentation is a short, stiff neck with a low hairline. Instability can occur between 2 fused segments or at the interface of the fused and more normal vertebrae. Acute neurologic complications occur infrequently in children with this syndrome; more often, weakness and clinical signs have a delayed onset, often in middle age, and neurologic sequelae can occur insidiously and progressively.19
Also, the underlying spinal cord is smaller than normal in this syndrome.20
This finding might explain the insidious loss of neural function with the delayed recognition reported in some cases of Klippel-Feil syndrome and in other congenital cervical spine problems.21
22q11.2 deletion syndrome. This chromo-some abnormality is one of the most common genetic syndromes and encompasses a wide spectrum of abnormalities including cardiac, pal-ate, and immunologic anomalies. In a recent series, upper cervical spine anomalies on plain radiographs were noted in 79 cases of this syndrome.22 At least 1 developmental variation of the occiput or cervical spine is observed in each case; occipital variations include platybasia and basilar impression. Atlas variations involve dysmorphic shape, an open posterior arch, and occipitalization, whereas axis variations occur as dysmorphic dens and dysmorphic spinous pro-cess. A range of cervical vertebral fusions was noted in these patients, most commonly C2–C3. Increased segmental motion as observed by translation in flexion or extension in the cervical spine was noted in more than 50% of patients with this syndrome, and more than one-third of patients have increased segmental motion sug-gestive of instability at multiple levels.
pOSt-Surgical inStaBility
Progressive deformity of the pediatric spine may occur with growth following multiple laminec-tomies. Lonstein et al23
have reported significant, severe, and progressive spinal deformities after laminectomy in as many as 50% of cases in their series. Risk factors for deformity are extensive laminectomy, neurologic involvement, and young age (usually < 10 years) at surgery. Therefore, pediatric laminectomy should be avoided or per-
P e d i a t r i c C e r v i c a l S p i n e I n s t a b i l i t y
www.turner-white.com Orthopaedic Surgery Volume 8, Part 1 15
formed only with concurrent arthrodesis. Alterna-tively, laminoplasty can be performed.
manaGement of CerViCal SPine inStaBilitY
Protocols for managing pediatric patients who have acute trauma with an established or potential spinal
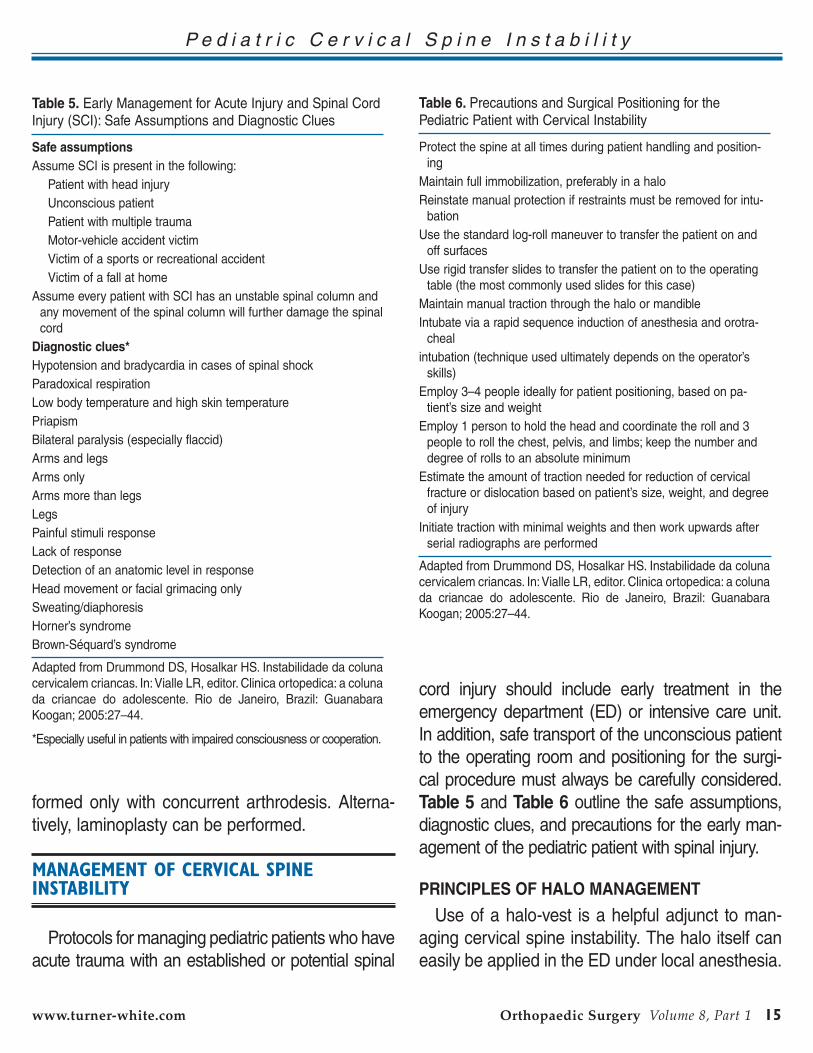
cord injury should include early treatment in the emergency department (ED) or intensive care unit. In addition, safe transport of the unconscious patient to the operating room and positioning for the surgi-cal procedure must always be carefully considered. table 5 and table 6 outline the safe assumptions, diagnostic clues, and precautions for the early man-agement of the pediatric patient with spinal injury.
