Embed Size (px)
Citation preview

Pectoralis major rupture in the elderly
Clinical and sonographic findings
Yichayaou Belooseskya,*, Joseph Grinblata, Miriam Katzb,David Hendelc, Rochelle Sommerb
aDepartment of Geriatrics, Rabin Medical Center, Beilinson Campus, Sackler School of Medicine, Tel Aviv University, Tel Aviv, IsraelbDepartment of Imaging, Rabin Medical Center, Golda Campus, Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel
cDepartment of Orthopedics, Rabin Medical Center, Golda Campus, Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel
Abstract
We describe clinical and sonographic features of pectoralis major rupture in the elderly, which is relatively rare and unknown.
Patients presented with a large pectoral ecchymosis extending to the axilla, chest wall, breast and arm. The pectoral area was sensitive,
sometimes with a visible and palpable defect in the axilla. Ultrasound examination showed a large hypoechoic, well-circumscribed
structure representing a hematoma within the pectoralis major muscle, partially replacing the normal echo muscle pattern.
Ultrasonography is a useful, low cost diagnostic tool, and is recommended in the investigation of pectoralis major rupture in the elderly.
D 2003 Elsevier Inc. All rights reserved.
Keywords: Pectoralis major rupture; Ultrasonography; Elderly
1. Introduction
Pectoralis major rupture is an uncommon injury occur-
ring in male athletes and manual laborers, mainly between
the ages of 20–40. Approximately 150 cases have been
reported in the literature [1,2]. The injury mechanism is
most commonly indirect, resulting from sudden forceful
overload applied to a maximally contracting muscle [3], or
less commonly by direct trauma [2]. Whereas excessive
muscle tension causes avulsions from insertion on the
humerus or rupture at the musculo-tendinous junction, direct
trauma causes tears in the muscle belly [1]. Recently, we
reported pectoralis major rupture in nursing home patients
occurring during common nursing procedures such as
positioning and transferring [4]. When a frail patient is held
by or under the axillary region, rapid transfer can cause a
brisk tearing movement to a stiff and atrophic pectoral
muscle, resulting in severe force being applied to the
pectoral muscle. Direct trauma to the muscle must also be
considered, either as a result of abuse or when a patient is
turned accidentally into a bed rail. To our knowledge, the
ultrasonographic (US) findings of pectoralis major rupture
in elderly patients have not been described. We therefore
report the clinical and US findings of four affected patients.
2. Materials and methods
During 1998 to May 2002, we diagnosed 13 cases of
pectoralis major rupture. In four patients, US was done. The
patients were female aged 73, 87 and 97, respectively, and
an 83-year-old man. The first was an independent housewife
whose chest and shoulder were accidentally crushed by a
pneumatic bus door. The second and the fourth were fully
dependent and demented nursing home residents whose
chest hematomas were discovered while changing their
clothes. The third was a partially dependent, obese, cogni-
tively normal woman who was hospitalized for functional
deterioration and weakness followed by anemia and increas-
ing heart failure. On admission, a large ecchymosis of the
right pectoral area was found, secondary to a partial pector-
alis major rupture probably due to inadequate care. All
patients were hospitalized in the geriatric department and
had undergone extensive evaluations including orthopedic
0899-7071/03/$ – see front matter D 2003 Elsevier Inc. All rights reserved.
doi:10.1016/S0899-7071(02)00548-X
* Corresponding author. Department of Geriatrics, Rabin Medical
Center, Beilinson Campus, Petach Tikvah 49100, Israel. Tel.: +972-3-937-
6820; fax: +972-3-937-6817.
E-mail address: [email protected] (Y. Beloosesky).
Journal of Clinical Imaging 27 (2003) 261–264
examinations. The US images were obtained and interpreted
by senior radiologists (R.S. and M.K.) using an ATL 3000
ultrasound machine with a 5– 10-mHz linear probe
(Advanced Technological Laboratories, Bothell, WA,
USA). The examination included scanning all soft tissues
including the subcutaneous fat and the pectoralis muscle as
far as the ribs posteriorly. The contralateral nonaffected side
was compared in each patient.
