Embed Size (px)
Citation preview

BOSTON CHICAGO DALLAS DENVER LOS ANGELES MENLO PARK MONTREAL NEW YORK SAN FRANCISCO WASHINGTON
October, 2014
Future strategies for pricing and market access in oncologyDiscussion document

PAGE 1MARKET ACCESS USA ■ OCTOBER 2014
We review the situation of pricing and market access (PMA) in oncology in 3 steps:
Agenda
1. Historical perspective
2. Recent changes / situation today
3. Future developments

PAGE 2MARKET ACCESS USA ■ OCTOBER 2014
Value seen primarily in extending survival (OS)
Focus on US market:
High value market (bulk of sales, “free” pricing and price increases)
Key role of NCCN guidelines and copayment support
Ex-US focus on EU-5:
Increasing use of patient restrictions by payers to limit budget impact/burden
NICE often key EU market access focus, however standard “by-pass” through Cancer Drug Funds
Not representative of broader EU response/opportunity
Japan often an afterthought (limited MA barriers/regulated pricing)
Little or no focus on emerging markets (e.g. pricing mostly in line with EU)
Historically, oncology PMA has been an “exception”
Oncology sales 2013 by region (% of total)
US41%
EU-524%
Japan10%
ROW25%
Source: IMS MIDAS
Total = $90.8bnin 2013

PAGE 3MARKET ACCESS USA ■ OCTOBER 2014
Gleevec
Avastin
HerceptinRevlimid
Velcade
Alimta
Zytiga
Rituxan
Afinitor
Effient
Tracleer
VentavisLetairis
Gilenya
Avonex
Rebif
Betaseron
CopaxoneNeulasta
AranespProcrit
Simponi
Remicade
Orencia
Cimzia
Victoza
$0
$500
$1,000
$1,500
$2,000
$2,500
$3,000
$3,500
$4,000
$0 $50 $100 $150 $200 $250 $300 $350
Oncology
CV
MS
Supp. Care(oncology)Immunology
Other CNS agents
Other therapeutics
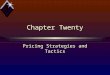
Historically, oncology PMA has been an “exception” (cont.)Sa
les
in $
mill
ions
Cost per day (in $) – Unit basis
US drug sales and price of therapies across selected therapeutic areas
• Similar picture observed for EU-5• Oncology top therapeutic area
spend (>># 2 diabetes)• Oncology over 30% of preclinical
and phase I R&D activity
Oncology products stand out in their ability to achieve “high prices” and sales
HumiraEnbrel

PAGE 4MARKET ACCESS USA ■ OCTOBER 2014
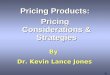
The price of oncology drugs has increased rapidly over the past 20 years, and a new launch product now typically exceeds $10,000 per month
US
pric
e pe
r mon
th (i
n 20
13 $
)
Time
US launch price per month (in 2013 dollars)
$0
$5,000
$10,000
$15,000
$20,000
$25,000
$30,000
$35,000
$40,000
$45,000
1965 1975 1985 1995 2005 2015
Yervoy ‐ BMS (ipilimumab)
Provenge ‐ Dendreon(sipuleucel‐T)
Campath ‐ Sanofi(alemtuzumab)
Arranon ‐ GSK(nelarabine)Proleukin ‐ Nestle
(aldesleukin)
Adcetris ‐ Seattle G.(brentuximab)
Cyramza ‐ Lilly(ramucirumab)
Source: Memorial Sloan Kettering (Peter Bach)

PAGE 5MARKET ACCESS USA ■ OCTOBER 2014
Oncology PMA today at a cross-road
Oncology PMA has been an
“exception”
Future
Business as usual?Historically
Oncology PMA evolves yet remains
an exception?
Transition to “standard PMA”?

