Embed Size (px)
Citation preview
7
Neurological Office Procedures; Editor in Chief, Karen L. Roos, M.D.; Guest Editor, Karen L. Roos, M.D. Seminars in Neurology, Volume 23,Number 1, 2003. Address for correspondence and reprint requests: Omkar N. Markand, M.D., Indiana University School of Medicine, 550North University Blvd., Room 1711, Indianapolis, IN 46202. 1Department of Neurology, Indiana University School of Medicine, Indianapolis,Indiana. Copyright © 2003 by Thieme Medical Publishers, Inc., 333 Seventh Avenue, New York, NY 10001, USA. Tel: +1(212) 584-4662. 0271-8235,p;2003,23,01,007,046,ftx,en;sin00226x.
Pearls, Perils, and Pitfalls in the Use of the ElectroencephalogramOmkar N. Markand, M.D., F.R.C.P.C.1
ABSTRACT
Despite advances in neuroimaging techniques over the past three decades thathave helped in identifying structural lesions of the central nervous system, electroen-cephalography (EEG) continues to provide valuable insight into brain function bydemonstrating focal or diffuse background abnormalities and epileptiform abnormalities.It is an extremely valuable test in patients suspected of epilepsy and in patients with al-tered mental status and coma. Patterns in the EEG make it possible to clarify the seizuretype; it is indispensable for the diagnosis of nonconvulsive status epilepticus and for sepa-rating epileptic from other paroxysmal (nonepileptic) episodes. There are EEG patternspredictive of the cause of the encephalopathy (i.e., triphasic waves in metabolic en-cephalopathy) or the location of the lesion (i.e., focal polymorphic delta activity in lesionsof the subcortical white matter). The various EEG characteristics of infantile, childhood,and adult epilepsies are described as well as the EEG patterns that are morphologicallysimilar to interictal/ictal epileptiform discharges but unrelated to epilepsy. An EEG ismost helpful in determining the severity and, hence, the prognosis of cerebral dysfunc-tion. Lastly, EEG is extremely helpful in assessing normal or abnormal brain functioningin a newborn because of the serious limitation in performing an adequate neurologic ex-amination on the neonate who is intubated or paralyzed for ventilatory control. Undersuch circumstances, the EEG may be the only available tool to detect an encephalopathicprocess or the occurrence of epileptic seizures.
KEYWORDS: Electroencephalogram, normal and variant EEG findings, epilepsy,encephalopathies, neonatal EEG, status epilepticus
Objectives: Upon completion of this article, the reader will understand “normal abnormalities” in the normal EEG, the EEG in en-cephalopathies, the proper identification of diagnostic epileptiform abnormalities, the classic patterns of infantile childhood andadult epilepsies, the EEG patterns morphologically similar to interictal/ictal epileptiform discharges but unrelated to epilepsy, andneonatal EEG abnormalities.Accreditation: The Indiana University School of Medicine is accredited by the Accreditation Council for Continuing Medical Educa-tion to provide continuing medical education for physicians.Credit: The Indiana University School of Medicine designates this educational activity for a maximum of 1.0 hours in category onecredit toward the AMA Physicians Recognition Award. Each physician should claim only those hours of credit that he/she actuallyspent in the educational activity.Disclosure: Statements have been obtained regarding the author’s relationships with financial supporters of this activity. There is noapparent conflict of interest related to the context of participation of the author of this article.
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.

8 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003
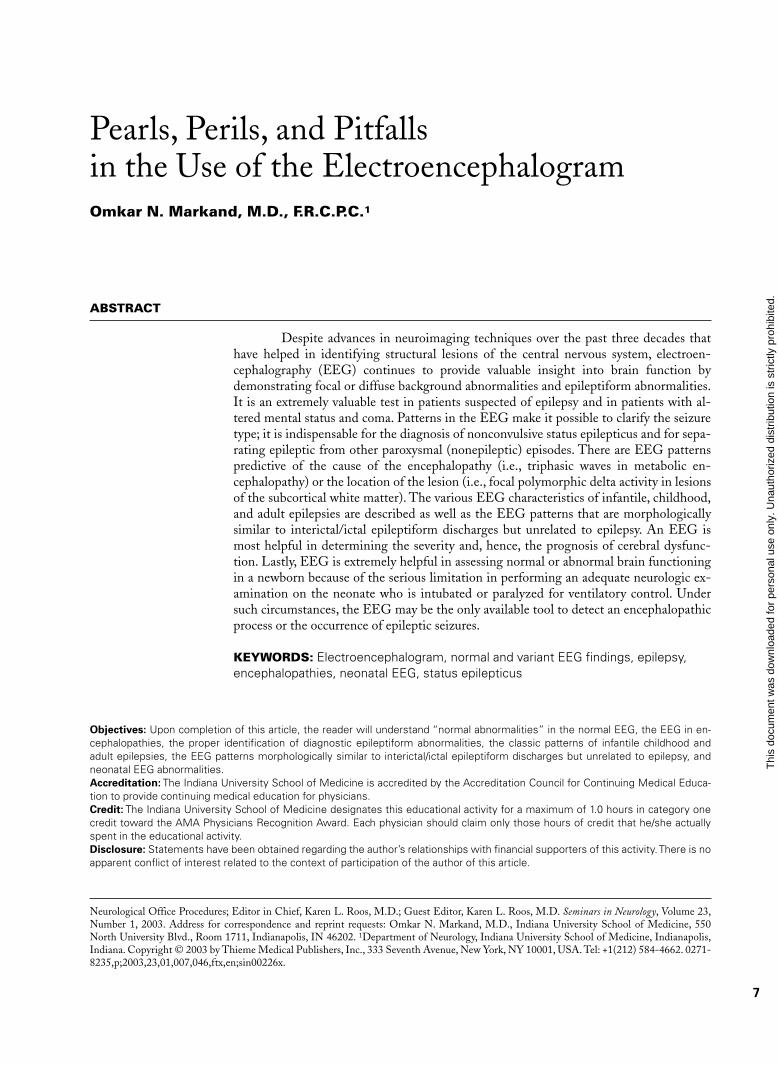
preters inexperienced with children’s EEGs (Fig. 1).Similarly, positive occipital sharp transients(POSTs), when high in amplitude and sharp in con-figuration, can be easily misinterpreted as abnormalspikes, especially in linkages where occipital elec-trodes are connected to input terminal 2 (grid 2) ofthe amplifier (e.g., “double banana run”).
4. In a small proportion of normal adult subjects,clearly identifiable and countable alpha rhythm maybe entirely absent. The background may consist of ir-regular mixtures of low amplitude (<20 µV) activi-ties, mostly from 5.0 to 30.0 cps without a dominantfrequency. Such low-voltage EEGs have been stud-ied in detail.2 The EEG is reactive to various physio-logic stimuli such as sleep, drugs, and pathologic pro-cesses. In over half of the patients with low-voltageEEGs, hyperventilation may bring out an alpharhythm. During sleep, normal activities such as ver-tex sharp transients and sleep spindles may be gener-ated. It is essential that low-voltage tracings beclearly distinguished from EEGs showing electro-cerebral inactivity, which have a grave prognosis.These EEGs lack reactivity and lability, and with in-creased instrumental sensitivities show no electricalactivity of cerebral origin. Low-voltage EEGs aregenerally considered to be a normal variant occurringin 7 to 10% of normal subjects over the age of 20years. The low-voltage EEG does not correlate withneurologic or psychiatric disease.
5. Changes in the EEG during normal senescence hasbeen described in detail.3–5 The most frequent changeis the slowing of the alpha frequency. By the age of 70years, the mean alpha frequency decreases to 9.0 to9.5 cps and decreases further to 8.5 to 9.0 cps beyondthe age of 80 years. In healthy elderly subjects, even ator over the age of 100 years, the frequency of thealpha rhythm remains well above 8.0 cps.6,7 There-fore, an average alpha frequency of less than 8.0 cpsmeasured with the patient fully alert must be consid-ered abnormal in elderly patients at all ages.
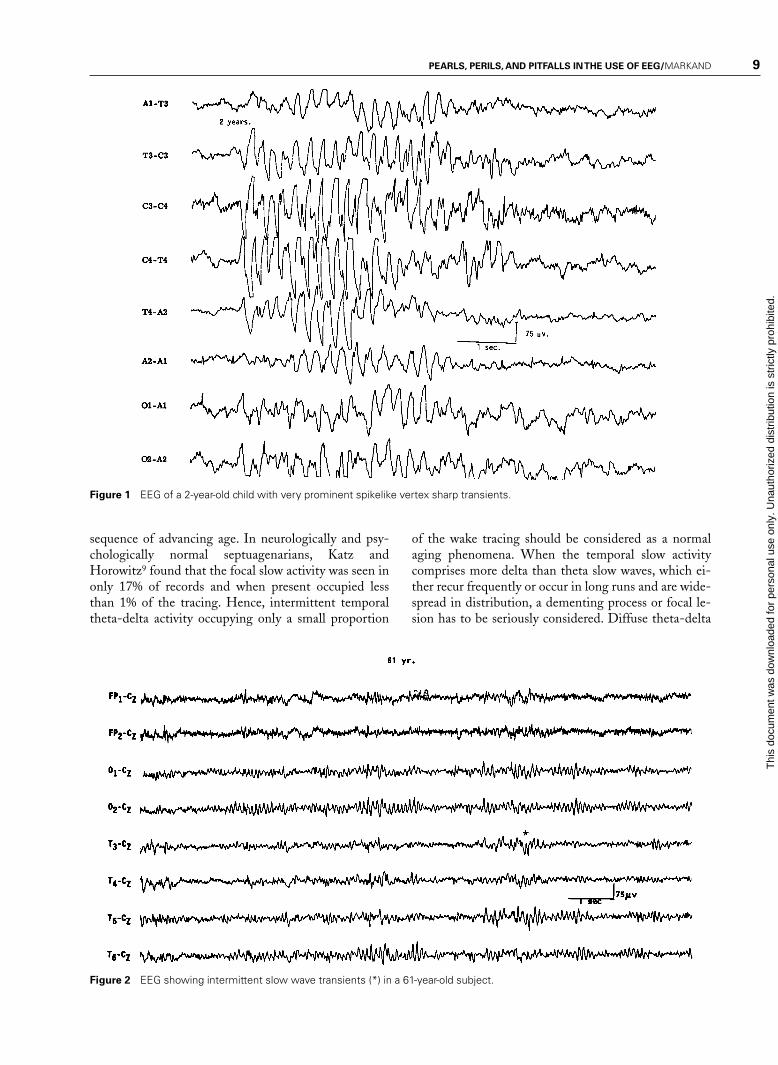
Another EEG finding is the presence of isolatedtransients of irregular focal slowing in the theta-deltafrequency range over the anterior temporal region, re-ported in 40% of healthy elderly subjects.4,5,8 They aremost frequent over the left temporal area particularlyduring drowsiness (Fig. 2). Sometimes poorly definedsharp waves are interspersed with focal slow compo-nents. The left-sided accentuation of this activity re-mains unexplained. Such intermittent slow activity,with or without sharp components over the temporalregion, has no correlation with intellectual or cognitivefunctioning or presence of a seizure disorder. More re-cent investigations suggest that the temporal slowing inthe awake tracing may, in fact, not be the inevitable con-
Electroencephalography (EEG) is the tech-nique of recording from the scalp the spontaneous elec-trical activity of the brain and correlating it to the un-derlying brain function. Since the first recording of ahuman EEG in 1929 by Hans Berger, improvement inelectronics and technology has made EEG one of themost widely used laboratory tests for clinical evaluationof neurologic disorders. However, in the past threedecades with continuing advances in neuroimaging,particularly magnetic resonance imaging (MRI), therole of clinical EEG has become restricted and progres-sively more focused. Its major utility at present is in theevaluation of focal and diffuse encephalopathies, co-matose conditions, epileptic disorders, and cerebral dis-orders affecting neonates and infants. The present arti-cle is not an attempt to describe EEG comprehensivelyin normal subjects and in different disease processes butto highlight its usefulness/limitation and emphasizeprecautions/care needed in its optimal utility. The sub-ject will be discussed under seven sections: EEG in nor-mal subjects, EEG in patients with altered mental sta-tus or diffuse encephalopathies, EEG in focal orlateralized cerebral hemispheric lesions, EEG in parox-ysmal disorders, EEG in generalized epilepsies, EEG inneonates, and EEG in status epilepticus.
EEG IN NORMAL SUBJECTSThe EEG in the normal awake child and adult is wellknown and needs no detailed description. The followingare points of emphasis:
1. Alpha rhythm in the two hemispheres is very similarin frequency. A consistent difference of even 0.5 to1.0 cps on the two sides is significant; the side show-ing a slower frequency may have a hemispheric dys-function. Amplitude asymmetry is of relatively lesssignificance, unless the asymmetry is prominent. Ingeneral, the alpha rhythm is higher in amplitude overthe right hemisphere. If the amplitude of the alpharhythm on the right side is more than 11⁄2 times thaton the left side, the asymmetry is usually regarded assignificant. When the alpha rhythm is over 25%higher in amplitude on the left side than the rightside, this constitutes a significant asymmetry.1
2. Significant theta activity (4 to 7 Hz) is present in theEEG of children and adolescents. Delta activity inthe awake tracing is rarely seen after the age of 5years. A common EEG pattern in adolescents is thepresence of intermittent delta waves intermixed withalpha rhythm over the posterior head regions, the so-called “slow waves of youth.”
3. The EEG during non-rapid eye movement(NREM) sleep in children shows very prominentspikelike vertex sharp transients, which are oftenmistaken for epileptiform activity by EEG inter-
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
PEARLS, PERILS, AND PITFALLS IN THE USE OF EEG/MARKAND 9
Figure 2 EEG showing intermittent slow wave transients (*) in a 61-year-old subject.
Figure 1 EEG of a 2-year-old child with very prominent spikelike vertex sharp transients.
sequence of advancing age. In neurologically and psy-chologically normal septuagenarians, Katz andHorowitz9 found that the focal slow activity was seen inonly 17% of records and when present occupied lessthan 1% of the tracing. Hence, intermittent temporaltheta-delta activity occupying only a small proportion
of the wake tracing should be considered as a normalaging phenomena. When the temporal slow activitycomprises more delta than theta slow waves, which ei-ther recur frequently or occur in long runs and are wide-spread in distribution, a dementing process or focal le-sion has to be seriously considered. Diffuse theta-delta
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.

10 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003
activity in elderly subjects are likely to occur in thosewith intellectual impairment.5
EEG IN PATIENTS WITHALTERED MENTAL STATUS OR DIFFUSE ENCEPHALOPATHIESThe term encephalopathy is usually applied to patientsdisplaying altered mental status as a result of a diffusedisturbance of brain function. Common en-cephalopathies are divided into metabolic, toxic, inflam-matory (encephalitis), anoxic, and degenerative types.The EEG in most encephalopathies shows an alterationof background activities and emergence of varying de-grees of theta-delta slowing. Remember that the EEGfindings are generally nonspecific from a differentialstandpoint. The EEG is unable to distinguish betweendifferent etiologies. The main contribution of the EEGis in providing an objective measure of severity of en-cephalopathy, prognosis, and effectiveness of therapy.10
There is a good correlation between the severityof the EEG changes, the severity of the encephalopathy,and the clinical state of the patient. In mild encephalopa-thy associated with mild clouding of consciousness andconfusion, there is at first slowing of the posterior domi-nant rhythm, which decreases from a higher to a loweralpha frequency and then into the theta frequency range.More severe encephalopathy is associated with deeperlevels of coma, and the background consists mainly ofhigh-amplitude irregular delta activity. With further de-terioration in the encephalopathy, the amplitude of allactivities drop below 20 µV and the EEG may consist ofrelatively low-amplitude, invariant delta activity. Sometracings reveal suppression-burst pattern where there isregular alternation of very-low-amplitude EEG with rel-atively higher-amplitude EEG segments. The most ex-treme type of abnormality is, of course, lack of any cere-bral activity (i.e., electrocerebral inactivity). Presence ofthe later three types of EEG patterns (invariant low-am-plitude delta, suppression-burst, and electrocerebral in-activity) carry a grave prognosis, if drug intoxication canbe excluded as the cause of encephalopathy. If due todrug intoxication, these severely abnormal patterns arequite reversible with treatment, with a high potential forcomplete recovery of neurologic functioning.
Besides the degree of background slowing, thereare two other features in the EEG that must be evalu-ated to determine the severity of encephalopathy. Theseare spontaneous variability of the EEG over several sec-onds to minutes, and reactivity to painful stimulation.In milder encephalopathies, the EEG shows sponta-neous variability during the recording period and evi-dence of EEG reactivity to painful stimulation. Whenthe EEG shows reactivity, painful stimulation com-monly results in reduction of the amplitude, increase infrequency of the background activity, and reduction in
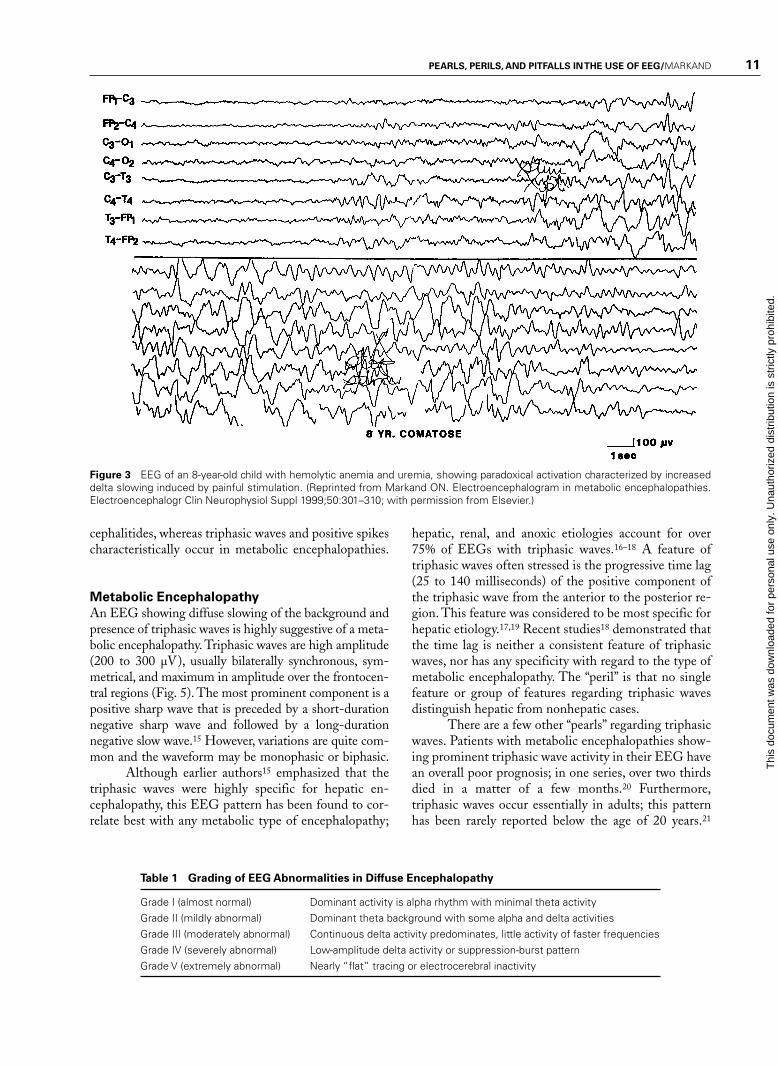
the slow activity. There is often a “paradoxical activa-tion,” which is a period of more severe delta slowing fol-lowing painful stimulation (Fig. 3). The presence of anytype of reactivity (reduction in slow activity or increasein the degree of slowing) on painful stimulation sug-gests a lower grade of encephalopathy, whereas theEEG lacking spontaneous variability (invariant EEG)and total lack of any reactivity to intense and prolongedstimulation suggests a severe degree of encephalopathy.
A grading system of EEG abnormalities inadults is shown in Table 1, similar to other rating sys-tems.11,12 It is helpful in prognosis, evaluation of effec-tiveness of therapy, and comparing serial EEG studies.The slow activities associated with an encephalopathyare usually widespread and symmetrical over the twohemispheres. In children, the slowing may predominateover the posterior hemisphere, and in adults, usuallyover the frontal areas. These are simply maturation-re-lated spatial EEG features, which do not signify thatthe encephalopathy is more severe posteriorly in chil-dren and anteriorly in adults.
It is unusual to see prominent focal or lateralizedEEG findings with a diffuse encephalopathy unless thereis an associated focal process, such as an old infarct ortumor. An exception is nonketotic hyperosmolar coma, aform of metabolic encephalopathy, which is very often as-sociated with focal clinical (e.g., focal seizures) and focalEEG findings. Herpes simplex encephalitis andCreutzfeldt-Jakob disease (in the early stages) may alsoproduce lateralized EEG slowing related to unilateralemphasis of the associated pathologic process (see below).
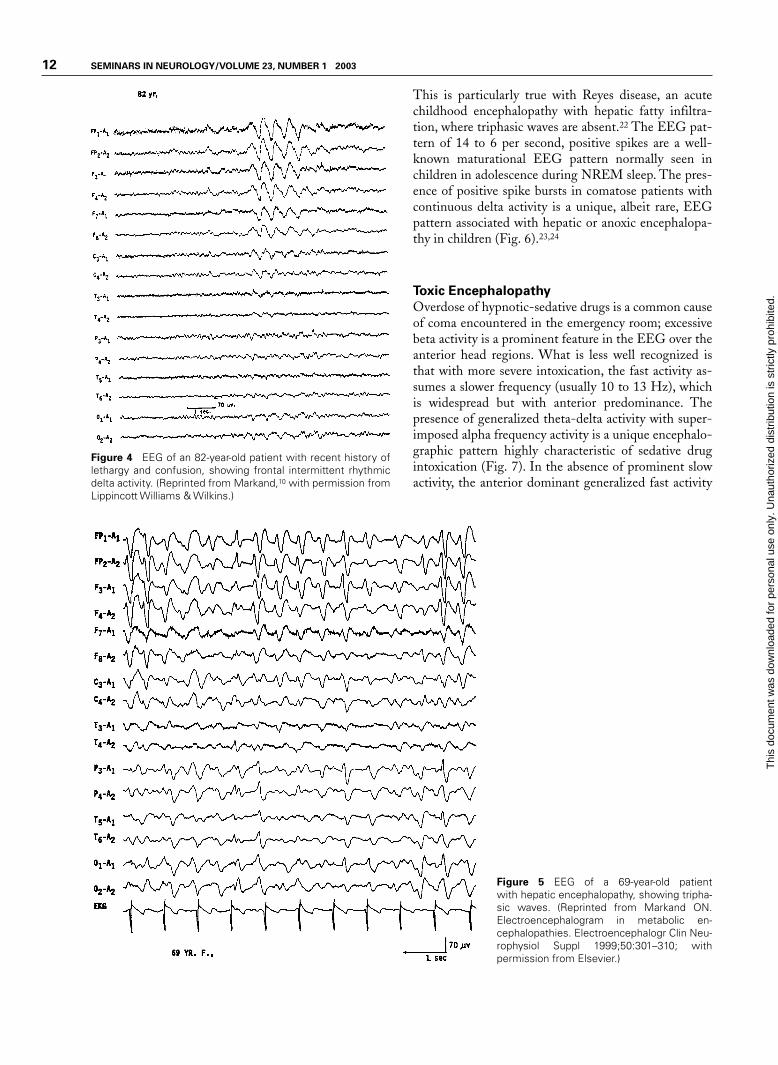
Another EEG pattern associated with a mildform of encephalopathy is the presence of bursts of in-termittent rhythmic delta activity (IRDA) superimposedon a more or less normal background activity. Depend-ing on the area of predominance, the IRDA is furtherdivided into frontal or occipital types. IRDA has beentraditionally considered a “projected rhythm” and a hall-mark of EEG findings in patients with deep midline le-sions of diencephalic, upper brain stem, or posteriorfossa locations.13 Critical evaluations subsequently havecast serious doubts on this classic concept because thisEEG pattern has been found in a large variety of patho-logical conditions and is often absent in deep midline le-sions. As a matter of fact, the most common etiology ofIRDA is a mild to moderate encephalopathy associatedwith some disturbance in consciousness (Fig. 4).14
Are there any unique or specific EEG featuresthat help narrow the differential diagnosis of diffuse en-cephalopathy and point toward a more specific etiology?There are a few EEG patterns (e.g., triphasic waves,positive spikes, and periodic complexes) that, althoughnot commonly encountered in encephalopathic pa-tients, when present suggest a specific etiology for theencephalopathy. Periodic patterns are specifically en-countered in anoxic encephalopathy and certain en-
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
PEARLS, PERILS, AND PITFALLS IN THE USE OF EEG/MARKAND 11
Figure 3 EEG of an 8-year-old child with hemolytic anemia and uremia, showing paradoxical activation characterized by increaseddelta slowing induced by painful stimulation. (Reprinted from Markand ON. Electroencephalogram in metabolic encephalopathies.Electroencephalogr Clin Neurophysiol Suppl 1999;50:301–310; with permission from Elsevier.)
cephalitides, whereas triphasic waves and positive spikescharacteristically occur in metabolic encephalopathies.
