Embed Size (px)
Citation preview

Abstract:The frequency of national and inter-national disaster events, increasedmedia attention, and regulatorychanges have all contributed to animproved public awareness of thevital role hospitals play in a crisis.Although hospital disaster prepa-redness efforts have matured dra-matically since the September 11th2001 terrorist attacks, much workstill remains to prepare all hospitalsfor potential pediatric victims. Thisarticle emphasizes key emergencyresponse aspects of hospital pre-paredness for disasters involvingchildren, in particular (1) hospital-based incident command, (2) stra-tegies for operational continuity, (3)pediatric principles of surge capa-city, (4) development of decontami-nation protocols, (5) infectioncontrol, (6) sheltering in place, and(7) evacuation strategies.
Keywords:pediatric hospital preparedness;
infection control; shelter in place;
evacuation
*Department of Patient Services, Center for
Biopreparedness, Children’s Hospital Bos-
ton, Harvard Medical School, Boston, MA;
†Division of Emergency Medicine, Depart-
ment of Pediatrics, Center for Bioprepared-
ness, Children’s Hospital Boston, Harvard
Medical School, Boston, MA; ‡Division of
Infectious Diseases, Children’s Hospital
Boston, Harvard Medical School, Boston,
MA; §Department of Medicine, Children’s
Hospital Boston, Harvard Medical School,
Boston, MA; ODepartment of Laboratory
Medicine, Children’s Hospital Boston, Har-
vard Medical School, Boston, MA; ¶Depart-
ment of Pediatrics, Children’s Hospital
Boston, HarvardMedical School, Boston,MA.
Reprint requests and correspondence:
Stephen Monteiro, MS, EMT-P,
Children’s Hospital Boston, 300
Longwood Ave, Boston, MA 02115.
216 VOL. 10, NO. 3 • PEDIATRIC ASPECTS OF HOSP
Pediatric Aspectsof Hospital
Preparedness
ITAL PREPAREDNESS / MONTEIRO
Stephen Monteiro, MS, EMT-P,*Michael Shannon, MD, MPH,†
Thomas J. Sandora, MD, MPH,‡§OOO¶Sarita Chung, MD†
s our nation continues to develop and enhance itsdisaster response capabilities, the recent economic
Adownturn and fierce competition for federal dollarshave hampered progress. This was one of the keyconclusions reported in the most recent annual report from theTrust for America's Health (TAH) and the Robert Wood JohnsonFoundation, Ready or Not? 2008.1 Among the most vulnerablepopulations affected by this slowing of progress are children. Asa group, children represent 22% to 30% of the total population;because of their unique characteristics (ie, psychological,developmental, physiological and anatomical), children demandspecial consideration when conducting disaster planning. Inaddition, the TAH report supports the claim that children havesignificantly higher mortality rates in disasters when comparedwith adults. The TAH concludes that response planning remainsincomplete for critical preparedness areas such as surgecapacity, rapid disease detection, and food safety.2 Because oftheir unique vulnerabilities, children and their needs must beincorporated into all stages of disaster planning to improve theresponse chain.
Hospitals are not exempt from this process. Given that 90% ofAmerica's children seek emergency care at general hospitals,3 allhospitals must include pediatric needs in their emergencypreparedness plans. In this article, we will discuss centralcomponents of hospital-based emergency preparedness programswith emphasis on pediatric preparedness. In addition, we willidentify unique challenges to providing emergency response tochildren. Key emergency response aspects of hospital prepared-ness for disasters involving children include (1) hospital-based
ET AL.

1522-8401/$ - see front matter
Published by Elsevier Inc.
PEDIATRIC ASPECTS OF HOSPITAL PREPAREDNESS / MONTEIRO ET AL. • VOL. 10, NO. 3 217
incident command, (2) strategies for operationalcontinuity, (3) pediatric principles of surge capacity,(4) development of decontamination protocols, (5)infection control, (6) sheltering in place, and (7)evacuation strategies.
HOSPITAL INCIDENT COMMAND SYSTEMSOne of the cornerstones of any emergency
preparedness effort is the establishment of anIncident Command System (ICS). These crisismanagement systems are invaluable because theycreate a platform upon which to build a customizedresponse to any hazard. Advantages provided by theICS include the benefit of a clear reporting structure(chain of command), the ability to maintainaccountability and management of multiple respon-ders (span of control), and the standardization ofterms that facilitates multidisciplinary coordinationand decreases confusion (common language).
Hospitals have been using ICS for many years withthe latest version of this system, Hospital IncidentCommand System (HICS) released in October 2006.A significant advantage of HICS is its reflection of themedical mission and infrastructure of a typicalhospital while incorporating the standard ICSstructure, enabling a seamless interface with otherICS agencies involved in disaster response. It isessential that health care agencies adopting HICStake the necessary steps to customize the system toreflect their own institutional capabilities and com-plexity. The standardHICS systemmodel is shown inFigure 1. Highlighted in the figure are roles thatshould include pediatric focus.
Crisis Management Training for KeyLeadership Roles
Strategies used by Children's Hospital Boston tosupport HICS activations include (1) limiting thenumber of eligible incident commanders, (2) support-ing the incident commander pool with specializedtraining, and (3) creating a confidential review forumwhere each HICS activation is reviewed. Keeping thepool of potential incident commanders small increaseseach member's exposure to command opportunities
and facilitates more intensive training on advancedHICS strategies. In institutions that provide care forboth adults and children having at least 1 of themembers of this pool with pediatric expertise will helpothers understand the vulnerabilities and uniqueneeds of children. Creating a confidential reviewforum allows for all HICS activations to be reviewedand critiqued. Modeled after Morbidity and Mortalityrounds, this forum allows for open discussion of eachevent and after action recommendations and allowsfor all members to gain from the combined experi-ences. Additional data support for this forum can beachieved through an event-tracking process wherefrequency of activation, type, and duration of eventare noted, analyzed, and reported.
Institutions that do not have an abundance ofpediatric-trained staff should also consider buildingcustomized HICS roles that would be dedicated toaddressing pediatric concerns for roles such asmedical (inpatient and outpatient unit leaders) andmental health care, family support unit leader, supply,pharmacy, nutrition, and security. Specific pediatricresponsibilities for these roles may include a pharma-cist with pediatric experience that can compoundadult tablets into size-appropriate oral solutions.Another example is having trained child life specia-lists in the mental health care unit to provide age-appropriate distraction to pediatric victims. A com-prehensive list of pediatric-specific HICS roles andtheir responsibilities is shown in Table 1.