PAGE 6MARKET ACCESS USA ■ OCTOBER 2014
Pricing in the US in the spotlight: We are now in the post-Zaltrap era
CEOs under pressure -- may be the target of investigations (e.g. Sovaldi)
Increasing US payer appetite for managing oncology category
Clinical pathway experimentation
Impact of oral oncology on pharmacy budgets
Generic substitution; biosimilar entry next?
New ACO channel and physician practice/provider consolidation
Oncology PMA today at a cross-road – US vs EU vs EM
EU = post-AMNOG world
Germany: from open access to highly constrained access with AMNOG
France: Introduction of economic considerations in HAS assessments
Italy: Systematic use of “risk-sharing” (only reimburse for responders)
Spain: Budgetary pressures on new oncology spend
UK: Cancer drug funding extended till March 2016
Emerging markets
Brazil: mandated coverage for oral therapies by private sector and private/government tiered-pricing
China: End of high quality = “high prices”?
Russia: DLO/regional access critical yet trends murky

PAGE 7MARKET ACCESS USA ■ OCTOBER 2014
Zaltrap demonstrated broadly KOLs’ ability to impact price and access
At Memorial Sloan-Kettering Cancer Center, we recently made a decision that should have been a no-brainer: we are not going to give a phenomenally expensive new cancer drug to our patients.The reasons are simple: The drug, Zaltrap, has proved to be no better than a similar medicine we already have for advanced colorectal cancer, while its price — at $11,063 on average for a month of treatment — is more than twice as high.In most industries something that offers no advantage over its competitors and yet sells for twice the price would never even get on the market. But that is not how things work for drugs. The Food and Drug Administration approves drugs if they are shown to be “safe and effective.” It does not consider what the relative costs might be once the new medicine is marketed.
In an unusual move, a big drug company [Sanofi] said on Thursday that it would effectively cut in half the price of a new cancer drug after a leading cancer center said it would not use the drug because it was too expensive.The move — announced by Sanofi for the colon cancer drug Zaltrap — could be a sign of resistance to the unfettered increase in the prices of cancer drugs, some of which cost more than $100,000 a year and increase survival by a few months at best.Zaltrap came to market in August at a price of about $11,000 a month. Soon after, Memorial Sloan-Kettering Cancer Center in New York decided not to use the drug, saying it was twice as expensive but no more effective than a similar medicine, Avastin from Genentech. Both drugs improved median survival by 1.4 months, doctors there said.

PAGE 8MARKET ACCESS USA ■ OCTOBER 2014
Pricing needs to be more rigorous, evidence-based
Need to manage PR/advocacy opportunity/risk proactively
Portfolio approach needed - need to be consistent from asset to asset
ASCO’s “value algorithm” - a significant PMA risk?
Key role of high impact evidence development
PMA needs to come in early - Pricing and market access considerations should be brought in the clinical decision making early in the process
Need for integrated approaches that maximize opportunities while providing a robust/step-wise factbasefor pricing decisions
Need to prioritize – e.g. key geographies / other key issues
Developing economies: A growing need for tier-pricing and other innovative approaches
Future – End of the “oncology exception”?

PAGE 9MARKET ACCESS USA ■ OCTOBER 2014
Are KOLs/clinicians the main potential barrier to access for the future?
ASCO task force on “Value in Cancer” Care is developing an algorithm scorecard to evaluate drugs’ value based on their: Cost
Efficacy
Side effects
Right now the value framework is intended for doctors to use exclusively on an individual basis with their patients
ASCO does not intend to publish rankings or any other generalizable information about the overall value of specific treatments
Could ASCO’s algorithm transform the US into France or Germany?
Timing uncertainty (i.e. 1st version may not bite but the 2nd could…)
Post-Zaltrap, there is a significant risk that payers use physicians to reduce costs (if physicians don’t do it on their own…)
We are trying to be an honest broker in helping oncologists and patients make their best-informed treatment decisions based on
effectiveness and cost—Lowell E. Schnipper, MD
Chair of ASCO’s Value in Cancer Care Taskforce and Chief of Hematology/Oncology at BIDMC in Boston