principleS Of halO ManageMent
Use of a halo-vest is a helpful adjunct to man-aging cervical spine instability. The halo itself can easily be applied in the ED under local anesthesia.
table 5. Early Management for Acute Injury and Spinal Cord Injury (SCI): Safe Assumptions and Diagnostic Clues
Safe assumptionsAssume SCI is present in the following:
Patient with head injuryUnconscious patientPatient with multiple traumaMotor-vehicle accident victimVictim of a sports or recreational accidentVictim of a fall at home
Assume every patient with SCI has an unstable spinal column and any movement of the spinal column will further damage the spinal cord
diagnostic clues*Hypotension and bradycardia in cases of spinal shockParadoxical respirationLow body temperature and high skin temperaturePriapismBilateral paralysis (especially flaccid)Arms and legsArms onlyArms more than legsLegsPainful stimuli responseLack of responseDetection of an anatomic level in responseHead movement or facial grimacing onlySweating/diaphoresisHorner’s syndromeBrown-Séquard’s syndrome
Adapted from Drummond DS, Hosalkar HS. Instabilidade da coluna cervicalem criancas. In: Vialle LR, editor. Clinica ortopedica: a coluna da criancae do adolescente. Rio de Janeiro, Brazil: Guanabara Koogan; 2005:27–44.
*Especially useful in patients with impaired consciousness or cooperation.
table 6. Precautions and Surgical Positioning for the Pediatric Patient with Cervical Instability
Protect the spine at all times during patient handling and position-ing
Maintain full immobilization, preferably in a haloReinstate manual protection if restraints must be removed for intu-
bationUse the standard log-roll maneuver to transfer the patient on and
off surfacesUse rigid transfer slides to transfer the patient on to the operating
table (the most commonly used slides for this case)Maintain manual traction through the halo or mandibleIntubate via a rapid sequence induction of anesthesia and orotra-
chealintubation (technique used ultimately depends on the operator’s
skills)Employ 3–4 people ideally for patient positioning, based on pa-
tient’s size and weightEmploy 1 person to hold the head and coordinate the roll and 3
people to roll the chest, pelvis, and limbs; keep the number and degree of rolls to an absolute minimum
Estimate the amount of traction needed for reduction of cervical fracture or dislocation based on patient’s size, weight, and degree of injury
Initiate traction with minimal weights and then work upwards after serial radiographs are performed
Adapted from Drummond DS, Hosalkar HS. Instabilidade da coluna cervicalem criancas. In: Vialle LR, editor. Clinica ortopedica: a coluna da criancae do adolescente. Rio de Janeiro, Brazil: Guanabara Koogan; 2005:27–44.

P e d i a t r i c C e r v i c a l S p i n e I n s t a b i l i t y
16 Hospital Physician Board Review Manual www.turner-white.com
Once in place, the halo is readily connected to a halo-vest or other orthoses. Useful guidelines for halo placement follow.
First, the pediatric skull is thin and areas of maxi-mal thickness differ among patients. Because no skull areas are sure to be safe, CT scans of the skull are useful in patients younger than age 3 years to choose the safest area for pin placement. The tem-poral artery should be palpated and avoided. Sec-ond, the pediatric skull is softer than that of the ado-lescent or adult. Accordingly, placement of at least 8 halo pins inserted at 2 to 4 in/lb is recommended for patients younger than age 6 years; placement of 4 halo pins inserted at 4 to 6 in/lb is recommended for patients age 6 to 8 years; and placement of 4 halo pins inserted at 6 to 8 in/lb is recommended for older children and adolescents. Complications include pin-tract loosening and infection.