STRATEGIES FOR OPERATIONALCONTINUITY
At the core of every hospital's mission is a desireto provide essential services to all who seek them.Disasters and unplanned disruptions threaten ahospital's ability to deliver on this mission. Strate-gies to enhance operational continuity and chal-lenges are presented.
Emergency Staffing Strategies
When disasters occur, hospitals in the affectedarea often experience inadequate staffing. A largeinflux of patients seeking care can overwhelm thecapacity of on-hand hospital staff. Concurrently,there will be immediate loss of some staff due tochild care, eldercare, or pet care obligations withothers unwilling to come to work.4 Hospitalsmaintaining higher nurse-to-patient ratios arebetter positioned to surge with on-hand staff.Through the use of departmental emergency callback procedures, these same hospitals may also be
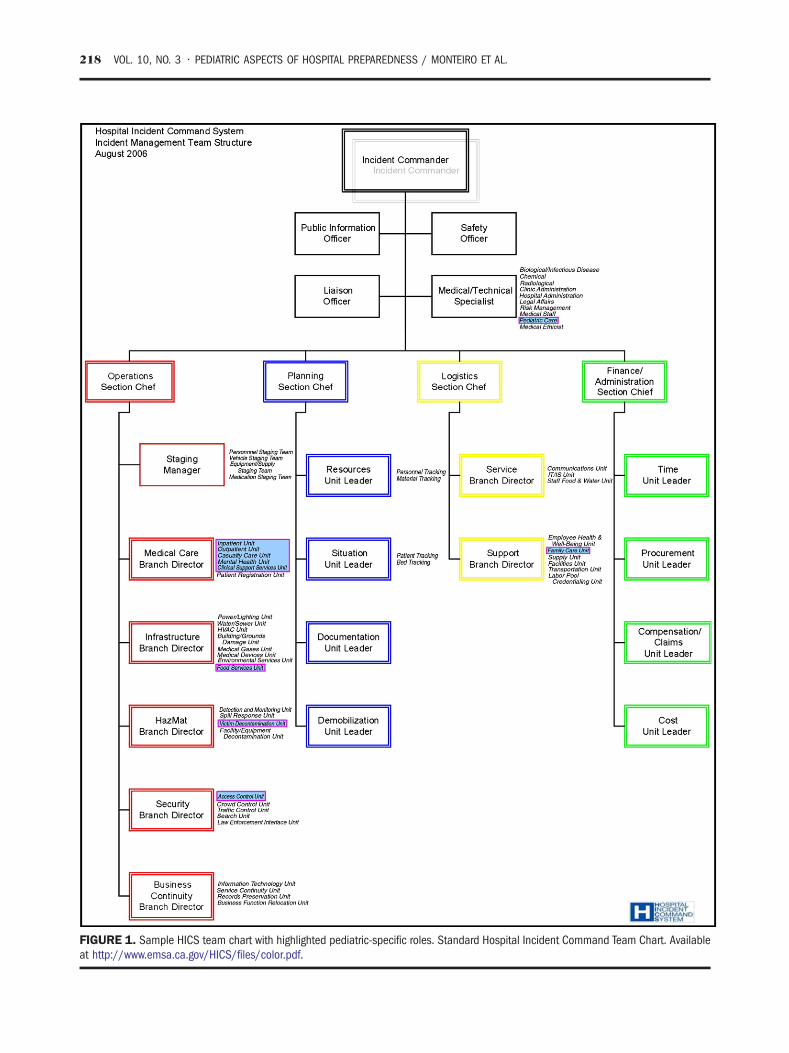
IGURE 1. Sample HICS team chart with highlighted pediatric-specific roles. Standard Hospital Incident Command Team Chart. Availablet http://www.emsa.ca.gov/HICS/files/color.pdf.
218 VOL. 10, NO. 3 • PEDIATRIC ASPECTS OF HOSPITAL PREPAREDNESS / MONTEIRO ET AL.
Fa

TABLE 1. Highlighted pediatric-specific roles.
HICS PositionRationale for Pediatric-
Specific Role
Medical technologyspecialist-pediatrician
Works within the incident commandgroup to identify potential pediatriccare related concerns and strategies
Family care unit Helps coordinate issues of reunificationand psychosocial issues of family(not victims)
Supply unit Concerned with obtaining anddistributing pediatric-specificequipment
Inpatient unit Responsible for overall inpatientpediatric care (includes pediatricintensive care unit level care)
Outpatient unit Responsible for overall outpatientpediatric care
Casualty care unit Responsible for overall emergencydepartment pediatric care
Mental health unit Responsible for pediatric victimpsychosocial and behavioral response
Food service unit Responsible for nutritional needsof children
Victim decontaminationunit
Responsible for providingage-appropriate communication andassistance while pediatric patientsare undergoing decontamination
Access control unit Responsible for security of pediatricpatients (injured and well) andenforcing disaster credentialingidentification/reunification policiesas they relate to access control.
PEDIATRIC ASPECTS OF HOSPITAL PREPAREDNESS / MONTEIRO ET AL. • VOL. 10, NO. 3 219
better positioned to surge their available pool ofduty staff.
Another often-sited source for emergency volun-teers is the Medical Reserve Corps (MRC). However,the number of pediatric-trained MRC volunteers isnot known, and due to limited pediatric resources,those with pediatric knowledge may already becommitted to their primary institution. A notablepediatric-specific issue is the lack of a requiredCriminal Offender Record Information or back-ground check. For example, Children's HospitalBoston requires all employees and volunteers to
complete Criminal Offender Record Informationchecks before being hired and credentialed. Applyingthese criteria to MRC's and other disaster volunteersmay help to identify convicted sex offenders or otherpersons who should not have access to childrenduring a disaster. Lastly, variable host hospitalcredentialing processes may force some MRC volun-teers to be recredentialed to meet Joint Commissionstandards, causing potential delays.
Other challenges associated with disaster creden-tialing include registration, emergency credential-ing, and verification. Several systems and methodsexist to enable volunteer health care professionals topreregister in advance of a disaster with variousmedical response groups (eg, MRC, Red Cross,Community Emergency Response Teams, etc).However, standards for vetting information (eg,medical license source verification) vary fromgroup to group. Often, volunteers are responsiblefor maintaining records of their credentialing andtraining. Therefore, it is possible that a health careworker who has recently been suspended by theirlicensing board may choose not to inform themedical response group.