Metabolic Encephalopathy
An EEG showing diffuse slowing of the background andpresence of triphasic waves is highly suggestive of a meta-bolic encephalopathy. Triphasic waves are high amplitude(200 to 300 µV), usually bilaterally synchronous, sym-metrical, and maximum in amplitude over the frontocen-tral regions (Fig. 5). The most prominent component is apositive sharp wave that is preceded by a short-durationnegative sharp wave and followed by a long-durationnegative slow wave.15 However, variations are quite com-mon and the waveform may be monophasic or biphasic.
Although earlier authors15 emphasized that thetriphasic waves were highly specific for hepatic en-cephalopathy, this EEG pattern has been found to cor-relate best with any metabolic type of encephalopathy;
hepatic, renal, and anoxic etiologies account for over75% of EEGs with triphasic waves.16–18 A feature oftriphasic waves often stressed is the progressive time lag(25 to 140 milliseconds) of the positive component ofthe triphasic wave from the anterior to the posterior re-gion. This feature was considered to be most specific forhepatic etiology.17,19 Recent studies18 demonstrated thatthe time lag is neither a consistent feature of triphasicwaves, nor has any specificity with regard to the type ofmetabolic encephalopathy. The “peril” is that no singlefeature or group of features regarding triphasic wavesdistinguish hepatic from nonhepatic cases.
There are a few other “pearls” regarding triphasicwaves. Patients with metabolic encephalopathies show-ing prominent triphasic wave activity in their EEG havean overall poor prognosis; in one series, over two thirdsdied in a matter of a few months.20 Furthermore,triphasic waves occur essentially in adults; this patternhas been rarely reported below the age of 20 years.21
Table 1 Grading of EEG Abnormalities in Diffuse Encephalopathy
Grade I (almost normal) Dominant activity is alpha rhythm with minimal theta activityGrade II (mildly abnormal) Dominant theta background with some alpha and delta activitiesGrade III (moderately abnormal) Continuous delta activity predominates, little activity of faster frequenciesGrade IV (severely abnormal) Low-amplitude delta activity or suppression-burst patternGrade V (extremely abnormal) Nearly “flat” tracing or electrocerebral inactivity
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
12 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003
Figure 4 EEG of an 82-year-old patient with recent history oflethargy and confusion, showing frontal intermittent rhythmicdelta activity. (Reprinted from Markand,10 with permission fromLippincott Williams & Wilkins.)
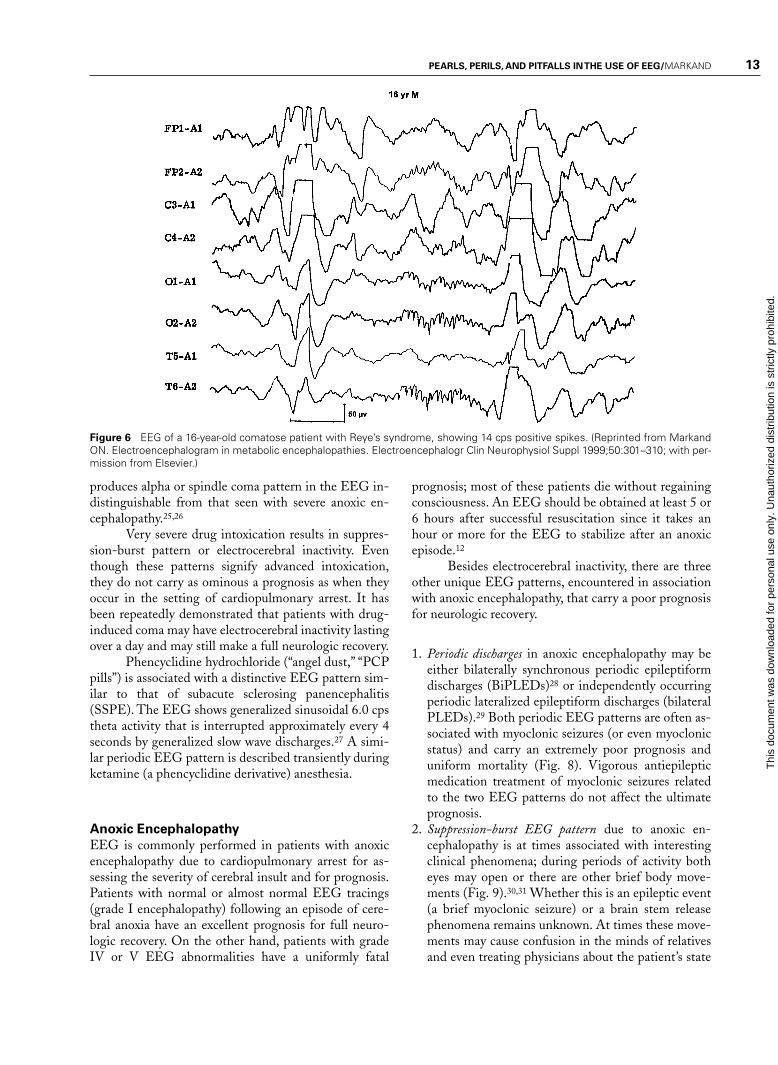
This is particularly true with Reyes disease, an acutechildhood encephalopathy with hepatic fatty infiltra-tion, where triphasic waves are absent.22 The EEG pat-tern of 14 to 6 per second, positive spikes are a well-known maturational EEG pattern normally seen inchildren in adolescence during NREM sleep. The pres-ence of positive spike bursts in comatose patients withcontinuous delta activity is a unique, albeit rare, EEGpattern associated with hepatic or anoxic encephalopa-thy in children (Fig. 6).23,24
Toxic Encephalopathy
Overdose of hypnotic-sedative drugs is a common causeof coma encountered in the emergency room; excessivebeta activity is a prominent feature in the EEG over theanterior head regions. What is less well recognized isthat with more severe intoxication, the fast activity as-sumes a slower frequency (usually 10 to 13 Hz), whichis widespread but with anterior predominance. Thepresence of generalized theta-delta activity with super-imposed alpha frequency activity is a unique encephalo-graphic pattern highly characteristic of sedative drugintoxication (Fig. 7). In the absence of prominent slowactivity, the anterior dominant generalized fast activity
Figure 5 EEG of a 69-year-old patient with hepatic encephalopathy, showing tripha-sic waves. (Reprinted from Markand ON.Electroencephalogram in metabolic en-cephalopathies. Electroencephalogr Clin Neu-rophysiol Suppl 1999;50:301–310; with permission from Elsevier.)
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
PEARLS, PERILS, AND PITFALLS IN THE USE OF EEG/MARKAND 13
Figure 6 EEG of a 16-year-old comatose patient with Reye’s syndrome, showing 14 cps positive spikes. (Reprinted from MarkandON. Electroencephalogram in metabolic encephalopathies. Electroencephalogr Clin Neurophysiol Suppl 1999;50:301–310; with per-mission from Elsevier.)
produces alpha or spindle coma pattern in the EEG in-distinguishable from that seen with severe anoxic en-cephalopathy.25,26
Very severe drug intoxication results in suppres-sion-burst pattern or electrocerebral inactivity. Eventhough these patterns signify advanced intoxication,they do not carry as ominous a prognosis as when theyoccur in the setting of cardiopulmonary arrest. It hasbeen repeatedly demonstrated that patients with drug-induced coma may have electrocerebral inactivity lastingover a day and may still make a full neurologic recovery.
Phencyclidine hydrochloride (“angel dust,” “PCPpills”) is associated with a distinctive EEG pattern sim-ilar to that of subacute sclerosing panencephalitis(SSPE). The EEG shows generalized sinusoidal 6.0 cpstheta activity that is interrupted approximately every 4seconds by generalized slow wave discharges.27 A simi-lar periodic EEG pattern is described transiently duringketamine (a phencyclidine derivative) anesthesia.
Anoxic Encephalopathy
EEG is commonly performed in patients with anoxicencephalopathy due to cardiopulmonary arrest for as-sessing the severity of cerebral insult and for prognosis.Patients with normal or almost normal EEG tracings(grade I encephalopathy) following an episode of cere-bral anoxia have an excellent prognosis for full neuro-logic recovery. On the other hand, patients with gradeIV or V EEG abnormalities have a uniformly fatal
prognosis; most of these patients die without regainingconsciousness. An EEG should be obtained at least 5 or6 hours after successful resuscitation since it takes anhour or more for the EEG to stabilize after an anoxicepisode.12
Besides electrocerebral inactivity, there are threeother unique EEG patterns, encountered in associationwith anoxic encephalopathy, that carry a poor prognosisfor neurologic recovery.
1. Periodic discharges in anoxic encephalopathy may beeither bilaterally synchronous periodic epileptiformdischarges (BiPLEDs)28 or independently occurringperiodic lateralized epileptiform discharges (bilateralPLEDs).29 Both periodic EEG patterns are often as-sociated with myoclonic seizures (or even myoclonicstatus) and carry an extremely poor prognosis anduniform mortality (Fig. 8). Vigorous antiepilepticmedication treatment of myoclonic seizures relatedto the two EEG patterns do not affect the ultimateprognosis.
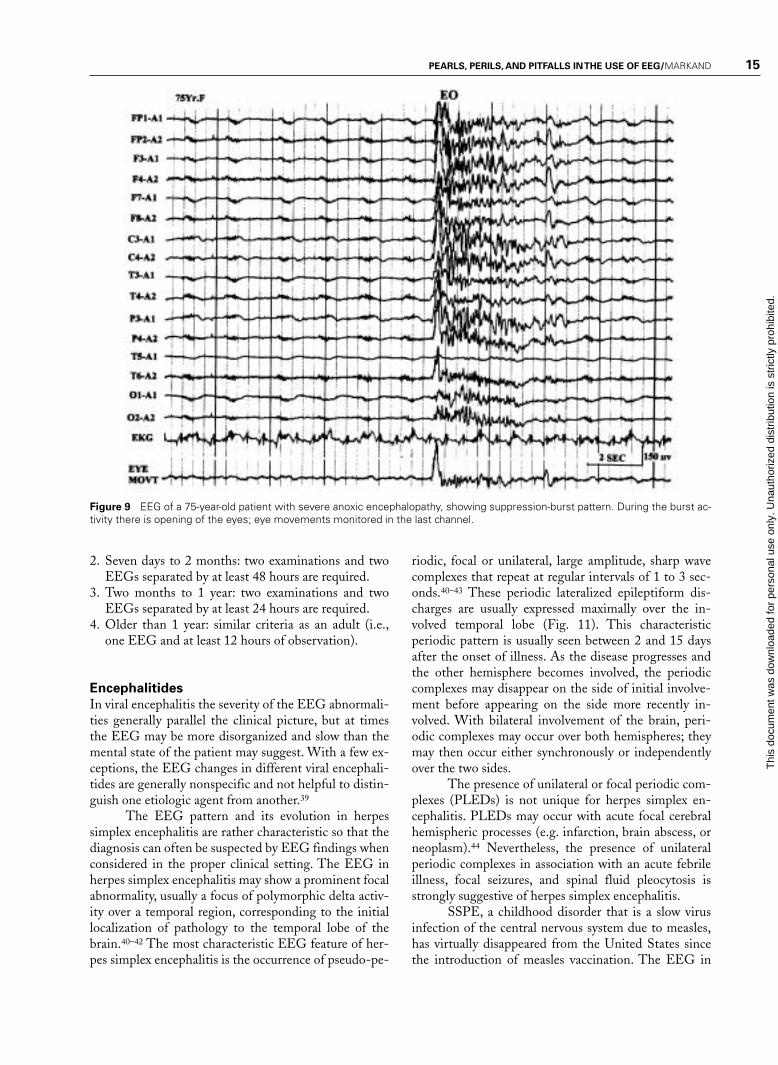
2. Suppression-burst EEG pattern due to anoxic en-cephalopathy is at times associated with interestingclinical phenomena; during periods of activity botheyes may open or there are other brief body move-ments (Fig. 9).30,31 Whether this is an epileptic event(a brief myoclonic seizure) or a brain stem releasephenomena remains unknown. At times these move-ments may cause confusion in the minds of relativesand even treating physicians about the patient’s state
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.

14 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003
Figure 7 EEG of an 18-year-old patient with phenobarbital in-toxication, showing generalized theta-delta activity with super-imposed beta frequencies (A) followed in 3 days by normaliza-tion of the EEG (B). (Reprinted from Markand,10 withpermission from Lippincott Williams & Wilkins.)
of consciousness, as they may mimic volitional motoractivity.
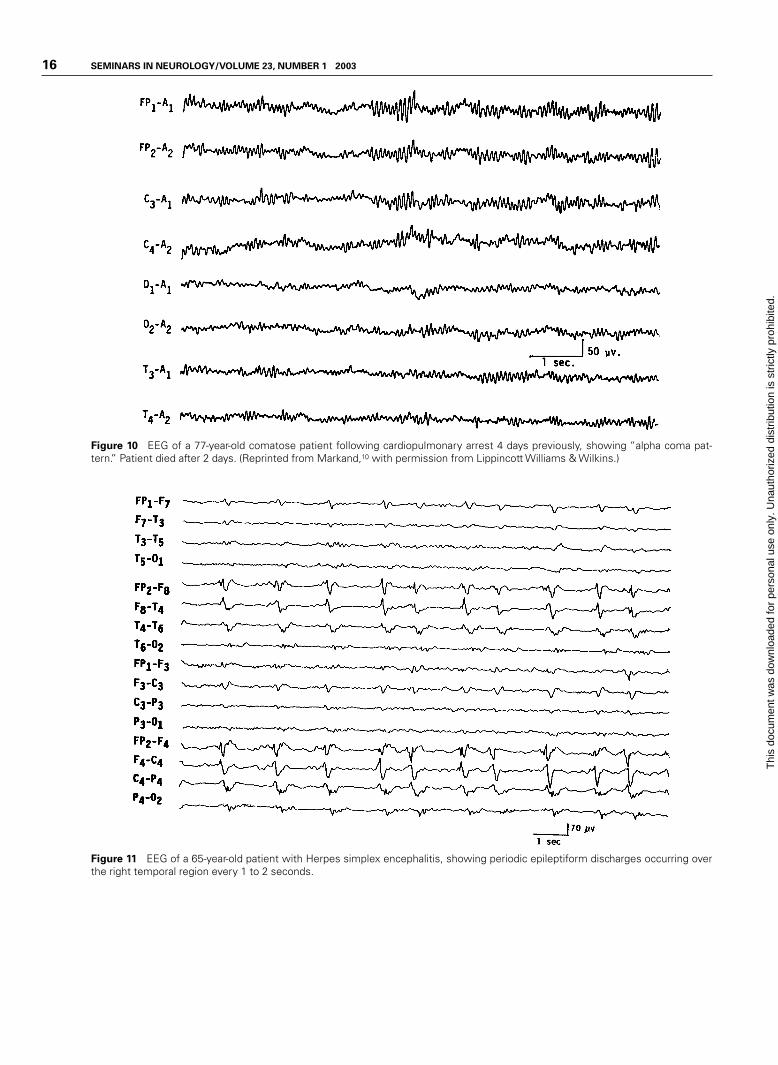
3. A rare EEG pattern seen in severe anoxic en-cephalopathy is the alpha coma pattern, denoting theconjunction of clinical coma associated with alphafrequency activity.32–34 Because in such tracings thedominant frequency is alpha frequency activity with-out significant slower frequencies, the EEG superfi-cially resembles that of an “awake” person, but thereare major differences. The alpha frequency activity inalpha pattern coma is widespread in distribution andis often prominent over the anterior head regions(Fig. 10). Reactivity to any type of sensory stimula-tion is usually absent. The prognosis of alpha patterncoma is extremely poor; all patients have either diedor survived in chronic vegetative state.
Remember that EEG findings of alpha patterncoma are also seen in the setting of sedative/hypnotic drugintoxication25,35 and in association with intrinsic brainstem lesions36 with a much more favorable prognosis.
Cerebral Death
The EEG is being employed with increasing frequencyfor the determination of cerebral death in patients withirreversible coma, particularly when organs have to besalvaged for transplantation. It cannot be overempha-sized that the absence of cerebral activity on the EEG isonly one of the criteria, and should always be consideredalong with the clinical findings and blood flow studiesfor brain death. To properly identify very-low-voltagecerebral activity, to distinguish physiological or instru-mental artifacts, and to eliminate the possibility of er-rors through malfunctioning equipment or inadequatetechniques, the American EEG Society37 has a numberof recommendations that must be followed during EEGrecordings in all cases of suspected brain death. In such“flat” tracings, EEG activity may be obscured by very-low-amplitude fast activity due to sustained contractionof scalp muscles, which can be eliminated by giving ashort-acting neuromuscular blocking agent (succinyl-choline, 20 to 40 mg IV). This step, which is very easyto undertake, is often overlooked to obtain a satisfactoryrecording in such patients.
A single EEG and a 6- to 12-hour clinical obser-vation after an unequivocal acute cerebral insult areminimum requirements for brain death evaluation in anadult. In young children, the guidelines are slightly dif-ferent because of the more difficult task of confirmingbrain death in this age group. A special task force38 rec-ommended the following:
1. Brain death should not be determined until at least 7days of age.
Figure 8 EEG of a 49-year-old comatose patient following se-vere anoxic encephalopathy, showing bisynchronous periodicepileptiform discharges synchronous with jerks of the left lowerextremity monitored on a separate channel.
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
PEARLS, PERILS, AND PITFALLS IN THE USE OF EEG/MARKAND 15
Figure 9 EEG of a 75-year-old patient with severe anoxic encephalopathy, showing suppression-burst pattern. During the burst ac-tivity there is opening of the eyes; eye movements monitored in the last channel.
2. Seven days to 2 months: two examinations and twoEEGs separated by at least 48 hours are required.
3. Two months to 1 year: two examinations and twoEEGs separated by at least 24 hours are required.
4. Older than 1 year: similar criteria as an adult (i.e.,one EEG and at least 12 hours of observation).
Encephalitides
In viral encephalitis the severity of the EEG abnormali-ties generally parallel the clinical picture, but at timesthe EEG may be more disorganized and slow than themental state of the patient may suggest. With a few ex-ceptions, the EEG changes in different viral encephali-tides are generally nonspecific and not helpful to distin-guish one etiologic agent from another.39
The EEG pattern and its evolution in herpessimplex encephalitis are rather characteristic so that thediagnosis can often be suspected by EEG findings whenconsidered in the proper clinical setting. The EEG inherpes simplex encephalitis may show a prominent focalabnormality, usually a focus of polymorphic delta activ-ity over a temporal region, corresponding to the initiallocalization of pathology to the temporal lobe of thebrain.40–42 The most characteristic EEG feature of her-pes simplex encephalitis is the occurrence of pseudo-pe-
riodic, focal or unilateral, large amplitude, sharp wavecomplexes that repeat at regular intervals of 1 to 3 sec-onds.40–43 These periodic lateralized epileptiform dis-charges are usually expressed maximally over the in-volved temporal lobe (Fig. 11). This characteristicperiodic pattern is usually seen between 2 and 15 daysafter the onset of illness. As the disease progresses andthe other hemisphere becomes involved, the periodiccomplexes may disappear on the side of initial involve-ment before appearing on the side more recently in-volved. With bilateral involvement of the brain, peri-odic complexes may occur over both hemispheres; theymay then occur either synchronously or independentlyover the two sides.
The presence of unilateral or focal periodic com-plexes (PLEDs) is not unique for herpes simplex en-cephalitis. PLEDs may occur with acute focal cerebralhemispheric processes (e.g. infarction, brain abscess, orneoplasm).44 Nevertheless, the presence of unilateralperiodic complexes in association with an acute febrileillness, focal seizures, and spinal fluid pleocytosis isstrongly suggestive of herpes simplex encephalitis.
SSPE, a childhood disorder that is a slow virusinfection of the central nervous system due to measles,has virtually disappeared from the United States sincethe introduction of measles vaccination. The EEG in
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
16 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003
Figure 10 EEG of a 77-year-old comatose patient following cardiopulmonary arrest 4 days previously, showing “alpha coma pat-tern.” Patient died after 2 days. (Reprinted from Markand,10 with permission from Lippincott Williams & Wilkins.)
Figure 11 EEG of a 65-year-old patient with Herpes simplex encephalitis, showing periodic epileptiform discharges occurring overthe right temporal region every 1 to 2 seconds.
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
PEARLS, PERILS, AND PITFALLS IN THE USE OF EEG/MARKAND 17
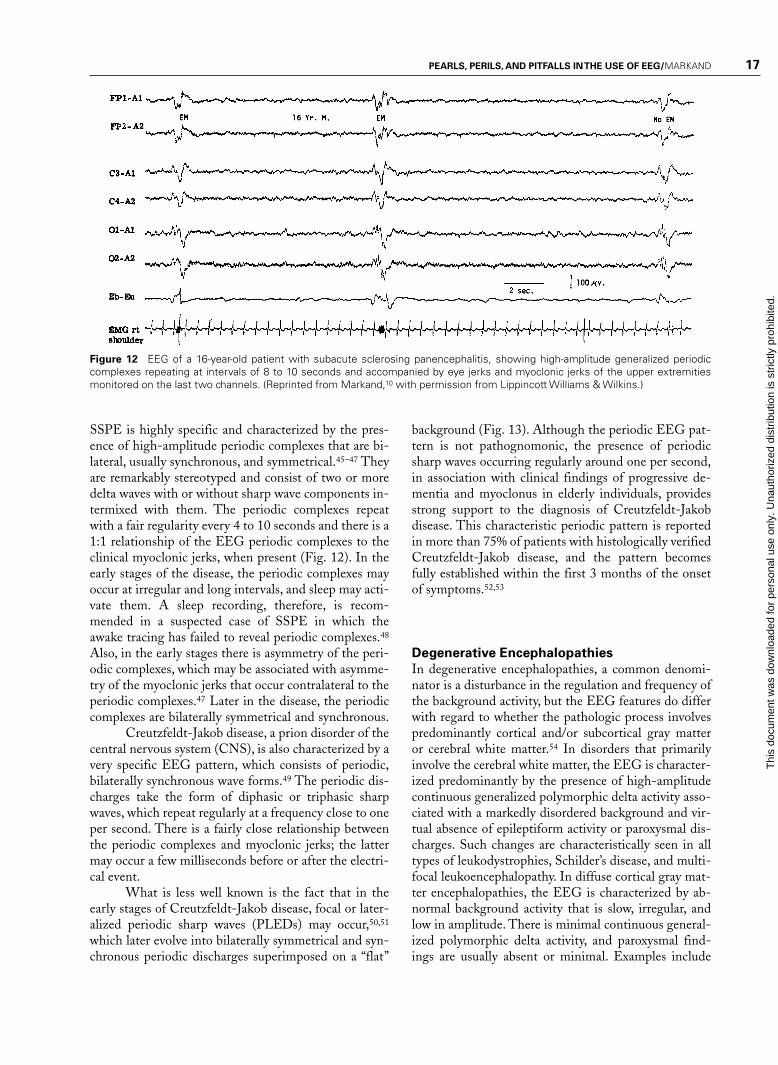
Figure 12 EEG of a 16-year-old patient with subacute sclerosing panencephalitis, showing high-amplitude generalized periodiccomplexes repeating at intervals of 8 to 10 seconds and accompanied by eye jerks and myoclonic jerks of the upper extremitiesmonitored on the last two channels. (Reprinted from Markand,10 with permission from Lippincott Williams & Wilkins.)