3. Results
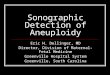
All patients suffered pain, increasing on palpation of the
pectoralis area, necessitating analgesic and careful care. A
large pectoral bulging hematoma and an ecchymosis
extending to the axilla, chest wall and breast were found
(Figs. 1 and 2). The amounts of blood loss calculated by
subtracting the pre-injury with the post-injury hemoglobin
level were 2.6, 2.2, 1.7 and 4.6 g/dl, in the first, second,
third and fourth patients, respectively. Three patients were
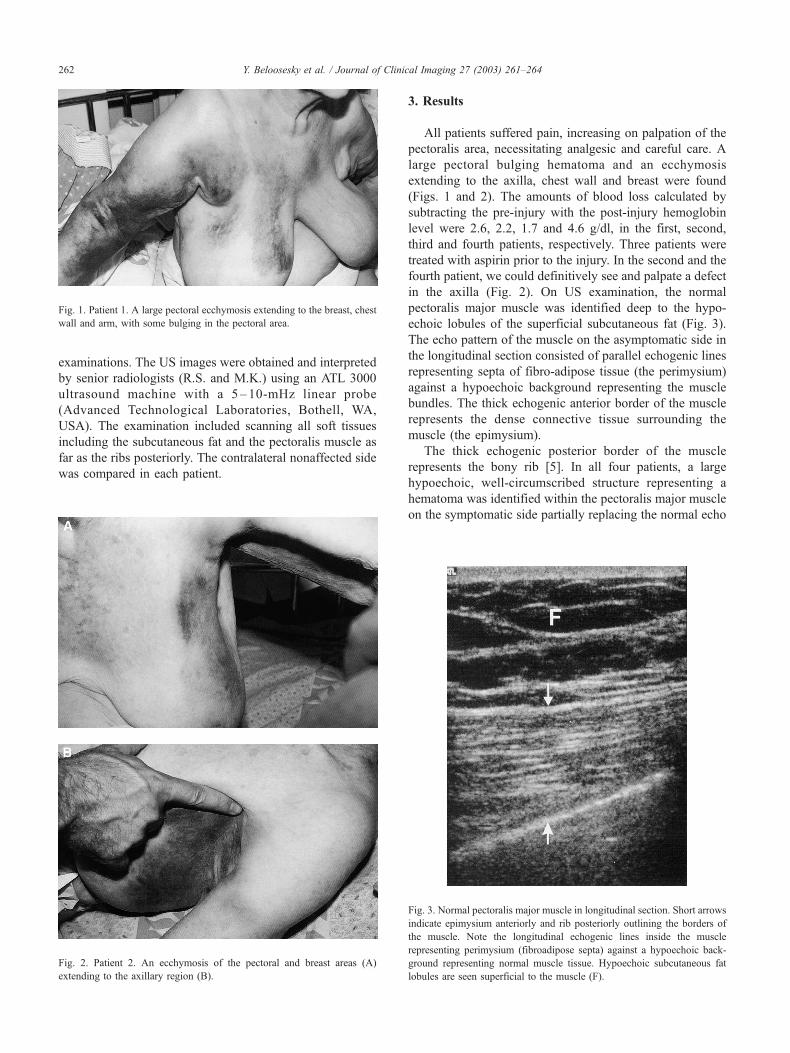
treated with aspirin prior to the injury. In the second and the
fourth patient, we could definitively see and palpate a defect
in the axilla (Fig. 2). On US examination, the normal
pectoralis major muscle was identified deep to the hypo-
echoic lobules of the superficial subcutaneous fat (Fig. 3).
The echo pattern of the muscle on the asymptomatic side in
the longitudinal section consisted of parallel echogenic lines
representing septa of fibro-adipose tissue (the perimysium)
against a hypoechoic background representing the muscle
bundles. The thick echogenic anterior border of the muscle
represents the dense connective tissue surrounding the
muscle (the epimysium).