Although neighboring facilities may have anabundance of licensed and available health careworkers, without appropriate credentialing by thehost site, these potential volunteers are prohibitedfrom providing care. The creation and standardiza-tion of a hospital-based tool (ie, centralized data-base) housing privileged information on all theinstitution's licensed health care professionals havebeen proposed in the literature. One theoreticaladvantage is that linking such databases with acounty health care agency or mutually acceptableorganization will result in practitioners gainingdisaster privileges faster and be able to assistimpacted hospitals.5
Emergency Caches of Equipment
In the event that a disaster targets children, theuse of predetermined pediatric disaster formularieswill expedite disaster response. Formularies are acollection of prescribed items or supplies that can berequested through a single order number or code.Disaster formularies may include medical andpharmaceutical surge supplies and should augmentthe core pediatric equipment thatmay already be on-hand. Specific subformularies can be designed forspecific hazards such as infectious outbreak, trauma,burns or hazardous material exposure, and contam-ination. Advantages of creating pediatric disasterformularies include the preidentification of essentialequipment and pharmacological supplies, as well as a
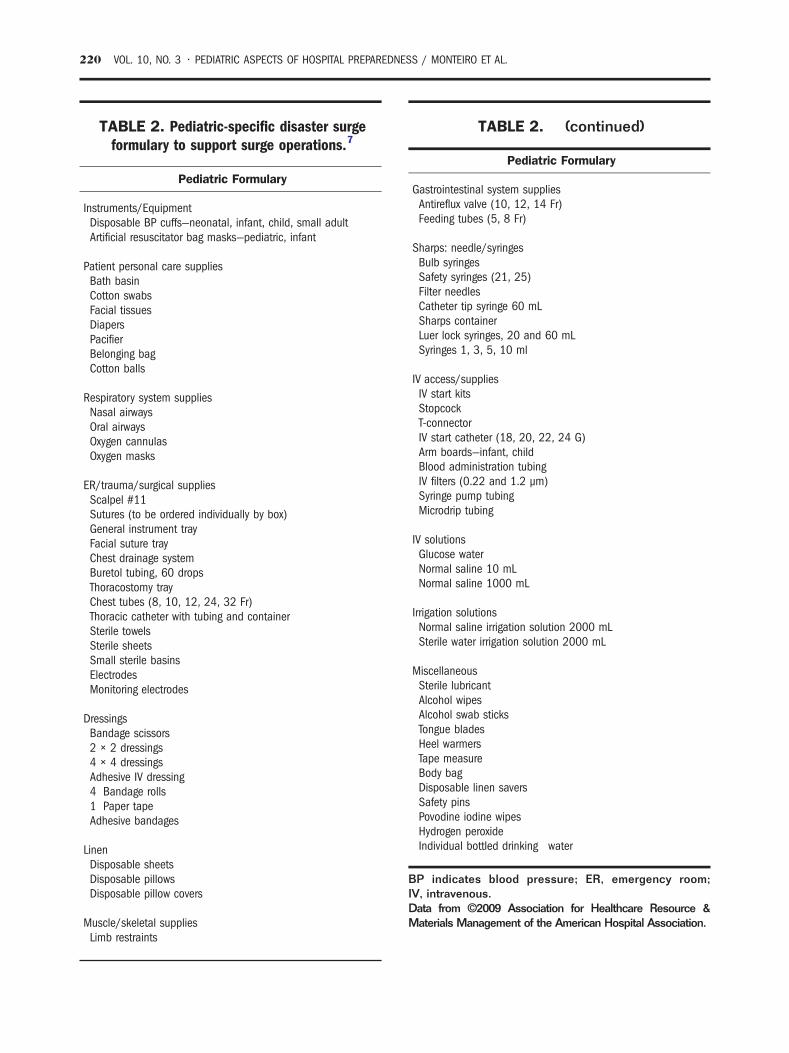
TABLE 2. Pediatric-specific disaster surgeformulary to support surge operations.7
Pediatric Formulary
Instruments/EquipmentDisposable BP cuffs—neonatal, infant, child, small adultArtificial resuscitator bag masks—pediatric, infant
Patient personal care suppliesBath basinCotton swabsFacial tissuesDiapersPacifierBelonging bagCotton balls
Respiratory system suppliesNasal airwaysOral airwaysOxygen cannulasOxygen masks
ER/trauma/surgical suppliesScalpel #11Sutures (to be ordered individually by box)General instrument trayFacial suture trayChest drainage systemBuretol tubing, 60 dropsThoracostomy trayChest tubes (8, 10, 12, 24, 32 Fr)Thoracic catheter with tubing and containerSterile towelsSterile sheetsSmall sterile basinsElectrodesMonitoring electrodes
DressingsBandage scissors2 × 2 dressings4 × 4 dressingsAdhesive IV dressing4 Bandage rolls1 Paper tapeAdhesive bandages
LinenDisposable sheetsDisposable pillowsDisposable pillow covers
Muscle/skeletal suppliesLimb restraints
TABLE 2. (continued)
Pediatric Formulary
Gastrointestinal system suppliesAntireflux valve (10, 12, 14 Fr)Feeding tubes (5, 8 Fr)
Sharps: needle/syringesBulb syringesSafety syringes (21, 25)Filter needlesCatheter tip syringe 60 mLSharps containerLuer lock syringes, 20 and 60 mLSyringes 1, 3, 5, 10 ml
IV access/suppliesIV start kitsStopcockT-connectorIV start catheter (18, 20, 22, 24 G)Arm boards—infant, childBlood administration tubingIV filters (0.22 and 1.2 μm)Syringe pump tubingMicrodrip tubing
IV solutionsGlucose waterNormal saline 10 mLNormal saline 1000 mL
Irrigation solutionsNormal saline irrigation solution 2000 mLSterile water irrigation solution 2000 mL
MiscellaneousSterile lubricantAlcohol wipesAlcohol swab sticksTongue bladesHeel warmersTape measureBody bagDisposable linen saversSafety pinsPovodine iodine wipesHydrogen peroxideIndividual bottled drinking water
BP indicates blood pressure; ER, emergency room;IV, intravenous.Data from ©2009 Association for Healthcare Resource &Materials Management of the American Hospital Association.