SSPE is highly specific and characterized by the pres-ence of high-amplitude periodic complexes that are bi-lateral, usually synchronous, and symmetrical.45–47 Theyare remarkably stereotyped and consist of two or moredelta waves with or without sharp wave components in-termixed with them. The periodic complexes repeatwith a fair regularity every 4 to 10 seconds and there is a1:1 relationship of the EEG periodic complexes to theclinical myoclonic jerks, when present (Fig. 12). In theearly stages of the disease, the periodic complexes mayoccur at irregular and long intervals, and sleep may acti-vate them. A sleep recording, therefore, is recom-mended in a suspected case of SSPE in which theawake tracing has failed to reveal periodic complexes.48
Also, in the early stages there is asymmetry of the peri-odic complexes, which may be associated with asymme-try of the myoclonic jerks that occur contralateral to theperiodic complexes.47 Later in the disease, the periodiccomplexes are bilaterally symmetrical and synchronous.
Creutzfeldt-Jakob disease, a prion disorder of thecentral nervous system (CNS), is also characterized by avery specific EEG pattern, which consists of periodic,bilaterally synchronous wave forms.49 The periodic dis-charges take the form of diphasic or triphasic sharpwaves, which repeat regularly at a frequency close to oneper second. There is a fairly close relationship betweenthe periodic complexes and myoclonic jerks; the lattermay occur a few milliseconds before or after the electri-cal event.
What is less well known is the fact that in theearly stages of Creutzfeldt-Jakob disease, focal or later-alized periodic sharp waves (PLEDs) may occur,50,51
which later evolve into bilaterally symmetrical and syn-chronous periodic discharges superimposed on a “flat”
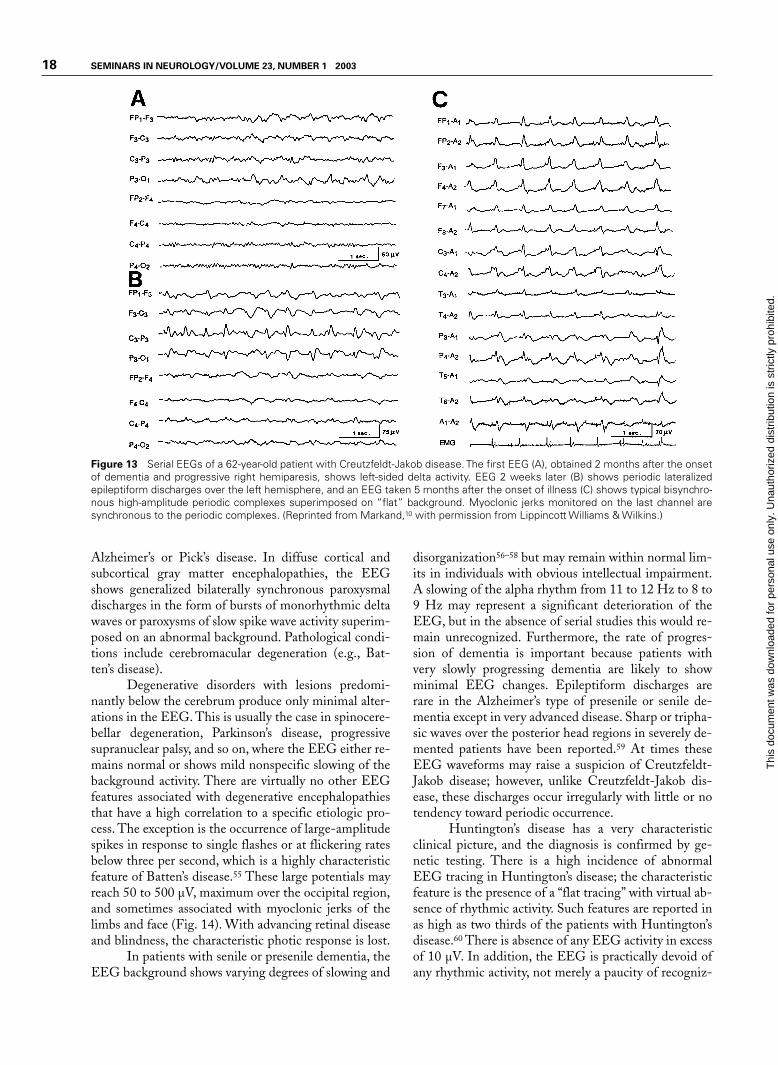
background (Fig. 13). Although the periodic EEG pat-tern is not pathognomonic, the presence of periodicsharp waves occurring regularly around one per second,in association with clinical findings of progressive de-mentia and myoclonus in elderly individuals, providesstrong support to the diagnosis of Creutzfeldt-Jakobdisease. This characteristic periodic pattern is reportedin more than 75% of patients with histologically verifiedCreutzfeldt-Jakob disease, and the pattern becomesfully established within the first 3 months of the onsetof symptoms.52,53
Degenerative Encephalopathies
In degenerative encephalopathies, a common denomi-nator is a disturbance in the regulation and frequency ofthe background activity, but the EEG features do differwith regard to whether the pathologic process involvespredominantly cortical and/or subcortical gray matteror cerebral white matter.54 In disorders that primarilyinvolve the cerebral white matter, the EEG is character-ized predominantly by the presence of high-amplitudecontinuous generalized polymorphic delta activity asso-ciated with a markedly disordered background and vir-tual absence of epileptiform activity or paroxysmal dis-charges. Such changes are characteristically seen in alltypes of leukodystrophies, Schilder’s disease, and multi-focal leukoencephalopathy. In diffuse cortical gray mat-ter encephalopathies, the EEG is characterized by ab-normal background activity that is slow, irregular, andlow in amplitude. There is minimal continuous general-ized polymorphic delta activity, and paroxysmal find-ings are usually absent or minimal. Examples include
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
18 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003
Figure 13 Serial EEGs of a 62-year-old patient with Creutzfeldt-Jakob disease. The first EEG (A), obtained 2 months after the onsetof dementia and progressive right hemiparesis, shows left-sided delta activity. EEG 2 weeks later (B) shows periodic lateralizedepileptiform discharges over the left hemisphere, and an EEG taken 5 months after the onset of illness (C) shows typical bisynchro-nous high-amplitude periodic complexes superimposed on “flat” background. Myoclonic jerks monitored on the last channel aresynchronous to the periodic complexes. (Reprinted from Markand,10 with permission from Lippincott Williams & Wilkins.)
Alzheimer’s or Pick’s disease. In diffuse cortical andsubcortical gray matter encephalopathies, the EEGshows generalized bilaterally synchronous paroxysmaldischarges in the form of bursts of monorhythmic deltawaves or paroxysms of slow spike wave activity superim-posed on an abnormal background. Pathological condi-tions include cerebromacular degeneration (e.g., Bat-ten’s disease).
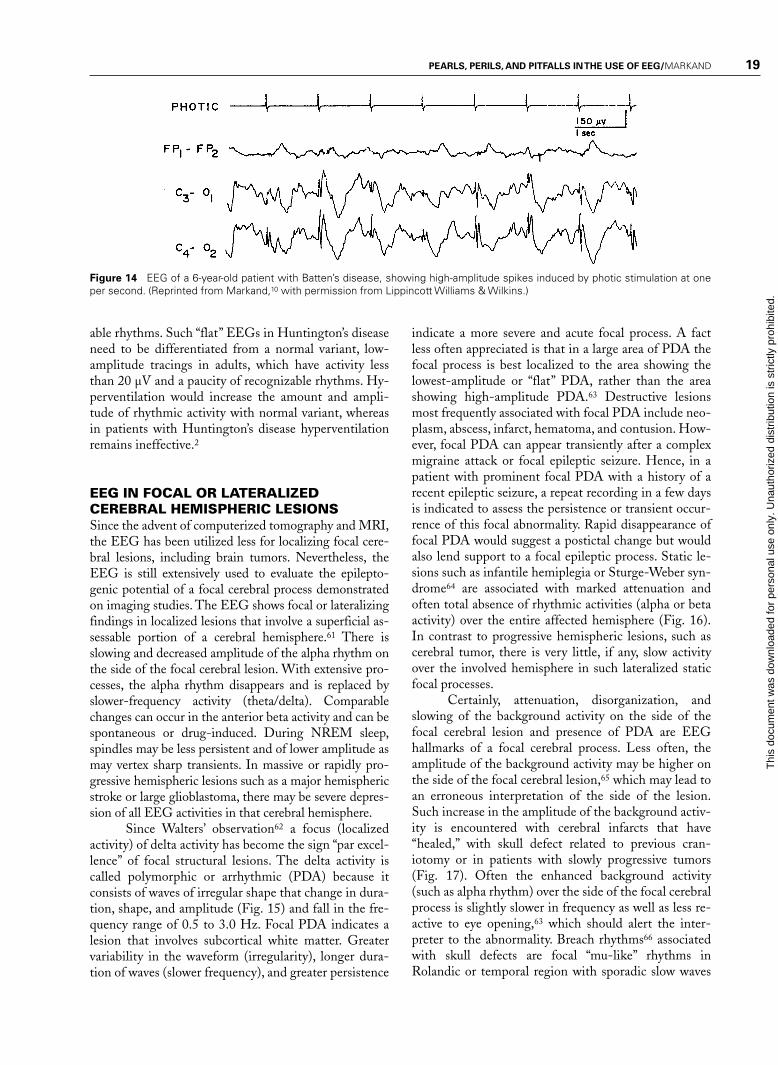
Degenerative disorders with lesions predomi-nantly below the cerebrum produce only minimal alter-ations in the EEG. This is usually the case in spinocere-bellar degeneration, Parkinson’s disease, progressivesupranuclear palsy, and so on, where the EEG either re-mains normal or shows mild nonspecific slowing of thebackground activity. There are virtually no other EEGfeatures associated with degenerative encephalopathiesthat have a high correlation to a specific etiologic pro-cess. The exception is the occurrence of large-amplitudespikes in response to single flashes or at flickering ratesbelow three per second, which is a highly characteristicfeature of Batten’s disease.55 These large potentials mayreach 50 to 500 µV, maximum over the occipital region,and sometimes associated with myoclonic jerks of thelimbs and face (Fig. 14). With advancing retinal diseaseand blindness, the characteristic photic response is lost.
In patients with senile or presenile dementia, theEEG background shows varying degrees of slowing and
disorganization56–58 but may remain within normal lim-its in individuals with obvious intellectual impairment.A slowing of the alpha rhythm from 11 to 12 Hz to 8 to9 Hz may represent a significant deterioration of theEEG, but in the absence of serial studies this would re-main unrecognized. Furthermore, the rate of progres-sion of dementia is important because patients withvery slowly progressing dementia are likely to showminimal EEG changes. Epileptiform discharges arerare in the Alzheimer’s type of presenile or senile de-mentia except in very advanced disease. Sharp or tripha-sic waves over the posterior head regions in severely de-mented patients have been reported.59 At times theseEEG waveforms may raise a suspicion of Creutzfeldt-Jakob disease; however, unlike Creutzfeldt-Jakob dis-ease, these discharges occur irregularly with little or notendency toward periodic occurrence.
Huntington’s disease has a very characteristicclinical picture, and the diagnosis is confirmed by ge-netic testing. There is a high incidence of abnormalEEG tracing in Huntington’s disease; the characteristicfeature is the presence of a “flat tracing” with virtual ab-sence of rhythmic activity. Such features are reported inas high as two thirds of the patients with Huntington’sdisease.60 There is absence of any EEG activity in excessof 10 µV. In addition, the EEG is practically devoid ofany rhythmic activity, not merely a paucity of recogniz-
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
PEARLS, PERILS, AND PITFALLS IN THE USE OF EEG/MARKAND 19
Figure 14 EEG of a 6-year-old patient with Batten’s disease, showing high-amplitude spikes induced by photic stimulation at oneper second. (Reprinted from Markand,10 with permission from Lippincott Williams & Wilkins.)
able rhythms. Such “flat” EEGs in Huntington’s diseaseneed to be differentiated from a normal variant, low-amplitude tracings in adults, which have activity lessthan 20 µV and a paucity of recognizable rhythms. Hy-perventilation would increase the amount and ampli-tude of rhythmic activity with normal variant, whereasin patients with Huntington’s disease hyperventilationremains ineffective.2
EEG IN FOCAL OR LATERALIZEDCEREBRAL HEMISPHERIC LESIONSSince the advent of computerized tomography and MRI,the EEG has been utilized less for localizing focal cere-bral lesions, including brain tumors. Nevertheless, theEEG is still extensively used to evaluate the epilepto-genic potential of a focal cerebral process demonstratedon imaging studies. The EEG shows focal or lateralizingfindings in localized lesions that involve a superficial as-sessable portion of a cerebral hemisphere.61 There isslowing and decreased amplitude of the alpha rhythm onthe side of the focal cerebral lesion. With extensive pro-cesses, the alpha rhythm disappears and is replaced byslower-frequency activity (theta/delta). Comparablechanges can occur in the anterior beta activity and can bespontaneous or drug-induced. During NREM sleep,spindles may be less persistent and of lower amplitude asmay vertex sharp transients. In massive or rapidly pro-gressive hemispheric lesions such as a major hemisphericstroke or large glioblastoma, there may be severe depres-sion of all EEG activities in that cerebral hemisphere.
Since Walters’ observation62 a focus (localizedactivity) of delta activity has become the sign “par excel-lence” of focal structural lesions. The delta activity iscalled polymorphic or arrhythmic (PDA) because itconsists of waves of irregular shape that change in dura-tion, shape, and amplitude (Fig. 15) and fall in the fre-quency range of 0.5 to 3.0 Hz. Focal PDA indicates alesion that involves subcortical white matter. Greatervariability in the waveform (irregularity), longer dura-tion of waves (slower frequency), and greater persistence
indicate a more severe and acute focal process. A factless often appreciated is that in a large area of PDA thefocal process is best localized to the area showing thelowest-amplitude or “flat” PDA, rather than the areashowing high-amplitude PDA.63 Destructive lesionsmost frequently associated with focal PDA include neo-plasm, abscess, infarct, hematoma, and contusion. How-ever, focal PDA can appear transiently after a complexmigraine attack or focal epileptic seizure. Hence, in apatient with prominent focal PDA with a history of arecent epileptic seizure, a repeat recording in a few daysis indicated to assess the persistence or transient occur-rence of this focal abnormality. Rapid disappearance offocal PDA would suggest a postictal change but wouldalso lend support to a focal epileptic process. Static le-sions such as infantile hemiplegia or Sturge-Weber syn-drome64 are associated with marked attenuation andoften total absence of rhythmic activities (alpha or betaactivity) over the entire affected hemisphere (Fig. 16).In contrast to progressive hemispheric lesions, such ascerebral tumor, there is very little, if any, slow activityover the involved hemisphere in such lateralized staticfocal processes.
Certainly, attenuation, disorganization, andslowing of the background activity on the side of thefocal cerebral lesion and presence of PDA are EEGhallmarks of a focal cerebral process. Less often, theamplitude of the background activity may be higher onthe side of the focal cerebral lesion,65 which may lead toan erroneous interpretation of the side of the lesion.Such increase in the amplitude of the background activ-ity is encountered with cerebral infarcts that have“healed,” with skull defect related to previous cran-iotomy or in patients with slowly progressive tumors(Fig. 17). Often the enhanced background activity(such as alpha rhythm) over the side of the focal cerebralprocess is slightly slower in frequency as well as less re-active to eye opening,63 which should alert the inter-preter to the abnormality. Breach rhythms66 associatedwith skull defects are focal “mu-like” rhythms inRolandic or temporal region with sporadic slow waves
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.

20 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003
Figure 15 EEG of a 43-year-old patient with right temporal glioma, showing polymorphic delta activity and low-amplitude spike dis-charges (*) over the right temporal region. (Reprinted from Daly and Markand,61 with permission from Lippincott Williams & Wilkins.)
Figure 16 EEG of a 16-year-old patient with Sturge-Weber syndrome of the right hemisphere, showing total absence of rhythmicactivities over the entire affected hemisphere. (Reprinted from Daly and Markand,61 with permission from Lippincott Williams &Wilkins.)
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.

PEARLS, PERILS, AND PITFALLS IN THE USE OF EEG/MARKAND 21
Figure 17 EEG of a 47-year-old patient with a low-grade glioma of the left temporal lobe, showing slightly slow but higher ampli-tude alpha on the left side.
and spiky or sharp transients (Fig. 18). These rhythmsare unrelated to epilepsy and do not indicate recurrenceof a tumor. The “spiky” grapho-elements should not beoverinterpreted as epileptogenic discharges. For properassessment of EEG asymmetries, it is therefore essentialto know if the patient has had a craniotomy or skull de-fect, which may enhance background activities on theside of the breach of the skull.
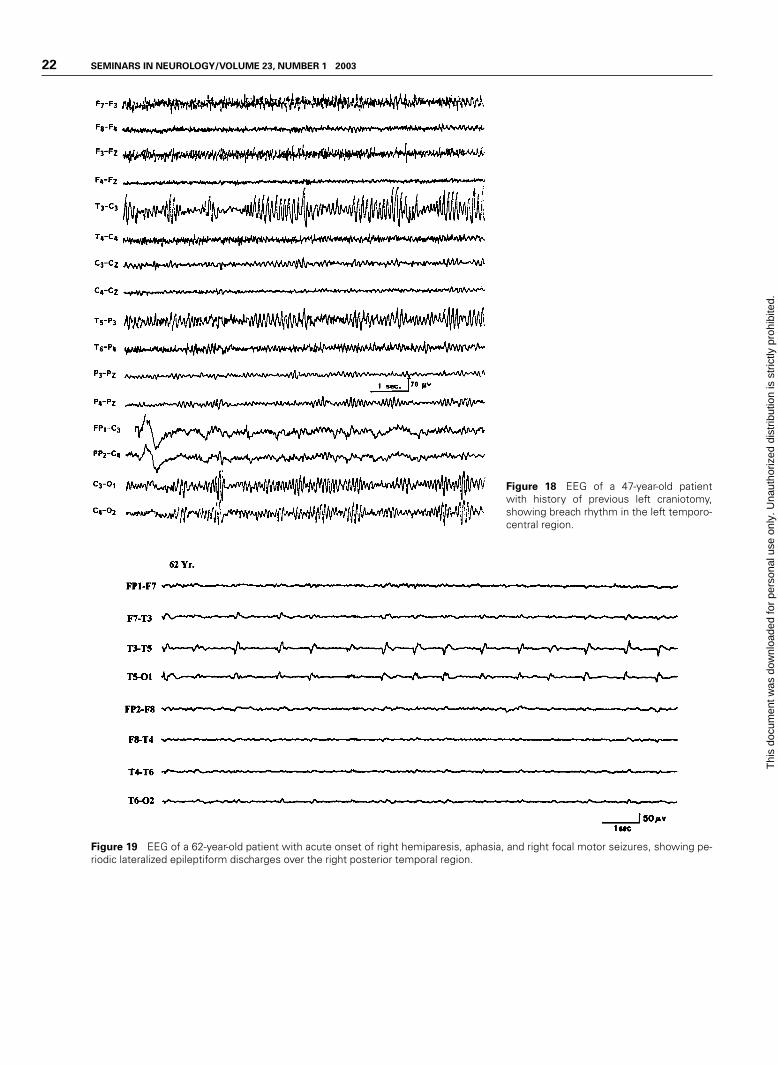
Epileptiform activity, such as focal spikes, sharpwaves, or spike wave discharges, also occur in localizedhemispheric lesions usually of an indolent or static na-ture. With acute hemispheric lesions, epileptiform discharges are less common but when seen often have aperiodic character. PLEDs consist of sharp waves, re-peating more or less regularly at one per second over arelatively large area of the hemicranium during most ofthe EEG study (Fig. 19). This distinctive focal periodicpattern usually occurs in patients with acute hemi-spheric strokes, brain abscess, primary (usually glioblas-toma) or metastatic neoplasms, and herpes simplex en-cephalitis.44,67
EEG IN PAROXYSMAL DISORDERSAn EEG is the most common and most useful test per-formed in evaluating patients suspected of epilepsy.There are many areas where an EEG has unique contri-butions. The value of an EEG lies in the fact that it notonly shows specific ictal discharges during a clinical
seizure but also characteristic epileptiform abnormali-ties in a high proportion of epileptic patients even in theinterictal period. Furthermore, an EEG may be the onlytest demonstrating focal abnormalities responsible forthe patient’s epileptic seizures. Specific patterns in theEEG make it possible to classify the seizure type, whichis an essential prerequisite to institute proper anti-epileptic medication. An EEG is indispensable for thediagnosis of nonconvulsive epileptic status presenting asprolonged “twilight” state or a prolonged episode of ab-normal behavior. In a patient with bizarre motor activ-ity, the recording of an EEG during such an episodemay be the only way to establish whether the abnormalbehavior is due to an epileptic seizure or a nonepilepticevent, physiologic or nonphysiologic. Finally, the EEGis indispensable to localize the epileptogenic (seizureproducing) zone before resective surgery (excision of theepileptogenic zone) is undertaken in a patient withmedically refractory focal epilepsy.
Epileptiform Abnormalities
Paroxysmal EEG activities, whether focal or general-ized, are often termed “epileptiform activities.” They arethe EEG hallmark of epilepsy as they are highly corre-lated with the occurrence of clinical seizures. Epilepti-form abnormalities are usually divided into “interictal”discharges, which appear in the interval between clini-cal seizures, and “ictal” discharges, which accompany
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
22 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003
Figure 18 EEG of a 47-year-old patientwith history of previous left craniotomy,showing breach rhythm in the left temporo-central region.
Figure 19 EEG of a 62-year-old patient with acute onset of right hemiparesis, aphasia, and right focal motor seizures, showing pe-riodic lateralized epileptiform discharges over the right posterior temporal region.
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.