PAGE 10MARKET ACCESS USA ■ OCTOBER 2014
$1,000
$3,000$1,000
$200
$200
$200
$400
Prod
uct X
val
ue v
s. S
oC(6
-mon
th tr
eatm
ent
basi
s, k
$)
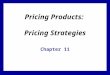
SoC Cost Product Xvalue
∆ Survival benefit
∆ burden of administration ∆ RW
survival due to longertreatment duration
∆ AE costs
∆ qualityof life
Evidence-based articulation of the value generated is likely to become key for a new therapy to achieve significant premium pricing, particularly in Europe
Key role of high impact evidence development
For such value-based pricing approaches, the “monetization” is typically based on current payments
made by payers for similar level of outcomes
Potential upside from incremental evidence

PAGE 11MARKET ACCESS USA ■ OCTOBER 2014
Conduct appropriate PMA situation analysis prior to initial clinical investments
Identify PMA-specific evidence needs
Update as clinical development progresses
Establish early PMA representation on GPT and GBT teams
Explicit consideration of market access and pricing challenges and opportunities
Clear accountability for local data initiatives
Develop common framework across portfolio
PMA needs to be brought in early in decision-making
Emerging “early PMA” best practicesCommon past PMA pitfalls
Late and/or rushed assessment of potential market access barriers/considerations Sub-optimal pricing and launch decisions
Poorly designed clinical programs that don’t address payer needs, particularly ex-US
Pursue local data initiatives (key for local advocacy)
Lack of consistency from asset to asset, and across geographies
What works for today’s asset may hurt the next company’s blockbuster

PAGE 12MARKET ACCESS USA ■ OCTOBER 2014
Need for integrated approaches that maximize opportunities while providing a robust/step-wise factbase for pricing decisions
Project Summary: Approach
Pricing needs to be rigorous
Payers1
Patients3
Quantitative Research (option for qualitative research)Estimate preference share for Product X: impact of formulary (e.g. restrictions and – for the US - copayment tiers) on physician prescribing behavior
Qualitative and Quantitative Research Impact of product benefits and price on Product X market access (e.g. restrictions and – for the US - copayment tiers) by price point and payer (type)
Quantitative Research (US only)Impact of patient out-of-pocket costs on patient preferences and requests for a lower cost alternative therapy or non-compliance
Model Integration Steps
Fully integrated share –Apply impact of price on physician-driven shares to patient share based on out-of-pocket costs estimate patient demand, therapy requests, and physician compliance. Combines and
Research and Analysis Steps
Physician-driven share – Apply market access outcome (e.g. restrictions and – for the US - copayment tiers) to estimate physician therapy preference shares based on price-access relationship. Combines and .
Fully IntegratedShare and Price5
4 Physician-Driven Share
3 4
1 2
Physicians2