220 VOL. 10, NO. 3 • PEDIATRIC ASPECTS OF HOSPITAL PREPAREDNESS / MONTEIRO ET AL.

PEDIATRIC ASPECTS OF HOSPITAL PREPAREDNESS / MONTEIRO ET AL. • VOL. 10, NO. 3 221
cost-effective method of identifying disaster surgesupplies without having to incur costs or mainte-nance challenges associated with storing these itemson-site. Such pediatric disaster formularies mustinclude equipment with varying sizes to accommo-date children of all ages. Lists of basic pediatricequipment are widely available.6 Examples of pedia-tric disaster formularies have been created by theAssociation for HealthCare Resources and MaterialManagement and can be found at http://www.ahrmm.org/ahrmm/news_and_issues/issues_ and_initiatives/files/disaster_formularies.pdf. An example of such aformulary can be found in Table 2.
Emergency Notification Systems
The ability to communicate effectively is a toppriority during a disaster. Emergencies anddisaster response can place immediate stress onan organization, and it is essential that staff,external organizations, patients, and their familiesare all well informed.8 Health care institutionshave recently placed a high priority on massnotification systems to help maintain communi-cations throughout an event. Advantages includethe ability to organize intended receivers intogroups (ie, staff by department or role, patients,and their families, etc), send messages in avariety of forms (voice and/or text) with differentcommunication devices (mobile and landlinephones, pagers, computers, etc), and administerthese messages by providing tools that prioritizeand confirm message path progress. These massnotification systems can be combined with othercommunication tools such as the GovernmentEmergency Telecommunications System. Auto-mated mass notification systems offer a numberof advantages over traditional emergency calltrees. However, they are potentially vulnerableto system disruptions, and therefore, the tradi-tional maintenance of emergency call treesremains an essential planning strategy and shouldbe exercised routinely.
In contrast to the information “push” strategiesoutlined above, another mass notification system isthe utilization of customizable Web sites whereresponders and interested parties can “pull” neces-sary information. A well-designed event-specificWeb site can be an extremely valuable and scalablemethod of communicating to a variety of differentstakeholders. This is especially useful when theinformation is rapidly changing, and the only otheralternative is to continue to barrage a widedistribution list with numerous “blasts” updates.
Alternate Care Sites
Alternate Care Sites (ACS) can be called uponwhen disasters strike and threaten to overwhelm thecurrent health care infrastructure. They are typi-cally buildings of opportunity that can be quicklyconverted for the purposes of providing care outsideof typical health care infrastructure. Alternate CareSites can be used in a variety of roles including aprimary triage point, public distribution of medica-tions or vaccines, or a low-acuity patient care site.9
Pediatric planning for ACS must include caring forchildren without guardians as well as children withtheir families. Additional attention to childproofingACS for safety, providing adequate staff to care forpediatric victims, and assigning security is neededto prevent possible harm to children.
Enabling the Response, Staff Safety
Among reasons for staff not being able to report towork during a disaster are transportation issues,childcare and eldercare responsibilities, personalhealth concerns, and pet care obligations. Histori-cally, the reasons cited for not being willing to reportinclude fear and concern for family and for self.4
Including alternative transportation options like carpools or arrangements with local emergency man-agement agencies may enable staff to respond toemergency requests. In addition, the importance ofcomprehensive staff support, for example, child/elder and pet care, and mental health supportoptions must be addressed and communicated tostaff in advance. Although staff response may stilldiffer based on the nature of the catastrophe,generally staff awareness of the various forms ofsupport services offered to staff will likely correlatewith an increase in the number of employees whoare able to respond. Lastly, the importance for eachemployee to create a personal preparedness planshould be supported by the institution. Without apersonal preparedness plan, staff will have littlealternative but to leave the response effort to tend tofamily-related needs.
In addition to providing the support servicesnecessary to enable response, hospitals must alsostockpile personal protective equipment. Stockpilesof N95 respirators, chemical decontamination orbiohazard suits, and positive air-purifying respira-tors, and others, are critical to conveying to staffthat their safety concerns have been adequatelyaddressed. Also of paramount importance is thepurchase and maintenance of pharmaceutical coun-termeasures and prophylactic agents for employees

222 VOL. 10, NO. 3 • PEDIATRIC ASPECTS OF HOSPITAL PREPAREDNESS / MONTEIRO ET AL.
and their families. Purchases of pharmacologicalagents may vary based on local community risks.
Lastly, hospitals must consider how they willfurther incentivize disaster response. AlthoughMaryland and South Carolina have pursuedlegislation that obligate health care workers torespond to emergency requests for assistance orface a range of sanctions, this approach raises anumber of ethical and legal concerns. An alternatestrategy to increase disaster resources mayinclude financial incentives, the use of volunteernetworks, and protection from disaster-relatedliability.10 For example, the California DisasterService Worker Volunteer Program provides work-ers' compensation insurance coverage in the eventa disaster service worker volunteer is injuredwhile performing assigned disaster duties.11 Hos-pitals that effectively create department-specificcontingency plans and communicate comprehen-sive safety plans will ensure maintaining theiroperational continuity.
PEDIATRIC PRINCIPLES OF SURGECAPACITY AND SURGE CAPABILITY
Before 2004, an established federal surge capa-city planning guideline did not exist. Hospitals inrural and urban settings each crafted surge planningscenarios based on perceived risk and anticipatedpatient volumes. For example, Children's HospitalBoston established 2 different levels of surgeresponse, the first dealing with 5 to 50 patientsand the second dealing with more than 450 patients.In 2004, Health Resource and Services Administra-tion set a critical benchmark for all States toestablish a system that allows for the triage,treatment, and disposition of 500 adult and pedia-tric patients per 1 million population during adisaster.12 One obvious advantage of moving to apopulation-based planning metric is that it isscalable. In addition, basing surge planning onpopulation density facilitates a closer examinationof the availability of pediatric specialty careresources within a local area.
Surge Capacity planning can be dissected into 2planning categories: (1) surge capacity—defined asthe ability to respond to a markedly increasednumber of patients, and (2) surge capability—defined as the ability to address unusual or veryspecialized medical needs.13 By focusing on surgecapabilities, specific pediatric planning aspects canbe identified.