PEARLS, PERILS, AND PITFALLS IN THE USE OF EEG/MARKAND 23
clinical seizures. The distinction is arbitrary because thedesignation “ictal” or “interictal” often depends on howclosely the patient was clinically observed because mini-mal behavioral alterations associated with the EEGparoxysms can be easily missed. Morphologically, interic-tal epileptiform abnormalities consist of spikes and poly-spikes, sharp waves, spike-slow wave complexes, multiple(poly) spike wave complexes, and sharp-slow wave com-plexes. Spike is defined as an EEG transient clearly dis-tinguished from the background, with a pointed peak atconventional paper speed and a duration of 20 to 70 mil-liseconds. Sharp waves are transients of similar characteras spikes but have a duration of longer than 70 millisec-onds and less than 200 milliseconds. Spike-slow wavesand sharp-slow wave complexes are constituted by spikesor sharp waves followed by a high-amplitude slow wave.
Morphologic characteristics of epileptiform dis-charges have little correlation with different types ofepileptic seizures. The topographic distribution of thesedischarges are more important in the classification ofepilepsies. Generalized discharges that are bilaterallysynchronous and symmetrical are associated with gener-alized epilepsies, whereas focal or lateralized dischargesconstitute the EEG “signature” of partial (focal) epilep-sies. Most patients do not have their epileptic seizuresduring the brief period of routine EEG; hence, the inter-ictal epileptiform abnormalities are the ones heavily re-lied on for the diagnosis of epilepsy. Although the inter-ictal epileptiform abnormalities have a high correlationwith the occurrence of clinical seizures, they do notthemselves mean that the patient has epilepsy. The ir-refutable evidence of epileptic seizure is a clinical seizureassociated simultaneously with ictal discharges in theEEG, although such evidence is often difficult to obtainexcept during prolonged video EEG monitoring.
“Ictal” or an electrographic seizure pattern ischaracterized by repetitive EEG discharges with rela-tively abrupt onset and termination, and characteristicpattern of evolution lasting at least several seconds. Thecommonest waves or complexes vary in form, frequency,and topography. The ictal pattern is generally rhythmicand frequently displays increasing amplitude, decreasingfrequency, and spatial spread during the seizure. Thethree EEG characteristics of a focal “ictal” pattern,therefore, consist of sudden onset/termination, occur-rence of a rhythmic pattern of activity during theepileptic seizure, and its characteristic evolution withrespect to amplitude, frequency, and spatial distribution.
Proper Identification of Diagnostic
Epileptiform Abnormalities in the EEG
In the evaluation of abnormalities in the EEG, oneneeds to be constantly aware that there are manyEEG transients that morphologically resemble epi-
leptiform discharges and that need to be distin-guished from diagnostically crucial epileptiform ab-normalities to avoid overdiagnosis or misdiagnosis.These include:
1. Artifacts: for example, electrode pop, muscle poten-tials, eye movements, electrocardiogram (EKG), etc.
2. Normal components of ongoing background activity:for example, vertex sharp transients of sleep, POSTs,mu rhythm, lambda waves, drowsy activity duringsleep in children that may often be associated withsharp components, etc.
3. Epileptiform variants of dubious clinical signifi-cance: there are a large number of benign epilepti-form variants that must be recognized, lest they bemisinterpreted. Although morphologically similar,they are nonepileptogenic as they have no establishedrelationship with the process responsible for generat-ing epileptic seizures. Such sharp transients include14 to 6 per second positive spikes, small sharp spikesor benign epileptiform transients of sleep, 6 Hz spikewave or phantom spike wave, wicket spikes, psy-chomotor variant pattern or rhythmic midtemporaldischarges, breach rhythm, etc. Sleep not only acti-vates diagnostically useful epileptiform EEG pat-terns, but also unmasks several types of nonepilepto-genic sharp transients.
It is critical that the EEG interpreter has clearcriteria for distinguishing diagnostically relevantepileptiform discharges from sharply contoured back-ground activity or benign variants. Useful criteria havebeen formulated for identification of epileptiformevents68,69:
1. Epileptiform discharges (spikes, sharp waves, andspike wave complexes) should be unarguably discreteevents, not just accentuation of part of an ongoingsequence of waves. They should be clearly separablefrom ongoing background activity, not only by theirhigher amplitude but also by their morphology andduration.
2. Most epileptiform discharges have a bi- or triphasicwaveform and they have a more complex morphol-ogy than even high-voltage background rhythms.
3. The epileptiform events are not sinusoidal but rathershow asymmetric, rising and falling phases.
4. Most spikes and sharp waves are followed by a slowwave.
5. Finally, they should have a physiological potentialfield involving more than one electrode that helps todistinguish them from electrode-related artifacts ormuscle potentials.
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
24 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003
Specificity of Interictal Epileptiform
Abnormalities
Are “hard-core” epileptiform abnormalities encoun-tered in normal children and adults who do not have ahistory of epileptic seizures? Different studies, some inchildren70,71 and others in all age groups,72–74 found anincidence of less than 2 to 4% of epileptiform abnor-malities in the EEG of nonepileptic subjects. In an in-teresting study on EEG findings in 13,658 males ages17 to 25 without a previous history of significant illnesswho were medically screened for training in the RoyalAir Force of England, 69 (0.5%) had unequivocalepileptiform discharges.75 Hence, the incidence ofepileptiform abnormalities in the healthy populationwas significantly lower than the 2 to 4% noted in thenonepileptic patients referred to hospital EEG labora-tories.
One can certainly conclude that if an individualhas a “blackout spell” or episodic loss of consciousness,it is very likely to be an epileptic seizure if there are unequivocal epileptiform discharges recorded in theEEG. To reemphasize, interictal epileptiform dis-charges in the EEG are never diagnostic of epilepsy bythemselves, but in the appropriate clinical setting, theyprovide important circumstantial evidence for the diag-nosis of epilepsy.
Sensitivity of EEG and Techniques
to Improve the Yield of Interictal and
Ictal EEG Abnormalities in Patients
with Epileptic Disorders
Some patients with unequivocal epilepsy, especiallyfocal epilepsy, may have repeatedly normal or nonspe-cific EEG studies. A single routine EEG consisting ofhalf an hour recording during wakefulness, hyperventi-lation, and intermittent photic stimulation (IPS) pro-vides diagnostic findings in approximately half of thepatients with epilepsy.76 The following describes a fewways to increase the yield of epileptiform abnormalitiesin an interictal EEG study.
SERIAL EEG STUDIES
EEGs recorded on more than one occasion will increasethe chance for recording a specific epileptiform abnor-mality. Research76 has demonstrated that serial EEGstudies increase the yield for epileptiform abnormalitiesfrom 50% in the first record to 84% by the third EEG,and in 92% by the fourth EEG. There was little addi-tional yield to serial EEGs beyond this point.76 Thus,four or five EEG studies spread over a few years providediagnostic abnormalities in over 90% patients withepilepsy. An opposite corollary is also true; serial nega-
tive EEG studies in a patient with continuing paroxys-mal events should raise suspicion of nonepileptic epi-sodes. It is also well known that interictal epileptiformdischarges markedly increase after a clinical seizure77;hence, obtaining an EEG promptly after a clinicalseizure will increase the chances of capturing interictalepileptiform discharges.
ACTIVATING PROCEDURES
Activating procedures (e.g., hyperventilation, IPS), re-cording during sleep, are very well known to activateepileptiform discharges not recorded in the awake trac-ing. Hyperventilation and IPS are potent activators ofgeneralized spike wave discharges associated with pri-mary generalized epilepsies. On the other hand, sleeptends to bring out focal epileptiform abnormalities inpatients experiencing focal epileptic seizures. Sleep acti-vates virtually all focal epileptiform abnormalities;therefore, every patient suspected of epilepsy shouldhave a sleep recording unless there is an unequivocaland specific abnormality displayed optimally duringwakefulness. One of the best ways to ensure a sleepEEG is to instruct the patient to come for the EEG testafter remaining awake during the entire or at least amajor part of the previous night. Sleep deprivation ap-pears to have a further activating effect that is additiveto natural sleep itself, particularly in patients with com-plex partial seizures and in patients with juvenile my-oclonic epilepsy.
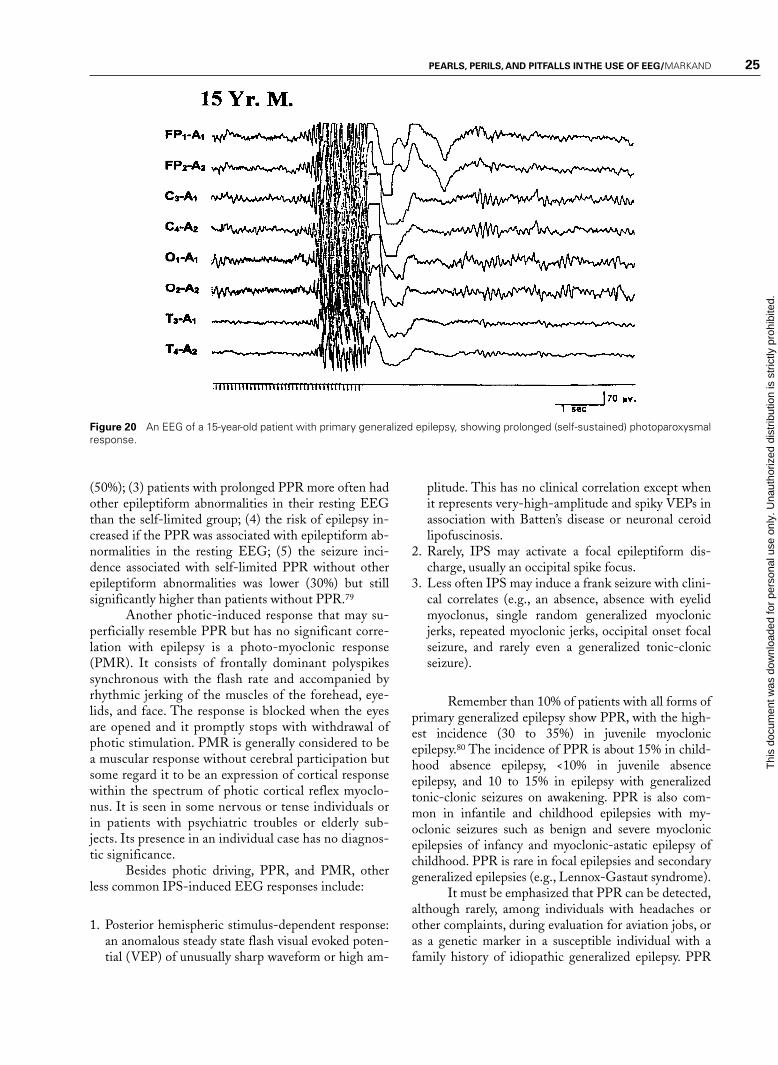
Normal response to IPS includes photic driving(photic following) at flash rate or at harmonics. In about5% of patients, asymmetric photic driving response(>50% difference in amplitude) may occur, which by it-self (without asymmetric awake and/or sleep activities)has no clinical significance. IPS is especially helpful inpatients with primary generalized epilepsy in elicitingabnormal paroxysmal discharges. Photoparoxysmal re-sponse (PPR) has a high correlation with clinicalepilepsy. It is characterized by the occurrence of gener-alized bilaterally synchronous spike wave or multiplespike wave discharges occurring with IPS. The most ef-fective frequency is around 15 flashes per second butother frequencies may be equally effective. Reilly andPeters distinguished two types of PPR: prolonged (self-sustained), which continues for a short period after thestimulus has been withdrawn (Fig. 20), and self-limited,which cease before the flashes stop.78 There is a muchhigher incidence of epilepsy in patients with prolonged(93%) compared with the self-limited (52%) PPR. A1992 meta-analysis of the studies on PPR concluded:(1) PPR, prolonged or self-limited, had a significantlyhigher incidence of seizures than controls; (2) a pro-longed PPR was associated with a much higher inci-dence of seizures (85%) than the self-limited group
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
PEARLS, PERILS, AND PITFALLS IN THE USE OF EEG/MARKAND 25
Figure 20 An EEG of a 15-year-old patient with primary generalized epilepsy, showing prolonged (self-sustained) photoparoxysmalresponse.
(50%); (3) patients with prolonged PPR more often hadother epileptiform abnormalities in their resting EEGthan the self-limited group; (4) the risk of epilepsy in-creased if the PPR was associated with epileptiform ab-normalities in the resting EEG; (5) the seizure inci-dence associated with self-limited PPR without otherepileptiform abnormalities was lower (30%) but stillsignificantly higher than patients without PPR.79
Another photic-induced response that may su-perficially resemble PPR but has no significant corre-lation with epilepsy is a photo-myoclonic response(PMR). It consists of frontally dominant polyspikessynchronous with the flash rate and accompanied byrhythmic jerking of the muscles of the forehead, eye-lids, and face. The response is blocked when the eyesare opened and it promptly stops with withdrawal ofphotic stimulation. PMR is generally considered to bea muscular response without cerebral participation butsome regard it to be an expression of cortical responsewithin the spectrum of photic cortical reflex myoclo-nus. It is seen in some nervous or tense individuals orin patients with psychiatric troubles or elderly sub-jects. Its presence in an individual case has no diagnos-tic significance.
Besides photic driving, PPR, and PMR, otherless common IPS-induced EEG responses include:
1. Posterior hemispheric stimulus-dependent response:an anomalous steady state flash visual evoked poten-tial (VEP) of unusually sharp waveform or high am-
plitude. This has no clinical correlation except whenit represents very-high-amplitude and spiky VEPs inassociation with Batten’s disease or neuronal ceroidlipofuscinosis.
2. Rarely, IPS may activate a focal epileptiform dis-charge, usually an occipital spike focus.
3. Less often IPS may induce a frank seizure with clini-cal correlates (e.g., an absence, absence with eyelidmyoclonus, single random generalized myoclonicjerks, repeated myoclonic jerks, occipital onset focalseizure, and rarely even a generalized tonic-clonicseizure).
Remember than 10% of patients with all forms ofprimary generalized epilepsy show PPR, with the high-est incidence (30 to 35%) in juvenile myoclonicepilepsy.80 The incidence of PPR is about 15% in child-hood absence epilepsy, <10% in juvenile absenceepilepsy, and 10 to 15% in epilepsy with generalizedtonic-clonic seizures on awakening. PPR is also com-mon in infantile and childhood epilepsies with my-oclonic seizures such as benign and severe myoclonicepilepsies of infancy and myoclonic-astatic epilepsy ofchildhood. PPR is rare in focal epilepsies and secondarygeneralized epilepsies (e.g., Lennox-Gastaut syndrome).
It must be emphasized that PPR can be detected,although rarely, among individuals with headaches orother complaints, during evaluation for aviation jobs, oras a genetic marker in a susceptible individual with afamily history of idiopathic generalized epilepsy. PPR
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.

26 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003
in nonepileptic subjects has a prevalence of 1 to 4%; theresponse then is usually brief and less prominent.
IPS is not a totally benign activating procedure.One can induce a generalized tonic-clonic convulsion(often the first one) if photic stimulation is continuedover a long duration in a patient who shows prominentPPR. It is recommended that the photic stimulation belimited to short periods (1 to 5 seconds) and terminatedpromptly as soon as generalized spike wave activity isrecorded (Fig. 20).
SPECIAL ELECTRODES
Although the standard 10 to 20 international system ofelectrode placement provides reasonable coverage of thewhole head, certain areas that have high epileptogenic-ity, such as the mesial temporal lobes in patients withmesial temporal sclerosis, are not fully explored by con-ventional placement and may require additional elec-trodes. Nasopharyngeal electrodes have been widelyused in the past in patients suspected to have with tem-poral lobe epilepsy. They are associated with variabledegrees of discomfort and may prevent the patient fromattaining sleep during the EEG recording. They havenow been largely replaced by the use of anterior tempo-ral electrodes, which are placed 1 cm above and onethird the distance along the line from the external audi-tory meatus to the external canthus of the eye.81
In a comparison of the percentages of spikes de-tected by standard scalp electrodes, anterior temporal,mini-sphenoidal, surface sphenoidal, and nasopharyngealelectrodes in patients with suspected complex partialseizures, the anterior temporal electrodes provided signif-icant improvement in detecting epileptiform abnormali-ties.82 Recordings from standard scalp electrodes detected58% of the discharges. Anterior temporal electrodes werethe best; they detected 70% of all the discharges by them-selves, and 81% in combination with standard scalp elec-trodes. It can be concluded that recordings from anteriortemporal electrodes must be done to improve the detec-tion of interictal epileptiform abnormalities in patientssuspected of having temporal lobe epilepsy. Sphenoidalelectrodes are almost invariably employed during videoEEG monitoring as a part of the presurgical evaluation ofpatients with medically intractable complex partialseizures. The yield of abnormality from sphenoidal re-cordings is certainly greater than that with nasopharyn-geal or anterior temporal electrodes, but it is difficult tojustify the use of invasive electrode placement in routineEEG study for paroxysmal disorders.
ACTIVATION OF AN ACTUAL SEIZURE
DURING ROUTINE EEG STUDY
All efforts must be made to capture the patient’s habit-ual episode during a routine EEG. If precipitating fac-tors are known, these are appropriately exploited. Hy-
perventilation, a potent precipitator of an absenceseizure in a child with primary generalized epilepsy,must always be utilized for at least 5 minutes, once inthe beginning and again at the end of a routine EEGstudy. In rare patients with reflex epilepsy, playing spe-cific music in musicogenic epilepsy, asking a patient toread from a book in reading epilepsy, bathing the pa-tient in bathing epilepsy, asking the patient to eat hismeals (eating epilepsy), smelling gasoline, and so on,may all be carried out to promote an ictal event.
In patients with possible pseudoseizures, sugges-tion protocols are often useful in precipitating episodesand demonstrating EEG changes.83 It is important toemphasize that induced seizures must be clinically typi-cal of a patient’s habitual episodes before the diagnosisof pseudoseizures is strongly considered.
Some Interpretive Challenges of EEG
Findings During Paroxysmal Events
Some of the pitfalls regarding ictal EEG changes dur-ing an actual seizure need to be stressed. All epilepticseizures are not associated with distinctive concomi-tant surface EEG changes. Seizures that remain verylocalized, including epilepsia partialis continua andsimple partial seizures (focal seizures with preservedconsciousness), may not have changes in the scalpEEG because the diagnostic discharge may be deep-seated or involve only a small pool of neuronal tissue.However, epileptic seizures manifested by loss of con-sciousness, on the other hand, are accompanied bydemonstrable changes in the scalp EEG. Therefore,absence of such changes during a clinical episode of“unconsciousness” or bilateral widespread motor activ-ity (resembling grand mal seizure) can be particularlyimportant in making the diagnosis of nonepilepticevents or pseudoseizures. Ten to 20% of patients withpseudoseizures do have epileptic seizures as well. Themost one can say is that at least some of the clinicalepisodes appear to be functional, and this must beconsidered within the context of the entire clinicalpicture.
In evaluating patients with muscle jerks or otherbrief motor events, it needs to be established whetherthese represent epileptic phenomena. Simultaneous re-cording by placing two electrodes over the involvedmuscle may be very helpful in establishing the relation-ship of, or lack of, the EEG and the motor recordings.In patients with myoclonic seizures, it is not always easyto establish whether an electrical event synchronouswith the motor jerk is indeed a cerebral discharge orsimply a movement artifact. The presence of morpho-logically similar EEG discharges in other portions ofthe tracing but unassociated with obvious motor activitywill establish that they represent a genuine cortical dis-
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.

PEARLS, PERILS, AND PITFALLS IN THE USE OF EEG/MARKAND 27
charge rather than an artifact generated by suddenmovement.
EEG IN GENERALIZED EPILEPSIESThe epileptic process in generalized epilepsies involveslarge areas of the brain at the outset of the seizure, andthe EEG is characterized by bilaterally synchronousgeneralized paroxysms of spikes and spike wave dis-charges. Generalized epilepsies are subcategorized asprimary (idiopathic) and secondary (symptomatic).
A patient with primary generalized epilepsy(PGE) has no identifiable etiology, normal brain imag-ing, and normal neurocognitive functioning. Theepilepsy has a strong genetic basis and is highly respon-sive to antiepileptic medication. The patient may sufferfrom absence (petit mal), myoclonic, and tonic-clonicseizures, among other generalized seizures. Many dif-ferent syndromes of PGE have been recognized de-pending upon the predominant seizure type and the ageof onset. Classically, the presence of rhythmic, anterior-dominant generalized bisynchronous 3 Hz spike wavedischarges superimposed on a normal background areconsidered to be the EEG hallmark of PGE.
However, the most common EEG abnormalityassociated with PGE is the so-called “irregular” or“atypical” or “rapid spike” wave activity. This is charac-terized by generalized paroxysms of spikes or spike wavecomplexes occurring with an irregular frequency ofabout 3 to 5 Hz. Although some spike wave complexeswill approximate 3 Hz, the overall impression is that theEEG abnormality is much less regular than the classic 3Hz spike wave discharges (Fig. 21). Transient asymme-
try of the bisynchronous spike wave activity and isolated“focal” spikes are common. Atypical generalized spikewaves are not only seen in PGE but also in secondarygeneralized epilepsies such as progressive myoclonusepilepsies of different etiologies.
Besides the presence of brief (1 to 3 seconds)generalized spike wave discharges, there are no interic-tal epileptiform abnormalities that are specific for indi-vidual syndromes included under PGE (childhood ab-sence epilepsy, juvenile absence epilepsy, juvenilemyoclonic epilepsy, epilepsy with myoclonic absences,and generalized tonic-clonic seizures on awakening).There are a few EEG features that are more commonwith certain syndromes: (1) polyspike wave dischargesare more common with myoclonic epilepsies; (2)paroxysms of occipital-dominant rhythmic delta activ-ity in the EEG is a feature most commonly encoun-tered with childhood absence epilepsy; (3) short parox-ysms of spike wave discharges of higher frequency (4.0to 4.5 Hz) are more common with PGE manifestingprimarily with generalized tonic-clonic seizures; and(4) PPR is most common with juvenile myoclonicepilepsy.
In patients with PGE, a routine EEG may cap-ture one or more absence seizures or epileptic myoclonicjerks. In children an absence seizure may be inducedduring the EEG study by hyperventilation with charac-teristic generalized 3 Hz spike wave discharge, which issustained for more than 3 seconds in duration. Epilepticmyoclonic jerks are associated in the EEG with high-amplitude generalized polyspike wave discharges in as-sociation with myoclonic jerks. Not well recognized isthe fact that the EEG in patients with PGE may record
Figure 21 EEG of a 46-year-old patientwith primary generalized epilepsy, showingatypical generalized bisynchronous spikewave activity.
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
28 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003
focal or lateralized spikes in addition to the overwhelm-ing generalized bisynchronous spike wave activity.84,85
Similarly, spike or spike wave activity occurring bilater-ally but restricted to the frontal areas (where the gener-alized paroxysms are usually maximum) is also com-mon. Such discharges are often called “abortive” spikewave complexes. Roughly one quarter of patients with 3Hz spike wave activity in their EEG may show suchfocal or lateralized discharges,84 which should generallybe viewed as isolated fragments or limited expression ofwhat is fundamentally a generalized epileptic abnormal-ity. Such focal epileptiform discharges often shift fromone electrode to the other and from one side to theother.
Secondary generalized epilepsy (SGE) is a moreserious disorder, secondary to known diffuse cerebralhemispheric insult. Patients are children who have fre-quent seizures of generalized type, usually medically re-fractory. Many have significant developmental delay andneurocognitive deficits. In contrast to PGE, the back-ground activity of the EEG in SGE syndrome is disor-ganized and there are variable degrees of slowing. In ad-dition, there are several paroxysmal EEG patternsassociated with SGE syndrome: (1) irregular bisynchro-nous spike wave activity described above, which canoccur both with PGE or SGE; (2) slow spike wave (2.5Hz or slower in frequency) discharges; (3) hypsarrhyth-mia; (4) independent multifocal spike discharges(IMSD); and (4) generalized paroxysmal fast activity(GPFA). These EEG patterns are largely nonspecific foretiology but are expressions of severe neocortical insult.Many of these EEG patterns are also age-dependent.
