Embed Size (px)
Citation preview

Daniele SantiniUniversity Campus Bio-Medico
Rome, Italy

Anti EGFR therapy and colorectal cancer
Adapted from Ciardiello F. and Tortora G. NEJM 2008;358:1160-74
Cetuximab or Panitumumab

Responders (15-20%) Non-Responders
Who will benefit from treatment with antibodies targeting EGFR in mCRCs ?
Bardelli and Siena, J Clin Oncol 2010

Targeted therapies: primary resistance

PTEN
SOS
K-Ras
B-Raf
MEK
MAPK
EGFR
ShcGrb2
S6K
AKT
PDK
PI3K
GSK
DUSPs
Genetic alterations of the EGFR signalling pathway predict response to cetuximab
Sartore-Bianchi A et al., Cancer Res 2009
Siena,Di Nicolantonio and Bardelli JNCI 2009
Benvenuti et al., Cancer Research. 2007
Di Nicolantonio et al., J Clin Oncol. 2008
Moroni et al., Lancet Oncology 2005
Bardelli and Siena J Clin Oncol 2010
De Roock, Martini et al Lancet Oncology 2010
Di Nicolantonio, Arena et al., JCI 2011
De Roock, Di Nicolantonio et al, JAMA 2011
Bertotti et al., Cancer Discovery 2011
HER2
Prahallad et al., Nature 2012
Misale et al., Nature 2012
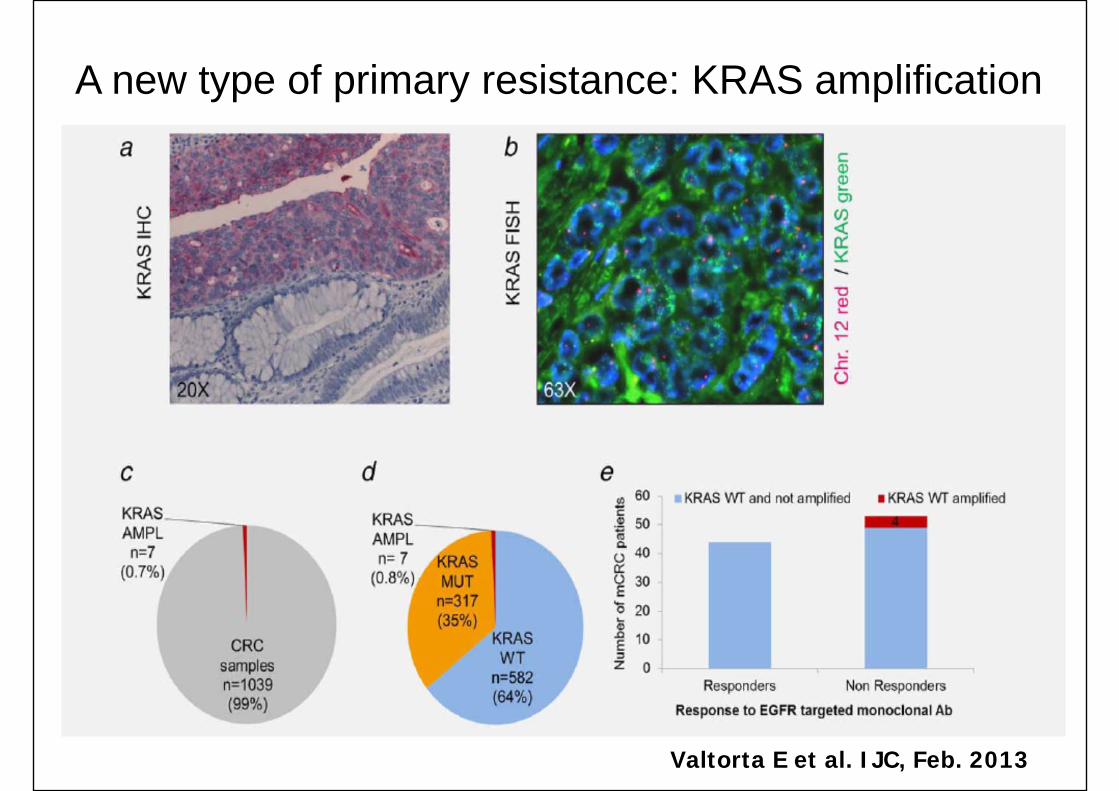
A new type of primary resistance: KRAS amplification
Valtorta E et al. IJC, Feb. 2013