The thick echogenic posterior border of the muscle
represents the bony rib [5]. In all four patients, a large
hypoechoic, well-circumscribed structure representing a
hematoma was identified within the pectoralis major muscle
on the symptomatic side partially replacing the normal echo
Fig. 1. Patient 1. A large pectoral ecchymosis extending to the breast, chest
wall and arm, with some bulging in the pectoral area.
Fig. 2. Patient 2. An ecchymosis of the pectoral and breast areas (A)
extending to the axillary region (B).
Fig. 3. Normal pectoralis major muscle in longitudinal section. Short arrows
indicate epimysium anteriorly and rib posteriorly outlining the borders of
the muscle. Note the longitudinal echogenic lines inside the muscle
representing perimysium (fibroadipose septa) against a hypoechoic back-
ground representing normal muscle tissue. Hypoechoic subcutaneous fat
lobules are seen superficial to the muscle (F).
Y. Beloosesky et al. / Journal of Clinical Imaging 27 (2003) 261–264262

pattern. In the first patient, the hematoma was situated deep
inside the muscle, also demonstrating obvious posterior
enhancement indicating the fluid nature of the structure
(Fig. 4). In the second patient, a large expansive hematoma
involving almost the whole width of the muscle was
demonstrated (Fig. 5). The same patient showed an ill-
defined similar hypoechoic structure in the subcutaneous
fat, indicating an additional hematoma in the superficial soft
tissue (Fig. 6).
4. Discussion
The pectoralis major is a broad, thick muscle ranging
from the anterior thorax to the clavicle. The fibers converge
like a fan into three laminae that twist upon each other at 90�before coalescing into a single tendon of insertion. The
fibers of the anterior laminae (clavicular head) arising from
the clavicle and upper sternum, remain parallel as they
course toward the humeral insertion. The manubrial portion
of the sternal head makes up the bulk of the muscle, arising
from the midportion of the sternum and the coastal cartilage
of ribs 1 through 5. The lower or abdominal portion of the
sternal head arises from ribs 5 and 6 and fascia of the
external oblique and transversal muscles. The manubrial and
abdominal portions become the middle and posterior lam-
inae, which coil upon each other so that the abdominal
fibers insert highest on the humerus, while the manubrial
fibers insert inferiorly [2,6].
Muscle rupture is caused by two different mechanisms:
(a) most commonly by distraction (indirect trauma) and (b)
less commonly by compression (direct trauma). In distrac-
tion injury, the muscle fibers are torn as a result of an
intrinsic force generated from sudden forceful overload
applied to a maximally contracting muscle [3,5]. This is
apparently the mechanism of the rupture in the second, third
and fourth cases. In compression injuries, as in the first case
(the closing bus door), the muscle is crushed against the
bone by external force. Muscle fibers are macerated along
with associated vessels leading to hematoma formation.
Healing is slow with extensive scar formation and long-
term functional deficit [5].
Fig. 4. Patient 1. Partial rupture of pectoralis major muscle. Large well-
defined hypoehoic structure with posterior enhancement representing fresh
hematoma situated deep inside the muscle (long arrow). Normal muscle
tissue is seen anterior to the hematoma (M).
Fig. 5. Patient 2. Partial rupture of pectoralis major muscle involving almost
the whole width of the muscle. Well-circumscribed hypoechoic hematoma
within the muscle (long arrow), with posterior enhancement. Arrowheads
indicate anterior border of the muscle. Echogenic posterior border of the
muscle represents a rib (R).
Fig. 6. Patient 2. Superficial hematoma. Irregular hypoechoic structure with
posterior enhancement in subcutaneous fat representing fresh hematoma
(long arrow).
Y. Beloosesky et al. / Journal of Clinical Imaging 27 (2003) 261–264 263

Age related changes in skeletal muscles might increase
the probability of injury. Older muscles have an increased
susceptibility to contraction induced mechanical injuries.