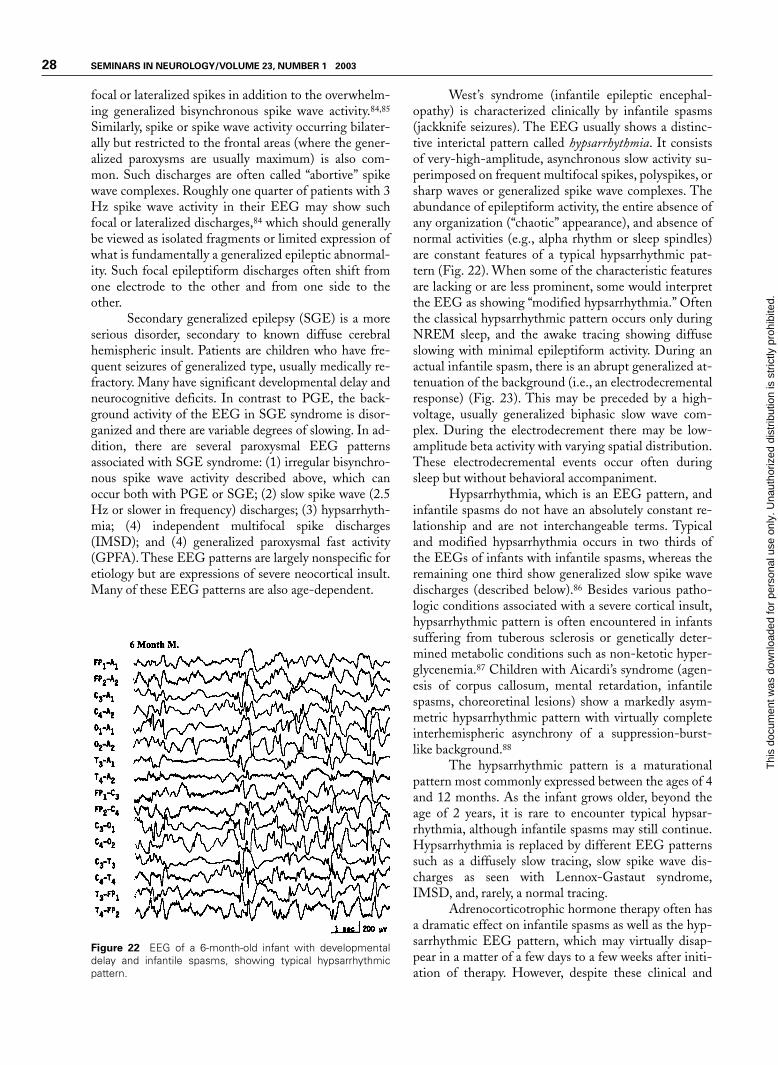
West’s syndrome (infantile epileptic encephal-opathy) is characterized clinically by infantile spasms(jackknife seizures). The EEG usually shows a distinc-tive interictal pattern called hypsarrhythmia. It consistsof very-high-amplitude, asynchronous slow activity su-perimposed on frequent multifocal spikes, polyspikes, orsharp waves or generalized spike wave complexes. Theabundance of epileptiform activity, the entire absence ofany organization (“chaotic” appearance), and absence ofnormal activities (e.g., alpha rhythm or sleep spindles)are constant features of a typical hypsarrhythmic pat-tern (Fig. 22). When some of the characteristic featuresare lacking or are less prominent, some would interpretthe EEG as showing “modified hypsarrhythmia.” Oftenthe classical hypsarrhythmic pattern occurs only duringNREM sleep, and the awake tracing showing diffuseslowing with minimal epileptiform activity. During anactual infantile spasm, there is an abrupt generalized at-tenuation of the background (i.e., an electrodecrementalresponse) (Fig. 23). This may be preceded by a high-voltage, usually generalized biphasic slow wave com-plex. During the electrodecrement there may be low-amplitude beta activity with varying spatial distribution.These electrodecremental events occur often duringsleep but without behavioral accompaniment.
Hypsarrhythmia, which is an EEG pattern, andinfantile spasms do not have an absolutely constant re-lationship and are not interchangeable terms. Typicaland modified hypsarrhythmia occurs in two thirds ofthe EEGs of infants with infantile spasms, whereas theremaining one third show generalized slow spike wavedischarges (described below).86 Besides various patho-logic conditions associated with a severe cortical insult,hypsarrhythmic pattern is often encountered in infantssuffering from tuberous sclerosis or genetically deter-mined metabolic conditions such as non-ketotic hyper-glycenemia.87 Children with Aicardi’s syndrome (agen-esis of corpus callosum, mental retardation, infantilespasms, choreoretinal lesions) show a markedly asym-metric hypsarrhythmic pattern with virtually completeinterhemispheric asynchrony of a suppression-burst-like background.88
The hypsarrhythmic pattern is a maturationalpattern most commonly expressed between the ages of 4and 12 months. As the infant grows older, beyond theage of 2 years, it is rare to encounter typical hypsar-rhythmia, although infantile spasms may still continue.Hypsarrhythmia is replaced by different EEG patternssuch as a diffusely slow tracing, slow spike wave dis-charges as seen with Lennox-Gastaut syndrome,IMSD, and, rarely, a normal tracing.
Adrenocorticotrophic hormone therapy often hasa dramatic effect on infantile spasms as well as the hyp-sarrhythmic EEG pattern, which may virtually disap-pear in a matter of a few days to a few weeks after initi-ation of therapy. However, despite these clinical and
Figure 22 EEG of a 6-month-old infant with developmentaldelay and infantile spasms, showing typical hypsarrhythmicpattern.
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
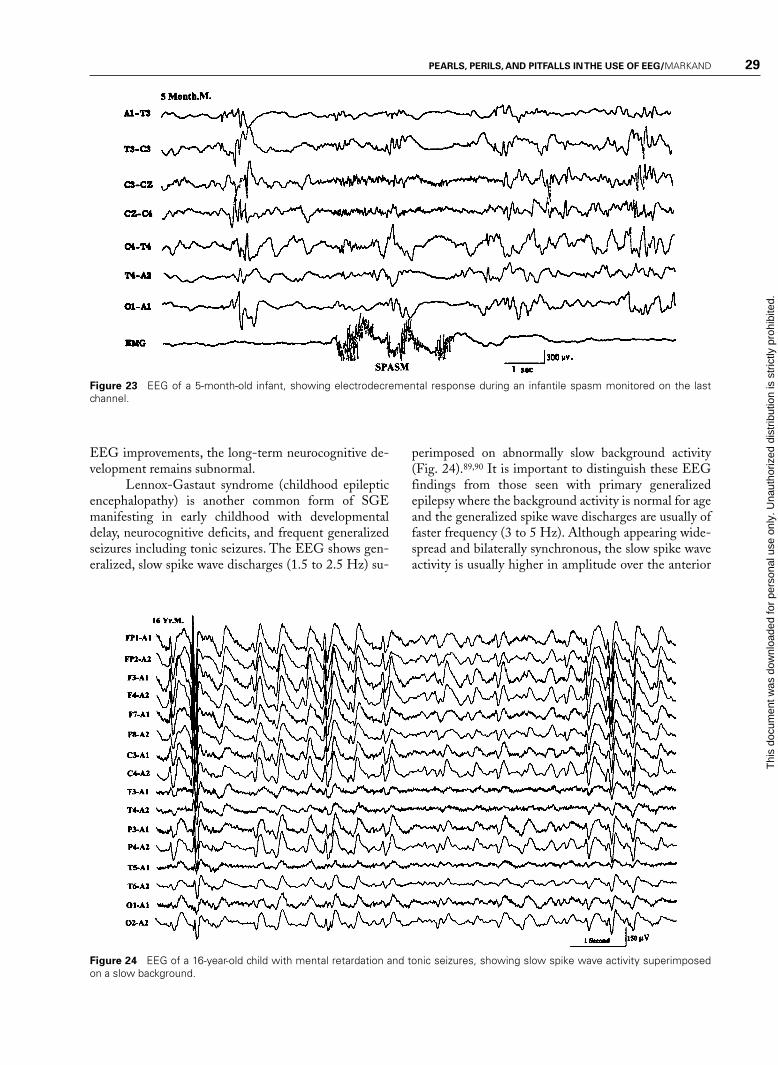
PEARLS, PERILS, AND PITFALLS IN THE USE OF EEG/MARKAND 29
Figure 23 EEG of a 5-month-old infant, showing electrodecremental response during an infantile spasm monitored on the lastchannel.
EEG improvements, the long-term neurocognitive de-velopment remains subnormal.
Lennox-Gastaut syndrome (childhood epilepticencephalopathy) is another common form of SGEmanifesting in early childhood with developmentaldelay, neurocognitive deficits, and frequent generalizedseizures including tonic seizures. The EEG shows gen-eralized, slow spike wave discharges (1.5 to 2.5 Hz) su-
perimposed on abnormally slow background activity(Fig. 24).89,90 It is important to distinguish these EEGfindings from those seen with primary generalizedepilepsy where the background activity is normal for ageand the generalized spike wave discharges are usually offaster frequency (3 to 5 Hz). Although appearing wide-spread and bilaterally synchronous, the slow spike waveactivity is usually higher in amplitude over the anterior
Figure 24 EEG of a 16-year-old child with mental retardation and tonic seizures, showing slow spike wave activity superimposedon a slow background.
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
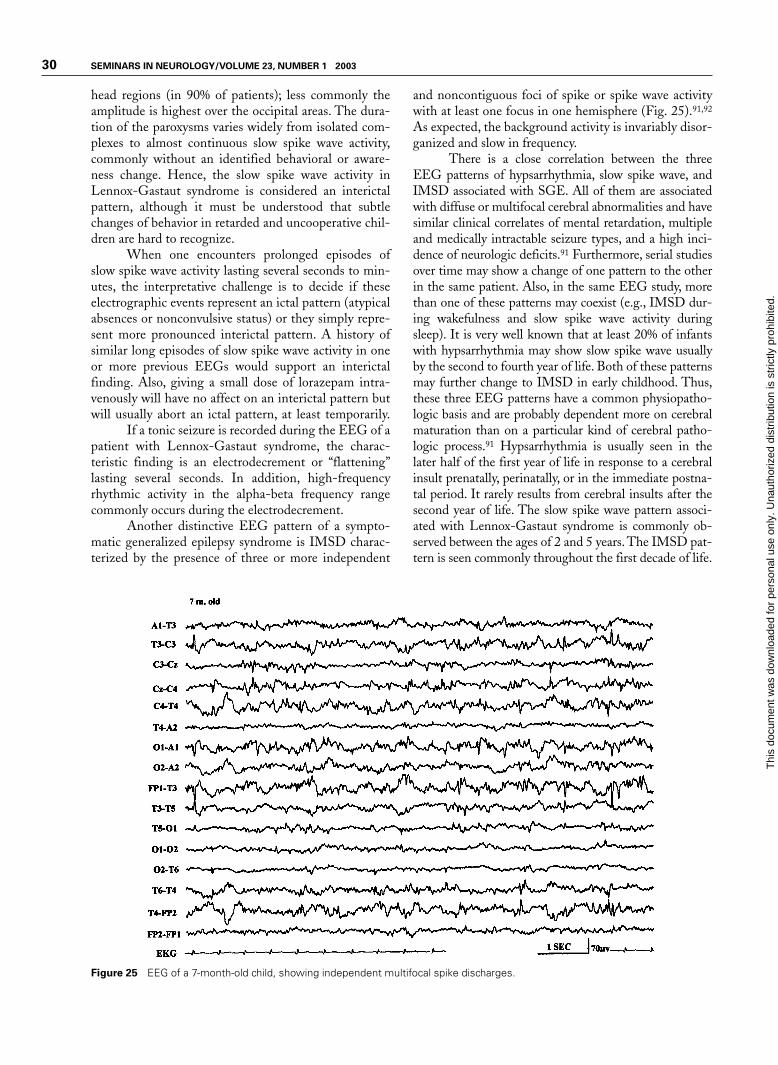
30 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003
head regions (in 90% of patients); less commonly theamplitude is highest over the occipital areas. The dura-tion of the paroxysms varies widely from isolated com-plexes to almost continuous slow spike wave activity,commonly without an identified behavioral or aware-ness change. Hence, the slow spike wave activity inLennox-Gastaut syndrome is considered an interictalpattern, although it must be understood that subtlechanges of behavior in retarded and uncooperative chil-dren are hard to recognize.
When one encounters prolonged episodes ofslow spike wave activity lasting several seconds to min-utes, the interpretative challenge is to decide if theseelectrographic events represent an ictal pattern (atypicalabsences or nonconvulsive status) or they simply repre-sent more pronounced interictal pattern. A history ofsimilar long episodes of slow spike wave activity in oneor more previous EEGs would support an interictalfinding. Also, giving a small dose of lorazepam intra-venously will have no affect on an interictal pattern butwill usually abort an ictal pattern, at least temporarily.
If a tonic seizure is recorded during the EEG of apatient with Lennox-Gastaut syndrome, the charac-teristic finding is an electrodecrement or “flattening”lasting several seconds. In addition, high-frequencyrhythmic activity in the alpha-beta frequency rangecommonly occurs during the electrodecrement.
Another distinctive EEG pattern of a sympto-matic generalized epilepsy syndrome is IMSD charac-terized by the presence of three or more independent
and noncontiguous foci of spike or spike wave activitywith at least one focus in one hemisphere (Fig. 25).91,92
As expected, the background activity is invariably disor-ganized and slow in frequency.
There is a close correlation between the threeEEG patterns of hypsarrhythmia, slow spike wave, andIMSD associated with SGE. All of them are associatedwith diffuse or multifocal cerebral abnormalities and havesimilar clinical correlates of mental retardation, multipleand medically intractable seizure types, and a high inci-dence of neurologic deficits.91 Furthermore, serial studiesover time may show a change of one pattern to the otherin the same patient. Also, in the same EEG study, morethan one of these patterns may coexist (e.g., IMSD dur-ing wakefulness and slow spike wave activity duringsleep). It is very well known that at least 20% of infantswith hypsarrhythmia may show slow spike wave usuallyby the second to fourth year of life. Both of these patternsmay further change to IMSD in early childhood. Thus,these three EEG patterns have a common physiopatho-logic basis and are probably dependent more on cerebralmaturation than on a particular kind of cerebral patho-logic process.91 Hypsarrhythmia is usually seen in thelater half of the first year of life in response to a cerebralinsult prenatally, perinatally, or in the immediate postna-tal period. It rarely results from cerebral insults after thesecond year of life. The slow spike wave pattern associ-ated with Lennox-Gastaut syndrome is commonly ob-served between the ages of 2 and 5 years. The IMSD pat-tern is seen commonly throughout the first decade of life.
Figure 25 EEG of a 7-month-old child, showing independent multifocal spike discharges.
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.

PEARLS, PERILS, AND PITFALLS IN THE USE OF EEG/MARKAND 31
Figure 26 EEG of an 11-year-old patientwith Lennox-Gastaut syndrome, showinggeneralized paroxysmal fast activity (B).
A unique EEG pattern of GPFA is seen pre-dominantly during sleep consisting of high-frequency,12 to 25 Hz repetitive spike discharges occurring syn-chronously over both hemispheres (Fig. 26).93 It is asso-ciated most commonly with SGE (usually Lennox-Gastaut syndrome) but it may rarely occur also withPGE or in patients with focal seizures, particularly witha frontal lobe focus. This EEG pattern is usually not as-sociated with an obvious clinical change, although sub-tle tonic seizures (opening of eyes and jaw, eye deviationupward) may be missed. In rare patients with PGE and3 Hz generalized spike wave, the awake EEG may ap-pear rather benign but the presence of GPFA duringsleep is a warning that more severe encephalopathy maybe present. In such patients, motor seizures are commonand the disorder is likely to persist in adulthood.94
EEG in Focal or Localization-Related Epilepsies
Focal epilepsies are usually categorized into two sub-groups: (1) asymptomatic (secondary) localization-related epilepsies due to acquired focal cortical pro-cesses; and (2) idiopathic (primary) localization-relatedepilepsies, which are largely age-dependent and geneti-cally based disorders, the best-known being benignRolandic epilepsy (BRE).
The hallmark of focal epilepsy in the interictalEEG is the presence of a focus of epileptiform activity(i.e., spikes, spike waves, or spike wave complexes). Theinterictal paroxysmal activity is characteristically ran-
dom, occurring at inconstant intervals. Intuitively, thepositive correlation of an abundance of epileptiformdischarges with a more frequent occurrence of clinicalseizures would be expected. This is, however, not true.Abundance and rate of repetition of epileptiform dis-charges correlate very poorly with the frequency of clin-ical seizures. It is not uncommon to see rare interictalspikes in a patient who has frequent complex partialseizures. The reverse is also true, as in BRE where thechild may have only rare clinical seizures but very abun-dant epileptiform discharges, particularly during sleep.An important fact regarding interictal epileptiform dis-charges is that they become much more frequent in theEEG immediately after a clinical focal seizure.77
Another characteristic of the interictal EEG is thepresence of a focal abnormality of the background activity.This may take the form of intermittent low-voltage slowwaves and attenuation of faster rhythm with the same lo-calization as that of the epileptiform discharges. In gen-eral, when the focal epileptiform activity occurs alongwith abnormal focal organization, the possibility of astructural lesion is more likely and the focal epilepsy ismost likely to be symptomatic. On the other hand, occur-rence of random focal spikes without any accompanyingfeatures of focal disorganization of the background activ-ity is usual with idiopathic or primary localization-related epilepsies such as BRE or benign occipitalepilepsy.
The majority (85%) of patients with complexpartial seizures have temporal lobe onset, whereas a
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
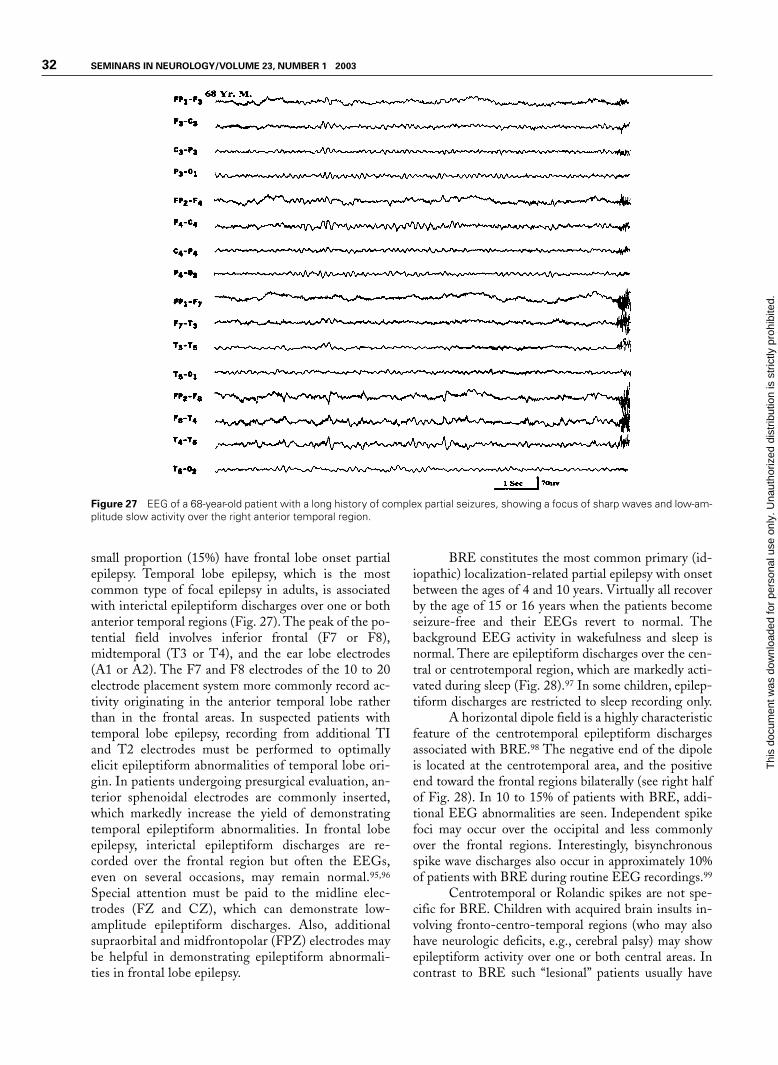
32 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003
Figure 27 EEG of a 68-year-old patient with a long history of complex partial seizures, showing a focus of sharp waves and low-am-plitude slow activity over the right anterior temporal region.
small proportion (15%) have frontal lobe onset partialepilepsy. Temporal lobe epilepsy, which is the mostcommon type of focal epilepsy in adults, is associatedwith interictal epileptiform discharges over one or bothanterior temporal regions (Fig. 27). The peak of the po-tential field involves inferior frontal (F7 or F8),midtemporal (T3 or T4), and the ear lobe electrodes(A1 or A2). The F7 and F8 electrodes of the 10 to 20electrode placement system more commonly record ac-tivity originating in the anterior temporal lobe ratherthan in the frontal areas. In suspected patients withtemporal lobe epilepsy, recording from additional TIand T2 electrodes must be performed to optimallyelicit epileptiform abnormalities of temporal lobe ori-gin. In patients undergoing presurgical evaluation, an-terior sphenoidal electrodes are commonly inserted,which markedly increase the yield of demonstratingtemporal epileptiform abnormalities. In frontal lobeepilepsy, interictal epileptiform discharges are re-corded over the frontal region but often the EEGs,even on several occasions, may remain normal.95,96
Special attention must be paid to the midline elec-trodes (FZ and CZ), which can demonstrate low-amplitude epileptiform discharges. Also, additionalsupraorbital and midfrontopolar (FPZ) electrodes maybe helpful in demonstrating epileptiform abnormali-ties in frontal lobe epilepsy.
BRE constitutes the most common primary (id-iopathic) localization-related partial epilepsy with onsetbetween the ages of 4 and 10 years. Virtually all recoverby the age of 15 or 16 years when the patients becomeseizure-free and their EEGs revert to normal. Thebackground EEG activity in wakefulness and sleep isnormal. There are epileptiform discharges over the cen-tral or centrotemporal region, which are markedly acti-vated during sleep (Fig. 28).97 In some children, epilep-tiform discharges are restricted to sleep recording only.