Children can be victims of a catastrophic event ordirect targets of terrorism. After an event, children
may be transported to a hospital for stabilizationwith limited pediatric resources. After large-scaledisasters, most victims are not transported byambulance; instead, they arrive at hospitals bytheir own means.14 Therefore, reliance on prehos-pital responders to triage and transport children tospecialized pediatric care hospitals will not mitigatethe likelihood of all hospitals receiving injuredchildren. Unfortunately, many emergency depart-ments lack the basic equipment to adequately carefor pediatric patients and remain unprepared forpediatric emergencies.15
Solutions and Recommendations for Pediatric Surge
The availability of pediatric equipment, trainedmedical staff, guidelines, and protocols for the careof injured children are essential to a successfulresponse to catastrophic events. The AmericanAcademy of Pediatrics has created numerous toolsto assist hospitals attempting to enhance theirpediatric disaster response capability. Among themis a comprehensive guideline for pediatricians thatcan be found at http://www.aap.org/disasters/pdf/DisasterPrepPlanforPeds.pdf. In addition to theclinical guidance, there are numerous child careand school-based resources available at the Amer-ican Academy of Pediatrics disaster Web site athttp://www.aap.org/disasters/index.cfm.
Stockpiling critical supplies is another essentialelement of surge response. The potential for supplychain disruptions increases with the size andmagnitude of the event. Therefore, hospital emer-gency management leaders must ensure adequatesupplies by maintaining updated inventories on siteand easy accessibility of supplies stored off site.
In planning for a surge of pediatric patients,it is essential to acquire and maintain plans forthe following:
• pediatric equipment (ie, medical and non-medical supply);
• pediatric-trained emergency and intensivecare unit staff;
• psychosocial support (ie, pediatric socialworkers, child life specialists, psychiatry,and psychology);
• pharmacological inventories (both treatmentand prophylaxis medications) and protocolsfor weight-based dosing and pediatric-appro-priate preparations (need reference here); and
• security protocols—for specialized holdingareas for injured and noninjured unaccompa-nied children.16 Recommendations for thecare and oversight of noninjured children

PEDIATRIC ASPECTS OF HOSPITAL PREPAREDNESS / MONTEIRO ET AL. • VOL. 10, NO. 3 223
include at minimum security/supervisoryratios of:
1 adult to 4 infants;1 adult to 10 preschool children; and1 adult to 20 school-aged children.
There is a significant amount of literature thatproposes several surge strategies. Most immediateactivities involve clearing the emergency depart-ment of minor injuries and canceling electiveprocedures and admissions to conserve capacity.17
Other emergency department surge strategies incor-porated at Children's Hospital Boston include thedivision of the emergency department to disastervictims and nondisaster victims, separate entrancesfor each group, and establishment of unidirectionalflow of patients. In addition, pediatric victims shouldbe cohorted to minimize confusion and prevent themisplacement of these victims.
Infection Control Issues in Response to anInflux of Contagious Patients
The possibility of transmission of infectiousagents and environmental contamination must beconsidered as part of surge planning. Hospitalsmust be prepared for the possibility of a largeinflux of infectious patients and must have plansin place to address infection control issues in thatscenario. In Chapter 5 of the New York CityDepartment of Health and Mental Hygiene Chil-dren in Disasters Tool Kit, the authors provide acomprehensive overview of infection controlissues based on point-of-entry infection controlmeasure, response to the asymptomatic exposedchild, and a well-organized scenario-based seriesof response strategies.18
An event may involve as little as 1 patient infectedwith an epidemiologically significant pathogen(such as smallpox) or a large number of patientsinfected with a more common pathogen (such asinfluenza A). The precise response is contingent onthe nature and magnitude of the event and the modeof transmission of the infecting organism. Regard-less of the pathogen, a health care facility'sresources may become stressed in regard to staffing,equipment, and supplies. Pediatric facilities may bedisproportionately affected during infectious events,as many of the organisms with the potential to causelarge outbreaks (including respiratory viruses suchas influenza) are transmitted more easily amongchildren as compared with adults because offrequent close contact with age-group peers and
suboptimal hand hygiene and respiratory etiquetteamong young children.
Surveillance systems may indicate a potentialinfectious event in the early stages. A variety ofsurveillance activities from both internal andexternal sources are likely to be useful in thisregard. Infection control departments at pediatrichospitals conduct routine surveillance to detectunusual infections or clusters of patients or staffwith similar symptoms. In addition, emergencydepartments and public health authorities mayperform real-time syndromic surveillance to iden-tify clusters across a wider scale. These activitiescan facilitate a more timely response and initiationof the appropriate isolation precautions, which willminimize the risk of exposure and subsequenttransmission of infection. Early response to apotential or actual influx of contagious patientsshould involve a collaborative effort between emer-gency services, hospital epidemiologists and infec-tion control departments, pediatric infectiousdisease physicians, occupational health services,local and state public health authorities, and theincident commander for the facility.
One of the first steps in surge planning forinfectious events is identifying a location for triagingor holding large numbers of patients that maypresent to a pediatric facility. Facilities shouldconsider both outdoor locations (which may behelpful during an influx of patients with symptomsthat may require airborne precautions) and indoorlocations (for patients with symptoms requiringstandard, contact, or droplet precautions). Oneimportant pediatric-specific aspect of this planningis consideration of the containment of youngchildren who are ambulatory; safety is a primeconcern in this setting (eg, if a parking lot or trafficcircle is to be used during an influx, facilities mustensure that vehicles are not being driven throughareas where large numbers of small children may berunning freely).
Interventions to reduce the risk of exposure andtransmission of infectious diseases among patients,families, and staff members will depend on thespecific infecting organism and its mode of trans-mission. However, until a diagnosis is confirmed,there are several general precautions that can betaken to minimize these risks. For symptom com-plexes that suggest potential airborne or droplettransmission (such as fever with respiratory symp-toms and/or rash), facilities should consider thefollowing actions: (1) supply patients and familymembers with surgical masks (donning masks is notalways feasible for young children, and families mayrequire assistance in placing masks on their

TABLE 3. A comprehensive pediatric and adultmedical countermeasure stockpile.
Atropine DTPA bulk
BAL in oil Hydroxocobalamin Pralidoxime
Calcium DTPA Mark I kits Prussian blue
Cidofovir Mark I trainers Pyridostigmine
Midazolam Rimantadine
Ciprofloxacin Oseltamivir
Cyanide antidote kits Pediatric atropine Zanamivir
Doxycycline Potassium iodide Zinc DTPA
DTPA indicates diethylenetriamine pentaacetic acid. BALindicates dimercaprol injections USP.