Surgical MethOdS fOr StaBiliZatiOn and arthrOdeSiS
In acute traumatic cases, initial halo stabilization is fol-lowed by surgical stabilization (often after 3–6 weeks), including decompression and/or arthrodesis likely with instrumentation. In cases of chronic instability, patients usually undergo elective arthrodesis with stabilization.
atlanto-axial arthrodesis and patient positioningFor most of the arthrodesis techniques described
below, the patient is positioned prone following ap-plication of a halo device. In cases of associated spinal instability, great care in patient transport is critical, and spinal cord monitoring should be used throughout this maneuver. Lateral radiographs confirm the reduction and position of the cervical spine. The halo should then be fixed to the Mayfield frame (type of skull fixation and traction device) or a similar device on the operating table, and lateral radiographs should again verify the reduction.
gallie technique. Exposure is accomplished via a midline incision between the occiput and C3. The bifid spinous process of C2 and tubercle of the occiput are identified by palpation. It is important to avoid overexposure to prevent inad-vertent fusion of adjacent levels. The posterior arch of the atlas is identified in the deeper lay-ers, and the periosteum is incised and elevated for passage of sublaminar wires or cables. The vertebral artery can be avoided by taking care to not expose more than 1 cm lateral from the mid-line in small children and not more than 1.5 cm in adolescents and adults. An 18- or 20-gauge wire or cable can be passed around the arch at this point to secure the bone graft. A bicortical graft is then harvested from the posterior iliac crest and shaped to fit against the posterior aspect of the atlas and around the spinous process of the axis. With the graft in position, the wire loop is folded over the graft and around the spinous process of the axis. The free ends of the wire are then united from the lateral edge of the graft and twisted in the midline, thus securing it and providing cervical stability. Continuous spinal cord monitoring and intraoperative imaging to confirm the reduction and graft position are important. These authors prefer the routine use of a halo-vest to protect the fusion and fixation.
Brooks arthrodesis. Exposure for Brooks arthrodesis is the same as that for the Gallie technique. The Brooks fixation differs in that a double 18-gauge wire is passed around the arch of the atlas and lamina of the axis. These authors suggest using braided cable wire because it is soft and relatively safe to pass, resists fatigue well, and provides excellent fixation. Two rectan-gular grafts 1.25 x 3.5 cm (breadth and length, respectively) are harvested from the iliac crest, and the cancellous surface is prepared to fit into

P e d i a t r i c C e r v i c a l S p i n e I n s t a b i l i t y
www.turner-white.com Orthopaedic Surgery Volume 8, Part 1 17
the C1–C2 interval. The grafts help to prevent hy-perextension and contribute to the stability of the Brooks procedure.
Occipito-cervical Stabilization and arthrodesisStabilization. Treatment of traumatic atlanto-
occipital disruption consists of reduction using gentle skull traction and stabilization in a halo-vest. Care should be taken not to distract the spine. Decompression of large hematomas at the cervi-comedullary junction may be necessary. Systemic steroids can be useful to reduce edema. Reduction should be confirmed radiographically and stability achieved by immobilization alone or by arthrodesis (see below).
In most patients, fusion can be restricted to exten-sion from the occiput to C2, thus preserving as much motion as possible in the neurologically intact patient. Bone grafts may be taken from the rib or iliac crest. However, rib grafts can be readily contoured to span 2 or more segments, if that degree of span is needed. In late cases of unreduced dislocation, reduction should not be forcefully attempted; instead fusion in situ with a suboccipital craniectomy (to relieve poste-rior impingement) is usually sufficient.
arthrodesis. Precautions in positioning are the same as described for occipito-cervical stabiliza-tion by halo. The exposure is an extension of that described for atlanto-axial arthrodesis—the midline incision extends from the occiput to the spinous pro-cess of C3. There are 2 techniques for arthrodesis of the occiput to C2 or lower. With both procedures, fixation wires or cables are passed through cranial burr holes created as 2 pairs on either side of the midline. The first technique, described in 1995,24 is based on a shaped structural graft harvested from the iliac crest, which is then fixed by wire or cable to a trough prepared at the base of the occiput and fit over the spinous process of the axis. With the sec-
ond technique, described in 2001,25 the structural
graft used is from the rib rather than the autogenous iliac crest. Paired autogenous rib grafts are har-vested and fixed to the occiput and to the axis by sublaminar wires or braided cable. The rib’s natural curve has the advantage of fitting closer to the cervi-cal spine anatomy and fusion bed. This procedure appears well tolerated and the stability is equivalent to that of the iliac onlay technique. The patient is im-mobilized in a halo-vest or a 4-post cervical orthosis postoperatively.