A horizontal dipole field is a highly characteristicfeature of the centrotemporal epileptiform dischargesassociated with BRE.98 The negative end of the dipoleis located at the centrotemporal area, and the positiveend toward the frontal regions bilaterally (see right halfof Fig. 28). In 10 to 15% of patients with BRE, addi-tional EEG abnormalities are seen. Independent spikefoci may occur over the occipital and less commonlyover the frontal regions. Interestingly, bisynchronousspike wave discharges also occur in approximately 10%of patients with BRE during routine EEG recordings.99
Centrotemporal or Rolandic spikes are not spe-cific for BRE. Children with acquired brain insults in-volving fronto-centro-temporal regions (who may alsohave neurologic deficits, e.g., cerebral palsy) may showepileptiform activity over one or both central areas. Incontrast to BRE such “lesional” patients usually have
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
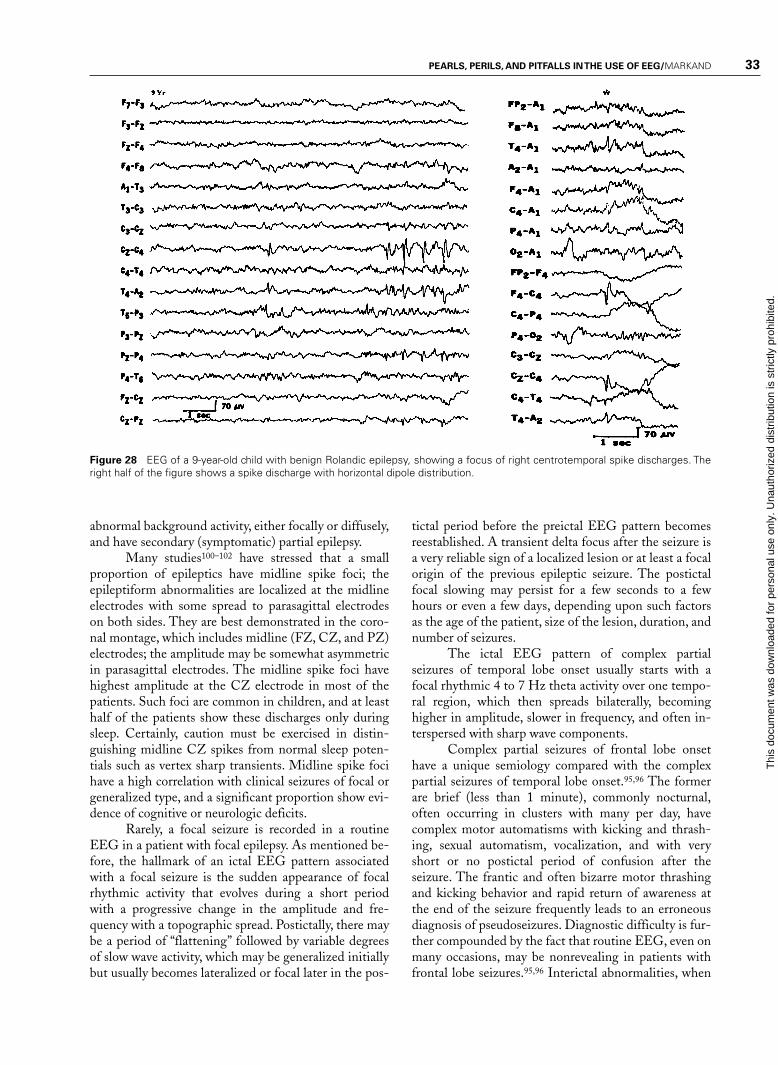
PEARLS, PERILS, AND PITFALLS IN THE USE OF EEG/MARKAND 33
Figure 28 EEG of a 9-year-old child with benign Rolandic epilepsy, showing a focus of right centrotemporal spike discharges. Theright half of the figure shows a spike discharge with horizontal dipole distribution.
abnormal background activity, either focally or diffusely,and have secondary (symptomatic) partial epilepsy.
Many studies100–102 have stressed that a smallproportion of epileptics have midline spike foci; theepileptiform abnormalities are localized at the midlineelectrodes with some spread to parasagittal electrodeson both sides. They are best demonstrated in the coro-nal montage, which includes midline (FZ, CZ, and PZ)electrodes; the amplitude may be somewhat asymmetricin parasagittal electrodes. The midline spike foci havehighest amplitude at the CZ electrode in most of thepatients. Such foci are common in children, and at leasthalf of the patients show these discharges only duringsleep. Certainly, caution must be exercised in distin-guishing midline CZ spikes from normal sleep poten-tials such as vertex sharp transients. Midline spike focihave a high correlation with clinical seizures of focal orgeneralized type, and a significant proportion show evi-dence of cognitive or neurologic deficits.
Rarely, a focal seizure is recorded in a routineEEG in a patient with focal epilepsy. As mentioned be-fore, the hallmark of an ictal EEG pattern associatedwith a focal seizure is the sudden appearance of focalrhythmic activity that evolves during a short periodwith a progressive change in the amplitude and fre-quency with a topographic spread. Postictally, there maybe a period of “flattening” followed by variable degreesof slow wave activity, which may be generalized initiallybut usually becomes lateralized or focal later in the pos-
tictal period before the preictal EEG pattern becomesreestablished. A transient delta focus after the seizure isa very reliable sign of a localized lesion or at least a focalorigin of the previous epileptic seizure. The postictalfocal slowing may persist for a few seconds to a fewhours or even a few days, depending upon such factorsas the age of the patient, size of the lesion, duration, andnumber of seizures.
The ictal EEG pattern of complex partialseizures of temporal lobe onset usually starts with afocal rhythmic 4 to 7 Hz theta activity over one tempo-ral region, which then spreads bilaterally, becominghigher in amplitude, slower in frequency, and often in-terspersed with sharp wave components.
Complex partial seizures of frontal lobe onsethave a unique semiology compared with the complexpartial seizures of temporal lobe onset.95,96 The formerare brief (less than 1 minute), commonly nocturnal,often occurring in clusters with many per day, havecomplex motor automatisms with kicking and thrash-ing, sexual automatism, vocalization, and with veryshort or no postictal period of confusion after theseizure. The frantic and often bizarre motor thrashingand kicking behavior and rapid return of awareness atthe end of the seizure frequently leads to an erroneousdiagnosis of pseudoseizures. Diagnostic difficulty is fur-ther compounded by the fact that routine EEG, even onmany occasions, may be nonrevealing in patients withfrontal lobe seizures.95,96 Interictal abnormalities, when
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
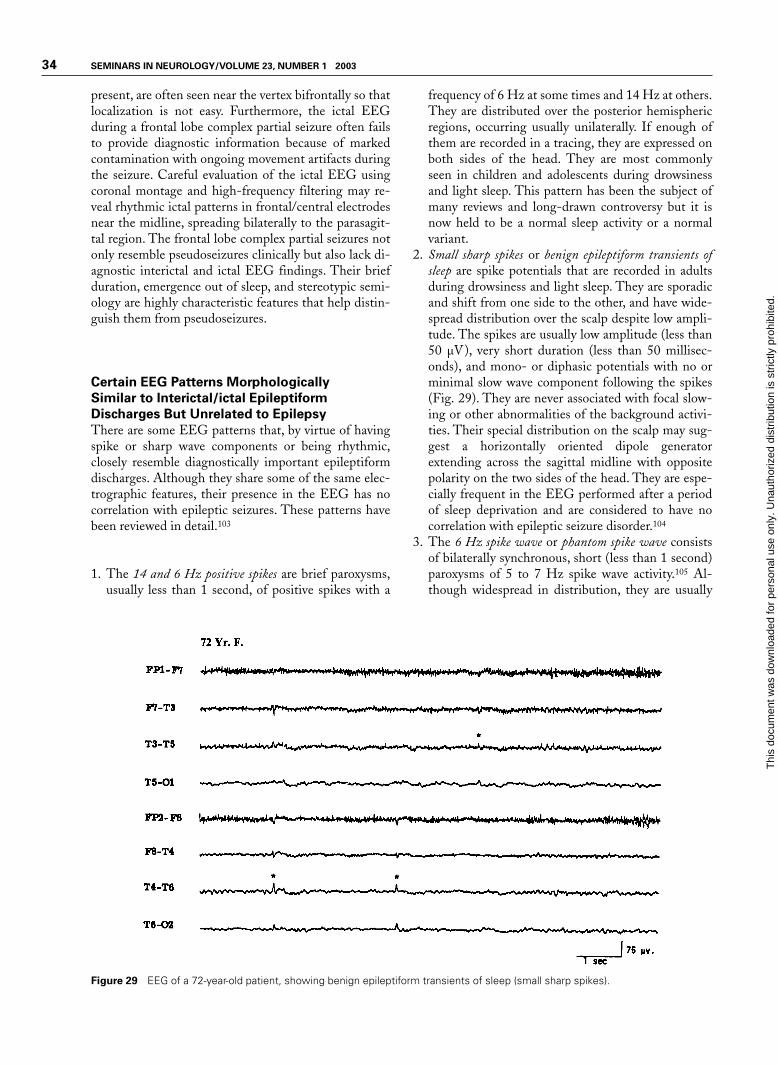
34 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003
present, are often seen near the vertex bifrontally so thatlocalization is not easy. Furthermore, the ictal EEGduring a frontal lobe complex partial seizure often failsto provide diagnostic information because of markedcontamination with ongoing movement artifacts duringthe seizure. Careful evaluation of the ictal EEG usingcoronal montage and high-frequency filtering may re-veal rhythmic ictal patterns in frontal/central electrodesnear the midline, spreading bilaterally to the parasagit-tal region. The frontal lobe complex partial seizures notonly resemble pseudoseizures clinically but also lack di-agnostic interictal and ictal EEG findings. Their briefduration, emergence out of sleep, and stereotypic semi-ology are highly characteristic features that help distin-guish them from pseudoseizures.
Certain EEG Patterns Morphologically
Similar to Interictal/ictal Epileptiform
Discharges But Unrelated to Epilepsy
There are some EEG patterns that, by virtue of havingspike or sharp wave components or being rhythmic,closely resemble diagnostically important epileptiformdischarges. Although they share some of the same elec-trographic features, their presence in the EEG has nocorrelation with epileptic seizures. These patterns havebeen reviewed in detail.103
1. The 14 and 6 Hz positive spikes are brief paroxysms,usually less than 1 second, of positive spikes with a
frequency of 6 Hz at some times and 14 Hz at others.They are distributed over the posterior hemisphericregions, occurring usually unilaterally. If enough ofthem are recorded in a tracing, they are expressed onboth sides of the head. They are most commonlyseen in children and adolescents during drowsinessand light sleep. This pattern has been the subject ofmany reviews and long-drawn controversy but it isnow held to be a normal sleep activity or a normalvariant.
2. Small sharp spikes or benign epileptiform transients ofsleep are spike potentials that are recorded in adultsduring drowsiness and light sleep. They are sporadicand shift from one side to the other, and have wide-spread distribution over the scalp despite low ampli-tude. The spikes are usually low amplitude (less than50 µV), very short duration (less than 50 millisec-onds), and mono- or diphasic potentials with no orminimal slow wave component following the spikes(Fig. 29). They are never associated with focal slow-ing or other abnormalities of the background activi-ties. Their special distribution on the scalp may sug-gest a horizontally oriented dipole generatorextending across the sagittal midline with oppositepolarity on the two sides of the head. They are espe-cially frequent in the EEG performed after a periodof sleep deprivation and are considered to have nocorrelation with epileptic seizure disorder.104
3. The 6 Hz spike wave or phantom spike wave consistsof bilaterally synchronous, short (less than 1 second)paroxysms of 5 to 7 Hz spike wave activity.105 Al-though widespread in distribution, they are usually
Figure 29 EEG of a 72-year-old patient, showing benign epileptiform transients of sleep (small sharp spikes).
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
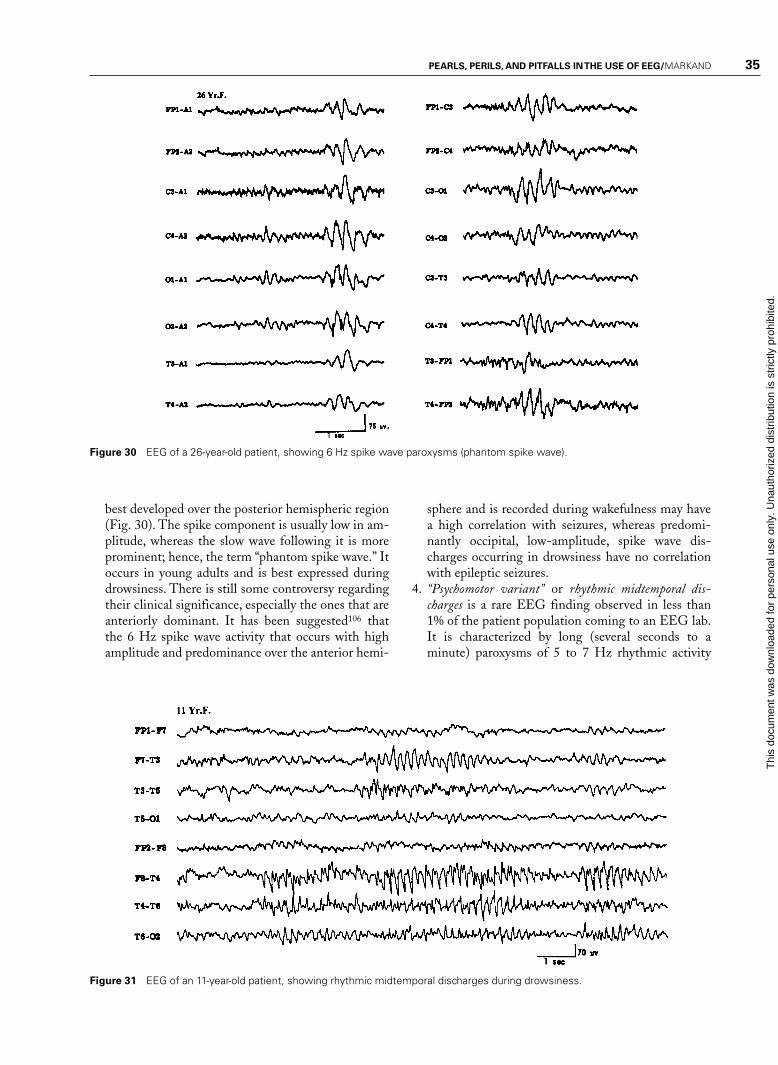
PEARLS, PERILS, AND PITFALLS IN THE USE OF EEG/MARKAND 35
Figure 30 EEG of a 26-year-old patient, showing 6 Hz spike wave paroxysms (phantom spike wave).
best developed over the posterior hemispheric region(Fig. 30). The spike component is usually low in am-plitude, whereas the slow wave following it is moreprominent; hence, the term “phantom spike wave.” Itoccurs in young adults and is best expressed duringdrowsiness. There is still some controversy regardingtheir clinical significance, especially the ones that areanteriorly dominant. It has been suggested106 thatthe 6 Hz spike wave activity that occurs with highamplitude and predominance over the anterior hemi-
sphere and is recorded during wakefulness may havea high correlation with seizures, whereas predomi-nantly occipital, low-amplitude, spike wave dis-charges occurring in drowsiness have no correlationwith epileptic seizures.
4. “Psychomotor variant” or rhythmic midtemporal dis-charges is a rare EEG finding observed in less than1% of the patient population coming to an EEG lab.It is characterized by long (several seconds to aminute) paroxysms of 5 to 7 Hz rhythmic activity
Figure 31 EEG of an 11-year-old patient, showing rhythmic midtemporal discharges during drowsiness.
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
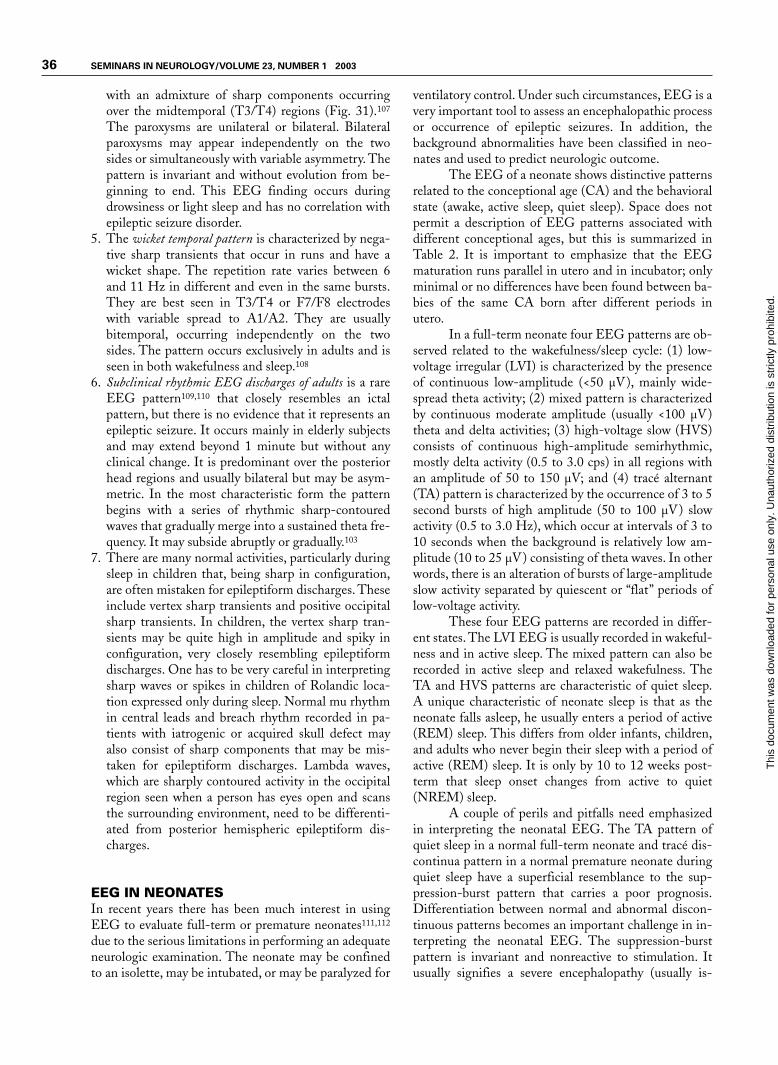
36 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003
with an admixture of sharp components occurringover the midtemporal (T3/T4) regions (Fig. 31).107
The paroxysms are unilateral or bilateral. Bilateralparoxysms may appear independently on the twosides or simultaneously with variable asymmetry. Thepattern is invariant and without evolution from be-ginning to end. This EEG finding occurs duringdrowsiness or light sleep and has no correlation withepileptic seizure disorder.
5. The wicket temporal pattern is characterized by nega-tive sharp transients that occur in runs and have awicket shape. The repetition rate varies between 6and 11 Hz in different and even in the same bursts.They are best seen in T3/T4 or F7/F8 electrodeswith variable spread to A1/A2. They are usuallybitemporal, occurring independently on the twosides. The pattern occurs exclusively in adults and isseen in both wakefulness and sleep.108
6. Subclinical rhythmic EEG discharges of adults is a rareEEG pattern109,110 that closely resembles an ictalpattern, but there is no evidence that it represents anepileptic seizure. It occurs mainly in elderly subjectsand may extend beyond 1 minute but without anyclinical change. It is predominant over the posteriorhead regions and usually bilateral but may be asym-metric. In the most characteristic form the patternbegins with a series of rhythmic sharp-contouredwaves that gradually merge into a sustained theta fre-quency. It may subside abruptly or gradually.103
7. There are many normal activities, particularly duringsleep in children that, being sharp in configuration,are often mistaken for epileptiform discharges. Theseinclude vertex sharp transients and positive occipitalsharp transients. In children, the vertex sharp tran-sients may be quite high in amplitude and spiky inconfiguration, very closely resembling epileptiformdischarges. One has to be very careful in interpretingsharp waves or spikes in children of Rolandic loca-tion expressed only during sleep. Normal mu rhythmin central leads and breach rhythm recorded in pa-tients with iatrogenic or acquired skull defect mayalso consist of sharp components that may be mis-taken for epileptiform discharges. Lambda waves,which are sharply contoured activity in the occipitalregion seen when a person has eyes open and scansthe surrounding environment, need to be differenti-ated from posterior hemispheric epileptiform dis-charges.
EEG IN NEONATESIn recent years there has been much interest in usingEEG to evaluate full-term or premature neonates111,112
due to the serious limitations in performing an adequateneurologic examination. The neonate may be confinedto an isolette, may be intubated, or may be paralyzed for
ventilatory control. Under such circumstances, EEG is avery important tool to assess an encephalopathic processor occurrence of epileptic seizures. In addition, thebackground abnormalities have been classified in neo-nates and used to predict neurologic outcome.
The EEG of a neonate shows distinctive patternsrelated to the conceptional age (CA) and the behavioralstate (awake, active sleep, quiet sleep). Space does notpermit a description of EEG patterns associated withdifferent conceptional ages, but this is summarized inTable 2. It is important to emphasize that the EEGmaturation runs parallel in utero and in incubator; onlyminimal or no differences have been found between ba-bies of the same CA born after different periods inutero.
In a full-term neonate four EEG patterns are ob-served related to the wakefulness/sleep cycle: (1) low-voltage irregular (LVI) is characterized by the presenceof continuous low-amplitude (<50 µV), mainly wide-spread theta activity; (2) mixed pattern is characterizedby continuous moderate amplitude (usually <100 µV)theta and delta activities; (3) high-voltage slow (HVS)consists of continuous high-amplitude semirhythmic,mostly delta activity (0.5 to 3.0 cps) in all regions withan amplitude of 50 to 150 µV; and (4) tracé alternant(TA) pattern is characterized by the occurrence of 3 to 5second bursts of high amplitude (50 to 100 µV) slowactivity (0.5 to 3.0 Hz), which occur at intervals of 3 to10 seconds when the background is relatively low am-plitude (10 to 25 µV) consisting of theta waves. In otherwords, there is an alteration of bursts of large-amplitudeslow activity separated by quiescent or “flat” periods oflow-voltage activity.
These four EEG patterns are recorded in differ-ent states. The LVI EEG is usually recorded in wakeful-ness and in active sleep. The mixed pattern can also berecorded in active sleep and relaxed wakefulness. TheTA and HVS patterns are characteristic of quiet sleep.A unique characteristic of neonate sleep is that as theneonate falls asleep, he usually enters a period of active(REM) sleep. This differs from older infants, children,and adults who never begin their sleep with a period ofactive (REM) sleep. It is only by 10 to 12 weeks post-term that sleep onset changes from active to quiet(NREM) sleep.
A couple of perils and pitfalls need emphasizedin interpreting the neonatal EEG. The TA pattern ofquiet sleep in a normal full-term neonate and tracé dis-continua pattern in a normal premature neonate duringquiet sleep have a superficial resemblance to the sup-pression-burst pattern that carries a poor prognosis.Differentiation between normal and abnormal discon-tinuous patterns becomes an important challenge in in-terpreting the neonatal EEG. The suppression-burstpattern is invariant and nonreactive to stimulation. Itusually signifies a severe encephalopathy (usually is-
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.