Beginning in middle age or earlier, there is a decrease in the
number and size of muscle cells, resulting in a loss of mass
and strength [7]. In young patients and in complete tears,
surgery is recommended to restore full strength and function
and to resume athletic activity in individuals who require
full use of their upper extremities. MR imaging allows
accurate evaluation of injuries and enables identification
of patients who would benefit from surgical repair [8].
However, the functional limitation of the muscle rupture is
not of great concern among the elderly. Therefore, US
images, as shown in this study, are sufficient in the elderly
in the diagnosis of pectoralis major injury. US is more
readily available than MRI, less costly and can be performed
in the patient’s room. Moreover, US is a simple quick
diagnostic method, does not require the older patient to lie
still in a narrow cylinder and is not contraindicated in the
presence of ferromagnetic implants and splints, and thus is
the ideal imaging technique for elderly patients. Although
infected hematoma has rarely been described in cases of
pectoralis major rupture [9], the US modality can be very
useful in guiding needle aspiration and for follow-up if such
a complication is suspected.
Ultrasound is most frequently used in traumatic and
inflammatory disorders in which a non-invasive method is
greatly appreciated by the patient [10]. Acute hematomas
present differently depending on their age. Initially, they
are seen as hypoechoic areas within the muscle (indic-
ating muscle fiber ruptures), and remain hypoechoic as
hemolysis proceeds. Subsequently, they develop internal
echoes of increasing complexity as they became more
organized [10]. Ultrasound was found to be very useful in
diagnosing other muscular injuries such as rectus sheath
hematoma [11]. This unusual but well-described entity
shares some similarities with the pectoralis major rupture
in the elderly. In both cases, there is frequently a
background of cardiovascular disease and use of anti-
coagulant or anti-aggregate agents, precipitating factors
such as sudden exertion and direct trauma, the presence
of pain and mass, and finally hematocrit decrease sec-
ondary to the bleeding.
In conclusion, these cases demonstrate that ultrasonog-
raphy is a useful, readily available, low cost diagnostic tool,
recommended in investigating pectoralis major rupture in
the elderly.
References
[1] Bak K, Cameron EA, Henderson IJP. Rupture of the pectoralis major:
a meta-analysis of 112 cases. Knee Surg, Sports Traumatol, Arthrosc
2000;8:113–9.
[2] Travis RD, Doane R, Burkhead WZ. Tendon ruptures about the
shoulder. Orthop Clin North Am 2000;31:313–30.
[3] Berson BL. Surgical repair of pectoralis major rupture in an athlete.
Am J Sports Med 1979;7:348–51.
[4] Beloosesky Y, Hendel D, Weiss A, Rosenberg PH, Grinblat J. Pector-
alis major rupture in nursing home resident. Am J Med 2001;111:
233–5.
[5] Holsbeeck MV, Introcaso JH. Musculoskeletal ultrasound. St. Louis:
Mosby-Year Book, 1991.
[6] Wolfe SW, Wickiewicz TL, Cavanaugh JT. Rupture of the pectoralis
major muscle. An anatomic and clinical analysis. Am J Sports Med
1992;20:587–93.
[7] Buckwalter JA, Woo SL, Goldberg VM, et al. Soft tissue aging and
musculoskeletal function. J Bone Jt Surg Am 1993;75:1533–48.
[8] Connell DA, Potter HG, Sherman MF, Wickiewicz TL. Injuries of the
pectoralis major muscle: evaluation with MR imaging. Radiology
1999;210:785–91.
[9] Chapple K, Kelty C, Irwin LR, Millner PA. Traumatic abscess of
pectoralis major. Arch Orthop Trauma Surg 2000;120:479–81.
[10] O’Keeffe D, Mamtora H. Ultrasound in clinical orthopedics. J Bone Jt
Surg Br 1992;74-B:488–94.
[11] Moreno Gallego A, Aguayo JL, Flores B, et al. Ultrasonography and
computed tomography reduce unnecessary surgery in abdominal rec-
tus sheath haematoma. Br J Surg 1997;84:1295–7.
Y. Beloosesky et al. / Journal of Clinical Imaging 27 (2003) 261–264264