Subaxial injuriesThese injuries represent only 25% of all pe-
diatric cervical spine injuries.26 Fractures and
subluxations in the lower cervical spine are more common in older children and adolescents. Treatment follows the principles for adult injury. Despite a slightly improved prognosis for liga-ment healing in children, flexion–extension views should be used after immobilization for patients with subluxation and dislocation to verify healing and stability.
Subaxial arthrodesis. When internal fixation is limited by the patient’s size, the Dewar technique appears to work well.27
A modified procedure, using the button-wire implants developed for sco-liosis correction, has been described.28–30
Patients are usually immobilized in a cervical collar for 6 to 8 weeks postoperatively.31
Other Surgical techniques for Spinal Stabilizationlateral mass plate fixation. In adolescents
and teenagers, fixation with lateral mass screws and plates can be considered.30 Posterior plate fixation may also include the C1–C2 motion seg-ment. The advantage of this fixation is that pro-longed immobilization in a halo-vest may not be necessary.

P e d i a t r i c C e r v i c a l S p i n e I n s t a b i l i t y
18 Hospital Physician Board Review Manual www.turner-white.com
transarticular fixation. This fixation for C1–2 fusion may be rarely indicated for failed arthrod-esis or in case of defective posterior elements and may be performed via the posterior or lateral approach. Screw placement is critical, and good intraoperative imaging is necessary because the margin for error is very small.
anterior cervical instrumentation. Anterior cervical plating is not routinely used in the pedi-atric spine. It may have a role in adolescents and teenagers in the presence of significant instability following vertebrectomy or corpectomy. One ad-vantage is that posterior stabilization should not be required. Although there is little experience with this technique in the pediatric population, it is an option for the extraordinary situation.
SummarY
The evaluation of a child with a potential injury or instability of the cervical spine begins with the recognition of the unique anatomy and physiology in this age-group. Preventive efforts may reduce the incidence of pediatric spinal injury includ-ing: proper use of seat belts, education on safe participation in sports activities, and recognition of the signs of child abuse. Clinicians need to be aware of the common congenital and develop-mental conditions associated with the occurrence of cervical spine instability to be able to recognize them. Although advanced imaging techniques can be useful in the evaluation of subtle spine injuries and instability, a thorough knowledge of normal anatomic variants is essential for appropri-ate management.
Acknowledgment: The authors gratefully acknowledge Jennifer Goebel, Clinical Research Coordinator, for her assistance with manuscript preparation.
referenCeS
1. McGrory BJ, Klassen RA, Chao EY, et al. Acute frac-tures and dislocations of the cervical spine in children and adolescents. J Bone Joint Surg Am 1993;75:988–95.
2. Patel JC, Tepas JJ, Mollitt DL, Pieper P. Pediatric cervi-cal spine injuries: defining the disease. J Pediatr Surg 2001;36:373–6.
3. Flynn J, Dormans J. Spine trauma in children. Semin Spine Surg 1998;10:7–16.
4. Dormans JP. Evaluation of children with suspected cer-vical spine injury. Instr Course Lect 2002;51:401–10.
5. Drummond DS, Hosalkar HS. Treatment of cervical spine instability in the pediatric patient. In: Clark CR, editor. The cervical spine. 4th ed. Philadephia: Lippincott Williams & Wilkins; 2005:427–47.
6. Auerbach JD, Flynn JM. Pediatric cervical spine trauma. In: Drummond DS, editor. Pediatric topics. Rosemont (IL): American Academy of Orthopaedic Surgeons; 2006:397–405.
7. Viccellio P, Simon H, Pressman BD, et al. A prospective multicenter study of cervical spine injury in children. Pediatrics 2001;108:E20.
8. McCall T, Fassett D, Brockmeyer D. Cervical spine trauma in children: a review. Neurosurg Focus 2006;20:E5.
9. Hosalkar HS, Cain EL, Horn D, et al. Traumatic atlanto-occipital dislocation in children. J Bone Joint Surg Am 2005;87:2480–8.
10. Hosalkar HS, Greenbaum J, Gaugler R, et al. Odon-toid fractures in children. Presented at the Annual Meeting of the American Academy of Orthopaedic Surgeons; 2007 Feb 14–18; San Diego, CA. Available at www3.aaos.org/education/anmeet/anmt2007/poster/ poster.cfm?Pevent=P379. Accessed 20 Jun 2007.