PEARLS, PERILS, AND PITFALLS IN THE USE OF EEG/MARKAND 37
Table 2 EEG Maturation in Preterm Neonates
EEG Features 24–27 Weeks CA 28–31 Weeks CA 32–35 Weeks CA 36–38 Weeks CA
Continuity Discontinuous, long Discontinuous or Discontinuous 50% of Continuous duringflat periods or tracé tracé discontinua time, more or less awake and AS; TAdiscontinua continuous 50% during QS
Differentiation of No differentiation No differentiation Wake/sleep diff. seen; Goodawake and sleep also AS/QS diff.
later in this periodTemporal theta Present Prominent Decreasing AbsentOccipital theta Prominent Decreasing Decreasing AbsentDelta brushes None or minimal Prominent, Present, mainly in QS, Rare in QS
AS > QS less or none in ASTracé alternant (TA) None None Prominent during QS Present in QS
(tracé discontinua)Interhemispheric Short bursts of Prominent Progressively Minor asynchrony
synchrony synchronous asynchrony more synchrony may still persistEEG activity
Sharp wave Some (temporal) Some scattered Often prominent Sharp waves lesstransients sharp activity sharp activity multifocal sharp prominent, seen
during bursts waves over frontal/temporal during QS
AS, active sleep; QS, quiet sleep; CA, conceptional age; diff., difference.
chemic/hypoxic), although it may occur transiently dueto recent intravenous sedative/hypnotic medication. Onthe other hand, the TA and tracé discontinua patternassociated with quiet sleep in full-term and prematureneonates, respectively, are state dependent and react tostimulation. In addition, long recordings would demon-strate activities characteristic of wakefulness and activesleep in normal full-term and premature (over 32 weeksCA) neonates. The TA pattern gradually disappearsover 6 weeks postterm when the HVS pattern becomesthe sole EEG accompaniment of quiet sleep.113
Another striking feature of the neonatal EEG isthe frequent occurrence of multifocal sharp transientsduring indeterminate and quiet sleep. These start ap-pearing at 35 weeks CA and constitute a normal findingin full-term neonates. The clinical significance of thesesharp transients remains controversial. It is difficult toclearly separate abnormal (pathologic) sharp wavesfrom normal sharp transients of the neonate. In general,the normal sharp transients are infrequent in occur-rence, usually blunt in morphology (rather than assum-ing spiky configuration), arise from any scalp locationbut are common over frontal and temporal regions, aretruly random in occurrence, without persistent focality,and largely confined to the burst phase of the TA pat-tern. However, no universal criteria have been estab-lished to separate normal sharp transients of the new-born from the abnormal sharp wave activity. Unless thesharp wave discharges are repetitive, periodic, or local-ized over one region, an epileptogenic significance mustnot be assigned to them. When the multifocal sharp
transients are very frequent and occur even during ac-tive sleep and wakefulness, the EEG is considered to beabnormal but suggestive merely of a nonspecific en-cephalopathic process.
A unique EEG pattern of pathologic signifi-cance is the presence of positive Rolandic sharp waves(PRS).114 PRS may be confined to one hemisphere; ifthey are bilateral they may be consistently more abun-dant over one hemisphere. They are usually maximumat CZ but may be lateralized to C3 or C4 electrodes(Fig. 32). Their positive polarity is a distinctive featurein addition to their localization. Although initially de-scribed as the EEG correlates of the intraventricularhemorrhage, PRS waves may be seen in other condi-tions, including periventricular leukomalacia, paren-chymal hemorrhage, hydrocephalus, hypoxic/ischemicinsult, and other conditions.112,115–117 Presently, theview is that PRS waves represent a marker of differentwhite matter lesions rather than being specific forperiventricular/intraventricular hemorrhage. Positivepolarity sharp waves at other locations (especially in thetemporal region) have no distinctive significance andmay just be a part of multifocal sharp transients in theneonates.
Abnormalities of the background activity in full-term neonates are usually classified as either severe ormild118–120 and are summarized in Table 3. The severeEEG abnormalities indicate severe impairment of brainfunction and carry a poor prognosis for survival and/orneurologic development. Severely abnormal EEG pat-terns consist of: (1) isoelectric EEG showing activity
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
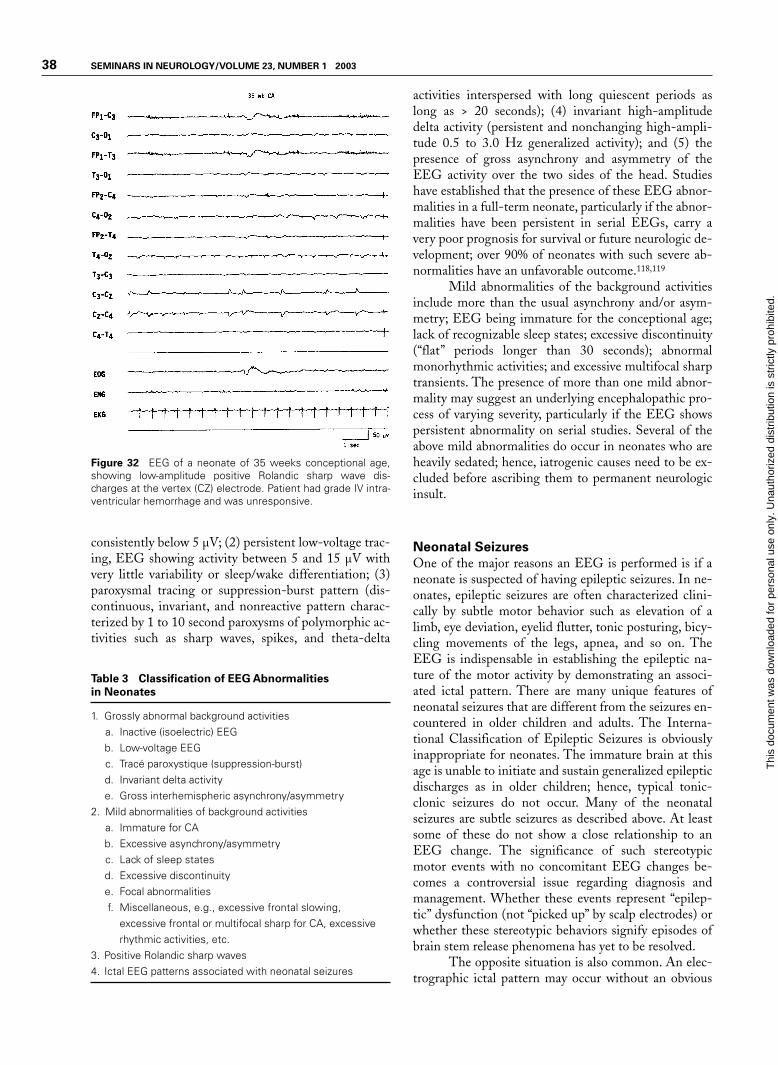
38 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003
Figure 32 EEG of a neonate of 35 weeks conceptional age,showing low-amplitude positive Rolandic sharp wave dis-charges at the vertex (CZ) electrode. Patient had grade IV intra-ventricular hemorrhage and was unresponsive.
consistently below 5 µV; (2) persistent low-voltage trac-ing, EEG showing activity between 5 and 15 µV withvery little variability or sleep/wake differentiation; (3)paroxysmal tracing or suppression-burst pattern (dis-continuous, invariant, and nonreactive pattern charac-terized by 1 to 10 second paroxysms of polymorphic ac-tivities such as sharp waves, spikes, and theta-delta
activities interspersed with long quiescent periods aslong as > 20 seconds); (4) invariant high-amplitudedelta activity (persistent and nonchanging high-ampli-tude 0.5 to 3.0 Hz generalized activity); and (5) thepresence of gross asynchrony and asymmetry of theEEG activity over the two sides of the head. Studieshave established that the presence of these EEG abnor-malities in a full-term neonate, particularly if the abnor-malities have been persistent in serial EEGs, carry avery poor prognosis for survival or future neurologic de-velopment; over 90% of neonates with such severe ab-normalities have an unfavorable outcome.118,119
Mild abnormalities of the background activitiesinclude more than the usual asynchrony and/or asym-metry; EEG being immature for the conceptional age;lack of recognizable sleep states; excessive discontinuity(“flat” periods longer than 30 seconds); abnormalmonorhythmic activities; and excessive multifocal sharptransients. The presence of more than one mild abnor-mality may suggest an underlying encephalopathic pro-cess of varying severity, particularly if the EEG showspersistent abnormality on serial studies. Several of theabove mild abnormalities do occur in neonates who areheavily sedated; hence, iatrogenic causes need to be ex-cluded before ascribing them to permanent neurologicinsult.
Neonatal Seizures
One of the major reasons an EEG is performed is if aneonate is suspected of having epileptic seizures. In ne-onates, epileptic seizures are often characterized clini-cally by subtle motor behavior such as elevation of alimb, eye deviation, eyelid flutter, tonic posturing, bicy-cling movements of the legs, apnea, and so on. TheEEG is indispensable in establishing the epileptic na-ture of the motor activity by demonstrating an associ-ated ictal pattern. There are many unique features ofneonatal seizures that are different from the seizures en-countered in older children and adults. The Interna-tional Classification of Epileptic Seizures is obviouslyinappropriate for neonates. The immature brain at thisage is unable to initiate and sustain generalized epilepticdischarges as in older children; hence, typical tonic-clonic seizures do not occur. Many of the neonatalseizures are subtle seizures as described above. At leastsome of these do not show a close relationship to anEEG change. The significance of such stereotypicmotor events with no concomitant EEG changes be-comes a controversial issue regarding diagnosis andmanagement. Whether these events represent “epilep-tic” dysfunction (not “picked up” by scalp electrodes) orwhether these stereotypic behaviors signify episodes ofbrain stem release phenomena has yet to be resolved.
The opposite situation is also common. An elec-trographic ictal pattern may occur without an obvious
Table 3 Classification of EEG Abnormalities
in Neonates
1. Grossly abnormal background activitiesa. Inactive (isoelectric) EEGb. Low-voltage EEGc. Tracé paroxystique (suppression-burst)d. Invariant delta activitye. Gross interhemispheric asynchrony/asymmetry
2. Mild abnormalities of background activitiesa. Immature for CAb. Excessive asynchrony/asymmetryc. Lack of sleep statesd. Excessive discontinuitye. Focal abnormalitiesf. Miscellaneous, e.g., excessive frontal slowing,
excessive frontal or multifocal sharp for CA, excessiverhythmic activities, etc.
3. Positive Rolandic sharp waves4. Ictal EEG patterns associated with neonatal seizures
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.

PEARLS, PERILS, AND PITFALLS IN THE USE OF EEG/MARKAND 39
clinical change. Such “subclinical” seizures are commonwith a pharmacologic neuromuscular blockade, stuporand coma following severe hypoxic/ischemic en-cephalopathy, multifocal status epilepticus, and follow-ing apparently successful treatment of status epilepticususing antiepileptic drugs.
The EEG ictal pattern is highly variable but con-sists of rhythmic activity of some sort, which is well lo-calized to a relatively small area of the brain. With rareexception, the ictal pattern in neonates is focal, unifocal,or multifocal. When multifocal, the ictal pattern mayoccur over two different regions at the same time butthe discharges have different waveforms and differentrepetition rates. Multifocal seizures simultaneously oc-curring on the two sides is a unique feature of neonatalepileptogenesis.
Interictal epileptiform abnormalities are rarelypresent to aid in the diagnosis of neonatal seizures. Multi-focal sharp transients over the frontal and temporal re-gions are common even in healthy neonates and, as men-tioned above, do not correlate with present or futureoccurrence of epileptic seizures. It appears that in neo-nates the epileptic process exhibits “all or none” features:either a seizure manifests overtly with appropriate electro-graphic features or has no interictal epileptiform markers.
Ictal EEG patterns associated with neonatalseizures are of four basic types111:
1. Focal spikes or spike wave discharges superimposedon a more or less normal background is an ictal pat-tern most commonly located over the Rolandic re-
gion (C3 or C4), and the frequency of the ictal dis-charge is usually over two per second (Fig. 33). Inneonates, focal EEG discharges and clinical seizuresdo not necessarily imply focal brain lesions. Com-mon etiologies include metabolic disturbances, suchas hypocalcemia or hypoglycemia, and subarachnoidhemorrhage. Such an ictal pattern, when associatedwith normal a EEG background, is prognostically favorable.
2. Another focal ictal pattern consists of slow-fre-quency sharp waves or complex waveforms repeatingapproximately one per second, never recruiting at afaster rate (Fig. 34). This pattern is similar toPLEDs. The background activity is almost alwayslow in amplitude. This pattern, called “depressed”brain discharges,121 is associated with a severe cere-bral insult (e.g., hypoxic/ischemic encephalopathy,encephalitis, cerebrovascular accident, etc.). The ac-companying clinical seizures are usually subtle or theEEG discharges are entirely subclinical.
3. Focal monorhythmic pattern in the beta, theta, anddelta frequency is a unique ictal pattern in neonates. Itmay start with low-amplitude focal 8 to 14 Hz activ-ity that slows down to 4 to 7 Hz and then to 0.5 to 3.0Hz rhythmic pattern. All types of combinations ofthe frequency band are possible but some ictal discharges may remain essentially monorhythmic(“alpha band” seizures) during a given seizure (Fig.35). The background is always abnormal and usuallylow in amplitude. This type of pattern has been re-ferred to as pseudo-beta-alpha-theta-delta ictal pat-
Figure 33 EEG of a 5-day-old neonate, showing focal ictal pattern characterized by rhythmic sharp waves in the left Rolandic re-gion.
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
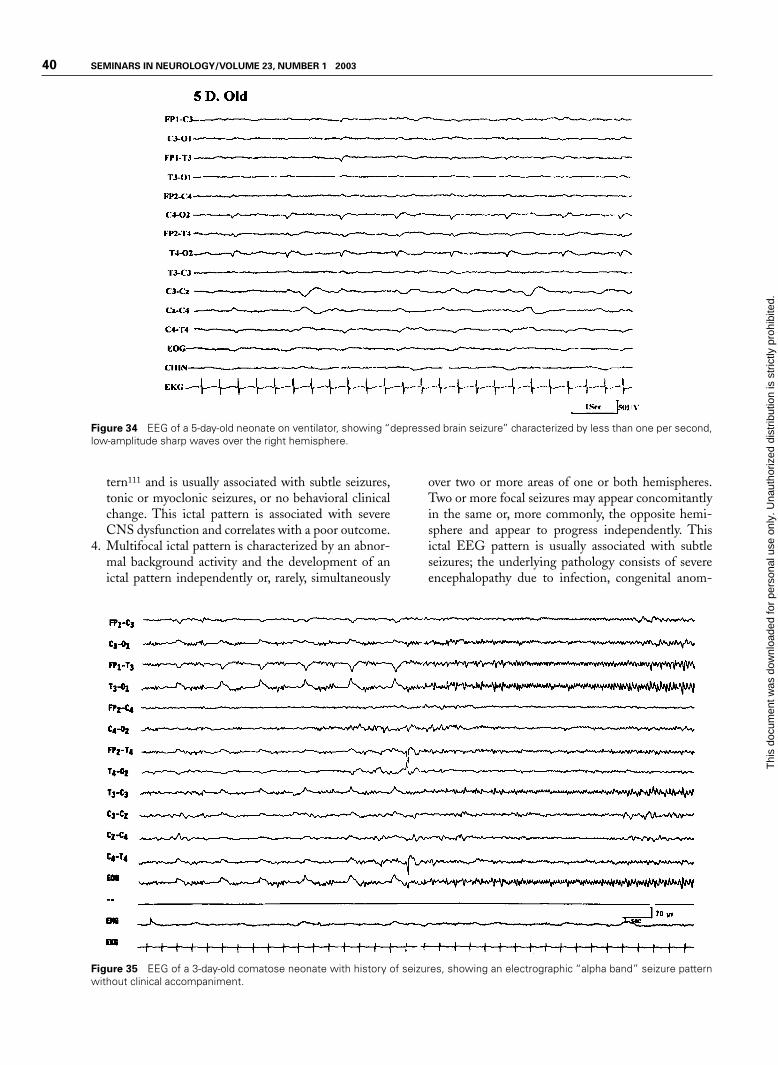
40 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003
Figure 34 EEG of a 5-day-old neonate on ventilator, showing “depressed brain seizure” characterized by less than one per second,low-amplitude sharp waves over the right hemisphere.
tern111 and is usually associated with subtle seizures,tonic or myoclonic seizures, or no behavioral clinicalchange. This ictal pattern is associated with severeCNS dysfunction and correlates with a poor outcome.
4. Multifocal ictal pattern is characterized by an abnor-mal background activity and the development of anictal pattern independently or, rarely, simultaneously
over two or more areas of one or both hemispheres.Two or more focal seizures may appear concomitantlyin the same or, more commonly, the opposite hemi-sphere and appear to progress independently. Thisictal EEG pattern is usually associated with subtleseizures; the underlying pathology consists of severeencephalopathy due to infection, congenital anom-
Figure 35 EEG of a 3-day-old comatose neonate with history of seizures, showing an electrographic “alpha band” seizure patternwithout clinical accompaniment.
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.

PEARLS, PERILS, AND PITFALLS IN THE USE OF EEG/MARKAND 41
alies, birth trauma, or anoxia. This pattern carries apoor prognosis for normal neurologic development.
Technical aspects
Several technical points are of crucial importance to op-timize neonatal EEG recording. The study should belong enough to include active and quiet sleep; the totalduration of the recording may exceed the usual 30 min-utes recommended in adults. In most neonates it may benecessary to record the EEG for 45 to 60 minutes. Thepresence of sleep differentiation is an important matu-rational feature for EEG interpretation. Some abnor-mal patterns such as the degree of discontinuity, asyn-chrony and asymmetry, presence of multifocal sharptransients, or delta brushes can be evaluated only inquiet sleep. Additionally, polygraphic variables must beroutinely recorded in addition to several channels ofscalp EEG. These include respiration, extraocularmovements, EKG, and chin activity. These non-EEGvariables are critical in identifying different states(awake, active sleep, or quiet sleep) and recognition ofvarious artifacts. A neonatal EEG lacking such poly-graphic variables is difficult to interpret unless it isgrossly abnormal.
EEG IN STATUS EPILEPTICUSStatus epilepticus (SE) is usually defined as continuousseizure activity persisting for more than 30 minutes ormore than one sequential seizure without full recoveryof consciousness between seizures. A very common rea-son for ordering an emergency EEG is for the diagnosisand management of SE. A simplified classification ofSE includes: (1) generalized convulsive status, charac-terized by motor seizures with loss of consciousness; (2)simple partial or focal status, characterized by focalmotor seizures repeating frequently or epilepsia partialiscontinua with the patient remaining fully conscious;and (3) nonconvulsive status (NCSE) characterized by avariable alteration of consciousness with minimal or nomotor activity.
NCSE poses many challenging nosologic, diag-nostic, and therapeutic problems. NCSE includes: (1)absence status, occurring in the setting of generalizedepilepsy (idiopathic or symptomatic) and (2) complexpartial status associated with focal or partial epilepsy offrontal or temporal onset. In both types, the patient maypresent with mental status alteration (e.g., slowness inbehavior and mentation, confusion, and, rarely, stuporor coma). Then, there are patients who after treatmentof generalized convulsive status continue to be ob-tunded or comatose and show epileptiform dischargesin their EEG. These patients are often designated ashaving “subtle” SE or lumped under NCSE.
It is relatively easy to diagnose NCSE associ-ated with focal epilepsy when there are frequent elec-trographic focal seizures with an ictal EEG patternthat evolves over time with change in the amplitude,frequency, and spatial distribution. However, it isquite common for the ictal EEG pattern associatedwith complex partial status associated with focalepilepsy to be generalized spikes or sharp waves re-peating at 1 to 6 Hz frequency. Such a generalizedEEG pattern is similar to that seen in typical absencestatus associated with idiopathic generalized epilepsy(absence epilepsy) and atypical absence status in chil-dren with secondary generalized epilepsy of theLennox-Gastaut type. To complicate the situationeven further, patients with Lennox-Gastaut syndromeinterictally have generalized 1.0 to 3.0 cps spike wavedischarges that may be very frequent, and one needs todecide if they represent an ictal pattern (hence atypi-cal absence status) or simply represent a prominent in-terictal pattern. Some waxing or waning of such gen-eralized epileptiform discharges may not help in thedistinction because this may be simply related to statechanges.
Some helpful criteria are proposed by Young etal122 in patients who show almost continuously occur-ring generalized, nonevolving epileptiform dischargesin their EEGs, including repetitive generalized or focalepileptiform discharges (spikes, sharp waves, and spikewaves) that repeat at a rate faster than three per second,very likely represent an ictal pattern. Such repetitivedischarges at a frequency slower than three per secondare likely to be ictal if significant clinical and/or EEGimprovement is demonstrated following small doses ofintravenous lorazepam or diazepam. Rhythmic sinu-soidal waves of any frequency (ranging from � to � fre-quency) may represent an ictal pattern if there is anevolving pattern at the onset (increasing amplitudeand/or decreasing frequency) or a decrement pattern atthe termination (decremental amplitude or frequency)or postdischarge slowing or voltage attenuation.
In a patient with obtundation or mental statuschange of recent onset, an EEG is indicated to rule outNCSE. If repetitive generalized epileptiform dischargesare recorded in the EEG, 1 to 2 mg of lorazepam or 5 to10 mg of diazepam are injected intravenously while theEEG is running. A marked clinical improvement of ob-tundation and disappearance of generalized paroxysmalactivity in the EEG would strongly support the diagno-sis of NCSE (Figs. 36 and 37). Such a rewarding expe-rience is most common in typical absence status and lesscommon in other forms of NCSE.
Reviewing the previous EEG and obtaining fol-low-up EEG studies also provide a helpful distinctionbetween ictal and interictal basis for the repetitive gen-eralized spike wave discharges seen in children with
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
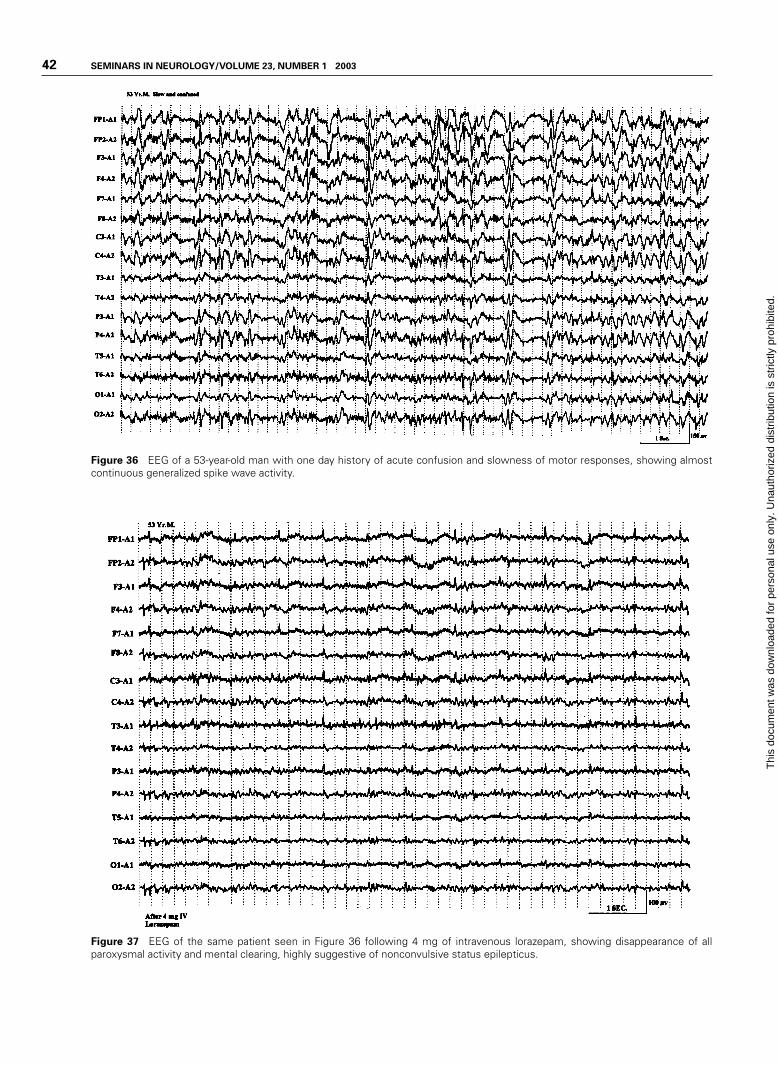
42 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003
Figure 36 EEG of a 53-year-old man with one day history of acute confusion and slowness of motor responses, showing almostcontinuous generalized spike wave activity.
Figure 37 EEG of the same patient seen in Figure 36 following 4 mg of intravenous lorazepam, showing disappearance of allparoxysmal activity and mental clearing, highly suggestive of nonconvulsive status epilepticus.
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.