Targeted therapies: primary resistance
Three small “Caveat”

KRAS p.G13D Mutation and OS With Cetuximab in mCRC
De Roock W, et al. JAMA. 2010;304:1812-1820.
Per
cent
age
Aliv
e
100806040200
Months Since Randomizationor Start of Cetuximab
0 5 10 15 20 25
p.G13D Mutation
Any cetuximab therapyNo cetuximab therapy*Log-rank P < .001
Months Since Randomizationor Start of Cetuximab
Other KRAS Mutation
Log-rank P = .49
0 5 10 15 20 25Months Since Randomization
or Start of Cetuximab
KRAS WT
Log-rank P < .001
0 5 10 15 20 25
Per
cent
age
Aliv
e
100806040200
Months Since Randomizationor Start of Cetuximab
0 2 4 6
Cetuximab monotherapyNo cetuximab therapy
Log-rank P = .02
Months Since Randomizationor Start of Cetuximab
0 2 4 10 12 14
Log-rank P > .99
Months Since Randomizationor Start of Cetuximab
0
Log-rank P < .001
6 8 2 4 10 12 146 8
*The no-cetuximab group for all patients from the pooled data set is the best supportive care group from the CO.17 trial. Horizontal axis in blue indicates range of time since randomization from 0 though 6 mos.

CRYSTAL: OS by BRAF Mutation Status
• “There was no evidence of an independent treatment by tumor BRAF mutation status interaction. Thus, with the current data set, BRAF mutation status cannot be shown to be predictive of treatment effects of cetuximab plus FOLFIRI.”
Van Cutsem E, et al. J Clin Oncol. 2011;29:2011-2019.
Ove
rall
Sur
viva
l (pr
opor
tion)
1.0
0.8
0.6
0.4
0.2
00 6 12 18 24 30 36 42 48 54 60
Time (months)
FOLFIRI BRAF MT (n = 33)Cetuximab + FOLFIRIBRAF MT (n = 26)FOLFIRI BRAF WT (n = 289)Cetuximab + FOLFIRIBRAF WT (n = 277)
Events33
22229
207
Median(months)
10.3
14.121.6
25.1
95% CI8.4 to 14.9
8.5 to 18.520.0 to 24.9
22.5 to 28.7

Cetuximab e Pyrosequencing
Direct sequencing analysis and Real-time PCR are commonly used. The detection limit of these two methods is around 20% of the mutation rate
Pyrosequencing has recently emerged as a new powerful sequencing methodology for SNP/mutation analysis. The detection limit is less than 20% of the analysed sample.
Risk to overscore KRAS mutated patients?
• Formalin-fixed paraffin-embedded tumor samples from 29 patients with primary CRC k-ras wild type for codon 12/13 were identified. Other main selection criteria were: tumour tissue availability, clinical response (partial or complete response) following cetuximab + irinotecan after progression on prior irinotecan-based therapy
• Of 29 patients, 3 (10.3%) were identify as K-ras mutant in codon 12 G for 12D mutation by pyrosequencing whereas all of them were reconfirmed k-ras wild type by Real time-PCR.
• These observations would advice oncologists in considering critically pyrosequencing as routine diagnostic test to mandatory discriminate patients eligible to receive anti-egfr therapy in clinical practice.
Santini D et al. J Clin Oncol, 2011

Responder (15%)
PIK3CA mutated and/or PTEN loss (15-20%)
BRAF mutated (8%)
KRAS/PIK3CA mutated
BRAF/PIK3CA mutatedKRAS-NRAS mutated (35-45%)
20-25% ? (quadruple negative)
Martini et al., Nat Rev Clin Oncology, 2011

Targeted therapies: secondary resistance

Responders (15-20%)
Non-Responders
Secondary resistance to EGFR targeted therapies

Responders (15-20%)
Non-Responders
Secondary resistance to EGFRtargeted therapies
6-12 months later

Emergence of KRAS mutations and acquired resistance to anti EGFR therapy in colorectal cancer
R1
R2
+ cetuximab
DiFi: 350 nM
Lim1215: 1400 nM
+ cetuximab
DiFi: 3.5 nM
Lim1215: 350 nM
+ cetuximab
DiFi: 35 nM
Lim1215: 700 nM
+ cetuximab
DiFi: 350 nM
Lim1215: 1400 nM
+ cetuximab
DiFi: 350 nM
Lim1215: 1400 nM
+ cetuximab
DiFi: 350 nM
Lim1215: 1400 nM
R1: Constant dosage
R2: Incremental dosage
Sandra Misale, Sebastijan Hobor
Misale et al., Nature 2012