PAGE 13MARKET ACCESS USA ■ OCTOBER 2014
US60%
EU-58%
Japan11%
ROW21%
The “No brainer”: Avoid the time wasters (e.g. Australia)
“More difficult yet key”: Assess launch sequencing / timing options from a PMA perspective
EU pricing barriers – Now bypassing/delaying entry in some EU-5 countries a real consideration
Challenging innovation/clinical benefit ratings and economics (Germany post-AMNOG, France, etc.)
Pricing spillovers on other countries (e.g. Japan)
Japan matters (potential bigger than EU-5?, HTA risk?)
Keep it simple!
Need flexibility as things change
Sales volume uncertainty will remain (even for big countries like Brazil, Russia and China)
Managing price differentials is challenging (exchange rate fluctuations, US price increases,…)
Need to prioritize – e.g. key geographies / other key issues
Data inputs Outputs
Market Share, Revenue, Profit
Financials
Impact of Price on Access
Calculations
Impact of Access on Utilization
0
100
200
300
400
500
600
700
800
900
1,266 2,743 4,219 5,696 7,172 8,649 10,125
Profit (per Patient)
Optimal Price
User Selected Price
0%10%20%30%40%50%60%70%80%90%
100%
1,266 2,683 4,101 5,518 6,936 8,353 9,771
13.3%
86.7%
0.0%
31.8%
68.2%
0.0%0%
20%
40%
60%
80%
100%
Specialist & GP
Specialist only Not Reimbursed
Specialist & GP
Specialist only Not Reimbursed
Distribution of Payer Access
0%
5%
10%
15%
20%
25%
30%
HeFH
Seve
re PAD
High risk C
AD
Acute AC
S
Statin intolerant
Stroke
Type
2 Diabe
tes
All Patient
Segm
ents
11.3%
9.4%
38.9%
32.5%
23.6%
19.7%
0% 20% 40% 60% 80% 100%
At Optimal Price (€6,050)
At User Selected Price (€ 4,010)
Market Share by segment
Prof it-maximizing Price
US Calculations
EU Calculations
Market share by segment
Market share by segment
Distribution of access by segment
Distribution of access by segment
Other assumptions
Scenario analysis controls
Definitions/new molecule customization
Sensitivities to Payer Access
Clinical Trial ResultsHigh Impact 30.0%Medium Impact 20.0%Market Access TrendsHigh Reduction 10.0%Small Reduction 5.0%
% Increase in Price where 0% of Patients are Reimbursed
Sensitivities to Utilization
Patient SensitivitySevere 5.0% 10.0%Clinical Trial ResultsHigh Impact 7.0% 10.0%Medium Impact 3.0% 5.0%Copay AssistanceAssistance 0.0% 0.0%SamplingHigh Sampl ing 0.0% 0.0%
Percentage Point Increase in Specialist & GP Market Share
% Decrease in Δ Market Share
between Prescriber Types
UtilizationUtilization of Less Severe Patients (Assuming Default Clinical Trial Results, Copay Assistance, and Sampling)
Special ist & GP Market Share if First Entrant (% of Patients)
50%
Special ist & GP Market Share for Order of Entry Selected in Outputs Tab (4th)
25%
Market Share (% of Patients) Specialist & GP Special ist only
Not Reimbursed at
Pmin
Not Reimbursed at
PmaxDecrease in Market Share Relative to Specialist & GP
0.0% 60.0% 95.0% 95.0%
Market Share by Prescriber Type 25.0% 10.0% 1.3% 1.3%
Distribution of Payer Access by Patient Segment (Assuming Default Clinical T
Patient Segment Specialist & GP Special ist onlyHeFH € 1,266 € 7,594Severe PAD € 1,898 € 7,594High risk CAD € 1,898 € 7,594Acute ACS € 6,328 € 5,063Statin intolerant € 5,063 € 6,328Stroke € 5,063 € 7,594Type 2 Diabetes € 3,797 € 7,594
Price where 0% of Patients are Reimbursed
Access
Data Type Patient
Minimum Price € 1,266Maximum Price € 10,125
Patient Segment
Number of LDL>100 Patients
Number of LDL>130 Patients
Sensitivity to Util ization
HeFH 986 493 SevereSevere PAD 451 173 SevereHigh risk CAD 3,400 1,700 SevereAcute ACS 1,511 570 Less SevereStatin intolerant 687 344 Less SevereStroke 1,112 438 Less SevereType 2 Diabetes 1,125 563 Less SevereAll Patient Segments 9,272 4,281
Ranges of Price s to Consider
Patient Segment Assumptions
Patient segment characteristics
DirectionsLight green boxes allow you to enter new names that will be used throughout the model.Delete extra Patient Segments if you do not want to include them in the model.
Competitive Landscape Terms Assumption Terms
Least Restrictive Tier Tier 2 Large Population LDL>100Moderately Restrictive Tier Tier 3 or Restricted Small Population (Default) LDL>130Most Restrictive Tier Not Reimbursed
Very Sensitive SevereTier 1 (Highest Tier) Specialist & GP Less Sensitive (Default) Less SevereTier 2 Specialist onlyTier 3 (Lowest Tier) Not Reimbursed
Significantly Positive Results High ImpactModerate Results Medium Impact
Segment 1 HeFH Less Significant Results Low ImpactSegment 2 Severe PADSegment 3 High risk CADSegment 4 Acute ACS Assistance AssistanceSegment 5 Statin intolerant Limited Assistance (Default) No/Limited AssistanceSegment 6 StrokeSegment 7 Type 2 DiabetesSegment 8 High Sampling High SamplingSegment 9 Low Sampling (Default) No/Limited SamplingSegment 10
High Reduction in Access High ReductionMedium Reduction in Access Small ReductionNo Change in Access (Default) None
Copay Assistance
Sampling
Market Access Trends
US Payer Access Tiers
EU Payer Access Prescriber Types
Patient Segments
Targetable Population
Patient Sensitivity to Payer Access & Utilization
Clinical Trial Results ( Impact on Access & Utilization)
PMA scenario modeling can help!
Product X expected peak net sales