PEARLS, PERILS, AND PITFALLS IN THE USE OF EEG/MARKAND 43
Lennox-Gastaut syndrome. A period of frequent repet-itive generalized spike wave discharges associated withclinical deterioration of mental status is more likely anepisode of atypical absence status, particularly if theprevious EEGs or follow-up EEGs display dramaticallyfewer epileptiform abnormalities.
“Subtle” SE commonly includes patients whohad a known episode of convulsive or generalized tonic-clonic status, brought under control by intravenousantiepileptic therapy (e.g., phenytoin, lorazepam, andbarbiturates), but continue to remain obtunded or co-matose without significant motor activity. EEG of suchpatients often show repetitive discharges, which may in-clude lateralized periodic discharges (e.g., PLEDs orBiIPLEDS) or generalized periodic discharges (PEDs).Some epileptologists123 are of the opinion that progres-sive sequential EEG changes occur during generalizedconvulsive SE with an “intermediary” pattern of PEDsand PLEDs (unilateral or bilateral) before disappear-ance of all paroxysmal EEG activities, and that thepresence of these “intermediary” EEG patterns necessi-tate further aggressive therapeutic measures (e.g., in-ducing pentobarbital coma, etc.). Such views are notuniversal. Many, on the other hand, consider PED andPLED patterns observed during the course of convul-sive status not an ictal pattern but suggestive of a severeepileptic encephalopathy reflective of a neuronal dys-function from underlying brain damage.124
Refractory SE is usually treated by continuousintravenous anesthesia maintained by pentobarbital,propofol, or medazolam. The dose is regulated such asto control all clear-cut clinical or electrographic seizuresand to maintain a suppression-burst pattern in theEEG. Therefore, continuous bedside EEG is moni-tored. There is no consensus as to the duration of“burst” and “flat” periods for optimal dosing. Most con-sider that establishing and maintaining any degree ofsuppression-burst pattern is adequate.
One final note of caution is that focal motorseizures including epilepsia partialis continua may notshow ictal changes in the EEG because of the limited sizeof neuronal tissue involved during the epileptic seizure orbecause the ictal pattern in the EEG may be obscured byartifacts. Careful review of the EEG using different mon-tages (especially a transverse bipolar montage goingthrough the midline electrodes) and use of appropriatemuscle filters may reveal a low-amplitude ictal pattern.
REFERENCES
1. Markand ON. Alpha rhythms. J Clin Neurophysiol 1990;7:163–189
2. Adams A. Studies on the flat electroencephalogram in man.Electroencephalogr Clin Neurophysiol 1959;11:35–41
3. Obrist WD. The electroencephalogram of normal agedadults. Electroencephalogr Clin Neurophysiol 1954;6:235–244
4. Busse EM, Obrist WD. Significance of focal electroen-cephalographic changes in the elderly. Postgrad Med 1963;34:179–182
5. Orbrist WD. Problems of aging. In: Remond A, ed. Hand-book of Electroencephalography and Clinical Neurophysiol-ogy. Vol. 6A. Amsterdam: Elsevier; 1976:275–292
6. Hubbard O, Sunde D, Goldenshon ES. The EEG changesin centenarians. Electroencephalogr Clin Neurophysiol1976;40:407–417
7. Torres F, Faovo A, Loewenson R, et al. The electroen-cephalogram of elderly subjects revisited. Electroenceph-alogr Clin Neurophysiol 1983;56:391–398
8. Kooi KA, Gurener AM, Tupper CJ, et al. Electroencephalo-graphic patterns of the temporal region in normal adults.Neurology 1964;14:1029–1035
9. Katz RI, Horowitz GR. Electroencephalogram in septuage-narian: studies in a normal geriatric population. J Am Geri-atr Soc 1982;3:273–275
10. Markand ON. Electroencephalography in diffuse encephal-opathies. J Clin Neurophysiol 1984;1:357–407
11. Hockaday JM, Potts F, Epstein E, et al. Electroencephalo-graphic changes in acute cerebral anoxia from cardiac or res-piratory arrest. Electroencephalogr Clin Neurophysiol 1965;18:575–586
12. Prior PF. The EEG in Acute Cerebral Anoxia. Amsterdam:Excerpta Medica; 1973
13. Cordeau JP. Monorhythmic frontal delta activity in humanelectroencephalogram: a study of 100 cases. Electroenceph-alogr Clin Neurophysiol 1959;11:733–746
14. Schaul N, Lüders H, Sachdev K. Generalized, bilaterallysynchronous bursts of slow waves in the EEG. Arch Neurol1981;38:690–692
15. Bickford RG, Butt HR. Hepatic coma: the electroen-cephalographic pattern. J Clin Invest 1955;34:790–799
16. Simsarian JP, Harner RN. Diagnosis of metabolic en-cephalopathy: significance of triphasic waves in the elec-troencephalogram [abstract]. Neurology 1972;22:456
17. Karnze DS, Bickford RG. Triphasic waves: a reassessment oftheir significance. Electroencephalogr Clin Neurophysiol1984;57:193–198
18. Fisch BJ, Klass DW. The diagnostic specificity of triphasicwave patterns. Electroencephalogr Clin Neurophysiol 1988;70:1–8
19. Reiher J. The electroencephalogram in the investigation ofmetabolic comas. Electroencephalogr Clin Neurophysiol1970;28:104
20. Bahmon-Dussan JE, Celesia GG, Grigg-Damberger MM.Prognostic significance of EEG triphasic waves in patientswith altered states of consciousness. J Clin Neurophysiol1989;6:313–319
21. MacGillivray BB, Kennedy J. The “triphasic waves” of he-patic encephalopathy [abstract]. Electroencephalogr ClinNeurophysiol 1970;28:428P
22. Aoki Y, Lombroso CT. Prognostic value of electroencephalog-raphy in Reye’s syndrome. Neurology 1973;23: 333–343
23. Yamada T, Young S, Kimura J. Significance of positive spikebursts in Reye’s syndrome. Arch Neurol 1977;34:376–380
24. Drury I. 14-and-6 positive bursts in childhood encephal-opathies. Electroencephalogr Clin Neurophysiol 1989;72:479–485
25. Carroll WM, Mastaglia FL. Alpha and beta coma in drugintoxication uncomplicated by cerebral hypoxia. Electroen-cephalogr Clin Neurophysiol 1979;46:95–105
26. Kuroiwa Y, Furukawa T, Inaki K. Recovery from drug-in-duced alpha-coma. Neurology 1981;31:1359–1361
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
44 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003
27. Stockard TJ, Werner SS, Albers JA, et al. EEG findings inphencyclidine intoxication. Arch Neurol 1976;33:200–203
28. Kuroiwa Y, Celesia GG, Chung HD. Periodic EEG dis-charges and status spongiosus of the cerebral cortex inanoxic encephalopathy: a necropsy case report. J NeurolNeurosurg Psychiatry 1982;45:740–742
29. Paz D, Brenner RD. Bilateral independent periodic lateral-ized epileptiform discharges, clinical significance. ArchNeurol 1981;38:713–715
30. McCarty GE, Marshall DW. Transient eyelid opening asso-ciated with postanoxic EEG suppression-burst pattern.Arch Neurol 1981;38:754–756
31. Reeves AL, Westmoreland BF, Klass DW. Clinical accom-paniments of the burst-suppression EEG pattern. J ClinNeurophysiol 1997;14:150–153
32. Chokroverty S. “Alpha-like” rhythms in electroencephalo-grams in coma after cardiac arrest. Neurology 1975;25:655–663
33. Westmoreland BF, Klass DW, Sharbrough FW, et al. “Alphacoma:” electroencephalographic, clinical, pathological andetiological correlation. Arch Neurol 1975;32:713–718
34. Alving J, Miller M, Sindrup E, et al. Alpha-pattern comafollowing cerebral anoxia. Electroencephalogr Clin Neuro-physiol 1979;47:95–101
35. Kuroiwa Y, Furukawa T. EEG prognostication in drug re-lated alpha coma [letter]. Arch Neurol 1981;38:200
36. Chatrian GE, White LE Jr, Shaw CM. EEG pattern resem-bling wakefulness in unresponsive decerebrate state follow-ing traumatic brainstem infarct. Electroenceph Clin Neuro-physiol 1964;16:285–289
37. American EEG Society. Guideline three: minimum techni-cal standards for EEG recording in suspected cerebral death.J Clin Neurophysiol 1994;11:10–13
38. Report of Special Task Force. Guidelines for the determina-tion of brain death in children. Pediatrics 1987;80:298–300
39. Markand ON. EEG in the diagnosis of CNS infections. In:Roos KL, ed. Central Nervous System Infectious Diseasesand Therapy. New York: Marcel Dekker; 1997:667–689
40. Illis LS, Taylor RM. The electroencephalogram in herpessimplex encephalitis. Lancet 1972;1:718–721
41. Gupta PC, Seth P. Periodic complex in herpes simplex en-cephalitis: a clinical and experimental study. Electroen-cephalogr Clin Neurophysiol 1973;35:67–74
42. Chien LT, Boehm RM, Robinson H, et al. Characteristicearly electroencephalographic changes in herpes simplex en-cephalitis: clinical and virologic studies. Arch Neurol 1977;34:361–364
43. Upton A, Gumpert J. Electroencephalography in the diag-nosis of herpes simplex encephalitis. Lancet 1970;1:650–652
44. Markand ON, Daly DD. Pseudoperiodic lateralized parox-ysmal discharges in electroencephalogram. Neurology 1971;21:975–981
45. Cobb W, Hill D. Electroencephalogram in subacute pro-gressive encephalitis. Brain 1950;73:392–404
46. Cobb W. The periodic events of subacute sclerosingleukoencephalitis. Electroenceph Clin Neurophysiol 1966;21:278–294
47. Markand ON, Panszi JG. The electroencephalogram in sub-acute sclerosing panencephalitis. Arch Neurol 1975;32:719–726
48. Westmoreland BF, Gomex MR, Blume WT. Activation ofperiodic complexes of subacute sclerosing panencephalitis bysleep. Ann Neurol 1977;1:185–187
49. Burger LJ, Rowan J, Goldenshon E. Creutzfeldt-Jakob dis-ease. Arch Neurol 1972;26:428–433
50. Au WJ, Gabor AJ, Viyan N, Markand ON. Periodic lateral-ized epileptiform complexes (PLEDs) in Creutzfeldt-Jakobdisease. Neurology 1980;30:611–617
51. Furlan A, Henry CE, Sweeny PI, et al. Focal EEG abnor-malities in Heidenhain’s variant of Jakob-Creutzfeldt dis-ease. Arch Neurol 1981;38:312–314
52. Chiofalo N, Fuentes A, Galvez S. Serial EEG findings in 27cases of Creutzfeldt-Jakob disease. Arch Neurol 1980;37:143–145
53. Chiappa KH, Burke CJ, Young RR. Creutzfeldt-Jakob dis-ease: periodic sharp waves in the EEG as an invariant ele-ment of the clinical syndrome. Presented at the AmericanAcademy of Neurology Meeting, Chicago, 1979
54. Gloor P, Kalaby O, Giard N. The electroencephalogram indiffuse encephalopathies: electroencephalographic correlatesof gray and white matter lesion. Brain 1968;91:779–802
55. Pampiglione G, Harden A. Neurophysiological identifica-tion of a late infantile form of “neuronal lipidosis.” J NeurolNeurosurg Psychiatry 1973;36:68–74
56. Letemendia F, Pampiglione G. Clinical and EEG observa-tion in Alzheimer’s disease. J Neurol Neurosurg Psychiatry1958;21:167–172
57. Liddell DW. Investigation of EEG findings in presenile de-mentia. J Neurol Neurosurg Psychiatry 1958;21:173–176
58. Gordon EB, Sim M. The EEG in presenile dementia. JNeurol Neurosurg Psychiatry 1967;30:285–291
59. Muller HF, Kral VA. The electroencephalogram in advancedsenile dementia. J Am Geriatr Soc 1967;15:415–426
60. Margerison JH, Scott DF. Huntington’s chorea: clinicalEEG and neuropathological findings [abstract]. Electroen-cephalogr Clin Neurophysiol 1965;19:314
61. Daly DD, Markand ON: Focal brain lesions. In: Daly DD,Pedley TA, eds. Current Practice of Clinical Electroen-cephalography. 2nd ed. New York: Raven Press; 1990:335–370
62. Walter WG. The location of cerebral tumours by electroen-cephalography. Lancet 1936;11:305–308
63. Arfel G, Fischgold H. EEG-signs in tumours of the brain.Electroencephalogr Clin Neurophysiol 1961;19(suppl):36–50
64. Brenner R, Sharbrough F. Electroencephalographic evaluationin Sturge-Weber syndrome. Neurology 1976;26:629–632
65. Kershmann J, Conde A, Gibson WC. Electroencephalogra-phy in differential diagnosis of supratentorial tumors. ArchNeurol Psychiatry (Chicago) 1949;62:255–268
66. Cobb WA, Guillof RJ, Cast J. Breach rhythm: the EEG re-lated to skull defects. Electroencephalogr Clin Neurophysiol1979;47:251–271
67. Chatrian GE, Shaw CM, Leftman H. The significance ofperiodic lateralized epileptiform discharges in EEG: anelectrographic, clinical and pathological study. Electroen-cephalogr Clin Neurophysiol 1964;17:177–193
68. Maulsby RL. Some guidelines for assessment of spikes andsharp waves in EEG tracings. Am J EEG Technol 1971;11:3–16
69. Gloor P. The EEG and differential diagnosis of epilepsy. In:Van Duijn H, Donker DNJ, Van Huffelen AC, eds. CurrentConcepts in Clinical Neurophysiology. The Netherlands:NV Drukkerij Trio; 1977:9–21
70. Petersen I, Eeg-Olofsson O, Sellden U. Paroxysmal activityin EEG of normal children. In: Kellaway P, Petersen I, eds.Clinical Electroencephalography of Children. New York:Grune & Stratton; 1968:167–188
71. Eeg-Olofsson O, Petersen I, Sellden U. The development ofthe electroencephalogram in normal children from the age
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
PEARLS, PERILS, AND PITFALLS IN THE USE OF EEG/MARKAND 45
of one through fifteen years: paroxysmal activity. Neuropedi-atrie 1971;4:375–404
72. Zivin L, Ajmone-Marsan C. Incidence and prognostic sig-nificance of “epileptiform” activity in the EEG of nonepilep-tic subjects. Brain 1968;91:751–778
73. Goodin DS, Aminoff MJ. Does the interictal EEG have arole in the diagnosis of epilepsy. Lancet 1984;1:837–839
74. Bridgers SL. Epileptiform abnormalities discovered on elec-troencephalographic screening of psychiatric inpatients.Arch Neurol 1987;44:312–316
75. Gregory RP, Oates T, Merry RTG. Electroencephalogramepileptiform abnormalities in candidates for aircrew train-ing. Electroencephalogr Clin Neurophysiol 1993;86:75–77
76. Salinsky M, Kanter R, Dasheiff R. Effectiveness of multipleEEGs in supporting the diagnosis of epilepsy: an opera-tional curve. Epilepsia 1987;28:331–334
77. Gotman J, Marciani MG. Electroencephalographic spikingactivity, drug levels and seizure occurrence in epileptic pa-tients. Ann Neurol 1985;17:597–603
78. Reilly EL, Peters JF. Relationship of some varieties of elec-troencephalographic photosensitivity to clinical convulsivedisorders. Neurology 1973;23:1050–1057
79. Puglia JF, Brenner RP, Soso MJ. Relationship between pro-longed and self-limited photoparoxysmal responses andseizure incidence: study and review. J Clin Neurophysiol1992;9:137–144
80. Wolf P, Gooses R. Relation of photosensitivity to epilepticsyndromes. J Neurol Neurosurg Psychiatry 1986;49:1386–1391
81. Silverman D. The anterior temporal electrode and the ten-twenty system. Electroencephalogr Clin Neurophysiol 1960;12:735–737
82. Goodin DA, Aminoff MJ, Laxer KD. Detection of epilepti-form activity by different noninvasive EEG methods incomplex partial epilepsy. Ann Neurol 1990;27:330–334
83. Markand ON. Psychogenic seizures (pseudoseizures). In:Radhakrishnan K, ed. Medically Refractory Epilepsy.Trivandrum, India: Sree Chitra Tirunal Institute of MedicalSciences and Technology; 1999:61–75
84. Gabor AJ, Ajmone-Marsan C. Co-existence of focal and bi-lateral diffuse paroxysmal discharges in epileptics. Epilepsia1969;10:453–472
85. Lombroso CT. Consistent EEG focalities detected in sub-jects with primary generalized epilepsies monitored for twodecades. Epilepsia 1997;38:797–812
86. Jeavons PM, Bower BD. Infantile spasms. In: Vinken PJ,Bruyn GW, eds. Handbook of Clinical Neurology. Vol. 15,The Epilepsies. New York: American Elsevier; 1974:219–234
87. Markand ON, Garg BP, Brandt IK. Nonketotic hyper-glycenemia: electroencephalographic and evoked potentialabnormalities. Neurology 1982;32:151–156
88. Fariello RG, Chun RW, Doro JM, Buncic JR, Pritchard JS.EEG recognition of Aicardi’s syndrome. Arch Neurol 1977;34:563–566
89. Blume WT, David RB, Gomez MR. Generalized sharp andslow wave complexes: associated clinical features and long-term follow-up. Brain 1973;96:289–306
90. Markand ON. Slow spike wave activity in EEG and associ-ated clinical features: often called “Lennox” or “Lennox-Gastaut” syndrome. Neurology 1977;27:746–757
91. Noriega-Sanchez A, Markand ON. Clinical and electroen-cephalographic correlation of independent multifocal spikedischarges. Neurology 1976;26:667–672
92. Blume WT. Clinical and electrographic correlates of themultiple independent spike foci pattern in children. AnnNeurol 1978;4:541–547
93. Brenner RP, Atkinson R. Generalized paroxysmal fast activ-ity: electroencephalographic and clinical features. Ann Neu-rol 1981;11:386–390
94. Gabor AJ, Seyal M. Effect of sleep on the electrographicmanifestations of epilepsy. J Clin Neurophysiol 1986;3:23–38
95. Williamson PD, Spencer DD, Spencer SS, Novelly RA,Mattson RH. Complex partial seizures of frontal lobe ori-gin. Ann Neurol 1985;18:497–504
96. Morris HH, Dinner DD, Lüders H. Supplementary motorseizures: clinical and electrographic findings. Neurology1988;38:1075–1082
97. Blom S, Heijbel J. Benign epilepsy of children with centro-temporal EEG foci: discharge rates during sleep. Epilepsia1975;16:133–140
98. Gregory DL, Wong PK. Topographical analysis of the cen-tro-temporal discharges in benign Rolandic epilepsy ofchildhood. Epilepsia 1984;25:705–711
99. Lerman P, Kivity S. Benign focal epilepsy of childhood: afollow-up study of 100 recovered patients. Arch Neurol1975; 32:261–264
100. Pedley TA, Tharp BR, Herman K. Clinical and electroen-cephalographic characteristics of midline parasagittal foci.Ann Neurol 1981;9:142–149
101. Pourmand RA, Markand ON, Thomas C. Midline spikedischarges: clinical and EEG correlations. Clin Electroen-cephalogr 1984;15:232–237
102. Fischer RA, Clancy RR. Midline foci of epileptiform activ-ity in children and neonates. J Child Neurol 1987;2:224–228
103. Klass DW, Westmoreland BF. Nonepileptogenic epilepti-form electroencephalographic activity. Ann Neurol 1985;18:627–635
104. White JC, Langston JW, Pedley TA. Benign epileptiformtransients of sleep: clarification of the “small sharp spike”controversy. Neurology 1977;27:1061–1068
105. Thomas JE, Klass DW. Six-per-second spike and wave pat-tern in the electroencephalogram. Neurology 1968;18:587–593
106. Hughes JR. Two forms of the 6/sec spike and wave com-plex. Electroencephalogr Clin Neurophysiol 1980;48:535–550
107. Lipman IL, Hughes JR. Rhythmic midtemporal discharges:an electroclinical study. Electroencephalogr Clin Neuro-physiol 1969;27:43–47
108. Reiher J, Lebel M. Wicket spikes: clinical correlates of apreviously undescribed EEG pattern. Can J Neurol Sci1977;4:39–47
109. Westmoreland BF, Klass DW. A distinctive rhythmic EEGdischarge of adults. Electroencephalogr Clin Neurophysiol1981;51:186–191
110. Westmoreland BF, Klass DW. Unusual variants of sub-clinical rhythmic electrographic discharge of adults(SREDA). Electroencephalogr Clin Neurophysiol 1997;102:1–4
111. Lombroso CT. Neonatal polygraphy in full-term and pre-mature infants: a review of normal and abnormal findings. JClin Neurophysiol 1985;2:105–155
112. Aso K, Scher MS, Barmada MA. Neonatal electroen-cephalography and neuropathology. J Clin Neurophysiol1989;6:103–123
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.
46 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003
113. Ellingson RJ, Peters JP. Development of EEG and daytimesleep patterns in normal full-term infants during the firstthree months of life: longitudinal observations. Electroen-cephalogr Clin Neurophysiol 1980;49:112–124
114. Cukier F, Andre M, Monod N, Dreyfus-Brisac C. Apportde I’EEG au diagnostic des hemorragies intra-ventriculairesdu premature. Rev Electroencephalogr Neurophysiol 1972;2:318–322
115. Clancy R, Tharp B. Positive Rolandic sharp waves in theelectroencephalograms of premature neonates with intra-ventricular hemorrhage. Electroencephalogr Clin Neuro-physiol 1984;57:395–404
116. Marret S, Parain D, Samson-Dollfus D. Positive Rolandicsharp waves and periventricular leukomalacia in the new-born. Neuropediatrics 1986;17:199–202
117. Novotny EJ, Tharp BR, Coen RW, Bejar R, Enzmann D,Vaucher YE. Positive Rolandic sharp waves in the EEG ofthe premature infant. Neurology 1987;37:1481–1486
118. Monod N, Pajot N, Guidasci S. The neonatal EEG: statisti-cal studies and prognostic value in full-term and pre-termbabies. Electroencephalogr Clin Neurophysiol 1972;32:529–544
119. Lombroso C. Quantified electrographic scales on 10 pre-term healthy newborns followed up to 40–43 weeks of con-ceptional age by serial polygraphic recordings. Electroen-cephalogr Clin Neurophysiol 1979;46:460–474
120. Tharp BR, Cukier P, Monod N. The prognostic value of theelectroencephalogram in premature infants. Electroenceph-alogr Clin Neurophysiol 1981;51:219–236
121. Hrachovy RA, Mizrahi EM, Kellaway P. Electroenceph-alography of newborn. In: Daly DD, Pedley TA, eds. Cur-rent Practice of Clinical Electrophysiology. New York:Raven Press; 1990:201–242
122. Young GB, Jordan KG, Dowig GS. An assessment of non-convulsive seizures in the intensive care unit using continu-ous EEG monitoring: an investigation of variables associ-ated with mortality. Neurology 1996;47:83–89
123. Treiman DM, Walton NY, Kendrick C. A progressive se-quence of electroencephalographic changes during general-ized convulsive status epilepticus. Epilepsy Res 1990;5:49–60
124. Brenner RP. Is it status? Epilepsia 2002;43(suppl 3):103–113
Thi
s do
cum
ent w
as d
ownl
oade
d fo
r pe
rson
al u
se o
nly.
Una
utho
rized
dis
trib
utio
n is
str
ictly
pro
hibi
ted.





