DiFi DiFi R
EGFR
KRAS
DiFi
DiFi R
Misale et al., Nature 2012
De novo acquisition of KRAS mutations during cetuximab treatment

DiFi DiFi R2
KRAS Mutations Lim Lim R1 Lim R2
G12R 0% 20% 0%
G13D 0.22% 0% 47%
Marcello Gambacorta & Salvatore Siena
De novo acquisition of KRAS mutations during cetuximab treatment

How about patients ?

KRAS mutations and acquired resistance to anti EGFR targeted therapies in CRC patients
With David Solit MSKCC
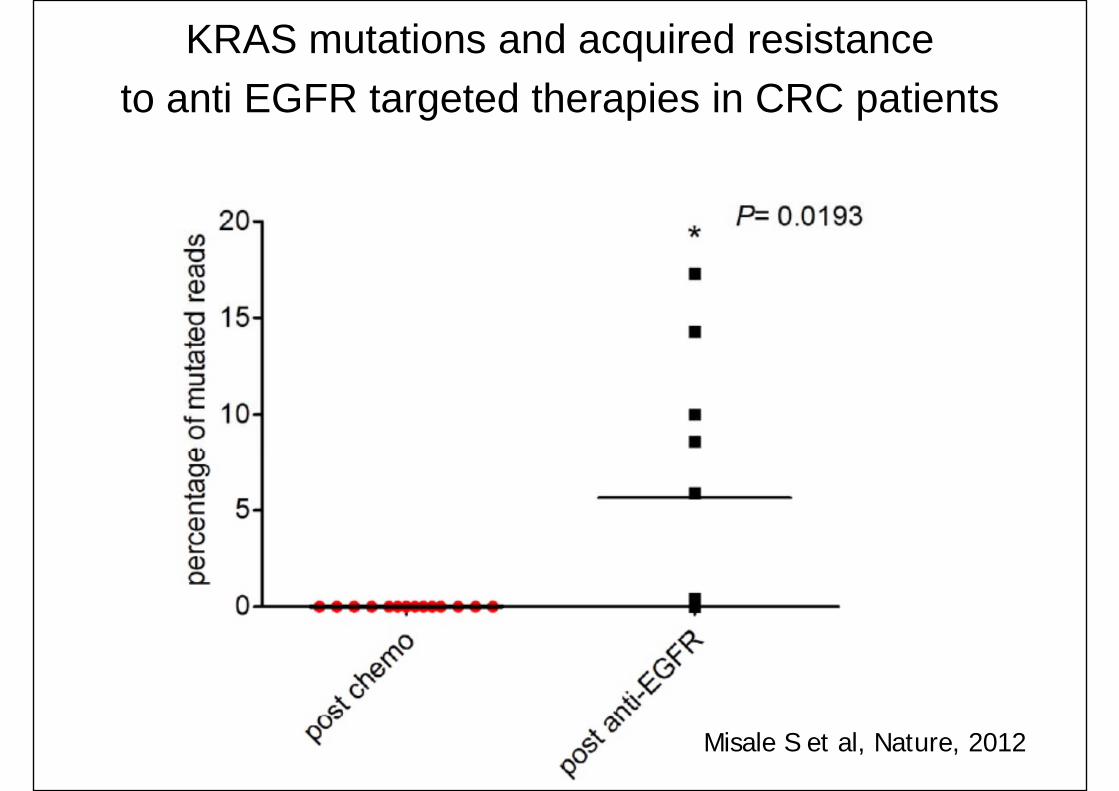
KRAS mutations and acquired resistance to anti EGFR targeted therapies in CRC patients
Misale S et al, Nature, 2012

# Total Patients
# Patients who develop KRAS mutations/amplification at resistance %
Misale et al., 2012 11 7 63.6%
Diaz et al., 2012 28 13 46%
KRAS‐mediated acquired resistance to anti‐EGFR therapy
KRAS gene alterations mediates acquired resistance to anti-EGFR therapy in CRC patients

Eduardo Vilar & Josep Tabernero
Editorial; Nature 2012
How to measure acquired resistance ?The potential role of KRAS-mutant ctDNA