224 VOL. 10, NO. 3 • PEDIATRIC ASPECTS OF HOSPITAL PREPAREDNESS / MONTEIRO ET AL.
children); (2) provide coverage (such as cleansheets or hospital gowns) for rashes or skin lesionsthat may be a source of transmission; (3) instructpatients and family members on cough etiquetteand provide tissues, hand sanitizer, and red bagtrash receptacles; (4) instruct patients and familiesto maintain at least 3 ft of spatial separation fromother patients, if feasible; and (5) provide fittedrespirators (eg, N95s) or powered air-purifyingrespirators, surgical masks, gowns, and/or gloves toemployees caring for patients. In addition, forcertain infections (such as viral hemorrhagicfevers), additional supplies may be required, includ-ing impermeable gowns, eye protection, and headand foot coverage. For symptom complexes thatsuggest potential contact transmission (such asvomiting and/or diarrhea), facilities should considerthe following actions: (1) provide hand sanitizerand instruct patients, families, and staff membersabout the importance of careful hand hygiene; (2)provide emesis basins and instruct patients touse only dedicated bathrooms or portable toiletfacilities; (3) provide gowns and gloves for employ-ees caring for patients; and (4) emphasize propercleaning and disinfection of the environment toreduce contamination.
Transporting patients with potentially contagiousillnesses requires careful advance planning. Patientswho are isolated should only leave the environmentfor essential medical purposes. If transporting apatient is necessary, isolation precautions must bemaintained and appropriate supplies (such assurgical masks) must be supplied. Receiving depart-ments must always be notified about the transportin advance so that appropriate precautions can betaken in the receiving location. Additional transportinterventions, such as evacuation and securing ofthe transport route and elevators, may be requireddepending on the infecting organism.
Managing supplies is a critical component ofsurge planning for infectious events. Specificsupplies that should be monitored include respira-tors (including both N95 and powered air-purifyingrespirators), surgical masks, gowns, gloves, eyeprotection (face shields or goggles), and handhygiene agents (both alcohol-based hand sanitizersand soap). For pediatric events, consideration mustbe given to supplies of both pediatric- and adult-sized personal protective equipment such asmasks. A dashboard showing each item, thenumber in stock, and the ideal par level can beupdated daily and is helpful for planning purposesduring such a scenario. When supplies are limited,facilities may consider alternative sources such aspublic health agencies or neighboring hospitals,
which may be able to lend supplies if the event isnot widespread.
In addition to personal protective equipment,infectious events may necessitate the use ofmedications (such as antibiotics or antivirals usedfor prophylaxis or treatment), vaccines, or otheragents. A pharmacological stockpile can alsohelp to allay fear and uncertainty among theworkforce that can drive absenteeism, especiallyas it relates to potentially infectious agents.4,19
Limited resources prohibit the purchase of allagents for all potential scenarios, and stockpilesshould ideally reflect the perceived and knownrisks inherent to each institution and patientpopulation. Having a memorandum of understand-ing in place across institutions in a region allowsfor pharmaceutical supplies to be easily transferredto those hospitals in need. An example of acomprehensive pediatric and adult pharmaceuticalstockpile may be found in Table 3.
Developing tiers that separate health care workersin different levels of risk exposure can be a usefulstrategy. The type of health care worker and thequantity in each tier will differ depending on theinfectious agent and the route of exposure. Thesetiers enable planning groups to more accuratelyanticipate the costs associated with purchasing andmaintaining a workforce protection pharmacystockpile. Hospitals that have committed funds tothe purchase and maintenance of a workforcepharmacological stockpile must also develop plansfor emergency distribution. “Closed” or nonpublicpoints of distribution plans should focus on the
PEDIATRIC ASPECTS OF HOSPITAL PREPAREDNESS / MONTEIRO ET AL. • VOL. 10, NO. 3 225
logistics of priority distribution of medication toidentified essential staff. These plans should includehow to distribute the on-hand workforce stockpilesas well as the method for requesting and obtainingadditional distributions from regional caches (eg,Center for Disease Control and Prevention chem-paks) and national push-paks from the StrategicNational Stockpile.
Finally, communication is a key component ofmanaging an influx of contagious patients. Timelydissemination of information to staff members,patients and families, public health authorities, andthe media can ensure that education aboutsymptoms and instructions about patient manage-ment are rapidly and widely circulated. Thiscommunication can also alleviate anxiety amongpatients, family members, and staff. Informationabout case counts, modes of transmission, andinfection control measures may change rapidlyduring an infectious event, and facilities should usea variety of strategies to update key stakeholders,including signs, electronic communication, andWeb sites that can be used for rapid posting ofreal-time updates and that can serve as a centra-lized source of current information and guidance.Pediatric facilities should be prepared to act asvocal advocates for pediatric-specific issues (suchas school closures or instructions for childcareprograms) during collaborations with neighboringfacilities and local and state public health agencies,which often focus on strategies that are tailored toadult patients and may forget about necessarymodifications for children.
DECONTAMINATIONGiven the number of victims that will bypass
prehospital systems and come directly to thehospital, each hospital must have plans for deconta-mination. Building a successful decontaminationprogram requires understanding placement andaccessibility of equipment, staff training, and com-munication capabilities for bothworkers and victims.
There are a number of issues that arise in thedevelopment of pediatric-specific decontaminationstrategies. To effectively prepare for these pediatric-specific challenges, all decontamination programsshould include having sufficient on-hand supply ofage-appropriate equipment (eg, decontaminationcubbies for infants), a communication programthat prepares children for the decontaminationexperience through visual and verbal communica-tion channels, warm water to prevent hypothermia,age-appropriate protocols that minimize psychoso-cial issues of privacy, and a method of assuring
security and implementing tracking measures intoall phases of the decontamination process.
SHELTERING IN PLACEThe importance of a substantial shelter in place
capability is not only for the patients and familiesbut also for the community. The former JointCommission Vice President for Accreditation FieldOperations, J. Cappiello recently identified hospi-tals as “critical to the survival and sustainability ofthe community during times of disaster…becausehospitals may be the most fortified structure in thecommunity”.20 Hospitals are able to use emer-gency generators for power and climate controland normally maintain stockpiles of food andmedication. Buttressing this belief, 2008 standardsby The Joint Commission explicitly require hospi-tals to adopt a “96-hour” stand-alone rule (Ele-ment of Performance: EM.02.01.01- 3), where eachcritical access hospital must carefully identify its“stand-alone” capability, should the communityservices and primary supply chains be disruptedor unavailable.