PAGE 14MARKET ACCESS USA ■ OCTOBER 2014
Developing economies: A growing need for tier-pricing and other innovative approaches
Bubble size proportional to region’s category
market size
Income per capita (in USD/annum)
Prod
uct X
mar
ket s
hare
(% o
f tot
al)
In this example, high correlation between a
region’s Product X performance and income per
capita
High share performance in cities where income is highest
Low share performance in poorer regions/rural areas
Subsequent analysis helped identify new price
approaches to increase the value of Product X in India
and other developing countries
As drug budgets rise in emerging markets, so is pressure on manufacturers to enable more patients to have access to
modern medicine

PAGE 15MARKET ACCESS USA ■ OCTOBER 2014
Physician/patient advocacy require formalized processes
Critical importance of advocacy is generally recognized
Still few companies have adequate processes for it
Some accountability for performance of advocacy support required
Develop local data early on [for key geographies]
Key enabler for advocacy and innovative pricing
Can help reduce evidence hurdle (e.g. achieve access with Phase II data)
Innovative pricing approaches (MEAs, risk-sharing, etc.)
Win-wins and PR deals?
Italy risk-sharing model spillover to other countries?
Need to ensure outcomes are maximized for payers
The rising importance of effective collaborations with a broader set of stakeholders
500
600
700
800
900
1,000
1,100
1,200
1,300
1,400
1,500
0.0% 7.5% 15.0% 22.5% 30.0% 37.5% 45.0% 52.5% 60.0% 67.5% 75.0%
Net Costs ($m)
Annual Rate of Relapse
Payer Perspective
Without Contract
With ContractBase Value
12.2%
n/aBreakeven value:
Base value:
100
110
120
130
140
150
160
170
180
190
200
0.0% 7.5% 15.0% 22.5% 30.0% 37.5% 45.0% 52.5% 60.0% 67.5% 75.0%
Net Sales ($m)
Annual Rate of Relapse
Manufacturer Perspective
Without ContractWith ContractBase ValueBreakeven Value
12.2%
29.6%Breakeven value:
Base value:
Assessing and Evaluating Options both from your and payers’ perspective
KOL advocacy can greatly facilitate achieving access with payers, particularly ex-US

PAGE 16MARKET ACCESS USA ■ OCTOBER 2014
In conclusion:
Move early
Early PMA involvement, KOL/local data advocacy development
Be bold
“High stakes” in PMA in oncology as in other high value-based pricing
Think local
Delegate / develop effective early collaborations with key geographies (provide tools and processes to support these collaborations)
Monitor access and key initiatives (e.g. local data generation)
Keep it simple
You can’t do everything
Learn from other therapeutic areas!
Oncology has traditionally been insular…However, no need to reinvent the wheel or revisiting errors from other TAs…
If you don’t, stakeholders (e.g. payers) may do it at your expense…

PAGE 17MARKET ACCESS USA ■ OCTOBER 2014
THANK YOU!
Christian FroisVice-PresidentAnalysis Group, Inc.Boston, MA USATel: 617 425 8304Email: [email protected]