Diaz & Vogelstein, Nature 2012
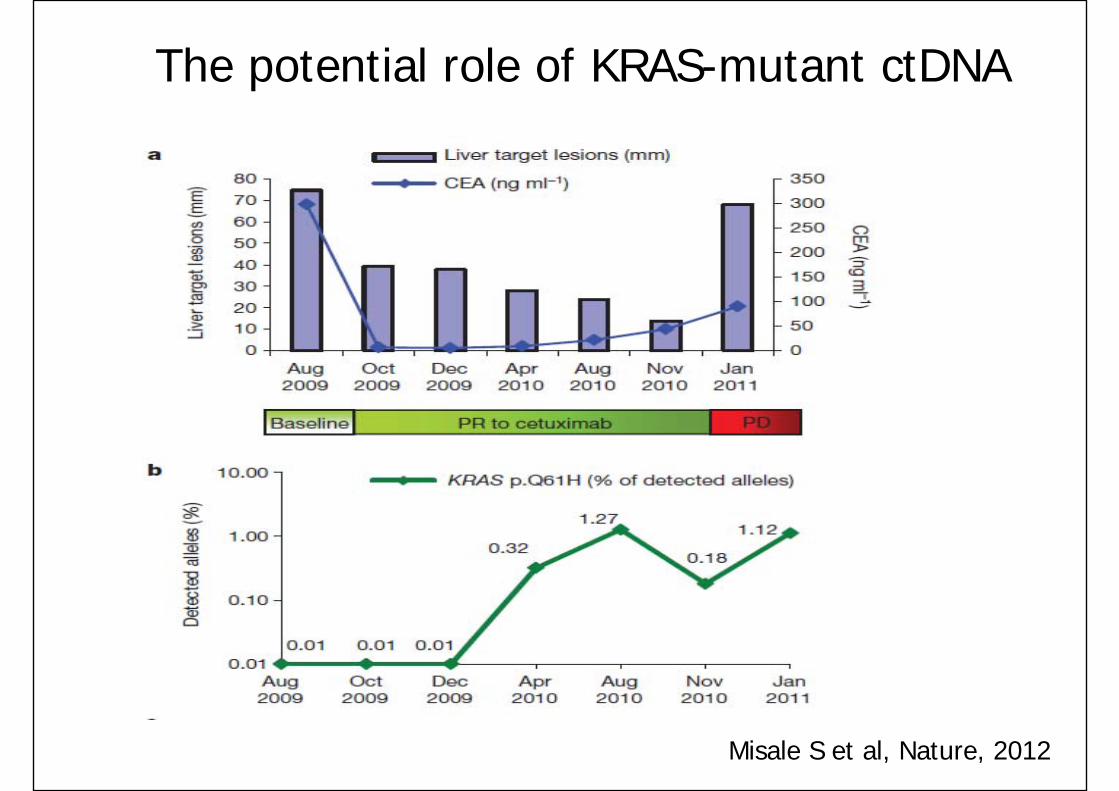
The potential role of KRAS-mutant ctDNA
Misale S et al, Nature, 2012

A new type of secondary resistance

Acquired EGFR ectodomain mutation (S492R) that prevents cetuximab binding and confers resistance to cetuximab
A subject with cetuximab resistance harboring the S492R mutation responded to treatment with panitumumab.
Montagut C, Nature Med, 2012

How to overcome secondary resistance?

Cetuximab treatment and rechallenge in irinotecan‐refractory mCRC
Erbitux* + irinotecan-based CT**
Erbitux* + irinotecan-based CT**
Treat until
PD or tox
Phase II, multicenter, prospective study Eligibility: patients with KRAS wt irinotecan-refractory mCRC
PDPDErbitux* + irinotecan-based CT**
Erbitux* + irinotecan-based CT**
SD (≥6 m) or PR/CR, then PD
SD: n=4PR: n=29CR: n=6
CT***
Median no. of therapy lines before Erbitux rechallenge: 4 (range 3–7)*Erbitux: Loading dose 400 mg/m2 followed by weekly infusions of 250 mg/m2
**Irinotecan-based CT: irinotecan monotherapy or FOLFIRI; during Erbitux treatment irinotecan was administered at 180 mg/m2 as a 90-minute infusion ***CT: 5-Fluorouracil- or oxaliplatin- or irinotecan-based CT +/− bevacizumab
PDPD
Santini D, et al. Ann Oncol 2012;Mar 5 [Epub ahead of print]
Irinotecan-based CT**
n=39 n=39
Median interval between first Erbitux treatment and rechallenge: 6 months (range 2–12 months)