Important shelter-in-place strategies shouldinclude contingency planning for (1) food andwater; (2) medical, nonmedical, and pharmacologi-cal supplies; (3) communication systems; (4) redun-dant and resilient infrastructure; and (5) informationmanagement procedures during “downtime.”
Food stockpiling, both which items to store andhow much, should be carefully considered becausefood preparation equipment may be adverselyaffected by the event. Also, items in the stockpilemust meet the nutritional and developmental needsof all ages including formula for infants and tablefood for toddlers. Specific medical and nonmedicalsupplies were previously mentioned; however,where to store disaster supplies and issues ofemergency access should be carefully considered.Telecommunication systems are jugular to anyemergency response. Investing in redundant tele-communication systems decreases the likelihood ofa complete failure. A strategy used at Children'sHospital Boston is to have 2 different telephonesystems: traditional landline based and voice-overinternet protocol telephone systems. Combined,these 2 systems greatly reduce the likelihood of acomplete telecommunication failure. This redun-dant system strategy can be replicated for othermission critical systems such as potable water,electrical power, and reverse osmosis water filtra-tion system (provided that your institution needssuch a system to provide dialysis care). Forhospitals that are migrating toward computer-

226 VOL. 10, NO. 3 • PEDIATRIC ASPECTS OF HOSPITAL PREPAREDNESS / MONTEIRO ET AL.
based documentation, considerations for alternateor “down-time” procedures must be created, shouldthese electronic systems become inaccessible.Paper-based documentation forms and proceduresshould be well understood and easily accessible,even if the institution is committed to migrating toan online medical record.
By acknowledging the potential emotional andphysical vulnerability of pediatric victims, plan-ning efforts will consider the mental health andsecurity implications of caring for children. Speci-fically, by providing (1) specific pediatric HICSroles (Family Care Unit Leader, Psychosocial UnitLeader, etc), (2) enhanced security, (3) pediatricand “safe” shelters, children are more protectedthroughout a shelter in place response. FamilyCare Unit leaders can assist families by providingupdates and serving in reunification efforts for lostor missing children. Psychosocial responders (eg,psychologist, social workers, child life specialists)can also be useful in reducing fear and anxiety forpediatric victims. Enhanced security trackingsystems can assist by limiting access to disastervictims. This is important because the number ofon-hand security officers will likely not meet thedemand caused by the disaster. Automated dooraccess systems, surveillance cameras, and alarmsall serve to help segregate and protect thevulnerable pediatric population while they arereceiving care or awaiting reunification. Lastly,not all pediatric victims seeking shelter aremedically injured. Plans for creating “safe” shelterconditions for uninjured children should also bedeveloped. This is an area where hazards havebeen removed and age-appropriate toys andresources are available.
EVACUATIONEvacuation remains the final option for hospitals
unable to function during and following a disaster.Over the last 5 years, numerous hospitals havebeen forced to partially or completely evacuatetheir patient population. Irrespective of the causefor evacuation, there are many risks associatedwith moving hospital patients. Preplanning forevacuation routes is essential. Identifying appro-priate receiving facilities, security concerns, andfamily reunification all increase the complexity ofevacuating children.
Universal recommendations for evacuation plan-ning include mobilizing transportation resourcesin advance. This can be facilitated by creating acomprehensive evacuation memorandum of under-standing with local and regional emergency ser-
vices providers. One challenge of transferringpediatric patients is that there are limited num-bers of pediatric facilities compared with adulttertiary care centers (pediatric to adult hospitalratio: 75:4000). By understanding the regionalpediatric capabilities, standard “distance-from-facility” mapping of potential receiving facilitiescan be developed. This reference would summar-ize the type and resource care capability bypediatric specialty in a region and be depicted bydistance from the evacuation site (ie, 50-, 100-,and 150+-mile radius).
To ensure pediatric patients are transferred to theappropriate acute care facilities, a new evacuationconcept is being tested at Children's HospitalBoston. This matrix uses a modified currentinpatient acuity early-warning assessment tool21
and cross references these scores to potentialpediatric receiving facilities based on their capabil-ity. Although in draft form, this tool may enable staffto quickly assign potential evacuees to appropriatereceiving facilities using data that is collectedcontinuously in real time.
Other pediatric challenges for evacuationinclude lack of small child evacuation devicesand the increased number of services and special-ties that are necessary when attempting toprovide age-appropriate care during an evacua-tion. For example, Sled-like evacuation devicesare designed for adolescent and large children;however, they are not ideal for toddlers and infants.Depending on the age and the ability of theevacuee to understand the evacuation event, age-appropriate explanations must be provided con-stantly. The use of child life specialists andpediatric-trained psychosocial responders canhelp an evacuating pediatric patient cope withpotential fears and confusion associated with theevent. Increased security is necessary becausechildren are at higher risk for unintentionalseparation from a parent or guardian. Althoughextremely challenging, tracking children through-out the evacuation process is essential becausechildren may not be able to identify themselves orfamily members.
In every evacuation plan, there is a smallsegment of pediatric patients that cannot followthe standard plan. For example, patients withcystic fibrosis who harbor Burkholderia dolosa shouldbe directly transported. Ideally, this group ofpatients should be cohorted to decrease spread toother cystic fibrosis patients. Immunocompromisedpatients should also be directly transported to thereceiving facilities. Patients who are currentlyreceiving life-saving care such as extracorporeal

PEDIATRIC ASPECTS OF HOSPITAL PREPAREDNESS / MONTEIRO ET AL. • VOL. 10, NO. 3 227
membrane oxygenation and high-frequency venti-lation will need specialized protocols and resourcesfor transfer.
ALTERED STANDARDS OF CAREAltered standards of care (ASC) is a topic of
concern for many public health officials and healthcare providers. The failure to create a plan toaddress ASC will result in the perception of unjustallocation of resources, or actual unjust alloca-tions.22 The Massachusetts Department for PublicHealth guidelines for the development of ASCinclude (1) maximize positive patient outcomeswhen health care needs exceed available resourcesand (2) establish principles and guidelines to assisthealth care providers to continue to provide care inan ethical manner during circumstances that makedelivery of [normal] health care…difficult, if notimpossible.23 A summary of specific ASC sugges-tions was outlined by a task force assembled by theAmerican College of Chest Physicians. The taskforce organized their suggestions into categoriesincluding (1) optimizing surge capacity, (2) medicalresources, and (3) a framework for allocation ofscarce resources in mass critical care.22 Althoughwork on developing comprehensive pediatric-altered care standards for hospitals has begun,significant gaps still exist.