11. Drummond DS, Tahernia A, Delfico A, et al. Congenital anomalies of the upper cervical spine: identifying pa-tients at risk for myelopathy. Presented at the Annual Meeting of the Pediatric Orthopaedic Society of North America; 1997 May 15–17; Banff, Alberta.
12. Copley LA, Dormans JP. Cervical spine disorders in infants and children. J Am Acad Orthop Surg 1998;6:204–14.
BOard review QueStiOnSTest your knowledge of this topic.
go to www.turner-white.com and select Orthopaedic Surgery from the drop-down menu of specialties.

P e d i a t r i c C e r v i c a l S p i n e I n s t a b i l i t y
www.turner-white.com Orthopaedic Surgery Volume 8, Part 1 19
13. Guille JT, Sherk HH. Congenital osseous anomalies of the upper and lower cervical spine in children. J Bone Joint Surg Am 2002;84:277–88.
14. Hensinger RN. Osseous anomalies of the cranioverte-bral junction. Spine 1986;11:323–33.
15. Spierings EL, Braakman R. The management of os odontoideum. Analysis of 37 cases. J Bone Joint Surg Br 1982;64:422–8.
16. Gholve PA, Hosalkar HS, Ricchetti ET, et al. Occipita-lization of the atlas in children. Morphologic classifica-tion, associations, and clinical relevance. J Bone Joint Surg Am 2007;89:571–8.
17. Smoker WR. MR imaging of the craniovertebral junc-tion. Magn Reson Imaging Clin N Am 2000;8:635–50.
18. Sankar WN, Wills BP, Dormans JP, Drummond DS. Os odontoideum revisited: the case for a multifactorial etiol-ogy. Spine 2006;31:979–84.
19. Scolville WB, Sherman IJ. Platybasia, report of 10 cases. Ann Surg 1951;133:496–502.
20. Auerbach J, Hosalkar HS, Kusuma S, et al. Spinal cord dimensions in children with Klippel-Feil syndrome: impli-cations for neurologic outcomes. Presented at the An-nual Meeting of the American Academy of Orthopaedic Surgeons; 2007 Feb 14–18; San Diego, CA. Available at www3.aaos.org/education/anmeet/anmt2007/poster/poster.cfm?Pevent=P390. Accessed 20 Jun 2007.
21. Tracy MR, Dormans JP, Kusumi K. Klippel-Feil syn-drome: clinical features and current understanding of etiology. Clin Orthop 2004;424: 183–90.
22. Ricchetti ET, States L, Hosalkar HS, et al. Radiographic
study of the upper cervical spine in the 22q11.2 deletion syndrome. J Bone Joint Surg Am 2004;86:1751–60.
23. Lonstein JE. Post-laminectomy kyphosis. Clin Orthop 1977;128:93–100.
24. Dormans JP, Drummond DS, Sutton LN, et al. Oc-cipitocervical arthrodesis in children. A new tech-nique and analysis of results. J Bone Joint Surg Am 1995;77:1234–40.
25. Cohen MW, Drummond DS, Flynn JM, et al. A tech-nique of occipitocervical arthrodesis in children using autologous rib grafts. Spine 2001;26:825–9.
26. McLain RF, Clark CR, el-Khoury GY. C6-7 dislocation in a neurologically intact neonate. A case report. Spine 1989;14:125–7.
27. Davey JR, Rorabeck CH, Bailey SI, et al. A technique of posterior cervical fusion for instability of the cervical spine. Spine 1985;10:722–8.
28. Francis WR, Fielding JW, Hawkins RJ, et al. Traumatic spondylolisthesis of the axis. J Bone Joint Surg Br 1981;63:313–8.
29. Pizzutillo PD, Rocha EF, D’Astous J, et al. Bilateral frac-ture of the pedicle of the second cervical vertebra in the young child. J Bone Joint Surg Am 1986;68:892–6.
30. Drummond DS, Hosalkar H. Treatment of cervical spine instability in the pediatric patient. In: Clark CR, Benzel EC, Currier BL, et al, editors. The cervical spine. 4th ed. Philadelphia [PA]: Lippincott Williams & Wilkins; 2004:443–5.
31. Drummond DS. Pediatric cervical instability: diagnosis and treatment concepts. Semin Spine Surg 1996;8–14.
Copyright 2013 by Turner White Communications Inc., Wayne, PA. All rights reserved.