Tumor response after Erbitux treatment and rechallenge: Outcomes
Clinical outcomes after Erbitux treatment and rechallenge (n=39)% Patients (95% CI)
ORR 53.8 (39.1–63.7)PR 48.7CR 5.1SD 35.9 (24.7–51.6)
DCR 89.8PD 10.2
• Median PFS after first Erbitux therapy: 10 months (range 3–30 months)
• Median PFS after Erbitux rechallenge: 6.6 months (95% CI: 4.1–9.1)
Santini D, et al. Ann Oncol 2012;Mar 5 [Epub ahead of print]
Median interval between first Erbitux treatment and rechallenge: 6 months (range 2–12 months)

Erbitux treatment and rechallenge: Potential benefit for some patients
Clinical response after first and second Erbitux‐based therapy (n=39)Best response:First Erbitux
Best response:Erbitux
rechallenge
No. of patients Total no. of patients (%)
PRCR
12 (5)
CR 1SD
PR1
19 (49)PR 14CR 4SD
SD3
14 (36)PR 10CR 1PR PD 4 4 (10)
Santini D, et al. Ann Oncol 2012;Mar 5 [Epub ahead of print]

Santini D, et al. Ann Oncol 2012;Mar 5 [Epub ahead of print]
Erbitux-resistant cloneErbitux-sensitive clone
1st line CT + Erbitux
2nd line CT - Erbitux
3rd line CT + Erbitux
PD PD
KRAS and cetuximab-driven selection in CRC cells

Tumor response after cetuximab treatment and panitumumab rechallenge: the PANERB STUDY
Porneuf m. et al, ESMO, 2012
Among the patients who had an OR with cetuximab, 31% also had an OR with panitumumab and 16% were stabilized with panitumumab (clinical benefit 47%).
In case of cetuximab resistance, only 14% of the patients had a clinical benefit with panitumumab.
The median OS for the patients who achieved a response with both targeted therapies was 25.4 months IC 95% [22.4-42.6] vs 15.0 months IC 95% [12.9-18.3] for the patients who did not (p < 0.0001).

The “Rechallenge” TrialPhase II, multicenter, prospective, proof of concept study Eligibility: patients with KRAS wt mCRC
• Primary objective: to evaluate the activity in terms of response rate according to RECIST 1.1• Secondary objectives: Progression-free survival; Disease control rate; Safety profile;Traslational studies (KRAS mutated ctDNA, tissue samples at different time points)
*CT: 5-Fluorouracil- and oxaliplatin or CPT-11- CT +/− bevacizumab (window therapy)
Cetuximab based CT
(oxaliplatin or CPT-11 or both)
Cetuximab based CT
(oxaliplatin or CPT-11 or both)
Treat until
PD or tox
PDPD cetuximab + CPT-11
cetuximab + CPT-11
SD (≥6 m) or PR/CR, then PD
WindowCT *PDPD
PDPD Study exit
Inclusion in the study
1 line 2 line rechallenge

Cetuximab beyond progressionThe “CAPRI” Trial
• Primary objectives: • Of 1st line treatment: PFS time when treated with Erbitux + FOLFIRI• Of 2nd line treatment: PFS when treated with Erbitux + FOLFOX after progression of
1st line treatment with Erbitux + FOLFIRI• Screen ~600 for KRAS, enroll at least 320 for 1st line, randomize 240 to 2nd line
• Enrollment for 1st line completed in July 2012; 80 patients in 2nd line.
Erbitux + FOLFIRIErbitux + FOLFIRI
Treat until PD or tox
Treat until PD or tox
2nd line1st line mFOLFOX4 +
ErbituxmFOLFOX4 +
Erbitux
mFOLFOX
Treat until PD or tox
Treat until PD or tox
Phase II, multicenterEligibility: Patients with KRAS wt mCRC

Which are the “best” patients for rechallenge?

Only clinical predictive factors
• KRAS wild‐type and…• First‐line cetuximab‐containing therapy achieving response or stable disease ≥6 months and ….
• Progression after a second “window” therapy line

Thank you very much for your attention





