SUMMARYChildren are among the most vulnerable popula-
tions effected by disasters. Once a community hasbeen impacted, the opportunities to build pediatriccapabilities in a “just in time” fashion will beseverely limited. The most successful planningefforts will include the needs of children and buildon daily operational strategies. Hospital-based plan-ning must anticipate and respond to the uniqueaspects of pediatric emergency preparedness.
ACKNOWLEDGMENTSThis work was supported in part by Emergency
Medical Services for Children Targeted Issue grantH34MC10575. Supported in part byHealthResourcesand Service Administration (EMSC Targeted Issues)Grant # H34MC10575.
REFERENCES1. Levi J, Vitner S, St. Laurent R, et al. Protecting the public's
health from diseases, disasters, and bioterrorism. In: Readyor Not? Washington, DC: Trust for America's Health & RobertWood Johnson Foundation; 2008. p. 121.
2. Richardson L. Report finds economic crisis hurting U.S.preparedness for health emergencies. Trust for America'sHealth; 2009. Available at: http://healthyamericans.org/newsroom/releases/?releaseid=150. Accessed 6/19/09.
3. Institute of Medicine Committee on the Future of EmergencyCare in the United States Health System. Emergency care forchildren: growing pains. Future of emergency care. Washing-ton, DC: National Academies Press; 2007.
4. Qureshi K, Gershon RR, Sherman MF, et al. Health careworkers' ability and willingness to report to duty duringcatastrophic disasters. J Urban Health 2005;82:378-88.
5. Schultz CH, Stratton SJ. Improving hospital surge capacity: anew concept for emergency credentialing of volunteers. AnnEmerg Med 2007;49:602-9.
6. American Academy of Pediatrics, Committee on PediatricEmergency Medicine. Care of children in the emergencydepartment: guidelines for preparedness. Pediatrics 2001;107:777-81.
7. Association for Healthcare Resource and Materials Manage-ment. Medical-Surgical Supply Formulary By Disaster Sce-nario. Available at: http://www.ahrmm.org/ahrmm/news_and_issues/issues_and_initiatives/files/disaster_formularies.pdf. Accessed 6/19/09.
8. Farmer CJ. Are you prepared. In: Mokke J, editor. Chapter 3,Communicating during emergencies. Hospital EmergencyManagement Guidebook. Oakbrook Terrace (Ill): JointCommission Resources; 2006. p. 61.
9. Roberts M, Hodge J, Gabriel E, et al. In: Sally RN, Phillips J,Knebel A, editors. Alternative care sites in mass medical carewith scarce resources: a community planning guide. Rock-ville (Md): Agency for Healthcare Research and Quality;2007. p. 75-100.
10. Powell T. Carrots and sticks: keeping healthcareworkers on thejob in a public health disaster. Am J Bioethics 2008;8:20-1.
11. Moussa CB, Chant A, Wagner P, et al. Disaster Service WorkerVolunteer Program Guidance; 2001.
12. AcademyHealth, Bioterrorism and Health System Prepared-ness, Issue Brief No. 3 - Optimizing Surge Capacity: HospitalAssessment and Planning. Rockville (Md): Agency forHealthcare Research and Quality; 2004. p. 4.
13. Barbera JA, Macintyre AG. Medical surge capacity andcapability: a management system for integrating medicaland health resources during large-scale emergencies. Alex-andria: U.S. Department of Health andHuman Services; 2004.
14. Auf der Heide E. The importance of evidence-based disasterplanning. Ann Emerg Med 2006;47:34-49.
15. Seidel J, Tittle S, Hodge D, et al. Guidelines for pediatricequipment and supplies for emergency departments. Com-mittee on Pediatric Equipment and Supplies for EmergencyDepartments. National Emergency Medical Services forChildren Resource Alliance. J Emerg Nurs 1998;24:45-8.
16. Illinois Emergency Medical Services for Children Program.Pediatric disaster preparedness checklist—resourceguide. Available at: http://www.luhs.org/depts/emsc/disaster_preparedness/checklist_resources_website.doc; 2008.Accessed 6/19/09.
17. Hick JL, Hanfling D, Burstein JL, et al. Health care facility andcommunity strategies for patient care surge capacity. AnnEmerg Med 2004;44:253-61.
18. The Centers for Bioterrorism Preparedness (CBPP) PediatricTask Force. Children in disasters: hospital guidelines forpediatric preparedness. New York City Department of Healthand Mental Hygiene. Available at: http://www.nyc.gov/html/doh/downloads/pdf/bhpp/hepp-peds-childrenindisasters-010709.pdf; 2008. Accessed 6/19/09.

228 VOL. 10, NO. 3 • PEDIATRIC ASPECTS OF HOSPITAL PREPAREDNESS / MONTEIRO ET AL.
19. Syrett JI, Benitez JG, Livingston WH, et al. Will emergencyhealth care providers respond to mass casualty incidents?J Healthnc Proc Manage 2007;23:27-40.
20. Cappiello J, O'Toole E. Moving into 2008 and beyond the newJoint Commission standards—some practical advice andstrategies to make your organization resilient. Des Moines(Iowa): Simulation Services, Inc; 2008[cited 2009 March26]. Available at: http://www.simulationed.com/resources/wp_ emergencyreadiness2008_colour_print.pdf. Accessed6/19/09.
21. Duncan H, Hutchison J, Parshuram CS. The Pediatric EarlyWarning System score: a severity of illness score to predict
urgent medical need in hospitalized children. J Crit Care2006;21:271-8.
22. Devereaux AV, Dichter JR, Christian MD, et al. Definitive carefor the critically ill during a disaster: a framework forallocation of scarce resources in mass critical care: from aTask Force for Mass Critical Care summit meeting, January26-27, 2007, Chicago, IL. Chest 2008;133(5 Suppl):51S-66S.
23. Guidelines for the development of altered standards of carefor influenza pandemic (Draft2007). Massachusetts Depart-ment of Public Health. Available at: http://www.mass.gov/Eeohhs2/docs/dph/emergency_prep/asc_guidelines_draft.pdf. Accessed 6/19/09.